 Danielle Pessoa Lima1,2*†
Danielle Pessoa Lima1,2*† Pauliana Alencar Monteiro3†João Rafael Gomes de Luna1
Pauliana Alencar Monteiro3†João Rafael Gomes de Luna1 Antonio Brazil Viana-Júnior4Lucas Tadeu Rocha Santos1
Antonio Brazil Viana-Júnior4Lucas Tadeu Rocha Santos1 Samuel Brito de Almeida1Rayanne Rego Ferreira Saldanha2Madeleine Sales de Alencar1Fábia Karine de Moura Lopes4
Samuel Brito de Almeida1Rayanne Rego Ferreira Saldanha2Madeleine Sales de Alencar1Fábia Karine de Moura Lopes4 Átila Pereira Alencar1Raisa Carvalho de Brito Arcanjo Chaves1Wallena Cavalcante Brito1
Átila Pereira Alencar1Raisa Carvalho de Brito Arcanjo Chaves1Wallena Cavalcante Brito1 Paulo Ribeiro Nóbrega5Alexandre Bastos Lima1
Paulo Ribeiro Nóbrega5Alexandre Bastos Lima1 Pedro Braga-Neto5,6Jarbas de Sá Roriz-Filho1
Pedro Braga-Neto5,6Jarbas de Sá Roriz-Filho1 Renan Magalhaes Montenegro Júnior4
Renan Magalhaes Montenegro Júnior4- 1Division of Geriatrics, Department of Clinical Medicine, Federal University of Ceará, Fortaleza, Brazil
- 2Medical School, University of Fortaleza, Fortaleza, Brazil
- 3Postgraduate Program in Public Health, Medical School, Federal University of Ceará, Fortaleza, Brazil
- 4Clinical Research Unit of Walter Cantídio Universitary Hospital, Federal University of Ceará, Fortaleza, Brazil
- 5Division of Neurology, Department of Clinical Medicine, Federal University of Ceará, Fortaleza, Brazil
- 6Center of Health Sciences, State University of Ceará, Fortaleza, Brazil
Parkinson’s disease (PD) is a progressive neurodegenerative disorder characterized by motor and non motor symptoms. Nutritional status, particularly protein intake, plays a crucial role in managing PD symptoms and preventing complications such as sarcopenia. In Brazil, only 38% of the elderly frequently consume protein-rich foods. The aim of this study was to evaluate the association of protein quantity in the diet of patients with mild to moderate PD with clinical, physical, and body composition factors. A cross-sectional study was conducted involving PD patients in Hoehn and Yahr (HY) stages 1 to 3. Protein intake was assessed using dietary recall, body composition was measured using dual-energy X-ray absorptiometry (DXA), and sarcopenia was assessed following the Revised European Consensus of Sarcopenia. The mean SARC-F score was 3.97, with 51% patients screening positive for sarcopenia. The average handgrip strength was 29, 20% patients had low handgrip strength. The average Short Physical Performance Battery (SPPB) score was 8.87. Confirmed sarcopenia was present in 10% of the sample. Low protein intake (<1 g/kg/day) was observed in 35% of patients and was associated with positive screening of sarcopenia (SARC-F ≥ 4), low lean appendicular mass, and high fat mass index. We did not include patients with severe disease who exhibit more malnutrition, dysphagia, cognitive impairment, dyskinesias, and consequently more sarcopenia. We cannot, therefore, extrapolate these results to all patients with PD. Accordingly, a deeper understanding of the relationship between protein intake and body composition in PD may enhance long-term outcomes for patients.
1 Introduction
Parkinson’s disease (PD) is a progressive neurodegenerative disease with both motor (bradykinesia, rigidity, tremor and postural instability) and non-motor symptoms, including gastroparesis, constipation, depression, anxiety, and cognitive impairment in addition to dopaminergic medication side effects, which can make it difficult to maintain proper nutrition (1). Besides, levodopa absorption is impaired by amino acids in the small intestine. Spacing meals and redistributing proteins to allow a gap of 1 hour between levodopa administration and eating enhances the drug’s bioavailability. This non-pharmacological approach is often used to improve levodopa brain levels (2).
PD is the most rapidly increasing neurological disorder globally, with a 60% rise in age standardized prevalence between 1990 and 2021. With an aging population, the impact of PD and the resulting strain on health and social care systems are expected to rise, making this increase in prevalence a public health issue. Currently, PD is the second most prevalent neurodegenerative disorder worldwide. While the global prevalence of PD has increased over recent decades, there are significant geographic variations in this trend, with a particularly higher increase observed in countries such as China and the United States (3).
A systematic review and meta-analysis identified a continuous increase in PD prevalence from 1980 to 2023, with a more pronounced acceleration between 2004 and 2023. This growth is associated with various risk factors beyond population aging, including environmental and metabolic influences, lifestyle factors, and dietary habits, all of which are impacted by industrialization and urbanization. Environmental exposures, such as air pollution, pesticides, solvents, and heavy metals, are more prevalent in countries with higher socioeconomic indices, including the Sociodemographic Index (SDI) and Human Development Index (HDI), and may contribute to the rising prevalence of PD in these regions (3).
This discrepancy suggests that environmental factors may play a crucial role in the rising incidence of PD. In response to this growing concern, the World Health Organization (WHO) has recommended reducing exposure to specific environmental factors associated with PD development, with particular emphasis on pesticides, trichloroethylene, and air pollution (4).
Sarcopenia is characterized by a loss of muscle mass and strength and is associated with unfavorable outcomes such as falls, frailty, loss of physical function, loss of independence and poorer quality of life (5). Although recognized as a muscle disease since 2016, the diagnosis of sarcopenia is rarely made or documented in medical records (5, 6). Decreased caloric intake may result in a decline in muscle mass and quality (7). Nutrition is a significant contributing factor in the intricate causes of sarcopenia and frailty (8). In Brazil, according to the Household Budget Survey published in 2020, only 38% of the elderly frequently consume protein-rich foods (9). Additionally, the prevalence of low protein intake reaches 21.5, 46.7%, or 70.8% when the adopted cut-off point is 0.8 g/kg/day, 1.0 g/kg/day, or 1.2 g/kg/day, respectively (10).
Sarcopenia is more prevalent in patients with PD due to multiple factors, including mitochondrial dysfunction, chronic inflammation, an imbalance between protein synthesis and degradation, and reduced physical activity (11, 12). Studies indicate that the prevalence of sarcopenia among individuals with PD ranges from 10.9 to 31.4%, depending on the diagnostic criteria applied (7). Furthermore, the coexistence of sarcopenia and PD is associated with a reduced quality of life, an increased risk of falls, and accelerated mobility decline (5, 7). Despite these findings, the role of dietary protein intake in sarcopenia-related outcomes in PD remains insufficiently understood. Investigating this relationship is essential for the development of targeted nutritional strategies aimed at mitigating sarcopenia and its associated impairments in individuals with PD. Adequate protein ingestion may affect the net balance of muscle protein production (13, 14).
An adequate protein diet may reverse or at least delay functional decline in frail older persons. There is a scarcity of evidence on protein intake in PD (15). The aim of this study was to evaluate the association of protein quantity in the diet of patients with mild to moderate PD with clinical, physical, and body composition factors.
2 Materials and methods
2.1 Study design
This study was carried out from May 2021 to April 2022 in the Neurology outpatient clinic at a public tertiary Brazilian hospital. The clinical diagnosis of PD and classification in stages 1 to 3 on the modified Hoehn & Yahr scale were eligibility criteria, as well as having the ability to stand and walk without assistance and being aged 50 years or older. Figure 1 shows the flowchart of the recruitment process of the study.
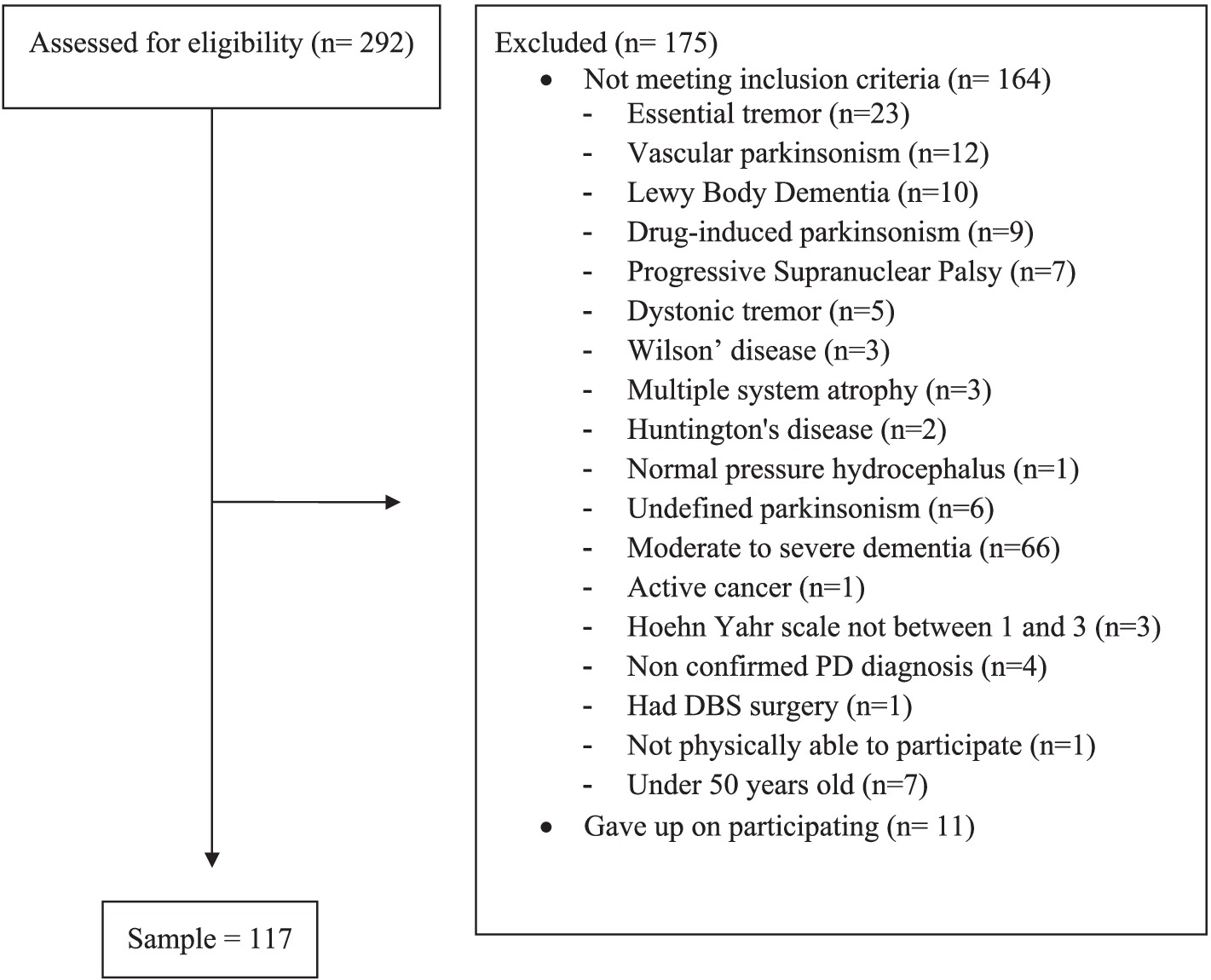
Figure 1. Flowchart of the recruitment process.
