 Ying Shen1
Ying Shen1 Xiangyan Lv
Xiangyan Lv- 1Department of Critical Care Medicine, The Second Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, China
- 2Nursing Department, The Second Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, China
Introduction: Organizational silence is prevalent in healthcare and negatively affects nurses and organizational development. This study determined whether coworker support mediates the relationship between organizational silence and work engagement among nurses.
Methods: A quantitative cross-sectional survey was conducted using convenience sampling. The Utrecht Work Engagement Scale-17, Peer Supporting Scale, and Employee Silence Behavior Survey Questionnaire were used to measure the key variables. Descriptive statistics, Pearson correlation analysis, and a structural equation modeling with bootstrap method were performed.
Results: A total of 597 registered nurses from 21 general hospitals in China participated. Nurses’ work engagement (72.09 ± 20.33), coworker support (108.60 ± 20.66), and organizational silence (32.23 ± 11.06) were at moderate levels. Work engagement was positively correlated with coworker support, while both work engagement and coworker support were negatively correlated with organizational silence (all p < 0.01). Mediation analysis indicated that the direct effect value of work engagement on organizational silence was −0.155 (95% CI: −0.217 ~ −0.094, p < 0.001). The indirect effect value of work engagement on organizational silence through coworker support was −0.197 (95% CI: −0.236 ~ −0.160, p < 0.001), accounting for 56.13% of the total effect (−0.351; 95%CI: −0.410 ~ −0.292, p < 0.001).
Conclusion: Work engagement was negatively correlated with organizational silence, in which coworker support played a partial mediating role. It is recommended to enhance the positive impact of work engagement on organizational behavior through strengthening coworker support among nurses, thereby reducing organizational silence, fostering a better work environment, and ultimately enhancing the quality of nursing care.
1 Introduction
Organizational silence is defined as the intentional withholding of ideas, concerns, or information related to organizational improvement by employees (1). This phenomenon is prevalent in healthcare institutions (2). However, due to its nature as an absence of verbal expression and observable behavior, it is often inconspicuous and difficult for managers to detect, making it easily overlooked by the organization. Prolonged organizational silence can exert negative impacts on both individuals and the organization. At the individual level, when nurses’ voices are ignored or their concerns remain unaddressed, they may experience increased burnout (3), decreased job satisfaction (4), lower job performance (5), and even elevated turnover intention (6). At the organizational level, nurses’ silence can hinder managers’ ability to make timely and accurate decisions, reduce the efficiency and quality of organizational decision-making, and impede team development and innovation (7). Moreover, Jones and Durbridge (8) and Okuyama et al. (9) have reported that organizational silence among healthcare staff may jeopardize patient safety. Therefore, understanding the mechanisms that reduce nurses’ organizational silence is crucial for improving nurses’ job satisfaction, decreasing turnover intention, and ensuring the quality of nursing care. Additionally, it plays an important role in promoting hospital innovation and sustainable development within healthcare institutions.
Existing research indicates that the emergence of organizational silence is influenced by multiple factors at the individual [e.g., character, seniority, self-efficacy, work engagement (10, 11)], organizational [e.g., leadership style, organizational climate, coworker support (12–14)], and societal levels [e.g., hierarchy and national culture (15)]. Among these, work engagement and coworker support represent two significant influencing factors. Coworker support refers to the emotional concern, informational assistance, and tangible aid provided by colleagues, constituting a key dimension of social support (16). Meanwhile, work engagement—a positive psychological state characterized by vigor, dedication, and absorption (17)—has been found to be a critical personal resource that enhances performance and career satisfaction (18–20).
Previous studies have demonstrated that both work engagement and coworker support are negatively correlated with organizational silence (21). Furthermore, Li et al. (22), using structural equation modeling, have elucidated the mechanism through which work engagement influences silence behavior: nurses with higher levels of work engagement were more likely to break the silence and proactively voice their opinions and ideas to the organization. It has also been observed that nurses’ work engagement may be closely associated with support from nurse supervisors (23). However, no study to date has examined the role of coworker support in the pathway between work engagement and silence behavior among nurses. Given the importance of teamwork and peer support in nursing practice (24, 25), it is essential to investigate the underlying mechanisms linking these three constructs.
The Conservation of Resources (COR) theory was proposed by American psychologist Hobfoll (26) in 1989. It predicts behavior from a resource-based perspective, explaining not only motivation but also the resource-related conditions under which behavior occurs (27). This theoretical framework provides a valuable basis for understanding individuals’ behavioral choices in resource-limited contexts. Therefore, the present study employed COR theory to explore the relationships among nurses’ work engagement, coworker support, and organizational silence.
First, COR theory categorizes resources into four dimensions: object resources (e.g., shelter and clothing), personal characteristic resources (e.g., personality traits and coping abilities), condition resources (e.g., social relationships, job status, and health), and energy resources (e.g., time, knowledge, and skills) (28). In this study, work engagement and coworker support are conceptualized as personal characteristic and conditional resources, respectively. Second, the basis of COR theory is that individuals are motivated to conserve, maintain, and acquire resources that they value (26). When any of these four resources are threatened or lost, individuals experience stress. Individuals with abundant resources are more capable of acquiring new resources and are more willing to invest them, whereas those with scarce resources tend to adopt defensive strategies to prevent further loss (26). Moreover, the theory explains behavior through the lens of imbalance between resource investment and return: when resource investment fails to yield expected returns, individuals are likely to exhibit negative behavioral responses; conversely, when investment results in satisfactory returns, individuals are motivated to engage in positive behaviors (26).
Based on COR theory, this study proposes the following hypotheses: (1) Nurses with more personal characteristic resources (higher work engagement) are less likely to adopt resource-conservation strategies (organizational silence). Thus, work engagement is negatively associated with organizational silence. (2) Nurses with more conditional resources (higher coworker support) are less likely to adopt resource-conservation strategies (organizational silence). Thus, coworker support is negatively associated with organizational silence. (3) Nurses with abundant personal characteristic resources (higher work engagement) are more likely to acquire new conditional resources (higher coworker support). Thus, work engagement is positively associated with coworker support. (4) When nurses’ investment of personal characteristic resources (work engagement) leads to conditional resource returns (coworker support), they are more likely to engage in proactive behaviors such as speaking up; conversely, inadequate resource returns or losses may increase the likelihood of organizational silence. Thus, coworker support serves as a mediating factor between work engagement and organizational silence. The theoretical framework of this study is presented in Figure 1.
