 Nicolas Vignier1,2,3,4,5*
Nicolas Vignier1,2,3,4,5* Sohela Moussaoui1,3,6
Sohela Moussaoui1,3,6 Antoine Marsaudon1Jérome Wittwer6Florence Jusot1,7
Antoine Marsaudon1Jérome Wittwer6Florence Jusot1,7 Paul Dourgnon1
Paul Dourgnon1- 1Institut de recherche et documentation en économie de la santé, IRDES, Paris, France
- 2Centre d'Investigation Clinique Antilles Guyane, CIC INSERM 1424, Centre hospitalier de Cayenne, Cayenne, French Guiana
- 3Sorbonne Université, INSERM UMR 1136, Institut Pierre Louis d'Épidémiologie et de Santé Publique, IPLESP, Department of Social Epidemiology, Paris, France
- 4French Collaborative Institute on Migration, Institut Convergences Migrations, ICM, Aubervilliers, France
- 5Université Sorbonne Paris Nord, UFR SMBH, IAME, INSERM UMR 1137, Hôpital Avicenne, Hôpitaux Universitaires Paris Seine-Saint-Denis, AP-HP, Department of Infectious and Tropical diseases, Bobigny, France
- 6Bordeaux University, Bordeaux Population Health, INSERM U1219, Economic and Management of Healthcare Organizations Team, Emos Team, Bordeaux, France
- 7Université Paris-Dauphine, PSL-Research University, Leda-Legos, Paris, France
Introduction: An increase in migration rates to the European Union has been observed over the last few years. Part of these migrants is undocumented. This work aimed to describe the reported frequency of infectious diseases and their associated factors among unselected samples of undocumented migrants in France.
Methodology: The Premier Pas survey is a cross-sectional epidemiological survey of a random sample (two-stage sample design) conducted among undocumented migrants recruited in Paris and the Bordeaux region, in places and facilities likely to be frequented by undocumented migrants. The percentages were weighted. The analysis was performed using Stata 15.1 software.
Results: A total of 1,223 undocumented migrants were recruited from 63 places and facilities, with a participation rate of 50%. Most of them were between 30 and 40 years of age (36%), 69% were men, aged mainly 30–40 (36%) years old, from sub-Saharan Africa (60%) or North Africa (25%), and 60% had arrived <3 years earlier. Among the participants, 24.8% declared a poor perceived health status and 33.5% a chronic health condition. Dental infections concerned 43.2% of the participants. Apart from dental issues, 12.9% reported suffering from at least one infectious disease: HIV infection (3.5%), chronic hepatitis B virus infection (3.1%), upper respiratory tract infection (1.7%), skin mycosis (1.2%), skin and soft tissue infection (0.8%), chronic hepatitis C infection (0.8%), urinary tract infection (0.7%), lower respiratory tract infection (0.7%), scabies (0.3%), tuberculosis disease (0.2%), vaginal mycosis (0.6%), and herpes (0.1%). Regarding HIV, HBV, and HCV infections, 56, 71, and 89%, respectively, were diagnosed after their arrival. Chronic viral infections were more often reported by undocumented migrants from sub-Saharan Africa and Latin America. In multivariate analysis, a higher risk of reporting chronic viral infection was observed among people food insecure.
Conclusion: This original study on a large random sample confirms the frequency of infectious diseases among undocumented migrants in France and the importance of integrating their screening during a health Rendezvous and their management into early access to care and inclusive medico-psycho-social management.
Introduction
The international organization of migration (IOM) defined a migrant as a person who moves away from his or her place of usual residence, whether within a country or across an international border, temporarily or permanently, and for a variety of reasons (1). With 281 million migrants in the world in 2020, ~3.6% of the world population living outside their usual residences (2). Increased rates of migration to the European Union were observed over the last few years. Currently, ~10% of the population of the WHO European Region is estimated to be migrants (3). Migration is a growing phenomenon, influencing the health and development of both migrant and host communities.
Migrants generally do not represent a threat to the health of the host population (4). However, some subgroups of migrants are particularly vulnerable to infectious diseases and may be less well-cared for as compared to the host population (4–8).
Part of these migrants is undocumented [i.e., persons born abroad, of foreign nationality, and who have no right of residence in the country of residence (9, 10)]. Limited data are available in Europe and France on the health of undocumented immigrants (9, 11, 12). It was estimated that 1.9–3.8 million undocumented migrants live in the European Union (EU) (11). Despite the existence in France of social assistance for health cover for undocumented migrants (the State Medical Aid, AME), it is estimated that 49% of eligible undocumented migrants have not applied for their rights in Paris and the Bordeaux area (13). There were 315,000 AME beneficiaries in 2019. Several studies in Europe highlight their poor perceived health, poorest health-related quality of life, poor mental health, food insecurity, and cumulative health problems, namely, metabolic, musculoskeletal, and digestive disorders (14–16).
According to the data from the healthcare system and NGOs, undocumented migrants are unequally affected by infectious and tropical diseases in relation to the epidemiology in the countries of origin and poor living conditions in the host countries (11, 17, 18). A recent study observed an increase in ICU admissions in France for undocumented migrants, who were younger and more severely ill than other patients admitted (19).
However, no study has assessed the frequency of these infectious diseases in an unselected sample of undocumented migrants. Studies, to date, rely only on data collected in healthcare places dedicated to vulnerable populations. We improve upon the existing dataset by collecting information on various places of assistance (e.g., administrative, health, cultural, food, and housing) dedicated to vulnerable populations (13, 20, 21). This study, based on multidisciplinary approaches, aims to better understand the experience of undocumented migrants living in France regarding their health status and access to rights and healthcare.
The present work aimed to describe the reported frequency of infectious diseases, the location of their diagnosis, and their associated factors among undocumented migrants in France.
