 Achil Tia1,2*
Achil Tia1,2* Jonas Hauser3
Jonas Hauser3 Amoin G. Konan2,4Olivier Ciclet5Yohan Grzywinski5
Amoin G. Konan2,4Olivier Ciclet5Yohan Grzywinski5 Fabio Mainardi3Gioele Visconti5
Fabio Mainardi3Gioele Visconti5 Adrien Frézal5Charlemagne Nindjin1,2
Adrien Frézal5Charlemagne Nindjin1,2- 1Unité de Formation et de Recherche Sciences et Technologies des Aliments, Université Nangui Abrogoua, Abidjan, Côte d'Ivoire
- 2Centre Suisse de Recherches Scientifiques en Côte d'Ivoire, Abidjan, Côte d'Ivoire
- 3Nestlé Institute of Health Sciences, Nestlé Research, Société des Produits Nestlé S.A., Lausanne, Switzerland
- 4Unité de Formation et de Recherche Biosciences, Université Félix-Houphouët-Boigny, Abidjan, Côte d'Ivoire
- 5Nestlé Institute of Food Safety and Analytical Sciences, Nestlé Research, Société des Produits Nestlé S.A., Lausanne, Switzerland
Background: Nutritional deficiencies are one of the main factors that affect cognitive development. In Côte d'Ivoire, although nutritional deficiencies have been reported among schoolchildren, their association with cognitive function or academic performance remains unexplored.
Objective: The objective of this study was to investigate the relationship between nutritional status, cognition, and school performance in school-aged children from Taabo, Côte d'Ivoire.
Methods: A sample of 252 schoolchildren (6–12 years) was recruited. Nutrient biomarkers were measured in blood samples, cognition (fluid intelligence) was assessed using the Raven's Colored Progressive Matrices (RCPM), and school performance was quantified based on academic results in mathematics and literature.
Results: Overall scores were 15.4 ± 4.4 for the RCPM, 6.0 ± 2.4 for mathematics, and 5.4 ± 1.8 for literature (out of a maximum of 36, 10, and 10, respectively). Most of the children had normal nutritional status, but all had inadequate plasma levels of iron, folate, thiamine, and vitamin B12. Significant correlations (p < 0.05) were found between biomarkers of iron, folate, tryptophan, calcium, potassium, and omega-3 fatty acids with cognition or school performance. In contrast, no associations were found with zinc, iodine, riboflavin, vitamin B12, or vitamin D. After adjusting for sociodemographic factors in regression models, calcium was identified as a predictor of cognitive skills (R2 = 0.3, p = 0.020; 95% CI: 8.2 × 10−6−9.3 × 105) and folate as a predictor of performance in both mathematics (R2 = 0.1, p = 0.006; 95% CI: 0.1–0.3) and literature (R2 = 0.1, p = 0.005; 95% CI: 0.1–0.2).
Conclusion: This study found high rates of B vitamins and iron deficiencies in Ivorian school-aged children. Iron, folate, tryptophan, calcium, potassium, and omega-3 fatty acid biomarkers showed promising correlations with cognition and academic performance. Further research aimed at investigating such relationships is needed.
1 Introduction
School performance is a multidimensional concept that includes educational outcomes, academic achievement, and the quality of education (1). It is often measured through examination results and test scores, which serve as primary indicators of academic success (2). In addition, cognition has been analyzed as a strong predictor of academic success among schoolchildren (3). Cognitive function, which can be divided into crystallized (acquired knowledge) and fluid intelligence (reasoning capability to drive decision making), plays a crucial role in learning, memory performance, reasoning, problem solving, and adapting to new situations, which are essential for overcoming challenges in educational settings (4). The relationship between school performance and cognitive processes has been relevant and investigated for more than a century. Studies have shown that academic achievement is related to the individual characteristics of basic cognitive processes such as information processing speed, visuospatial working memory, or fluid intelligence (5). Cognitive development is crucial for children to acquire factual knowledge, behavioral and social skills, and learning and good academic performance (6).