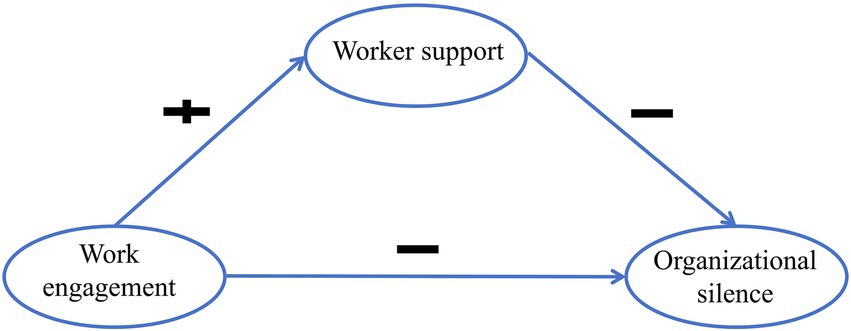
Figure 1. Hypothetical model of this study.
The aim of this study was to examine the relationships among nurses’ work engagement, coworker support, and organizational silence, and to verify the mediating effect of coworker support between work engagement and organizational silence.
2 Methods
2.1 Study design and setting
This quantitative cross-sectional study was conducted between January and March 2024 at 21 general hospitals in Hangzhou, China.
2.2 Participants
Registered nurses from the 21 hospitals were recruited through convenience sampling. Eligible participants were those aged 18 years or older and holding at least an associate nursing degree. Nurses who were interns, on rotation or standardized training, pursuing further education, or on sick or maternity leave were excluded from the study.
2.3 Sample size
The sample size was determined based on structural equation model (SEM) parameter considerations. In the hypothesized model, we estimated 11 variance parameters, 4 direct and indirect path coefficients among latent variables, and 8 factor loadings, yielding a total of 23 free parameters. Following the rule of at least 10 observations per free parameter for SEM (29, 30), a minimum of 230 participants was required. Considering 10% of invalid response rate, the final required sample size was set at 256.
2.4 Measurements
1. Demographic information: demographic characteristics encompassed sex, age, educational background, department, professional title, position, and marital status.
2. The Chinese version of Utrecht Work Engagement Scale (UWES-17): the Chinese version of UWES-17, adapted by Zhang and Gan (31), was used to assess nurses’ work engagement in this study. The Chinese version includes three subscales: vigor (6 items), dedication (5 items), and absorption (6 items), using a 7-point Likert scale, with higher scores indicating higher levels of work engagement. The overall Cronbach’s α coefficient of the scale was approximately 0.9 (31). In this study, the Cronbach’s α of the scale was 0.954.
3. Peer Supporting Scale (PSS): this scale was developed by Ye et al. (32), based on the support scale created by Greene et al. (54), and adapted for the Chinese nursing population. The scale consists of two parts. Scale A is the Nurse Supervisor Support Scale, comprising 9 items, which reflects nurses’ evaluation of the support provided by their nurse supervisors. Scale B, which contains 21 items, measures nurses’ perceptions of peer support among colleagues and is subdivided into seven dimensions: subjective support, collaboration, empathy, awareness enhancement, goal setting, action planning, and process management evaluation. Both Scale A and B use a 5-point Likert scale, where higher scores indicate higher perceived support from colleagues. The Cronbach’s α coefficients for Scale A and Scale B are 0.922 and 0.959, respectively (32). In this study, the Cronbach’s α of the scale was 0.991.
4. Employee Silence Behavior Survey Questionnaire: this questionnaire, developed by Zheng et al. (33) in 2008 for the Chinese context, includes three dimensions: acquiescent silence, defensive silence, and disregardful silence (4 items per dimension). A 5-point Likert scale is used, with higher scores indicating a greater level of organizational silence among employees. The overall Cronbach’s α coefficient of the questionnaire was 0.89, and structural validity analysis showed a Kaiser-Meyer-Olkin (KMO) measure of 0.895 and a CFI of 0.94. In this study, the Cronbach’s α of the scale was 0.949.
2.5 Data collection and quality control
Data were collected between January and March 2024. The research team first contacted the nursing departments of 21 general hospitals in Hangzhou to explain the study objectives and ethical principles. After obtaining administrative approval, a designated nurse manager in each hospital assisted in distributing the online questionnaire link (created via the “Wenjuanxing” platform) to nurses through departmental WeChat groups. The survey included information about the study, an informed consent statement, and instructions for completion. Participation was voluntary and anonymous.
To ensure data quality, the questionnaire required completion of all items and limited each IP address to one submission. All responses were completed independently by participants. Two researchers reviewed and cleaned the data, excluding invalid questionnaires (e.g., those with repetitive answers or unrealistically short completion times).
2.6 Statistical analysis
Data were analyzed using SPSS 23.0 and AMOS 26.0. Categorical variables were presented as frequencies and percentages, while continuous variables with normal distribution were expressed as means and standard deviations. Pearson correlation analysis was used to examine the relationship between nurse work engagement, coworker support, and organizational silence.
SEM was used to test the hypothesized model (Figure 1), and mediating effects were assessed through bootstrap method with 5,000 samples and 95% bias-corrected confidence intervals (34). Confirmatory factor analysis (CFA) evaluated the reliability and validity of the measurement model. Composite reliability (CR) values above 0.70 indicated good internal consistency (35), while average variance extracted (AVE) values above 0.50 supported convergent validity (36). Discriminant validity was confirmed when the square root of each construct’s AVE exceeded its correlations with other constructs (37).
Model fit was assessed using multiple indices: χ2/df < 3, GFI, AGFI, and IFI > 0.90, and RMSEA < 0.08 indicated acceptable fit (38). Sociodemographic variables (age, education, and department) were controlled for in the mediation models. Statistical significance was set at p < 0.05.
3 Results
3.1 Participants
A total of 613 questionnaires were collected in this study, of which 597 were valid, resulting in an effective return rate of 97.4%. Table 1 presents the characteristics of the participants. Among the 597 nurses included in this study, 527 (88.3%) were female, and 70 (11.7%) were male, with a mean age of 31.5 ± 6.9 years (range: 20–54 years). The majority of participants held a bachelor’s degree (84.9%). Participants were primarily from general wards (48.9%) and intensive care units (30.0%), with smaller proportions from outpatient clinics (9.4%), emergency departments (6.7%), and operating rooms (5.0%). Most nurses held no official position (80.9%), and their primary title was senior nurse (45.2%). Additionally, 56.6% of the nurses were married.

Table 1. Baseline characteristics of the participants (n = 597).
3.2 Nurses’ scores on work engagement, coworker support, and organizational silence
The results of the self-assessment scale indicated that the total score for nurses’ organizational silence was 32.23 ± 11.06. And the mean item score was 2.69 ± 0.92. Compared to the midpoint value of 3, nurses’ organizational silence was at a moderate level. Among the dimensions, acquiescent silence had the highest mean score, while disregardful silence had the lowest. The total scores for nurses’ work engagement and coworker support were 72.09 ± 20.33 and 108.60 ± 20.66, respectively, which were also at a medium level. The specific scores are presented in Table 2.
