 Yanni Lan
Yanni Lan Shou Chen2†
Shou Chen2† Cun Li
Cun Li Jiyong Wei
Jiyong Wei- 1Department of Pharmacy, The People’s Hospital of Guangxi Zhuang Autonomous Region & Guangxi Academy of Medical Sciences, Nanning, China
- 2Departments of Spine Orthopedics, The Fourth Affiliated Hospital of Guangxi Medical University, Liuzhou, China
- 3Department of Bone Surgery, The Eight People’s Hospital of Nanning, Nanning, China
- 4Department of Orthopedic Surgery, The First People’s Hospital of Nanning, The Fifth Affiliated Hospital of Guangxi Medical University, Nanning, China
Background: Fractures of the vertebral column, encompassing various spinal injuries, represent a significant public health burden worldwide. These injuries can lead to long-term disability, reduced quality of life, and substantial healthcare costs.
Methods: We utilized comprehensive data sources from the Global Health Data Exchange (GHDx). The study employed the incidence, prevalence, and years lived with disability (YLDs) metric to quantify the burden. First, numbers and age-standardized rates (ASRs) of incidence, prevalence, and YLDs were assessed globally and by sub-types including sex, age, socio-demographic index (SDI) regions, Global Burden of Disease Study (GBD) regions, and countries in 2021. Furthermore, the temporal trend of the disease burden was explored by the linear regression model from 1990 to 2021. The cluster analysis was used to evaluate the changing pattern of related disease burden across GBD regions. Finally, the age-period-cohort (APC) model were used to predict the future disease burden in the next 25 years.
Results: Exposure to fracture of vertebral column contributed to 7,497,446 incidence, 5,371,438 prevalence, and 545,923 YLDs globally in 2021. The disease burden was higher in males than in females. And it was higher in older adults. High SDI regions were high-risk areas. From 1990 to 2021, the number of cases showed the increasing trend, and the ASRs showed the decreasing trend. The predicted results showed that the number of cases for both genders would still increase from 2022 to 2046.
Conclusion: Our findings highlight the substantial and growing global burden of vertebral column fractures, with significant variations across regions and countries. Targeted interventions to address modifiable risk factors, such as osteoporosis and falls, are essential to mitigate the burden.
Introduction
Fractures of the vertebral column, which encompass injuries to the spine including those to the cervical, thoracic, lumbar, and sacral regions, represent a significant and multifaceted health burden globally. These injuries can result in varying degrees of disability, chronic pain, reduced quality of life, and substantial economic costs (1, 2). Despite advancements in trauma care and rehabilitation, the incidence and associated morbidity of vertebral column fractures remain high, particularly in aging populations and in low- and middle-income countries (LMICs) (3, 4).
Previous studies have documented the significant impact of vertebral column fractures on individual and societal levels. For instance, a systematic review by Sing et al. (5) reported that spinal fractures are a major contributor to the global burden of osteoporosis-related fractures, with a substantial increase in incidence projected over the next few decades due to population aging. Similarly, a study by Murray et al. (6) in the Global Burden of Disease Study 2010 highlighted the substantial disability-adjusted life years (DALYs) lost due to spinal injuries, emphasizing the need for targeted interventions to reduce this burden.
Regional variations in the burden of vertebral column fractures have also been well-documented. In high-income countries (HICs), while the incidence of traumatic spinal injuries may be declining due to improved road safety and workplace regulations, the burden of fragility fractures, particularly in the older adult, continues to rise (7, 8). Conversely, in LMICs, the burden is often exacerbated by a combination of factors including limited access to healthcare, inadequate trauma care infrastructure, and high rates of road traffic accidents and falls (9, 10).
Moreover, recent literature has emphasized the role of modifiable risk factors in the etiology of vertebral column fractures. Osteoporosis, a major underlying condition, is increasingly recognized as a global public health issue, with a high prevalence across all age groups and in both genders (11). Other risk factors such as smoking, alcohol consumption, and sedentary lifestyles have also been implicated in the development of fragility fractures (12, 13).
Despite these advancements in understanding the burden and etiology of vertebral column fractures, there remains a significant gap in the comprehensive assessment of global, regional, and national trends over extended periods. The Global Burden of Disease Study (GBD) provides a unique opportunity to fill this gap by leveraging a comprehensive and standardized approach to estimate the burden of diseases, injuries, and risk factors across different populations and time periods (14). The latest iteration of the GBD, the GBD 2021, includes updated data sources, methodologies, and risk factor estimates, providing a robust platform for analyzing trends in the burden of vertebral column fractures.
In this study, we analyze the global, regional, and national burden of vertebral column fractures from 1990 to 2021 using data from the GBD 2021. By examining trends in incidence, prevalence, and years lived with disability (YLDs), we aim to provide a comprehensive assessment of the burden of vertebral column fractures and identify key areas for intervention. Through this analysis, we hypothesize that our findings may reveal evolving epidemiological patterns of vertebral column fractures and could inform the prioritization of future research and policy development.
Methods
Study design and data sources
This study employed a comprehensive, retrospective analysis to estimate the global, regional, and national burden of vertebral column fractures from 1990 to 2021. Data were sourced from the GBD Study 2021, a collaborative effort involving hundreds of researchers worldwide to quantify health loss due to diseases, injuries, and risk factors. The GBD database integrates various data streams, including population-based surveys, hospital records, vital registration systems, and published literature, ensuring a robust and comprehensive dataset for analysis (15, 16).
Case definition and classification
Vertebral column fractures, encompassing fractures of the cervical, thoracic, and lumbar spine, were defined according to the International Classification of Diseases (ICD) codes. Specifically, ICD-9 codes 805.0–806.9 and ICD-10 codes S12.0-S12.9, S22.0-S22.1, and S32.0 were utilized to identify cases. Fractures were further classified as traumatic or non-traumatic based on the underlying cause, with traumatic fractures attributed to external forces such as falls, motor vehicle accidents, or violence, and non-traumatic fractures often associated with underlying medical conditions like osteoporosis (17).
