 Azadeh Lak
Azadeh Lak Soheila Khodakarim2
Soheila Khodakarim2 Phyo K. Myint
Phyo K. Myint Hamid R. Baradaran
Hamid R. Baradaran- 1Faculty of Architecture and Urban Planning, Shahid Beheshti University, Tehran, Iran
- 2Department of Biostatistics, School of Medicine, Shiraz University of Medical Sciences, Shiraz, Iran
- 3Ageing Clinical and Experimental Research Team, Institute of Applied Health Sciences, University of Aberdeen, Aberdeen, United Kingdom
- 4Department of Epidemiology, School of Public Health, Iran University of Medical Sciences, Tehran, Iran
Background: Public open spaces (POSs) is considered a feature of the built environment that is important for physical, mental, and social health during life and contributes to active aging. Hence, policymakers, practitioners, and academics have recently focused on indicators of elder-friendly environments, particularly in developing countries.
Objective: This study aimed to examine the attributes of POSs and socio-demographic status that positively influence older people’s health in Tehran’s deprived neighborhoods using a pathway model.
Methods: We employed a pathway model to explore the relationships between place function, place preferences, and process in the environment as the perceived (subjective) positive features of POSs associated with older adults’ health, compared to the objective attributes of POSs. We also included personal characteristics, including physical, mental, and social dimensions, to explore how these factors are related to the health of older adults. To assess the subjective perception of POSs attributes, 420 older adults were asked to complete Elder-Friendly Urban Spaces Questionnaire (EFUSQ) from April 2018 to September 2018 in the 10th District of Tehran. We used the SF-12 questionnaire and “The self-Rated Social Health of Iranians Questionnaire to measure older people’s physical and mental health and elder social health.” Geographical Information System (GIS) measures (Street connectivity, Residential density, Land use mix, Housing quality) were derived as objective measures of neighborhood features.
Results: According to our findings, the personal aspect, socio-demographic status (such as Gender, Marital status, Education, Occupation as well as Frequency of being present in POSs), place preferences (Security, Fear of Falling, Way Finding and Perceived Aesthetics), and process in the environment’s latent (Social Environment, Cultural Environment, Place Attachment, and Life Satisfaction)constructs collectively influenced the elders’ health.
Conclusion: We found positive associations between Place preference, Process-in-environment, and personal health-related factors to elders’ health (social, mental, and physical). The path model presented in the study could be guided in future research in this area and inform the development of evidence-based urban planning and design interventions for improve older adults health and social functioning and quality of life.
Introduction
The number of people above 65, i.e., older adults, will double by 2050 (1). Physiologically speaking, aging results from accumulated molecular and cellular damage, gradually decreasing physical and mental capacities and increasing chronic diseases (2). There is growing evidence to support late-life living environments as well as associations between the features of the outdoor environment and health outcomes (3–5). Well-maintained public open spaces (POSs) can enhance older adults’ physical and mental health and well-being (6–8). Changes in mortality, physical function, disease prevalence, and mental health status in different environments can support this relationship (9). With other attributes of the building, say, walkability, and public transport infrastructure, POSs bring about various benefits, such as promoting physical activity (7, 10) and creating social cohesion in neighborhoods ((10, 11); (7)). Older adults’ health depends on some elements, including lifestyle, genetic predisposition, social relationships, and environment (7).
Besides, the research found an association between POSs and chronic health conditions like obesity (4, 7), cardiovascular disease (12), diabetes (7, 12), respiratory health (13), and mental health (e.g., stress, anxiety, depression, and attention) deficit disorders (7, 12). In line with this body of research, POS in this study refers to local green spaces in neighborhoods.
Studies of older adults have found that some characteristics of POSs are likely to increase walking activities in residential neighborhoods (14–16). These characteristics include walking for transportation (17), recreational physical activity (15) in local streets (18), and urban parks (19, 20), including amenities like shade structures, toilets, trees and plants, and well-paved surfaces and like to experience minimal traffic and seat along walkways (1), “trees/plant” (20) and park seating (21).
The provision of appropriate POSs is a major social determinant of health contributing to an area’s livability, particularly in deprived urban neighborhoods (22), regarded as “safe, secure, attractive, socially cohesive and inclusive, and environmentally sustainable; with affordable and diverse housing linked to employment, education, public open space, local shops, health and community services, and leisure and cultural opportunities; via convenient public transport, walking and cycling infrastructure” (23).
To examine the impact of individual and environmental factors on the presence of older adults in POSs and on their health outcomes, our study adopts such an ecological perspective (24), which includes three potential mechanisms of older adults’ health as physical activity in outdoor spaces, social interaction, and contact with nature (25).
As Iranian society’s traditional structure disapproves of sending senior people to nursing homes, aging in place is the appropriate solution to help older adults in Iran remain physically and mentally healthy. Creating elder-friendly POSs can help them live active and healthy life and experience an acceptable quality of life (26). Although many researchers have already studied the relationship between POSs and older adults’ health, there is still a shortage of robust evidence to support contemporary policy demands in an aging society (12). Besides, the health status of older adults in the POSs of neighborhood’ was addressed internationally (7, 23), but there is a significant gap in Iran’s quantitative research (27, 28). A 2015 report by Tehran Municipality states that although Iran is a group of 33 countries involved in moving toward age-friendly cities, the government is not equipped with the necessary infrastructure (29–31). The collected data show that theoretical findings have led to neither a deep understanding of the local preferences of older adults in Iran nor practical guidelines for designing and developing age-friendly POSs. With this in mind, this study aims to explore the relationship between self-related health and features of POSs to enhance the presence of the elderly in POSs in the deprived neighborhoods of Tehran, Iran.
Materials and methods
Study site
This study was carried out in public spaces (POSs), including parks, squares, and neighborhood hangouts, in Tehran’s 10th district. Tehran’s 10th district has relatively the highest population among Tehran’s regions and the highest number of older adults. It has a relatively low area of residential use; therefore, most older adults use public spaces in their neighborhoods (32). Of 287,476 people in the 10th district of Tehran, more than 10 percent are above 60 years old (33).
Study design
This cross-sectional study was conducted on 420 older people who regularly used public outdoor spaces (POSs) in Tehran’s 10th district neighborhoods over 4 months during Spring/Summer in 2018. Participants were asked to complete three questionnaires, the SF-12 questionnaire, the Self-Rated Social Health of Iranians Questionnaire, and an elder-friendly urban spaces questionnaire (EFUSQ), after obtaining their written consent assisted by research assistants. Trained research assistants facilitated this through face-to-face interviews. They all received a three-hour training which covered how to introduce questionnaires and administer interviews to ensure standardized facilitation for accuracy, completeness, and reliability. Data collection for each participant took about 20–30 min. The Iran University of Medical Sciences (IUMS) granted ethical approval, and all participants signed informed consent before participating in this research.
Participants
From April through September 2018, participants were chosen using a purposeful (non-random) sampling technique. To be considered, the individuals had to frequent the open areas (parks, squares, and streets) in the District 10 neighborhoods of Tehran at least three times each week. Those with severe physical disabilities who could not use POSs and had communication problems were not considered for this study.
Measurements
The subjective measure of the neighborhood’s perceived environment, which we used here, was measured through an adapted version of the Elder-Friendly Urban Spaces Questionnaire (EFUSQ) (28). The questionnaire consists of 50 items divided into three parts in terms of environmental dimensions plus one piece which is related to socio-demographic status:
1. Place functions (amenities, density, safety, traffic, objective aesthetics, urban landscape, comfort, and environmental cleanness).
