 Qingnv Zhou1
Qingnv Zhou1 Huafei Huang
Huafei Huang- 1Department of Pediatrics, Jiaxing Maternity and Child Health Care Hospital, Affiliated Women and Children Hospital of Jiaxing University, Jiaxing, Zhejiang, China
- 2Department of Neonatology, Xinhua Hospital Affiliated to School of Medicine Shanghai Jiao Tong University, Shanghai, China
Objectives: Pediatric obesity is an increasingly serious global problem. Although much attention has been paid to the role of nutrition in pediatric obesity, no prior study has examined the association between the composite dietary antioxidant index (CDAI), the main measure of an antioxidative diet, and pediatric obesity, and this research aims to investigate this relationship.
Methods: Using the National Health and Nutrition Examination Survey (NHANES) for the period 2009–2018, we examined the relationship between CDAI and pediatric obesity: body mass index (BMI) and waist-to-height ratio (WHtR) using multivariate linear regression models and smoothing fit curves. Furthermore, subgroup analyses were conducted to observe differences in these associations across various stratifying factors.
Results: Our study encompassed 10,019 participants aged 6–18 years with complete data. There was a significant negative correlation between CDAI and BMI (β = −0.04, 95% CI: −0.09, −0.00, p = 0.0367) and WHtR (β = −0.08, 95% CI: −0.15, −0.02, p = 0.0089). Additionally, a one-unit increase in CDAI was linked to a 1.9% decrease in the odds of obesity as defined by WHtR (OR = 0.98, 95% CI: 0.96, 1.00, p = 0.0342). Notably, the negative associations between CDAI and both BMI and WHtR varied across subgroups.
Conclusion: Our findings reveal a linear negative relationship between CDAI and both BMI and WHtR among American children and adolescents, offering novel insights into the potential protective role of antioxidant-rich diets against pediatric obesity.
1 Introduction
Pediatric obesity poses a worldwide health problem. From 1975 to 2016, there was a steady global rise in childhood and adolescent obesity rates after adjusting for age. Specifically, the obesity rate increased by 4.9% in girls and by 6.9% in boys (1). Pediatric obesity has a substantial impact on economically advanced nations. Notably, from 2017 to 2020, the obesity rate in the United States reached 19.7% (2). A 2019 report by the World Obesity Federation projects that pediatric obesity will affect 206 million individuals by 2025 (3). If not addressed in time, pediatric obesity can result in several health complications, including neurological, cardiovascular, and psychosocial problems (4). Effective weight management is crucial for ensuring normal growth and maintaining the physical and mental well-being of children and adolescents.
Healthy eating habits constitute an effective strategy for promoting weight loss in children and adolescents (5). In recent years, studies have investigated associations between various dietary factors and pediatric obesity, including caffeine intake, flavanone intake, and adherence to the Mediterranean diet pattern, among others (6–8). Studies have highlighted the significant role of dietary antioxidants in the prevention and treatment of obesity (9). The composite dietary antioxidant index (CDAI) (10) is considered one of the most reliable and effective indicators for the assessment of an individual’s antioxidant intake. So far, however, no research has investigated whether CDAI is associated with pediatric obesity in the United States.
Body mass index (BMI) is a widely used obesity indicator in epidemiological studies and clinical settings due to its simplicity, practicality, and ease of use. However, it does not differentiate between different types of body fat and is not accurate or reliable as a proxy for fat mass, which may restrict its use in certain studies (11). Central obesity, also known as abdominal obesity, has increasingly prominent detrimental effects on various metabolic diseases compared to generalized obesity (12). The waist-to-height ratio (WHtR) is a validated indicator of abdominal fat accumulation and provides an accurate measure of central obesity. Studies have demonstrated that WHtR outperforms other conventional anthropometric measures in assessing obesity among adults, children, and adolescents (13). Consequently, the present study aims to investigate the relationship between CDAI and pediatric obesity, as assessed by BMI and WHtR.
2 Materials and methods
2.1 Selection of participating populations
This study exclusively utilized data from the National Health and Nutrition Examination Survey (NHANES) database, a nationally representative resource created by the National Center for Health Statistics. The database uses advanced probabilistic sampling methodologies and diverse approaches for assessing the nutritional status and health of Americans. It contains a wide array of information, encompassing demographic details, dietary patterns, health examinations, laboratory findings, and surveys.
This study initially included data from all participants in the NHANES database spanning 10 years from 2009 to 2018. From the initial pool of 49,693 participants, we excluded those aged outside the 6–18 range (N = 36,736), as well as those with missing data (N = 2,938), among which 1,821 lacked CDAI data, 270 lacked BMI or WHtR data, and 847 lacked data for any of the covariates. Ultimately, 10,019 pediatric and adolescent participants were included in the study. Figure 1 illustrates the specific participant selection process in detail.