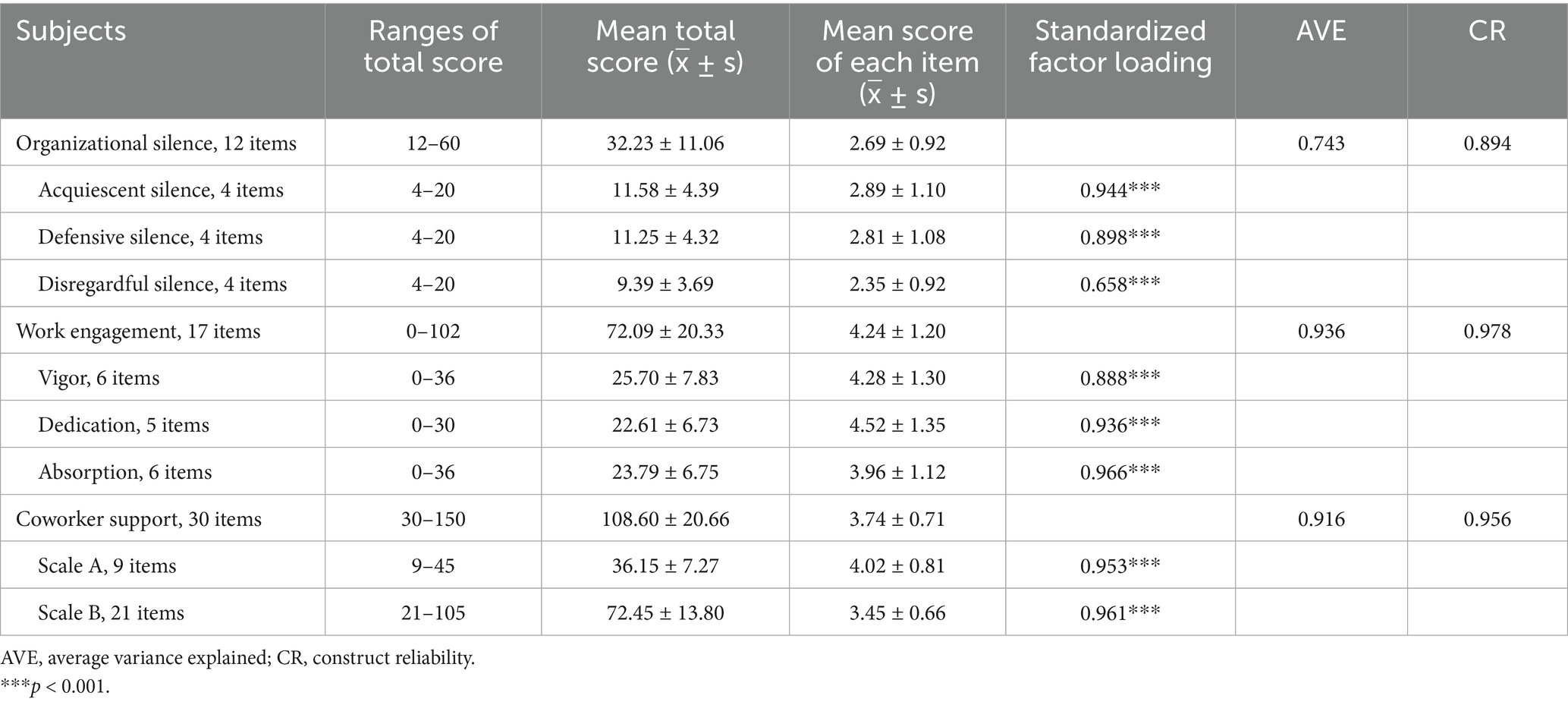
Table 2. Work engagement, coworker support, and organizational silence scores among 597 nurses.
3.3 Correlation analysis of nurses’ work engagement, coworker support, and organizational silence
Correlation analysis revealed that nurses’ work engagement was significantly negatively correlated with organizational silence (r = −0.498, p < 0.01). Similarly, coworker support was significantly negatively correlated with the organizational silence (r = −0.604, p < 0.01). Moreover, there was a significant positive correlation between work engagement and coworker support (r = 0.511, p < 0.01). The trend in the correlations between the dimensions was consistent with the trend between the total scores of the scales (as shown in Table 3).
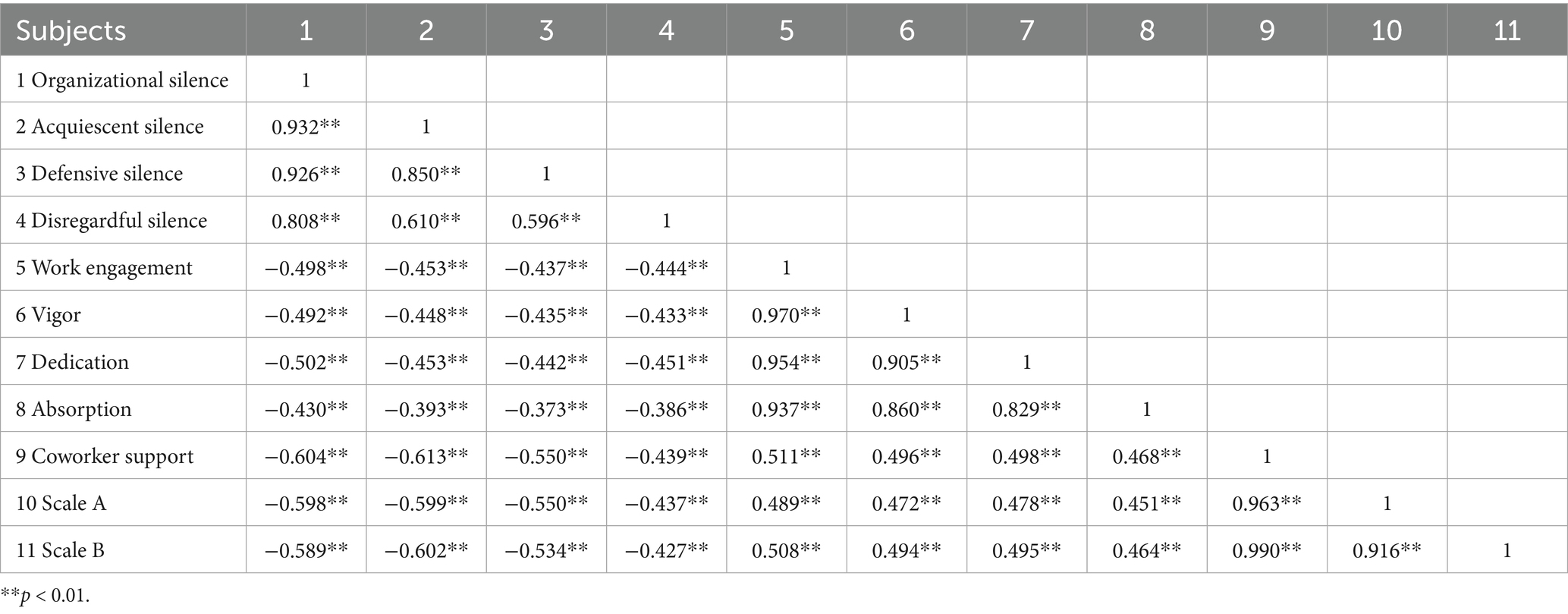
Table 3. Correlation analysis of nurses’ work engagement, coworker support, and organizational silence.
