 Büşra Açıkalın Göktürk
Büşra Açıkalın Göktürk Nevin Sanlier
Nevin Sanlier- 1Department of Gastronomy and Culinary Arts, Faculty of Fine Arts, Design and Architecture, Ankara Medipol University, Ankara, Türkiye
- 2Department of Nutrition and Dietetics, School of Health Sciences, Ankara Medipol University, Ankara, Türkiye
Rheumatoid arthritis (RA) is a chronic inflammatory autoimmune disease that causes progressive joint destruction. It affects ~1% of the world population and is more common in women aged 20–45 years than in men. RA causes involvement of small joints such as the joints of the hands and feet, pain, swelling, stiffness and loss of function in the joints. In recent years, Mediterranean diet and anti-inflammatory diet models have attracted attention in the medical nutrition therapy of patients with RA. These dietary patterns have been suggested to reduce disease risk and complications and improve disease manifestations. Mediterranean and inflammatory dietary patterns contain antioxidant vitamins and minerals, omega-3, polyunsaturated fatty acids and may have effects on inflammation and pain. In addition, dietary patterns may be effective in preventing free radical formation and increased cytokine levels due to their antioxidant and anti-inflammatory properties. In addition, by decreasing inflammatory markers and increasing antioxidant mechanism, it may be effective in reducing the level of disease activity, clinical and biochemical findings and increasing the quality of life. While the Mediterranean Diet and diet inflammatory index (DII) show promise in managing RA, it is important to consider the variability of individual responses to dietary interventions. There are conflicting results regarding the efficacy of the MedDiet in reducing disease activity and further research is needed to establish robust evidence-based dietary recommendations for RA patients. Overall, incorporating dietary strategies with anti-inflammatory properties may offer a valuable addition to conventional RA management and potentially improve patient outcomes and quality of life.
Introduction
Rheumatoid arthritis (RA) is a systemic and chronic inflammatory autoimmune disease affecting ~1% of the world population (1). RA is usually observed between the ages of 20–45 years and more frequently in women than in men (2) and is characterized by pain, swelling, stiffness and loss of function in the joints. Involvement of small joints such as hand and foot joints is common in the body. This disease seriously affects quality of life with increasing morbidity and mortality (3).
The etiology of RA is considered multifactorial as it involves both genetic and environmental factors. Immune mechanisms such as the production of inflammatory cytokines [tumor necrosis factor-α (TNF-α), interleukin-1 (IL-1), interleukin-6 (IL-6)] and increased cell-mediated immune response are known to play an important role in RA formation (4, 5). Recently, nutritional interventions and dietary patterns have become important to improve RA symptoms as RA patients perceive rapid changes in pain and/or swelling after consumption of certain foods. Adoption and maintenance of an appropriate nutritional plan in these patients contributes to the reduction of the severity of disease symptoms and achievement of remission (6). In general, it has been reported that adequate dietary protein and energy intake and a diet rich in antioxidant vitamins and minerals and omega-3 polyunsaturated fatty acids may prevent tissue damage and suppress the inflammatory process in rheumatologic diseases (7). These nutrients have been shown to be effective in preventing free radical formation and increased cytokine levels (8). The nutritional plan may modulate RA symptoms by influencing the patient's metabolic profile and increasing antioxidant levels, as well as altering the intestinal microflora (9). The Mediterranean Diet and Anti-inflammatory Diet have a positive effect on the course of the disease because it contains all the energy, nutrients and polyphenols required for adequate and balanced nutrition (10).
Although the Mediterranean Diet and Anti-inflammatory diet or dietary inflammatory index, which is part of the Mediterranean diet show promise in managing RA, the variability of individual responses to dietary interventions should be taken into account. There are conflicting results regarding the efficacy of DII and MedDiet in reducing disease activity. It is reported that more research is needed to establish robust evidence-based dietary recommendations for RA patients (11). However, while dietary interventions can complement pharmacologic treatments, they should not replace standard medical care. In addition, the inclusion of dietary strategies with anti-inflammatory properties may contribute to RA management and potentially improve patient outcomes and quality of life.
The aim of this review is to examine the current evidence and controversy on the relationship between DII was shaped as the infrastructure of Mediterranean-style eating habits and MedDiet approaches in the nutritional management of RA and their impact on disease course and symptoms, and to develop recommendations for the future.
Materials and methods
A literature search was conducted using electronic databases, MEDLINE, Embase, Cochrane Library, CINAHL, Clinical Trials.gov, Scopus, Pubmed, Google academic, ScienceDirect and Web of Science. The reference articles were obtained from databases using the keywords: [RA] and [diet] or [dietary pattern] or [diet quality] or [nutrition] or [dietary inflammatory index] and [MedDiet] and [mechanism] and [pathway].
Searches were performed by the authors and full texts were categorized according to studies published between 2018 and 2025, their availability in English full-text format, and their status as original research, review, traditional review, systematic and meta-analysis, and letter to the editor.
Articles written in languages other than English or published as preprint versions were excluded during the screening process. We also excluded articles that were considered to be of low relevance or irrelevant to our areas of interest, as indicated by their titles and subtitles. Publications deemed appropriate for review were carefully evaluated, full-text review and discussion were conducted where necessary, and some suggestions for the future were presented.
Effect of Mediterranean diet and dietary inflammatory index (DII) in patients with RA
Although the clinical findings of RA vary according to the stage of the disease and the joints involved, the most prominent findings are symmetrical swelling of the joints and intense pain (12). In addition to these, morning stiffness, fever, fatigue and weakness are other findings of the disease which progress slowly over a few weeks (13). Adoption and maintenance of an appropriate nutritional plan in patients with rheumatoid arthritis contributes to the improvement of the disease, reduction of the symptoms and risk of complications of the disease, and achievement of the patients' remission period and may positively affect the quality of life. Therefore, a nutrition plan is recommended to complement existing treatments (14, 15). Nutrition may have a direct role in disease development through the provision of (anti)-inflammatory food components. In addition, it may have an indirect effect through its effects on BMI, visceral fat accumulation and contributing to the prevention of the development of chronic diseases such as diabetes and CVD as complications (16). Although there is no clear evidence on the effect of dietary plan and treatment on disease activity, various nutrients in the diet may affect disease activity by interacting with the immune system and suppressing inflammation (17). In this context, the dietary plan for RA aims to alleviate inflammation by changing the ratio of ω-6 to ω-3 fatty acids and increasing antioxidants. It is emphasized that reducing arachidonic acid (AA), a ω-6 fatty acid, is particularly important and AA is a precursor of eicosanoids. Eicosanoids are mediators of inflammation and the amount of AA released from the cell membrane can determine the intensity of inflammation (18). It has been reported that various nutrients, phenolic substances, spices such as ginger and turmeric, various vitamins and probiotics control the activity of inflammatory molecules involved in the pathophysiology of RA and thus are successful in slowing down the course of the disease (19). Since nutrients are found in combination in foods, dietary patterns are investigated rather than the effect of a single nutrient on disease. Therefore, the relationship between certain dietary patterns and health is examined instead of considering foods or nutrients alone (20).
The Mediterranean diet (MedDiet), dietary inflammatory index (DII) and its relationship with RA
The MedDiet is one of the most widely studied and well-known dietary models worldwide. The traditional MedDiet model is closely related to individuals‘ social behaviors and lifestyles (21). The Mediterranean diet (MedDiet) is increasingly recognized for its potential benefits in the treatment of rheumatoid arthritis (RA), primarily due to its anti-inflammatory and immunomodulatory properties (22). The diet, rich in fruits, vegetables, whole grains, olive oil, and fish, is thought to affect RA through several mechanisms, including modulation of inflammatory pathways, improvement of gut microbiota, and reduction of disease activity scores (23). Collectively, these mechanisms may contribute to alleviating RA symptoms and improving patients' quality of life. The effect of MedDiet and Antiinflammatory DII on RA is shown in Figures 1, 2.
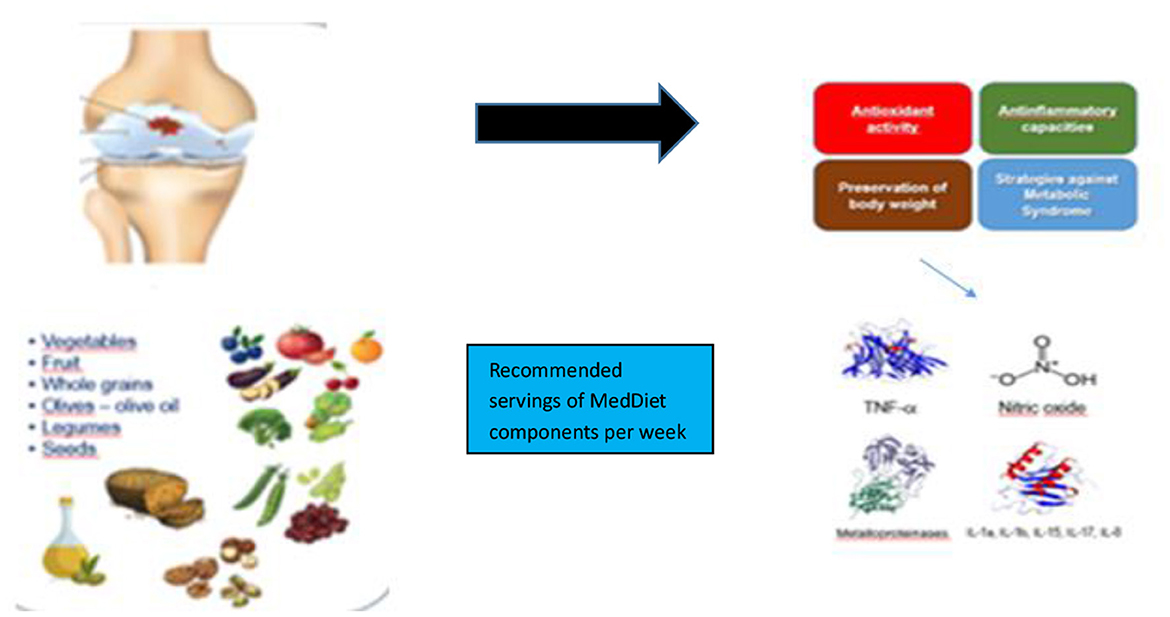
Figure 1. The effect of MedDiet on RA.
