Abstract
Background:
This study investigated the satisfaction of migrant populations in Guangzhou with primary care and explored how community integration and economic development at the district level influenced this satisfaction. This study aimed to provide empirical evidence and recommendations for improving primary care utilization and community integration among migrant populations.
Methods:
We conducted a stratified random sampling of 1,996 migrant individuals from seven districts in Guangzhou. A custom-designed questionnaire was used to collect data on demographic characteristics, satisfaction with primary care, and community integration, including willingness to seek help, neighborhood interactions, and participation in community activities. Multi-variate linear regression analysis was used to identify factors associated with satisfaction with primary care.
Results:
The mean satisfaction score for primary care was 3.29 ± 0.76. Participation in community activities was positively associated with satisfaction, with participants often reporting higher scores (increases of 0.08 and 0.28 points, respectively; p < 0.05). Greater neighborhood interaction and willingness to seek assistance from local authorities also increased satisfaction (0.11 and 0.37 points, respectively; p < 0.05). Residing in districts with moderate or good economic conditions further enhanced satisfaction (0.37 and 0.10 points, respectively; p < 0.05).
Conclusion:
Although migrant populations in Guangzhou generally report high satisfaction with primary care, their level of community integration remains limited. Enhancing community public services and fostering a stronger sense of community belonging are promising strategies for improving primary care management and services for migrant populations.
1 Introduction
Industrialization and urbanization in China have driven a massive migration of residents to cities. By the end of 2022, migrant populations accounted for approximately 18% of the total population, according to the China Migrant Population Development Report (2022). These individuals face heightened health risks owing to occupational hazards and poor living conditions. In their destination cities, migrant populations often encounter inadequate access to immunization, infectious disease control, and occupational health protection (1). Moreover, they frequently face disadvantages when accessing routine medical services and insurance benefits (2). The World Health Organization (WHO) emphasizes that everyone should have access to essential healthcare (3). As such, ensuring that the primary care needs of migrant populations are met is a critical public issue that must be addressed (4). In China, primary care is primarily provided by primary care institutions, including township hospitals and community health centers within community settings.
The community not only serves as the primary location for migrant populations to access primary care services, but also as their foothold and foundation for integration into urban life. Community integration refers to the process of interaction, exchange, adaptation, and acceptance among individuals, groups, and cultures, and reflects the degree of participation, identification, and acceptance within a specific society. Most studies have indicated that community integration facilitates the utilization of primary care services by migrant populations. For instance, research by Bu et al. found that older adult migrant populations with better community integration tend to use more public health services (5). Jing discovered that enhancing the community integration of migrant parents effectively increased the utilization rate of healthcare services among migrant children (6). Studies have also suggested that receiving public health services can improve community integration among migrant populations (7). These findings highlight a mutually reinforcing relationship between community integration and health service utilization. Strengthening community integration can enhance the access of migrant populations to primary care services, reinforcing their sense of identity and community integration. However, academic research on the relationship between the access of migrant populations to primary care services and community integration remains limited and warrants further attention.
In urban China, primary care provision is predominantly funded at the district level by government fiscal income. Therefore, the economic development level of districts significantly influences the primary medical service capacity and institutional construction level of the entire region (8). In economically developed districts, governments have stronger financial capabilities to support the development of primary care, enabling them to create high-quality medical environments, purchase advanced medical equipment, attract a large number of medical professionals, and provide higher-quality primary medical services (9). In contrast, economically underdeveloped areas face relatively backward primary medical service capabilities and institutional construction levels due to limited financial resources (10). These regional disparities in primary medical service capabilities and institutional construction levels further affect the satisfaction of migrant populations with primary care (11).
However, the satisfaction of migrant populations with primary care is not only influenced by primary care provision, but also impacted by their perception and experience of integrating into urban life (12). Some other studies suggest that migrants working or living in higher economic development regions may face more difficulty in integrating into local community, which may negatively affect their satisfaction with primary care (13). This duality underscores the need for context-specific policy interventions to reconcile economic growth, community integration promotion and primary care provision. Therefore, alongside enhancing primary healthcare capacity and institutional development, attention must be given to migrants’ perceptions and experiences of urban integration. Systematic approaches involving cross-sector collaboration and policy coordination are required to address the complex interactions among economic development, social integration, and healthcare provision, thereby improving migrants’ overall satisfaction with primary care (14).
Guangzhou, as the capital of Guangdong Province and a megacity of southern China, is a major destination for migrants with a resident population exceeding 22 million and managing over 10 million migrant residents (15). Addressing the healthcare needs of the migrant population and ensuring their health and sustainable development are the primary responsibilities of the Guangzhou government (16). To ensure migrant populations access basic medical resources and promote social integration, Guangdong Province has enacted policies guaranteeing migrants’ equal access to primary care, family planning, public cultural and sports services, employment services, and compulsory education (17). The government also prioritizes migrant health education and promotion by establishing model enterprises, schools, and healthy families, using diverse approaches to encourage migrants’ local integration, health management participation, and service utilization (18).
Therefore, this study investigated the satisfaction of migrant populations in Guangzhou with primary care and analyzed the association between community integration and district-level economic development with satisfaction. It also explored the factors that enhance the utilization of primary care among migrant populations.
2 Methods
2.1 Sample size
Guangzhou comprises 11 districts, with its 7 central urban districts (Tianhe, Yuexiu, Haizhu, Liwan, Baiyun, Huangpu, and Panyu) collectively hosting 83.98% of the city’s migrant population (19). Therefore, these 7 urban districts were selected as the study sites.(See Appendix 1 for details).