Estimation procedures
The burden of vertebral column fractures was assessed using incidence, prevalence, and YLDs. Incidence and prevalence were estimated by age, sex, location, and year using DisMod-MR 2.1, a Bayesian meta-regression tool developed by the Institute for Health Metrics and Evaluation (IHME) (18). DisMod-MR leverages available data to produce internally consistent, cause-specific estimates by fitting a series of mathematical models to the data.
YLDs were calculated by multiplying the prevalence of vertebral column fractures by the disability weights derived from population-based surveys. Disability weights reflect the severity of health loss associated with specific conditions on a scale from 0 (perfect health) to 1 (death). For vertebral column fractures, disability weights varied based on the type and severity of the injury, as well as the duration of recovery (16).
Uncertainty analysis
To account for uncertainty in the estimates, 95% uncertainty intervals (UIs) were calculated for all metrics. These intervals reflect the precision of the estimates, with narrower intervals indicating greater certainty. Uncertainty was incorporated into the DisMod-MR model through the use of prior distributions and likelihood functions, which allowed for the propagation of uncertainty from input data to final estimates (18).
Geographical
The GBD 2021 study categorizes 204 countries and territories into five socio-demographic index (SDI) quintiles—low, low-middle, middle, high-middle, and high SDI regions—based on a composite metric of development status. The SDI is calculated as the geometric mean of three normalized indicators: (1) per capita income (lag-distributed income per capita), (2) average educational attainment (years of schooling for individuals aged 15+), and (3) total fertility rate under age 25 (16). These SDI groups are not geographically contiguous but instead reflect comparable levels of socioeconomic development. For instance, high SDI regions include countries such as the United States and Japan, while low SDI regions encompass nations like Niger and Somalia. This stratification enables the identification of burden patterns tied to development disparities rather than geographic proximity alone. A full list of SDI classifications by country is available in the GBD 2021 methodology report.
Statistical analysis
First, the number of incidence, prevalence, and YLDs of fracture of vertebral column and their corresponding ASRs were reported in 2021 globally and by different sub-types including sex, age, SDI regions, GBD regions, and countries. Second, the temporal trend of the disease burden was explored globally and by sub-types from 1990 to 2021. The estimated annual percentage change (EAPC) value was estimated by linear regression model. Based on the EAPC values, the cluster analysis was used to evaluate the changing pattern of related disease burden across GBD regions. Finally, the future disease burden from 2020 to 2044 was predicted by using the age-period-cohort (APC) model under the maximum likelihood framework.
When the p-value was less than 0.05, it was considered statistically significant. The R (version 4.0.2) software was used for database construction, collation, and analysis.
Results
The disease burden attributable to fracture of vertebral column in 2021
In 2021, the number of fracture of vertebral column-related incidence was 7,497,446 [95% uncertainty intervals (UI): 5,834,963–9,737,255]. The corresponding age-standardized incidence rate (ASIR) was 92.75 (95% UI: 72.12–119.99) per 100,000 population. The number of fracture of vertebral column-related prevalence was 5,371,438 (95% UI: 4,703,837–6,196,132) in 2021. The corresponding age-standardized prevalence rate (ASPR) was 65.19 (95% UI: 56.89–75.28) per 100,000 population. The number of YLDs attributable to fracture of vertebral column was 545,923 (95% UI: 366,571–757,099). And the corresponding ASR of YLDs was 6.62 (95% UI: 4.43–9.20) per 100,000 population (Tables 1–3).

Table 1. The number of incidence cases and the age-standardized incidence rate attributable to fracture of vertebral column in 1990 and 2021, and its trends from 1990 to 2021 globally.

Table 2. The number of prevalence cases and the age-standardized prevalence rate attributable to fracture of vertebral column in 1990 and 2021, and its trends from 1990 to 2021 globally.

Table 3. The number of YLDs cases and the age-standardized YLDs rate attributable to fracture of vertebral column in 1990 and 2021, and its trends from 1990 to 2021 globally.
In 2021, the number of incidence, prevalence, and YLDs cases were 1.33, 1.01, and 1.04 times higher in males than females. And the corresponding ASRs were 1.40, 1.17, and 1.19 times, respectively (Supplementary Figure S1, Tables 1–3).
Incidence, prevalence, and YLDs across age groups separately in 2021 were available in Supplementary Figure S2. The ASIR, ASPR, and age-standardized YLDs rate was consistently increasing with age. However, the number of incidence, prevalence, and YLDs cases first increased with age and then decreased after reaching the peak (Supplementary Figure S2, Tables 1–3).
At the SDI region level, the high SDI region had the most number of incidence cases at 2,141,941 (95% UI: 1,580,376–2,884,480), prevalence cases at 2,469,882 (95% UI: 2,144,431–2,817,433), and YLDs cases at 245,574 (95% UI: 163,359–339,966). And the highest ASRs also occurred in the high SDI region, which was 157.17 (95% UI: 119.04–207.76) for ASIR, 131.65 (95% UI: 114.84–149.24) for ASPR, and 13.36 (95% UI: 8.95–18.51) for the age-standardized YLDs rate, respectively (Supplementary Figure S3, Tables 1–3).
Across the 54 GBD regions, Asia ranked the top one in fracture of vertebral column-related incidence, followed by Advanced Health System and Basic Health System. Advanced Health System ranked the top one for number of prevalence and YLDs cases, followed by World Bank High Income and Asia. However, Oceania rank the bottom one for number of cases. For the corresponding ASRs, the top GBD region was Australasia, the bottom was Commonwealth Low Income, followed by Western Africa and Western Sub-Saharan Africa (Supplementary Figure S4, Tables 1–3).
The disease burden of fracture of vertebral column varied considerably across the world, with the top ASRs observed in Andorra in 2021. The lowest ASRs for incidence, prevalence, and YLDs were in Kiribati, followed by Madagascar. As for the absolute number, the highest number of incidence cases was observed in China, followed by India and United States of America. And the highest number of prevalence and YLDs cases was also observed in United States of America in 2021, followed by China and India. The lowest number of cases were all observed in Tokelau, followed by Niue (Figure 1, Tables 1–3).

