 Xin Hua1†
Xin Hua1† Zhi-Qing Long2†
Zhi-Qing Long2† Si-Fen Wang2†
Si-Fen Wang2† Fei Xu1Meng-Di Wang1
Fei Xu1Meng-Di Wang1 Jia-Yi Chen1Yu-Ling Zhang3*Wei-Qiong Ni1*
Jia-Yi Chen1Yu-Ling Zhang3*Wei-Qiong Ni1* Yun-Sheng Gao1*
Yun-Sheng Gao1*- 1Department of Radiation Oncology, Shanghai Jiao Tong University Medical School Affiliated Ruijin Hospital, Shanghai, China
- 2State Key Laboratory of Oncology in South China, Guangdong Key Laboratory of Nasopharyngeal Carcinoma Diagnosis and Therapy, Sun Yat-sen University Cancer Center, Guangzhou, China
- 3Department of Endocrinology, Jiangxi Provincial People's Hospital, The First Affiliated Hospital of Nanchang Medical College, Nanchang, China
Background: Recent studies indicate that the novel lymphocyte–C-reactive protein ratio (LCR) is strongly associated with the survival of various tumors, but its prognostic value in nasopharyngeal carcinoma (NPC) is understudied. This study aimed to explore the relationship between LCR and overall survival (OS) in NPC and develop a predictive model.
Methods: A total of 841 NPC patients who received concurrent chemoradiotherapy (CCRT) between January 2010 and December 2014 were retrospectively enrolled and randomly divided into a training cohort (n = 589) and a validation cohort (n = 252), and 122 patients between January 2015 and March 2015 were included as an additional validation cohort. Univariate and multivariate Cox analyses were performed to identify variables associated with OS and construct a predictive nomogram. The predictive accuracy of the nomogram was evaluated and independently validated.
Results: The LCR score differentiated NPC patients into two groups with distinct prognoses (HR = 0.53; 95% CI: 0.32–0.89, P = 0.014). Multivariate analysis showed that age, T stage, N stage, EBV-DNA status, and LCR score were independently associated with OS, and a predictive nomogram was developed. The nomogram had a good performance for the prediction of OS [C-index = 0.770 (95% CI: 0.675–0.864)]. and outperformed the traditional staging system [C-index = 0.589 (95% CI: 0.385–0.792)]. The results were internally and additionally validated using independent cohorts.
Conclusion: The pretreatment LCR could independently predict the overall survival in NPC patients. A novel LCR-based prognostic model of an easy-to-use nomogram was established, and it outperformed the conventional staging system in terms of predictive power. Further external verification remains necessary.
Introduction
Nasopharyngeal carcinoma (NPC) is a relatively rare malignancy around the world but is endemic in East and Southeast Asia. More than 130,000 newly diagnosed NPC cases are reported worldwide annually, and more than 70% of these cases are locoregionally advanced (1, 2). Concurrent chemoradiotherapy (CCRT) has been widely recommended as the mainstay care for locoregionally advanced NPC (3, 4). In current clinical practice, tumor node metastasis staging is the primary and, to some extent, the only tool used for predicting prognosis and guiding treatment (5, 6). However, the survival outcome of patients at the same Tumor, Node, and Metastasis (TNM, a cancer staging system used to describe the extent or spread of solid tumors) stage differs largely (7), with up to 30% of patients in the same stage and received similar treatment regimens exhibit disease progress (8), suggesting that prognosis prediction and individualized treatment determined by anatomical staging system alone is not sufficient. Therefore, it remains imperative to explore novel markers to enhance the current traditional staging system.
Tumor-related nutrition and inflammation have been recognized as crucial factors in the development and progression of various types of cancer (9, 10). Over the past years, numerous nutritional-inflammatory prognostic indexes, including the neutrophil–lymphocyte ratio, platelet–lymphocyte ratio, the monocyte–lymphocyte ratio, the systemic immune-inflammation index, the Glasgow prognostic score, the prognostic nutritional index, and the Controlling Nutritional Status, have been established and applied clinically in various tumors including NPC (11–17). Recently, a novel nutrition-inflammation marker of the lymphocyte–C-reactive protein ratio (LCR), calculated by lymphocyte count and C-reactive protein (CRP), was found to be an effective prognostic marker in numerous tumors (18–21). However, whether the LCR score could predict survival outcomes in NPC patients remains unclear.
Herein, this study sought to explore the prognostic significance of the LCR score and establish a predictive model for individualized survival predictions in patients with NPC receiving CCRT.
Methods
Patients
This retrospective study enrolled consecutive NPC patients who received platinum-based CCRT between January 2010 and March 2015 at the Sun Yat-sen University Cancer Center. The following were the inclusion criteria: (i) treatment-naïve non-metastatic NPC verified by histological and radiographic evaluations; (ii) with pretreatment peripheral blood and Epstein–Barr virus (EBV) DNA examinations; (iii) with radical intensity-modulated radiotherapy plus weekly/triweekly platinum-based concurrent chemotherapy; and (iv) without any chronic inflammatory disease. All the patients updated staging according to the 8th AJCC TNM system. The participants who enrolled between January 2010 and December 2014 were randomly divided into the training and validation cohorts at a ratio of 7:3, and 122 patients who enrolled between January 2015 and March 2015 were included as an additional validation cohort. The Research Ethics Committee of Sun Yat-sen University Cancer Center approved this study, and all the patients provided written informed consent before treatment.
Data collection and follow-up
The primary laboratory data were collected within a week of diagnosis, and clinicopathological data were obtained from patients' medical records (refer to our previously published article) (22). Real-time quantitative polymerase chain reaction was used to measure the plasma EBV-DNA levels (copies/ml) (23). Body mass index (BMI) was calculated as weight (kg)/square of the height in meters (m2), and patients were classified as obese (BMI ≥ 28), overweight (24 ≤ BMI < 28) and non-obese/overweight (BMI < 24). The treatment and follow-up protocols were in accordance with the guidelines previously described (23). Overall survival (OS) was defined as the time from the date of diagnosis to the date of death or last follow-up.
Statistical analysis
Prior sample size calculations were not performed because of the lack of evidence for building prognostic models. However, the enrolled participants were 841, and the events of this study amounted to 86, with an excess rate of 10 events per variable in multivariate models, indicating sufficient evaluating power (24). The optimal cutoff value was determined by the maximally selected rank statistics with survival status as the endpoint using the “maxstat” package (25). The Kaplan–Meier method was used to produce the survival curves and compared using log-rank tests. Schoenfeld residuals were used to test the proportional hazards hypothesis. To develop and validate the prognostic model, the Cox proportional hazards model was used to perform univariate and multivariate analyses, and variables with a p-value of < 0.05 in the univariate analysis would be included in the multivariate analysis to identify the independent risk factors. A prognostic model was constructed using the independent risk factors identified in the multivariate analysis of the training cohort and was graphically presented as a nomogram. Harrell's concordance index (C-index) calculated by the “rms” package, time-dependent receiver operative characteristics (tROC) conducted by the “timeROC” package, and decision curve analysis (DCA) conducted by the “ggDCA” package were used to measure the models' discriminative ability in both the training and validation cohorts. C-index, calibration curve, the area under the curve (AUC) of the tROC analysis, and DCA curve were used to measure the nomogram's performance. A two-tailed p-value of < 0.05 was considered statistically significant. Statistical analyses were conducted using R 4.2.1.