The minimum sample size was calculated using a standard formula for the population proportion estimation (20):
where n is the sample size, z is the confidence interval, is the estimated population proportion, and Δ is the margin of error.
Based on the 2019 national migrant population proportion of 17%, with a margin of error of 2% and a 95% confidence interval, the minimum sample size was calculated as 1,355. Considering a 10% nonresponse rate, the final minimum sample size was adjusted to 1,491.
We categorized the 7 sampled districts into three economic levels (low, medium, and high) based on their 2019 GDP levels and ensured balanced sampling across these levels. A total of 2,050 questionnaires were distributed. After excluding invalid responses, we obtained 1,996 valid questionnaires with a response rate of 97.37%. The distribution was balanced across the economic levels: high (773, 38.73%), medium (602, 30.16%), and low (621, 31.11%). The specific sampling data for each district are shown in Figure 1.
Figure 1
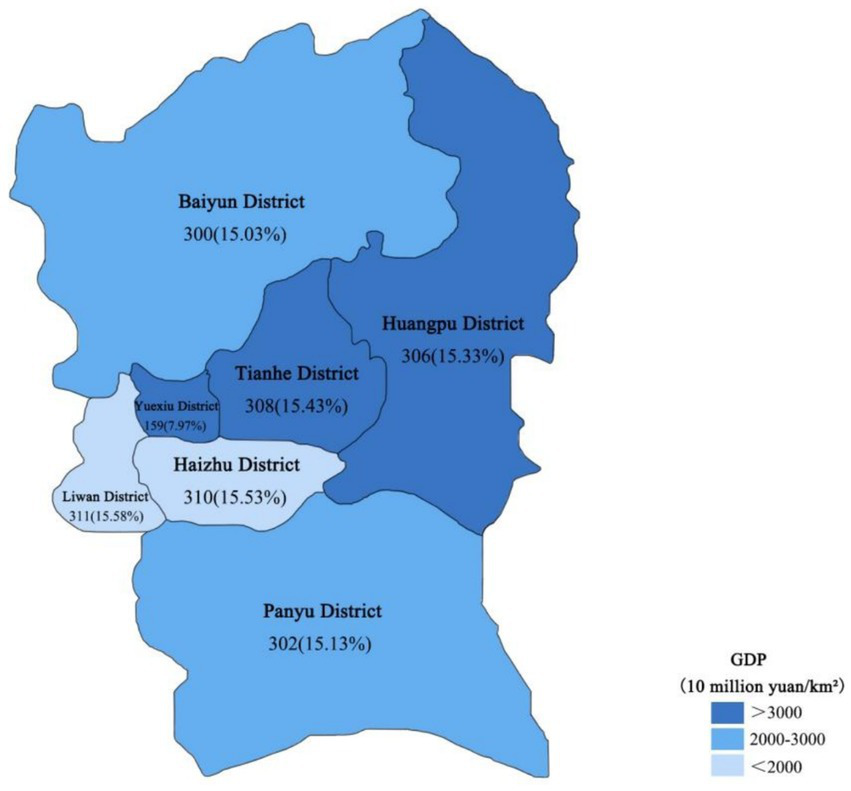
Regional economic characteristics and sampling methodology of the investigated areas in Guangzhou.
2.2 Questionnaire and survey
The questionnaire was designed based on a literature review, expert interviews, and a pilot survey. Trained investigators conducted the survey using a paper-based questionnaire. The questionnaire primarily covered demographic information (e.g., age, sex, household registration, occupation, length of residence), satisfaction with primary care, and community integration.
The survey was conducted between January and March, 2019. Paper questionnaires were distributed through community-based outreach and recruitment at community health centers, migrant service centers, labor markets, and other channels within the sub-districts (towns). Questionnaires were checked for quality immediately upon completion. The participants provided informed consent and cooperation to ensure the integrity and consistency of their responses. Face-to-face interviews were conducted to ensure complete and consistent data collection. Participants met the following criteria: (1) residing in Guangzhou for at least 6 months; (2) non-Guangzhou household registration; and (3) able to fill out the questionnaire independently or with assistance; (4) age ≥18 years old. All participants were informed and agreed to participate in the study.
2.3 Main variables
2.3.1 Satisfaction with primary care
Satisfaction with primary care was defined as the migrants’ comprehensive evaluation of community-based healthcare services across four domains: service quality, facility environment, staff attitudes, and procedural efficiency. Responses were quantified using a 5-point Likert Scale (1 = Very Dissatisfied, 5 = Very Satisfied).
2.3.2 Community integration
With rapid economic growth and internal migration, promoting community integration of the migrant population has become a key management focus. Communities are both the primary living spaces for migrants and central sites for governance and public service delivery. As a subset of social integration, community integration emphasizes interactions between residents and their communities and their outcomes. Primary care, as an integrated public service model, plays a crucial role in advancing migrant social integration (21). Based on China’s context, scholars have developed a four-dimensional framework-economic integration, social adaptation, cultural acquisition, and psychological identification that includes help-seeking, neighborhood interaction, and community participation (22). The 2013 Survey on Social Integration of the Migrant Population in China confirmed the validity of indicators like community participation and help-seeking willingness (23).
In this study, community integration was measured through three items:
Neighborhood interaction: it refers to the social interaction and emotional relationships among nearby residents, including various activities such as visiting others, providing mutual support, and offering mutual care (24). Neighborhood relationships are a key factor in the social integration of migrant populations because they can provide employment opportunities, build social trust, and offer social activities (25). Neighborhood networks are considered a fundamental component of community integration, particularly for vulnerable groups in society (26).