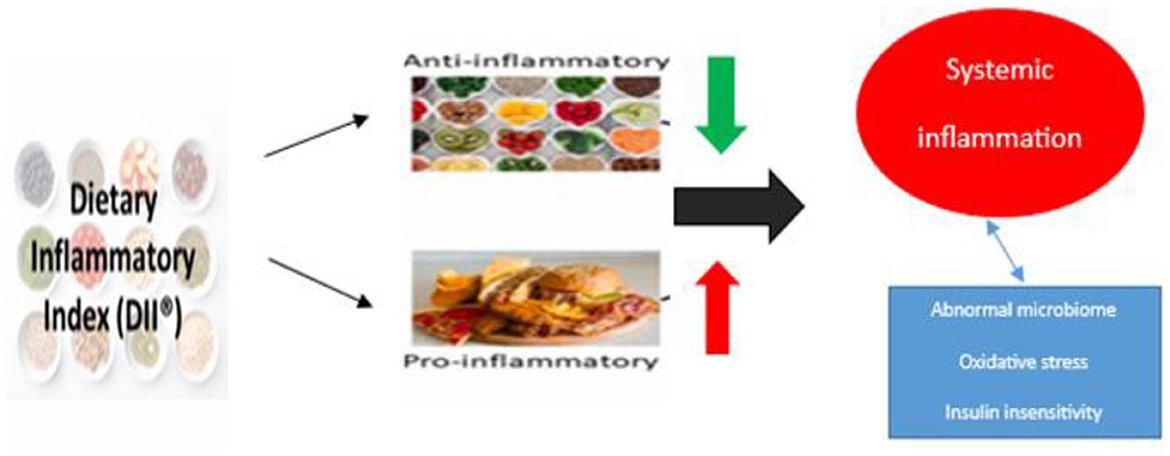
Figure 2. The effect of dietary inflammatory index on RA.
Effective mechanisms and signaling pathways of MedDiet and dietary inflammatory index on RA
MedDiet can reduce disease symptoms and improve the quality of life of individuals with RA through effective mechanisms such as suppressing inflammation, stimulating the immune system and regulating microbiota (24).
Anti-inflammatory effects
The MedDiet has been shown to affect RA-related signaling pathways, primarily through its anti-inflammatory and immunomodulatory effects. Components of the diet, such as omega-3 fatty acids, antioxidants and polyphenols, play an important role in regulating inflammatory pathways central to the pathogenesis of RA. These dietary components can influence the expression of pro-inflammatory genes and the activity of immune cells. Thus, they can potentially reduce disease activity and improve patient outcomes (25). In addition, omega-3 fatty acids, antioxidants and polyphenols in MedDiet content may reduce the inflammatory response in RA patients by down-regulating pro-inflammatory gene expression. MedDiet adherence has been reported to be associated with decreased CRP levels, a marker of inflammation, and reduced disease activity scores (DAS28) in RA patients (26). MedDiet is rich in omega-3 polyunsaturated fatty acids (PUFAs), which regulate the function of lymphocytes and monocytes, key players in the immune response. These fatty acids can inhibit the arachidonic acid cascade by reducing the production of pro-inflammatory eicosanoids (27). The antioxidants in the MedDiet, such as those found in fruits, vegetables and nuts, have powerful anti-inflammatory properties. They may inhibit NF-kB activity, a critical transcription factor in the inflammatory response, and thus reduce inflammation in RA (28). MedDiet is also high in phenolic substances as it contains fruits and vegetables and can reduce oxidative stress. These compounds can scavenge ROS, and because they have several hydroxyl groups, polyphenols can neutralize free radicals by giving them a hydrogen atom, thus polyphenols strengthen the endogenous antioxidant defense system (29).
Modulation of the gut microbiota
The MedDiet can influence the composition of the gut microbiota, which plays an important role in immune system regulation. High adherence to the MedDiet has been associated with a healthier gut microbiota profile characterized by a reduction of proinflammatory bacteria such as Prevotella copri. This gut microbiota modulation is thought to contribute to the reduced disease activity observed in RA patients following the MedDiet (30). In addition, MedDiet may also affect the immune system by acting as an epigenetic regulator. It affects the gastrointestinal epithelial barrier and mucosal immune system, which are important in the pathogenesis of autoimmune diseases such as RA. Components such as curcumin and capsaicin found in spices, which are an integral part of the MedDiet, have been shown to regulate oxidative stress and inflammation by blocking NF-kB and cyclooxygenase 2 pathways (31). Among the factors that play a key role in the pathogenesis of RA are the reactions of leukocytes and proinflammatory cytokines such as TNF-a. In addition, cytokines increase the production of CRP by the liver, which is a strong indicator of synovial inflammation (32). In addition, ROS contribute to the development of joint damage in RA. These compounds cause destruction of hyaluronic acid and damage membrane function by oxidation of collagen, proteoglycans, protease inhibitors and membrane fatty acids (33).
Improvement in disease activity and quality of life
It reported that RA patients who adhered to the MedDiet experienced significant improvements in disease activity scores, physical function and quality of life. The MEDRA study found that patients on the MedDiet had better physical function and quality of life compared to those following standard dietary guidelines (34). The effect of the MedDiet in reducing RA disease activity is also supported by findings showing a correlation between higher MedDiet adherence scores and lower DAS28 scores. It has been emphasized that MedDiet adherence is associated with a decrease in DAS28 in RA patients, indicating that the diet may positively affect disease activity scores (35).
Potential for disease prevention
Longitudinal studies suggest that adherence to the MedDiet may reduce the risk of developing RA. This protective effect is partly mediated by reductions in BMI and CRP levels, emphasizing the role of diet in preventing the onset of RA (36). It has been reported that there is an inverse relationship between the Mediterranean Adherence Score and RA risk and that high adherence to the MedDiet reduces the risk of RA development by 21% compared to low adherence (37). On the contrary, it has also been reported that the Mediterranean diet has no significant protective effect on the risk of RA development (38). In a case-control study, it was reported that MedDiet had no protective effect on the risk of RA development in individuals followed for a period of 7 years before the onset of RA symptoms (39). It has been reported that there is no association between the Mediterranean diet and the risk of RA development. However, it has been emphasized that it can provide an improvement in the clinical symptoms of RA, including disease activity, inflammatory markers and physical function (26).
A diet low in (pro-inflammatory) foods and nutrients such as refined grains, red meat, trans fatty acids, saturated fatty acids, omega-3 fatty acids, monounsaturated fatty acids, antioxidants, phytochemicals, flavonoids, and vitamin D is low in DII, while a diet rich in foods and nutrients such as fruits containing proteolytic enzymes such as papain and bromelain (papaya, mango, pineapple), ginger, turmeric, black pepper, green tea, and legumes is high in DII (anti-inflammatory) (40). These nutrition approach work through several mechanisms, including reducing systemic inflammation, regulating gut microbiota and improving overall nutritional status, which collectively contribute to alleviating RA symptoms (41).
Food intake and pathways of inflammation
Anti-inflammatory diets are rich in polyunsaturated fatty acids, polyphenols and antioxidants, which have been shown to reduce inflammation and oxidative stress, important contributors to RA pathology (42). Certain nutrients, such as omega-3 fatty acids found in fish oil, have been associated with reduced production of pro-inflammatory eicosanoids, leading to reduced joint pain and swelling (18). Higher intakes of micronutrients such as vitamin C, niacin and magnesium have been linked to lower disease activity scores in RA patients, suggesting their role in regulating inflammatory responses (43). Increased intake of cereal fiber has been associated with a decreased prevalence of RA, and DII has been shown to mediate this relationship, emphasizing the importance of dietary fiber in the management of RA due to its anti-inflammatory effects (44). While consumption of oily fish is associated with suppression of inflammation and lower disease activity and fatigue in RA patients, consumption of processed meat has been reported to have the opposite effect (45). Monounsaturated and polyunsaturated fatty acids in the anti-inflammatory diet are thought to prevent tissue damage and reduce inflammation (46). Se, an antioxidant mineral, has been reported to have a suppressive effect on inflammation by scavenging ROS and increasing glutathione peroxidase (GPx) enzyme activity (47).
Modulation of gut microbiota and metabolism
Dietary interventions can alter the gut microbiome, which in turn affects systemic inflammation. Anti-inflammatory diet has been shown to alter the composition of the gut microbiota and metabolome, which is associated with pain response in RA patients. The presence of certain gut microbes such as Akkermansia, which are enhanced by anti-inflammatory diets, may be linked to the production of short-chain fatty acids with anti-inflammatory properties (48). Furthermore, most dietary fiber is fermented by intestinal bacteria and thus microbial metabolites lead to the production of short-chain fatty acids (SCFAs). SCFAs have been shown to contribute to the gut microbiota (49). Reduced dietary fiber intake and increased fat and sugar intake in Western diets have been shown to contribute to gut microbial dysbiosis by depleting specific bacterial taxa of the gut microbiota. It has been emphasized that microbial dysbiosis in the gut promotes severe immunological dysfunctions that may contribute to the immune imbalance observed in RA (50). In this context, it has been suggested that the onset and severity of clinical arthritis symptoms may be reduced depending on gut microbiota composition, which may be affected by dietary fiber supplementation in RA diseases (51).
