 Katherine Simbaña-Rivera1,2,3*†
Katherine Simbaña-Rivera1,2,3*† Jesús Endara-Mina3†
Jesús Endara-Mina3† Damary S. Jaramillo-Aguilar3†
Damary S. Jaramillo-Aguilar3† Leonardo D. Mera-Lojano3†
Leonardo D. Mera-Lojano3† Ruth Jimbo-Sotomayor2,3
Ruth Jimbo-Sotomayor2,3 Xavier Sánchez2,3María Cristo Rodríguez-Pérez4Manuel Enrique Fuentes-Ferrer4,5
Xavier Sánchez2,3María Cristo Rodríguez-Pérez4Manuel Enrique Fuentes-Ferrer4,5 Luis D. Boada1
Luis D. Boada1- 1Toxicology Unit, Research Institute of Biomedical and Health Sciences (IUIBS), University of Las Palmas de Gran Canaria (ULPGC), Las Palmas de Gran Canaria, Spain
- 2Centro de Investigación para la Salud en América Latina (CISeAL), Facultad de Medicina, Pontificia Universidad Católica del Ecuador (PUCE), Quito, Ecuador
- 3ECUAVOLCAN Research Group, Faculty of Medicine, Pontificia Universidad Católica del Ecuador (PUCE), Quito, Ecuador
- 4Canary Health Service, Research Unit, University Hospital Nuestra Señora de Candelaria and Primary Care Authority of Tenerife, Santa Cruz de Tenerife, Spain
- 5Preventive Medicine Department, University Hospital Nuestra Señora de Candelaria, Canary Health Service, Santa Cruz de Tenerife, Spain
Background: Volcanic eruptions pose substantial health risks to populations living in proximity to active volcanoes, impacting respiratory, cardiovascular, ocular, dermatological, and mental health systems. With a growing number of people globally exposed to volcanic activity, there is a critical need for an interdisciplinary understanding of these health consequences, particularly concerning their pathophysiological mechanisms, epidemiological patterns, and public health implications.
Methods: This scoping review systematically synthesized evidence from studies conducted near 27 volcanoes across diverse geographic regions. The analysis integrated clinical, epidemiological, and public health perspectives to characterize health outcomes and associated risk factors, including geographic location, eruption magnitude, and type of exposure. A novel schematic framework was developed to map pathophysiological mechanisms across multiple organ systems.
Findings: The results indicate that volcanic emissions—such as sulphur dioxide, fine tephra, and volcanic ash—exacerbate pre-existing conditions and contribute to increased morbidity. The most frequently reported health outcomes included acute respiratory symptoms, conjunctivitis, dermatitis, hypertension, and post-traumatic stress disorder. Variability in health impacts was observed across sex, age, and region, with vulnerable groups such as children and older adults disproportionately affected. Chronic exposure was associated with persistent health issues, revealing critical gaps in long-term health surveillance and intervention strategies.
Conclusion: This scoping review highlights the multifaceted health impacts of volcanic eruptions, emphasizing the complex interactions between volcanic emissions and human health. The findings underscore the need for tailored public health interventions, proactive education, and further research to strengthen preparedness and resilience in exposed communities.
1 Introduction
Volcanic activity poses substantial public health risks for populations residing in proximity to active or potentially active volcanoes. Globally, there are approximately 1,500 potentially active volcanoes, of which more than 550 have erupted in the past century (1). A significant concentration—over 75%—is distributed along the Pacific Ring of Fire, which spans densely populated regions of Asia and the Americas. Countries such as Indonesia, Japan, the United States, Russia, Chile, and the Philippines account for the highest number of active volcanoes (2).
While volcanoes such as Colima (Mexico), Mount Etna (Italy) (1), and Dukono (Indonesia) are often cited due to frequent activity, other volcanoes—Fuego (Guatemala), Popocatépetl (Mexico), Tungurahua (Ecuador), and Merapi (Indonesia)—have generated eruptions with greater explosivity and more pronounced health and social consequences (3).
The term “volcanic products” refers to a complex mixture of solid, liquid, and gaseous materials expelled during both eruptive and non-eruptive phases. These include primary emissions such as tephra (ash, lapilli, and blocks), pyroclastic flows, lava, and gas plumes composed of sulfur dioxide (SO₂), hydrogen sulfide (H₂S), carbon dioxide (CO₂), hydrochloric acid (HCl), and hydrofluoric acid (HF), among others (4). Chronic emissions during quiescent periods—such as diffuse degassing of CO₂ or radon (222Rn)—also pose long-term environmental and health risks (5, 6). The physical and chemical composition of these products, as well as particle size and solubility, critically determine their toxicological profile, and biological uptake. Marine and subaerial volcanoes differ significantly in their emission profiles. Submarine systems, for instance, have been shown to release higher quantities of metal pollutants such as lead, selenium, and mercury due to increased magmatic volatility under hydrostatic pressure (7). These pollutants may bioaccumulate in food chains or contaminate water sources, with repercussions on human health.
Beyond these geophysical drivers, global challenges amplify health risk. Intensifying extreme-weather regimes associated with climate change are expected to modulate secondary volcanic hazards (e.g., rainfall-triggered lahars and ash remobilization), increasing exposure in already vulnerable settlements (8). Social determinants—including rapid, unplanned urban growth, poverty, and low educational attainment—constrain household and system-level preparedness, while gaps in land-use regulation and enforcement allow expansion into high-hazard zones, compounding risk (9).
Between 1,500 and 2017, volcanic activity caused over 278,000 deaths and affected more than 800 million individuals living within 100 km of volcanic centers (10, 11). Epidemiological studies highlight both acute and chronic health outcomes related to exposure. However, few reviews have synthesized this evidence in an integrated, system-based manner. Existing efforts, including foundational work by the International Volcanic Health Hazard Network (IVHHN), have primarily addressed specific health outcomes or isolated events (12).
This scoping review aims to comprehensively assess the health impacts of volcanic activity across five major systems—respiratory, cardiovascular, ocular, dermatological, and mental—focusing on studies involving human populations exposed during both eruptive and non-eruptive periods. Special emphasis is placed on the chemical and physical properties of volcanic products, exposure types, eruption magnitude, and geographic context. By integrating clinical, epidemiological, and environmental health perspectives, this review provides an updated synthesis to inform public health policies, risk mitigation strategies, and future interdisciplinary research.
2 Methods
2.1 Review design
This review was conducted using the scoping review methodological framework proposed by Arksey and O’Malley (13) and further developed by the Joanna Briggs Institute (JBI) (14). The study protocol was developed in accordance with the PRISMA Extension for Scoping Reviews (PRISMA-ScR) (Supplementary Table 1) (15).
2.2 Eligibility criteria
We included peer-reviewed articles assessing the impact of volcanic activity on human health, irrespective of study design (e.g., cross-sectional, cohort, case–control, case reports, ecological studies, and both systematic and non-systematic literature reviews). The inclusion of reviews was justified by the global scope of this study, aimed at comprehensively synthesizing all existing evidence on the health effects of volcanic activity. Studies were selected based on a modified PICO framework (16): Population (P) included individuals or communities residing in volcanic areas; Intervention/Exposure (I) encompassed direct or indirect exposure to volcanic products such as lava, ash, gases, aerosols, and contaminated water; Comparison (C) was not explicitly required given the descriptive nature of the synthesis; Outcomes (O) focused on health effects including respiratory, cardiovascular, dermatological, ocular, and mental health impacts. We excluded studies with unclear exposure descriptions, animal or in vitro studies, opinion pieces, and editorials.
2.3 Information sources and search strategy
A comprehensive search was conducted in PubMed, MEDLINE, Web of Science, Scopus, Virtual Health Library, Medes, and the British Library database up to August 3, 2023. No language or publication date restrictions were applied. Search terms included combinations of keywords and MeSH terms related to volcanic activity (e.g., “volcanic eruption,” “volcanic gas,” “volcanic ash”) and health outcomes (e.g., “respiratory diseases,” “cardiovascular,” “dermatologic,” “ocular,” “mental health”). The full search strategy is detailed in Supplementary Table 2.
2.4 Study selection and data extraction
Articles were screened independently by two reviewers using Rayyan software (www.rayyan.ai). Duplicate records were identified and removed prior to the screening process. Discrepancies were resolved by consensus. A data extraction form was developed and pilot-tested, collecting information on study location, volcano characteristics, eruption type (eruptive or non-eruptive), exposure type (acute or chronic), volcanic products involved (ash, gases, etc.), population characteristics, health outcomes, and study design. Some studies addressed more than one PICO element simultaneously, reflecting multiple exposures and outcomes. These were classified as multicriteria studies by consensus between the reviewers. This classification also included systematic and non-systematic literature reviews, along with a subset of original studies that met multiple PICO criteria, ensuring consistent categorization across heterogeneous sources.
2.5 Data analysis
Studies were grouped by health systems affected: respiratory, cardiovascular, ocular, dermatological, and mental health. Data were summarized in tables using Microsoft Excel, documenting eruption year, volcano, country, authors, publication date, objectives, study type, statistical methods, population characteristics, results, pathophysiological causes, and public health implications (Supplementary Table 3). Three team members (J. E. M., D. S. J. A., L. D. M. L.) performed initial filtering and compilation, followed by review and evaluation by two additional members (K. S. R., L. D. B.). Cross-checking and discussions ensured accuracy and relevance (K. S. R., X. S., R. J. S).
Frequencies and percentages were used to describe study characteristics globally; multicriteria studies were counted as single units to avoid overrepresentation in distribution analyses by country and continent. Indeed, to avoid overestimation, the findings reported in systematic and non-systematic reviews (n = 11) were not incorporated into the descriptive statistical calculations. For individual disease categories, aggregate proportions were analyzed alongside median, minimum, and maximum values. The mechanistic elements illustrated in the figures were directly extracted from the included source studies, which reported these pathways in association with exposure metrics and clinical outcomes. Visual representations of health effects were developed by the authors using BioRender (www.biorender.com).
2.6 Quality appraisal and risk of bias assessment
A risk of bias assessment was conducted as per PRISMA-ScR guidelines (15). However, no articles were excluded due to bias, as this is not mandatory in scoping reviews, the appraisal aimed to systematically map existing research in the field.
3 Results
The database search yielded a total of 2,077 records. After the removal of duplicates, 1,627 articles remained for title and abstract screening. This process led to the full-text assessment of 173 studies, with 83 ultimately meeting the inclusion criteria (Figure 1). Articles addressing more than one PICO criterion were classified as multicriteria studies, following consensus among reviewers. The most common reasons for exclusion included inadequate description of exposure, irrelevant outcomes, or unclear study design.
