 Jinwen Chen
Jinwen Chen Changhong Shi
Changhong Shi- 1Department of Neonatology, Hefei Maternal and Child Health Hospital, Hefei, Anhui, China
- 2School of Public Health, Guangzhou Medical University, Guangzhou, Guangdong, China
Objective: Overweight and obesity among children and adolescents has emerged as a critical global public health issue. Oxidative stress, a key factor in obesity-related inflammation and metabolic dysregulation, underscore the importance of dietary antioxidants. The composite dietary antioxidant index (CDAI), which integrates vitamins A, C, E, carotenoids, selenium, and zinc, provide a comprehensive measure of overall dietary antioxidant intake. However, the relationship between CDAI and overweight/obesity in children and adolescents remains insufficient explored.
Methods: This study utilized data from the National Health and Nutrition Examination Survey (NHANES) collected between 2011 and 2016, including 17,919 participants aged 6–19 years. The CDAI were calculated based on dietary intake data from 24-hour dietary recalls. To account for total energy intake, two widely recognized adjustment methods were used: the standard regression model and the nutrient density model. In the nutrient density model, an energy-standardized CDAI (E-CDAI) was computed. Logistic regression models were conducted to examine associations between CDAI, E-CDAI, mCDAI, mE-CDAI, and overweight/obesity risk, adjusting for potential confounders such as age, gender, race, physical activity, and socioeconomic status.
Results: The analysis showed a significant negative association between CDAI and overweight/obesity risk among adolescents aged 12–19 years. However, no significant association was observed in children aged 6–11 years. In contrast, E-CDAI showed no significant association with overweight/obesity risk in adolescents (OR = 0.87; 95% CI: 0.71–1.07). Notably, selenium exhibited a negative association with overweight/obesity in the standard regression model but a positive association in the nutrient density model. After excluding the selenium from the original 6 antioxidants included in the CDAI, the modified CDAI (mCDAI) demonstrated a significant negative association with overweight/obesity in both the standard regression model (OR = 0.74; 95% CI: 0.63–0.86) and nutrients density model (OR = 0.78; 95% CI: 0.69–0.89).
Conclusion: This study developed a modified CDAI, comprising of vitamins A, C, E, carotenoids, and zinc, and identified a consistent negative association between mCDAI and overweight/obesity risk, irrespective of energy adjustment method. These findings suggest that a diet rich in antioxidants may play a protective role in preventing obesity in adolescent aged 12–19 years.
1 Introduction
Overweight and obesity have emerged as critical global public health challenges, particularly among children and adolescents. According to the latest World Health Organization (WHO) report, more than 300 million children and adolescents aged 5–19 years worldwide are classified as overweight or obese (1). The prevalence of overweight has increased nearly fivefold, while obesity rates have risen approximately sevenfold compared to levels four decades ago (2). In the United States, this trend is particularly pronounced, with the obesity rate among children and adolescent escalating from 17.7% in 2011 to 21.5% by 2020 (3). Obesity is now widely recognized as a complex, multifactorial disease that adversely impacts multiple physiological systems and can profoundly affect a child's intellectual, behavioral, psychological, and sexual development, with consequences that often persist throughout the lifespan (4, 5). Moreover, childhood obesity is strongly associated with an increased susceptibility to chronic condition in adulthood, including cardiovascular disease, type 2 diabetes mellitus (T2DM), non-alcoholic fatty liver disease (NAFLD) and certain types of cancer (6, 7). These compelling health implications underscore the urgent need for developing and implementing effective prevention and intervention strategies to mitigate the growing burden of childhood obesity.
Emerging evidence suggests that oxidative stress plays a pivotal role in the development and progression of obesity-related metabolic complications (8, 9). Excessive adipose tissue in obesity is a major source of reactive oxygen species (ROS), which can trigger chronic inflammation, contributing to insulin resistance, endothelial dysfunction, and other metabolic disturbances (10). These findings have sparked increasing interest in the potential protective effect of dietary antioxidants against obesity and its related disorders (11, 12). Some studies indicated that regions with high rates of antioxidant nutrient deficiencies also experience greater obesity prevalence (13). A recent systematic review found that obese individuals tend to have a lower concentration of antioxidants, particularly carotenoids, vitamins E and C, zinc, magnesium and selenium (14). However, contradictory results have been regarding the association between obesity and dietary antioxidants, especially in adolescents. For example, Galan et al. found no significant association between zinc and selenium concentration and obesity in 3,128 participants (15). Similarly, Yang et al. (16) found that selenium was not an independent protective factor against obesity in US adults but rather showed a positive association with obesity risk.
Although the health benefits of individual antioxidants have been extensively investigated, recent research has increasingly focused on the synergistic effects of multiple dietary antioxidants. Several studies have explored the relationship between weight status and various antioxidant indices, including the dietary antioxidant index (DAI) (17), total antioxidant capacity (TAC) (18), and dietary antioxidant quality score (DAQS)(19). Using weighted quantile sum (WQS) regression, Yang et al. (16) demonstrated that a combination of 11 antioxidants was negatively related to prevalence of obesity and abdominal obesity. The composite dietary antioxidant index (CDAI) is a comprehensive metric designed to assess overall dietary antioxidant intake by incorporating various key antioxidants (20), including vitamins A, C, E, carotenoids, selenium, and zinc. Previous studies have demonstrated an association between higher CDAI and reduced markers of oxidative stress and inflammation (21–24). Despite distinct dietary patterns and metabolic profiles in children and adolescents, the potential impact of overall antioxidant intake on obesity risk in this population remains underexplored.
This study aims to address this gap by examine the association between the composite dietary antioxidant index (CDAI) and the prevalence of overweight or obesity among children and adolescents in the United States, using data from the National Health and Nutrition Examination Survey (NHANES) from 2011 to 2016. We hypothesize that higher CDAI, indicative of greater antioxidant intake, is associated with a lower risk of overweight and obesity in this population. Total energy intake may represent a key confounder in the relationship between CDAI and overweight/obesity risk (25). To account for this, we employed two distinct models, the standard regression model and the nutrient density model (26). In the nutrient density model, we developed an energy-standardized CDAI (E-CDAI) score. Additionally, the dietary antioxidant quality score (DAQS) was calculated by comparing antioxidants intakes to their respective age-specified daily recommended intake values. Logistic regression models were conducted to examine associations between CDAI, E-CDAI, DAQS, and overweight/obesity risk, adjusting for potential confounders such as age, gender, race, physical activity, and socioeconomic status.
2 Methods
2.1 Study design and population
This study used data from the National Health and Nutrition Examination Survey (NHANES) conducted between 2011 and 2016. NHANES employs a complex, stratified, multistage probability sampling method to collect health and nutritional information from a representative sample of the civilian, non-institutionalized U.S. population. The survey protocol was approved by the NCHS Research Ethics Review Committee, and written informed consent was obtained from all participants. Detailed information on the NHANES design and procedures can be found in previous studies.
Inclusion criteria required participants to have completed at least two 24-h dietary recalls. Exclusion criteria included missing data on key variables such as BMI, energy intake, or household income. The NHANES database provides information on various parameters such as age, gender, race, socioeconomic status, physical activity, energy intake, dietary components, and anthropometric measurements for study participants. This process resulted in a final sample of 17,919 participants. A detailed study flowchart is depicted in Figure 1.
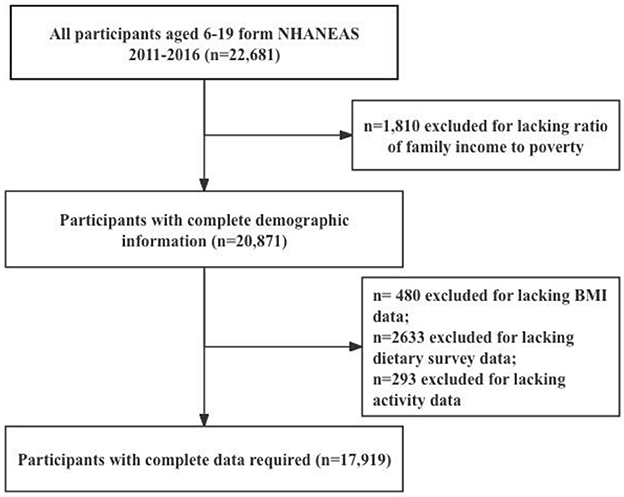
Figure 1. Flow chart of inclusion and exclusion criteria for the study sample. NHANES, National Health and Nutrition Survey; BMI, Body Mass Index.
