 Jeanne Perpétue Vincent
Jeanne Perpétue Vincent Carolyn Nyamasege
Carolyn Nyamasege Su Wang3
Su Wang3 Yoann Madec
Yoann Madec Yusuke Shimakawa
Yusuke Shimakawa- 1Unité d'Épidémiologie des Maladies Émergentes, Institut Pasteur, Paris, France
- 2Department of Health and Human Services, Institute for Health Policy and Practice, University of New Hampshire, Concord, NH, United States
- 3Viral Hepatitis Program, Cooperman Barnabas Medical Center, Livingston, NJ, United States
Background: Viral hepatitis causes an important global health burden. In 2016, the World Health Assembly adopted an objective to globally eliminate this as a public health threat by 2030. However, significant gaps exist between countries in their progress. Haiti is the last country that has introduced infant hepatitis B vaccines into the routine immunization program in the Region of the Americas, and its schedule still does not incorporate birth dose vaccines. As the first step to raise awareness of viral hepatitis in this country, we conducted a systematic review and meta-analysis to estimate the prevalence of hepatitis B (HBV), C (HCV), and D (HDV) viruses in Haiti.
Methods: We searched PubMed, EMBASE, Web of Science and Scopus for studies reporting the prevalence of HBV, HCV and HDV among Haitian, with no language restriction, published until November 30th, 2021. Prevalence was pooled via a random-effects meta-analysis using a generalized linear mixed model with the logit link.
Results: Of 453 articles retrieved, 25 studies were included: 16 reported the prevalence of hepatitis B surface antigen (HBsAg), three for anti-HCV antibody, and six for both HBsAg and anti-HCV. No study was found for HDV prevalence. The pooled prevalence of HBsAg was 0.7% [95% confidence interval (CI): 0.3–1.4, I2 = 77.7%] among children, 3.5% (95% CI: 2.8–4.4, I2 = 93.2%) in the general adult population and 7.4% (95% CI: 4.0–13.3, I2 = 83.9%) in high-risk adult population. The pooled prevalence of anti-HCV antibody was 0.9% (95% CI: 0.6–1.4, I2 = 93.5%) among the general population and 1.4% (95% CI: 0.4–4.2, I2 = 0.0%) in high-risk adult population. No study reported the prevalence of anti-HCV antibody exclusively in children.
Interpretation: The prevalence of blood-borne hepatitis, particularly that of HBV, is substantial in Haiti. The introduction of birth dose hepatitis B vaccines and improving access to testing and treatment services should be urgently considered to meet the elimination goal.
Systematic review registration: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022298081, identifier: PROSPERO (CRD42022298081).
Background
An estimated 354 million people live with hepatitis B (HBV) or hepatitis C virus (HCV) worldwide, and among them more than one million die yearly from complications such as hepatocellular carcinoma or cirrhosis (1). The majority of this burden is borne by people in Africa and Asia. In the Americas, the number of people chronically infected with HBV and HCV were estimated at 14 million (2). The number of deaths related to HBV and HCV in 2019 for the region were estimated at 15,000 and 31,000, respectively (1).
As these chronic viral infections progress asymptomatically over the years until serious liver damage is established, most people chronically infected with HBV or HCV remain undiagnosed unless there is a screening program for these infections targeting asymptomatic people. In fact, The World Health Organization (WHO) estimates that only 10% of people living with HBV and 21% of those living with HCV have been diagnosed (1). The WHO presently aims to achieve the worldwide elimination of hepatitis B and C as public health threat by 2030 (3).
Haiti is a small country of 11 million people located in the Caribbean, where little attention has been paid to viral hepatitis. The country was the last in the Americas to introduce hepatitis B vaccines into the routine infant immunization program in 2012 using pentavalent vaccines scheduled at 6, 10, and 14 weeks of life (4). In 2020, 8 years after the introduction of the hepatitis B vaccines, coverage of three-dose pentavalent vaccines still remained low at 51% among 1-year-old children according to the WHO/UNICEF data (5). Moreover, the birth dose vaccination is not yet introduced into the national immunization program and pregnant women are not systematically screened for HBV to prevent mother-to-child transmission (MTCT) despite the WHO's recommendations (6). There is no national program targeting chronic viral hepatitis in Haiti.
To date, there is no systematic review specific to Haiti to estimate the prevalence of chronic viral hepatitis in this country. Regarding the prevalence of HBsAg, studies on a global or regional scale have provided country-specific estimates including that of Haiti, but with marked variations between studies. In a systematic review and meta-analysis by Schweitzer et al. (7) published in 2015, an estimated 13.6% (95% CI: 9.0–19.9) of Haitians were positive for HBsAg. Kowdley et al. also conducted a systematic review and meta-analysis, and reported a pooled prevalence of 4.8% (95% CI: 3.9–5.7) in their first publication in 2011 and 4.6% (95% CI: 3.2–6.0) in their updated publication in 2021 (8, 9). On the basis of a combination of literature review and expert opinions, the Polaris Observatory Collaborators estimated that the prevalence of HBsAg in Haiti in 2016 was 2.9% (95% CI: 2.7–4.1) (10). Most recently, the Global Burden of Disease (GBD) study reported a decrease in prevalence of HBV from 1.9% (95% CI: 1.5–2.2) in 1990 to 1.6% (95% CI: 1.3–1.9) in 2019, using a combination of systematic review and mathematical modeling (11). Interpretation of these heterogeneous estimates is complicated. Moreover, besides the articles by Kowdley et al., these estimations were based on a small number of studies (two for Schweitzer et al., four for Polaris, and one for GBD). Regarding HCV and hepatitis D virus (HDV), none of the previous systematic reviews estimating the global prevalence of these infections included a study from Haiti (12–15).
We, therefore, conducted a systematic review and meta-analysis specific to Haiti for the prevalence of HBV, HCV, and HDV among three groups: (i) children, (ii) the general adult population, and (iii) the high-risk adult population. The data generated by this work can serve as baseline data before any public health interventions targeting these infections are implemented in this country.
Methods
Search strategy and eligibility criteria
This systematic review was conducted following a protocol registered in PROSPERO (CRD42022298081) and reported according to the PRISMA guidelines (16). Four databases (PubMed, EMBASE, Web of Science and Scopus) were searched from their inception until November 30, 2021, without language restriction. Following search terms and their respective variations were used: “Haiti” AND “(“HBV” OR “HCV” OR “HDV”)” (detailed search strategy in Supplementary material). References of included studies were also manually searched. Original articles and conference abstracts of any study design were eligible if they reported the numerator (number with a positive result) and the denominator (number who had a test) enabling us to calculate the prevalence of viral hepatitis markers in individuals of any age living in Haiti or immigrants of Haitian origin (i.e., those born in Haiti and residing in other countries). Gray literature, including government reports or WHO reports, was also eligible if it provided these data. We primarily considered the following markers: HBsAg, anti-HCV antibody, and anti-HDV antibody. In addition, as secondary outcomes we considered the following: HBV DNA and hepatitis B e antigen (HBeAg) in people positive for HBsAg, HCV RNA in people positive for anti-HCV, and HDV RNA in people positive for anti-HDV antibody. Clinical definition of chronic HBV infection is the persistence of HBsAg for at least 6 months (17). In contrast, for an epidemiological study in a country with high HBV endemicity, positive HBsAg at a single time point can be reasonably considered as a chronic HBV infection (18).
Data selection
Titles and abstracts of all the articles identified through the search strategy were independently screened for relevance by two reviewers (JPV and CN). Following the selection of potentially eligible articles through the screening, a full-text reading was performed to review and extract the data. Any discrepancies between two reviewers were resolved through discussion within the team. A standardized form was edited to extract, by the same two reviewers, the following data from each study: first author's name, year of publication, journal name, language used to report the study, study setting, type of study population, period of data collection, participants' baseline characteristics, inclusion and exclusion criteria, type of assay used for viral hepatitis markers, total number of people tested for each of viral hepatitis markers (i.e., denominators), and total number of people tested positive for each of viral hepatitis markers (i.e., numerators).
The study population was classified into three groups: children, the general adult population and the high-risk adult population. We defined adults as those aged ≥15 years. The high-risk adult population includes people living with other comorbidities (e.g., HIV, tuberculosis) as well as refugees, and those with symptoms related to liver disease (e.g., ascites). The general adult population was defined as those not presenting the characteristics defined above as high risk. Whenever possible, population-specific estimates were obtained in a study that recruited different groups of people.
Whenever information was missing in the full-text paper that limits our ability to make a final decision on whether to include the study, corresponding authors were systematically contacted by e-mail. The risk of bias was evaluated using a framework introduced by Hoy et al. (19).
Data analysis
The outcomes of interest were as below: the prevalence of HBsAg, the prevalence of HBeAg or positive HBV DNA in HBsAg-positive individuals, the prevalence of anti-HCV antibody or HCV RNA, the prevalence of anti-HDV antibody or HDV RNA in people chronically infected with HBV. The prevalence of each marker was computed by dividing the number of people tested positive by the total number of people tested. Meta-analysis was carried using the “metaprop” command with R 4.2.2 (R Foundation for Statistical Computing, Vienna, Austria) and RStudio Desktop 2022.07.2 (Rstudio, PBC, Boston, MA, USA) (20). Proportions were pooled via a random-effects meta-analysis using a generalized linear mixed model (GLMM) with a logit link approach. The percentage of total variation between studies due to heterogeneity was evaluated using the I2 statistic. Subgroup analyses were conducted by place of residence at the time of testing (Haiti or outside), and by recruitment period (before or after the year 2000) among the general adult population. We also analyzed the subgroups of pregnant women and people living with HIV (PLHIV).
