 Sophie A. Korenhof1
Sophie A. Korenhof1 Ellen V. Rouwet1Liset E. M. Elstgeest1,2
Ellen V. Rouwet1Liset E. M. Elstgeest1,2 Irene N. Fierloos1Siok Swan Tan1,3Marta M. Pisano-Gonzalez4An L. D. Boone5
Irene N. Fierloos1Siok Swan Tan1,3Marta M. Pisano-Gonzalez4An L. D. Boone5 Yves-Marie Pers6,7
Yves-Marie Pers6,7 Alberto Pilotto8,9Mónica López-Ventoso4Isabel Diez Valcarce4Xuxi Zhang1,10 For EFFICHRONIC Consortium
Alberto Pilotto8,9Mónica López-Ventoso4Isabel Diez Valcarce4Xuxi Zhang1,10 For EFFICHRONIC Consortium Hein Raat1*
Hein Raat1*- 1Department of Public Health, Erasmus University Medical Center, Rotterdam, Netherlands
- 2Reinier Academy, Reinier de Graaf Hospital, Delft, Netherlands
- 3Research Group City Dynamics, InHolland University of Applied Sciences, Rotterdam, Netherlands
- 4Research Group “Community Health and Active Aging” of the Research Institute of Asturias (IPSA), General Directorate of Care, Ministry of Health, Oviedo, Spain
- 5Public Health General Directorate, Ministry of Health of the Principality of Asturias, Oviedo, Spain
- 6IRMB, University of Montpellier, INSERM, CHU Montpellier, Montpellier, France
- 7Clinical Immunology and Osteoarticular Diseases Therapeutic Unit, Department of Rheumatology, Lapeyronie University Hospital, Montpellier, France
- 8Department of Geriatric Care, Orthogeriatrics and Rehabilitation, Galliera Hospital, Genoa, Italy
- 9Department of Interdisciplinary Medicine, University of Bari, Bari, Italy
- 10Department of Social Medicine and Health Education, School of Public Health, Peking University, Beijing, China
Introduction: Chronic non-communicable diseases (NCDs) are predominantly related to modifiable health behaviors and account for 74% of global deaths at present. Behavior modification through self-management is a strategy to prevent NCDs. Chronic Disease Self-Management Programs (CDSMPs) have demonstrated improvements in health behaviors, health status, and use of healthcare.
Objective: We evaluated the effects of a 6-week CDSMP on self-efficacy, health behaviors, mental health, health-related quality of life (HR-QoL), and health responsibilities among vulnerable populations with chronic disease in Europe.
Methods: A prospective cohort study with a 6-month pre-post single-group design was conducted in five European countries. The intervention targeted adults with chronic conditions and low socioeconomic status, as well as their caregivers. The intervention was a 6-week community-based CDSMP in a group setting. Outcomes were measured per self-report questionnaire at baseline and 6-month follow-up: self-efficacy, health behaviors, mental health, HR-QoL, and health responsibilities.
Results: Of 1,844 participants, 1,248 (67.7%) completed follow-up and attended ≥4 sessions. For the chronic condition group, the following outcome measures at follow-up significantly improved compared with baseline (all P < 0.002): self-efficacy (SEMCD-6 6.7 vs. 6.4), mental health (PHQ-8 6.3 vs. 7.0), HR-QoL (SF-12 PCS 42.3 vs. 40.2, SF-12 MCS 42.8 vs. 41.4), health utility (EQ-5D-5L 0.88 vs. 0.86), self-rated health (EQ-5D-5L 67.2 vs. 63.9), communication with healthcare providers (2.28 vs. 2.11), understanding information (3.10 vs. 3.02), number of doctor visits (3.61 vs. 4.97), accident and emergency department visits (0.25 vs. 0.48), total nights in a hospital (0.65 vs. 1.13), and perceived medical errors (19.6 vs. 28.7%). No significant changes were detected in dietary habits, physical activity, substance use, and sleep and fatigue. For caregivers without a chronic condition, only doctor visits significantly decreased (1.54 vs. 2.25, P < 0.001).
Discussion: This CDSMP was associated with improvement in self-efficacy, depression, HR-QoL, and health responsibilities over 6 months in a diverse European population with a chronic condition. However, additional interventions targeting lifestyle risk factors are needed to improve health outcomes.
Introduction
Chronic non-communicable diseases (NCDs) are currently the most common cause of morbidity and mortality, accounting for 74% of all global deaths (1–3). It is estimated that chronic diseases will cost $47 trillion in gross domestic product from 2011 to 2025 globally (4). The development of the most common NCDs is largely related to modifiable lifestyle factors, including smoking, physical activity, stress, and poor dietary habits (5, 6). Hence, lifestyle-related chronic diseases are currently targeted with measures to manage modifiable risk factors, such as increasing physical activity, improving dietary habits, smoking cessation, and stress management (7, 8). Behavior modification is, thus, a crucial strategy for the prevention and treatment of lifestyle-related chronic diseases (9). Programs that enhance self-management may be useful in improving behavioral risk factors (10, 11). Chronic Disease Self-Management Programs (CDSMPs) have demonstrated significant improvements in health behaviors and health status as well as reduced healthcare utilization (12).
Vulnerable populations carry a higher burden of lifestyle risk factors and lifestyle-related chronic diseases (13–17). A vulnerable population can be defined as those at increased risk for chronic non-communicable diseases and refers to a wide range of groups, such as economically disadvantaged people, along with uninsured, racial, and ethnic minorities, older people, and those who meet barriers when accessing healthcare (18, 19). Especially, currently, with overloaded healthcare systems, it has become increasingly important to lower the burden of chronic diseases and reduce health disparities; thus, CDSMPs could be a potential low-cost solution. The objective of our study was to evaluate the effects of a 6-week CDSMP on self-efficacy, health behaviors, mental health, HR-QoL, and health responsibilities among vulnerable populations in five European regions.
Methods
Study design
The evaluation study of the EFFICHRONIC project was a prospective cohort study with a 6-month pre-post single-group design and was conducted between January 2018 and November 2020 in five European countries [the Netherlands, Italy, the United Kingdom (UK), Spain, and France]. The EFFICHRONIC project aimed to evaluate the benefits of a CDSMP in managing and maintaining the health of citizens with a low socioeconomic status (SES) and one or more chronic conditions, as well as their caregivers (20). For full details of the study design and protocol, see Tan et al. (20). There were no major deviations from the published protocol study. ISRCTN registry number is ISRCTN70517103 and the date of registration was 20 June 2018. Participant data were collected before the start of the first workshop session at baseline and 6-month follow-up. Ethical approval was provided by the human research ethics board of the study sites (20). All participants provided written informed consent.
Recruitment and eligibility criteria
Participants were recruited to participate in a CDSMP intervention in their local study site (Occitanie region in France, Genoa province in Italy, Rotterdam region in the Netherlands, Principality of Asturias in Spain, and a region of London in the UK). Citizens were recruited through clinicians, public events and announcements, local patient or volunteer organizations, and community advocates. Recruitment sites were chosen based on their location in distinct environments. Vulnerability maps were constructed in three study sites (Occitanie region, Genoa province, and Principality of Asturias) based on EUROSTAT's NUTS-3 level geographical areas, in which the prevalence of the target population was high (21). For complete recruitment strategies, see Alvarez Rosete et al. (22).
