 Raquel Cueto-Galán1,2
Raquel Cueto-Galán1,2 Andres Fontalba-Navas1,2,3*
Andres Fontalba-Navas1,2,3* Mario Gutiérrez-Bedmar1,2,4
Mario Gutiérrez-Bedmar1,2,4 Miguel Ruiz-Canela5,6
Miguel Ruiz-Canela5,6 Miguel A. Martínez-González5,6,7
Miguel A. Martínez-González5,6,7 Lilian Alves8
Lilian Alves8 Nancy Babio6,9,10
Nancy Babio6,9,10 Montserrat Fitó6,11
Montserrat Fitó6,11 Emilio Ros6,12Miquel Fiol6,13
Emilio Ros6,12Miquel Fiol6,13 Ramón Estruch6,14Fernando Arós6,15Luis Serra-Majem6,16
Ramón Estruch6,14Fernando Arós6,15Luis Serra-Majem6,16 Xavier Pintó6,17
Xavier Pintó6,17 Carlos Muñoz-Bravo1,2
Carlos Muñoz-Bravo1,2 Antonio García-Rodríguez1,2
Antonio García-Rodríguez1,2 Enrique Gómez-Gracia1,2
Enrique Gómez-Gracia1,2- 1Department of Public Health and Psychiatry, School of Medicine, University of Málaga, Málaga, Spain
- 2Biomedical Research Institute of Malaga (IBIMA), Málaga, Spain
- 3Antequera Hospital, Northern Málaga Integrated Healthcare Area, Antequera, Spain
- 4CIBER Cardiovascular Diseases (CIBERCV), Instituto de Salud Carlos III (ISCIII), Madrid, Spain
- 5Department of Preventive Medicine and Public Health, School of Medicine, University of Navarra, Pamplona, Spain
- 6CIBER Fisiopatología de la Obesidad y Nutrición (CIBEROBN), Instituto de Salud Carlos III (ISCIII), Madrid, Spain
- 7Department of Nutrition, Harvard T.H. Chan School of Public Health, Boston, MA, United States
- 8Gastroenterology Department, Hospital Salut Sant Joan, Institut d'Investigació Sanitària Pere Virgili, Food, Nutrition, Development, and Mental Health Group, Reus, Spain
- 9Universitat Rovira i Virgili, Departament de Bioquímica i Biotecnologia, Grupo ANUT-DSM, Reus, Spain
- 10Institut d'Investigació Sanitària Pere Virgili, Reus, Spain
- 11Cardiovascular Risk and Nutrition Research Group, Hospital Del Mar Medical Research Institute (IMIM), Barcelona, Spain
- 12Lipid Clinic, Endocrinology and Nutrition Service, Institut d'Investigations Biomèdiques August Pi I Sunyer (IDIBAPS), Hospital Clínic, Barcelona, Spain
- 13Health Research Institute of the Balearic Islands (IdISBa), Hospital Son Espases, Palma de Mallorca, Spain
- 14Department of Internal Medicine, IDIBAPS, Hospital Clínic, University of Barcelona, Barcelona, Spain
- 15Department of Cardiology, Hospital Universitario de Álava, Vitoria, Spain
- 16Department of Clinical Sciences and Research Institute of Biomedical and Health Sciences, Universidad de Las Palmas de Gran Canaria, Las Palmas, Spain
- 17Lipid and Vascular Risk Unit, Internal Medicine Service, Hospital Universitario de Bellvitge, L'Hospitalet de Llobregat, Spain
Background: Little is known about the potential preventive effect of adherence to the Mediterranean diet (MedDiet) on the development of metabolic dysfunction-associated steatotic liver disease (MASLD).
Aim: This study aims to determine the impact of adherence to the MedDiet on the progression of MASLD, measured using the hepatic steatosis index (HSI) at baseline and annually over a 5-year follow-up period within the framework of the PREvención con DIeta MEDiterránea (PREDIMED) study.
Method: Participants from the PREDIMED trial with sufficient available data (n = 3,145) were examined annually over 5 years. Adherence to the MedDiet was evaluated using the Mediterranean Diet Adherence Screener (MEDAS) questionnaire, and the presence/severity of hepatic steatosis was determined according to the HSI. Linear mixed models were used to analyze the association between the study variables and HSI.
Results: The participants (57% female, 43% male) had a mean age of 67.2 (SD 6.2) years. Among the cardiovascular risk factors considered, the mean BMI was 29.81 (SD 3.62); 47% of participants had type 2 diabetes, 70% had hypercholesterolaemia, and 84% had hypertension. Over the 5-year follow-up, average adherence to the MedDiet and physical activity generally increased, while alcohol consumption, calorie intake, tobacco use, hypercholesterolaemia, and hypertension decreased. The fully adjusted multivariate model reflected a statistically significant decrease in the HSI per unit increase in adherence to the MedDiet (β = −0.075; 95% CI: −0.128, −0.021).
Conclusion: In individuals at high cardiovascular risk, adherence to the MedDiet is significantly associated with improvements in HSI. These longitudinal findings highlight the important role of the MedDiet in delaying or slowing the natural progression of MASLD, contributing to both its prevention and clinical management.
Introduction
The nomenclature for the condition formerly known as non-alcoholic fatty liver disease (NAFLD) has evolved significantly. Traditionally, NAFLD was defined as a fatty accumulation in the liver (steatosis ≥5% of hepatocytes) in the absence of significant alcohol consumption (<20–30 g/day of alcohol intake), liver viral infection, or relevant medication/drug use (1). In 2020, Eslam et al. (2) introduced the term metabolic dysfunction-associated fatty liver disease (MAFLD), characterized by hepatic steatosis identified through imaging, blood biomarkers, or liver histology. Diagnosis requires the individual to be overweight or obese, to have type 2 diabetes mellitus (T2D), or to exhibit at least two metabolic risk factors. In 2023, an internationally guided Delphi process was conducted to standardize diagnostic criteria and enhance the comparability of research findings. This process led to the definition of metabolic dysfunction-associated steatotic liver disease (MASLD) (3), in which the term “steatotic” rather than “fatty” was used to mitigate the stigma associated with the condition (4). Up to 99% of individuals diagnosed with NAFLD also meet the criteria for MASLD (5).
MASLD is defined as steatotic liver disease occurring in the presence of one or more cardiometabolic risk factors and with alcohol intake < 20 g/day (6). However, MASLD may coexist with moderate alcohol intake, resulting in a distinct condition known as metabolic dysfunction-associated alcohol-related liver disease (MetALD).
MetALD represents a separate category from “pure” MASLD, where alcohol consumption plays a significant role in the development and progression of the disease. It is characterized by a weekly alcohol intake of 140–350 g for women and 210–420 g for men, exceeding the threshold for MASLD but not meeting the criteria for alcoholic liver disease (7).
MASLD is the most common liver disease, with a global prevalence of 38.7% (8, 9), ranging from 55.33% in Europe to 36.31% in Asia and 35.99% in North America (10). The condition is pandemic, transcending national and regional differences in economic development and socioeconomic status. Moreover, it is a major risk factor for hepatocellular carcinoma and the third overall cause of death from cancer (8.3%) (11). The accumulation of free fatty acids and triglycerides in the liver generates oxidative stress and inflammation, facilitating the progression to steatohepatitis, fibrosis, and liver cancer (12, 13). Moreover, the rising prevalence of obesity, T2D, and metabolic syndrome has significantly contributed to the growing burden of MASLD (14). The coexistence of these conditions further amplifies the risk and severity of MASLD, making it an increasingly important risk factor for cardiovascular events (15, 16). A major and as yet unresolved problem is that of accurately diagnosing MASLD. In clinical practice, ultrasound is the safest, most accessible, and most cost-effective imaging test; however, its low sensitivity makes it inadequate for distinguishing between simple steatosis and steatohepatitis. Liver biopsy is the current gold standard diagnostic tool, but there is no consensus on its routine use (17), due to potential complications and the high prevalence of MASLD, which hampers large-scale implementation. Consequently, increasing attention is being paid to disease prevention, both to reduce the burden on healthcare systems and to improve clinical outcomes (8, 18).
Non-invasive methods such as serological markers and radiological techniques are currently the most widely used for predicting and detecting MASLD. Discussions continue about incorporating these methods as a first step in screening the general population for advanced liver disease, thus enabling clinicians to identify individuals who might require further, invasive investigation (19–21).
Several serological markers have been developed and validated, both for the general population and for individuals with obesity, offering a reliable assessment of the presence of steatosis, although these markers do not quantify hepatic fat content (22). Among them, the most widely used and strongly validated are the fatty liver index (FLI) and the hepatic steatosis index (HSI). Recent studies suggest that, in terms of sensitivity and specificity, the HSI more specifically detects steatosis in at-risk populations (those with diabetes and/or obesity), whereas the FLI is more effective as a screening tool for the general population (23).