2.2 Overweight and obesity data
Overweight and obesity data, including height and weight, were collected using standardized procedures. BMI was calculated as weight in kilograms divided by height in meters squared. Based on the CDC growth charts, participants were classified into the following categories (24): underweight (BMI below the 15th percentile), normal weight (BMI between the 15th and 85th percentiles), overweight (BMI between the 85th and 95th percentiles), and obesity (BMI at or above the 95th percentile).
2.3 Composite dietary antioxidant index
The composite dietary antioxidant index (CDAI) was computed using dietary data from the NHANES 24-h recall interviews. The index encompasses 6 key antioxidants: vitamins A, C, E, carotenoids, selenium, and zinc. To calculate the CDAI, we used the method proposed by Wright et al. (20), which involves standardizing each antioxidant by subtracting the global mean and dividing by the global standard deviation, which is calculated as follows:
where xi represents the daily antioxidant intake, mean(xi) indicates the mean amount of these antioxidants within the study cohort, and std(xi) denotes the standard deviation. By leveraging these 24-h dietary recall data, CDAI scores can provide a comprehensive evaluation of the antioxidant intake at the individual level.
To adjust for total energy intake in the analysis, we employed two widely recognized adjustment approach, the standard regression model and the nutrient density model (26). Within the nutrient density model, we calculated the density of each antioxidant nutrient by dividing the absolute antioxidant intake by the total energy intake, expressed as yi = xi/energy. Subsequently, we derived an energy-standardized CDAI (E-CDAI) using the following formula:
2.4 Covariates
NHANES adjusted for individual characteristics using several covariates, including age, sex, race, ethnicity, BMI, physical activity, poverty-income ratio and vitamin D. Detailed information on measurement procedures is available on the CDC website. Physical activity data were collected following World Health Organization guidelines. For adolescents, physical activity was categorized according to the 2018 Physical Activity Guidelines Advisory Committee report (27), participants who reported <10 min of moderate-to-vigorous physical activity per week were labeled as inactive. For children, physical activity was categorized into two groups: active (≥4 days) or inactive (<4 days) according to the question: “Days physically active at least 60 min.”
2.5 Statistical analysis
The study conducted descriptive analyses on the entire sample, with data further stratified by age group (children aged 6–11 years vs. adolescents aged 12–19 years). Results were presented as weighted median with interquartile range [median (interquartile range)] or percentage (%) for baseline characteristics. Continuous variables were analyzed using the Wilcoxon test or Kruskal–Wallis test. The association between categorical variables was examined using the Chi-square test. Multiple logistic regression was employed to assess the association between CDAI or E-CDAI and weighted-related measures (overweight/obesity, obesity). We construct 3 models to comprehensively evaluate the relationship between them: Model 1 includes age, gender, race, and household income-to-poverty ratio (PIR); Model 2 includes adjustments for physical activity. In model 3, we further adjusted for total energy intake. After dividing CDAI or E-CDAI into quartiles, trends tests were utilized to analyze their linear association trend. The results were presented as odds ratios (ORs) with 95% confidence intervals (CIs) across quartiles of CDAI and E-CDAI. All analyses were conducted using R software (version 4.4.2), with significance set at a p-value of < 0.05.
3 Results
3.1 Baseline characteristics
The study included 17,919 participants from the NHANES 2011–2016 dataset, consisting of 9,052 males (51.5%) and 8,867 females (48.5%). Participants were stratified into two age groups: children (6–11 years 43.1%) and adolescents (12–19 years, 56.9%). There were no statistically significant differences in gender, race/ethnicity, BMI status, energy intake, or poverty-income ratio between children and adolescents. However, adolescents had significantly lower average intakes of certain micronutrient, including vitamin D, vitamin A, vitamin C, and carotenoids, than children (p < 0.001). Conversely, selenium intake was higher in adolescents (p < 0.001). Overall, adolescents exhibited lower scores for both the composite dietary antioxidant index (CDAI) and the energy-standardized CDAI (E-CDAI) compared to children (CDAI: p = 0.025; E-CDAI: p < 0.001). These differences may reflect age-related changes in dietary habits, with adolescents possibly consuming more processed foods with lower antioxidant content. Table 1 details these baseline characteristics.
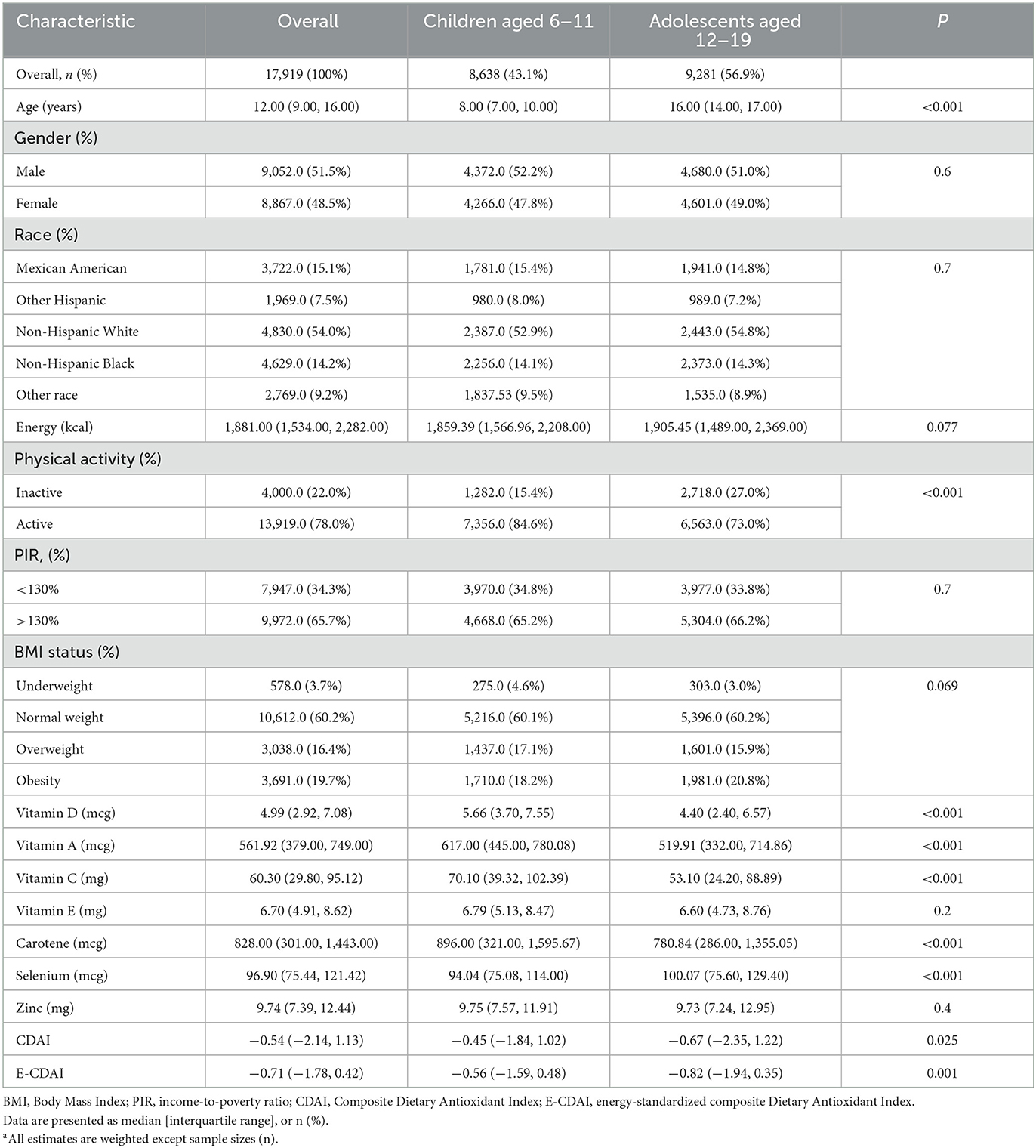
Table 1. Baseline characteristics of US children and adolescents aged 6–19 years, NHANES 2011–2016.a
3.2 Univariate analysis of overweight/obesity
As presented in Table 2, univariate analyses were conducted to evaluated factors associated with the risk of overweight/obesity. Ethnicity emerged as a significant factor, with Non-Hispanic White participants demonstrating the highest rates of overweight/obesity (p < 0.001). Lower income-to-poverty ratios were significant associated with a higher prevalence of overweight/obesity in both children (p = 0.023) and adolescents (p = 0.035). Among adolescents, overweight/obese individuals had significantly lower CDAI scores compared to their normal-weight counterparts (p < 0.001), whereas no significant differences were observed for the E-CDAI. In children, neither CDAI nor E-CDAI showed significant differences between BMI categories. Notably, overweight/obese adolescents had significant lower average intake of all assessed micronutrients, including vitamin D, vitamin A, vitamins C, vitamin E, carotene, selenium, and zinc (all p < 0.05). In contrast, no such difference were observed in children. These findings suggest that the role of dietary antioxidants in overweight/obesity may vary by age group, reflecting difference in metabolic profile and dietary patterns between children and adolescent.