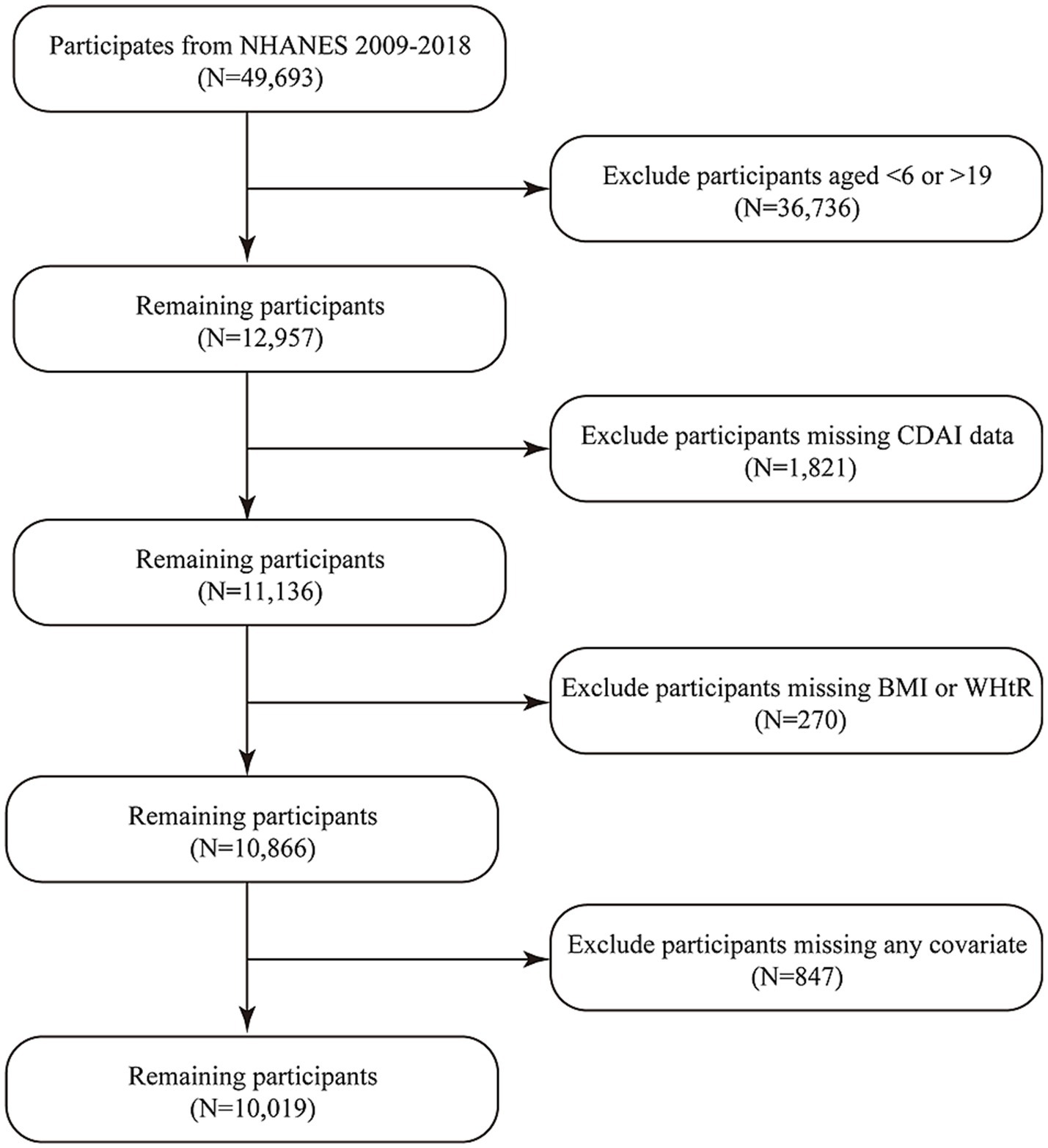
Figure 1. Process of participants’ inclusion.
2.2 Exposure variable: CDAI
The data utilized for calculating the CDAI were derived from the intake of six antioxidants recorded during two separate 24-h food recall interviews in the NHANES database, with the final results considered as the midpoint between the two measurements. The six antioxidants in question are carotenoids (including α-carotene, β-carotene, β-cryptoxanthin, lycopene, lutein, and zeaxanthin), along with vitamin A, vitamin C, vitamin E, zinc, and selenium. It is important to recognize that the CDAI values exclude dosages of antioxidants obtained through dietary supplements or pharmaceuticals.
The CDAI values were computed using an adapted version created by Wright et al. (10). The standardization process involved three sequential steps: first, the mean consumption value for each antioxidant was deducted from its corresponding 2-day mean intake; next, the data were normalized by dividing each value by the population’s standard deviation; and finally, the standardized values for all antioxidants were summed (14). In other words, the CDAI is the cumulative result of each antioxidant being standardized before summation.
2.3 Outcome variables: BMI and WHtR
The data utilized for calculating BMI were derived from anthropometric measurements in the NHANES database, collected by trained health professionals at mobile examination centers. BMI is found by dividing weight by the square of height, in units of kg/m2. A higher BMI value indicates a higher degree of generalized obesity. Apart from continuous BMI data, we also used these data to evaluate the prevalence of childhood and adolescent obesity. Obesity in children between 2 and 19 years is categorized by the Centers for Disease Control and Prevention (CDC) using BMI growth charts (15), classifying those with a BMI at or above the 95th percentile as obese. Notably, due to the characteristics of the growth charts, the cutoff values vary across different ages and genders.
Similarly, the data utilized for calculating the WHtR also originate from anthropometric measurements in the NHANES database. The WHtR is determined by dividing waist size by height, using the same measurement units for both, and is expressed as a percentage (%). A higher WHtR value indicates a higher degree of central obesity. Central obesity, as assessed by WHtR, is defined as a WHtR of 50% or greater (16).
2.4 Covariates
Based on previous related studies (17–19), we selected seven variables that may potentially influence the association between CDAI and pediatric obesity as covariates to analyze potential confounding factors. These seven variables are: gender, age, ethnicity, poverty–income ratio (PIR), protein intake (g), carbohydrate intake (g), and fat intake (g).
The representation of gender is in the form of boys or girls, while racial categories include Mexican American, other Hispanic, Non-Hispanic White, Non-Hispanic Black, and other ethnicities. Additionally, for statistical analysis and convenience, continuous variables are grouped as follows: age is classified into children (6–8 years) and adolescents (9–18 years); PIR is categorized as low (≤1.3), medium (>1.3, ≤3.5), and high (>3.5); and protein, carbohydrate, and fat intakes are each divided into tertiles, denoted as T1, T2, and T3, respectively, in ascending order.
2.5 Statistical analysis
The exposure variable in this study was the value of CDAI, while the outcome variables were BMI and WHtR. Multivariable logistic regression analysis was used to investigate the relationship between the exposure variable and the outcome variables. Three models were constructed by adjusting for different covariates. In particular, no adjustment was made for any covariates in the crude model. Model 1 made a minimal adjustment for sex, age, and ethnicity. Model 2, a fully adjusted model, adjusted for all covariates, including sex, age, ethnicity, PIR, protein intake, carbohydrate intake, and fat intake. The correlation was measured by calculating the corresponding β coefficients, the odds ratio (OR), and the 95% confidence interval (CI).
