Abstract
Introduction:
Physical therapy encompasses a broad range of treatment options, often utilized in clinical settings where pharmaceutical interventions are standard. The potential for physical therapy to contribute to sustainable healthcare by reducing environmental impact, while maintaining the quality of care, remains underexplored. This study aimed to map existing research comparing physical therapy to pharmaceuticals, with a specific focus on whether these studies address aspects of sustainable development.
Methods:
A scoping review was conducted, systematically searching the PubMed, Cinahl, and Pedro databases using keywords related to physical therapy, pharmaceuticals, and comparative studies. Two assessors independently reviewed and selected relevant studies, followed by data extraction and summarization of results.
Results:
A total of 27 studies were included, varying in design, population, and healthcare context. The most commonly addressed conditions were osteoarthritis and musculoskeletal pain, with analgesics being the most frequently studied pharmaceutical interventions. While several studies touched upon economic and social dimensions of sustainable development, none examined environmental sustainability. This highlights a critical gap in current research.
Discussion:
Future studies are needed to assess how physical therapy, when compared to pharmaceutical treatments, can contribute to sustainable healthcare by offering a low-carbon, resource-efficient alternative without compromising social sustainability through adverse effects. This knowledge could be instrumental in guiding healthcare systems toward more sustainable practices.
Systematic review registration:
A study protocol was registered in Open Science Framework 2023-03-31 (Available from: https://osf.io/we58g).
Introduction
Healthcare accounts for a significant share of global greenhouse gas emissions, i.e., carbon footprint, and the largest share is due to the production, transport and consumption of goods and services such as pharmaceuticals and other chemicals, foods and medical equipment (1, 2). Thus, healthcare has a responsibility to actively participate in the transition towards sustainable development (2), defined as ‘development that meets the needs of the present without compromising the ability of future generations to meet their own needs’, involving economic, environmental and social sustainability (3). A sustainable healthcare builds on the three dimensions of sustainable development (2, 4), and is defined as a system that maintains and improves the health of current generations while minimizing damage to the environment and ensuring health for future generations (4). Four key elements have been identified to enable sustainable healthcare (5): disease prevention and health promotion to reduce the need for healthcare; self-management and empowerment of patients to take a greater role in managing their own health and healthcare; lean service delivery and; prioritizing low carbon alternatives (2).
The three dimensions of sustainable development are further described in the business framework the Triple Bottom Line (6). This framework argues that for a business to be sustainable, it needs to consider not only the economic aspect, but also the environmental and social aspects of operations. In other words, it must consider for example air pollution and greenhouse gas emissions, and the health and wellbeing of employees and clients (6). Triple Bottom Line has since its’ introduction been employed in studies (2, 4, 7). The Triple Bottom Line has been found particularly interesting in healthcare since health is directly and indirectly determined by ecological and social aspects (8).
From the perspective of physical therapy (PT), individuals have inherent resources to maintain or improve their health on their own or with the facilitation of others (9). In PT, support for behavioral change, maintenance and resumption of activities, function and abilities, and the promotion of patient empowerment are central concepts (7). The concept of empowerment is based on the idea that people themselves have the ability and resources to define their own problems and devise action strategies to deal with them. Behavior change is an important part of health promotion and disease prevention (10), together with patient education and rehabilitation (10). The fact that PT is a treatment option without the direct environmental impact of, for example, pharmaceuticals (11) implies PT is key for sustainable healthcare.
Pharmaceutical care is the responsible provision of pharmaceuticals (e.g., drugs, medicines) for the purpose of achieving outcomes that improve a patient’s quality of life (12). Pharmaceuticals affect physiological processes in the body, usually by binding to various proteins (13). Pharmaceuticals are usually chemically stable substances, allowing them to withstand a certain passage through the body before they reach their area of action (13). These properties and ways of acting in pharmaceuticals are primarily intended to promote treatment outcomes, but they can also have negative effects through various adverse effects in the user as well as a negative impact on the environment (13).
The adverse effects of pharmaceuticals can vary in severity and depend, among other things, on the substance used, who is using them, and in what dose (3). Side effects of pharmaceuticals have a major impact on society, leading to high costs, increased morbidity requiring care, and risk of death (12). The production and consumption of pharmaceuticals contribute to a global problem of pollution in water and soil (5, 6). These pollutants affect human health and the lives of plants and animals and have been identified as major problems in several countries (14–16). The groups of pharmaceuticals most abundant in the environment are analgesics, specifically Non-steroidal Anti-Inflammatory Drugs (NSAIDs) (17).
The use of pharmaceuticals leads to negative environmental impact and possible negative side effects for the individual. PT as a treatment has been shown to have an effect in several areas where pharmaceuticals are commonly used, such as high blood pressure, depression, diabetes, and osteoarthritis (11, 18). However, there is a lack of collective knowledge about the areas in which PT could influence pharmaceutical use. This is an important area, as this knowledge could contribute the transition to sustainable healthcare. The aim of this study was to investigate what research, in form of scientific articles, is available that study PT in relation to pharmaceuticals. The aim was also to investigate whether this research relates their results to sustainable development regarding environmental-, social- or economic aspects.
Methods
Study design
This study utilized a scoping review methodology to investigate the extent and type of available research. The methodological framework proposed by Arksey and O’Malley (19) was followed, with some additions from Levac et al. (20). A study protocol was registered in Open Science Framework 2023-03-31 (Available from: https://osf.io/we58g) and the PRISMA ScR Checklist was used when reporting the results (21).
Research questions
The research questions guiding this scoping review were formulated as follows:
-
What research exists that compares PT and pharmaceutical treatments, or that assesses pharmaceutical use/prescription as outcomes from PT?
-
To what extent are aspects of sustainable development addressed, in articles on PT in relation to pharmaceuticals?
Literature search
A comprehensive literature search was conducted on 2023-02-20 to identify relevant studies. PubMed, Cinahl, and PEDro databases were searched using combinations of keywords related to PT, pharmaceuticals, and comparative studies, with no limitation on the date (Table 1). The search strategy was adjusted based on sample searches, and consultations with a librarian, to optimize search results.
Table 1
| Search | Hits | |
|---|---|---|
| PubMed | (physical therapy modalities OR physical therapy specialty OR physiotherapy) AND (pharmaceutical preparations OR pharmaceutical intervention OR drugs) AND (comparative study) NOT (animals OR animal experimentation) | 771 |
| Cinahl | (physical therapy modalities OR physical therapy specialty OR physiotherapy) AND (pharmaceutical preparations OR pharmaceutical intervention OR drugs) AND (comparative study) NOT (animals OR animal experimentation) | 229 |
| PEDro | physi* pharmaceutical* compar* | 63 |
| physi* drugs* compar* | 191 |
Overview of the search strategy.