Results
A total of 453 articles were identified after the removal of duplicates. Following the independent screening by two reviewers, 42 full-text articles were assessed for eligibility, and 21 met the eligibility criteria. In addition, four more eligible articles were manually identified from the references of the included studies and other review articles. Finally, 25 studies were included in the meta-analysis for the following hepatitis markers: HBsAg only (16 studies), anti-HCV antibody only (three studies), and both HBsAg and anti-HCV antibody (6 studies). There was no study assessing HDV prevalence among Haitian (Figure 1).
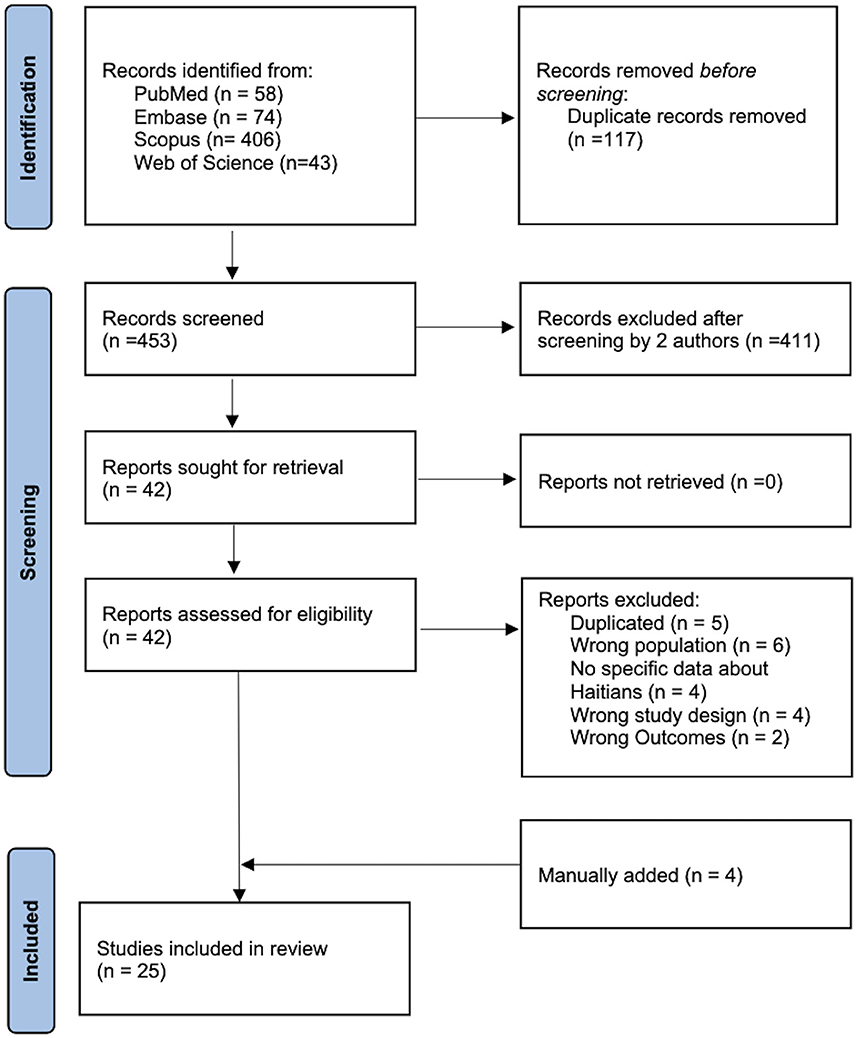
Figure 1. PRISMA flow diagram showing the study selection process.
Of the 22 studies reporting the prevalence of HBsAg, six were classified as having a low risk of bias, seven as a moderate, and nine as a high risk. Of the nine studies reporting the prevalence of anti-HCV antibody, two were classified as a low risk of bias, six as moderate, and one as high. There was a wide variation in the recruitment sites. For HBsAg, seven studies recruited participants in hospitals, seven during antenatal or perinatal care, two from blood bank, and six in community survey. For anti-HCV antibody, four studies recruited in hospital, two during antenatal care, two from blood bank, and three in community survey.
HBV prevalence
Twenty studies evaluated adult population, including two with a mixed population of adults and children, and two studies exclusively evaluated children (Table 1). Eleven studies were conducted on people residing in Haiti, nine on immigrants and two on refugees. Of 20 adult studies, 15 reported prevalence in a single population and five reported prevalence in separate groups of people. Consequently, a total of 27 estimates were derived: 19 for the general adult population (including four for blood donors and seven for women during antenatal or perinatal care visit), and eight for the high-risk adult population (including four estimates for PLHIV, one for patients with tuberculosis, two for refugees, and one for patients with ascites). The characteristics of the studies reporting HBsAg prevalence were summarized in Table 1.
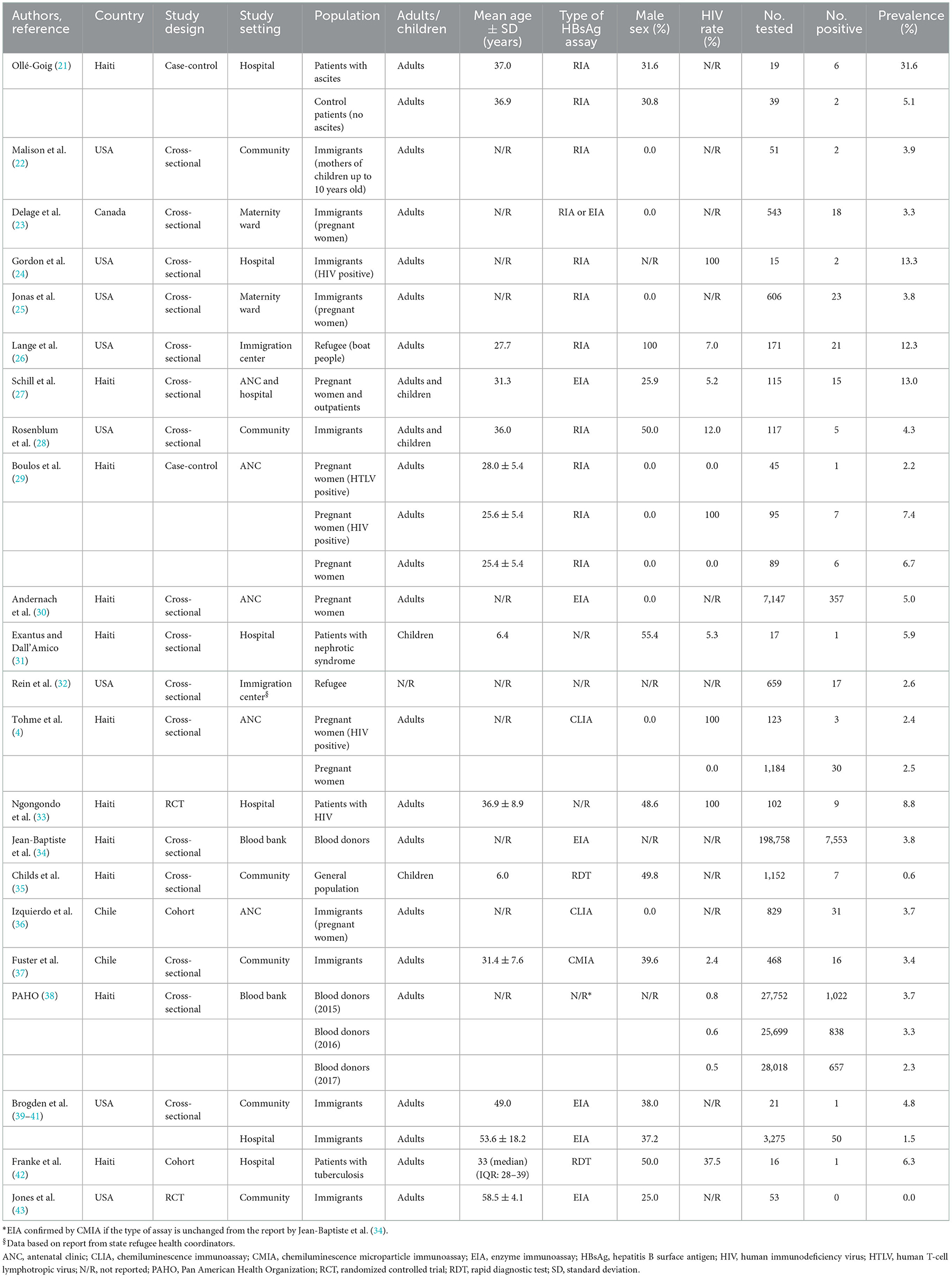
Table 1. Studies reporting the prevalence of HBsAg among Haitians.
A total of 297,178 individuals were assessed for HBsAg. In children, the pooled prevalence was 0.7% (95% CI: 0.3–1.4, I2 = 77.7%). Exantus et al. (31) studied a group of children with nephrotic syndrome evaluated from 1990 to 2008, before the introduction of HBV vaccines in the national program, while Childs et al. (35) conducted a nationally representative community-based survey in 2017 among 5–7 year-olds, including both children born before and after the hepatitis B immunization program.