Results
Patient characteristics
Table 1 shows the baseline clinicopathological characteristics of the training and validation cohorts, and they were comparable between the two groups. Supplementary Table 1 shows the baseline clinicopathological characteristics of the additional validation cohort. In total, 287 (48.7%) patients and 126 (50.0%) patients aged more than 45 years were included in the training and validation cohorts, respectively. Of the total number of patients in the training and validation cohorts, 434 (73.7%) patients were included in the former, while the latter consisted of 192 (76.2%) male patients. Most of the enrolled patients were pathologically diagnosed with histological type WHO grade III, and 200 (34.0%) patients and 78 (31.0%) patients had an EBV-DNA value of ≥4,000 copies/ml in the training and validation cohorts, respectively. Then, patients in the training cohort were divided into the high-LCR group (scored ≥1.04, n = 335) and the low-LCR group (scored <1.04, n = 254), based on the optimal LCR cutoff value of 1.04 established by the maximally selected rank statistics (Supplementary Figure 1). Using the same cutoff value of 1.04, patients in the validation cohort were also divided into the high-LCR group (scored ≥1.04, n = 148) and the low-LCR group (scored <1.04, n = 104).
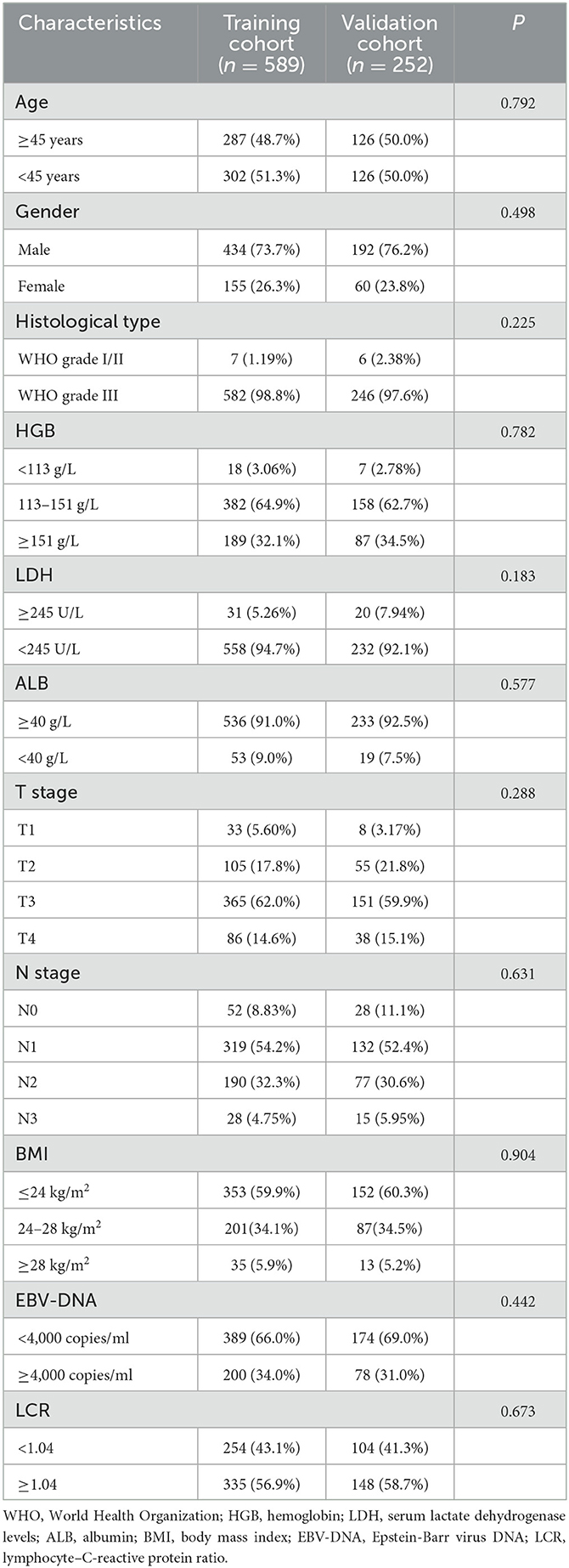
Table 1. Patient demographics and clinical characteristics between the training and validation cohorts.
Prognostic value of LCR score for OS in NPC
In the whole cohort of 841 patients, the median follow-up was 64.1 months (IQR: 58.3–76.5 months), and the median OS was 62.5 months (IQR: 46.6–74.8 months). There were 86 death events observed in the whole cohort, with 60 in the training cohort and 26 in the validation cohort. In the whole cohort, the 1-, 3-, and 5-year OS rates were 97.4%, 94.4%, and 91.1%, respectively. In the training cohort, the 1-, 3-, and 5-year OS rates were 97.6%, 94.2%, and 90.8%, respectively. In the validation cohort, the 1-, 3- and 5-year OS rates were 96.8%, 94.8%, and 91.7%, respectively. There was no significant difference in OS between the training and validation cohorts (Supplementary Figure 2, P = 0.96). Kaplan–Meier curves demonstrated that patients in the high-LCR group had significantly better survival than those in the low-LCR group in the training, validation, and additional cohorts (Figure 1A, HR = 0.53; 95% CI: 0.32–0.89, P = 0.014; Figure 1B, HR = 0.27; 95% CI: 0.11–0.63, P = 0.001; Supplementary Figure 3, HR = 0.28; 95% CI: 0.09–0.91, P = 0.024).