Dietary patterns and disease activity
An anti-inflammatory diet high in fruits, vegetables, whole grains and healthy fats has been associated with reduced disease activity and improved disease manifestations in RA (52). It shows that adherence to anti-inflammatory dietary patterns can lead to significant improvements in pain, joint swelling and overall quality of life in RA patients (1). Dietary Inflammatory Index (DII) scores show that diets with lower inflammatory potential are associated with reduced disease activity scores in RA patients (53). Omega-3 fatty acids, one of the anti-inflammatory dietary components, have been reported to reduce morning stiffness and the number of tender and swollen joints in patients with RA (54). In a review study, it was reported that 2.1–9.1 g/day omega-3 supplementation reduced the pain level in patients with RA (55). After anti-inflammatory dietary intervention, it was reported that RA had a positive effect on disease activity score and joint findings (such as pain, swelling, stiffness) and CRP level (56). In a case-control study in RA patients, it was reported that the group consuming 2.36 mg/day n3-fatty acid-enriched foods for 10 weeks showed a significant improvement in clinical findings such as disease activity, pain and fatigue compared to the control group (57). While evidence supports the beneficial role of anti-inflammatory diets in managing RA, it is important to consider variability in individual responses to dietary interventions. Factors such as basic dietary habits, genetic predispositions, and current gut microbiota composition may influence the efficacy of dietary changes.
Signaling pathways for the effects of an dietary inflammatory index on RA
The signaling pathways involved in the effect of an anti-inflammatory diet on RA are complex and multifaceted and involve various molecular and cellular mechanisms. An anti-inflammatory diet rich in nutrients with antioxidant properties has been shown to reduce disease activity and improve symptoms in RA patients. This dietary approach affects several important signaling pathways, including NF-κB, JAK/STAT and the cholinergic anti-inflammatory pathway. These pathways play important roles in regulating inflammation and immune responses in RA (58).
NF-κB signaling pathway
NF-κB is a critical transcription factor involved in the regulation of genes responsible for inflammation and immune responses. Inhibition of the NF-κB pathway is seen as a therapeutic target in RA as it can reduce the expression of pro-inflammatory cytokines and other mediators of inflammation. Nutraceuticals and dietary components that inhibit NF-κB activation can potentially alleviate RA symptoms by reducing inflammation (59). Polyphenols in the anti-inflammatory diet have been reported to increase NF-κB phosphorylation and down-regulate AMPK phosphorylation (60). The abnormal NF-κB signaling pathway in RA may cause inflammation. Anti-inflammatory diet significantly decreases RAW 264.7 inflammatory activity, nitric oxide production, PGE2, proinflammatory cytokines (TNF-α, IL-1β and IL-6) and PTGES2 in RAW 264.7 macrophages. This mechanism leads to decreased phosphorylation of NF-κB, a transcription factor that modulates inflammatory proteins including JNK, ERK1/2 and p38, downregulating the MAPK signaling pathway (61). It has also been emphasized that phenolics, one of the anti-inflammatory diet components, significantly reduce the protein expression of COX-2, iNOS and IL-1β and inhibit the PI3K/AKT/NFκB pathway, which is closely linked to RA (62).
JAK/STAT signaling pathway
The JAK/STAT pathway is activated by various cytokines, including interleukins and interferons, which are involved in the inflammatory processes of RA. Anti-inflammatory diets can regulate this pathway by affecting the expression of cytokines and their receptors, thereby reducing inflammation and disease activity. Some anti-inflammatory cytokines such as IL-4 and IL-10 also activate the JAK/STAT pathway, emphasizing the complexity of its regulation in RA (63). Flavonoids, a component of the anti-inflammatory diet, are involved in the regulation of Janus kinase (JAK) signal transducer and activator of transcription (STAT) [(Janus kinase (JAK)-signal transducer and activator of transcription (STAT); JAK STAT)] signaling pathways (64). Zinc is thought to play a role in modulation of the NF-kB signaling pathway through A20 zinc finger and OS attenuation, decreasing ROS levels and reducing chronic inflammation by preventing NF-kB activation. A20 up-regulates A20 expression in response to various stimuli such as ROS, TNF-α and IL-1b and has been reported to act as an important inhibitor of NF-kB activation contributing to the down-regulation of inflammation (65).
Cholinergic anti-inflammatory pathway (CAP)
The cholinergic anti-inflammatory pathway (CAP) is known as a classic neuroimmune pathway consisting of the vagus nerve, acetylcholine (ACh), the main neurotransmitter of the vagus nerve, and its receptors. This pathway can activate and regulate the activities of immune cells, inhibit cell proliferation and differentiation, and suppress cytokine release, thus playing an anti-inflammatory role (66). This mechanism is associated with acetylcholine's ability to suppress the release of pro-inflammatory cytokines through nAChR activation. Vagus nerve stimulation (VNS) has been shown to activate CAP leading to reduced systemic inflammation and improvement of RA symptoms (67). CAP activates nAChRs to suppress pro-inflammatory cytokine release, a pathway that plays an important role in the modulation of inflammation in RA, In particular, it interacts with α7nAChR to reduce inflammation and improve clinical outcomes (68). The cholinergic anti-inflammatory pathway regulates the proliferation and differentiation activities of various immune cell subsets through peripheral nerve communication with immune cells. This pathway represents a potential target for the treatment of autoimmune diseases such as rheumatoid arthritis, characterized by marked inflammation and decreased vagal tone (69). RA is widely recognized as a disease driven by CD4+ T cells. As an important component of innate immunity, macrophages also contribute significantly to the immune abnormalities associated with RA. Manipulating CAP in immune cells is seen as a viable way to treat RA (70). This is because the cholinergic anti-inflammatory pathway (CAP) has been identified as an important aspect of neuro-immune regulatory feedback and the interaction between acetylcholine and the alpha 7 nicotinic acetylcholine receptor (α7nAChR) underlies this signaling. Consistent with its immunomodulatory functions, α7nAChR is densely expressed by immune cells and CAP activation greatly affects the differentiation and function of α7nAChR-expressing immune cells (71).
Cytokine signaling and iNOS regulation
Proinflammatory cytokines such as IL-1, TNF-α and IL-6 can stimulate ROS production through activation of various cellular pathways. Excessive ROS production leads to oxidative stress and cellular damage and both endogenous and exogenous antioxidants can reduce the inflammatory response and ROS production by regulating cytokine production and activity. Antioxidants scavenge ROS and protect cells from oxidative damage, thus alleviating cytokine-induced inflammation and maintaining redox balance (72). Cytokines such as TNF-α, IL-1 and IL-6 are the main mediators of inflammation in RA. Dysregulation of cytokines plays a role in various diseases, especially autoimmune disorders. In RA, abnormal production or signaling of proinflammatory cytokines such as TNF-α and IL-6 contribute to chronic inflammation and tissue damage and are considered good targets for dietary interventions (73, 74). The cytokine signaling network regulating iNOS includes pathways such as IFN and IL-10, which are upregulated in RA synovium, while the TGF-β pathway is downregulated. The transcription factor STAT1 and the iNOS-interacting protein RAC2 are consistently upregulated in RA, indicating that they are involved in the regulation of NO production and chronic inflammation. iNOS regulation by cytokines is crucial in RA as it contributes to inflammation and tissue damage. Anti-inflammatory diets may reduce nitric oxide production and inflammation by affecting cytokine and iNOS expression (75).
Dietary impact on inflammatory markers
It has been shown that an anti-inflammatory diet can lead to a reduction in disease activity scores (DAS-28) and improve quality of life in RA patients (76). Nutrients such as iron, vitamin C, niacin and magnesium, which are generally higher in anti-inflammatory diets, have been associated with reduced inflammation and improved clinical outcomes in RA (77). An anti-inflammatory diet for patients with rheumatoid arthritis may be effective in improving the symptoms of the disease by reducing gene expression of markers such as IL-1, IL-6 and TNF-α, which are effective in the inflammation processes of RA (78). It has been emphasized that Se intake improves some disease states in RA patients, such as alleviating pain, reducing the number of tender joints and shortening the duration of morning stiffness (79). In a study, it was shown that there was a weak but significant relationship between DII scores and RA disease activity. DAS-28 scores of patients consuming an anti-inflammatory diet were found to be lower compared to those consuming a proinflammatory diet (80). In a case-control study examining the effect of antioxidant minerals on rheumatoid arthritis, it was observed that the patient group had significantly low intake and low plasma concentration of zinc mineral. As a result, it was suggested that zinc deficiency in rheumatoid arthritis patients decreased the activity of antioxidant enzymes (superoxide dismutase and glutathione peroxidase) and increased OS (81). In a single-blind, randomized, crossover study on patients with RA, after a 1-month washout period, the groups were crossed and intervention and control diets were administered again for 10 weeks. AD (3–4 times/week fish (mainly salmon), 1–2 times/week legumes and potatoes, whole grains, fruits (pomegranate, blueberries), vegetables, low-fat milk, yogurt, oil seeds, probiotic juices and spices) was used as intervention diet. Disease Activity Score 28-Erythrocyte Sedimentation Rate (DAS28-ESR) was found to be lower after the intervention period compared to the control period. However, no significant difference was found between the intervention and control periods in terms of DAS28-ESR (65).
Although anti-inflammatory diet shows promise in the management of RA, it is important to consider the complexity of the disease and individual variability in response to dietary interventions. The interaction between different signaling pathways and the impact of diet on these pathways requires further research to develop comprehensive dietary guidelines for RA patients. In addition, the potential of dietary interventions to complement pharmacological treatments and improve overall quality of life in RA patients emphasizes the need for continued research in this area.
