 Sarah E. Turner1,2
Sarah E. Turner1,2 Stephanie Goguen1,2
Stephanie Goguen1,2 Brenden Dufault3
Brenden Dufault3 Teresa Mayer4
Teresa Mayer4 Piushkumar J. Mandhane5,6
Piushkumar J. Mandhane5,6 Theo J. Moraes7
Theo J. Moraes7 Stuart E. Turvey8
Stuart E. Turvey8 Elinor Simons1,2,9
Elinor Simons1,2,9 Padmaja Subbarao10
Padmaja Subbarao10 Meghan B. Azad1,2,9*
Meghan B. Azad1,2,9*- 1Children’s Hospital Research Institute of Manitoba, Winnipeg, MB, Canada
- 2Department of Community Health Sciences, University of Manitoba, Winnipeg, MB, Canada
- 3Center for Health Care Innovation, University of Manitoba, Winnipeg, MB, Canada
- 4General Child and Family Services Authority, Winnipeg, MB, Canada
- 5Department of Pediatrics, University of Alberta, Edmonton, AB, Canada
- 6Faculty of Medicine, UCSI University, Negeri Sembilan, Malaysia
- 7Department of Pediatrics, Hospital for Sick Children, University of Toronto, Toronto, ON, Canada
- 8Department of Pediatrics, Child and Family Research Institute, BC Children’s Hospital, University of British Columbia, Vancouver, BC, Canada
- 9Department of Pediatrics and Child Health, University of Manitoba, Winnipeg, MB, Canada
- 10Department of Pediatrics, Physiology and Dalla Lana School of Public Health, Hospital for Sick Children, University of Toronto, Toronto, ON, Canada
Introduction: Early child development sets the stage for lifelong health. Identifying early life factors related to child development can help guide programs and policies to bolster child health and wellbeing. The objective of this research was to examine how a broad range of predictors, measured prenatally to the third year of life, are related to child development at kindergarten.
Methods: We linked survey data from the Manitoba site of the CHILD Cohort Study with data from the Early Development Instrument (EDI) assessment, completed in kindergarten by the Manitoba public school system (n = 442 children). The EDI measures five domains of development (ex. language, physical), scored to indicate the bottom 10% (i.e., ‘vulnerable’) of the population on one or more domains. Using structural equation modelling, we grouped 23 predictors of child development into six latent factors including prenatal exposures, child health and lifestyle, family stress, and socioeconomic status (SES). We examined the associations between each latent factor and EDI vulnerability.
Results: Overall, 20.1% of children were vulnerable on one or more EDI domains. Higher family stress at 1 year and 3 years was related to a 0.20 (p-value ≤0.001) and 0.33 (p-value ≤0.001) standardized increase of EDI vulnerability. Higher SES was related to a-0.26 (p-value =0.01) standardized decrease of EDI vulnerability, and this link was partially mediated through family stress at 3 years (10.6% mediated). Prenatal exposures (e.g., maternal diet quality), as well as child health and lifestyle factors (e.g., weekday sleep) were not related to EDI vulnerability.
Conclusion: Supporting parental mental health and programs to reduce early life parenting stress, as well as targeting supports to those living with low SES, appear to be priority areas that could help to improve early child development.
Introduction
Early child development is critical for later life mental and physical health, learning and behaviour (1–3). Investing in early childhood development yields the largest economic returns compared to any other time period or life stage (4); it prevents later life challenges and also promotes health equity by providing a standard foundation of health to all children. The theory of the Developmental Origins of Health and Disease, posits that early life exposures and experiences play a critical role in laying the foundation for health and well-being throughout the lifespan (5, 6). For example, higher child development scores at school entry are related to lower social emotional problems and lower likelihood of being overweight in adolescence (3). Further to this, self-reported wellbeing in adolescence is related to lower levels of depression, anxiety and relationship problems in adulthood (7).
The Early Development Instrument (EDI) is an internationally-recognized, standardized tool for assessing child development and readiness to learn in kindergarten (8). The EDI consists of five domains: (1) physical health and well-being, (2) social competence, (3) emotional maturity, (4) language and thinking skills and (5) communication skills and general knowledge. Each domain has established cut offs to indicate if the child is vulnerable or not (i.e., in the bottom 10th percentile of the population). In Canada, individual provinces have assessed early child development using the EDI since 2005. Between 2010 and 2019, approximately 30% of children in Manitoba had vulnerable scores on one or more EDI domains (9). Understanding early life experiences that predict EDI vulnerability can help governments and organizations identify target areas for intervention to help support positive childhood development.
Previous research has identified several early life factors related to poorer EDI scores including maternal depression, lower family socioeconomic status, having a teen mother, maternal smoking during pregnancy and poorer child overall health (10–13). However, these studies are limited by studying single predictors, examining only one time point, grouping all predictors into one model or using administrative data which only captures information from service use records. To address these knowledge gaps, we harnessed the rich survey data from the CHILD Cohort and included information on 23 predictors including prenatal exposures, child health and lifestyle, family stress, and socioeconomic status. We grouped predictors into categories, instead of examining them individually, to help gain a more holistic picture of the child’s exposures (14). Our objective was to determine how different categories of exposures during the prenatal period and throughout the first 3 years of life are related to child development at kindergarten, as measured by the EDI.
Methods
Study population
We used a subset of data from the CHILD Cohort Study, a national population-based birth cohort beginning in 2008 and recruiting from four centers across Canada; Toronto, Manitoba (including participants from Winnipeg, Morden and Winker), Edmonton and Vancouver. Details of the cohort can be found elsewhere (15). The current analysis was limited to the Manitoba site (n = 998). CHILD data were linked with data from the Government of Manitoba (GOM) using Personal Health Identification Numbers. Every other year, the GOM routinely collects Early Development Instrument (EDI) data during kindergarten. The biennial data collection of the EDI limits the sample for the current study to approximately half that of the Manitoba CHILD site. CHILD participants who consented to administrative data linkage and had complete EDI data were included in the study (n = 442; Supplementary Figure 1). Informed written consent was obtained by all participating parents prior to data collection and this study was approved by the Human Research Ethics Boards at McMaster University and University of Manitoba.
The Early Development Instrument
The EDI is a 104 item questionnaire that measures children’s readiness for school at kindergarten across five domains of child development; (1) physical health and well-being, (2) social competence, (3) emotional maturity, (4) language and thinking skills, and (5) communication skills and general knowledge (8). Each domain has a score ranging from 0 to 10 with higher scores indicating better development. The EDI categorizes children into one of four categories in each domain based on percentile cutoffs in the population: top (highest 25%); middle (middle 50%), at risk (bottom 25–10%) and vulnerable (bottom 10%). We used percentile data from the entire population of Canadian children and applied the score cut offs to our CHILD cohort sample (Supplementary Table 1). Following this, we derived an outcome variable that classified children as vulnerable or not on one or more EDI domains (i.e., EDI vulnerability) (8).
Latent factors comprising predictors of child development
Latent factors are unobserved variables that are calculated and measured by observed variables (10, 16). In collaboration with early child development experts from the University of Manitoba and the GOM, we developed a hypothesized model of predictors of child development at kindergarten using available CHILD data and grouped the individual variables into latent factors based on previous literature and our study team’s expertise. We evaluated a range of potential predictor variables across 8 original latent factors (n = 35 variables considered in total) and used model fit statistics to select and refine each latent factor by reclassifying variables into new latent factors or omitting variables entirely when they impeded good fit. This process left us with n = 23 total predictor variables classified into 6 latent factors in the final hypothesized model. The latent factors included: (1) prenatal risk behaviours; (2) family stress at 1 year; (3) child health at 1 year; (4) child health and lifestyle at 3 years; (5) family stress at 3 years; and (6) socioeconomic status. Descriptions of the latent factors are below.
