 Sukyoung Jung
Sukyoung Jung Eunjin Jang2,3†
Eunjin Jang2,3† Sohyun Park
Sohyun Park- 1Chungnam National University Hospital Biomedical Research Institute, Daejeon, Republic of Korea
- 2Department of Food Science and Nutrition, Hallym University, Chuncheon, Republic of Korea
- 3The Korean Institute of Nutrition, Hallym University, Chuncheon, Republic of Korea
- 4National Food Safety Information Service, Seoul, Republic of Korea
Background: Excessive consumption of ultra-processed foods (UPFs) has been linked to an increased risk of cardiovascular disease. We aimed to investigate the association between the percentage of energy intake from UPFs and the American Heart Association’s cardiovascular health (CVH) metrics in Korean adults.
Methods: This study analyzed adults aged 40 years and older using data from the Korean National Health and Nutrition Examination Survey 2016–2018 (n = 9,351). All foods or beverages reported in a 24-h dietary recall were categorized using the NOVA system, and the percentage of energy from UPFs was calculated. Each CVH metric was scored 0–2 (poor, intermediate, ideal). The sum of six component scores was classified as inadequate, average, or optimum. Multinomial logistic regression models were used to estimate the covariate-adjusted odds ratios (ORs) and 95% confidence intervals (CIs) for inadequate and average CVH versus optimum CVH.
Results: The mean percentage of energy from UPFs was 24.2%. After adjusting for covariates, participants in the highest UPF quartile had 26% higher odds of having inadequate CVH than those in the lowest quartile (OR 1.26, 95% CI 0.94–1.69, P-trend = 0.03). The percentage of energy from UPFs was positively associated with current smoking, physical inactivity, body mass index, and total cholesterol and was inversely associated with blood pressure and fasting glucose.
Conclusion: The percentage of energy from UPFs accounted for one-fourth of total calorie intake in Korean adults aged 40 years and older. Higher UPF consumption was associated with poorer CVH, underscoring the potential of limiting UPF consumption as a preventative measure for cardiovascular diseases.
Introduction
Cardiovascular diseases (CVDs) are the leading cause of death globally, responsible for 32% of all deaths in 2019 (1). In Korea, heart disease is the second leading cause of death in 2019, accounting for 59.6 and 61.3 deaths per 100,000 population for males and females (2). To monitor and improve CVD rates, the American Heart Association (AHA) has developed seven cardiovascular health (CVH) metrics consisting of smoking status, physical activity, healthy diet score, body mass index, total cholesterol, blood pressure, and fasting glucose (3). These metrics align with the leading modifiable global CVD risk factors, according to the Global Burden of Disease Study (4). Research indicates that having more ideal CVH metrics is associated with a considerably lower risk of CVD incidence and mortality (5, 6).
Among the behavioral risk factors for CVD, dietary factors contribute the most to CVD mortality (4). Ultra-processed foods (UPFs) have drawn attention due to their harmful impact on health and increasing consumption (7). UPFs, as defined by NOVA, are often energy-dense, high in sugar, unhealthy fat, and salt, and low in fiber, protein, vitamins, and minerals (8). Examples include sweetened beverages, energy drinks, packaged snacks, processed cheese, instant sauces, nuggets, sausages, hot dogs, and ready-to-eat foods (8). Although UPFs are convenient to eat, tasty, and inexpensive (8), a growing body of evidence indicates their negative effects on health. According to previous studies, the consumption of UPFs is associated with lower nutritional quality of diets (9) and higher risks of chronic disease incidence including type 2 diabetes (10), cancer (11), cardiovascular disease (12), as well as mortality (13), and metabolic conditions including overweight and obesity (14), dyslipidemia (15), and hypertension (16).
Few studies have examined the relationship between UPF intake and CVH metrics, which assess cardiovascular risk comprehensively. In the United States, two studies have found an inverse association between UPF consumption and CVH metrics in both adults and adolescents (17, 18). Given an increasing trend in UPF consumption (19) and the burden of CVDs in Korea (2), it is necessary to examine the association between UPF consumption and CVH. Therefore, this study aimed to investigate the association between the percentage of energy intake (%E) from UPFs and the AHA’s CVH metrics (excluding diet) in Korean adults aged 40 years and older, using data from the Korea National Health and Nutrition Examination Survey (KNHANES) 2016–2018. We hypothesized that higher UPF consumption would be associated with poorer CVH.
Methods
Study population
The KNHANES, administered by the Korea Disease Control and Prevention Agency, is an ongoing, cross-sectional, and nationally representative survey to monitor the health and nutritional status of the noninstitutionalized civilian population in Korea (20). To ensure the representativeness of the noninstitutionalized Korean population, KNHANES used a complex and multistage probability sampling design (20). KNHANES data collection includes health interviews, health examinations, and nutrition surveys. More information on the rationale, design, and methods of the KNHANES is detailed elsewhere (20). For the 7th KNHANES (2016–2018), 31,689 persons were screened, and 24,269 participants completed at least one or more surveys of health interviews, health examinations, and nutrition surveys (response rate: 76.6%) (21).
Among 13,959 adults aged 40 years and older, we excluded participants if they had the following conditions: missing information on dietary data or implausible energy intakes (<500 kcal or > 5,000 kcal) (n = 2,430); pregnant or lactating (n = 4); self-reported severe diseases (n = 1,290); missing information on CVH metrics (n = 884). The final analytic sample included 9,351 adults (Supplementary Figure 1). The study protocol was approved by the Institutional Review Board of Hallym University (HIRB-2021-087-R-CR).
Assessment of ultra-processed food consumption
The nutrition survey was administered 1 week after the health interviews and examinations. Trained dieticians collected dietary information (description, quantity, and time and place of eating) on all foods and beverages consumed using a 24-h dietary recall. The respondents reported the quantity of consumed foods and beverages in units of volume with the assistance of standard measuring tools and/or guides. The multiple-pass method was used to obtain a complete food recall while minimizing respondent burden. Daily energy and nutrient intakes were estimated from the Ninth Edition of the Korean Food Composition Table of the Rural Development Administration (22).