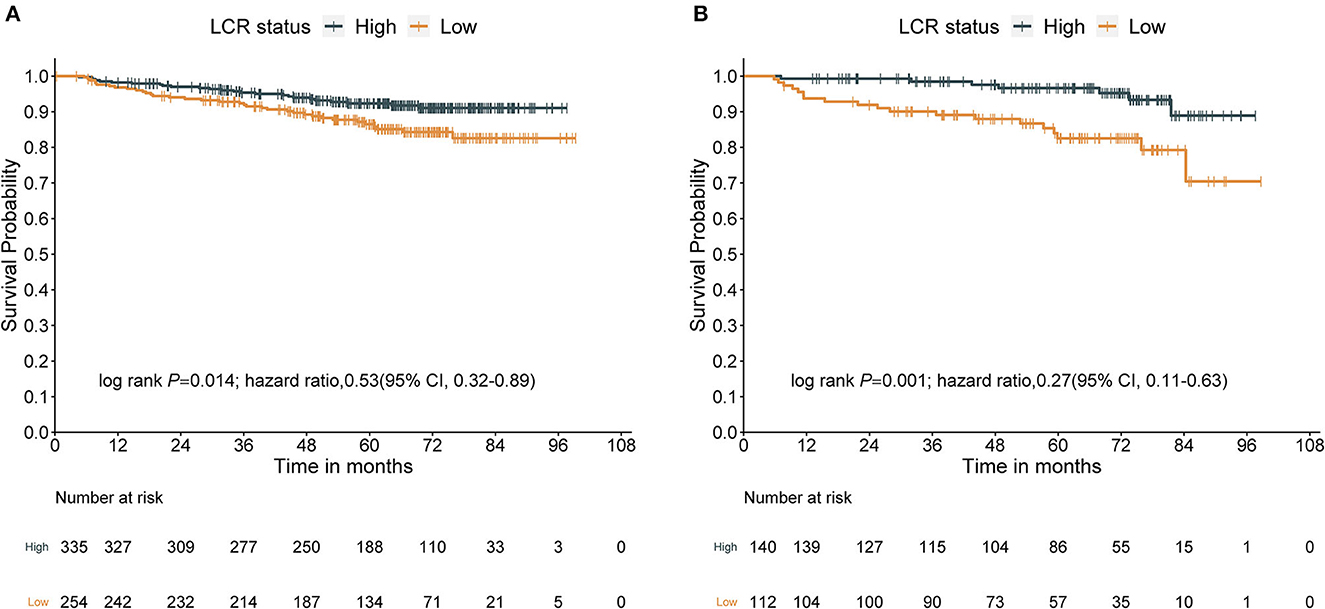
Figure 1. Survival curves obtained with Kaplan–Meier analysis between different LCRs. Groups (the HRs reported were unadjusted). (A) Survival curves in the training cohort. (B) Survival curves in the validation cohort. LCR, lymphocyte–C-reactive protein ratio; HR, hazard ratios; CI, confidence interval.
Univariate and multivariate Cox regression analyses of OS in NPC
Univariate and multivariate Cox regression analyses were conducted both in the training and validation cohorts. In the training cohort, variables that met the prespecified significance threshold (P < 0.05) in the univariate Cox model, including age, T stage, N stage, EBV-DNA status, and LCR score, were entered into the multivariate Cox regression model. A multicollinearity diagnostic test was conducted by calculating the variance inflation factors (VIFs) of the above variables (all VIFs < 10), indicating that no severe multicollinearity exists. According to the proportional hazards diagnostic plots (Supplementary Figure 4), the multivariable modeling satisfied the proportional hazards assumption. The results of multivariate modeling demonstrated that age, N stage, EBV-DNA status, and the LCR score were independently associated with OS for patients with NPC receiving concurrent chemoradiotherapy in the training cohort (Table 2) and validation cohort (Table 3).
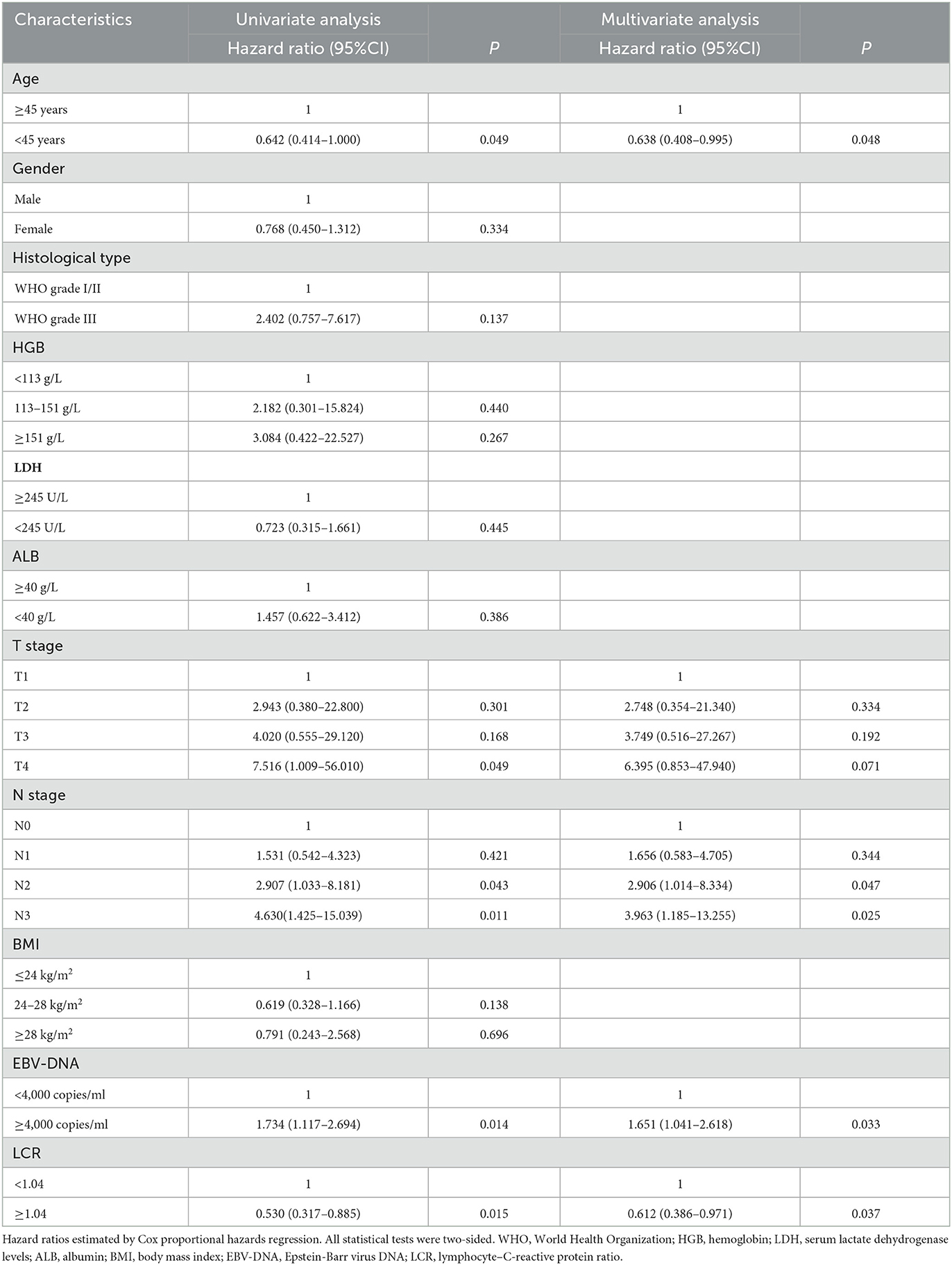
Table 2. Univariate and multivariate Cox regression analyses of overall survival in the training cohort.