Figure 1. Numbers and age-standardized rates of fracture of vertebral column-related incidence, prevalence, and YLDs across countries and territories in 2021.
Temporal trend for fracture of vertebral column-related disease burden from 1990 to 2021
The number of incidence cases of fracture of vertebral column increased from 5,856,226 (95% UI: 4,615,149–7,402,697) in 1990 to 7,497,446 (95% UI: 5,834,963–9,737,255) in 2021 globally. However, the corresponding ASIR changed in the opposite direction, with the decrease from to 115.75 (95% UI: 91.28–145.92) to 92.75 (95% UI: 72.12–119.99). Prevalence and YLDs estimate followed the same pattern, with the number of prevalence cases increased from 3,400,460 (95% UI: 2,958,279–3,925,843) to 5,371,438 (95% UI: 4,703,837–6,196,132), the number of YLDs cases increased from 352,960 (95% UI: 235,711–491,606) to 545,923 (95% UI: 366,571–757,099), the ASPR decreased from 81.55 (95% UI: 71.55–93.04) to 65.19 (95% UI: 56.89–75.28), and the age-standardized YLDs cases decreased from 8.33 (95% UI: 5.61–11.49) to 6.62 (95% UI: 4.43–9.2) per 100,000 population (Figure 2, Tables 1–3).
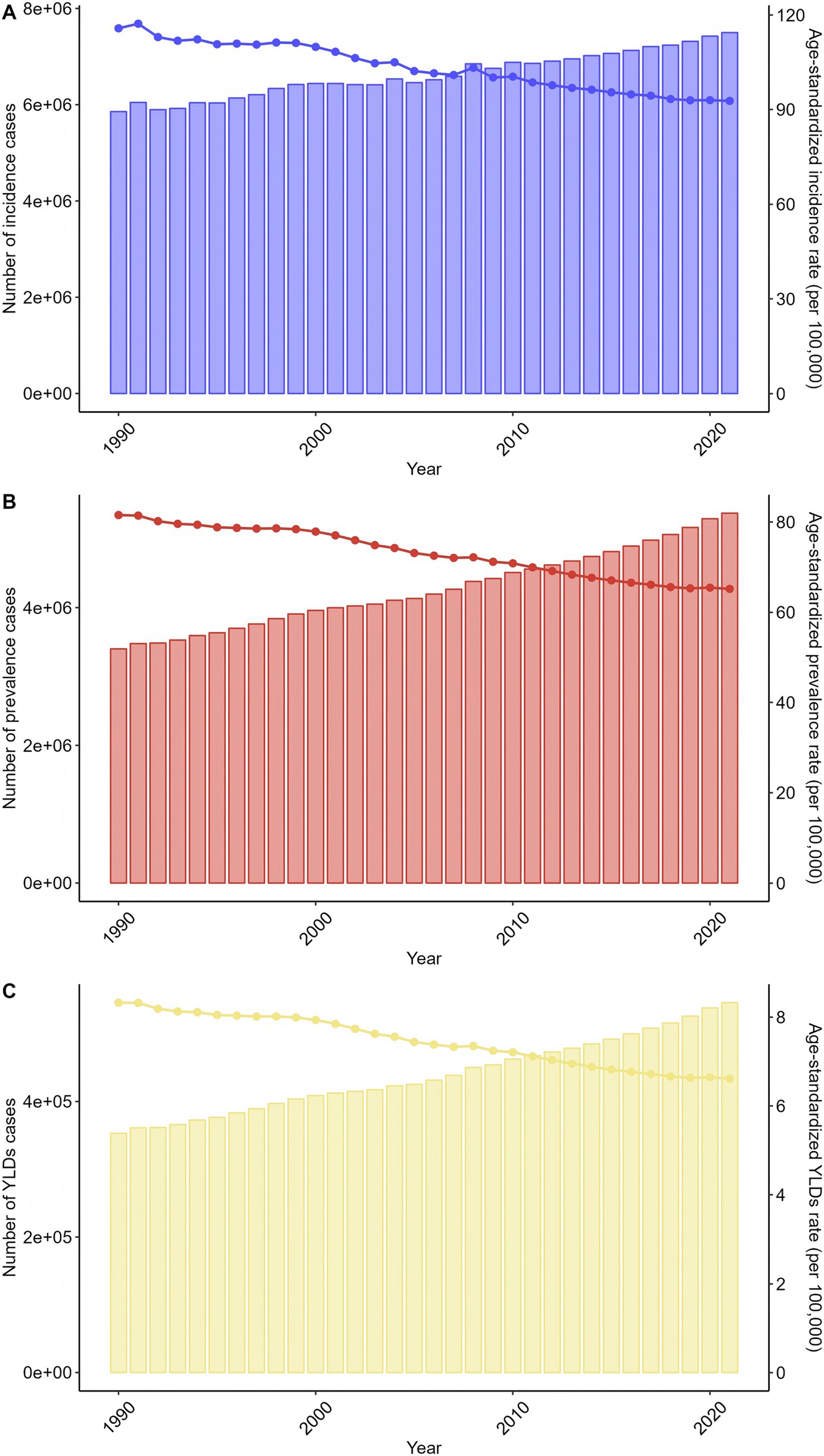
Figure 2. Trends in the numbers and age-standardized rates of fracture of vertebral column-related incidence, prevalence, and YLDs globally from 1990 to 2021.
The trends in males and females alone were consistent with the whole population (Supplementary Figure S5, Tables 1–3). Moreover, the trends were also consistent for most age groups except for older adults (Supplementary Figure S6, Tables 1–3). At the SDI region level, all SDI regions showed the same trend as the whole population (Supplementary Figure S7, Tables 1–3).
Across GBD regions, the trend of the fracture of vertebral column-related disease burden varied. The results of cluster analysis were shown in Figure 3. The significant incidence, prevalence, and YLDs rate increase occurred in Caribbean, while the significant decrease was in North Africa and Middle East, Eastern Mediterranean Region, Middle East & North Africa-WB, East Asia, Oceania, Commonwealth High Income, Australasia, Basic Health System, Southern Latin America, Western Sub-Saharan Africa, Western Africa, North America, High-income North America, Commonwealth Middle Income, South Asia-WB, South Asia, Limited Health System, World Bank Low Income, and Minimal Health System (Figure 3).