MASLD has a multifactorial etiology, with significant genetic and environmental components. Effective prevention and treatment are essential to slow its progression, and lifestyle interventions such as diet and physical exercise appear to play a significant role in this respect (24, 25). Nevertheless, no evidence-based practical dietary recommendations for the prevention of MASLD have yet become widely accepted (26–29).
The effectiveness of dietary modifications on MASLD depends not only on calorie restriction but also on the type of calories consumed (24, 30, 31). The Mediterranean diet (MedDiet), which is characterized by a high intake of vegetables, fruits, beans, lentils, nuts, whole grains, and fish, might reduce the risk of MASLD, improve cardiometabolic health, and mitigate the adverse outcomes associated with the disease (32–34). This effect appears to be partly attributable to its high content of antioxidants and fiber, low levels of saturated fats and animal protein, and a balanced ratio of omega-3 to omega-6 fatty acids (35). The MedDiet is considered the most suitable dietary approach for patients with MASLD, primarily due to its impact on reducing oxidative stress, modulating gut microbiota and reactive oxidative species (ROS) levels, and activating autophagy (Figure 1) (35–37). Furthermore, adherence to the MedDiet is associated with improved metabolic regulation and, potentially, with the modulation of mitochondrial proteins such as Sirtuin 4, which play a role in managing oxidative stress and inflammation pathways (38). These combined effects underscore the potential of the MedDiet for the prevention and treatment of MASLD.
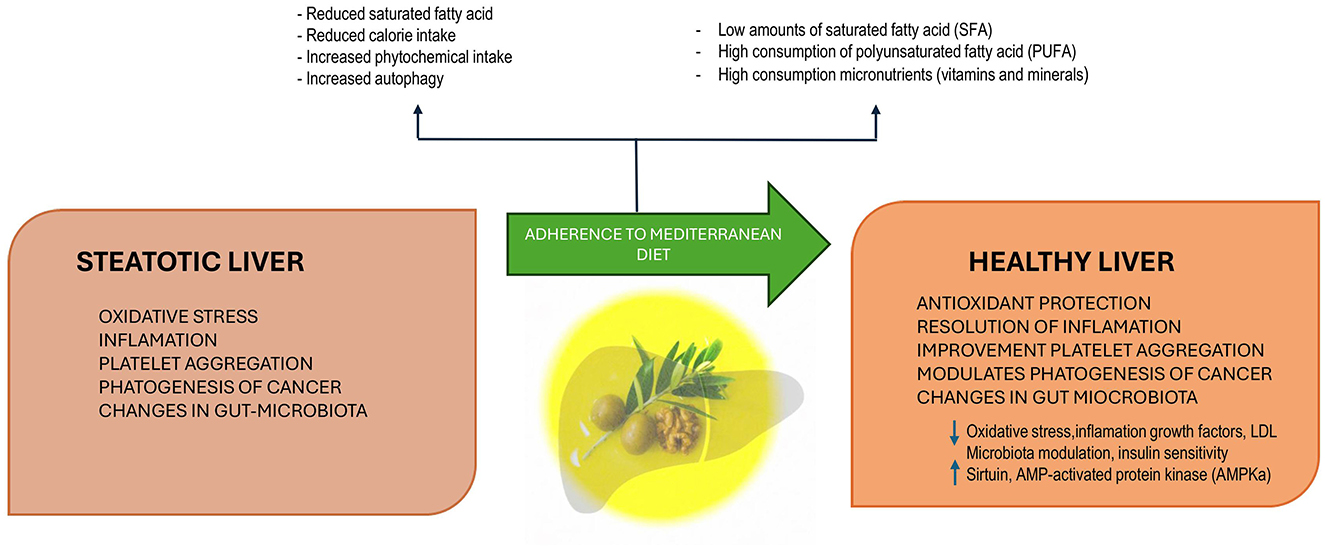
Figure 1. The Mediterranean diet, characterized by low saturated fatty acids (SFA), high polyunsaturated fatty acids (PUFA), and abundant micronutrients (vitamins and minerals), promotes metabolic benefits through reduced calorie intake, increased phytochemical intake, and enhanced autophagy. These mechanisms counteract oxidative stress, inflammation, platelet aggregation, and cancer pathogenesis while modulating gut microbiota. By decreasing oxidative stress, inflammation, growth factors, and LDL, and improving insulin sensitivity and microbiota composition, the Mediterranean diet enhances antioxidant protection, resolves inflammation, improves platelet function, and modulates cancer pathogenesis, contributing to liver health.
The few studies conducted on the MedDiet and its impact on MASLD have used widely varying designs, making it difficult to compare the information reported (39–41). Furthermore, research data for real, multi-pathological populations, including extensive long-term follow-up, are almost non-existent (41, 42).
To our knowledge, no previous large-scale, long-term population-based analysis has evaluated the effects of adherence to the MedDiet on the prevention and progression of MASLD. The aim of the present study is to investigate the long-term association between MedDiet adherence and HSI outcomes among participants in the PREvención con DIeta MEDiterránea (PREDIMED) trial.
Materials and methods
The PREDIMED randomized clinical trial was conducted in Spain to determine the effect of a MedDiet supplemented with either extra virgin olive oil (EVOO) or nuts on the prevention of cardiovascular disease in men and women at high vascular risk, compared to a low-fat diet (43, 44). PREDIMED is registered on the Current Controlled Trials Register as ISRCTN 35739639 (http://www.predimed.es).
The study protocol complied with the principles of the Declaration of Helsinki and was approved by the Institutional Review Boards at all the recruiting centers involved. Signed informed consent was obtained from every participant.
Study design and sample
The design, population, and methods of the PREDIMED trial have been published previously (45). In short, 7,447 men (aged 55–80 years) and women (aged 60–80 years), without documented cardiovascular disease at baseline, were recruited into the study. All presented either T2D or at least three of the following cardiovascular risk factors: current smoking habit, hypertension (blood pressure >140/90 mmHg or treatment with antihypertensives), elevated plasma low-density lipoprotein cholesterol (>160 mg/dl or treatment with lipid-lowering agents), low plasma high-density lipoprotein cholesterol (< 50 mg/dl in women and < 40 mg/dl in men), and body mass index ≥25 kg/m2 or family history of early coronary heart disease. All those with a history of cardiovascular disease, any serious chronic disease, or a low predicted probability of changing dietary habits (according to the stages of change model) were excluded from the trial.
The present study included 3,145 patients from the PREDIMED trial, with baseline data and 5 years of longitudinal follow-up data using yearly repeated measurements allowing to calculate the incidence and severity of HSI. At baseline, all participants reported baseline alcohol consumption of < 20 g/day (women) or < 30 g/day (men).
Study variables
Data for the following variables were collected: age, sex, HSI, BMI, adherence to the MedDiet, fasting glucose, total cholesterol, pattern of physical activity, total calorie intake, and alcohol consumption. Data on educational background and the presence or otherwise of T2D, hypertension, hypercholesterolemia, and smoking habits were also recorded.
The HSI equation and its interpretation are shown in Annex 1.
Physical exercise and adherence to the Mediterranean diet
Adherence to the MedDiet was assessed by the Mediterranean Diet Adherence Screener (MEDAS), a validated 14-item questionnaire (46, 47) that presents 12 questions on food consumption frequency and 2 on food consumption habits characteristic of the MedDiet in Spain. The final score that can be obtained with this questionnaire ranges from 0 to 14 points.
Physical activity (amount and intensity) was recorded using the Minnesota Leisure Time Physical Activity Questionnaire and measured in metabolic equivalents per year (48, 49). The validated Spanish version of the questionnaire includes 67 different activities and expresses the average metabolic rate as kJ/day (50, 51), based on the energy expenditure associated with these activities.
Statistical analysis
The study variables are summarized by percentages (categorical variables) or by means and standard deviations (quantitative variables). Baseline measurements were compared using analysis of variance (ANOVA) for the quantitative variables and the chi-square test for the qualitative ones. Yearly changes in the variables during the 5-year follow-up were evaluated using repeated measures ANOVA with Greenhouse–Geisser correction for the numerical variables and the chi-square test for the qualitative ones. The longitudinal association between repeated measures of the HSI and adherence to the MedDiet was analyzed using linear mixed models with random intercept. In the models, the HSI was taken as a dependent variable. The independent variables were follow-up time and adherence to the MedDiet (both with random slopes). Adjustment for the remaining study variables was performed as follows: unadjusted (Model 1), age- and sex-adjusted (Model 2), and all study variables (including the PREDIMED intervention group)-adjusted (Model 3). All models reflected the interaction between follow-up time and MedDiet adherence, with the inclusion of a multiplicative interaction term (time x MedDiet adherence). All statistical tests were two-tailed with a significance level of 0.05 and a confidence level of 95% and were performed with Stata 18.0 software.
Results
The mean age of the 3,145 participants was 67.2 years (± 6.2 SD); 57% were female, and 75% had at least primary education. The baseline characteristics of the intervention group and the low-fat diet recommendation group are shown in Table 1. There were no significant baseline differences between the randomized groups in terms of HSI, BMI, or the prevalence of hypertension, T2D, or hypercholesterolemia. Notably, 85% were non-smokers, and the mean BMI was 29.81 (SD 3.62), which represents overweight. The baseline prevalence of cardiometabolic disorders was T2D 47%, hypercholesterolemia 70%, and hypertension 84%.