2. Place preferences (PP) (crime security, fear of falling, fear of losing, and image).
3. Process in environments (cultural environment, social environment, life satisfaction, and sense of belonging).
4. Socio-demographic statuses like gender, age, marital status, and occupation.
The objective measures of the environment of neighborhoods were based on the variables of the Geographical Information System (GIS), which were measured in Euclidean or straight-line distances buffer within 500 m of the centroid of a neighborhood using ArcGIS® version 10 (34).
1. Street connectivity: Based on the number of real intersections in an area, street connectivity is defined by the number of links between streets divided by the number of street nodes in the buffer area.
2. Residential density: The number of dwelling units was divided by the residential land area in this region to obtain this measure.
3. Land use mix: Land use mix is the distribution of development among five types of use (i.e., residential, commercial, recreational, industrial, and others).
4. Housing quality: This shows whether or not a person’s home is located inside a deteriorated neighborhood.
5. Frequency of POS uses: This measure refers to the number of visits older person’s weekly make to POSs (never, once a week, twice a week, more than three times a week).
In the Self-reported Quality of Life (SF-12), the participant’s self-rated health was reported as ‘excellent,’ ‘very good,’ ‘good,’ ‘poor,’ or ‘very poor.’ Physical and mental quality of life was recorded using 12 questions from the simplified Iranian version of Medical Outcomes Study Short Form 12 (SF-12 v2) Health Survey. The survey has already been validated in Iranian populations and is widely used to evaluate the general population’s health (35). According to Montazeri et al. (35), the evaluation of physical health requires a combination of four subscales [general health (one item), physical functioning (two items), physical role (two items), and bodily pain (one item)]. Evaluation of mental health, too, requires a combination of four subscales [vitality (one item), social functioning (one item), emotional role (two items), and mental health (two items)]. These physical and mental health component scores were calculated using normative subscale scores for the Iranian population (35).
Also, we used the “Self-Rated Social Health of Iranians Questionnaire,” which consists of 33 items to evaluate social health (36). The total score was the sum of all 33 items (minimum one and maximum 5 points/item), and the total score lies between 33 and 165, with higher scores indicating better self-reported social health. This scale comprises three domains; community, family, friends, and relatives, with 19, 6, and 8 items for each. Family refers to all household members, and “friends and relatives” refer to those with whom an individual has a close relationship. Other social activities/communications are included under the “community domain.” The psychometric parameters of this scale were verified in the context of the Iranian population (36).
Data analysis
We applied Partial Least Square Structural Equation Modeling (PLS-SEM) to understand better the influencing factors of the health of older people in POSs’ attributes-regarding social, mental, and physical domains of health-and to develop a conceptual model. PLS-SEM is a causal predictive analysis of both formative and reflective variables (37). It is a common multivariate analysis method for calculating variance-based structural equation models and is widely applied in social sciences (38). Moreover, it also provides an opportunity to resolve the multi-dimensional causal relationships that are otherwise difficult to explore. PLS-SEM can be used to assess the path coefficient (or connection strengths) as parameters of the model estimating effective connectivity. Furthermore, PLS-SEM also handles data distribution using the bootstrapping technique to calculate the significance value for coefficients of the model (pathway).
The proposed model was analyzed using a two-step process. First, the model deals with latent variables (measurement models) that define the association between latent indicators and their manifest variables. Second, an SEM describes the associations between the latent variables. This model explains the relationships between the latent variables and their related manifest variables. A total of 27 factors derived from the literature were recognized as the observed variables and categorized into five groups called exogenous latent constructs. They included the place function factor, place preference factor, process-in-environment factor, the factor related to objective attributes of the outdoor environment, and personal factor.
Therefore, the endogenous latent variable (an older person’s health) consisted of five exogenous (observed) variables. Figure 1 shows the conceptual model that illustrates the relationships between endogenous latent constructs and exogenous latent constructs. Therefore, our overarching hypothesis is that five primary constructs influence the health of older adults assessed using physical and mental HRQoL dimensions and social health.
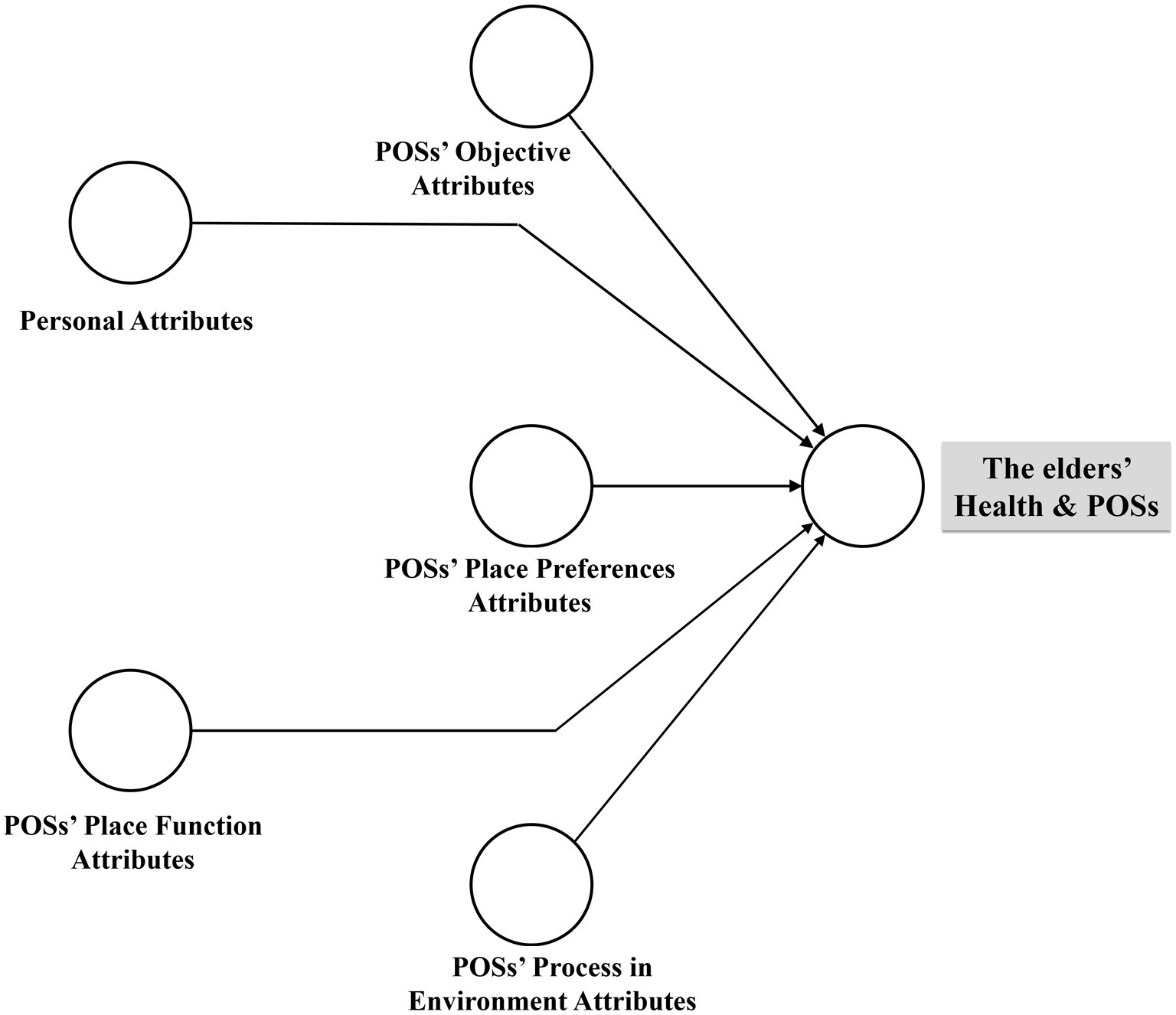
Figure 1. The proposed conceptual framework.