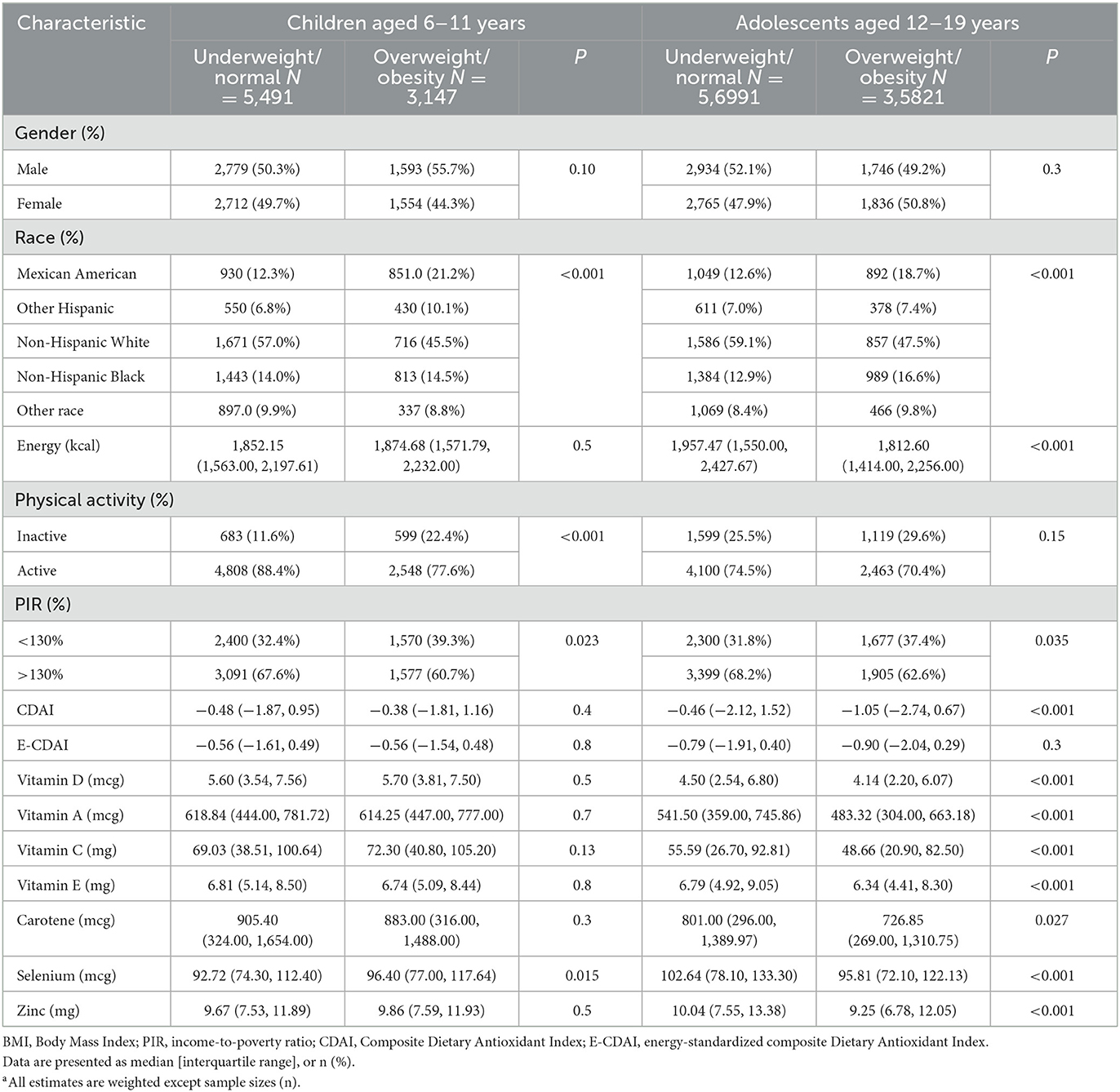
Table 2. Univariate analysis of overweight/obesity in US children and adolescents aged 6–19 years, NHANES 2011–2016.a
3.3 Association between CDAI and overweight/obesity
Logistic regression models were conducted to explore the relationship between the composite dietary antioxidant index (CDAI), energy-standardized CDAI (E-CDAI), and overweight/obesity risk across different age groups, as presented in Table 3.
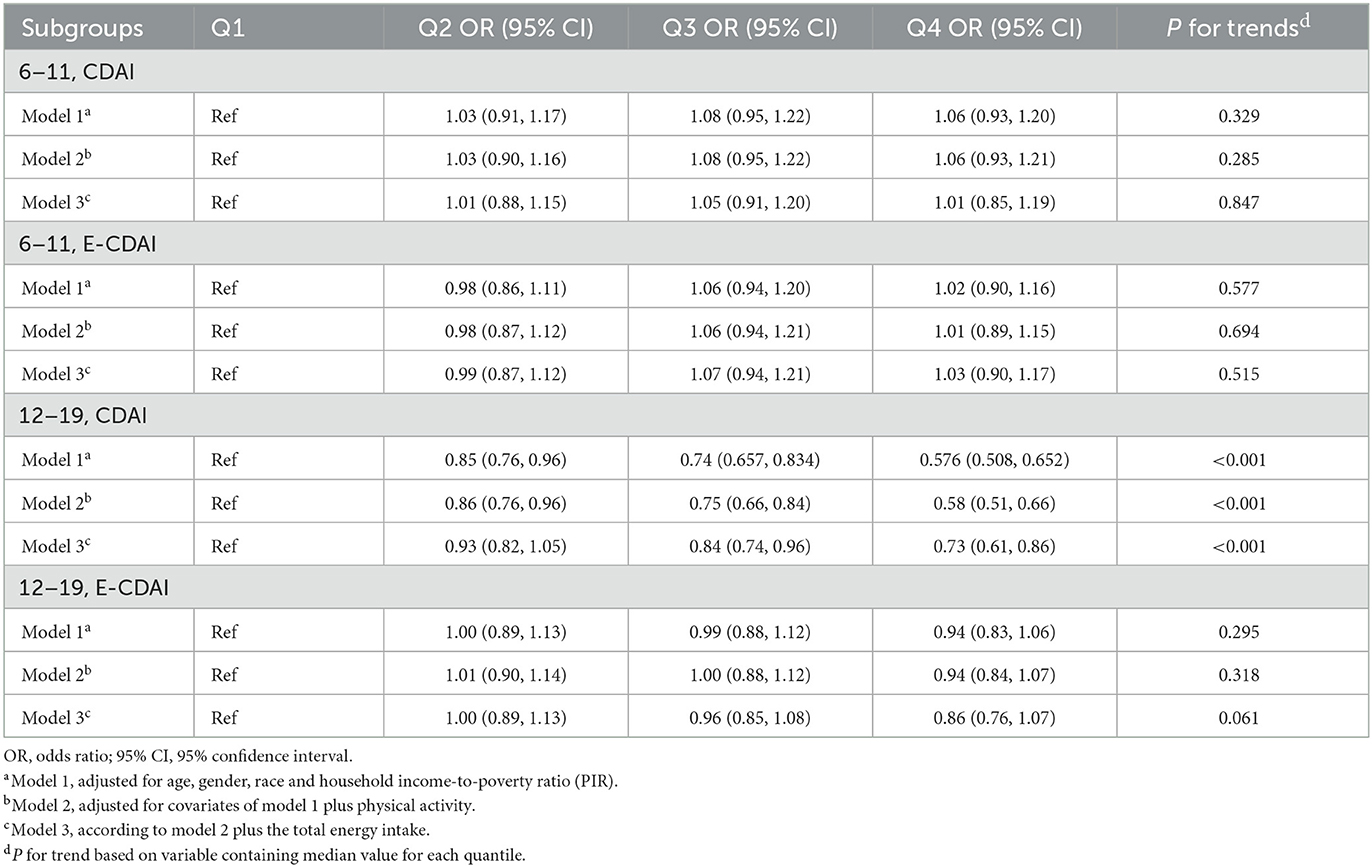
Table 3. Association between overweight/obesity and CDAI, E-CDAI in children and adolescents in US, NHAENS 2011–2016.