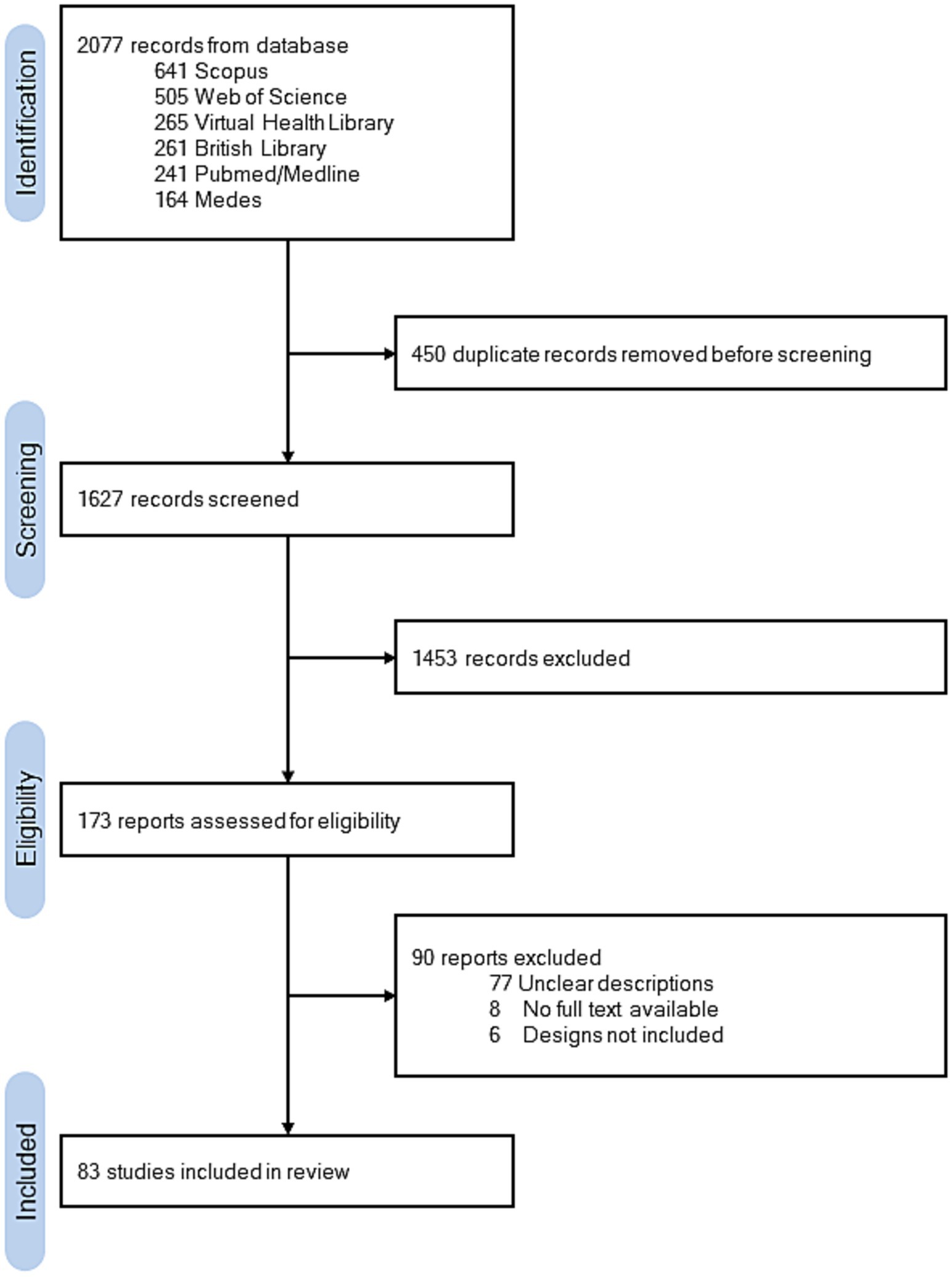
Figure 1. PRISMA flow diagram of the study selection process.
Geographically, 16 studies (22.22%) were conducted in the United States, followed by Japan with 15 studies (20.83%), and Iceland with 9 studies (12.5%). A total of 27 volcanoes were represented in the literature, with Mount St. Helens (n = 8; 11.11%), Kīlauea Volcano (n = 7; 9.72%), Eyjafjallajökull Volcano (n = 6; 8.33%), and Miyakejima Volcano (n = 6; 8.33%) being the most studied (Figure 2). Toxic gases (n = 24; 33.33%) and volcanic ash (n = 21; 29.17%) were the most frequently assessed volcanic products. The majority of studies focused on adult populations (n = 61; 84.72%), with fewer studies investigating children (n = 7; 9.72%).
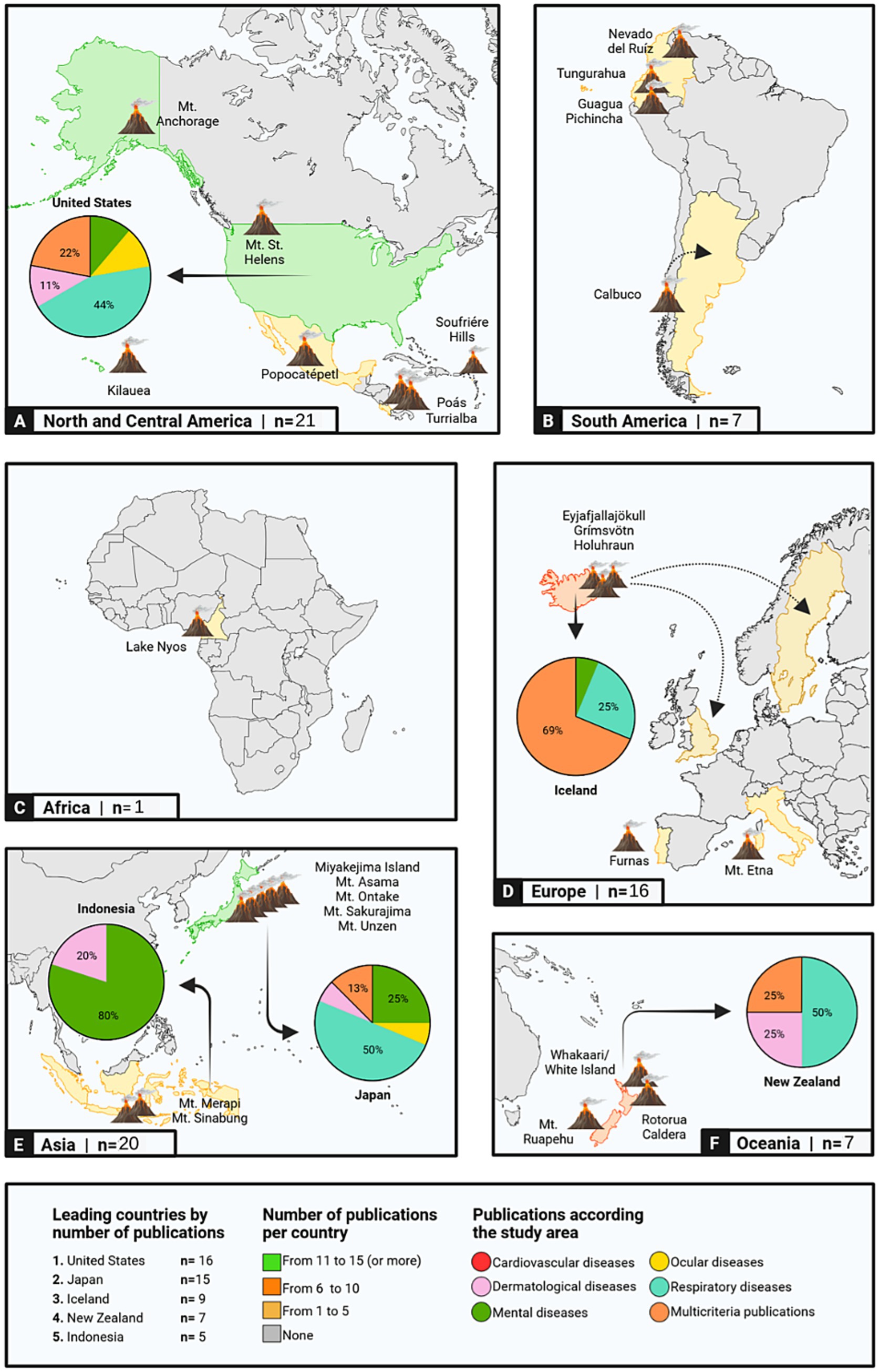
Figure 2. Global geographical distribution of reviewed studies on the health effects of volcanic activity. The figure highlights the number of publications per continent and identifies the top five countries with the highest publication counts within their territories. Pie charts illustrate the percentage distribution of publications across disease categories for each of these top five countries. Additionally, dashed arrows indicate populations affected by eruptions from specific volcanoes and their impact on neighboring nations (This figure was created using Biorender.com).
Notable contributors included Carlsen HK, Longo BM, and Baxter PJ, each authoring four studies (4.82%). Peak publication years were 2019 and 2021, with six studies published in each year (7.23%). The earliest included study dated back to 1982.
Five major health domains were identified across the reviewed literature: respiratory, mental health, ocular, dermatological, and cardiovascular effects. Respiratory diseases were the most frequently reported outcomes (n = 50; 51.55%), followed by mental health disorders (n = 20; 20.62%) and ocular conditions (n = 11; 11.34%). The count of studies by category reflects these multicriteria contributions, thereby ensuring that the synthesis captures the full breadth of volcanic health impacts.
In total, 90 distinct health manifestations were associated with volcanic exposure (Figure 3). Among these, respiratory outcomes comprised 35.56% (n = 32), mental health 23.33% (n = 21), and ocular effects 16.67% (n = 15).
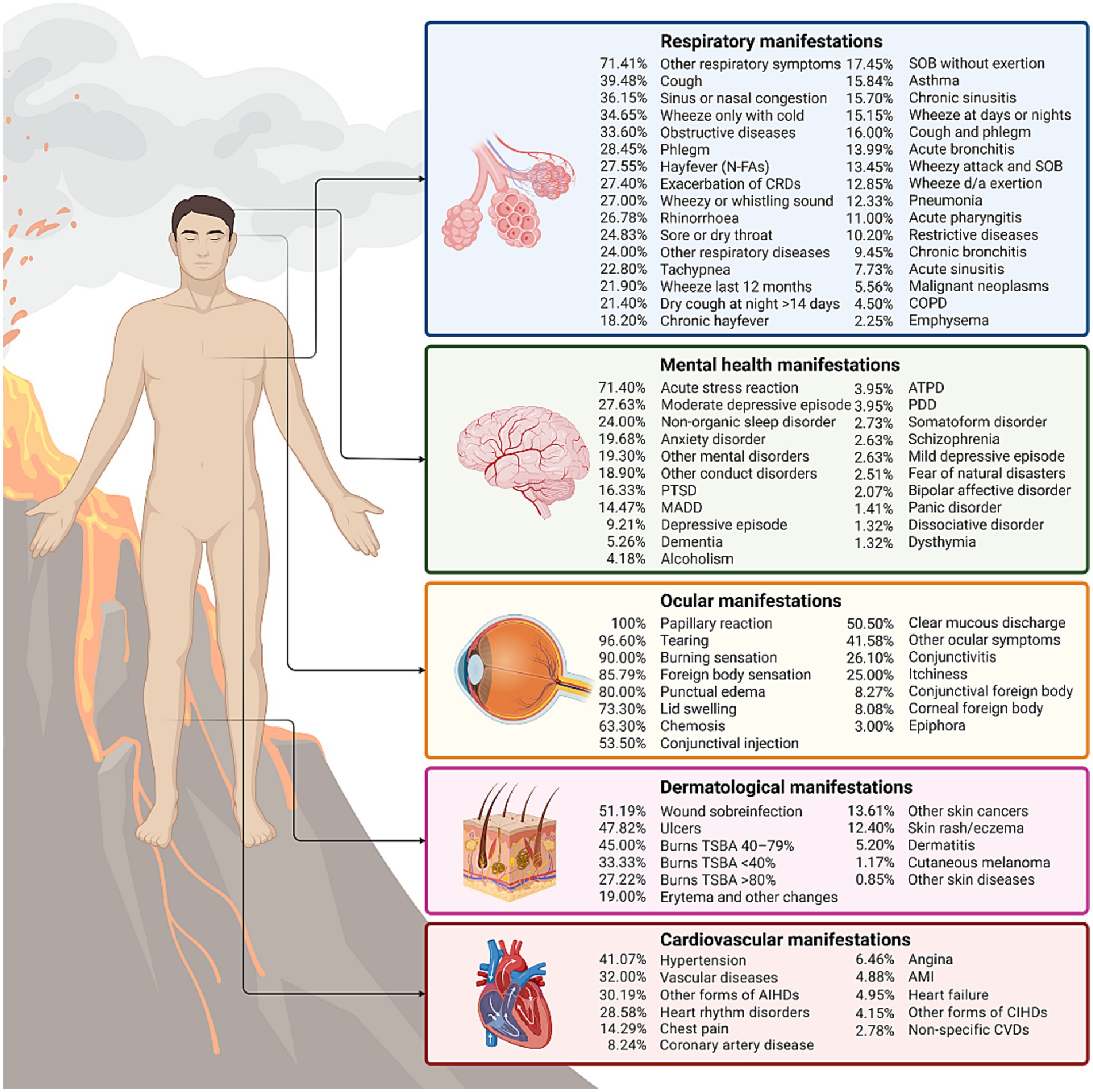
Figure 3. Percentage distribution of multisystemic clinical manifestations associated with volcanic activity exposure, ranked from highest to lowest across each analyzed category. AIHDs, acute ischemic heart diseases; AMI: acute myocardial infarction; ATPD, acute and transient psychotic disorder; CIHDs, chronic ischemic heart diseases; COPD, chronic obstructive pulmonary disease; CRDs, chronic respiratory diseases; d/a, during or after; CVDs: cardiovascular diseases; MADD, mixed anxiety and depression disorder; N-FAs, non-food allergies; PDD, persistent delusional disorder; PTSD, post-traumatic stress disorder; SOB, shortness of breath; TBSA, total body surface area (This figure was created using Biorender.com).