Some studies on the relationship between MedDiet and dietary inflammatory index with RA
The MedDiet can reduce RA symptoms by suppressing inflammation, altering the lipid profile, increasing antioxidant levels and changing the microflora of the gut (82). The American College of Rheumatology conditionally recommends the MedDiet for RA management because of its potential to improve physical function, reduce joint swelling, and relieve pain (83). In one study, patients with RA were given MedDiet for 2 weeks and significant improvements were found in pain score and health assessment score (84). In another study, it was reported that compliance with MedDiet led to a decrease in disease activity (85). A 12-week randomized study in patients with RA showed a decrease in disease activity, improvement in physical function and increase in vitality as a result of MedDiet intervention (86). In another study, high intake of monounsaturated fatty acids due to MedDiet intervention was found to be a determinant of disease remission in patients with RA (87). In a randomized controlled trial, MedDiet was found to have positive effects on disease activity in RA (88), while in contrast, another study on women with RA found no significant association between MedDiet adherence and RA risk (86). MedDiet has also been associated with lower levels of depression, a common comorbidity in RA patients, due to its anti-inflammatory properties (89). In a randomized clinical trial, patients with RA were divided into MedDiet+dynamic exercise program (DEP), DEP only, MedDiet only, and control group. It was reported that health-related quality of life increased by 15 points in the AD+DEP and DEP groups and increased by 3.5 points in the MedDiet group, while a decrease of 4.6 points was observed in the control group (90). In another study, it was reported that ellagic acid, one of the phenolic acids found in pomegranate, decreased inflammation (91). The anti-inflammatory effects of pomegranate and its products (extract and juice) are reported to be mediated through inhibition of cell signaling pathways, including suppression of cyclo-oxygenase-2 and inducible nitric oxide expression, inhibition of NF-κB activation and inhibition of phosphorylation of MAPK proteins (92). In a case-control study, the intervention group received 2 capsules of 250 mg POMx and the control group received 2 capsules of 250 mg cellulose daily for 8 weeks. Compared to the placebo group, those who received pomegranate extract (POMx) supplementation significantly reduced the DAS28 score, which may be associated with a reduction in the number of swollen and tender joints, pain intensity and ESR levels. It was also reported that POMx reduced HAQ score and morning stiffness and increased GPx concentrations (1). In another study, it was suggested that gut microbiota plays a role in the pathogenesis of RA. It was found that POMx could change the gut microbiota and lead to health benefits (93). Despite positive findings, some studies have reported that there is no significant relationship between MedDiet and RA disease activity. One study found no significant difference in disease activity between different levels of MedDiet adherence (94). Another study indicated that MedDiet may have a weak but significant effect in controlling disease activity, but the evidence was not strong enough to provide specific dietary recommendations for RA management (86). There is further evidence of the effects of MedDiet on RA outcomes. In a 3-month randomized controlled trial in RA patients, a MedDiet-based intervention improved markers of disease activity, including CRP and ESR, and the MedDiet group showed significant improvements in physical function and health-related quality of life compared to the control group (95). Another randomized controlled trial, the MEDRA study, found greater improvements in physical function and quality of life in RA patients on the MedDiet (96). MedDiet may also play a role in primary prevention of RA. A prospective cohort study found that higher adherence to the MedDiet was associated with a reduced risk of RA, especially among smokers. This suggests that the MedDiet may attenuate the proinflammatory effects of smoking, a known risk factor for RA (97). The protective effects of the MedDiet on RA risk may be mediated through its anti-inflammatory properties. MedDiet components such as olive oil, fish and antioxidants have been shown to regulate inflammatory pathways and reduce the production of proinflammatory cytokines, which are central to RA pathogenesis (41).
A study using NHANES data (1999–2018) found that higher DII levels were associated with an increased risk of anemia in RA patients, suggesting that dietary inflammation may exacerbate RA-related complications (98). A case-control study found that individuals with the highest DII scores, indicating a more proinflammatory diet, had more than three times the risk of developing RA compared to those with the lowest scores (55). A study analyzing data from NHANES 2003–2018 found that adherence to a healthy and anti-inflammatory diet characterized by a low DII score was associated with reduced all-cause mortality in RA patients. This suggests that dietary changes may be a strategy to improve long-term health outcomes in RA (99). High DII scores were positively associated with SII and NLR in RA patients. It has been stated that this may indicate that a pro-inflammatory diet may exacerbate systemic inflammation (65). In a cross-sectional study, it was determined that CRP and disease activity scores were significantly lower in patients with RA who consumed fish twice a week or more frequently than those who consumed fish never or once a month or less (100). In a study examining RA risk with spices, another important component of an anti-inflammatory diet, it was reported that consumption of 1.5 g/day ginger for 3 months reduced the risk of disease activity and CRP level compared to the control group (101). In another study, it was reported that consumption of 2 g/day cinnamon for 2 months significantly improved disease activity scores and reduced the number of swollen joints compared to the placebo group (102). Another study found that consumption of 100 mg/day saffron for 3 months improved disease activity and joint pain compared to the control group (103). B6, another antioxidant vitamin, is associated with the risk of rheumatoid arthritis (104). In a study, circulating PLP was found to be inversely correlated with C-reactive protein (CRP), erythrocyte sedimentation rate, pain level, morning stiffness and disability score in RA patients, and low vitamin B6 intake was associated with high inflammation (105). In a meta-analysis study, RA patients were shown to have low serum Zn concentrations compared to healthy controls (106). In RA patients, low plasma zinc levels can be attributed to a change in zinc homeostasis that triggers an acute inflammatory response and removes zinc from plasma to the liver. This process is mediated by IL-1b through nitric oxide induction and IL-6 upregulating ZIP14 antibody in the liver, which can cause zinc sequestration and redistribution, leading to an inflammatory response (107). In a study by Rajaee et al. (108) a statistically significant inverse relationship was observed between serum Zn levels and DAS28 score. In another study, it was reported that the activity of SOD and GPx enzymes, which are important for the antioxidant defense system, was significantly lower in the RA group compared to the control group (109). It has been observed that consumption of dietary fiber, another important component of the anti-inflammatory diet, increases the dietary DDI index and shows a significant inverse correlation with the incidence of RA (110). In a study, it was found that RA patients who were fed a diet rich in dietary fiber for 3 years had a significant decrease in DAS28 scores and an increase in quality of life assessed by HAQ and SF-36 health questionnaires compared to control patients (111).
Some studies examining the effects of Mediterranean Type and Anti-Inflammatory Nutritional Therapy on the risk of RA development and disease symptoms are presented in Table 1.
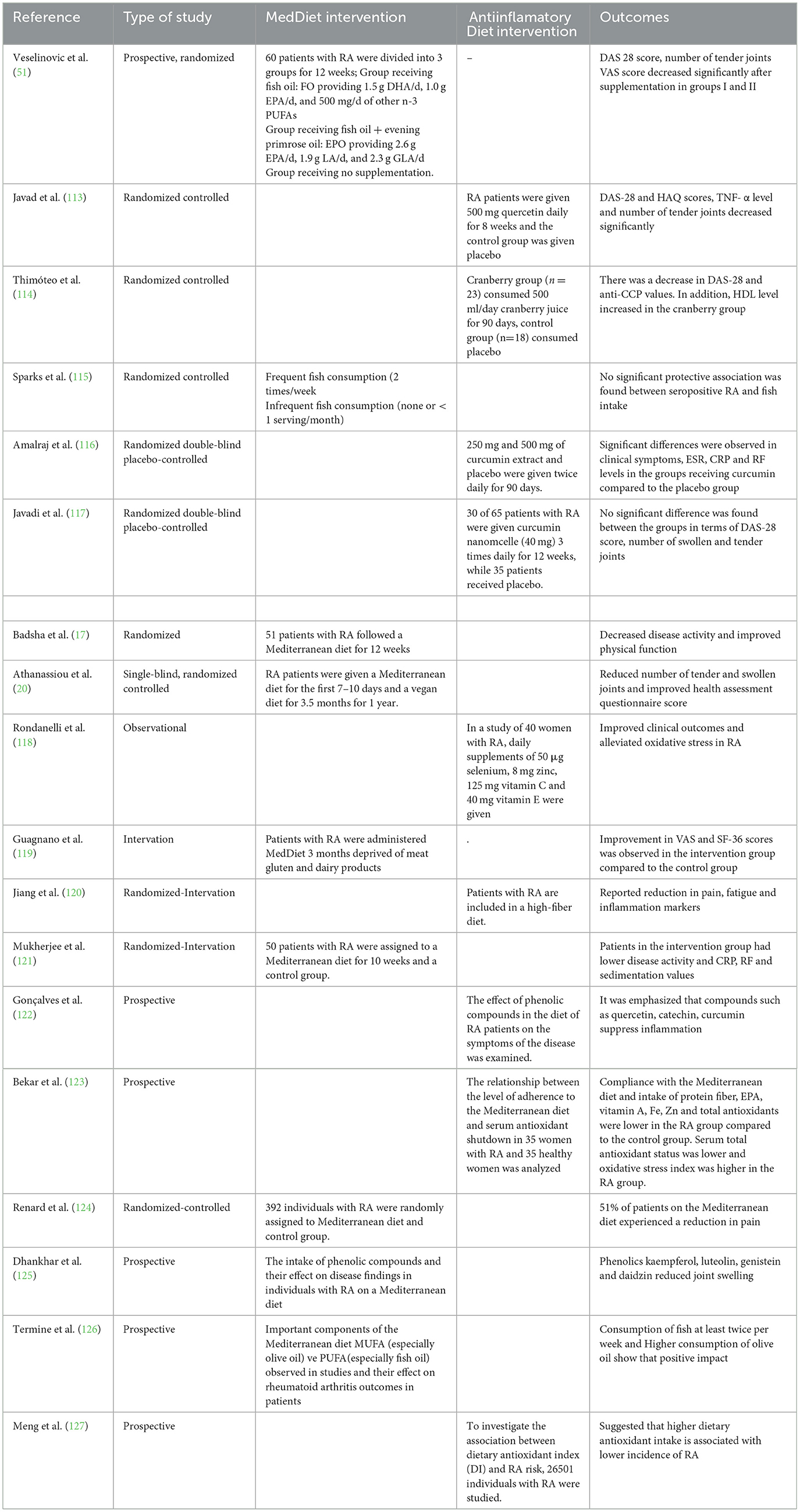
Table 1. Some studies on Mediterranean and anti-inflammatory dietary interventions in the treatment of RA.
Conclusions
Rheumatoid arthritis (RA) is an autoimmune, inflammatory, progressive disease that results in joint damage and has an unknown cause. Although nutritional therapy affects the risk of developing RA, it can improve clinical and biochemical symptoms (such as ERS, CRP) such as disease activity, morning stiffness, joint pain, and fatigue in individuals diagnosed with RA (112).
While The Mediterranean diet and its anti-inflammatory properties show promise in managing RA, it is important to consider that dietary interventions alone may not be sufficient for all patients. The complexity and multifactorial nature of RA requires a comprehensive approach that includes lifestyle modifications as well as pharmacologic therapies. Many studies are observational or have small sample sizes. Therefore, findings may not be generalizable to all populations. In addition, the lack of standardized tools to assess adherence to the MedDiet and DII across studies may contribute to inconsistencies in results. Some studies have suggested significant improvements in disease activity and quality of life, while others have found no significant effect.