In children aged 6–11 years, no statistically significant associations were observed between either CDAI or E-CDAI and overweight/obesity in children across all adjusted models. The odds ratios (ORs) for overweight/obesity show no significant variation across quartiles of CDAI (p for trend > 0.05). Similarly, E-CDAI also demonstrated no significant association with overweight/obesity in this age group (p for trend > 0.05).
Among adolescents aged 12–19 years, a significant negative association was observed between CDAI and the risk of overweight/obesity among adolescents. Participants in the highest quartile of CDAI had a significantly lower odds of being overweight/obese compared to those in the lowest quartile (Model 3 OR = 0.73; 95% CI: 0.61–0.86; p for trend < 0.001). However, in the nutrient density model, E-CDAI showed no significant association with overweight/obesity risk (p for trend = 0.061). This discrepancy suggest that the method of energy adjustment may significantly influence the observed association between antioxidants indices and overweight/obesity.
3.4 Association of antioxidants with overweight/obesity
We explored the relationship between overweight/obesity and both the absolute intake and nutrient density of individual antioxidants included in the CDAI, such as carotenoids, vitamins E and C, zinc, magnesium, and selenium. Comparative analyses of these measures are presented in Tables 4, 5. Nutrient density for each antioxidant nutrient was calculated as the ratio of absolute antioxidant intake to total energy intake.
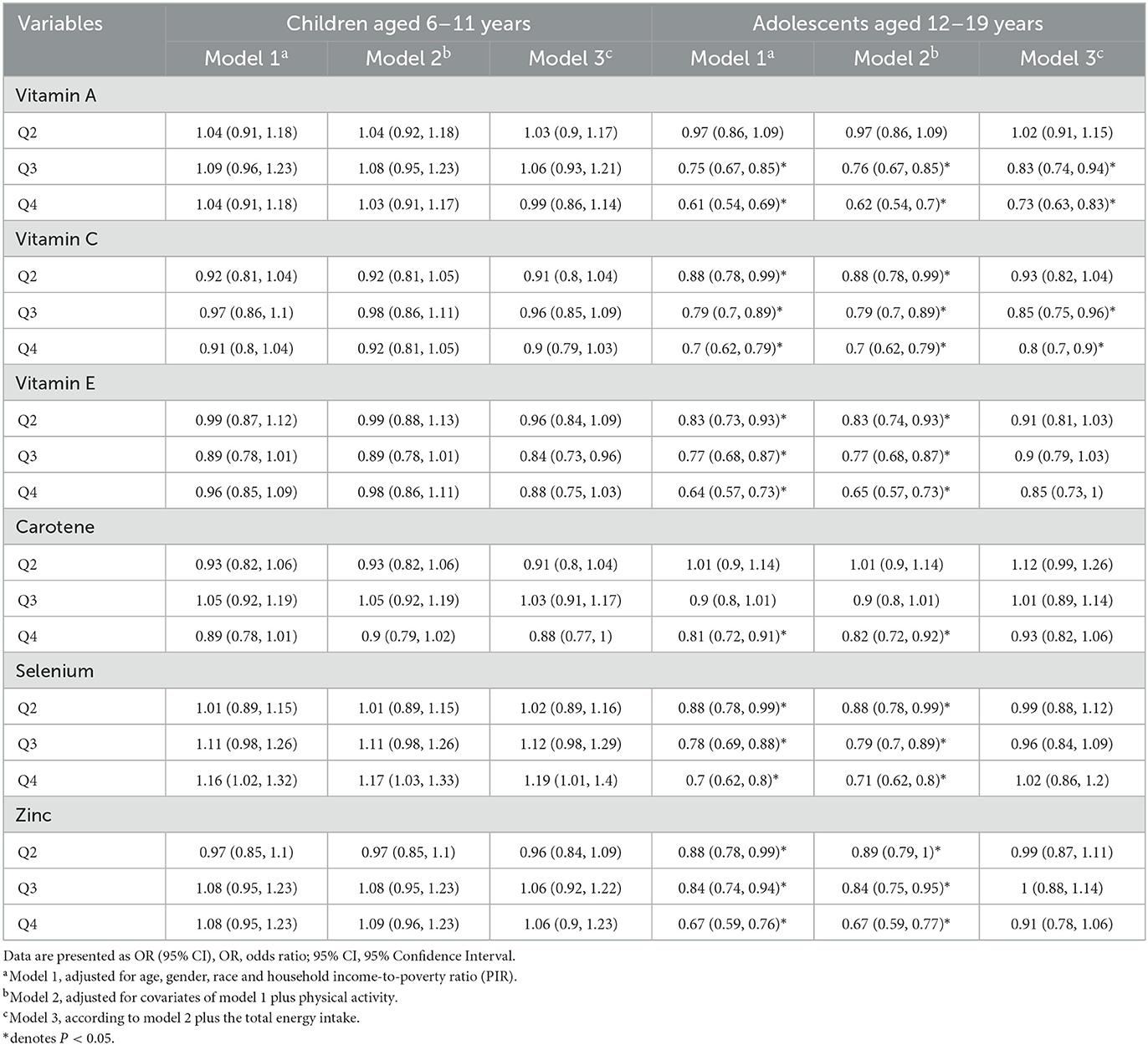
Table 4. Association between overweight/obesity and individual antioxidants in children and adolescents.

Table 5. Association between overweight/obesity and antioxidantsd density in children and adolescents.
In children aged 6–11 years, no significant associations were found between the intake of individual antioxidants (vitamins A, C, E, carotenoids, selenium, and zinc) and the risk of overweight/obesity in children after adjustment for potential confounding factors.
Among adolescents aged 12–19 years, higher intakes of vitamins A, C, and E were significantly associated with a reduced risk of overweight/obesity in adolescents. Specifically, individual in the highest quartile of vitamin A intake had a 27% lower risk of overweight/obese compared to those in the lowest quartile (Model 3 OR = 0.73; 95% CI: 0.63–0.83). A similar protective effect was observed for vitamin C intake (Model 3 OR = 0.80; 95% CI: 0.70–0.90). Notably, these reverse association remained statistically significant in the nutrient density model (Table 6). Interestingly, while selenium density showed a positive association with overweight/obese (Model 2 OR = 1.23; 95% CI: 1.09–1.39; Table 5), absolute selenium showed negative association (Model 2 OR = 0.71, 95% CI: 0.62–0.80) (Table 4), suggesting a complex relationship between selenium and weight status.