Participation in community activity: this reflects an individual’s concern for and willingness to participate in or engage in community affairs. Migrants’ involvement in public activities helps foster a sense of belonging to the city (27).
Willingness to seek help: this indicates the degree of willingness to seek help from local community service offices or neighborhood committees when facing difficulties. This reflects an individual’s tendency to seek help when problems arise and indicates the level of community integration. If migrant populations are more inclined to make friends with locals or seek help from employers, the government, or lawyers rather than remaining within circles of fellow migrants, their social integration is generally higher (28).
2.3.3 Covariates
The covariates included age, sex, household registration, marital status, educational level, occupation, length of residence, average monthly income, and industry classification. Occupations were categorized according to the Three-Industry Classification Regulations (2012) in China into service industry (e.g., service staff, salespersons, and cashiers), manufacturing industry (e.g., construction workers), and others (occupations not easily categorized).
2.3.4 Statistical analysis
Valid questionnaires were entered into Epidata 3.1 to build the dataset, and statistical analysis was performed using Stata MP 16.0. Descriptive statistics included means and percentages. Chi-square and rank-sum tests were conducted for the relevant categories. Stepwise multi-variate linear regression was used to analyze the factors influencing migrant populations’ satisfaction with primary care. Differences were considered statistically significant at p < 0.05.
3 Results
3.1 Characteristics of respondents
Table 1 presents the sociodemographic characteristics of the migrant population. Among the 1,996 migrant individuals surveyed in Guangzhou, 1,041 were female (52.15%), and the majority were young adults who were aged 18–29 years (53.06%). Regarding educational background, a high proportion held junior high school or high school diplomas (54.01%). Married people accounted for 51.75% of the population. Most migrant individuals held rural Hukou registrations (62.88%), and the majority resided locally for 1–5 years (51.75%). The average satisfaction score for primary care was 3.29 ± 0.76.
Table 1
| Variables | Category | All n (%) |
Levels of GDP n (%) | ||
|---|---|---|---|---|---|
| Low | Medium | High | |||
| Total | 1996 (100.0) | 621 (31.11) | 602 (30.16) | 773 (38.73) | |
| Sex | Male | 955 (47.85) | 259 (41.71) | 330 (54.82) | 366 (47.35) |
| Female | 1,041 (52.15) | 362 (58.29) | 272 (45.18) | 407 (52.65) | |
| Age | ≤29 | 1,059 (53.06) | 350 (56.36) | 330 (54.82) | 379 (49.02) |
| 30–39 | 510 (25.55) | 153 (24.64) | 160 (26.58) | 197 (25.49) | |
| ≥40 | 427 (21.39) | 118 (19.00) | 112 (18.60) | 197 (25.49) | |
| Education | Primary and lower | 90 (4.51) | 19 (3.06) | 19 (3.16) | 52 (6.73) |
| Junior/senior high | 1,078 (54.01) | 360 (57.97) | 347 (57.64) | 371 (47.99) | |
| College and above | 828 (41.48) | 242 (38.97) | 236 (39.20) | 350 (45.28) | |
| Medical insurance | Yes | 1,484 (74.35) | 474 (76.33) | 483 (80.23) | 527 (68.18) |
| No | 512 (25.65) | 147 (23.67) | 119 (19.77) | 246 (31.82) | |
| Marriage | Single/divorced | 963 (48.25) | 313 (50.40) | 302 (50.17) | 348 (45.02) |
| Married | 1,033 (51.75) | 308 (49.60) | 300 (49.83) | 425 (54.98) | |
| Hukou registration | Rural | 1,255 (62.88) | 427 (68.76) | 291 (48.34) | 537 (69.47) |
| Urban | 741 (37.12) | 194 (31.24) | 311 (51.66) | 236 (30.53) | |
| Monthly income (RMB) | ≤3,500 | 560 (28.06) | 152 (24.48) | 167 (27.74) | 241 (31.18) |
| 3,501–6,500 | 1,159 (58.07) | 402 (64.73) | 279 (46.35) | 478 (61.84) | |
| ≥6,501 | 277 (13.88) | 67 (10.79) | 156 (25.91) | 54 (6.99) | |
| Years of migration | ≤1 year | 479 (24.00) | 174 (28.02) | 123 (20.43) | 182 (23.54) |
| 1–5 years | 1,033 (51.75) | 267 (43.00) | 340 (56.48) | 426 (55.11) | |
| ≥ 5 years | 484 (24.25) | 180 (28.99) | 139 (23.09) | 165 (21.35) | |
| Occupation | Service Industry | 1,231 (61.67) | 457 (73.59) | 373 (61.96) | 401 (51.88) |
| Manufacturing Industry | 312 (15.63) | 72 (11.59) | 131 (21.76) | 109 (14.10) | |
| Others | 453 (22.70) | 92 (14.81) | 98 (16.28) | 263 (34.02) | |
| Satisfaction to primary care (mean ± SD) | 3.29 ± 0.76 | 3.13 ± 0.87 | 3.53 ± 0.80 | 3.23 ± 0.58 | |
Characteristics of participants and disparity analysis across levels of GDP (N = 1996).
3.2 Community integration of the migrant population
Overall, more than half the respondents reported a relatively negative social integration (Table 2). The frequency of neighborhood interactions was low, with 62.88% reporting infrequent interactions and 18.93% reporting no interactions. Regarding participation in community activities, the majority either did not participate (36.97%) or participated infrequently (50.50%). In terms of willingness to seek help from street offices or residents’ committees when faced with difficulties, 43.14% reported low willingness and 35.97% expressed no willingness. Notably, more economically developed regions exhibited poorer overall social integration, with statistically significant differences (p < 0.001).