Study selection
Based on the following inclusion and exclusion criteria, studies were selected from the search result:
Inclusion Criteria:
-
Original articles and study protocols that in some way compare PT and pharmaceuticals as treatment options, with PT explicitly mentioned as PT by the authors, or interventions performed or supervised by a physical therapist, or performed in a PT clinic.
-
Studies that evaluate pharmaceutical consumption as an outcome measure via either intake or via prescription, or by evaluating a pharmaceutical treatment as an intervention.
Exclusion Criteria:
-
Articles involving animal studies.
-
Articles not available in English.
The selection process was performed by two assessors independently (PS and MJ), with the help of Rayyan.ai software, and started with screening of titles and abstracts. Relevant articles were further assessed by reading their full texts. Inclusion and exclusion criteria were applied individually by the authors. The selection was based on agreement and discrepancies were identified and resolved through discussion within the author group, until consensus was reached.
Data charting
Data from the included studies were extracted and organized into a table. The collected information included author details, year of publication, study location, study design, intervention type, study population, research purpose, methodology, outcome measures, significant results, and aspects of sustainable development.
Collating, summarizing, and reporting the results
The included articles were analyzed and presented in relation to the research questions, in terms of their characteristics, physical therapy interventions, types of pharmaceuticals, pharmaceutical consumption as an outcome measure, and discussions related to sustainable development. The scoping review aimed to provide an overview of the available research rather than conducting a synthesis of the evidence.
Results
The search in PubMed, Cinahl and PEDro resulted in 1254 articles (Figure 1) of which 45 duplicates were detected and deleted, leaving 1,209 unique articles for title screening. Out of 1,209 articles, 68 were selected for further review of abstract after the title screening based on the study’s inclusion- and exclusion criterium. The abstracts were then reviewed, and 66 studies were selected for full-text review. Finally, 27 articles (22–48) were included after the study selection process, the most common reason for studies not being included was that they did not address PT explicitly as treatment (Figure 1).
Figure 1
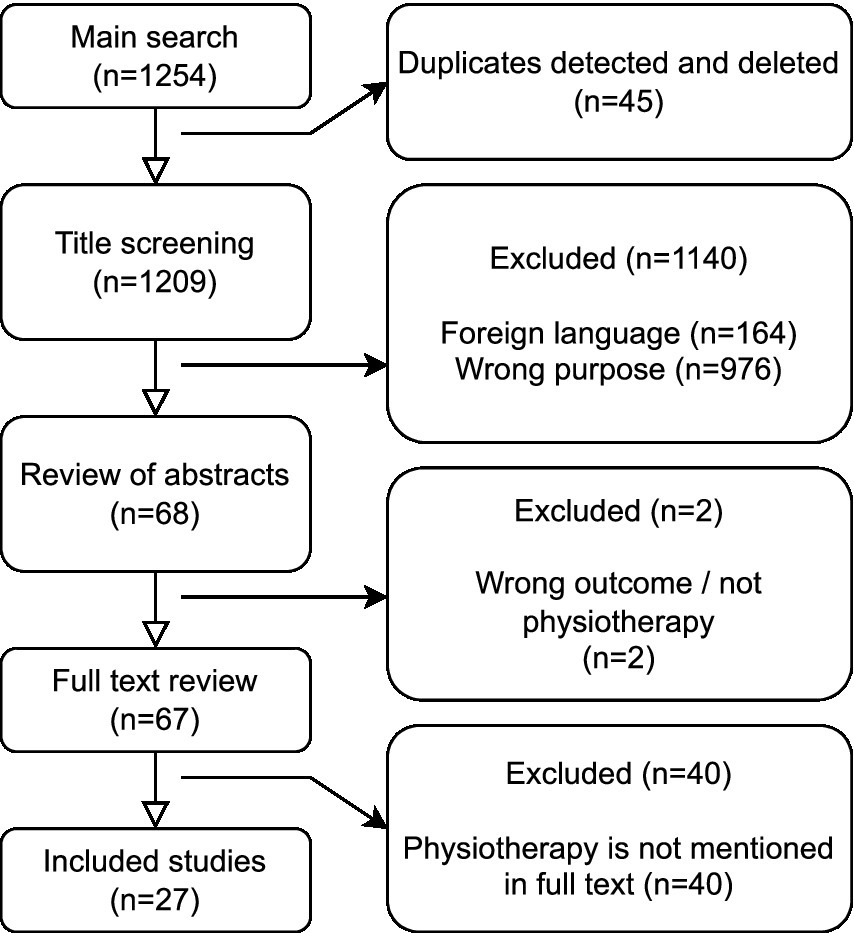
Flow chart of main search and inclusion process.
The included studies (22–48) were published between 1998 and 2022 and conducted in 15 different countries, with the most studies conducted in Turkey (23, 37, 39–41, 47, 48) and the USA (24, 25, 34, 46) (Table 2). Most of the studies (17 out of 27) were randomized controlled trials (23, 24, 28–31, 35, 39–42, 44–48), and another four had a randomized design (26, 27, 37, 38), three of the studies where retrospective (25, 34, 36), one was a prospective observational study (43), one was an open-label alternate patient treatment allocation study (33) and two were study protocols (27, 32). The most common diagnoses in the included studies were osteoarthritis (OA), back pain and shoulder pain. The other studies commonly included musculoskeletal diagnoses, but also respiratory and gynecological diagnoses.