Our research hypotheses are as follows:
Hypothesis 1 (H1). The place function factor (PF) significantly and positively affects older adults’ health.
Hypothesis 2 (H2). The place preference factor (PP) significantly and positively affects older adults’ health.
Hypothesis 3 (H3). The process-in-environment factor (PE) significantly and positively affects older adults’ health.
Hypothesis 4 (H4). The factor related to the outdoor environment objective attributes (OB) significantly and positively affects older adults’ health.
Hypothesis 5 (H5). Personal factor (PR) significantly and positively affects older adults’ health.
To validate the model, the standardized root mean square residual (SRMR) was employed as an index used to show the average of standardized residuals between the observed and the hypothesized covariance matrices (39). SRMR is counted as a measure of the estimated model fit; if SRMR = < 0.08, the study model can be claimed to have a good fit (40), with lower SRMR values indicating a better fit.
Results
Baseline data
Data were drawn from the survey conducted on 420 older residents of district 10, Tehran municipality. The study participants’ mean (SD) age was 76.3 ± 9.2 years, 61.3% males, 73.5% married, and 27.2% without a high-school diploma (Table 1). Twenty participants were excluded from the leading models due to high missing data levels.
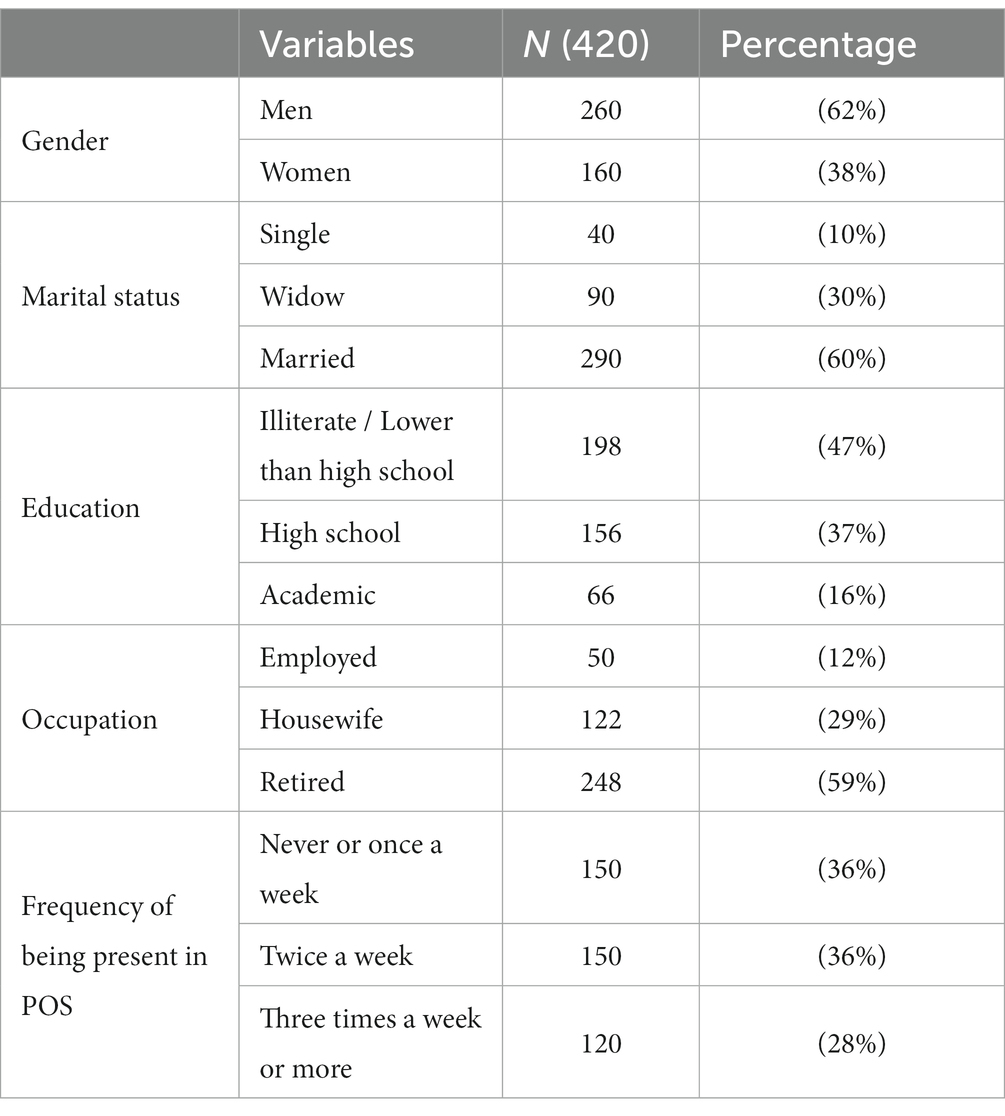
Table 1. Descriptive characteristics of the study participants (n = 420).
The simulation to calculate the impact of the observed variables and their latent constructs on the health of older adults was analyzed using smart-PLS version 3.2.7.
Evaluation of the outer measurement model
The outer measurement model calculates the internal consistency of observed variables (measured by the questionnaire) and their reliability, validity, and unobserved variables (41). Evaluations of consistency are based on a single observed variable and construct reliability tests, while validity is assessed by convergent and discriminant validity (38).
A single observed variable reliability is supposed to describe the variance of an individual observed compared to an unobserved variable by assessing the standardized outer loadings of the observed variables (42). An outer loading of 0.7 or greater means that the observed variables are considered exceedingly acceptable (38), whereas a value of less than 0.7 should be discarded (43). In this study, the cut-off value accepted for the outer loading was 0.7, and 0.4 or greater values are acceptable for exploratory analyses. As listed in Table 2, the outer loadings range between 0.191 and 0.823. Cronbach’s alpha and Composite Reliability (CR) values were used to evaluate internal consistency in construct reliability.