Table 2
| Variables | Category | Total n(%) | Levels of GDP n (%) | Chi | p | ||
|---|---|---|---|---|---|---|---|
| Low | Medium | High | |||||
| Neighborhood interactions | Rarely | 378 (18.93) | 118 (19.00) | 67 (11.13) | 193 (24.97) | 127.52 | <0.001 |
| Sometimes | 1,255 (62.88) | 346 (55.72) | 384 (63.79) | 525 (67.92) | |||
| Often | 363 (18.19) | 157 (25.28) | 151 (25.08) | 55 (7.11) | |||
| Community activity participation | Rarely | 738 (36.97) | 197 (31.72) | 214 (35.55) | 327 (42.30) | 27.16 | <0.001 |
| Sometimes | 1,008 (50.50) | 359 (57.81) | 296 (49.17) | 353 (45.67) | |||
| Often | 250 (12.53) | 65 (10.47) | 92 (15.28) | 93 (12.03) | |||
| Willingness to seek help | None | 417 (20.89) | 141 (22.70) | 154 (25.58) | 122 (15.78) | 21.84 | <0.001 |
| Low | 861 (43.14) | 267 (43.00) | 244 (40.53) | 350 (45.28) | |||
| High | 718 (35.97) | 213 (34.30) | 204 (33.89) | 301 (38.94) | |||
Disparities in community integration across levels of GDP.
3.3 Satisfaction with primary care
The satisfaction scores for primary care services varied significantly across different levels of neighborhood interactions, community activity participation, and willingness to seek help, with all differences being statistically significant (p < 0.001) (Table 3). Those who often participated in neighborhood interactions or community activities generally reported higher satisfaction scores, especially in medium-GDP regions. However, economic development level was inversely related to social integration, with more developed regions showing poorer integration and lower satisfaction scores in some categories.
Table 3
| Variables | Category | Levels of GDP | F | p | ||
|---|---|---|---|---|---|---|
| Low | Medium | High | ||||
| Neighborhood interactions | Rarely | 3.20 (1.20) | 3.72 (0.74) | 3.21 (0.65) | 17.02 | <0.001 |
| Sometimes | 3.09 (0.80) | 3.40 (0.75) | 3.23 (0.55) | |||
| Often | 3.17 (0.71) | 3.78 (0.80) | 3.35 (0.62) | |||
| Community activity participation | Rarely | 3.11 (0.73) | 3.36 (0.86) | 3.14 (0.51) | 20.46 | <0.001 |
| Sometimes | 3.10 (0.87) | 3.53 (0.73) | 3.25 (0.59) | |||
| Often | 3.38 (1.17) | 3.95 (0.72) | 3.46 (0.70) | |||
| Willingness to seek help | None | 2.77 (0.84) | 3.56 (0.79) | 3.15 (0.64) | 39.27 | <0.001 |
| Low | 2.95 (0.63) | 3.33 (0.72) | 3.13 (0.45) | |||
| High | 3.59 (0.94) | 3.75 (0.82) | 3.39 (0.65) | |||
Satisfaction with primary care across levels of community integration and GDP per capita.
3.4 Multivariate analysis of social integration and satisfaction with primary care
We conducted a multivariate analysis with satisfaction with primary care as the dependent variable. Model 1 included three variables representing social integration, Model 2 included economic district variables, and Model 3 incorporated control variables such as culture and income. The results demonstrated the robustness of the models.
In Model 3, after controlling for relevant variables, community activity participation, district economic development level, neighborhood interactions, willingness to seek help, average monthly income, gender, and marital status all had statistically significant effects on satisfaction with primary care (p < 0.05). Specifically, compared to non-participants, those who occasionally and frequently participated in community activities reported increased satisfaction scores by 0.08 (p = 0.016) and 0.28 (p < 0.001) points, respectively.
Frequent neighborhood interactions increased satisfaction by 0.11 (p = 0.048) points compared with those with no interactions. The willingness to seek assistance from street offices or resident committees when faced with difficulties increased satisfaction by 0.37 (p < 0.001) points compared to those unwilling to seek help. In terms of regional economic influence, satisfaction scores increased by 0.37 (p < 0.001) and 0.10 (p = 0.020) points in areas with moderate and good economic conditions, respectively, compared with less economically developed areas. Females reported lower satisfaction than males. Married individuals had higher satisfaction, with an increase of 0.08 (p = 0.043) points compared to unmarried or divorced individuals. For those with a monthly income between 3,501 and 6,500 yuan, satisfaction decreased by 0.09 (p = 0.015) points compared to those earning 3,500 yuan or less (Table 4).