Methods
Type of study and sampling
The Premier Pas survey is a cross-sectional epidemiological survey of a random sample (two-stage sample design) of undocumented migrants recruited in Paris and the Bordeaux area in places and facilities likely to be frequented by undocumented migrants, between February and April 2019 (20). A first sampling constituted a sample of places and structures likely to be frequented by undocumented immigrants. A sample of organizations was subsequently drawn from the list compiled in the first stage. Information on attendance was collected in a pre-survey of the facilities. The “Structures” survey was conducted by telephone with 736 sites and organizations. The list comprised sites and organizations in central Paris, Bordeaux, and communes in the city's suburbs (Cenon, Lormont, Mérignac, Pessac, and Talence). It was compiled from sources available to the migrants, and listed in local resources for deprived individuals and migrants. These public sources were complemented by several associative sources that provided a broad representation of the services available to the individuals studied in the survey. This approach was not intended to be comprehensive; it was reproducible and was based on identical sources in Paris and Bordeaux; 87% of the organizations contacted, that catered to undocumented immigrants, agreed to participate in the survey. In the sample of surveyed organizations, we selected all the 113 organizations that declared they had at least 20 eligible users a week in the “Structures.” A total of 63 (56%) of the 113 selected organizations agreed to have the survey conducted on their premises.
In a second stage, organizations were sampled, asked to participate, and if they agreed, a sample of undocumented immigrants was recruited in the selected places. Inclusion criteria were to be undocumented, living in France and to be over 18 years old. Fourteen different languages were used to translate the questionnaire and interact with participants. The detailed methodology has been described elsewhere (15, 16). The structures included “Espace Solidarité Insertion” which is a structure offering a daytime shelter and social and health services to people living on the streets of Paris, NGOs, free outpatient health clinics (“Permanence d'Accès aux Soins de Santé”), which are mostly inside hospitals and provide free medical care and social assistance to vulnerable populations; the local health insurance centers (“Caisses Primaires d'Assurance Maladie”), which operates at a departmental level and deal with several benefits/allowances for insured people such as sickness, pregnancy, invalidity or death, and shower baths; the free health centers of Doctors of the Word NGO (“CASO”); the Point of Access to Rights (“Point d'accès aux droits”), which is a free and permanent reception area providing information, orientation, and local advice in response to legal or administrative problems; and maternal and child protection centers (“Protection Maternelle et Infantile”), which is a departmental service responsible for ensuring the health protection of mothers and children and other places. The Paris region was chosen because it is the region that faces most of the new migrant arrivals in France and where the accommodation and support structures are congested. Bordeaux is a place of arrival for migrants and adds to the study the representativeness of a small metropolis concerned by migration, with probably more means to accompany them.
Data collection
In total, 21 interviewers were recruited and trained directly by the team that designed the survey, 18 of whom covered the Paris area and 3 of whom covered the Bordeaux area. All of them spoke English and more than 75% of them also spoke another language in which they were able to conduct the questionnaire. Most of the interviewers were social sciences graduates. A complete range of socioeconomic indicators was collected, namely, age, gender, social characteristics, migration characteristics, social isolation, material living conditions, access to care, and the place of recruitment. Educational level was defined as the number of years at school. In addition, participants were asked if they were currently experiencing infectious diseases or other health conditions. Questions about health problems were understood at the time of the survey. If the individual answered yes to one of the conditions, more specific questions were asked to specify the disease or the symptom. For each condition, the time of diagnostic before or after the arrival in France and diagnostic modalities were assessed. Dental pain and missing or broken teeth or infected teeth (cavities) status were collected. Participants were also asked if they had skin or gynecological problems. A detailed list of infectious diseases was also sought.
Data analysis
First, we described the prevalence of infectious diseases by frequency order using percentages. Infectious diseases have been validated and reclassified by senior medical doctors and specialists in infectious and tropical diseases. The major diseases were compared by gender using a chi-square test. Data were weighted based on the probability of inclusion. The weighting considered the sampling plan and types of organizations and services provided to users. The collection of each respondent who visits the participating organizations enabled multiple inclusions to be considered in the weights' calculation. We calculated survey weights by taking into account the facility type, attendance, and type of services provided. More precisely, we collect the weekly average number of undocumented immigrants attending each of these places. For each place, we then weight undocumented immigrants according to this average number. That is, we compensate for a deviation from this average by giving higher (lower, respectively) weights for those that are below (above, respectively) the weekly average. The percentages were weighted using those weights. The percentages presented are based on the data reported. Numbers without missing data are systematically reported.
Then we performed univariate and multivariate analyses using logistic regression for having declared at least one chronic viral infection (HIV, HBV, or HCV). Associations were expressed using odds ratios (ORs) with 95% CIs. The multivariate analysis by logistic regression used a stepwise backward variable selection method with a p-value threshold of 5%. All analyses have been performed with Stata© 15.1 software (StataCorp, College Station, TX, USA).
Ethics and funding
Participation in the survey was free and anonymous. No information was transmitted to any administration. The information collected in the survey was only used by researchers. The study was carried out by the French Institute for Research and Documentation in Health Economics (IRDES, Institut de recherche et documentation en économie de la santé) under the supervision of the French Data Protection Authority (CNIL), which guarantees respect for anonymity, privacy, and the protection of personal data. The project was supported by the French National Research Agency (Agence Nationale de la Recherche, ANR) through the 2015 Generic ANR Call for Projects.
Result
A total of 1,223 undocumented migrants were recruited in Paris (86%) and the Bordeaux (14%) area, in 63 places and structures (selected from 736 places and structures listed). The places of recruitment were associations (44%), solidarity and integration spaces (12.7%), shower-baths (9.5%), free health centers (9.5%), health centers (9.5%), and health insurance centers (6.3%), Doctor of the World NGO (3.2%), maternal and child protection centers (3.2%), social action centers (1.6%), family planning centers (1.6%), and access to rights points (1.6%). The participation rate of the organizations approached was 56%, and of eligible migrants was 49%. The interview was mainly conducted in French (75%), English (7%), Arabic (8%), or Spanish (4%). The language barrier was an obstacle in only 5% of the cases.
The sample was composed of 69% men, aged mainly 18–30 (32%) or 30–40 (36%) years old participants, from sub-Saharan Africa (60%), North Africa (25%), or Latin America (7%); 27% had arrived in France less than a year before, 33% had arrived in France 1–3 years before, and 26% had arrived in France more than 5 years before (Table 1).