A NOVA classification system was used to classify all reported foods or underlying ingredients of mixed dishes into one of four food categories based on the extent and purpose of food processing. In NOVA, the first group indicates unprocessed or minimally processed foods; the second group indicates processed culinary ingredients; the third group indicates processed foods; and the fourth group indicates UPFs (23). A Korean NOVA system, based on the matrix maintenance of natural foods and traditional eating experiences, was used to account for the uniqueness of Korean cuisine (dish-based with multiple ingredients) (24). For example, Korean fermented sauces (e.g., soybean paste) can be classified as UPFs in the original NOVA system, while they could be classified as either ultra-processed or processed foods in the Korean NOVA system, depending on whether they are produced through mass production or traditionally. Detailed examples are available elsewhere (24). During the 24-h dietary recall interview, participants reported consuming 3,894 items in 2016–2018. Unprocessed or minimally processed foods included raw vegetables, fruits, meats, and grains (966 items). Processed culinary ingredients comprised condiments and oils (247 items). Processed foods include soups, stews, kimchi, and grilled or marinated vegetables and meat (504 items). Ultra-processed foods included mass-produced bread, snacks, soft drinks, and noodles (2,177 items).
Two investigators (S.J. and JY.K.) classified all foods and ingredients of mixed dishes into one of the four food groups in NOVA, and the entire classification was thoroughly cross-checked against one another. For dishes with multiple ingredients, we first sorted out the main ingredient in the mixed dishes using a standard recipe for Korean dishes and the ingredient database. The main ingredient was identified as the ingredient with the largest proportion of the total amount of dishes. When disagreement occurred, we then checked the following: (1) the product name and manufacturer information to identify the raw ingredients; and (2) the amount of sodium or sugar in such items based on the food code in the nutrient database. This is due to the likelihood that more processed foods tend to have more sodium and/or sugar content. All food items and ingredients were mutually exclusively classified into one of the four NOVA groups. Our focus was on the fourth group of the NOVA classification that is UPFs.
Calculation of cardiovascular health metrics
The CVH metrics were based on the Life’s Simple 7 set of risk factors proposed by the AHA (3). Originally, there were seven health components, including smoking status, physical activity, healthy diet score, body mass index, total cholesterol, blood pressure, and fasting plasma glucose (3). In this study, the main exposure of interest was UPF consumption, and thus the diet component was omitted from the final CVH metrics calculation. We used the definitions of optimum, average, and inadequate CVH as described in Supplementary Table 1.
Smoking status
Current smokers were defined as those who are currently smoking cigarettes every day or some days. Former smokers were defined as those who had smoked at least 100 cigarettes in their lifetime but had quit for less than 12 months. Never smokers were defined as those who had smoked no more than 100 cigarettes in their lifetime or those who had smoked at least 100 cigarettes in their lifetime but had quit for more than 12 months. The status of never smokers, former smokers, and current smokers was defined as ideal, intermediate, and poor, respectively.
Physical activity
Participants reported the frequency and duration of any physical activity they engaged in for transportation, work, leisure, or exercise in a typical week. In KNHANES 2016–2018, there are five modes of activities, including vigorous work-related activity, moderate work-related activity, walking or bicycling, vigorous leisure-time activity, and moderate leisure-time activity. Physical activity (minutes per week) was quantified for each mode of activity by multiplying the frequency and duration. The physical activity component calculation used the following definitions: ideal was defined as “≥75 min of vigorous activity” or “≥150 min of moderate activity” or “≥150 min of combined moderate and vigorous physical activity”; intermediate was defined as more than 0 min of physical activity but less than recommendations; and poor was defined as 0 min of physical activity per week.
Body mass index
Anthropometric measurements were collected throughout the health examination using standardized examination procedures and calibrated equipment (20). Standing height (cm) was measured on a stadiometer, and body weight (kg) was measured with a metric weight scale, with sample participants in light clothing. Body mass index (BMI) was computed using the ratio of measured weight (kg) to standing height squared (m2). The Korean Society for the Study of Obesity defined 18–22.9 of BMI as normal and ≥ 25 of BMI as obesity (25). Thus, the BMI component calculation used the following definitions: ideal was defined as <23; intermediate was defined as 23–24.9; and poor was defined as ≥25.
Total cholesterol
Ideal was defined as less than 200 mg/dL of untreated total cholesterol level; intermediate was defined as 200–239 mg/dL of untreated total cholesterol level or taking cholesterol-lowering medication and being treated to goal (<240 mg/dL); and poor was defined as ≥240 mg/dL of untreated total cholesterol level or taking cholesterol-lowering medication but not being treated to goal.
Blood pressure
Ideal was defined as untreated systolic blood pressure (SBP) <120 mmHg and untreated diastolic blood pressure (DBP) <80 mmHg; intermediate was defined as SBP 120–139 mmHg or DBP 80–89 mmHg or taking antihypertensive medication and being treated to goal (SBP <140 mmHg and DBP <90 mmHg); and poor was defined as SBP ≥140 mmHg or DBP ≥90 mmHg or taking antihypertensive medication but not being treated to goal.
Fasting plasma glucose
Ideal was defined as less than 100 mg/dL of untreated fasting plasma glucose level; intermediate was defined as 100–125 mg/dL of untreated fasting plasma glucose level or taking insulin or medication to lower blood glucose and being treated to goal (<126 mg/dL); and poor was defined as ≥126 mg/dL of untreated fasting plasma glucose level or taking medication for diabetes but not being treated to goal.
Scoring
Each of the CVH metric components received a score of 2 if categorized as ideal, 1 if categorized as intermediate, and 0 if categorized as poor. A total score was calculated by summing the scores of six components (range: 0–12). For the analysis, the total score was classified into three groups: inadequate (0–4), average (5–8), or optimum (9–12) (17).
Assessment of covariates
Potential covariates included age (40–49, 50–59, or ≥ 60 years), sex (male or female), residential area (urban or rural), education level (less than high school graduate, high school graduate or higher), monthly household income (quartiles of equivalized household income), and marital status (married or not).
Statistical analysis
In this study, UPF consumption was presented as %E from UPFs. To describe the general characteristics of the study participants, we presented the weighted means and their standard errors (SEs) for continuous variables and the weighted prevalence and their SEs for categorical variables by CVH metrics categories (inadequate, average, or optimum). The significance of differences between CVH metrics categories was assessed by a student t-test for continuous variables and a chi-square test for categorical variables.
The restricted cubic spline model was fitted with 3 knots determined at the 5th, 50th, and 95th percentiles to test deviation from a linear association between %E from UPFs and CVH scores (26); no evidence of a nonlinear association was observed (p = 0.58 for nonlinearity). We also presented the adjusted differences in CVH scores by using the median of the lowest UPF consumption quartile (5.2% of calories from UPFs) as a reference (Supplementary Figure 2).