The intervention targeted a vulnerable population of citizens of ≥18 years and with a low SES with one or more chronic conditions as specified in the International Classification of Primary Care (ICPC-2) present for at least 6 months (23). Caregivers of the participants with a chronic condition were also included. Citizens were only eligible to participate if they were able to comprehend the information provided in the local language and were likely to complete the 6-month study duration. Citizens were not eligible to participate when they were experiencing a crisis period, their basic housing needs were not met, they were diagnosed with severe mental health problems, or they suffered from active addictive disorders or cognitive impairment.
Intervention
The CDSMP is a six-session (2.5 h weekly) community-based intervention built on the self-efficacy theory (10, 24, 25), a well-established program developed by Stanford University and assessed for over 20 years by the Self-Management Resource Center (24, 26). Each group session was led by trained (public) health professionals and trained laypersons in groups of up to 20 participants in the local language (27). Session leaders were trained by certified trainers, following the Stanford methodology (26). Topics included in the sessions were as follows: an overview of self-management and chronic health conditions, making an action plan, relaxation and management of cognitive symptoms, problem-solving, emotions (anger, fear, and/or frustration), fitness, fatigue management, healthy eating, advance directives, communication, medication, making treatment decisions, depression, informing the healthcare team, and working with healthcare professionals (12). The program focused on problem-solving, decision-making, confidence building, management of emotions, positive health and efficient communication to strengthen self-efficacy (i.e., the confidence in one's ability to accomplish a specific task or reach a goal), and managing different aspects of one's health functioning (25).
Outcome measures
Outcomes were obtained through self-report questionnaires at the start of the first session (baseline) and 6-month follow-up. Caregivers filled out the questionnaires by themselves but not for the individuals with a chronic condition they cared for. The degree of self-efficacy was measured with the Self-Efficacy for Managing Chronic Diseases 6-item scale (SEMCD-6), with scores ranging from 6 to 60, with higher scores corresponding to higher self-efficacy (28). The following health behaviors were assessed: (1) dietary habits: two items on the intake of fruit and vegetables; (2) physical activity: six items on physical exercise (12) and one item on sedentary behavior: International Physical Activity Questionnaire (IPAQ) (29); (3) substance use: current smoking, yes/no; frequency of alcohol use, one item from the Alcohol Use Disorders Identification Test (AUDIT-C) (30); and (4) sleep and fatigue: visual analog scale (VAS), with scores ranging from 0 to 10, with higher values indicating worse sleep/more fatigue. Depression severity was assessed with the Patient Health Questionnaire 8-item scale (PHQ-8), with scores ranging from 0 to 24, with higher values indicating a higher severity, score ≥10 corresponding to current depression (31). Health-related quality of life (HR-QoL) was assessed with the 12-item Short-Form Health Survey (SF-12), with scores ranging from 0 to 100; the EuroQol-5 Dimensions-5 levels (EQ-5D-5L), using the United Kingdom value sets, with scores ranging from 0 to 1, with higher values indicating better health utility (32, 33); and EQ-VAS, with scores ranging from 0 to 100, with higher values indicating better HR-QoL.
Health responsibilities were assessed as follows: (1) communication with healthcare professionals: three items on preparing a list of questions, asking questions, and discussing personal problems (12); (2) health literacy: two items on the Health Literacy Questionnaire (HLQ) (34); (3) healthcare utilization in the past 6 months was assessed with four items on the number of doctor visits, the number of accident and emergency department visits, number of overnight stays in the hospital, and the total number of nights spent in the hospital; (4) medication adherence: six items from the Simplified Medication Adherence Questionnaire (SMAQ) (35); and (5) perceived medical errors: three items on the understandability of a healthcare professional's explanation and prevalence of perceived medical errors from the American Association of Retired Persons (AARP) “survey beyond 50.09” questionnaire (36).
Other measures
Sociodemographic characteristics were assessed using self-report questionnaires: age, sex, household composition, educational level, income, migration background, employment situation, housing situation, social relationships, and social support. The participant's household composition, income, housing situation, social relationships, and social support were measured by an adapted version of Gijón's Social-Familial Evaluation Scale (SFES) (37). The subjective improvement in the most important outcomes of the CDSMP intervention experienced by the participants was evaluated with seven items at the 6-month follow-up: change in doing at least one activity for health; not letting health problems control their life; the ability to make decisions; the ability to express themselves; in the way of communication with family, friends, and others; confidence in the health system understanding their needs; and satisfaction with the intervention as a whole.
Statistical methods
Participant characteristics were described using mean (SD) or number of participants (%) for the total study sample. Participant's sociodemographic characteristics and health outcomes were evaluated at baseline after stratification for chronic disease status. Caregivers with a chronic condition were added to the “chronic condition group,” and caregivers without a chronic condition were added to the “no chronic condition group.” T-tests were used to compare the means for continuous variables and Pearson's chi-squared tests for categorical variables. To assess the effects of the intervention on continuous outcome measures, linear regression analyses were conducted with a change in the outcome measure between baseline and follow-up as a dependent variable and the beta of the intercept indicating the effect. For dichotomous outcome measures, paired McNemar's tests were used. Outcome analyses were stratified by chronic disease status. In addition, stratified linear regression analyses were run for country, educational level, sex, and age (age <65 years or ≥65 years). Supplementary Tables 2B–E considering 26 outcome measures, the two-sided significance threshold, after Bonferroni correction for multiple testing, was set at a P-value = 0.05/26 = 0.0019. In the protocol study, two outcome measures were considered in five countries. Analyses were conducted with SPSS version 25.0 (IBM SPSS Statistics for Windows, IBM Corp., Armonk, NY, USA).
Results
Description of participants
Participants were recruited for the project between January 2018 and March 2020; 2,759 participants who fulfilled the inclusion criteria provided informed consent and started the intervention. Of the 1,693 participants who filled in the baseline questionnaire and had an available chronic disease status, 1,377 (81.3%) were citizens with a chronic condition, and 316 (18.7%) were caregivers. Participants were included in the five European study sites: the Netherlands (n = 388), Italy (n = 331), the United Kingdom (n = 345), Spain (n = 568), and France (n = 212). Table 1 shows the baseline characteristics of the study sample stratified by chronic disease status, i.e., having a chronic condition or being a caregiver without a chronic condition. Supplementary Table 1A presents the baseline characteristics of the total study population, and Supplementary Table 1B describes the baseline characteristics at the country level. Compared with caregivers without a chronic condition (the no chronic condition group), citizens with a chronic condition were, on average, less often female, reported more current depression, more often lived alone, had a lower educational status, had a lower income, less often had a migration background, and less often worked.

Table 1. Baseline characteristics of the study sample stratified by chronic condition status (n = 1,693).