3.4 Mediation analysis of nurses’ work engagement, coworker support, and organizational silence
3.4.1 Reliability and validity evidence
The composite reliability and convergent validity of the latent variables in the measurement model are shown in Table 2. Each latent variable had a CR greater than 0.70, indicating good internal consistency. All standardized factor loadings of the observational variables were greater than 0.50, and the AVE values for each latent variable exceeded 0.50, demonstrating acceptable convergent validity. As shown in Supplementary Table S1, the absolute values of the correlation coefficients between latent variables were all below 0.7, and the square root of each latent variable’s AVE was greater than its correlations with other latent variables, indicating good discriminant validity. Overall, these results suggest that the latent variables were successfully derived from their corresponding observed variables.
3.4.2 Model fit
The measurement model developed for this study is illustrated in Figure 2. In the measurement model, the fit indices were as follows: χ2/df = 2.687 (<3), GFI = 0.982, AGFI = 0.961, IFI = 0.994 (all >0.9), and RMSEA = 0.053 (<0.08), indicating that the model demonstrated a good fit and accurately reflected the latent variables. Similarly, the structural model also showed satisfactory fit indices: χ2/df = 2.703, GFI = 0.981, AGFI = 0.961, IFI = 0.994, and RMSEA = 0.053. These results suggest that both the measurement and structural models achieved good overall fit. The established model structure is reasonable and effectively explains the path relationships among the variables.
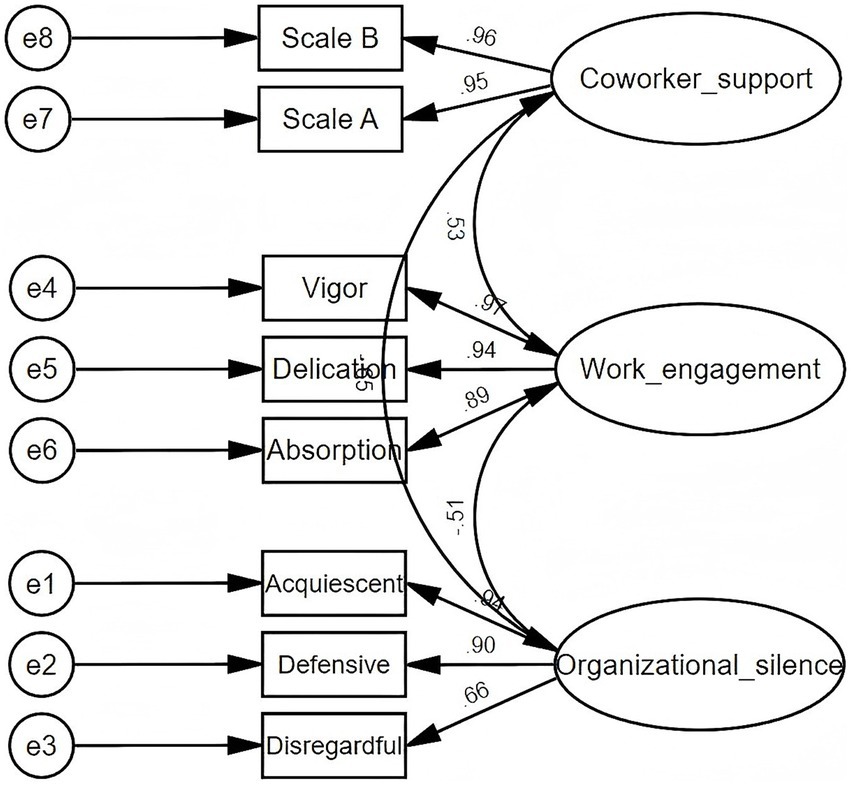
Figure 2. Confirmatory factor analysis of work engagement, coworker support, and organizational silence.
3.4.3 Hypothesis testing
The mediating role of coworker support was further examined by developing SEM through AMOS. SEM was constructed with work engagement as the independent variable, organizational silence as the dependent variable, and coworker support as the mediator. As shown in Figure 3, Table 4, work engagement was directly and negatively related to organizational silence (β = −0.22, p < 0.001). Work engagement was positively related to coworker support (β = 0.53, p < 0.001), while coworker support was negatively related to organizational silence (β = −0.54, p < 0.001). Additionally, coworker support partially mediated the relationship between work engagement and organizational silence. And the indirect effect (−0.197) accounted for 56.13% of the total effect (−0.351). After adjusting for the sociodemographic factors of age, education level, and department of nurses, the magnitude of the effects changed only minimally (<10%) and statistical significance remained unchanged, confirming the robustness of the results (Table 4). These findings align with the hypotheses presented in Figure 1.