Multinomial logistic regression models were used to estimate the covariate-adjusted odds ratios (ORs) and 95% confidence intervals (CIs) for inadequate and average CVH versus optimum CVH, comparing quartiles 2, 3, and 4 with quartile 1 of %E from UPFs. We also examined the association between %E from UPFs and individual components of CVH metrics. We presented the covariate-adjusted ORs and 95% CIs for poor and intermediate individual CVH components versus ideal, comparing quartiles 2, 3, and 4 with quartile 1 of %E from UPFs. To assess potential linear trends, the median %E from UPFs in each quartile was treated as a continuous variable in multinomial logistic regression models. We presented two adjusted models: (1) an age and sex-adjusted model; and (2) a multivariable-adjusted model including age, sex, residential area, high school graduate, monthly household income quartiles, and marital status. When analyzing individual CVH metrics separately, the multivariable-adjusted model additionally included other individual CVH components except for itself.
Potential interaction effects of %E from UPFs and selected sociodemographic covariates were tested by including the cross-product term of UPF consumption and each covariate. The only significant interaction found was between education and %E from UPFs (p = 0.04); consequently, estimates are presented overall and by education level (less than high school graduate vs. high school graduate or above).
For all analyses, sample weights accounting for the complex sampling design of the KNHANES were incorporated. SAS software (version 9.4, SAS Institute Inc., Cary, NC, United States) was used to analyze the data. All tests were two-sided, and the level of significance was set at 0.05.
Results
Participant characteristics
General characteristics of the sample by CVH metrics categories are shown in Table 1. Of the 9,351 participants, the mean age was 56.3 years (≥65 years, 24.3%), 51.5% were females, 84.8% were urban residents, 67.8% were at least high school graduates, 32.7% had the highest quartile of monthly household income, and 80.3% were married. The weighted prevalence of inadequate, average, and optimum CVH was 6.4, 55.0, and 38.7%, respectively. Participants with lower CVH scores were more likely to be male, reside in rural areas, have lower levels of education and monthly household income, and be unmarried.
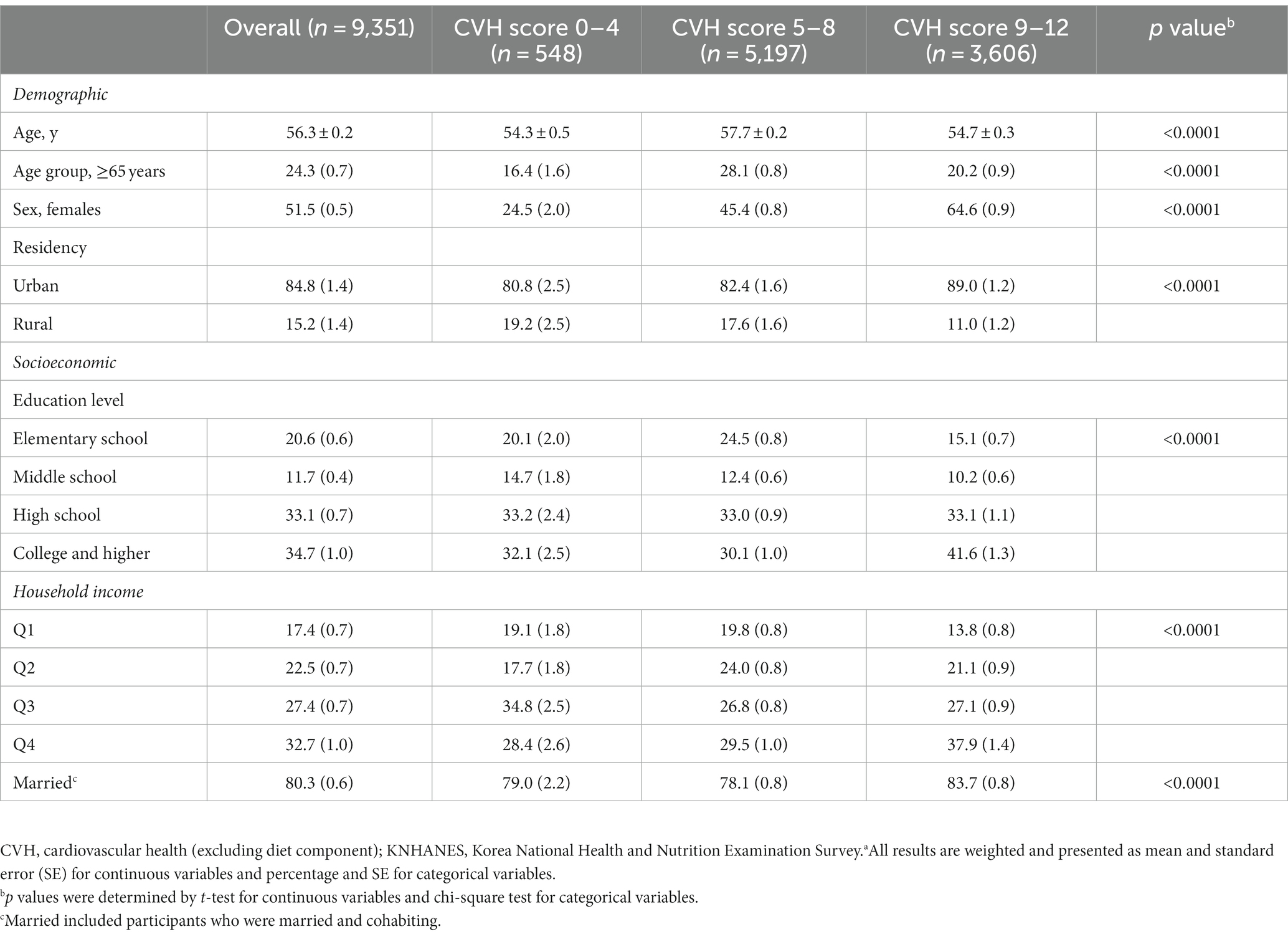
Table 1. General characteristics by cardiovascular health metric categories among Korean adults aged 40 years and older, KNHANES 2016–2018a.