Adherence to interventions and follow-up attrition
Of all included participants (n = 2,759), 2,277 (82.5%) attended at least four out of six sessions of the CDSMP intervention. Attending ≥4 out of six group sessions was defined as “good adherence” (38). A total of 1,844 participants (66.8% out of 2,759) took part in the baseline questionnaire, and 1,252 participants took part in the follow-up questionnaire. Four participants only took part in the follow-up questionnaire. The number of participants that completed both baseline and follow-up was 1,248. Overall, 1,152 out of 1,844 (62.5%) participants took part in both baseline and 6-month follow-up questionnaires, attended ≥4 sessions, had an available chronic disease status, and were included as the study sample for further analyses. The baseline characteristics of the 692 excluded participants were compared with the included participants. On average, the excluded participants were younger, more often female, more often a current smoker, and spent less time on aerobic physical activity; there were also significant differences in country, education level, income, and housing adaptation (see Supplementary Table 3). A flow chart of the participants is shown in Figure 1.
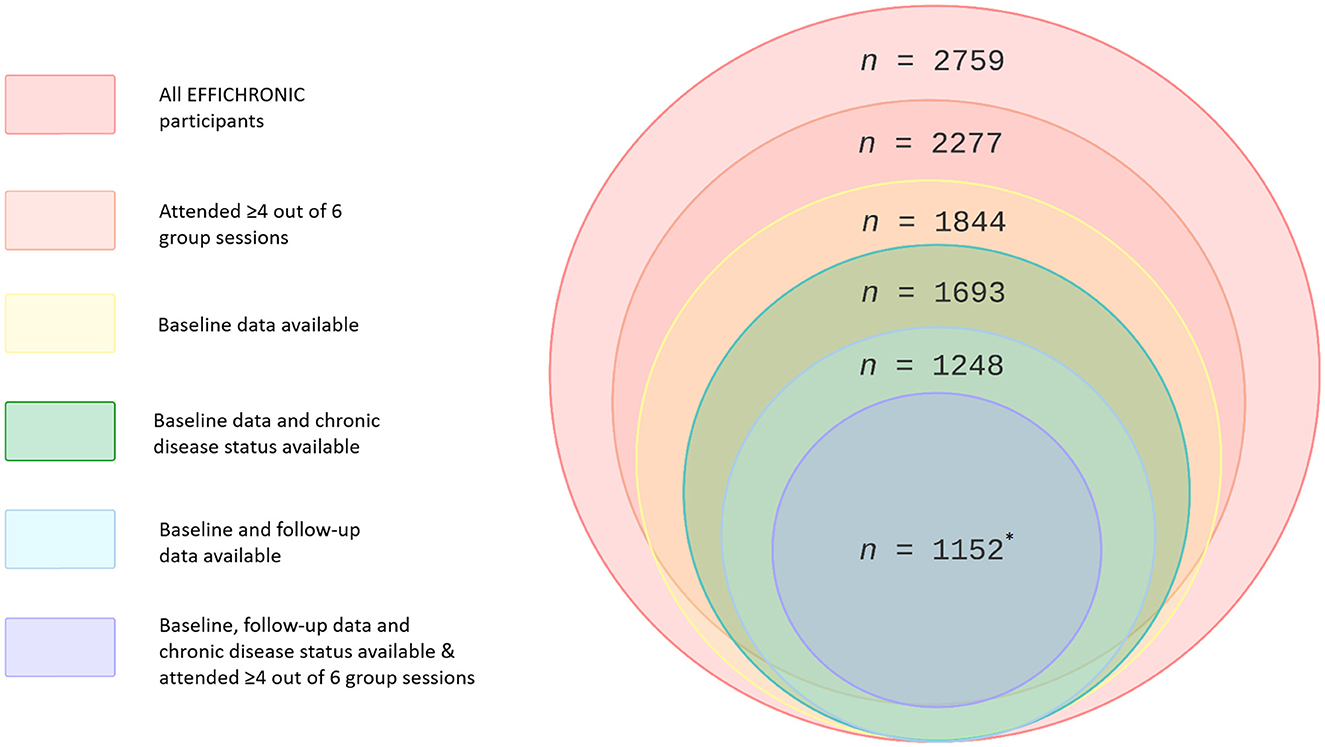
Figure 1. Participant flow chart. *Number per country: Netherlands, n = 194; Italy, n = 214; United Kingdom, n = 275; Spain, n = 336; France, n = 133.
Outcomes
Table 2 presents the outcome scores of the 1,152 participants who completed both the baseline and follow-up questionnaire, attended ≥4 sessions, and had an available chronic disease status. Among participants with a chronic condition (n = 951), there were significant improvements at follow-up compared with baseline (all P < 0.002) in self-efficacy (SEMCD-6 6.7 vs. 6.4), PHQ depression scores (6.3 vs. 7.0), physical and mental HR-QoL (PCS 42.3 vs. 40.2, MCS 42.8 vs. 41.4), health utility (EQ-5D-5L 0.88 vs. 0.86), and self-rated overall health (EQ-5D-5L 67.2 vs. 63.9). In addition, a significant improvement was shown in communication with healthcare providers (2.28 vs. 2.11) and understanding information (3.10 vs. 3.02). Furthermore, within the healthcare utilization, the number of doctor visits (3.61 vs. 4.97), Accident and Emergency department visits (0.25 vs. 0.48), and total nights spent in a hospital (0.65 vs. 1.13), all measured over the last 6 months, significantly diminished. Finally, the percentage of perceived medical errors (19.6 vs. 28.7%) decreased. No significant changes were shown in dietary habits, physical activity, substance use, and sleep and fatigue. In addition, finding health information, the number of overnight hospital visits, medication adherence, perceived unclear communication with the doctor, and perceived experienced medical errors as a problem did not change.