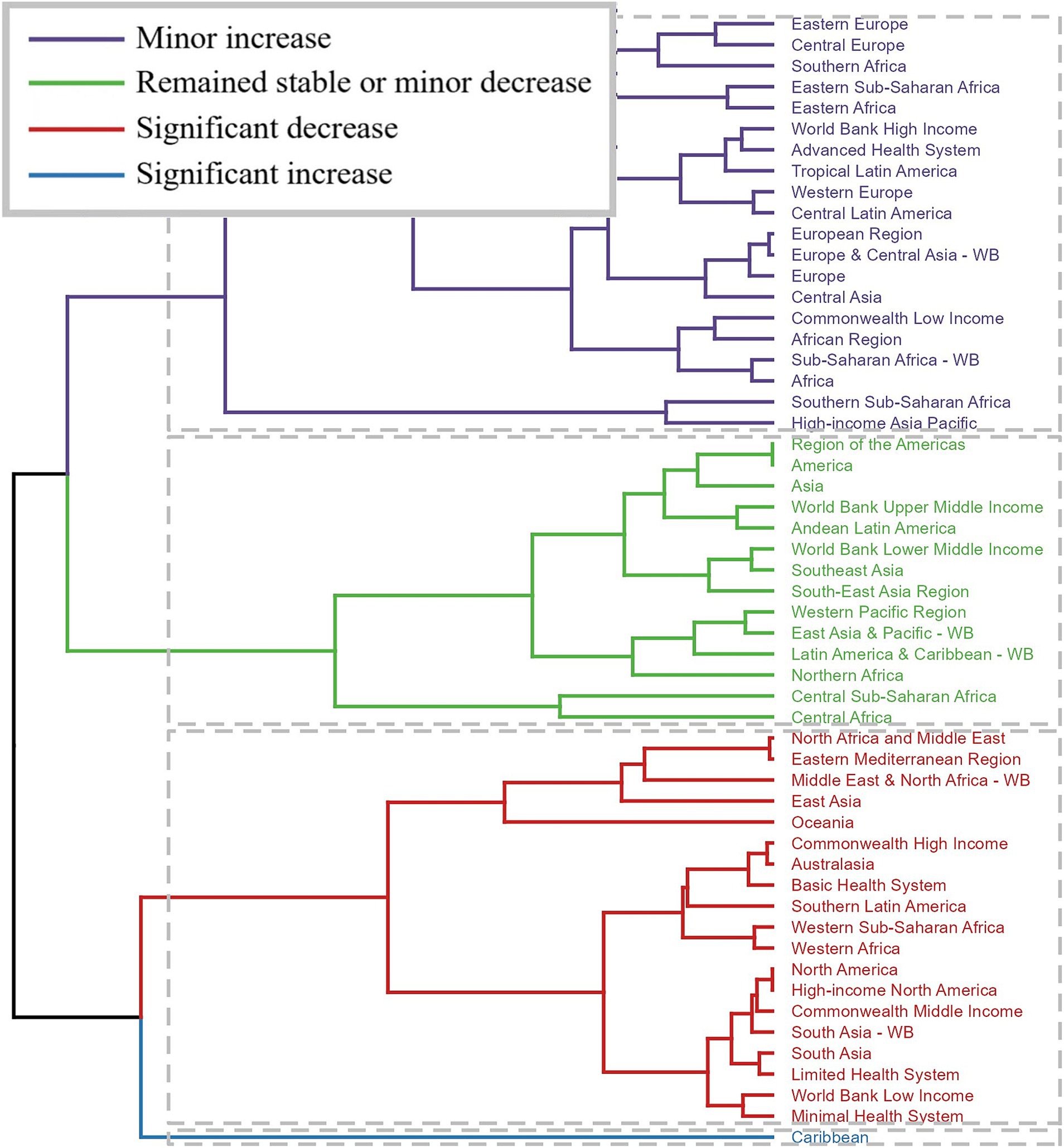
Figure 3. Results of cluster analysis based on the EAPC values of the fracture of vertebral column-related age-standardized rates for incidence, prevalence, and YLDs from 1990 to 2021.
Across countries and territories, the changing trend was also different. The most pronounced increase in ASIR [EAPC = 5.24, 95% confidence interval (CI): 3.34–7.19], ASPR (EAPC = 4.79, 95% CI: 3.53–6.06), and the age-standardized YLDs cases (EAPC = 4.81, 95% CI: 3.53–6.12) from 1990 to 2021 was observed in Syrian Arab Republic. The most pronounced decrease in ASIR (EAPC = −4.61, 95% CI: −6.07 to −3.12) was Timor-Leste. And the most pronounced decrease in ASPR (EAPC = −2.35, 95% CI: −2.57 to −2.13) and the age-standardized YLDs cases (EAPC = −2.33, 95% CI: −2.55 to −2.12) was Latvia (Figure 4, Tables 1–3).

Figure 4. The EAPC of fracture of vertebral column-related ASRs from 1990 to 2021.
The predicted results from 2022 to 2046
The predicted results of the APC model showed that the number of incidence, prevalence, and YLDs cases for both genders would increase from 2022 to 2046. The number of incidence cases for males was 4,412,932 in 2021, and was 276,314 in 2046. The number of prevalence cases was 2,766,006 in 2022, and was 4,031,334 in 2046. And the number of YLDs was 285,497 in 2022, and was 407,631 in 2046. For females, the number of incidence cases increased from 3,306,504 in 2022 to 4,620,813 in 2046. The number of prevalence cases increased from 2,743,602 to 4,764,050 during this period. And the number of YLDs cases increased from 273,619 to 460,041. Although the predicted results show the number of cases will continue to increase, but the ASRs showed the decreasing trend over the next 25 years for both genders. In 2021, the ASIR for males was 108.50 per 100,000 population, and was 102.79 in 2046. The ASPR for males was 69.60 in 2022, and was 63.57 in 2046. During the same period, the age-standardized YLDs cases decreased from 7.15 to 6.52. For females, the ASIR decreased from 77.48 to 74.59, the ASPR decreased from 59.65 to 56.13, and the age-standardized YLDs cases decreased from 5.97 to 5.55 (Figure 5, Table 4).