3.1 Respiratory effects
This section presents a synthesis of 50 studies that investigated respiratory outcomes associated with volcanic exposure. Of these, 45 were original epidemiological studies (90%) and five were literature reviews (10%) categorized as multicriteria studies. Volcanoes most frequently studied included Kīlauea (n = 6; 13.33%), Eyjafjallajökull (n = 5; 11.11%), Miyakejima (n = 5; 11.11%), Mount St. Helens (n = 4; 8.89%), Rotorua Caldera (n = 3; 6.67%), Mount Sakurajima (n = 3; 6.67%), and 19 other volcanoes of global relevance.
The reported respiratory effects were linked to both the physicochemical properties of volcanic emissions and the exposure context. Ash particles varied in size, morphology, and composition, including crystalline silica, iron, aluminum, copper, and vanadium. Inhalation exposures also involved toxic gases, including carbon monoxide (CO), carbon dioxide (CO₂), sulfur dioxide (SO₂), hydrogen chloride (HCl), hydrogen sulfide (H₂S), and nitrogen dioxide (NO₂), volatile elemental compounds such as diatomic chlorine (Cl₂), elemental sulfur (S₈), and hot water vapor (H₂O), all of which can be harmful to health at high concentrations (17–22). Particles measuring between 2.5 and 10 μm predominantly affected the upper respiratory tract, whereas fine particles (<2.5 μm) penetrated deeply into alveoli (23–25). Sulfurous gases and acidic aerosols showed significant absorption (40–90%) within upper respiratory mucosa, with remaining fractions reaching distal airways via mucociliary clearance.
Exposure to these substances at elevated concentrations triggered oxidative stress and lipid peroxidation, initiating complex pathophysiological cascades including epithelial injury, deoxyribonucleic acid (DNA) damage, cell apoptosis, immune dysregulation, and neurogenic inflammation. Chronic inflammatory processes and epithelial barrier disruption increased susceptibility to respiratory infections, alterations in pulmonary microbiota, fibrosis, and impaired pulmonary function. Clinical outcomes reported included asthma, chronic obstructive pulmonary disease (COPD), silicosis, pneumoconiosis, and lung cancer (Figure 4) (17, 18, 20, 21, 24–41). Furthermore, respirable volcanic particles crossing the alveolar-capillary barrier may contribute to systemic pathologies such as cardiovascular and cerebrovascular diseases.
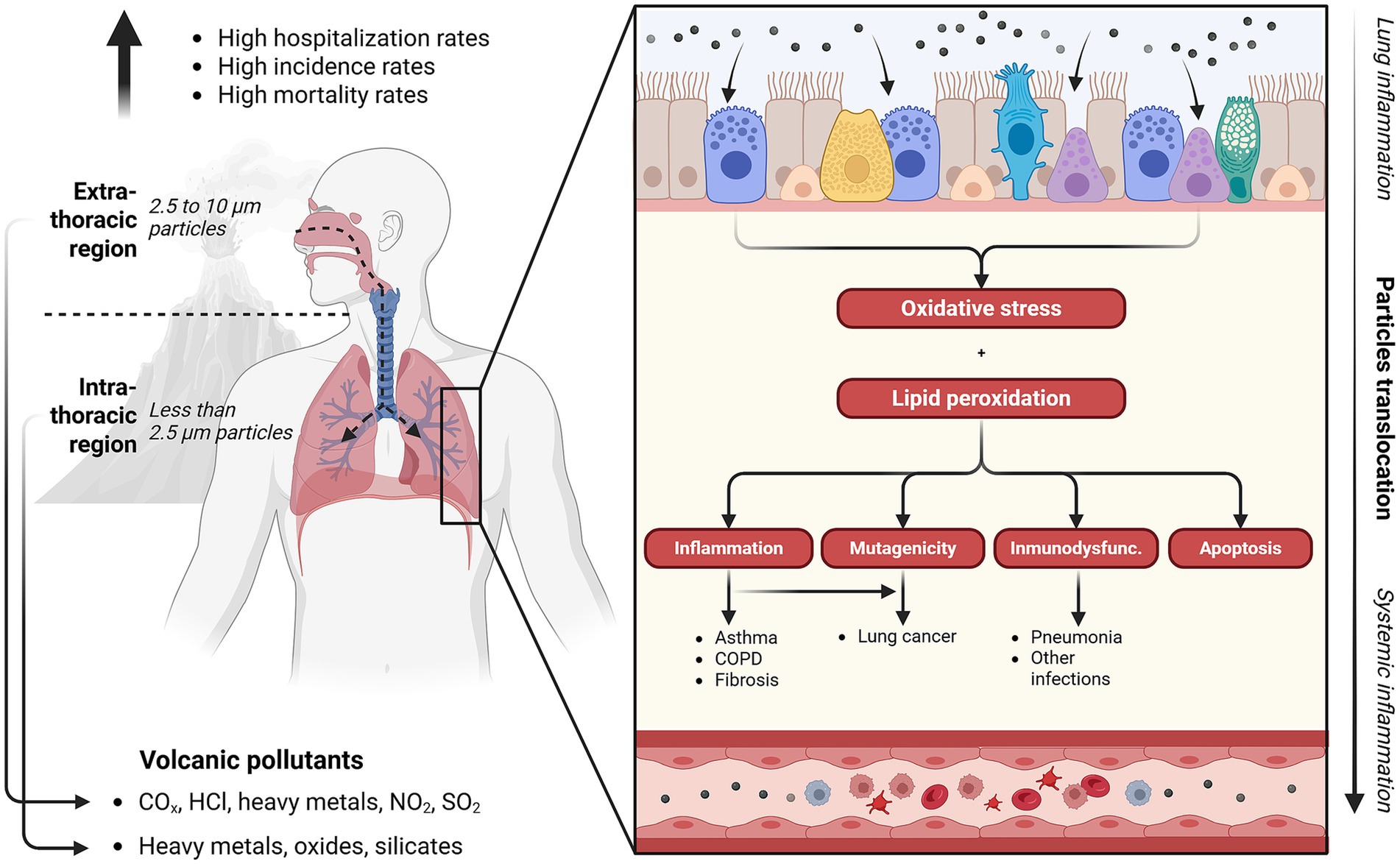
Figure 4. Impact of volcanic activity on respiratory health. COPD, chronic obstructive pulmonary disease; COx, carbon oxides; HCl, hydrochloric acid; immunodysfunc., immunodysfunction; NO2, nitrogen dioxide; SO2, sulfur dioxide; μm, micrometers. (This figure was created using Biorender.com).
Epidemiological data consistently associated acute exposure to volcanic emissions with increased respiratory morbidities, including cough, sputum production, dyspnea, chest tightness, and wheezing (18, 31, 41–44). Elevated emergency visits due to asthma and COPD exacerbations were documented during eruption events (17, 24–26, 32, 35, 36, 38, 42, 43, 45–48). Severe cases, frequently requiring hospitalization or intensive care, predominantly occurred among older adults and individuals with pre-existing cardiorespiratory conditions, occasionally presenting radiologically as bibasilar atelectasis (18, 29, 36, 49).
Acute respiratory events were particularly pronounced shortly after eruptions (20, 25, 26, 32, 50–53), Acute respiratory events were particularly pronounced shortly after eruptions (26). Conversely, pediatric populations displayed increased susceptibility to upper and lower respiratory tract infections, including sinusitis and bronchitis, particularly among children under 15 years (37, 42, 44, 52, 54). Gender-specific trends emerged, with women exhibiting increased vulnerability to chronic bronchitis and pharyngeal irritation (55).
Comparative analyses between exposed and unexposed cohorts consistently revealed higher incidences of chronic respiratory conditions and symptom exacerbations in ash-impacted areas (25, 30, 32, 40, 44, 47). Symptomatic improvement correlated with decreasing pollutant concentrations over time (27, 47, 48, 56, 57). Some studies suggested increased incidence of respiratory tract cancers (28) and elevated overall mortality rates among exposed populations (20, 41, 46, 58, 59).
Certain studies reported contradictory or inconclusive findings, observing minimal or no significant respiratory outcome differences between exposed and control populations, encompassing both adults and children. Investigations conducted before and after high-level SO2 exposure revealed no notable changes in lung function, airway restriction, or inflammatory markers. Such inconsistencies likely reflect methodological limitations, including inadequate sample sizes, short follow-up durations, baseline health disparities, and varying exposure assessments, highlighting the need for more comprehensive, standardized longitudinal studies incorporating detailed biomonitoring (19, 44, 46, 47, 50, 60–66).
3.2 Cardiovascular effects
Five epidemiological studies addressing cardiovascular outcomes were identified, conducted in the United States (n = 1; 20%), Italy (n = 3; 60%), and New Zealand (n = 1; 20%). These studies evaluated the health impacts associated with eruptions from Kīlauea Volcano (1983–ongoing), Mount Etna (2002), Mount Ruapehu (1996), and the Colli Albani volcanic complex (quiescent) (17, 21, 46, 67, 68).
Historically, volcanic eruptions were not perceived to significantly impact cardiovascular health acutely (46). In this review, “acute” refers to exposure occurring within eruptive events, while “chronic” denotes persistent exposure to volcanic degassing emissions or prolonged pollutant presence. Recent evidence, however, highlights that acute exposure to elevated concentrations of volcanic ash exacerbates existing cardiovascular conditions, particularly among older adults (17, 67). Specifically, there were significant increases in exacerbations of circulatory system disorders, ischemic heart disease, and acute myocardial infarction by 18, 31, and 34%, respectively. This exposure also correlated with increased frequency and number of cardiovascular-related hospital visits and admissions (17, 67). For instance, Lombardo et al. (17) reported a 1.3% increase in cardiovascular hospital visits following Mount Etna’s eruption between 2001 and 2002 (17). Moreover, elevated mortality risks from ischemic heart disease and myocardial infarction were documented during volcanic eruption periods; however, the reviewed studies did not statistically quantify the magnitude of this risk (67).
Conversely, chronic exposure to volcanic pollutants could trigger a significantly higher prevalence of these diseases (21, 67). Longo et al. (21) assessed the cardiorespiratory impacts of prolonged SO₂ and sulfate aerosols emitted by Kīlauea Volcano, identifying increased prevalence of cardiovascular conditions such as angina, congestive heart failure, and coronary artery disease, particularly among populations exposed to elevated sulfate aerosol concentrations. Statistically significant increased risks were specifically documented for essential hypertension (OR ranging from 1.7 to 2.0) and abnormal blood pressure readings during clinical assessments. Furthermore, an accelerated increase in resting heart rate (mean increase of 8.50 beats/min) was notably prevalent among exposed individuals over 65, non-smokers, and those not receiving cardiovascular medications (21).