Table 2
| Author, year, country, study design | Objectives | Population (age, diagnosis, sex, number) | Physical therapy | Pharmaceuticals | Outcomes | Overall results | Sustainable development perspective |
|---|---|---|---|---|---|---|---|
| Uygur, E. et al. (2019), Turkey (48) Randomized controlled trial |
To compare dry needling with cortisone injection as treatment for plantar fasciitis. | 96 patients with plantar fasciitis that required continued treatment after 3 weeks of initial treatment. 66% female. Mean age ≈ 49.6. |
Dry needling in the plantar fascia 2 times per week on 5 occasions. |
Corticosteroid containing: Methylprednisolone acetate; Bupivacaine. 1 injection into the plantar fascia. |
Pain, Proms function | Positive effects in favor of dry needling, when compared with injections after 6 months. | Environmental: no Economic: yes Social: no |
| Deyle, Gail D. et al. (2020), USA (46) Randomized controlled trial |
To examine differences in treatment effectiveness for pain and physical function in the short and long term regarding injection and PT. | 156 patients with knee OA. 48% female. Mean age ≈ 56.1. |
Passive joint mobilization and strength training ≤8 sessions over 4–6 weeks +1–3 sessions at the time of the 4-month and 9-month reassessments |
Glucocorticoid steroids containing: Triamcinolone acetonide; Lidocaine. 1–3 injections. |
Proms function, Health economics, Functional tests | Positive effects on pain and physical function in favor of PT, when compared to injections after 12 months. | Environmental: no Economic: yes Social: no |
| Bakilan, F. & Ortanca, B. (2021), Turkey (37) Non-randomized controlled trial |
To compare the patient satisfaction and pain relief firstly between patients who received pharmacological treatment and non-pharmacological treatment. | 109 patients with chronic low back pain. 65.14% female. Mean age ≈ 47.9. |
Hotpack; Therapeutical ultrasound; TENS | NSAID; Myorelaxant; Lidocaine | Pain, Proms satisfaction | Positive effects on pain and satisfaction in favor of PT, when compared to pharmaceutical care. | Environmental: no Economic: yes Social: no |
| Bisset, L. et al. 2006, Australia (22) Randomized controlled trial |
To investigate the efficacy of PT compared with a wait and see approach or corticosteroid injections over 52 weeks in tennis elbow. | 198 adults with a clinical diagnosis of tennis elbow ≥6 weeks, who had not received any other active treatment by a health practitioner in the previous 6 months. 35% female. Mean age ≈ 47.6. |
8 sessions of elbow manipulation and therapeutic exercises over 6 weeks + home exercise with resistance exercise band. Patient education to all participants. |
Corticosteroid containing: Lidocaine; Triaminolone acetonide. 1–2 injections. Patient education to all participants. |
Pain, Proms function, Function tests, Assessor rating of severity | Positive effects in favor of CSI, compared with PT after 6 weeks. Positive effects in favor of PT at long time assessment when compared to CSI. | Environmental: no Economic: no Social: no |
| Hamzat, Talhatu K. et al. (2011), Nigeria (38) Quasi-experimental study |
To determine the respective and combined effects of NSAIDs and PT in management of pain and reduced functional limitation among patients with concurrent hypertension and knee OA. | 33 patients with both high blood pressure and knee OA of which 29 completed the study. 65.52% female. Mean age ≈ 65.7. |
TENS; Strength training 3 times per week 8 weeks treatment period. |
Anti-hypertensive drugs; NSAID 8 weeks treatment period. |
Pain, Proms function | No significant differences between groups. | Environmental: no Economic: yes Social: yes |
| el Refaye, G. E. et al. (2019), Egypt (45) Randomized, single-blind, controlled trial |
To determine which is more effective in alleviating primary dysmenorrhea: PEMF or diclofenac drugs. | 50 females with regular menstruation. Mean age ≈ 21.88. |
PEMF on the pelvic region. 3 occasions per menstrual cycle during 3 cycles |
Diclofenac when in pain during 3 menstrual cycles. | Pain, Blood test, Proms symptoms | Positive effects on all outcomes, in favor of PT, when compared to pharmaceuticals. | Environmental: no Economic: no Social: no |
| Gür, A. et al. (2002), Turkey (47) Randomized, single-blind, placebo-controlled study |
To examine the effectiveness of low power laser and low-dose amitriptyline therapy and to investigate effects of these therapy modalities on clinical symptoms and QoL in patients with fibromyalgia. | 75 patients with fibromyalgia. 80% female. Mean age ≈ 30. |
Laser therapy. Every weekday for 2 weeks. |
Amitriptyline daily for 8 weeks. | Pain, pain assessment, proms symptoms, proms QoL and mental health | Positive effects on pain and fatigue, in favor of PT, when compared to pharmaceuticals. Positive effects on mental health, in favor of pharmaceuticals, when compared to PT. | Environmental: no Economic: no Social: yes |
| Koc, Z. et al. (2009), Turkey (39) Randomized, single-blind, controlled trial |
To compare the effects of epidural steroid injections and PT on pain and function in patients with LSS. | 29 patients with lumbar spinal stenosis. 72.41% female. Mean age ≈ 59.1. |
Ultrasound; Hot pack; TENS 5 times per week for 2 weeks; All participants: home-exercise for 6 months, diclofenac for 2 weeks. |
Steroid containing: Triamcinolon acetonide; Bupivacaine hydrochloride; Physiologic saline. Epidural injection. All participants: home-exercise for 6 months, diclofenac for 2 weeks. |
Pain, functional tests | No significant differences between groups. | Environmental: no Economic: no Social: no |
| Atamaz, F. et al. (2006), Turkey (40) Randomized, single-blind study |
To compare the effects of PT and two different intra-articular hyaluronan drugs (sodium hyaluronate (NaHA) and hylan G-F 20) on knee OA. | 82 patients with knee OA. 81.71% female. Mean age ≈ 60. |
Infrared; Short-wave diathermy pulsed patterns; Interferential therapy. | NaHA containing: 15 mg Sodium hyaluronate and 9 mg Sodium chloride. Hylan G-F 20 containing: 8 mg HA, 0.16 mg Sodium chloride and 0.04 mg Sodium dihydrogen phosphate hydrate. Intraarticular injection. |
Pain, functional tests, Proms function, Proms QoL | Positive effects on pain and QoL, in favor of PT, when compared to injections. Positive effects on mental health, in favor of Injections, when compared to PT. | Environmental: no Economic: yes Social: yes |
| Paker, N. et al. (2006), Turkey Prospective Randomized Study |
To investigate the efficacy of TENS and of intra-articular hylan G-F 20 injection in terms of pain, functional status, and QoL parameters in patients with knee OA, and to monitor effects of treatment over a 26-week follow-up period. | 52 patients with knee OA. No information regarding gender. Mean age ≈ 58.92. |
TENS 20 min 5 times per week for 3 weeks. |
Hylan G-F 20 3 intraarticular knee injections once per week. |
Pain, Functional tests, Proms function, Proms QoL | No significant differences between groups. | Environmental: no Economic: no Social: no |
| Sadeghifar, Amirreza et al. (2022), Iran (36) Retrospective comparative study |
To evaluate the efficacy of Subacromial CSI, HA injection and PT in patients with SIS to determine which treatment is most effective. | 88 patients with subacromial impingement syndrome. 53.41% female. Mean age ≈ 43. |
Stretching exercises; Specific strength training for shoulder muscles; Hot pack; TENS; Ultrasound. 3 sessions per week for 3 weeks followed by home exercises for 1 month |
