 Lyagamula Kisia1*
Lyagamula Kisia1* Shukri F. Mohamed1†Grace Kyule2†
Shukri F. Mohamed1†Grace Kyule2† Christelle Tchoupé3,4†Olatunbosun Abolarin5Retselisitsoe Pokothoane6,7†Terefe Gelibo6,8†Samuel Iddi2†Boscow Okumu2†Nelson Mbaya2†Damazo T. Kadengye2†Didier M. Mirindi4†
Christelle Tchoupé3,4†Olatunbosun Abolarin5Retselisitsoe Pokothoane6,7†Terefe Gelibo6,8†Samuel Iddi2†Boscow Okumu2†Nelson Mbaya2†Damazo T. Kadengye2†Didier M. Mirindi4† Akinsewa Akiode9†Thompson Ademola9†Uche Okezie5
Akinsewa Akiode9†Thompson Ademola9†Uche Okezie5 Noreen Dadirai Mdege10,11 on behalf of the Data on Youth and Tobacco in Africa (DaYTA) consortium
Noreen Dadirai Mdege10,11 on behalf of the Data on Youth and Tobacco in Africa (DaYTA) consortium- 1Chronic Disease Management Unit, African Population and Health Research Center, Nairobi, Kenya
- 2Data Synergy and Evaluation Unit, African Population and Health Research Center, Nairobi, Kenya
- 3Laboratory for Survey & Research for Development, Douala-Bonanjo, Cameroon
- 4Research Initiatives for Social Development, Bukavu, Democratic Republic of Congo
- 5APIN Public Health Initiatives, Abuja, Nigeria
- 6Development Gateway: An IREX Venture, Washington, DC, United States
- 7Research Unit on the Economics of Excisable Products (REEP), School of Economics, University of Cape Town, Cape Town, South Africa
- 8Public Health, ICAP at Columbia University Mailman School of Public Health, Addis Ababa, Ethiopia
- 9Research and Communications Services (RCS), Lagos, Nigeria
- 10Department of Health Sciences, University of York, York, United Kingdom
- 11Centre for Research in Health and Development, York, United Kingdom
Introduction: The use of tobacco among adolescents in low- and middle-income countries is a public health issue of concern. The tobacco industry’s aggressive marketing tactics target young people in African countries, leading to early initiation of tobacco use. While existing evidence focuses on 13-15-year-olds, data from Sub-Saharan Africa indicates that smoking initiation ranges from as young as 7 years old to around 16 years old. The lack of data on adolescent tobacco use in African countries limits policymakers’ ability to implement evidence-based tobacco control policies. This study aims to address the critical lack of quality and timely primary data on adolescent tobacco use, thereby enhancing the country’s capacity to target interventions effectively, engage local governments, and attract global attention and funding for adolescent health initiatives.
Methods: We will conduct a cross-sectional nationwide survey among adolescents aged 10–17 years in urban and rural areas of the Democratic Republic of Congo (DRC), Kenya and Nigeria. This household-based survey will utilize a multi-stage stratified sample design to ensure representation across diverse geographic and demographic characteristics. The sample size calculations resulted in nationally representative samples of 6,701 adolescents in Kenya, 4,803 adolescents in the DRC, and 7,948 adolescents in Nigeria.
Discussion: Through this initiative, we aim to catalyze action at national and international levels to combat the tobacco epidemic among adolescents in Sub Saharan Africa. The findings from the study will empower stakeholders to advocate effective tobacco control measures, promote adolescent health, and safeguard future generations from the harmful effects of tobacco use.
Introduction
The Data on Youth and Tobacco in Africa (DaYTA) program is designed to address critical data gaps in tobacco control, focusing on tobacco use among adolescents in Sub-Saharan Africa (SSA). This region has one of the youngest populations globally. For instance, 57.6% of the population in the Democratic Republic of Congo (DRC) and 52% of the population in Nigeria is under 19 years old (1, 2). The tobacco industry targets these young populations through aggressive marketing strategies, including celebrity endorsements, advertising near schools and playgrounds, and distributing free products. The industry also produce youth-oriented flavors such as those in tobacco products like shisha (hookah/waterpipe) which were traditionally uncommon among young people but are increasingly becoming popular in this population. Additionally, the production of new and emerging tobacco and nicotine products such as e-cigarettes and heated tobacco products (HTPs) present another opportunity for risky behavior. There is a perception among many adolescents that these products are ‘safer’ than cigarettes (3–5). Evidence suggests that in addition to the immediate health risks associated with the use of these products, adolescents who use e-cigarettes/vapes are three times more likely to have ever smoked combustible cigarettes and twice more likely to be current smokers (6, 7). Those who start using e-cigarettes earlier in their adolescence are also more likely to use cigarettes later in life than those who start using them later (8). Yet, data on the use of these products in Africa remains sparse, and existing policy interventions are lagging and often based on those of traditional tobacco products.
All in all, African countries have made commendable efforts to control tobacco and nicotine product use. The majority (44) of the countries in the WHO AFRO region have ratified the Framework Convention on Tobacco Control (FCTC) (9). The framework includes provisions such as promotion of smoke-free environments, implementation of cessation programs, increased taxation, graphic health warnings and front of package labeling, and regulation on tobacco advertising, promotion and sponsorship (TAPS). However, many of these African countries have still not aligned with several of the MPOWER best practice measures such as achieving 75% or above tax share in the retail price of tobacco products (10). Additionally, less than 35% of African countries are in complete compliance with bans on TAPS and adherence to smoke-free laws (10).
Most data on adolescent smoking in SSA are derived from school-based surveys such as the Global Youth Tobacco Survey (GYTS) and Global School-based Student Health Surveys (GSHS), which target 13–15-year-olds. However, these studies have notable limitations: they exclude out-of-school adolescents and do not capture early (i.e., ages 10 years) and late (i.e., ages 18–19 years) adolescents (11). Evidence suggests that smoking initiation can occur as early as 7 years old in some SSA countries (8, 10). In SSA, a substantial proportion of children are not enrolled in school, with 20% of those aged 6–11 years, 33% of 12–14 years, and 48% of 15–17 years currently out of school (11). Research indicates that out-of-school adolescents are more likely to initiate smoking than those who are in school (11, 12). Furthermore, there are concerns about social desirability bias in school-based surveys where tobacco use is prohibited. In some SSA countries such as Kenya, tobacco is the most widely known and used psychoactive substance among those aged 14 years and younger in primary school (13). Additionally, school-based data in many SSA countries is outdated. For example, the latest GYTS in Nigeria and DRC were conducted in 2008; they also covered limited geographical areas, thereby missing a significant proportion of adolescents (13, 14). In Kenya, the most recent nationally representative survey on tobacco use among 11-17-year-olds is more than a decade old (15). While previous research on adolescent tobacco use in SSA has relied on school-based surveys, this study adopts a household-level approach to capture a more representative population, including out-of-school adolescents. This methodological shift addresses a critical evidence gap, as the current lack of comprehensive data hinders policymakers’ ability to design targeted, evidence-based tobacco control interventions.