Description of latent factors
“Prenatal risk behaviours” is comprised of data from prenatal questionnaires. Mother’s smoking status during pregnancy was a binary variable (no smoking compared to any smoking during pregnancy). Maternal stress was measured using the Perceived Stress Scale (PSS), a widely used 10-item instrument for measuring perception of stress in the last month (17, 18). The PSS ranges from 0 to 40, with higher scores indicating more stress. Maternal depression was measured using the Centre for Epidemiologic Studies Depression (CES-D) scale, a 20-item measure which asks caregivers to rate their experiences of symptoms associated with depression over the last week (19). CES-D scores range from 0 to 60, with higher scores indicating more depressive symptoms. The stress and depression variables were used as continuous measures. Mother’s diet was collected using the updated Healthy Eating Index (HEI) 2010 total score (range 0 to 130). HEI is a measure of diet quality that meets standards of the United States dietary guidelines using 12 components; higher scores indicate better diet quality (20).
“Family stress at 1 year” is comprised of data from postnatal questionnaires at 6 months and 1 year. These included maternal stress (using the PSS) and depression (using the CES-D) at 6 months, and parenting stress at 1 year. Parenting stress was measured using the Parent–Child Dysfunctional Interaction (P-CDI) sub-scale from the Parenting Stress Index. The P-CDI scale is a 12-items parent-reported measure of parent satisfaction with the interactions with their child (21). The scale ranges from 12 to 60; higher scores indicate more parenting stress between the parent and child. All stress and depression variables were used as continuous measures.
“Child health at 1 year” is comprised of data from hospital birth charts, survey questionnaires at birth and 1 year, and a clinical assessment at 1 year. Weight gain was calculated as the change in weight for age z-scores from birth to 1 year and characterized into a binary variable (weight gain velocity ≤ 0.67, or weight gain velocity > 0.67 (22)). Atopic conditions were characterized into a binary variable (no atopic conditions compared to one or more) using clinical and questionnaire data asking about: child wheezing, atopic dermatitis (physician diagnosis) and atopic conditions to food (using a skin prick test). Smoking in the home was defined as anyone smoking in the home at 1 year of age (yes or no). Number of emergency room (ER) visits were measured in the first year of life and categorized as none, one, two, or three or more.
“Child health and lifestyle at 3 years” is comprised of data from the one and a half to three-year questionnaires. Categories of fruit, vegetables, and sugar-sweetened beverages were created based on questions asked in the child food frequency questionnaire at 3 years. Fruits and vegetables were combined and dichotomized as less than or equal to five servings per day and greater than five servings per day. Sugar sweetened beverages was dichotomized as no servings or any servings per day. Sleep was derived from combining number of hours of night sleep and nap time durations during the weekday from the child three-year questionnaire. Number of ER visits were measured between one and a half and 3 years of age and categorized as none, one, two, or three or more.
“Family stress at 3 years” is comprised of data from the three-year questionnaires. These included maternal stress (using the PSS), maternal depression (using the CES-D) and parenting stress (using the P-CDI). All variables were used as continuous measures.
“Socioeconomic status” is comprised of data from the prenatal questionnaires. Total household income was categorized as < $80,000 or ≥$80,000. Marital status was defined as married/common law or single/never married/divorced/separated. Education was categorized as no post-secondary degree or completed a post-secondary degree. Since most mothers in the CHILD cohort completed some form of university, we were unable to use more granular categories for education. Perceived socioeconomic status was measured using a picture of a ladder with the top of the ladder being defined as people who have the highest standing in their community, and the bottom of the ladder being defined as people who have the lowest standing in their community. Participants scored where they believed they best fit within the community ladder (23).
Statistical analysis
Step 1: Exploring predictors of child development
Characteristics of the entire population (n = 442) were stratified by EDI vulnerability. We used univariate logistic regression to determine associations between each of the 23 early-life predictors and EDI vulnerability.
Step 2: Developing latent factors of predictors of child development
Structural equation modelling (SEM) was used to develop each latent factor by combining early-life predictors. We tested the goodness of fit of the latent factors using four model fit statistics: Confirmatory Factor Index (CFI), Tucker Lewis Index (TLI), Root Mean Square Error Approximation (RMSEA) and Standardized Root Mean Square Residual (SRMR). CFI and TLI are goodness of fit statistics with values ranging between 0 and 1; values ≥0.90 are considered good fit (24). RMESA and SRMR are badness of fit statistics with values ranging between 0 and 1; values of ≤0.10 are considered good fit (24, 25). To improve model fit for some latent factors, we used modification indices to select additional model parameters including residual covariance or regression between two variables. Models were adjusted for: child sex (male or female, from the GOM dataset), child age at EDI assessment (continuous in months, from the GOM dataset), maternal race (White or other, from the CHILD dataset) and older siblings (none or one or more, from the CHILD dataset).
Step 3: Testing latent factors in a predictive model
SEM was performed to understand the relationship between each latent factor and EDI vulnerability using the diagonally weighted least squares estimate for categorical and continuous predictors (26). In the case of ordinal and dichotomous outcomes, SEM uses a probit regression approach and assumes that categorical variables have an underlying normal distribution, and therefore estimated path coefficients can be interpreted as a regular linear effect. Standardized coefficients from each SEM were reported to facilitate comparison between models and estimate the relative importance of each latent factor in predicting EDI vulnerability. Standardized coefficients range from 0 to 1, with larger coefficients indicating a stronger relationship with the outcome (27). To further understand the pathways in which early childhood exposures are related to child development, we ran two mediation models using latent factors that were significantly related to EDI vulnerability. We tested if the latent factors of family stress at 1 year or family stress at 3 years mediated (explained) the relationship between socioeconomic status and EDI vulnerability. Analyses were performed using RStudio (28) and R (29) (R version 4.2.1 (2022-06-23 ucrt)) using the lavaan package.
Results
In our CHILD Study sample, 8.4% of children were vulnerable on physical health and wellbeing; 5.9% were vulnerable on social competence, 9.0% were vulnerable on emotional maturity, 6.6% were vulnerable on language and thinking skills and 5.4% were vulnerable on communication skills and general knowledge (Supplementary Table 1). Overall, 20.1% (89/442) were vulnerable on one or more domains (Table 1).