In this study, we used the t-test to analyze continuous data and the chi-square test to show categorical data as percentages. A p-value less than 0.05 meant the results were statistically significant. All relevant statistical tests and methods were conducted using R-Software version 4.0.
3 Results
3.1 Baseline characteristics of participants
The research encompassed 10,019 participants, both adolescents and children, aged between 6 and 18 years. Table 1 shows an in-depth overview of the initial attributes of the participants, categorized according to age. Adolescents had higher CDAI values compared to children (0.09 ± 4.18 vs. -0.29 ± 3.07), exhibited higher BMI values (22.96 ± 6.14 vs. 17.58 ± 3.58) and WHtR values (49.49 ± 8.57 vs. 47.94 ± 6.30), and were more likely to be classified as having general obesity (21.64% vs. 19.13%) and central obesity (38.30% vs. 27.36%).
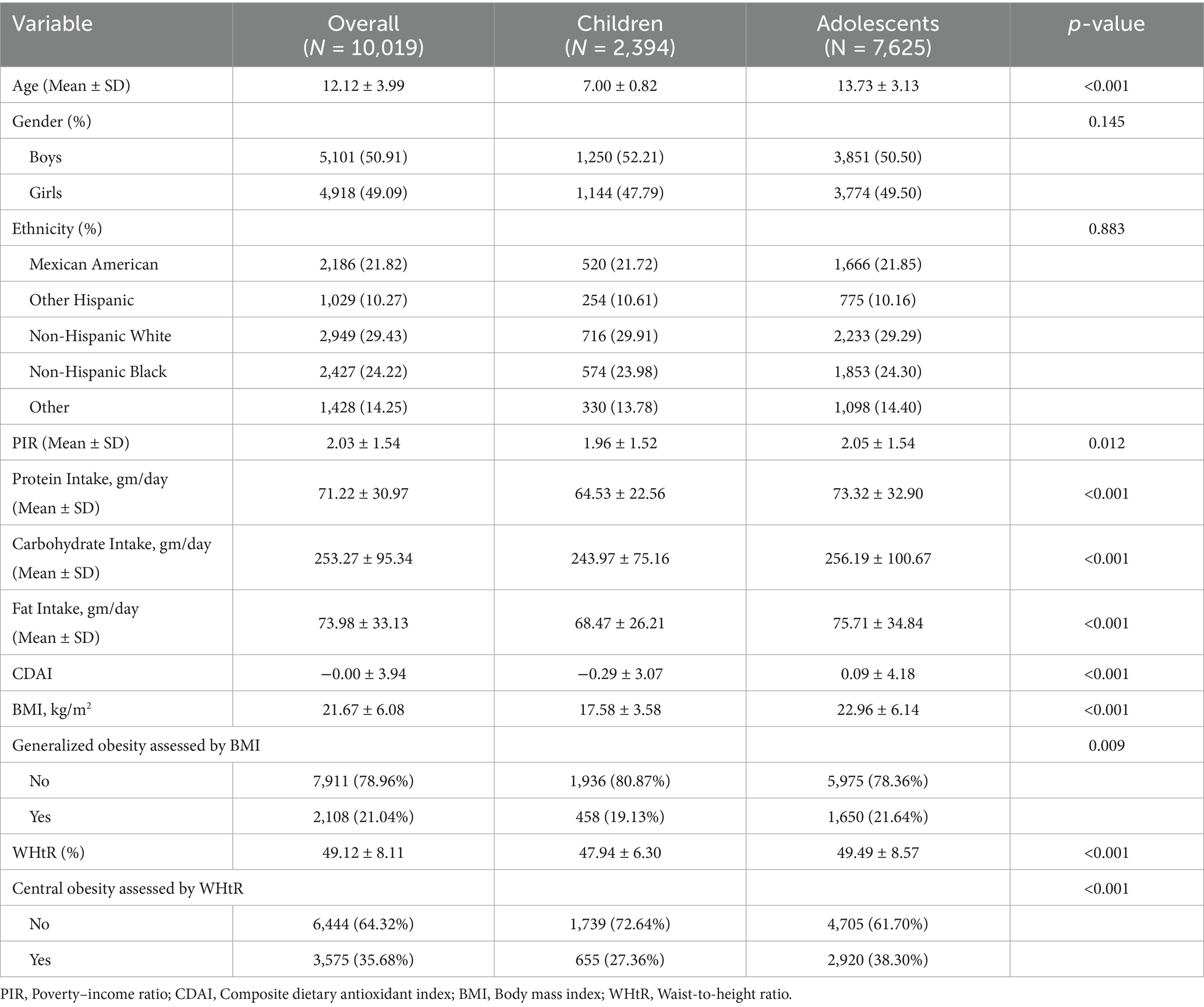
Table 1. Characteristics of the study population stratified by age groups.
3.2 Associations of CDAI with BMI and WHtR
Table 2 displays the outcomes of a multivariate logistic regression study examining the link between CDAI and BMI, along with CDAI and WHtR. There was an inverse relationship between CDAI and BMI (β = − 0.05, 95% confidence interval: −0.08, −0.02) as well as WHtR (β = −0.18, 95% CI: −0.22, −0.14). After adjustment for gender, age, and ethnicity (Model 1), there was still a significant correlation between CDAI and BMI, as well as between CDAI and WHtR, with β values between −0.08 (95% CI, −0.11, −0.05) and −0.17 (95% CI, −0.21, −0.13). Similarly, CDAI had a negative association with BMI (β = −0.04, 95% CI: −0.09, −0.00, p = 0.0367) and WHtR (β = −0.08, 95% CI: −0.15, −0.02, p = 0.0089). These findings suggest that for every additional unit of CDAI, BMI decreases by approximately 4%, while WHtR decreases by 8%.
