 Weirui Ren
Weirui Ren Chuang Zhang2
Chuang Zhang2- 1Department of Gastroenterology, Hebei Medical University Third Hospital, Shijiazhuang, China
- 2Department of Clinical Medicine, Shijiazhuang Medical College, Shijiazhuang, China
- 3Department of Gastroenterology, The Second Hospital of Hebei Medical University, Shijiazhuang, China
- 4Department of Graduate College, Hebei Medical University, Shijiazhuang, China
Background: Carotenoids, known for their antioxidant properties and potential health benefits, have attracted considerable attention. Nonetheless, the association between carotenoid levels and gallstone prevalence has not been adequately explored. This study aimed to investigate the association between serum carotenoid levels and gallstone risk in an adult population.
Methods: This cross-sectional study utilized the 2017–2018 NHANES data. Multivariate logistic regression analyses were performed to assess the association between serum carotenoid levels and gallstone prevalence. Subgroup and interaction analyses were conducted to confirm these findings. Additionally, generalized additive model (GAM) regression combined with smooth curve fitting techniques was utilized to clarify potential non-linear associations, and a mediation analysis was conducted to identify possible mediators in the association between serum carotenoid levels and gallstones.
Results: This study included 3,809 participants aged ≥20 years, among whom 412 had gallstones. After adjusting for confounders (Model 3), serum carotenoid levels were inversely associated with gallstone prevalence. The participants in the highest quartile of total carotenoid levels had a 48% lower gallstone risk than those in the lowest quartile (Q4: odds ratio [OR] = 0.52, p = 0.0005). Individual carotenoids showed similar trends: α-carotene (49% lower risk, OR = 0.51, p = 0.0010), α-cryptoxanthin (54% lower risk, Q4: OR = 0.46, p < 0.0001), β-carotene (47% lower risk, Q4: OR = 0.53, p = 0.0010), β-cryptoxanthin (42% lower risk, Q4: OR = 0.58, p = 0.0061), lutein/zeaxanthin (44% lower risk, Q4: OR = 0.56, p = 0.0025), and lycopene (30% lower risk, Q4: OR = 0.70, p = 0.0441). GAM analysis detected non-linear associations between carotenoids and gallstone risk. The subgroup and interaction analyses confirmed these results. Mediation analysis revealed that body mass index (BMI) accounted for 16.7% of the total effect.
Conclusion: Observational data demonstrated inverse associations between serum carotenoid levels and gallstone prevalence, with BMI mediating 16.7% of the total effect. These findings suggest that maintaining high serum carotenoid levels may reduce the gallstone risk. Future studies should explore the protective mechanisms of carotenoids and validate their causal relationships using longitudinal studies.
1 Introduction
Gallstones, a common digestive disease worldwide, affect approximately 10–20% of the adult population, imposing a heavy medical and economic burden globally (1, 2). Regional variations in prevalence exist, with rates of 10–15% in the United States, 9–21% in Europe, and 10% in Asian populations, all showing a global upward trend (3, 4). Gallstone formation is associated with various genetic and environmental factors including race, sex, age, family history, obesity, diet, lifestyle, and medication (5, 6). Although most gallstone patients remain asymptomatic throughout their lives, approximately 10% eventually develop clinical manifestations such as significant abdominal discomfort and digestive dysfunction (7). Additionally, 1–2% of gallstone patients develop complications, such as cholecystitis, acute suppurative cholangitis, and pancreatitis, which seriously affect their health and quality of life (5, 8, 9). Furthermore, gallstone disease is associated with an increased risk of hepatobiliary and pancreatic malignancies and is an independent risk factor for gallbladder cancer-related mortality (10, 11). Given its status as a major global public health challenge and its potential serious consequences, further exploration of the underlying causes of gallstones and preventive measures are crucial to reduce the global public health burden associated with this disease.
Gallstone development is a complex, multifactorial phenomenon in which oxidative stress and inflammatory processes play important role (12). Studies have shown that the occurrence of gallstones is associated with elevated oxidative stress levels and decreased antioxidant capacity, and the levels of oxidative stress markers (such as malondialdehyde and superoxide dismutase) in patients with gallstones (13, 14). Oxidative stress damages the gallbladder mucosal epithelial cells and triggers lipid peroxidation by generating reactive oxygen species, thereby instigating inflammatory cascades. Activation of inflammatory mediators stimulates macrophages, resulting in the release of pro-inflammatory substances and the establishment of a chronic inflammatory milieu (15–17). This interaction leads to bile cholesterol supersaturation and irregular bilirubin metabolism, ultimately promoting gallstone formation of gallstones (18, 19).
Carotenoids, which are prevalent natural antioxidants, encompass a range of compounds including α-carotene, α-cryptoxanthin, β-carotene, β-cryptoxanthin, lutein/zeaxanthin, and lycopene, collectively representing over 95% of carotenoids found in human serum (20). These serum carotenoids have significant biological functions and exhibit antioxidant, anti-inflammatory, and anticancer properties that are essential for mitigating various health concerns, particularly cardiovascular diseases, metabolic syndromes, and other chronic disorders (21–23). Under normal circumstances, there is a good correlation between the dietary intake of certain fruits and vegetables and the concentration of carotenoids in the blood. However, compared to the intake of dietary carotenoids, serum carotenoids show a stronger and more linear negative correlation with the occurrence of diseases (24). Given their bioactive potential, carotenoids may contribute to gallstone prevention by alleviating oxidative stress and inflammation. However, the association between serum carotenoid levels and gallstone prevalence in large adult cohorts remains inadequately explored. This study aimed to analyze National Health and Nutrition Examination Survey (NHANES) data to examine the association between serum carotenoid levels and gallstone risk among adults in the United States. We hypothesized that higher serum carotenoid levels would correlate with lower gallstone risk. To test this, we used multiple methods including multivariate logistic regression, generalized additive model (GAM), and mediation analysis. Our findings are expected to offer new insights and strategies for gallstone prevention and intervention, supporting clinical and public health decision-making.
2 Materials and methods
2.1 Data sources and study population
This study used data derived from the NHANES. Administered by the National Center for Health Statistics (NCHS), the NHANES uses a stratified multistage sampling framework to evaluate the nutritional and health profiles of adults and children across the United States (25). The research methodology was approved by the NCHS Institutional Review Board, and all participants provided written informed consent prior to their participation. Given that the data utilized in this study originated exclusively from the NHANES public database, individual patient identifiers were substituted with identification codes, thereby eliminating the need for ethical approval from the authors’ affiliated institutions (26). The dataset for this study was collected during the 2017–2018 NHANES cycle and presented extensive data on serum carotenoid levels and gallstone prevalence. Initially, the study included 9,254 participants. The exclusion criteria were as follows: (1) individuals younger than 20 years (n = 3,685), (2) participants lacking gallstone data (n = 9), and (3) participants with missing carotenoid data (n = 1,751). Following the application of these exclusion criteria, the final dataset comprised 3,809 participants, including 412 individuals diagnosed with gallstones and 3,397 individuals without gallstones (Figure 1).
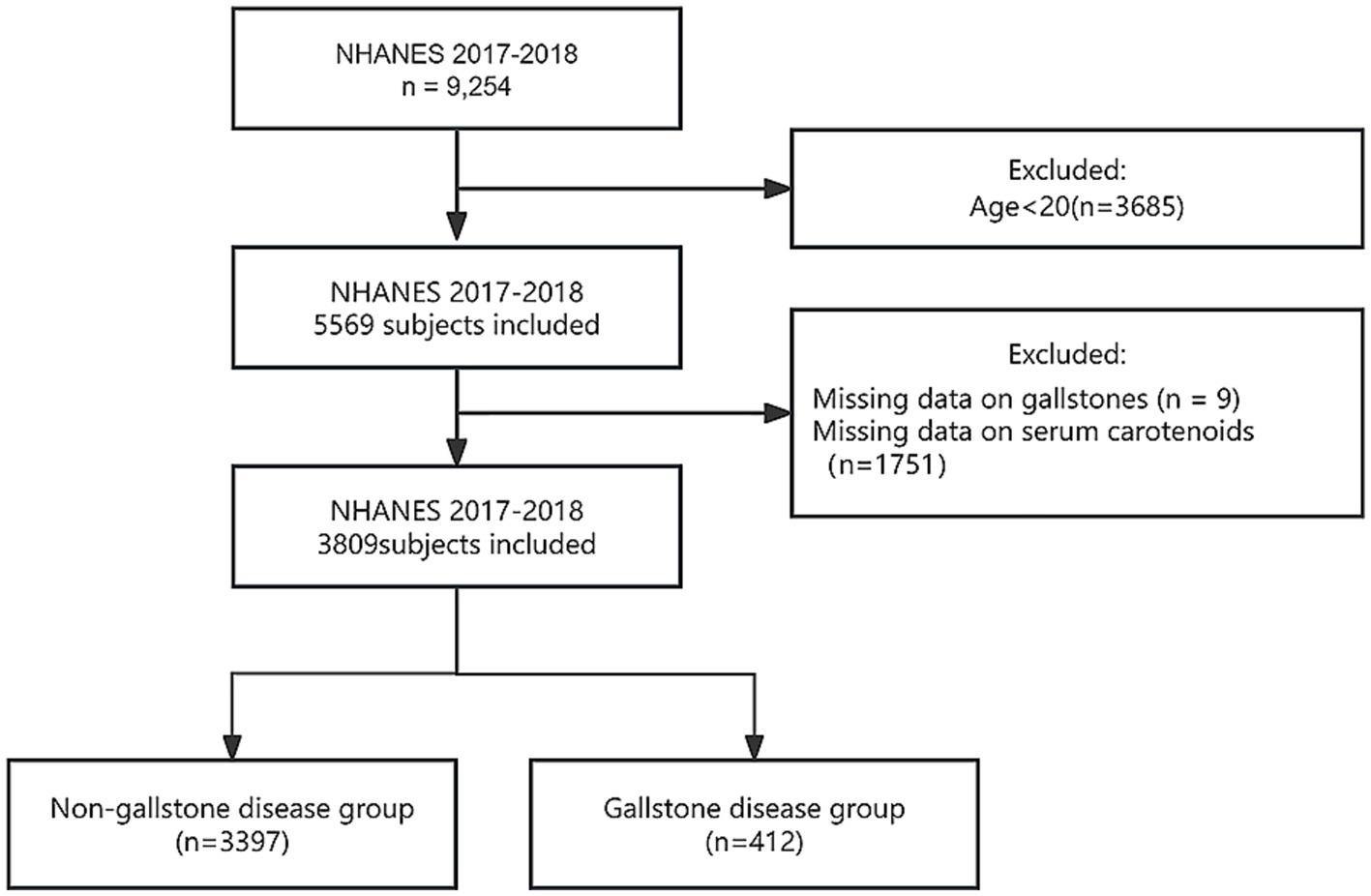
Figure 1. Flowchart of participant screening.