Cognitive development is affected by numerous factors, including nutrition. A growing body of literature indicates a connection between enhanced nutritional status and cognitive performance (7, 8). Several nutrients play crucial roles in biological processes relevant for cognition, for example, docosahexaenoic acid (DHA) and arachidonic acid (AA) are the building blocks of the brain and are involved in several metabolic and enzymatic processes in neuronal and glial cells. In total, 60% of the dry weight of the human brain is made up of these essential fatty acids (EFAs), including DHA and AA. DHA supplementation in school-aged children has been associated with increased reading and behavior in subjects that they were poorly performing (9). In addition to fatty acids, micronutrients are also important. Iron is involved in brain energy production, neurotransmitter synthesis, and myelination. Its deficiency has adverse effects on cognitive development and subsequent school achievement. A recent meta-analysis of iron supplementation in school-aged children reported a positive effect of iron supplementation on intelligence, attention, and memory (10). Zinc deficiency may also affect cognitive functions such as attention, activity, and motor development, while iodine deficiency affects the central nervous system through neurogenesis, axon and dendrite growth, and myelination alteration (11). Zinc supplementation has been shown to improve specific cognitive abilities, namely verbal intelligence quotient, in school-age children (12). In addition, B vitamins, riboflavin (B2), folate (B9), and cobalamin (B12) are also known as key nutrients associated with cognitive development. Riboflavin is involved in several biological processes, including the metabolism of carbohydrates, fats, proteins, energy production, and the metabolism of other B vitamins, such as pyridoxine and folate, and niacin (13). Folate is involved in neural stem cell proliferation and homocysteine and S-adenosylmethionine biosynthesis, while vitamin B12 has an important role in axon myelination and neuron protection from degeneration (14, 15). Any deficiency in one or multiple of these nutrients may significantly affect cognitive development and result in poor school performance. Such an impact might be even more important in the case of multiple deficiencies.
While most studies were performed in Western countries, only a limited number of studies in sub-Saharan Africa were conducted among school-aged children, which found significant correlations between micronutrients such as iron, zinc, iodine, riboflavin, folate, or vitamin B12 and better performance on cognitive tests (16–19). Further correlations were observed between serum ferritin or hemoglobin levels and cognitive scores (6). Thus, there is a need to further understand the situation regarding their impact on cognition and school performance in sub-Saharan Africa.
Specifically, in Côte d‘Ivoire, research has shown that 5.8–40% of school-aged children suffer from undernutrition, 20–39% of them from anemia and iron deficiency, and 31% of them from vitamin A deficiency (20–22). Other studies have reported significant influences of sociodemographic factors (23), fruit- and vegetable-based diets (24), and undernutrition indices such as stunting and underweight (25, 26) on school performance in school-aged children. However, despite the high prevalence of nutrient deficiencies, their association with cognition has not yet been assessed in these children. Understanding the relationship between nutrient profile and cognitive capacity, as well as school performance in Ivorian school-age children, could help to take corrective actions and promote school achievement. Therefore, the objective of this study is to investigate the association between nutritional status, cognitive abilities, and school performance among school-aged children in Côte d'Ivoire.
2 Materials and methods
2.1 Study design and area
A cross-sectional observational study design was used for this research (Figure 1). The study was conducted between January and April 2023 in seven public primary schools within the Health and Demographic Surveillance System (HDSS) of Taabo, Côte d'Ivoire. The HDSS site is located approximately 150 km northwest of Abidjan, the economic capital of Côte d‘Ivoire, and 60 km south of Yamoussoukro, the political capital. It covers an area of 980 km2 between latitudes 6°00′ and 6°20′ N and longitudes 4°55′ and 5°15′ W (Figure 2). The HDSS is predominantly rural and includes 13 main villages, over 100 small hamlets, and a small urban center called Taabo-Cité with a population of 7,514 inhabitants. The total population of the HDSS is estimated at 42,480 inhabitants under surveillance since 2013 (27). The participants for this study were from six villages (Tokohiri, Ndenou, Ahouati, Leleblé, Ahouakro, and Adikouassikro) and a small town, Taabo-Cité. The main activity of the local population is agriculture, including the cultivation of yams, bananas, maize, and cassava, as well as cash crops such as cocoa and coffee. There is also some livestock production (cattle, small ruminants, pigs, and poultry) and fishing.