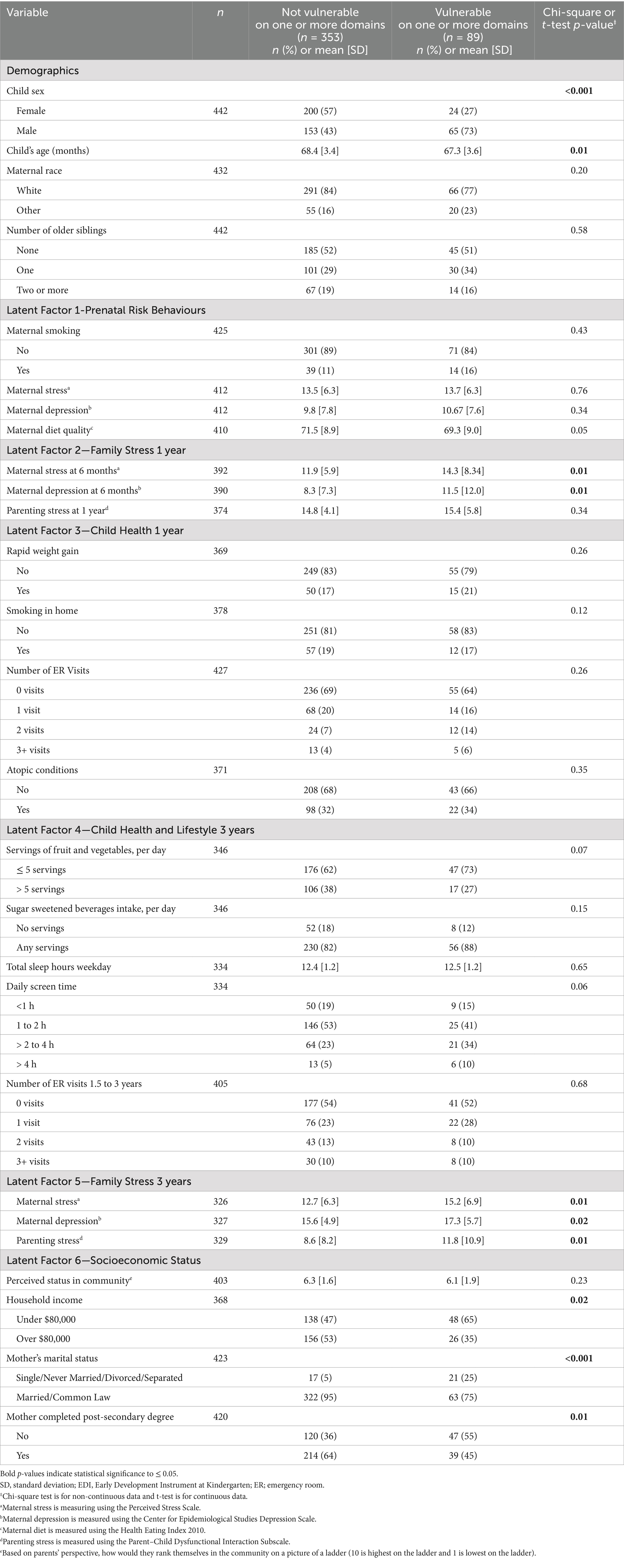
Table 1. Demographics of Manitoba CHILD cohort study participants, stratified by EDI vulnerability at kindergarten.
Early life factors related to child development
Males were over 3 times more likely than females to be vulnerable on one or more EDI domains (odds ratio (OR): 3.54, 95% confidence interval (CI): 2.14–6.01, Figure 1). Children were slightly younger in the vulnerable group (9% decrease in being vulnerable per each additional month of age; OR 0.91 95% CI: 0.85–0.98). Having two or more visits to an ER in the first year of life, compared to no visits, was associated with a 2.02-fold increased odds (95% CI: 1.06–3.76) of EDI vulnerability. Daily screen time of greater than 2 hours was associated with a 2.02-fold increased odds (95% CI: 1.14, 3.57) of EDI vulnerability. A one standard deviation increase in maternal stress and depression scores at 6 months or 3 years and parenting stress scores at 3 years were all associated with increased odds of EDI vulnerability (increased odds between 39 and 43% at 6 months and 33 and 45% at 3 years). Protective sociodemographic factors, including having a household income over $80,000 (OR 0.48; 95% CI: 0.28–0.81), a mother who was married or common law (OR 0.16; 95% CI: 0.08–0.32), or a mother who had completed a post-secondary degree (OR 0.47; 95% CI: 0.29–0.75), were associated with lower EDI vulnerability. A one standard deviation increase in maternal prenatal diet quality was associated with a 21% decreased odds (OR 0.79; 95% CI: 0.62–1.00) of EDI vulnerability. Other hypothesized predictors of child development were not statistically different between the vulnerable and not vulnerable groups (ex. older siblings, weekday sleep duration).
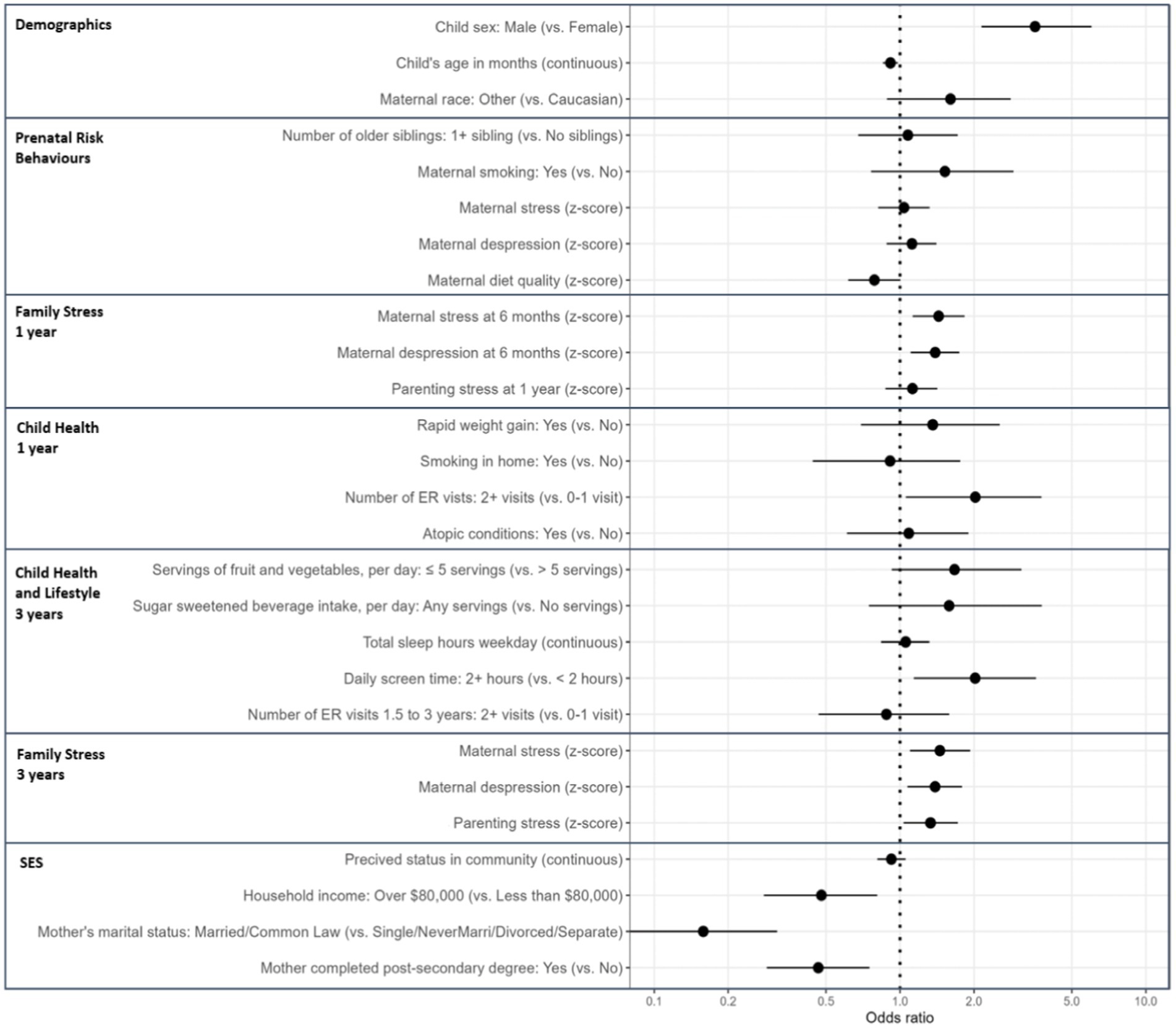
Figure 1. Univariate logistic regression between early life predictors and EDI vulnerability at kindergarten in the Manitoba CHILD cohort study. Odds ratios predict the odds of being vulnerable on one or more Early Development Instrument (EDI) domains for a one point/category change in the exposure variable. SES, socioeconomic status; ER, emergency room. Maternal stress is measuring using the Perceived Stress Scale; Maternal depression is measured using the Center for Epidemiological Studies Depression Scale; Maternal diet is measured using the Health Eating Index 2010; Parenting stress is measured using the Parent–Child Dysfunctional Interaction Subscale; Perceived status in community is based on parents’ perspective, how would they rank themselves in the community on a picture of a ladder (10 is highest on the ladder and 1 is lowest on the ladder). For this table only, maternal depression, maternal stress and parenting stress at 1 and 3 years and prenatal healthy eating index are z-score transformed with a mean of zero and a standard deviation of one to allow for more direct comparisons between variables.