2.2 Serum carotenoids measurement
This study focuses on essential serum carotenoids, which encompass α-carotene, α-cryptoxanthin, β-carotene, β-cryptoxanthin, lutein/zeaxanthin, and lycopene. The serum concentration of β-carotene is derived by aggregating the amounts of trans-β-carotene and cis-β-carotene. The total serum carotenoid (TSC) level was determined by summing the levels of six primary carotenoids. The NHANES database utilizes photodiode array detection (PDAD) to quantify the serum levels of these carotenoids (27). To ensure precision of the measurements, the research team formulated comprehensive laboratory procedures and quality control measures documented in the NHANES Laboratory/Medical Technologists Procedures Manual (28).
2.3 Definition of gallstones
Gallstones were identified as the outcome variables in the context of this study. We assessed patients with gallstones through self-reported interviews using the Medical Condition Questionnaire (MCQ) from the NHANES (2017–2018) dataset. Participants were asked the question, “Has a doctor or other health professional ever informed you that you have gallstones?” Those responding “yes” were categorized as having gallstones, whereas those denying this diagnosis were classified as not having gallstones.
2.4 Assessment of covariates
To improve the precision and thoroughness of the analysis examining the association between serum carotenoid levels and gallstones in adults, the research team recognized several covariates based on clinical expertise and prior studies (29–31). The significant covariates included demographic factors, comorbid conditions, and other pertinent variables, as outlined in Table 1. In the analysis, the poverty income ratio (PIR) was stratified into three categories: <1.3, 1.3–3.5, and >3.5. Recorded comorbidities included hypertension, diabetes, coronary heart disease (CHD), thyroid disorders, stroke, and cancer or malignancy. Hypertension is defined by satisfying at least one of the following criteria: (i) average systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg, measured three times on the same day; (ii) current utilization of antihypertensive medication; (iii) self-reported hypertension through the questionnaire. Diabetes is similarly characterized by meeting one of these criteria: (i) hemoglobin A1c (HbA1c) level ≥6.5%; (ii) fasting blood glucose (FBG) level ≥126 mg/dL; (iii) self-reported diabetes diagnosis or current use of insulin or antidiabetic medications. Definitions of CHD and other related complications were based on responses to the medical history questionnaire. Smoking history was defined as having smoked a minimum of 100 cigarettes over a lifetime. Participants who consumed at least 12 alcoholic beverages per year were classified as alcohol drinkers.
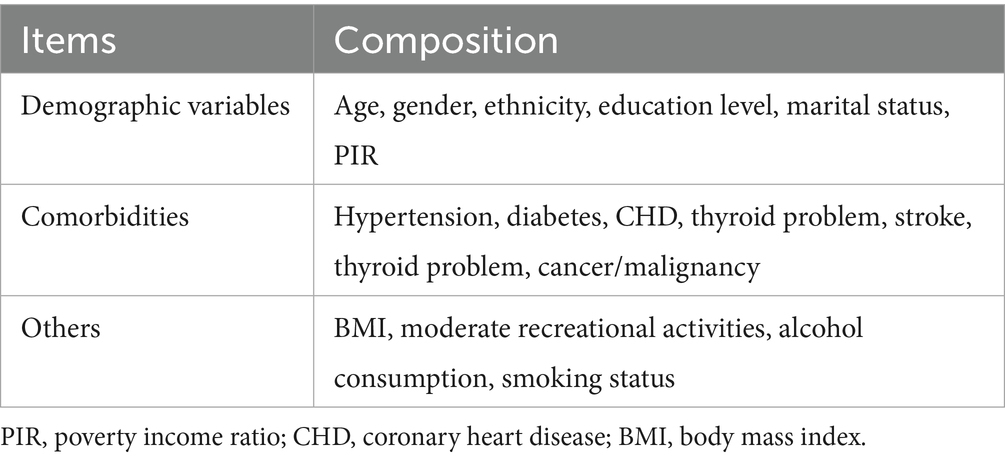
Table 1. Covariates extracted from the 2017–2018 NHANES.
2.5 Statistical analysis
The statistical evaluation conducted in this study adhered to the guidelines set forth by the NHANES and incorporated appropriate sampling weights. Categorical variables were represented as unweighted frequencies and weighted percentages, whereas continuous variables were characterized by weighted medians and interquartile ranges because of their non-normal distribution. Chi-square and Mann–Whitney U tests were used to compare categorical and continuous variables. To examine the association between serum carotenoid levels and the presence of gallstones, carotenoid levels were stratified into quartiles, with the lowest quartile serving as the reference group. Three distinct logistic regression models were developed: Model 1 was unadjusted; Model 2 was controlled for variables such as age, sex, ethnicity, marital status, educational level, and PIR; and Model 3 was additionally adjusted for the covariates included in Model 2, as well as for body mass index (BMI), smoking, alcohol consumption, physical activity, diabetes, hypertension, CHD, stroke, thyroid disorders, and cancer/malignancy. We computed p-values for trends to determine whether the odds ratio (OR) for gallstones fluctuated with ascending carotenoid quartiles. Moreover, GAM regression combined with smooth curve fitting was utilized to assess potential non-linear associations, with effective degrees of freedom (EDF) serving as an indicator of curvature. An EDF value of 1 reflects a linear association, whereas values exceeding 1 indicate a more intricate association. Spearman’s correlation coefficients were calculated to evaluate the associations between serum carotenoids, and weighted quantile sum (WQS) regression was applied to investigate the cumulative effects of the six carotenoids on gallstone occurrence. Further analyses involving subgroups and interaction tests were performed to discern consistency across various subpopulations and to scrutinize the influences and interactions of covariates, such as age, sex, ethnicity, educational level, PIR, BMI, diabetes, and CHD. Potential mediators that might influence the association between serum carotenoids and gallstones were also explored, including liver function markers (alanine aminotransferase [ALT], aspartate aminotransferase [AST], gamma-glutamyl transferase [GGT], total bilirubin), uric acid, inflammatory markers (C-reactive protein [CRP], neutrophil count, ferritin), obesity metrics (BMI), lipid profiles (triglycerides, total cholesterol), along with diabetes and insulin resistance indicators (HbA1c, FBG, fasting serum insulin). All statistical analyses were performed using R software version 4.3.21 and EmpowerStats software version 4.22. Statistical significance was set at p < 0.05.
3 Results
3.1 Baseline characteristics of study participants
Table 2 provides a comprehensive overview of participants’ baseline characteristics. A total of 3,809 individuals were analyzed, of which 412 (10.8%) were diagnosed with gallstones. In comparison to those without gallstones, individuals with gallstones were significantly older (mean age of 59.00 years versus 47.00 years, p < 0.0001) and exhibited a greater proportion of females (74.76% compared to 49.29%, p < 0.0010). Examination of the racial distribution within the gallstone cohort revealed that 7.89% were Hispanic Americans, 70.31% were non-Hispanic White, 6.92% were non-Hispanic Black, and 14.88% were from other racial backgrounds (p = 0.0488). Patients with gallstones displayed markedly elevated rates of hypertension (60.12% vs. 37.57%, p < 0.0001), diabetes (27.23% vs. 14.94%, p = 0.0001), CHD (8.44% vs. 3.86%, p = 0.0023), thyroid disorders (23.27% vs. 10.90%, p < 0.0010), and stroke (6.92% vs. 3.04%, p = 0.0010) compared to their counterparts without gallstones. Additionally, the prevalence of malignancies was significantly higher among patients with gallstones (18.35%, 79/412) than among those without gallstones (9.82%, 310/3,397, p < 0.0010). With respect to BMI, patients with gallstones had a significantly higher proportion (56.45%) with BMI > 30 kg/m2 than patients without gallstones (39.48%) (p < 0.0001). Biochemical markers indicated that patients with gallstones had significantly elevated FBG level (6.05 vs. 5.66, p = 0.0166), triglyceride level (1.25 vs. 1.02, p = 0.0654), white blood cell count (7.70 vs. 7.00, p = 0.0055), and neutrophil count (4.50 vs. 4.10, p = 0.0009). Moreover, serum carotenoid levels were significantly lower in individuals with gallstones than in those without (p < 0.05). No significant disparities were noted between gallstone and non-gallstone patients regarding education levels, smoking habits, alcohol consumption, moderate leisure activities, PIR, and total bilirubin, total cholesterol, ferritin, ALT, AST, GGT, lactate dehydrogenase, TB, and uric acid levels (p > 0.05).