Associations between UPF consumption and CVH
Table 2 shows the covariate-adjusted association between %E from UPFs and CVH. The mean %E from UPFs was 24.2% (with a median of 5.2% in quartile 1 and 45.6% in quartile 4). In the multivariable-adjusted model, participants in the highest UPF quartile had 26% higher odds of inadequate CVH than those in the lowest quartile (OR 1.26, 95% CI 0.94–1.69, P-trend = 0.03). After adjusting for confounders, the highest UPF consumption (quartile 4) was associated with 14% higher odds of average CVH compared to quartile 1, but was not statistically significant (OR 1.14, 95% CI 0.97–1.33, P-trend = 0.08). The age- and sex-adjusted results were not statistically significant.
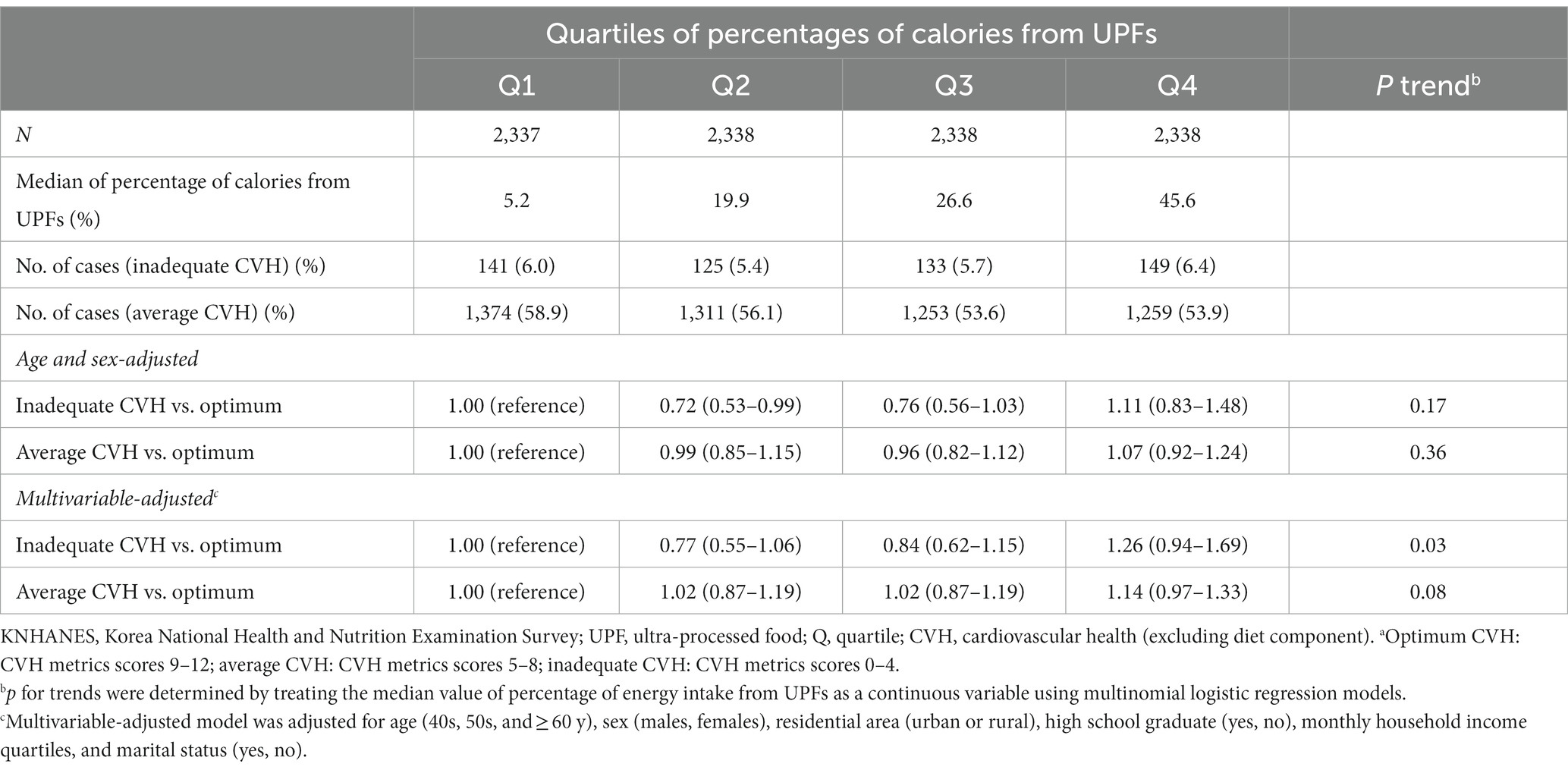
Table 2. Weighted odds ratios (95% confidence intervals) for cardiovascular health metrics across quartiles of ultra-processed food consumption among adults aged 40 years and older, KNHANES 2016–2018a.
Figure 1 shows the covariate-adjusted association between %E from UPFs and each individual CVH metric. The percentage of energy from UPFs was positively associated with poor CVH, including current smoking, physical inactivity, higher BMI, and higher total cholesterol, and was inversely associated with blood pressure and fasting glucose. The percentage of energy from UPFs was only positively associated with an intermediate CVH for BMI.