Mediterranean diet and anti-inflammatory eating habits, another aspect of the Mediterranean diet may be effective in reducing the risk and symptoms of the disease by reducing inflammatory markers or increasing antioxidant defenses. Since drug therapy is costly and causes side effects in patients, dietary therapy should be supported. In addition, patients' dietary habits, nutrient and nutrient intakes, biochemical findings, physiological findings, physical activity level and quality of life level should be evaluated in detail and individualized nutrition plans may be beneficial in RA patients (128). In addition, although beneficial effects of MedDiet and anti-inflammatory diet have been shown, individual responses may vary and further research is needed to fully understand the mechanisms and optimize dietary recommendations for RA patients.
Limitations
While this review provides an insight into the potential role of nutrition in the management of this complex condition, it is also important to recognize certain limitations of the research. First of all, there are very few studies investigating the direct effects of dietary patterns in the treatment of RA. While the majority of studies show a positive effect on RA, it is difficult to determine precisely which dietary intervention is effective on specific patient subgroups or specific symptoms. There is also considerable heterogeneity between different studies, as study designs, methodologies, and number of patients vary greatly. It is therefore difficult to generalize from the results. It is difficult to establish a link between different dietary dietary models and RA, which address hormonal, genetic, immune and environmental factors related to the development of the disease, primarily because dietary model studies in humans unfortunately do not delve deeply into these issues. Furthermore, experimental studies are mostly in vivo, in vitro and in vitro studies and human studies are scarce. Therefore, it is difficult to generalize the results to the general population and this is a limiting factor of this study.
Future perspective
There are not enough well-designed randomized controlled trials in the scientific literature to assess the short-term and long-term impact of dietary plans on the onset, progression or treatment of RA. There are not many studies examining the effect of different dietary interventions on RA. Future research should focus on improving the bioavailability of dietary patterns in the treatment of RA and during attack periods. In addition, larger and longer clinical trials are needed to identify well-defined endpoints, to clarify the patients who will benefit from dietary intervention, and to fill the gaps in the literature on disease dietary modifications and their use in the clinic. This review is promising in terms of bridging the gap between nutrition and RA, raising awareness, and the relevance and applicability of the observed results.
Author contributions
BA: Writing – review & editing. NS: Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Bustamante MF, Agustín-Perez M, Cedola F, Coras R, Narasimhan R, Golshan S, et al. Design of an anti-inflammatory diet (ITIS diet) for patients with rheumatoid arthritis. Contemp Clin Trial Commun. (2020) 17:100524. doi: 10.1016/j.conctc.2020.100524
2. Mahan LK, Raymond JL. Krause Besin ve Beslenme Bakim Süreci. Ankara: Ankara Nobel Tip Kitabevleri. (2019)
3. Tedeschi SK, Frits M, Cui J, Zhang ZZ, Mahmoud T, Iannaccone C, et al. Diet and rheumatoid arthritis symptoms: survey results from a rheumatoid arthritis registry. Arth. Care Res. (2017) 69:1920–1925. doi: 10.1002/acr.23225
4. Sahebari M, Ayati R, Mirzaei H, Sahebkar A, Hejazi S, et al. Serum trace element concentrations in rheumatoid arthritis. Biol Trace Elem Res. (2016). 171:237–245. doi: 10.1007/s12011-015-0501-6
5. Bäcklund R, Drake I, Bergström U, Compagno M, Sonestedt E, Turesson C. Diet and the risk of rheumatoid arthritis–A systematic literature review. Seminar Arthritis Rheumat. (2023) 58:152118. doi: 10.1016/j.semarthrit.2022.152118
6. Derrien M, Veiga P. Rethinking diet to aid human–microbe symbiosis. Trends Microbiol. (2017) 25:100–12. doi: 10.1016/j.tim.2016.09.011
7. Riaz R, Younis W, Uttra AM, Malik MNH, Manzoor W, Qasim S, et al. Anti-arthritic and anti-inflammatory activity of linalool against formaldehyde and complete Freund's adjuvant induced arthritis in rats. Biochem Biophys Res Commun. (2025) 776:151462. doi: 10.1016/j.bbrc.2025.151462
8. Carocho M, Ferreira IC. A review on antioxidants, prooxidants and related controversy: natural and synthetic compounds, screening and analysis methodologies and future perspectives. Food Chem Toxicol. (2013) 51:15–25. doi: 10.1016/j.fct.2012.09.021
9. Schroeder BO, Bäckhed F. Signals from the gut microbiota to distant organs in physiology and disease. Nat Med. (2016) 22:1079–89. doi: 10.1038/nm.4185
10. Aksu MB, Öney B. Romatoid artrite güncel beslenme yaklaşimlari. Curr Perspect Health Sci. (2023) 4:96–103. doi: 10.58208/cphs.1261860
11. Schioppo T, Hoxha M, Iodice S, Pergoli L, De Lucia O, Murgo A, et al. Ab0141 the role of air pollution on extracellular vesicles as a potential pro-inflammatory stimulus in rheumatoid arthritis. Ann Rheum Dis. (2019) 78:1529. doi: 10.1136/annrheumdis-2019-eular.2180
12. Uke P, Maharaj A, Adebajo A. A review on the epidemiology of rheumatoid arthritis: An update and trends from current literature. Best Pract Res Clin Rheumatol. (2025) 39:102036. doi: 10.1016/j.berh.2025.102036
13. Wu CY, Yang HY, Luo SF, Lai JH. From rheumatoid factor to anti-citrullinated protein antibodies and anti-carbamylated protein antibodies for diagnosis and prognosis prediction in patients with rheumatoid arthritis. Int J Mol Sci. (2021) 22:686. doi: 10.3390/ijms22020686
14. Verma A, Dubey N, Agrawal A, Goyal A. Dietary, herbal and nutritional interventions for managing rheumatoid arthritis: a review. Curr Pharm Biotechnol. (2024) 25:125–32. doi: 10.2174/1389201024666230807155529
15. Dhruvi S, Honey K, Rahul P. A systemic review of treatment of rheumatoid arthritis using herbal plants. Int J Sci Res Tech. (2025) 2. Available online at: www.ijsrtjournal.com
16. Nikiphorou E, Philippou E. Nutrition and its role in prevention and management of rheumatoid arthritis. Autoimmun Rev. (2023) 22:103333. doi: 10.1016/j.autrev.2023.103333
17. Badsha, H. Role of diet in influencing rheumatoid arthritis disease activity. Open Rheumatol. J. (2018) 12:19–28. doi: 10.2174/1874312901812010019
18. Schönenberger KA, Schüpfer AC, Gloy VL, Hasler P, Stanga Z, Kaegi-Braun N, et al. Effect of anti-inflammatory diets on pain in rheumatoid arthritis: a systematic review and meta-analysis. Nutrients. (2021) 13:4221. doi: 10.3390/nu13124221
19. Nelson J, Sjöblom H, Gjertsson I, Ulven SM, Lindqvist HM, Bärebring L. Do interventions with diet or dietary supplements reduce the disease activity score in rheumatoid arthritis? A systematic review of randomized controlled trials. Nutrients. (2020) 12:2991. doi: 10.3390/nu12102991
20. Athanassiou P, Athanassiou L, Kostoglou-Athanassiou I. Nutritional pearls: diet and rheumatoid arthritis. Mediterr J Rheumatol. (2020) 31:319. doi: 10.31138/mjr.31.3.319
21. Dinu M, Pagliai G, Casini A, Sofi F. Mediterranean diet and multiple health outcomes: an umbrella review of meta-analyses of observational studies and randomised trials. Eur J Clin Nutr. (2018) 72:30–43. doi: 10.1038/ejcn.2017.58
22. van Delft MA, Huizinga TW. An overview of autoantibodies in rheumatoid arthritis. J Autoimmun. (2020) 110:102392. doi: 10.1016/j.jaut.2019.102392
23. Dürholz K, Hofmann J, Iljazovic A, Häger J, Lucas S, et al. Dietary short-term fiber interventions in arthritis patients increase systemic SCFA levels and regulate inflammation. Nutrients (2020) 12:3207. doi: 10.3390/nu12103207
24. Godos J, Guglielmetti M, Ferraris C, Frias-Toral E, Domínguez Azpíroz I, et al. Mediterranean diet and quality of life in adults: a systematic review. Nutrients. (2025) 17:577. doi: 10.3390/nu17030577
25. Berna-Rico E, Pérez-García B, Abbad-Jaime de Aragón C, Neria F, Monge D, et al. Impact of the Mediterranean Diet on Patients With Psoriasis: Protocol for a Randomized Controlled Trial. JMIR Res Protoc. (2025) 14:e64277. doi: 10.2196/64277