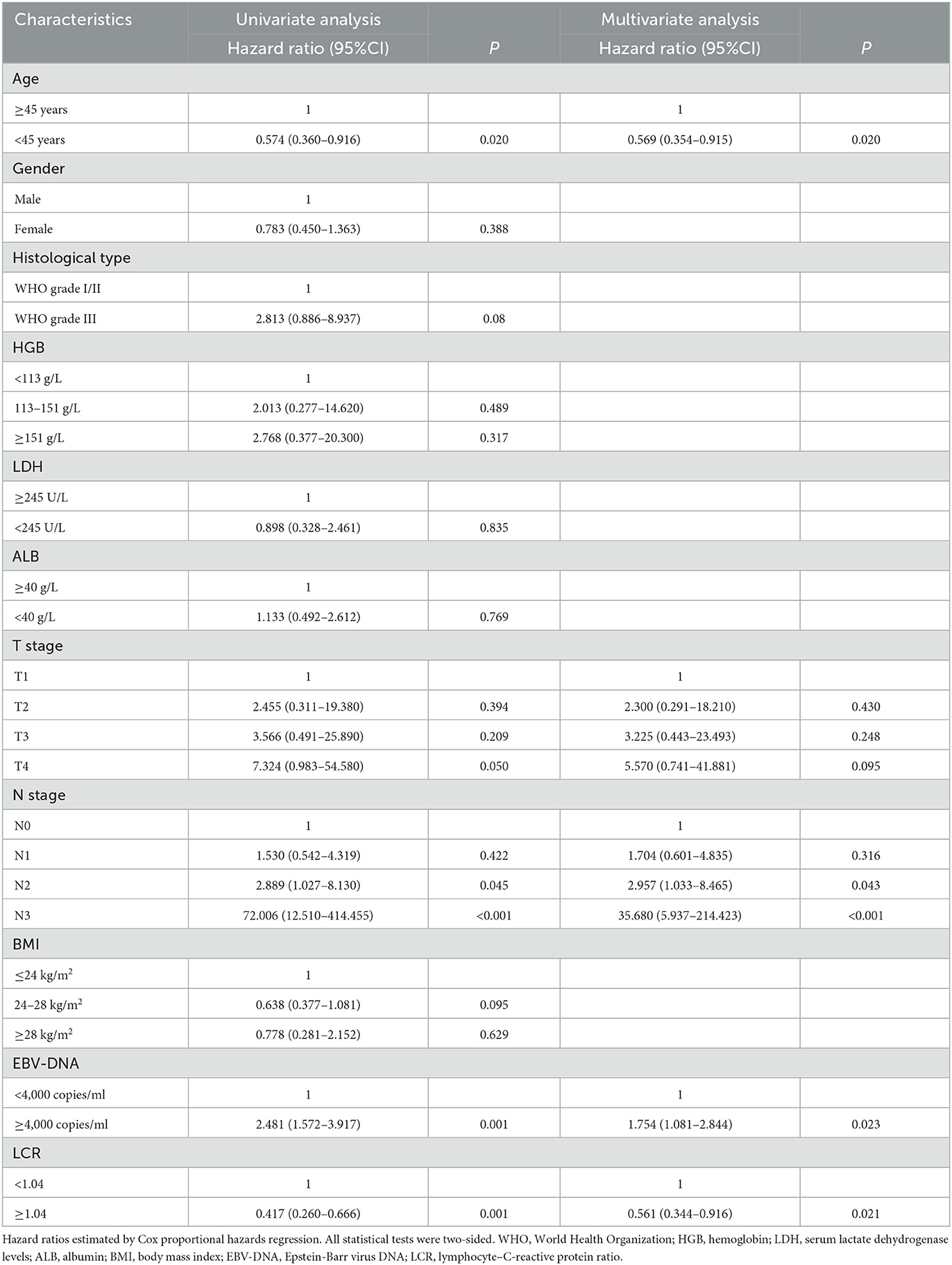
Table 3. Univariate and multivariate Cox regression analyses of overall survival in the validation cohort.
Development of a novel prognostic model based on LCR
A novel prognostic model of a nomogram for individual survival prediction at 1-, 3-, and 5-year was developed, based on the above four independent indicators from the multivariate modeling (Figure 2). Before the implementation of CCRT, each patient's total score could be calculated by adding the scores from each of the four prognostic factor subclasses, and the 1-, 3-, and 5-year OS probabilities could be forecasted by positioning the total score on the survival rate scale. For example, one patient who was 40 years old was presented with N3 stage, EBV-DNA of ≥4,000 copies/ml, and an LCR score of <1.04; hence, the total point was 0 + 10 + 4.8 + 4.75 = 19.55, and the corresponding 1-, 3-, and 5-year OS probabilities were 95%, 86%, and 77%, respectively.
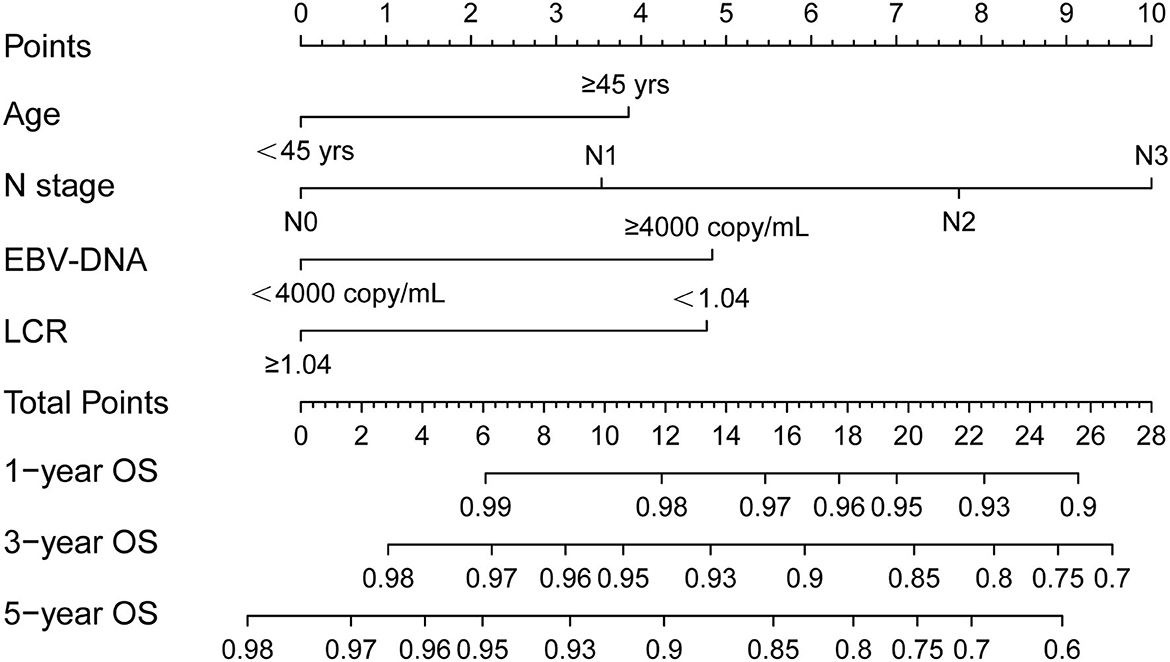
Figure 2. Nomogram of the current prognostic model for individualized survival predictions. OS, overall survival; LCR, lymphocyte–C-reactive protein ratio; EBV-DNA, Epstein-Barr virus DNA.