Development of six latent factors to predict child development
All six latent factors passed the thresholds for having good model fit (i.e., CFI or TLI scores ≥0.90 and RMSEA and SRMR scores ≤0.10; Table 2). Most variables (17/23) had standardized loadings that were ≥0.32, which fall under Tabachnick and Fidell’s rule of thumb for minimum loading onto a factor (30). Some variables were < 0.32, but were still included in the model to leverage the richness of the CHILD study data and adhere to our theoretical model of the variables. In addition, variables with low standardized loadings were distributed across the latent factors, rather than grouped onto a single factor, therefore they were not viewed as problematic (31).
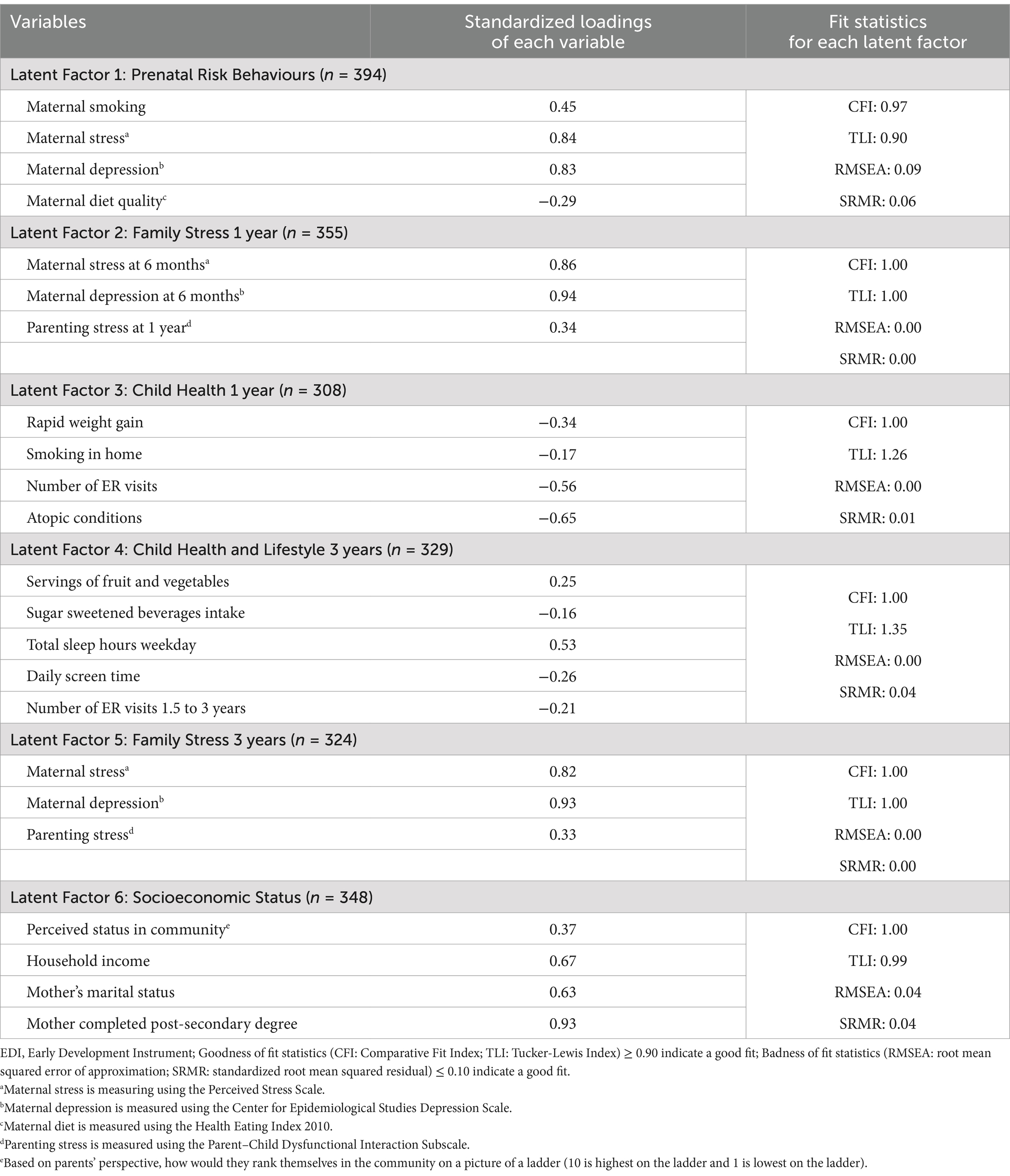
Table 2. Loadings and model fit statistics for latent factors of predictors of EDI vulnerability at kindergarten in the Manitoba CHILD cohort study.
Family stress and socioeconomic status predict child development
Adjusted, standardized coefficients modeling the relationships between each of the latent factors and EDI vulnerability are represented in Figure 2 and Supplementary Table 2. All models maintained good model fit as indicated by the fit indices (Supplementary Table 2). The prenatal risk behaviours latent factor (comprised of prenatal maternal stress, depressing, smoking and diet), was not significantly associated with EDI vulnerability at kindergarten (standardized estimate = 0.09, p = 0.39). Higher family stress at 1 year and 3 years was significantly related to EDI vulnerability: a one standard deviation (SD) increase in family stress at 1 year was associated with a 0.20 standardized increase in EDI vulnerability (p ≤ 0.001); and the association was even stronger for family stress at 3 years (standardized estimate = 0.33, p ≤ 0.001). Higher socioeconomic status (SES, latent class comprised of maternal education and marital status, household income and perceived status) was related to lower EDI vulnerability (standardized estimate = −0.26, p = 0.01). Our latent factor measures of child health at 1 year (standardized estimate = −0.04, p = 0.77) and child health and lifestyle at 3 years (standardized estimate = −0.21, p = 0.18) were not statistically related to lower risk of EDI vulnerability at kindergarten.