2.2 Elegibility criteria
We excluded patients with severe health conditions or uncontrolled chronic disease that could compromise their safety in carrying out the research procedures or the interpretation of findings, such as: heart failure functional class III and IV of the New York Heart Association; chronic kidney disease on dialysis; neurological diseases with motor impairment (except PD); moderate to severe dementia (Clinical Dementia Rating 2 and 3); severe chronic obstructive pulmonary disease (dyspnea with minor efforts) or very severe (dyspnea at rest and/or oxygen therapy); diagnosis of cancer, except localized prostate cancer and localized skin cancer, and patients with conditions that would complicate the interpretation of the dual-energy x-ray absorptiometry (DEXA) (use of oral contrast or radio-nuclides in the last 72 h; pregnancy; deep brain stimulation; cardiac pacemaker).
2.3 Medical and neurological evaluation
All patient evaluations and examinations were carried out 1 to 3 h after the patients had taken their antiparkinsonian medication (ON phase) and followed their normal medication schedules throughout the data collection phase of the study.
We performed a general medical assessment (demographic data, symptoms/complaints, comorbidities, medications in use), assessed depressive symptoms through the Geriatric Depression Scale-15 (GDS-15) and cognitive status using the Mini Mental Status Exam (MMSE). We also evaluated the number of falls in the last year. Clinical assessment of PD was performed evaluating symptoms/complaints, HY staging, the motor parkinsonian symptoms through the Movement Disorders Society-Unified Parkinsonian Disease Severity-part III (UPDRS-III), levodopa equivalent dose (LED) and capacity of daily living by Schwab and England (SE).
2.4 Sarcopenia assessment
We followed the Revised European Sarcopenia Consensus (EWGSOP2) to investigate sarcopenia. We performed the sarcopenia screening tool called SARC-F, anthropometric measurements (right calf, weight, height), muscular strength assessment (handgrip, using a SAEHAN dynamometer) and physical performance through the Short Physical Performance Battery (SPPB). The SARC-F questionnaire includes five questions that assess hand strength for lifting a 5 kg weight, thigh strength for standing up from a chair, strength and balance for walking between rooms and climbing 10 flights of stairs, and a history of falls (5).
2.5 Body composition analysis
We evaluated body composition using the DEXA Lunar Prodigy Advance (General Electric Healthcare) software enCORE version 17. Whole-body DEXA scans were obtained using the manufacturer’s recommendations. The following parameters were analyzed: fat mass (kg), lean mass (kg), percentage of total body fat (%BF), fat mass index (FMI, kg/m2), volume of visceral adipose tissue (VAT), percentage of fat by body segments, and relative skeletal muscle index (RSMI). We interpreted the FMI (total mass fat/height2) according to the National Health and Nutrition Survey (NHANES III) cutoff points (16), considering a normal range for women of 5 to 9 kg/m2 and for men of 3 at 6 kg/m2.
2.6 Dietary assessment
We assessed protein intake using the retrospective dietary survey, 24-h dietary recall. We calculated protein and calcium measurements per kilogram of weight per day from the 24-h dietary recall using Dietbox® Nutrition Software. We considered a protein intake of 1 g/kg/day or more as the minimum adequate for good muscle health in this study (17).
2.7 Definitions
We used the following definition of LED: the dose that produces the same level of symptomatic control as 100 mg of immediate-release L-dopa, according to the systematic review of Tomlinson et al. (18). A fall was considered a situation in which the patient involuntarily fell to the floor or another lower level and was not due to a convulsive event, vehicle or bicycle accident or syncope. The Calf Circumference (CC) measurement was taken using a non-stretchable tape measure, with the patient seated and the knee bent at 90°, feet spaced 20 cm apart, at the maximum circumference in the plane perpendicular to the longitudinal line of the calf. The patient had to remove his/her clothing on the lower body to measure the CC on bare skin. Subcutaneous tissues were not compressed (19).
We followed the recommendations of the EWGSOP2 regarding the measurement of manual handgrip strength and cutoff points (<27 kg for men and <16 kg for women) (5). We used the Southampton protocol to measure the handgrip strength (the patient seated with forearms supported on the arms of the chair, wrist just above the end of the chair arm, in a neutral position, thumb pointing upwards, feet flat on the floor, three attempts on each side, alternating sides, with the highest score from all six attempts recorded) (20).
The SPPB was developed to assess physical performance. The test includes measures of standing balance, 4-meter gait speed, and the time it takes to get up from a chair five times. Patients were told to keep their balance by standing with their feet together before spending 10 s in each of the semi-tandem and tandem postures, which involve positioning one foot’s heel near to the other foot’s big toe. Participants were told to walk along an 8-meter track (with 2-meters of acceleration and 2-meters of deceleration) at their normal pace to assess their gait speed with a stopwatch. Participants were taught to stand up and sit down five times as fast as they could with their arms crossed over their chests to assess their ability to get out of a chair. This was not done until individuals demonstrated that they could stand up once without using their arms. The overall SPPB score was calculated, with a score of less than 8 indicating inadequate physical performance and a maximum score of 12 (21).
Probable sarcopenia was defined as low handgrip strength. Confirmed sarcopenia was diagnosed according to EWGSOP 2 as follows: low muscle strength and low muscle mass—according to the relative skeletal muscle index (RSMI) obtained through DEXA < 7 kg/m2 for men and < 5.5 kg/m2 for women (5). The RSMI is obtained by the appendicular lean mass adjusted for height squared in meters. Low muscle mass is defined as a decrease in appendicular muscle mass two standard deviations below the mean for young healthy adults (5).
2.8 Ethical considerations
All individuals involved in the study gave their written consent after being fully informed about the research, which was approved by the Research Ethics Committee of Hospital Universitário Walter Cantidio (registration number 91075318.1.0000.5045). The study’s researchers spoke with and assessed each patient.
2.9 Statistical analysis
Descriptive statistics were presented as numbers (percentage) for categorical variables and as mean ± standard deviation (median) for quantitative variables. Bivariate analysis for probable and confirmed sarcopenia were performed using the Pearson’s chi-squared test and Fisher’s exact test for categorial variables. Spearman correlation coefficients were calculated to verify the association between protein intake and markers of interest. The Mann–Whitney U test was used to assess quantitative independent variables since they were not normally distributed except for calf circumference, for which Student’s T-test was used. Variables with p < 0.05 entered logistic regression to identify those independently associated with protein intake <=1 g/kg/d. Statistical analyses were performed using RStudio 2023.03.0.
3 Results
Table 1 presents the clinical characteristics of the sample. The study included 117 patients, with 48 (41%) being women. The average age of the participants was 66 years (± 11 years). The most common comorbidities were hypertension (n = 52, 44%), depression (n = 34, 29%), dyslipidemia (n = 18, 15%), and type 2 diabetes mellitus (n = 15, 13%). The average protein intake was 1.19 ± 0.41 g/kg/day, and the average calcium intake was 666 ± 348 mg/day. Low protein intake was observed in 35% (n = 41) of the patients. On average, patients were taking 5.3 ± 2.29 medications, with antidepressants and antihypertensives being the most used.