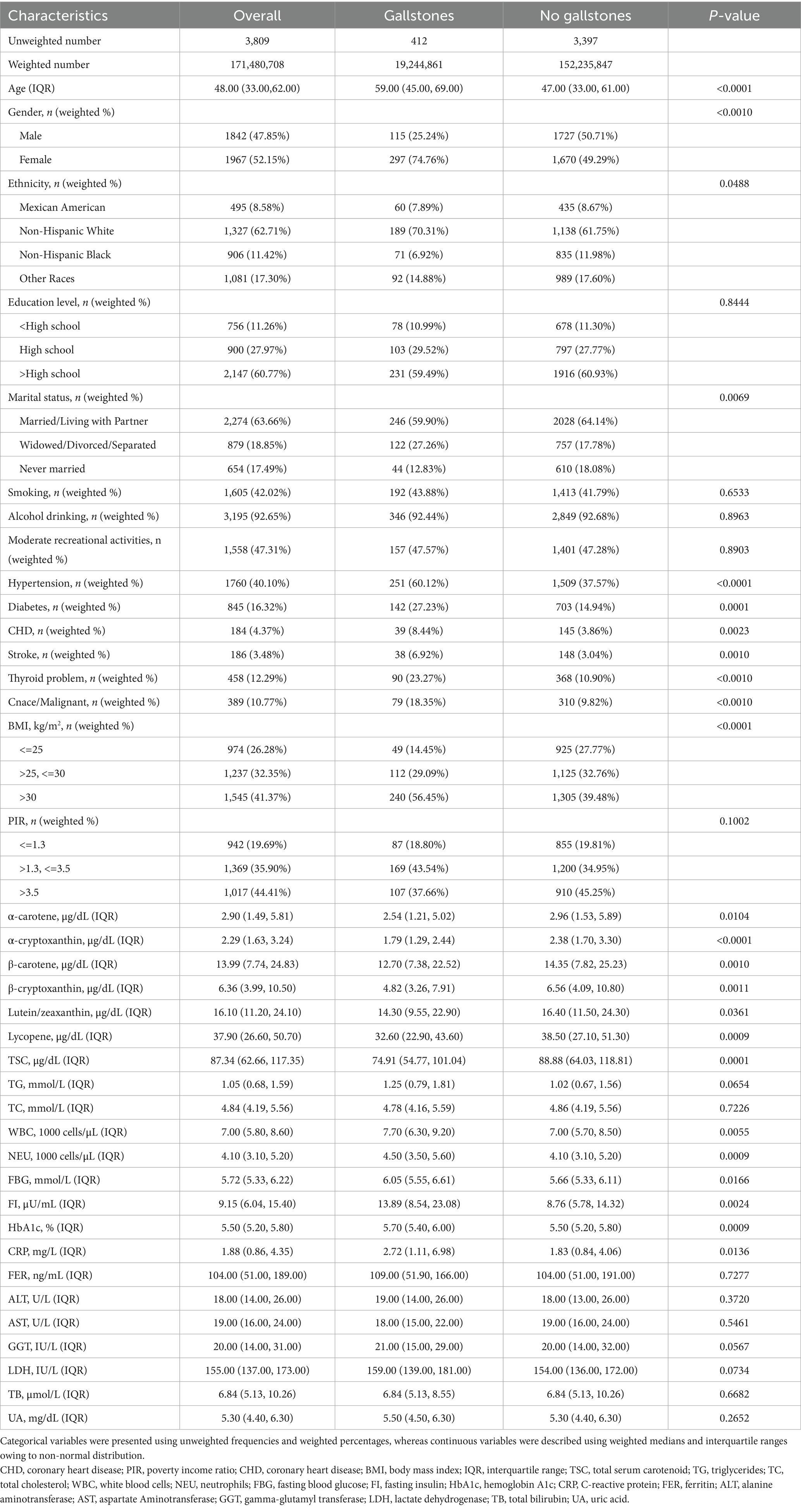
Table 2. Baseline characteristics of the participants.
3.2 The association between serum carotenoids and gallstones in adults
Table 3 summarizes the results of the association analysis between serum carotenoid levels and gallstone prevalence. After adjusting for confounding variables in Model 3, a significant negative correlation was identified between serum carotenoid levels and gallstone prevalence. Specifically, total carotenoid levels were negatively associated with gallstone prevalence, with ORs of 0.51 (p = 0.0002) for Q3 and 0.52 (p = 0.0005) for Q4, indicating a 48% reduction in gallstone prevalence among individuals in the highest quartile. For α-carotene, the OR values were 0.72 (p = 0.0446) for Q2, 0.54 (p = 0.0008) for Q3, and 0.51 (p = 0.0010) for Q4, demonstrating a negative correlation with gallstone prevalence. For α-cryptoxanthin, the OR values were 0.61 (p = 0.0015) for Q2, 0.44 (p < 0.0001) for Q3, and 0.46 (p < 0.0001), also showing a negative correlation with gallstone prevalence. Similarly, β-carotene exhibited OR values of 0.71 (p = 0.0365) for Q2, 0.46 (p < 0.0001) for Q3, and 0.53 (p = 0.0010) for Q4, further confirming this negative association. Additionally, β-cryptoxanthin displayed negative correlations, with OR values of 0.70 (p = 0.0290) for Q2, 0.65 (p = 0.0174) for Q3, and 0.58 (p = 0.0061) for Q4. Lutein/zeaxanthin also showed a significant negative correlation with Q3 (OR = 0.64, p = 0.0119) and Q4 (OR = 0.56, p = 0.0025). Furthermore, Lycopene levels were negatively correlated with gallstone prevalence in Q3 (OR = 0.53, p = 0.0005) and Q4 (OR = 0.70, p = 0.0441). Trend tests further supported the existence of a significant negative correlation between serum carotenoid levels and gallstone prevalence.
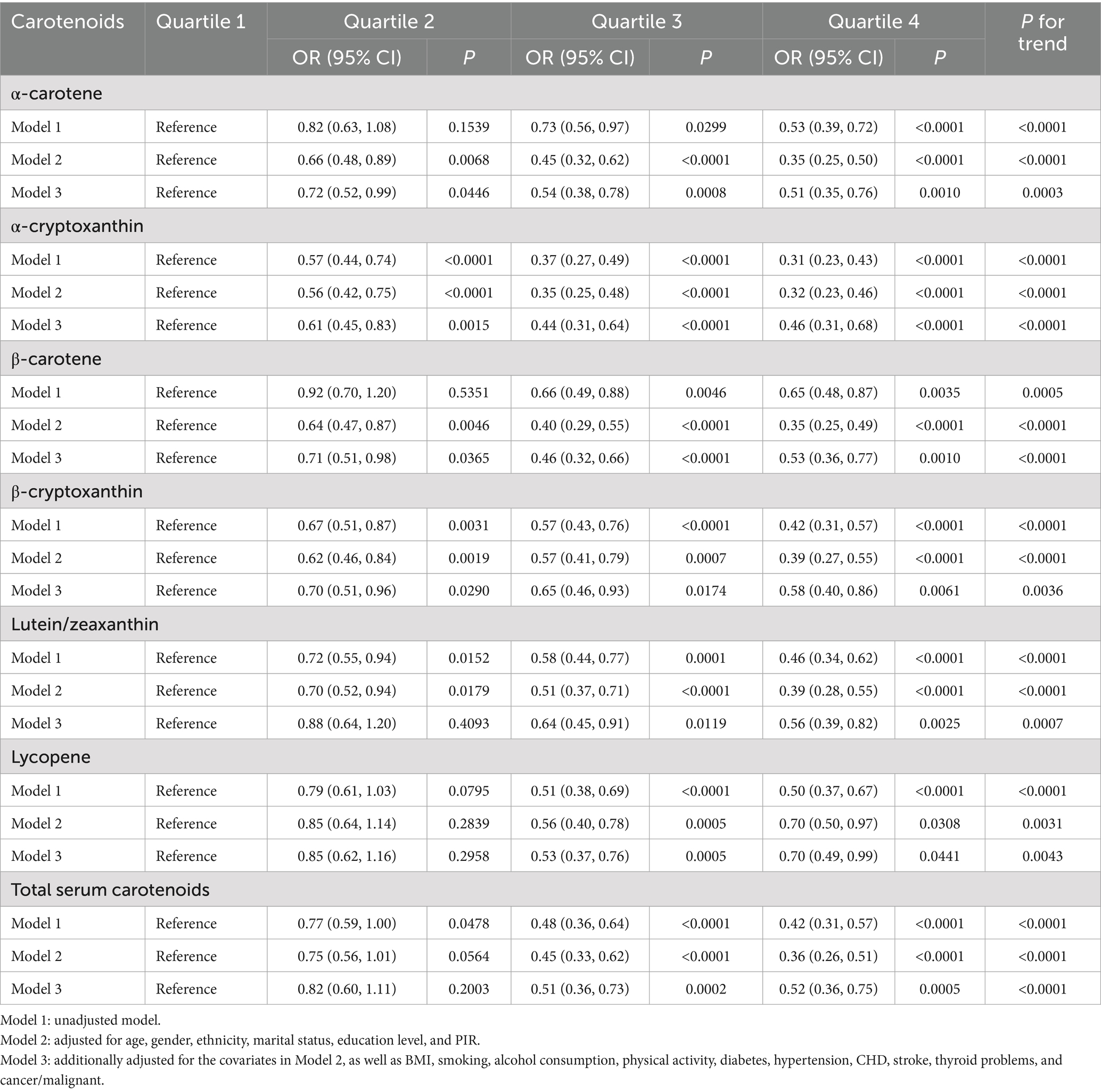
Table 3. Multivariate-adjusted association between serum carotenoid quartiles and gallstone prevalence.