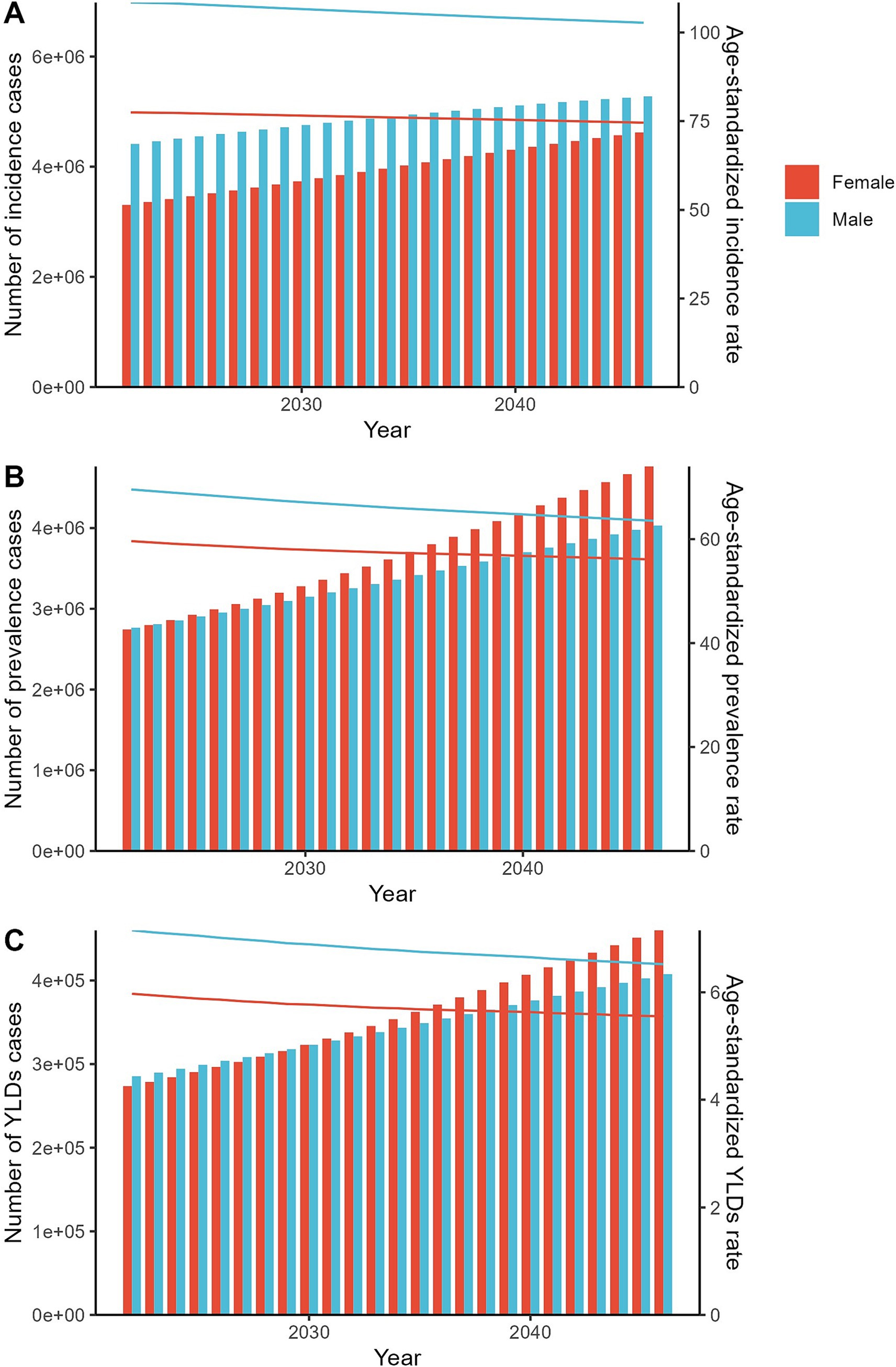
Figure 5. The predicted results in the fracture of vertebral column-related numbers and age-standardized rates of incidence, prevalence, and YLDs by sex globally from 2022 to 2046 of the APC model.

Table 4. The predicted results in the fracture of vertebral column-related numbers and age-standardized rates of incidence, prevalence, and YLDs by sex globally from 2022 to 2046 of the APC model.
Discussion
As far as we know, this was the latest study to comprehensively assess and quantify fracture of vertebral column-related disease burden globally and then predict the future tendency of the disease burden. Globally, fracture of vertebral column caused a severe disease burden in 2021, and significant differences in the disease burden existed between sexes and across ages, SDI regions, GBD regions, and countries. From 1990 to 2021, there was an decreasing trend for the ASRs globally. However, the number of cases were still very severe which showed an increasing trend. Furthermore, our predicted results showed that the number of cases would still increase in the next 25 years.
The incidence and prevalence of vertebral column fractures reported in this study align with a growing body of literature highlighting the significant burden of spinal fractures globally. Our findings indicate a vertebral column fracture incidence of 92.75 per 100,000 population, which is comparable to previous estimates by Johnell and Kanis (17) and Zheng et al. (3), who reported similar incidence rates. The prevalence of 65.19 per 100,000 echoes the trends observed in recent systematic reviews (5, 19). Notably, the number of YLDs attributed to vertebral column fractures, at 545,923, underscores the considerable impact on health outcomes, corroborating the findings of previous study which emphasized the substantial morbidity associated with these fractures (2). The ASR of YLDs of 6.62 per 100,000 further emphasizes the need for preventive measures and improved management strategies. These results emphasize the urgent need for targeted interventions to mitigate the rising incidence and prevalence of vertebral column fractures.