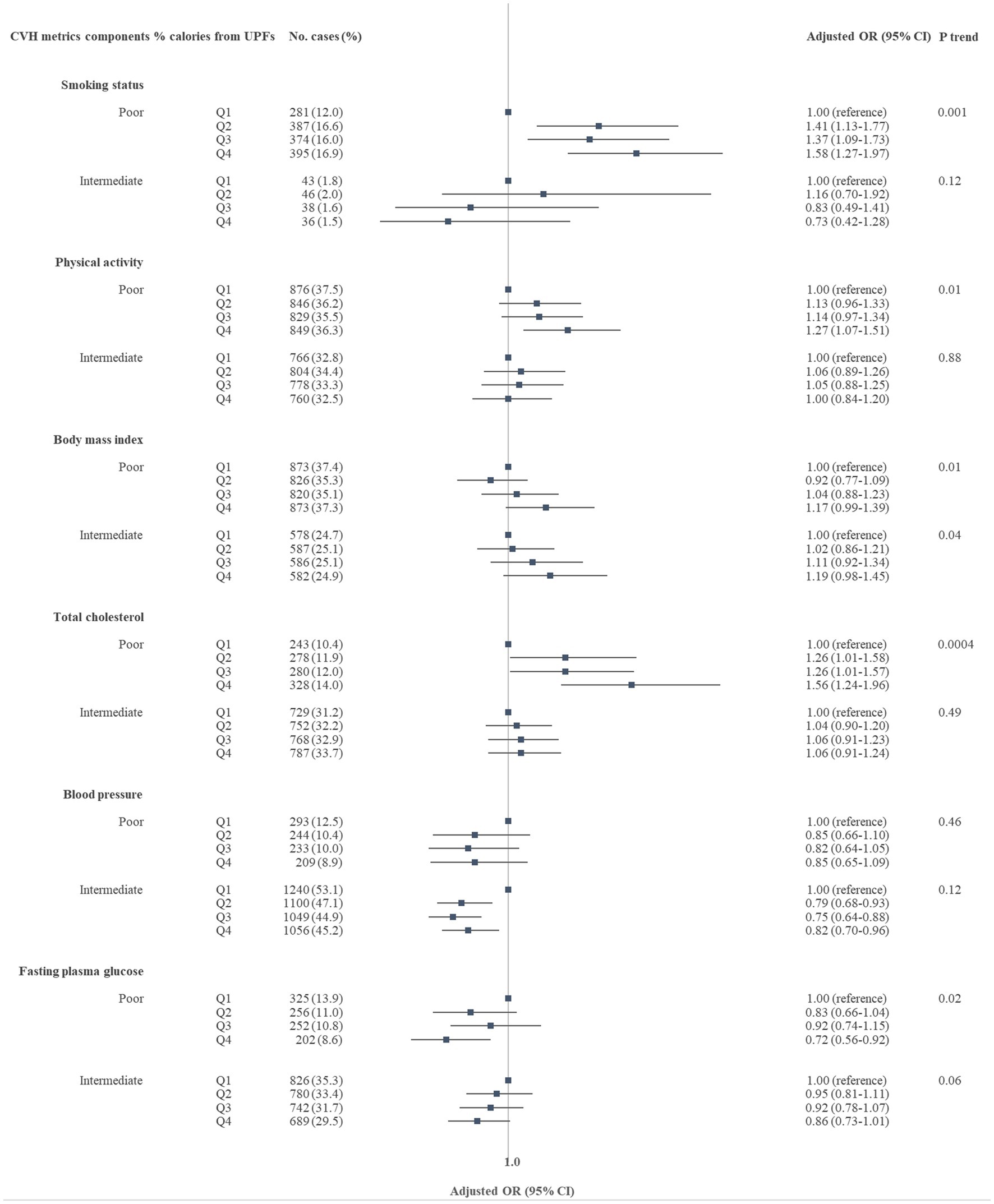
Figure 1. Adjusted odds ratios (95% confidence intervals) for poor or intermediate cardiovascular health metric (CVH) of each individual CVH metric associated with percentage of energy intake from ultra-processed foods, Korean adults aged 40 years and older, KNHANES 2016–2018. KNHANES, Korea National Health and Nutrition Examination Survey; UPFs, ultra-processed foods; Q, quartile; CVH, cardiovascular health (excluding diet component). Multinomial logistic regression models were used to estimate odds ratios and corresponding 95% CIs. All estimated were weighted and adjusted for age (40s, 50s, and ≥ 60 y), sex (males, females), residential area (urban or rural), high school graduate (yes, no), monthly household income quartiles, marital status (yes, no), and other individual CVH components except itself. The median value of percentages of energy intake from UPFs were 5.2% for quartile 1, 19.9% for quartile 2, 26.6% for quartile 3, and 45.6% for quartile 4, respectively.
Subgroup analysis
Education-level stratified analysis shows that the positive association between %E from UPFs and inadequate CVH was greater for participants with a lower education level than those with a higher education level (p-interaction = 0.04) (Table 3). Participants with a lower education level in the highest quartile of %E from UPFs had 1.79 times higher odds of inadequate CVH than those in the lowest quartile (OR 1.79, 95% CI 1.11–2.89, p-trend = 0.02). Participants with a higher education level in the highest quartile of %E from UPFs had 1.28 times higher odds of inadequate CVH than those in the lowest quartile (OR 1.28, 95% CI 1.06–1.55, P-trend = 0.84).
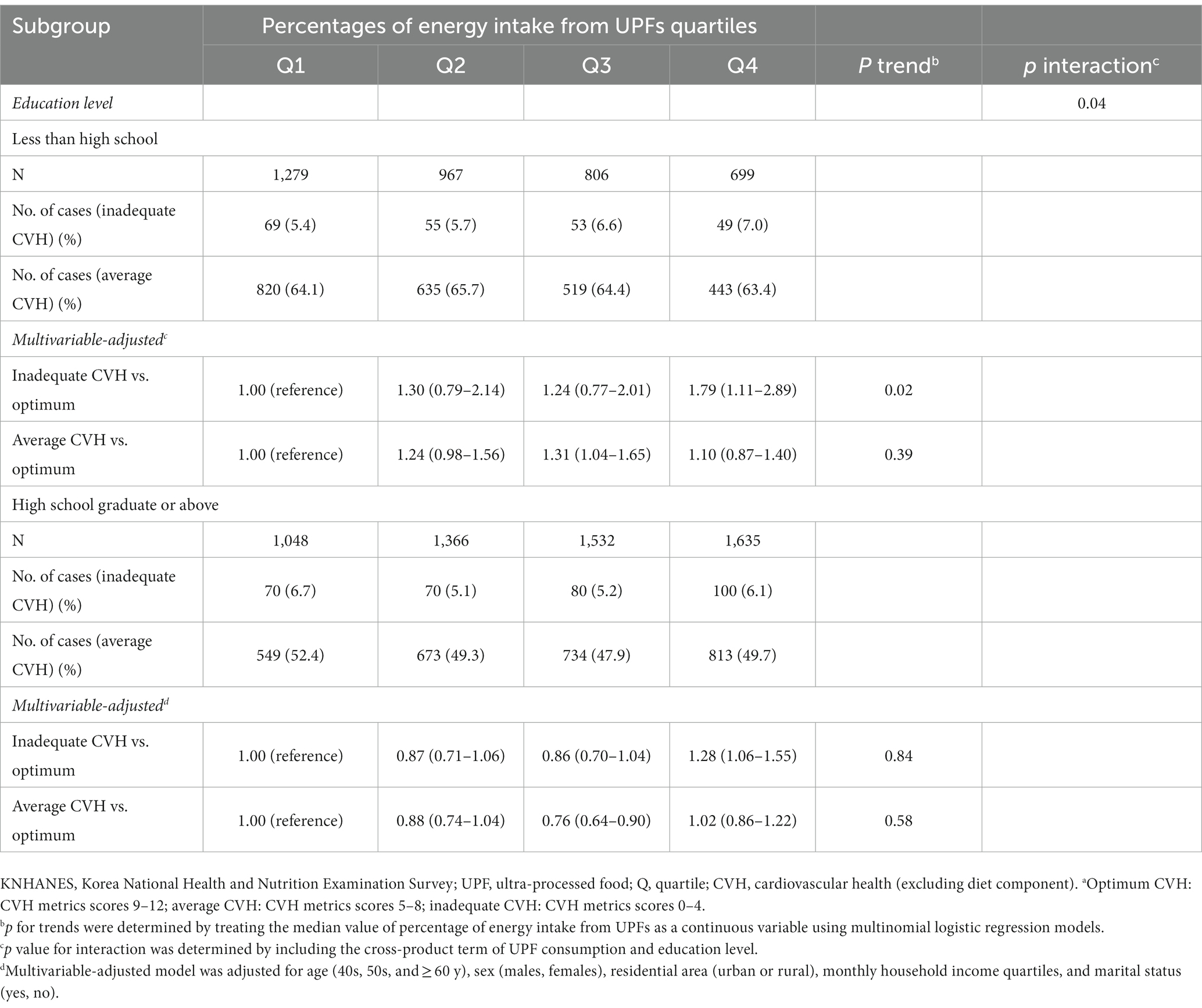
Table 3. Weighted odds ratios (95% confidence intervals) for cardiovascular health metrics across quartiles of ultra-processed food consumption and education level, Korean adults aged 40 years and older, KNHANES 2016–2018a.