In the general adult population, the pooled prevalence of HBsAg was 3.5% (95% CI: 2.8–4.4, I2 = 93.2%); this was significantly lower than that in high-risk populations (7.4%, 95% CI: 4.0–13.3, I2 = 83.9%, p for heterogeneity between groups < 0.001, Figure 2). In the general adult population, the prevalence tended to be lower in studies conducted after the year 2000 (3.1%, 95% CI: 2.5–3.8, I2 = 95.8%) than in those conducted before 2000 (4.8%, 95% CI: 3.2–7.2, I2 = 66.4%, p for heterogeneity between groups = 0.05, Figure 3). The prevalence in the general adult population did not significantly vary according to their place of residence at the time of testing: 4.0 % (95% CI: 2.9–5.4, I2 = 96.0%) in those recruited in Haiti and 2.9% (95% CI: 2.1–3.9, I2 = 69.5%) in immigrants of Haitian origin (p for heterogeneity between groups = 0.16, Figure 4). In pregnant women, no difference was observed in the prevalence between those not infected with HIV (3.8%, 95% CI: 3.0–4.8, I2 = 69.1%) and those infected with HIV (4.5%, 95% CI: 2.1–9.4, I2 = 63.0%, p for heterogeneity between groups = 0.68) (Figure 5A). In PLHIV the prevalence was estimated at 6.3% (95% CI: 3.7–10.5, I2 = 39.6%) (Supplementary Figure 1).
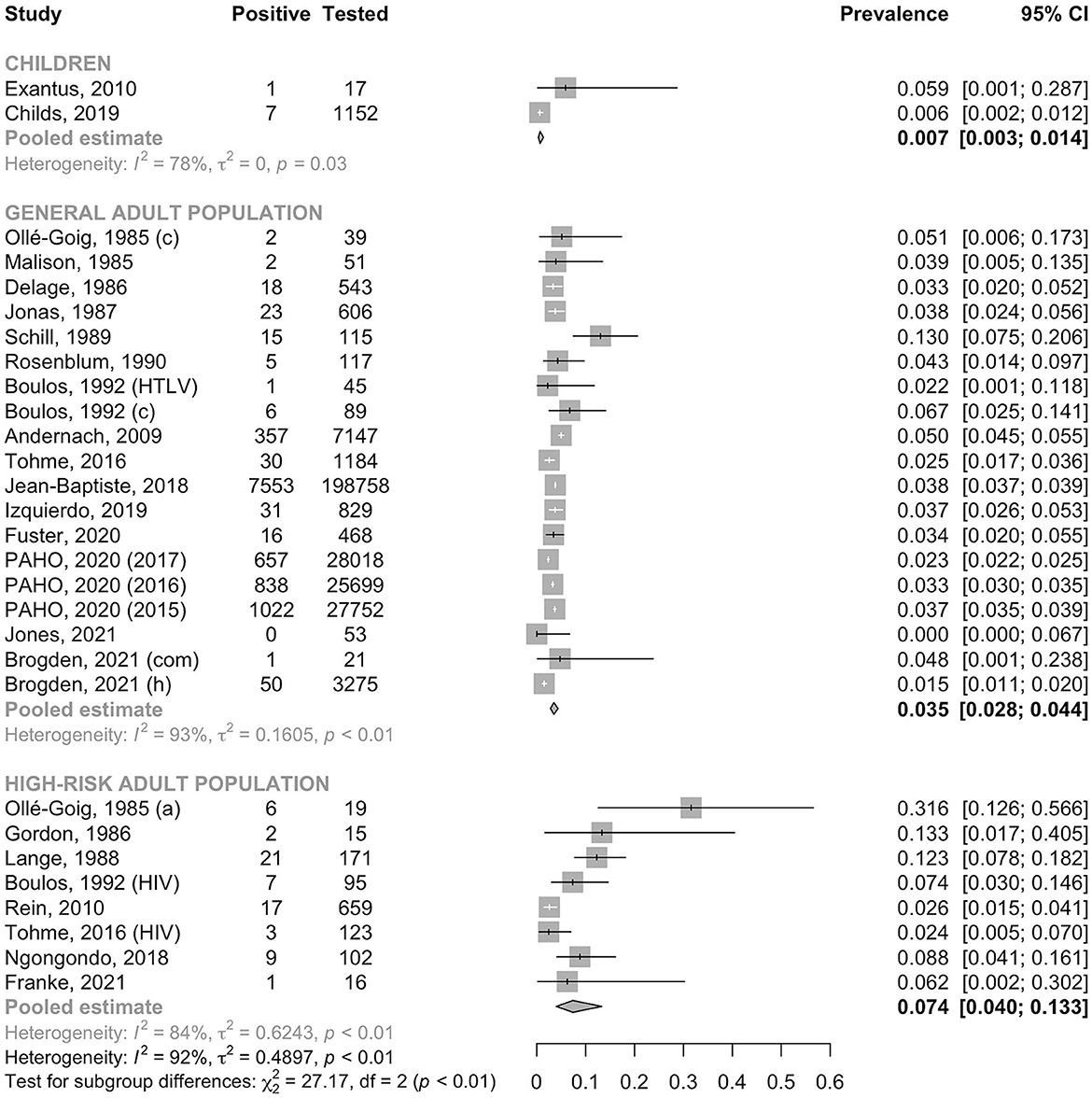
Figure 2. Prevalence of HBsAg in children, the general adult population and the high-risk adult population. a, ascites group; c, control group; com, community recruitment; h, hospital recruitment; HIV, human immunodeficiency virus positive group; HTLV, human T-cell lymphotropic virus positive group; PAHO, Pan American Health Organization.
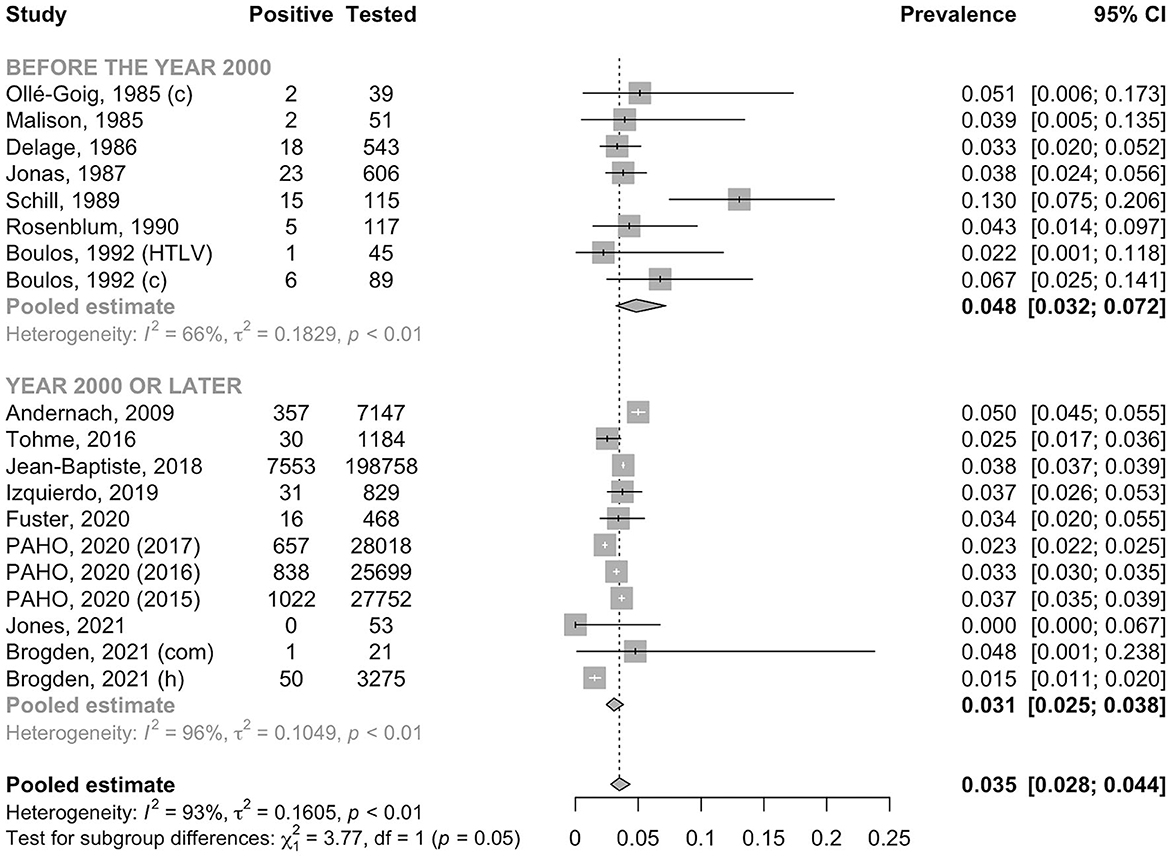
Figure 3. Prevalence of HBsAg in the general adult population by year. c, control group; com, community recruitment; h, hospital recruitment; HTLV, human T-cell lymphotropic virus positive group; PAHO, Pan American Health Organization.