The DaYTA program seeks to bridge these gaps by conducting a population-based household survey in the DRC, Kenya, and Nigeria. This survey will capture data on tobacco and nicotine product use among adolescents aged 10–17 years, ensuring a comprehensive and timely assessment of tobacco and nicotine use.
Methods and analysis
Aim
The primary goal of this study is to collect bespoke, nationally representative data in the DRC, Kenya, and Nigeria on tobacco and nicotine product use among adolescents aged 10–17 years. We will address the following specific research questions:
What is the prevalence of tobacco and nicotine product use among adolescents aged 10–17 years?
What are the multi-level (e.g., individual-, household- and environment-level) factors associated with tobacco and nicotine product use among adolescents?
Design and study population
A nationally representative population-based household survey will be conducted in each of the three countries. The surveys will focus on adolescents aged 10–17 years and their caretakers.
Eligibility criteria
To be eligible for inclusion, households must have at least one adolescent aged 10–17 years. In this study, a household is defined as a person or group of related or unrelated persons who live together in the same dwelling unit(s), who acknowledge one adult male or female as the head of the household, who pool some, or all, of their income and wealth, who consume certain types of goods and services collectively, mainly housing and food and who are considered a single unit (15, 16). Household participation requires consent from the head of the household.
An adolescent will be eligible for the study if they are aged 10–17 years and are a member of a participating household. We will exclude adolescents who are unable to consent due to either refusal or inability to comprehend study information, adolescents who do not have the capacity to understand the questions being asked, and those with significant physical disabilities (e.g., hearing and speech impairment) that prevent the interviewer from oral administration of the surveys.
Study settings
The survey will be conducted in three SSA countries: the DRC, Kenya, and Nigeria. The selection of these three countries was informed by several factors. First, the Tobacco Control Data Initiative (TCDI) (17) identified a gap on nationally representative data on adolescent tobacco and nicotine use across the region. Second, a rapid assessment was conducted together with key stakeholders to identify the priorities, data needs and challenges related to tobacco use among adolescents. Third, the inclusion of anglophone (Kenya and Nigeria) and francophone (DRC) countries ensures linguistic and regional diversity, enhancing the generalizability of findings across different policy environments in SSA. This three-country approach not only addresses evidence gaps but also facilitates cross-country comparisons of tobacco use patterns and regulatory frameworks.
The DRC is the largest country by land size in SSA. The study will be implemented in 16 provinces, that is, 15 randomly sampled provinces and Kinshasa which has been selected with certainity as it is the capital of the DRC. According to DRC’s health pyramid, each province is divided into health zones (well-defined geographical areas, within the territorial boundaries of a municipality or territory, with a population of approximately 50,000 to 100,000 inhabitants in rural areas and 150,000 to 200,000 inhabitants in urban areas), and each health zone into health areas (geographical area with a population of approximately 5,000 inhabitants in rural areas and 10,000 inhabitants in urban areas) (18). Kenya is a devolved system of governance made up of 47 county governments. The administrative structure of the counties comprises sub-counties, wards, and villages. In Kenya, the study will be implemented in 16 counties, that is, 15 randomly sampled counties and Nairobi which has been selected with certainty as it is the capital and largest city. On the other hand, Nigeria is divided into six geopolitical zones based on the 36 states. Each state is divided into Local Government Areas (LGAs), and the LGAs are further divided into localities. The study will be implemented in 13 states, where 12 will be randomly selected and the Federal Capital Territory (FCT) will be selected with certainty due to its cultural and ethnic diversity. It also hosts Abuja which is Nigeria’s administrative and political capital.
Sampling procedures
In each country, the survey will utilize a multi-stage stratified cluster sample design, with slight modifications taking into consideration the context of each country. In Kenya and Nigeria, stratification will be carried out based on the administrative divisions and the sampling frames will be obtained from the Kenya National Bureau of Statistics (KNBS) and the National Population Commission (NPC) respectively. The lists will consist of data that allow multi-stage sampling, for example, information on administrative structures (e.g., zones/states/regions/counties/provinces, residential areas (rural/urban), and enumeration areas (EA)) and the relevant bodies will also provide maps and where available the list of households in each EA (cluster) in the selected counties. In the absence of a sampling frame for households, a household listing will be carried out to identify eligible households. In DRC, stratification will be carried out based on the health pyramid structure delineated by the Minstry of Public Health, Hygiene and Prevention into provinces, health zones (HZs), and health areas (HAs). Avenues/villages within the health area will serve as clusters. The sampling frame will be obtained from the National Program for Countering Drug Addiction and Toxic Substances (PNLTC). The health pyramid will serve as the sampling framework and the list and maps covering the country will be obtained from the Ministry of Health representative in each HZ. Household listing will be carried out in each selected avenue/village to identify eligible households.
Sampling strategy for DRC
In the DRC, the first stage will involve stratified random sampling of the provinces. Given the vast size of the country and the constraints of time and financial resources, a stratified random sampling approach will be employed. In the first stage, the 26 provinces will be stratified into six former provinces of the country (1947–1963): Katanga, Kasaï, Léopoldville, Équateur, Orientale, and Kivu (Figure 1a). This approach will ensure a representative selection and will be done in consultation with key stakeholders from the health and academic sector in the DRC. Provinces within each stratum share common historical, cultural, and socio-economic characteristics that may influence behaviors and attitudes toward smoking. In the second stage, three HZs (one in an urban area and two in rural areas) will be randomly selected in each of these provinces. In the third stage, three HAs will be selected in each of the participating HZs. For the fourth stage, in the HAs, one avenue (in urban areas) or village (in rural areas) will be selected randomly. In the fifth stage, in each of these avenues/villages, a proportion of households (and therefore of one adolescent aged 10 to 17 per household) will be randomly selected and surveyed. This systematic approach will guarantee a comprehensive and representative coverage of different geographic strata within the DRC. For consistency across the countries, avenue or village in DRC will be referred to as EAs like in Kenya and Nigeria.