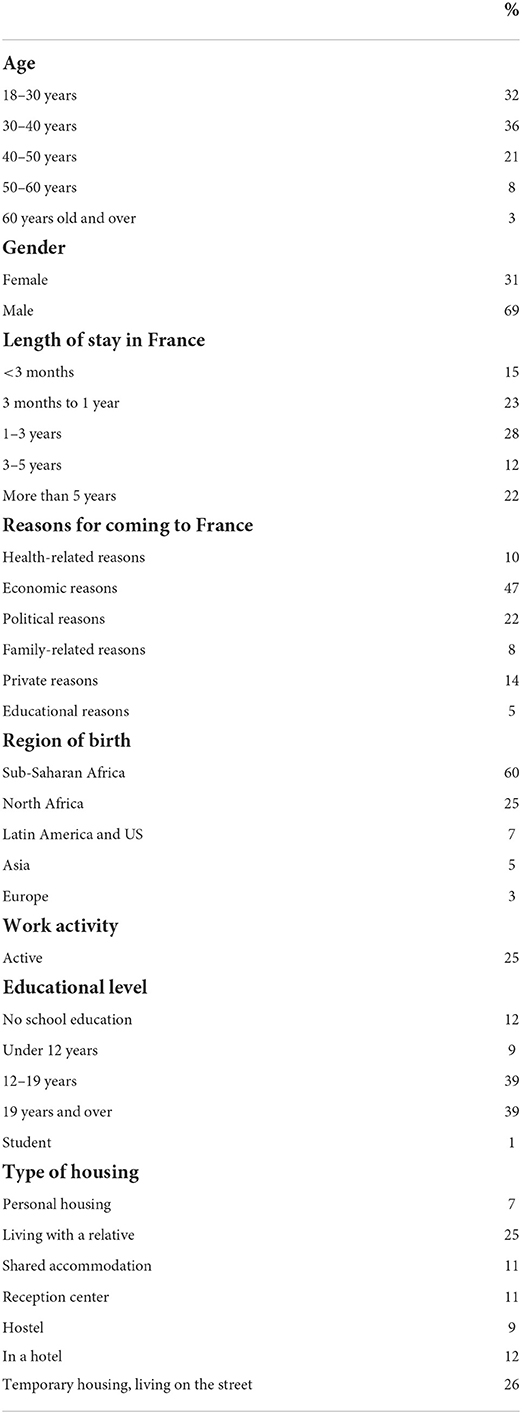
Table 1. Sociodemographic characteristics of undocumented migrants in Paris and Bordeaux, Premier Pas survey (n = 1.223).
Among the participants (n = 1.219), 24.8% declared a poor or very poor perceived health status, 22.2% an average status, and 53.0% a good or very good health status. A chronic health condition or disease (infectious or non-infectious) was reported by 33.5% of respondents (n = 1.219). In addition, 68.2% (432/1,189) reported an acute health issue or disease at the time of the survey (Figure 1).
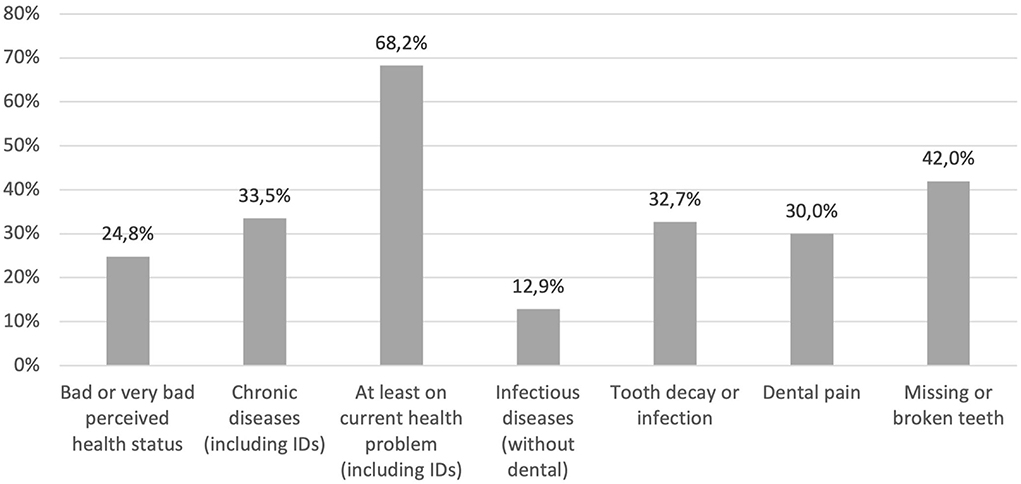
Figure 1. Frequency of health problems and infectious diseases among undocumented migrants in Paris and Bordeaux, Premier Pas survey (n = 1.188).
Dental infections (cavities, infection, or pain) concerned 43.2% of the participants: 32.7% cavities or infection, and 30.0% dental pain. As cavities may no longer be an active infection process, this percentage may overestimate the frequency of active infections. Moreover, 42.0% had broken or missing teeth. So, a total of 58.5% had a present or past dental disorder.
Besides these dental issues, 12.9% reported suffering from at least one other current infectious disease: HIV infection (3.5%), chronic hepatitis B infection (3.1%), upper respiratory tract infection (1.7%), skin mycosis (1.2%), skin and soft tissue infection (0.8%), chronic hepatitis C infection (0.8%), urinary tract infection (0.7%), lower respiratory tract infection (0.7%), scabies (0.3%), tuberculosis disease (0.2%), vaginal mycosis 0.6%, and herpes 0.1%. In addition, 7.9% of the respondent reported a skin disorder without the infectious or non-infectious nature being specified.
Regarding HIV, HBV, and HCV infections, 56, 71, and 89%, respectively, reported having been diagnosed after their arrival in France. This was also the case for all the few cases of tuberculosis disease.
Human immunodeficiency virus (HIV) infection was more frequent for participants from sub-Saharan Africa (2.3%) and America than among those of North African origin (0.3%) (p < 0.001) (Table 2). Conversely, no statistically significant difference was reported for chronic infection by HBV or HCV according to country of origin. The association with the other covariates is detailed in Table 2.