26. Picchianti Diamanti A, Panebianco C, Salerno G, Di Rosa R, Salemi S, et al. Impact of Mediterranean diet on disease activity and gut microbiota composition of rheumatoid arthritis patients. Microorganisms. (2020) 8:1989. doi: 10.3390/microorganisms8121989
27. Philippou E, Petersson SD, Rodomar C, Nikiphorou E. Rheumatoid arthritis and dietary interventions: systematic review of clinical trials. Nutr Rev. (2021) 79:410–28. doi: 10.1093/nutrit/nuaa033
28. Barrow M. An Overview of the NF-kB mechanism of pathophysiology in rheumatoid arthritis, investigation of the NF-kB ligand RANKL and related nutritional interventions. Autoimmun Rev. (2021) 20:102741. doi: 10.1016/j.autrev.2020.102741
29. Pu B, Gu P, Zheng C, Ma L, Zheng X, Zeng Z. Self-reported and genetically predicted effects of coffee intake on rheumatoid arthritis: epidemiological studies and Mendelian randomization analysis. Front Nutr. (2022) 9:926190. doi: 10.3389/fnut.2022.926190
30. Guo Q, Jin Y, Chen X, Ye X, Shen X, Lin M, et al. NF-κB in biology and targeted therapy: new insights and translational implications. Signal Transduct Target Ther. (2024) 9:53. doi: 10.1038/s41392-024-01757-9
31. Ding Q, Hu W, Wang R, Yang Q, Zhu M, Li M, et al. Signaling pathways in rheumatoid arthritis: implications for targeted therapy. Signal Transduct Target Ther. (2023) 8:68. doi: 10.1038/s41392-023-01331-9
32. Alunno A, Nikiphorou E, Philippou E, Daien C, Wiek D, Kouloumas M, et al. Nutrition in RMDs: is it really food for thought? Focus on rheumatoid arthritis. BMC Rheumatol. (2020) 4:1–5. doi: 10.1186/s41927-020-0113-4
33. Rosillo MA, Alarcón-de-la-Lastra C, Sánchez-Hidalgo M. (2016). An update on dietary phenolic compounds in the prevention and management of rheumatoid arthritis. Food Funct. 7:2943-2969. doi: 10.1039/C6FO00485G
34. Raad T, George E, Griffin A, Larkin L, Fraser A, Kennedy N, et al. Effects of a telehealth-delivered Mediterranean diet intervention in adults with Rheumatoid Arthritis (MEDRA): a randomised controlled trial. BMC Musculoskeletal Disorders. (2024) 25:631. doi: 10.1186/s12891-024-07742-1
35. Alawadhi, B., Alsaber, A., Shatawan, I., Al-Herz, A., Setiya, P., Saleh, K., et al. (2023). Adherence to the Mediterranean diet is associated with a reduced DAS28 index among patients with rheumatoid arthritis: Case study from KRRD. International Journal of Rheumatic Diseases, 26(12), 2430-2440. doi: 10.1111/1756-185X.14928
36. Hu P, Lee EKP, Tam LS, Wong SYS, Poon PKM, Yip BHK. Mediterranean diet and incident rheumatoid arthritis: a nine-year cohort study among UK Biobank participants. Clinical Nutrition ESPEN. (2023) doi: 10.1016/j.clnesp.2023.09.286
37. Wang J, Zhang B, Peng L, Wang J, Xu K, Xu P. The causal association between alcohol, smoking, coffee consumption, and the risk of arthritis: A meta-analysis of Mendelian randomization studies. Nutrients. (2023) 15:5009. doi: 10.3390/nu15235009
38. Malek Mahdavi A, Seyedsadjadi N, Javadivala Z. Potential effects of pomegranate (Punica granatum) on rheumatoid arthritis: a systematic review, International Journal of Clinical Practice, (2021) 75:1–12. doi: 10.1111/ijcp.13999
39. Ghavipour M, Sotoudeh G, Tavakoli E, Mowla K, Hasanzadeh J, Mazloom Z. Pomegranate extract alleviates disease activity and some blood biomarkers of inflammation and oxidative stress in Rheumatoid Arthritis patients, European Eur J Clin Nutr. (2017) 71, 92–96 doi: 10.1038/ejcn.2016.151
40. Vadell AK, Bärebring L, Hulander E, Gjertsson I, Lindqvist HM, Winkvist A. Anti-inflammatory Diet In Rheumatoid Arthritis (ADIRA)—a randomized, controlled crossover trial indicating effects on disease activity. Am J Clin Nutr. (2020) 111:1203–13. doi: 10.1093/ajcn/nqaa019
41. Abdel-Aal NM, Kamil RM, Tayel DI, Hamed RH, Ragab MM, Abd El-Azeim AS. Impact of adding Mediterranean diet to aerobic and strengthening exercise program on pain, inflammation, and muscle performance in females with rheumatoid arthritis: a randomized controlled trial. Physiother Theory Pract. (2025) 41:571–87. doi: 10.1080/09593985.2024.2358122
42. Toussirot E, Béreau M, Vauchy C, Saas P. Could sodium chloride be an environmental trigger for immune-mediated diseases? An overview of the experimental and clinical evidence. Front Physiol. (2018) 9:440. doi: 10.3389/fphys.2018.00440
43. Baygin H, Siriken F, Sargin G, Çildag S, Ozturk H, Senturk T. The relationship between dietary inflammatory index scores and rheumatoid arthritis disease activity. Reumatología Clínica. (2024) 20:305–11. doi: 10.1016/j.reuma.2024.02.001
44. Hulander E, Bärebring L, Wadell AT, Gjertsson I, Calder PC, Winkvist A, et al. Proposed anti-inflammatory diet reduces inflammation in compliant, weight-stable patients with rheumatoid arthritis in a randomized controlled crossover trial. J Nutr. (2021) 151:3856–64. doi: 10.1093/jn/nxab313
45. Fedkov D, Peine C, Khalil A, Lang F. Disease activity and fatigue in inflammatory arthritis patients with different dietary preferences: a retrospective exploratory cross-sectional study. Reumatologia. (2024) 62:161. doi: 10.5114/reum/190272
46. Uysal B, Sahin N, Kara H. Effects of nutritional status and foods consumed on inflammation and disease activity in patients with rheumatoid arthritis. Medicina. (2024) 60:1197. doi: 10.3390/medicina60081197
47. Zamani B, Taghvaee F, Akbari H, Mohtashamian A, Sharifi N. Effects of selenium supplementation on the indices of disease activity, inflammation and oxidative stress in patients with rheumatoid arthritis: A randomized clinical trial. Biol Trace Elem Res. (2024) 202:1457–67. doi: 10.1007/s12011-023-03782-1
48. Coras R, Martino C, Gauglitz JM, Cedola F, Tripathi A, Jarmusch AK, et al. (2022). Baseline microbiome and metabolome are associated with response to ITIS diet in an exploratory trial in patients with rheumatoid arthritis. Clin Transl Med. (2022) 12:e959. doi: 10.1002/ctm2.959
49. Yao Y, Cai X, Zheng Y, Zhang M, Fei W, et al. (2022). Short-chain fatty acids regulate B cells differentiation via the FFA2 receptor to alleviate rheumatoid arthritis. Br J Pharmacol. 179:4315-4329. doi: 10.1111/bph.15852
50. Levy M, Kolodziejczyk AA, Thaiss CA, Elinav E. Dysbiosis and the immune system. Nat Rev Immunol. (2017) 17:219–32. doi: 10.1038/nri.2017.7
51. Veselinovic M, Vasiljevic D, Vucic V, Arsic A, Petrovic S, Tomic-Lucic A, et al. (2017). Clinical benefits of n-3 PUFA and γ-linolenic acid in patients with rheumatoid arthritis. Nutrients. 9:325. doi: 10.3390/nu9040325
52. Gioia C, Lucchino B, Tarsitano MG, Iannuccelli C, Di Franco M. (2020). Dietary habits and nutrition in rheumatoid arthritis: can diet influence disease development and clinical manifestations? Nutrients. 12:1456. doi: 10.3390/nu12051456
53. Jandari S, Mosalmanzadeh N, Shadmand Foumani Moghadam MR, Soleimani D, Shivappa N, Hébert JR, et al. Dietary inflammatory index and healthy eating index-2015 are associated with rheumatoid arthritis. Public Health Nutr. (2021) 24:6007–6014. doi: 10.1017/S1368980021001105
54. Dawczynski C, Dittrich M, Neumann T, Goetze K, Welzel A, et al. Docosahexaenoic acid in the treatment of rheumatoid arthritis: a double-blind, placebo-controlled, randomized cross-over study with microalgae vs. sunflower oil. Clin Nutr. (2018) 37:494–504. doi: 10.1016/j.clnu.2017.02.021
55. Gao Z, Alishahi F, Faridpour A, Nezamoleslami S, Nezamoleslami S, Ghiasvand R, et al. The association between dietary inflammatory index with risk rheumatoid arthritis: a case-control study. Prostagland Other Lipid Mediat. (2024) 175:106916. doi: 10.1016/j.prostaglandins.2024.106916
56. Abdulrazaq M, Innes JK, Calder PC. Effect of ω-3 polyunsaturated fatty acids on arthritic pain: A systematic review. Nutrition. (2017) 39:57–66. doi: 10.1016/j.nut.2016.12.003
57. Aryaeian N, Shahram F, Mahmoudi M, Tavakoli H, Yousefi B, Arablou T, et al. The effect of ginger supplementation on some immunity and inflammation intermediate genes expression in patients with active Rheumatoid Arthritis. Gene. (2019) 698:179–85. doi: 10.1016/j.gene.2019.01.048
58. Wang F, Liu J. The dual anti-inflammatory and anticoagulant effects of Jianpi Huashi Tongluo prescription on Rheumatoid Arthritis through inhibiting the activation of the PI3K/AKT signaling pathway. Front Pharmacol. (2025) 16:1541314. doi: 10.3389/fphar.2025.1541314
