 Sandra Bohórquez-Blanco1,2
Sandra Bohórquez-Blanco1,2 Regina Allande-Cussó3Cristina Martín-López4
Regina Allande-Cussó3Cristina Martín-López4 Juan Gómez-Salgado5,6*
Juan Gómez-Salgado5,6* Juan Jesús García-Iglesias5*Javier Fagundo-Rivera7
Juan Jesús García-Iglesias5*Javier Fagundo-Rivera7 Carlos Ruiz-Frutos5,6
Carlos Ruiz-Frutos5,6- 1Physiotherapy School, Industrial University of Santander, Bucaramanga, Santander, Colombia
- 2Labour Risks Prevention Master, Faculty of Labour Sciences, University of Huelva, Huelva, Spain
- 3Department of Nursing, Nursing, Physiotherapy, and Podiatry School, University of Seville, Seville, Spain
- 4Rehabilitation Area, Riotinto Hospital, Huelva, Spain
- 5Department of Sociology, Social Work and Public Health, Faculty of Labour Sciences, University of Huelva, Huelva, Spain
- 6Safety and Health Postgraduate Programme, Universidad Espíritu Santo, Guayaquil, Ecuador
- 7Centro Universitario de Enfermería Cruz Roja, University of Seville, Seville, Spain
Background: The role of the physiotherapist is vital in the recovery of post-COVID-19 patients, but fear of contagion is a possible feeling among healthcare professionals. The objective of this study is to assess the mental health effects that COVID-19 has had on healthcare workers, including rehabilitation care, in times of pandemic.
Methods: A systematic review was conducted using the PRISMA format in the Pubmed, SCOPUS, and Web of Science databases between July and September 2022. Keywords included were “healthcare providers,” “COVID-19,” “Mental Health,” and “Psychological Distress.” Methodological quality was assessed using the Joanna Briggs Institute critical appraisal tools.
Results: A total of 14 studies were included in this review. The study population was healthcare professionals including the rehabilitation services. In total, 4 studies reported exclusively on anxiety and stress levels in physiotherapists providing care during the pandemic.
Conclusions: The mental health of healthcare professionals has been compromised during the pandemic. However, initially, research was only focused on physicians and nurses, so the need arises to include those professionals, such as physiotherapists, who are also in direct contact with COVID-19 patients.
Systematic review registration: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=367664, identifier: CRD42022367664.
Background
COVID-19 is a disease caused by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) (1), so defined because of its similarities to the 2003 SARS-CoV virus, with which it shares RNA characteristics but can cause both mild and severe respiratory infections. As the pandemic has progressed, the World Health Organization (WHO) has been regularly updating the classifications of SARS-CoV-2 by considering its phenotypic characteristics, degree of complexity, mode of manifestation, and geographical distribution (1). According to WHO, those most at risk of severe SARS are people over 60 years of age and those with comorbidities or pre-existing diseases, such as people with diabetes, obesity, cancer, or hypertension, among others. However, any person, regardless of age or health status, can develop complications, as can be seen by the high mortality rates, with a total of 6,547,162 deaths and 618,144,676 diagnosed cases worldwide as of October 2022, according to the Johns Hopkins Coronavirus Resource Center (2). The impact on the health system is massive as well as on Physical Rehabilitation Medicine services throughout the countries (3).
For COVID-19 to be declared a pandemic in March 2020, it had to show alarming levels of spread and severity affecting a large number of people, as well as outbreaks in more than one continent. Some of the consequences of SARS-CoV-2 implied limitations in participation and restrictions in access to different care spaces and services. Many of the diagnosed patients and others with different pathologies began to receive care through online appointments, leaving face-to-face consultations for more serious cases in order to combat the onslaught of the disease and its spread (4, 5). In addition, borders and some facilities were closed to help mitigating the psychological, environmental, and economic effects of COVID-19 (6, 7).
COVID-19 also has a serious impact on people's mental health (8). Psychological stress, including depression and anxiety, has been reported by healthcare workers with high frequency during the time of the pandemic (8, 9). Several factors increase the risk of mental health issues, including exposure to social, economic, geopolitical, and environmental circumstances. Mental health risks and protective factors are found in society at different scales, although, the most vulnerable people have taken the greatest impact (10). Global threats increase the risk of mental illness, including disease outbreaks, humanitarian emergencies, and forced displacement, among others (8, 11). But there are more vulnerable groups of professionals which had been affected by this pandemic, in example, those who worked in nursing homes, where access to protection measures was scarce and consequences went lethal both for professionals and residents (3). The pandemic has left great changes in its waves, with an impact on the mental health of people. Therefore, it is important to design and adopt protection strategies for the mental health of health professionals, as well as the early diagnosis of possible mental health problems (10).
The Job Demands-Resources (JD-R) model, in contrast to the theories of job design and job stress, highlights the role of job stressors, being used to predict burnout, engagement, and additionally, to identify the consequences of sickness absenteeism and job performance. With the JD-R model, it is possible to explain, understand, and predict employees' wellbeing. According to the theory, work environments can be divided into job demands and job resources, and this can be applied to all occupations. However, there are job demands and job resources specifically relevant to each occupation or profession (11). Job demands refer to those physical, psychological, organizational, or social aspects (e.g., work pressure, emotional demands, burnout) of work that require sustained effort, while job resources refer to those variants that can reduce the demands of work (e.g., social support, autonomy, development opportunities, organizational climate, commitment, etc.). In this sense, job resources are necessary to cope with job demands. Therefore, the interventions to be undertaken at the company level are both personal and organizational, applied in the redesign of the job, the job position, and/or by providing training resources that meet the objective of the intervention (11, 12).
According to a systematic review, some of the risk factors most associated with psychological distress during the COVID-19 pandemic were being female, from lower socioeconomic status (lower income, lower level of education, and unemployment), belonging to rural areas, and those at higher risk of COVID-19 infection (healthcare professionals, older people, or people with comorbidities). These population groups showed a higher prevalence of suffering episodes of depression and anxiety compared to other groups (12). In fact, during the first months of the pandemic, between 70 and 90% of health workers who were exposed to high risks, triggered various health problems, including stress, anguish, anxiety, fear, irritability, among others. This led to potentiate negative effects on the mental health of health workers, including the development of post-traumatic stress as part of a long-term problem resulting from this pressure (13, 14).