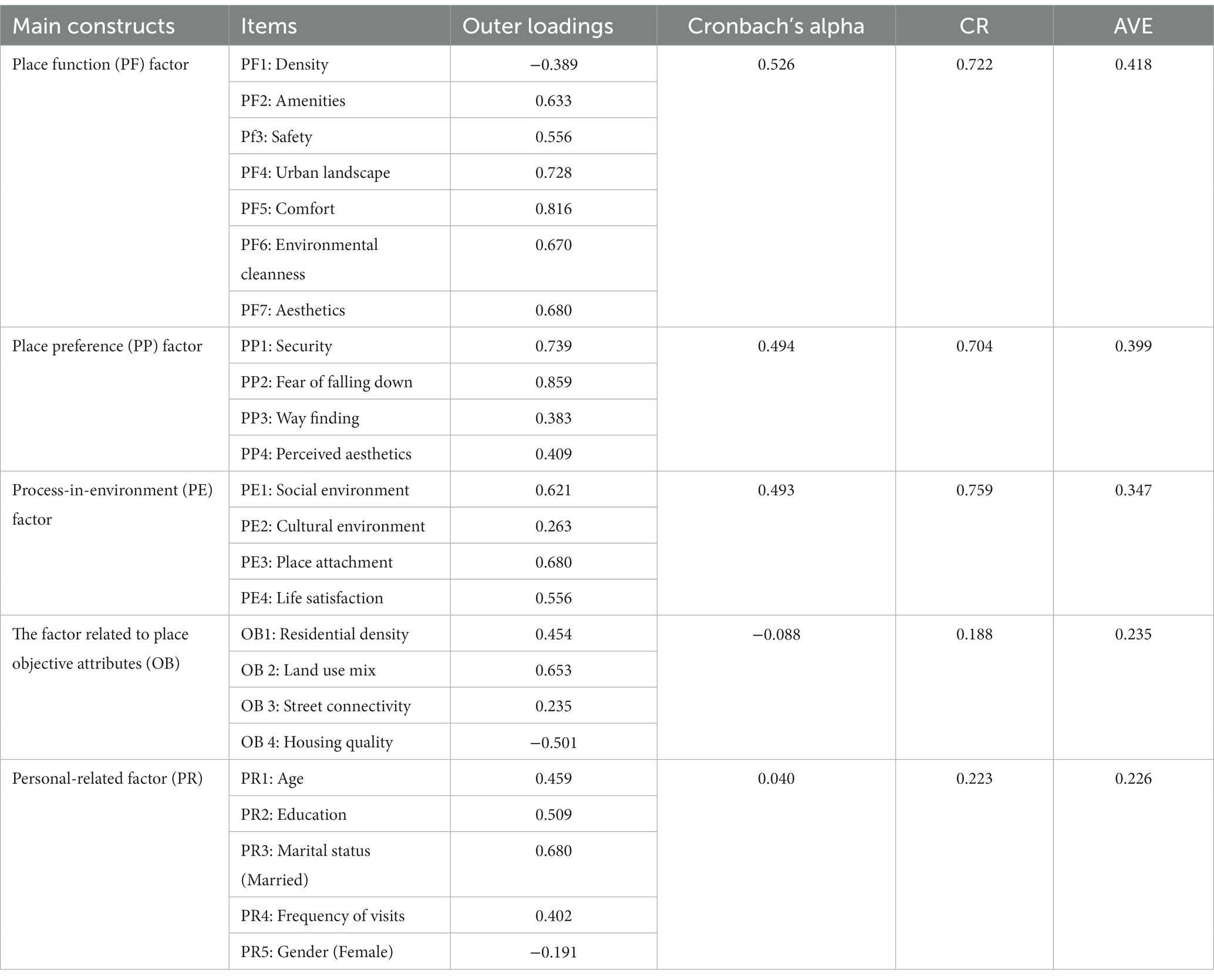
Table 2. Construct reliability and validity.
Compared with Cronbach’s alpha, CR is supposed to evaluate internal consistency better because it preserves the observed variables’ standardized loadings (44). In our work, however, Cronbach’s alpha and the CR value produced the same results. As seen in Table 2, Cronbach’s alpha was not greater than 0.7, whereas CR for the latent constructs 1, 2, and 3 was more significant than 0.70. Thus, the scales were confirmed as reasonably reliable, indicating that all latent constructs values were more significant than the minimum threshold level of 0.70. The Average Variance Extracted (AVE) of each latent construct was calculated to verify the variables convergent validity (44). The latent constructs in the model should take the lowest 50% of the observed variable variance. This shows that AVE’s value for all the constructs should be greater than 0.5 (45). To achieve discriminant validity, the square root of AVE for each latent variable should be greater than the correlations among the latent variables. So, convergent validity was confirmed for this study model. These results confirmed the convergent validity and the internal consistency of this model.
The next step was to measure the discriminant validity of the latent constructs. The notion of discriminant validity indicates that the manifest variable in any construct should be distinguished from other constructs in the path model in which the cross-loading value in the latent variable is higher than in any other construct (46). We used the Fornell and Larcker criterion and cross-loadings to assess the discriminant validity (44). The proposed standard is that a construct should not indicate the same variance as any other construct more significant than its AVE value (46).
Table 3 lists the Fornell and Larcker criterion test results in which the squared correlations were compared with correlations from other latent constructs. As shown in this table, all correlations were smaller than the squared root of average variance exerted along the diagonals, which implies adequate discriminant validity. All constructs observed variables correspond to the given latent variable, confirming the model’s discriminant validity. As a result of proper reliability, convergent validity, and discriminant validity, the suggested conceptual model proved relatively acceptable.
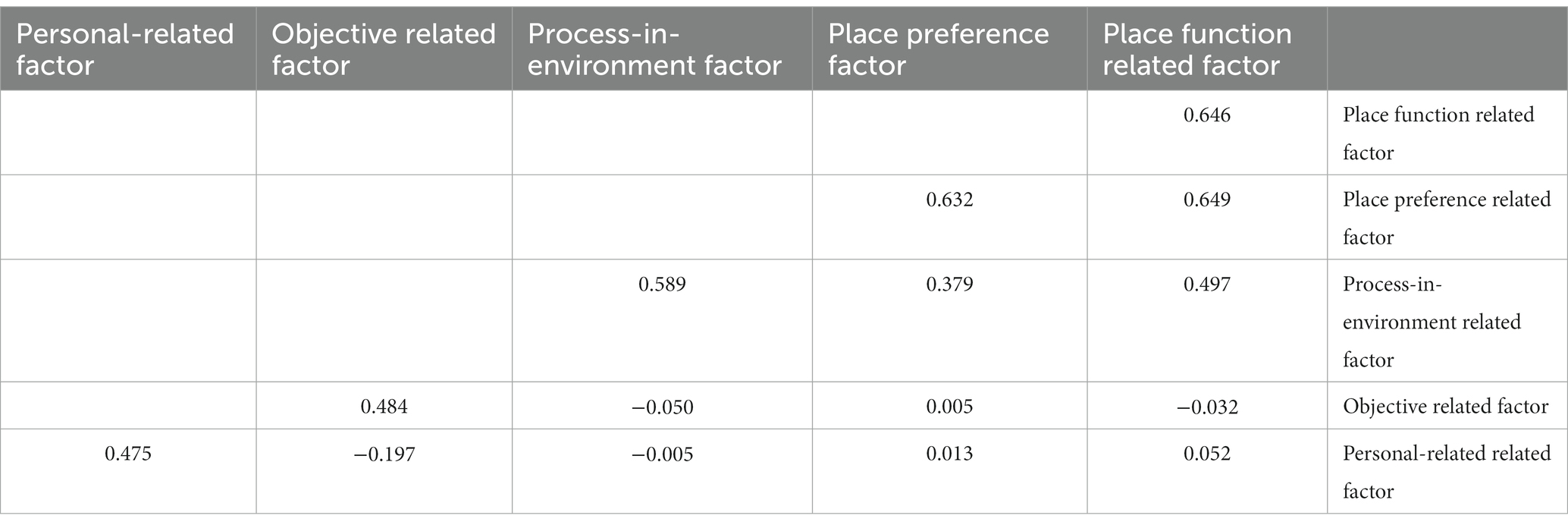
Table 3. Fornell–Larcker criterion test.