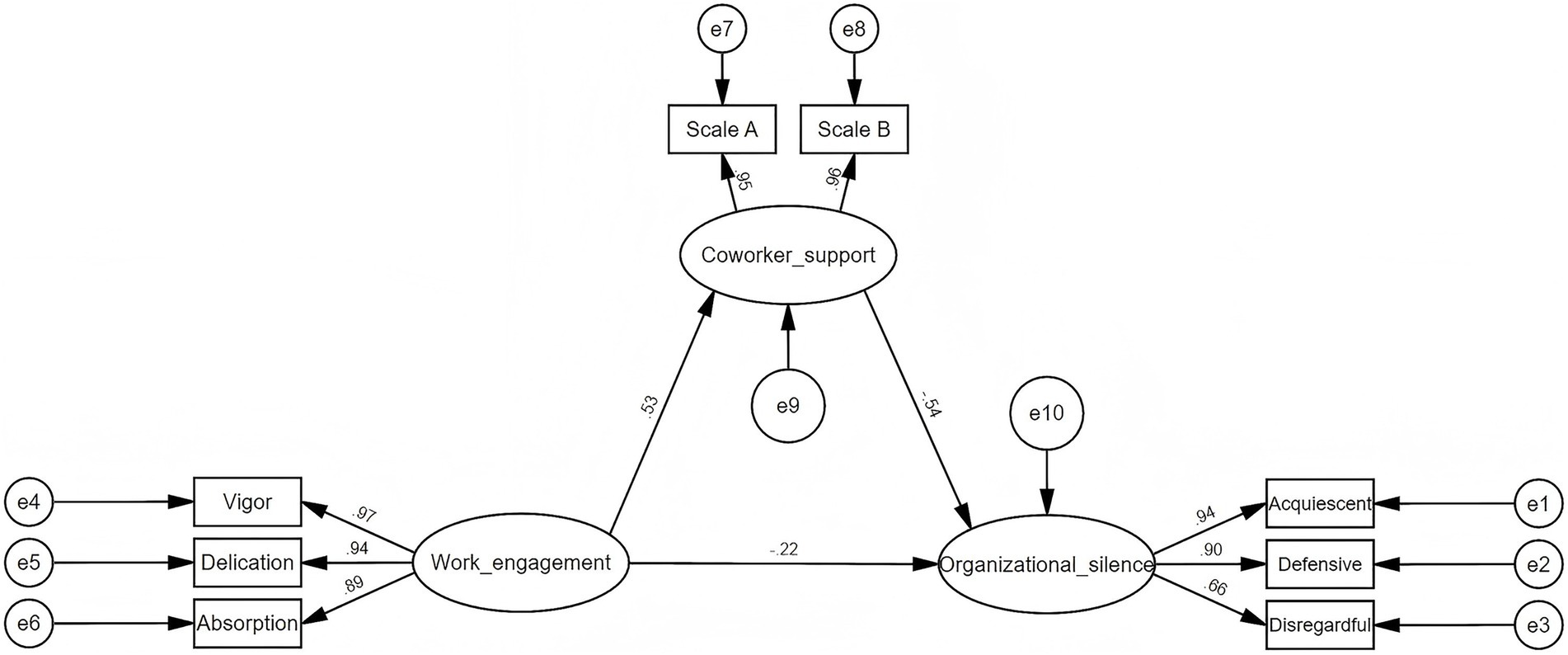
Figure 3. The structural equation model of work engagement, coworker support, and organizational silence.
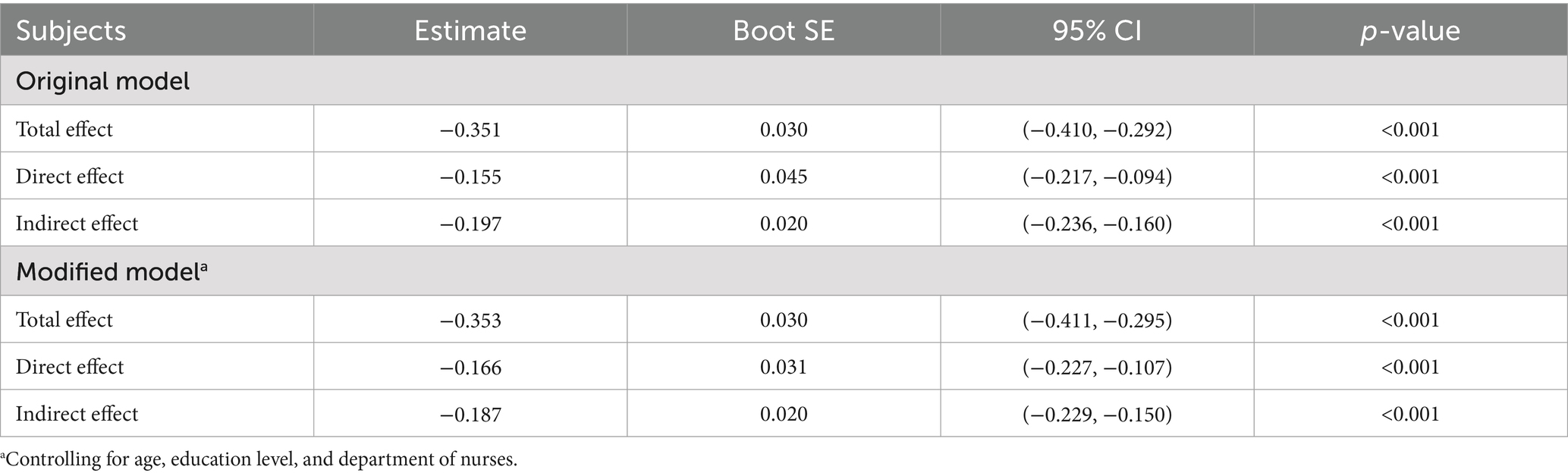
Table 4. Mediation analysis of nurses’ work engagement, coworker support, and organizational silence.
4 Discussion
This study surveyed 597 nurses from 21 general hospitals in China to explore the relationship between work engagement, coworker support, and organizational silence. Consistent with our hypothesis, both work engagement and coworker support were negatively correlated with organizational silence, while work engagement was positively associated with coworker support. Moreover, coworker support was found to partially mediate the relationship between work engagement and organizational silence. These findings offer a novel theoretical perspective on organizational silence behavior among nurses and provide an evidence-based foundation for nursing management practices.
Wen et al. (39) conducted a meta-analysis involving nurses from China, South Korea, and Turkey, and reported that the average level of organizational silence among 13,394 nurses was moderate. Similarly, the nurses in this study also exhibited a moderate level of organizational silence. In contrast, studies conducted among nurses in the Philippines (40) and Egypt (41) reported slightly higher levels of organizational silence, which may be attributed to cultural or methodological differences. These findings suggested that organizational silence is a widespread phenomenon across hospitals in different countries (10). Further analysis of the three dimensions of organizational silence revealed that the mean scores ranked from highest to lowest as follows: acquiescent silence, defensive silence, and disregardful silence. This indicated that nurses’ silence is not a blind or passive behavior but rather a rational and deliberate response.
With the β = −0.22 and p < 0.001 values, the SEM results indicated a significant negative association between work engagement and organizational silence among nurses. Similar findings were reported by Lv et al. (21), who concluded that nurses with lower outpatient service, contract employment, fewer years of experience, and less work engagement were more likely to exhibit silence behavior. Conversely, other studies have interpreted this relationship in the opposite direction, suggesting that organizational silence negatively affects nurses’ work engagement. For example, from the perspective of the Job Demand-Resource model, Zhu et al. (11) argued that a culture of organizational silence restricts employees’ participation and autonomy (job demands), which may reduce their access to job resources and, consequently, lead to lower work engagement. Likewise, Yağar and Dökme Yağar (5) reported that a low-silence environment contributes to higher engagement and job performance.