There is the fact that research during this time of pandemic has yielded significant outcomes in different areas, being one of them healthcare professionals. However, it is understood that “those in the front line” are only physicians and nurses (13), leaving aside other key occupations in the recovery process of patients. For this reason, generating knowledge and evidence from other healthcare professions such as rehabilitation professionals is crucial to understand the effects of the pandemic (1).
Healthcare professionals play a major role in the care and contact with people with COVID-19, many of them being part of the first line of defense against the virus (13). They may also be afraid of infecting their family and friends, suffering from social discrimination, and experiencing increased work stress due to the high demand of patients in care, even leading to, in some cases, a decrease in the quality of care (15, 16). For all these reasons, the healthcare personnel may experience emotional disorders (anxiety, fear, depression), sleep problems, and even post-traumatic stress in those who have participated in previous outbreaks. Therefore, the physical and mental wellbeing of healthcare staff is compromised, and its preservation may be essential to combat the effects that COVID-19 leaves in its wake (16).
Due to the impact of the pandemic on all health services, a restructuring of rehabilitation services was initiated as Physical Therapy areas were transformed into temporary hospitalization rooms. In fact, the Spanish Society of Physical Medicine and Rehabilitation (17), published in 2020 recommendations in relation to health care and home restrictions, considering the consequences of the pandemic on population's health and leading health professionals (including rehabilitation services) to take on new challenges in patient care, appropriate treatment, and protocols to prevent the spread of the virus (3). That was a primary concern that required all rehabilitation professionals to participate in a comprehensive assessment in search of optimal care measures with focus on the patient's recovery, but also in controlling the spread of COVID-19. With this publication, it was reassured the necessity of knowing about the psychological impact of the pandemic on rehabilitation professionals, including, as part of future research, relating or reviewing differences with respect to other similar pandemics (e.g., SARS-CoV-1 and MERS) (14).
The aim of this study was to assess the effects that COVID-19 has on the mental health, i.e., the psychological distress, of healthcare workers of the rehabilitation services when caring for patients in times of pandemic.
Methods
Study design
A systematic review was conducted following the guidelines of the PRISMA statement (18) (Preferred Reporting Items for Systematic reviews and Meta-Analyses). For this purpose, the authors used a protocol to carry out this systematic review, which was registered in the International Prospective Register for Systematic Reviews (CRD42022367664).
Databases and search strategy
The search was carried out in the following electronic databases: Pubmed, SCOPUS, and Web of Science. It was based on the key words provided by the research question that followed the PICOT strategy (Table 1). Gray literature resources were not assessed.
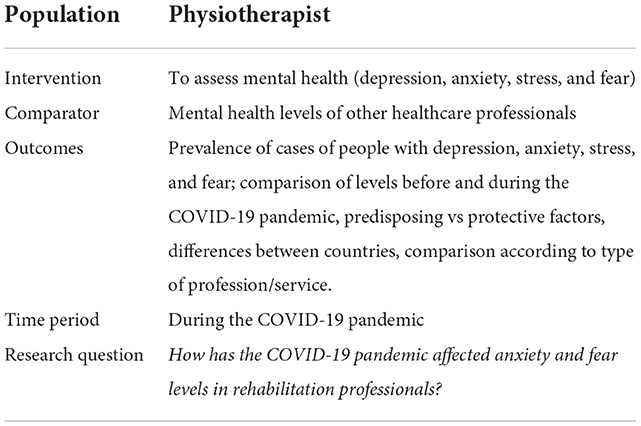
Table 1. PICO format: keywords (rehabilitation and COVID-19, Spain, 2022).
Following these keywords, the Medical Subject Headings (MeSH) thesaurus was consulted, yielding the descriptors health personnel and physiotherapists, mental health, physiological stress, anxiety, depression, and COVID-19. In order to enlarge the scope of the search, synonymous terms were used to complete the search based on the Medical Subject Headings (MeSH) descriptors (Table 2), linked by the Boolean operators AND and OR.
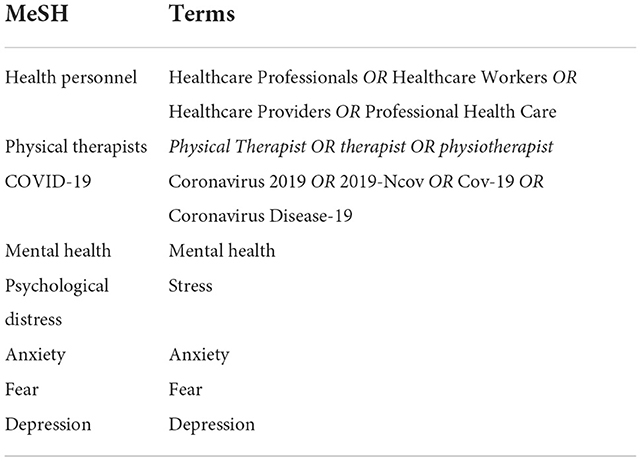
Table 2. Terms used in the search (Rehabilitation and COVID-19, Spain, 2022).
Table 3 shows the search strategy used on 27 July 2022 for each of the above databases during the search process.
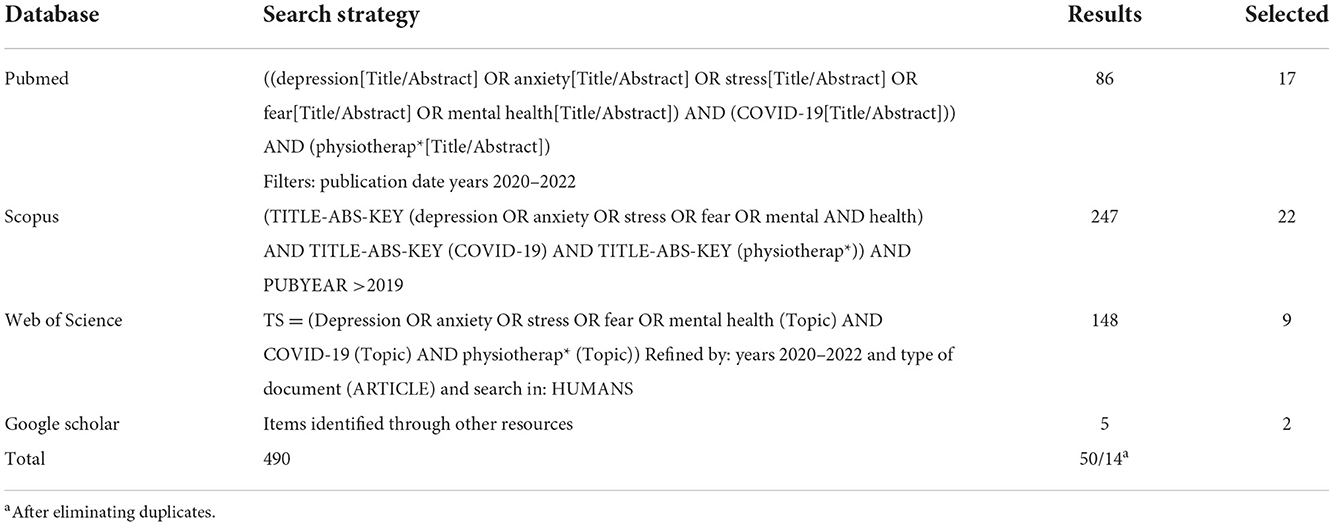
Table 3. Search strategy used by database (rehabilitation and COVID-19, Spain, 2022).