Subsequently, GAM regression combined with smooth curve fitting techniques were used to comprehensively explore the potential association between serum carotenoid levels and gallstones in adults (Figure 2). The results indicate a complex non-linear negative association between these carotenoids and gallstones in adults, with increased carotenoid levels potentially associated with a statistically significant reduction in gallstone prevalence.
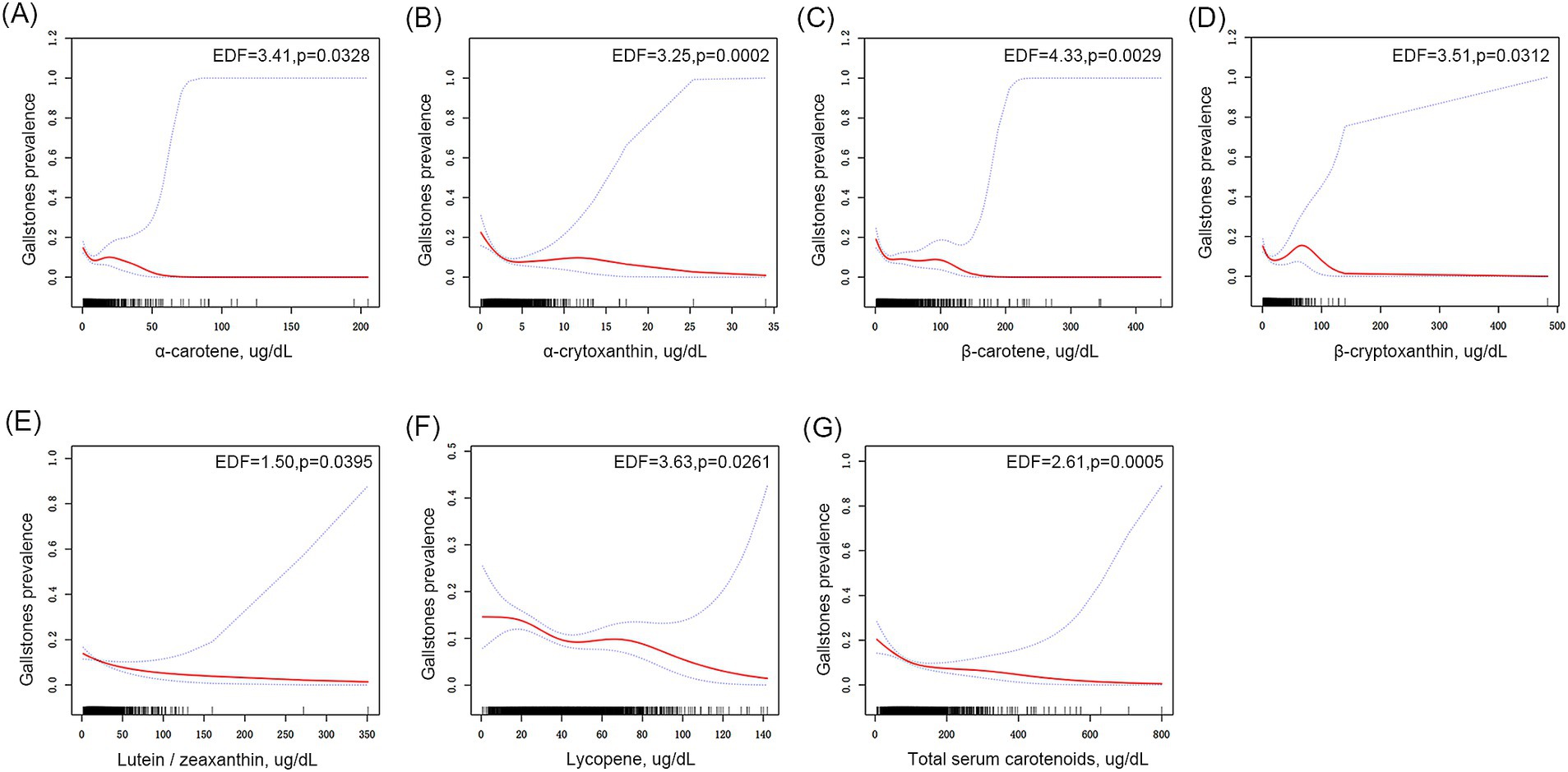
Figure 2. Association between serum carotenoid levels and gallstones in adults. (A) α-Carotene, (B) α-cryptoxanthin, (C) β-carotene, (D) β-cryptoxanthin, (E) lutein/zeaxanthin, (F) lycopene, and (G) total carotenoids in relation to gallstone prevalence. The area between the upper and lower dashed lines represents 95% confidence intervals (CI).
3.3 Associations between the combine of six serum carotenoids and gallstones in adults
The pairwise Spearman correlation coefficients among the six serum carotenoids ranged from 0.25 to 0.80, reflecting varying degrees of inter-correlation (Figure 3A). Weighted quantile sum (WQS) regression analysis indicated that lycopene made the most substantial contribution to the association with gallstones, accounting for 37.86%, followed by β-carotene at 22.57% and lutein/zeaxanthin at 20.8% (Figure 3B). These results suggest a robust association between the levels of the three serum carotenoids and reduced gallstone prevalence.
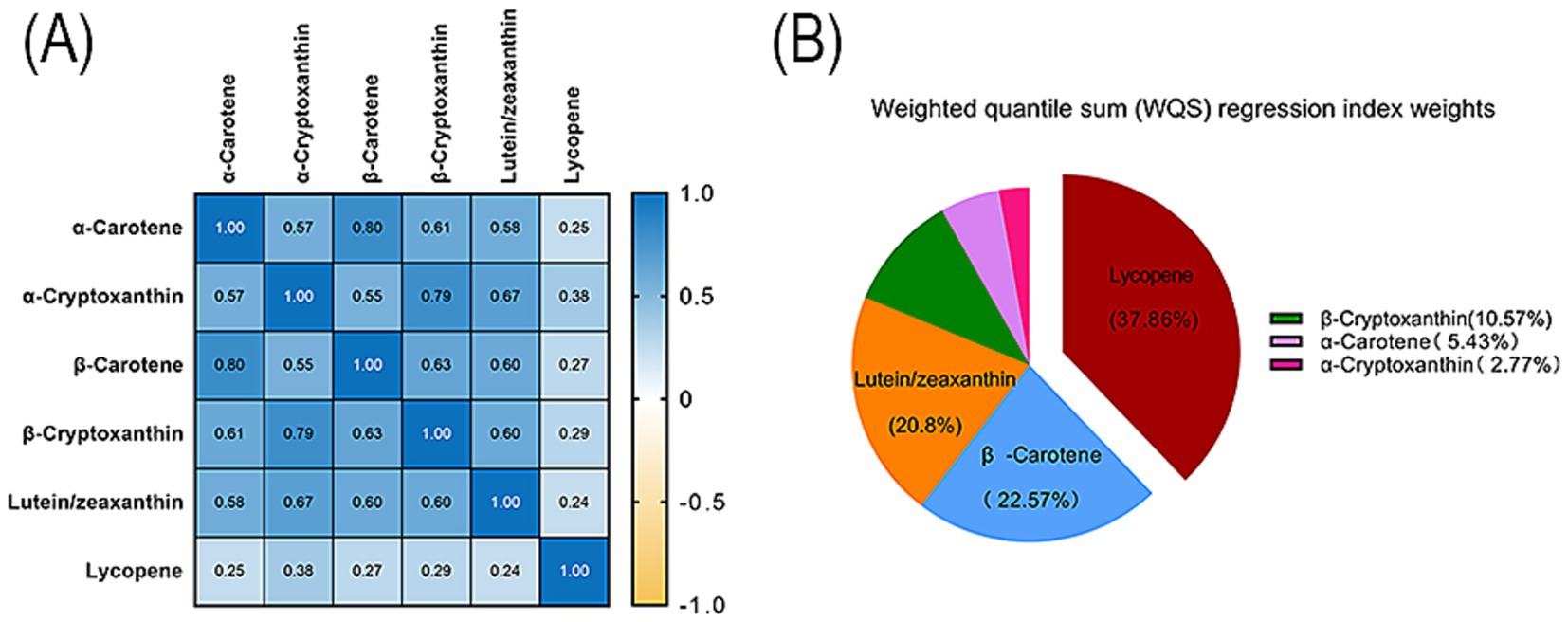
Figure 3. Association between the combination of the six serum carotenoids and gallstones in adults. (A) Pairwise Spearman correlation coefficients for serum carotenoids. (B) The WQS regression index weights for each carotenoid in adults with gallstones. The WQS regression was adjusted for age, sex, ethnicity, marital status, education level, PIR, BMI, smoking, alcohol consumption, physical activity, diabetes, hypertension, coronary heart disease, stroke, thyroid problems, and cancer/malignancy.