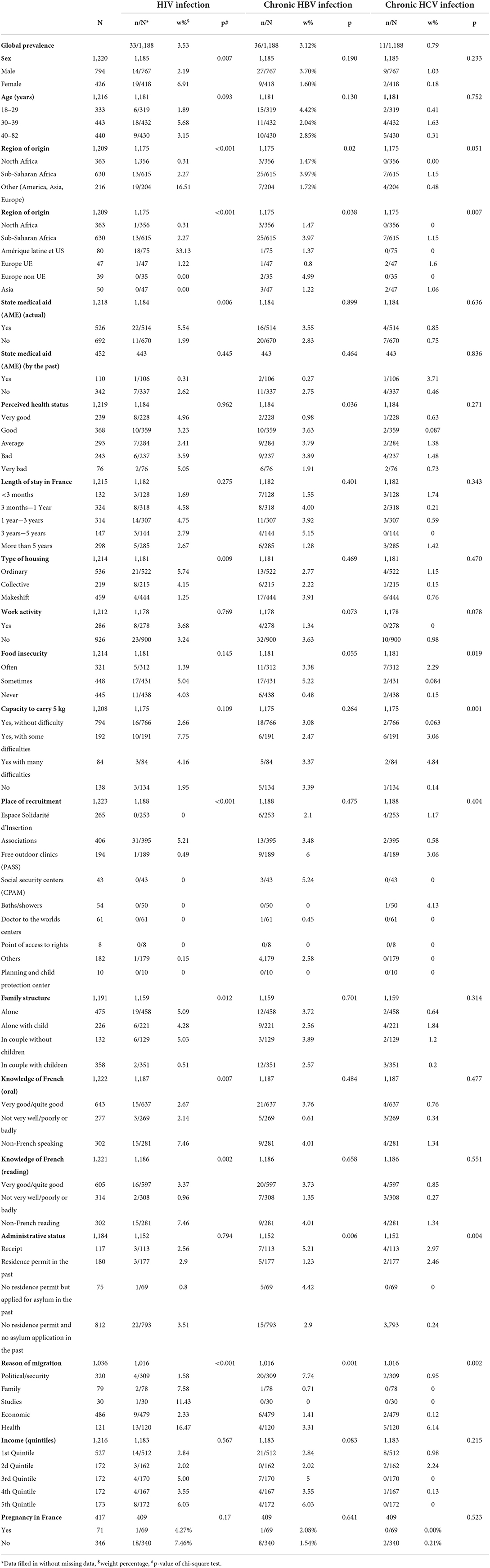
Table 2. Reported prevalence of chronic viral infections (HIV, HBV, or HCV infection) among undocumented migrants in Paris and Bordeaux according to sociodemographic characteristics, Premiers Pas survey (n = 1.167).
Chronic viral infections were more often reported by undocumented migrants from sub-Saharan Africa and Latin America (Table 3). In multivariate analysis, a higher risk of reporting chronic viral infection was observed among people coming from Latin America and Europe, among the food insecure, among those recruited from an association, a free health center, or a social security center, and for single persons with children or couples without children. The association with South American origin is mainly driven by a higher prevalence of HIV among people from South America which will be discussed below (Figure 2). Conversely, people who had migrated for economic reasons and those who had never applied for a residence permit or asylum in France were less likely to report a chronic viral infection (Table 3).
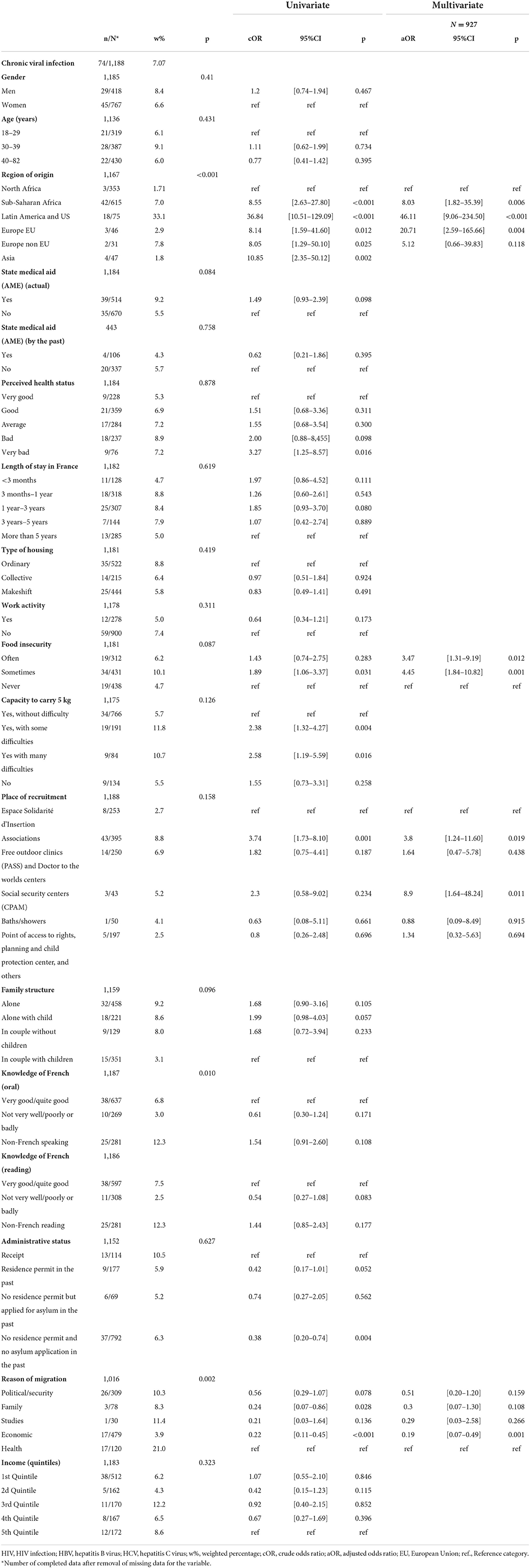
Table 3. Reported prevalence of chronic viral infections (HIV, HBV, or HCV infection) among undocumented migrants in Paris and Bordeaux, univariate and multivariate analyses with backward stepwise logistic regression (p = 0.05 threshold), Premiers Pas survey (n = 1,188).