Selection criteria
Original articles, including meta-analyses, systematic reviews, cohorts, cross-sectional, and case-control studies published in English and Spanish were included in this review.
The following criteria were used for the selection of articles:
Inclusion criteria
• Original articles published in English and Spanish.
• Articles published from 2020 to date.
• Type: original articles, meta-analysis, case reports.
• Articles measuring any of the following values and/or effects: level of depression, level of stress and level of anxiety, number of cases of professionals with depression, stress and/or anxiety, comparison of levels before vs. during the COVID-19 pandemic, and comparison according to country or type of profession/service.
Exclusion criteria
• Studies that did not meet the previously established inclusion criteria, that did not answer the research question, or that were not related to the objective of the review.
• Studies of low scientific-technical quality after applying the quality assessment tool.
• Study population other than healthcare professionals and which did not include rehabilitation professionals.
• Typology: opinion articles, commentaries, editorials and letters to the editor/head, and quasi-experimental.
Data collection and extraction
Initially, two researchers independently carried out the searches, as set out in the search strategy for each of the chosen databases. Subsequently, one researcher eliminated duplicate articles and those that did not meet the previous criteria, and finally included studies accordingly, after reading the titles and abstracts. Subsequently, one author reviewed the full text of the potential studies for the review and made the decision to include or exclude them. Discrepancies were resolved by the first two authors.
Assessment of methodological quality
The methodological quality of the selected studies was determined using the critical appraisal tools of the Joanna Briggs Institute (JBI) of the University of Adelaide (19). The purpose of this tool is to assess the methodological quality of a study and to determine the extent to which a study has excluded or minimized the possibility of bias in its design, conduct, and/or analysis. The versions for quantitative cross-sectional studies (19) (8 items), the JBI checklist for analytical cohort studies (20) (11 items), and for qualitative studies (21) (10 items) were used, setting the cut-off point at 6 for acceptance for inclusion in this review (see Supplementary Tables S1–S3 in Supplementary material).
Table 4 shows the characteristics of each of the 14 final articles for this review, and it is based on the Iberoamerican Cochrane Centre Handbook guidelines (22). These characteristics were categorized by authors and year of publication, geographical context, objective, type of study, participants, measurement instrument(s), and main findings; in addition, the results of the JBI critical appraisal tool were added.
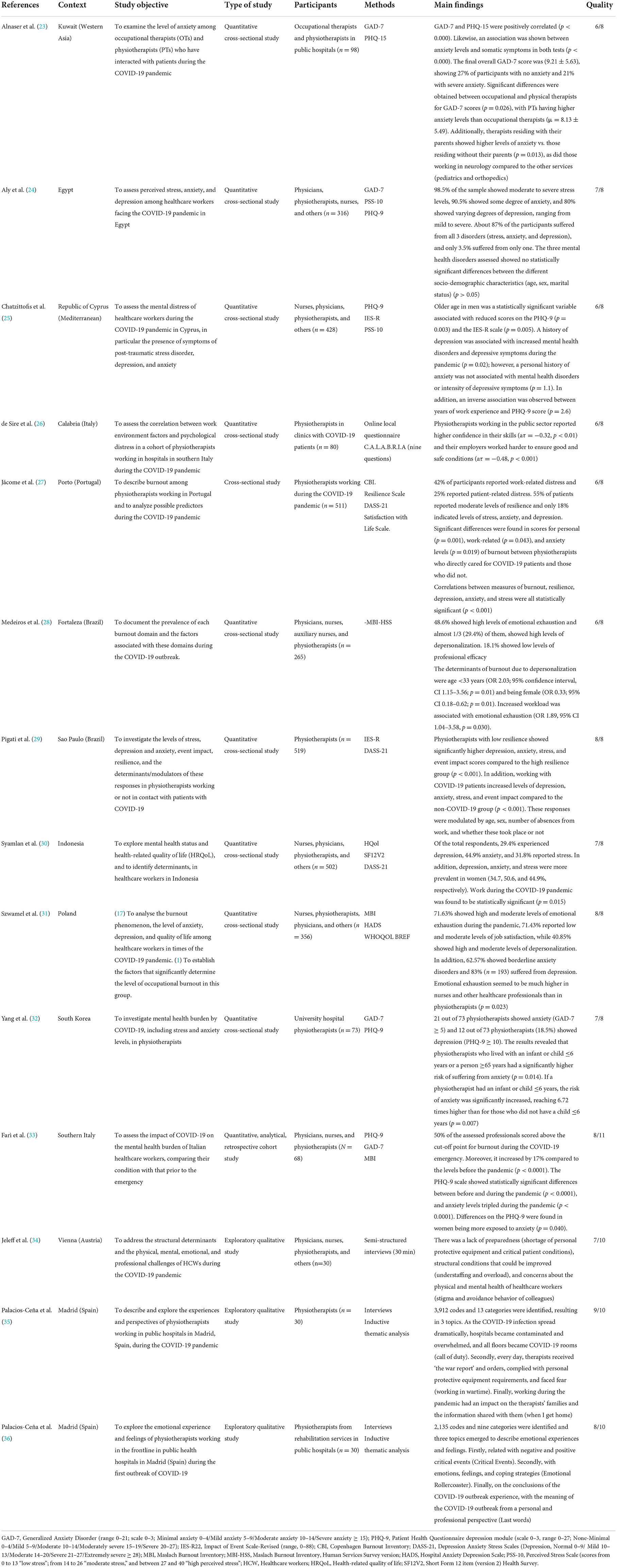
Table 4. Characteristics of the studies included in the systematic review (rehabilitation and COVID-19, Spain, 2022).