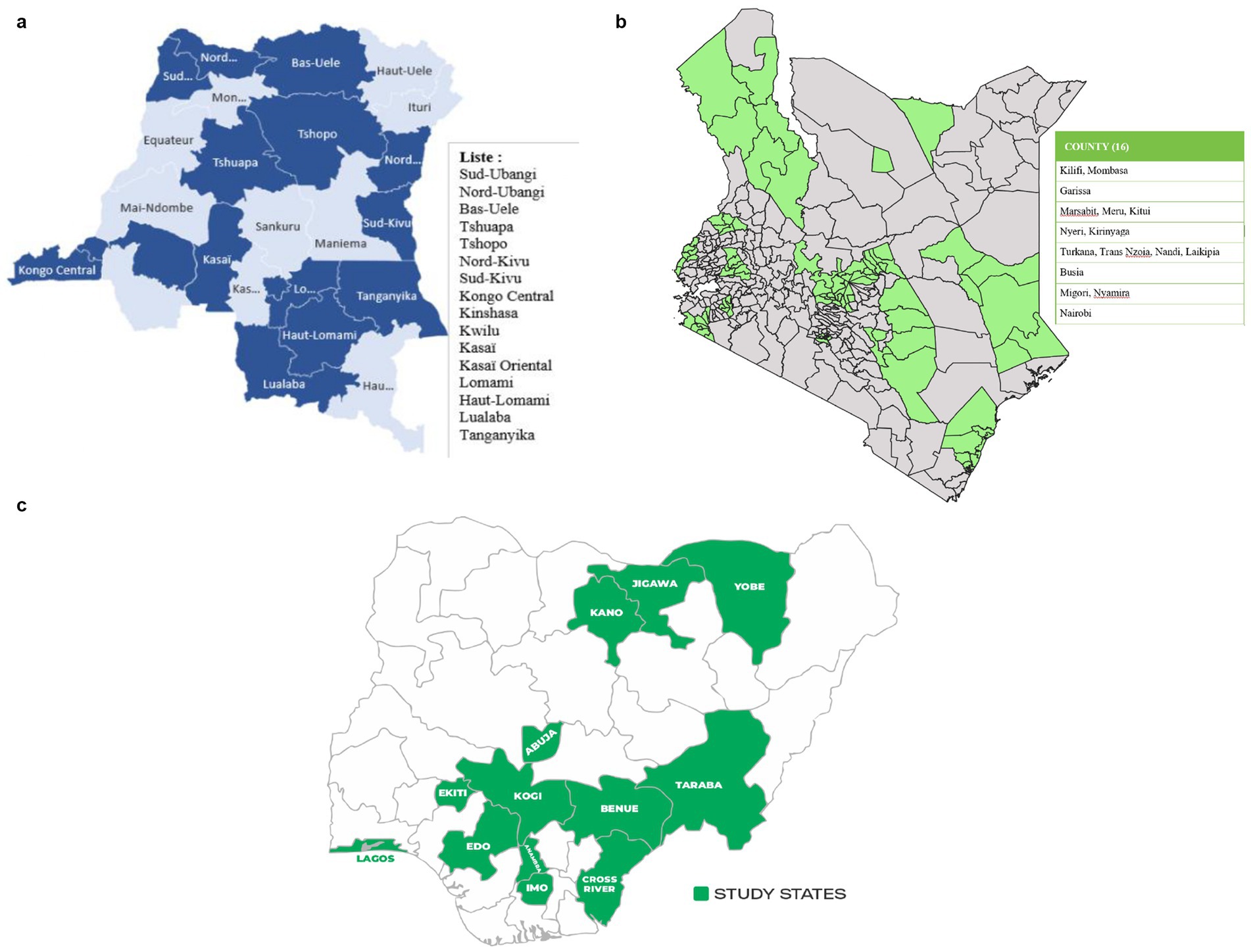
Figure 1. (a–c) Map of expected study areas. a - DRC, b- Kenya, c - DRC.
Sampling strategy for Kenya
In Kenya, the first sampling stage will involve selecting counties from the county sampling frame. The selected counties included Nairobi, Kilifi, Mombasa, Marsabit, Meru, Kitui, Garissa, Nyeri, Kirinyaga, Busia, Migori, Nyamira, Nandi, Laikipia, Turkana, and Trans-Nzoia. Figure 1b shows the distribution sub counties per county. The second stage will involve random sampling of EAs from the selected counties with a probability proportional to the size of the sampled counties. The survey team will carry out a household listing operation in all selected EAs before the start of fieldwork. The household list will serve as the sampling frame for the third stage of sample selection, where a fixed number of households (30) to be interviewed will be selected from each EA using a systematic random sampling technique. In each of the selected households, one adolescent aged 10–17 will be interviewed. All households will be listed prior to sampling and selection of eligible households. In the event that some EAs cannot be accessed, e.g., due to insecurity, they will be replaced.
Sampling strategy for Nigeria
The sampling strategy in Nigeria is like that of Kenya. The first stage involves selecting states from the state sampling frame. The selected states were: South West (SW): Lagos and Ekiti; North East (NE): Yobe and Taraba; South East (SE): Imo and Anambra; North Central (NC): Benue and Kogi; North West (NW): Kano and Jigawa; and South South (SS): Cross River and Edo (Figure 1c). The second stage involves randomly sampling EAs from the selected states and finally selecting a fixed number of households (30) from the selected EAs in each state. Population density and rural urban balance will be accounted for during the sampling design through stratification of the sampling frame by residence (urban/rural) prior to EA selection. This will ensure proportional representation of both settings in the final sample. Additionally, post-stratification adjustments will be incorporated during weighting to align with population distributions across urban and rural areas.
Participant recruitment
The survey team will conduct a household listing within the selected EAs working closely with the local and community leaders/representatives to demarcate EA boundaries. Within these boundaries each household will be visited to identify if there is an adolescent aged 10–17 years living in the house who is available to participate in the questionnaire. This process will establish a sampling frame from which eligible households will be randomly selected for inclusion. The survey teams will obtain consent from the head or acting head of the randomly selected household prior to administering the household survey. During the household survey, a household roster will be populated, and all eligible adolescents within the household will be identified. In households with more than one eligible adolescent, one will be randomly selected for participation in the study. Parental consent and adolescent assent will be sought prior to administering the adolescent survey questionnaire. For emancipated minors (those living independently from parents and competent to make their own decisions), consent will be sought directly from the adolescent prior to the questionnaires being administered.