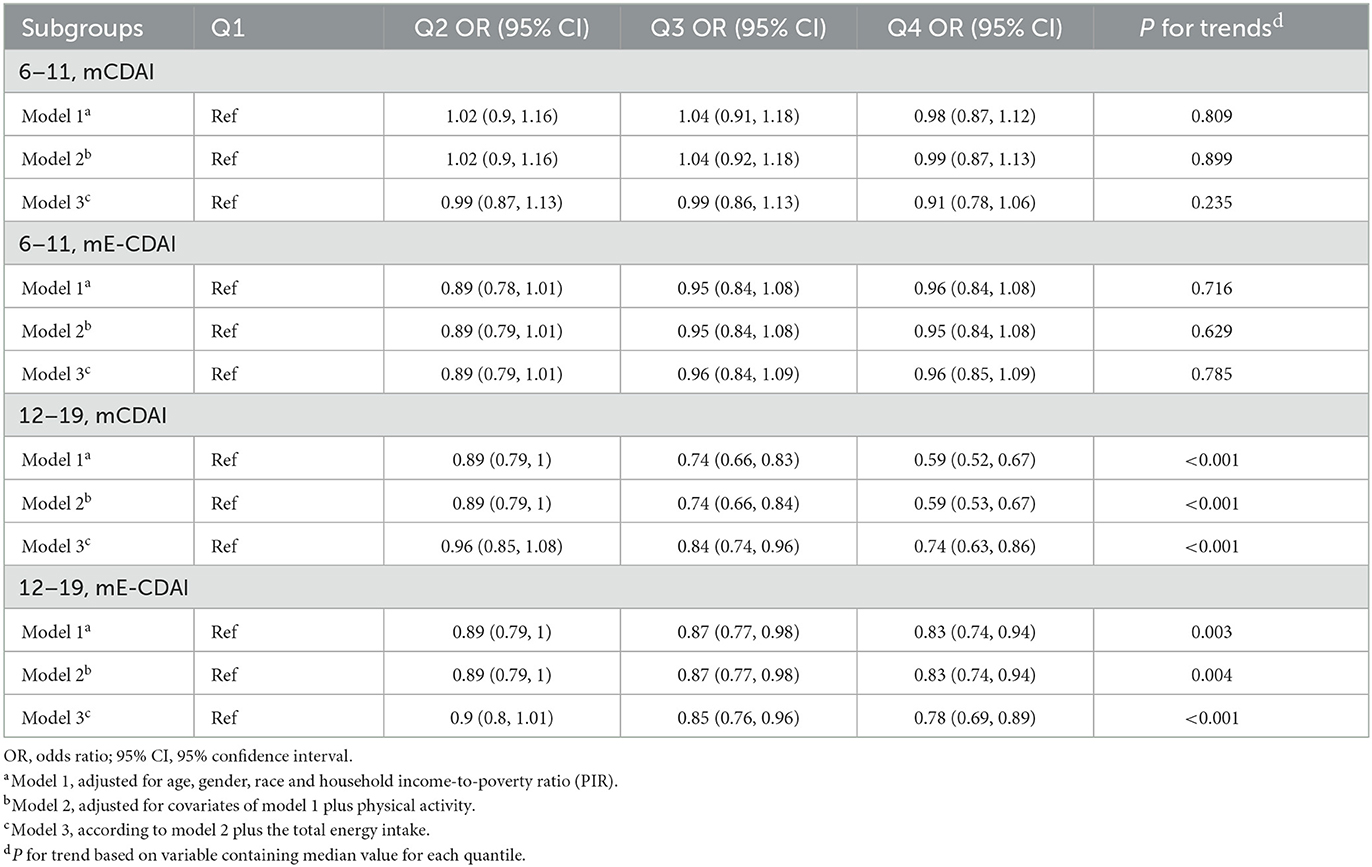
Table 6. Association between overweight/obesity and mCDAI, mE-CDAI in children and adolescents in US, NHAENS 2011–2016.
3.5 Association between modified CDAI and overweight/obesity
The above analysis demonstrated that the method of energy adjustment can reverse the direction of the association between selenium and weight status, potentially explaining the lack of a significant association between E-CDAI and overweight/obesity was observed in the multivariate nutrient density model. To address this, we developed a modified CDAI (mCDAI) score by excluding selenium from the original 6 antioxidants included in the CDAI. Following the same analytical apporach, we applied both the standard regression model and nutrient density model to adjust the confounding effect of total energy intake. Logistic regression models were conducted to explore the relationship between the modified composite dietary antioxidant index (mCDAI), modified energy-standardized CDAI (mE-CDAI), and overweight/obesity risk across different age groups, as detailed in Table 6.
In children aged 6–11 years, no statistically significant associations were observed between either mCDAI or mE-CDAI and overweight/obesity in children across all adjusted models. In contrast, among adolescents aged 12–19 years, a significant negative association was observed between mCDAI and the risk of overweight/obesity among adolescents in both standard regression model (Model 3 OR = 0.74; 95% CI: 0.63–0.86; p for trend < 0.001) and multivariate nutrient density model (Model 3 OR = 0.78; 95% CI: 0.69–0.89; p for trend < 0.001). These findings suggest that the exclusion of selenium from the CDAI may enhance the robustness of the association between dietary intake and overweight/obesity. In addition, there was no sex difference in the relationship between mCDAI, mE-CDAI and overweight/obesity (Table 7).
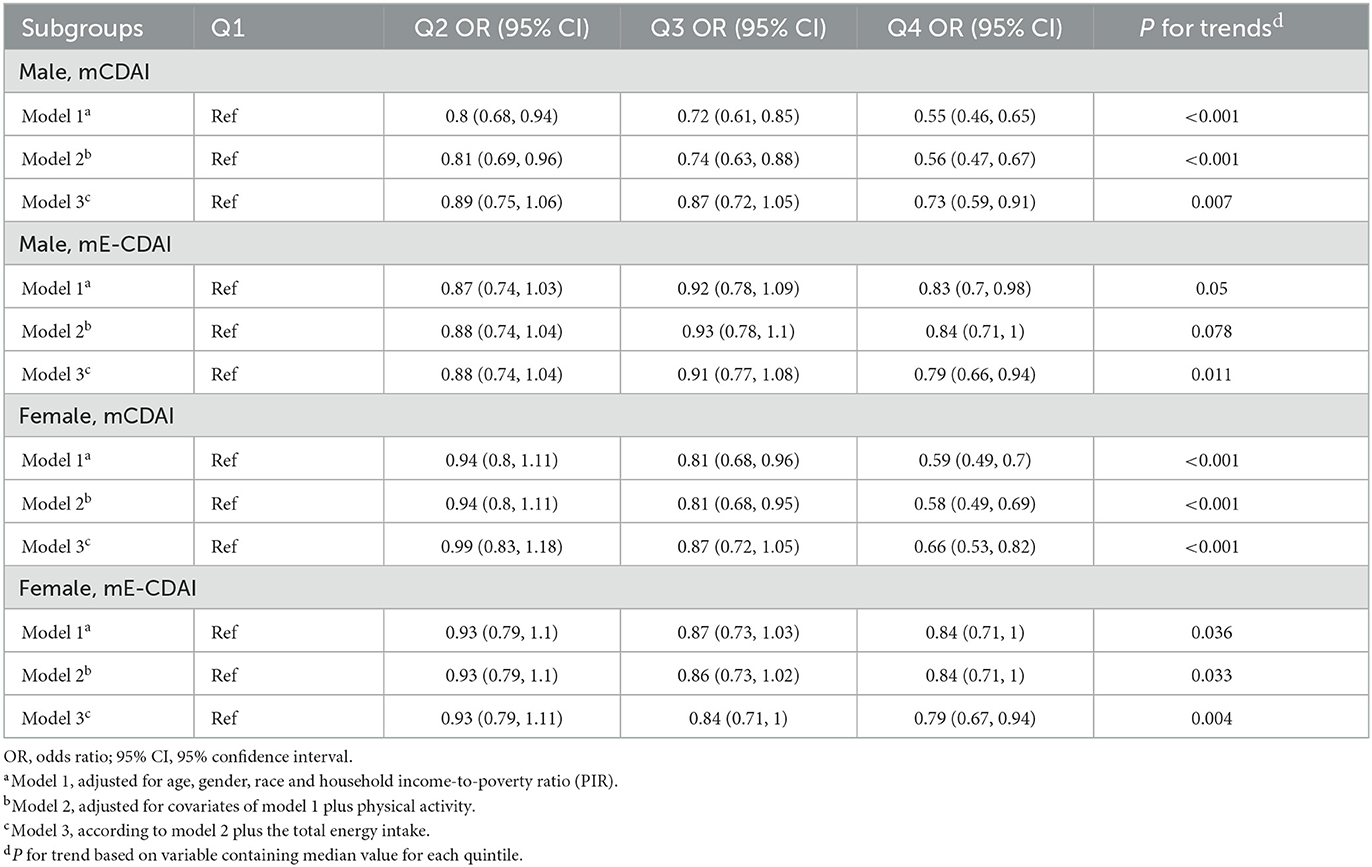
Table 7. Association between obesity and mCDAI, mE-CDAI in adolescents aged 12–19 years by sex NHAENS 2011–2016.