Results
The initial search strategies identified a total of 490 references, which were screened according to the topic of this review. A total of 14 articles were finally selected (Figure 1), 11 of which were quantitative (ten cross-sectional and one retrospective cohort) and three qualitative.
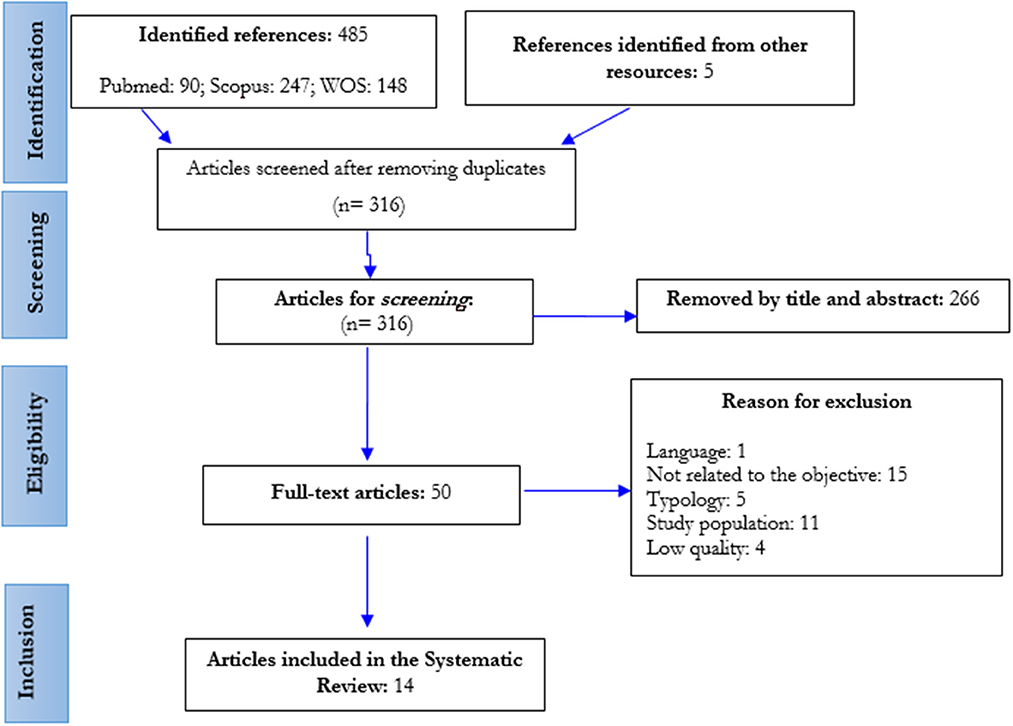
Figure 1. Flowchart of the study selection process (PRISMA) (rehabilitation and COVID-19, Spain, 2022).
There was a variety of countries identified in the studies, among them, two were conducted in Spain, two in Brazil, two in Italy, and one in other countries such as Portugal, Korea, Austria, Indonesia, and Egypt, among others. In relation to the sample, in 6 of the 14 studies included in the review, the sample was exclusively composed by physiotherapists.
The included articles were assessed with the JBI critical appraisal tool, where both quantitative and qualitative studies obtained medium-high scores.
Level of anxiety
To assess anxiety levels, the different studies used the following scales: GAD-7, DASS-21, and HADS. The Generalized Anxiety Disorder tool (GAD-7) is a self-administered screening test designed to identify probable cases and severity of anxiety. The GAD-7 is used in adults >18 years old and includes 7 items on a Likert-type scale (0 = not at all; 1 = several days; 2 = More than half the days; 3 = Nearly every day). Scoring ranges from 0 to 21, with scores of 5, 10, and 15 set as cut-off points for mild, moderate, and severe anxiety, respectively. Further assessment is recommended when the score is 10 or higher (23).
The level of anxiety can also be assessed with the DASS-21 “Anxiety subscale,” which has been one of the preferred assessing instruments during the COVID-19 pandemic (27, 30, 37, 38). This version consists of a 21-item, four-point Likert questionnaire which includes three self-report subscales designed to measure the negative emotional states of depression, anxiety, and stress (which apply to the participant from not at all to most of the time). Scores for each subscale range from 0 to 21, with higher scores indicating a more negative emotional state.
Level of depression
The Center for Epidemiologic Studies Depression Scale (CES-D), the Patient Health Questionnaire depression module (PHQ-9), the Depression Anxiety Stress Scales (DASS-21: Depression subscale), the Hamilton Depression Scale (HAMD-17), and the Self-rating Depression Scale (SDS) (39) are available to assess depressive symptoms.
The HADS is one of the scales used in the assessed studies to evaluate depression and anxiety. It had been used before with nursing staff in Poland (31, 39). It originally contained 7 items assessing anxiety and 7 items related to depressive states. After modification, 2 items for irritation and aggression were added. In total, the scale consists of 16 closed questions with 4 possible response options. Each answer can be scored between 0 and 3 points. The categories are distinguished individually for the anxiety and depression subscales (0–7: no disorders; 8–10: borderline state; 11–21: present disorder).
In addition, the level of depression was qualitatively assessed through semi-structured interviews to record and code the emotional experiences of healthcare professionals, including the rehabilitation services, in times of pandemic (34–36).
Level of stress
The Perceived Stress Scale (PSS-10) consists of 10 questions about feelings and thoughts during the last month. Responses are given for each question on a 5-point scale which ranges from “never” to “very often.” Then, the total is calculated. Scores ranging from 0 to 13 are regarded as low stress; scores from 14 to 26, moderate stress; and between 27 and 40, scores are considered high perceived stress (24, 25).
The 22-item Impact of Events Scale-Revised (IES-R) is used to assess post-traumatic stress symptoms during the past 7 days. Each item is scored from 0 to 4. The total scale score ranges from 0 to 88. Values above the cut-off point of 33 indicate a clinically relevant symptom (25, 29).