Discussion
In this cross-sectional study of Korean adults, we observed a positive association between %E from UPFs and inadequate CVH after adjusting for sociodemographic characteristics. A higher %E from UPFs was associated with poorer individual CVH metrics, specifically current smoking, physical inactivity, higher BMI, and higher total cholesterol. Unexpectedly, there was an inverse association between UPF consumption and blood pressure and fasting plasma glucose. When stratified by education level, a stronger positive association between UPF consumption and inadequate CVH was observed in participants with a lower education level than in those with a higher education level.
A previous cross-sectional study reported that a higher %E from UPFs is linearly associated with 1.4–2.6 times higher odds of inadequate CVH in US adults (17). In our study, comparing quartiles 2, 3, and 4 with quartile 1 of %E from UPFs, the multivariable-adjusted ORs for inadequate CVH (compared with optimum) were 0.8, 0.8, and 1.3, respectively. This discrepancy may be explained by the considerable differences in the amount of UPF consumption between US and Korean adults. The midpoint of %E from UPFs ranged from 40.4 to 70.5% in US adults (17), while it ranged from 5.2 to 45.6% in Korean adults. Considerably lower levels of UPF consumption among Korean adults may not be enough to detect significant associations with CVH.
Regarding individual metabolic CVH metrics, collective evidence suggests a positive association between UPF consumption and the risk of obesity, type 2 diabetes, and hypertension (10, 14, 16). A cohort study in older Spanish adults showed that higher UPF consumption is associated with a higher risk of dyslipidemia incidence (15). In Korea, high UPF consumption is positively associated with obesity only in women and an increased prevalence of elevated blood pressure in adults (27, 28). In our sample, there were positive associations between %E from UPFs and BMI and total cholesterol. As well supported both in the literature (8, 9) and our study, UPFs are high in energy density, trans and saturated fats, sodium, and sugar, but low in dietary fiber and several vitamins and minerals. Biological plausibility between unfavorable profiles of these nutrients in UPFs and metabolic risk factors for CVD includes increased oxidative stress and inflammation, enhancing visceral adipocyte hypertrophy, and glucose intolerance (29–31). Furthermore, high-intensity flavorings and low fiber content may disrupt digestion and satiety, which facilitate overeating and inhibit the glycemic response (32, 33). Some UPFs also contain harmful materials added during processing (e.g., food additives) and chemicals added while packaging (e.g., bisphenol A), which may be associated with negative health outcomes (34, 35).
In contrast to our hypothesis, we observed an inverse association between UPF consumption and blood pressure and fasting blood glucose. One possible explanation for this finding is that UPFs may include some dairy products (e.g., yogurt), which may play a beneficial role in diabetes or high blood pressure (36–38). In our sample, participants in the highest UPF consumption quartile group are likely to consume more dairy products than those in the lowest quartile group (Q1 vs. Q4, 53.1 g/day vs. 88.5 g/day) (Supplementary Table 2). Alternatively, it is possible that individuals with diabetes or hypertension may change their diets to be healthier and reduce UPF consumption, leading to potential reverse causation and biasing our findings. Further studies, using a cohort study design, are warranted to address this issue.
We found that the positive association between UPF consumption and inadequate CVH was more prominent in participants with lower education levels compared to those with higher education levels. Although participants with higher education levels consumed a higher %E from UPFs, it is possible that they consume more “premium” UPFs that tend to have healthier ingredients and functional attributes, such as granola with probiotics, than traditional UPFs. Premium UPFs can be expensive, and individuals with lower sociodemographic status may not have easy access to or cannot afford these products (39, 40). Further research is necessary to explore this matter and better understand the role of specific ingredients in the UPFs consumed, particularly in populations with different socioeconomic backgrounds.
This study has strengths. To our knowledge, this study is the first to evaluate the association between UPF consumption and CVH metrics in a nationally representative sample of Korean adults aged 40 years and older. A Korean NOVA system used in this study, based on the matrix maintenance of natural foods and traditional eating experiences, allowed us to consider the characteristics of Korean cuisine, which is dish-based with the combination of many different specific ingredients, and thus classify UPFs more accurately (24). There were several limitations. First, our findings were based on a cross-sectional survey, which precludes making causal inferences. Second, despite adjusting for several covariates, the results might still have been impacted by unidentified or unmeasured variables. Third, the use of only one 24-h dietary recall may not accurately reflect an individual’s usual intake due to day-to-day variation (a source of within-person error). Fourth, there are inevitable measurement errors due to the use of several self-reported variables (e.g., smoking status). Fifth, the simplistic definition, one of the unresolved issues of the NOVA classification system (41), may make it challenging to differentiate premium UPFs from conventional ones.