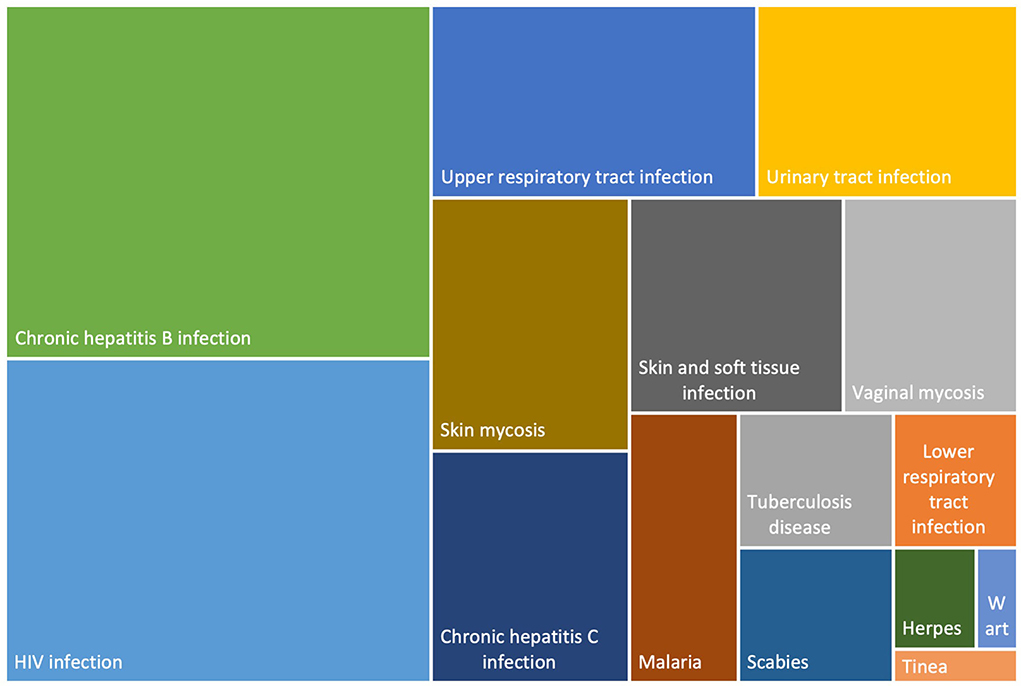
Figure 2. Distribution of infectious diseases among undocumented migrants in Paris and Bordeaux, Premier Pas survey (n = 1.188).
In terms of prevention of infectious diseases, 54.7% reported having been tested for HIV since arriving in France and 46.2% have had a chest X-ray for tuberculosis disease screening. Catch-up vaccination was started in only 35.4% of participants.
Discussion
This original study on the frequency of infectious diseases among undocumented migrants in Bordeaux and Paris highlights the healthcare needs of this vulnerable population.
The study reports a high prevalence of dental abnormalities and infections, a public health issue that is often neglected in studies of migrant health. A review of studies analyzing the oral health status of migrants from middle-income and low-income countries to Europe reported a high prevalence of caries experience and lack of dental health in the host countries (22). A recent study has been conducted in France in a health center offering dental consults to migrants (23). In this study, of the migrants who were assessed by a dentist, 72.3% of migrants had cavities and 59% needed extensive oral care.
The concern around infectious diseases and migration is an issue, as migrants are disproportionately exposed to infectious and tropical diseases (4). This includes an increased risk of COVID-19, HIV, hepatitis B, tuberculosis, schistosomiasis, and malaria (11, 24, 25). This issue is linked to the epidemiology of infectious diseases in the countries of origin, but also to poor conditions of migration resulting in exposure to infectious diseases and, in some countries, to the lack of access to a healthcare system and to insurance coverage among migrants (12, 17, 26, 27). Existing evidence from different countries highlights the difficulties that migrants face in accessing health services, which contributes to the burden of excess morbidity and mortality faced by migrants (9, 28–30).
Participants frequently reported common infectious diseases including skin and soft tissue infections, upper air tract infections, urinary, and gynecological infections (31–34). This is in line with the findings of other work carried out among the migrant populations. These infections may be linked to poor living conditions and sexual vulnerability that some migrants in deprived situations may experience.
Migrants are a key population affected by HIV (8). While the prevalence of HIV infection is linked to the prevalence in the country of origin, it has been shown that precariousness and poor migration conditions increase the risk of acquiring HIV after arrival in the country of destination (35). It is likely that the prevalence of HIV infections has been overrepresented here in connection with better social and healthcare support for this population, and therefore a higher chance of being met in the partner facilities. France is a French-speaking country. Migration from South America, the majority of which is Spanish speaking, is limited in number and most often concerns migration for professional or family reasons of people in a regular administrative situation. On the other hand, France is home to a community of transgender sex workers women often living with HIV (36). Some of them are accompanied by a part of the Parisian investigation structures. Despite these selection biases, the study's sample remains original in terms of its size and the diversity of the recruitment sites used. It is also important to learn that most HIV infections were diagnosed after their arrival on the territory. This should be weighed against the risk of being infected by HIV after arrival, which is estimated in France at up 50% (35).
Tuberculosis is a rare disease in Europe where migrants represent a large part of residual cases (6). Tuberculosis in migrants is commonly the result of reactivation of latent infection with the bacteria Mycobacterium tuberculosis acquired outside the host country. Without treatment, it is possibly a serious illness. It is also the most advanced disease that can become contagious. An early diagnosis and access to healthcare are therefore essential to prevent complications and secondary transmissions. Tuberculosis can be detected before the onset of the disease by screening for latent tuberculosis infection. Our results confirm the relative rarity of visible diagnosed tuberculosis, without prejudging the frequency of latent forms.
Parasitic diseases are frequent among migrants from endemic countries and can reveal themselves through symptoms, in particular digestive symptoms. Malaria is an important febrile disease that is mainly observed in travelers visiting migrants to non-endemic countries (37). Other parasitic diseases can be asymptomatic but carry significant morbidity, such as schistosomiasis and strongyloidiasis (38). It is therefore likely that these infections are underestimated in this study, which is declarative because they are asymptomatic and not diagnosed.