Other data
All studies included questionnaires covering socio-demographic data (age, sex, marital status, and occupation). However, some of them included questions related to the health of the participants (25, 28) and others about the way of working during the pandemic (face-to-face, telework, etc.) (27).
Regarding mental health, some studies (26–29, 34, 36) used the Patient Health Questionnaire (PHQ) to measure the level of somatisation. It is a self-administered version of the PRIME-MD (Primary Care Evaluation of Mental Disorders) diagnostic instrument for common mental disorders (24, 25, 32, 33). The PHQ-15 (23) comprises 15 somatic symptoms from the PHQ. The 15 items are scored on a 3-point Likert scale (0 = does not bother me at all; 1 = bothers me a little; and 2 = bothers me a lot). However, due to cultural sensitivities, two items (question no. 4: menstrual cramps or other problems with your periods and no. 11: pain or problems during intercourse) were removed from the questionnaire and the mPHQ-15 (modified version) with 13 somatic symptoms emerged. The mPHQ-15 total score ranged from 0 to 26 and scores of 3, 18 and 13 were set as cut-off points for mild, moderate, and severe somatisation levels, respectively. The PHQ-15 has demonstrated high reliability and validity for application in clinical and occupational health care settings (23).
The Maslach Burnout Inventory (MBI), on the other hand, assesses the level of burnout. It is composed of 22 items designed to evaluate the three dimensions of burnout: Emotional Exhaustion (nine items); Depersonalization (five items); and Personal Accomplishment (8 items). All MBI items are scored using seven-level frequency ratings, from “never” (=0) to “every day” (=6). Burnout is confirmed by obtaining high scores on the subscales that assess emotional exhaustion (0–54 items) and depersonalization (0–30 items) and low scores on the Personal Accomplishment subscale (0–48 items) (28, 31, 33). Similarly, the Copenhagen Burnout Inventory (CBI) is a scale designed to measure burnout, including 19 items in subscales (personal, work-related, and client-related). All items are scored on a five-point Likert scale (Always/To a very high degree = 100; Often/To a high degree = 75; Sometimes/Somewhat = 50; Seldom/To a low degree = 25; and Never/Almost never/To a very low degree = 0) (27).
The WHOQOL measures health-related quality of life. It was assessed using the Polish version of the abbreviated World Health Organization instrument (WHOQOL BREF). It has 4 domains: D1-Physical; D2-Psychological; D3-Social Relationships; and D4-Environmental, and consists of 26 questions. The respondents rate each aspect on five-point Likert scales. The domain score reflects an individualized perception of each quality-of-life domain, and it is scaled in a positively framed direction: the higher the score, the higher the health-related quality of life (30, 31).
Discussion
The COVID-19 pandemic has radically led to a change in lifestyle, affecting different aspects (work, family, personal, among others) (40). Newly published research studies recommend the work of the physiotherapist in the recovery of post-COVID-19 patients. However, though mental health is a determining factor in people's wellbeing and it should not be disregarded, fear of contagion is latent in healthcare professionals and leads to an increase in their levels of stress, anxiety, and fear of providing care to patients.
Regarding the qualitative assessment, three of the analyzed studies have something in common (34–36), namely that the experiences of the COVID-19 outbreak have led to emotional disturbances, which have required coping strategies, not only on a personal, but also on a family and professional level. However, one study, in contrast to the others, included in its conclusions some experiences such as “But not everything was bad. I have learned a lot” (35). A Spanish study highlighted that not being single, having a number of years of professional experience and being a man, was associated with a greater use of coping techniques that protect against stressors and threatening emotions. Young people have shown that they have suffered more from isolation from their physical, family and social environment (10). Another issue to highlight is the importance of access to and use of personal protective equipment, as part of the contagion was due to the lack of resources or their misuse (35).
One of the qualitative studies (35), two quantitative studies (23, 32), and one systematic review (40) mention that the latent fear in healthcare workers was that they might infect their family members. This fear sometimes led to self-stigmatization or avoidance behaviors (sleeping in separate beds, not sharing objects/space with family members, among others). In addition, gratitude and appreciation were important issues for most healthcare workers.
On the other hand, most of the quantitative studies, with the exception of one (33), followed a cross-sectional method for measuring and obtaining study results. Among the commonalities between studies, they all shared the assessment of anxiety and stress levels. Also, the most commonly used instruments were the PHQ-9 and GAD-7. Several studies (24, 25, 28) showed associations between anxiety levels and somatic symptoms. Aly et al. (24) indicated that the vast majority of participants suffered from mental health disorders. However, they showed no differences related to age or sex. On the contrary, Chatzittofis et al. (25) and Farì et al. (33) do show in their results significant differences by age and sex, though with opposing results, indicating in the first study that men and older subjects showed increased levels of anxiety while, in the second study, women were more exposed to increased levels of anxiety. In addition, Syamlan et al. (30) indicated that women had a higher prevalence of suffering from depression, anxiety, and stress.
Farì et al. (33) concluded that there were differences in the level of anxiety before and during the pandemic. Only the study by Medeiros et al. (28) mentioned professional efficacy during the pandemic, indicating that just 18% showed low levels of professional efficacy. However, other studies mention that rehabilitation professionals identified negative effects on the quality of services they provided as a consequence of COVID-19 (41, 42). Fear is a human response to threatening situations, and SARS-CoV-2 has become a major global threat, generating this feeling. Emotional burden, perceived risk factors, as well as lack of well-evidenced information, may be associated with the perception of fear of COVID-19 and the impact on health (14).
As for the differences found between types of healthcare professionals, only Szwamel et al. (31) showed that emotional exhaustion was higher in nurses than in the other professionals evaluated, such as physiotherapists. Del Pozo-Herce et al. (14) showed that the pandemic has left a great psychological impact on health professionals, both in terms of stress and in the use of coping strategies, and they indicated that professionals who did not have appropriate working conditions (i.e., type of contract and salary) or those with less years of experience, were more affected in mental health than others.
Strengths and limitations of study
This study allowed to examine professionals in the area of rehabilitation as an important part of health care during the pandemic. Including this population in the investigation and carrying out research to generate new interventions in mental health are the strongest parts of this research. Likewise, the assessment of rigor and methodological quality of the included studies, and their variables, permit to support solid conclusions and generalizations. Despite the results of interest provided in this research, it would be pertinent to continue deepening the subject of study.