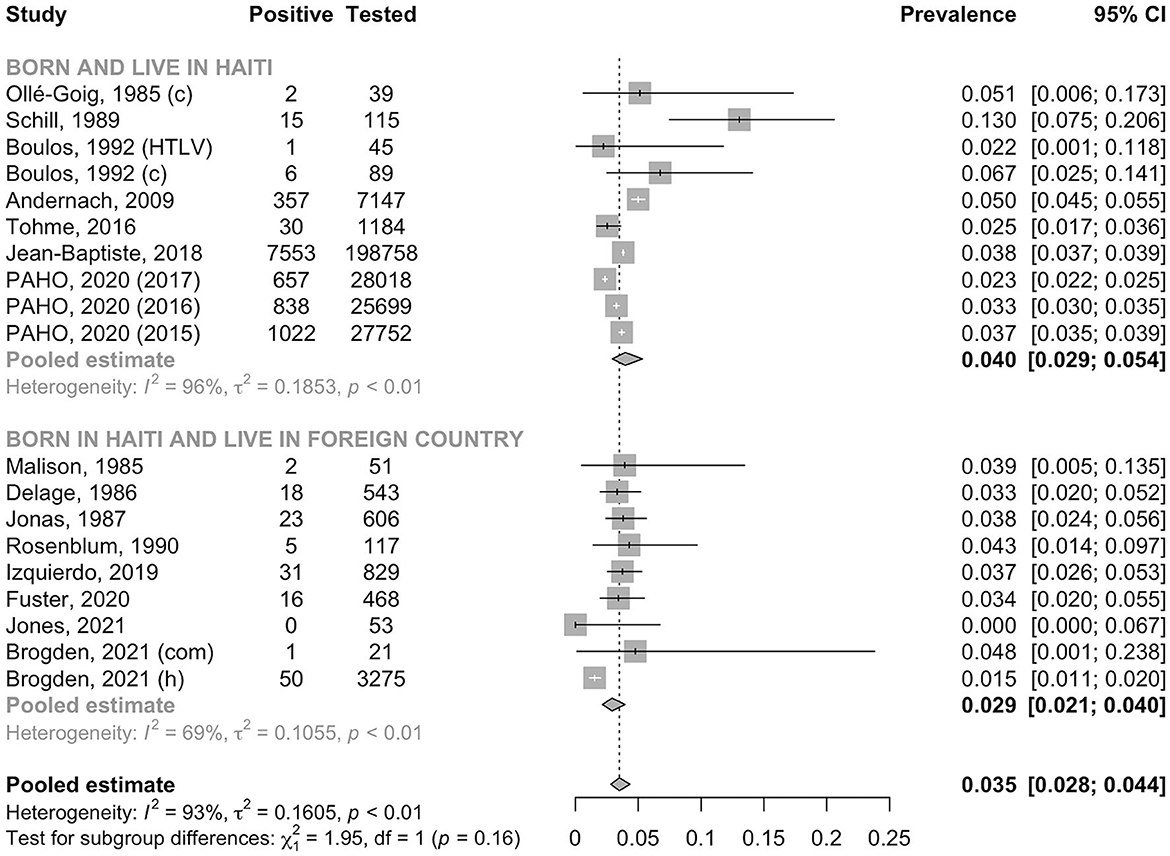
Figure 4. Prevalence of HBsAg in the general adult population by place of residence. a, ascites group; c, control group; com, community recruitment; h, hospital recruitment; HIV, human immunodeficiency virus positive group; HTLV, human T-cell lymphotropic virus positive group; PAHO, Pan American Health Organization.
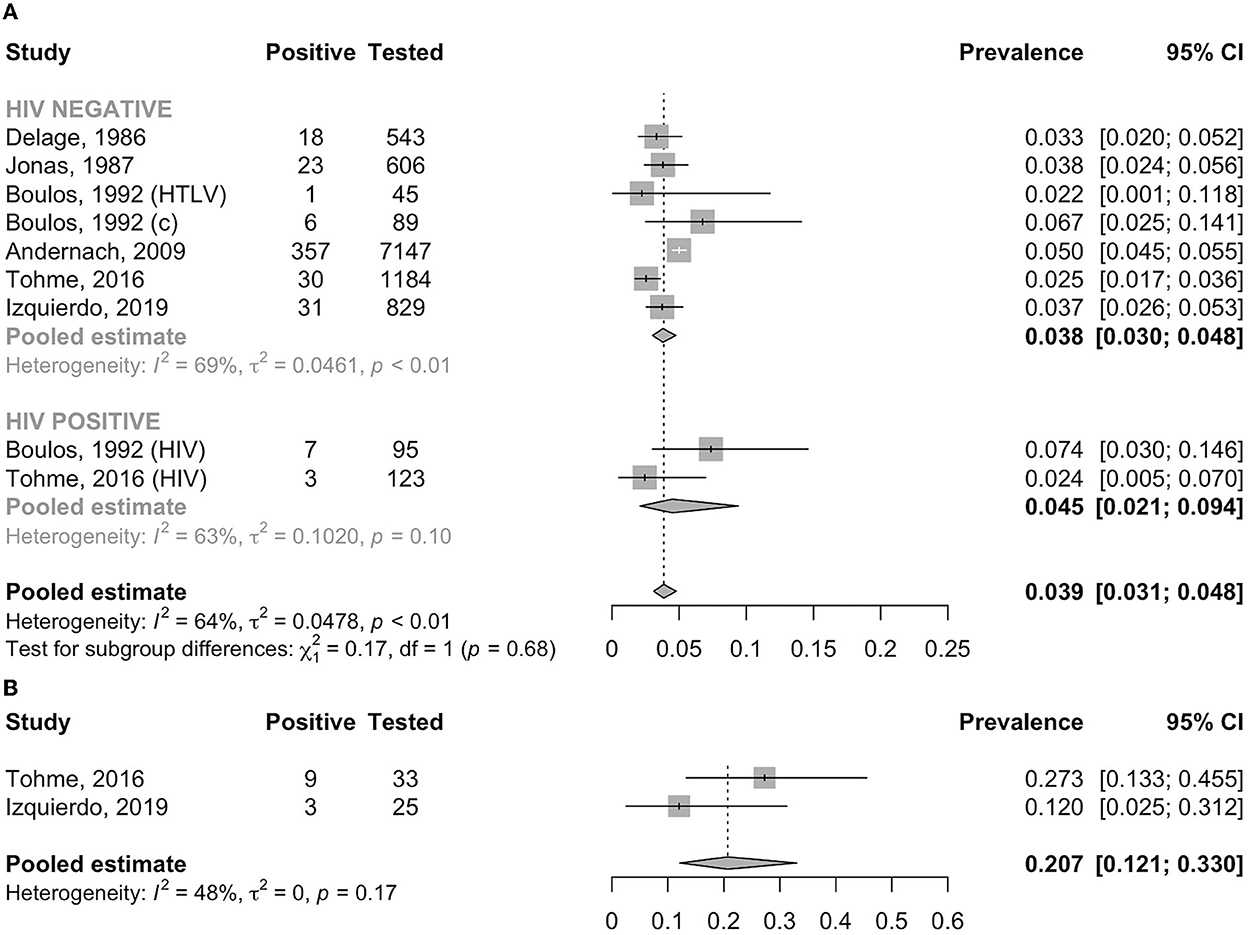
Figure 5. (A) Prevalence of HBsAg in pregnant women by HIV status. c, control group; HIV, human immunodeficiency virus positive group; HTLV, human T-cell lymphotropic virus positive group. (B) Prevalence of high viral load (≥200,000 IU/ml) in HBsAg-positive pregnant women.
Sixteen studies only tested HBsAg as the sole marker of HBV, three studies tested HBsAg and HBeAg (22–24), two studies tested HBsAg and HBV DNA (4, 30), and one study tested both HBeAg and HBV DNA in addition to HBsAg (36). In four studies reporting HBeAg sero-status, two studied pregnant women (23, 36), one studied mothers of children up to 10 years of age (22), and one studied PLHIV (24). Delage et al. and Malison et al. found none of HBsAg-positive women were positive for HBeAg (0/32 and 0/2, respectively) (22, 23). In contrast, Izquierdo et al. found that 12.9% (4/31) of the HBsAg-positive pregnant women carried HBeAg (36). The pooled prevalence of HBeAg among HBsAg-positive mothers was 6.7% (95% CI: 1.0–34.2, I2 = 0.0%) (Supplementary Figure 2). In PLHIV, Gordon et al. identified two HBeAg-positive participants out of two HBsAg-positive (24).
Three studies reported HBV DNA PCR test results in people identified to carry HBsAg (4, 30, 36). Tohme et al. (4) detected HBV DNA among 78.8% (26/33) of HBsAg-positive pregnant women, with nine (27.3%) having viral load >200,000 IU/ml using an in-house quantitative PCR with a lower limit of detection of 50 IU/ml. Izquierdo et al. (36) detected HBV DNA in 92.0% (23/25) of HBsAg-positive pregnant women using the Abbott RealTime HBV assay with a lower limit of quantitation of 10 IU/ml; three (12.0%) women had viral load ≥200,000 IU/ml. The pooled prevalence of HBV DNA viral load ≥200,000 IU/ml among pregnant women was 20.7% (95% CI: 12.1–33.0, I2 = 48.1%) (Figure 5B).
Andernach et al. detected HBV DNA in 77.2% (247/320) of HBsAg-positive pregnant women by an in-house PCR. The later was the only study that analyzed HBV genotypes and reported that the majority (71.5%, 128/179) of the infections were caused by HBV genotype A (including A1, A2, and A5), followed by D (22.3%, 40/179; including D3 and D4) and E (6.1%, 11/179) (30).