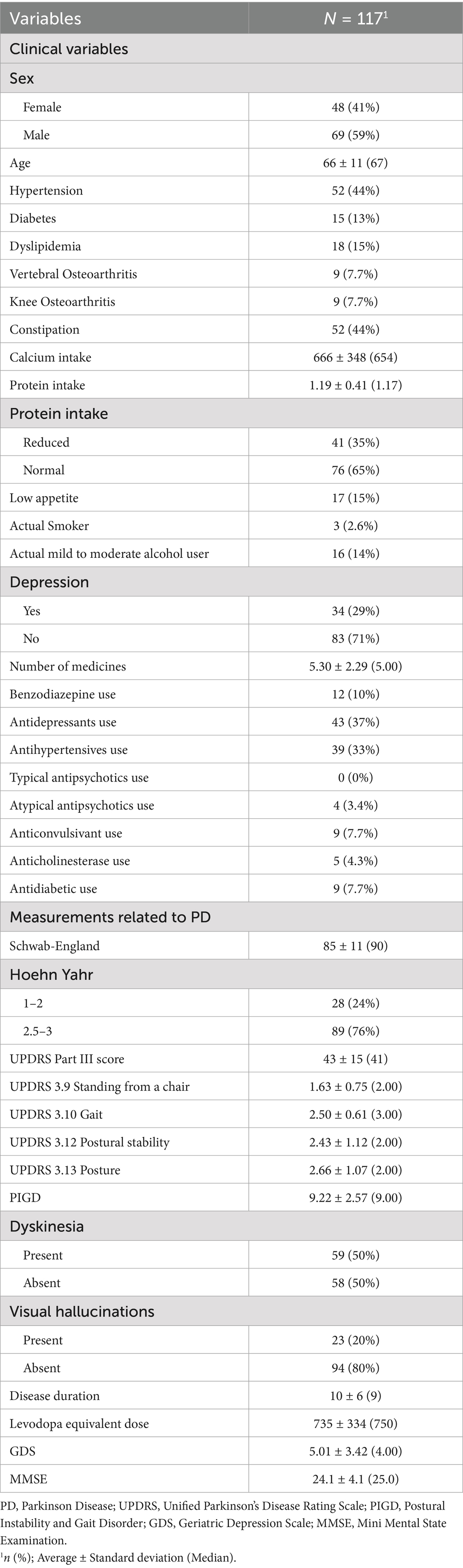
Table 1. Clinical and parkinsonian features of the sample.
Regarding PD characteristics, 28 (24%) patients were in the early stages of the disease (HY 1–2), while 89 (76%) were in the moderate stages (HY 2.5–3). The average disease duration was 10 ± 6 years, with a mean levodopa equivalent dose of 735 ± 334 mg/day. The average UPDRS part 3 score was 43 ± 15. Approximately half of the patients (n = 59) experienced dyskinesias, and 23 (20%) reported visual hallucinations.
The mean SARC-F score was 3.97 ± 2.74, with 59 (51%) patients screening positive for sarcopenia. The average handgrip strength was 29 ± 11 kg, and 23 (20%) patients had low handgrip strength. The average SPPB score was 8.87 ± 2.60. Regarding body composition, the average BMI was 26.2 ± 4.4 kg/m2, the average calf circumference was 33.5 ± 3.6 cm, and the average RSMI was 7.27 ± 1.23 kg/m2. Confirmed sarcopenia was present in 10% (n = 12) of the sample.
Table 2 details physical performance and body composition results. The average number of falls in the past 6 months was 3.85 ± 18.76, and the average walking speed was 1.38 ± 0.52 m/s.
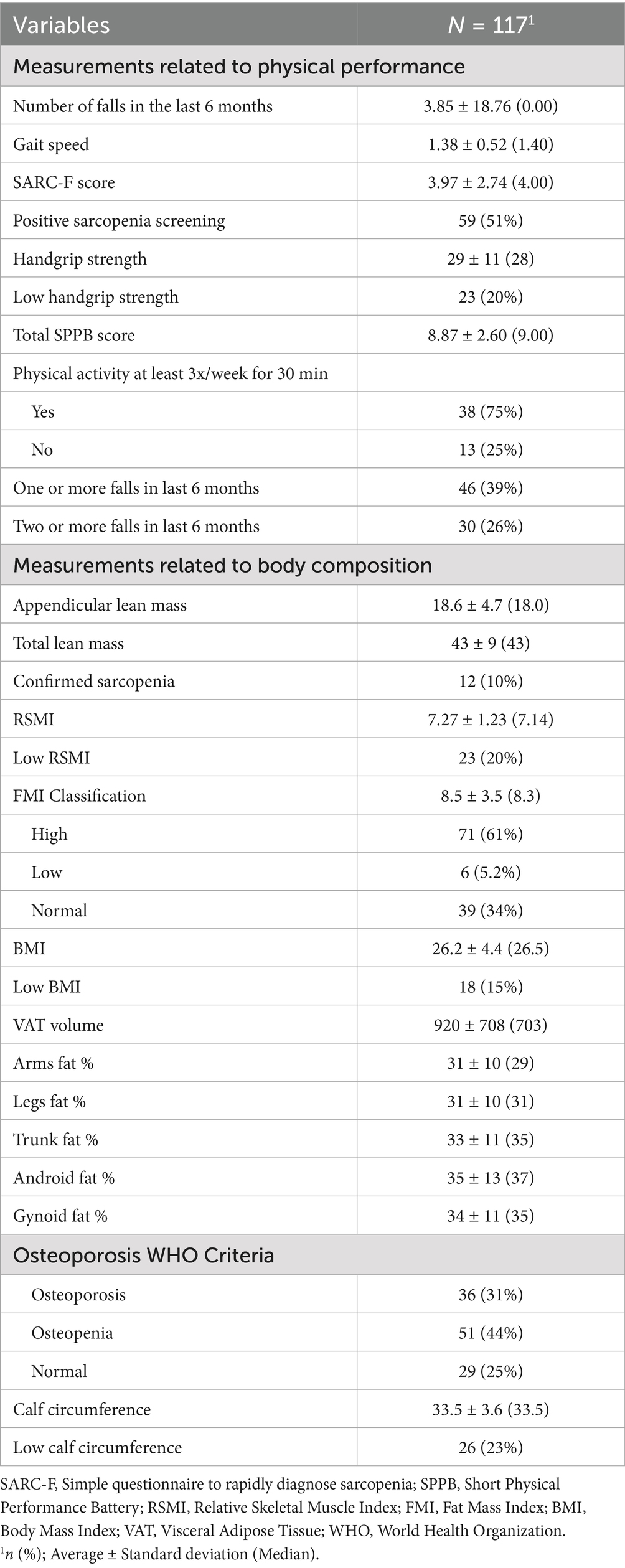
Table 2. Physical performance and body composition features of the sample.
Table 3 shows the bivariate analysis results comparing clinical variables between patients with low and normal protein intake. Low protein intake was significantly associated with female gender, lower calcium intake and decreased appetite.
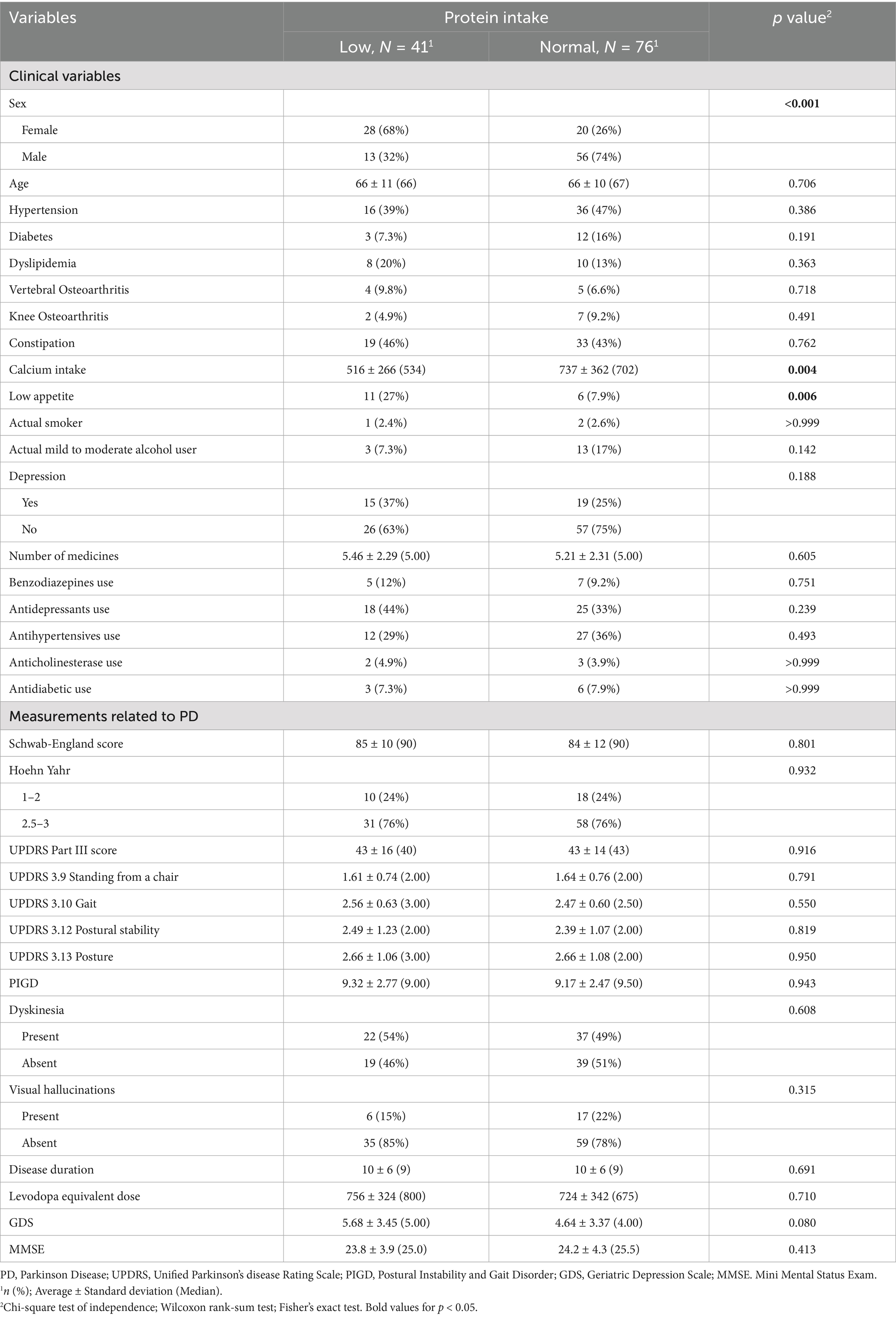
Table 3. Bivariate analysis of clinical variables and protein intake.