Drawing on Hobfoll’s COR theory, this study provides new evidence supporting the idea that higher work engagement may help break organizational silence among nurses. We believed that highly engaged nurses tend to invest substantial cognitive and emotional resources in their work, forming a strong professional identity characterized by vigor, dedication, and absorption. This positive psychological state not only enhances professional competence but also strengthens the psychological safety required to express opinions, thereby reducing the tendency toward silence (3, 42). Supporting this view, Kaya and Eskin Bacaksiz (43) found that positive psychological capital is negatively associated with organizational silence, while numerous studies have shown a significant positive correlation between positive psychological capital and work engagement (44–46).
Another important finding of this study is that coworker support played a mediating role—accounting for 56.13% of the total effect—between work engagement and organizational silence. The positive association between work engagement and coworker support has been supported by previous research (23). Specifically, nurses with higher work engagement tend to demonstrate stronger responsibility, motivation, and collaboration, making them more likely to develop reciprocal social support networks and receive coworker support (47). However, few studies have examined the direct link between coworker support and organizational silence. To our knowledge, this may be the first study using SEM to confirm that coworker support is significantly and negatively related to nurses’ organizational silence and mediates the relationship between work engagement and silence behavior. Although prior research has not directly tested this pathway, existing evidence indicates that coworker support mediates the relationship between work engagement and proactive career behaviors (48). And higher coworker support is associated with lower burnout from work-related stressors (49). Combined with COR theory, these findings suggest that nurses can strengthen their ability to cope with stress by accumulating resources including coworker support, thereby reducing defensive behaviors such as organizational silence (26).
4.1 Theoretical implications
This study makes an important contribution to the theory of organizational behavior in nursing. It found that Chinese nurses exhibited a moderate level of organizational silence, providing new empirical evidence for the cross-cultural universality of this phenomenon. Most importantly, it is the first study to verify the mediating role of coworker support between work engagement and organizational silence, suggesting that highly engaged nurses can reduce silence by building reciprocal support networks. Unlike previous studies that mainly focused on the impact of toxic workplace environments on employees (50), this research reveals a pathway for reducing silence behavior among nurses and highlights the importance of horizontal coworker support in improving communication and fostering teamwork. In addition, by applying COR theory to explain nurses’ organizational silence, this study extends its applicability to the nursing context and offers a new theoretical lens for understanding the psychological mechanisms underlying silence behavior.
4.2 Practical implications
The findings of this study provide actionable strategies to reduce organizational silence among nurses. Firstly, healthcare institutions need to strengthen coworker support networks, including support from nurse supervisors and peers. This can be achieved by creating regular communication platforms, anonymous feedback channels, or appointing a suitable nurse as a liaison to alleviate nurses’ concerns about speaking up in a hierarchical culture (1, 51). Secondly, optimizing resource allocation and working policy is crucial. High work engagement among nurses, when not accompanied by sufficient resource support, may result in organizational silence due to excessive resource depletion. Managers can reduce overload by implementing flexible scheduling to prevent emotional resource exhaustion (52). Finally, incentive mechanisms and cultural reshaping need to be advanced simultaneously. Consistent with this study, research has shown that acquiescent silence is the most prevalent among nurses, which is closely linked to the passive compliance culture within organizations (10). Hospitals can foster an open and inclusive team atmosphere by recognizing proactive contributors or establishing a “no-punishment” error reporting system. For instance, Lee et al. (53) found in their study of Korean hospitals that nurse managers could create more supportive environments for nurses’ outspoken behaviors by inviting and valuing staff opinions and by helping physicians and senior nurses recognize the importance of all nurses’ voices.
4.3 Limitations
This study has several limitations. Although probability sampling is more desirable for ensuring representativeness, it would have required full administrative support across 21 general hospitals to access complete nursing rosters and considerable time and manpower for random or stratified selection, which was beyond the available resources of this unfunded project. Convenience sampling was therefore adopted in this study, as it allowed us to achieve an adequate sample size while maintaining sample heterogeneity across hospitals, departments, and professional ranks. In addition, potential bias was mitigated by controlling for confounding variables in the structural equation model. Second, all data were collected via self-reported questionnaires at a single time point, raising concerns about common method bias. While validated scales and anonymous participation were used to minimize this risk, the possibility of inflated associations among variables cannot be fully excluded. Third, the cross-sectional design prevents causal inferences among the variables. Future studies using probability-based sampling, larger and more diverse samples, multi-source data, and longitudinal designs are recommended to validate and extend these findings.
5 Conclusion
Work engagement was negatively associated with organizational silence, in which coworker support played a partial mediating role. It is recommended to enhance the positive impact of work engagement on organizational behavior through strengthening coworker support among nurses, thereby reducing organizational silence, fostering a better work environment, and ultimately enhancing the quality of nursing care and employee satisfaction.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The requirement of ethical approval was waived by the Ethics Committee of the Second Affiliated Hospital of Zhejiang Chinese Medical University for the studies involving humans. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
YS: Methodology, Conceptualization, Writing – review & editing, Writing – original draft, Investigation. XC: Writing – review & editing, Conceptualization, Writing – original draft. HZ: Formal analysis, Data curation, Writing – review & editing. XL: Conceptualization, Writing – review & editing, Data curation, Formal analysis.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1660100/full#supplementary-material