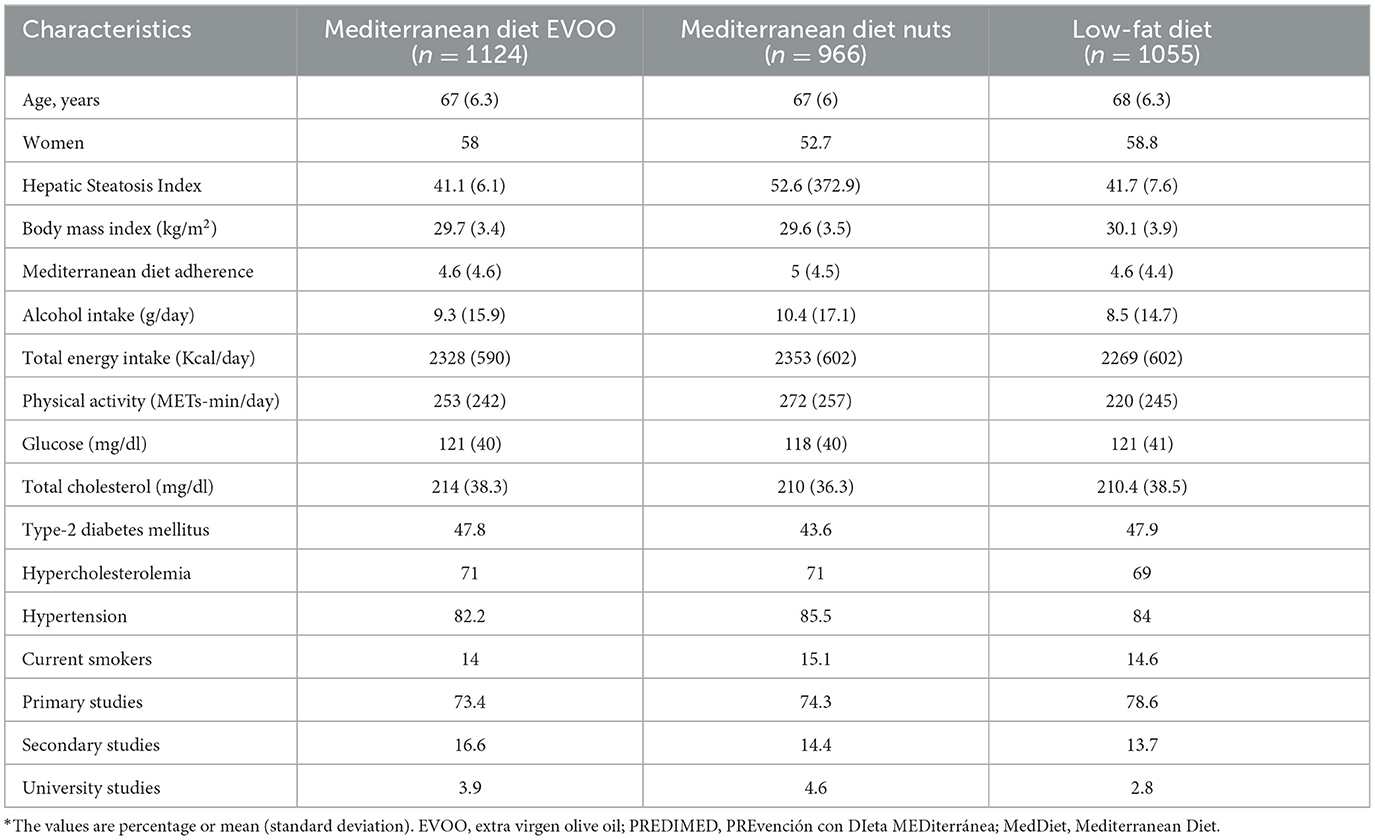
Table 1. Clinical and baseline epidemiological characteristics according to the intervention and control groups of the PREDIMED trial.
Table 2 shows the significant changes observed in these values during the follow-up period. In short, the HSI decreased by 0.6 units (p < 0.001), while adherence to the MedDiet increased from 8.84 to 10.55 units (p < 0.001). Significant decreases were observed in alcohol intake (from 9.52 to 7.76 g/day, p < 0.001) and energy intake (from 2,348.37 to 2,160.04 Kcal/day, p < 0.001), and also in the prevalence of current smoking (from 14.53% to 5.85%, p < 0.001), hypercholesterolemia (from 70.37% to 17.48%, p < 0.001), and hypertension (from 83.82% to 23.56%, p < 0.001). The average glucose level decreased during the first 2 years, but increased in the third, fourth, and 5th years.
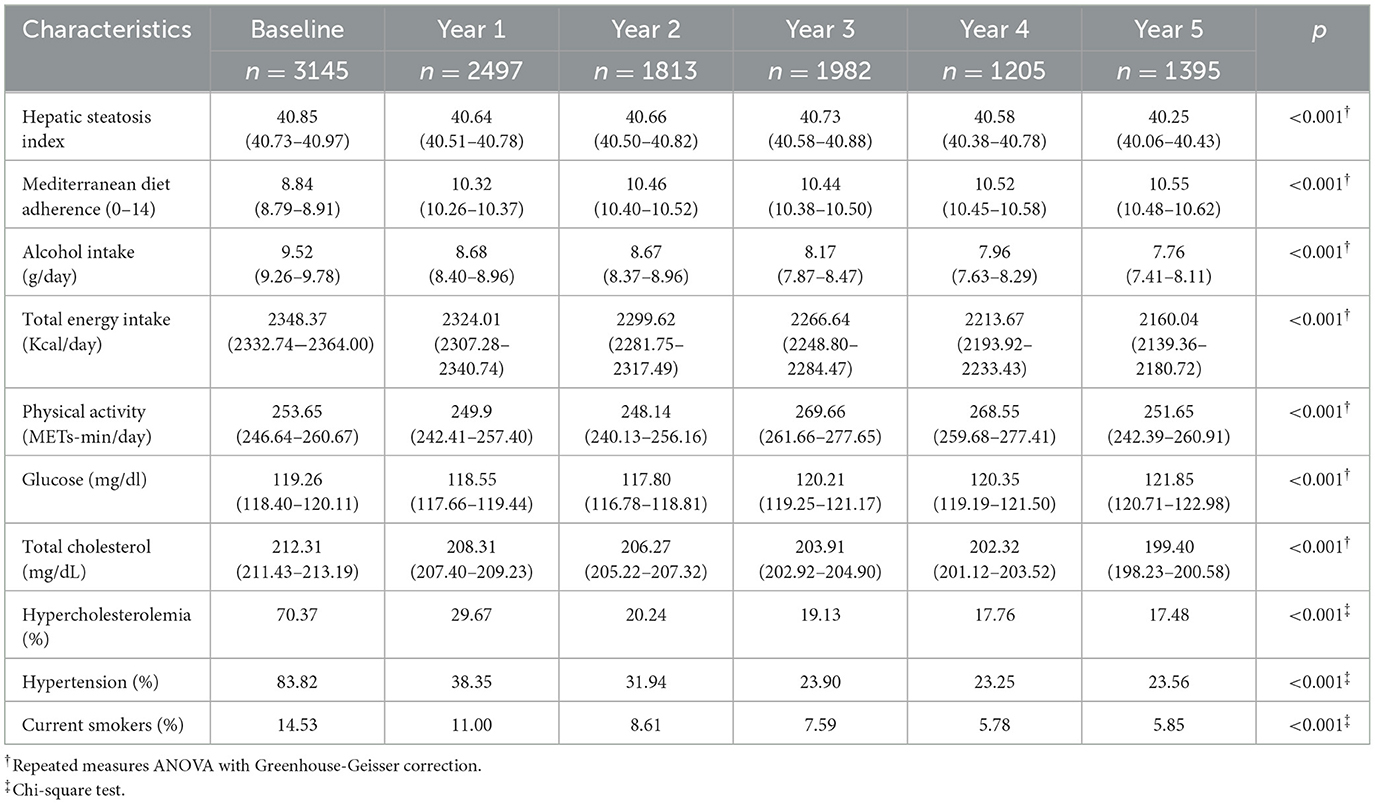
Table 2. Description of characteristics throughout the follow-up.
Table 3 shows the relationship between the study variables and the HSI. The interaction (product*term) assessing the effect of the randomized intervention on changes over time in HSI was not statistically significant in any of the three models, yielding p-values of 0.087, 0.097, and 0.230 in Models 1, 2, and 3, respectively. In all cases, however, the HSI decreased over time. As additional variables were incorporated into the models (from Models 1–3), the time coefficient increased slightly but remained negative. Thus, the association is consistent, even after adjusting for age, sex, alcohol intake, physical activity, and other covariates. Although the effect of time was attenuated in Model 3, it remained statistically significant. Additionally, significant inverse associations were observed between the HSI and the level of adherence to the MedDiet.