3.6 Association of DAQS with overweight/obesity
Recognizing that nutritional requirement vary significantly across different developmental stages, particularly within the broad age range of 6–19 years, we evaluated individual antioxidant against the daily recommended intake (DRI) established by the National Academies of Science, Engineering, and Medicine (NASEM) (28). Given the absence of an official DRI for carotenoids, this nutrient was excluded from the analysis. For each of five remained nutrients, a binary scoring system was implemented: a score of 0 was assigned if the nutrient intake fell below the age-specific DRI, and a score of 1was assigned if the intake meets or exceeded the age-specific DRI. Subsequently, we calculated the dietary antioxidant quality score (DAQS) by summing the score for the five antioxidants, resulting in a scale ranging from 0 (very poor quality) to 5 (high quality).
We further examined the association between overweight/obesity and both individual antioxidant score and the DAQS, as presented in Table 8. In children aged 6–11 years, no statistically significant associations were observed between overweight/obesity and either DAQS or individual antioxidant across all adjusted models. In contrast, among adolescents aged 12–19 years, a significant negative association was observed between DAQS and the risk of overweight/obesity (OR = 0.91; 95% CI: 0.86–0.96). Additionally, vitamins A (OR = 0.83; 95% CI: 0.73–0.94) and vitamins C (OR = 0.88; 95% CI: 0.86–0.96) demonstrated significant inverse association with overweight/obesity in this age group. However, no significant associations were observed between overweight/obesity and Vitamin E, Selenium or Zinc in adolescents.
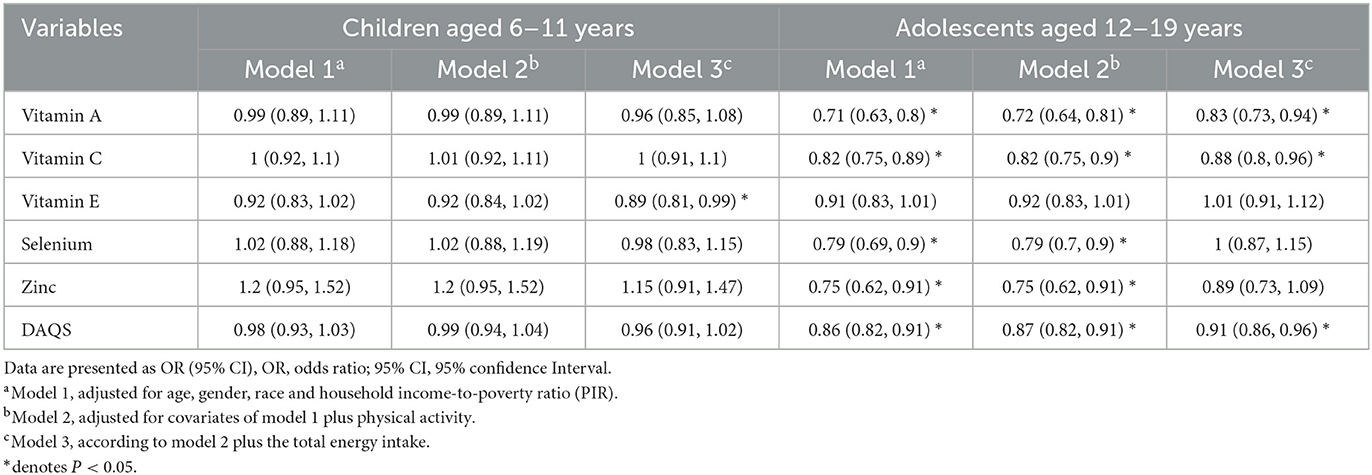
Table 8. Association between overweight/obesity and DAQS and individual antioxidants score in children and adolescents.
4 Discussion
In this cross-sectional study, we investigate the relationship between the composite dietary antioxidant index (CDAI) and overweight/obesity among 17,919 participants aged 6–19 years in the United States, utilizing data from NHANES spanning 2011–2016. We employed two distinct models, the standard regression model and the nutrient density model, to adjust for total energy intake. In the standard regression model, a significant negative association was observed between CDAI score and overweight/ obesity among adolescents, but not among children. Similarly, the dietary antioxidant quality score (DAQS) was also inversely associated with overweight/obesity in adolescents. However, in the nutrient density model, no significant association was found between the energy standardized CDAI (E-CDAI) score and overweight/obesity in either age group. Interestingly, we find that selenium showed a negative association with overweight/obesity in the standard regression model, but a positive association in the nutrient density model. After excluding the selenium from the original 6 antioxidants included in the CDAI, the modified CDAI (mCDAI) demonstrated a significant negative association with overweight/obesity in both the standard regression model.
Oxidative stress plays a critical role in the pathogenesis of obesity (29), characterized by an imbalance between reactive oxygen species (ROS) production and the body's antioxidant defenses. Increased adiposity is linked with heightened ROS production, leading to oxidative damage and chronic inflammation (30), which can further exacerbate fat accumulation and metabolic dysregulation. Numerous studies have investigated the association between individual antioxidants and obesity, as well as the underlying causal mechanism. For instance, Aeberli et al. (31) found that dietary intake of antioxidant vitamins (vitamin E, A, and C) was significantly associated with leptin level in Swedish children, suggesting that low concentration of these vitamins may alter the leptin genetic expression, contributing to leptin resistance and increases obesity risk. Similarly, Puchau et al. (18) reported that obese children and adolescents consumed lower amounts of vitamin E and C compared to their non-obese counterparts. A case-control study in Thailand further identified a negative association between BMI, waist, and serum concentrations of vitamins E (32). These findings align with our partial results, which indicate that vitamins A, C, and E were inversely associated with overweight/obesity in adolescents, both in the standard regression model and nutrient density model. Previous research has also demonstrated significant associations between dietary carotene intake and blood carotenoid levels, with lower serum carotene concentrations often observed in obese individuals (33). Our analysis similarly revealed a negative association between absolute carotene intake and obesity risk; however, this association became non-significant in the nutrient density model. Interestingly, selenium exhibits a negative association with obesity risk in adolescents in the standard regression model, but this relationship shifted to a positive association in the nutrient density model. Some studies have reported a significant correlation between dietary selenium intake and obesity. For example, Yang et al. (16) found that selenium was not an independent protective factor against obesity in US adults but was positive associated with it. Emerging evidence suggests that selenium toxicity can manifests as oxidative stress, impaired biofilm development, and suppression of enzyme function when present in excessive amounts (34, 35). These findings are consistent with our results.
Given that the effect of antioxidants is often dependent on their interaction with one another, their collective effect on weight status may differ from that of individual antioxidant. Therefore, in this study we focus on the association between the composite dietary antioxidant index (CDAI) and overweight/obesity in children and adolescents. To our knowledge, few studies have explored similar relationships using alternative dietary antioxidant indices. Notably, Kokkou et al. conducted a cross-sectional study involving 1,580 students aged 10–12 years, utilizing a dietary antioxidant index (DAI) that incorporated magnesium instead of carotenoids (17). Their findings revealed a significant inverse correlation between DAI scores and body weight status. Similarly, Aminnejad et al. investigated a modified version of DAI (including manganese rather than carotenoids) in a cohort of 593 adolescent boys (12–16 years), demonstrating a beneficial association between elevated antioxidant intake and improved weight status (36). In contrast, a study employing the dietary antioxidant quality score (DAQS) (excluding magnesium) in a larger sample of 4,270 participants aged 6–18 years paradoxically found that overweight and obese children exhibited higher intakes of certain dietary antioxidants compared to their normal-weight counterparts (19). These findings provide valuable insights for further research and underscore the need for standardized assessment of dietary antioxidant capacity in future studies.