Triamcinolone; HA 2 CSI with 2 week interval. |
Pain, Proms function | Positive effects, in favor of CSI, when compared to PT at 3 and 6 months. | Environmental: no Economic: no Social: no |
| Arslan, S. & Celiker, R (2001), Turkey (23) Randomized controlled trial |
To compare the efficacy of local steroid injection and PT measures for treating adhesive capsulitis. | 20 patients with shoulder pain and limited ROM. 50% female. Mean age ≈ 56. |
Hot pack; Ultrasonic therapy; Passive glenohumeral joint stretching exercises; Specific shoulder exercises such as wall climbing | NSAID; Steroid containing: Methylprednisolone acetate. Local CSI. |
Pain, ROM | No significant differences between groups. | Environmental: no Economic: no Social: no |
| Naikmasur, V. G. et al. (2009), India (42) Randomized controlled trial |
To assess the effectiveness of PT methods in myofascial pain patients and to compare with pharmacotherapy comprising of a combination of muscles relaxants and NSAID. | 40 patients with myofascial pain of masticatory muscles. 57% female. Mean age ≈ 34.76. |
TENS; Ultrasound; Helium-neon laser | Ibuprofen; Paracetamol; Chlorzoxazone. 2 times per day for 5 days |
Pain, pain assessment, Functional tests, Proms function | Positive effects on pain and function, in favor of PT, when compared to pharmaceutical care. | Environmental: no Economic: yes Social: yes |
| Lahti, M. et al. (2008), New Zealand (26) Pilot randomized trial. |
To assess the ease of the day-to-day running and to review the implementation of the trial protocol. The secondary objective for the pilot study was to compare the treatments, that is, the primary objective for the main study. | 57 female with predominant urge urinary incontinence experiencing at least monthly leakage. Mean age ≈ 55. |
Bladder retraining therapy containing: Patient information and education; Pelvic floor muscle training. 3 months. |
Anticholinergic drug: Oxybutynin; Tolterodin 3 months. |
Proms QoL, Proms symptoms | No significant differences between groups. | Environmental: no Economic: yes Social: yes |
| Galán-Martín, Miguel A. et al. (2019), Spain (27) Study protocol for a randomized, multicenter clinical trial |
To evaluate the effectiveness and cost-effectiveness of a program based on active coping strategies that include Pain Neuroscience Education and physical exercise by means of a randomized clinical trial compared to usual care in primary care PT. | Patients with non-specific back pain of ≥6 months. Age 18–70 years. |
Pain neuroscience education program in 6 sessions (10 h) + group exercise 18 sessions led by physical therapist; Usual primary care PT consisting of 15 sessions of analgesic electrotherapy, thermotherapy and standardized physical exercise. | - | Pain, pain assessment, Proms QoL, Proms symptoms, Satisfaction, Pharmaceutical use.; Health Services visits; | Not applicable (study protocol) | Environmental: no Economic: yes Social: yes |
| Henderson, J. et al. (2020), Australia (43) A prospective observational study |
To identify if a collaborative care ED PCP after-hours service would result in improvements in ED treatment times for musculoskeletal and simple orthopedic presentations compared with patients managed under a secondary contact model of care. Secondary aims to identify if there were differences in orthopedic, follow-up plans on discharge, and analgesia prescriptions. | 1,640 patients in ED setting. No information regarding gender. Age ≥ 16 years. |
Primary or secondary contact for patients in ED | Analgesics | Mean treatment time, orthopedic or GP referrals, Prescribed analgesics | Positive effects on referrals, prescriptions and early discharge, in favor of primary contact PT, when compared to secondary contact PT. | Environmental: no Economic: yes Social: no |
| den Hertog, A. et al. (2012), Germany (28) Randomized prospective clinical study |
To investigate fast-track rehabilitation concept in terms of a measurable effect on the early recovery after TKA. | 147 patients that had underwent TKA surgery. 70.75% female. Mean age ≈ 67. |
Fast-track rehabilitation: Group therapy; Early mobilization and individual PT. Standard rehabilitation: Individual postoperative care according to existing protocol. |
Analgesics | Proms function, Length of hospital stay, Consumption of analgesics | Positive effects on function, Consumption of analgesics, and length of stay, in favor of Fast-track rehabilitation, when compared to standard rehabilitation. | Environmental: no Economic: yes Social: no |
| Rhon, Daniel I. et al. (2014), USA (24) Randomized controlled trial |
To compare the effectiveness of 2 common non-surgical treatments for SIS. | 98 patients with subacromial impingement syndrome. 31.63% female. Mean age ≈ 41. |
Joint and soft-tissue mobilizations; Manual stretches; Contract-relax techniques; Reinforcing exercises directed to the shoulder girdle or thoracic/cervical spine | Triamcinolone acetonide. CSI. |
Pain, Proms function, Shoulder-related health care use, Number of additional injections | Positive effects on health care use, in favor of PT, when compared to CSI. No significant differences between groups in pain and function. | Environmental: no Economic: yes Social: no |
| Brose, Steven W. et al. (2019), USA (25) Retrospective analysis |
To determine the success of a multidisciplinary project to manage chronic pain while reducing reliance on opioids in a population of patients with spinal cord injury. | Individuals with spinal chord injury receiving outpatient care. | Exercises. | Opioids | Opioid prescription rate; Number of patients receiving opioids; Equivalent morphine quantity | Positive effects on opioid prescription rate and number of patients receiving opioids, in favor or the multidisciplinary project, compared to previous care. | Environmental: no Economic: no Social: yes |
| Gallefoss, F. (2004), Norway (35) Randomized controlled trial |
To explore the effects and health economic consequences of patient education in patients with COPD in a 12-month follow-up. | 62 patients with mild to moderate COPD. 50% female. Mean age ≈ 58. |
Patient education regarding breathing and coughing, exercising and management of attacks. | Beta2-agonist inhalation; Ipratropium bromide; Salbutamol | Number of GP consultations; Proportions in need of GP consultations; Utilization of rescue pharmaceuticals; Patient satisfaction | Positive effects on GP consultations, in favor of patient education, when compared to a group with no education. | Environmental: no Economic: yes Social: no |
| van Baar, M. E. et al. (1998), Netherlands (30) Randomized, single-blind, clinical trial |
To determine the effectiveness of exercise therapy in patients with OA of hip or knee. | 201 patients with osteoarthritis of the hip or knee. 78.11% female. Mean age ≈ 68. |
Exercise therapy from physical therapist. 12 weeks |
NSAID; Paracetamol | Pain, Functional tests, Proms effect, ROM, Pharmaceutical use. | Positive effects on pain, function and pharmaceutical use, in favor of PT, when compared to treatment as usual. | Environmental: no Economic: no Social: no |
| van Baar, M. E. et al. (2001), Netherlands (29) Randomized, single-blind, clinical trial |
To determine whether the effects of exercise therapy in patients with OA of hip or knee are sustained after 6 and 9 months’ follow up. | 183 patients with osteoarthritis of the hip or knee. 85.79% female. Mean age ≈ 68. |