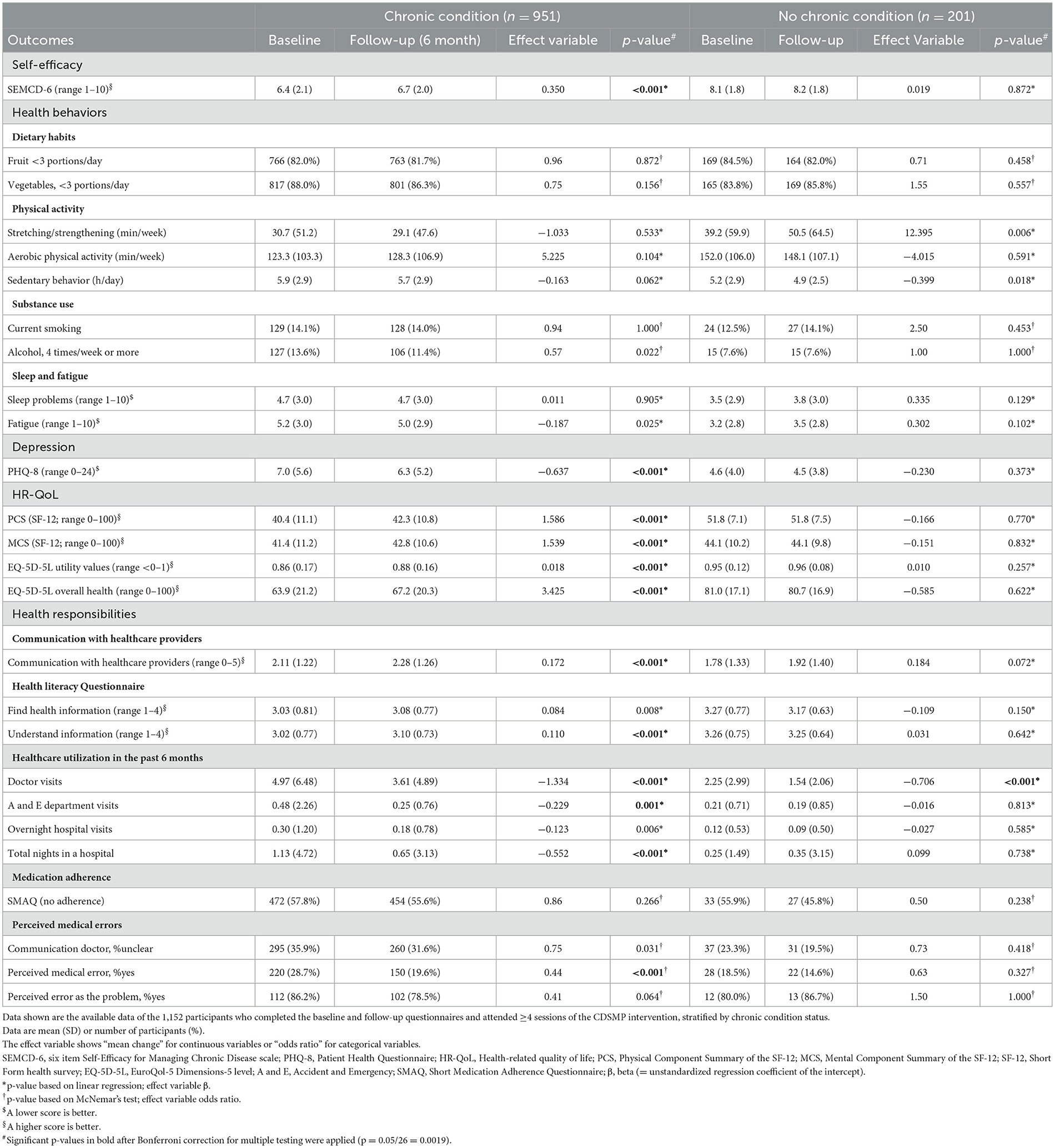
Table 2. Effects of the EFFICHRONIC intervention stratified by chronic condition status (n = 1,152).
Among caregivers without a chronic condition (n = 201), only a significant decrease in doctor visits was reported (1.54 vs. 2.25, P < 0.001). Supplementary Table 2A presents the effects of the EFFICHRONIC intervention on the total study population, and Supplementary Tables 2B–E presents the effects of the EFFICHRONIC intervention per country, educational level, sex, and age group. To determine the relevance of the statistically significant effects of the intervention, the differences in outcome scores before and after the intervention were compared with the minimal clinically important differences (MCIDs) of the respective outcome measures (39). The differences in the effect size of the depression score (PHQ-8), HR-QoL score (SF-12), health utility score (EQ-5D-5L), and overall health score (EQ-VAS) did not meet the MCIDs of these parameters (40–42). No MCIDs were available for the other parameters.
Satisfaction and adverse events
Participants who completed the questions on experienced outcome changes at follow-up (n = 1,248) reported an improvement in doing at least one activity for health (85.2%), not letting health problems control their life (80.3%), ability to make decisions (56.0%), ability to express themselves (49.3%), communication with family, friends, and others (51.1%), and confidence in the healthcare system understanding their needs (45.1%) (Supplementary Table 4). The average satisfaction score with the intervention was 8.3 ± 1.7 on a scale from 0 (lowest) to 10 (highest) (Supplementary Table 4). No adverse events were reported for the intervention.
Discussion
In this multicenter pre-post cohort study among a diverse European population, a 6-week chronic disease self-management program modestly improved self-efficacy, depression, HR-QoL, and health responsibilities in citizens with a chronic condition. However, considering these improvements, the differences shown for a part of the outcome measures (depression, HR-QoL, health utility, and overall health) were tested and found to not be clinically relevant when compared with their respective MCIDs. In addition, health behaviors did not improve.
Since the organization of healthcare in European countries varies substantially per country and, more importantly, also affects the accessibility of care (45), secondary analyses were conducted to investigate the differences between subgroups of different sociodemographic backgrounds (Supplementary Table 2B). Hardman et al. suggested a moderating effect of socioeconomic background on self-management support interventions in favor of people with high socioeconomic backgrounds (Supplementary Table 2C) (43). There is no known difference in the effect of CDSMPs between men and women; however, since mostly women participate in CDSMPs, studies might have lacked the statistical power to investigate the effect sufficiently in men (Supplementary Table 2D). Similarly, people aged 65 years and older more often finish CDSMP programs, among others participants, due to higher motivation. However, the impact of older age on the CDSMP effect remains largely unknown (Supplementary Table 2E) (44). Additional analyses show the effects per country, education level, sex, and age group; the outcome patterns of the whole study population are reflected in Supplementary Tables 2B–E, respectively; however, because the subgroups have lower numbers, there are less significant results.
Modifiable lifestyle risk factors (i.e., health behaviors) are the main drivers of chronic diseases (1), as shown in multiple well-established cohort studies, such as the Whitehall study (45), Framingham Heart Study (46), Women's Health Initiative (47), Nurses' Health Study (48), EPIC study (European Prospective Investigation into Cancer and Nutrition) (49), MESA study (Multi-Ethnic Study on Atherosclerosis) (50), and Mediators of Atherosclerosis in South Asians Living in America (MASALA) study (51). While there is a widespread belief in the importance of self-management programs for improving health behaviors in people with chronic conditions (10, 52, 53), the present study failed to show the effects of a well-established CDSMP on health behaviors. A recent study of a comparable CDSMP also reported no effect on health behaviors (54). Similarly, a meta-analysis and systematic review of self-management intervention studies showed improvement in subjective wellbeing, but overall, there were no effects on physical activity, diet and nutrition, smoking, alcohol consumption, and blood pressure (55, 56). The lack of improvement in health behaviors may be related to the intensity of the program as various systematic reviews on lifestyle interventions showed that intensive follow-up monitoring, a higher number of contact moments, face-to-face counseling, targeting multiple behaviors, and including common behavior change techniques were the most distinct factors within these interventions for changing one's health behaviors (57–60). There is no consistent evidence to substantiate that the lack of improvement could be related to the group-based community setting and/or low SES (61–63). Previous studies of the CDSMP conducted with a limited number of participants in low-SES populations showed improvements in self-efficacy, symptom management, general health, pain, and fatigue (64, 65). In contrast, interventions that target lifestyle risk factors more specifically and extensively, such as the Diabetes Prevention Program, the PREDIMED-Reus intervention, and CHIP (Complete Health Improvement Program), have proven successful in reducing the incidence of diabetes, inducing weight loss, and/or lowering blood glucose (66–68). Interestingly, a meta-analysis and a systematic review showed that behavioral treatment strategies and mitigating participation barriers improved adherence to lifestyle interventions (69, 70), which suggests that a behavior change intervention, such as the CDSMP, combined with an intervention addressing lifestyle-related risk factors, could work synergistically to reduce the burden of non-communicable chronic diseases.