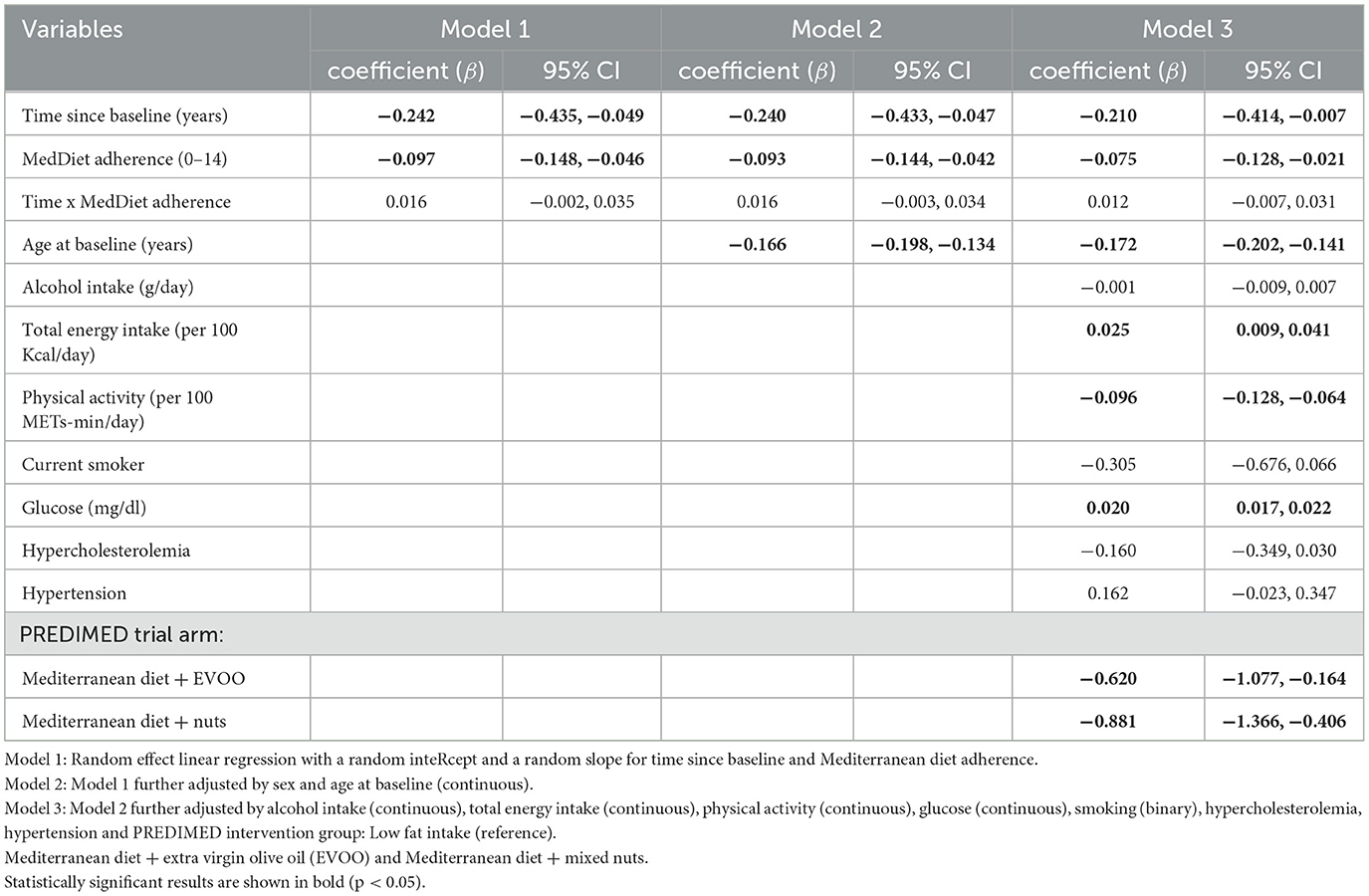
Table 3. Influence of study variables on hepatic steatosis index.
HSI values were significantly lower among the participants who entered the PREDIMED trial at an older age (Model 2: β = −0.166; 95% CI: −0.198, −0.134; Model 3: β = −0.172; 95% CI: −0.202, −0.14) and those who engaged in greater daily physical activity (β = −0.001; 95% CI: −0.0013, 0.0006). By contrast, values were significantly higher in participants with higher blood glucose levels (β = 0.020; 95% CI: 0.017, 0.022) and in those with a higher daily calorie intake (β = 0.0003; 95% CI: 0.0001, 0.0004).
In Model 3, the MedDiets supplemented with either EVOO or nuts were both inversely associated with the HSI, with statistical significance. Among the participants who consumed the MedDiet with EVOO, the HSI was 0.620 units (β = −0.620, 95%CI: −1.077, −0.164) less than in the reference group (low-fat diet), while for those who consumed the MedDiet with nuts, the corresponding difference was 0.881 units (β = −0.881, 95% CI: −1.366, −0.406).
Discussion
This study investigates the relationship between adherence to the MedDiet and the presence and progression of MASLD, as assessed by longitudinal changes in the HSI, in a large cohort of patients with cardiometabolic disorders followed for 5 years. Better adherence to the MedDiet is associated with a lower HSI. Specifically, the linear regression model, adjusted for potential confounders, shows that each one-point increase in the MEDAS score is associated with a 0.07-unit reduction in the HSI.
These findings are consistent with previous research in this field, suggesting that adherence to the MedDiet may positively affect cardiometabolic health and liver function (52–55). For instance, Baratta et al. demonstrated that adherence to the MedDiet was associated with a lower prevalence of liver steatosis (low adherence vs. high adherence: 96.5% vs. 71.4%; P < 0.001) (56). Additionally, Ryan et al. conducted a 6-week crossover dietary intervention study with the MedDiet and observed a significant reduction in liver steatosis and improved insulin sensitivity in insulin-resistant patients with MASLD (40).
In another study, Abenavoli et al. found that adherence to the MedDiet resulted in a sustained reduction in hepatic steatosis rates for up to 1 year (57). Similarly, a 6-month single-arm counseling intervention with MedDiet decreased the percentage of patients with steatosis grade 2 or higher from 93% to 48% (58). Moreover, our findings align with the results of the cross-sectional analysis of two studies conducted on over 13,000 participants across two population-based cohorts in Switzerland and England. The results showed that higher adherence to the MedDiet was associated with a lower prevalence of hepatic steatosis, assessed using abdominal ultrasound and FLI in the Fenland study (England), and the FLI and the MASLD score in the CoLaus study (Switzerland) (59). Furthermore, our findings are also consistent with two analyses conducted within the PREDIMED and PREDIMED-Plus cohorts. In the PREDIMED trial, participants with demographic and clinical profiles similar to those in the present study showed a direct correlation between liver damage (defined as >50th percentile FLI) and both a pro-inflammatory dietary pattern and lower adherence to the MedDiet in obese individuals (60). In the PREDIMED plus study, which included 278 participants from the Navarra-Nutrition node, adherence to the MedDiet negatively correlated with the HSI score, in both men (r = −0.18, p = 0.032) and women (r = −0.19, p = 0.027) (61). In a study of 276 PREDIMED-Málaga participants, the rate of change in FLI among the control group increased over time (1.13 ± 0.4; p = 0.006), suggesting that the MedDiet intervention delayed or slowed the natural progression of MASLD (62). A recent meta-analysis of six randomized controlled trials (total sample size: 250 participants) reported that the Mediterranean diet significantly reduced FLI compared to the control diet (standardized mean difference: −1.06, 95% CI: −1.95 to −0.17; p = 0.02) (63). In our study, the average HSI among participants who adhered to the MedDiet significantly decreased over the follow-up period, with a difference of −0.6 units between the first and fifth years.
The MedDiet is known to have beneficial health effects, especially in helping prevent cardiovascular disease (64–67). These benefits are probably mediated through the reduction of systemic inflammation, independent of changes in lipid levels or body weight (68). This association underscores the anti-inflammatory properties of the Mediterranean dietary pattern as a critical mechanism in mitigating cardiovascular risk and disease progression. These mechanisms are likely to exert also an impact on the development, prevention, and treatment of MASLD (43, 69–71). A recent publication highlighted the important role of diet in the preventive treatment of MASLD, although it also pointed out that no large-scale long-term population studies have yet been conducted to test the effects of structured lifestyle intervention programs on preventing this disease (72). The favorable outcomes achieved by the MedDiet for MASLD in our study may be explained, at least in part, by the fact that this dietary pattern is rich in polyphenols, carotenoids, vitamins, and other biomolecules that have anti-inflammatory and antioxidant effects (73–75). This characteristic seems to be relevant, since inflammation and oxidative stress are involved in the pathogenesis of MASLD (76). Moreover, the monounsaturated fatty acids present in the MedDiet, in olive oil, for example, improve the lipid profile, which is consistent with the significant decrease in the HSI observed in the intervention groups (MedDiet plus EVOO or nuts).