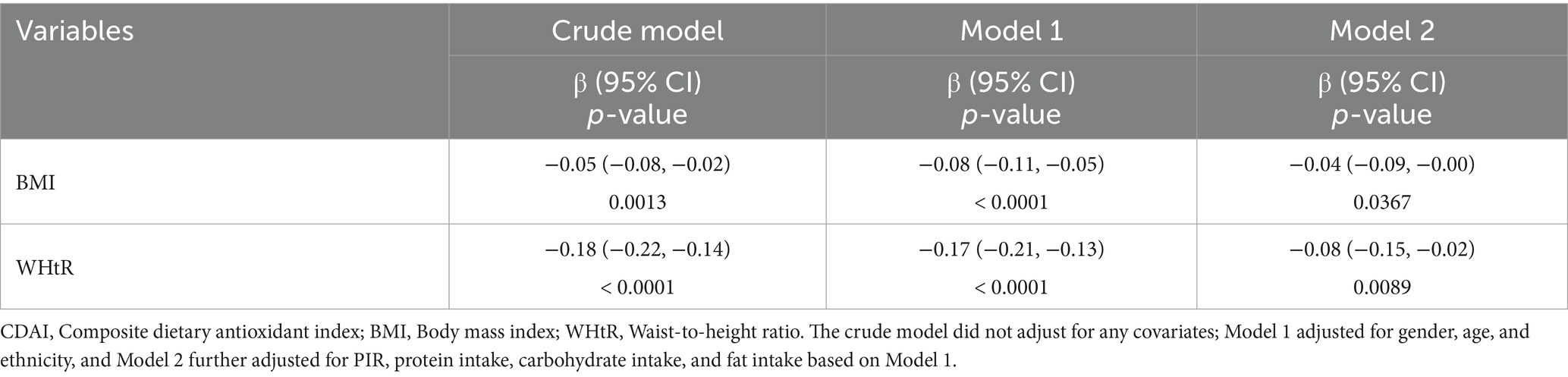
Table 2. Association of CDAI and BMI, WHtR.
Furthermore, we represented BMI and WHtR as categorical variables indicating the presence or absence of generalized obesity and central obesity, respectively, to further examine the association between CDAI and pediatric obesity, with the results presented in Table 3. Both the crude model and Model 1 similarly demonstrated significant negative correlations between CDAI and generalized obesity, as well as between CDAI and central obesity. After adjusting for all covariates, the odds of being classified as central obese according to WHtR decreased by 1.9% for each additional unit of CDAI (OR 95% CI: 0.963, 0.999, p = 0.03419). Interestingly, Model 2 showed no significant association between CDAI and BMI-defined generalized obesity (OR = 0.982, 95% CI: 0.962, 1.003, p = 0.09812).
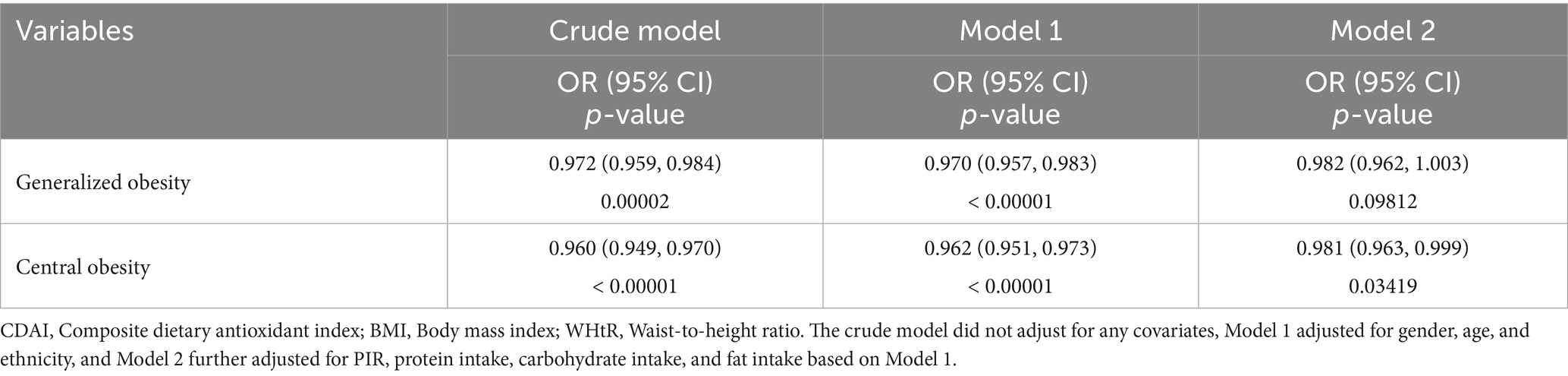
Table 3. Association between CDAI and obesity as measured by BMI and WHtR.
3.3 Smooth curve fitting
The results of the smooth curve fitting are shown in Figure 2, indicating that no non-linear relationships were detected between CDAI and either BMI or WHtR.