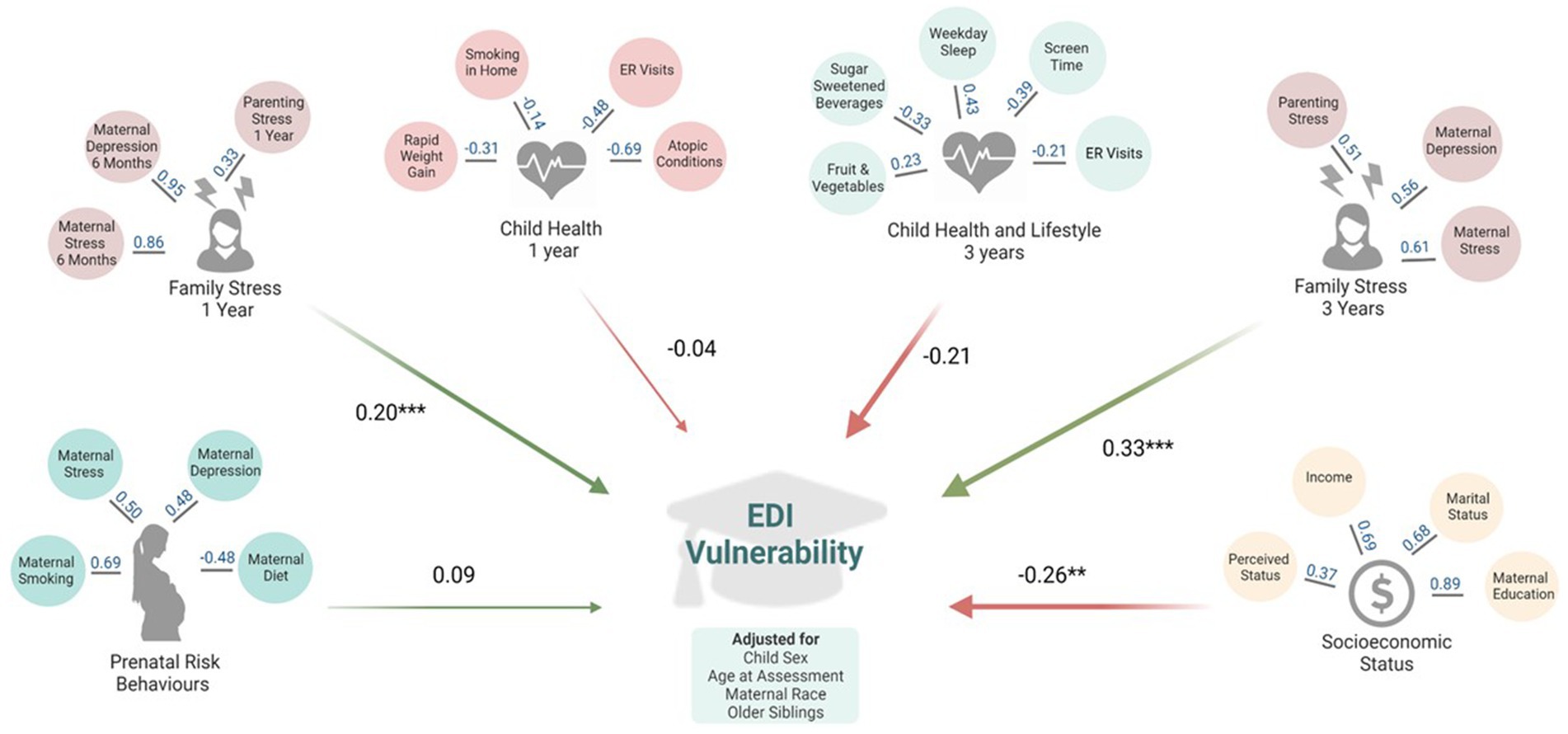
Figure 2. Adjusted models of associations between latent factors of early life predictors and EDI vulnerability at kindergarten in the Manitoba CHILD cohort study. All models are adjusted for: child sex, age at Early Development Instrument (EDI) assessment, maternal race, and older siblings. ER, emergency room. This figure represents the results from six separate structural equation models, one for each latent factor. Values in blue indicate factor loadings for each variable onto the latent factor in adjusted regression models. Values in black indicate standardized regression estimates between the latent factor EDI vulnerability. Fit statistics for each structural equation model are in Supplementary Table 2. *p ≤ 0.05; **p ≤ 0.01, ***p ≤ 0.001. Created with BioRender.com.
Family stress at 3 years mediates the relationship between socioeconomic status and child development
To explore whether the observed association between higher SES and decreased EDI vulnerability could be explained by experiencing lower family stress, we performed a mediation analysis using parametric SEM models. After adjustment for covariates, lower family stress at 3 years was a significant mediator in the relationship between SES and EDI vulnerability, accounting for 10.6% of the total path standardized estimate (indirect path standardized estimate = −0.05, p ≤ 0.05; Figure 3 and Supplementary Table 3). Family stress at 1 year did not significantly mediate this relationship (indirect path standardized estimate = −0.03; Figure 3 and Supplementary Table 3); however, it did account for 9.7% of the total path standardized estimate.
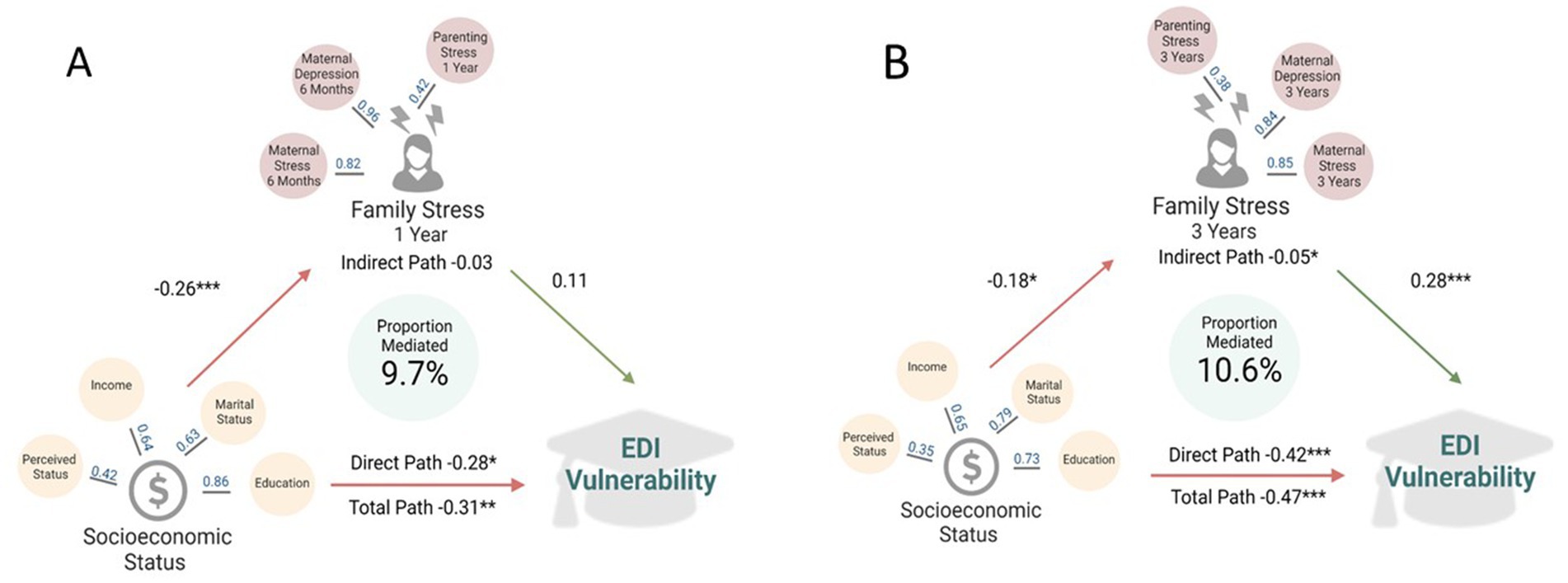
Figure 3. Family stress at one (A) and three (B) years as a mediator of the relationship between socioeconomic status and EDI vulnerability at kindergarten in the Manitoba CHILD cohort study. All models are adjusted for: child sex, age at Early Development Instrument (EDI) assessment, maternal race and older siblings. Values in blue indicate factor loadings for each variable onto the latent factor in adjusted regression models. Values in black indicate standardized regression estimates between the exposure and outcome. Total path is the change in EDI vulnerability for a one standard deviation increase in the socioeconomic status latent factor. Indirect path is the change in EDI vulnerability, through the family stress latent factors. Direct path is the change in EDI vulnerability for a one standard deviation increase in socioeconomic status, not through family stress. Fit statistics for each structural equation mediation model are located in Supplementary Table 3. *p ≤ 0.05; **p ≤ 0.01, ***p ≤ 0.001. Created with BioRender.com.