Assessment of predictive performance of the prognostic model
The generated prognostic model showed well-discriminative ability with a good C-index of 0.770 (95% CI: 0.675–0.864), 0.698 (95% CI: 0.623–0.774), and 0.727 (95% CI: 0.492–0.961) in the training, validation, and additional validation cohorts, compared with the C-index of 0.589 (95% CI: 0.385–0.792), 0.641 (95% CI: 0.532–0.749), and 0.644 (95% CI: 0.410–0.879) of traditional staging system; 0.662 (95% CI: 0.534–0.791), 0.646 (95% CI: 0.440–0.853), and 0.564 (95% CI: 0.282–0.845) of age; 0.694 (95% CI: 0.575–0.812), 0.651 (95% CI: 0.448–0.854), and 0.540 (95% CI: 0.254–0.825) of EBV-DNA; and 0.555 (95% CI: 0.351–0.758), 0.602 (95% CI: 0.493–0.710), and 0.651 (95% CI: 0.417–0.886) of the N stage, respectively. The calibration plots (the Y-axis represents the actual observed survival, while the X-axis represents the nomogram predicted survival) for the 1-, 3-, and 5-year OS present good agreement between predicted OS and observed OS in the training (Figure 3A), validation (Figure 3B), and additional validation (Supplementary Figure 5A) cohorts. The prognostic accuracy of this prognostic model for customized OS was evaluated using time-dependent ROC curves, and it outperformed the conventional tumor node metastasis (TNM) stage in the training (Figure 3C), validation (Figure 3D), and additional validation (Supplementary Figure 5B) cohorts. Also, the DCA curves demonstrated that the application of nomogram provided a better prediction effect than the TNM stage in the training (Figure 3E), validation (Figure 3F), and additional validation (Supplementary Figure 5C) cohorts.
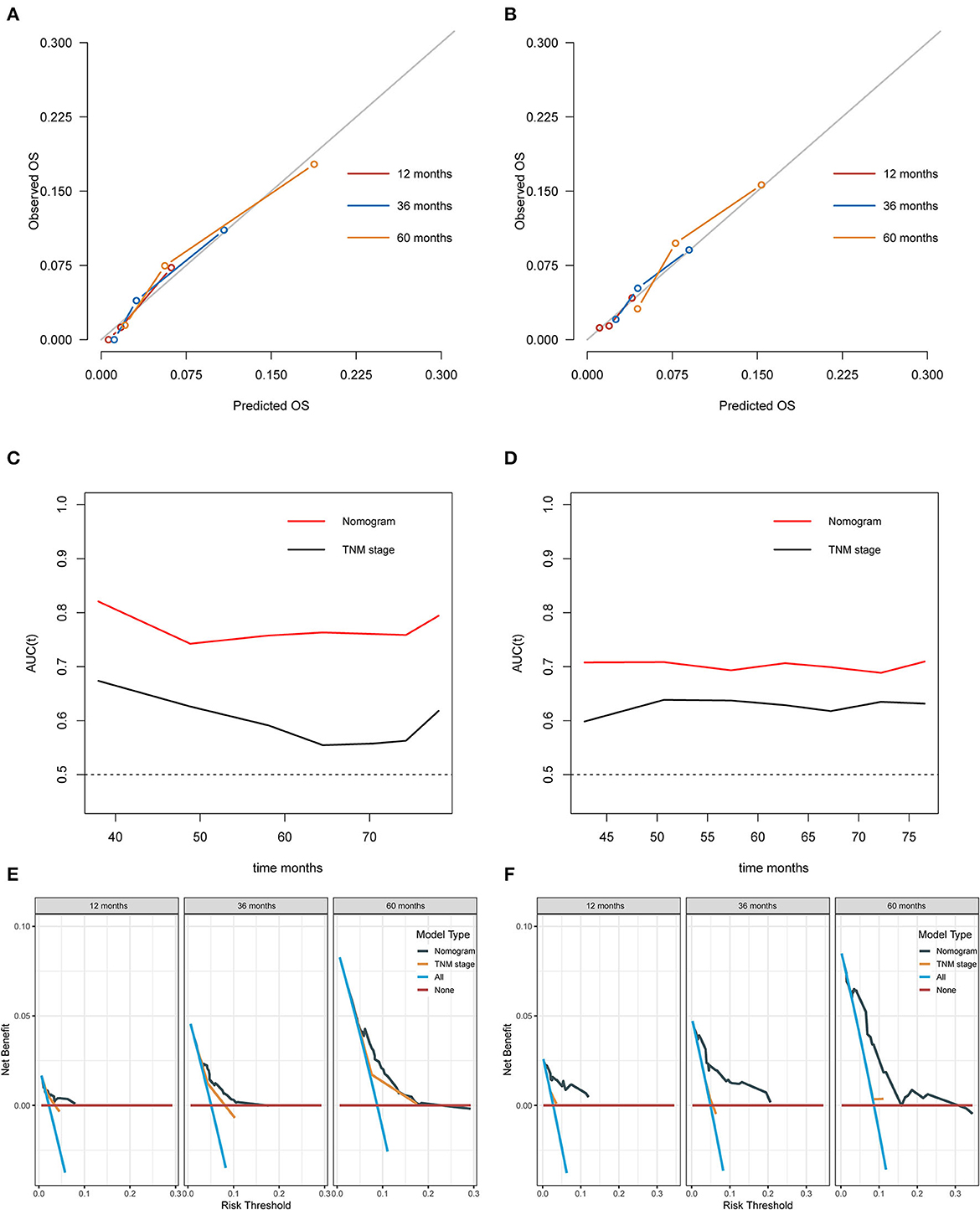
Figure 3. Assessment of predictive performance of the prognostic model. (A) Calibration plot of the nomogram model at 1, 3, and 5 years in the training cohort. (B) Calibration plot of the nomogram model at 1, 3, and 5 years in the validation cohort. (C) Time-independent ROC curves compared the predictive accuracy of the current model and the traditional TNM stage in the training cohort. (D) Time-independent ROC curves compared the predictive accuracy of the current model and the traditional TNM stage in the validation cohort. (E) DCA curves compared the net benefit rate of the current model and the traditional TNM stage in the training cohort. (F) DCA curves compared the net benefit rate of the current model and the traditional TNM stage in the validation cohort. OS, overall survival; AUC, area under the curve; TNM, tumor node metastasis.
Discussion
In this study, we investigated that the pretreatment LCR could independently predict the OS in NPC patients, and a novel LCR-based prognostic model of an easy-to-use nomogram was established. The findings were also reproducible in the validation cohort. Given that the traditional anatomical TNM staging system alone is not sufficient for prognosis prediction in NPC patients who underwent CCRT, the novel nutrition-inflammation marker of LCR and LCR-based prognostic model could serve as a simplified, affordable, easy-to-obtain, non-invasive, and readily promotive biomarker to clinically make individualized prognostic recommendations in this heterogeneous patient population.
NPC is biologically highly heterogeneous, with quite different outcomes for the same staging patients receiving similar regimens of CCRT (7). In recent years, highly sophisticated gene examination and liquid biopsy have been used to interpret the comprehensive molecular mechanisms of NPC to discriminate its heterogeneity and prognosis (26–29). However, these tools are currently expensive and have complicated testing procedures with unreliable repeatability; therefore, they are not yet widely applied in clinical practice. Since the term “biomarker” was initially proposed by The National Institutes of Health Biomarkers Definition Working Group (30), increasing studies have explored and developed numerous novel prognostic markers in NPC. Nowadays, the optimal prognostic biomarkers are generally recognized as signatures that could identify an individual's prognosis independent of traditional classifications (i.e., the TNM staging system) to improve clinical survival outcomes and are affordable, easily accessible, simplified, and use standard approaches, which can be scaled up on a large scale. Although there is numerous established evidence of the TNM staging system for evaluating the risk of disease progress and prognosis in NPC patients, the huge heterogeneity of prognostic outcomes in patient groups with the same stage and received similar treatment regimens highlights the urgent need for novel efficient biomarkers to identify patients at high risk for long-term clinical outcomes in NPC.