Complementing these findings, Carapezza et al. (68) evaluated chronic exposure to endogenous CO₂-rich and H₂S emissions in a residential area of the Metropolitan City of Rome, reporting increased male cardiovascular mortality (HR 1.60, 95% CI 0.95–2.70) and higher risk of myocardial infarction (HR 2.11, 95% CI 0.91–4.90). Comparable risks were also observed in women, underscoring the long-term cardiovascular burden of non-eruptive degassing scenarios (68).
Figure 5 illustrates the mechanistic pathways linking both short- and long-term exposure to volcanic particulate matter (PM2.5, PM10), toxic volcanic gases (CO2, H2S, SO2), and heavy such as lead (Pb), cadmium (Cd), and arsenic (As) to systemic oxidative stress and chronic inflammation. These pathophysiological processes induce endothelial dysfunction, disrupt autonomic balance, and promote arterial plaque formation, consequently facilitating atherosclerosis development. Additional pathways involve heavy-metal-induced vascular toxicity, resulting in platelet hyperactivation and impaired fibrinolysis. Collectively, these mechanisms amplify risks of developing coronary artery disease, peripheral arterial disease, heart failure, and overall cardiovascular mortality (17, 21, 67).

Figure 5. Effects of volcanic activity on cardiovascular health. PM, particulate matter (This figure was created using Biorender.com).
3.3 Ophthalmological effects
This review identified 11 articles addressing ophthalmological impacts associated with volcanic eruptions. The studied volcanoes included Eyjafjallajökull (n = 2; 18.18%), Kīlauea (n = 2; 18.18%), Miyakejima (n = 1; 9.09%), Mount St. Helens (n = 1; 9.09%), Poás and Turrialba (n = 1; 9.09%), and Sakurajima (n = 1; 9.09%), along with three literature reviews (27.27%) that analyzed multiple volcanic events.
Populations exposed to volcanic fog (vog)—a secondary air pollutant formed when SO2 and other volcanic gases oxidize and react with atmospheric moisture and sunlight—exhibited numerous ocular manifestations. Commonly reported symptoms included conjunctival injection, clear mucous discharge, papillary reactions, punctate epithelial erosions, eyelid edema, and chemosis, each varying in prevalence based on exposure duration and intensity (69). The ocular conditions termed “vog-induced conjunctivitis” result from both irritative and allergic responses (69). Oxidation of SO₂ produces sulfuric acid (H₂SO₄) aerosols and sulfate particulates, which irritate ocular mucosa and sensory nerves, eliciting tearing, hyperemia, and ocular discomfort. Concurrent allergic mechanisms involve histamine release, exacerbating symptoms such as itching, eyelid swelling, and sub-conjunctival fluid accumulation (Figure 6) (20, 69). For instance, a significant prevalence of ocular irritation (69%) was documented among workers exposed to high atmospheric concentrations of SO₂, H₂S, HCl, HF, and nitric acid (HNO₃) from the Poás and Turrialba volcanoes in Costa Rica (70).
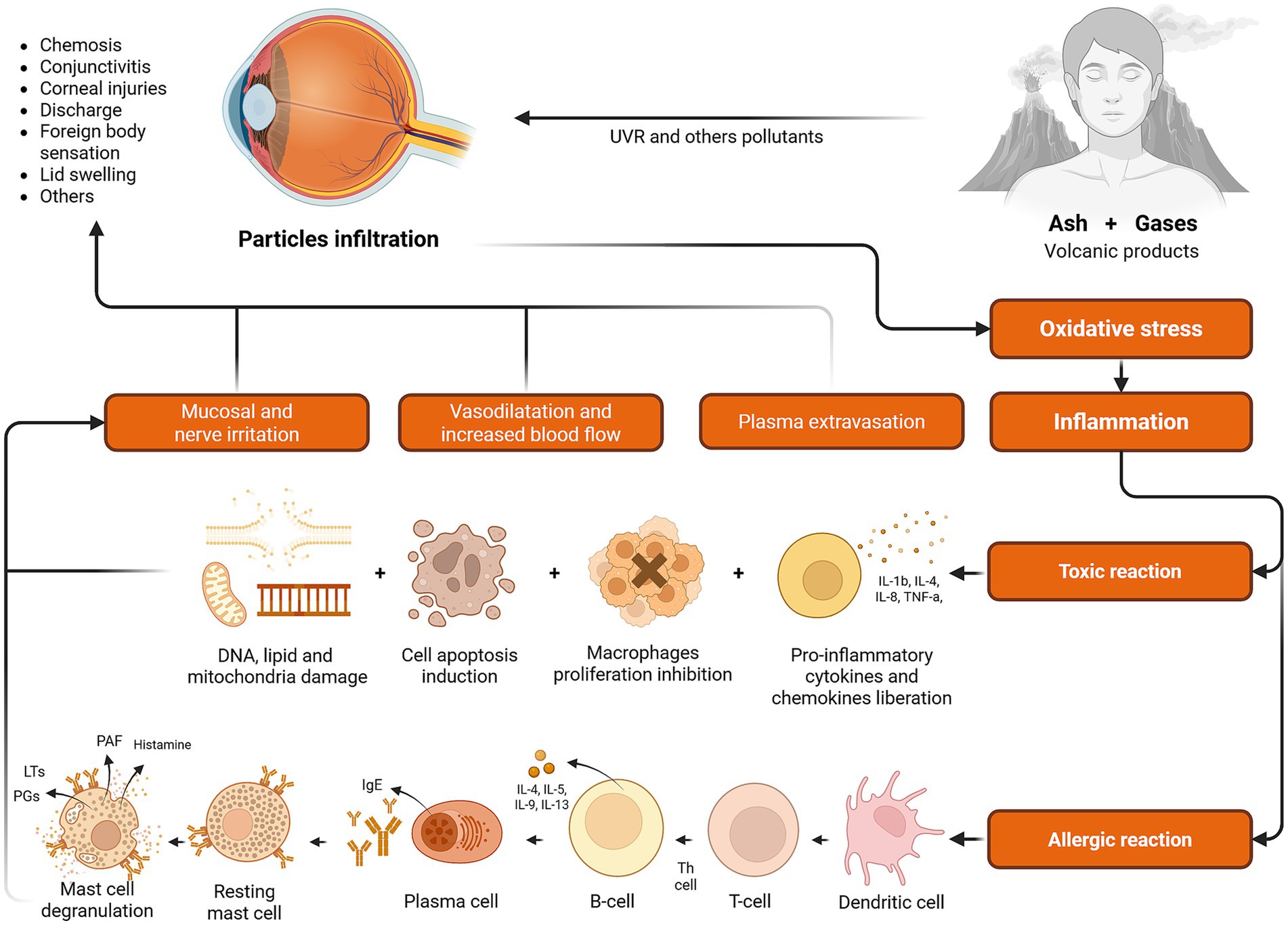
Figure 6. Effects of volcanic activity on ocular health. DNA, deoxyribonucleic acid; IgE, immunoglobulin E; IL, interleukin; LTs, leukotrienes; PAF, platelet-activating factor; PGs, prostaglandins; Th cell, T helper cell; TNF-a, tumor necrosis factor alpha; UVR, ultraviolet radiation (This figure was created using Biorender.com).
Volcanic ash also poses substantial ocular health risks due to its physical and chemical characteristics, such as particle size distribution, mineralogical composition, and surface reactivity (71, 72). Mechanical abrasion from ash particles accumulating within the conjunctival sac frequently results in corneal epithelial damage and conjunctival inflammation. Even minimal exposure to gaseous volcanic emissions can markedly irritate ocular surfaces (27, 73). These adverse effects can be potentiated by concurrent exposure to ultraviolet radiation, environmental pollutants, and organic solvents. Prolonged corneal epithelial disruption further increases susceptibility to severe corneal infections. Areas with substantial volcanic ash exposure consistently reported higher incidences of ocular complaints, predominantly characterized by conjunctival hyperemia, foreign body sensation, mucopurulent discharge, and pruritus (30, 50, 74). Fraunfelder et al. documented a 72% prevalence of foreign body sensation and conjunctivitis among forestry workers exposed to volcanic ash from Mount St. Helens, highlighting the severe impact of airborne volcanic particulates on ocular health (75).
3.4 Dermatological effects
Eleven studies addressing dermatological outcomes associated with volcanic eruptions were analyzed (17, 31, 71, 76–83). Epidemiological research constituted the majority (n = 6; 54.55%), supplemented by case series (n = 3; 27.27%) and literature reviews classified as multicriteria studies (n = 2; 18.18%). Investigations encompassed geographically diverse volcanic eruptions: Mount Etna in Italy (n = 2; 18.18%), Whakaari/White Island in New Zealand (n = 2; 18.18%), Eyjafjallajökull in Iceland (n = 1; 9.09%), Mount Merapi in Indonesia (n = 1; 9.09%), Mount Sakurajima in Japan (n = 1; 9.09%), Mount St. Helens in the United States (n = 1; 9.09%), and Lake Nyos in Cameroon (n = 1; 9.09%) (71, 79).
Dermatological effects of volcanic exposure primarily resulted from contact with volcanic ash fallout and gas emissions. Thermal burns represented the predominant acute injury type; however, physical abrasions and chemical burns were also recorded (76, 80). Exposure to hot volcanic gases and ash clouds at extreme temperatures for 60–90 s frequently resulted in severe burns, predominantly affecting exposed skin regions (77, 78, 81). Heat transmission mechanisms included conduction from accumulated ash deposits, convection from heated volcanic clouds, and thermal radiation (78). Burn mortality was substantial, averaging 47.6%, with affected body surface areas ranging from 9 to 90% (76, 78–81). Primary causes of death among burn victims included inhalation injuries and systemic infections predominantly caused by Aspergillus fumigatus (76, 78). Notably, elevated sulfate particle concentrations were detected in postmortem skin tissues following the 1980 eruption of Mount St. Helens (81). Recent evidence indicates that volcanic burn injuries necessitated increased surgical intervention time, prolonged hospitalization, and higher healthcare utilization compared to predictive models, reflecting their severity and complexity (76, 80).
Chronic dermatological sequelae were significantly more prevalent in volcanically exposed populations compared to non-exposed groups, with an overall increase of 11.60% (31). Frequently observed chronic conditions included eczema, dermatitis, nonspecific eruptions (12.4%), erythema (19%), and ulcerative lesions primarily localized to the face, extremities, and other anatomical regions (47.82%) (76, 80, 82). Bacterial wound infections were common (51.20%), involving pathogens such as Chryseobacterium indologenes, Elizabethkingia miricola, Staphylococcus epidermidis, Staphylococcus aureus, and Streptococcus viridans (76, 81). Volcanic particulates, characterized by abrasive properties and chemical irritants, promoted oxidative stress, sustained local inflammation, and disrupted skin and mucosal barriers, potentially exacerbating pre-existing dermatological conditions such as eczema, dermatitis, and acne (Figure 7) (31, 71). Additional documented injuries included lacerations, penetrating trauma, compartment syndrome, tetanus, and necrotizing fasciitis (79, 83).

Figure 7. Effects of volcanic activity on skin health. DNA, deoxyribonucleic acid; ROS, reactive oxygen species (This figure was created using Biorender.com).
Long-term volcanic ash exposure has also been implicated in dermatological carcinogenesis, with documented cases including melanoma (1.20%) and non-melanoma skin cancers (13.60%) (82). The carcinogenic potential is attributed to chronic inflammatory responses induced by silica-rich ash containing ferric ions and other carcinogenic elements, leading to DNA damage and subsequent malignant transformation (17). Nonetheless, geographical variability and eruption-specific factors influenced the incidence and severity of these dermatological outcomes. For instance, a comparative study following the 2002 Mount Etna eruption revealed no statistically significant difference in dermatological emergency visits between eruption and quiescent periods (17).