Exercise therapy from physical therapist. 12 weeks |
NSAID; Paracetamol | Pain, Functional tests, Proms effect, ROM, Pharmaceutical use. | Positive effects on pain, in favor of PT, was found at 24 weeks, but no differences remained at 36 weeks. | Environmental: no Economic: no Social: no |
| Hay, E. M. et al. (2006), UK (31) Pragmatic multicenter randomized clinical trial. |
To compare the clinical effectiveness, in primary care, of enhanced pharmacy review or community PT with that of a control intervention (advice leaflet reinforced by atelephone call) in the treatment of adults aged 55 years and over consulting their GP with knee pain. | 325 adults with knee pain. 64.33% female. Mean age ≈ 67.7. |
Patient education about the safety and importance of exercise, pacing, pain relief, and coping strategies; Individualized exercise program. | NSAID; Analgesics | Pain, Proms function | Self-reported use of NSAID and simple analgesia was significantly lower in the PT group compared to the control group. For the pharmacy group, the use of NSAID was significantly lower and the use of simple analgesia significantly higher compared to the control group. | Environmental: no Economic: yes Social: yes |
| Clausen, B. et al. (2014), Denmark (32) Study protocol for a randomized, single-blind, controlled trial |
To compare the efficacy of a specific neuromuscular exercise program with optimized analgesics and anti-inflammatory drug use on knee loads, as well as pain and physical function in people with mild to moderate medial tibiofemoral knee OA. | 100 patients with knee OA. Age 40–70 years. |
Exercises to improve balance, muscle activation, functional alignment, and functional joint stability. | NSAID; Acetaminophen | Pain, Functional tests, QoL, Pharmaceutical use. | Not applicable (study protocol) | Environmental: no Economic: yes Social: yes |
| Joshi, M. N. et al. (2009), India (33) Open-label alternate patient treatment allocation |
To compare the performance of PT and amitriptyline for disability reduction in patients with fibromyalgia. To determine which clinical features at baseline would predict benefit with either therapy. | 156 outpatients with fibromyalgia syndrome. 96.15% female. Mean age ≈ 39. |
Specific exercises; Relaxation; Stretching; Strength training | Amitriptyline; Tramadol | Proms function, Pharmaceutical use (tramadol). | No significant differences between groups. | Environmental: no Economic: yes Social: yes |
| Gagnon, R. et al. (2021), Canada (44) Randomized controlled trial |
To compare the effects of direct-access PT to usual care provided by an emergency physician for patients presenting to the ED with a MSKD. | 78 patients with minor MSKD. 44% female. Mean age ≈ 40.2. |
Direct access to physical therapist in the ED including: Physical examination; Patient education; Interventions based on the clinical analysis and physical therapists diagnosis (technical aids, imaging, prescribed or over-the-counter medication, consults with other health care professionals) |
Opioids; Over-the-counter drugs | Pain, Utilization of services and resources at ED; Health care professionals consulted; Imaging tests recommended | Positive effects on clinical outcomes and utilization of services and resources, in Favor of the direct access PT, when compared to usual care after discharge and 3 months later. | Environmental: no Economic: yes Social: yes |
| Kim, Howard S. et al. (2019), USA (34) Retrospective cohort study |
To compare analgesic prescribing among ED visits for back or neck pain receiving PT versus usual care. | 464 patients with back pain visiting ED. 59% female. Mean age ≈ 48.2. |
Physical examination of patient; Guidance on activity progression; Home exercises; Patient information and education | Benzodiazepine; Other opioid drugs | Pain; Prescription of opioids or benzodiazepine at discharge | ED back and neck pain visits receiving PT were no less likely to receive an opioid prescription and were more likely to receive a benzodiazepine than visits receiving usual care. | Environmental: no Economic: yes Social: yes |
Characteristics of included studies.
OA, osteoarthritis; TKA, Total knee arthroplasty; ROM, Range of motion; COPD, Chronic obstructional pulmonary disease; ED, Emergency department; MSKD, Musculoskeletal Disorders; LSS, Lumbar spinal stenosis; SIS, Subacromial impingement Syndrome; PCP, Primary Care Provider; NSAID, Non-Steroid Anti-inflammatory Drug; PT, Physical therapy; PEMF, Pulsed Electromagnetic Field Therapy; TENS, Transcutan Electronic Nerve Stimulation; HA, Hyaluronic acid; GP, General Practitioner; Proms, Patient reported outcome measures; QoL, Quality of Life; BMI, Body Mass Index; FIQ, Fibromyalgia Impact Questionnaire; WOMAC, The Western Ontario and McMaster Universities Arthritis Index; VAS, Visual Analog Scale; SPADI, Shoulder Pain and Disability Index; GRC, Global Rating of Change; NPRS, Numeric Pain Rating Scale; CSI, Corticosteroid injections; AKSS, American Knee Society Score; HRQoL, Health-related Quality of Life; SF-12, 12-Item Short Form Survey; SF-36, 36-Item Short Form Survey.
In the included studies, many different types of PT interventions were described, comprising various exercise interventions (20 of 27) (22–36, 38, 42–44, 46) and interventions where the patient passively received treatment (15 of 27) (22–24, 27, 36–42, 45–48) (Table 2). Other interventions found in the included studies were patient education (22, 26, 27, 31, 34, 35) and organizational health care changes (Table 2) (34, 43, 44).
Of the pharmaceuticals that appeared in the studies, the most common type was analgesics; primary NSAIDs, followed by cortisone or other injections, muscle relaxants, and pharmaceuticals for depression and anxiety. Other pharmaceuticals that occurred were blood pressure lowering substances, anti-choleric, and pharmaceuticals to facilitate breathing (Table 2).
Twelve of the studies (24, 25, 28–35, 43, 44) had pharmaceutical use- or prescription as an specified outcome measure. Of these studies, nine compared PT with treatment as usual (25, 27–30, 34, 35, 43, 44), one study compared PT with pharmaceutical review (31) and two studies compared PT with pharmaceutical interventions (32, 33). Of the studies that compared PT with usual treatment, three (34, 43) compared PT at the ED with either no-PT ED care or PT at a later stage. Two studies (29, 30) compared PT with standard treatment by a physician, one with standard treatment by physical therapist (27), one compared fast-track rehabilitation with rehabilitation according to routine (28), and two studies (25, 35) compared multimodal therapy and educational programs containing PT with treatment as usual and routine PT.
Fifteen studies compared PT interventions, without pharmaceutical treatment, with pharmaceutical interventions but did not specify pharmaceutical use as a direct outcome measure (22, 23, 26, 36–42, 45–48). In one of these studies the participants still reported their pharmaceutical intake, which was presented in the results (22). Of the 15 studies, nine compared PT with some type of injection (22–24, 36, 39–41, 46, 48) (cortisone, hyaluronic, NaHa, or steroid). The types of pharmaceuticals in the other six studies were: anticholinergics (26), NSAIDs or other analgesics (37, 38, 42, 45), muscle relaxants (37, 42), blood pressure lowering pharmaceuticals (38) and antidepressants (47).