Discussion
Using structural equation modelling, we evaluated the association of 23 diverse early life factors with child development at kindergarten, measured by the widely-used EDI. Latent factors reflecting family stress at 1 and 3 years of life, as well as low SES, were related to EDI vulnerability. To enhance interpretation for policy and decision makers, we discuss implications of low SES on increased EDI vulnerability, instead of high SES on decreased EDI vulnerability, which is the direction that was measured in our models. Family stress at 3 years had the largest effect size on EDI vulnerability, and partly explained the link between low SES and EDI vulnerability. Other factors reflecting prenatal risk and early childhood health and lifestyle were relatively unrelated to EDI vulnerability. These results highlight the importance of supporting parents of young children (particularly those of low SES) to minimize family stress throughout the early years to bolster child development.
In this sample of Manitoba children from the CHILD cohort study, 20.1% of participants were classified as vulnerable on one or more EDI domains. Population-level data from Manitoba since 2010 has shown that approximately 30% of children are vulnerable on one or more domains (9), indicating that CHILD participants were doing better than the average Manitoba child. This is not surprising given that vulnerable populations are frequently underrepresented in research studies; but it limits the generalizability of our results. Similar to a previous report, being a boy and being younger were associated with EDI vulnerability (12). Differences in these non-modifiable factors justify conducting sex and age-stratified analysis; however, we did not have adequate sample size in our study.
Socioeconomic status and family stress are related to child development and partially act along the same pathway
Low SES and family stress at 1 and 3 years were significant predictors of EDI vulnerability. The detrimental associations between low SES with child development has been established through decades of previous research (32, 33). Single parenthood, maternal and paternal occupation, living in a more disadvantaged area, and lower household income all have significant relationships with EDI vulnerability (12, 13). While measures of SES are often not directly modifiable, these results demonstrate the need to provide extra support to children living with lower SES.
The family stress latent factor in our analysis, comprised of maternal stress and depression and parenting stress at 1 and 3 years, are modifiable predictors of EDI vulnerability that can be targeted to improve child development. Previous work has established postnatal maternal depression and anxiety as strong predictors of EDI scores (11, 34). It has been suggested that maternal mental health may interfere with the ability for mothers to be engaged in learning with their child, respond sensitively and consistently, and form secure attachments (35–37). Infant attachment insecurity has been associated with poorer child executive functioning at kindergarten (38). Furthermore, in the current study, family stress at 3 years was a significant mediator in the link between SES and early EDI vulnerability at kindergarten. Other studies have examined the interplay between the family environment, SES and child development (10, 33, 34). In line with our study, previous research shows SES and family stress have both independent and combined effects on child development.
Together, our results could support the funding and implementation of early child and parenting support programs among low SES communities in Manitoba. One example is the Abecedarian Program (39), which has been operating in some low SES neighbourhoods in Manitoba since 2012 (40). The Abecedarian approach in Manitoba supports child development through four pillars: language priority, conversational reading, interaction games and enriched caregiving (41). Using a randomized design, the program was shown to improve child language scores, and through qualitative analysis, was shown to strengthen parents’ role in supporting their child’s development in Manitoba (40, 41). The current study could be used as evidence to support the importance of programs, such as Abecedarian, that can bolster child development, particularly in low SES settings. Future work could link participation in the Abecedarian Program with EDI scores, and could use a randomized design to test the effectiveness of other interventions aimed to reduce family and parenting stress on improving child EDI scores.
Prenatal maternal health and postnatal child health latent factors are not related to child development
Child health and lifestyle factors at 1 and 3 years of age did not emerge as significant predictors of EDI vulnerability. However, the standardized estimate of child health and lifestyle at 3 years was of similar magnitude to that of family stress at 1 year (a significant predictor of EDI), indicating that it may still be an important predictor regardless of statistical significance. Contrary to our findings, a previous cross-sectional analysis, found that poorer child health, measured using the Health Utility Index, was significantly related to being vulnerable on one or more EDI domains (12). The Health Utility Index differs from our measure of health as it is a more comprehensive, standardized assessment and was measured at the time of EDI assessment in the aforementioned cross-sectional analysis.
Prenatal risk behaviours were also not related to EDI vulnerability in the current study. Previous studies have shown that prenatal smoking (10, 13) and prenatal maternal depression and anxiety (34) are related to poorer EDI scores. In the current analysis, prenatal maternal depression and stress were not related to EDI vulnerability, however, these same mental health measures at 1 and 3 years were related to EDI vulnerability. Previous work has highlighted the potential deleterious effects of exposure to chronic maternal depression and anxiety (34). While our study did not explicitly measure chronic stress, children exposed to depression or stress at 3 years may also have been exposed to it at earlier time points, indicating a possible chronic exposure. Further research should focus on the associations of chronic stress during the first 3 years of life on child EDI scores. Such analysis was beyond the scope of this paper and would require a larger sample size than what was available in the current study.
Strengths and limitations
This study is strengthened by combining rich longitudinal survey data from the CHILD cohort with a population-based validated measure of child development. The EDI is teacher reported, removing parental bias on reports of child functioning. Compared to previous research, our study expands the number of predictors evaluated and incorporates groups of predictors into statistically and theoretically coherent latent factors, providing a more holistic approach for examining childhood exposures. The current study is limited by a relatively small sample size compared to previous population-based studies, which may result in type two error whereby significant associations exist, but cannot be detected due to lower power. Further, the observational nature of the data limits our ability to draw causal conclusions about relationships between early childhood factors and EDI scores. Future work using randomized designs of potential interventions to address family stress, particularly among those with low SES, could provide stronger evidence for our conclusions. Third, while our models meet the traditional thresholds for good model fit, SEM fit indices may have complicated behaviour as functions of the true underlying model, number of parameters, and sample size (42); the reader may wish to interpret our results with caution. Fourth, we used complete case analysis and found that missing data were not completely at random, potentially biasing our results [i.e., there was more missing data among those who were vulnerable on one or more EDI domains (Supplementary Figure 2)]. Fifth, the CHILD cohort is comprised of a higher SES profile than the general Manitoba population, limiting the generalizability of our results, especially for the most vulnerable. Finally, we lacked information on some key variables that are known to impact child development such as father’s mental health, quality of the home learning environment and participation in early pre-school, daycare or nurseries (43, 44).