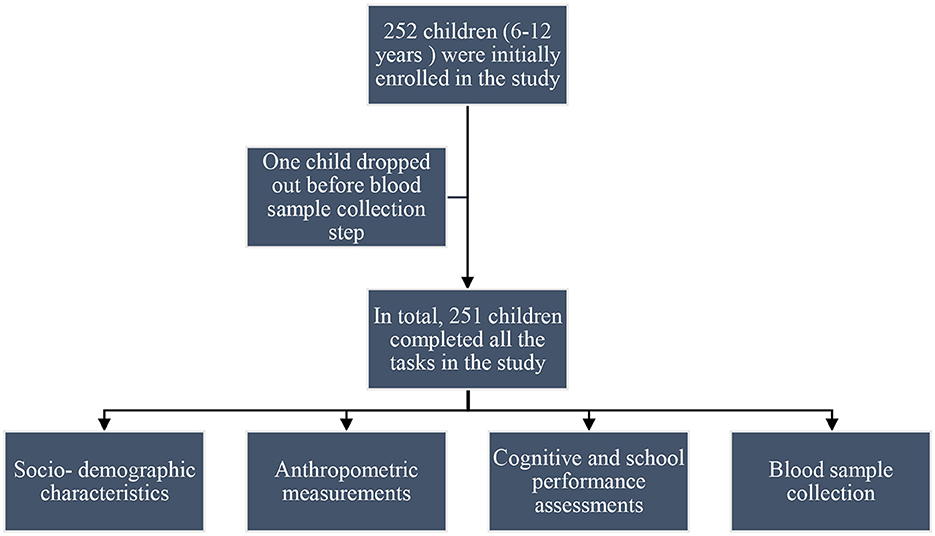
Figure 1. Flowchart of the school-based, cross-sectional observational study conducted in the Taabo Health and Demographic Surveillance System (HDSS). Data were collected at a single time point through structured interviews with children, review of school records, administration of the Raven's Colored Progressive Matrices (RCPM), and collection of blood samples for nutrient biomarker analysis.
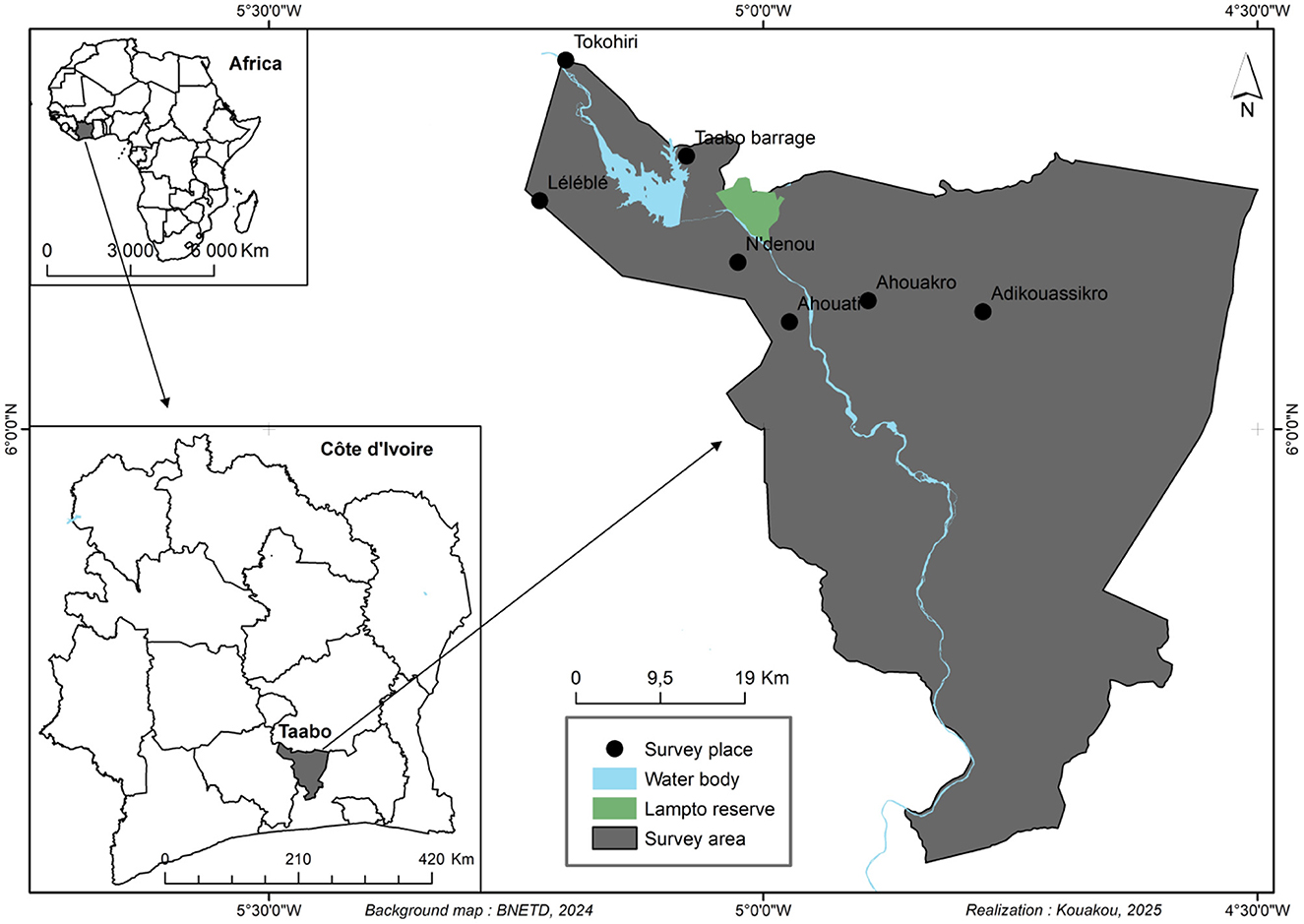
Figure 2. Map showing the study area in south-central Côte d'Ivoire within the Taabo Health and Demographic Surveillance System (HDSS).
2.2 Sample size and sampling procedure
A total of 252 school-aged children (6–12 years) were recruited for this observational study. The sample size was determined based on the population of school-aged children in public primary schools involved in the study using Yamane's formula (6), as given below.
where N is the total population of school-aged children in grades one to six (N = 681), and e is the margin of error, set at 0.05 (5%). A two-stage stratified random sampling method was used to choose the participants. In the first stage, all primary schools in the HDSS were stratified into three education sectors: the Taabo-Barrage, Taabo-EECI, and Leleble sectors. Seven schools, namely, Ahouakro Public Primary School (PPS), Tokohiri PPS, Ndenou PPS, Tokohiri PPS Ahouati PPS, N'Denou PPS, Leleble PPS, and Taabo Barrage PPS, were then randomly selected from the list of eligible public primary schools within these sectors. In the second stage, children from grades one to six were selected using a systematic random sampling technique. In each school, 36 children were selected, regardless of sex, and included in the study. Before sampling, children who were ill, as well as those participating in nutritional intervention programs or outside the required age range, were excluded from the sampling list.
2.3 Ethical considerations
Ethical approval for this study was obtained from the National Committee on Ethics in Life Sciences and Health under the Ministry of Health, Public Hygiene and Universal Health Coverage of Côte d'Ivoire (N/Ref: 118-22/MSHPCMU/CNESVS-kp). In addition, written informed consent was obtained from the parents or legal guardians of all participants.