The global incidence of vertebral column fractures has increased from 5,856,226 in 1990 to 7,497,446 in 2021, despite a decrease in the ASIR from 115.75 to 92.75 per 100,000 population over the same period. This trend is mirrored by the prevalence and YLDs estimates, with an increase in the number of cases but a decline in the ASPR and age-standardized YLDs rate per 100,000 population. Our findings contrast with previous studies (3, 17) that reported stable or declining incidence rates of vertebral fractures, possibly due to variations in data sources, study populations, or improvements in fracture prevention and management strategies in recent years. The observed decrease in ASPR and age-standardized YLDs may reflect advancements in healthcare, including early detection, better treatment options, and increased awareness of fracture risk factors (20, 21). However, the overall increase in incidence and prevalence cases highlights the continued need for effective interventions to reduce the burden of vertebral column fractures globally.
Our study reveals significant gender disparities in the incidence, prevalence, and YLDs due to a specific health condition in 2021, with males experiencing 1.33, 1.01, and 1.04 times higher case counts, respectively, compared to females. Correspondingly, the ASRs for males were 1.40, 1.17, and 1.19 times those of females. These findings align with previous research (22, 23) indicating higher vulnerability to this condition among males, potentially attributed to biological, behavioral, and environmental factors. Notably, the observed trends in both males and females followed a similar pattern to the overall population, suggesting that gender-specific risk factors may be influencing the disease burden similarly across different demographics. However, the magnitude of gender disparities in ASRs underscores the need for tailored prevention and management strategies to address the unique needs of males and females, ultimately aiming to reduce the overall disease burden.
Our findings in 2021 indicate a consistent increase in ASIR, ASPR, and age-standardized YLDs rate with advancing age, suggesting an age-related vulnerability to the health condition studied. However, the absolute number of incidence, prevalence, and YLDs cases followed a biphasic pattern, peaking in middle age before declining in older adults, which contrasts with some previous studies reporting a monotonic increase with age (24). This discrepancy might be attributed to differential survival rates among age groups or varying severity of the condition. The trends observed were generally consistent across most age groups, except for older adults, where deviations could be influenced by comorbidities and competing risks of mortality. Our results emphasize the importance of age-specific interventions tailored to address the peak incidence and prevalence periods while considering the decline in cases among the oldest adults, aligning with recommendations from recent literature (25) that advocate for life-course approaches to chronic disease management.
Our results demonstrate that the high SDI region reported the highest number of incidence, prevalence, and YLDs cases for the health condition studied, with 2,141,941 incidence cases, 2,469,882 prevalence cases, and 245,574 YLDs cases, respectively. Consistent with these findings, the highest ASIR, ASPR, and age-standardized YLDs rate were also observed in the high SDI region. These values were 157.17 for ASIR, 131.65 for ASPR, and 13.36 for the age-standardized YLDs rate, respectively. This trend aligns with previous studies (24, 26) that have reported a positive correlation between SDI and the burden of non-communicable diseases. However, it is noteworthy that despite the varying SDI levels, all regions exhibited similar trends to the overall population, indicating a ubiquitous nature of the risk factors associated with this health condition. These findings underscore the need for comprehensive and equitable healthcare strategies across different SDI regions to address the rising burden of this health condition.
In our study, the geographical distribution of vertebral column fracture-related incidence and burden varied significantly across the 54 GBD regions. Asia emerged as the leading region in terms of incidence, followed by regions with Advanced and Basic Health Systems, aligning with previous studies highlighting the high prevalence of spinal injuries in developing countries due to road traffic accidents and occupational hazards (2, 15). However, in contrast to incidence, the Advanced Health System region topped the charts for prevalence and YLDs, followed by World Bank High Income and Asia, suggesting better diagnostic capabilities and longer survival with disability in developed healthcare systems (27, 28). Notably, Oceania reported the lowest number of cases, potentially due to its smaller population and better safety standards. The ASRs revealed Australasia at the peak and Commonwealth Low Income regions at the bottom, indicating a socio-economic gradient in disease burden, consistent with findings from global health disparities research (29). The cluster analysis further elucidated contrasting trends, with Caribbean regions experiencing significant increases in incidence, prevalence, and YLDs, whereas multiple regions, including North Africa, Middle East, and high-income areas like North America, exhibited decreases. These trends might be attributed to improvements in trauma care and public health interventions in some regions, while others still grapple with rising risk factors such as aging populations and osteoporosis (11, 30). Overall, our findings underscore the need for tailored intervention strategies considering regional variations in vertebral column fracture burden.
Our findings reveal substantial variations in the disease burden of fracture of vertebral column globally, with Andorra exhibiting the highest ASRs in 2021, contrasting with the lowest ASRs observed in Kiribati and Madagascar. The absolute numbers indicate China, India, and the USA as the countries with the highest incidence, prevalence, and YLDs cases, while Tokelau and Niue reported the lowest. These observations align partially with prior studies highlighting regional disparities in fracture incidence and outcomes (2, 24). Notably, the Syrian Arab Republic showed the most significant increase in ASIR, ASPR, and YLDs cases from 1990 to 2021, potentially linked to the ongoing conflict and subsequent healthcare disruptions (31). Conversely, Timor-Leste and Latvia experienced notable decreases, suggesting improvements in healthcare infrastructure and injury prevention measures (32). The diverse trends across countries underscore the need for tailored interventions to address the burden of vertebral column fractures, considering socio-economic, political, and healthcare factors.
The APC model’s predictions indicate a rise in incidence, prevalence, and YLDs cases for both genders from 2022 to 2046, aligning with previous forecasts in global health literature (33). However, our study uniquely reveals a concurrent decline in ASRs for these outcomes over the next 25 years. This finding contrasts with studies that projected sustained increases in ASRs for similar conditions (2, 34), suggesting potential improvements in disease prevention, early detection, or management strategies. The observed decrease in ASRs for both males and females, despite the overall increase in case numbers, implies a favorable shift in population health dynamics. These trends highlight the need for continued investment in healthcare infrastructure and interventions to maintain and potentially accelerate the decline in ASRs, while also addressing the growing absolute number of cases. Continuous monitoring and policy adaptations are essential to mitigate the increasing disease burden.