3.5 Mental health effects
Twenty studies examining the mental health impacts associated with exposure to volcanic ash, gases, and debris were reviewed. The majority comprised epidemiological studies (n = 18; 90%), conducted primarily in Iceland (n = 5; 27.78%), Indonesia (n = 4; 22.22%), Japan (n = 4; 22.22%), Colombia (n = 3; 16.67%), and the United States (n = 2; 11.11%). Volcanic eruptions studied included Eyjafjallajökull (n = 4; 22.22%), Mount Merapi (n = 3; 16.67%), Nevado del Ruiz (n = 3; 16.67%), Mount St. Helens (n = 2; 11.11%), Mount Unzen (n = 2; 11.11%), among others (n = 4; 22.22%). Additionally, two multicriteria literature reviews (10%) addressing mental health impacts were included.
Psychological outcomes were categorized temporally as immediate (e.g., post-traumatic stress disorder (PTSD)), medium-term (e.g., delayed-onset PTSD, major depressive disorder, generalized anxiety disorder), and long-term effects (e.g., psychosomatic disorders) (84–89).
The most frequently reported mental health diagnoses during intervention periods were prolonged depression (27.63%), PTSD (11.84%), and depressive episodes (9.21%). Less common psychiatric diagnoses included dementia (5.26%), alcohol dependence (3.95%), schizophrenia (2.63%), and various other disorders (84). The incidence of PTSD was notably higher in individuals residing in highly exposed areas or among those reporting multiple physical symptoms related to volcanic exposure (Figure 8) (31, 90–92).
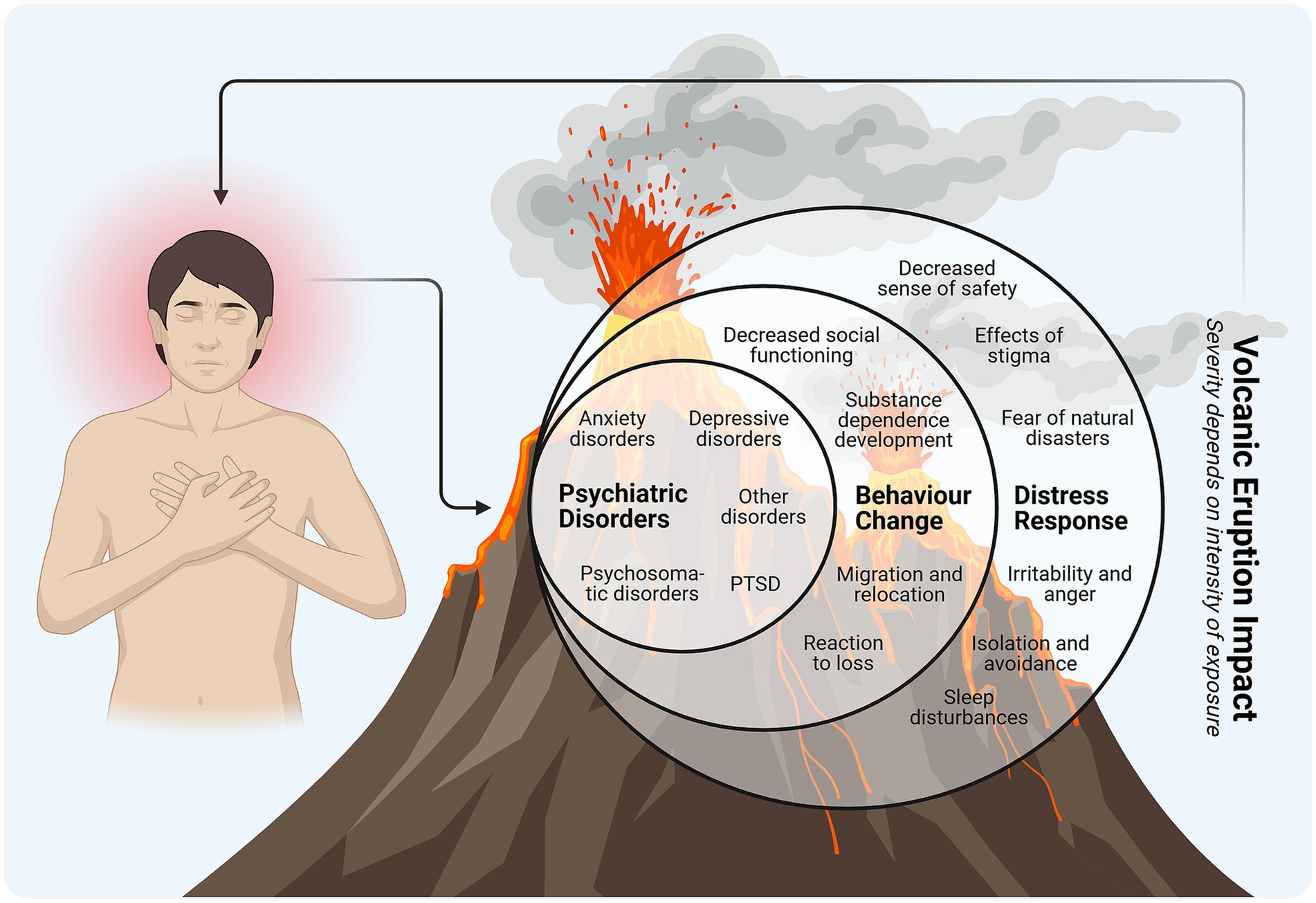
Figure 8. Effects of volcanic activity on mental health. PTSD, post-traumatic stress disorder (This figure was created using Biorender.com).
Significant risk factors correlated with higher PTSD incidence included widowhood or divorce, lower socioeconomic status (p = 0.033), occupations such as farming or fishing (p = 0.011), and pet loss (p = 0.002). Additionally, individuals with frequent relocations reported significantly increased PTSD symptoms compared to less frequently relocated individuals. Depressive symptoms strongly correlated with lower socioeconomic status, widowhood, prolonged residence in affected areas, and prior disaster-related evacuation experiences, with older adults particularly affected (87, 91). Persistent physical and psychological symptoms were documented among children, with anxiety levels significantly elevated in moderately exposed (OR = 2.39, 95% CI: 1.67–3.45) and highly exposed (OR = 2.77, 95% CI: 1.81–4.27) groups, underscoring the necessity of targeted preventive and supportive psychological interventions for pediatric populations (42, 86, 93). In the included studies, the terms “low,” “moderate,” and “high exposure,” as well as “frequent relocations,” were operationalized by the original authors, typically according to geographic proximity to the volcano or the number of displacement events, rather than by quantitative exposure metrics.
Gender disparities in mental health outcomes were apparent; generalized anxiety disorder, major depression, and PTSD were more prevalent among women. Compared to low-exposure areas, women in high-exposure areas exhibited an 11-fold increase in risk, whereas men showed a 12.3-fold increase (94).
Additional prevalent psychological symptoms included sadness (83.40%), anger (65.10%), anxiety (42–52%), distress (76.60%), anergia, and social dysfunction (95, 96). However, some studies reported stress, anxiety, or depression symptoms affecting fewer than 10% of individuals in moderately exposed regions (50).
Research addressing mental health impacts following volcanic eruptions remains limited, potentially due to the significant stigma associated with mental health disorders. Such stigma often leads to denial as a coping mechanism among affected populations (30, 85, 97).
Furthermore, mental health outcomes post-eruption are influenced substantially by socioeconomic factors (98), with evidence suggesting that post-disaster relocation accompanied by adequate resources significantly enhances mental health recovery (96, 99).
4 Discussion
This review synthesizes evidence regarding the diverse health impacts associated with volcanic eruptions, highlighting significant respiratory, ocular, dermatological, cardiovascular, and mental health outcomes. The severity and prevalence of these effects are influenced by eruption magnitude, exposure type, and local environmental and socio-economic contexts, underscoring the necessity of a holistic approach to evaluating and managing health risks posed by volcanic emissions, including particulate matter such as volcanic ash and toxic gases.
Existing literature reveals that exposure to volcanic emissions, particularly SO2, poses significant risks to respiratory, cardiovascular and ocular health (19, 27, 33, 69, 75). Multiple studies have documented a high prevalence of acute conditions such as sinusitis, bronchitis, arterial hypertension, dermatitis, anxiety, PTSD, conjunctivitis, and ocular foreign body sensation among populations exposed to volcanic ash and gases (17, 37, 52, 67, 69–73, 75, 78, 79, 84–87). Chronic exposure to volcanic emissions is particularly concerning, as it fosters sustained inflammatory processes and systemic toxicity. Prolonged contact with SO2, sulphate aerosols, heavy metals, and naturally degassing gases, even from quiescent volcanoes, has been linked to progressive respiratory impairment, increased cardiovascular vulnerability, and potential carcinogenic pathways (17, 21, 31, 41, 58, 59, 67, 68, 82). These long-term sequelae often evolve gradually, complicating detection and frequently eluding conventional health surveillance.
Geographical factors critically modulate the observed health impacts among exposed populations. Areas with high volcanic activity report elevated incidences of acute and chronic diseases, highlighting occupational vulnerabilities and the amplifying role of local environmental conditions in health risks (21, 46, 63, 67, 71). Workers regularly exposed to volcanic pollutants show distinct susceptibilities, emphasizing the importance of considering occupational exposure in public health strategies (55, 70). Moreover, eruption frequency and intensity significantly affect symptom prevalence, suggesting heightened risks for populations experiencing repeated or intense volcanic activity (31, 42).
Effective public health management of volcanic hazards requires an integrated approach, combining health monitoring, environmental management, and socio-economic interventions. Respiratory conditions such as asthma and chronic bronchitis, frequently exacerbated by volcanic emissions, place substantial pressure on healthcare systems, a phenomenon notably evident during crises such as the COVID-19 pandemic, and likely applicable to communities near active volcanoes (31). Vulnerable groups, particularly children, older adults, and individuals with pre-existing medical conditions, exhibit heightened susceptibility, underscoring the critical need for targeted monitoring and robust public health interventions to mitigate long-term morbidity (29, 30).
Beyond respiratory concerns, volcanic emissions significantly compromise water and air quality, impacting food security and community health. Contamination with heavy metals (e.g., lead, mercury, arsenic) linked to volcanic activity poses substantial health risks, including neurodevelopmental impairments, cancer, thyroid disruption, immunosuppression, and malnutrition, especially in developing countries with limited healthcare infrastructure (100–102). These environmental health threats necessitate rigorous monitoring and targeted mitigation strategies, including improvements in water and food quality, enhanced sanitation systems, timely communication of volcanic activity and comprehensive volcano monitoring to safeguard community health, particularly among vulnerable populations such as children (103).
Forced displacement due to volcanic hazards further exacerbates health outcomes, affecting mental health, substance use, and perinatal health (104–106). Evidence increasingly suggests that traumatic events, including forced relocations, directly influence health outcomes. Displacement disrupts livelihoods, social support networks, and cultural continuity, amplifying existing health disparities and straining healthcare resources (107, 108). Comprehensive public health interventions addressing social, mental, and physical health, combined with sustainable economic support and community-driven resilience-building programs, are essential for mitigating these impacts.
Public education, preparedness, and policy interventions play crucial roles in reducing health risks associated with volcanic emissions. Early warning systems, protective equipment guidelines, regular emergency drills, effective communication strategies, and accessible emergency shelters are integral components for enhancing community resilience and rapid response capabilities (109, 110). Policies emphasizing continuous air quality monitoring, targeted support for vulnerable groups, and sustainable funding for preventive infrastructure substantially strengthen community preparedness and healthcare system resilience against volcanic hazards (111).
4.1 Limitations of the study
This review acknowledges certain limitations, notably the heterogeneity of study designs, complicating direct comparisons. The absence of a systematic risk-of-bias assessment could affect the robustness of conclusions, although such assessments are not mandatory for scoping reviews. Although meta-analysis was not feasible due to methodological diversity, the synthesis allows for the identification of trends and priority areas for future research. In this study, some pollutants of high toxicological relevance, such as fluoride, were not considered, as their primary effects involve the skeletal system, which was beyond the scope of this review. Other organ systems potentially affected by volcanic emissions, also did not emerge in the selected literature. Furthermore, exposure levels were often defined indirectly rather than measured concentrations, limiting dose–response inference. Nevertheless, findings presented offer valuable insights into volcanic eruption health impacts, highlighting the necessity for standardized methodologies and sustained health monitoring to improve comparability and reliability across studies.