None of the included articles discussed sustainable development, and none performed evaluations from a Triple Bottom Line since environmental aspects of sustainable development were not addressed in any study. Eight of the studies did not address any aspect of sustainable development (22, 23, 29, 30, 36, 39, 41, 45). Economic aspects of sustainable development related to costs and healthcare utilization, were discussed in 17 of the included studies (24, 26–28, 31–35, 37, 38, 40, 42–44, 46, 48). Six of those studies compared costs and utilization between their intervention and control groups (2, 24, 27, 28, 35, 44). One study (26) suggests for future studies that cost analyses should be carried out. Social aspects of sustainable development were addressed in 12 of the included studies (25–27, 31–34, 38, 40, 42, 44, 47). One study (33) addresses poverty, education level and unequal access to care. Quality of life or physical and mental health were included as outcome measures in eight studies (26, 27, 31–33, 40, 44, 47), but they were not discussed from a sustainable development perspective. Three studies discussed patient abilities and active participation in care (31, 42, 44) and two discussed risks to patients, such as overmedication (25, 34). In one study, TENS was suggested as an alternative for pain management if pharmaceutical treatments where contraindicated (38). Negative effects of prolonged NSAID use, and the positive effects on coping through active patient engagement in PT were highlighted (42). Empowerment and self-management was discussed as possible reasons for lowered use of health care services and resources in PT treatment (44).
Discussion
This scoping review found that investigations on PT in relation to pharmaceuticals as treatment hold a variation of characteristics with different study designs, study samples and in a range of areas within healthcare. The perspective of sustainable development was not applied in any of the included studies, and environmental aspects were not considered at all. However, several studies did consider economic or social sustainability to some extent.
Among the 27 included studies, many different types of interventions were described as PT. Physical exercise in different forms, was the most frequent type of PT treatment in the studies and TENS was the second most frequent form of PT intervention. In most of the included articles PT was referred to as specific rehabilitation exercises (22–36), in some it was referred to as TENS (36–43) and, in one study, PT was referred to as electromagnetic field treatment (45). These examples mirror the diversity of interventions within the PT discipline, highlighting the importance to mention PT in the title, abstract or keywords when addressing an intervention within the wide scope of PT, when applicable. Nevertheless, to describe an intervention solely as ‘physical therapy’ would not be of sufficient detail (49). Thus, we argue that a clear description of the intervention, including if it is delivered within the PT discipline is necessary to facilitate systematic study of interventions delivered within the PT profession.
None of the included studies were found to address all three dimensions of sustainable development, i.e., the Triple Bottom Line. That absence of evaluations regarding environmental sustainability in any study, can be considered a missed opportunity as the high carbon footprint and pollution from pharmaceuticals is a well-known problem where an effective PT alternative could pose an important contribution to sustainable healthcare. The environmental impact of PT on for example facilities and water use should not be ignored, but could be considered minor compared to the total emissions from health care, especially when compared to pharmaceuticals (2). However, some studies did discuss economic and social aspects of sustainable development. Economic evaluations mainly concerned costs and utilization of health care resources where evaluations of social aspects involved patient participation and empowerment as means for reduced healthcare utilization over time. The importance of patient empowerment for sustainable healthcare has been recognized by the WHO and is proposed by the Centre for Sustainable Healthcare as a cornerstone for sustainable healthcare (2, 4). Another aspect of sustainability that was addressed in the included studies was over medication (25) and the negative consequences from side effects were discussed in another (38). In line with this, the inconvenience of side effects from pharmaceuticals compared with PT interventions has been described previously in research of pain management (50), and patients have previously been found to prefer non-pharmacological pain management over opioids as treatment (51). Hence, increasing societal knowledge and awareness of PT as a non-pharmacological, non-invasive pain treatment is essential (52). Evaluation from the triple bottom line has been suggested in PT research (53). For such evaluations, cooperation between physical therapists, environmental scientists and economists could be of great value for assuring that all parts of the triple bottom line are considered in a holistic perspective on sustainable healthcare.
A strength of our study is the systematic methodology and following the stepwise process described by Arksey and O’malley with additions by Levac et al. (19, 20). Combining these two when conducting a scoping review is recommended for a structured methodology (54). The choice of study design was appropriate to be able to chart in which areas comparisons of PT and pharmaceuticals exist, in order to address gaps in knowledge and identify areas where systematic reviews would be possible. There have also been at least two reviewers of all articles at all stages. Making the selection of studies in a team is something recommended by Levac et al. (20).
One limitation of this study is that grey literature was not included. The primary reason we only searched databases is because we were mainly interested in scientific sources. This could have led to publications bias and a possible lack of included studies with non-significant results. Another limitation is only including articles in English, which may have meant that we missed interesting research that could have contributed to our results; the reduction in linguistic and cultural variation could have led to lower generalizability. The result could also be limited due to the choice to only include three databases in the search strategy, as well as the specific choice of databases. Further, the decision to only include studies that used certain terminology concerning PT, it was noted during the exclusion process that many potentially interesting studies were to be excluded. By only including studies where PT was mentioned explicitly, many studies that involved exercise interventions, TENS, acupuncture, and other interventions that may well be referred to as PT were excluded. This is problematic since similar interventions would be stated as PT in the included studies but were excluded due to the lack of mentioning of PT. However, it would not have been appropriate to define PT by naming all possible interventions, considering the wide range shown already in this study. Therefore, we emphasize the importance of carefully consider terminology in studies evaluating PT interventions, to facilitate future systematic research in the field of PT.
Conclusion
There is a need for further research on the role of PT interventions in relation to pharmaceuticals as treatment. Studies are lacking that consider sustainable development, and studies comparing PT and pharmaceuticals that evaluate outcomes from a perspective of sustainable development could contribute with knowledge about how PT can be a low-carbon, resource efficient alternative to pharmaceuticals, without their negative impact on social sustainability in terms of adverse effects, and thus contribute to sustainable healthcare.
Statements
Data availability statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Author contributions
PS: Conceptualization, Data curation, Project administration, Formal analysis, Investigation, Methodology, Software, Writing – original draft. MJ: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Writing – original draft. AP: Conceptualization, Supervision, Validation, Writing – review & editing. EL: Conceptualization, Supervision, Writing – review & editing, Data curation, Project administration.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We would like to acknowledge Mathias Andersson, at the School of Health and Welfare, Dalarna University, for supporting the idea of the study and for contributing to the initiation of this work.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that Generative AI was used in the creation of this manuscript. During the preparation of this work the authors used OpenAI in order to edit language. After using this tool, the authors reviewed and edited the content as needed and takes full responsibility for the content of the publication.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1.
Fatta-Kassinos D Meric S Nikolaou A . Pharmaceutical residues in environmental waters and wastewater: current state of knowledge and future research. Anal Bioanal Chem. (2011) 399:251–75. doi: 10.1007/s00216-010-4300-9
2.
Mortimer F Isherwood J Wilkinson A Vaux E . Sustainability in quality improvement: redefining value. Future Healthc J. (2018) 5:88–93. doi: 10.7861/futurehosp.5-2-88
3.
World Commission on Environment and Development ed. Our common future. Oxford; New York: Oxford University Press (1987).
4.
Palstam A Sehdev S Barna S Andersson M Liebenberg N . Sustainability in physiotherapy and rehabilitation. Orthop Trauma. (2022) 36:279–83. doi: 10.1016/j.mporth.2022.07.005
5.
Engel GL . The need for a new medical model: a challenge for biomedicine. Science. (1977) 196:129–36. doi: 10.1126/science.847460
6.