The present study shows some limitations. Firstly, it should be noted that one article written in German was rejected, as no translation could be found, so it is possible that some articles that met the rest of the inclusion criteria were left out for this language reasons. In addition, eleven articles were rejected for not having the exact study population, i.e., only included physicians and nurses but not rehabilitation professionals, or there was not a clear statement about their inclusion in the study. The vast majority of studies was also found to not show strategies to control for confounding factors, except for two articles that do mention this aspect.
Some of the studies did not show a balance between men and women, so it was not possible to assess sex differences related to the variables described in the objective. On the other hand, certain articles did not include a variety of professional groups that would allow establishing differences between professionals/services. Therefore, the findings may have a limited possibility for generalization to all healthcare professionals as the studies only considered physiotherapists to study the professionals of rehabilitation services, and did not include other groups of important professionals, i.e., occupational therapists, speech therapists, etc. Likewise, although there is a variety of countries in the total number of studies, the quantity is not sufficient, and therefore, the representativeness of the results found cannot be extrapolated to the rest of the health professionals who carry out their healthcare work in the rest of the countries of the world.
Implications and contributions to the field of knowledge
Professionals of the rehabilitation services indicated that the quality of services has been affected by COVID-19, compromising the effectiveness of care (41, 42). For this reason, some activities were temporarily suspended during the last 2 years of the pandemic, and programmes based on work from home were implemented in order to reduce contact with patients. It is therefore relevant to continue researching those factors that compromise the comprehensive care of users in order to implement new care strategies that do not diminish the quality of the service, but allow for continuity.
The use of technology is a good strategy for communication and medical intervention, including rehabilitation. In this sense, it is also important to carry out studies that compare results between professionals in the same health care area, i.e., not only taking into account physiotherapists as the only ones involved in rehabilitation, though this may not be applicable in all cases, as telerehabilitation allows contact to be maintained without fear of contagion. Technology applied to medicine may also empower the patient in their treatment to become an active participant in their recovery, and would also enable the caregiver to assume their role while avoiding overload and being supportive in the process of rehabilitation of the patient, without requiring the continuous presence of the professional in charge.
Equally, the information on the psychological impact of the pandemic throughout the last 2 years contributes to expand knowledge and increases the interest on intervention strategies focused on the health worker's mental health, including professionals in the rehabilitation area. These interventions can be designed to modulate or reduce the risks and consequences of mental health deterioration, as part of a method of prevention of occupational diseases.
Conclusion
Mental health of healthcare professionals, in general, has been compromised as the COVID-19 pandemic has progressed, compared to before the onset of the pandemic. Women were also found to be more likely to suffer increased levels of anxiety, burnout, and depression, and professionals with children and families showed higher levels of distress and anxiety in caring for patients with COVID-19. Additionally, professionals who were in the front line of the battle against the virus have seen their mental health compromised but with values below those of the general population.
Changes in working hours and care settings, patient overload, fear of becoming infected and infecting loved ones and/or patients, among others, may be precipitating factors for an alteration in the mental health of healthcare professionals in times of the COVID-19 pandemic. Such an alteration can be a major problem at a personal, family, and professional level and can increase the risk of professional malpractice.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
Author contributions
Conceptualization: SB-B, RA-C, JG-S, CM-L, JG-I, JF-R, and CR-F. Data curation: SB-B, JG-I, and RA-C. Formal analysis: SB-B, RA-C, JG-S, CM-L, CR-F, JG-I, and CR-F. Investigation: SB-B, RA-C, JG-S, CM-L, JG-I, and JF-R. Methodology: SB-B, JG-S, CM-L, CR-F, and JF-R. Project administration: JG-S and CR-F. Resources: RA-C, JG-S, CM-L, JG-I, and JF-R. Software: SB-B, RA-C, JG-S, and JF-R. Supervision: JG-S, JF-R, JG-I, and CR-F. Validation: RA-C, JG-S, CM-L, and CR-F. Visualization: JF-R and JG-I. Writing—original draft: SB-B, RA-C, JG-I, and JG-S. Writing—review and editing: JG-S, CM-L, JF-R, and CR-F. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.1085820/full#supplementary-material
Abbreviations
CBI, Copenhagen Burnout Inventory; CES-D, Center for Epidemiologic Studies Depression Scale; COVID-19, Coronavirus Disease 2019; DASS-21, Depression Anxiety Stress Scales; GAD-7, Generalized Anxiety Disorder Tool; HADS, Hospital Anxiety and Depression Scale; HAMD-17, Hamilton Depression Scale; IES-R, Impact of Events Scale-Revised; JBI, Joanna Briggs Institute; JD-R, Job Demands-Resources; MBI, Maslach Burnout Inventory; MeSH, Medical Subject Headings; PHQ, Patient Health Questionnaire; PRIME-MD, Primary Care Evaluation of Mental Disorders; PRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses; PSS-10, Perceived Stress Scale; RNA, Ribonucleic acid; SARS-CoV-2, Severe Acute Respiratory Syndrome Coronavirus 2; SDS, Self-rating Depression Scale; WHO, World Health Organization; WHOQOL BREF, World Health Organization Quality of Life.
References
1. World Health Organization. Tracking SARS-CoV-2 Variants. (2022). Geneva, Switzerland: World Health Organization. Available online at: https://www.who.int/activities/tracking-SARS-CoV-2-variants (accessed October 5, 2022).
2. Johns Hopkins Coronavirus Resource Center. COVID-19 Map. (2022). Baltimore, Maryland: Johns Hopkins Coronavirus Resource Center. Available online at: https://coronavirus.jhu.edu/map.html (accessed October 5, 2022).
3. Chaler J, Gil Fraguas L, Gómez García A, Laxe S, Luna Cabrera F, Llavona R, et al. Impact of Coronavirus disease 2019 outbreak on rehabilitation services and physical rehabilitation medicine and rehabilitation physicians' activities: perspectives from the Spanish experience. Eur J Phys Rehabil Med. (2020) 56:369–71. doi: 10.23736/S1973-9087.20.06304-2
4. World Health Organization. WHO Announces COVID-19 Outbreak a Pandemic. (2020). Geneva, Switzerland: World Health Organization. Available online at: http://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/news/news/2020/3/who-announces-covid-19-outbreak-a-pandemic (accessed October 5, 2022).