Conclusion
This study examined 23 early life predictors of EDI vulnerability to identify areas that would be most beneficial for targeting to improve child development at kindergarten. Living with low SES and experiencing family stress in the first 3 years of life were significantly associated with EDI vulnerability. Other early life factors, including prenatal risk factors and child health and lifestyle in the first 3 years of life, did not emerge as significant predictors of child development. This evidence supports the development of programs to promote positive parental mental health and parenting strategies that result in less family stress, with a focus on providing resources to those in low socioeconomic environments.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: a list of variables available in the CHILD Cohort Study is available at: https://childstudy.ca/for-researchers/study-data/. Researchers interested in collaborating on a project and accessing CHILD Cohort Study data should contact the Study’s National Coordinating Centre (NCC) to discuss their needs before initiating a formal request. More information about data access for the CHILD Cohort Study can be found at https://childstudy.ca/for-researchers/data-access/. Requests to access these datasets should be directed to Y2hpbGRAbWNtYXN0ZXIuY2E=.
Ethics statement
This study was approved by the Human Research Ethics Boards at McMaster University and University of Manitoba and conducted in accordance with the local legislation and institutional requirements. Written informed consent was obtained from all participating parents prior to data collection.
Author contributions
SaT: Conceptualization, Formal analysis, Methodology, Visualization, Writing – original draft. SG: Data curation, Formal analysis, Methodology, Visualization, Writing – original draft. BD: Methodology, Writing – review & editing. TMa: Conceptualization, Data curation, Methodology, Writing – review & editing. PM: Conceptualization, Writing – review & editing. TMo: Conceptualization, Writing – review & editing. StT: Conceptualization, Writing – review & editing. ES: Conceptualization, Writing – review & editing. PS: Conceptualization, Funding acquisition, Writing – review & editing. MA: Conceptualization, Funding acquisition, Resources, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The Canadian Institutes of Health Research (CIHR) and the Allergy, Genes and Environment Network of Centers of Excellence (AllerGen NCE) provided core support for the CHILD study (grants to founding CHILD director Malcolm Sears and current director Subbarao). S.E. Turner is funded by the Canadian Institute of Health Research as a Vanier Scholar. P.J.M. has active nominated principal investigator funding from CIHR, Women’s and Children’s Health Research Network, Public Health agency of Canada and Alberta Health. S.E. Turvey holds the Tier 1 Canada Research Chair in Pediatric Precision Health and the Aubrey J. Tingle Professor of Pediatric Immunology. P.S. holds the Tier 1 Canada Research Chair in Pediatric Asthma and Lung Health. M.B.A. holds the Tier 2 Canada Research Chair in Developmental Origins of Chronic Disease. She receives research funding from the Canadian Institutes of Health Research, the Canada Foundation for Innovation, the Bill and Melinda Gates Foundation, Research Manitoba, Mitacs, CIFAR, the Garfield Weston Foundation. She has consulted for DSM Nutritional Products and serves on the Malaika Vx and Tiny Health Scientific Advisory Boards.
Acknowledgments
We are grateful to all the families who are participating in the CHILD Study and the entire CHILD Study team, which includes interviewers, nurses, computer and laboratory technicians, clerical workers, research scientists, volunteers, managers, and receptionists. This article has been published as a preprint in medRxiv https://doi.org/10.1101/2024.11.06.24315323.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1529055/full#supplementary-material
References
1. Brinkman, S, Gregory, T, Harris, J, Hart, B, Blackmore, S, and Janus, M. Associations between the early development instrument at age 5, and reading and numeracy skills at ages 8, 10 and 12: a prospective linked data study. Child Indic Res. (2013) 6:695–708. doi: 10.1007/s12187-013-9189-3
2. Guhn, M, Gadermann, AM, Almas, A, Schonert-Reichl, KA, and Hertzman, C. Associations of teacher-rated social, emotional, and cognitive development in kindergarten to self-reported wellbeing, peer relations, and academic test scores in middle childhood. Early Child Res Q. (2016) 35:76–84. doi: 10.1016/j.ecresq.2015.12.027
3. Black, M, Barnes, A, Strong, M, Brook, A, Ray, A, Holden, B, et al. Relationships between child development at school entry and adolescent health—a participatory systematic review. Int J Environ Res Public Health. (2021) 18:1–36. doi: 10.3390/ijerph182111613
4. Heckman, JJ . Skill formation and the economics of investing in disadvantaged children. Science. (2006) 312:1900–2. doi: 10.1126/science.1128898
5. Barker, DJP . The origins of the developmental origins theory. J Intern Med. (2007) 261:412–7. doi: 10.1111/j.1365-2796.2007.01809.x
6. Baird, J, Jacob, C, Barker, M, Fall, C, Hanson, M, Harvey, N, et al. Developmental origins of health and disease: a lifecourse approach to the prevention of non-communicable diseases. Healthcare. (2017) 5:14. doi: 10.3390/healthcare5010014
7. Kansky, J, Allen, J, and Diener, E. Early adolescent affect predicts later life outcomes. Appl Psychol Heal Well-Being. (2016) 8:192–212. doi: 10.1111/aphw.12068
8. Janus, M, Brinkman, S, Duku, E, Hertzman, C, Santos, R, Sayers, M, et al. (2007). The early development instrument: a population-based measure for communities. pp. 1–44. Available online at: https://www.gov.mb.ca/healthychild/edi/edi_handbook_2007.pdf (Accessed December 2, 2022).
10. Brownell, MD, Ekuma, O, Nickel, NC, Chartier, M, Koseva, I, and Santos, RG. A population-based analysis of factors that predict early language and cognitive development. Early Child Res Q. (2016) 35:6–18. doi: 10.1016/j.ecresq.2015.10.004
11. Wall-Wieler, E, Roos, LL, and Gotlib, IH. Maternal depression in early childhood and developmental vulnerability at school entry. Pediatrics. (2020) 146:e20200794. doi: 10.1542/peds.2020-0794
12. Janus, M, and Duku, E. The school entry gap: socioeconomic, family, and health factors associated with children’s school readiness to learn. Early Educ Dev. (2007) 18:375–403. doi: 10.1080/10409280701610796a
13. Chittleborough, CR, Searle, AK, Smithers, LG, Brinkman, S, and Lynch, JW. How well can poor child development be predicted from early life characteristics? A whole-of-population data linkage study. Early Child Res Q. (2016) 35:19–30. doi: 10.1016/j.ecresq.2015.10.006
14. Browne, DT, Plamondon, A, Prime, H, Puente-Duran, S, and Wade, M. Cumulative risk and developmental health: an argument for the importance of a family-wide science. Wiley Interdiscip Rev Cogn Sci. (2015) 6:397–407. doi: 10.1002/wcs.1349
15. Subbarao, P, Anand, SS, Becker, AB, Befus, AD, Brauer, M, Brook, JR, et al. The Canadian healthy infant longitudinal development (CHILD) study: examining developmental origins of allergy and asthma. Thorax. (2015) 70:998–1000. doi: 10.1136/thoraxjnl-2015-207246
16. Rosseel, Y . Lavaan: an R package for structural equation modeling. J Stat Softw. (2012) 48:1–93. doi: 10.18637/jss.v048.i02
17. Cohen, S . (1994). Perceived stress scale. pp. 1–3. Available online at: http://www.mindgarden.com/products/pss.htm (Accessed December 2, 2022).