Table 4 presents the bivariate analysis results for physical performance and body composition variables. Significant associations with low protein intake included higher SARC-F scores, positive sarcopenia screening, lower handgrip strength, lower appendicular and total lean mass, lower RSMI, higher fat mass index, higher arms, legs, trunk, android and gynoid fats and osteoporosis. Variables that were statistically significant in the bivariate analysis were included in the logistic regression model. Positive sarcopenia screening and higher fat mass index were independently associated with low protein intake in the final model, as shown in Table 5. We excluded SARC-F total score, lower appendicular and total lean mass and the segmentary fat mass due to high multicollinearity based in the Variance Inflation Factor (VIF).
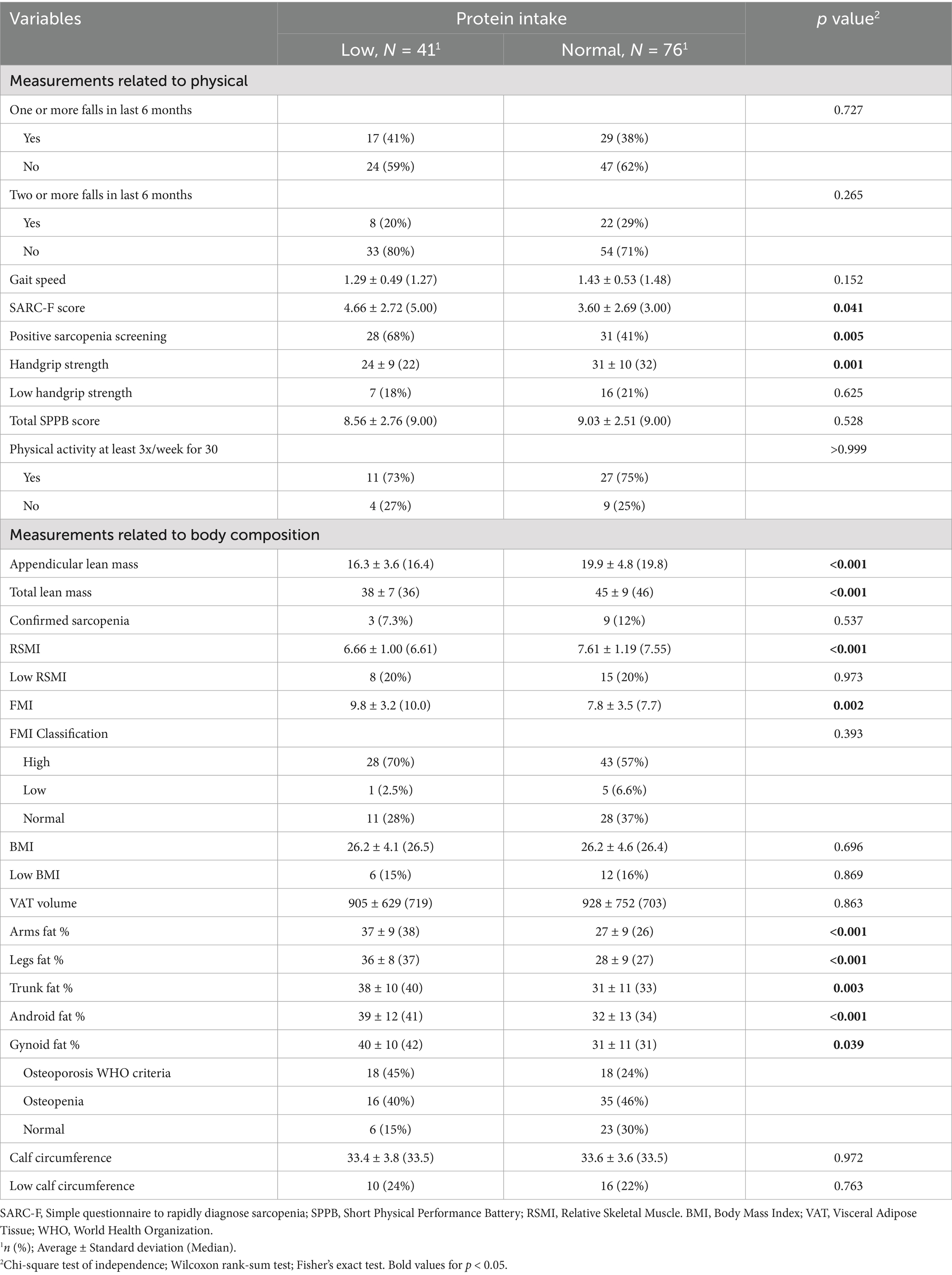
Table 4. Bivariate analysis of physical performance, body composition and protein intake.
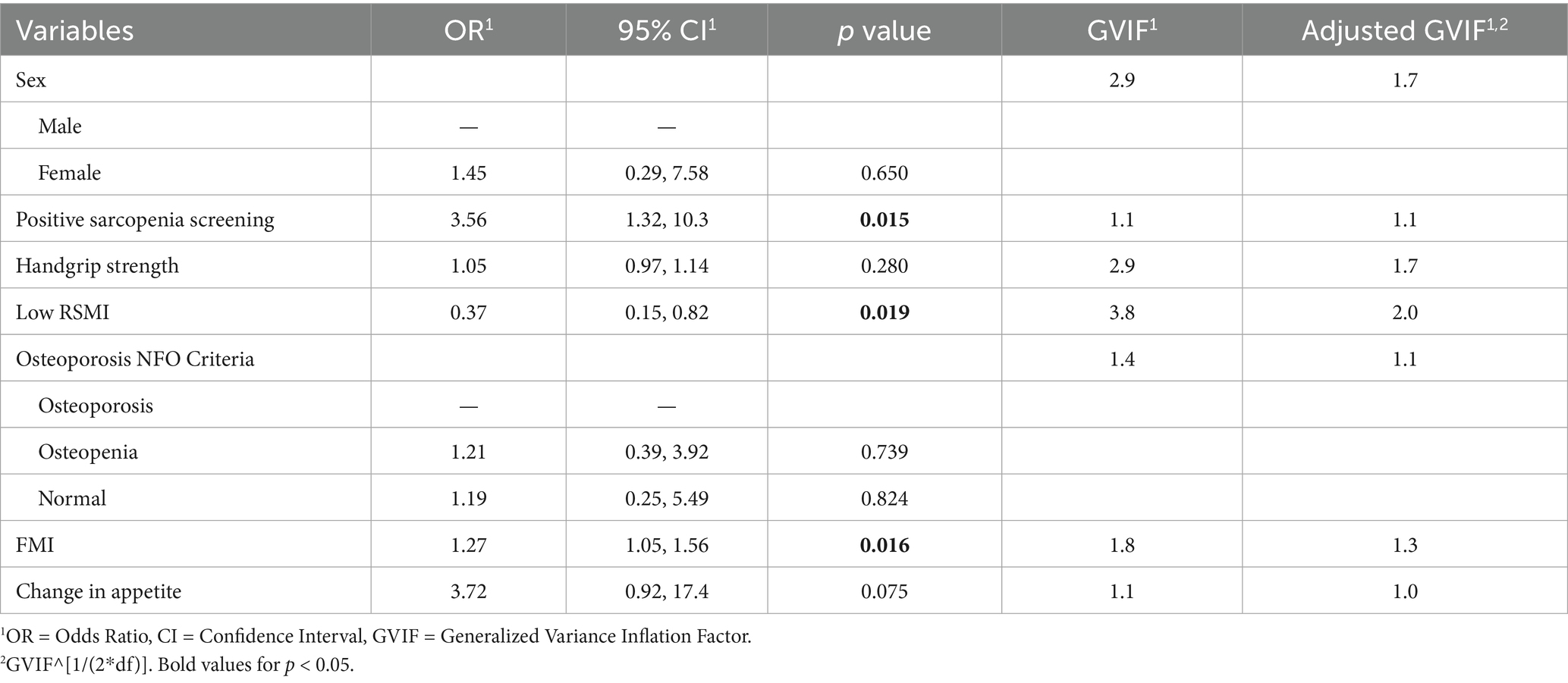
Table 5. Multivariate analysis of protein intake.
The results concerning the Spearman correlation analyses between protein intake and clinical, anthropometric, and body composition variables are presented in Table 6. Fat mass index (rho −0.29; p 0.002) and Geriatric Depression Scale score (rho −0.21; p 0.021) showed a statistically significant inverse correlation with protein intake. Conversely, gait speed (rho 0.19; p 0.042), handgrip strength (rho 0.31; p < 0.001), and appendicular skeletal muscle mass index (rho 0.29; p 0.002) exhibited a statistically significant direct correlation with protein intake.