3.4 Subgroup analysis and mediation analysis
This study selected the TSC level for subgroup and mediation analyses. Given the correlation between carotenoids, the use of the TSC level simplified the analytical process, allowing for a clearer identification of its association with gallstone prevalence. The results showed that, as shown in Table 4, there was a general negative association between the TSC level and gallstone prevalence. However, this correlation was not statistically significant in any subgroup. Specifically, among participants younger than 40 years, those with high school education or less, and individuals with a PIR of 1.3 or lower, the link between carotenoid levels and gallstone prevalence was not statistically significant. In contrast, within the subgroup of participants aged over 40 years, especially among those between 41 and 60 years and those over 61 years, a significant association was observed, wherein increased carotenoid levels were correlated with a reduced gallstone prevalence. Sex-specific analysis revealed that women in the third and fourth quartiles experienced a statistically significant decrease in gallstone prevalence (p < 0.05), whereas men demonstrated a notable reduction in gallstone prevalence in quartile three (p = 0.0134) and a nearly significant reduction in quartile four (p = 0.0547). Additionally, variables such as marital status, educational attainment, ethnicity, BMI, hypertension, and diabetes exhibited comparable trends in the specific subgroups. Overall, a consistent association emerged wherein increased serum carotenoid levels were associated with a lower gallstone prevalence across the majority of subgroups, with the exception of those participants younger than 40, possessing a high school education or lower, and having a PIR of 1.3 or less, where this association was less evident. The interaction analysis did not reveal any significant interactions (p > 0.05), indicating that the association between carotenoid levels and gallstone prevalence remained relatively stable across various subgroups.
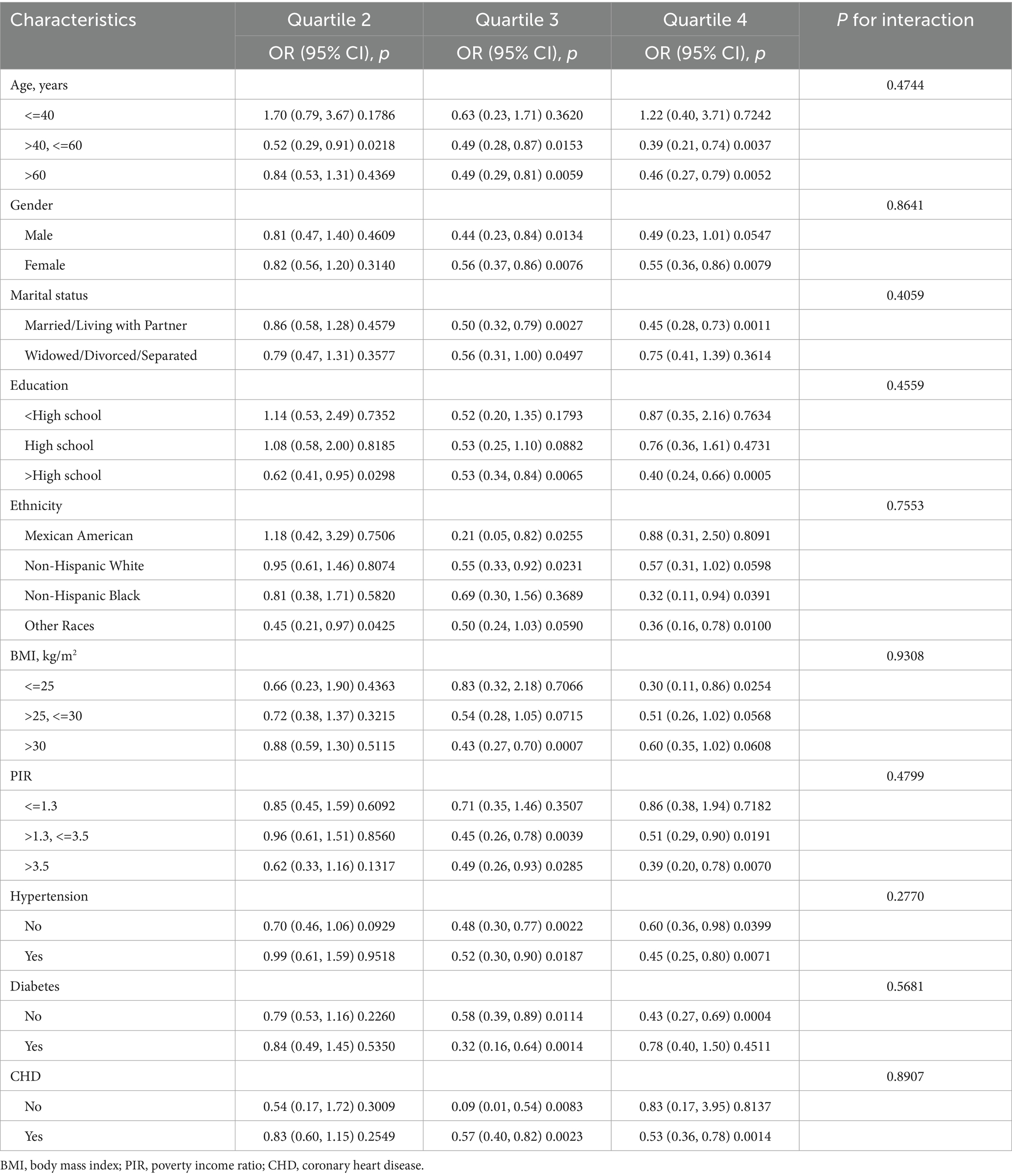
Table 4. Subgroup analysis of the association between total serum carotenoid level and gallstones.
Mediation analysis was performed to assess the influence of different mediating variables on the association between the TSC level and gallstone prevalence. The models and pathways used for the mediation analysis are depicted in Figure 4. After controlling for potential confounding variables, the findings revealed that although the indirect effects of most indicators were not significant, the indirect effects related to neutrophil count (−0.001, p = 0.0100), CRP (−0.001, p = 0.0020), and GGT (−0.001, p = 0.0600) were statistically significant. Furthermore, the total effect of BMI was calculated at −0.029, with an indirect effect of −0.005 and a direct effect of −0.024, yielding a mediation proportion of 16.7%. This result highlights the potential impact of BMI on this association; although the mediation proportion of 16.7% is not particularly high, it is considered significant in this study. In summary, carotenoids may indirectly mitigate the gallstone risk by affecting variables such as obesity and inflammation while potentially providing a direct protective effect. Table 5 summarizes the mediation analysis results, encompassing direct effects, indirect effects, total effects, and mediation ratios.
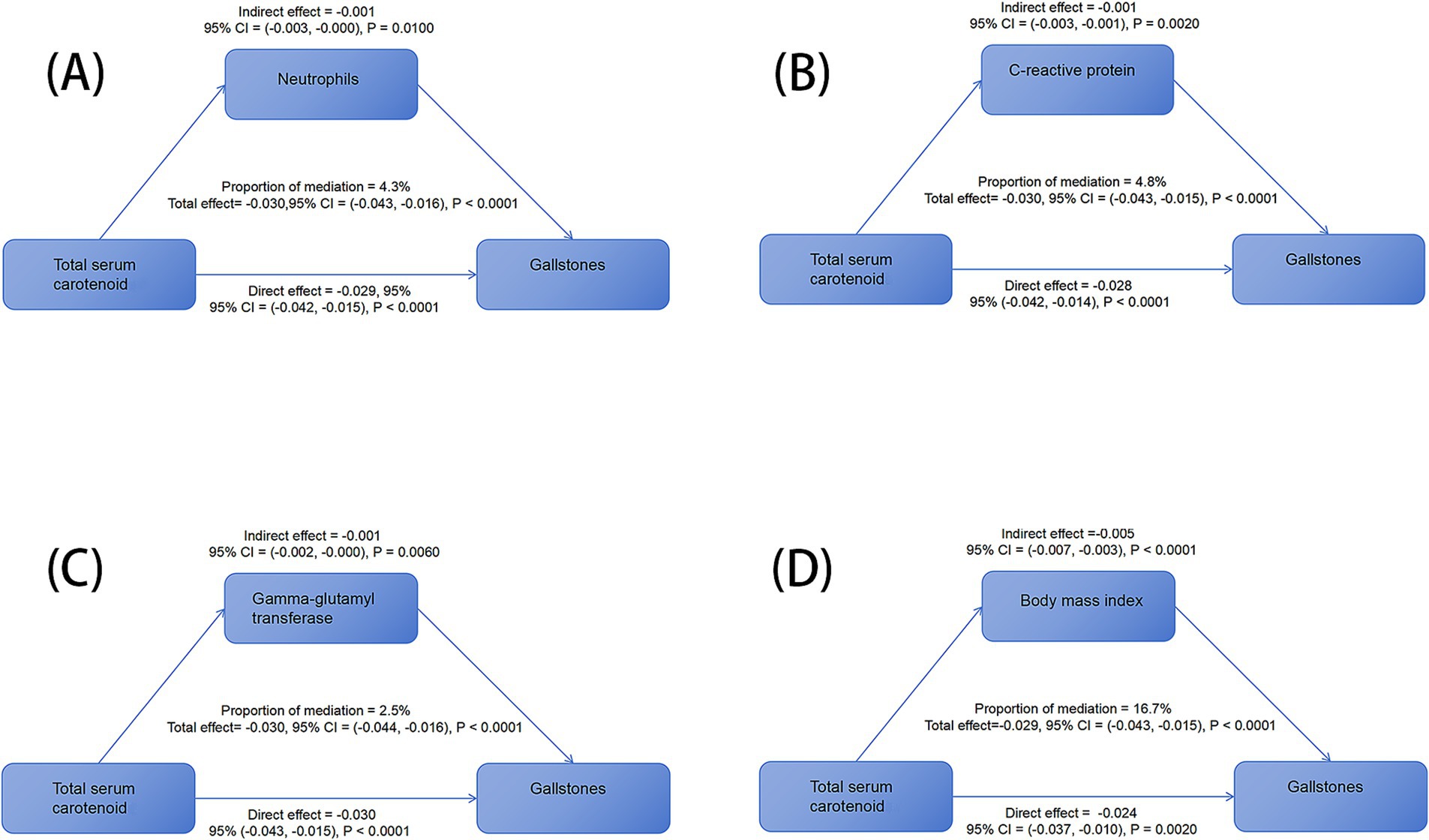
Figure 4. Different mediating variables on the association between total serum carotenoid level and gallstone prevalence. (A) Neutrophil count, (B) C-reactive protein, (C) gamma-glutamyl transferase, and (D) BMI in mediation analysis of the association between total serum carotenoid level and gallstone prevalence.