In this study, the novel nutrition-inflammation marker of LCR was demonstrated as being significantly related to survival outcomes in NPC patients who underwent CCRT. Those individuals with high systemic inflammation and malnutrition risk factors were more likely to have a poor prognosis and an insufficient response to radiation and chemotherapy than patients without these risk factors. Our findings were consistent with those of earlier studies investigating certain nutritional or inflammatory markers in NPC (31–33). Poorer survival outcomes in NPC have been linked to higher CRP levels and severe lymphopenia risks. Our findings suggested that evaluations of the nutritional and inflammatory status of the LCR score may accurately reflect the genuine tumor condition and forecast the effectiveness of CCRT in NPC. An under-appreciated sub-population of patients who have a low LCR score may need individualized treatment.
However, the molecular mechanisms underpinning the association between LCR status and prognosis are still not fully understood. Complex connections between the tumor and host immunological and inflammatory responses are associated with cancer-related nutrition and inflammation, and these interactions could serve as potential targets for cancer therapies (9, 34). The mechanisms of the prognostic significance of the LCR status in NPC may be partially explained by the physiological and pathologic roles of lymphocytes and CRP in tumors. By causing cytotoxic cell death and obstructing tumor cell proliferation and migration, lymphocytes play a significant role in tumor immune surveillance and defense (34). Malnutrition could decrease the prognosis of patients by weakening the host's immune system functioning and cell-mediated immunity, which is crucial for the host's ability to prevent cancer and is indicated by the lymphocyte level (35). Malnutrition has been linked to worse prognosis for a variety of malignant cancers, due to the increased adverse effects, treatment pauses, reduced chemotherapy intensity, decreased radiation sensitivity and/or chemotherapy sensitivity, and compromised immune function of the host (36–38). Cancer-related inflammation is a recognized hallmark of cancer that regulates essentially all stages of malignancy, including susceptibility, initiation, progression, dissemination, and death (39). Circulating immune cells, circulating cytokines, tiny inflammatory proteins, and acute-phase proteins are all mediators of systemic inflammation (34). CRP is an acute-phase protein that is largely produced in hepatocytes in reaction to proinflammatory cytokines before being released into the bloodstream. Moreover, there is a vicious facilitation between inflammation and malnutrition (40). Therefore, it is crucial to identify patients at high risk of infection and malnutrition, thus providing anti-infective and nutritional interventions as soon as possible are essential to improve clinical outcomes.
Apart from the LCR score, the age, N stage, and EBV-DNA status were independently associated with OS for patients with NPC receiving CCRT. Age is one of the important prognostic factors in many tumors including NPC, and previous studies have confirmed that elder patients have progressively worse survival in NPC (41, 42). Our previous study also found that patients over 45 years old had a high risk to develop low skeletal muscle mass (malnutrition) (43). Theoretically, an increased risk of malnutrition and radiotherapy/chemotherapy-related toxicities may have occurred with advancing age due to the accumulation of cellular damage, declining immune function, and impaired organ function (42). The N stage was also found to be associated with the nutritional status of NPC patients. For example, Du et al. found that a higher N stage was related to severe weight loss in NPC patients, and Wei et al. revealed that nodal metastasis status was correlated to the patient's nutritional index (44, 45). Chronic inflammation induced by EB virus infection has been shown to play a crucial role in the progression and invasiveness of NPC (46, 47). Also, Tang et al. found that EBV-DNA was related to the patient's nutritional index in NPC, and many studies demonstrated adding the prognostic value of EBV-DNA to nutritional and inflammatory biomarkers (48–50).
Limitations
There are certain unavoidable limitations to this cohort study. First, this study was conducted retrospectively, and there exists an inherent potential selection bias. Second, the patient cohorts used in this study are not necessarily typical of all cancer patients who are diagnosed and treated at the institution because the study population was centered on patients who had adequate measurements for the chosen markers. Moreover, there was no external validation conducted for the prognostic model due to our inability to obtain high-quality data from other centers. Therefore, further multicenter external validation would be necessary to strengthen our findings. Additionally, the LCR status can be influenced by several clinical situations, and it can change over time. Therefore, we will collect more data to undertake dynamic analysis to produce more results, and we are also planning further prospective studies to confirm these findings.
Conclusion
The pretreatment LCR could independently predict the overall survival in NPC patients. A novel LCR-based prognostic model of an easy-to-use nomogram was established, and it outperformed the conventional staging system in terms of predictive power. The LCR score may enable oncologists to estimate individualized survival outcomes more accurately, thus supporting the appropriate pre-CCRT and post-CCRT management of NPC patients. Further external verification of LCR and LCR-based prognostic model remains necessary.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
Ethics statement
The Research Ethics Committee of Sun Yat-sen University Cancer Center approved this study, and all the patients provided written informed consent before treatment.
Author contributions
XH performed the literature search and designed the study. XH, Z-QL, S-FW, FX, M-DW, J-YC, Y-LZ, W-QN, and Y-SG participated in the analysis and interpretation of data. XH and Y-SG developed an early draft. All authors contributed to the manuscript revision and approved the final version before submission.