In conclusion, a higher %E from UPFs may be associated with poorer CVH in a nationally representative sample of Korean adults. The positive association between UPF consumption and CVH was more evident among those with a lower education level. Although our study is cross-sectional and cannot establish causality, our results could be used as evidence to recommend limiting UPF consumption for CVH improvement. Further studies with a prospective study design are required to establish a causal relationship, and investigating the underlying mechanisms of the association between UPF consumption and CVH can provide more definite evidence.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by the Institutional Review Board of Hallym University. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author contributions
SJ: methodology, data curation, formal analysis, visualization, writing – original draft preparation, and writing – reviewing and editing. EJ and HL: writing – original draft preparation. JK: data curation and methodology. SP: conceptualization, writing – reviewing and editing, and supervision. All gave final approval and agreed to be accountable for all aspects of ensuring integrity and accuracy. All authors contributed to the article and approved the submitted version.
Funding
This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (2021R1I1A3060248 and 2021R1A6A1A03044501).
Acknowledgments
The authors would like to thank all the participants and colleagues for their contribution to this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2023.1219216/full#supplementary-material
References
1. World Health Organization. Cardiovascular diseases (CVDs) fact sheet. WHO (2023). Available at: www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed February 26, 2023).
2. Noh, H, Seo, J, Lee, S, Yi, N, Park, S, and Huh, S. Statistical analysis of the cause of death in Korea in 2019. J Korean Med Assoc. (2022) 65:748–57. doi: 10.5124/jkma.2022.65.11.748
3. Lloyd-Jones, DM, Hong, Y, Labarthe, D, Mozaffarian, D, Appel, LJ, van Horn, L, et al. Defining and setting national goals for cardiovascular health promotion and disease reduction: the American Heart Association's strategic impact goal through 2020 and beyond. Circulation. (2010) 121:586–613. doi: 10.1161/circulationaha.109.192703
4. Vaduganathan, M, Mensah, GA, Turco, JV, Fuster, V, and Roth, GA. The global burden of cardiovascular diseases and risk: a compass for future health. J Am Coll Cardiol. (2022) 80:2361–71. doi: 10.1016/j.jacc.2022.11.005
5. Guo, L, and Zhang, S. Association between ideal cardiovascular health metrics and risk of cardiovascular events or mortality: a meta-analysis of prospective studies. Clin Cardiol. (2017) 40:1339–46. doi: 10.1002/clc.22836
6. Aneni, EC, Crippa, A, Osondu, CU, Valero-Elizondo, J, Younus, A, Nasir, K, et al. Estimates of mortality benefit from ideal cardiovascular health metrics: a dose response Meta-analysis. J Am Heart Assoc. (2017) 6:6. doi: 10.1161/jaha.117.006904
7. Popkin, BM, and Ng, SW. The nutrition transition to a stage of high obesity and noncommunicable disease prevalence dominated by ultra-processed foods is not inevitable. Obes Rev. (2022) 23:e13366. doi: 10.1111/obr.13366
8. Monteiro, CA, Cannon, G, Moubarac, JC, Levy, RB, Louzada, MLC, and Jaime, PC. The UN decade of nutrition, the NOVA food classification and the trouble with ultra-processing. Public Health Nutr. (2018) 21:5–17. doi: 10.1017/s1368980017000234
9. Martini, D, Godos, J, Bonaccio, M, Vitaglione, P, and Grosso, G. Ultra-processed foods and nutritional dietary profile: a meta-analysis of nationally representative samples. Nutrients. (2021) 13:13. doi: 10.3390/nu13103390
10. Delpino, FM, Figueiredo, LM, Bielemann, RM, da Silva, BGC, dos Santos, FS, Mintem, GC, et al. Ultra-processed food and risk of type 2 diabetes: a systematic review and meta-analysis of longitudinal studies. Int J Epidemiol. (2022) 51:1120–41. doi: 10.1093/ije/dyab247
11. Fiolet, T, Srour, B, Sellem, L, Kesse-Guyot, E, Allès, B, Méjean, C, et al. Consumption of ultra-processed foods and cancer risk: results from NutriNet-Santé prospective cohort. BMJ. (2018) 360:k322. doi: 10.1136/bmj.k322
12. Yuan, L, Hu, H, Li, T, Zhang, J, Feng, Y, Yang, X, et al. Dose–response meta-analysis of ultra-processed food with risk of cardiovascular events and all-cause mortality: evidence from prospective cohort studies. Food Funct. (2023) 14:2586–96. doi: 10.1039/D2FO02628G
13. Taneri, PE, Wehrli, F, Roa-Díaz, ZM, Itodo, OA, Salvador, D, Raeisi-Dehkordi, H, et al. Association between ultra-processed food intake and all-cause mortality: a systematic review and Meta-analysis. Am J Epidemiol. (2022) 191:1323–35. doi: 10.1093/aje/kwac039
14. Askari, M, Heshmati, J, Shahinfar, H, Tripathi, N, and Daneshzad, E. Ultra-processed food and the risk of overweight and obesity: a systematic review and meta-analysis of observational studies. Int J Obes. (2020) 44:2080–91. doi: 10.1038/s41366-020-00650-z
15. Donat-Vargas, C, Sandoval-Insausti, H, Rey-García, J, Moreno-Franco, B, Åkesson, A, Banegas, JR, et al. High consumption of ultra-processed food is associated with incident dyslipidemia: a prospective study of older adults. J Nutr. (2021) 151:2390–8. doi: 10.1093/jn/nxab118
16. Wang, M, Du, X, Huang, W, and Xu, Y. Ultra-processed foods consumption increases the risk of hypertension in adults: a systematic review and Meta-analysis. Am J Hypertens. (2022) 35:892–1. doi: 10.1093/ajh/hpac069
17. Zhang, Z, Jackson, SL, Martinez, E, Gillespie, C, and Yang, Q. Association between ultraprocessed food intake and cardiovascular health in US adults: a cross-sectional analysis of the NHANES 2011-2016. Am J Clin Nutr. (2021) 113:428–6. doi: 10.1093/ajcn/nqaa276
18. Zhang, Z, Jackson, SL, Steele, EM, Gillespie, C, and Yang, Q. Relationship between Ultraprocessed food intake and cardiovascular health among U.S. adolescents: results from the National Health and nutrition examination survey 2007-2018. J Adolesc Health. (2022) 70:249–7. doi: 10.1016/j.jadohealth.2021.09.031
19. Shim, JS, Shim, SY, Cha, HJ, Kim, J, and Kim, HC. Socioeconomic characteristics and trends in the consumption of ultra-processed foods in Korea from 2010 to 2018. Nutrients. (2021) 13:13. doi: 10.3390/nu13041120
20. Kweon, S, Kim, Y, Jang, MJ, Kim, Y, Kim, K, Choi, S, et al. Data resource profile: the Korea National Health and nutrition examination survey (KNHANES). Int J Epidemiol. (2014) 43:69–77. doi: 10.1093/ije/dyt228
21. Korea Disease Control and Prevention Agency. Korea health statistics (2018): Korea National Health and nutrition examination survey (KNHANES VIII). Sejong: Korea Disease Control and Prevention Agency (2019).