References
1. Montgomery, A, Lainidi, O, Johnson, J, Creese, J, Baathe, F, Baban, A, et al. Employee silence in health care: charting new avenues for leadership and management. Health Care Manag Rev. (2023) 48:52–60. doi: 10.1097/hmr.0000000000000349
2. Harmanci Seren, AK, Topcu, İ, Eskin Bacaksiz, F, Unaldi Baydin, N, Tokgoz Ekici, E, and Yildirim, A. Organisational silence among nurses and physicians in public hospitals. J Clin Nurs. (2018) 27:1440–51. doi: 10.1111/jocn.14294
3. Lee, SE, Seo, JK, and Squires, A. Voice, silence, perceived impact, psychological safety, and burnout among nurses: a structural equation modeling analysis. Int J Nurs Stud. (2024) 151:104669. doi: 10.1016/j.ijnurstu.2023.104669
4. Parlar Kılıç, S, Öndaş Aybar, D, and Sevinç, S. Effect of organizational silence on the job satisfaction and performance levels of nurses. Perspect Psychiatr Care. (2021) 57:1888–96. doi: 10.1111/ppc.12763
5. Yağar, F, and Dökme Yağar, S. The effects of organizational silence on work engagement, intention to leave and job performance levels of nurses. Work. (2023) 75:471–8. doi: 10.3233/wor-210192
6. Çaylak, E, and Altuntaş, S. Organizational silence among nurses: the impact on organizational cynicism and intention to leave work. J Nurs Res. (2017) 25:90–8. doi: 10.1097/jnr.0000000000000139
7. Dellve, L, and Jendeby, MK. Silence among first-line managers in eldercare and their continuous improvement work during Covid-19. Inquiry. (2022) 59:469580221107052. doi: 10.1177/00469580221107052
8. Jones, C, and Durbridge, M. Culture, silence and voice: the implications for patient safety in the operating theatre. J Perioper Pract. (2016) 26:281–4. doi: 10.1177/175045891602601204
9. Okuyama, A, Wagner, C, and Bijnen, B. Speaking up for patient safety by hospital-based health care professionals: a literature review. BMC Health Serv Res. (2014) 14:61. doi: 10.1186/1472-6963-14-61
10. Zou, J, Zhu, X, Fu, X, Zong, X, Tang, J, Chi, C, et al. The experiences of organizational silence among nurses: a qualitative meta-synthesis. BMC Nurs. (2025) 24:31. doi: 10.1186/s12912-024-02636-y
11. Zhu, W, Liao, H, and Wu, Q. Organizational silence and work engagement among Chinese clinical nurses: the mediating role of career calling. J Nurs Manag. (2025) 2025:7522633. doi: 10.1155/jonm/7522633
12. Hu, G, Guo, Z, Wang, Y, and Wang, L. The differential association between leadership styles and organizational silence in a sample of Chinese nurses: a multi-Indicator and multicause study. J Nurs Manag. (2025) 2025:9626175. doi: 10.1155/jonm/9626175
13. De Los Santos, JAA, Rosales, RA, Falguera, CC, Firmo, CN, Tsaras, K, and Labrague, LJ. Impact of organizational silence and favoritism on nurse’s work outcomes and psychological well-being. Nurs Forum. (2020) 55:782–92. doi: 10.1111/nuf.12496
14. Morrow, KJ, Gustavson, AM, and Jones, J. Speaking up behaviours (safety voices) of healthcare workers: a metasynthesis of qualitative research studies. Int J Nurs Stud. (2016) 64:42–51. doi: 10.1016/j.ijnurstu.2016.09.014
15. Lee, SE, Choi, J, Lee, H, Sang, S, Lee, H, and Hong, HC. Factors influencing nurses' willingness to speak up regarding patient safety in East Asia: a systematic review. Risk Manag Healthc Policy. (2021) 14:1053–63. doi: 10.2147/rmhp.s297349
16. Winning, AM, Merandi, JM, Lewe, D, Stepney, LMC, Liao, NN, Fortney, CA, et al. The emotional impact of errors or adverse events on healthcare providers in the NICU: the protective role of coworker support. J Adv Nurs. (2018) 74:172–80. doi: 10.1111/jan.13403
17. Mukaihata, T, Kato, Y, Swa, T, and Fujimoto, H. Work engagement of psychiatric nurses: a scoping review protocol. BMJ Open. (2022) 12:e062507. doi: 10.1136/bmjopen-2022-062507
18. Hetzel-Riggin, MD, Swords, BA, Tuang, HL, Deck, JM, and Spurgeon, NS. Work engagement and resiliency impact the relationship between nursing stress and burnout. Psychol Rep. (2020) 123:1835–53. doi: 10.1177/0033294119876076
19. Eguchi, H, Inoue, A, Kachi, Y, Miyaki, K, and Tsutsumi, A. Work engagement and work performance among Japanese workers: a 1-year prospective cohort study. J Occup Environ Med. (2020) 62:993–7. doi: 10.1097/jom.0000000000001977
20. Rafiq, M, Farrukh, M, Attiq, S, Shahzad, F, and Khan, I. Linking job crafting, innovation performance, and career satisfaction: the mediating role of work engagement. Work. (2023) 75:877–86. doi: 10.3233/wor-211363
21. Lv, X, Gu, Y, Solomon, OM, Shen, Y, Ren, Y, and Wei, Y. Status and influencing factors of nurses’ organizational silence in general hospitals in eastern coastal cities of China. BMC Nurs. (2024) 23:757. doi: 10.1186/s12912-024-02419-5
22. Li, Y, Zhou, J, Yang, N, Pan, Y, Tian, XX, Nie, WL, et al. Study on influence of nurses work engagement based on structural equation model on organization silence. Chinese Nurs Res. (2014) 28:1181–3. doi: 10.3969/j.issn.1009-6493.2014.10.012
23. Poulsen, MG, Khan, A, Poulsen, EE, Khan, SR, and Poulsen, AA. Work engagement in cancer care: the power of co-worker and supervisor support. Eur J Oncol Nurs. (2016) 21:134–8. doi: 10.1016/j.ejon.2015.09.003
24. Andrews, MC, Woolum, A, Mesmer-Magnus, J, Viswesvaran, C, and Deshpande, S. Reducing turnover intentions among first-year nurses: the importance of work centrality and coworker support. Health Serv Manag Res. (2024) 37:88–98. doi: 10.1177/09514848231165891
25. De Regge, M, Van Baelen, F, Aerens, S, Deweer, T, and Trybou, J. The boundary-spanning behavior of nurses: the role of support and affective organizational commitment. Health Care Manag Rev. (2020) 45:130–40. doi: 10.1097/hmr.0000000000000210
26. Hobfoll, SE. Conservation of resources. A new attempt at conceptualizing stress. Am Psychol. (1989) 44:513–24. doi: 10.1037//0003-066x.44.3.513
27. Deng, H, Coyle-Shapiro, J, and Yang, Q. Beyond reciprocity: a conservation of resources view on the effects of psychological contract violation on third parties. J Appl Psychol. (2018) 103:561–77. doi: 10.1037/apl0000272
28. Prapanjaroensin, A, Patrician, PA, and Vance, DE. Conservation of resources theory in nurse burnout and patient safety. J Adv Nurs. (2017) 73:2558–65. doi: 10.1111/jan.13348
29. Wolf, EJ, Harrington, KM, Clark, SL, and Miller, MW. Sample size requirements for structural equation models: an evaluation of power, Bias, and solution propriety. Educ Psychol Meas. (2013) 76:913–34. doi: 10.1177/0013164413495237
30. Demsash, AW, Kalayou, MH, and Walle, AD. Health professionals’ acceptance of mobile-based clinical guideline application in a resource-limited setting: using a modified UTAUT model. BMC Med Educ. (2024) 24:689. doi: 10.1186/s12909-024-05680-z
31. Zhang, YW, and Gan, YQ. The Chinese version of Utrecht work engagement scale: an examination of reliability and validity. Chin J Clin Psychol. (2005) 13:268–81. doi: 10.3969/j.issn.1005-3611.2005.03.005
32. Ye, T, Xue, J, He, M, Gu, J, Lin, H, Xu, B, et al. Psychosocial factors affecting artificial intelligence adoption in health care in China: cross-sectional study. J Med Internet Res. (2019) 21:e14316. doi: 10.2196/14316
33. Zheng, XT, Ke, JL, Shi, JT, and Zheng, XS. Measurement of employee silence and the impact of trust on it in the Chinese context. Acta Psychol Sin. (2008) 40:219–27.