Acknowledgments
The authors would like to thank the patients who participated in this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2023.1162280/full#supplementary-material
References
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660
2. Zhang Y, Chen L, Hu GQ. Gemcitabine and cisplatin induction chemotherapy in nasopharyngeal carcinoma. N Engl J Med. (2019) 381:1124–35. doi: 10.1056/NEJMoa1905287
3. Chen YP, Chan ATC, Le QT, Blanchard P, Sun Y, Ma J. Nasopharyngeal carcinoma. Lancet. (2019) 394:64–80. doi: 10.1016/S0140-6736(19)30956-0
4. Ng WT, Tung SY, Lee V. Concurrent-adjuvant chemoradiation therapy for stage III-IVB nasopharyngeal carcinoma-exploration for achieving optimal 10-year therapeutic ratio. Int J Radiat Oncol Biol Phys. (2018) 101:1078–86. doi: 10.1016/j.ijrobp.2018.04.069
5. Tang LL, Chen YP, Chen CB, Chen MY, Chen NY, Chen XZ, et al. The Chinese society of clinical oncology (CSCO) clinical guidelines for the diagnosis and treatment of nasopharyngeal carcinoma. Cancer Commun. (2021) 41:1195–227. doi: 10.1002/cac2.12218
6. Chen Y-P, Ismaila N, Chua MLK, Colevas AD, Haddad R, Huang SH, et al. Chemotherapy in combination with radiotherapy for definitive-intent treatment of stage II-IVA nasopharyngeal carcinoma: CSCO and ASCO guideline. J Clin Oncol. (2021) 39:840–59. doi: 10.1200/JCO.20.03237
7. Hui EP, Li WF, Ma BB, Lam WKJ, Chan KCA, Mo F, et al. Integrating postradiotherapy plasma Epstein-Barr virus DNA and TNM stage for risk stratification of nasopharyngeal carcinoma to adjuvant therapy. Ann Oncol. (2020) 31:769–79. doi: 10.1016/j.annonc.2020.03.289
8. Zhang L, Huang Y, Hong S, Yang Y, Yu G, Jia J, et al. Gemcitabine plus cisplatin versus fluorouracil plus cisplatin in recurrent or metastatic nasopharyngeal carcinoma: a multicentre, randomised, open-label, phase 3 trial. Lancet. (2016) 388:1883–92. doi: 10.1016/S0140-6736(16)31388-5
9. Zitvogel L, Pietrocola F, Kroemer G. Nutrition, inflammation and cancer. Nat Immunol. (2017) 18:843–50. doi: 10.1038/ni.3754
10. Hanahan D. Hallmarks of cancer: new dimensions. Cancer Discov. (2022) 12:31–46. doi: 10.1158/2159-8290.CD-21-1059
11. Chua ML, Tan SH, Kusumawidjaja G. Neutrophil-to-lymphocyte ratio as a prognostic marker in locally advanced nasopharyngeal carcinoma: a pooled analysis of two randomised controlled trials. Eur J Cancer. (2016) 67:119–29. doi: 10.1016/j.ejca.2016.08.006
12. Sun W, Zhang L, Luo M, Hu G, Mei Q, Liu D, et al. Pretreatment hematologic markers as prognostic factors in patients with nasopharyngeal carcinoma: Neutrophil-lymphocyte ratio and platelet-lymphocyte ratio. Head Neck. (2016) 38(Suppl 1:E):1332–40. doi: 10.1002/hed.24224
13. Li J, Jiang R, Liu WS. A large cohort study reveals the association of elevated peripheral blood lymphocyte-to-monocyte ratio with favorable prognosis in nasopharyngeal carcinoma. PLoS ONE. (2013) 8:e83069. doi: 10.1371/journal.pone.0083069
14. Jiang W, Chen Y, Huang J, Xi D, Chen J, Shao Y, et al. Systemic immune-inflammation index predicts the clinical outcome in patients with nasopharyngeal carcinoma: a propensity score-matched analysis. Oncotarget. (2017) 8:66075–86. doi: 10.18632/oncotarget.19796
15. Chen C, Sun P, Dai QS, Weng HW Li HP, Ye S. The Glasgow Prognostic Score predicts poor survival in cisplatin-based treated patients with metastatic nasopharyngeal carcinoma. PLoS One. (2014) 9:e112581. doi: 10.1371/journal.pone.0112581
16. Tu X, Ren J, Zhao Y. Prognostic value of prognostic nutritional index in nasopharyngeal carcinoma: a meta-analysis containing 4,511 patients. Oral Oncol. (2020) 110:104991. doi: 10.1016/j.oraloncology.2020.104991
17. Lu H, Guo S, Liu L, Chen Q, Liang Y, Liu S, et al. Prognostic significance of a combined and controlled nutritional status score and EBV-DNA in patients with advanced nasopharyngeal carcinoma: a long-term follow-up study. Cancer Biol Med. (2021) 19:551–64. doi: 10.20892/j.issn.2095-3941.2020.0627
18. Okugawa Y, Toiyama Y, Yamamoto A. Lymphocyte-c-reactive protein ratio as promising new marker for predicting surgical and oncological outcomes in colorectal cancer. Ann Surg. (2020) 272:342–51. doi: 10.1097/SLA.0000000000003239
19. Okugawa Y, Toiyama Y, Yamamoto A. Lymphocyte-to-C-reactive protein ratio and score are clinically feasible nutrition-inflammation markers of outcome in patients with gastric cancer. Clin Nutr. (2020) 39:1209–17. doi: 10.1016/j.clnu.2019.05.009
20. Yamamoto A, Toiyama Y, Okugawa Y, Ichikawa T, Imaoka H, Yasuda H, et al. Clinical implications of the preoperative lymphocyte C-reactive protein ratio in esophageal cancer patients. Surg Today. (2021) 51:745–55. doi: 10.1007/s00595-020-02166-5
21. Zhang HY, Xie HL, Ruan GT, Zhang Q, Ge YZ, Liu XY, et al. Lymphocyte to C-reactive protein ratio could better predict the prognosis of patients with stage IV cancer. BMC Cancer. (2022) 22:1080. doi: 10.1186/s12885-022-10145-x
22. Hua X, Liao JF, Huang X, Huang HY, Wen W, Long ZQ, et al. Sarcopenia is associated with higher toxicity and poor prognosis of nasopharyngeal carcinoma. Ther Adv Med Oncol. (2020) 12:1758835920947612. doi: 10.1177/1758835920947612
23. Hua X, Li WZ, Huang X, Wen W, Huang HY, Long ZQ, et al. Modeling sarcopenia to predict survival for patients with nasopharyngeal carcinoma receiving concurrent chemoradiotherapy. Front Oncol. (2021) 11:625534. doi: 10.3389/fonc.2021.625534
24. Riley RD, Ensor J, Snell KIE, Jr FEH, Martin GP, Reitsma JB, et al. Calculating the sample size required for developing a clinical prediction model. BMJ. (2020) 368:m441. doi: 10.1136/bmj.m441
25. Hua X, Duan F, Zhai W. A novel inflammatory-nutritional prognostic scoring system for patients with early-stage breast cancer. J Inflamm Res. (2022) 15:381–94. doi: 10.2147/JIR.S338421
26. Tang XR, Li YQ, Liang SB, Jiang W, Liu F, Ge WX, et al. Development and validation of a gene expression-based signature to predict distant metastasis in locoregionally advanced nasopharyngeal carcinoma: a retrospective, multicentre, cohort study. Lancet Oncol. (2018) 19:382–93. doi: 10.1016/S1470-2045(18)30080-9
27. Dai W, Chung DL-S, Chow LK-Y, Yu VZ, Lei LC, Leong MM-L, et al. Clinical outcome-related mutational signatures identified by integrative genomic analysis in nasopharyngeal carcinoma. Clin Cancer Res. (2020) 26:6494–504. doi: 10.1158/1078-0432.CCR-20-2854