This study is subject to several limitations. The GBD 2021 data rely extensively on statistical modeling, particularly in regions with sparse original data (such as sub-Saharan Africa and parts of Southeast Asia), where input sources may be limited to surveys, hospital registries, or indirect estimates (35). While the GBD consortium employs rigorous Bayesian meta-regression tools (DisMod-MR) to minimize bias and cross-validate estimates, residual uncertainty persists in settings with incomplete vital registration systems (36). Importantly, excluding these modeled data would disproportionately erase the health burden representation of populations in low-resource settings, where fragility fractures are often underdiagnosed and underreported. Retaining these estimates, despite their limitations, allows for a more equitable global perspective, albeit with the caveat that trends in such regions may reflect modeled approximations rather than empirical observations. Furthermore, sensitivity analyses conducted by the GBD collaborators suggest that modeled estimates for spinal fractures in data-scarce regions exhibit wider UIs compared to high-quality data regions. This implies that while absolute values (incidence rates) in these areas should be interpreted cautiously, relative trends (age-standardized rate changes over time) remain robust due to internal consistency in modeling assumptions. To mitigate these limitations, we emphasize that our conclusions prioritize identifying geographic and socioeconomic disparities rather than absolute burden quantification. Future studies incorporating primary data from emerging national registries (the WHO Fracture Risk Audit in LMICs) are urgently needed to validate these models.
Conclusion
In conclusion, this systematic analysis of the global, regional, and national burden of fracture of vertebral column, with projections to 2046, represents a significant step forward in addressing the challenges posed by this disease. By providing comprehensive and timely data, our study aims to inform evidence-based policies and interventions aimed at reducing the incidence, prevalence, and YLDs lost due to fracture of vertebral column worldwide.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and the institutional requirements.
Author contributions
YL: Formal analysis, Writing – original draft. SC: Methodology, Writing – original draft. GL: Software, Writing – original draft. CL: Data curation, Writing – original draft. JW: Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The work was financially supported by Natural Science Foundation of Guangxi Zhuang Autonomous Region, China (No. 2024GXNSFBA010004); and Self-Funded Research Project by Administration of Traditional Chinese Medicine of Guangxi Zhuang Autonomous Region, China (No. GXZYA20240457).
Acknowledgments
We would like to thank all the professionals who contributed to the discussion and elaboration of this minireview.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1573888/full#supplementary-material
References
1. Kondo, KL. Osteoporotic vertebral compression fractures and vertebral augmentation. Semin Intervent Radiol. (2028) 25:413–24. doi: 10.1055/s-0028-1103000
2. Lems, WF, Paccou, J, Zhang, J, Fuggle, NR, Chandran, M, Harvey, NC, et al. International osteoporosis foundation fracture working group. Vertebral fracture: epidemiology, impact and use of DXA vertebral fracture assessment in fracture liaison services. Osteoporos Int. (2021) 32:399–411. doi: 10.1007/s00198-020-05804-3
3. Zheng, XQ, Xu, L, Huang, J, Zhang, CG, Yuan, WQ, Sun, CG, et al. Incidence and cost of vertebral fracture in urban China: a 5-year population-based cohort study. Int J Surg. (2023) 109:1910–8. doi: 10.1097/JS9.0000000000000411
4. Lan, Z, Liu, C, Wang, H, Wang, Y, Kan, S, Jiao, Y, et al. Temporal trends in the burden of vertebral fractures caused by falls in China and globally from 1990 to 2021: a systematic analysis of the global burden of disease study 2021. Arch Public Health. (2025) 83:42. doi: 10.1186/s13690-025-01500-y
5. Sing, CW, Lin, TC, Bartholomew, S, Bell, JS, Bennett, C, Beyene, K, et al. Global epidemiology of hip fractures: secular trends in incidence rate, post-fracture treatment, and all-cause mortality. J Bone Miner Res. (2023) 38:1064–75. doi: 10.1002/jbmr.4821
6. Murray, CJ, Vos, T, Lozano, R, Naghavi, M, Flaxman, AD, Cmichaud, M, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the global burden of disease study 2010. Lancet. (2012) 380:2197–223. doi: 10.1016/S0140-6736(12)61689-4
7. Kumar, R, Lim, J, Mekary, RA, Rattani, A, Dewan, MC, Sharif, SY, et al. Traumatic spinal injury: global epidemiology and worldwide volume. World Neurosurg. (2018) 113:e345–63. doi: 10.1016/j.wneu.2018.02.033
8. Mitchell, PJ, Chan, DD, Lee, JK, Tabu, I, and Alpuerto, BB. The global burden of fragility fractures – what are the differences, and where are the gaps. Best Pract Res Clin Rheumatol. (2022) 36:101777. doi: 10.1016/j.berh.2022.101777
9. Olufadewa, I, Adesina, M, and Ayorinde, T. Global health in low-income and middle-income countries: a framework for action. Lancet Glob Health. (2021) 9:e899–900. doi: 10.1016/S2214-109X(21)00143-1
10. Sharma, A, Singh, A, Dar, MA, Kaur, RJ, Charan, J, Iskandar, K, et al. Menace of antimicrobial resistance in LMICs: current surveillance practices and control measures to tackle hostility. J Infect Public Health. (2022) 15:172–81. doi: 10.1016/j.jiph.2021.12.008
11. Xiao, PL, Cui, AY, Hsu, CJ, Peng, R, Jiang, N, Xu, XH, et al. Global, regional prevalence, and risk factors of osteoporosis according to the World Health Organization diagnostic criteria: a systematic review and meta-analysis. Osteoporos Int. (2022) 33:2137–53. doi: 10.1007/s00198-022-06454-3
12. Kim, Y. The effects of smoking, alcohol consumption, obesity, and physical inactivity on healthcare costs: a longitudinal cohort study. BMC Public Health. (2025) 25:873.