Table 4
| Variable | Model 1 | Model 2 | Model 3 | |
|---|---|---|---|---|
| β (95% CI) | β (95% CI) | β (95% CI) | ||
| Neighborhood interactions | Rarely | Ref | Ref | Ref |
| Sometimes | −0.03 (−0.11, 0.06) | −0.07 (−0.15, 0.01) | −0.06 (−0.14, 0.03) | |
| Often | 0.15 (0.04, 0.25)** | 0.09 (−0.01, 0.20) | 0.11 (0, 0.21)* | |
| Community activity participation | Rarely | Ref | Ref | Ref |
| Sometimes | 0.08 (0.01, 0.15)* | 0.09 (0.02, 0.16)* | 0.08 (0.02, 0.15)* | |
| Often | 0.32 (0.21, 0.43)*** | 0.29 (0.19, 0.40)*** | 0.28 (0.18, 0.39) | |
| Willingness to seek help | None | Ref | Ref | Ref |
| Low | −0.03 (−0.12, 0.05) | −0.01 (−0.09, 0.07) | −0.02 (−0.10, 0.07) | |
| High | 0.35 (0.26, 0.44)*** | 0.37 (0.29, 0.46)*** | 0.37 (0.28, 0.46)*** | |
| Levels of GDP | Low | Ref | Ref | |
| Medium | 0.40 (0.32, 0.48)*** | 0.37 (0.29, 0.46)*** | ||
| High | 0.12 (0.04, 0.19)** | 0.10 (0.02, 0.18)* | ||
| Gender | Male | Ref | ||
| Female | −0.07 (−0.13, 0)* | |||
| Age | ≤29 | Ref | ||
| 30–39 | 0.01 (−0.08, 0.11) | |||
| ≥40 | −0.08 (−0.19, 0.03) | |||
| Education | Primary and lower | Ref | ||
| Junior/senior high | −0.14 (−0.30, 0.02) | |||
| College and above | −0.06 (−0.23, 0.11) | |||
| Marriage | Single/divorced | Ref | ||
| Married | 0.08 (0, 0.16)* | |||
| Hukou registration | Rural | Ref | ||
| Urban | −0.03 (−0.10, 0.04) | |||
| Monthly income (RMB) | ≤3,500 | Ref | ||
| 3,501–6,500 | −0.09 (−0.16, -0.02)* | |||
| ≥6,500 | 0.01 (−0.10, 0.12) | |||
| Duration of residence | ≤ 1 year | Ref | ||
| 1–5 years | 0.06 (−0.02, 0.13) | |||
| ≥ 5 years | 0.08 (−0.02, 0.18) | |||
| Occupation | Other | Ref | ||
| Manufacturing Industry | −0.01 (−0.12, 0.11) | |||
| Service Industry | −0.02 (−0.10, 0.06) | |||
Multivariate analysis of social integration and primary care satisfaction.
*p < 0.05, **p < 0.01, ***p < 0.001.
4 Discussion
Our study revealed moderate satisfaction with primary care, but insufficient community integration among migrant populations in Guangzhou. Meanwhile, both community integration and district-level economic development significantly influenced migrants’ satisfaction with primary care.
Our study reported the migrant population’s satisfaction with primary care score of 3·29 ± 0·76 out of 5, indicating a moderate level. This finding aligns with other research in the Greater Bay Area. For instance, Huo assessed the primary care experiences of migrants in the Guangdong-Hong Kong-Macao Greater Bay Area using the Primary Care Assessment Tools (PCAT), reporting an average score of 3.12 ± 0·02 out of 4. Among subdomains, scores for first-contact care in terms of access and ongoing care were lowest, at 2.89 and 2.98 respectively, reflecting migrants’ limited recognition of core primary care attributes such as accessibility and continuity of care (29). International migration studies similarly identify access to care as a major barrier, contributing to migrants’ lower primary care satisfaction compared to native populations (30–32). This study also found that positive social integration significantly influences migrants’ satisfaction with primary healthcare, suggesting that enhancing social integration may help overcome access barriers and improve satisfaction with primary care.
We also found that community integration among migrants in Guangzhou is generally low, with over 80% reporting little or no participation in community activities. This low engagement poses a significant barrier to both community integration and access to primary care. Several factors may contribute to this phenomenon. Occupational segregation may diminish migrants’ sense of identity, as their social networks often remain confined within their professional circles, limiting interaction with local residents and reducing involvement in community activities (33). Long working hours and demanding jobs leave migrants with insufficient time and energy to participate. Third, community activities tend to cater predominantly to local residents’ interests-such as older adult dance groups or cultural lectures-while neglecting migrants’ needs, including vocational training or cross-regional social events (34). Moreover, activities are frequently scheduled during weekday daytime hours, conflicting with migrants’ work schedules. The information dissemination is often inefficient; reliance on traditional methods like community bulletin boards, combined with migrants’ limited access to local communication channels, restricts timely awareness of available activities (35). Addressing these barriers is essential to enhance migrants’ community participation and, consequently, their social integration and access to primary care.
Migrants in Guangzhou who participate in community activities report higher satisfaction with community health services, consistent with the findings of Feng et al. (36). Participation in community activities provides migrants with direct exposure to community health services and more comprehensive, tangible information about these services. In China, coordinated efforts among primary healthcare institutions, grassroots government agencies (such as subdistrict offices and neighborhood committees), and social organizations promote health education through distributing health materials, setting up information boards, and disseminating disease prevention knowledge. Health promotion activities, including free clinics and health lectures, further facilitate migrants’ engagement with primary care, thereby enhancing their awareness and satisfaction (37).
Our study found that migrants with more frequent neighborhood interactions reported higher satisfaction with primary healthcare, consistent with the findings of Kong et al. (38). The reasons for limited neighborhood interaction in Guangzhou are multifaceted. The significant spatial separation between residential and work areas results in low overlap in daily life trajectories, hindering the formation of intertwined social networks and depriving migrants of natural opportunities and social ties to engage in community activities (35). Many low-income migrants cluster in urban villages or peripheral communities, creating physical segregation from local residents and limiting cross-network interactions (39). Third, unique linguistic and cultural barriers in Guangdong-such as the Cantonese dialect-impede migrants’ integration into local social settings, while differences in traditional festivals may further contribute to cultural alienation (40). These factors underscore the need for grassroots governance in Guangzhou to actively create opportunities for neighborhood interaction, as increased resident engagement fosters mutual understanding and trust, thereby enhancing utilization and satisfaction with community health services (36, 41).