Evaluation of the inner structural model
The validity and reliability of the measurement model were confirmed in this analysis through Inner Structural Model. This entailed an examination of the predictive relevancy of the model and the relationships between the constructs. The primary standards for assessing the inner structural model are the coefficient of determination (R2), path coefficient (β value), and T-statistic.
Measuring the value of R2
The coefficient of determination measures the overall effect and variance defined in the endogenous construct for the structural equation model. Therefore, it is a measure of the predictive accuracy of the model. In our study, the inner path model’s value was 0.490 for the quality endogenous latent construct, meaning the five independent constructs can explain 49% of older adults’ health variance. According to Henseler et al. (47) and Hair et al. (46), an R2 value of 0.75 is considered substantial, 0.50 as moderate, and 0.26 as weak. Based on this, the R2 value in this study was moderate.
Estimation of path coefficients (β) and T-statistics
The regression analysis showed a similarity between the PLS path coefficients and the standardized β coefficient. The significance of the hypothesis was examined using the β value. The β denoted the dependent construct’s expected variation for a unit variation in the independent construct(s). For every path in the hypothesized model, we calculated the β values. A more excellent β value meant a more substantial effect on the endogenous latent construct. We verified the significant level of β value using the T-statistics test. We used the bootstrapping procedure to assess the hypothesis’s significance (48). The importance of the path coefficient and T-statistics values was tested through a bootstrapping method using 5,000 subsamples. Table 4 summarizes our results.

Table 4. Path coefficient and T-statistics.
As to H1, the PF factor (β = 0.053, T = 838, p > 0.05) did not significantly and positively influence older adults’ health. This was also the case for the OB factor (β = −0.068, T = 0.875, p > 0.05). Therefore, this model could not support H4. As predicted, the findings in Table 4 show that the PR factor significantly influenced health (β = 0.224, T = 3.194, p = 0.014). Thus, H5 was robustly supported. Concerning the direct and positive effect of the PE factor on health (H3), the results in Table 4 confirm that this factor highly significantly affects the health status in older adults (β = 0.218, T = 4.715, p < 0.001), thereby confirming H3. The influence of place preferences (PP factor) on health in older adults was significant and positive (β = 0.180, T = 3.196, p = 0.01), which supports H2.
A more significant beta coefficient (β) among the supported latent variables would indicate a more robust effect from an exogenous latent construct on the endogenous latent construct. Table 4 and Figure 2 show that PF and PE factors had the highest path coefficient (β = 0.224 and β = 0.218) compared to other β values in the model. This indicates that these factors had a more significant variance and a more substantial effect on older people’s health. The PP-related factors had the slightest impact on health (β = 0.180).
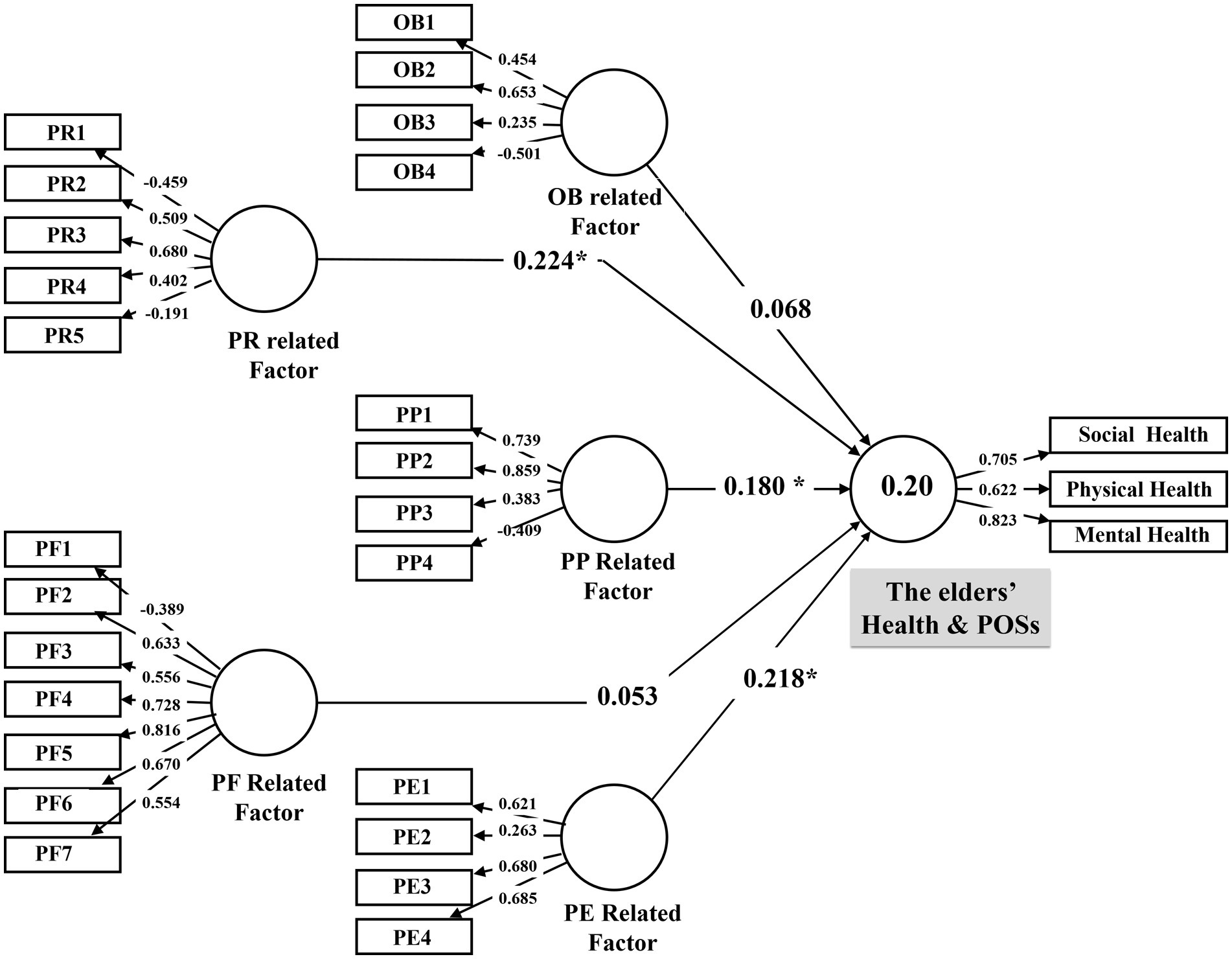
Figure 2. The path model. (Coefficient *p < 0.05).
To Emphasize the model fit, our results indicate that the SRMR of our model was 0.095, showing that the model has moderate goodness to fit. The associated Chi-Square value was 1866.461, and NFI was 0.211.
Discussion
By adopting an ecological approach, we examined the relationship between the perceived and objective aspects of urban POSs and the health domains of older adults in poor urban neighborhoods of Tehran, Iran. Three health domains (social, mental, and physical) were evaluated based on an individual’s perception of the place, which has its roots in the person-environment relationship, place features (both perceived and objective), and socio-demographic status. Thus, we have hypothesized and proposed a predictive path model. Based on the findings, the physical, mental, and social health in older adults is associated with some attributes of POSs as place preferences (Security, Fear of Falling Down. Way Finding and Perceived Aesthetics) and processes in the environment (Social Environment, Cultural Environment, Place Attachment and Life Satisfaction). Our study also emphasized the role of the personal aspect and socio-demographic status (such as Gender, Marital status, Education, and Occupation) in making older people healthy by using POSs in their neighborhoods, mainly the Frequency of being present in POS.