4.2 Recommendation for further research
Further research should elucidate how volcanic products enter the body and their associated physiological, biochemical, and immunological impacts, particularly regarding cardiovascular health. Targeted studies are needed for vulnerable groups, including children, pregnant women, older adults, and displaced populations in high-risk areas. Moreover, research should expand beyond currently studied systems to include metabolic, hepatic, nephrological, reproductive, and skeletal outcomes, and evaluate emergent burdens such as cancer, neurodegenerative and maternal–child health disorders. Likewise, incorporating grey literature and operational reports would complement peer-reviewed evidence, thereby enhancing contextual understanding and guiding preparedness strategies. The integration of social determinants of health is essential to ensure the development of interventions tailored to community needs.
5 Conclusion
This scoping review provides a comprehensive overview of the health impacts associated with volcanic eruptions, highlighting the complex interactions between volcanic emissions and human health, particularly in communities near active volcanoes. Health consequences frequently result from direct exposure to volcanic ash and gases or indirect contact through polluted air and water sources. Notably, volcanic emissions can aggravate pre-existing medical conditions and elevate morbidity rates, with variability in health outcomes observed according to demographic factors such as age and sex. These findings underscore the necessity for tailored, evidence-based interventions, proactive public health education, and further research to enhance community preparedness, resilience, and reduce long-term health vulnerabilities.
Data availability statement
The published article and supplemental information include all data generated and analysed during this study. Any additional information required to reanalyse the data reported in this paper is available from the lead contact, Katherine Simbaña-Rivera (a2F0aGVyaW5lLnNpbWJhbmExMDFAYWx1LnVscGdjLmVz), upon request.
Author contributions
KS-R: Conceptualization, Data curation, Project administration, Validation, Methodology, Supervision, Writing – review & editing, Funding acquisition, Writing – original draft, Resources, Investigation, Formal analysis, Visualization, Software. JE-M: Writing – original draft, Visualization, Software, Formal analysis, Writing – review & editing, Data curation, Project administration, Validation, Methodology, Supervision, Investigation. DJ-A: Project administration, Visualization, Writing – original draft, Formal analysis, Validation, Data curation, Supervision, Writing – review & editing, Methodology, Investigation, Software. LM-L: Data curation, Methodology, Writing – original draft, Software, Investigation, Validation, Writing – review & editing, Formal analysis. RJ-S: Investigation, Resources, Validation, Writing – original draft, Funding acquisition, Writing – review & editing, Formal analysis. XS: Formal analysis, Resources, Funding acquisition, Writing – original draft, Writing – review & editing, Validation, Investigation. MR-P: Writing – original draft, Formal analysis, Investigation, Writing – review & editing, Validation. MF-F: Writing – review & editing, Validation, Formal analysis, Writing – original draft, Investigation. LB: Funding acquisition, Resources, Validation, Conceptualization, Supervision, Investigation, Methodology, Writing – review & editing, Formal analysis, Writing – original draft.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The publication fees related to this manuscript was financed by Pontificia Universidad Católica del Ecuador (PUCE).
Acknowledgments
The authors thank Pontificia Universidad Católica del Ecuador (PUCE) for supporting the publication fee.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1658384/full#supplementary-material
References
1. Global Volcanism Program. Data from: [Database] Volcanoes of the World (v. 5.2.4; 21 Oct 2024). Distributed by Smithsonian Institution, compiled by Venzke, E. (2024). doi: 10.5479/si.GVP.VOTW5-2024.5.2
2. Masum, M, and Akbar, A. The Pacific ring of fire is working as a home country of geothermal resources in the world. IOP Conf Ser Earth Environ Sci. (2019) 249:012020. doi: 10.1088/1755-1315/249/1/012020
3. El Hadri, H, Goujon, M, and Paris, R. A database of the economic impacts of historical volcanic eruptions. Etudes Doc. (2021) 14:1–42.
4. Edmonds, M, Mather, TA, and Liu, EJ. A distinct metal fingerprint in arc volcanic emissions. Nat Geosci. (2018) 11:790–4. doi: 10.1038/s41561-018-0214-5
5. Boada, LD, Simbaña-Rivera, K, Rodríguez-Pérez, C, Fuentes-Ferrer, M, Henríquez-Hernández, LA, López-Villarrubia, E, et al. Assessing the hidden dangers of volcanic CO2 exposure: a critical review of health impacts. Front Public Health. (2024) 12:1465837. doi: 10.3389/fpubh.2024.1465837
6. Viveiros, F, and Silva, C. Hazardous volcanic CO2 diffuse degassing areas–a systematic review on environmental impacts, health, and mitigation strategies. Iscience. (2024) 27:110990. doi: 10.1016/j.isci.2024.110990
7. Ilyinskaya, E, Mason, E, Wieser, PE, Holland, L, Liu, EJ, Mather, TA, et al. Rapid metal pollutant deposition from the volcanic plume of Kīlauea, Hawai’i. Commun Earth Environ. (2021) 2:1–15. doi: 10.1038/s43247-021-00146-2
8. Farquharson, JI, and Amelung, F. Volcanic hazard exacerbated by future global warming-driven increase in heavy rainfall. R Soc Open Sci. (2022) 9:220275. doi: 10.1098/rsos.220275
9. Thouret, J-C, Wavelet, E, Taillandier, M, Tjahjono, B, Jenkins, SF, Azzaoui, N, et al. Defining population socio-economic characteristics, hazard knowledge and risk perception: the adaptive capacity to persistent volcanic threats from Semeru, Indonesia. Int J Disaster Risk Reduct. (2022) 77:103064. doi: 10.1016/j.ijdrr.2022.103064
10. Brown, SK, Jenkins, SF, Sparks, RSJ, Odbert, H, and Auker, MR. Volcanic fatalities database: analysis of volcanic threat with distance and victim classification. J Appl Volcanol. (2017) 6:15. doi: 10.1186/s13617-017-0067-4
11. Pan, H, Shi, P, Ye, T, Xu, W, and Wang, J. Mapping the expected annual fatality risk of volcano on a global scale. Int J Disaster Risk Reduct. (2015) 13:52–60. doi: 10.1016/j.ijdrr.2015.03.004
12. Horwell, CJ, Baxter, PJ, Damby, DE, Elias, T, Ilyinskaya, E, Sparks, RSJ, et al. The international volcanic health hazard network (IVHHN): reflections on 20 years of progress. Front Earth Sci. (2023) 11:1213363. doi: 10.3389/feart.2023.1213363
13. Arksey, H, and O’Malley, L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. (2005) 8:19–32. doi: 10.1080/1364557032000119616
14. Peters, MDJ, Godfrey, CM, Khalil, H, McInerney, P, Parker, D, and Soares, CB. Guidance for conducting systematic scoping reviews. Int J Evid Based Healthc. (2015) 13:141–6. doi: 10.1097/XEB.0000000000000050
15. Tricco, AC, Lillie, E, Zarin, W, O'Brien, K, Colquhoun, H, Levac, D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. (2018) 169:467–73. doi: 10.7326/M18-0850
16. Richardson, WS, Wilson, MC, Nishikawa, J, and Hayward, RS. The well-built clinical question: a key to evidence-based decisions. ACP J Club. (1995) 123:A12–3. doi: 10.7326/ACPJC-1995-123-3-A12
17. Lombardo, D, Ciancio, N, Campisi, R, Di Maria, A, Bivona, L, Poletti, V, et al. A retrospective study on acute health effects due to volcanic ash exposure during the eruption of Mount Etna (Sicily) in 2002. Multidiscip Respir Med. (2013) 8:51. doi: 10.1186/2049-6958-8-51
18. Baxter, PJ. Health hazards of volcanic eruptions. J R Coll Physicians Lond. (1983) 17:180–2. doi: 10.1016/S0035-8819(25)02629-7
19. Carlsen, HK, Aspelund, T, Briem, H, Gislason, T, Johannsson, T, Valdimarsdottir, U, et al. Respiratory health among professionals exposed to extreme SO2 levels from a volcanic eruption. Scand J Work Environ Health. (2019) 45:312–5. doi: 10.5271/sjweh.3783
20. Longo, BM. The Kilauea volcano adult health study. Nurs Res. (2009) 58:23–31. doi: 10.1097/NNR.0b013e3181900cc5
21. Longo, BM, Rossignol, A, and Green, JB. Cardiorespiratory health effects associated with sulphurous volcanic air pollution. Public Health. (2008) 122:809–20. doi: 10.1016/j.puhe.2007.09.017
22. Grob, BE, Oyarzún, GM, Cavieres, CI, Zarges, TP, and Bustamante, MG. ¿Son las cenizas volcánicas un riesgo para la salud respiratoria?: Revisión a propósito de la erupción del cordón del Caulle en junio de 2011. Rev Chil Enferm Respir. (2012) 28:294–302. doi: 10.4067/S0717-73482012000400005
23. Stewart, C, Damby, DE, Horwell, CJ, Elias, T, Ilyinskaya, E, Tomašek, I, et al. Volcanic air pollution and human health: recent advances and future directions. Bull Volcanol. (2021) 84:11. doi: 10.1007/s00445-021-01513-9
24. Gudmundsson, G. Respiratory health effects of volcanic ash with special reference to Iceland. A review. Clin Respir J. (2011) 5:2–9. doi: 10.1111/j.1752-699X.2010.00231.x
25. Baxter, PJ, Ing, R, Falk, H, and Plikaytis, B. Mount St. Helens eruptions: the acute respiratory effects of volcanic ash in a north American community. Arch Environ Health. (1983) 38:138–43. doi: 10.1080/00039896.1983.10543994
26. Carlsen, HK, Ilyinskaya, E, Baxter, PJ, Schmidt, A, Thorsteinsson, T, Pfeffer, MA, et al. Increased respiratory morbidity associated with exposure to a mature volcanic plume from a large Icelandic fissure eruption. Nat Commun. (2021) 12:2161. doi: 10.1038/s41467-021-22432-5
27. Kochi, T, Iwasawa, S, Nakano, M, Tsuboi, T, Tanaka, S, Kitamura, H, et al. Influence of sulfur dioxide on the respiratory system of Miyakejima adult residents 6 years after returning to the island. J Occup Health. (2017) 59:313–26. doi: 10.1539/joh.16-0256-OA
28. Amaral, A, Rodrigues, V, Oliveira, J, Pinto, C, Carneiro, V, Sanbento, R, et al. Chronic exposure to volcanic environments and cancer incidence in the Azores, Portugal. Sci Total Environ. (2006) 367:123–8. doi: 10.1016/j.scitotenv.2006.01.024
29. Buist, AS, Vollmer, WM, Johnson, LR, Bernstein, RS, and McCamant, LE. A four-year prospective study of the respiratory effects of volcanic ash from Mt. St. Helens. Am Rev Respir Dis. (1986) 133:526–34. doi: 10.1164/arrd.1986.133.4.526
30. Carlsen, HK, Hauksdottir, A, Valdimarsdottir, UA, Gislason, T, Einarsdottir, G, Runolfsson, H, et al. Health effects following the Eyjafjallajokull volcanic eruption: a cohort study. BMJ Open. (2012) 2:e001851. doi: 10.1136/bmjopen-2012-001851
31. Hlodversdottir, H, Petursdottir, G, Carlsen, HK, Gislason, T, and Hauksdottir, A. Long-term health effects of the Eyjafjallajökull volcanic eruption: a prospective cohort study in 2010 and 2013. BMJ Open. (2016) 6:e011444. doi: 10.1136/bmjopen-2016-011444
32. Horwell, CJ, and Baxter, PJ. The respiratory health hazards of volcanic ash: a review for volcanic risk mitigation. Bull Volcanol. (2006) 69:1–24. doi: 10.1007/s00445-006-0052-y
33. Ishigami, A, Kikuchi, Y, Iwasawa, S, Nishiwaki, Y, Takebayashi, T, Tanaka, S, et al. Volcanic sulfur dioxide and acute respiratory symptoms on Miyakejima island. Occup Environ Med. (2008) 65:701–7. doi: 10.1136/oem.2007.033456
34. Linhares, D, Ventura Garcia, P, Viveiros, F, Ferreira, T, and dos Santos Rodrigues, A. Air pollution by hydrothermal volcanism and human pulmonary function. Biomed Res Int. (2015) 2015:326794. doi: 10.1155/2015/326794
35. Maldonado Cajiao, F, Maldonado Coronel, K, Maldonado Coronel, F, and Silva Jara, JVS. Restrictive-obstructive respiratory diseases and ash of the Tungurahua volcano in 2007. Cienc Al Serv Salud Nutr. (2019) 9:7–13.