13. Bassatne, A, Harb, H, Jaafar, B, Romanos, J, Ammar, W, and El-Hajj Fuleihan, G. Disease burden of osteoporosis and other non-communicable diseases in Lebanon. Osteoporos Int. (2020) 31:1769–77. doi: 10.1007/s00198-020-05433-w
14. GBD 2021 Risk Factors Collaborators. Global burden and strength of evidence for 88 risk factors in 204 countries and 811 subnational locations, 1990-2021: a systematic analysis for the global burden of disease study 2021. Lancet. (2024) 403:2162–203. doi: 10.1016/S0140-6736(24)00933-4
15. GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet. (2020) 396:1223–49. doi: 10.1016/S0140-6736(20)30752-2
16. Murray, CJLGBD 2021 Collaborators. Findings from the global burden of disease study 2021. Lancet. (2024) 403:2259–62. doi: 10.1016/S0140-6736(24)00769-4
17. Johnell, O, and Kanis, JA. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int. (2006) 17:1726–33.
18. GBD 2017 SDG Collaborators. Measuring progress from 1990 to 2017 and projecting attainment to 2030 of the health-related sustainable development goals for 195 countries and territories: a systematic analysis for the global burden of disease study 2017. Lancet. (2018) 392:2091–138. doi: 10.1016/S0140-6736(18)32281-5
19. Ballane, G, Cauley, JA, Luckey, MM, and El-Hajj Fuleihan, G. Worldwide prevalence and incidence of osteoporotic vertebral fractures. Osteoporos Int. (2017) 28:1531–42. doi: 10.1007/s00198-017-3909-3
20. Kanis, JA, Johnell, O, Oden, A, Sernbo, I, Redlund-Johnell, I, Dawson, A, et al. Long-term risk of osteoporotic fracture in Malmö. Osteoporos Int. (2000) 11:669–74. doi: 10.1007/s001980070064
21. Alsoof, D, Anderson, G, McDonald, CL, Basques, B, Kuris, E, and Daniels, AH. Diagnosis and management of vertebral compression fracture. Am J Med. (2022) 135:815–21. doi: 10.1016/j.amjmed.2022.02.035
22. Cullen, KW, Koehly, LM, Anderson, C, Baranowski, T, Prokhorov, A, Basen-Engquist, K, et al. Gender differences in chronic disease risk behaviors through the transition out of high school. Am J Prev Med. (1999) 17:1–7. doi: 10.1016/s0749-3797(99)00038-0
23. Adhikari, K, Gupta, N, and Koshy, AK. Gender differences on risk factors of non-communicable diseases – a community based cross-sectional study in Central Nepal. J Nepal Health Res Counc. (2014) 12:89–93.
24. GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the global burden of disease study 2017. Lancet. (2018) 392:1736–88. doi: 10.1016/S0140-6736(18)32203-7
25. Ford, ES, Ajani, UA, Croft, JB, Critchley, JA, Labarthe, DR, Kottke, TE, et al. Explaining the decrease in U.S. deaths from coronary disease, 1980-2000. N Engl J Med. (2007) 356:2388–98.
26. GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet. (2020) 396:1204–22. doi: 10.1016/S0140-6736(20)30925-9
27. Global Burden of Disease Study 2013 Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990-2013: a systematic analysis for the global burden of disease study 2013. Lancet. (2015) 386:743–800. doi: 10.1016/S0140-6736(15)60692-4
28. Beran, D, Pedersen, HB, and Robertson, J. Noncommunicable diseases, access to essential medicines and universal health coverage. Glob Health Action. (2019) 12:1670014. doi: 10.1080/16549716.2019.1670014
29. Engelgau, MM, Rosenthal, JP, Newsome, BJ, Price, L, Belis, D, and Mensah, GA. Noncommunicable diseases in low- and middle-income countries: a strategic approach to develop a global implementation research workforce. Glob Heart. (2018) 13:131–7. doi: 10.1016/j.gheart.2018.05.001
30. Ferrari, AJ, Somerville, AJ, Baxter, AJ, Norman, R, Patten, SB, Vos, T, et al. Global variation in the prevalence and incidence of major depressive disorder: a systematic review of the epidemiological literature. Psychol Med. (2013) 43:471–81. doi: 10.1017/S0033291712001511
31. Kampalath, V, Tarakji, A, Hamze, M, Loutfi, R, Cohn, K, and Abbara, A. The impacts of the Syrian conflict on child and adolescent health: a scoping review. J Public Health. (2022) 45:621–30.
32. Heynen, AP, MacGinley, TJ, and Aguilar, LE. Electrification in post-conflict Timor-Leste: opportunities for energy services to enhance rural agricultural development. Energy Res Soc Sci. (2024) 110:103433. doi: 10.1016/j.erss.2024.103433
33. Dong, Y, Peng, R, Kang, H, Song, K, Guo, Q, Zhao, H, et al. Global incidence, prevalence, and disability of vertebral fractures: a systematic analysis of the global burden of disease study 2019. Spine J. (2022) 22:857–68. doi: 10.1016/j.spinee.2021.12.007
34. Mathers, CD, and Loncar, D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. (2006) 3:e442. doi: 10.1371/journal.pmed.0030442
35. Cen, J, Wang, Q, Cheng, L, Gao, Q, Wang, H, and Sun, F. Global, regional, and national burden and trends of migraine among women of childbearing age from 1990 to 2021: insights from the global burden of disease study 2021. J Headache Pain. (2024) 25:96. doi: 10.1186/s10194-024-01798-z
Keywords: fracture of vertebral column, global burden of disease, incidence, prevalence, years lived with disability
Citation: Lan Y, Chen S, Lan G, Li C and Wei J (2025) Global, regional, and national burden of fracture of vertebral column, 1990–2021: analysis of data from the global burden of disease study 2021. Front. Public Health. 13:1573888. doi: 10.3389/fpubh.2025.1573888
Edited by:
Jingwen Hu, University of Michigan, United StatesReviewed by:
Alypio Nyandwi, Ministry of Health, RwandaArben Boshnjaku, University of Gjakova ‘Fehmi Agani’, Albania
Copyright © 2025 Lan, Chen, Lan, Li and Wei. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jiyong Wei, NTQ5NzYxNjg1QHFxLmNvbQ==
†These authors have contributed equally to this work and share first authorship