The predictive model revolves around the relationship between older adults’ health and urban space features. It depends on place function (safety, landscape design, place aesthetics, cleanliness, amenities, and sense of comfort), older adults’ place preferences (security of the environment, subject aesthetics, fear of falling down, and fear of getting lost), and place processes (social background, cultural features, sense of belonging to the place, and life satisfaction). In addition, the model examines the relationship between objective dimensions such as the density of land uses, residential density, the number of intersections in the unit of area, and the quality of the residential environment (new or deteriorated), as well as individual profiles such as gender, age, marital status, and frequency of visits to a POSs and health.
The results suggest that personal features, the process of place-time relationships, and place preferences are related to older adults’ health. Older adults’ health in urban spaces is a function of mental, social, and physical health. In contrast to most studies focusing mainly on physical health (49), the present study shows that social and mental health is more substantial among older adults in deprived areas. Accordingly, mental health’s effect on general health is more vital than physical health (50). Also, for older adults, their physical and psychological health depends on their social health and social relationships.
In agreement with other studies (51), socio-demographic status substantially affects marital status. Education has the closest relationship with health among older adults since they cause individuals to pay more attention to their health and health-related behaviors. Having a spouse decreases the sense of loneliness and abandonment, enhancing one’s health and quality of life. In this study, increasing presence in urban spaces influences older adults’ health. The gender dimension shows that presence in urban spaces only affects the health of males. This is in line with the study on the health of older adults conducted in Japan (12).
Studying the relationship between health and the perceived features of urban space shows that the formation of place function that builds upon non-physical aspects of the environment has a closer relationship with older adults’ health than place preferences and place function. In the non-physical dimension of place, older adults’ most influential health factors are life satisfaction, sense of belonging to the neighborhood and urban space, attachment to the social environment, and cultural factors. The sense of belonging, formed by being rooted in a place and having a place-bound identity, creates stability and mental security in an individual. In addition, older people are usually unwilling to move to another place because they are bound to a place for their memories. Previous studies have mentioned the effect of place attachment on social health (52). Satisfaction with one’s residential environment and belonging to the neighborhood and urban space creates a sense of comfort in older adults. Thus, urban space and local parks in dense neighborhoods act like one’s own courtyard, enhancing a sense of control in older adults (53).
The role of the social environment as an opportunity for social interactions prevents the sense of abandonment and loneliness in older adults. Most studies regarded social relationships as a trigger of trust and support in older adults, increasing mental health and preventing anxiety and distress. Moreover, it will also enhance the social functioning of older adults, thus resulting in better relationships with family members and friends and boosting the sense of belonging in society. Thus, relatedness is the sense of belonging and being a member of the social environment, which was demonstrated to have strong relationships with positive feelings, life purposes, perceived vitality, personal development, and life satisfaction in older people (54).
Cultural factors such as the segregation of men and women and the limited presence of house pets due to Iran’s cultural restrictions have less remarkable effects on older adults’ health (7, 11, 53, 55).
After the process of the person-place relationship, place preferences have the most substantial effect on the relationship between health and urban space. Lack of fear of falling, sense of security, and empirical-affective aesthetics of urban spaces contribute to place preferences on older adults’ health. Fear of falling down is a major preventive factor that depends on the individual’s background (56), which has its roots in older adults’ physical and mental health. The sense of security that results from the low level of crimes and uncivilized behavior can create a sense of comfort in the elderly and make them feel like they are in their courtyard in POSs.
Consistent with our findings, Fuller (57) states that the perceived difficulty of tasks, such as those used to control body posture, has a strong relationship with the prediction of risk, which is indicative of an emotional reflex to dangers, e.g., fear of falling (57). Therefore, anybody with a fear of falling down should limit outdoor physical activities, which, if not considered, eliminates the people with the fear of falling from the group at risk (1). Besides, if this feeling of fear through specially designed environmental spaces decreases, an increase will result in individuals’ physical activity (56, 58), which may promote active aging (59).
Finally, the aesthetic experience of older adults, which results from perceiving harmony and geometry, could result in mental comfort and overall health. According to previous studies, protection against traffic, walking level and safe parks, the intensity of street noise (60), physical barriers, aesthetics, and crime (61) impact the health-related quality of life of older adults. Although previous studies have shown that the objective dimensions of place affect the health of older adults (34, 60, 62), the present study does not confirm such a relationship. In addition, this study does not show any relationship between older adults’ perception of place function and their health.
One limitation of the present study is the restriction of the study scale only to deprived neighborhoods. Furthermore, our study was conducted over 3 months; this can lead to different results if conducted at different time points of the year since it is most likely that older adults’ perception of POSs differs between seasons.
This study’s results can contribute to the design of public environments for older adults to improve their social, mental, and physical health. This makes possible the idea of aging in place through physical and non-physical interventions and providing a high-quality urban environment that meets the older peoples’ sense of belonging and preferences. Our study highlights the importance of appropriate housing and providing POSs tailored to their needs for them to be able to socialize and participate in social-cultural events. Increasing social capital is another way to form social networks and social cohesion. Moreover, our study highlights the need to design spaces without barriers suitable for walking, provide protection against crime, and prepare the environment with fewer falls risk.
Conclusion
We found positive associations between Place preference, Process-in-environment, and personal health-related factors to elders’ health (social, mental, and physical). Therefore, we recommend that older adults’ preferences concerning outdoor spaces and their life satisfaction and relatedness (i.e., social interaction and place attachment) could be considered for planning and designing outdoor spaces’ features before implementing urban management policies. The path model presented is a suitable approach to using various dimensions of the neighborhood environment, including objective and perceived features.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by the Iran University of Medical Sciences. The patients/participants provided their written informed consent to participate in this study.
Author contributions
HB and AL created the study’s concept and design. AL conducted the research, developed the methodology, and authored the article. SK used SPSS to analyze the analysis. PM offered thorough criticism of the manuscript. All authors contributed to the article and approved the submitted version.