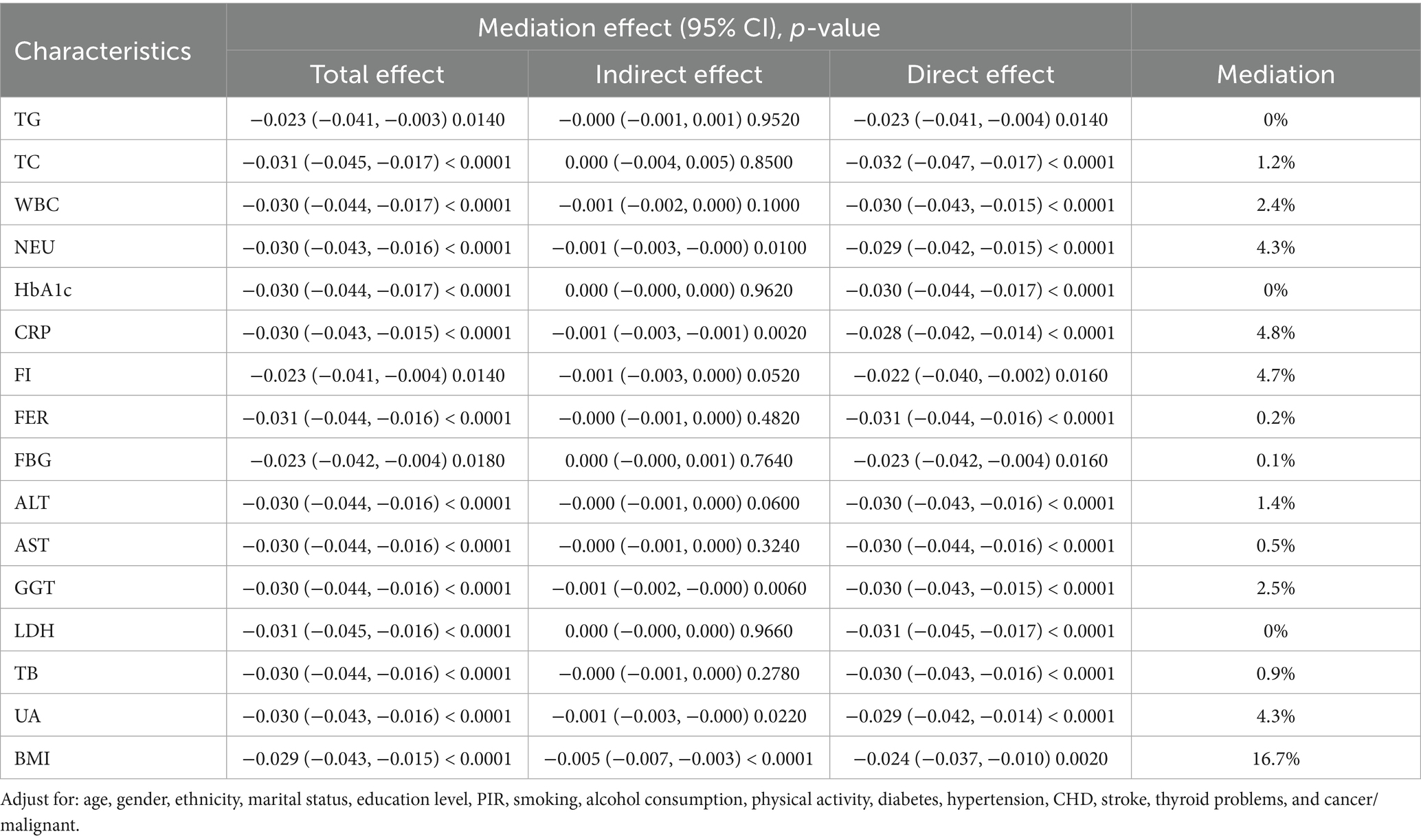
Table 5. Mediation analysis of liver function, uric acid, inflammatory markers, obesity, blood lipids, diabetes, and insulin resistance in the association between total serum carotenoid level and gallstones.
4 Discussion
This study used data from the 2017–2018 National Health and Nutrition Examination Survey (NHANES) to investigate the association between serum carotenoid levels and the occurrence of gallstones in adult populations. These findings revealed a significant inverse association between serum carotenoid levels and the likelihood of gallstone development. Individuals in the highest quartile of total carotenoid levels exhibited a 48% lower risk of gallstone formation than those in the lowest quartile. Similar trends are observed for specific carotenoids: α-carotene is associated with a 49% decrease in risk (Q4: OR = 0.51, p = 0.0010), α-cryptoxanthin with a 54% decrease (Q4: OR = 0.46, p < 0.0001), β-carotene with a 47% reduction (Q4: OR = 0.53, p = 0.0010), β-cryptoxanthin with a 42% reduction (Q4: OR = 0.58, p = 0.0061), lutein/zeaxanthin with a 44% reduction (Q4: OR = 0.56, p = 0.0025), and lycopene with a 30% reduction (Q4: OR = 0.70, p = 0.0441). These results imply that elevated serum carotenoid levels may confer protective effects against gallstone development.
Serum carotenoid levels not only reflect an individual’s dietary habits but are also associated with various health conditions. Research has found an inverse correlation between serum carotenoid concentrations and the risk of several chronic diseases, including mortality rates in patients with metabolic syndrome, endometriosis, osteoarthritis, cardiovascular-renal-metabolic syndrome, suicidal thoughts, adult migraines, hyperuricemia, and so on (28, 32–35). While certain studies have examined the relationships among oxidative balance scores, dietary quality metrics, and gallstones, potentially considering the dietary intake of carotenoids (5, 31), these metrics are distinct from serum carotenoid levels, which more accurately reflect the actual bioavailability and metabolic activity. The use of serum carotenoid levels reduced the likelihood of recall bias and inaccuracies. To our knowledge, this is the first study to evaluate the association between serum carotenoid levels and gallstones in adult cohorts using a large sample size.
Subgroup analyses reveal that the inverse association between serum carotenoid levels and gallstone risk remains consistent across various demographics, with the exception of individuals younger than 40 years, those with a high school education or lower, and those with a PIR of ≤1.3, where this correlation is less evident. This variation may be due to multiple factors. First, metabolic characteristics, inflammatory responses, and oxidative stress levels can differ markedly between younger and older populations (36). Gallbladder function and bile metabolism in individuals aged <40 years may exhibit reduced sensitivity to the protective effects of carotenoids. Second, socioeconomic factors may exert a considerable influence; individuals with lower educational and income levels may experience heightened nutritional deficiencies and lifestyle challenges, which could affect their dietary patterns, antioxidant capacity, and overall health (37), thereby affecting carotenoid bioavailability (38).
This study identified potential mediating factors in the association between serum carotenoid levels and gallstone formation through mediation analysis. The mediating roles of neutrophil count, CRP, and GGT highlighted the significance of inflammation and liver function in this association. Previous research has found that carotenoid supplementation significantly reduces levels of CRP, IL-6, and TNF-α, with β-carotene and lutein/zeaxanthin showing particularly pronounced effects on lowering CRP levels (39). Additionally, carotenoid oxidation products generated after oxidative stress may induce neutrophil apoptosis, potentially shortening the duration of inflammation (40). Furthermore, carotenoids may protect liver function by enhancing antioxidant capacity and inhibiting GGT elevation (41). These findings provide strong explanations for the results. Moreover, previous studies have reported a negative association between serum carotenoid levels and the prevalence of metabolic disorders, such as obesity, overweight, and lipid metabolism disorders (42). Our study demonstrated that BMI played a pivotal, partially mediating role in the association between carotenoid levels and gallstone formation, with a significant negative mediating effect. This indicates that the effect of serum carotenoid levels on gallstone formation is likely to a large extent driven by their influence on obesity. Specifically, higher serum carotenoid levels are associated with lower BMI, which in turn may reduce the risk of gallstone formation. This finding is consistent with previous research characterizing obesity as chronic low-grade inflammation and increased oxidative stress, suggesting that serum carotenoid levels may indirectly regulate the risk of gallstone formation by affecting BMI (43). The fact that BMI partially mediated this association further underscores the importance of weight management for the favorable effects of serum carotenoid levels on gallstones.