59. Lanspa M, Kothe B, Pereira MR, Kesselman MM, Petrosky SN. A systematic review of nutritional interventions on key cytokine pathways in rheumatoid arthritis and its implications for comorbid depression: Is a more comprehensive approach required? Cureus. (2022) 14:e28031. doi: 10.7759/cureus.28031
60. Chen H, Zhang Z, Lu C, Ding Y, Huang Z, Li M, et al. Urolithin a attenuates rheumatoid arthritis by inhibiting inflammation and pyroptosis in fibroblasts via the AMPK/NF-κB signaling pathway. Int Immunopharmacol. (2025) 155:114604. doi: 10.1016/j.intimp.2025.114604
61. Jo HM, Choi IH. Anti-inflammatory activity of Akebia quinata D. extracts by inhibiting MAPK and NF-κB signaling pathways in LPS-induced RAW 2647 cells according to extraction solvents. Mol Cel Toxicol. (2025) 21:315–23. doi: 10.1007/s13273-024-00477-z
62. Yao Y., Wang J., Zhang H., Peng T., Sun Y., Zhang R., et al. Ammopiptanthus nanus (M. Pop.) Cheng f. stem ethanolic extract ameliorates rheumatoid arthritis by inhibiting PI3K/AKT/NF-κB pathway-mediated macrophage infiltration. J. Ethnopharmacol. (2025) 338:118974 doi: 10.1016/j.jep.2024.118974
63. Malemud CJ. The role of the JAK/STAT signal pathway in rheumatoid arthritis. Ther Adv Musculoskelet Dis. (2018) 10:117–27. doi: 10.1177/1759720X18776224
64. Işkin AE, Kizmaz MA, Budak F. Otoimmün Hastaliklarda Luteolin Bileşiginin Rolü. J Facul Pharm Ankara Univ. (2024) 48:1201–18. doi: 10.33483/jfpau.1459098
65. Lu Z, Xie Z, Shen K, Wu X, Feng E. Association of dietary inflammatory index with immune-inflammatory biomarkers in rheumatoid arthritis patients: results from NHANES 1999–2018. Front Nutr. (2024) 11:1353964. doi: 10.3389/fnut.2024.1353964
66. Lv J, Ji X, Li Z, Hao H. The role of the cholinergic anti-inflammatory pathway in autoimmune rheumatic diseases. Scand J Immunol. (2021) 94:e13092. doi: 10.1111/sji.13092
67. Hajiasgharzadeh K, Khabbazi A, Mokhtarzadeh A, Baghbanzadeh A, Asadzadeh Z, Adlravan E, et al. Cholinergic anti-inflammatory pathway and connective tissue diseases. Inflammopharmacology. (2021) 29:975–86. doi: 10.1007/s10787-021-00812-z
68. Bai X, Zhou B, Wu S, Zhang X, Zuo X, Li T. Gts-21 alleviates murine collagen-induced arthritis through inhibition of peripheral monocyte trafficking into the synovium. Int Immunopharmacol. (2023) 122:110676. doi: 10.1016/j.intimp.2023.110676
69. Zouali M. Pharmacological and electroceutical targeting of the cholinergic anti-inflammatory pathway in autoimmune diseases. Pharmaceuticals. (2023) 16:1089. doi: 10.3390/ph16081089
70. Pan S, Wu YJ, Zhang SS, Cheng XP, Olatunji OJ, Yin Q, et al. The effect of α7nAChR signaling on T cells and macrophages and their clinical implication in the treatment of rheumatic diseases. Neurochem Res. (2022) 1–14. doi: 10.1007/s11064-021-03480-1
71. Ye X, Ren D, Chen Q, Shen J, Wang B, Wu S, et al. Resolution of inflammation during rheumatoid arthritis. Front Cell Dev Biol. (2025) 13:1556359. doi: 10.3389/fcell.2025.1556359
72. Bhol NK, Bhanjadeo MM, Singh AK, Dash UC, Ojha RR, Majhi S et al. The interplay between cytokines, inflammation, and antioxidants: Mechanistic insights and therapeutic potentials of various antioxidants and anti-cytokine compounds. Biomed Pharmacother. (2024) 178:117177. doi: 10.1016/j.biopha.2024.117177
73. Cutolo M, Nikiphorou E. Don't neglect nutrition in rheumatoid arthritis! RMD open. (2018) 4:e000591. doi: 10.1136/rmdopen-2017-000591
74. Gul B, Anwar R, Saleem M, Noor A, Ullah MI. C assia absus-mediated upregulation of IL-4, IL-10 and downregulation of IL-1β, IL-6, TNF-α, NF-κB, IFN-γ in CFA-induced arthritis model. Inflammopharmacology. (2023) 31:1241–56. doi: 10.1007/s10787-023-01185-1
75. Dey P, Panga V, Raghunathan S. A cytokine signalling network for the regulation of inducible nitric oxide synthase expression in rheumatoid arthritis. PLoS One. (2016) 11:e0161306. doi: 10.1371/journal.pone.0161306
76. Winkvist A, Bärebring L, Gjertsson I, Ellegård L, Lindqvist HM. A randomized controlled cross-over trial investigating the effect of anti-inflammatory diet on disease activity and quality of life in rheumatoid arthritis: the Anti-inflammatory Diet In Rheumatoid Arthritis (ADIRA) study protocol. Nutr J. (2018) 17:1–8. doi: 10.1186/s12937-018-0354-x
77. Fekete M, Csípo T, Fazekas-Pongor V, Fehér Á, Szarvas Z, Kaposvári C, et al. The effectiveness of supplementation with key vitamins, minerals, antioxidants and specific nutritional supplements in COPD—a review. Nutrients (2023) 15:2741. doi: 10.3390/nu15122741
78. Prasad P, Verma S, Surbhi, Ganguly NK, Chaturvedi V, Mittal SA. Rheumatoid arthritis: advances in treatment strategies. Mol Cell Biochem. (2023) 478:69–88. doi: 10.1007/s11010-022-04492-3
79. Turrubiates-Hernández FJ, Márquez-Sandoval YF, González-Estevez G, Reyes-Castillo Z, Muñoz-Valle JF. The Relevance of Selenium Status in Rheumatoid Arthritis, Nutrients. (2020) 12:3007. doi: 10.3390/nu12103007
80. Li J, Xie X, Chen X, Xie L, Luo M, et al. Dietary habit and risk of rheumatoid arthritis: a mendelian randomization study identifying protective and risk factors. Eur J Nutr. (2025) 64:3. doi: 10.1007/s00394-024-03518-4
81. Yokokawa H, Fukuda H, Saita M, Miyagami T, Takahashi Y, Hisaoka T, et al. Serum zinc concentrations and characteristics of zinc deficiency/marginal deficiency among Japanese subjects. J Gen Family Med. (2020) 21:248–55. doi: 10.1002/jgf2.377
82. Nayebi A, Soleimani D, Mostafaei S, Elahi N, Pahlavani N et al. Association between dietary inflammatory index scores and the increased disease activity of rheumatoid arthritis: a cross-sectional study. Nutr J. (2022). 21:53. doi: 10.1186/s12937-022-00805-w
83. Everett, S. 2022 American college of rheumatology (ACR) guideline for exercise, rehabilitation, diet, and additional integrative interventions for rheumatoid arthritis. Arthr Res. (2023) 75:1629–1630. doi: 10.1002/acr.25119
84. Sundström B, Johansson I, Rantapää-Dahlqvist S. Diet and alcohol as risk factors for rheumatoid arthritis: a nested case–control study. Rheumatol Int. (2015) 35:533–9. doi: 10.1007/s00296-014-3185-x
85. Forsyth C, Kouvari M, D'Cunha NM, Georgousopoulou EN, Panagiotakos DB, Mellor DD, et al. The effects of the Mediterranean diet on rheumatoid arthritis prevention and treatment: a systematic review of human prospective studies. Rheumatol Int. (2018) 38:737–747. doi: 10.1007/s00296-017-3912-1
86. Johansson K, Askling J, Alfredsson L, Di Giuseppe, D., and & EIRA Study Group. (2018). Mediterranean diet and risk of rheumatoid arthritis: a population-based case-control study. Arthr Res Therapy. 20:1–8. doi: 10.1186/s13075-018-1680-2
87. García-Morales JM, Lozada-Mellado M, Hinojosa-Azaola A, Llorente L, Ogata-Medel M, et al. Effect of a dynamic exercise program in combination with Mediterranean diet on quality of life in women with rheumatoid arthritis. J Clin Rheumatol. (2020) 26:S116-S122. doi: 10.1097/RHU.0000000000001064
88. Raad T, George E, Griffin A, Larkin L, Fraser A, Kennedy N, et al. A randomised controlled trial of a Mediterranean Dietary Intervention for Adults with Rheumatoid Arthritis (MEDRA): Study protocol. Contemp Clin Trials Commun. (2022) 28:100919. doi: 10.1016/j.conctc.2022.100919
89. Ma L, Yuan J, Yang X, Yan M, Li Y, Niu M. Association between the adherence to Mediterranean diet and depression in rheumatoid arthritis patients: a cross-sectional study from the NHANES database. J Health Populat Nutr. (2024) 43:103. doi: 10.1186/s41043-024-00572-w
90. Asoudeh F, Dashti F, Jayedi A, Hemmati A, Fadel A, Mohammadi H. Caffeine, coffee, tea and risk of rheumatoid arthritis: systematic review and dose-response meta-analysis of prospective cohort studies. Front Nutr. (2022) 9:822557. doi: 10.3389/fnut.2022.822557
91. Lee F, Bae KH, Ng S, Yamashita A, Kurisawa M. Hyaluronic acid–green tea catechin conjugates as a potential therapeutic agent for rheumatoid arthritis. RSC Adv. (2021) 11:14285–94. doi: 10.1039/D1RA01491A
92. Rambod M, Nazarinia M, Raieskarimian F. The impact of dietary habits on the pathogenesis of rheumatoid arthritis: a case-control study, Clin Rheumatol. (2018) 37:2643–2648. doi: 10.1007/s10067-018-4151-x
93. Mahan LK. Krause's Food & the Nutrition Care Process-E-Book: Krause's Food & the Nutrition Care Process-E-Book. Elsevier Health Sciences. (2016).