Acknowledgments
The authors would like to acknowledge our community partner in the municipality of Tehran in the 10th district.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1.Boccardi, V. Population ageing: The need for a care revolution in a world 2.0. Geriatrics. (2019) 4:47. doi: 10.3390/geriatrics4030047
2.Baquero Larriva, MT, and Higueras García, E. Confort térmico de adultos mayores: Una revisión sistemática de la literatura científica. Rev Esp Geriatr Gerontol. (2019) 54:280–95. doi: 10.1016/j.regg.2019.01.006
3.Lee, H, and Waite, LJ. Cognition in context: The role of objective and subjective measures of neighborhood and household in cognitive functioning in later life. Gerontologist. (2018) 58:159–69. doi: 10.1093/geront/gnx050
4.Tuckett, AG, Banchoff, AW, Winter, SJ, and King, AC. The built environment and older adults: A literature review and an applied approach to engaging older adults in built environment improvements for health. Int J Older People Nursing. (2018) 13:e12171. doi: 10.1111/opn.12171
5.Winters, M, Voss, C, Ashe, MC, Gutteridge, K, McKay, H, and Sims-Gould, J. Where do they go and how do they get there? Older adults’ travel behaviour in a highly walkable environment. Soc Sci Med. (2015) 133:304–12. doi: 10.1016/j.socscimed.2014.07.006
6.Lak, A, Rashidghalam, P, Myint, PK, and Baradaran, HR. Comprehensive 5P framework for active aging using the ecological approach: An iterative systematic review. BMC Public Health. (2020) 20:33. doi: 10.1186/s12889-019-8136-8
7.Levy-Storms, L, Chen, L, and Loukaitou-Sideris, A. Older adults’ needs and preferences for open space and physical activity in and near parks: A systematic review. J Aging Phys Act. (2018) 26:682–96. doi: 10.1123/japa.2016-0354
8.Yung, EHK, Wang, S, and Chau, C. Thermal perceptions of the elderly, use patterns and satisfaction with open space. Landsc Urban Plan. (2019) 185:44–60. doi: 10.1016/j.landurbplan.2019.01.003
9.Zhu, B-W, Zhang, J-R, Tzeng, G-H, Huang, S-L, Xiong, L, Rosenberg, M, et al. Public open space development for elderly people by using the DANP-V model to establish continuous improvement strategies towards a sustainable and healthy aging society. Sustainability. (2017) 9:420. doi: 10.3390/su9030420
10.Yung, EHK, Conejos, S, and Chan, EHW. Public open spaces planning for the elderly: The case of dense urban renewal districts in Hong Kong. Land Use Policy. (2016) 59:1–11. doi: 10.1016/j.landusepol.2016.08.022
11.Yung, EHK, Conejos, S, and Chan, EHW. Social needs of the elderly and active aging in public open spaces in urban renewal. Cities. (2016) 52:114–22. doi: 10.1016/j.cities.2015.11.022
12.Koohsari, MJ, McCormack, GR, Nakaya, T, Shibata, A, Ishii, K, Yasunaga, A, et al. Urban design and Japanese older adults’ depressive symptoms. Cities. (2019) 87:166–73. doi: 10.1016/j.cities.2018.09.020
13.Lee, ACK, Jordan, HC, and Horsley, J. Value of urban green spaces in promoting healthy living and wellbeing: Prospects for planning. Risk Manag Healthc Policy. (2015) 8:131. doi: 10.2147/RMHP.S61654
14.Alves, S, Aspinall, PA, Thompson, CW, Sugiyama, T, Brice, R, and Vickers, A. Preferences of older people for environmental attributes of local parks. Facilities. (2008) 26:433–53. doi: 10.1108/02632770810895705
15.Cole, R, Koohsari, MJ, Carver, A, Owen, N, and Sugiyama, T. Are neighborhood environmental attributes more important for older than for younger adults’ walking? Testing effect modification by age. J Aging Phys Act. (2019) 27:354–9. doi: 10.1123/japa.2018-0009
16.Sugiyama, T, and Thompson, CW. Outdoor environments, activity and the well-being of older people: Conceptualising environmental support. Environ Plan A. (2007) 39:1943–60. doi: 10.1068/a38226
17.Sugiyama, T, and Ward Thompson, C. Associations between characteristics of neighbourhood open space and older people’s walking. Urban For Urban Green. (2008) 7:41–51. doi: 10.1016/j.ufug.2007.12.002
18.Curl, A, Thompson, CW, and Aspinall, P. The effectiveness of ‘shared space’ residential street interventions on self-reported activity levels and quality of life for older people. Landsc Urban Plan. (2015) 139:117–25. doi: 10.1016/j.landurbplan.2015.02.019
19.Esther, HKY, Winky, KOH, and Edwin, HWC. Elderly satisfaction with planning and design of public parks in high density old districts: An ordered logit model. Landsc Urban Plan. (2017) 165:39–53. doi: 10.1016/j.landurbplan.2017.05.006
20.Wang, X, and Rodiek, S. Older adults’ preference for landscape features along urban park walkways in Nanjing, China. Int J Environ Res Public Health. (2019) 16:3808. doi: 10.3390/ijerph16203808
21.Gibson, SC. “Let’s go to the park.” An investigation of older adults in Australia and their motivations for park visitation. Landsc Urban Plan. (2018) 180:234–46. doi: 10.1016/j.landurbplan.2018.08.019
22.Guo, S, Song, C, Pei, T, Liu, Y, Ma, T, Du, Y, et al. Accessibility to urban parks for elderly residents: Perspectives from mobile phone data. Landsc Urban Plan. (2019) 191:103642. doi: 10.1016/j.landurbplan.2019.103642
23.Aspinall, PA, Thompson, CW, Alves, S, Sugiyama, T, Brice, R, and Vickers, A. Preference and relative importance for environmental attributes of neighbourhood open space in older people. Environ Plan B Plan Des. (2010) 37:1022–39. doi: 10.1068/b36024
24.Schehl, B, and Leukel, J. Associations between individual factors, environmental factors, and outdoor independence in older adults. Eur J Ageing. (2020) 17:291–8. doi: 10.1007/s10433-020-00553-y
25.World Health Organization. World report on ageing and health. Geneva: World Health Organization (2015).
26.Sharifian, A, and Rezaei, H. Comparison of life satisfaction, general health and functionality of elderly residents in public and private nursing homes in Tehran. J socail Work Res. (2016) 2:77–111. doi: 10.22054/rjsw.2016.8657
27.Fallahi, B, Momtaz, YA, Heriyanto, B, Susanti, N, Setiawaty, V, Shoja, M, et al. Urban space preferences among older adults from a sociodemographic perspective characterization and identification of poliovirus from the environment in Indonesia 2015 the alterations of XRCC1 gene’s polymorphism with a different SNP is involved in breast. Bali Med J. (2018) 7:544–9. doi: 10.15562/bmj.v7i3.1183
28.Lak, A, Aghamolaei, R, Baradaran, HR, and Myint, PK. Development and validation of elder-friendly urban spaces questionnaire (EFUSQ). BMC Geriatr. (2019) 19:336. doi: 10.1186/s12877-019-1355-0
29.Bastani, F, Haghani, H, and Goodarzi, P. Age–friendly cities features from the elderly’s perspectives underscoring community support and health services. J Client Cent Nurs Care. (2016) 2:103–14. doi: 10.32598/jccnc.2.2.103
30.Ghahfarrokhi, SH, Khankeh, HR, Akbari Kamrani, AA, and Fadayevatan, R. What is a key step in the falling process in older people? A qualitative study in an Iranian context. Educ Gerontol. (2016) 42:209–19. doi: 10.1080/03601277.2015.1089694
31.Sharqi, A, Zarghami, E, Olfat, M, and Salehi Kousalari, F. Evaluating status of global indices of age-friendly city in tehran metropolis (AFC). Archit Civ Eng Environ. (2016) 9:35–52. doi: 10.21307/acee-2016-034
32.Rashedi, V, Asadi-Lari, M, Foroughan, M, Delbari, A, and Fadayevatan, R. Prevalence of disability in Iranian older adults in Tehran, Iran: A population-based study. J Heal Soc Sci. (2016) 1:251–62. doi: 10.19204/2016/prvl26
34.Nyunt, MSZ, Shuvo, FK, Eng, JY, Yap, KB, Scherer, S, Hee, LM, et al. Objective and subjective measures of neighborhood environment (NE): Relationships with transportation physical activity among older persons. Int J Behav Nutr Phys Act. (2015) 12:108. doi: 10.1186/s12966-015-0276-3
35.Montazeri, A, Vahdaninia, M, Mousavi, SJ, and Omidvari, S. The Iranian version of 12-item short form health survey (SF-12): Factor structure, internal consistency and construct validity. BMC Public Health. (2009) 9:341. doi: 10.1186/1471-2458-9-341
36.Abachizadeh, K, Omidnia, S, Hajebi, A, Asadi, A, Rassouli, M, and Leila, B. Measuring self-rated social health of Iranians: A population based survey in three cities. Nov Biomed. (2014) 2:79–84. doi: 10.22037/nbm.v2i3.6107
37.Hussain, S, Fangwei, Z, Siddiqi, AF, Ali, Z, and Shabbir, MS. Structural equation model for evaluating factors affecting quality of social infrastructure projects. Sustainability. (2018) 10:1415. doi: 10.3390/su10051415
38.Hair, JF, Sarstedt, M, Ringle, CM, and Mena, JA. An assessment of the use of partial least squares structural equation modeling in marketing research. J Acad Mark Sci. (2012) 40:414–33. doi: 10.1007/s11747-011-0261-6
39.Chen, FF. Sensitivity of goodness of fit indexes to lack of measurement invariance. Struct Equ Model Multidiscip J. (2007) 14:464–504. doi: 10.1080/10705510701301834
40.Hu, L, and Bentler, PM. Fit indices in covariance structure modeling: Sensitivity to underparameterized model misspecification. Psychol Methods. (1998) 3:424–53. doi: 10.1037/1082-989X.3.4.424
41.Ho, R. Handbook of univariate and multivariate data analysis with IBM SPSS. Boca Raton, FL: CRC Press (2013).