Sample size calculations
Sample size calculations will adhere to established methodologies tailored to each country. The United Nations (UN)'s formula for prevalence studies (19) will guide sample size computation in Kenya and Nigeria, while the DRC’s formula will be adapted from the Multiple Indicator Cluster Survey (MICS)-Palu RDC 2017–2018 (1), with a confidence level of 95% for all the countries. The sample design effect will be set at 2 for Kenya, 2.5 for Nigeria, and 1.5 for the DRC, and considering non-response rate of 10% for Kenya and the DRC (20), and 20% for Nigeria. The estimated level of tobacco prevalence for the countries are based on each country’s most recent estimates from recent studies. The adolescent population proportions are estimated based on national statistics from the three countries and are 20.45% for Kenya (21), 17.9% for Nigeria (22), and 23% for the DRC (16). The average household size is 3.9 (21), 4.7 (22), and 5.25 (1) for Kenya, Nigeria, and the DRC, respectively. This will result in a nationally representative samples of 6,701 adolescents in Kenya, 4,803 adolescents in the DRC, and 7,948 adolescents in Nigeria.
Questionnaire development process
The DaYTA standardized questionnaire (Supplementary Table 1) was developed through intensive review of literature, drawing insights from internationally recognized survey tools such as the CDC National Youth Tobacco Survey (NYTS) (23); The GYTS (24); Global Adult Tobacco Survey (GATS) (25); ASH Smoke free Great Britain Youth Survey (ASH-Y) (26); International Tobacco Control (ITC)-Youth Surveys (26); and the WHO Tobacco Questions for Surveys of Youth (TQS-Youth) (27). This review process was complemented by consultations with key country stakeholders (Figure 2), involving one-on-one interviews to understand their data needs and priorities for decision-making. Stakeholder input guided the questionnaire drafting process, culminating in country-level workshops where the questionnaire was presented and refined based on feedback from local stakeholders. A cross-country workshop further ensured relevance and appropriateness across the three participating countries. The questionnaires will undergo rigorous field testing before finalization and use.
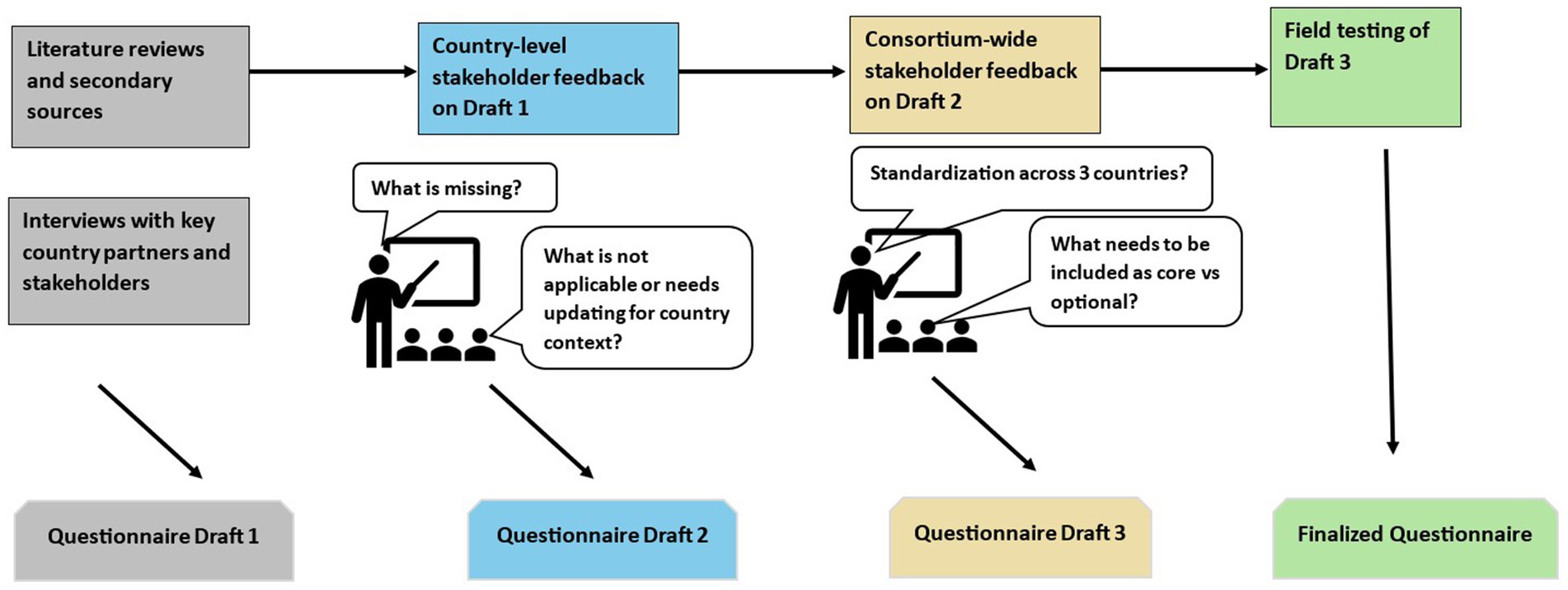
Figure 2. Questionnaire development process.
The household questionnaire will be administered to the consenting head of household or acting head of household and consists of two distinct modules focusing on demographics and socio-economic status. The first module, a household roster, will collect demographic details including sex, age, income, disability status, marital status, health insurance cover, and education of the de facto members of the household. The second module will collect information on household characteristics pertinent to socio-economic assessment such as sources of drinking water, access to sanitation and cooking facilities, housing structure and materials, and ownership of assets.
The adolescent questionnaire will be administered to participating adolescents and includes 12 modules aimed at collecting socio-demographic characteristics, tobacco and nicotine product use behaviors, and multi-level (e.g., individual-, household- and environment-level) factors associated with tobacco use and nicotine products. The questionnaire will cover the following:
• Socio-demographic characteristics such as age, sex, school year (if in school), average weekly spending money, in-school/out-of-school status, parents/guardians/other family members’ tobacco use histories, and tobacco use amongst close friends; functional difficulties, i.e., vision, mobility, cognition remembering, self-care and communication.