94. Mostafaei R, Elahi N, Moludi J, Moradi F, Solouki L, Nachvak SM, et al. Association of Mediterranean diet pattern with disease activity in the patients with rheumatoid arthritis: a cross-sectional study on Iranian patients. Clin Nutr ESPEN. (2024) 60:95–101. doi: 10.1016/j.clnesp.2024.01.012
95. Venetsanopoulou AI, Virvili A, Koletsos N, Kaltsonoudis E, Gerolymatou N, Memi TE, et al. Effectiveness of a mediterranean diet-based intervention in rheumatoid arthritis patients: a 3-month prospective study. Ann Rheumat Dis. (2024) 83:835. doi: 10.1136/annrheumdis-2024-eular.4862
96. Raad T, Griffin A, Larkin L, Kennedy N, Tierney A. The effect of a Mediterranean diet on physical function and quality of life in patients with rheumatoid arthritis–the Medra study. Ann Rheum Dis. (2022) 81:361. doi: 10.1136/annrheumdis-2022-eular.4259
97. Nguyen Y, Salliot C, Gelot A, Gambaretti J, Mariette X, Boutron-Ruault MC, et al. Mediterranean diet and risk of rheumatoid arthritis: Findings from the French E3N-EPIC cohort study. Arthr Rheumatol. (2021) 73:69–77. doi: 10.1002/art.41487
98. Song J, Zhang Y, Li A, Peng J, Zhou C, Cheng X, et al. (2024). Prevalence of anemia in patients with rheumatoid arthritis and its association with dietary inflammatory index: a population-based study from NHANES 1999 to 2018. Medicine. 103:e38471. doi: 10.1097/MD.0000000000038471
99. Wang P, Wang D, Sui J, Liu S, Kong Y, Lei H, et al. The comprehensive relationship between combined anti-inflammatory and healthy diets and all-cause mortality in rheumatoid arthritis: results from NHANES 2003–2018. Arthritis Res Ther. (2024) 26:226. doi: 10.1186/s13075-024-03462-y
100. Shishehbor F, Rezaeyan Safar M, Rajaei E, Haghighizadeh MH. Cinnamon consumption improves clinical symptoms and inflammatory markers in women with rheumatoid arthritis. J Am Coll Nutr. (2018) 37:685–90. doi: 10.1080/07315724.2018.1460733
101. Hamidi Z, Aryaeian N, Abolghasemi J, Shirani F, Hadidi M, Fallah S, et al. The effect of saffron supplement on clinical outcomes and metabolic profiles in patients with active rheumatoid arthritis: a randomized, double-blind, placebo-controlled clinical trial. Phytotherapy Res. (2020) 34:1650–8. doi: 10.1002/ptr.6633
102. Buondonno I, Rovera G, Sassi F, Rigoni MM, Lomater C, Parisi S, et al. Vitamin D and immunomodulation in early rheumatoid arthritis: a randomized double-blind placebo-controlled study. PLoS One. (2017) 12:e0178463. doi: 10.1371/journal.pone.0178463
103. Prasad AS, Bao B. Molecular mechanisms of zinc as a pro-antioxidant mediator: clinical therapeutic implications. Antioxidants. (2019) 8:164. doi: 10.3390/antiox8060164
104. Liu Y, Wang X, You M, Zheng M, Yu M, Leng X. Association between vitamin B6 levels and rheumatoid arthritis: a two-sample Mendelian randomization study. Front Nutr. (2024) 11:1442214. doi: 10.3389/fnut.2024.1442214
105. Fang J, Du X, Wang D, Liu C, Zhang H, Lin, Z. Associations of dietary niacin, vitamin B6, and folate intakes with risk of rheumatoid arthritis: an analysis using NHANES Data from 2003-2018. (2023) doi: 10.21203/rs.3.rs-3269305/v1
106. Xin L, Yang X, Cai G, Fan D, Xia Q, Liu L, et al.. Serum levels of copper and zinc in patients with rheumatoid arthritis: a meta-analysis. Biol Trace Elem Res. (2015) 168:1–10. doi: 10.1007/s12011-015-0325-4
107. Frangos T, Maret W. Zinc and cadmium in the aetiology and pathogenesis of osteoarthritis and rheumatoid arthritis. Nutrients. (2020) 13:53. doi: 10.3390/nu13010053
108. Rajaee E, Mowla K, Ghorbani A, Dargahi-Malamir M, Zarei M, Rahimikhah FA. The relationship between serum zinc levels and rheumatoid arthritis activity. Front Biol. (2018) 13:51–5. doi: 10.1007/s11515-017-1474-y
109. Fang D, Jiang D, Shi G, Song Y. The association between dietary zinc intake and osteopenia, osteoporosis in patients with rheumatoid arthritis. BMC Musculoskel Disord. (2024) 25:710. doi: 10.1186/s12891-024-07768-5
110. Wan H, Zhang Y, Ning Z, Liu M, Yang S. Associations of cereal fiber intake with rheumatoid arthritis mediated by dietary inflammatory index: insights from NHANES 2011–2020. Sci Rep. (2024) 14:2415. doi: 10.1038/s41598-024-52806-w
111. Tehsin F, Rasheed A, Hafeez U, Alam A, Nawaz AU, Khan K. Role of Diet in Influencing DAS28 Score in Rheumatoid Arthritis: Diet and DAS28 in Rheumatoid Arthritis. J Health Rehab Res. (2024) 4:1–5. doi: 10.61919/jhrr.v4i3.1581
112. Sharma P, Brown S, Sokoya EM. Re-evaluation of dietary interventions in rheumatoid arthritis: can we improve patient conversations around food choices? Rheumatol Int. (2024) 44:1409–1419. doi: 10.1007/s00296-024-05541-4
113. Javadi F, Ahmadzadeh A, Eghtesadi S, Aryaeian N, Zabihiyeganeh M, Rahimi Foroushani A, et al. The effect of quercetin on inflammatory factors and clinical symptoms in women with rheumatoid arthritis: a double-blind, randomized controlled trial. J Am Coll Nutr. (2017) 36:9–15. doi: 10.1080/07315724.2016.1140093
114. Thimóteo NSB, Iryioda TMV, Alfieri DF, Rego BEF, Scavuzzi BM, et al. Cranberry juice decreases disease activity in women with rheumatoid arthritis. Nutrition. (2019) 60:112–117. doi: 10.1016/j.nut.2018.10.010
115. Sparks JA, O'Reilly ÉJ, Barbhaiya M, Tedeschi SK, Malspeis S, et al. Association of fish intake and smoking with risk of rheumatoid arthritis and age of onset: a prospective cohort study. BMC Musculoskelet Disord. (2019) 20:1–13. doi: 10.1186/s12891-018-2381-3
116. Amalraj A, Varma K, Jacob J, Divya C, Kunnumakkara AB, Stohs SJ, et al. A novel highly bioavailable curcumin formulation improves symptoms and diagnostic indicators in rheumatoid arthritis patients: a randomized, double-blind, placebo-controlled, two-dose, three-arm, and parallel-group study. J Med Food. (2017) 20:1022–30. doi: 10.1089/jmf.2017.3930
117. Javadi M, Khadem Haghighian H, Goodarzy S, Abbasi M, Nassiri-Asl M. Effect of curcumin nanomicelle on the clinical symptoms of patients with rheumatoid arthritis: A randomized, double-blind, controlled trial. Int J Rheum Dis. (2019) 22:1857–62. doi: 10.1111/1756-185X.13688
118. Rondanelli M, Perdoni F, Peroni G, Caporali R, Gasparri C, Riva A, et al. Ideal food pyramid for patients with rheumatoid arthritis: A narrative review. Clin Nutr. (2021). 40:661-689. doi: 10.1016/j.clnu.2020.08.020
119. Guagnano MT, D'Angelo C, Caniglia D, Di Giovanni P, Celletti E, et al. Improvement of inflammation and pain after three months' exclusion diet in rheumatoid arthritis patients. Nutrients. (2021). 13:3535. doi: 10.3390/nu13103535
120. Jiang L, Shang M, Yu S, Liu Y, Zhang H, Zhou Y, et al. A high-fiber diet synergizes with Prevotella copri and exacerbates rheumatoid arthritis. Cell Mol Immunol. (2022) 19:1414–1424. doi: 10.1038/s41423-022-00934-6
121. Mukherjee MS, Han CY, Sukumaran S, Delaney CL, Miller MD. Effect of anti-inflammatory diets on inflammation markers in adult human populations: A systematic review of randomized controlled trials. Nutr Rev. (2023) 81:55–74. doi: 10.1093/nutrit/nuac045
122. Gonçalves AC, Rodrigues S, Fonseca R, Silva LR. Potential Role of Dietary Phenolic Compounds in the Prevention and Treatment of Rheumatoid Arthritis: Current Reports. Pharmaceuticals. (2024) 17:590. doi: 10.3390/ph17050590
123. Bekar C, Armagan B, Sari A, Ayaz A. Evaluation of serum total antioxidant level, nutritional status and Mediterranean diet adherence of adult women with rheumatoid arthritis: a case–control study. Br J Nutr. (2025) 133:239–245. doi: 10.1017/S0007114524003386
124. Renard D, Tuffet S, Dieudé P, Claudepierre P, Gossec L, Fautrel B, et al. Factors associated with dietary practices and beliefs on food of patients with rheumatic and musculoskeletal diseases: a multicentre cross-sectional study. Joint Bone Spine. (2025) 92:105778. doi: 10.1016/j.jbspin.2024.105778
125. Dhankhar S, Kumar J, Chauhan S, Zahoor I, Wani SN, Saini M, et al. Flavonoids and flavonoid-based nanoparticles for the treatment of arthritis. Inflammopharmacology. (2025) 33:2193-2216. doi: 10.1007/s10787-025-01722-0
126. Termine M, Davidson Z, Choi T, Leech M. What do we know about dietary perceptions and beliefs of patients with rheumatoid arthritis? A scoping review. Rheumatol Int. (2024) 44:1861–74. doi: 10.1007/s00296-024-05691-5
127. Meng Q, Dong S, Ge J, Qin C, Zhang G, Fu C, et al. Association between composite dietary antioxidant index and rheumatoid arthritis: results from NHANES 2003-2018. Int J Med Sci. (2025) 22:1184. doi: 10.7150/ijms.107332
Keywords: Rheumatoid arthritis, Mediterranean diet, anti-inflammatory, diet pattern, DIET pathway
Citation: Açıkalın Göktürk B and Sanlier N (2025) Genetic factors may load the gun, but environmental factors pull the trigger: MedDiet and DII in rheumatoid arthritis. Front. Nutr. 12:1629896. doi: 10.3389/fnut.2025.1629896
Received: 16 May 2025; Accepted: 21 August 2025;
Published: 17 September 2025.
Edited by:
Dongsheng Di, Anhui Medical University, ChinaReviewed by:
Beatrice Scazzocchio, National Institute of Health (ISS), ItalyAnil Kumar Mavi, University of Delhi, India
M. Thenmozhi, Vels Institute of Science, Technology & Advanced Studies (VISTAS), India
Copyright © 2025 Açıkalın Göktürk and Sanlier. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Büşra Açıkalın Göktürk, YnVzcmEuYWNpa2FsaW5AYW5rYXJhbWVkaXBvbC5lZHUudHI=