42.Götz, O, Liehr-Gobbers, K, and Krafft, M. Evaluation of structural equation models using the partial least squares (PLS) approach In: V Esposito Vinzi, W Chin, J Henseler, and H Wang, editors. Handbook of partial least squares. Berlin, Heidelberg: Springer (2010). 691–711.
43.Chin, WW. “The partial least squares approach to structural equation modeling,” In: Modern methods for business research 295. (1998):295–336.
44.Fornell, C, and Larcker, D. Evaluating structural equation models with unobservable variables and measurement error. J Mark Res. (1981) 18:39–50. doi: 10.1177/002224378101800104
45.Barclay, D, Higgins, C, and Thompson, R. The partial least squares (PLS) approach to casual modeling: Personal computer adoption and use as an Illustration. Technol Stud. (1995) 2:285–309.
46.Hair, JF, Ringle, CM, and Sarstedt, M. Partial least squares structural equation modeling: Rigorous applications, better results and higher acceptance. Long Range Plan. (2013) 46:1–12. doi: 10.1016/j.lrp.2013.01.001
47.Henseler, J, Ringle, CM, and Sinkovics, RR. The use of partial least squares path modeling in international marketing In: RR Sinkovics and PN Ghauri, editors. New challenges to international marketing. Bingley: Emerald Group Publishing Limited (2009)
48.Chin, WW. The partial least squares approach to structural equation modeling. Mod Methods Bus Res. (1998) 295:295–336.
49.Ghasemi, S, Keshavarz Mohammadi, N, Mohammadi Shahboulaghi, F, and Ramezankhani, A. A critical review of studies on health needs assessment of elderly in the world. Elder Heal J. (2017) 3:1–9. doi: 20.1001.1.24236179.2017.3.1.1.8
50.Marsillas, S, De Donder, L, Kardol, T, van Regenmortel, S, Dury, S, Brosens, D, et al. Does active ageing contribute to life satisfaction for older people? Testing a new model of active ageing. Eur J Ageing. (2017) 14:295–310. doi: 10.1007/s10433-017-0413-8
51.Giummarra, MJ, Haralambous, B, Moore, K, and Nankervis, J. The concept of health in older age: Views of older people and health professionals. Aust Health Rev. (2007) 31:642–50. doi: 10.1071/AH070642
52.Huang, J, Zhou, C, Zhuo, Y, Xu, L, and Jiang, Y. Outdoor thermal environments and activities in open space: An experiment study in humid subtropical climates. Build Environ. (2016) 103:238–49. doi: 10.1016/j.buildenv.2016.03.029
53.Chippendale, T, and Boltz, M. The neighborhood environment: Perceived fall risk, resources, and strategies for fall prevention. Gerontologist. (2015) 55:575–83. doi: 10.1093/geront/gnu019
54.Yu, Y, Fong, VW-I, Lau, JT-F, Sum, RK-W, Leung, EF-L, and Mo, PK-H. The associations between psychological needs, health-related quality of life and subjective well-being among Chinese older people: A cross-sectional study. Health Soc. Care Commun. (2020). doi: 10.1111/hsc.13160
55.Wen, C, Albert, C, and Von Haaren, C. The elderly in green spaces: Exploring requirements and preferences concerning nature-based recreation. Sustain Cities Soc. (2018) 38:582–93. doi: 10.1016/j.scs.2018.01.023
56.Wijlhuizen, GJ, de Jong, R, and Hopman-Rock, M. Older persons afraid of falling reduce physical activity to prevent outdoor falls. Prev Med. (2007) 44:260–4. doi: 10.1016/J.YPMED.2006.11.003
57.Fuller, R. Towards a general theory of driver behaviour. Accid Anal Prev. (2005) 37:461–72. doi: 10.1016/J.AAP.2004.11.003
58.Fiatarone, MA, O’Neill, EF, Ryan, ND, Clements, KM, Solares, GR, Nelson, ME, et al. Exercise training and nutritional supplementation for physical frailty in very elderly people. N Engl J Med. (1994) 330:1769–75. doi: 10.1056/NEJM199406233302501
59.Annear, M, Keeling, S, Wilkinson, T, Cushman, G, Gidlow, B, and Hopkins, H. Environmental influences on healthy and active ageing: A systematic review. Ageing Soc. (2014) 34:590–622. doi: 10.1017/S0144686X1200116X
60.Parra, DC, Gomez, LF, Sarmiento, OL, Buchner, D, Brownson, R, Schimd, T, et al. Perceived and objective neighborhood environment attributes and health related quality of life among the elderly in Bogotá, Colombia. Soc Sci Med. (2010) 70:1070–6. doi: 10.1016/J.SOCSCIMED.2009.12.024
61.Zhao, Y, and Chung, P-K. Neighborhood environment walkability and health-related quality of life among older adults in Hong Kong. Arch Gerontol Geriatr. (2017) 73:182–6. doi: 10.1016/j.archger.2017.08.003
Keywords: public open space (POS), elderly health, perceived attributes, PLS-SEM, neighborhoods
Citation: Lak A, Khodakarim S, Myint PK and Baradaran HR (2023) The influencing factors of elder-friendly public open spaces promoting older adults’ health in deprived urban neighborhoods: Partial Least Square Structural Equation Modeling approach. Front. Public Health. 11:1143289. doi: 10.3389/fpubh.2023.1143289
Edited by:
Diogo Guedes Vidal, University of Coimbra, PortugalReviewed by:
Daniella do Amaral Mello Bonatto, Federal University of Espirito Santo, BrazilSílvio Manuel da Rocha Brito, Instituto Politécnico de Tomar (IPT), Portugal
Copyright © 2023 Lak, Khodakarim, Myint and Baradaran. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Azadeh Lak, YV9sYWtAc2J1LmFjLmly