It is also found that fewer than one-third of migrants expressed a strong willingness to seek help from grassroots government agencies (including subdistrict offices or neighborhood committees) when facing difficulties. This low help-seeking intention may stem from migrants’ limited familiarity with urban community participation and assistance mechanisms, placing them at a disadvantage in accessing community service resources and leading them to either forgo help or seek alternative channels (42, 43). Meanwhile, data indicate that a higher willingness to seek help from grassroots government agencies significantly improves migrants’ satisfaction with primary care services. This may be because migrants who are willing to seek help have established stronger social ties and trust with local government, thereby enhancing their recognition of primary care (44). Migrants’ social networks are typically confined to their residential communities, and their willingness to seek help reflects a high dependence on community governance and service institutions, underscoring the critical role of grassroots government in delivering essential public health products and services (45). Therefore, it is recommended that grassroots government address the current lack of dedicated public welfare or volunteer groups serving migrants, which limits the provision of public services and support (24).
The migrants living in economically better-off districts reported higher satisfaction with primary care compared to those in less developed regions. This finding confirms our hypothesis that districts with better economic development can offer more fiscal directions and allocate more resources to healthcare services and community activities, whereas economically disadvantaged areas may face constraints due to limited fiscal revenue (46). Similar findings have been reported internationally, where migrants in high-income countries tend to express higher satisfaction with public health services (47). Interestingly, we also observed that migrants in districts with better economic level exhibited lower levels of neighborhood interaction, community participation, and willingness to seek assistance from grassroots government. This suggests an inverse relationship between district economic development and migrants’ willingness to integrate into community integration in Guangzhou. Therefore, it is advisable for local authorities in Guangzhou to integrate community integration initiatives with primary care and other public services, promoting coordinated implementation (48).
Furthermore, our findings indicate that female migrants and those with middle-level income reported significantly lower satisfaction with primary care. This underscores the need for policymakers to pay closer attention to the specific service needs and quality preferences of these subgroups and to provide targeted support and interventions accordingly (49, 50).
5 Conclusion
This study investigated the satisfaction of migrant populations in Guangzhou with primary healthcare and examined the relationships between social integration, regional economic development, and community health services. The findings indicate that migrants’ satisfaction with community health services is moderate. Both community integration and the level of district economic development positively influence migrants’ satisfaction with primary care. Therefore, we recommend that all levels of government in Guangzhou not only strengthen the infrastructure of public services but also focus on the channels and programs for enhancing community integration. Encouraging migrants to engage in public activities through community platforms can effectively promote the utilization of community health services.
6 Limitations
First, due to constraints in time and funding, this study collected data solely from Guangzhou, limiting regional representativeness. Future research should expand the geographic scope to enhance generalizability. Second, as this study employed a cross-sectional design, causal relationships cannot be established. Third, objective health indicators such as physical examination results and blood test data were not included due to data collection limitations. Future studies should consider the role of disease severity and overall health status in mediating the relationship between social integration and satisfaction with primary healthcare. Fourth, it is important to note that treatment burden is a critical factor affecting patients’ access to primary care; however, this study did not address this aspect. Subsequent research should comprehensively incorporate treatment burden alongside other factors to better elucidate the multifaceted determinants of primary care accessibility and utilization, thereby providing a more complete understanding of the issue.
Statements
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Ethical approval was not required for the studies involving humans because in accordance with regulations, this study is categorized as a routine project with minimal ethical risk. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
YX: Conceptualization, Data curation, Investigation, Methodology, Writing – original draft, Writing – review & editing. SZ: Conceptualization, Investigation, Methodology, Validation, Writing – review & editing. LC: Data curation, Formal analysis, Supervision, Writing – review & editing. DX: Formal analysis, Methodology, Supervision, Writing – review & editing. WH: Investigation, Validation, Writing – review & editing. SW: Project administration, Resources, Validation, Writing – review & editing. LZ: Conceptualization, Formal analysis, Project administration, Resources, Writing – original draft.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The project has received support from Plan on Enhancing Scientific Research in Guangzhou Medical University (Grant#2024-SRP-223), the Teaching Quality of higher education and teaching reform project in Guangzhou (Grant#2024-YLKC-016) and the Development Planning of philosophy and social sciences project in Guangzhou (Grant#2023-GZQN-73), Guangdong Provincial Medical Research Fund Directive Project: Study on the Provision and Quality Supervision Assessment of Tertiary Rehabilitation Services for Stroke in Guangdong Province (Grant#2 C2023058) and Guangdong Provincial Medical Research Fund Directive Project: Exploratory Study on Enhancing the Public Health Emergency Management Service Capacity of Primary Healthcare Institutions” (Grant#C2020061).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1604736/full#supplementary-material
References
1.
Francisco Rossetti A Obelleiro Nadal S de Quijano G Miceli F Garcia-Gozalbes J Jiménez Lozano AI et al . Syndromic approach in migrant patients: fever, diarrhea, anemia, eosinophilia and chronic cough. Aten Primaria. (2024) 56:102924. doi: 10.1016/j.aprim.2024.102924
2.
Acquadro-Pacera G Valente M Facci G Kiros BM Corte FD Barone-Adesi F et al . Exploring differences in the utilization of the emergency department between migrant and non-migrant populations: a systematic review. BMC Public Health. (2024) 24:1–16. doi: 10.1186/s12889-024-18472-3
3.
World Health Organization. Report of the international conference on primary health care [internet]. USSR; (1978). Available online at:https://www.who.int/publications/i/item/9241800011.
4.
World-health organization . Refugee and migrant health. (2024). Available online at:https://www.who.int/news-room/fact-sheets/detail/refugee-and-migrant-health.
5.