The strengths of this study are as follows: First, based on NHANES data, it included 3,809 adults aged 20 and older, ensuring a large sample size. The stratified, multistage sampling design guarantees broad representativeness of the sample. Covariates were assessed using standardized questionnaires, minimizing measurement bias, and enabling the findings to be widely applied to the adult population in the United States. Second, multiple statistical methods were employed, including multivariate logistic regression, GAM with smoothing curve-fitting techniques, and subgroup analyses. These methods have examined the association between serum carotenoid levels and gallstones from various perspectives. The mediation analysis also provided new insights into the potential mechanisms underlying the effects of carotenoids on gallstone risk. Third, serum carotenoid levels were directly measured rather than relying on dietary recall, avoiding recall bias and allowing for a more accurate assessment. However, this study had several limitations. The cross-sectional nature of this study limited causal inferences. Relying on self-reported data for gallstone diagnosis may introduce bias owing to subjective recall errors, underreporting of asymptomatic cases, or misinterpretation of symptoms (e.g., mistaking other digestive disorders for gallstones), thereby impacting the validity of the results. Although this study highlighted the potential protective effects of serum carotenoids, it is important to consider the effects of dietary sources and lifestyle factors on carotenoid levels and gallstone risk. Variations in dietary habits, physical activity levels, and overall nutritional health can significantly influence carotenoid bioavailability and efficacy, thereby affecting the interpretation of results. Additionally, the NHANES data primarily reflect the adult population of the United States, limiting the extrapolation of findings to regions with significantly different dietary patterns or genetic susceptibilities related to bile metabolism. Finally, because gallstone formation is a long-term process, a single measurement of serum carotenoid levels at a single time point may not fully capture the effects of long-term exposure.
In this study, to ensure methodological validity, we used NHANES stratified sampling to represent the United States adult population and excluded irrelevant subgroups (individuals aged <20 years and those with missing data) to minimize selection bias. Our statistical models underwent rigorous validation: stepwise-adjusted multivariate regression (models 1–3) isolated carotenoids’ independent effects; GAM regression combined with smooth curve fitting confirmed non-linear associations (EDF > 1, p < 0.05); WQS regression identified key components (lycopene, β-carotene, and lutein/zeaxanthin). The consistent inverse associations across carotenoid subtypes (OR: 0.46–0.70) and most subgroups (except young/low-education/low-income ones) further strengthened the results’ reliability. Acknowledging the limitations of the cross-sectional design in terms of causal inference, we interpreted the data with caution. However, our findings align with the existing literature on the antioxidant and anti-inflammatory properties of carotenoids and their established benefits in reducing various chronic disease risks, supporting the plausibility of our results. Mediation analysis also indicated that BMI played a significant intermediary role, suggesting that the protective effect of carotenoids on gallstone risk might partly result from their impact on body weight. Overall, our comprehensive evaluation of the methods, results, and data interpretation indicates this study offers valuable insights into the potential protective link between serum carotenoid levels and gallstone risk, suggesting that maintaining higher serum carotenoid levels may reduce the risk of developing gallstones. For populations at a high gallstone risk, such as those with obesity, dietary interventions or dietary supplements to increase serum carotenoid levels may help reduce the gallstone risk. Future research should further explore the specific mechanisms by which carotenoids act as protective factors against gallstones and validate the causal relationships through longitudinal studies to provide a more targeted theoretical basis for the prevention and management of gallstones.
5 Conclusion
This cross-sectional analysis based on NHANES data involving 3,809 adults showed a significant negative association between serum carotenoid levels and gallstone risk. The highest quartile of total carotenoids was associated with a 48% lower gallstone risk than the lowest quartile. Six specific carotenoids, including α-carotene and α-cryptoxanthin, exhibited dose-dependent protective effects, and GAM analysis further confirmed the non-linear inverse association between them. Subgroup analyses yielded robust results, and mediation analysis indicated that BMI mediated 16.7% of the total effect. This study is the first to demonstrate a negative association between serum carotenoid levels and gallstone occurrence in adults using large-sample data. Although a cross-sectional design cannot establish causality, the results suggest that maintaining high serum carotenoid levels may reduce the gallstone risk. For populations at a high gallstone risk, such as those with obesity, dietary interventions or dietary supplements to increase serum carotenoid levels may help reduce the gallstone risk. Future research is needed to further elucidate the protective mechanisms of serum carotenoids and validate causal relationships through longitudinal studies, thus laying a solid scientific foundation for the prevention and management of gallstones.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/supplementary material.
Ethics statement
The research studies involving human participants received approval from the ethics review board of the Centers for Disease Control and Prevention (CDC). These studies were conducted in accordance with local laws and institutional guidelines. The participants provided their written informed consent to participate in this study.
Author contributions
WR: Project administration, Software, Writing – review & editing, Methodology, Writing – original draft, Investigation. CZ: Writing – original draft, Supervision, Writing – review & editing, Software. JY: Writing – review & editing, Supervision, Methodology. JR: Software, Writing – review & editing, Supervision. HS: Data curation, Software, Writing – review & editing. XW: Writing – review & editing, Supervision. JW: Writing – review & editing, Resources, Funding acquisition, Supervision, Project administration.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was financially supported by the Excellent Talent Fund of Hebei Province (ZF2024073).
Acknowledgments
We thank the participants and staff of the National Health and Nutrition Examination Survey and National Center for Health Statistics for their significant contributions.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
NHANES, National Health and Nutrition Examination Survey; GAM, generalized additive model; PIR, poverty income ratio; OR, odds ratio; BMI, body mass index; HbA1c, hemoglobin A1c; FBG, fasting blood glucose; ALT, alanine aminotransferase; AST, aspartate aminotransferase; GGT, gamma-glutamyl transferase; TSC, total serum carotenoid; CRP, C-reactive protein; CHD, coronary heart disease; FI, fasting insulin.
Footnotes
References
1. Wang, X, Yu, W, Jiang, G, Li, H, Li, S, Xie, L, et al. Global epidemiology of gallstones in the 21st century: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. (2024) 22:51. doi: 10.1016/j.cgh.2024.01.051
2. Yuan, L, Wang, S, Wang, D, and Wang, E. Association of cardiometabolic index with gallstone disease and insulin resistance based on NHANES data. BMC Gastroenterol. (2025) 25:354. doi: 10.1186/s12876-025-03950-8
3. Shooli, ZK, Fotros, D, Hekmatdoost, A, Ghorbani, M, Sadeghi, A, and Yari, Z. The association between dietary acid load and risk of gallstone: a case-control study. J Health Popul Nutr. (2025) 44:141. doi: 10.1186/s41043-025-00894-3
4. Gu, Y, Zhou, Z, Zhao, X, Ye, X, Qin, K, Liu, J, et al. Inflammatory burden index (IBI) and body roundness index (BRI) in gallstone risk prediction: insights from NHANES 2017–2020. Lipids Health Dis. (2025) 24:63. doi: 10.1186/s12944-025-02472-2
5. Wu, W, Pei, Y, Wang, J, Liang, Q, and Chen, W. Association of dietary quality indicators with gallstones in the US: NHANES 2017-2020. BMC Public Health. (2025) 25:976. doi: 10.1186/s12889-025-21783-8
6. Zhou, J, Chen, L, Zhang, Z, and Wu, B. Analysis of risk factors for the increased incidence of gallstone caused by hepatectomy: a retrospective case–control study. Front Surg. (2023) 10:1097327. doi: 10.3389/fsurg.2023.1097327
7. Yang, S, Jiao, N, Wang, J, and Zhang, T. Association between dietary potassium intake and the prevalence of gallstones in American adults: an assessment of data from the national health and nutrition examination survey. BMC Gastroenterol. (2025) 25:197. doi: 10.1186/s12876-025-03744-y
8. Huang, D, Lee, J, Song, N, Cho, S, Choe, S, and Shin, A. Gallstones, cholecystectomy and the risk of hepatobiliary and pancreatic cancer: a nationwide population-based cohort study in Korea. J Cancer Prev. (2020) 25:164. doi: 10.15430/jcp.2020.25.3.164
9. Lin, X, Lin, H, Xu, J, Yang, S, and Miao, L. Relative fat mass as a predictor of gallstones: insights from national health and nutrition examination survey data. Lipids Health Dis. (2025) 24:78. doi: 10.1186/s12944-025-02480-2
10. Ryu, S, Chang, Y, Yun, KE, Jung, H-S, Shin, JH, and Shin, HJOACG. Gallstones and the risk of gallbladder cancer mortality: a cohort study. Am J Gastroenterol. (2016) 111:1476–87. doi: 10.1038/ajg.2016.345
11. Yu, W, Zhou, J, Luo, J, Xia, J, Li, S, Xie, L, et al. The associations between gallstone disease and Pan-Cancer incidence risk based on over 13 million participants. Cancer Med. (2025) 14:e70857. doi: 10.1002/cam4.70857
12. Ghorbani, M, Hekmatdoost, A, Darabi, Z, Sadeghi, A, and Yari, ZJB. Dietary inflammatory index and risk of gallstone disease in Iranian women: a case-control study. BMC Gastroenterol. (2023) 23:311. doi: 10.1186/s12876-023-02943-9
13. Zhu, H, Jin, L, Zhang, Z, Lu, C, Jiang, Q, Mou, Y, et al. Oxidative balance scores and gallstone disease: mediating effects of oxidative stress. Nutr J. (2025) 24:4. doi: 10.1186/s12937-025-01073-0
14. Sadiem, OS, Taher, MA, and Amin, SSJBU. Association of oxidative stress markers with cholelithiasis. Iraqi J. Pharm. Sci. (2014) 2. doi: 10.31351/vol23iss2pp57-61
15. Sanikidze, T, and Chikvaidze, EJRPD. Role of the free radicals in mechanisms of gallstone formation: an EPR study. Radiat Prot Dosim. (2016) 172:317–24. doi: 10.1093/rpd/ncw237
16. Shengelia, M, Intskirveli, N, and Gogebashvili, NJGMN. Inflammatory markers of gallstones disease in menopausal women (2012) 208:52–5.