HCV prevalence
The characteristics of the nine studies reporting anti-HCV antibody prevalence are presented in Table 2. Seven studies exclusively recruited adults while two recruited both adults and children. Five studies were conducted in people residing in Haiti and four in immigrants. The nine adults studies provided 13 estimates: 11 for the general adult population (including four groups of blood donors, one group of pregnant women during antenatal care, three groups of adults recruited in community settings and three from hospitals among outpatients, surgery patients and those attending emergency room) and two for the high-risk adult population (including one with outpatients presenting AIDS suggestive symptoms and another comprising patients with tuberculosis).
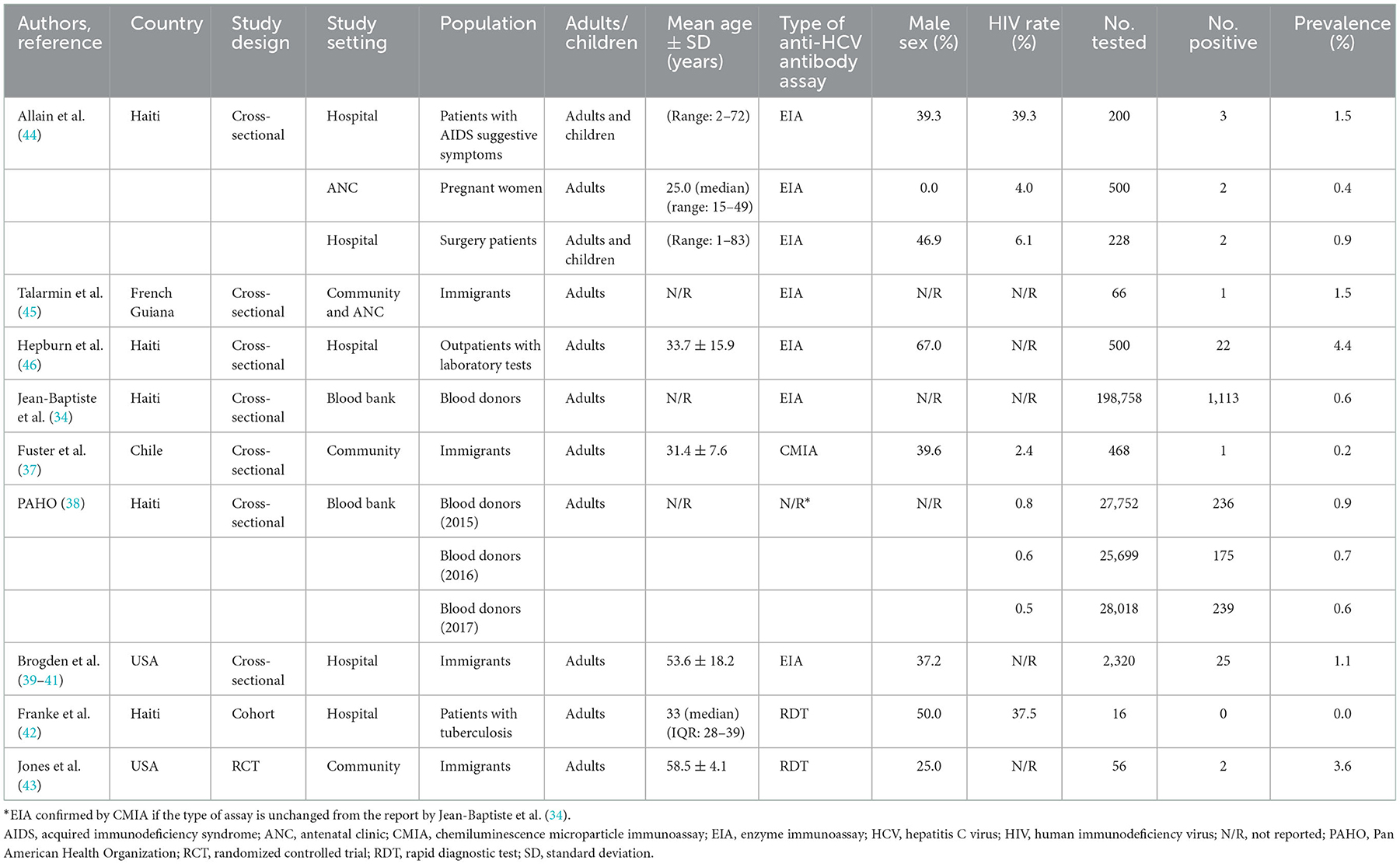
Table 2. Studies reporting the prevalence of anti-HCV antibody among Haitians.
A total of 284,581 individuals were assessed for anti-HCV antibody. The pooled prevalence was 0.9% (95% CI: 0.6–1.4, I2 = 93.5%) in the general adult population and 1.4% (95% CI: 0.4–4.2, I2 = 0.0%) in the high-risk group (p for heterogeneity between groups = 0.50) (Figure 6). In the general adult population, there was no evidence for the difference in the prevalence between the studies conducted before the year 2000 (0.6%, 95% CI: 0.3–1.5, I2 = 0.0%) and after 2000 (1.0%, 95% CI: 0.6–1.6, I2 = 95.4%) (p for heterogeneity between groups = 0.40) (Figure 7). Similarly, there was no evidence for the difference in the prevalence in the general adult population between those residing in Haiti and in foreign countries at the time of testing (0.9%, 95% CI: 0.5–1.5, I2 = 95.7% and 1.0%, 95% CI: 0.7–1.4, I2 = 46.5%, respectively) (p for heterogeneity between groups = 0.76) (Figure 8).
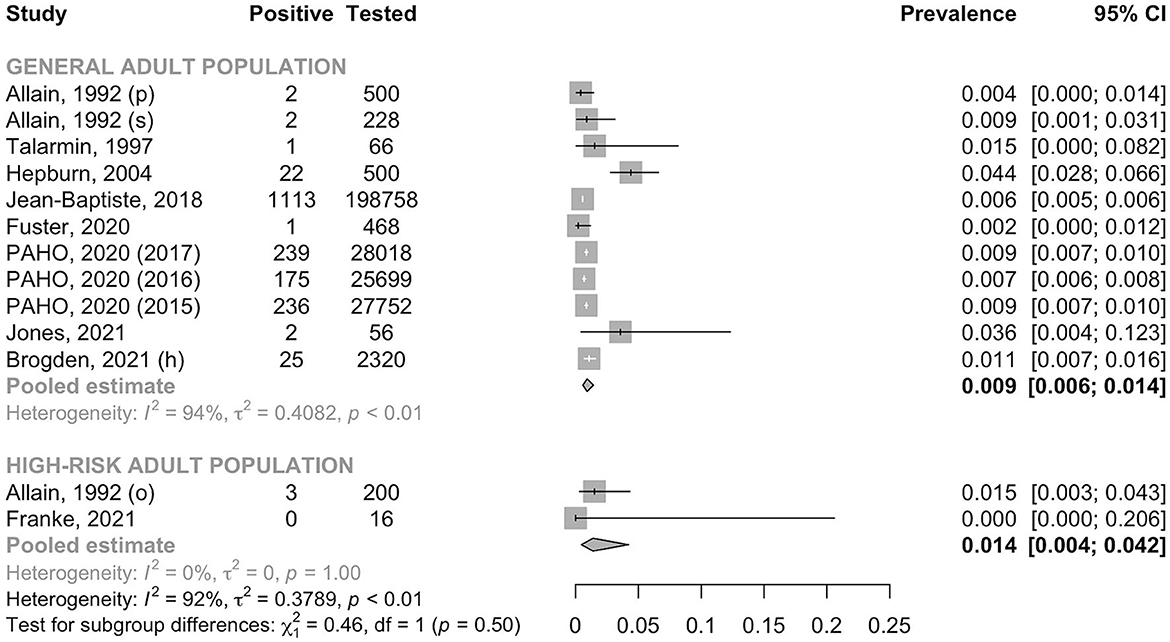
Figure 6. Prevalence of anti-HCV antibody in the general adult population and the high-risk adult population. h, hospital recruitment; o, outpatient; p, pregnant women; PAHO, Pan American Health Organization; s, surgery patient.