5. Atalan A. Is the lockdown important to prevent the COVID-19 pandemic? Effects on psychology, environment and economy-perspective. Erratum in: Ann Med Surg (Lond). 56, 217. Ann Med Surg (Lond). (2020) 56, 38–42. doi: 10.1016/j.amsu.2020.07.001
6. Jiménez-Pavón D, Carbonell-Baeza A, Lavie CJ. Physical exercise as therapy to fight against the mental and physical consequences of COVID-19 quarantine: special focus in older people. Prog Cardiovasc Dis. (2020) 63:386–8. doi: 10.1016/j.pcad.2020.03.009
7. Salari N, Hosseinian-Far A, Jalali R, Vaisi-Raygani A, Rasoulpoor S, Mohammadi M, et al. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: a systematic review and meta-analysis. Global Health. (2020) 16:1–11. doi: 10.1186/s12992-020-00589-w
8. Pappa S, Ntella V, Giannakas T, Giannakoulis VG, Papoutsi E, Katsaounou P, et al. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: a systematic review and meta-analysis. Brain Behav Immun. (2020) 88:901–7. doi: 10.1016/j.bbi.2020.05.026
9. Huang Y, Zhao N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: a web-based cross-sectional survey. Psychiatry Res. (2020) 288:112954. doi: 10.1016/j.psychres.2020.112954
10. Santolalla-Arnedo I, Pozo-Herce PD, Viñaspre-Hernandez D, Gea-Caballero RR, Juarez-Vela V, Gil-Fernandez R, et al. Psychological impact on care professionals due to the SARS-CoV-2 virus in Spain. Int Nurs Rev. (2022) 69:520–8. doi: 10.1111/inr.12748
11. Bakker AB, Demerouti E. La teoría de las demandas y los recursos laborales. Rev Psicol Trabajo Organ. (2013) 29:107. doi: 10.5093/tr2013a16
12. Wang Y, Kala MP, Jafar TH. Factors associated with psychological distress during the coronavirus disease 2019 (COVID-19) pandemic on the predominantly general population: a systematic review and meta-analysis. PLoS ONE. (2020) 15:e0244630. doi: 10.1371/journal.pone.0244630
13. Dichter MN, Sander M, Seismann-Petersen S, Köpke S. COVID-19: It is time to balance infection management and person-centered care to maintain mental health of people living in German nursing homes. Int. Psychogeriatr. (2020) 2020:1–11. doi: 10.1017/S1041610220000897
14. Del Pozo-Herce P, Garrido-García R, Santolalla-Arnedo I, Gea-Caballero V, García-Molina P, Viñaspre-Hernández R, et al. Psychological impact on the nursing professionals of the Rioja Health Service (Spain) due to the SARS-CoV-2 virus. Int J Environ Res Public Health. (2021) 18:580. doi: 10.3390/ijerph18020580
15. Kang L, Li Y, Hu S, Chen M, Yang C, Xiang-Yang B, et al. The mental health of medical workers in Wuhan, China dealing with the 2019 novel coronavirus. Lancet Psychiatry. (2020) 7:e14. doi: 10.1016/S2215-0366(20)30047-X
16. Xiang YT, Yang Y, Li W, Zhang L, Zhang Q, Cheung T, et al. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry7. (2020) 228–9. doi: 10.1016/S2215-0366(20)30046-8
17. Spanish Society of Physical Medicine Rehabilitation (SERMEF). SERMEF Recommendations to COVID-19. (2020). Available online at: https://www.sermef.es/recomendaciones-sermef-ante-covid-19/ (accessed November 19, 2022).
18. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. Declaración PRISMA 2020: una guía actualizada para la publicación de revisiones sistemáticas. Rev Españ Cardiol (English Edition). (2021) 74:790–9. doi: 10.1016/j.rec.2021.07.010
19. Moola S, Munn Z, Tufanaru C, Aromataris E, Sears K, Sfetcu R, et al. Chapter 7: Systematic reviews of etiology and risk. In: Aromataris E, Munn Z, editors. JBI Manual for Evidence Synthesis. Adelaida: The Joanna Briggs Institute (2020). doi: 10.46658/JBIMES-20-08
20. Moola S, Munn Z, Tufanaru C, Aromataris E, Sears K, Sfetcu R, et al. Chapter 5: Systematic reviews of etiology and risk. In: Aromataris E, Munn Z, editors. Joanna Briggs Institute Reviewer's Manual. Adelaida: The Joanna Briggs Institute (2017).
21. Lockwood C, Munn Z, Porritt K. Qualitative research synthesis: methodological guidance for systematic reviewers utilizing meta-aggregation. Int J Evid Based Healthc. (2015) 13:179–87. doi: 10.1097/XEB.0000000000000062
22. Centro Cochrane Iberoamericano traductores. Manual Cochrane de Revisiones Sistemáticas de Intervenciones, versión 5, 1.0 (actualizada en marzo de 2011). Barcelona: Centro Cochrane Iberoamericano (2012). Available online at: http://www.cochrane.es/?q=es/node/269 (accessed October 5, 2022).