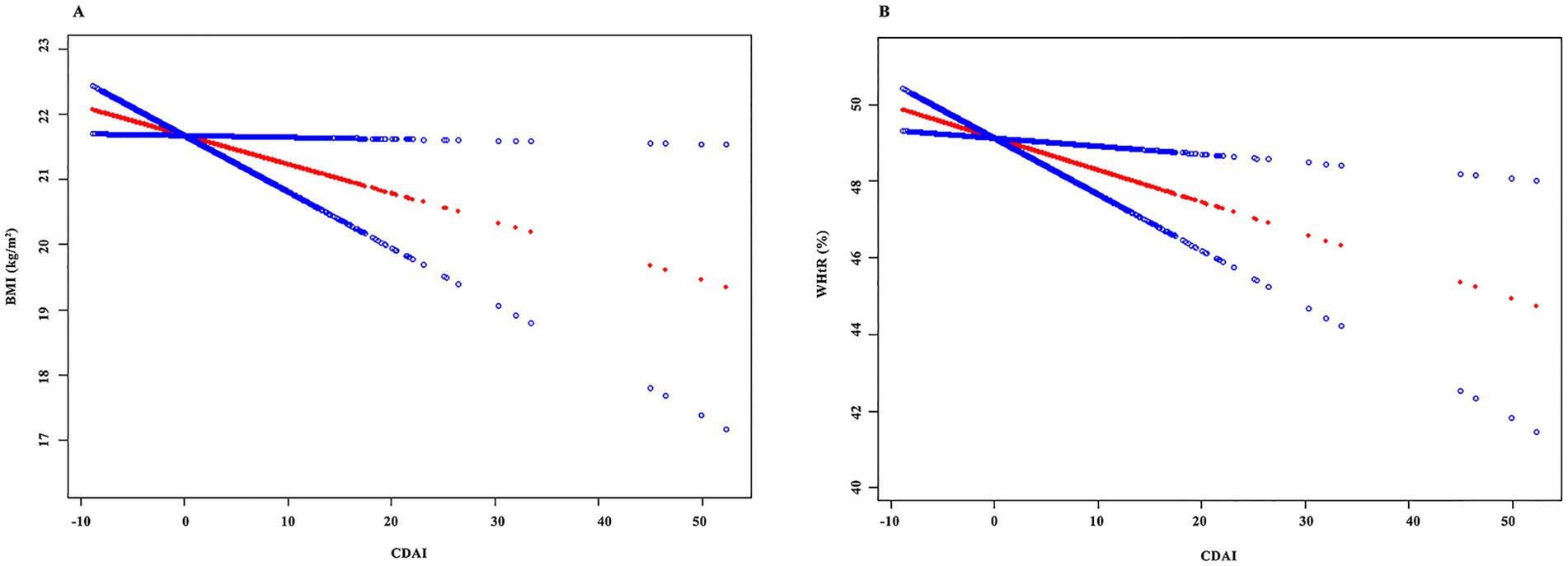
Figure 2. Results of the smooth curve fitting. (A) CDAI and BMI; (B) CDAI and WHtR.
3.4 Subgroup analysis
Our analysis of subgroups was segmented according to multiple criteria, including gender, age, ethnic background, PIR, protein intake, carbohydrate intake, and fat intake. The results, shown in Figure 3, show that the relationships vary.
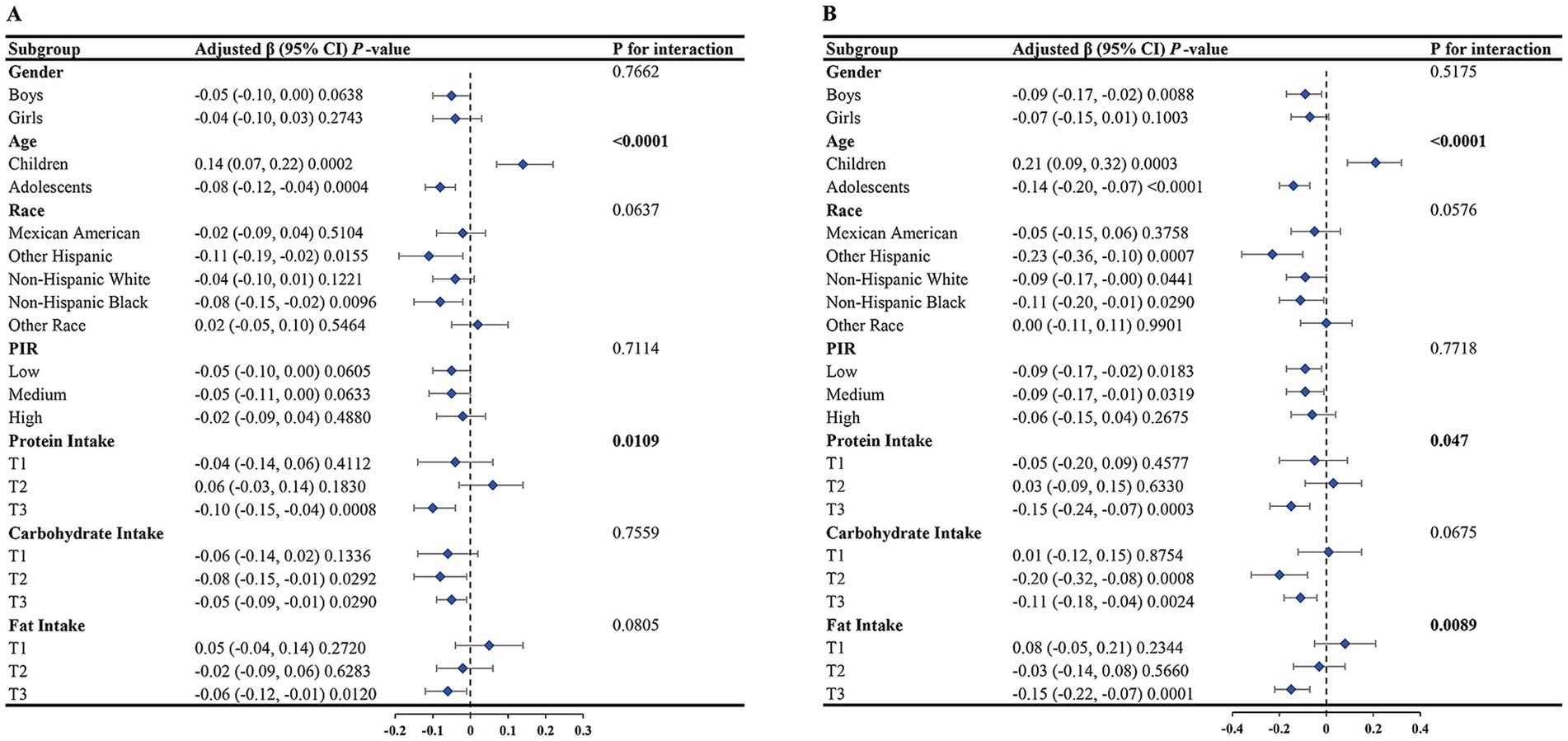
Figure 3. Results of the subgroup analysis. (A) CDAI and BMI; (B) CDAI and WHtR.
Notably, we found statistically significant interaction effects (p < 0.05) for the relationship between CDAI and BMI within subgroups defined by age and protein consumption, but not within other subgroups. The inverse relationship between the two was more evident in adolescents and in individuals with higher protein consumption.