Bu X Wang T Dong Q Liu C . Heterogeneity in public health service utilization and its relationship with social integration among older adult migrants in China: a latent class analysis. Front Public Health. (2024) 12:12. doi: 10.3389/fpubh.2024.1413772
6.
Jing Z Zhang S Zhang N Sun M Zhou C . The effect of parental social integration on the physical examination utilization for young migrant children: a national cross-sectional study in China. Front Public Health. (2022) 9:755726. doi: 10.3389/fpubh.2021.755726
7.
Xiaoyu L . Empirical research on the influence of community public health service on social integration of floating elderly population based on propensity score matching. Chin Health Serv Manag. (2023) 40:408–12.
8.
Li Z Hung P He R Zhang L . Association between direct government subsidies and service scope of primary care facilities: a cross-sectional study in China. Int J Equity Health. (2020) 19:135. doi: 10.1186/s12939-020-01248-7
9.
Li X-x . A preliminary discussion about the influences of regional economic development on the migration of population. China Bus Mark. (2013) 27:58–64. doi: 10.14089/j.cnki.cn11-3664/f.2013.12.006
10.
Tang L . The Chinese community patient’s life satisfaction, assessment of community medical service, and trust in community health delivery system. Health Qual Life Outcomes. (2013) 11:18. doi: 10.1186/1477-7525-11-18
11.
Ma L Cheng L He Y . Survey on community residents’ satisfaction with community health services and analysis of influencing factors in Jiaodaokou area. Nanjing Rehabilitation Medical Association: Beijing City (2024).
12.
Radwan NM Alkattan AN Haji AM Alabdulkareem KI . Evaluation of levels and determinants of patient satisfaction with primary health care services in Saudi Arabia: a systematic review and meta-analysis. Dr Sulaiman Al Habib Med J. (2023) 5:128–37. doi: 10.1007/s44229-023-00039-w
13.
Ming T . Local factors effects on the urban integration for the floating population. Geogr Sci. (2017) 37:997–1005. doi: 10.13249/j.cnki.sgs.2017.07.004
14.
Alotaibi M Alazemi T Alazemi F Bakir Y . Patient satisfaction with primary health-care services in Kuwait. Int J Nurs Pract. (2015) 21:249–57. doi: 10.1111/ijn.12257
15.
Guohui Wen . Report on the work of Guangzhou municipal government in 2020 [internet]. Guangzhou Munic. Peoples Gov. Off. (2020). Available online at:https://www.gz.gov.cn/zwgk/zjgb/zfgzbg/content/post_5894347.html.
16.
Liu X Yang F Wang X Huang N Cheng T Guo J . Related factors and equity of health status among floating population in China based on geographic information system analysis. Beijing Da Xue Xue Bao. (2024) 56:223–9. doi: 10.19723/j.issn.1671-167X.2024.02.004
17.
The Standing Committee of Guangdong Provincial People’s Congress . Regulations on the Service Management of Migrant Populations in Guangdong Province 2019 [internet]. (2019). Available online at:https://www.gd.gov.cn/zwgk/wjk/zcfgk/content/post_2726812.html.
18.
Health Commission of Guangdong Province . Implementation plan for health education and promotion actions for the floating population in Guangdong Province. (2016). Available online at:https://wsjkw.gd.gov.cn/zwgk_gsgg/content/post_1946009.html
19.
Tu C He J Tan Y Wang F . Analysis and forecast on social situation of Guangzhou in China, vol. 2021. Beijing: Social Sciences Academic Press (2021).
20.
Zheng W He F . Sample size estimate for cross-sectional study. Prev Med. (2020) 32:647–8. doi: 10.19485/j.cnki.issn2096-5087.2020.06.028
21.
The Central Committee of the Communist Party of China , The state Counci. National new-type Urbanization Plan (2014–2020). (2014). Available online at:https://www.gov.cn/gongbao/content/2014/content_2644805.htm.
22.
Juhua Y . Economic Integration of Internal Migrants in China. Beijing:Social sciences academic press. (2013) 61–79:203–4.
23.
Xiaozhuang L . The practice mode and policy analysis of social integration of floating population in China. J Natl Sch Adm. (2017) 110-115:148. doi: 10.14063/j.cnki.1008-9314.2017.04.018
24.
Yang C Xu H . Direct and spillover effects: how do community-based organizations impact the social integration of passive migrants?Sustain For. (2024) 16:4530. doi: 10.3390/su16114530
25.
Elisa R . Sources of negative attitudes toward immigrants in europe: a multi-level analysis 1. Int Migr Rev IMR. (2010) 44:53–77. doi: 10.1111/j.1747-7379.2009.00798.x
26.
Forrest R Kearns A . Social cohesion, social capital and the neighbourhood. Urban Stud. (2001) 38:2125–43. doi: 10.1080/00420980120087081
27.
Zhang Y You C Pundir P Meijering L . Migrants’ community participation and social integration in urban areas: a scoping review. Cities. (2023) 141:104447. doi: 10.1016/j.cities.2023.104447
28.
Yang X Jin X Xiao Q Bai M . Situation and policy study on rural migrant workers’ social support and social integration: a case of Shenzhen. China Soft Sci. (2007) 12:18–26.
29.
Kjøllesdal M Indseth T Iversen HH Bjertnaes O . Patient experiences with general practice in Norway: a comparison of immigrant groups and the majority population following a national survey. BMC Health Serv Res. (2020) 20:1106. doi: 10.1186/s12913-020-05963-3
30.
Zeng J Shi L Zou X Chen W Ling L . Rural-to-urban migrants’ experiences with primary care under different types of medical institutions in Guangzhou. China PLOS ONE. (2015) 10:e0140922. doi: 10.1371/journal.pone.0140922
31.