36. Mannino, DM, Ruben, S, Holschuh, FC, Holschuh, TC, Wilson, MD, and Holschuh, T. Emergency department visits and hospitalizations for respiratory disease on the island of Hawaii, 1981 to 1991. Hawaii Med J. (1996) 55:48–54.
37. Naumova, EN, Yepes, H, Griffiths, JK, Sempértegui, F, Khurana, G, Jagai, JS, et al. Emergency room visits for respiratory conditions in children increased after Guagua Pichincha volcanic eruptions in April 2000 in Quito, Ecuador observational study: time series analysis. Env Health. (2007) 6:21. doi: 10.1186/1476-069X-6-21
38. Shimizu, Y, Dobashi, K, Hisada, T, Ono, A, Todokoro, M, Iijima, H, et al. Acute impact of volcanic ash on asthma symptoms and treatment. Int J Immunopathol Pharmacol. (2007) 20:9–14. doi: 10.1177/03946320070200S203
39. Tam, E, Miike, R, Labrenz, S, Sutton, AJ, Elias, T, Davis, J, et al. Volcanic air pollution over the island of Hawai’i emissions, dispersal, composition association with respiratory symptoms and lung function in Hawai’i Island schoolchildren. Env Int. (2016) 92-93:543–52. doi: 10.1016/j.envint.2016.03.025
40. Yano, E, Yokoyama, Y, and Nishii, S. Chronic pulmonary effects of volcanic ash: an epidemiologic study. Arch Environ Health. (1986) 41:94–9. doi: 10.1080/00039896.1986.9937416
41. Yano, E, Yokoyama, Y, Higashi, H, Nishii, S, Maeda, K, and Koizumi, A. Health effects of volcanic ash: a repeat study. Arch Environ Health. (1990) 45:367–73. doi: 10.1080/00039896.1990.10118757
42. Hlodversdottir, H, Thorsteinsdottir, H, Thordardottir, EB, Njardvik, U, Petursdottir, G, and Hauksdottir, A. Long-term health of children following the Eyjafjallajökull volcanic eruption: a prospective cohort study. Eur J Psychotraumatol. (2018) 9:1442601. doi: 10.1080/20008198.2018.1442601
43. Shiozawa, M, Lefor, A, Sata, N, Yasuda, Y, and Nagai, H. Effects of the Miyakejima volcano eruption on public health. Int J Crit Care Emerg Med. (2018) 4:40. doi: 10.23937/2474-3674/1510040
44. Zabert, I, Benítez, S, Maldonado PDC,, Uribe Evhevarría, L, and Zabert, GE. Prevalence of asthma at risk symptoms in adolescents exposed to volcanic ash, in two Patagonian cities. Rev Fac Cien Med Univ Nac Cordoba. (2020) 77:261–7. doi: 10.31053/1853.0605.v77.n2.27927
45. Durand, M, and Wilson, JG. Spatial analysis of respiratory disease on an urbanized geothermal field. Environ Res. (2006) 101:238–45. doi: 10.1016/j.envres.2005.08.006
46. Hickling, J, Clements, M, Weinstein, P, and Woodward, A. Acute health effects of the mount Ruapehu (New Zealand) volcanic eruption of June 1996. Int J Environ Health Res. (1999) 9:97–107. doi: 10.1080/09603129973236
47. Iwasawa, S, Kikuchi, Y, Nishiwaki, Y, Nakano, M, Michikawa, T, Tsuboi, T, et al. Effects of SO2 on respiratory system of adult Miyakejima resident 2 years after returning to the island. J Occup Health. (2009) 51:38–47. doi: 10.1539/joh.l8075
48. Kraemer, MJ, and McCarthy, MM. Childhood asthma hospitalization rates in Spokane County, Washington: impact of volcanic ash air pollution. J Asthma. (1985) 22:37–43. doi: 10.3109/02770908509079882
49. Bergin, CJ, Wilton, S, Taylor, MH, and Locke, M. Thoracic manifestations of inhalational injury caused by the Whakaari/White Island eruption. J Med Imaging Radiat Oncol. (2021) 65:301–8. doi: 10.1111/1754-9485.13159
50. Carlsen, HK, Gislason, T, Benediktsdottir, B, Kolbeinsson, TB, Hauksdottir, A, Thorsteinsson, T, et al. A survey of early health effects of the Eyjafjallajökull 2010 eruption in Iceland: a population-based study. BMJ Open. (2012) 2:e000343. doi: 10.1136/bmjopen-2011-000343
51. Longo, BM, Yang, W, Green, JB, Crosby, FL, and Crosby, VL. Acute health effects associated with exposure to volcanic air pollution (vog) from increased activity at Kilauea volcano in 2008. J Toxic Environ Health A. (2010) 73:1370–81. doi: 10.1080/15287394.2010.497440
52. Longo, BM, and Yang, W. Acute bronchitis and volcanic air pollution: a community-based cohort study at Kilauea volcano, Hawai’i, USA. J Toxicol Environ Health A. (2008) 71:1565–71. doi: 10.1080/15287390802414117
53. Nieto-Torres, A, and Del Martin- Pozzo, AL. Ash emission from a long-lived eruption at Popocatépetl volcano and mapped respiratory effects. Bull Volcanol. (2021) 83:68. doi: 10.1007/s00445-021-01490-z
54. Forbes, L, Jarvis, D, Potts, J, and Baxter, PJ. Volcanic ash and respiratory symptoms in children on the island of Montserrat, British West Indies. Occup Environ Med. (2003) 60:207–11. doi: 10.1136/oem.60.3.207
55. Yglesias-González, M, and Chamizo-García, HA. Susceptibilidad y síntomas respiratorios asociados a la exposición a dióxido de carbono y dióxido de azufre provenientes del volcán Turrialba, Costa Rica. Poblac Salud En Mesoamérica. (2014) 12:1–14. doi: 10.15517/psm.v12i1.15140
56. Choudhury, AH, Gordian, ME, and Morris, SS. Associations between respiratory illness and PM10 air pollution. Arch Environ Health. (1997) 52:113–7. doi: 10.1080/00039899709602873
57. Rojas-Ramos, M, Catalan-Vazquez, M, Pozzo, ALM-D, Garcia-Ojeda, E, Villalba-Caloca, J, and Perez-Neria, J. A seven months prospective study of the respiratory effects of exposure to ash from Popocatepetl volcano, Mexico. Environ Geochem Health. (2001) 23:379–92. doi: 10.1023/A:1012244311557
58. Higuchi, K, Koriyama, C, and Akiba, S. Increased mortality of respiratory diseases, including lung Cancer, in the area with large amount of Ashfall from mount Sakurajima volcano. J Environ Public Health. (2012) 2012:1–4. doi: 10.1155/2012/257831
59. Bernstein, RS, Baxter, PJ, Falk, H, Ing, R, Foster, L, and Frost, F. Immediate public health concerns and actions in volcanic eruptions: lessons from the Mount St. Helens eruptions, may 18-October 18, 1980. Am J Public Health. (1986) 76:25–37. doi: 10.2105/AJPH.76.Suppl.25
60. Fano, V, Cernigliaro, A, Scondotto, S, Perucci, CA, and Forastiere, F. The fear of volcano: short-term health effects after Mount Etna’s eruption in 2002. Eur Respir J. (2010) 36:1216–8. doi: 10.1183/09031936.00078910
61. Oudin, A, Carlsen, H, Forsberg, B, and Johansson, C. Volcanic ash and daily mortality in Sweden after the Icelandic volcano eruption of may 2011. Int J Environ Res Public Health. (2013) 10:6909–19. doi: 10.3390/ijerph10126909
62. Bates, MN, Garrett, N, Crane, J, and Balmes, JR. Associations of ambient hydrogen sulfide exposure with self-reported asthma and asthma symptoms. Environ Res. (2013) 122:81–7. doi: 10.1016/j.envres.2013.02.002
63. Bates, MN, Crane, J, Balmes, JR, and Garrett, N. Investigation of hydrogen sulfide exposure and lung function, asthma and chronic obstructive pulmonary disease in a geothermal area of New Zealand. PLoS One. (2015) 10:e0122062. doi: 10.1371/journal.pone.0122062
64. Elliot, AJ, Singh, N, Loveridge, P, Harcourt, S, Smith, S, Pnaiser, R, et al. Syndromic surveillance to assess the potential public health impact of the Icelandic volcanic ash plume across the United Kingdom, April 2010. Euro Surveill. (2010) 15:19583. doi: 10.2807/ese.15.23.19583-en
65. Iwasawa, S, Nakano, M, Tsuboi, T, Kochi, T, Tanaka, S, Katsunuma, T, et al. Effects of sulfur dioxide on the respiratory system of Miyakejima child residents 6 years after returning to the island. Int Arch Occup Environ Health. (2015) 88:1111–8. doi: 10.1007/s00420-015-1037-y
66. Zabert, I, Benítez, S, and Gustavo, G. Impact on the respiratory airways of acute exposure to volcanic ash in the Patagonia: cross-sectional study. RAMR. (2019) 2:199–24.
67. Fano, V, Cernigliaro, A, Scondotto, S, Cuccia, M, Forastiere, F, Nicolosi, A, et al. Health effects of environmental contamination due to volcanic ash of Mount Etna in autumn 2002. Epidemiol Prev. (2005) 29:180–7. doi: 10.1097/00001648-200611001-00400
68. Carapezza, ML, Tarchini, L, Ancona, C, Forastiere, F, Ranaldi, M, Ricci, T, et al. Health impact of natural gas emission at cava Dei Selci residential zone (metropolitan city of Rome, Italy). Environ Geochem Health. (2023) 45:707–29. doi: 10.1007/s10653-022-01244-6
69. Camara, JG, and Lagunzad, JKD. Ocular findings in volcanic fog induced conjunctivitis. Hawaii Med J. (2011) 70:262–5.