The relationship between CDAI and WHtR demonstrated statistically significant interaction effects across subgroups defined by age, protein consumption, and fat consumption (p < 0.05), whereas it was insignificant in other subgroups.
4 Discussion
In our research, we investigated the relationships among CDAI, BMI, and WHtR in US youth aged 6–18. After taking into account all the relevant variables, we found that CDAI was associated with both BMI and WHtR significantly, indicating a trend where higher CDAI values correlate with decreased BMI and WHtR levels. This implies that boosting antioxidant consumption in daily meals could aid in combating and handling pediatric obesity.
To the best of our understanding, the present analysis marks an initial attempt to assess the linkage between CDAI and pediatric obesity in the US. Despite the scarcity of research on this connection, similar discoveries can be traced back to prior studies. Key research areas focusing on the relationship between antioxidant-rich diets and obesity predominantly concentrate on adults: a study involving US adults (20) exhibited an inverse relationship between CDAI and areas of visceral fat, hinting that an elevated CDAI might ameliorate visceral obesity. Another study targeting elderly Americans (21) unveiled an L-shaped inverse relationship between CDAI and sarcopenic obesity. Furthermore, a prospective study involving middle-aged and elderly individuals in Rotterdam (22) suggested that dietary antioxidant intake could favorably influence lean body mass and overall body composition in this demographic. These conclusions broadly align with our findings. Research on children and adolescents is scarce, with just one comparable study (23) identified: a cross-sectional examination among Greek elementary school students aged 10–12 exploring the connection between the dietary antioxidant index and BMI. When BMI was considered a continuous measure, a negative association was noted, mirroring our results. However, when BMI was categorized to evaluate obesity, that study still demonstrated a significant negative correlation, which was not apparent in our study. Variations in research results could stem from disparities in the size of the sample, age demographics, and geographical locations.
It is worth mentioning that in our study, after adjusting for all confounding factors, the association between CDAI and generalized obesity (measured by body mass index, BMI) was not statistically significant (p > 0.05). In contrast, a significant inverse association (p < 0.05) persisted between CDAI and central obesity (measured by waist-to-height ratio, WHtR). This finding highlights a notable divergence in the relationship between CDAI and different types of obesity. In previous research, we have also noted variations in the associations between BMI and WHtR with different health conditions. A comprehensive analysis conducted by Ashwell et al. (24) revealed that WHtR is more effective than BMI in identifying cardiometabolic risk. Conversely, a meta-analysis by Lo et al. (25) indicated that BMI is more accurate than WHtR in screening for hypertension.
Although the exact mechanisms by which the CDAI is associated with pediatric obesity remain incompletely understood, they may be related to the biochemical mechanisms between oxidative stress and obesity. Biochemical imbalance, characterized by an imbalance between antioxidants and free radicals, serves as a pivotal aspect in the development of obesity and its associated issues (26). Diet holds a fundamental position in regulating blood redox status and affording protection against oxidative and nitrosative agents (27). Research has shown that diets abundant in antioxidant substances can safeguard living beings from biochemical imbalances (28). The CDAI offers a thorough assessment of total antioxidant consumption derived from food, incorporating six components that play vital parts in mitigating stress-triggered oxidant alterations (29). It has been reported that vitamin A serves as an important regulator of adipose tissue development (26). Vitamin C exhibits antioxidant and protective effects against oxidative stress and obesity (30). Vitamin E can diminish fat tissue scarring, irritation, and oxidative damage, thereby enhancing the physiological condition of obese patients (31). The double-bond system endows carotenoids with antioxidant properties, and carotenoids and their metabolites trigger anti-obesity activities through multiple mechanisms (32). Zinc and selenium play vital roles in safely combating inflammation and maintaining redox balance (33). Overall, the CDAI can be used to comprehensively assess dietary antioxidant intake.
Subgroup analysis revealed significant differences in the associations between CDAI and BMI, as well as between CDAI and WHtR, across age groups. This may be attributed to factors such as growth and development characteristics, nutritional needs, and dietary habits of children and adolescents at different age stages. For instance, during childhood, due to rapid growth and development and high nutritional demands (34), the intake of antioxidants in the diet may have a more pronounced impact on obesity and growth and development. In contrast, during adolescence, with differences in growth and development characteristics, dietary variations, and changes in lifestyle (35, 36), the relationship between dietary antioxidant intake and obesity may undergo alterations. Similarly, protein intake also modifies the relationship between CDAI and obesity. Protein is a vital macronutrient needed for growth and maturation, indispensable for maintaining the health of muscles, bones, the immune system, and more (37). Variations in protein intake may influence weight gain, body fat distribution, and metabolic status among children and adolescents (38). One study suggests that the effect of high protein intake on obesity varies by age (39). In particular, we found that CDAI and WHtR were significantly different among fat intake subgroups (p < 0.05). According to one study, high-fat intake increases oxidative stress levels (40), which may be more evident in terms of abdominal manifestations.
The research presents multiple advantages. Initially, it uses a substantial sample that represents the entire nation. Secondly, the comprehensive assessment of obesity through BMI and WHtR facilitates the observation of differences between these two indicators. Additionally, a variety of models were utilized to account for numerous possible confounding elements, and analyses of subgroups were performed to bolster the solidity of our results. Nonetheless, acknowledging the constraints of our study is crucial. Our capacity to deduce causal links is constrained by the study’s cross-sectional nature. Although many covariates are included, other factors affect the results. Finally, the potential for confounding bias and reporting bias remains.
5 Conclusion
The findings of our research reveal a direct inverse relationship between CDAI and both BMI and WHtR in American youths and adolescents. Consuming a diet high in antioxidants could be beneficial in preventing and alleviating pediatric obesity.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found at: https://wwwn.cdc.gov/nchs/nhanes/default.aspx.