• Use of smoked tobacco (manufactured/factory-made cigarettes, roll-your-own (RYO)/hand-rolled cigarettes, shisha/waterpipe/hookah, and other smoked tobacco products, e.g., cigars, cheroots, cigarillos), heated tobacco products, smokeless tobacco (chewing tobacco such as tobacco leaf, and lime; kuber, applying tobacco such as tobacco toothpaste-dentobac etc.; tobacco tooth powder-lal, etc.; snuff), electronic cigarettes, and nicotine pouches. For each product, or product type, we will collect information including quantity, frequency, dependency, age of initiation, where they smoke, and with whom, and access (how they access, where and for how much).
• Knowledge, attitudes, perceptions, and intentions regarding tobacco use and its consequences including exposure to tobacco advertising, promotion or sponsorship, and exposure to anti-tobacco messages.
• Information on cessation of tobacco use (for those using tobacco products), and second-hand exposure to tobacco smoke within the home and in indoor and outdoor public places.
Translations and back translations of study documents
Translations and back-translations of survey tools and consent/assent forms will be conducted to ensure linguistic accuracy and to maintain the integrity of the content. First, the survey tools and consent/assent forms will be translated from English into the identified language(s) by a professional translator who is a native speaker. Subsequently, a different native speaker of the language(s) will perform a back translation, without prior knowledge of the original text, to verify that the intended meanings were preserved and accurately presented. Instruments will be harmonized to ensure consistency and coherence in the textual content across all survey materials.
Data collection process
Prior to data collection, field interviewers will be recruited and selected based on their level of education, prior data collection experience, proficiency in the common national and local languages, and familiarity with the selected study areas. The training will consist of comprehensive sessions on the survey objectives, survey tools, data collection techniques, quantitative research, ethical considerations, and safeguarding on protecting people’s health, wellbeing, and human rights. Additional sessions on conducting household listing exercises and understanding the harms of using tobacco and nicotine products will also be given. All field interviewers will be required to attend all sessions, and participate in mock interviews and role plays to demonstrate their understanding of the study, the study questions and ethical considerations.
Data will be collected by trained field interviewers with prior experience working with similar surveys and who possess knowledge of the local context and selected languages in each country. Experienced researchers will supervise the data collection process. Data collection will be done in person using interviewer-administered electronic questionnaires programmed in Survey CTO on tablets. Data will be transmitted to online secure servers for storage after all quality checks are completed. Interviews with adolescents will be done in a private setting to avoid interference from parents or caregivers. During the consenting process parents will be informed about the topics that will be discussed with the adolescents and advised not to interfere once consent is given. Interviewers will be advised to end the interview if privacy cannot be maintained.
To ensure improved data quality, data will be collected electronically. The questionnaires will be programmed into a Computer Aided Program Interface (CAPI) that will include appropriate mandatory fields and real-time prompts to reduce missing data. Logical flows and validation rules will also be applied. Spot checks will also be conducted on at least 5% of the sample to verify data accuracy. Field interviewers will ensure that every question has been asked and that responses are recorded clearly and accurately before completing each interview. Regular data validation and verification checks will also be run on all the data collected using a syntax script to ensure completeness, correctness, and consistency. Supervisors will maintain regular communication with the central coordination team to discuss progress and address any operational challenges, facilitating adjustments to the data collection process as needed.
Data management
The data will be collected using the offline module and will be uploaded onto a secure server using internet connectivity or mobile data. Backup of the data will remain on the tablets until the end of field activities. Data transmitted to the central servers will be password protected to allow access to only authorized users. Households and individuals who have consented to participate in the study will be assigned a unique study identification number. This identification number will be associated with all participant’s data that is collected, entered, and analyzed for the study. To ensure confidentiality, all personal identifiers (name, identity numbers, phone numbers and places of residence) collected during data collection or for recruitment procedures will be removed from analytical datasets before any data is shared or used in analysis. The raw data will be cleaned and transformed as needed for the statistical analysis. The codes for this purpose will be written in do-files from STATA or R-scripts, to allow traceability and verification of the cleaning operations carried out. This process will involve identifying and addressing missing values, outliers, responses coded as ‘other’ and any data inconsistencies. With the clean data, we shall produce detailed reports with completed tables on different variables as well as a more condensed summary of the results.
Statistical analysis
Descriptive statistics will be used to explore the prevalence and distribution of tobacco use among adolescents at the country and county/province/state levels, including disaggregation by variables of interest such as sex, in-school/out-of-school, rural/urban, socioeconomic differences, and other household- or person-level characteristics. Survey weighted proportions and percentages, means, medians, and standard deviations of variables will also be computed and presented. Visualization techniques such as graphs and charts will be used to represent the variables of interest and results of the analysis to help in communicating key findings and insights effectively.
The analysis of product use will begin with a broad assessment of overall usage, followed by disaggregation into specific product categories. Initially, we will identify users of any tobacco and/or nicotine products. This will include those who use both tobacco and nicotine products. We will then differentiate between users of tobacco products and those using nicotine products, acknowledging that some tobacco users may also be classified as nicotine users. Further disaggregation will include separate analyses for smoked tobacco, smokeless tobacco, cigarette use, and each individual product. This approach will allow us to capture usage patterns across all relevant product categories.
Since the survey is a multi-stage stratified cluster sample, initial sampling weights will be calculated by multiplying the inverse of the probability of selection at each stage of the sampling plan. Adjustments to the weight will be made to account for non-response and calibration adjustment factors and thus, final weights will be computed by multiplying the initial weights, the non-response adjustment factor, and the calibration or post-stratification factor for each sampled unit. The final weights will be normalized to match population totals.
Survey weighted multivariable models (i.e., logistic regression) will be fitted to estimate adjusted odds ratios for the relationships between tobacco use with other explanatory variables including individual factors (e.g., age, sex, ethnicity, education level, knowledge/perceptions about tobacco products), household factors (e.g., household size, family structure, wealth index) and environment-level factors (e.g., residence (rural/urban), geographical location (province/county/state), exposure to tobacco advertising, access to the products). Confounding will be addressed by including theoretically relevant and evidence-based covariates in the multivariable logistic regression models. Variables will be selected based on prior literature, domain knowledge, and bivariate associations with the outcome. Where appropriate, variable selection methods (e.g., stepwise or LASSO regression) may also be applied to identify key predictors while avoiding overfitting. These statistical techniques will account for the sampling design (stratification and clustering) and the computed sampling weights.
Discussion
The study seeks to fill critical gaps in knowledge regarding tobacco use among adolescents aged 10–17 years in three SSA countries: the DRC, Kenya, and Nigeria.