34. Zewude, GT, Gosim, D, Dawed, S, Nega, T, Tessema, GW, and Eshetu, AA. Investigating the mediating role of emotional intelligence in the relationship between internet addiction and mental health among university students. PLOS Digit Health. (2024) 3:e0000639. doi: 10.1371/journal.pdig.0000639
35. Dias, SB, Oikonomidis, Y, Diniz, JA, Baptista, F, Carnide, F, Bensenousi, A, et al. Users’ perspective on the AI-based smartphone PROTEIN app for personalized nutrition and healthy living: a modified technology acceptance model (mTAM) approach. Front Nutr. (2022) 9:898031. doi: 10.3389/fnut.2022.898031
36. Wang, X, and Leng, X. Dialogue pathways and narrative analysis in health communication within the social media environment: an empirical study based on user behavior-a case study of China. Front Public Health. (2025) 13:1649120. doi: 10.3389/fpubh.2025.1649120
37. Youssef, N, Saleeb, M, Gebreal, A, and Ghazy, RM. The Internal Reliability and Construct Validity of the Evidence-Based Practice Questionnaire (EBPQ): Evidence from Healthcare Professionals in the Eastern Mediterranean Region. Healthcare (Basel, Switzerland). (2023) 11:2168. doi: 10.3390/healthcare11152168
38. Zhang, Q, Huang, F, Zhang, L, Li, S, and Zhang, J. The effect of high blood pressure-health literacy, self-management behavior, self-efficacy and social support on the health-related quality of life of Kazakh hypertension patients in a low-income rural area of China: a structural equation model. BMC Public Health. (2021) 21:1114. doi: 10.1186/s12889-021-11129-5
39. Wen, S, Ji, W, Gao, D, Lu, X, Zhao, T, Gao, J, et al. Heeding the voices of nurses: a systematic review and meta-analysis of organizational silence levels among clinical nurses. BMC Nurs. (2025) 24:552. doi: 10.1186/s12912-025-03138-1
40. Labrague, LJ, and De Los Santos, JA. Association between nurse and hospital characteristics and organisational silence behaviours in nurses: a cross-sectional study. J Nurs Manag. (2020) 28:2196–204. doi: 10.1111/jonm.13101
41. Farghaly Abdelaliem, SM, and Abou Zeid, MAG. The relationship between toxic leadership and organizational performance: the mediating effect of nurses’ silence. BMC Nurs. (2023) 22:4. doi: 10.1186/s12912-022-01167-8
42. Inoue, A, Eguchi, H, Kachi, Y, and Tsutsumi, A. Perceived psychosocial safety climate, psychological distress, and work engagement in Japanese employees: a cross-sectional mediation analysis of job demands and job resources. J Occup Health. (2023) 65:e12405. doi: 10.1002/1348-9585.12405
43. Kaya, G, and Eskin Bacaksiz, F. The relationships between nurses’ positive psychological capital, and their employee voice and organizational silence behaviors. Perspect Psychiatr Care. (2022) 58:1793–800. doi: 10.1111/ppc.12990
44. Tian, L, Wu, A, Li, W, Huang, X, Ren, N, Feng, X, et al. Relationships between perceived organizational support, psychological capital and work engagement among Chinese infection control nurses. Risk Manag Healthc Policy. (2023) 16:551–62. doi: 10.2147/rmhp.s395918
45. Xu, J. The interplay between Chinese EFL teachers’ positive psychological capital and their work engagement. Heliyon. (2023) 9:e13151. doi: 10.1016/j.heliyon.2023.e13151
46. Saleem, MS, Isha, ASN, Yusop, YM, Awan, MI, and Naji, GMA. The role of psychological capital and work engagement in enhancing construction workers' safety behavior. Front Public Health. (2022) 10:810145. doi: 10.3389/fpubh.2022.810145
47. Mori, T, Nagata, T, Odagami, K, Nagata, M, Adi, NP, and Mori, K. Workplace social support and work engagement among Japanese workers: a nationwide cross-sectional study. J Occup Environ Med. (2023) 65:e514–9. doi: 10.1097/jom.0000000000002876
48. Zhang, J. The mediating effect of coworker support on the relationship between work engagement and proactive work behavior among nurses. J Nurses Train. (2023) 38:1191–5. doi: 10.16821/j.cnki.hsjx.2023.13.009
49. Jenkins, R, and Elliott, P. Stressors, burnout and social support: nurses in acute mental health settings. J Adv Nurs. (2004) 48:622–31. doi: 10.1111/j.1365-2648.2004.03240.x
50. Rasool, SF, Wang, M, Tang, M, Saeed, A, and Iqbal, J. How toxic workplace environment effects the employee engagement: the mediating role of organizational support and employee wellbeing. Int J Environ Res Public Health. (2021) 18:18. doi: 10.3390/ijerph18052294
51. Liu, T, and Xu, M. Research progress and enlightenment of influence factors of nurses’ organizational silence. Chin Nurs Manag. (2019) 10:712–5. doi: 10.3969/j.issn.1672-1756.2019.05.014
52. Clendon, J, and Walker, L. Nurses aged over 50 and their perceptions of flexible working. J Nurs Manag. (2016) 24:336–46. doi: 10.1111/jonm.12325
53. Lee, SE, Dahinten, VS, Ji, H, Kim, E, and Lee, H. Motivators and inhibitors of nurses' speaking up behaviours: a descriptive qualitative study. J Adv Nurs. (2022) 78:3398–408. doi: 10.1111/jan.15343
Keywords: organizational silence, work engagement, coworker support, mediating role, nurses
Citation: Shen Y, Chen X, Zhang H and Lv X (2025) The work engagement and organizational silence among nurses: the mediating role of coworker support. Front. Public Health. 13:1660100. doi: 10.3389/fpubh.2025.1660100
Edited by:
Federica Vallone, University of Naples Federico II, ItalyReviewed by:
Jacopo Fiorini, Policlinico Tor Vergata, ItalyEdmund Nana Kwame Nkrumah, Nobel International Business School, Ghana
Copyright © 2025 Shen, Chen, Zhang and Lv. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiangyan Lv, MTk5ODQwMjBAemNtdS5lZHUuY24=