As well as the direct relation observed between the HSI and adherence to the MedDiet, it is also indirectly related to the participants' age of entry into the study and their level of physical activity. Thus, for every additional point scored for physical activity, the HSI decreased by 0.096 units, a statistically significant relation. This association aligns with previous research findings, according to which physical activity is helpful for patients with MASLD because it improves their metabolic condition (77). However, for this improvement to be effective, physical activity must be accompanied by an appropriate dietary intervention, such as the MedDiet, including antioxidants such as EVOO (78). With respect to the participants' age at entry, for each additional year at baseline, the HSI improved (i.e., fell) by 0.2 units. Although age is a predisposing factor for MASLD, we believe the latter finding may also reflect the baseline characteristics of our participants, in that those who met the inclusion criteria and were younger probably presented a higher level of deterioration than those who started later and would have been taking better care of themselves. If this were so, it would not be surprising that participants who began the study at an older age had a better prognosis and a lower HSI.
Our results show that the HSI is positively associated with the baseline glucose level and kilocalorie intake. Specifically, for every additional unit of the blood glucose level, the HSI increases (significantly) by 0.02 units. This could be because the accumulation of intrahepatic fat is associated with that of intrahepatic ceramides and diacylglycerols, which inhibit insulin signaling and, therefore, promote hepatic insulin resistance (79). With this increased hepatic insulin resistance, MASLD negatively affects glycaemic control in patients with T2D (78). In fact, patients with both T2D and MASLD generally require more intensive antidiabetic therapies to achieve optimal glycaemic control compared to patients with T2D alone (80). Regarding the relationship between the HSI and calorie intake, for every additional calorie consumed, the HSI increased by 0.025 units. Nevertheless, the participants' calorie intake decreased significantly during the 5-year follow-up. As is well known, excessive calorie consumption promotes obesity and related comorbidities such as MASLD, a relation that is corroborated in our study results and those of other investigations (81–84).
In our study, all participants reported baseline alcohol consumption within the defined limits of < 20 g/day for women and < 30 g/day for men. These thresholds align with widely accepted guidelines for low-to-moderate alcohol intake in clinical research. However, recent evidence suggests that even very moderate alcohol consumption, such as 66–96 g/week, may increase the risk of significant fibrosis progression compared to no or low alcohol consumption. This may be explained by the role of alcohol metabolism in exacerbating oxidative stress and inflammation, which are key mechanisms driving the progression of NAFLD and MASLD (85). Among smokers, there is a strong and dose-dependent correlation between MASLD and a smoking history of >10 pack-years. Moreover, ex-smokers who quit < 10 years ago are more susceptible to the disease than those who have never smoked (86). Stratifying participants by finer consumption thresholds and by the duration of smoking cessation could provide greater clarity on the dose- and time-dependent effects of alcohol and tobacco on liver histology and fibrosis progression. These findings highlight the need for cautious interpretation of the impact of moderate alcohol consumption and the time elapsed since smoking cessation on MASLD management.
Finally, as observed above, very few observational or field studies have assessed the impact of the MedDiet on the progression of hepatic steatosis, and those available differ significantly in terms of design, sample characteristics, and means of assessing adherence to the MedDiet, which makes any comparison difficult (87–89). In general, however, these papers report a beneficial effect of the MedDiet on hepatic steatosis, which is in line with our findings. The present study, moreover, was carried out on a sample of over 3,000 patients aged over 67 years, and presenting high cardiovascular risk (83% were hypertensive, 70% hypercholesterolaemic, and 47% diabetic), with a mean baseline BMI >29 kg/m2 and an HSI >30. This population, therefore, presented challenges for the effective management of MASLD. For these patients, the MedDiet may represent a valuable therapeutic option, as it is relatively easy to sustain, in contrast to the difficulties often experienced with more restrictive interventions in achieving sustained weight loss (90, 91).
Strengths and limitations
A multicenter randomized controlled trial study design is considered the gold standard for evaluating the efficacy and safety of dietary interventions. However, in the present case, despite the large sample size considered and the 5-year follow-up period, the study design has limitations, such as its use of an indirect estimator to measure MASLD. However, the HSI is a validated marker of hepatic steatosis that is based on a non-invasive and easy-to-determine measurement, which makes it suitable for large epidemiological studies. Previous studies have shown their results to be consistent (92–97). Additionally, the gold standard for assessing MASLD—liver biopsy—is an invasive method that cannot be implemented in large-scale epidemiological studies with predominantly healthy participants. Moreover, liver biopsies are costly and may introduce sampling errors and procedural complications (88). Another study limitation is the fact that the study sample was composed of older adults, all at high cardiovascular risk and living in the Mediterranean region. This profile limits the generalizability of our results to other age groups or ethnicities. However, as the intervention generated beneficial results in such a complex population, we would expect the results for the general population to be better still.
Conclusion
The findings of this study suggest that adherence to the Mediterranean diet is significantly associated with a long-term reduction in hepatic steatosis in patients with multimorbidity and at high cardiovascular risk, and highlight its potential as an effective strategy for reducing liver fat accumulation, particularly in individuals at risk of MASLD. Promoting the inclusion of the MedDiet as a supplementary strategy for preventing MASLD could generate substantial health improvements in at-risk populations, including individuals with obesity, T2D, dyslipidaemia, or hypertension, and particularly among older adults.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Ethics Committee for Research of Málaga. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
RC-G: Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AF-N: Writing – original draft, Writing – review & editing. MG-B: Writing – original draft, Writing – review & editing. MR-C: Writing – original draft, Writing – review & editing. MM-G: Writing – original draft, Writing – review & editing. LA: Writing – original draft, Writing – review & editing. NB: Writing – original draft, Writing – review & editing. MoF: Writing – original draft, Writing – review & editing. ER: Writing – original draft, Writing – review & editing. MiF: Writing – original draft, Writing – review & editing. RE: Writing – original draft, Writing – review & editing. FA: Writing – original draft, Writing – review & editing. LS-M: Writing – original draft, Writing – review & editing. XP: Writing – original draft, Writing – review & editing. CM-B: Writing – original draft, Writing – review & editing. AG-R: Writing – original draft, Writing – review & editing. EG-G: Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This research was funded by the Fundación Progreso y Salud (Project No. AP-0306-2022-C3-F2). The funder provided financial support for the professional translation of the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Ludwig J, Viggiano TR, McGill DB, Oh BJ. Nonalcoholic steatohepatitis: Mayo Clinic experiences with a hitherto unnamed disease. Mayo Clin Proc. (1980) 55:434–8. doi: 10.1016/S0025-6196(24)00530-5