Similarly, HTLV1 infection, which is most often asymptomatic, is largely unrecognized and underscreened among migrants in host countries (39). It was therefore predictable that it would not be measured in this study. However, it is an infection that can be transmitted through sexual intercourse or breastfeeding and can be complicated by leukemia or severe neurological damage.
Even though our study took place just before the pandemic, people living in precarious or overcrowded conditions, including undocumented migrants, have been more severely impacted by the COVID-19 pandemic (40, 41). As with other vaccine-preventable diseases, ensuring equitable and unconditional access to vaccination uptake and ensuring hygiene is the first step in preventing these respiratory viruses.
The association between food insecurity and increased incidence of chronic viral infections is of concern. In the same study, it was shown that food insecurity was a key factor in the likelihood of developing post-traumatic stress disorder (42). Systematic detection of hunger and insecurity in terms of access to sufficient food in quantity and quality should be systematic.
This survey has several limitations. Despite the resources deployed, the language barrier may have remained an obstacle in a small proportion of cases. However, the main countries of origin were well-represented with an adapted interpreting offer. Despite the inclusion of key places and structures in the support of migrants in Paris and Bordeaux, the sample may misrepresent the migrants furthest from the structures or not be visible in the public space. Furthermore, as health and social support contribute to access to care and screening, the prevalence of infectious diseases may have been overestimated. The declarative health status is an important limitation of this work as it exposes classification bias and lack of awareness of undiagnosed pathologies. Moreover, a study based on declarative status is not as valuable as a study based on a thorough medical examination, especially in the absence of biological and radiological screening for asymptomatic conditions.
This survey also has many strengths. The interviews were conducted in the migrant's language by interviewers trained in public health and listening. Acceptability was good. The size of the sample is large. The diversity of the structures surveyed contributes to the representativeness of the sample. Systematic questioning on all major symptoms and disease families reduces the risk of reporting bias.
Conclusion
This survey conducted in France on the health of undocumented migrants highlights the frequency of infectious diseases among undocumented migrants. Systematic screening for symptoms suggestive of infectious diseases offers a comprehensive health check-up within 4 months of arrival, vaccine catch-up, and the extensive use of diversified prevention tools in an unconstrained framework are key elements of risk reduction (43). This check-up contributes to the diagnosis of combined infections. The precise contours of the deployment of this health check-up in the various places and structures welcoming newcomer migrants are still under construction. The identification of factors associated with the prevalence of chronic viral infections is thus likely to contribute to the prioritization of people and structures where the health check-up should be deployed. Given the links with food insecurity, it seems interesting to deploy this offer within solidarity grocery shops and social structures. In addition, the already existing link between the social security centers and the health examination centers should be strengthened.
Early diagnosis and case management of infectious diseases are compulsory. Access to healthcare for undocumented migrants is thus essential. Information and the implication of community actors about infectious diseases lead to the empowerment of migrants in terms of health, in addition to protecting them. Prevention programs should ensure that all migrants are provided with free and facilitated access to repeated HIV testing, linkage to care and treatment if they are HIV positive, and pre-exposure prophylaxis for HIV-negative migrants if relevant. The implementation of a health rendezvous offered to all and integrating a broad clinicobiological screening of prevalent infectious diseases is advisable (44). To reach migrants who are far from the healthcare system, mobile public health teams would be recommended. More generally, the prevention of infectious diseases and their consequences among migrants is based on a reduction of poverty and social exclusion, equitable access to healthcare, prevention measures, and social services, and a culturally sensitive patient-centered approach (45). In this respect, the recent setbacks in French law on access to healthcare for undocumented migrants are worrying (46). A complementary infectious diseases seroprevalence survey of a representative sample of undocumented migrants would be useful to highlight these findings and clarify the objectives of the health check-ups. Infectious disease screening and prevention programs are likely to have an important role in improving the health and social determinants of health for newly arrived and settled undocumented migrants.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Institute for Research and Documentation in Health Economics. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author contributions
JW, FJ, and PD: conceptualization. NV, SM, and PD: methodology and data processing. NV: writing—original draft. All authors writing—review and editing.
Funding
This work was funded by French National Research Agency (Agence nationale de la recherche, ANR).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. About, Migration. International Organization for Migration. Available online at: https://www.iom.int/about-migration (accessed April 30, 2022).
2. Data Research. International Organization for Migration. Available online at: https://www.iom.int/data-and-research (accessed April 30, 2022).
3. Migration and Health in the European Region. Available online at: https://www.euro.who.int/en/health-topics/health-determinants/migration-and-health/migration-and-health-in-the-european-region (accessed April 30, 2022).
4. ECDC issues migrant screening vaccination guidance. European Centre for Disease Prevention and Control. (2018). Available online at: https://www.ecdc.europa.eu/en/news-events/ecdc-issues-migrant-screening-and-vaccination-guidance (accessed April 30, 2022).
5. Bergevin A, Husain M, Cruz M, Blanc CL, Dieme A, Girardin ML, et al. Medical check-up of newly arrived unaccompanied minors: A dedicated pediatric consultation service in a hospital. Arch Pediatr. (2021) 28:689–95. doi: 10.1016/j.arcped.2021.09.012
6. Ködmön C, Zucs P, van der Werf MJ. Migration-related tuberculosis: epidemiology and characteristics of tuberculosis cases originating outside the European Union and European Economic Area, 2007 to 2013. Euro Surveill. (2016) 21:30164. doi: 10.2807/1560-7917.ES.2016.21.12.30164
7. Rossi C, Shrier I, Marshall L, Cnossen S, Schwartzman K, Klein MB, et al. Seroprevalence of chronic hepatitis B virus infection and prior immunity in immigrants and refugees: a systematic review and meta-analysis. PLoS ONE. (2012) 7:e44611. doi: 10.1371/journal.pone.0044611
8. Prosser AT, Tang T, Hall HI. HIV in persons born outside the United States, 2007-2010. JAMA. (2012) 308:601–7. doi: 10.1001/jama.2012.9046
9. Gray BH, van Ginneken E. Health care for undocumented migrants: European approaches. Issue Brief Commonw Fund. (2012) 33:1–12. Available online at: https://www.commonwealthfund.org/sites/default/files/documents/___media_files_publications_issue_brief_2012_dec_1650_gray_hlt_care_undocumented_migrants_intl_brief.pdf
10. Words, Matter: Illegal vs Undocumented Migrants ∙ PICUM. PICUM. Available online at: https://picum.org/words-matter/ (accessed June 13, 2022).