The findings from the study have the potential to significantly influence both policy and public health initiatives related to adolescent tobacco use in the DRC, Kenya, and Nigeria. Specifically, the evidence will inform policies such as stricter enforcement of age-restricted sales, taxation of nicotine products, and school- and community-based prevention programs targeting adolescents. To enable this, the study findings will be communicated at multiple levels to ensure broad impact and engagements with the stakeholders in the tobacco control space across the three countries. We will engage with diverse stakeholders including Ministries of Health, program managers, community and youth representatives, advocacy groups, civil society groups, and non-governmental organizations.
At the end of the study, a stakeholders meeting will be organized to share the findings with the DaYTA teams and stakeholders. Country-level dissemination meetings will also be conducted to engage stakeholders in strategy sessions, discuss actionable next steps, and disseminate key findings from the study report. Additionally, the study findings will be disseminated through peer-reviewed journal publications, and scientific conferences and made accessible on the Tobacco Control Data Initiative (TCDI) dashboard, https://tobaccocontroldata.org. The anonymized datasets generated and/or analyzed for Kenya and Nigeria during the current study will also be available on the APHRC microdata portal, http://microdataportal.aphrc.org/
Strengths of the study
The three study countries (DRC, Kenya, and Nigeria) are diverse in terms of ethnic, linguistic, ecological, environmental, religious, and other contexts, representing the East, Central, and Western regions of Africa. This diversity offers a novel empirical contribution by examining a range of distinct but independent dimensions of field operations. These dimensions include not only data collection and capacity but also the challenges and experiences of conducting surveys, as well as vital questions of context and diversity. Future studies could benefit, explore, and compare alternative methodologies in terms of coverage, mode of data collection, frequency, geographical detail, response rate, quality, cost, required resources, and timeliness. Additionally, another major strength of the study is the inclusion of out-of-school adolescents and collecting household-level data. This study will ensure representation of out-of-school adolescents, who face higher tobacco use risk yet remain underrepresented and are often overlooked in current tobacco control research. The comprehensive examination of different types of tobacco and nicotine products will also provide a detailed picture of tobacco and nicotine use by adolescents aged i.e. 10–17 years across various demographics.
Study limitations
While this study is designed to maximize reach and impact, there are inherent limitations to be acknowledged. First, despite the intention to conduct a nationwide survey, logistical challenges could impede access to certain remote and crisis-affected areas, potentially leading to data representation biases. To mitigate this, the teams will work in collaboration with the necessary national statistical institutions to ensure that any replacements made are proportional and representative of the original sampled EAs. Secondly, reliance on self-reported information introduces the risk of biases, as participants might misreport their tobacco use due to social desirability and recall errors. To address this, interviews will only be conducted when privacy is assured. Before and during the interviews, field interviewers will also reassure the adolescents of confidentiality. Additionally, several questions within the questionnaires will be adapted from internationally recognized and valiadated tools. All the countries will further conduct a pilot exercise to ensure the reliability and on vaildity of the survey tools before the main data collection.
Feasibility and logistical considerations
Implementing a survey of this magnitude requires careful consideration of feasibility, and logistical challenges and potential barriers. The success of such a survey hinge on meticulous planning and allocation of substantial resources. Securing the cooperation of local communities, and managing the nationwide survey, in diverse settings can pose significant challenges such as a lack of sufficient initial buy-in from key stakeholders. To mitigate this, we conducted country-specific assessments where we established that government officials and other key stakeholders were concerned about youth and the lack of adolescent data. We also conducted cross-country workshops to validate this concern and to gather more information. As is possible with all political engagements, shifting priorities and/or shifts in government positions or political instability may lead to what began as strong initial buy-in shifting to less buy-in and engagement or hindering implementation. The program will continue to work closely with the government to ensure they continue to provide feedback at each stage of the research, provide national and local context for survey activities, ensure cultural sensitivity in data collection, and guide dissemination activities. We hope that this will sustain high-level political buy-in. Cementing strong relationships with government ministries, institutions and other key stakeholders is also critical to ensuring high levels of trust in the data created, curated, and shared through this program.
Another challenge is the insecurity in certain areas that may hinder data collection and pose a significant risk to the field teams and investigators. Such areas were identified in collaboration with local authorities and relevant bodies, and they were removed prior to the selection of EAs. It may also be difficult to gain access to some of the selected EAs. This obstacle will be addressed through robust community mobilization strategies and the engagement of relevant local authorities to facilitate smooth operations and ensure the validity of the collected data. Additionally, sample size calculations will consider a 10 to 20% non-response rate to ensure sufficient statistical power, as highlighted in the sampling strategy.
Further research directions
The study lays the groundwork for future longitudinal studies aimed at tracking changes in tobacco and nicotine product use patterns over time among adolescents. Subsequent research could delve into evaluating the effectiveness of targeted anti-tobacco interventions that are informed by the data collected through this survey. Additionally, qualitative studies could unpack life experiences or contextual factors that shape tobacco and nicotine product use behaviors. Replicating this study in other regions could provide a broader perspective on youth tobacco use, contributing to a more comprehensive foundation for global health interventions aimed at curbing tobacco use among young populations.
Conclusion
This study protocol outlines a structured and strategic approach to investigating tobacco and nicotine product use among African adolescents. Despite the limitations, the strength of the study lies in its comprehensive designs and potential to impact public health policy such as national tobacco control laws and frameworks significantly. Additionally, the inclusion of out-of-school adolescents and household-based data collection provide a detailed picture of tobacco and nicotine use among adolescents. The study will also provide an opportunity to delve deeper into the use of new and emerging tobacco and nicotine products in SSA. Through this study, the researchers aim to equip stakeholders with the data necessary to develop effective, sustainable, and culturally sensitive anti-tobacco interventions tailored to adolescent populations across Africa.
Ethics statement
Each country obtained ethical approval from the relevant national ethical bodies. In DRC, ethical approval (001/DIR/RISD/2024) was received from the National Health Ethics Committee. In Kenya, ethical approval (P1570/2023) was received from AMREF Health Africa’s Research Ethics and Scientific Review Committee (ESRC) and a research license (NACOSTI/P/24/32385) from the National Commission for Science, Technology and Innovation (NACOSTI). In Nigeria, ethical approval (01/01/2007 – 19/01/2024) was received from the National Health Research Ethics Committee of Nigeria (MNHREC). Each country sought out additional approvals where necessary.