Next to self-efficacy, depression, and HR-QoL, our study also showed improvement in health responsibilities (in the participants with a chronic condition): Positive changes were observed in communication with healthcare providers, perceived medical errors, healthcare utilization, and health literacy. To date, little research has been conducted on the relationship between self-management programs and health responsibilities. Previous studies have shown more benefits of self-management programs in people with low health literacy compared to those with high health literacy (71). In addition, health literacy itself may improve with a self-management program (72).
Although most self-management programs target patients with a chronic disease, some studies also demonstrated improved self-efficacy and higher HR-QoL in caregivers (73, 74). In our study, the effect of the CDSMP was less in caregivers without a chronic condition as compared with people with a chronic condition. The caregivers were more often female and unemployed; therefore, it is unclear whether this is the reason that underlies the difference in effectiveness. Alternatively, a difference in receptivity for a behavioral intervention between people with and without a chronic condition may explain this discrepancy.
Limitations
First, a lack of a control group prevents the outcomes from being linked to the intervention since non-specific effects related to group-based intervention participation cannot be ruled out. The outcome measures were self-reported; therefore, a bias in the outcome estimates cannot be excluded and is probably less precise than objectively measured outcomes. Furthermore, the presence of selection or social desirability bias cannot be ruled out; we only have data on the sociodemographic characteristics of the participants who completed the baseline questionnaire, which makes it hard to infer the implications of our study. The intervention was targeted at a vulnerable population; however, we did not achieve in including those who are most vulnerable, for example, people who were not able to speak the local language were not able to participate. In addition, despite all efforts, many participants did not fill in one or both questionnaires and were thus excluded from analyses, resulting in a high attrition rate.
There were differences in sociodemographic variables and lifestyle factors between dropped-out participants and participants who completed the follow-up, which might have caused attrition bias. In addition, participants in the study sites were recruited in different ways. On the one hand, the heterogeneity of the study population might make it harder to infer the effects of the intervention. On the other hand, this heterogeneous study population with diverse backgrounds might enable the outcomes to reflect the general population more. As discussed above, a CDSMP intervention with a 6-week duration might have been too short for changing health behaviors since that is a complex matter, which needs lasting attention, support, and practice. Finally, the follow-up time was 6 months, which measured only “mid-term” effects.
Future directions
It might be worthwhile to conduct a meta-analysis of chronic disease self-management studies to assess the overall effectiveness and determining factors, such as duration, content, and setting. We also recommend a longer follow-up of behavioral and/or lifestyle intervention studies to assess the durability of any observed outcomes and to include objective measures, such as blood pressure, blood glucose, and BMI. Efforts should be made to involve vulnerable groups in chronic disease management programs to address health disparities. Communities in “Blue zones,” worldwide geographical regions where people live longer and healthier lives than the average, show that active engagement with social surroundings, a sense of belonging and purpose in life, plays a vital role in chronic disease prevention (63).
Conclusion
This CDSMP was associated with improvement in self-efficacy, depression, HR-QoL, and health responsibilities over 6 months in a diverse European population with a chronic condition. However, additional interventions targeting lifestyle risk factors are needed to improve health outcomes.
Data availability statement
The datasets presented in this article are not readily available because, only part of the participants have given additional permission to share their pseudonymized data to other research institutes for addressing scientific questions. However, the majority of the participants have not given permission for sharing their data with other research institutes. Requests to access the datasets should be directed to aC5yYWF0QGVyYXNtdXNtYy5ubA==.
Ethics statement
The studies involving humans were approved by Ethical Committee procedures have been followed in all study sites involved. The names of the review board and the references are: Occitanie, France: The Ethics Committee of the South-west and Oversees I in Toulouse (Comité de Protection des Personnes Sud-Ouest et Outre-Mer I) approved the study on 5 November 2018; study number NCT03840447. Genoa, Italy: The Regional Ethics Committee of Liguria (Il Comitato Etico della Regione Liguria) approved the study on 27 March 2018; study number 152-2018. Rotterdam, the Netherlands: The research proposal regarding the study site in the Netherlands was reviewed by the Medical Ethics Review Committee (Medische Ethische Toetsings Commissie; METC) of the Erasmus MC University Medical Center, Rotterdam. Based on their review, the Committee concluded that the rules laid down in the Dutch Medical Research Involving Human Subjects Act (also known by the Dutch abbreviation WMO, in full Wet Medisch-wetenschappelijk Onderzoek met mensen) do not apply to this study protocol (proposal number MEC-2017-1116), and gave permission to conduct this study at Erasmus Medical Center and to submit the results for publication in a scientific journal in the future (Letter FMS/ss/MEC-2017-1116; 23 November 2017). Asturias, Spain: The Research Ethics Committee of the Principality of Asturias (Comité de Ética de la Investigación del Principado de Asturias) approved the study on 31 January 2017; study number 20/17. London, United Kingdom: The results page from the HRA decision tool of the NHS Health Research Authority states there is not a need for NHS Research Ethics Committee (NHS REC) approval for sites in England regarding this study; followed by an e-mail of the Health Research Authority, London, UK on 28 March 2019 (Queries Line REF 76/76) saying: We can confirm that as long as the project does not involve the NHS then NHS REC review and HRA Approval are not required. And: … This decision is in line with: The harmonized UK-wide edition of the Governance Arrangements for Research Ethics Committees (GAfREC) 2018; UK Policy Framework for Health and Social Care Research (2017); The National Research Ethics Service (NRES) Defining Research table and the algorithm Does my project require review by a Research Ethics Committee? … and that … it may be provided to a journal or other body as evidence if required… The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. No potentially identifiable images or data are presented in this study.
Author contributions
HR: conceptualization, supervision, and funding acquisition. SK, ER, and HR: methodology and validation. SK: formal analysis and visualization. IF: investigation. SK, LE, and XZ: data curation. SK and ER: writing—original draft preparation. LE, IF, SST, MP-G, HR, AB, Y-MP, AP, ML-V, IDV, and XZ: writing—review and editing. IF, SST, and HR: project administration. All authors contributed to the article and approved the submitted version.
Funding
The enhancing health systems sustainability by providing cost-efficiency data of evidenced based interventions for chronic management in stratified population based on clinical and socio-economic determinants of health (EFFICHRONIC) project received funding from the European Union's Health Programme (2014–2020; grant agreement 738127).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1221675/full#supplementary-material
References
1. Vos T, Lim SS, Abbafati C, Abbas KM, Abbasi M, Abbasifard M, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. (2020) 396:1204–22. doi: 10.1016/S0140-6736(20)30925-9
2. World Health Organization. Noncommunicable Diseases. (2022). Available online at: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed January 27, 2023).