2. Eslam M, Sanyal AJ, George J. International consensus panel. MAFLD: a consensus-driven proposed nomenclature for metabolic associated fatty liver disease. Gastroenterology. (2020) 158:1999–2014.e1. doi: 10.1053/j.gastro.2019.11.312
3. Rinella ME, Lazarus JV, Ratziu V, Francque SM, Sanyal AJ, Kanwal F, et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. J Hepatol. (2023) 79:1542–56. doi: 10.1016/j.jhep.2023.06.003
4. Bilson J, Mantovani A, Byrne CD, Targher G. Steatotic liver disease, MASLD and risk of chronic kidney disease. Diabetes Metab. (2024) 50:101506. doi: 10.1016/j.diabet.2023.101506
5. Hagström H, Vessby J, Ekstedt M, Shang Y. 99% of patients with NAFLD meet MASLD criteria and natural history is therefore identical. J Hepatol. (2024) 80:e76–7. doi: 10.1016/j.jhep.2023.08.026
6. European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO). EASL-EASD-EASO Clinical Practice Guidelines on the management of metabolic dysfunction-associated steatotic liver disease (MASLD). J Hepatol. (2024) 81:492–542. doi: 10.1016/j.jhep.2024.04.031
7. Chan WK, Chuah KH, Rajaram RB, Lim LL, Ratnasingam J, Vethakkan SR. Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD): A State-of-the-Art Review. J Obes Metab Syndr. (2023) 32:197–213. doi: 10.7570/jomes23052
8. Miao L, Targher G, Byrne CD, Cao YY, Zheng MH. Current status and future trends of the global burden of MASLD. Trends Endocrinol Metab. (2024) 35:697–707. doi: 10.1016/j.tem.2024.02.007
9. Liu J, Ayada I, Zhang X, Wang L, Li Y, Wen T, et al. Estimating global prevalence of metabolic dysfunction-associated fatty liver disease in overweight or obese adults. Clin Gastroenterol Hepatol. (2022) 20:e573–82. doi: 10.1016/j.cgh.2021.02.030
10. Chan KE, Koh TJL, Tang ASP, Quek J, Yong JN, Tay P, et al. Global prevalence and clinical characteristics of metabolic-associated fatty liver disease: a meta-analysis and systematic review of 10 739 607 individuals. J Clin Endocrinol Metab. (2022) 107:2691–700. doi: 10.1210/clinem/dgac321
11. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660
12. Younossi Z, Anstee QM, Marietti M, Hardy T, Henry L, Eslam M, et al. Global burden of NAFLD and NASH: trends, predictions, risk factors and prevention. Nat Rev Gastroenterol Hepatol. (2018) 15:11–20. doi: 10.1038/nrgastro.2017.109
13. Friedman SL, Neuschwander-Tetri BA, Rinella M, Sanyal AJ. Mechanisms of NAFLD development and therapeutic strategies. Nat Med. (2018) 24:908–22. doi: 10.1038/s41591-018-0104-9
14. Owrangi S, Paik JM, Golabi P, de Avila L, Hashida R, Nader A, et al. Meta-analysis: global prevalence and mortality of cirrhosis in metabolic dysfunction-associated steatotic liver disease. Aliment Pharmacol Ther. (2025) 61:433–43. doi: 10.1111/apt.18451
15. Brea Á, Pintó X, Ascaso JF, Blasco M, Díaz Á, González-Santos P, et al. Sociedad Española de Arteriosclerosis. Nonalcoholic fatty liver disease, association with cardiovascular disease and treatment (I) Nonalcoholic fatty liver disease and its association with cardiovascular disease. Clin Investig Arterioscler. (2017) 29:141–8. doi: 10.1016/j.artere.2016.06.001
16. Byrne CD, Targher G. NAFLD. A multisystem disease. J Hepatol. (2015) 62:S47–64. doi: 10.1016/j.jhep.2014.12.012
17. Dixon JB, Bhathal PS, O'Brien PE. Nonalcoholic fatty liver disease: Predictors of nonalcoholic steatohepatitis and liver fibrosis in the severely obese. Gastroenterology. (2001) 121:91–100. doi: 10.1053/gast.2001.25540
18. Alexander M, Loomis AK, Fairburn-Beech J, van der Lei J, Duarte-Salles T, Prieto-Alhambra D, et al. Real-world data reveal a diagnostic gap in non-alcoholic fatty liver disease. BMC Med. (2018) 16:130. doi: 10.1186/s12916-018-1103-x
19. Castera L, Friedrich-Rust M, Loomba R. Noninvasive assessment of liver disease in patients with nonalcoholic fatty liver disease. Gastroenterology. (2019) 156:1264–81.e4. doi: 10.1053/j.gastro.2018.12.036
20. Lee JH, Kim D, Kim HJ, Lee CH, Yang JI, Kim W, et al. Hepatic steatosis index: a simple screening tool reflecting nonalcoholic fatty liver disease. Dig Liver Dis. (2010) 42:503–8. doi: 10.1016/j.dld.2009.08.002
21. Caballería L, Pera G, Arteaga I, Rodríguez L, Alumà A, Morillas RM, et al. High prevalence of liver fibrosis among European adults with unknown liver disease: a population-based study. Clin Gastroenterol Hepatol. (2018) 16:1138–45.e5 doi: 10.1016/j.cgh.2017.12.048
22. Fedchuk L, Nascimbeni F, Pais R, Charlotte F, Housset C, Ratziu V. Performance and limitations of steatosis biomarkers in patients with nonalcoholic fatty liver disease. Aliment Pharmacol Ther. (2014) 40:1209–22. doi: 10.1111/apt.12963
23. Tafur Sánchez CN, Durá Gil M, Alemán Domínguez Del Río A, Hernández Pérez CM, Mora Cuadrado N, de. la Cuesta SG, et al. The practical utility of non-invasive indices in metabolic hepatic steatosis. Endocrinol Diabetes Nutr (Engl Ed). (2022) 69:418–25. doi: 10.1016/j.endien.2022.06.009
24. Thoma C, Day CP, Trenell MI. Lifestyle interventions for the treatment of non-alcoholic fatty liver disease in adults: a systematic review. J Hepatol. (2012) 56:255–66. doi: 10.1016/j.jhep.2011.06.010
25. European Association for the Study of the Liver (EASL). European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO). EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J Hepatol. (2016) 64:1388–402. doi: 10.1016/j.jhep.2015.11.004
26. Gepner Y, Shelef I, Komy O, Cohen N, Schwarzfuchs D, Bril N, et al. The beneficial effects of Mediterranean diet over low-fat diet may be mediated by decreasing hepatic fat content. J Hepatol. (2019) 71:379–88. doi: 10.1016/j.jhep.2019.04.013
27. Touvier M, da Costa Louzada ML, Mozaffarian D, Baker P, Juul F, Srour B. Ultra-processed foods and cardiometabolic health: public health policies to reduce consumption cannot wait. BMJ. (2023) 383:e075294. doi: 10.1136/bmj-2023-075294
28. Lindstrom J, Ilanne-Parikka P, Peltonen M, Aunola S, Eriksson JG, Hemiö K, et al. Sustained reduction in the incidence of type 2 diabetes by lifestyle intervention: follow-up of the Finnish Diabetes Prevention Study. Lancet. (2006) 368:1673–9. doi: 10.1016/S0140-6736(06)69701-8
29. Schenk S, Horowitz JF. Acute exercise increases triglyceride synthesis in skeletal muscle and prevents fatty acid-induced insulin resistance. J Clin Invest. (2007) 117:1690–8. doi: 10.1172/JCI30566
30. Elias MC, Parise ER, de Carvalho L, Szejnfeld D, Netto JP. Effect of 6-month nutritional intervention on non-alcoholic fatty liver disease. Nutrition. (2010) 26:1094–9. doi: 10.1016/j.nut.2009.09.001
31. Yabe Y, Kim T, Oh S, Shida T, Oshida N, Hasegawa N, et al. Relationships of dietary habits and physical activity status with non-alcoholic fatty liver disease featuring advanced fibrosis. Int J Environ Res Public Health. (2021) 18:8918. doi: 10.3390/ijerph18178918
32. Tosti V, Bertozzi B, Fontana L. Health benefits of the Mediterranean diet: metabolic and molecular mechanisms. J Gerontol A Biol Sci Med Sci. (2018) 73:318–26. doi: 10.1093/gerona/glx227
33. Di Daniele N, Noce A, Vidiri MF, Moriconi E, Marrone G, Annicchiarico-Petruzzelli M, et al. Impact of Mediterranean diet on metabolic syndrome, cancer and longevity. Oncotarget. (2017) 8:8947–79. doi: 10.18632/oncotarget.13553
34. Uluçay Kestane V, Baş M. Efficacy of the Mediterranean diet containing different macronutrients on non-alcoholic fatty liver disease. Nutrients. (2024) 16:2699. doi: 10.3390/nu16162699
35. Li T, Zhao J, Cao H, Han X, Lu Y, Jiang F, et al. Dietary patterns in the progression of metabolic dysfunction-associated fatty liver disease to advanced liver disease: a prospective cohort study. Am J Clin Nutr. (2024) 120:518–27. doi: 10.1016/j.ajcnut.2024.07.015
36. Zou P, Wang L. Dietary pattern and hepatic lipid metabolism. Liver Res. (2023) 7:275–84. doi: 10.1016/j.livres.2023.11.006
37. Vancells Lujan P, Viñas Esmel E, Sacanella Meseguer E. Overview of Non-Alcoholic Fatty Liver Disease (NAFLD) and the role of sugary food consumption and other dietary components in its development. Nutrients. (2021) 13:1442. doi: 10.3390/nu13051442