Elkington J . Towards the sustainable corporation: win-win-win business strategies for sustainable development. Calif Manag Rev. (1994) 36:90–100. doi: 10.2307/41165746
7.
Vergunst F Berry HL Rugkåsa J Burns T Molodynski A Maughan DL . Applying the triple bottom line of sustainability to healthcare research—a feasibility study. Int J Qual Health Care. (2020) 32:48–53. doi: 10.1093/intqhc/mzz049
8.
Mortimer F Isherwood J Pearce M Kenward C Vaux E . Sustainability in quality improvement: measuring impact. Future Healthc J. (2018) 5:94–7. doi: 10.7861/futurehosp.5-2-94
9.
World physiotherapy . What is physiotherapy [internet]. World physiotherapy; (2022). Available at:https://world.physio/resources/what-is-physiotherapy (Accessed December 25, 2022)
10.
Dean E . Physical therapy in the 21st century (part II): evidence-based practice within the context of evidence-informed practice. Physiother Theory Pract. (2009) 25:354–68. doi: 10.1080/09593980902813416
11.
Banerjee S Maric F . Mitigating the environmental impact of NSAIDs - physiotherapy as a contribution to one health and the SDGs. Eur J Phys. (2021) 25:51–5. doi: 10.1080/21679169.2021.1976272
12.
Hepler CD Strand LM . Opportunities and responsibilities in pharmaceutical care. Am J Hosp Pharm. (1990) 47:533–43. PMID:
13.
Cizmas L Sharma VK Gray CM McDonald TJ . Pharmaceuticals and personal care products in waters: occurrence, toxicity, and risk. Environ Chem Lett. (2015) 13:381–94. doi: 10.1007/s10311-015-0524-4
14.
Boyd R Steele K Ashby B Karliner J Slotterback S . Health care’s climate footprint. How the health sector contributes to the global climate crisis and opportunities for action [internet]. Health care without harm; ARUP; (2019). Available at:https://noharm-global.org/sites/default/files/documents-files/5961/HealthCaresClimateFootprint_092319.pdf (Accessed December 25, 2022)
15.
Matongo S Birungi G Moodley B Ndungu P . Pharmaceutical residues in water and sediment of Msunduzi River, KwaZulu-Natal. South Africa Chemosphere. (2015) 134:133–40. doi: 10.1016/j.chemosphere.2015.03.093
16.
Fekadu S Alemayehu E Dewil R Van der Bruggen B . Pharmaceuticals in freshwater aquatic environments: a comparison of the African and European challenge. Sci Total Environ. (2019) 654:324–37. doi: 10.1016/j.scitotenv.2018.11.072
17.
Pichler PP Jaccard IS Weisz U Weisz H . International comparison of health care carbon footprints. Environ Res Lett. (2019) 14:064004. doi: 10.1088/1748-9326/ab19e1
18.
World physiotherapy . Noncommunicable Diseases – Policy statement. (2019). Available at:https://world.physio/sites/default/files/2020-04/PS-2019-Noncommunicable-diseases.pdf (Accessed November 20, 2023)
19.
Arksey H O’Malley L . Scoping studies: towards a methodological framework. Int J Soc Res Methodol. (2005) 8:19–32. doi: 10.1080/1364557032000119616
20.
Levac D Colquhoun H O’Brien KK . Scoping studies: advancing the methodology. Implement Sci. (2010) 5:69. doi: 10.1186/1748-5908-5-69
21.
Tricco AC Lillie E Zarin W O'Brien KK Colquhoun H Levac D et al . PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. (2018) 169:467–73. doi: 10.7326/M18-0850
22.
Bisset L Beller E Jull G Brooks P Darnell R Vicenzino B . Mobilisation with movement and exercise, corticosteroid injection, or wait and see for tennis elbow: randomised trial. BMJ. (2006) 333:939. doi: 10.1136/bmj.38961.584653.AE
23.
Arslan S Celiker R . Comparison of the efficacy of local corticosteroid injection and physical therapy for the treatment of adhesive capsulitis. Rheumatol Int. (2001) 21:20–3. doi: 10.1007/s002960100127
24.
Rhon DI Boyles RB Cleland JA . One-year outcome of subacromial corticosteroid injection compared with manual physical therapy for the management of the unilateral shoulder impingement syndrome: a pragmatic randomized trial. Ann Intern Med. (2014) 161:161–9. doi: 10.7326/M13-2199
25.
Brose SW Schneck H Bourbeau DJ . An interdisciplinary approach to reducing opioid prescriptions to patients with chronic pain in a spinal cord injury center. PM R. (2019) 11:135–41. doi: 10.1016/j.pmrj.2018.09.030
26.
Lauti M Herbison P Hay-Smith J Ellis G Wilson D . Anticholinergic drugs, bladder retraining and their combination for urge urinary incontinence: a pilot randomised trial. Int Urogynecol J Pelvic Floor Dysfunct. (2008) 19:1533–43. doi: 10.1007/s00192-008-0686-8
27.
Galán-Martín MA Montero-Cuadrado F Lluch-Girbes E Coca-López MC Mayo-Iscar A Cuesta-Vargas A . Pain neuroscience education and physical exercise for patients with chronic spinal pain in primary healthcare: a randomised trial protocol. BMC Musculoskelet Disord. (2019) 20:505. doi: 10.1186/s12891-019-2889-1
28.
den Hertog A Gliesche K Timm J Muhlbauer B Zebrowski S . Pathway-controlled fast-track rehabilitation after total knee arthroplasty: a randomized prospective clinical study evaluating the recovery pattern, drug consumption, and length of stay. Arch Orthop Trauma Surg. (2012) 132:1153–63. doi: 10.1007/s00402-012-1528-1
29.
van Baar ME Dekker J Oostendorp RA Bijl D Voorn TB Bijlsma JW . Effectiveness of exercise in patients with osteoarthritis of hip or knee: nine months’ follow up. Ann Rheum Dis. (2001) 60:1123–30. doi: 10.1136/ard.60.12.1123
30.
van Baar ME Dekker J Oostendorp RA Bijl D Voorn TB Lemmens JA et al . The effectiveness of exercise therapy in patients with osteoarthritis of the hip or knee: a randomized clinical trial. J Rheumatol. (1998) 25:252432–9.
31.
Hay EM Foster NE Thomas E Peat G Phelan M Yates HE et al . Effectiveness of community physiotherapy and enhanced pharmacy review for knee pain in people aged over 55 presenting to primary care: pragmatic randomised trial [with consumer summary]. BMJ. (2006) 333:995. doi: 10.1136/bmj.38977.590752.0B
32.
Clausen B Holsgaard-Larsen A Søndergaard J Christensen R Andriacchi TP Roos EM . The effect on knee-joint load of instruction in analgesic use compared with neuromuscular exercise in patients with knee osteoarthritis: study protocol for a randomized, single-blind, controlled trial (the EXERPHARMA trial). Trials. (2014) 15:444. doi: 10.1186/1745-6215-15-444
33.