3. Global Burden of Disease Viewpoint Collaborators. Five insights from the Global Burden of Disease Study 2019. Lancet. (2020) 396:1135–59. doi: 10.1016/S0140-6736(20)31404-5
4. Bloom DE, Cafiero ET, Jané-Llopis E, Abrahams-Gessel S, Bloom LR, Fathima S, et al. The Global Economic Burden of Noncommunicable Diseases. World Economic Forum: Geneva (2011).
5. World Health Organization. Noncommunicable Diseases Progress Monitor 2022. World Health Organization: Geneva (2022). p. 234.
6. O'Donnell MJ, Chin SL, Rangarajan S, Xavier D, Liu L, Zhang H, et al. Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): a case-control study. Lancet. (2016) 388:761–75. doi: 10.1016/S0140-6736(16)30506-2
7. Åkesson A, Larsson SC, Discacciati A, Wolk A. Low-risk diet and lifestyle habits in the primary prevention of myocardial infarction in men: a population-based prospective cohort study. J Am Coll Cardiol. (2014) 64:1299–306. doi: 10.1016/j.jacc.2014.06.1190
8. Palu E, MacMillan DF, McBride DKA, Thomson DR, Zarora R, Simmons D. Effects of lifestyle interventions on weight amongst Pasifika communities: a systematic review and meta-analysis. Lancet Reg Health West Pac. (2022) 25:100483. doi: 10.1016/j.lanwpc.2022.100483
9. Kim S, Park M, Song R. Effects of self-management programs on behavioral modification among individuals with chronic disease: a systematic review and meta-analysis of randomized trials. PLoS ONE. (2021) 16:e0254995. doi: 10.1371/journal.pone.0254995
10. Lorig KR, Hurwicz ML, Sobel D, Hobbs M, Ritter PL. A national dissemination of an evidence-based self-management program: a process evaluation study. Patient Educ Couns. (2005) 59:69–79. doi: 10.1016/j.pec.2004.10.002
11. Agency for Healthcare Research Quality. Self-Management Support. (2013). Available online at: https://www.ahrq.gov/ncepcr/tools/self-mgmt/self.html (accessed January 27, 2023).
12. Lorig KR, Sobel DS, Ritter PL, Laurent D, Hobbs M. Effect of a self-management program on patients with chronic disease. Eff Clin Pract. (2001) 4:256–62.
13. Gebreab SY, Roux AVD, Brenner AB, Hickson DA, Sims M, Subramanyam M, et al. The impact of lifecourse socioeconomic position on cardiovascular disease events in African Americans: the Jackson Heart Study. J Am Heart Assoc. (2015) 4:e001553. doi: 10.1161/JAHA.114.001553
14. Kivimäki M, Batty GD, Pentti J, Shipley MJ, Sipilä PN, Nyberg ST, et al. Association between socioeconomic status and the development of mental and physical health conditions in adulthood: a multi-cohort study. Lancet Public Health. (2020) 5:e140–9. doi: 10.1016/S2468-2667(19)30248-8
15. Allen L, Williams J, Townsend N, Mikkelsen B, Roberts N, Foster C, et al. Socioeconomic status and non-communicable disease behavioural risk factors in low-income and lower-middle-income countries: a systematic review. Lancet Glob Health. (2017) 5:e277–89. doi: 10.1016/S2214-109X(17)30058-X
16. De Vogli R, Gimeno D, Kivimaki M. Socioeconomic Inequalities in Health in 22 European Countries. N Engl J Med. (2008) 358:2468–81. doi: 10.1056/NEJMsa0707519
17. Marmot M. UCL Institute of Health Equity, Review of Social Determinants and the Health Divide in the WHO European Region: Final Report. Geneva: World Health Organization, Regional Office for Europe (2014).
18. Kim K, Choi JS, Choi E, Nieman CL, Joo JH, Lin FR, et al. Effects of community-based health worker interventions to improve chronic disease management and care among vulnerable populations: a systematic review. Am J Public Health. (2016) 106:e3–e28. doi: 10.2105/AJPH.2015.302987a
19. Centers for Disease Control Prevention. Minority Health and Health Equity. (2022). Available online at: https://www.cdc.gov/minorityhealth/index.html (accessed September 02, 2022).
20. Tan SS, Pisano MM, Boone AL, Baker G, Pers Y-M, Pilotto A, et al. Evaluation design of EFFICHRONIC: the chronic disease self-management programme (CDSMP) intervention for citizens with a low socioeconomic position. Int J Environ Res Public Health. (2019) 16:1883. doi: 10.3390/ijerph16111883
21. Eurostat. NUTS—Nomenclature of Territorial Units for Statistics—Background. (2021). Available online at: https://ec.europa.eu/eurostat/web/nuts/background (accessed April 13, 2023).
22. Alvarez Rosete A, Pisano-González MM, Boone ALD, Vazquez-Alvarez R, Peñacoba-Maestre D, Valsecchi V, et al. Crossing intersectoral boundaries to reach out to vulnerable populations with chronic conditions in five European regions. Archiv Commun Med Public Health. (2021) 7:182–90. doi: 10.17352/2455-5479.000159
23. WONCA. International Classification of Primary Care. (2015). Available online at: https://www.globalfamilydoctor.com/site/DefaultSite/filesystem/documents/Groups/WICC/International%20Classification%20of%20Primary%20Care%20Dec16.pdf (accessed June 24, 2022).
24. Self-Management Resource Center,. History of SMRC Self-Management Programs. (2021). Available online at: https://selfmanagementresource.com/wp-content/uploads/2021/05/SMRC_Programs_History.pdf (accessed June 08, 2022).
25. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. (1977) 84:191–215. doi: 10.1037/0033-295X.84.2.191
26. Lorig K, Gonzalez V, Laurent D. The Chronic Disease Self-Management Workshop—An Evidence-Based Self-Management Workshop Originally Developed at Stanford University—LEADER'S MANUAL. Stanford, CA: Stanford University (1999).