18. Cohen, S, Kamarak, T, and Mermelstein, R. A global measure of perceived stress. J Health Soc Behav. (1983) 24:385–96. doi: 10.2307/2136404
19. Radloff, LS . The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Meas. (1977) 1:385–401. doi: 10.1177/014662167700100306
20. Guenther, PM, Kirkpatrick, SI, Reedy, J, Krebs-Smith, SM, Buckman, DW, Dodd, KW, et al. The healthy eating Index-2010 is a valid and reliable measure of diet quality according to the 2010 dietary guidelines for Americans. J Nutr. (2014) 144:399–407. doi: 10.3945/jn.113.183079
21. Abidin, R. (1990). Parenting stress index– short form guide (PSI/SF). 88–90. Available online at: https://edge.edx.org/assets/courseware/v1/50118bb4c48f62c9f2f38a9ef276adf3/asset-v1:GeorgetownX+CCHD+2016+type@asset+block/PSI.pdf (Accessed December 2, 2022).
22. Azad, MB, Vehling, L, Chan, D, Klopp, A, Nickel, NC, McGavock, JM, et al. Infant feeding and weight gain: separating breast milk from breastfeeding and formula from food. Pediatrics. (2018) 142:1092. doi: 10.1542/peds.2018-1092
23. Adler, NE, Epel, ES, Castellazzo, G, and Ickovics, JR. Relationship of subjective and objective social status with psychological and physiological functioning: preliminary data in healthy white women. Health psychology: official journal of the Division of Health Psychology, American Psychological Association. (2000) 19:586–592. doi: 10.1037//0278-6133.19.6.586
24. Hu, LT, and Bentler, PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Model. (1999) 6:1–55. doi: 10.1080/10705519909540118
25. Steiger, JH . Understanding the limitations of global fit assessment in structural equation modeling. Personal Individ Differ. (2007) 42:893–8. doi: 10.1016/j.paid.2006.09.017
26. Li, CH . Statistical estimation of structural equation models with a mixture of continuous and categorical observed variables. Behav Res Methods. (2021) 53:2191–213. doi: 10.3758/s13428-021-01547-z
27. Grace, J, and Bollen, K. Interpreting the results from multiple regression and structural equation models. Contrib Comment. (2005) 86:283–95. doi: 10.1890/0012-9623(2005)86[283:ITRFMR]2.0.CO;2
28. RStudio Team. (2022). RStudio: Integrated development for R. RStudio, Inc Boston, MA. Available online at: http://www.rstudio.com/ (Accessed December 2, 2022).
29. R Core Team. (2022) R: a language and environment for statistical computing. R Found Stat Comput Vienna. Available online at: https://www.r-project.org/ (Accessed December 2, 2022).
30. Tabachnick, B, and Fidell, L. Using multivariate statistics. Sixth ed. Needham Heights, MA: Pearson (2013).
31. Cleare, S, Gumley, A, Cleare, CJ, and O’Connor, RC. An investigation of the factor structure of the self-compassion scale. Mindfulness (N Y). (2018) 9:618–28. doi: 10.1007/s12671-017-0803-1
32. Guhn, M, Emerson, SD, Mahdaviani, D, and Gadermann, AM. Associations of birth factors and socio-economic status with indicators of early emotional development and mental health in childhood: a population-based linkage study. Child Psychiatry Hum Dev. (2020) 51:80–93. doi: 10.1007/s10578-019-00912-6
33. Letourneau, NL, Duffett-leger, L, Levac, L, Watson, B, and Young-morris, C. Socioeconomic status and child development: a meta-analysis. J Emot Behav Disord. (2011) 21:211–24. doi: 10.1177/1063426611421007
34. Comaskey, B, Roos, NP, Brownell, M, Enns, MW, Chateau, D, Ruth, C, et al. Maternal depression and anxiety disorders (MDAD) and child development: a Manitoba population-based study. PLoS One. (2017) 12:e0177065. doi: 10.1371/journal.pone.0177065
35. Sohr-Preston, SL, and Scaramella, LV. Implications of timing of maternal depressive symptoms for early cognitive and language development. Clin Child Fam Psychol Rev. (2006) 9:65–83. doi: 10.1007/s10567-006-0004-2
36. Ierardi, E, Ferro, V, Trovato, A, Tambelli, R, and Crugnola, CR. Maternal and paternal depression and anxiety: their relationship with mother-infant interactions at 3 months. Arch Womens Ment Health. (2019) 22:527–33. doi: 10.1007/s00737-018-0919-x
37. Śliwerski, A, Kossakowska, K, Jarecka, K, Świtalska, J, and Bielawska-Batorowicz, E. The effect of maternal depression on infant attachment: a systematic review. Int J Environ Res Public Health. (2020) 17:2675. doi: 10.3390/ijerph17082675
38. Bernier, A, Beauchamp, MH, Carlson, SM, and Lalonde, G. A secure base from which to regulate: attachment security in toddlerhood as a predictor of executive functioning at school entry. Dev Psychol. (2015) 51:1177–89. doi: 10.1037/dev0000032
39. Ramey, CT, and Ramey, SL. Early learning and school readiness: can early intervention make a difference? Merril Palmer Quartr. (2004) 50:471–91. doi: 10.1353/mpq.2004.0034
40. Koshyk, J, Wilson, T, Stewart-Tufescu, A, D’Souza, M, Chase, RM, and Mignone, J. The ripple effect: examining the impact on parents of an abecedarian early child care intervention in an urban social housing development. J Early Child Res. (2021) 19:40–54. doi: 10.1177/1476718X20966696
41. Stevens, H, Santos, R, Jonasson, S, Young, C, Mann, S, Sass, C, et al. The abecedarian approach in a low-resource urban neighborhood in Canada: an impact evaluation in a child care setting. Int J Early Child. (2019) 51:217–32. doi: 10.1007/s13158-019-00245-4
42. Shi, D, Lee, T, and Maydeu-Olivares, A. Understanding the model size effect on SEM fit indices. Educ Psychol Meas. (2019) 79:310–34. doi: 10.1177/0013164418783530
43. Kahn, RS, Brandt, D, and Whitaker, RC. Combined effect of mothers’ and fathers’ mental health symptoms on children’s behavioral and emotional well-being. Arch Pediatr Adolesc Med. (2004) 158:721–9. doi: 10.1001/archpedi.158.8.721
44. Sylva, K, Melhuish, E, Sammons, P, Siraj-Blatchford, I, and Taggart, B. (2004). The effective provision of pre-school education (EPPE) project: Final report; Department for Education and Skills; Institute of Education: University of London. Available online at: http://www.dotwaidecentre.org.au/pdf/EPPE.pdf (Accessed February 1, 2025).
Keywords: early life exposure, early development instrument, school readiness, family stress, structural equation modelling, longitudinal cohort study
Citation: Turner SE, Goguen S, Dufault B, Mayer T, Mandhane PJ, Moraes TJ, Turvey SE, Simons E, Subbarao P and Azad MB (2025) Early life predictors of child development at kindergarten: a structural equation model using a longitudinal cohort. Front. Public Health. 13:1529055. doi: 10.3389/fpubh.2025.1529055
Edited by:
Jessica Kerr, Royal Children’s Hospital, AustraliaReviewed by:
John Pascoe, Wright State University, United StatesKatharina Kluczniok, Free University of Berlin, Germany
Copyright © 2025 Turner, Goguen, Dufault, Mayer, Mandhane, Moraes, Turvey, Simons, Subbarao and Azad. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Meghan B. Azad, TWVnaGFuLmF6YWRAdW1hbml0b2JhLmNh