Joshi MN Joshi R Jain AP . Effect of amitriptyline vs. physiotherapy in management of fibromyalgia syndrome: what predicts a clinical benefit?J Postgrad Med. (2009) 55:185–9. doi: 10.4103/0022-3859.57399
34.
Kim HS Kaplan SH McCarthy DM Pinto D Strickland KJ Courtney DM et al . A comparison of analgesic prescribing among ED back and neck pain visits receiving physical therapy versus usual care. Am J Emerg Med. (2019) 37:1322–6. doi: 10.1016/j.ajem.2018.10.009
35.
Gallefoss F . The effects of patient education in COPD in a 1-year follow-up randomised, controlled trial. Patient Educ Couns. (2004) 52:259–66. doi: 10.1016/S0738-3991(03)00100-9
36.
Sadeghifar A Saied A Abbaspour V Zandrahimi F . Comparison of the efficacy of physiotherapy, subacromial corticosteroid, and subacromial hyaluronic acid injection in the treatment of subacromial impingement syndrome: a retrospective study. Curr Orthop Pract. (2022) 33:442–6. doi: 10.1097/BCO.0000000000001150
37.
Bakilan F Ortanca B . Patient satisfaction in chronic low Back pain: a comparison between pharmacological treatment, physiotherapy and neural therapy. J Phys Med Rehabil Sci. (2021) 24:238–43. doi: 10.31609/jpmrs.2020-80720
38.
Hamzat TK Ajala AO Fehintola FA . Management of patients with concurrent hypertension and osteoarthritis of the knee: comparative effect of using non steroidal anti inflammatory drugs and physical therapy. Indian J Physiother Occup Ther. (2011) 5:64–8.
39.
Koc Z Ozcakir S Sivrioglu K Gurbet A Kucukoglu S . Effectiveness of physical therapy and epidural steroid injections in lumbar spinal stenosis. Spine Phila Pa. (1976) 34:985–9. doi: 10.1097/BRS.0b013e31819c0a6b
40.
Atamaz F Kirazli Y Akkoc Y . A comparison of two different intra-articular hyaluronan drugs and physical therapy in the management of knee osteoarthritis. Rheumatol Int. (2006) 26:873–8. doi: 10.1007/s00296-005-0096-x
41.
Paker N Tekdos D Kesiktas N Soy D Paker N Tekdös D et al . Comparison of the therapeutic efficacy of TENS versus intra-articular hyaluronic acid injection in patients with knee osteoarthritis: a prospective randomized study. Adv Ther. (2006) 23:342–53. doi: 10.1007/BF02850139
42.
Naikmasur VG Guttal KS Bhargava P Bathi RJ . Comparative evaluation of physiotherapy and pharmacotherapy in the management of temporomandibular joint myofascial pain. Indian J Physiother Occup Ther. (2009) 3:12–7.
43.
Henderson J Gallagher R Brown P Smith D Tang K . Emergency department after-hours primary contact physiotherapy service reduces analgesia and orthopaedic referrals while improving treatment times. Aust Health Rev. (2020) 44:485–92. doi: 10.1071/AH18259
44.
Gagnon R Perreault K Berthelot S Matifat E Desmeules F Achou B et al . Direct-access physiotherapy to help manage patients with musculoskeletal disorders in an emergency department: results of a randomized controlled trial. Acad Emerg Med. (2021) 28:848–58. doi: 10.1111/acem.14237
45.
el Refaye GE Botla AM Al-Din Hussein H Hamada HA Wadee AN . Electromagnetic field versus diclofenac drugs on primary dysmenorrhea: a single-blind randomized controlled trial: electromagnetic field versus diclofenac drugs on primary dysmenorrhea. J Clin Anal Med. (2019) 102:202–6. doi: 10.4328/JCAM.5890
46.
Deyle GD Allen CS Allison SC Gill NW Hando BR Petersen EJ et al . Physical therapy versus glucocorticoid injection for osteoarthritis of the knee. N Engl J Med. (2020) 382:1420–9. doi: 10.1056/NEJMoa1905877
47.
Gür A Karakoc M Nas K Cevik R Sarac J Ataoglu S . Effects of low power laser and low dose amitriptyline therapy on clinical symptoms and quality of life in fibromyalgia: a single-blind, placebo-controlled trial. Rheumatol Int. (2002) 22:188–93. doi: 10.1007/s00296-002-0221-z
48.
Uygur E Aktaş B Eceviz E Yilmazoğlu EG Poyanli O . Preliminary report on the role of dry needling versus corticosteroid injection, an effective treatment method for plantar fasciitis: a randomized controlled trial. J Foot Ankle Surg. (2019) 58:301–5. doi: 10.1053/j.jfas.2018.08.058
49.
Jull G Moore AP . Physiotherapy is not a treatment technique. Musculoskelet Sci Pract. (2021) 56:102480. doi: 10.1016/j.msksp.2021.102480
50.
Brown-Taylor L Beckner A Scaff KE Fritz JM Buys MJ Patel S et al . Relationships between physical therapy intervention and opioid use: a scoping review. PM&R. (2022) 14:837–54. doi: 10.1002/pmrj.12654
51.
Gallup, inc . Americans prefer drug-free pain management over opioids. (2017)
52.
Mintken PE Moore JR Flynn TW . Physical therapists’ role in solving the opioid epidemic. J Orthop Sports Phys Ther. (2018) 48:349–53. doi: 10.2519/jospt.2018.0606
53.
Palstam A Andersson M Lange E Grenholm A . A call to include a perspective of sustainable development in physical therapy research. Phys Ther. (2021) 101:pzaa228. doi: 10.1093/ptj/pzaa228
54.
Colquhoun HL Levac D O’Brien KK Straus S Tricco AC Perrier L et al . Scoping reviews: time for clarity in definition, methods, and reporting. J Clin Epidemiol. (2014) 67:1291–4. doi: 10.1016/j.jclinepi.2014.03.013
Summary
Keywords
physical therapy, physiotherapy, sustainable development, triple bottom line, scoping approach
Citation
Svensson P, Jacobsson M, Palstam A and Lange E (2025) Applying a sustainability perspective in the literature on physical therapy in relation to pharmaceuticals: a scoping review. Front. Public Health 12:1509677. doi: 10.3389/fpubh.2024.1509677
Received
11 October 2024
Accepted
23 December 2024
Published
07 January 2025
Volume
12 - 2024
Edited by
Filip Maric, UiT The Arctic University of Norway, Norway
Reviewed by
Guenka Ivanova Petrova, Medical University Sofia, Bulgaria
Donald Manlapaz, University of Santo Tomas, Philippines
Updates
Copyright
© 2025 Svensson, Jacobsson, Palstam and Lange.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Elvira Lange, elvira.lange@gu.se
†These authors have contributed equally to this work
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.