27. Ory MG, Ahn S, Jiang L, Lorig K, Ritter P, Laurent DD, et al. National study of chronic disease self-management: six-month outcome findings. J Aging Health. (2013) 25:1258–74. doi: 10.1177/0898264313502531
28. Ritter PL, Lorig K. The English and Spanish Self-Efficacy to Manage Chronic Disease Scale measures were validated using multiple studies. J Clin Epidemiol. (2014) 67:1265–73. doi: 10.1016/j.jclinepi.2014.06.009
29. Booth M. Assessment of physical activity: an international perspective. Res Q Exerc Sport. (2000) 71(Suppl.2):114–20. doi: 10.1080/02701367.2000.11082794
30. Bush K, Kivlahan DR, McDonell MB, Fihn SD, Bradley KA. The AUDIT alcohol consumption questions (AUDIT-C): an effective brief screening test for problem drinking. Ambulatory Care Quality Improvement Project (ACQUIP) alcohol use disorders identification test. Arch Intern Med. (1998) 158:1789–95. doi: 10.1001/archinte.158.16.1789
31. Kroenke K, Strine TW, Spitzer RL, Williams JBW, Berry JT, Mokdad AH. The PHQ-8 as a measure of current depression in the general population. J Affect Disord. (2009) 114:163–73. doi: 10.1016/j.jad.2008.06.026
32. Ware J, Kosinski M, Keller SD. A 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validity. Med Care. (1996) 34:220–33. doi: 10.1097/00005650-199603000-00003
33. Brooks R. EuroQol: the current state of play. Health Pol. (1996) 37:53–72. doi: 10.1016/0168-8510(96)00822-6
34. Hawkins M, Gill SD, Batterham R, Elsworth GR, Osborne RH. The Health Literacy Questionnaire (HLQ) at the patient-clinician interface: a qualitative study of what patients and clinicians mean by their HLQ scores. BMC Health Serv Res. (2017) 17:309. doi: 10.1186/s12913-017-2254-8
35. Ortega Suárez FJ, Sánchez Plumed J, Pèrez Valentín MA, Pereira Palomo P, Muñoz Cepeda MA, Lorenzo Aguiar D, et al. Validation on the simplified medication adherence questionnaire (SMAQ) in renal transplant patients on tacrolimus. Nefrologia. (2011) 31:690–6.
36. AARP. Beyond 50.09 Survey Report. (2009). Available online at: https://assets.aarp.org/rgcenter/health/beyond_50_hcr.pdf (accessed July 07, 2022).
37. Garcia-Caselles P, Miralles R, Arellano M, Torres RM, Aguilera A, Pi-Figueras M, et al. Validation of a modified version of the Gijon's social-familial evaluation scale (SFES): the “Barcelona SFES Version”, for patients with cognitive impairment. Arch Gerontol Geriatr Suppl. (2004) 28:201–6. doi: 10.1016/j.archger.2004.04.028
38. Kuyken W, Hayes R, Barrett B, Byng R, Dalgleish T, Kessler D, et al. The effectiveness and cost-effectiveness of mindfulness-based cognitive therapy compared with maintenance antidepressant treatment in the prevention of depressive relapse/recurrence: results of a randomised controlled trial (the PREVENT study). Health Technol Assess. (2015) 19:1–124. doi: 10.3310/hta19730
39. Angst F, Aeschlimann A, Angst J. The minimal clinically important difference raised the significance of outcome effects above the statistical level, with methodological implications for future studies. J Clin Epidemiol. (2017) 82:128–36. doi: 10.1016/j.jclinepi.2016.11.016
40. Kroenke K, Wu J, Yu Z, Bair MJ, Kean J, Stump T, et al. Patient health questionnaire anxiety and depression scale: initial validation in three clinical trials. Psychosom Med. (2016) 78:716–27. doi: 10.1097/PSY.0000000000000322
41. Díaz-Arribas MJ, Fernández-Serrano M, Royuela A, Kovacs FM, Gallego-Izquierdo T, Ramos-Sánchez M, et al. Minimal clinically important difference in quality of life for patients with low back pain. Spine. (2017) 42:1908–16. doi: 10.1097/BRS.0000000000002298
42. Hu X, Jing M, Zhang M, Yang P, Yan X. Responsiveness and minimal clinically important difference of the EQ-5D-5L in cervical intraepithelial neoplasia: a longitudinal study. Health Qual Life Outcomes. (2020) 18:324. doi: 10.1186/s12955-020-01578-8
43. Hardman R, Begg S, Spelten E. What impact do chronic disease self-management support interventions have on health inequity gaps related to socioeconomic status: a systematic review. BMC Health Serv Res. (2020) 20:150. doi: 10.1186/s12913-020-5010-4
44. Shi J, Ferretti L, McCallion P. Attending with family members, completion rate and benefits accrued from chronic disease self-management program. Chronic Illn. (2022) 18:784–95. doi: 10.1177/17423953211032263
45. Marmot MG, Smith GD, Stansfeld S, Patel C, North F, Head J, et al. Health inequalities among British civil servants: the Whitehall II study. Lancet. (1991) 337:1387–93. doi: 10.1016/0140-6736(91)93068-K
46. Mahmood SS, Levy D, Vasan RS, Wang TJ. The Framingham Heart Study and the epidemiology of cardiovascular disease: a historical perspective. Lancet. (2014) 383:999–1008. doi: 10.1016/S0140-6736(13)61752-3
47. Chomistek AK, Manson JE, Stefanick ML, Lu B, Sands-Lincoln M, Going SB, et al. Relationship of sedentary behavior and physical activity to incident cardiovascular disease: results from the Women's Health Initiative. J Am Coll Cardiol. (2013) 61:2346–54. doi: 10.1016/j.jacc.2013.03.031
48. Kessler KM. Primary prevention of coronary heart disease in women through diet and lifestyle. N Engl J Med. (2000) 343:16–22. doi: 10.1056/NEJM200007063430103
49. Pols MA, Peeters PH, Twisk JW, Kemper HC, Grobbee DE. Physical activity and cardiovascular disease risk profile in women. Am J Epidemiol. (1997) 146:322–8. doi: 10.1093/oxfordjournals.aje.a009273
50. German C, Makarem N, Fanning J, Redline S, Elfassy T, McClain A, et al. Sleep, sedentary behavior, physical activity, and cardiovascular health: MESA. Med Sci Sports Exerc. (2021) 53:724–31. doi: 10.1249/MSS.0000000000002534
51. Shah AD, Vittinghoff E, Kandula NR, Srivastava S, Kanaya AM. Correlates of prediabetes and type II diabetes in US South Asians: findings from the Mediators of Atherosclerosis in South Asians Living in America (MASALA) study. Ann Epidemiol. (2015) 25:77–83. doi: 10.1016/j.annepidem.2014.10.013
52. Perel P, Avezum A, Huffman M, Pais P, Rodgers A, Vedanthan R, et al. Reducing premature cardiovascular morbidity and mortality in people with atherosclerotic vascular disease: the world heart federation roadmap for secondary prevention of cardiovascular disease. Glob Heart. (2015) 10:99–110. doi: 10.1016/j.gheart.2015.04.003
53. Lorig KR, Ritter P, Stewart AL, Sobel DS, Brown BW, Bandura A, et al. Chronic disease self-management program: 2-year health status and health care utilization outcomes. Med Care. (2001) 39:1217–23. doi: 10.1097/00005650-200111000-00008