11. De Vito E, De Waure C, Specchia ML, Ricciardi W. Public Health Aspects of Migrant Health: A Review of the Evidence on Health Status for Undocumented Migrants in the European Region. World Health Organisation Regional Office for Europe. Copenhagen: WHO (2015).
12. André JM, Azzedine F. Access to healthcare for undocumented migrants in France: a critical examination of state medical assistance. Public Health Rev. (2016) 37:5. doi: 10.1186/s40985-016-0017-4
13. Jusot F, Dourgnon P, Wittwer J, Sarhiri J. Access to state medical aid by undocumented immigrants in France first findings of the Premiers pas survey. Questions d'économie de la santé. (2019). 1–8. Available online at: https://www.irdes.fr/english/issues-in-health-economics/245-access-to-state-medical-aid-by-undocumented-immigrants-in-france-first-findings-of-the-premiers-pas-survey.pdf
14. Fakhoury J, Burton-Jeangros C, Guessous I, Consoli L, Duvoisin A, Jackson Y. Self-rated health among undocumented and newly regularized migrants in Geneva: a cross-sectional study. BMC Public Health. (2021) 21:1198. doi: 10.1186/s12889-021-11239-0
15. Andersson LMC, Hjern A, Ascher H. Undocumented adult migrants in Sweden: mental health and associated factors. BMC Public Health. (2018) 18:1369. doi: 10.1186/s12889-018-6294-8
16. Jackson Y, Paignon A, Wolff H, Delicado N. Health of undocumented migrants in primary care in Switzerland. PLoS ONE. (2018) 13:e0201313. doi: 10.1371/journal.pone.0201313
17. Desgrées-du-Loû A, Pannetier J, Ravalihasy A, Le Guen M, Gosselin A, Panjo H, et al. Is hardship during migration a determinant of HIV infection? Results from the ANRS PARCOURS study of sub-Saharan African migrants in France. AIDS. (2016) 30:645–56. doi: 10.1097/QAD.0000000000000957
18. Coppola N, Alessio L, Gualdieri L, Pisaturo M, Sagnelli C, Caprio N, et al. Hepatitis B virus, hepatitis C virus and human immunodeficiency virus infection in undocumented migrants and refugees in southern Italy, January 2012 to June 2013. Euro Surveill. (2015) 20:30009. doi: 10.2807/1560-7917.ES.2015.20.35.30009
19. Hraiech S, Pauly V, Orleans V, Auquier P, Boyer L, Papazian L, et al. Undocumented migrants in French intensive care units in 2011-2018: retrospective nationwide study. Intensive Care Med. (2022) 48:290–9. doi: 10.1007/s00134-021-06606-9
20. Dourgnon P, Guillaume S, Jusot F, Wittwer J. A study of undocumented immigrants' access to health coverage and care in France: The “Premiers Pas” survey. Questions d'économie de la santé. (2019) 1–6. Available online at: https://www.irdes.fr/english/issues-in-health-economics/244-study-of-undocumented-immigrants-access-to-health-coverage-and-care-in-france-the-premiers-pas-survey.pdf
21. Wittwer J, Raynaud D, Dourgnin P, Jusot F. Providing healthcare coverage to undocumented immigrants in France. Questions d'économie de la santé. (2019) 1–8. Available online at: https://www.irdes.fr/english/issues-in-health-economics/243-providing-healthcare-coverage-to-undocumented-immigrants-in-france-what-we-know-and-what-we-don-t-about-state-medical-aid-ame.pdf
22. Lauritano D, Moreo G, Carinci F, Campanella V, Della Vella F, Petruzzi M. Oral health status among migrants from middle- and low-income countries to Europe: a systematic review. Int J Environ Res Public Health. (2021) 18:12203. doi: 10.3390/ijerph182212203
23. Pichemin C, Boyer E, Jarno P, Bertaud V, Meuric V, Couatarmanach A. Oral care needs amongst disadvantaged migrants in France. Int Dent J. (2022) 72:559–64. doi: 10.1016/j.identj.2021.12.002
24. Simon J, Kiss N, Laszewska A, Mayer S. Public Health Aspects of Migrant Health: A Review of the Evidence on Health Status for Labour Migrants in the European Region. (Health evidence network synthesis report 43). WHO regional Office for Europe. Copenhaguen: WHO (2015).
25. Epidemiological assessment of hepatitis B C among migrants in the EU/EEA. European Centre for Disease Prevention and Control. (2016). Available online at: https://www.ecdc.europa.eu/en/publications-data/epidemiological-assessment-hepatitis-b-and-c-among-migrants-eueea (accessed December 15, 2020).