Ethics statement
The studies involving humans were approved by the National Center for Health Statistics. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
QZ: Conceptualization, Methodology, Writing – original draft. YW: Writing – original draft, Software, Conceptualization. HuX: Writing – original draft, Software. HoX: Writing – original draft, Validation. RY: Validation, Writing – original draft. HH: Supervision, Writing – review & editing, Validation, Conceptualization.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
Our heartfelt thanks go out to every participant who offered data support for this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. NCD Risk Factor Collaboration. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet. (2017) 390:2627–42. doi: 10.1016/S0140-6736(17)32129-3
2. Stierman, B, Afful, J, Carroll, MD, Chen, TC, Davy, O, Fink, S, et al. National health and nutrition examination survey 2017–march 2020 prepandemic data files—development of files and prevalence estimates for selected health outcomes. (2021). Available online at: https://www.cdc.gov/nchs/data/nhsr/nhsr158-508.pdf (Accessed June 14, 2021).
3. Smith, JD, Fu, E, and Kobayashi, MA. Prevention and Management of Childhood Obesity and its Psychological and health comorbidities. Annu Rev Clin Psychol. (2020) 16:351–78. doi: 10.1146/annurev-clinpsy-100219-060201
4. Jebeile, H, Kelly, AS, O’Malley, G, and Baur, LA. Obesity in children and adolescents: epidemiology, causes, assessment, and management. Lancet Diabetes Endocrinol. (2022) 10:351–65. doi: 10.1016/S2213-8587(22)00047-X
5. Jin, J. Interventions for high BMI in children and teenagers. JAMA. (2024) 332:262. doi: 10.1001/jama.2024.11756
6. Qu, Y, Xu, W, Guo, S, and Wu, H. Association of sociodemographic and lifestyle factors and dietary intake with overweight and obesity among U.S. children: findings from NHANES. BMC Public Health. (2024) 24:637. doi: 10.1186/s12889-024-19637-w
7. Liu, Y, Liu, Z, and Wu, N. Association between intake of flavanones and the overweight/obesity and central obesity in children and adolescents: a cross-sectional study from the NHANES database. Front Nutr. (2024) 11:1430140. doi: 10.3389/fnut.2024.1430140
8. Zheng, X, Wang, H, and Wu, H. Association between diet quality scores and risk of overweight and obesity in children and adolescents. BMC Pediatr. (2023) 23:169. doi: 10.1186/s12887-023-03966-7
9. Mohammadi, S, Lotfi, K, Mirzaei, S, Asadi, A, Akhlaghi, M, and Saneei, P. Dietary total antioxidant capacity in relation to metabolic health status in overweight and obese adolescents. Nutr J. (2022) 21:54. doi: 10.1186/s12937-022-00806-9
10. Wright, ME, Mayne, ST, Stolzenberg-Solomon, RZ, Li, Z, Pietinen, P, Taylor, PR, et al. Development of a comprehensive dietary antioxidant index and application to lung cancer risk in a cohort of male smokers. Am J Epidemiol. (2004) 160:68–76. doi: 10.1093/aje/kwh173
11. Sweatt, K, Garvey, WT, and Martins, C. Strengths and limitations of BMI in the diagnosis of obesity: what is the path forward? Curr Obes Rep. (2024) 13:584–95. doi: 10.1007/s13679-024-00580-1
12. Chen, X, Shi, F, Xiao, J, Huang, F, Cheng, F, Wang, L, et al. Associations between abdominal obesity indices and nonalcoholic fatty liver disease: Chinese visceral adiposity index. Front Endocrinol (Lausanne). (2022) 13:831960. doi: 10.3389/fendo.2022.831960
13. Ashtary-Larky, D, Daneghian, S, Alipour, M, Rafiei, H, Ghanavati, M, Mohammadpour, R, et al. Waist circumference to height ratio: better correlation with fat mass than other anthropometric indices during dietary weight loss in different rates. Int J Endocrinol Metab. (2018) 16:e55023. doi: 10.5812/ijem.55023
14. Wu, D, Wang, H, Wang, W, Qing, C, Zhang, W, Gao, X, et al. Association between composite dietary antioxidant index and handgrip strength in American adults: Data from National Health and nutrition examination survey (NHANES, 2011-2014). Front Nutr. (2023) 10:1147869. doi: 10.3389/fnut.2023.1147869
15. Fryar, CD, and Afful, J. Prevalence of overweight, obesity, and severe obesity among children and adolescents aged 2–19 years: United States, 1963–1965 through 2017–2018. NCHS Health E-Stats.