70. Ortiz Apuy, E, Mora Barrantes, JC, and Sibaja Brenes, JP. Estudio preliminar con respecto a los efectos en la salud de trabajadores y su relación con la exposición a emisiones gaseosas volcánicas. Un caso de estudio en dos volcanes activos de Costa Rica. Uniciencia. (2022) 36:761–80. doi: 10.15359/ru.36-1.49
71. Gudmundsson, G, and Larsen, G. Effects of volcanic eruptions on human health in Iceland. Review. Laeknabladid. (2016) 102:433–41. doi: 10.17992/lbl.2016.10.101
72. Cook, A, and Weinstein, P. Volcanic and geothermal processes: Health effects. Encycl Environ Health. (2011):664–71. doi: 10.1016/B978-0-444-52272-6.00157-4
73. Grattan, J, Durant, M, and Taylor, S. Illness and elevated human mortality in Europe coincident with the Laki fissure eruption. Volcanic desassing Piccadilly Circus. London: The Geological Society of London. (2003) 401–414. doi: 10.1144/GSL.SP.2003.213.01.24
74. Kimura, K, Sakamoto, T, Miyazaki, M, Uchino, E, Kinukawa, N, and Isashiki, M. Effects of volcanic ash on ocular symptoms: results of a 10-year survey on schoolchildren. Ophthalmology. (2005) 112:478–81. doi: 10.1016/j.ophtha.2004.09.031
75. Fraunfelder, FT, Kalina, RE, Buist, AS, Bernstein, RS, and Johnson, DS. Ocular effects following the volcanic eruptions of mount St Helens. Arch Ophthalmol. (1960) 101:376–8. doi: 10.1001/archopht.1983.01040010376003
76. Baker, P, Locke, M, Moazzam, A, Taylor, M, Stapelberg, F, and Wong She, R. Burn lessons learned from the Whakaari White Island volcanic eruption. J Burn Care Res. (2022) 43:1105–13. doi: 10.1093/jbcr/irab246
77. Baxter, PJ, Kapila, M, and Mfonfu, D. Lake Nyos disaster, Cameroon, 1986: the medical effects of large scale emission of carbon dioxide? BMJ. (1989) 298:1437–41. doi: 10.1136/bmj.298.6685.1437
78. Baxter, PJ, Jenkins, S, Seswandhana, R, Komorowski, J-C, Dunn, K, Purser, D, et al. Human survival in volcanic eruptions: thermal injuries in pyroclastic surges, their causes, prognosis and emergency management. Burns. (2017) 43:1051–69. doi: 10.1016/j.burns.2017.01.025
79. Beylin, D, Mantal, O, Haik, J, Kornhaber, R, Cleary, M, Neil, A, et al. Soft tissue-related injuries sustained following volcanic eruptions: an integrative review. Burns. (2022) 48:1727–42. doi: 10.1016/j.burns.2021.09.008
80. Locke, M, Wilton, S, Borowczyk, K, Stapelberg, F, and Wong She, R. Comparison of predictive model of care requirements for burn patients with operative requirements following volcanic burns. J Burn Care Res. (2021) 42:1003–10. doi: 10.1093/jbcr/irab019
81. Parshley, PF, Kiessling, PJ, Antonius, JA, Connell, RS, Miller, SH, and Green, FH. Pyroclastic flow injury. Mount St. Helens, may 18, 1980. Am J Surg. (1982) 143:565–8. doi: 10.1016/0002-9610(82)90163-5
82. Russo, M, Malandrino, P, Addario, WP, Dardanoni, G, Vigneri, P, Pellegriti, G, et al. Several site-specific cancers are increased in the volcanic area in Sicily. Anticancer Res. (2015) 35:3995–4001.
83. Wakisaka, I, Yanagihashi, T, Sato, M, and Tomari, T. Health effects of volcanic air pollution--an analysis of the national health insurance. Nihon Eiseigaku Zasshi. (1989) 44:977–86. doi: 10.1265/jjh.44.977
84. Araki, K, Nakane, Y, Ohta, Y, and Kawasaki, N. The nature of psychiatric problems among disaster victims. Psychiatry Clin Neurosci. (1998) 52:S317–9. doi: 10.1111/j.1440-1819.1998.tb03256.x
85. Kokai, M, Fujii, S, Shinfuku, N, and Edwards, G. Natural disaster and mental health in Asia. Psychiatry Clin Neurosci. (2004) 58:110–6. doi: 10.1111/j.1440-1819.2003.01203.x
86. Takagi, Y, Takahashi, S, Fukuo, Y, Arai, T, and Tachikawa, H. Acute-stage mental health symptoms by natural disaster type: consultations of disaster psychiatric assistance teams (DPATs) in Japan. Int J Environ Res Public Health. (2021) 18:12409. doi: 10.3390/ijerph182312409
87. Warsini, S, Buettner, P, Mills, J, West, C, and Usher, K. Post-traumatic stress disorder among survivors two years after the 2010 mount Merapi volcano eruption: a survey study. Nurs Health Sci. (2015) 17:173–80. doi: 10.1111/nhs.12152
88. Lima, B, and Gaviria, M. Consecuencias Psicosociales de los Desastres: La Experiencia Latinoamericana. In: B Lima and M Gaviria, editors. Monografías Clínicas. 2nd ed. Chicago, United States: Hispanic American Family Center (1989). 265. Available at: http://cidbimena.bvs.hn/docum/ops/publicaciones/ph30/ph30.1.htm
89. Lima, B, Pai, S, Santacruz, H, and Lozano, J. Psychiatric disorders among poor victims following a major disaster: Armero, Colombia. J Nerv Ment Dis. (1991) 179:420–7. doi: 10.1097/00005053-199107000-00006
90. Shore, JH, Tatum, EL, and Vollmer, WM. Psychiatric reactions to disaster: the Mount St. Helens experience. Am J Psychiatry. (1986) 143:590–5. doi: 10.1176/ajp.143.5.590
91. Goto, T, Wilson, JP, Kahana, B, and Slane, S. The Miyake Island volcano disaster in Japan: loss, uncertainty, and relocation as predictors of PTSD and depression. J Appl Soc Psychol. (2006) 36:2001–26. doi: 10.1111/j.0021-9029.2006.00091.x
92. Gissurardóttir, ÓS, Hlodversdóttir, H, Thordardóttir, EB, Pétursdóttir, G, and Hauksdóttir, A. Mental health effects following the eruption in Eyjafjallajökull volcano in Iceland: a population-based study. Scand J Public Health. (2019) 47:251–9. doi: 10.1177/1403494817751327
93. Syapitri, H, Hutajulu, J, Poddar, S, and Bhaumik, A. Analysis of adaptation response of victims Sinabung mountain eruption post-traumatic stress disorder. Enferm Clin. (2020) 30:183–7. doi: 10.1016/j.enfcli.2019.11.051
94. Shore, JH, Tatum, EL, and Vollmer, WM. Evaluation of mental effects of disaster, Mount St. Helens eruption. Am J Public Health. (1986) 76:76–83. doi: 10.2105/ajph.76.suppl.76
95. Ohta, Y, Araki, K, Kawasaki, N, Nakane, Y, Honda, S, and Mine, M. Psychological distress among evacuees of a volcanic eruption in Japan: a follow-up study. Psychiatry Clin Neurosci. (2003) 57:105–11. doi: 10.1046/j.1440-1819.2003.01086.x
96. Warsini, S, Buettner, P, Mills, J, West, C, and Usher, K. The psychosocial impact of the environmental damage caused by the MT Merapi eruption on survivors in Indonesia. EcoHealth. (2014) 11:491–501. doi: 10.1007/s10393-014-0937-8
97. Vengoechea, J.. Consecuencias psicopatológicas y tratamiento en pacientes médico quirúrgicos de la tragedia de Armero: Conclusiones y recomendaciones., Atención de urgencias en situaciones de desastre. Memorias. Medellín: Comité Interinstitucional Metropolitano del Sector de la Salud en Atención de Desastres, Universidad de Antioquía, Asociación de Enfermeras de Antioquía, Cruz Roja Colombiana (1987). p. 13 Available online at: http://www.disaster-info.net/infovolcanes/pdf/spa/doc106/doc106.htm. [Accessed May 25, 2024]
98. Lima, B, Pai, S, Santacruz, H, Lozano, J, and Luna, J. Screening for the psychological consequences of a major disaster in a developing country: Armero, Colombia. Acta Psychiatr Scand. (1987) 76:561–7. doi: 10.1111/j.1600-0447.1987.tb02919.x
99. Muir, JA, Cope, MR, Angeningsih, LR, Jackson, JE, and Brown, RB. Migration and mental health in the aftermath of disaster: evidence from Mt. Merapi, Indonesia. Int J Environ Res Public Health. (2019) 16:2726. doi: 10.3390/ijerph16152726
100. Rai, PK, Lee, SS, Zhang, M, Tsang, YF, and Kim, K-H. Heavy metals in food crops: health risks, fate, mechanisms, and management. Environ Int. (2019) 125:365–85. doi: 10.1016/j.envint.2019.01.067
101. Al-Worafi, YM. “Quality of Healthcare Systems in Developing Countries: Status and Future Recommendations.,” Handbook of medical and health sciences in developing countries: Education, practice, and research. Cham: Springer International Publishing (2023). p. 1–28
102. Coelho, NM, Bernardo, F, Rodrigues, AS, and Garcia, P. Volcanic environments and thyroid disruption–a review focused on as, hg, and co. Sci Total Environ. (2025) 993:180018. doi: 10.1016/j.scitotenv.2025.180018
103. Habakaramo, PM, Boudoire, G, Calabrese, S, Rufino, F, Coyte, RM, and Tedesco, D. Impacts of volcanic hazards on rural communities and adaptative strategies: a case study of the Virunga Volcanic Province (Democratic Republic of Congo). Int J Disaster Risk Reduct. (2023) 86:103566. doi: 10.1016/j.ijdrr.2023.103566
104. Bauer, TK, Giesecke, M, and Janisch, LM. The impact of forced migration on mortality: evidence from German pension insurance records. Demography. (2019) 56:25–47. doi: 10.1007/s13524-018-0742-z
105. Weaver, H, and Roberts, B. Drinking and displacement: a systematic review of the influence of forced displacement on harmful alcohol use. Subst Use Misuse. (2010) 45:2340–55. doi: 10.3109/10826081003793920
106. Heslehurst, N, Brown, H, Pemu, A, Coleman, H, and Rankin, J. Perinatal health outcomes and care among asylum seekers and refugees: a systematic review of systematic reviews. BMC Med. (2018) 16:89. doi: 10.1186/s12916-018-1064-0
107. Shultz, JM, Rechkemmer, A, Rai, A, and McManus, KT. Public health and mental health implications of environmentally induced forced migration. Disaster Med Public Health Prep. (2019) 13:116–22. doi: 10.1017/dmp.2018.27
108. Adger, WN, Fransen, S, Safra de Campos, R, and Clark, WC. Migration and sustainable development. Proc Natl Acad Sci U S A. (2024) 121:e2206193121. doi: 10.1073/pnas.2206193121
109. Andreastuti, SD, Paripurno, ET, Subandriyo, S, Syahbana, DK, and Prayoga, AS. Volcano disaster risk management during crisis: implementation of risk communication in Indonesia. J Appl Volcanol. (2023) 12:3. doi: 10.1186/s13617-023-00129-2
110. Bonadonna, C, Frischknecht, C, Menoni, S, Romerio, F, Gregg, CE, Rosi, M, et al. Integrating hazard, exposure, vulnerability and resilience for risk and emergency management in a volcanic context: the ADVISE model. J Appl Volcanol. (2021) 10:7. doi: 10.1186/s13617-021-00108-5
Keywords: volcanic eruptions, respiratory tract diseases, cardiovascular diseases, eye diseases, skin diseases, mental disorders, public health, environmental exposure
Citation: Simbaña-Rivera K, Endara-Mina J, Jaramillo-Aguilar DS, Mera-Lojano LD, Jimbo-Sotomayor R, Sánchez X, Rodríguez-Pérez MC, Fuentes-Ferrer ME and Boada LD (2025) Mapping the global health burden of volcanic exposure: a scoping review approach. Front. Public Health. 13:1658384. doi: 10.3389/fpubh.2025.1658384
Edited by:
César Leal-Costa, University of Murcia, SpainReviewed by:
Fátima Viveiros, University of the Azores, PortugalJimmy Phuong, University of Washington, United States
Copyright © 2025 Simbaña-Rivera, Endara-Mina, Jaramillo-Aguilar, Mera-Lojano, Jimbo-Sotomayor, Sánchez, Rodríguez-Pérez, Fuentes-Ferrer and Boada. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Katherine Simbaña-Rivera, S2F0aGVyaW5lLnNpbWJhbmFAdWxwZ2MuZXM=
†These authors have contributed equally to this work and share first authorship