Author contributions
LK: Investigation, Writing – original draft, Writing – review & editing. SM: Funding acquisition, Investigation, Supervision, Writing – review & editing. GK: Investigation, Methodology, Writing – review & editing. CT: Investigation, Methodology, Writing – review & editing. OA: Investigation, Writing – review & editing. RP: Investigation, Methodology, Writing – review & editing. TeA: Investigation, Methodology, Writing – review & editing. SI: Investigation, Methodology, Writing – review & editing. BO: Investigation, Methodology, Writing – review & editing. NeM: Investigation, Methodology, Writing – review & editing. DK: Methodology, Writing – review & editing. DM: Investigation, Methodology, Writing – review & editing, Formal analysis. AA: Formal analysis, Investigation, Methodology, Writing – review & editing. ThA: Investigation, Methodology, Writing – review & editing. UO: Investigation, Writing – review & editing. NoM: Conceptualization, Funding acquisition, Investigation, Methodology, Supervision, Writing – review & editing.
On behalf of the Data on Youth and Tobacco in Africa (DaYTA) consortium
DRC: Patrice Milambo, National Program to Combat Drug Addiction and Toxic Substances (PNLCT); Dr. Célestin Banza Lubaba Nkulu, University of Lubumbashi; Dr. Josaphat Ndelo-di-Phanzu, University of Kinshasa; Hyppolite Phanzu Lusala, Local Initiative for Integrated Development (ILDI); Emmanuel Kandate, RISD; Dr. Patrick Shamba, Development Gateway (DG); Christus Miderho (DG). Kenya: Dorcas Kiptui, Ministry of Health; Anne Kendagor, Ministry of Health; Dr. Lydia Mucheru, Kenya Institute of Curriculum Development (KICD); Elias Nyaga, Kenya National Bureau of Statistics (KNBS); Edwin Metto, Kenya National Bureau of Statistics (KNBS); Jimi Kirimi, Kenya National Bureau of Statistics (KNBS); Jackline Chepkorir, Kenya National Bureau of Statistics (KNBS); Fabian Oriri, International Institute for Legislative Affairs (IILA); Winnie Awuor, DG; Rachel Kitonyo-Devotsu, DG. Nigeria: Dr. Malau Mangai Toma (head), Federal Ministry of Health NCD Division; Emmanuel Abraham, Federal Ministry of Health NCD Division; Emmanuel Davies, Federal Ministry of Health NCD Division; Dr. Adedeji Adeniran, Center for the Study of Economies of Africa (CSEA); Esther Aghotor, Gatefield; Philip Jakpor, Renevlyn Development Initiative (RDI); Chibuike Nwokorie, Nigeria Tobacco Control Alliance (NTCA); Uche Michael, APIN Public Health Initiatives, Mohammed Maikudi, DG. Additional members: Lauren Eby, DG; Franklin Koech, APHRC; James Amukohe Kavai, APHRC.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work is supported by the Bill & Melinda Gates Foundation (INV-048743). The Bill & Melinda Gates Foundation had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results. The findings and conclusions contained within are those of the authors and do not necessarily reflect the positions or policies of the Bill & Melinda Gates Foundation.
Acknowledgments
This study was conducted as part of the Data on Youth and Tobacco in Africa (DaYTA) program. The DaYTA program seeks to empower stakeholders to make timely, data-driven decisions by using evidence to inform policy and advance tobacco control efforts in sub-Saharan Africa. The program achieves this by addressing data gaps related to tobacco use among 10-17-year-olds in Kenya, Nigeria, and the Democratic Republic of Congo. The DaYTA program is led by Development Gateway: an IREX Venture (DG), a global non-profit organization that specializes in data for development. We are grateful to the participants in each country for the time they took to participate in the study.
Conflict of interest
AA, ThA were employed by Research and Communications Services (RCS).
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1562352/full#supplementary-material
References
1. INS. Enquête par grappes à indicateurs multiples 2017 - 2018: rapport de résultats de l’enquête. Kinshasa, DRC. (2019).
2. Adeloye, D, et al. (2019). Current prevalence pattern of tobacco smoking in Nigeria: A systematic review and meta-analysis. BMC Public Health 19:1–14. doi: 10.1186/S12889-019-8010-8/FIGURES/4
3. Ogwell, AEO, Aström, AN, and Haugejorden, O. (2003). Socio-demographic factors of pupils who use tobacco in randomly-selected primary schools in Nairobi province, Kenya. East Afr Med J 80:235–41. doi: 10.4314/EAMJ.V80I5.8693
4. Maina, WK, Nato, JN, Okoth, MA, Kiptui, DJ, and Ogwell, AO. (2013). Prevalence of Tobacco Use and Associated Behaviours and Exposures among the Youth in Kenya: Report of the Global Youth Tobacco Survey in 2007. Public Health Research 3:43–8. doi: 10.5923/J.PHR.20130303.03
5. Olawole-Isaac, A, Ogundipe, O, Amoo, EO, and Adeloye, DO. (2018). Substance use among adolescents in sub-Saharan Africa: a systematic review and meta-analysis. South African Journal of Child Health 12:79. doi: 10.7196/SAJCH.2018.V12I2B.1524
6. James, PB, Bah, AJ, Kabba, JA, Kassim, SA, and Dalinjong, PA. (2022). Prevalence and correlates of current tobacco use and non-user susceptibility to using tobacco products among school-going adolescents in 22 African countries: a secondary analysis of the 2013-2018 global youth tobacco surveys. Archives of Public Health 80:1–15. doi: 10.1186/S13690-022-00881-8/TABLES/5
7. Oyewole, BK, Animasahun, VJ, and Chapman, HJ. (2018). Tobacco use in Nigerian youth: A systematic review. PLoS One 13:e0196362. doi: 10.1371/JOURNAL.PONE.0196362
8. Chido-Amajuoyi, OG, Fueta, P, and Mantey, D. (2021). Age at Smoking Initiation and Prevalence of Cigarette Use Among Youths in Sub-Saharan Africa, 2014-2017. JAMA Netw Open 4. doi: 10.1001/JAMANETWORKOPEN.2021.8060
9. WHO AFRO. “Tobacco Control | WHO | Regional Office for Africa.” Available online at: https://www.afro.who.int/health-topics/tobacco-control
10. WHO. “WHO report on the global tobacco epidemic,”(2023). Available online at: https://iris.who.int/bitstream/handle/10665/372043/9789240077164-eng.pdf?sequence=1
11. Desai, R, Mercken, LAG, Ruiter, RAC, Schepers, J, and Reddy, PS. (2019). Cigarette smoking and reasons for leaving school among school dropouts in South Africa. BMC Public Health 19:1–10. doi: 10.1186/S12889-019-6454-5/TABLES/4
12. Veeranki, SP, et al. (2017). Age of smoking initiation among adolescents in Africa. Int J Public Health 62:63–72. doi: 10.1007/S00038-016-0888-7/METRICS
13. Warren, CW, Jones, NR, Eriksen, MP, and Asma, S. (2006). Patterns of global tobacco use in young people and implications for future chronic disease burden in adults. Lancet 367:749–53. doi: 10.1016/S0140-6736(06)68192-0
15. Kamenderi, M, Mutetei, J, Okioma, V, Kimani, S, Kanana, F, and Kahiu, C. (2019). Status of Drugs and Substance Abuse in Kenya. African Journal of Alcohol and Drug Abuse 1:54–9.