38. Barrea L, Tarantino G, Somma CD, Muscogiuri G, Macchia PE, Falco A, et al. Adherence to the Mediterranean diet and circulating levels of Sirtuin 4 in obese patients: a novel association. Oxid Med Cell Longev. (2017) 2017:6101254. doi: 10.1155/2017/6101254
39. Kontogianni MD, Tileli N, Margariti A, Georgoulis M, Deutsch M, Tiniakos D, et al. Adherence to the Mediterranean diet is associated with the severity of non-alcoholic fatty liver disease. Clin Nutr. (2014) 33:678–83. doi: 10.1016/j.clnu.2013.08.014
40. Ryan MC, Itsiopoulos C, Thodis T, Ward G, Trost N, Hofferberth S, et al. The Mediterranean diet improves hepatic steatosis and insulin sensitivity in individuals with non-alcoholic fatty liver disease. J Hepatol. (2013) 59:138–43. doi: 10.1016/j.jhep.2013.02.012
41. Trovato FM, Catalano D, Martines GF, Pace P, Trovato GM. Mediterranean diet and non-alcoholic fatty liver disease: the need of extended and comprehensive interventions. Clin Nutr. (2014) 34:86–8. doi: 10.1016/j.clnu.2014.01.018
42. Anania C, Perla FM, Olivero F, Pacifico L, Chiesa C. Mediterranean diet and nonalcoholic fatty liver disease. World J Gastroenterol. (2018) 24:2083–94. doi: 10.3748/wjg.v24.i19.2083
43. Estruch R, Ros E, Salas-Salvadó J, Covas MI, Corella D, Arós F, et al. Primary prevention of cardiovascular disease with a Mediterranean diet supplemented with extra-virgin olive oil or nuts. N Engl J Med. (2018) 378:e34. doi: 10.1056/NEJMoa1800389
44. Guasch-Ferré M, Hu FB, Martínez-González MA, et al. Olive oil intake and risk of cardiovascular disease and mortality in the PREDIMED Study. BMC Med. (2014) 12:78. doi: 10.1186/1741-7015-12-78
45. Martínez-González MÁ, Corella D, Salas-Salvadó J, Ros E, Covas MI, Fiol M, et al. Cohort profile: design and methods of the PREDIMED study. Int J Epidemiol. (2012) 41:377–85. doi: 10.1093/ije/dyq250
46. Schröder H, Fitó M, Estruch R, Martínez-González MA, Corella D, Salas-Salvadó J, et al. A short screener is valid for assessing Mediterranean diet adherence among older Spanish men and women. J Nutr. (2011) 141:1140–5. doi: 10.3945/jn.110.135566
47. Martínez-González MA, Fernández-Jarne E, Serrano-Martínez M, Wright M, Gómez-Gracia E. Development of a short dietary intake questionnaire for the quantitative estimation of adherence to a cardioprotective Mediterranean diet. Eur J Clin Nutr. (2004) 58:1550–2. doi: 10.1038/sj.ejcn.1602004
48. Martínez-González MA, Martínez JA, Hu FB, Gibney MJ, Kearney J. Physical inactivity, sedentary lifestyle and obesity in the European Union. Int J Obes Relat Metab Disord. (1999) 23:1192–201. doi: 10.1038/sj.ijo.0801049
49. Escolar Castellón JL, Pérez Romero de la Cruz C, Corrales Márquez R. Actividad física y enfermedad [Physical activity and disease]. An Med Interna. (2003) 20:427–33. doi: 10.4321/S0212-71992003000800010
50. Elosua R, Marrugat J, Molina L, Pons S, Pujol E. Validation of the Minnesota Leisure Time Physical Activity Questionnaire in Spanish men. The MARATHOM Investigators. Am J Epidemiol. (1994) 139:1197–209. doi: 10.1093/oxfordjournals.aje.a116966
51. Elosua R, Garcia M, Aguilar A, Molina L, Covas MI, Marrugat J. Validation of the minnesota leisure time physical activity questionnaire in Spanish women. Investigators of the MARATHON Group. Med Sci Sports Exerc. (2000) 32:1431–7. doi: 10.1097/00005768-200008000-00011
52. Vicinanza R, Troisi G, Cangemi R, De Martino MU, Pastori D, Bernardini S, et al. Aging and adherence to the Mediterranean diet: relationship with cardiometabolic disorders and polypharmacy. J Nutr Health Aging. (2018) 22:73–81. doi: 10.1007/s12603-017-0922-3
53. Pitsavos C, Panagiotakos DB, Chrysohoou C, et al. The adoption of Mediterranean diet attenuates the development of acute coronary syndromes in people with the metabolic syndrome. Nutr J 2, 1. (2003). doi: 10.1186/1475-2891-2-1
54. Panagiotakos DB, Arapi S, Pitsavos C, Antonoulas A, Mantas Y, Zombolos S, Stefanadis C. The relationship between adherence to the Mediterranean diet and the severity and short-term prognosis of acute coronary syndromes (ACS): The Greek Study of ACS (The GREECS). Nutrition. (2006) 22:722–30. doi: 10.1016/j.nut.2006.04.005
55. Buil-Cosiales P, Toledo E, Salas-Salvadó J, et al. Association between dietary fiber intake and fruit, vegetable or whole-grain consumption and the risk of CVD: results from the PREvención con DIeta MEDiterránea (PREDIMED) trial. Br J Nutr. (2016) 116:534–46. doi: 10.1017/S0007114516002099
56. Baratta F, Pastori D, Polimeni L, Bucci T, Ceci F, Calabrese C, et al. Adherence to Mediterranean diet and non-alcoholic fatty liver disease: effect on insulin resistance. Am J Gastroenterol. (2017) 112:1832–9. doi: 10.1038/ajg.2017.371
57. Abenavoli L, Milic N, Peta V, Alfieri F, De Lorenzo A, Bellentani S. Alimentary regimen in non-alcoholic fatty liver disease: Mediterranean diet. World J Gastroenterol. (2014) 20:16831–40. doi: 10.3748/wjg.v20.i45.16831
58. Gelli C, Tarocchi M, Abenavoli L, Di Renzo L, Galli A, De Lorenzo A. Effect of a counseling-supported treatment with the Mediterranean diet and physical activity on the severity of the non-alcoholic fatty liver disease. World J Gastroenterol. (2017) 23:3150–62. doi: 10.3748/wjg.v23.i17.3150
59. Khalatbari-Soltani S, Imamura F, Brage S, De Lucia Rolfe E, Griffin SJ, Wareham NJ, et al. The association between adherence to the Mediterranean diet and hepatic steatosis: Cross-sectional analysis of two independent studies, the UK Fenland Study and the Swiss CoLaus Study. BMC Med. (2019) 17:19. doi: 10.1186/s12916-019-1251-7
60. Cantero I, Abete I, Babio N, Aros F, Corella D, Estruch R, et al. Dietary Inflammatory Index and liver status in subjects with different adiposity levels within the PREDIMED trial. Clin Nutr. (2018) 37:1736–43. doi: 10.1016/j.clnu.2017.06.027
61. Bullón Vela MV, Abete I, Zulet MLÁ, Tur JA, Pintó X, Corbella E, et al. Risk factors differentially associated with non-alcoholic fatty liver disease in males and females with metabolic syndrome. Rev Esp Enferm Dig. (2020) 112:94–100. doi: 10.17235/reed.2019.6031/2018
62. Cueto-Galán R, Barón FJ, Valdivielso P, et al. Changes in fatty liver index after consuming a Mediterranean diet: 6-year follow-up of the PREDIMED-Malaga trial. Med Clin (Barc). (2017) 148:435–43. doi: 10.1016/j.medcle.2017.04.030
63. Kawaguchi T, Charlton M, Kawaguchi A, Yamamura S, Nakano D, Tsutsumi T, et al. Effects of Mediterranean diet in patients with nonalcoholic fatty liver disease: a systematic review, meta-analysis, and meta-regression analysis of randomized controlled trials. Semin Liver Dis. (2021) 41:225–34. doi: 10.1055/s-0041-1723751
64. Sofi F, Abbate R, Gensini GF, Casini A. Accruing evidence on benefits of adherence to the Mediterranean diet on health: an updated systematic review and meta-analysis. Am J Clin Nutr. (2010) 92:1189e96. doi: 10.3945/ajcn.2010.29673
65. Kastorini CM, Milionis HJ, Esposito K, Giugliano D, Goudevenos JA, Panagiotakos DB. The effect of Mediterranean diet on metabolic syndrome and its components: a meta-analysis of 50 studies and 534,906 individuals. J Am Coll Cardiol. (2011) 57:1299e313. doi: 10.1016/j.jacc.2010.09.073
66. Estruch R, Martínez-González MA, Corella D, et al. Effect of a high-fat Mediterranean diet on bodyweight and waist circumference: a prespecified secondary outcomes analysis of the PREDIMED randomized controlled trial. Lancet Diabetes Endocrinol. (2016) 4:666–76. doi: 10.1016/S2213-8587(16)30085-7
67. Ros E, Martínez-González MA, Estruch R, Salas-Salvadó J, Fitó M, Martínez JA, et al. Mediterranean diet and cardiovascular health: teachings of the PREDIMED Study. Adv Nutr. (2014) 5:330S−6S. doi: 10.3945/an.113.005389
68. Itsiopoulos C, Mayr HL, Thomas CJ. The anti-inflammatory effects of a Mediterranean diet: a review. Curr Opin Clin Nutr Metab Care. (2022) 25:415–22. doi: 10.1097/MCO.0000000000000872
69. Hassani Zadeh S, Mansoori A, Hosseinzadeh M. Relationship between dietary patterns and non-alcoholic fatty liver disease: a systematic review and meta-analysis. J Gastroenterol Hepatol. (2021) 36:1470–8. doi: 10.1111/jgh.15363