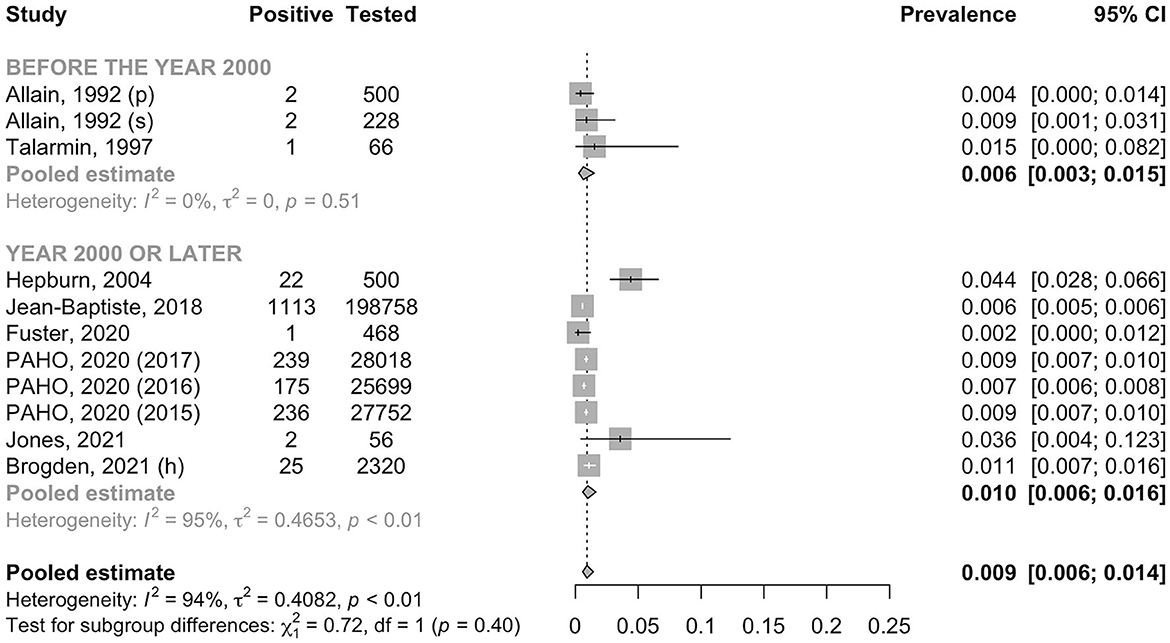
Figure 7. Prevalence of anti-HCV antibody in the general adult population by year. h, hospital recruitment; p, pregnant women; PAHO, Pan American Health Organization; s, surgery patient.
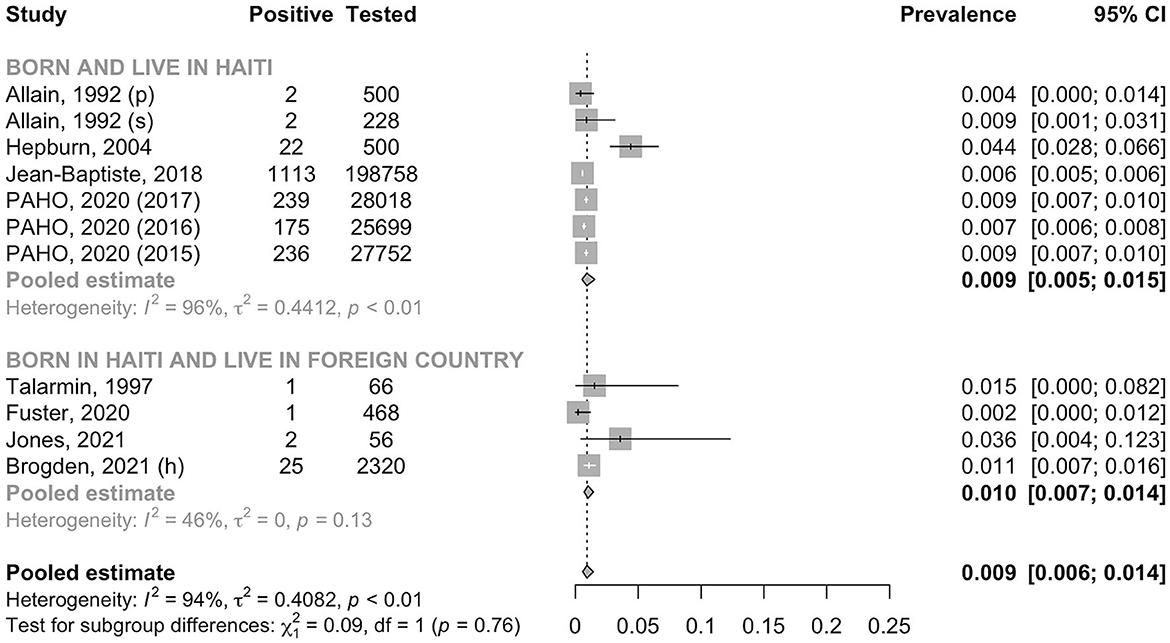
Figure 8. Prevalence of anti-HCV antibody in the general adult population by place of residence. h, hospital recruitment; p, pregnant women; PAHO, Pan American Health Organization; s, surgery patient.
HCV RNA results were available in two studies (37, 39). Of 468 participants screened for anti-HCV, Fuster at al. (37) identified one participant positive for anti-HCV; HCV RNA was not detected in this anti-HCV positive individual using a Roche COBAS Real-Time PCR. In 25 participants positive for anti-HCV, Brogden et al. (39) reported detectable HCV RNA in ten (40.0%) using Abbott Alinity m reverse transcription PCR.
Discussion
Through a systematic review and meta-analysis, the pooled prevalence of HBsAg was 3.5% (95% CI: 2.8–4.4) and that of anti-HCV was 0.9% (95% CI: 0.6–1.4) among the general adult population from Haiti. In this population, the prevalence of HBsAg might have decreased from 4.8% (before 2000) to 3.1% (after 2000), whilst such decrease was not observed for the prevalence of anti-HCV antibody. The prevalence of HBsAg did not considerably vary between people living in Haiti and those who migrated to other countries; a similar pattern was observed for anti-HCV. There was no study reporting the prevalence of HDV in Haitian.
To date, multiple studies reported a country-specific estimates for HBsAg in Haiti with marked variations. The highest estimate was provided by Schweitzer et al. (7) (13.6%, 95% CI: 9.0–19.9). That systematic review and meta-analysis only included two studies with a total of 155 participants (27, 29); importantly, they used the prevalence of HBsAg in people positive for hepatitis B core antibody (anti-HBc) that had been reported in one of the two included studies (29). It is obvious that those who have been exposed to HBV (i.e., anti-HBc positive) should have higher prevalence of HBsAg than the general population, thus leading to an overestimation of the HBV burden. The pooled prevalence of HBsAg among the general adult population in our meta-analysis (3.5%, 95% CI: 2.8–4.4) fell into the range of the previous estimate reported by the Polaris Observatory Collaborators (2.9%, 95% CI: 2.7–4.1) (10). Their hybrid method combining literature review, international expert interviews, meta-analysis, and modeling, yielded a pertinent estimate because it was based on large data on blood donors and pregnant women, all included as well in this review.
The prevalence observed in our systematic review was lower than the estimates in many of Asian or African countries, where about 6% of the population carry HBsAg (47–51), but much higher than the Americas' average (0.7%, 95% CI: 0.4–1.6) (2). Assuming that 3.5% of 7.8 million adults in Haiti are chronically infected with HBV, about 273,000 people would need follow-up and care for their chronic HBV infection (52). Our findings also suggest that HBV prevalence might be higher among high-risk groups, including patients with tuberculosis or those living with HIV.
As expected, the HBsAg prevalence in pregnant women (3.8%) was similar to the prevalence in the general adult population. Although the rate of HBeAg carriage in HBsAg-positive mothers was not high, a significant proportion presented a high viral load (20.7% had a viral load ≥200,000 IU/ml). This being a strong marker for MTCT (53), it is important to consider systematic measures for prevention of MTCT of HBV in Haiti.
We found a decreasing trend of HBsAg in the general adult population by comparing the pooled estimates before and after the year 2000. This decreasing trend might be underestimated by the use of non-sensitive assay before 2000; indeed, all the pre-2000 studies but one used radioimmunoassay to detect HBsAg, which has much lower analytical sensitivity than chemiluminescence or enzyme immunoassay that were used in studies conducted after 2000. This indicates that the true prevalence of HBsAg before 2000 could have been even higher than what we observed, further confirming the decreasing trend in HBsAg prevalence over time. This spontaneous decrease in HBsAg prevalence in adults, in the absence of a large impact from a recently introduced hepatitis B immunization program, could be explained by changes in demographic factors, such as decrease in sibship size or increase in maternal age at first childbirth in Haiti (54). Delaying the age of marriage and childbearing may result in a decrease in HBsAg prevalence because older mothers, if chronically infected with HBV, have a higher chance of having lost HBeAg and remaining in low viral load with a decrease in risk of transmitting HBV to their babies (55–57). Moreover, the reduction in sibship size may contribute to the reduction in horizontal transmission that mainly occurs between siblings within a household (58, 59). This aligns with the lower prevalence seen among children after 2000.
All but one study constantly showed that the prevalence of anti-HCV was below 1%, which is close to the average for the Americas (0.7%, 95% CI: 06–0.8). There was no significant variation of the anti-HCV prevalence between studies conducted before 2000 (0.6%, 95% CI: 0.3–1.5) and after 2000 (1.0%, 95% CI: 0.6–1.6). No considerable variation in anti-HCV prevalence was observed by place of residence (0.9%, 95% CI: 0.5–1.5 in Haiti and 1.0%, 95% CI: 0.7–1.4 abroad). Assuming a prevalence of anti-HCV at 0.9% among adults and a proportion of 75% of anti-HCV positive to carry HCV RNA (60), there could be about 50,000 people in Haiti that are chronically infected with HCV and would benefit from curative treatment with directly acting antiviral (DAA). Most Haitians pay for medical fee out of pocket; therefore, it will help if DAAs are financed like antiretroviral drugs for HIV.
This review had a few constrains. First, in two studies reporting on HBsAg, we could not separate adult from children population (27, 28), one of them also including pregnant women (27). Similarly, for one study reporting anti-HCV antibody, adults and children were considered together (44). Those three studies were analyzed as adult population. Second, the study by Jean-Baptiste et al. and the Pan American Health Organization evaluating blood donors did not distinguish first time donors from repeat blood donors (34, 38); including regular blood donors in this group could cause an underestimation of the prevalence. Finally, we did not have enough studies to estimate prevalence of anti-HCV antibody for pregnant women, for PLHIV or to estimate the prevalence of HBsAg in children born after 2012.