19. “UNdata | glossary,” UN. Available online at: http://data.un.org/Glossary.aspx?q=household
20. Croft, TN, Marshall, AMJ, and Allen, CK. Guide to DHS Statistics. Maryland, USA: Rockville (2018).
21. TCDI, “The Tobacco Control Data Initiative (TCDI) – Development Gateway: An IREX Venture – Data and digital solutions for international development.” Available online at: https://developmentgateway.org/casestudy/tcdi/
22. Kayembe, C, and Gyenano, M. (2024). RD Congo: Etude auprès des infrastructures sanitaires des facteurs à la base de la mortalité à Kinshasa - Democratic Republic of the Congo | ReliefWeb. OCHA. Accessed. Available online at: https://reliefweb.int/report/democratic-republic-congo/rd-congo-etude-auprès-des-infrastructures-sanitaires-des-facteurs-à
23. United Nations. Studies in Methods: Designing Household Survey Samples: Practical Guidelines, vol. F. 98th ed. New York. (2008).
24. Ecole de Santé Publique de Kinshasa, “ENQUETE DE COUVERTURE VACCINALE CHEZ LES ENFANTS DE 6-23 MOIS En République Démocratique du Congo 2021,” (2021).
25. Kenya National Bureau of Statistics, “2019 KENYA POPULATION AND HOUSING CENSUS: Volume 1,” (2019).
26. National Population Comission (NPC). “2018 Demographic and Health Survey Key Findings Nigeria,”(2019).
27. C. for Disease Control. “National Youth Tobacco Survey (NYTS) 2022 Questionnaire Thank You Very Much For Your Help,” (2022).
28. Global Youth Tobacco Survey Collaborative Group. Global Youth Tobacco Survey (GYTS) Core Questionnaire with Optional Questions GYTS Core Questionnaire with Optional Questions GYTS Sample Design and Weights GYTS Implementation Instructions GYTS Analysis and Reporting Package GYTS Data Dissemination Guida. Atlanta, GA: U.S. (2023).
29. Global Adult Tobacco Survey Collaborative Group. Global Adult Tobacco Survey (GATS) Core Questionnaire with Optional Questions. Atlanta, GA: U.S. (2020).
30. Action on Smoking and Health (ASH). “Use of e-cigarettes (vapes) among young people in Great Britain,” (2023).
31. World Health Organization and U.S. Centers for Disease Control and Prevention. In: Tobacco Questions for Surveys of Youth (TQS-Youth) A Subset of Key Questions from the Global Youth Tobacco Survey (GYTS). Geneva. (2019).
Glossary
ASH-Y - ASH Smoke free Great Britain Youth survey (ASH-Y)
CDC NYTS - Centers for Disease Control and Prevention National Youth Tobacco Survey
DaYTA - Data on Youth and Tobacco in Africa
DRC - Democratic Republic of Congo
EA - Enumeration Area
FCT - Federal Capital Territory
GATS - Global Adult Tobacco Survey
GSHS - Global School-based Student Health Survey
GYTS - Global Youth Tobacco Survey
ITC-Youth - International Tobacco Control (ITC)-Youth Surveys
KNBS - Kenya National Bureau of Statistics
MICS - Multiple Indicator Cluster Survey
SSA - Sub Saharan Africa
NPC - National Population Commission
PNLTC - National Program for the Fight against Drug Addiction and Toxic Substances
RYO - Roll-your-own
TAPS - Tobacco Advertisement, Promotion, and Sponsorship
TCDI - Tobacco Control Data Initiative
UN - United Nations
WHO TQS - World Health Organization Tobacco Questions for Surveys of Youth
Keywords: SSA, tobacco control, youth, low and middle income, nationally representative, Democratic Republic of Congo, Kenya, Nigeria
Citation: Kisia L, Mohamed SF, Kyule G, Tchoupé C, Abolarin O, Pokothoane R, Gelibo T, Iddi S, Okumu B, Mbaya N, Kadengye DT, Mirindi DM, Akiode A, Ademola T, Okezie U and Mdege ND (2025) Use of tobacco and nicotine products among adolescents in Sub-Saharan Africa: protocol for a population-based multi-country household survey. Front. Public Health. 13:1562352. doi: 10.3389/fpubh.2025.1562352
Edited by:
André Luiz Monezi Andrade, Pontifical Catholic University of Campinas, BrazilReviewed by:
Toshio Masumoto, Tottori University, JapanVenkatarao Epari, Institute of Medical Sciences and Sum Hospital, India
Copyright © 2025 Kisia, Mohamed, Kyule, Tchoupé, Abolarin, Pokothoane, Gelibo, Iddi, Okumu, Mbaya, Kadengye, Mirindi, Akiode, Ademola, Okezie and Mdege. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lyagamula Kisia, bC5ra2lzaWFAZ21haWwuY29t; bGtpc2lhQGFwaHJjLm9yZw==
†ORCID: Shukri Farah Mohamed, https://orcid.org/0000-0002-8693-1943
Grace Kyule, https://orcid.org/0009-0008-9721-6866
Retselisitsoe Pokothoane, https://orcid.org/0000-0001-8055-8394
Terefe Gelibo, https://orcid.org/0000-0001-7591-9669
Samuel Iddi, https://orcid.org/0000-0002-2366-2774
Boscow Okumu, https://orcid.org/0000-0002-5738-7256
Damazo T. Kadengye, https://orcid.org/0000-0001-7586-4928
Didier M. Mirindi, https://orcid.org/0009-0008-5761-4069
Christelle Tchoupé, https://orcid.org/0009-0006-6524-5115
Nelson Mbaya, https://orcid.org/0000-0001-5608-3042
Akinsewa Akiode, https://orcid.org/0009-0009-9168-5861
Thompson Ademola, https://orcid.org/0009-0008-7821-2368