Nutrient intake is generally correlated with total energy intake, as individuals who consume more energy tend to ingest larger quantities of most specific nutrients. As depicted in Figure 2A, CDAI shows a strong positive correlation with total energy intake. Total energy intake is a well-established risk factor for overweight/obesity, contributing to increased adiposity regardless of the dietary composition (37). Thus, total energy intake may represent a key confounder in the relationship between CDAI and overweight/obesity risk. To adjust for the total energy intake, we employed both the standard regression model and the nutrient density model (E-CDAI). As illustrated in Figure 2B, E-CDAI displayed a weak negative correlation with total energy intake. Our findings indicate a significant negative association between CDAI and the risk of overweight/obesity among adolescents, whereas no significant relationship was observed between E-CDAI and overweight/obesity in either age group. Further analysis revealed a negative association between overweight/obesity and absolute selenium intake, but a positive association between overweight/obesity and selenium density, potentially explaining the lack of a significant association between E-CDAI and overweight/obesity was observed in the nutrient density model. To address this, we developed a modified CDAI (mCDAI) score by excluding selenium from the original 6 antioxidants included in the CDAI. Further analysis demonstrated the modified CDAI (mCDAI) showed a significant negative association with overweight/obesity in both the standard regression model. Since Willet and Stampfer's 1986 publication (38), most nutritional epidemiology studies have routinely incorporated some form of energy adjustment. However, debate persist regarding the most appropriate approach (39, 40). The two models differ in their interpretation: in the standard regression model, the regression coefficient represents the apparent effect of increasing the antioxidant by 1 unit while maintaining a constant total energy intake; in the multivariate nutrient density model, the regression coefficients reflect the apparent effect of nutrient density in units of the percentage of energy from the nutrient. Given of the longstanding use of nutrient densities by nutritionists and the application of nutrient densities in public health recommendations (41, 42), the nutrient density model is widely adopted for estimating dietary effects.
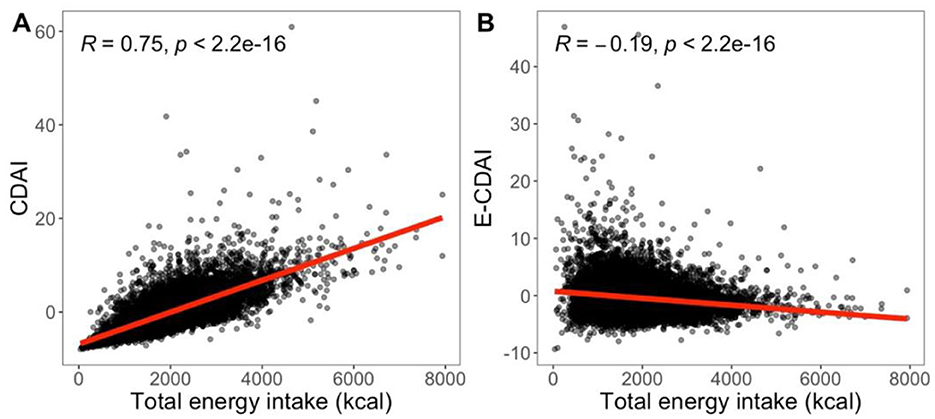
Figure 2. (A) CDAI has a high positive correlation with total energy intake (r = 0.75); (B) E-CDAI has a weak negative correlation with total energy intake (r = −0.19). Both were evaluated using the Spearman coefficient.
There are several limitations to this study that warrant consideration. The cross-sectional design prevents us from inferring causality between CDAI and obesity. Longitudinal studies are needed to explore whether increasing energy-standardized antioxidant intake can help prevent obesity over time. Additionally, the reliance on self-reported dietary recalls may introduce bias and inaccuracies in estimating antioxidant intake and energy consumption. Using objective biomarkers of antioxidant status and energy expenditure in future studies could provide more reliable data. Furthermore, this study did not account for other factors that could influence the relationship between antioxidants and obesity, such as individual genetics, hormonal status and gut microbiota. Future research should explore these factors to better understand the complex interactions between diet, oxidative stress, and obesity risk.
5 Conclusion
In conclusion, this study found that higher absolute dietary antioxidant intake, as measured by the composite dietary antioxidant index (CDAI), was significantly associated with a reduced risk of overweight and obesity among adolescents aged 12–19 years. However, the energy-standardized CDAI (E-CDAI) did not show a significant relationship with overweight/obesity. When selenium was excluded from the original CDAI, the modified CDAI (mCDAI) demonstrated a robust negative association with overweight/obesity in adolescents, irrespective of energy adjustment method. These findings suggest that a diet rich in antioxidants may play a protective role in preventing obesity in adolescent aged 12–19 years. Further longitudinal studies are needed to validate these findings and to elucidate the underlying mechanisms.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found at: http://www.cdc.gov/nchs/nhanes.htm.
Ethics statement
The studies involving humans were approved by NCHS Research Ethics Review Committee. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
Author contributions
JC: Writing – original draft, Writing – review & editing. CS: Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by the Natural Science Foundation of China (Grant No. 12001129) and Fuyang Municipal Health Commission Research Grant (Grant No. FYJS2024-003).
Acknowledgments
We thank the National Center for Health Statistics (NCHS) of the Center for Disease Control (CDC) and Prevention, and all participants who enrolled in the NHANES.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. World Health Organization. Obesity and Overweight. Available online at: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight#cms (accessed February 14, 2025).
2. Abarca-Gómez L, Abdeen ZA, Hamid ZA, Abu-Rmeileh NM, Acosta-Cazares B, Acuin C, et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128· 9 million children, adolescents, and adults. Lancet. (2017) 390:2627–42. doi: 10.1016/S0140-6736(17)32129-3
3. Hu K, Staiano AE. Trends in obesity prevalence among children and adolescents aged 2 to 19 years in the US from 2011 to 2020. JAMA Pediatr. (2022) 176:1037–9. doi: 10.1001/jamapediatrics.2022.2052
4. Horesh A, Tsur AM, Bardugo A, Twig G. Adolescent and childhood obesity and excess morbidity and mortality in young adulthood—a systematic review. Curr Obes Rep. (2021) 10:301–10. doi: 10.1007/s13679-021-00439-9
5. Lister NB, Baur LA, Felix JF, Hill AJ, Marcus C, Reinehr T, et al. Child and adolescent obesity. Nat Rev Dis Prim. (2023) 9:24. doi: 10.1038/s41572-023-00435-4
6. Reilly JJ, Kelly J. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: systematic review. Int J Obes. (2011) 35:891–8. doi: 10.1038/ijo.2010.222
7. Bendor CD, Bardugo A, Pinhas-Hamiel O, Afek A, Twig G. Cardiovascular morbidity, diabetes and cancer risk among children and adolescents with severe obesity. Cardiovasc Diabetol. (2020) 19:1–14. doi: 10.1186/s12933-020-01052-1
8. Jakubiak GK, Osadnik K, Lejawa M, Kasperczyk S, Osadnik T, Pawlas N. Oxidative stress in association with metabolic health and obesity in young adults. Oxid Med Cell Longev. (2021) 2021:9987352. doi: 10.1155/2021/9987352
9. Colak E, Pap D. The role of oxidative stress in the development of obesity and obesity-related metabolic disorders. J Med Biochem. (2021) 40:1. doi: 10.5937/jomb0-24652
10. Ahmed B, Sultana R, Greene MW. Adipose tissue and insulin resistance in obese. Biomed Pharmacother. (2021) 137:111315. doi: 10.1016/j.biopha.2021.111315
11. Ham D, Joung H. Understanding the associations between dietary antioxidants and obesity. J Obes Metab Syndr. (2020) 29:163. doi: 10.7570/jomes20070