Kieseppä V García Velázquez R Vehko T Kuusio H . Satisfaction with access to health services among foreign-born population in Finland: a survey-based study. BMC Health Serv Res. (2022) 22:781. doi: 10.1186/s12913-022-08155-3
32.
Yelland J Riggs E Small R Brown S . Maternity services are not meeting the needs of immigrant women of non-English speaking background: results of two consecutive australian population based studies. Midwifery. (2015) 31:664–70. doi: 10.1016/j.midw.2015.03.001
33.
Yue Z Fong E Yuan Y Li S . Life satisfaction and internal migration experience: migrant workers in Guangzhou, China. Asian Popul Stud. (2019) 15:302–18. doi: 10.1080/17441730.2019.1664525
34.
Yufeng Z Hu X . Ethnic differences in social participation of migrants: an empirical study based on China migrants dynamic survey in 2014. Northwest Popul J.. (2019) 40:25–35. doi: 10.15884/j.cnki.issn.1007-0672.2019.02.003
35.
Zhou C Zhan M An X Huang X . Social inclusion concerning migrants in Guangzhou City and the spatial differentiation. Sustain For. (2022) 14:48. doi: 10.3390/su142315548
36.
Ruan Y Wang D Li D . Influence of neighborhood-based identity and social participation on the social integration of the drifting elderly. Health Soc Care Community. (2023) 2023:1–11. doi: 10.1155/2023/2101202
37.
Hou Z Lin S Zhang D . Social capital, neighbourhood characteristics and utilisation of local public health services among domestic migrants in China: a cross-sectional study. BMJ Open. (2017) 7:e014224. doi: 10.1136/bmjopen-2016-014224
38.
Kong D Shi C . Sensation and cognition: the paradox logic between economic development and public service satisfaction. J Shanghai Adm Inst. (2020) 21:46–58.
39.
Jin X Ren T Mao N Chen L . To stay or to leave? Migrant workers’ decisions during urban village redevelopment in Hangzhou, China. Front Public Health. (2021) 9:782251. doi: 10.3389/fpubh.2021.782251
40.
Guo S Zhang J . Language, work, and learning: exploring the urban experience of ethnic migrant workers in China. Diaspora Indig Minor Educ. (2010) 4:47–63. doi: 10.1080/15595690903442330
41.
Zhou X Wang T Huang S . Analysis on the Operation Efficiency of Community Health Service System Based on Ultra-efficient DEA Model in Hunan Province. Chin Health Econ. (2013) 32:74–77.
42.
Moore J . Postmigration living difficulties, help-seeking and community resilience in the initial stages of migration: coproducing community practice with recent irish migrants to London. J Community Pract. (2018) 26:125–42. doi: 10.1080/10705422.2018.1450319
43.
McCann TV Mugavin J Renzaho A Lubman DI . Sub-saharan african migrant youths’ help-seeking barriers and facilitators for mental health and substance use problems: a qualitative study. BMC Psychiatry. (2016) 16:275. doi: 10.1186/s12888-016-0984-5
44.
Wangwang LI Shuaishuai F . Social service satisfaction of community residents and its normalization path from the perspective of population mobility. J Hebei Univ Soc Sci. (2022) 47:128. doi: 10.3969/j.issn.1005-6378.2022.05.015
45.
Liu S Qin B Wang D . How does social integration work when older migrants obtain health services from community? Evidence from national database in China. Front Public Health. (2023) 11:1283891. doi: 10.3389/fpubh.2023.1283891
46.
Jiali YU Shangguang YANG Zhiwang QIAN . Fiscal decentralization system and the efficiency of local fiscal expenditure on health care. J Beijing Inst Technol Soc Sci Ed. (2023) 25:172–88. doi: 10.15918/j.jbitss1009-3370.2023.2939
47.
Panagiotopoulos C Apostolou M Zachariades A . Assessing migrants’ satisfaction from health care services in Cyprus: a nationwide study. Int J Migr Health Soc Care. (2020) 16:108–18. doi: 10.1108/IJMHSC-10-2016-0037
48.
Kısar KE . The spatial context of social integration. Soc Indic Res. (2014) 119:49–71. doi: 10.1007/s11205-013-0481-x
49.
Krupic F Sadic S Fatahi N . Contact with health-care service expectation and reality of situation experienced by immigrants seeking swedish health-care. Mater Socio Medica. (2016) 28:141–5. doi: 10.5455/msm.2016.28.141-145
50.
Khalid H Anis MS Rizal AM . Middle eastern immigrants’ satisfaction with malaysian healthcare. Bus Manag Strategy. (2021) 12:238–68. doi: 10.5296/bms.v12i2.19103
Summary
Keywords
migrant population, primary care, satisfaction, social integration, economic level
Citation
Xiao Y, Zhong S, Chen L, Xiao D, Huang W, Wu S and Zhang L (2025) Community integration enhances migrants’ satisfaction with primary care across districts with varying economic levels: survey evidence from Guangzhou, China. Front. Public Health 13:1604736. doi: 10.3389/fpubh.2025.1604736
Received
02 April 2025
Accepted
28 May 2025
Published
11 June 2025
Volume
13 - 2025
Edited by
Lei Si, Western Sydney University, Australia
Reviewed by
Harry H. X. Wang, Sun Yat-sen University, China
Xiaoying Zhu, The University of Melbourne, Australia
Updates
Copyright
© 2025 Xiao, Zhong, Chen, Xiao, Huang, Wu and Zhang.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luwen Zhang, 067094@smu.edu.cn
†These authors have contributed equally to this work
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.