26. Vignier N, Desgrées du Loû A, Pannetier J, Ravalihasy A, Gosselin A, Lert F, et al. Access to health insurance coverage among sub-Saharan African migrants living in France: results of the ANRS-PARCOURS study. PLoS ONE. (2018) 13:e0192916. doi: 10.1371/journal.pone.0192916
27. Magalhaes L, Carrasco C, Gastaldo D. Undocumented migrants in Canada: a scope literature review on health, access to services, and working conditions. J Immigr Minor Health. (2010) 12:132–51. doi: 10.1007/s10903-009-9280-5
28. Rechel B, Mladovsky P, Ingleby D, Mackenbach JP, McKee M. Migration and health in an increasingly diverse Europe. Lancet Lond Engl. (2013) 381:1235–45. doi: 10.1016/S0140-673662086-8
29. Scheppers E, van Dongen E, Dekker J, Geertzen J, Dekker J. Potential barriers to the use of health services among ethnic minorities: a review. Fam Pract. (2006) 23:325–48. doi: 10.1093/fampra/cmi113
30. Guillot M, Khlat M, Elo I, Solignac M, Wallace M. Understanding age variations in the migrant mortality advantage: An international comparative perspective. PLoS ONE. (2018) 13:e0199669. doi: 10.1371/journal.pone.0199669
31. Holguin F, Moughrabieh MA, Ojeda V, Patel SR, Peyrani P, Pinedo M, et al. Respiratory health in migrant populations: a crisis overlooked. Ann Am Thorac Soc. (2017) 14:153–9. doi: 10.1513/AnnalsATS.201608-592PS
32. Ly TDA, Dao TL, Hoang VT, Braunstein D, Brouqui P, Lagier JC, et al. Pattern of infections in French and migrant homeless hospitalised at Marseille infectious disease units, France: a retrospective study, 2017-2018. Travel Med Infect Dis. (2020) 36:101768. doi: 10.1016/j.tmaid.2020.101768
33. Knudtzen FC, Mørk L, Nielsen VN, Astrup BS. Accessing vulnerable undocumented migrants through a health-care clinic including a community outreach program: a 12 year retrospective cohort study in Denmark. J Travel Med. (2021) taab128. doi: 10.1093/jtm/taab128
34. Laganà AS, Gavagni V, Musubao JV, Pizzo A. The prevalence of sexually transmitted infections among migrant female patients in Italy. Int J Gynaecol Obstet. (2015) 128:165–8. doi: 10.1016/j.ijgo.2014.08.013
35. Desgrées-du-Loû A, Pannetier J, Ravalihasy A, Gosselin A, Supervie V, Panjo H, et al. Sub-Saharan African migrants living with HIV acquired after migration, France, ANRS PARCOURS study, 2012 to 2013. Euro Surveill. (2015) 20. doi: 10.2807/1560-7917.ES.2015.20.46.30065
36. Mora M, Rincon G, Bourrelly M, Maradan G, Freire Maresca A, Michard F, et al. Living conditions, HIV and gender affirmation care pathways of transgender people living with HIV in France: a nationwide, comprehensive, cross-sectional, community-based research protocol (ANRS Trans&HIV). BMJ Open. (2021) 11:e052691. doi: 10.1136/bmjopen-2021-052691
37. Kendjo E, Houzé S, Mouri O, Taieb A, Gay F, Jauréguiberry S, et al. Epidemiologic trends in malaria incidence among travelers returning to metropolitan France, 1996-2016. JAMA Netw Open. (2019) 2:e191691. doi: 10.1001/jamanetworkopen.2019.1691
38. Deniaud F, Vignier N, Collignon A, Boo N, Hennequin C. Urogenital schistosomiasis detected in sub-Saharan African migrants attending primary healthcare consultations in Paris, France: a 14-year retrospective cohort study (2004-2017). Eur J Clin Microbiol Infect Dis. (2020) 39:1137–45. doi: 10.1007/s10096-020-03819-6
39. Gessain A, Cassar O. Epidemiological aspects and world distribution of HTLV-1 infection. Front Microbiol. (2012) 3:388. doi: 10.3389/fmicb.2012.00388
40. Papon S, Robert-Bobée I. An increase in deaths twice as high for people born abroad than for those born in France in March-April 2020. Insee Focus. (2020). Available online at: https://www.insee.fr/fr/statistiques/4627049
41. Price-Haywood EG, Burton J, Fort D, Seoane L. Hospitalization and mortality among black patients and white patients with Covid-19. N Engl J Med. (2020). 382:2534–43. doi: 10.1056/NEJMsa2011686
42. Prieur C, Dourgnon P, Jusot F, Marsaudon A, Wittwer J, Guillaume S. Une personne sans titre de séjour sur six souffre de troubles de stress post-traumatique en France. (2020). Available online at: https://www.irdes.fr/recherche/2022/qes-266-une-personne-sans-titre-de-sejour-sur-six-souffre-de-troubles-de-stress-post-traumatique-en-france.html (accessed June 13, 2022).
43. Haut conseil de la santé publique. Avis du 6 mai 2015 relatif aux recommandations concernant la visite médicale des étrangers primo-arrivants en provenance de pays tiers. Paris: HCSP (2015).
44. Vignier N, Halley des Fontaines V, Billette de Villemeur A, Cazenave-Roblot F, Hoen B, Chauvin F, et al. Public health issues and health rendezvous for migrants from conflict zones in Ukraine: A French practice guideline. Infect Dis Now. (2022) 52193–201. doi: 10.1016/j.idnow.2022.04.006
45. Donkin A, Goldblatt P, Allen J, Nathanson V, Marmot M. Global action on the social determinants of health. BMJ Glob Health. (2018) 3:e000603. doi: 10.1136/bmjgh-2017-000603
46. Décret n° 2020-1325 du 30 octobre 2020 relatif à l'aide médicale de l'Etat et aux conditions permettant de bénéficier du droit à la prise en charge des frais de santé pour les assurés qui cessent d'avoir une résidence régulière en France - Légifrance. Available online at: https://www.legifrance.gouv.fr/jorf/id/JORFTEXT000042483561 (accessed June 13, 2022).
Keywords: migrants, undocumented migrants, infectious diseases, HIV, dental infection, France, HBV
Citation: Vignier N, Moussaoui S, Marsaudon A, Wittwer J, Jusot F and Dourgnon P (2022) Burden of infectious diseases among undocumented migrants in France: Results of the Premiers Pas survey. Front. Public Health 10:934050. doi: 10.3389/fpubh.2022.934050
Received: 02 May 2022; Accepted: 11 July 2022;
Published: 04 August 2022.
Edited by:
Alessio Petrelli, National Institute for Health, Migration and Poverty (NIHMP), ItalyReviewed by:
Silvano Gabriele Cella, University of Milan, ItalyYves Jackson, Geneva University Hospitals (HUG), Switzerland
Copyright © 2022 Vignier, Moussaoui, Marsaudon, Wittwer, Jusot and Dourgnon. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nicolas Vignier, ZHIudmlnbmllckBnbWFpbC5jb20=