12. Pérez-Torres I, Castrejón-Téllez V, Soto ME, Rubio-Ruiz ME, Manzano-Pech L, Guarner-Lans V. Oxidative stress, plant natural antioxidants, and obesity. Int J Mol Sci. (2021) 22:1786. doi: 10.3390/ijms22041786
13. Astrup A, Bügel S. Overfed but undernourished: recognizing nutritional inadequacies/deficiencies in patients with overweight or obesity. Int J Obes. (2019) 43:219–32. doi: 10.1038/s41366-018-0143-9
14. Lapik IA, Galchenko AV, Gapparova KM. Micronutrient status in obese patients: a narrative review. Obesity Medicine. (2020) 18:100224. doi: 10.1016/j.obmed.2020.100224
15. Galan P, Viteri F, Bertrais S, Czernichow S, Faure H, Arnaud J, et al. Serum concentrations of β-carotene, vitamins C and E, zinc and selenium are influenced by sex, age, diet, smoking status, alcohol consumption and corpulence in a general French adult population. Eur J Clin Nutr. (2005) 59:1181–90. doi: 10.1038/sj.ejcn.1602230
16. Yang Y, Xu H, Zhang Y, Chen L, Tian C, Huang B, et al. Associations of dietary antioxidant micronutrients with the prevalence of obesity in adults. Front Nutr. (2023) 10:1098761. doi: 10.3389/fnut.2023.1098761
17. Kokkou S, Notara V, Kanellopoulou A, Antonogeorgos G, Rojas-Gil AP, Kornilaki E, et al. The association between the dietary antioxidant index and weight status in primary school students: an epidemiological study. Nutrients. (2024) 16:1667. doi: 10.3390/nu16111667
18. Puchau B, Ochoa MC, Zulet MÁ, Marti A, Martínez JA, Members G. Dietary total antioxidant capacity and obesity in children and adolescents. Int J Food Sci Nutr. (2010) 61:713–21. doi: 10.3109/09637481003757860
19. Azizi-Soleiman F, Khoshhali M, Heidari-Beni M, Qorbani M, Kelishadi R. Association between dietary antioxidant quality score and anthropometric measurements in children and adolescents: the weight disorders survey of the CASPIAN-IV Study. J Trop Pediatr. (2021) 67:fmaa065. doi: 10.1093/tropej/fmaa065
20. Wright ME, Mayne ST, Stolzenberg-Solomon RZ, Li Z, Pietinen P, Taylor PR, et al. Development of a comprehensive dietary antioxidant index and application to lung cancer risk in a cohort of male smokers. Am J Epidemiol. (2004) 160:68–76. doi: 10.1093/aje/kwh173
21. Yu YC, Paragomi P, Wang R, Jin A, Schoen RE, Sheng LT, et al. Composite dietary antioxidant index and the risk of colorectal cancer: findings from the Singapore Chinese Health Study. Int J Cancer. (2022) 150:1599–608. doi: 10.1002/ijc.33925
22. Wang L, Yi Z. Association of the Composite dietary antioxidant index with all-cause and cardiovascular mortality: a prospective cohort study. Front Cardiovasc Med. (2022) 9:993930. doi: 10.3389/fcvm.2022.993930
23. Wu M, Si J, Liu Y, Kang L, Xu B. Association between composite dietary antioxidant index and hypertension: insights from NHANES. Clin Exp Hypertens. (2023) 45:2233712. doi: 10.1080/10641963.2023.2233712
24. Sheng L-T, Jiang Y-W, Pan A, Koh W-P. Dietary total antioxidant capacity and mortality outcomes: the Singapore Chinese Health Study. Eur J Nutr. (2022) 61:2375–82. doi: 10.1007/s00394-022-02812-3
25. Qu Y, Xu W, Guo S, Wu H. Association of sociodemographic and lifestyle factors and dietary intake with overweight and obesity among US children: findings from NHANES. BMC Public Health. (2024) 24:2176. doi: 10.1186/s12889-024-19637-w
26. Willett WC, Howe GR, Kushi LH. Adjustment for total energy intake in epidemiologic studies. Am J Clin Nutr. (1997) 65:1220S−8S. doi: 10.1093/ajcn/65.4.1220S
27. King AC, Powell KE, Kraus WE. The US physical activity guidelines advisory committee report—Introduction. Med Sci Sports Exerc. (2019) 51:1203–5. doi: 10.1249/MSS.0000000000001946
28. Dietary Reference Intakes. The Essential Guide to Nutrient Requirements. Available online at: https://www.nationalacademies.org/our-work/summary-report-of-the-dietary-reference-intakes (accessed February 14, 2025).
29. Nijhawan P, Arora S, Behl T. Intricate role of oxidative stress in the progression of obesity. Obes Med. (2019) 15:100125. doi: 10.1016/j.obmed.2019.100125
30. Almoraie NM, Shatwan IM. The potential effects of dietary antioxidants in obesity: a comprehensive review of the literature. Healthcare. (2024) 2024:416. doi: 10.3390/healthcare12040416
31. Aeberli I, Molinari L, Spinas G, Lehmann R. l'Allemand D, Zimmermann MB. Dietary intakes of fat and antioxidant vitamins are predictors of subclinical inflammation in overweight Swiss children. Am J Clin Nutr. (2006) 84:748–55. doi: 10.1093/ajcn/84.4.748
32. Suriyaprom K, Kaewprasert S, Putpadungwipon P, Namjuntra P, Klongthalay S. Association of antioxidant status and inflammatory markers with metabolic syndrome in Thais. J Health, Popul Nutr. (2019) 38:1–7. doi: 10.1186/s41043-018-0158-9
33. Yao N, Yan S, Guo Y, Wang H, Li X, Wang L, et al. The association between carotenoids and subjects with overweight or obesity: a systematic review and meta-analysis. Food Funct. (2021) 12:4768–82. doi: 10.1039/D1FO00004G
34. Hawkes WC, Keim NL. Dietary selenium intake modulates thyroid hormone and energy metabolism in men. J Nutr. (2003) 133:3443–8. doi: 10.1093/jn/133.11.3443
35. Liu X, Shen H, Chen M, Shao J. Clinical relevance of selenium with liver stiffness and steatosis detected by transient elastography in adults. Biol Trace Elem Res. (2022) 200:3041–9. doi: 10.1007/s12011-021-02912-x
36. Aminnejad B, Roumi Z, Hasanpour Ardekanizadeh N, Vahid F, Gholamalizadeh M, Kalantari N, et al. Association of dietary antioxidant index with body mass index in adolescents. Obes Sci Pract. (2023) 9:15–22. doi: 10.1002/osp4.639
37. Romieu I, Dossus L, Barquera S, Blottière HM, Franks PW, Gunter M, et al. Energy balance and obesity: what are the main drivers? Cancer Causes Control. (2017) 28:247–58. doi: 10.1007/s10552-017-0869-z
38. Willett W, Stampfer MJ. Total energy intake: implications for epidemiologic analyses. Am J Epidemiol. (1986) 124:17–27. doi: 10.1093/oxfordjournals.aje.a114366
39. Tomova GD, Arnold KF, Gilthorpe MS, Tennant PW. Adjustment for energy intake in nutritional research: a causal inference perspective. Am J Clin Nutr. (2022) 115:189–98. doi: 10.1093/ajcn/nqab266
40. McCullough LE, Byrd DA. Total energy intake: implications for epidemiologic analyses. Am J Epidemiol. (2023) 192:1801–5. doi: 10.1093/aje/kwac071
41. Vossenaar M, Solomons NW, Muslimatun S, Faber M, García OP, Monterrosa E, et al. Nutrient density as a dimension of dietary quality: findings of the nutrient density approach in a multi-center evaluation. Nutrients. (2021) 13:4016. doi: 10.3390/nu13114016
Keywords: composite dietary antioxidant index, obesity, children and adolescents, antioxidant intake, NHANES
Citation: Chen J and Shi C (2025) Association between dietary antioxidant intake and overweight/obesity risk among children and adolescents: a cross-sectional analysis from NHANES 2011–2016. Front. Nutr. 12:1540303. doi: 10.3389/fnut.2025.1540303
Received: 05 December 2024; Accepted: 14 April 2025;
Published: 06 May 2025.
Edited by:
Mauro Serafini, University of Teramo, ItalyReviewed by:
Szymon Skoczen, Jagiellonian University Medical College, PolandGianvincenzo Zuccotti, University of Milan, Italy
Copyright © 2025 Chen and Shi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Changhong Shi, YXNoaV8yNDhAMTYzLmNvbQ==