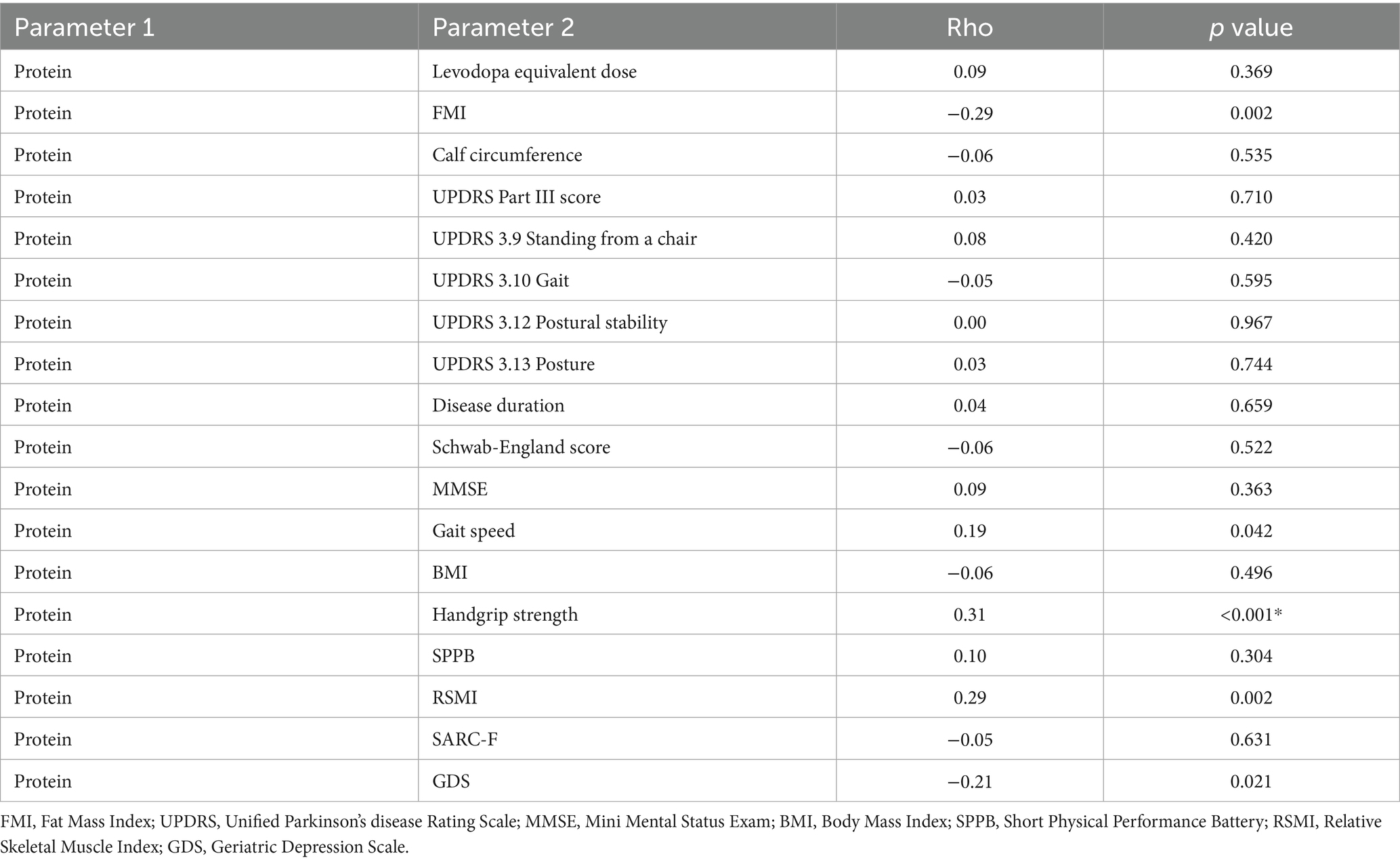
Table 6. Correlation of protein intake and clinical variables.
Besides the concerningly high prevalence of deficient protein intake in this population, the data point toward a significant association with female sex, which may suggest sex-specific dietary patterns or metabolic differences that warrant further exploration. Additionally, the correlation with reduced apetite and low calcium intake underscores potential nutritional deficits in this population, which could exacerbate disease progression or contribute to other health issues. The link between low protein intake and several variables related to sarcopenia highlights the critical role of dietary protein in muscle preservation and function. Furthermore, our results demonstrate an association between low protein intake and unfavorable changes in body composition, potentially reflecting metabolic alterations or lifestyle factors that influence nutritional habits.
4 Discussion
This study aimed to estimate the prevalence of normal and low protein intake in mild to moderate PD patients, which were, respectively, 65% (n = 76) and 35% (n = 41). Clinical, parkinsonian and body composition features of the study sample were also assessed. Low protein intake was independently associated with positive screening for sarcopenia using SARC-F, higher fat mass index and low RSMI.
The average protein intake in our sample was 1.19 ± 0.41 g/kg/day. There are few studies on protein intake in PD, and the prescription of proteins in PD is also controversial, making studies on this subject relevant (22–24). Barrichela et al. conducted an extensive survey examining the dietary habits of individuals with PD. They inter-viewed 600 PD patients (53.8% male) and 600 control subjects (69% from the community) from various regions of Italy. The study found that PD patients had lower body weight and BMI compared to the control group, although their abdominal fat levels were similar. Interestingly, despite having lower energy expenditure and total daily energy expenditure, PD patients had higher calorie intake. Moreover, their total intake of calories, macro-nutrients, and micronutrients were also higher than that of the controls. The authors also described the average daily protein intake of 1.0 g/kg in the control group compared to 1.2 g/kg in PD patients (p < 0.001), which were like our results. Another study performed by Marczewska et al. pointed to average protein consumption by the Parkinsonian population studied (23) was 1.2 g/kg/day. Morais et al. (25) and do Carmo and Ferreira (26) found the average intake of 1.0 g/kg/day, and 1.4 g/kg/day, respectively. As levodopa and amino acids both use the large-neutral amino acid transporter for absorption in the small intestine and at the blood–brain barrier, timing and amount of dietary protein intake are critical in this condition. Levodopa should be taken 30 min before or 1 h after meals to avoid competition and decreased absorption (27). Barichella et al. and other authors suggest a low protein-diet (up to 0.8 g/kg/day) (28–30) or a protein redistribution diet (31–33) such as eating the main protein meal in the evening to make levodopa more effective and reduce motor fluctuations. Most of studies on the interaction between food and medications, particularly for levodopa, were conducted more than 20 years ago (in the 1970s, 1980s, or 1990s) and with poor methodological quality (often non-randomized or without a control group), indicating the need for more studies with better methodology (34).
In older adults, PROT-AGE study group recommends average daily intake of protein in the range of 1.0 to 1.2 g/kg/day (35). ESPEN guideline also suggests protein daily amounts of 1.0–1.2 g/kg/day (19). Both recommendations are related to healthy older adults. According to PROT-AGE study group most older persons with acute or chronic diseases require higher dietary protein (1.2–1.5 g/kg BW/d); but people with severe sickness or injury or noticeable malnutrition may require up to 2.0 g/kg/day (35).
A study conducted in Brazil at the University of São Paulo with 295 older adults, with a mean age of 70.41 ± 7.48 years and a higher proportion of women (81.69%) compared to men (18.31%), found a prevalence of 69.15% of older adults with low protein intake (considered as less than 1 g/kg/day for those who are eutrophic and overweight and less than 1.2 g/kg/day for those who are undernourished) (36). The National Dietary Survey 2008–2009, involving a total of 4,286 Brazilian elderly individuals (aged 60–104 years), revealed the average protein intake of 75.5 grams. Women had a significantly lower average protein intake compared to men (83.6 grams versus 68.3 grams; p < 0.001). The northern region showed the highest protein-energy percentage (21.5%; 95% CI, p < 0.05), while the southern region had the lowest (17.9%; p < 0.01). The protein-energy percentage was greater in rural areas compared to urban areas (20.2% versus 19.8%; p < 0.05) (37).
A higher proportion of men had adequate protein intake comparing to women in the present study. Body composition varies between men and women, with women having proportionally greater fat mass and men having more muscle mass (38). Sex steroids can modulate disparities in body composition. For instance, reduced estrogen levels, such as those encountered during menopause, have been associated to a predilection for visceral adipose tissue (VAT) accumulation and an increased cardiometabolic risk (39). Additionally, decreasing testosterone levels in men can lead to increased visceral fat (40). Furthermore, new genome-wide association studies have identified genetic markers unique to each sex that promote fat formation (41). According to Bennett (42), women consume an average amount of 78 grams/day of protein, while men consume 86.9 grams/day. However, when adjusted for body weight, women’s protein consumption surpassed that of men (1.13 g/kg/day × 1.04 g/kg/day) (42). Regarding body composition, according to Schorr (38), men have a higher amount of muscle mass than women, resulting in an increased need for a higher protein intake (38).
Low protein intake was significantly associated with low handgrip strength in PD patients in the present study. Also, gait speed, handgrip strength and appendicular skeletal muscle mass index exhibited a direct correlation with protein intake. Several studies have also described that lower intake of protein has been linked with lower muscular strength (43–45). Indeed, these findings confirm how essential it is to consume enough protein to maintain muscle strength, especially for populations as older people and those with chronic diseases (44, 46, 47). However, caution is needed with these findings. It is essential to understand that protein intake alone may not fully explain changes in muscular strength, since other factors such as physical activity levels, total food quality, and genetic predispositions all play significant parts (48). The higher the total protein intake up to 1.5 g/kg combined with resistance training, the better effect in muscle strength according to a recent systematic review and meta-analysis (49).
We found an association between low protein intake and higher fat mass index. Protein plays a fundamental role in managing weight and body composition. Diets with a higher amount of protein favor the maintenance or increase of lean mass, in addition to contributing to a reduction in caloric intake (50). This caloric reduction is possibly due to the increase in satiety induced by this macronutrient, an effect that may be related to the stimulation of the secretion of gastrointestinal hormones, such as cholecystokinin and glucagon-like peptide-1 (GLP-1) (51, 52). A higher protein intake is associated with reduced total body fat, including the abdominal region, especially in overweight individuals who practice physical exercise (53–55). Although there is no consensus on the amount of protein needed to promote body fat reduction, evidence suggests that diets with protein intake equal to or greater than 25% of total daily caloric intake or ≥1 g/kg/day show benefits during the process of weight loss in older individuals, preserving lean mass and reducing body fat (56). Weight loss in PD is frequently reported and has been associated especially with the severity of the disease, however, an increase in BMI and a redistribution of body composition, characterized by an increase in body fat and a reduction in muscle mass, have also been shown concomitantly, associated with decreased protein intake (57). However, it is important to highlight that body composition is influenced by several factors in addition to protein intake, such as caloric intake, level and type of physical exercise, genetic aspects, associated diseases, and the use of medications, demonstrating the complexity of mechanisms that regulate body composition (58–61).