23. Alnaser MZ, Alotaibi N, Nadar MS, Manee F, Alrowayeh HN. Manifestation of generalized anxiety disorder and its association with somatic symptoms among occupational and physical therapists during the COVID-19 pandemic. Front Public Health. (2022) 10:891276. doi: 10.3389/fpubh.2022.891276
24. Aly HM, Nemr NA, Kishk RM, Elsaid NMAB. Stress, anxiety and depression among healthcare workers facing COVID-19 pandemic in Egypt: a cross-sectional online-based study. BMJ Open. (2021) 11:e045281. doi: 10.1136/bmjopen-2020-045281
25. Chatzittofis A, Karanikola M, Michailidou K, Constantinidou A. Impact of the COVID-19 pandemic on the mental health of healthcare workers. Int J Environ Res Public Health. (2021) 18:1435. doi: 10.3390/ijerph18041435
26. de Sire A, Marotta N, Raimo S, Lippi L, Inzitari MT, Tasselli A, et al. Psychological distress and work environment perception by physical therapists from Southern Italy during COVID-19 pandemic: the CALABRIA study. Int J Environ Res Public Health. (2021) 18:9676. doi: 10.3390/ijerph18189676
27. Jácome C, Seixas A, Serrão C, Teixeira A, Castro L, Duarte I, et al. Burnout in Portuguese physiotherapists during COVID-19 pandemic. Physiother Res Int. (2021) 26:e1915. doi: 10.1002/pri.1915
28. Medeiros AICD, Mesquita RBD, Macêdo FDS, Matos AGDC, Pereira ED. Prevalence of burnout among healthcare workers in six public referral hospitals in northeastern Brazil during the COVID-19 pandemic: a cross-sectional study. Sao Paulo Med J. (2022) 140:553–8. doi: 10.1590/1516-3180.2021.0287.r1.291021
29. Pigati PADS, Righetti RF, Nisiaymamoto BTC, Saraiva-Romanholo BM, Tibério IFLC. Resilience and its impact on the mental health of physiotherapists during the COVID-19 pandemic in São Paulo, Brazil. J Affect Disord. (2022) 310:422–8. doi: 10.1016/j.jad.2022.05.049
30. Syamlan AT, Salamah S, Alkaff FF, Prayudi YE, Kamil M, Irzaldy A, et al. Mental health and health-related quality of life among healthcare workers in Indonesia during the COVID-19 pandemic: a cross-sectional study. BMJ Open. (2022) 12:e057963. doi: 10.1136/bmjopen-2021-057963
31. Szwamel K, Kaczorowska A, Lepsy E, Mroczek A, Golachowska M, Mazur E, et al. Predictors of the occupational burnout of healthcare workers in Poland during the COVID-19 pandemic: a cross-sectional study. Int J Environ Res Public Health. (2022) 19:3634. doi: 10.3390/ijerph19063634
32. Yang S, Kwak SG, Ko EJ, Chang MC. The mental health burden of the COVID-19 pandemic on physical therapists. Int J Environ Res Public Health. (2020) 17:3723. doi: 10.3390/ijerph17103723
33. Farì G, de Sire A, Giorgio V, Rizzo L, Bruni A, Bianchi FP, et al. Impact of COVID-19 on the mental health in a cohort of Italian rehabilitation healthcare workers. J Med Virol. (2022) 94:110–8. doi: 10.1002/jmv.27272
34. Jeleff M, Traugott M, Jirovsky-Platter E, Jordakieva G, Kutalek R. Occupational challenges of healthcare workers during the COVID-19 pandemic: a qualitative study. BMJ Open. (2022) 12:e054516. doi: 10.1136/bmjopen-2021-054516
35. Palacios-Ceña D, Fernández-de-Las-Peñas C, Florencio LL, de-la-Llave-Rincón AI, Palacios-Ceña M. Emotional experience and feelings during first COVID-19 outbreak perceived by physical therapists: a qualitative study in Madrid, Spain. Int J Environ Res Public Health. (2020) 18:127. doi: 10.3390/ijerph18010127
36. Palacios-Ceña D, Fernández-de-Las-Peñas C, Palacios-Ceña M, De-La-Llave-Rincón AI, Florencio LL. Working on the frontlines of the COVID-19 pandemic: a qualitative study of physical therapists' experience in Spain. Phys Ther. (2021) 101:pzab025. doi: 10.1093/ptj/pzab025
37. Chew NWS, Ngiam JN, Tan BY, Tham SM, Tan CY, Jing M, et al. Asian-Pacific perspective on the psychological well-being of healthcare workers during the evolution of the COVID-19 pandemic. BJPsych Open. (2020) 6:e116. doi: 10.1192/bjo.2020.98
38. Wang C, Chudzicka-Czupała A, Tee ML, Núñez MIL, Tripp C, Fardin MA, et al. A chain mediation model on COVID-19 symptoms and mental health outcomes in Americans, Asians and Europeans. Sci Rep. (2021) 11:6481. doi: 10.1038/s41598-021-85943-7
39. Kliszcz J, Nowicka-Sauer K, Trzeciak B, Sadowska A. Poziom leku, depresji i agresji u pielegniarek, a ich satysfakcja z zycia i z pracy zawodowej [The level of anxiety, depression and aggression in nurses and their life and job satisfaction]. Med Pr. (2004) 55, 461–8 (in Polish). Available online at: https://silo.tips/download/poziom-lku-depresji-i-agresji-u-pielgniarek-a-ich-satysfakcja-z-ycia-i-z-pracy-z (accessed November 29, 2022).
40. García-Iglesias JJ, Gómez-Salgado J, Martín-Pereira J, Fagundo-Rivera J, Ayuso-Murillo D, Martínez-Riera JR, et al. Impacto del SARS-CoV-2 (COVID-19) en la salud mental de los profesionales sanitarios: una revisión sistemática [Impact of SARS-CoV-2 (COVID-19) on the mental health of healthcare professionals: a systematic review.]. Rev Esp Salud Publ. (2020). 94:e202007088 (in Spanish). Available online at: https://medes.com/publication/152295
41. Hoel V, von Zweck C, Ledgerd R, World Federation of Occupational Therapists. Was a global pandemic needed to adopt the use of telehealth in occupational therapy? Work. (2021). 68, 13–20. doi: 10.3233/WOR-205268
Keywords: health professionals, physiotherapist, rehabilitation, mental health, psychological stress, anxiety, depression, COVID-19
Citation: Bohórquez-Blanco S, Allande-Cussó R, Martín-López C, Gómez-Salgado J, García-Iglesias JJ, Fagundo-Rivera J and Ruiz-Frutos C (2022) Effects of the COVID-19 pandemic on the mental health of rehabilitation area professionals: A systematic review. Front. Public Health 10:1085820. doi: 10.3389/fpubh.2022.1085820
Received: 31 October 2022; Accepted: 22 November 2022;
Published: 08 December 2022.
Edited by:
Ali Davod Parsa, Anglia Ruskin University, United KingdomReviewed by:
Ivan Santolalla Arnedo, University of La Rioja, SpainMarija Jevtic, University of Novi Sad, Serbia
Copyright © 2022 Bohórquez-Blanco, Allande-Cussó, Martín-López, Gómez-Salgado, García-Iglesias, Fagundo-Rivera and Ruiz-Frutos. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Juan Gómez-Salgado, c2FsZ2Fkb0B1aHUuZXM=; Juan Jesús García-Iglesias, anVhbmplc3VzLmdhcmNpYUBkc3Rzby51aHUuZXM=