22. Rural Development Administration, National Institute of Agriculatural sciences (KR). Standard food composition table. 9th ed. Suwon: Rural development Administration, National Institute of Agriculatural Sciences (2016).
23. Monteiro, CA, Cannon, G, Levy, RB, Moubarac, JC, Louzada, MLC, Rauber, F, et al. Ultra-processed foods: what they are and how to identify them. Public Health Nutr. (2019) 22:936–1. doi: 10.1017/s1368980018003762
24. Park, HJ, Park, S, and Kim, JY. Development of Korean NOVA food classification and estimation of ultra-processed food intake among adults: using 2018 Korea National Health and nutrition examination survey. Kor J Commun Nutr. (2022) 27:455–7. doi: 10.5720/kjcn.2022.27.6.455
25. Korean Society for the Study of Obesity. Guideline for the management of obesity 2018. Seoul: Korean Society for the Study of Obesity (2018).
26. Desquilbet, L, and Mariotti, F. Dose-response analyses using restricted cubic spline functions in public health research. Stat Med. (2010) 29:1057. doi: 10.1002/sim.3841
27. Sung, H, Park, JM, Oh, SU, Ha, K, and Joung, H. Consumption of ultra-processed foods increases the likelihood of having obesity in Korean women. Nutrients. (2021) 13:698. doi: 10.3390/nu13020698
28. Shim, SY, Kim, HC, and Shim, JS. Consumption of ultra-processed food and blood pressure in Korean adults. Korean Circ J. (2022) 52:60–70. doi: 10.4070/kcj.2021.0228
29. Park, Y, Jang, J, Lee, D, and Yoon, M. Vitamin C inhibits visceral adipocyte hypertrophy and lowers blood glucose levels in high-fat-diet-induced obese C57BL/6J mice. Biomed Sci Lett. (2018) 24:311–8. doi: 10.15616/BSL.2018.24.4.311
30. Han, SF, Jiao, J, Zhang, W, Xu, JY, Zhang, W, Fu, CL, et al. Lipolysis and thermogenesis in adipose tissues as new potential mechanisms for metabolic benefits of dietary fiber. Nutrition. (2017) 33:118–4. doi: 10.1016/j.nut.2016.05.006
31. Prasad, K, and Dhar, I. Oxidative stress as a mechanism of added sugar-induced cardiovascular disease. Int J Angiol. (2014) 23:217–6. doi: 10.1055/s-0034-1387169
32. Fardet, A. Minimally processed foods are more satiating and less hyperglycemic than ultra-processed foods: a preliminary study with 98 ready-to-eat foods. Food Funct. (2016) 7:2338–46. doi: 10.1039/c6fo00107f
33. Holt, SH, Miller, JC, Petocz, P, and Farmakalidis, E. A satiety index of common foods. Eur J Clin Nutr. (1995) 49:675–09.
34. Ali, A, More, TA, and Shaikh, Z. Artificial sweeteners and their health implications: a review. Biosci Biotechnol Res Asia. (2021) 18:227–7. doi: 10.13005/bbra/2910
35. Rancière, F, Lyons, JG, Loh, VH, Botton, J, Galloway, T, Wang, T, et al. Bisphenol a and the risk of cardiometabolic disorders: a systematic review with meta-analysis of the epidemiological evidence. Environ Health. (2015) 14:46. doi: 10.1186/s12940-015-0036-5
36. Li, W, Ruan, W, Peng, Y, and Wang, D. Soy and the risk of type 2 diabetes mellitus: a systematic review and meta-analysis of observational studies. Diabetes Res Clin Pract. (2018) 137:190–9. doi: 10.1016/j.diabres.2018.01.010
37. Mosallanezhad, Z, Mahmoodi, M, Ranjbar, S, Hosseini, R, Clark, CCT, Carson-Chahhoud, K, et al. Soy intake is associated with lowering blood pressure in adults: a systematic review and meta-analysis of randomized double-blind placebo-controlled trials. Complement Ther Med. (2021) 59:102692. doi: 10.1016/j.ctim.2021.102692
38. Feng, Y, Zhao, Y, Liu, J, Huang, Z, Yang, X, Qin, P, et al. Consumption of dairy products and the risk of overweight or obesity, hypertension, and type 2 diabetes mellitus: a dose-response Meta-analysis and systematic review of cohort studies. Adv Nutr. (2022) 13:2165–79. doi: 10.1093/advances/nmac096
39. Monteiro, CA. Nutrition and health the issue is not food, nor nutrients, so much as processing. Public Health Nutr. (2009) 12:729–1. doi: 10.1017/s1368980009005291
40. Juul, F, Parekh, N, Martinez-Steele, E, Monteiro, CA, and Chang, VW. Ultra-processed food consumption among US adults from 2001 to 2018. Am J Clin Nutr. (2022) 115:211–1. doi: 10.1093/ajcn/nqab305
Keywords: ultra-processed foods, cardiovascular health, Korea National Health and Nutrition Examination Survey, Korea, odds ratio
Citation: Jung S, Jang E, Lee H, Kim JY and Park S (2023) Higher consumption of ultra-processed food is associated with cardiovascular risk in Korean adults: KNHANES 2016–2018. Front. Nutr. 10:1219216. doi: 10.3389/fnut.2023.1219216
Edited by:
Iain Brownlee, Northumbria University, United KingdomReviewed by:
Leila Itani, Beirut Arab University, LebanonSusmita Sinha, Khulna City Medical College and Hospital, Bangladesh
Copyright © 2023 Jung, Jang, Lee, Kim and Park. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sohyun Park, c29wYXJrQGhhbGx5bS5hYy5rcg==
†These authors have contributed equally to this work and share first authorship