Reduced appetite was associated with lower protein intake. Various factors may contribute to reduced appetite in PD, including “inflammaging” (62, 63), dysautonomic symptoms (such as constipation and dyspepsia) (64–66), dysphagia (67), antiparkinsonian side effects (66, 68, 69), depression (65, 69, 70) and dementia syndrome (71, 72). Additionally, these issues are exacerbated by age-related sarcopenia, which can result from inadequate nutrition, physical inactivity, and endocrine dysfunctions, contributing to a negative cycle of reduced appetite and consequently lower protein intake (73–76).
The study also showed association between low protein intake and lean appendicular mass index. Several studies already showed that dietary protein plays a crucial role as it is a modifiable factor that influences the growth and maintenance of skeletal muscle (10, 14, 48–53). A protein intake level of 1 to 1.2 g/kg/day for elderly individuals and those with chronic diseases, along with the consumption of 10 to 15 grams of essential amino acids (containing more than 3 grams of leucine), which corresponds to approximately 25 to 30 grams of high biological value protein in each of the three main meals, is recommended to improve protein synthesis (49, 51, 56, 77).
In the present study, sarcopenia identified by a positive SARC-F questionnaire was independently associated with low protein intake. Sarcopenia and PD are both conditions associated with aging that might have a shared underlying mechanism (78). The SARC-F questionnaire includes five questions that assess hand strength for lifting a 5 kg weight, thigh strength for standing up from a chair, strength and balance for walking between rooms and climbing 10 flights of stairs, and a history of falls (79). The items of the SARC-F are linked to functional performance, and functional performance is associated with adequate protein intake. The association between the SARC-F and protein intake can be explained by the well-established relationship between adequate protein intake and muscle strength (14, 44, 49). Elevated SARC-F scores were strongly correlated with disease severity and dependency in both activities of daily living (ADL) and instrumental activities of daily living (IADL) in the present study. It has been suggested that the SARC-F is more sensitive in detecting muscle function compared to muscle mass (80). Thus, SARC-F may be a tool to assess PD patients for the presence and functional decline.
This study has several limitations. First, it involves a small sample of patients with mild to moderate PD according to HY (1 to 3). Therefore, we did not include patients with severe disease who exhibit more malnutrition, dysphagia, cognitive alterations, dyskinesias, and consequently more sarcopenia. We cannot, therefore, extrapolate these results to all patients with PD. Additionally, the collection of the inventory of protein and calcium consumption was conducted through questions about intake over the last 24 h, which means the values found may be underestimated or overestimated since the information was collected only once. A three-day food intake record is considered a more accurate evaluation method than food frequency questionnaires and 24-h recall, as it allows participants to directly record their food intake and avoid memory bias. The prevalence of sarcopenia varies due to the use of different definitions and diagnostic tools for sarcopenia, as well as patient selection criteria, such as the inclusion of patients with more advanced PD (HY 4–5). Additionally, there are different ways to measure body composition and different diagnostic criteria. All these methodological differences create limitations for comparing our results. The sarcopenia cut-off points used in this study were derived from those recommended by EWGSOP 2 for healthy adults, as there are no defined cut-off points for patients with PD. Moreover, there are currently no validated methods for diagnosing dynapenia by assessing lower limb strength in PD patients. Implementing a validated method to measure lower limb strength is likely to enhance the accuracy of sarcopenia detection in PD patients.
The association between low protein intake and the increased risk of sarcopenia, as well as the reduction in muscle strength in patients with Parkinson’s disease (PD), highlights the importance of regular nutritional monitoring in the management of PD and the prevention of sarcopenia. It is essential to monitor dietary intake, with an emphasis on protein consumption, while also considering other nutritional aspects, such as daily caloric intake, overall diet quality, and related factors. This comprehensive monitoring contributes to the preservation of muscle strength, improved functionality, and the promotion of quality of life for patients. Future research directions include evaluating the impact of dietary changes over time on the progression of PD and complications such as sarcopenia and dynapenia. Studies on the effects of protein supplementation are also necessary, as well as investigations into how nutritional interventions interact with other clinical and lifestyle factors. Additionally, the implementation of technologies, such as dietary tracking apps, can be a valuable tool for conducting more frequent and accurate assessments, optimizing nutritional monitoring and clinical care for these patients.
Our study revealed a significant prevalence of low protein intake among PD patients at HY stages 1–3, based on the ESPEN recommendation (2022) of at least 1 g/kg/day of protein intake. This low intake was independently associated with positive sarcopenia screening through SARC-F, reduced lean appendicular mass, and a high fat mass index. A deeper understanding of the relationship between protein intake and body composition in PD may enhance long-term outcomes for patients. We suggest that healthcare providers inquire about both the quality and quantity of nutrition, as this population is at higher risk for sarcopenia and malnutrition.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Research Ethics Committee of Hospital Universitário Walter Cantídio. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
DL: Conceptualization, Data curation, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing. PM: Conceptualization, Investigation, Methodology, Writing – original draft. JG: Conceptualization, Investigation, Writing – original draft. AV-J: Formal analysis, Software, Writing – review & editing. LS: Writing – review & editing. SA: Writing – original draft. RS: Investigation, Writing – review & editing. MA: Writing – review & editing. FL: Investigation, Writing – original draft. ÁA: Writing – review & editing. RC: Validation, Visualization, Writing – review & editing. WB: Validation, Visualization, Writing – review & editing. PN: Validation, Writing – review & editing. AL: Writing – review & editing. PB -N: Project administration, Resources, Supervision, Visualization, Writing – review & editing. JR-F: Resources, Supervision, Visualization, Writing – review & editing. RM: Conceptualization, Methodology, Project administration, Resources, Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Kacprzyk, KW, Milewska, M, Zarnowska, A, Panczyk, M, Rokicka, G, and Szostak-Wegierek, D. Prevalence of malnutrition in patients with Parkinson’s disease: a systematic review. Nutrients. (2022) 14:5194. doi: 10.3390/nu14235194
2. Boelens Keun, JT, Arnoldussen, IA, Vriend, C, and van de Rest, O. Dietary approaches to improve efficacy and control side effects of levodopa therapy in Parkinson’s disease: a systematic review. Adv Nutr. (2021) 12:2265–87. doi: 10.1093/advances/nmab060
3. Zhu, J, Cui, Y, Zhang, J, Yan, R, Su, D, Zhao, D, et al. Temporal trends in the prevalence of Parkinson’s disease from 1980 to 2023: a systematic review and meta-analysis. Lancet Heal Longev. (2024) 5:e464–79. doi: 10.1016/S2666-7568(24)00094-1
4. Brolin, KA, Schaeffer, E, Kuri, A, and Rumrich, IK. Environmental risk factors for Parkinson’s disease: a critical review and policy implications. Mov Disord. (2025) 40:204–21. doi: 10.1002/mds.30067
5. Cruz-Jentoft, AJ, Bahat, G, Bauer, J, Boirie, Y, Bruyère, O, Cederholm, T, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. (2019) 48:16–31. doi: 10.1093/ageing/afy169
6. Cao, L, and Morley, JE. Sarcopenia is recognized as an independent condition by an international classification of disease, tenth revision, clinical modification (ICD-10-CM) code. J Am Med Dir Assoc. (2016) 17:675–7. doi: 10.1016/j.jamda.2016.06.001
7. Hart, A, Cordova-Rivera, L, Barker, F, Sayer, AA, Granic, A, and Yarnall, AJ. The prevalence of sarcopenia in Parkinson’s disease and related disorders- a systematic review. Neurol Sci. (2023) 44:4205–17. doi: 10.1007/s10072-023-07007-0
8. Volkert, D, Beck, AM, Cederholm, T, Cruz-Jentoft, A, Goisser, S, Hooper, L, et al. ESPEN guideline on clinical nutrition and hydration in geriatrics. Clin Nutr. (2019) 38:10–47. doi: 10.1016/j.clnu.2018.05.024
9. Gov Br (2020). Available online at: https://biblioteca.ibge.gov.br/visualizacao/livros/liv101749.pdf (Accessed September 1, 2024).