28. Liang Y, Li J, Li Q, Tang L, Chen L, Mao Y, et al. Plasma protein-based signature predicts distant metastasis and induction chemotherapy benefit in Nasopharyngeal Carcinoma. Theranostics. (2020) 10:9767–78. doi: 10.7150/thno.47882
29. Ko JM-Y, Vardhanabhuti V, Ng W-T, Lam K-O, Ngan RK-C, Lai-Wan Kwong D, et al. Clinical utility of serial analysis of circulating tumour cells for detection of minimal residual disease of metastatic nasopharyngeal carcinoma. Br J Cancer. (2020) 123:114–25. doi: 10.1038/s41416-020-0871-1
30. Biomarkers Definitions Working G. Biomarkers and surrogate endpoints: preferred definitions and conceptual framework. Clin Pharmacol Ther. (2001) 69:89–95. doi: 10.1067/mcp.2001.113989
31. Cai Z, Jiang J, Huang L, Yuan Y, Zheng R, Zhang J, et al. The prognostic impact of combined tumor-infiltrating lymphocytes and pretreatment blood lymphocyte percentage in locally advanced nasopharyngeal carcinoma. Front Oncol. (2021) 11:788497. doi: 10.3389/fonc.2021.788497
32. Xie X, Gong S, Jin H. Radiation-induced lymphopenia correlates with survival in nasopharyngeal carcinoma: impact of treatment modality and the baseline lymphocyte count. Radiat Oncol. (2020) 15:65. doi: 10.1186/s13014-020-01494-7
33. Zeng YC, Wu R, Xiao YP. Serum C-reactive protein predicts poor prognosis in patients with locoregionally advanced nasopharyngeal carcinoma treated with chemoradiotherapy. Curr Oncol. (2015) 22:20–4. doi: 10.3747/co.22.2178
34. Diakos CI, Charles KA, McMillan DC, Clarke SJ. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. (2014) 15:e493–503. doi: 10.1016/S1470-2045(14)70263-3
35. Weiss G. Nutrition and infection. Clin Microbiol Infect. (2018) 24:8–9. doi: 10.1016/j.cmi.2017.10.028
36. Lyu J, Li T, Xie C, Li J, Xing L, Zhang X, et al. Enteral nutrition in esophageal cancer patients treated with radiotherapy: a Chinese expert consensus 2018. Future Oncol. (2019) 15:517–31. doi: 10.2217/fon-2018-0697
37. Grace EM, Shaw C, Lalji A, Mohammed K, Andreyev HJN, Whelan K. Nutritional status, the development and persistence of malnutrition and dietary intake in oesophago-gastric cancer: a longitudinal cohort study. J Hum Nutr Diet. (2018) 31:785–92. doi: 10.1111/jhn.12588
38. Shen Q, Liu W, Quan H, Pan S, Li S, Zhou T, et al. Prealbumin and lymphocyte-based prognostic score, a new tool for predicting long-term survival after curative resection of stage II/III gastric cancer. Br J Nutr. (2018) 120:1359–69. doi: 10.1017/S0007114518002854
39. Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. (2011) 144:646–74. doi: 10.1016/j.cell.2011.02.013
40. McMillan DC. An inflammation-based prognostic score and its role in the nutrition-based management of patients with cancer. Proc Nutr Soc. (2008) 67:257–62. doi: 10.1017/S0029665108007131
41. Wu LR, Liu YT, Jiang N. Ten-year survival outcomes for patients with nasopharyngeal carcinoma receiving intensity-modulated radiotherapy: an analysis of 614 patients from a single center. Oral Oncol. (2017) 69:26–32. doi: 10.1016/j.oraloncology.2017.03.015
42. He Q, Huang Y, Wan G. A novel prognostic marker based on risk stratification with prognostic nutritional index and age for nasopharyngeal carcinoma patients who received neoadjuvant chemotherapy. Biomark Med. (2019) 13:1013–23. doi: 10.2217/bmm-2018-0401
43. Hua X, Liao J-F, Liu S, Zhang J, Huang H-Y, Wen W, et al. Low skeletal muscle mass impairs quality of life in nasopharyngeal carcinoma patients treated with concurrent chemoradiotherapy. Front Nutr. (2019) 6:195. doi: 10.3389/fnut.2019.00195
44. Du XJ, Tang LL, Mao YP, Guo R, Sun Y, Lin AH, et al. Value of the prognostic nutritional index and weight loss in predicting metastasis and long-term mortality in nasopharyngeal carcinoma. J Transl Med. (2015) 13:364. doi: 10.1186/s12967-015-0729-0
45. Wei GB, Lu YY, Liao RW, Chen QS, Zhang KQ. Prognostic nutritional index predicts prognosis in patients with metastatic nasopharyngeal carcinoma. Onco Targets Ther. (2016) 9:5955–61. doi: 10.2147/OTT.S114382
46. Elgui de. Oliveira D, Muller-Coan BG, Pagano JS. Viral carcinogenesis beyond malignant transformation: EBV in the progression of human. Cancers Trends Microbiol. (2016) 24:649–64. doi: 10.1016/j.tim.2016.03.008
47. Li Z, Duan Y, Cheng S, et al. EBV-encoded RNA via TLR3 induces inflammation in nasopharyngeal carcinoma. Oncotarget. (2015) 6:24291–303. doi: 10.18632/oncotarget.4552
48. Tang QN, Qiu HZ, Sun XQ, Guo SS, Liu LT, Wen YF, et al. Geriatric nutritional risk index as an independent prognostic factor in locally advanced nasopharyngeal carcinoma treated using radical concurrent chemoradiotherapy: a retrospective cohort study. Ann Transl Med. (2021) 9:532. doi: 10.21037/atm-20-6493
49. Xiong Y, Shi LL, Zhu LS, Ding Q, Ba L, Peng G. Prognostic efficacy of the combination of the pretreatment systemic Immune-Inflammation Index and Epstein-Barr virus DNA status in locally advanced Nasopharyngeal Carcinoma Patients. J Cancer. (2021) 12:2275–84. doi: 10.7150/jca.52539
50. Huang ZZ, Wen W, Hua X, Song C-G, Bi XW, Huang JJ, et al. Establishment and validation of nomogram based on combination of pretreatment C-reactive protein/albumin ratio-EBV DNA grade in nasopharyngeal carcinoma patients who received concurrent chemoradiotherapy. Front Oncol. (2021) 11:583283. doi: 10.3389/fonc.2021.583283
Keywords: LCR, nasopharyngeal carcinoma, concurrent chemoradiotherapy, prognosis, nomogram
Citation: Hua X, Long Z-Q, Wang S-F, Xu F, Wang M-D, Chen J-Y, Zhang Y-L, Ni W-Q and Gao Y-S (2023) Prognostic significance of the novel nutrition-inflammation marker of lymphocyte–C-reactive protein ratio in patients with nasopharyngeal carcinoma receiving concurrent chemoradiotherapy. Front. Nutr. 10:1162280. doi: 10.3389/fnut.2023.1162280
Received: 09 February 2023; Accepted: 27 June 2023;
Published: 20 July 2023.
Edited by:
Maicon Roberto Kviecinski, Federal University of Santa Catarina, BrazilReviewed by:
Qiao He, University of Electronic Science and Technology of China, ChinaBin Wang, Sichuan University, China
Shuang Huang, Zhejiang Cancer Hospital, China
Copyright © 2023 Hua, Long, Wang, Xu, Wang, Chen, Zhang, Ni and Gao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yun-Sheng Gao, Z3lzMTE4NTZAcmpoLmNvbS5jbg==; Wei-Qiong Ni, bndxMTIwMThAcmpoLmNvbS5jbg==; Yu-Ling Zhang, eXVsaW5nemhhbmcxOTY3QDE2My5jb20=
†These authors have contributed equally to this work and share first authorship