In conclusion, this systematic review pooled prevalence for HBsAg and anti-HCV antibody among Haitian people. High prevalence of HBsAg in this population requires an urgent intervention such as increase in coverage of infant hepatitis B immunization, integration of birth dose vaccines, and prevention of mother-to-child transmission of HBV by antenatal screening and provision of peripartum antiviral prophylaxis. The prevalence of anti-HCV antibody was not as high as HBsAg, but still requires an immediate intervention as thousands of people could avoid having liver-related morbimortality in Haiti. This systematic review also identified an important knowledge gap; the prevalence of HDV needs to be evaluated in Haiti.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
Author contributions
JV and YS developed the study protocol and wrote the manuscript. JV performed the search and data analysis. JV and CN screened the articles and extracted the data. SW provided data. YM provided statistical support. All authors reviewed and agreed with the final version of the manuscript.
Funding
JV was funded by a postdoctoral fellowship by the Institut Pasteur, Ambassade de France au Japon, and Fondation Pasteur Japon. JV is supported by the the Agence Nationale de Recherche sur le SIDA, les Hépatites Virales et les Maladies Infectieuses Émergentes (ANRS-MIE).
Acknowledgments
We acknowledge the following authors for answering to our queries about study participants: Molly Franke, Mina Hosseinipour, Xin Sun, Giannina Izquierdo, Ruth Brogden, Jaymie Yango, and David B. Rein. We thank Simon Galmiche for his help retrieving papers.
Conflict of interest
YS has received a research grant from Gilead and research materials from Abbott Laboratories and Fujirebio Inc. YM has received research materials from Abbott Laboratories and Roche Molecular Diagnostics.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.1099571/full#supplementary-material
References
1. World Health Organization. Global Progress Report on HIV, Viral Hepatitis and Sexually Transmitted Infections. Geneva: WHO (2021).
3. World Health Organization. Global Health Sector Strategies on, Respectively, HIV, Viral Hepatitis and Sexually Transmitted Infections for the Period 2022-2030. Geneva: WHO (2022).
4. Tohme RA, Andre-Alboth J, Tejada-Strop A, Shi R, Boncy J, François J, et al. Hepatitis B virus infection among pregnant women in Haiti: a cross-sectional serosurvey. J Clin Virol Off Publ Pan Am Soc Clin Virol. (2016) 76:66–71. doi: 10.1016/j.jcv.2016.01.012
5. World Health Organization. Data Portal. Available online at: https://platform.who.int/data/maternal-newborn-child-adolescent-ageing/indicator-explorer-new/mca/hepatitis-b-(hepb3)-immunization-coverage-among-1-year-olds-(-) (accessed October 14, 2022).
6. World Health Organization. Prevention of Mother-to-Child Transmission of Hepatitis B Virus: Guidelines on Antiviral Prophylaxis in Pregnancy. (2020). Available online at: http://www.ncbi.nlm.nih.gov/pubmed/32833415 (accessed December 28, 2022).
7. Schweitzer A, Horn J, Mikolajczyk RT, Krause G, Ott JJ. Estimations of worldwide prevalence of chronic hepatitis B virus infection: a systematic review of data published between 1965 and 2013. Lancet (London, England). (2015) 386:1546–55. doi: 10.1016/S0140-6736(15)61412-X
8. Kowdley K V, Wang CC, Welch S, Roberts H, Brosgart CL. Prevalence of chronic hepatitis B among foreign-born persons living in the United States by country of origin. Hepatology. (2012) 56:422–33. doi: 10.1002/hep.24804
9. Wong RJ, Brosgart CL, Welch S, Block T, Chen M, Cohen C, et al. An updated assessment of chronic hepatitis B prevalence among foreign-born persons living in the United States. Hepatology. (2021) 74:607–26. doi: 10.1002/hep.31782
10. Collaborators PO. Global prevalence, treatment, and prevention of hepatitis B virus infection in 2016: a modelling study. Lancet Gastroenterol Hepatol. (2018) 3:383–403. doi: 10.1016/S2468-1253(18)30056-6
11. Sheena BS, Hiebert L, Han H, Ippolito H, Abbasi-Kangevari M, Abbasi-Kangevari Z, et al. Global, regional, and national burden of hepatitis B, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Gastroenterol Hepatol. (2022) 7:796–829. doi: 10.1016/S2468-1253(22)00124-8
12. Gower E, Estes C, Blach S, Razavi-Shearer K, Razavi H. Global epidemiology and genotype distribution of the hepatitis C virus infection. J Hepatol. (2014) 61:S45–57. doi: 10.1016/j.jhep.2014.07.027
13. Collaborators POH. Global change in hepatitis C virus prevalence and cascade of care between 2015 and 2020: a modelling study. Lancet Gastroenterol Hepatol. (2022) 7:396–415. doi: 10.1016/S2468-1253(21)00472-6
14. Stockdale AJ, Kreuels B, Henrion MYR, Giorgi E, Kyomuhangi I, de Martel C, et al. The global prevalence of hepatitis D virus infection: systematic review and meta-analysis. J Hepatol. (2020) 73:523–32. doi: 10.1016/j.jhep.2020.04.008
15. Miao Z, Zhang S, Ou X, Li S, Ma Z, Wang W, et al. Estimating the global prevalence, disease progression, and clinical outcome of hepatitis delta virus infection. J Infect Dis. (2020) 221:1677–87. doi: 10.1093/infdis/jiz633
16. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 2021:372. doi: 10.1136/bmj.n71
17. World Health Organization. Guidelines on Hepatitis B and C Testing. Geneva: WHO (2017). doi: 10.1007/s00216-014-7926-1
18. Evans AA, O'Connell AP, Pugh JC, Mason WS, Shen FM, Chen GC, et al. Geographic variation in viral load among hepatitis B carriers with differing risks of hepatocellular carcinoma. Cancer Epidemiol Biomarkers Prev. (1998) 7:559–65.
19. Hoy D, Brooks P, Woolf A, Blyth F, March L, Bain C, et al. Assessing risk of bias in prevalence studies: modification of an existing tool and evidence of interrater agreement. J Clin Epidemiol. (2012) 65:934–9. doi: 10.1016/j.jclinepi.2011.11.014
20. Schwarzer G. General Package for Meta-Analysis. Cham: Springer (2022). doi: 10.1007/978-3-319-21416-0
21. Ollé-Goig JE. Hepatitis B markers in patients with and without ascites in Haiti. Trop Doct. (1985) 15:148.
22. Malison MD, Kane MA, Johnson JM, Schable CA, Gridley MJ, Polkowski J, et al. seroprevalence survey of hepatitis B markers among Haitians in a southwest Florida farming community. Am J Public Health. (1985) 75:1094–5. doi: 10.2105/ajph.75.9.1094
23. Delage G, Montplaisir S, Remy-Prince S, Pierri E. Prevalence or hepatitis B virus infection in pregnant women in the Montreal area. Can Med Assoc J. (1986) 134:897–901.
24. Gordon SC, Reddy KR, Gould EE, McFadden R, O'Brien C, De Medina M, et al. The spectrum of liver disease in the acquired immunodeficiency syndrome. J Hepatol. (1986) 2:475–84. doi: 10.1016/S0168-8278(86)80059-9
25. Jonas ERS, O'Sullivan MJ, de Medina M, Reddy KR, Jeffers LJ, Fayne T, et al. Failure of Centers for Disease Control Criteria to identify hepatitis B infection in a large municipal obstetrical population. Ann Intern Med. (1987) 107:335–7.
26. Lange WR, Cone EJ, Jaffe JH. Study of Haitian Boat people shows prevalence of HBV and HIV markers. Public Health Rep. (1988) 103:98–9.
27. Schill H, Bruneau B, Le Page B, Humeau O, Grimault C, Tampreau V, et al. Seroprevalence of anti-HIV antibodies in a rural Haitian population. Bull Soc Pathol Exot. (1989) 82:308–15.