17. Yang, X-T, Wang, J, Jiang, Y-H, Zhang, L, Du, L, Li, J, et al. Insight into the mechanism of gallstone disease by proteomic and metaproteomic characterization of human bile. Front Microbiol. (2023) 14:1276951. doi: 10.3389/fmicb.2023.1276951
18. Grattagliano, I, Ciampi, SA, and Portincasa, P. Gallbladder disease: relevance of oxidative stress. Gastrointestinal Tissue: Elsevier; (2017). 187–194.
19. Shiesh, S-C, Chen, C-Y, Lin, X-Z, Liu, Z-A, and Tsao, H-CJH. Melatonin prevents pigment gallstone formation induced by bile duct ligation in guinea pigs. Hepatology. (2000) 32:455–60. doi: 10.1053/jhep.2000.16332
20. Maiani, G, Periago Castón, MJ, Catasta, G, Toti, E, Cambrodón, IG, Bysted, A, et al. Carotenoids: actual knowledge on food sources, intakes, stability and bioavailability and their protective role in humans. Mol Nutr Food Res. (2009) 53:S194–218. doi: 10.1002/mnfr.200800053
21. Maria, AG, Graziano, R, and Nicolantonio, DOJFresearch n. Carotenoids: potential allies of cardiovascular health? Food Nutr Res. (2015) 59:26762. doi: 10.3402/fnr.v59.26762
22. Bohn, TJA. Carotenoids and markers of oxidative stress in human observational studies and intervention trials: implications for chronic diseases. Antioxidants. (2019) 8:179. doi: 10.3390/antiox8060179
23. Białkowska, A, Górnicka, M, Zielinska-Pukos, MA, Hallmann, E, and Hamulka, JJA. Plasma carotenoids and polyphenols and their association with MetS: the need for nutritional interventions. Antioxidants. (2023) 12:1336. doi: 10.3390/antiox12071336
24. Yao, Y, Goh, HM, and Kim, JEJA. The roles of carotenoid consumption and bioavailability in cardiovascular health. Antioxidants. (2021) 10:34943081. doi: 10.3390/antiox10121978
25. Wang, Z, Zhao, G, Cao, Y, Gu, T, and Yang, Q. Association between monocyte to high-density lipoprotein cholesterol ratio and kidney stone: insights from NHANES. Front Endocrinol. (2024) 15:1374376. doi: 10.3389/fendo.2024.1374376
26. Xiong, T, Chen, Z, Yi, J, Yu, T, and Wang, KJFN. Higher levels of oxidative balance score linked to lower risk of gallstones: findings from the 2017–2020 National Health and nutrition examination survey. Front Nutr. (2025) 12:1521882. doi: 10.3389/fnut.2025.1521882
27. Li, C, Liang, Y, Lu, Q, Lin, Y, Wen, S, Luo, X, et al. Protective effect of serum carotenoids on mortality among metabolic syndrome patients: attenuated by lipid-lowering drugs. Nutr J. (2025) 24:27. doi: 10.1186/s12937-025-01092-x
28. Huang, JJFN. Association between serum carotenoids levels and endometriosis risk: evidence from the National Health and nutrition examination survey. Front Nutr. (2025) 12:1513191. doi: 10.3389/fnut.2025.1513191
29. Deng, L, Wang, S, Wan, D, Zhang, Q, Shen, W, Liu, X, et al. Relative fat mass and physical indices as predictors of gallstone formation: insights from machine learning and logistic regression. Int J Gen Med. (2025) 18:509–27. doi: 10.2147/IJGM.S507013
30. Wang, J, Xie, F, Zhu, W, Ye, D, Xiao, Y, Shi, M, et al. Relationship between serum carotenoids and telomere length in overweight or obese individuals. Front Nutr. (2024) 11:1479994. doi: 10.3389/fnut.2024.1479994
31. Zhang, M, and Yang, AJFN. Association between oxidative balance score and gallstone disease: a population-based study from NHANES. Front Nutr. (2025) 12:1539969. doi: 10.3389/fnut.2025.1539969
32. Zhu, B, Li, G, Wu, K, Luo, Q, Wu, XJ, and Wu, X. Relationship between serum carotenoids and osteoarthritis or degenerative arthritis: a cross-sectional study using the National Health and nutrition examination survey. Nutr J. (2025) 24:25. doi: 10.1186/s12937-025-01087-8
33. Chen, M, Cai, S, Jia, Q, Suo, Y, Tang, Y, Shi, Y, et al. Inverse relationship between serum carotenoid levels and cardiovascular-kidney-metabolic syndrome among the general adult population. J Diabetes. (2025) 17:e70046. doi: 10.1111/1753-0407.70046
34. Hu, T, Chen, Y, Chen, S, and Xue, R. Association between serum carotenoids levels and severe headache or migraine in adults: a cross-sectional study from NHANES. Front Nutr. (2025) 11:1507503. doi: 10.3389/fnut.2024.1507503
35. Lv, J, Xu, T, Lou, S, Zhan, Z, Cheng, Z, and Fu, FJFN. Association between serum β-carotene and suicidal ideation in adults: a cross-sectional study. Front Nutr. (2024) 11. doi: 10.3389/fnut.2024.1500107
36. Liguori, I, Russo, G, Curcio, F, Bulli, G, Aran, L, Della-Morte, D, et al. Oxidative stress, aging, and diseases. Clin Interv Aging. (2018) 13:757–772. doi: 10.2147/CIA.S158513
37. Dammann, KWSmith, CJJone. Behavior. Factors affecting low-income women's food choices and the perceived impact of dietary intake and socioeconomic status on their health and weight. J Nutr Educ Behav. (2009) 41:242–53. doi: 10.1016/j.jneb.2008.07.003
38. Shilpa, S, Shwetha, HJ, Perumal, MK, Ambedkar, R, Hanumanthappa, M, Baskaran, V, et al. Turmeric, red pepper, and black pepper affect carotenoids solubilized micelles properties and bioaccessibility: capsaicin/piperine improves and curcumin inhibits carotenoids uptake and transport in Caco-2 cells. J Food Sci. (2021) 86:4877–91. doi: 10.1111/1750-3841.15926
39. Hajizadeh-Sharafabad, F, Zahabi, ES, Malekahmadi, M, Zarrin, R, Alizadeh, MJ, Alizadeh, M, et al. Carotenoids supplementation and inflammation: a systematic review and meta-analysis of randomized clinical trials. Crit Rev Food Sci Nutr. (2022) 62:8161–77. doi: 10.1080/10408398.2021.1925870
40. Salerno, C, Crifo, C, Capuozzo, E, Sommerburg, O, Langhans, CD, and Siems, WJB. Effect of carotenoid oxidation products on neutrophil viability and function. Biofactors. (2005) 24:185–92. doi: 10.1002/biof.5520240122
41. Khademalhosseini, M, Ranjbar, E, Mohammadi, R, Khalili, P, Mehran, M, Jalali, N, et al. Dietary antioxidants and liver enzymes in Rafsanjan, a region in Southeast Iran. Sci Rep. (2023) 13:8555. doi: 10.1038/s41598-023-35385-0
42. Iqbal, WA, Mendes, I, Finney, K, Oxley, A, and Lietz, GJIJFS. Reduced plasma carotenoids in individuals suffering from metabolic diseases with disturbances in lipid metabolism: a systematic review and meta-analysis of observational studies. Nutrition. (2021) 72:879–91. doi: 10.1080/09637486.2021.1882962
Keywords: serum carotenoids, gallstones, NHANES, BMI, cross-sectional study, antioxidants, inflammation, mediation analysis
Citation: Ren W, Zhang C, Yin J, Ren J, Song H, Wang X and Wang J (2025) Association between serum carotenoid levels and gallstones in adults: a cross-sectional study using the National Health and Nutrition Examination Survey. Front. Nutr. 12:1601010. doi: 10.3389/fnut.2025.1601010
Edited by:
Hui-Xin Liu, China Medical University, ChinaReviewed by:
Ivan Šoša, University of Rijeka, CroatiaDina Mostafa Mohammed, National Research Centre, Egypt
Copyright © 2025 Ren, Zhang, Yin, Ren, Song, Wang and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Junmin Wang, dGVhY2hlcjIwMjFAaGVibXUuZWR1LmNu