70. Yu C, Gao J, Ge X, Wang X, Ding Y, Tian T, et al. Healthy lifestyle is associated with reduced mortality in patients with non-alcoholic fatty liver disease. Nutrients. (2022) 14:3785. doi: 10.3390/nu14183785
71. Katsagoni C, Papatheodoridis G, Ioannidou P, Deutsch M, Alexopoulou A, Papadopoulos N, et al. Improvements in clinical characteristics of patients with non-alcoholic fatty liver disease after an intervention based on the Mediterranean lifestyle: A randomized controlled clinical trial. Br J Nutr. (2018) 120:164–75. doi: 10.1017/S000711451800137X
72. Romero-Gómez M, Zelber-Sagi S, Martín F, Bugianesi E, Soria B. Nutrition could prevent or promote non-alcoholic fatty liver disease: an opportunity for intervention. BMJ. (2023) 383:e075179. doi: 10.1136/bmj-2023-075179
73. Pintó X, Fanlo-Maresma M, Corbella E, et al. A Mediterranean diet rich in extra-virgin olive oil is associated with a reduced prevalence of nonalcoholic fatty liver disease in older individuals at high cardiovascular risk. J Nutr. (2019) 149:1920–9. doi: 10.1093/jn/nxz147
74. Abenavoli L, Boccuto L, Federico A, Dallio M, Loguercio C, Di Renzo L, et al. Diet and non-alcoholic fatty liver disease: the Mediterranean way. Int J Environ Res Public Health. (2019) 16:3011. doi: 10.3390/ijerph16173011
75. Barbouti A, Goulas V. Dietary antioxidants in the Mediterranean diet. Antioxidants. (2021) 10:1213. doi: 10.3390/antiox10081213
76. Salomone F, Godos J, Zelber-Sagi S. Natural antioxidants for non-alcoholic fatty liver disease: molecular targets and clinical perspectives. Liver Int. (2016) 36:5–20. doi: 10.1111/liv.12975
77. Farzanegi P, Dana A, Ebrahimpoor Z, Asadi M, Azarbayjani MA. Mechanisms of beneficial effects of exercise training on non-alcoholic fatty liver disease (NAFLD): Roles of oxidative stress and inflammation. Eur J Sport Sci. (2019) 19:994–1003. doi: 10.1080/17461391.2019.1571114
78. Marin-Alejandre BA, Abete I, Cantero I, Monreal JI, Elorz M, Herrero JI, et al. The metabolic and hepatic impact of two personalized dietary strategies in subjects with obesity and nonalcoholic fatty liver disease: the Fatty Liver in Obesity (FLiO) randomized controlled trial. Nutrients. (2019) 11:2543. doi: 10.3390/nu11102543
79. Birkenfeld AL, Shulman GI. Nonalcoholic fatty liver disease, hepatic insulin resistance, and type 2 diabetes. Hepatology. (2014) 59:713–23. doi: 10.1002/hep.26672
80. Ballestri S, Zona S, Targher G, Romagnoli D, Baldelli E, Nascimbeni F, et al. Nonalcoholic fatty liver disease is associated with an almost twofold increased risk of incident type 2 diabetes and metabolic syndrome. Evidence from a systematic review and meta-analysis. J Gastroenterol Hepatol. (2016) 31:936–44. doi: 10.1111/jgh.13264
81. Cusi K. Treatment of patients with type 2 diabetes and non-alcoholic fatty liver disease: current approaches and future directions. Diabetologia. (2016) 59:1112–20. 10.1007/s00125-016-3952–1. doi: 10.1007/s00125-016-3952-1
82. Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease: Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology. (2016) 64:73–84. doi: 10.1002/hep.28431
83. Romero-Gómez M, Zelber-Sagi S, Trenell M. Treatment of NAFLD with diet, physical activity and exercise. J Hepatol. (2017) 67:829–46. doi: 10.1016/j.jhep.2017.05.016
84. Konieczna J, Ruiz-Canela M, Galmes-Panades AM, et al. an energy-reduced Mediterranean diet, physical activity, and body composition: an interim subgroup analysis of the PREDIMED-Plus randomized clinical trial. JAMA Netw Open. (2023) 6:e2337994. doi: 10.1001/jamanetworkopen.2023.37994
85. Blomdahl J, Nasr P, Ekstedt M, Kechagias S. Moderate alcohol consumption is associated with significant fibrosis progression in NAFLD. Hepatol Commun. (2023) 7:e0003. doi: 10.1097/HC9.0000000000000003
86. Jang YS, Joo HJ, Park YS, Park EC, Jang SI. Association between smoking cessation and non-alcoholic fatty liver disease using NAFLD liver fat score. Front Public Health. (2023) 11:1015919. doi: 10.3389/fpubh.2023.1015919
87. Abenavoli L, Greco M, Milic N, Accattato F, Foti D, Gulletta E, Luzza F. Effect of Mediterranean diet and antioxidant formulation in non-alcoholic fatty liver disease: a randomized study. Nutrients. (2017) 9:870. doi: 10.3390/nu9080870
88. Fraser A, Abel R, Lawlor DA, Fraser D, Elhayany A. A modified Mediterranean diet is associated with the greatest reduction in alanine aminotransferase levels in obese type 2 diabetes patients: results of a quasi-randomized controlled trial. Diabetologia. (2008) 51:1616–22. doi: 10.1007/s00125-008-1049-1
89. Aller R, Izaola O, de. la Fuente B, De Luis Roman DA. Mediterranean diet is associated with liver histology in patients with nonalcoholic fatty liver disease. Nutr Hosp. (2015) 32:2518–24. doi: 10.3305/nh.2015.32.6.10074
90. Chalasani N, Younossi Z, Lavine JE, Charlton M, Cusi K, Rinella M, et al. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology. (2018) 67:328–57. doi: 10.1002/hep.29367
91. Rachakonda V, Wills R, DeLany JP, Kershaw EE, Behari J. Differential impact of weight loss on nonalcoholic fatty liver resolution in a North American cohort with obesity. Obesity. (2017) 25:1360–8. doi: 10.1002/oby.21890
92. Zou H, Ma X, Zhang F, Xie Y. Comparison of the diagnostic performance of twelve noninvasive scores of metabolic dysfunction-associated fatty liver disease. Lipids Health Dis. (2023) 22:145. doi: 10.1186/s12944-023-01902-3
93. Wang C, Cai Z, Deng X, Li H, Zhao Z, Guo C, et al. Association of hepatic steatosis index and fatty liver index with carotid atherosclerosis in type 2 diabetes. Int J Med Sci. (2021) 18:3280–9. doi: 10.7150/ijms.62010
94. Cicero A, D'Addato S, Reggi A, Reggiani G, Borghi C. Hepatic steatosis index and lipid accumulation product as middle-term predictors of incident metabolic syndrome in a large population sample: data from the Brisighella Heart Study. Intern Emerg Med. (2013) 8:265–7. doi: 10.1007/s11739-012-0875-9
95. Sviklāne L, Olmane E, Dzērve Z, Kupčs K, Pirāgs V, Sokolovska J. Fatty liver index and hepatic steatosis index for prediction of non-alcoholic fatty liver disease in type 1 diabetes. J Gastroenterol Hepatol. (2018) 33:270–6. doi: 10.1111/jgh.13814
96. Ruhl CE, Everhart JE. Fatty liver indices in the multiethnic United States National Health and Nutrition Examination Survey. Aliment Pharmacol Ther. (2015) 41:65–76. doi: 10.1111/apt.13012
97. Machado MV, Cortez-Pinto H. Non-invasive diagnosis of non-alcoholic fatty liver disease. A critical appraisal. J Hepatol. (2013) 58:1007–19. doi: 10.1016/j.jhep.2012.11.021
ANNEX
Annex 1. Hepatic Steatosis Index (HSI). The hepatic steatosis index is based on four variables: transaminases (ALT and AST), body mass index (BMI), sex, and type 2 diabetes (T2D): HSI = 8 × (ALT/AST ratio) + BMI. (+2, if female; +2, with T2D). The interpretation is as follows:
• HSI < 30, no steatosis.
• HSI > 36, hepatic steatosis.
Keywords: PREDIMED, dietary adherence, Mediterranean diet, randomized controlled trial, metabolic dysfunction-associated steatotic liver disease, hepatic steatosis index
Citation: Cueto-Galán R, Fontalba-Navas A, Gutiérrez-Bedmar M, Ruiz-Canela M, Martínez-González MA, Alves L, Babio N, Fitó M, Ros E, Fiol M, Estruch R, Arós F, Serra-Majem L, Pintó X, Muñoz-Bravo C, García-Rodríguez A and Gómez-Gracia E (2025) Adherence to the Mediterranean diet to prevent or delay hepatic steatosis: a longitudinal analysis within the PREDIMED study. Front. Nutr. 12:1518082. doi: 10.3389/fnut.2025.1518082
Received: 28 November 2024; Accepted: 22 April 2025;
Published: 21 May 2025.
Edited by:
Roberto Vicinanza, University of Southern California, United StatesReviewed by:
Ludovico Abenavoli, Magna Græcia University, ItalyGiovanni Tarantino, University of Naples Federico II, Italy
Sara Carnevale, Azienda Sanitaria Locale di Viterbo, Italy
Copyright © 2025 Cueto-Galán, Fontalba-Navas, Gutiérrez-Bedmar, Ruiz-Canela, Martínez-González, Alves, Babio, Fitó, Ros, Fiol, Estruch, Arós, Serra-Majem, Pintó, Muñoz-Bravo, García-Rodríguez and Gómez-Gracia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andres Fontalba-Navas, YWZvbnRhbGJhQHVtYS5lcw==