28. Rosenblum LS, Hadler SC, Castro KG, Lieb S, Jaffe HW. Heterosexual transmission of hepatitis B virus in Belle Glade, Florida. J Infect Dis. (1990) 161:407–11. doi: 10.1093/infdis/161.3.407
29. Boulos R, Ruff AJ, Nahmias A, Holt E, Harrison L, Magder L, et al. Herpes simplex virus type 2 infection, syphilis, and hepatitis b virus infection in Haitian women with human immunodeficiency virus type 1 and human T lymphotropic virus type I infections. J Infect Dis. (1992) 166:418–20. doi: 10.1093/infdis/166.2.418
30. Andernach IE, Nolte C, Pape JW, Muller CP. Slave trade and hepatitis B virus genotypes and subgenotypes in Haiti and Africa. Emerg Infect Dis. (2009) 15:1222–8. doi: 10.3201/eid1508.081642
31. Exantus J, Dall'Amico R. Nephrotic syndrome in Haitian children: about the prevalence and the evolution. Pediatr Nephrol. (2010) 25:1801. doi: 10.1007/s00467-0
32. Rein DB, Lesesne SB, O'Fallon A, Weinbaum CM. Prevalence of hepatitis B surface antigen among refugees entering the United States between 2006 and 2008. Hepatol. (2010) 51:431–4. doi: 10.1002/hep.23353
33. Ngongondo M, Miyahara S, Hughes MD, Sun X, Bisson GP, Gupta A, et al. Hepatotoxicity during isoniazid preventive therapy and antiretroviral therapy in people living with HIV with severe immunosuppression: a secondary analysis of a multi-country open-label randomized controlled clinical trial. J Acquir Immune Defic Syndr. (2018) 78:54–61. doi: 10.1097/QAI.0000000000001641
34. Jean Baptiste AE, Chevalier MS, Polo E, Noel E, Hulland EN, Archer WR. Trends in hepatitis B and hepatitis C seroprevalence among blood donors—Haiti, 2005–2014. ISBT Sci Ser. (2018) 13:150–7. doi: 10.1111/voxs.12427
35. Childs L, Adrien P, Minta AA, François J, Charles NPJ, Blot V, et al. Prevalence of chronic hepatitis B virus infection among children in Haiti, 2017. Am J Trop Med Hyg. (2019) 101:214–9. doi: 10.4269/ajtmh.19-0117
36. Izquierdo G, Bustos S, González Á, Córdova L, Riquelme P, Liendo F, et al. Screening of hepatitis B in high risk chilean and immigrant pregnant women: management of mother to child transmission [Cribado de virus de hepatitis B en mujeres embarazadas: Inmigrantes, y chilenas con conductas de riesgo]. Rev Chil Infectol. (2019) 36:576–84. doi: 10.4067/S0716-10182019000500576
37. Fuster F, Peirano F, Vargas JI, Zamora FX, López-Lastra M, Núñez R, et al. Infectious and non-infectious diseases burden among Haitian immigrants in Chile: a cross-sectional study. Sci Rep. (2020) 10:1–10. doi: 10.1038/s41598-020-78970-3
38. Pan American Health Organization. Supply of Blood for Transfusion in Latin America and Caribbean Countries 2016–2017. Washinton, DC: PAHO (2020). doi: 10.37774/9789275121719
39. Brogden R, Wang S, Xu B. Finding the missing millions: Integrating automated viral hepatitis screening in a hospital with care and treatment in a primary care setting. J Clin Oncol. (2021) 39(15_suppl):108. doi: 10.1200/JCO.2021.39.15_suppl.108
40. Xu B, Wang SH. Novel approaches to find the missing millions: community and emergency department (ED) hepatitis B screening with linkage to care in an integrated healthcare model. Gastroenterology. (2020) 158:S1317. doi: 10.1016/s0016-5085(20)33960-3
41. Wang S, Xu B, Brogden R, Huang S, Yango J, Gallipani A, et al. From emergency department automated hepatitis B & C screening to care and cure in a primary care practice. J Hepatol. (2020) 73:S829. doi: 10.1016/s0168-8278(20)32099-7
42. Franke MF, Khan P, Hewison C, Khan U, Huerga H, Seung KJ, et al. Culture conversion in patients treated with bedaquiline and/or delamanid. Am J Respir Crit Care Med. (2021) 203:111–9. doi: 10.1164/rccm.202001-0135OC
43. Jones PD, Gmunder K, Batrony S, Martin P, Kobetz E, Carrasquillo O. Acceptability and feasibility of home-based hepatitis B screening among haitian immigrants. J Immigr Minor Health. (2021) 23:1170–8. doi: 10.1007/s10903-021-01165-z
44. Allain JP, Hodges W, Einstein MH, Geisler J, Neilly C, Delaney S, et al. Antibody to HIV-1, HTLV-I, and HCV in three populations of rural Haitians. J Acquir Immune Defic Syndr. (1992) 5:1230–6.
45. Talarmin A, Kazanji M, Cardoso T, Pouliquen JF, Sankale-Suzanon J, Sarthou JL. Prevalence of antibodies to hepatitis A, C, and E viruses in different ethnic groups in French Guiana. J Med Virol. (1997) 52:430–5. doi: 10.1002/(sici)1096-9071(199708)52:4<430::aid-jmv15>3.0.co;2-k
46. Hepburn MJ, Lawitz EJ. Seroprevalence of hepatitis C and associated risk factors among an urban population in Haiti. BMC Gastroenterol. (2004) 4:31. doi: 10.1186/1471-230X-4-31
47. Lingani M, Akita T, Ouoba S, Sanou AM, Sugiyama A, Tarnagda Z, et al. High prevalence of hepatitis B infections in Burkina Faso (1996–2017): a systematic review with meta-analysis of epidemiological studies. BMC Public Health. (2018) 18:1–11. doi: 10.1186/s12889-018-5432-7
48. B E, Ou P, Ouoba S, Hussain MRA, Ko K, Nagashima S, et al. Prevalence and genotype distribution of viral hepatitis B in Cambodia between 1990 and 2020: a systematic review and meta-analysis. Arch Public Health. (2022) 80:119. doi: 10.1186/s13690-022-00880-9
49. Ajuwon BI, Yujuico I, Roper K, Richardson A, Sheel M, Lidbury BA. Hepatitis B virus infection in Nigeria: a systematic review and meta-analysis of data published between 2010 and 2019. BMC Infect Dis. (2021) 21:1120. doi: 10.1186/s12879-021-06800-6
50. Kafeero HM, Ndagire D, Ocama P, Kudamba A, Walusansa A, Sendagire H. Prevalence and predictors of hepatitis B virus (HBV) infection in east Africa: evidence from a systematic review and meta-analysis of epidemiological studies published from 2005 to 2020. Arch Public Health. (2021) 79:167. doi: 10.1186/s13690-021-00686-1
51. Wang H, Men P, Xiao Y, Gao P, Lv M, Yuan Q, et al. Hepatitis B infection in the general population of China: a systematic review and meta-analysis. BMC Infect Dis. (2019) 19:811. doi: 10.1186/s12879-019-4428-y
52. The World Bank. The World Bank Data. (2022). Available online at: https://data.worldbank.org/indicator/SP.POP.TOTL?locations=HT (accessed October 25, 2022).
53. Boucheron P, Lu Y, Yoshida K, Zhao T, Funk AL, Lunel-Fabiani F, et al. Accuracy of HBeAg to identify pregnant women at risk of transmitting hepatitis B virus to their neonates: a systematic review and meta-analysis. Lancet Infect Dis. (2021) 21:85–96. doi: 10.1016/S1473-3099(20)30593-4
54. Moutchia J, Njouom R, Rumpler E, Besombes C, Texier G, Tejiokem M, et al. Maternal age at first childbirth and geographical variation in HBV prevalence in Cameroon: important role of mother-to-child transmission. Clin Infect Dis. (2021). doi: 10.1093/cid/ciab548
55. Ott JJ, Stevens GA, Wiersma ST. The risk of perinatal hepatitis B virus transmission: hepatitis B e antigen (HBeAg) prevalence estimates for all world regions. BMC Infect Dis. (2012) 12:1–9. doi: 10.1186/1471-2334-12-131
56. Shimakawa Y, Lemoine M, Njai HF, Bottomley C, Ndow G, Goldin RD, et al. Natural history of chronic HBV infection in West Africa: a longitudinal population-based study from the Gambia. Gut. (2016) 65:2007–16. doi: 10.1136/gutjnl-2015-309892
57. Liu J, Zhang S, Liu M, Wang Q, Shen H, Zhang Y. Maternal pre-pregnancy infection with hepatitis B virus and the risk of preterm birth: a population-based cohort study. Lancet Glob Health. (2017) 5:e624–32. doi: 10.1016/S2214-109X(17)30142-0
58. Whittle H, Inskip H, Bradley AK, McLaughlan K, Shenton F, Lamb W, et al. The pattern of childhood hepatitis B infection in two Gambian villages. J Infect Dis. (1990) 161:1112–5. doi: 10.1093/infdis/161.6.1112
59. Shimakawa Y, Lemoine M, Bottomley C, Njai HF, Ndow G, Jatta A, et al. Birth order and risk of hepatocellular carcinoma in chronic carriers of hepatitis B virus: a case-control study in The Gambia. Liver Int. (2015) 35:2318–26. doi: 10.1111/liv.12814
Keywords: Haiti, hepatitis B, hepatitis C, hepatitis D, prevalence, epidemiology, elimination
Citation: Vincent JP, Nyamasege C, Wang S, Madec Y and Shimakawa Y (2023) Prevalence of hepatitis B, C, and D virus infection in Haiti: A systematic review and meta-analysis. Front. Public Health 10:1099571. doi: 10.3389/fpubh.2022.1099571
Received: 15 November 2022; Accepted: 22 December 2022;
Published: 11 January 2023.
Edited by:
Krzysztof Tomasiewicz, Medical University of Lublin, PolandReviewed by:
Antonio Rivero-Juarez, Maimonides Biomedical Research Institute of Cordoba (IMIBIC), SpainMaria Gabriella Verso, University of Palermo, Italy
Copyright © 2023 Vincent, Nyamasege, Wang, Madec and Shimakawa. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jeanne Perpétue Vincent,  amVhbm5lLnZpbmNlbnRAcGFzdGV1ci5mcg==; Yusuke Shimakawa, eXVzdWtlLnNoaW1ha2F3YUBnbWFpbC5jb20=
amVhbm5lLnZpbmNlbnRAcGFzdGV1ci5mcg==; Yusuke Shimakawa, eXVzdWtlLnNoaW1ha2F3YUBnbWFpbC5jb20=