54. Korenhof SA, Rouwet EV, Elstgeest LEM, Tan SS, Macchione S, Vasiljev V, et al. Evaluation of an intervention to promote self-management regarding cardiovascular disease: the social engagement framework for addressing the chronic-disease-challenge (SEFAC). Int J Environ Res Public Health. (2022) 19:2013145. doi: 10.3390/ijerph192013145
55. Sakakibara BM, Kim AJ, Eng JJ. A systematic review and meta-analysis on self-management for improving risk factor control in stroke patients. Int J Behav Med. (2017) 24:42–53. doi: 10.1007/s12529-016-9582-7
56. Melnyk BM, Kelly SA, Stephens J, Dhakal K, McGovern C, Tucker S, et al. Interventions to improve mental health, well-being, physical health, and lifestyle behaviors in physicians and nurses: a systematic review. Am J Health Promot. (2020) 34:929–41. doi: 10.1177/0890117120920451
57. Mosalman Haghighi M, Mavros Y, Fiatarone Singh MA. The effects of structured exercise or lifestyle behavior interventions on long-term physical activity level and health outcomes in individuals with type 2 diabetes: a systematic review, meta-analysis, and meta-regression. J Phys Act Health. (2018) 15:697–707. doi: 10.1123/jpah.2017-0589
58. Cabrera AG, Caballero P, Wanden-Berghe C, Sanz-Lorente M, López-Pintor E. Effectiveness of workplace-based diet and lifestyle interventions on risk factors in workers with metabolic syndrome: a systematic review, meta-analysis and meta-regression. Nutrients. (2021) 13:124560. doi: 10.3390/nu13124560
59. Bull ER, McCleary N, Li X, Dombrowski SU, Dusseldorp E, Johnston M. Interventions to promote healthy eating, physical activity and smoking in low-income groups: a systematic review with meta-analysis of behavior change techniques and delivery/context. Int J Behav Med. (2018) 25:605–16. doi: 10.1007/s12529-018-9734-z
60. Turner RR, Steed L, Quirk H, Greasley RU, Saxton JM, Taylor SJ, et ak. Interventions for promoting habitual exercise in people living with and beyond cancer. Cochrane Database Syst Rev. (2013) 2013:CD010192. doi: 10.1002/14651858.CD010192.pub2
61. Rautio N, Jokelainen J, Oksa H, Saaristo T, Peltonen M, Niskanen L, et al. Socioeconomic position and effectiveness of lifestyle intervention in prevention of type 2 diabetes: one-year follow-up of the FIN-D2D project. Scand J Public Health. (2011) 39:561–70. doi: 10.1177/1403494811408482
62. Abbott S, Smith E, Tighe B, Lycett D. Group versus one-to-one multi-component lifestyle interventions for weight management: a systematic review and meta-analysis of randomised controlled trials. J Hum Nutr Diet. (2021) 34:485–93. doi: 10.1111/jhn.12853
63. Rodrigues AL, Ball J, Ski C, Stewart S, Carrington MJ. A systematic review and meta-analysis of primary prevention programmes to improve cardio-metabolic risk in non-urban communities. Prev Med. (2016) 87:22–34. doi: 10.1016/j.ypmed.2016.02.011
64. Farrell K, Wicks MN, Martin JC. Chronic disease self-management improved with enhanced self-efficacy. Clin Nurs Res. (2004) 13:289–308. doi: 10.1177/1054773804267878
65. Swerissen H, Belfrage J, Weeks A, Jordan L, Walker C, Furler J, et al. A randomised control trial of a self-management program for people with a chronic illness from Vietnamese, Chinese, Italian and Greek backgrounds. Patient Educ Couns. (2006) 64:360–8. doi: 10.1016/j.pec.2006.04.003
66. Morton D, Rankin P, Kent L, Dysinger W. The complete health improvement program (CHIP): history, evaluation, and outcomes. Am J Lifestyle Med. (2016) 10:64–73. doi: 10.1177/1559827614531391
67. Salas-Salvadó J, Bulló M, Babio N, Martínez-González MÁ, Ibarrola-Jurado N, Basora J, et al. Reduction in the incidence of type 2 diabetes with the Mediterranean diet: results of the PREDIMED-Reus nutrition intervention randomized trial. Diabet Care. (2011) 34:14–9. doi: 10.2337/dc10-1288
68. Knowler WC, Barrett-Connor E, Fowler SE, Hamman RF, Lachin JM, Walker EA, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. (2002) 346:393–403. doi: 10.1056/NEJMoa012512
69. Burgess E, Hassmén P, Welvaert M, Pumpa KL. Behavioural treatment strategies improve adherence to lifestyle intervention programmes in adults with obesity: a systematic review and meta-analysis. Clin Obes. (2017) 7:105–14. doi: 10.1111/cob.12180
70. Deslippe AL, Soanes A, Bouchaud CC, Beckenstein H, Slim M, Plourde H, et al. Barriers and facilitators to diet, physical activity and lifestyle behavior intervention adherence: a qualitative systematic review of the literature. Int J Behav Nutr Phys Act. (2023) 20:14. doi: 10.1186/s12966-023-01424-2
71. Kim SH, Youn CH. Efficacy of chronic disease self-management program in older Korean adults with low and high health literacy. Asian Nurs Res. (2015) 9:42–6. doi: 10.1016/j.anr.2014.10.008
72. Muscat DM, Song W, Cvejic E, Ting JHC, Medlin J, Nutbeam D. The impact of the chronic disease self-management program on health literacy: a pre-post study using a multi-dimensional health literacy instrument. Int J Environ Res Public Health. (2019) 17:58. doi: 10.3390/ijerph17010058
73. Zhang SY, Wu F, Tang DL, Rong XS, Guo QH, Fang M, et al. Pilot testing the caregiver self-management intervention for caregivers of relatives with dementia. Geriatr Nurs. (2020) 41:147–57. doi: 10.1016/j.gerinurse.2019.08.006
74. Nightingale C, Sterba KR, Levine B, Tooze JA, Greven K, Frizzell B, et al. Feasibility and acceptability of a multi-modality self-management intervention for head and neck cancer caregivers: a pilot randomized trial. Integr Cancer Ther. (2022) 21:15347354221098984. doi: 10.1177/15347354221098984
Keywords: chronic disease management, self-management, risk factors, vulnerable populations, socioeconomic factors, caregivers
Citation: Korenhof SA, Rouwet EV, Elstgeest LEM, Fierloos IN, Tan SS, Pisano-Gonzalez MM, Boone ALD, Pers Y-M, Pilotto A, López-Ventoso M, Diez Valcarce I, Zhang X and Raat H (2023) The effect of a community-based group intervention on chronic disease self-management in a vulnerable population. Front. Public Health 11:1221675. doi: 10.3389/fpubh.2023.1221675
Received: 12 May 2023; Accepted: 24 July 2023;
Published: 21 August 2023.
Edited by:
Leo Pruimboom, Pontifical University of Salamanca, SpainReviewed by:
Ozayr Mahomed, University of KwaZulu-Natal, South AfricaChris Barton, Monash University, Australia
Copyright © 2023 Korenhof, Rouwet, Elstgeest, Fierloos, Tan, Pisano-Gonzalez, Boone, Pers, Pilotto, López-Ventoso, Diez Valcarce, Zhang and Raat. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hein Raat, aC5yYWF0QGVyYXNtdXNtYy5ubA==