16. Mokha, JS, Srinivasan, SR, Dasmahapatra, P, Fernandez, C, Chen, W, Xu, J, et al. Utility of waist-to-height ratio in assessing the status of central obesity and related cardiometabolic risk profile among normal weight and overweight/obese children: the Bogalusa heart study. BMC Pediatr. (2010) 10:73. doi: 10.1186/1471-2431-10-73
17. Wang, L, Liu, W, Bi, S, Zhou, L, and Li, L. Association between minerals intake and childhood obesity: a cross-sectional study of the NHANES database in 2007-2014. PLoS One. (2023) 18:e0295765. doi: 10.1371/journal.pone.0295765
18. Yang, B, Tang, C, Shi, Z, and Gao, L. Association of Macronutrients Intake with body composition and Sarcopenic obesity in children and adolescents: a population-based analysis of the National Health and nutrition examination survey (NHANES) 2011-2018. Nutrients. (2023) 15:307. doi: 10.3390/nu15102307
19. Zhang, L, Peng, H, Wang, Y, and Ba, H. Association of dietary inflammatory index with obesity among children and adolescents in the United States NHANES cohort: a population-based study. Ital J Pediatr. (2024) 50:14. doi: 10.1186/s13052-024-01586-0
20. Gu, X, Wang, X, Wang, S, Shen, Y, and Lu, L. Composite dietary antioxidant index is inversely associated with visceral adipose tissue area among U.S. adults: a cross-sectional study. Nutr Res. (2024) 124:13–20. doi: 10.1016/j.nutres.2024.01.011
21. Wu, H, Chen, X, Shi, Z, Liu, J, Meng, Z, Zheng, C, et al. The L-shaped relationship between composite dietary antioxidant index and sarcopenic obesity in elderly adults: a cross-sectional study. Front Nutr. (2024) 11:1428856. doi: 10.3389/fnut.2024.1428856
22. van der Schaft, N, Trajanoska, K, Rivadeneira, F, Ikram, MA, Schoufour, JD, and Voortman, T. Total dietary antioxidant capacity and longitudinal trajectories of body composition. Antioxidants (Basel). (2020) 9:728. doi: 10.3390/antiox9080728
23. Kokkou, S, Notara, V, Kanellopoulou, A, Antonogeorgos, G, Rojas-Gil, AP, Kornilaki, E, et al. The association between the dietary antioxidant index and weight status in primary school students: an epidemiological study. Nutrients. (2024) 16:667. doi: 10.3390/nu16111667
24. Ashwell, M, Gunn, P, and Gibson, S. Waist-to-height ratio is a better screening tool than waist circumference and BMI for adult cardiometabolic risk factors: systematic review and meta-analysis. Obes Rev. (2012) 13:275–86. doi: 10.1111/j.1467-789X.2011.00952.x
25. Lo, K, Wong, M, Khalechelvam, P, and Tam, W. Waist-to-height ratio, body mass index and waist circumference for screening paediatric cardio-metabolic risk factors: a meta-analysis. Obes Rev. (2016) 17:1258–75. doi: 10.1111/obr.12456
26. Bizerea-Moga, TO, Pitulice, L, Bizerea-Spiridon, O, and Moga, TV. Exploring the link between oxidative stress, selenium levels, and obesity in youth. Int J Mol Sci. (2024) 25:276. doi: 10.3390/ijms25137276
27. Pizzino, G, Irrera, N, Cucinotta, M, Pallio, G, Mannino, F, Arcoraci, V, et al. Oxidative stress: harms and benefits for human health. Oxidative Med Cell Longev. (2017) 2017:8416763. doi: 10.1155/2017/8416763
28. Winiarska-Mieczan, A, Mieczan, T, and Wójcik, G. Importance of redox equilibrium in the pathogenesis of psoriasis-impact of antioxidant-rich diet. Nutrients. (2020) 12:1841. doi: 10.3390/nu12061841
29. Zhu, Z, Han, Y, and Chen, H. Dietary antioxidants and nutritional risk in the elderly: insights from the composite dietary antioxidant index and geriatric nutritional risk index. Front Immunol. (2025) 16:1596663. doi: 10.3389/fimmu.2025.1596663
30. Drehmer, E, Navarro-Moreno, M, Carrera, S, Villar, VM, and Moreno, ML. Oxygenic metabolism in nutritional obesity induced by olive oil. the influence of vitamin C. Food Funct. (2019) 10:3567–80. doi: 10.1039/c8fo02550a
31. Alcalá, M, Sánchez-Vera, I, Sevillano, J, Herrero, L, Serra, D, Ramos, MP, et al. Vitamin E reduces adipose tissue fibrosis, inflammation, and oxidative stress and improves metabolic profile in obesity. Obesity (Silver Spring). (2015) 23:1598–606. doi: 10.1002/oby.21135
32. Bonet, ML, Ribot, J, Galmés, S, Serra, F, and Palou, A. Carotenoids and carotenoid conversion products in adipose tissue biology and obesity: pre-clinical and human studies. Biochim Biophys Acta Mol Cell Biol Lipids. (2020) 1865:158676. doi: 10.1016/j.bbalip.2020.158676
33. Cruz, KJC, de Oliveira, ARS, Fontenelle, LC, Morais, JBS, de Sousa Melo, SR, Dos Santos, LR, et al. Relationship between zinc, selenium, and magnesium status and markers of metabolically healthy and unhealthy obesity phenotypes. Biol Trace Elem Res. (2024) 202:3449–64. doi: 10.1007/s12011-023-03938-z
34. Saavedra, JM, and Prentice, AM. Nutrition in school-age children: a rationale for revisiting priorities. Nutr Rev. (2023) 81:823–43. doi: 10.1093/nutrit/nuac089
35. Hermanussen, M, and Meigen, C. Phase variation in child and adolescent growth. Int J Biostat. (2007) 3:Article 9. doi: 10.2202/1557-4679.1045
36. Zietz, S, Cheng, E, Lansford, JE, Deater-Deckard, K, Di Giunta, L, Dodge, KA, et al. Positive parenting, adolescent adjustment, and quality of adolescent diet in nine countries. J Adolesc. (2022) 94:1130–41. doi: 10.1002/jad.12089
37. Xiong, T, Wu, Y, Hu, J, Xu, S, Li, Y, Kong, B, et al. Associations between high protein intake, linear growth, and stunting in children and adolescents: a cross-sectional study. Nutrients. (2023) 15:821. doi: 10.3390/nu15224821
38. Switkowski, KM, Jacques, PF, Must, A, Fleisch, A, and Oken, E. Associations of protein intake in early childhood with body composition, height, and insulin-like growth factor I in mid-childhood and early adolescence. Am J Clin Nutr. (2019) 109:1154–63. doi: 10.1093/ajcn/nqy354
39. Garcia-Iborra, M, Castanys-Munoz, E, Oliveros, E, and Ramirez, M. Optimal protein intake in healthy children and adolescents: evaluating current evidence. Nutrients. (2023) 15:683. doi: 10.3390/nu15071683
Keywords: composite dietary antioxidant index, obesity, children and adolescents, population-based study, NHANES
Citation: Zhou Q, Wu Y, Xu H, Xie H, Yang R and Huang H (2025) Population-based analysis of the association between composite dietary antioxidant index and pediatric obesity. Front. Nutr. 12:1617384. doi: 10.3389/fnut.2025.1617384
Edited by:
Reza Rastmanesh, American Physical Society, United StatesReviewed by:
Anastasija Panić, University of Belgrade, SerbiaTeofana-Otilia Bizerea-Moga, Victor Babes University of Medicine and Pharmacy, Romania
Copyright © 2025 Zhou, Wu, Xu, Xie, Yang and Huang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Huafei Huang, aGhmanhmYnlAemp4dS5lZHUuY24=