10. Hengeveld, LM, Boer, JMA, Gaudreau, P, Heymans, MW, Jagger, C, Mendonça, N, et al. Prevalence of protein intake below recommended in community-dwelling older adults: a meta-analysis across cohorts from the PROMISS consortium. J Cachexia Sarcopenia Muscle. (2020) 11:1212–22. doi: 10.1002/jcsm.12580
11. Jankovic, J, and Tan, EK. Parkinson’s disease: etiopathogenesis and treatment. J Neurol Neurosurg Psychiatry. (2020) 91:795–808. doi: 10.1136/jnnp-2019-322338
12. Pradhan, S, and Kelly, VE. Quantifying physical activity in early Parkinson disease using a comercial activity monitor. Parkinsonism Relat Disord. (2019) 66:171–5. doi: 10.1016/j.parkreldis.2019.08.001
13. Stokes, T, Hector, A, Morton, R, McGlory, C, and Phillips, S. Recent perspectives regarding the role of dietary protein for the promotion of muscle hypertrophy with resistance exercise training. Nutrients. (2018) 10:180. doi: 10.3390/nu10020180
14. Morton, RW, Murphy, KT, McKellar, SR, Schoenfeld, BJ, Henselmans, M, Helms, E, et al. A systematic review, meta-analysis and meta-regression of the effect of protein supplementation on resistance training-induced gains in muscle mass and strength in healthy adults. Br J Sports Med. (2018) 52:376–84. doi: 10.1136/bjsports-2017-097608
15. Rusch, C, Flanagan, R, Suh, H, and Subramanian, I. To restrict or not to restrict? Practical considerations for optimizing dietary protein interactions on levodopa absorption in Parkinson’s disease. NPJ Parkinsons Dis. (2023) 9:98. doi: 10.1038/s41531-023-00541-w
16. Kelly, TL, Wilson, KE, and Heymsfield, SB. Dual energy X-ray absorptiometry body composition reference values from NHANES. PLoS One. (2009) 4:e7038. doi: 10.1371/journal.pone.0007038
17. Volkert, D, Beck, AM, Cederholm, T, Cruz-Jentoft, A, Hooper, L, Kiesswetter, E, et al. ESPEN practical guideline: clinical nutrition and hydration in geriatrics. Clin Nutr. (2022) 41:958–89. doi: 10.1016/j.clnu.2022.01.024
18. Tomlinson, CL, Stowe, R, Patel, S, Rick, C, Gray, R, and Clarke, CE. Systematic review of levodopa dose equivalency reporting in Parkinson’s disease. Mov Disord. (2010) 25:2649–53. doi: 10.1002/mds.23429
19. Tosato, M, Marzetti, E, Cesari, M, Savera, G, Miller, RR, Bernabei, R, et al. Measurement of muscle mass in sarcopenia: from imaging to biochemical markers. Aging Clin Exp Res. (2017) 29:19–27. doi: 10.1007/s40520-016-0717-0
20. Roberts, HC, Denison, HJ, Martin, HJ, Patel, HP, Syddall, H, Cooper, C, et al. A review of the measurement of grip strength in clinical and epidemiological studies: towards a standardised approach. Age Ageing. (2011) 40:423–9. doi: 10.1093/ageing/afr051
21. de Fátima Ribeiro Silva, C, Ohara, DG, Matos, AP, ACPN, P, and Pegorari, MS. Short physical performance battery as a measure of physical performance and mortality predictor in older adults: a comprehensive literature review. Int J Environ Res Public Health. (2021) 18:10612. doi: 10.3390/ijerph182010612
22. Lorefält, B, Ganowiak, W, Wissing, U, Granérus, A-K, and Unosson, M. Food habits and intake of nutrients in elderly patients with Parkinson’s disease. Gerontology. (2006) 52:160–8. doi: 10.1159/000091825
23. Marczewska, A, De Notaris, R, Sieri, S, Barichella, M, Fusconi, E, and Pezzoli, G. Protein intake in parkinsonian patients using the EPIC food frequency questionnaire. Mov Disord. (2006) 21:1229–31. doi: 10.1002/mds.20888
24. Barichella, M, Cereda, E, Cassani, E, Pinelli, G, Iorio, L, Ferri, V, et al. Dietary habits and neurological features of Parkinson’s disease patients: implications for practice. Clin Nutr. (2017) 36:1054–61. doi: 10.1016/j.clnu.2016.06.020
25. Morais, MB, de Fracasso, BM, Busnello, FM, Mancopes, R, and Rabito, EI. Doença de Parkinson em idosos: ingestão alimentar e estado nutricional. Rev Bras Geriatr Gerontol. (2013) 16:503–11. doi: 10.1590/S1809-98232013000300009
26. de Carmo, TPS, and CCD, F. Avaliação nutricional e o uso da levodopa com refeições proteicas em pacientes com doença de Parkinson do município de Macaé, Rio de Janeiro. Rev Bras Geriatr Gerontol. (2016) 19:223–34. doi: 10.1590/1809-98232016019.150141
27. Cooper, MK, Brock, DG, and McDaniel, CM. Interaction between levodopa and enteral nutrition. Ann Pharmacother. (2008) 42:439–42. doi: 10.1345/aph.1K450
28. Barichella, M, Marczewska, A, De Notaris, R, Vairo, A, Baldo, C, Mauri, A, et al. Special low-protein foods ameliorate postprandial off in patients with advanced Parkinson’s disease. Mov Disord. (2006) 21:1682–7. doi: 10.1002/mds.21003
29. Wang, L, Xiong, N, Huang, J, Guo, S, Liu, L, Han, C, et al. Protein-restricted diets for ameliorating motor fluctuations in Parkinson’s disease. Front Aging Neurosci. (2017) 9:9. doi: 10.3389/fnagi.2017.00206
30. Riley, D, and Lang, AE. Practical application of a low-protein diet for Parkinson’s disease. Neurology. (1988) 38:1026–6. doi: 10.1212/WNL.38.7.1026
31. Pincus, JH, and Barry, K. Protein redistribution diet restores motor function in patients with dopa-resistant “off” periods. Neurology. (1988) 38:481–3. doi: 10.1212/WNL.38.3.481
32. Karstaedt, PJ, and Pincus, JH. Protein redistribution diet remains effective in patients with fluctuating parkinsonism. Arch Neurol. (1992) 49:149–51. doi: 10.1001/archneur.1992.00530260049018
33. Cereda, E, Barichella, M, Pedrolli, C, and Pezzoli, G. Low-protein and protein-redistribution diets for Parkinson’s disease patients with motor fluctuations: a systematic review. Mov Disord. (2010) 25:2021–34. doi: 10.1002/mds.23226
34. Agnieszka, W, Paweł, P, and Małgorzata, K. How to optimize the effectiveness and safety of Parkinson’s disease therapy? – a systematic review of drugs interactions with food and dietary supplements. Curr Neuropharmacol. (2022) 20:1427–47. doi: 10.2174/1570159X19666211116142806
35. Bauer, J, Biolo, G, Cederholm, T, Cesari, M, Cruz-Jentoft, AJ, Morley, JE, et al. Evidence-based recommendations for optimal dietary protein intake in older people: a position paper from the PROT-AGE study group. J Am Med Dir Assoc. (2013) 14:542–59. doi: 10.1016/j.jamda.2013.05.021
36. Magalhães, NV, Waitzberg, DL, Lopes, NC, Vicedomini, ACC, Prudêncio, APA, Jacob-Filho, W, et al. High prevalence of energy and nutrients inadequacy among Brazilian older adults. Nutrients. (2023) 15:3246. doi: 10.3390/nu15143246
37. Previdelli, AN, Goulart, RMM, and de Aquino, R. Balanço de macronutrientes na dieta de idosos brasileiros: análises da Pesquisa Nacional de Alimentação 2008-2009. Rev Bras Epidemiol. (2017) 20:70–80. doi: 10.1590/1980-5497201700010006
38. Schorr, M, Dichtel, LE, Gerweck, AV, Valera, RD, Torriani, M, Miller, KK, et al. Sex differences in body composition and association with cardiometabolic risk. Biol Sex Differ. (2018) 9:28. doi: 10.1186/s13293-018-0189-3
39. Lovejoy, JC, Champagne, CM, de Jonge, L, Xie, H, and Smith, SR. Increased visceral fat and decreased energy expenditure during the menopausal transition. Int J Obes. (2008) 32:949–58. doi: 10.1038/ijo.2008.25
40. Allan, CA, Strauss, BJG, Burger, HG, Forbes, EA, and McLachlan, RI. Testosterone therapy prevents gain in visceral adipose tissue and loss of skeletal muscle in nonobese aging men. J Clin Endocrinol Metab. (2008) 93:139–46. doi: 10.1210/jc.2007-1291
41. Randall, JC, Winkler, TW, Kutalik, Z, Berndt, SI, Jackson, AU, Monda, KL, et al. Sex-stratified genome-wide association studies including 270, 000 individuals show sexual dimorphism in genetic loci for anthropometric traits. PLoS Genet. (2013) 9:e1003500. doi: 10.1371/journal.pgen.1003500
42. Bennett, E, Peters, SAE, and Woodward, M. Sex differences in macronutrient intake and adherence to dietary recommendations: findings from the UK biobank. BMJ Open. (2018) 8:e020017. doi: 10.1136/bmjopen-2017-020017
43. Granic, A, Jagger, C, Davies, K, Adamson, A, Kirkwood, T, Hill, TR, et al. Effect of dietary patterns on muscle strength and physical performance in the very old: findings from the Newcastle 85+ study. PLoS One. (2016) 11:e0149699. doi: 10.1371/journal.pone.0149699
44. Granic, A, Mendonça, N, Sayer, AA, Hill, TR, Davies, K, Adamson, A, et al. Low protein intake, muscle strength and physical performance in the very old: the Newcastle 85+ study. Clin Nutr. (2018) 37:2260–70. doi: 10.1016/j.clnu.2017.11.005
45. Choi, K-A, Heu, E, Nam, H-C, Park, Y, Kim, D, and Ha, Y-C. Relationship between low muscle strength, and protein intake: a preliminary study of elderly patients with hip fracture. J Bone Metab. (2022) 29:17–21. doi: 10.11005/jbm.2022.29.1.17
46. Beasley, JM, Shikany, JM, and Thomson, CA. The role of dietary protein intake in the prevention of sarcopenia of aging. Nutr Clin Pract. (2013) 28:684–90. doi: 10.1177/0884533613507607
47. Gamborg, M, Hvid, LG, Thrue, C, Johansson, S, Franzén, E, Dalgas, U, et al. Muscle strength and power in people with Parkinson disease: a systematic review and meta-analysis. J Neurol Phys Ther. (2023) 47:3–15. doi: 10.1097/NPT.0000000000000421
48. Schoufour, JD, Franco, OH, Kiefte-de Jong, JC, Trajanoska, K, Stricker, B, Brusselle, G, et al. The association between dietary protein intake, energy intake and physical frailty: results from the Rotterdam study. Br J Nutr. (2019) 121:393–401. doi: 10.1017/s0007114518003367
49. Tagawa, R, Watanabe, D, Ito, K, Otsuyama, T, Nakayama, K, Sanbongi, C, et al. Synergistic effect of increased total protein intake and strength training on muscle strength: a dose-response meta-analysis of randomized controlled trials. Sports Med Open. (2022) 8:8. doi: 10.1186/s40798-022-00508-w
50. Longland, TM, Oikawa, SY, Mitchell, CJ, Devries, MC, and Phillips, SM. Higher compared with lower dietary protein during an energy deficit combined with intense exercise promotes greater lean mass gain and fat mass loss: a randomized trial. Am J Clin Nutr. (2016) 103:738–46. doi: 10.3945/ajcn.115.119339
51. Paddon-Jones, D, Campbell, WW, Jacques, PF, Kritchevsky, SB, Moore, LL, Rodriguez, NR, et al. Protein and healthy aging. Am J Clin Nutr. (2015) 101:1339S–45S. doi: 10.3945/ajcn.114.084061
52. Mignone, LE, Wu, T, Horowitz, M, and Rayner, CK. Whey protein: the “whey” forward for treatment of type 2 diabetes? World J Diabetes. (2015) 6:1274–84. doi: 10.4239/wjd.v6.i14.1274
53. Brown, AF, Prado, CM, Ghosh, S, Leonard, SM, Arciero, PJ, Tucker, KL, et al. Higher-protein intake and physical activity are associated with healthier body composition and cardiometabolic health in Hispanic adults. Clin Nutr ESPEN. (2019) 30:145–51. doi: 10.1016/j.clnesp.2019.01.002
54. Arciero, PJ, Gentile, CL, Pressman, R, Everett, M, Ormsbee, MJ, Martin, J, et al. Moderate protein intake improves total and regional body composition and insulin sensitivity in overweight adults. Metabolism. (2008) 57:757–65. doi: 10.1016/j.metabol.2008.01.015
55. Arciero, PJ, Ormsbee, MJ, Gentile, CL, Nindl, BC, Brestoff, JR, and Ruby, M. Increased protein intake and meal frequency reduces abdominal fat during energy balance and energy deficit. Obesity (Silver Spring). (2013) 21:1357–66. doi: 10.1002/oby.20296
56. Jäger, R, Kerksick, CM, Campbell, BI, Cribb, PJ, Wells, SD, Skwiat, TM, et al. International Society of Sports Nutrition Position Stand: protein and exercise. J Int Soc Sports Nutr. (2017) 14:20. doi: 10.1186/s12970-017-0177-8
57. Kim, JE, O’Connor, LE, Sands, LP, Slebodnik, MB, and Campbell, WW. Effects of dietary protein intake on body composition changes after weight loss in older adults: a systematic review and meta-analysis. Nutr Rev. (2016) 74:210–24. doi: 10.1093/nutrit/nuv065
58. Locke, AE, Kahali, B, Berndt, SI, Justice, AE, Pers, TH, Day, FR, et al. Genetic studies of body mass index yield new insights for obesity biology. Nature. (2015) 518:197–206. doi: 10.1038/nature14177
59. Wang, R, Zhang, X, Ren, H, Zhou, H, Yuan, Y, Chai, Y, et al. Effects of different exercise types on visceral fat in young individuals with obesity aged 6–24 years old: a systematic review and meta-analysis. Front Physiol. (2022) 13:987804. doi: 10.3389/fphys.2022.987804
60. Jahangiri, S, Malek, M, Kalra, S, and Khamseh, ME. The effects of sodium–glucose cotransporter 2 inhibitors on body composition in type 2 diabetes mellitus: a narrative review. Diabetes Ther. (2023) 14:2015–30. doi: 10.1007/s13300-023-01481-7
61. Palmisano, BT, Zhu, L, Eckel, RH, and Stafford, JM. Sex differences in lipid and lipoprotein metabolism. Mol Metab. (2018) 15:45–55. doi: 10.1016/j.molmet.2018.05.008
62. Raglione, LM, Sorbi, S, and Nacmias, B. Osteoporosis and Parkinson’s disease. Clin Cases Miner Bone Metab. (2011) 8:16–8.
63. Li, X, Li, C, Zhang, W, Wang, Y, Qian, P, and Huang, H. Inflammation and aging: signaling pathways and intervention therapies. Signal Transduct Target Ther. (2023) 8:239–29. doi: 10.1038/s41392-023-01502-8
64. Kim, J-S, and Sung, H-Y. Gastrointestinal autonomic dysfunction in patients with Parkinson’s disease. J Mov Disord. (2015) 8:76–82. doi: 10.14802/jmd.15008
65. Paul, G, Paul, B, Singh, T, Jain, D, Singh, G, Kaushal, S, et al. Prevalence of malnutrition in Parkinson’s disease and correlation with gastrointestinal symptoms. Ann Indian Acad Neurol. (2019) 22:447–52. doi: 10.4103/aian.AIAN_349_18
66. Ma, K, Xiong, N, Shen, Y, Han, C, Liu, L, Zhang, G, et al. Weight loss and malnutrition in patients with Parkinson’s disease: current knowledge and future prospects. Front Aging Neurosci. (2018) 10:10. doi: 10.3389/fnagi.2018.00001
67. Umemoto, G, and Furuya, H. Management of dysphagia in patients with Parkinson’s disease and related disorders. Intern Med. (2020) 59:7–14. doi: 10.2169/internalmedicine.2373-18
68. Yang, T, Zhan, Z, Zhang, L, Zhu, J, Liu, Y, Zhang, L, et al. Prevalence and risk factors for malnutrition in patients with Parkinson’s disease. Front Neurol. (2020) 11:11. doi: 10.3389/fneur.2020.533731
69. Sheard, JM, Ash, S, Mellick, GD, Silburn, PA, and Kerr, GK. Markers of disease severity are associated with malnutrition in Parkinson’s disease. PLoS One. (2013) 8:e57986. doi: 10.1371/journal.pone.0057986
70. Wang, G, Wan, Y, Cheng, Q, Xiao, Q, Wang, Y, Zhang, J, et al. Malnutrition and associated factors in Chinese patients with Parkinson’s disease: results from a pilot investigation. Parkinsonism Relat Disord. (2010) 16:119–23. doi: 10.1016/j.parkreldis.2009.08.009
71. Keller, HH. Improving food intake in persons living with dementia. Ann N Y Acad Sci. (2016) 1367:3–11. doi: 10.1111/nyas.12997
72. Fávaro-Moreira, NC, Krausch-Hofmann, S, Matthys, C, Vereecken, C, Vanhauwaert, E, Declercq, A, et al. Risk factors for malnutrition in older adults: a systematic review of the literature based on longitudinal data. Adv Nutr. (2016) 7:507–22. doi: 10.3945/an.115.011254
73. Sakuma, K, and Yamaguchi, A. Sarcopenia and age-related endocrine function. Int J Endocrinol. (2012) 2012:1–10. doi: 10.1155/2012/127362
74. Ponsoni, A, Sardeli, AV, Costa, FP, and Mourão, LF. Prevalence of sarcopenia in Parkinson’s disease: a systematic review and meta-analysis. Geriatr Nurs. (2023) 49:44–9. doi: 10.1016/j.gerinurse.2022.11.006
75. Shafiee, G, Keshtkar, A, Soltani, A, Ahadi, Z, Larijani, B, and Heshmat, R. Prevalence of sarcopenia in the world: a systematic review and meta-analysis of general population studies. J Diabetes Metab Disord. (2017) 16:21. doi: 10.1186/s40200-017-0302-x
76. Tan, AH, Hew, YC, Lim, S-Y, Ramli, NM, Kamaruzzaman, SB, Tan, MP, et al. Altered body composition, sarcopenia, frailty, and their clinico-biological correlates, in Parkinson’s disease. Parkinsonism Relat Disord. (2018) 56:58–64. doi: 10.1016/j.parkreldis.2018.06.020
77. Antonio, J, Candow, DG, Forbes, SC, Ormsbee, MJ, Saracino, PG, and Roberts, J. Effects of dietary protein on body composition in exercising individuals. Nutrients. (2020) 12:1890. doi: 10.3390/nu12061890
78. Drey, M, Hasmann, SE, Krenovsky, J-P, Hobert, MA, Straub, S, Elshehabi, M, et al. Associations between early markers of Parkinson’s disease and sarcopenia. Front Aging Neurosci. (2017) 9:53. doi: 10.3389/fnagi.2017.00053
79. Voelker, SN, Michalopoulos, N, Maier, AB, and Reijnierse, EM. Reliability and concurrent validity of the SARC-F and its modified versions: a systematic review and meta-analysis. J Am Med Dir Assoc. (2021) 22:1864–1876.e16. doi: 10.1016/j.jamda.2021.05.011
Keywords: body composition, sarcopenia, protein intake, nutritional status, Parkinson’s disease
Citation: Lima DP, Monteiro PA, Gomes de Luna JR, Viana-Júnior AB, Santos LTR, de Almeida SB, Saldanha RRF, de Alencar MS, Lopes FKdM, Alencar ÁP, Chaves RCdBA, Brito WC, Nóbrega PR, Lima AB, Braga-Neto P, Roriz-Filho JS and Montenegro Júnior RM (2025) Assessment of body composition, sarcopenia and protein intake in mild to moderate Parkinson’s disease. Front. Nutr. 12:1507545. doi: 10.3389/fnut.2025.1507545
Edited by:
Laura Beth McIntire, NewYork-Presbyterian, United StatesReviewed by:
Khairiah Razali, International Islamic University Malaysia, MalaysiaCynthia López Botello, Monterrey Institute of Technology and Higher Education (ITESM), Mexico
Copyright © 2025 Lima, Monteiro, Gomes de Luna, Viana-Júnior, Santos, de Almeida, Saldanha, de Alencar, Lopes, Alencar, Chaves, Brito, Nóbrega, Lima, Braga-Neto, Roriz-Filho and Montenegro Júnior. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Danielle Pessoa Lima, ZHJhLmRhbmllbGxlbGltYUBnbWFpbC5jb20=
†These authors have contributed equally to this work and share first authorship