2.4 Sociodemographic data collection
Sociodemographic information was collected through face-to-face interviews using a semi-structured questionnaire. Data collected included participants' age and sex, household size, and the education and occupation of their parents or guardians. School information was also collected.
2.5 Anthropometric measurements
Height and weight were collected from each child in accordance with the World Health Organization's recommendations (28). Nutritional indicators, height-for-age z-score (HAZ), weight-for-age z-score (WAZ), and body mass index-for-age z-score (BAZ) were calculated using the WHO AnthroPlus software. Children with WAZ, HAZ, or BAZ values less than −2 standard deviations (-2 SD) from the WHO median were classified as underweight, stunted, or wasted, respectively. Children with z-scores greater than or equal to −2 SD were considered to have normal nutritional status (28).
2.5.1 Blood sample collection and analysis
In total, 8 mL of venous blood was collected from each child, with 4 mL in an ethylenediaminetetraacetic acid (EDTA)-treated tube and 4 mL in a serum separator tube. The blood sample was drawn by a qualified physician using a single-use sampling needle. After collection, the samples were immediately stored in a cooler on ice and sent to the HDSS laboratory. On arrival at the laboratory, hemoglobin concentration was determined on the same day on whole blood using a Sysmex XP-300 automated hematology analyzer. The concentrations were expressed in grams per deciliter (g/dL). A child with a hemoglobin level under < 11.5 g/dL was considered anemic (29). Plasma and serum samples were obtained by centrifugating at 4,000 rpm for 120 min at 4 °C and transferred to FluidX tubes. RBC samples were prepared from the remaining cells after plasma removal by adding 220 μL of lysis buffer. All samples were sent to Nestlé's Automated Bioanalytics Laboratory in Switzerland for nutrient biomarker analysis.
2.5.2 Nutrient biomarker analysis
2.5.2.1 Hydro-soluble vitamins targeted analysis by LC-MSMS
Hydro-soluble vitamins were measured in plasma. Sample preparation, including calibration curves, quality controls, and study samples, was automated and performed using a Microlab STAR M liquid handler (Hamilton, Reno, Nevada, USA). Briefly, plasma samples were thawed at room temperature, vortexed, and transferred to polypropylene plates containing internal standard, ascorbic acid, and DL-dithiothreitol. Samples were precipitated with 7.5% trichloroacetic acid and centrifuged at 2,500 rpm for 10 min. Then, the supernatant was transferred and filtered onto an AcroPrep Advance 96 filter plate with a 0.2-μm membrane (Pall, Port Washington, New York, USA) prior to LC-MS/MS analysis. Water-soluble vitamins analyses were performed on an Acquity I-class UPLC system (Waters, Milford, Massachusetts, USA) equipped with a binary solvent pump, a sample manager with a 10-μL fixed-loop injection system set at 6 °C, and a column oven equipped with an active preheater set at 25 °C. Separations were performed on an ACE Excel, 2 μm, C18-PFP 100 × 2.1 mm column (ACE, UK) in gradient mode using a solution containing 5% acetic acid with 0.2% heptafluorobutyric acid in Milli-Q water (Merck®, Germany) and acetonitrile as mobile phases. A constant flow rate of 600 μL/min was used, and a volume of 6 μL was systematically injected. The UPLC system was hyphenated to a Xevo TQ-XS triple quadrupole mass spectrometer (Waters, Milford, Massachusetts, USA). Electrospray ionization parameters were set as follows: capillary voltage: +0.4 kV; source temperature: 150 °C; desolvation temperature: 600 °C; desolvation gas flow rate (N2): 1,000 L/h. Argon was used as a collision gas with optimum collision energy and cone voltage determined for each compound. Data were acquired using MassLynx 4.2 software (Waters, Wilmslow, UK), and chromatographic peaks were integrated with TargetLynx (Waters, Wilmslow, UK). Data were uploaded to a LIMS system, “SLims” (Agilent, Santa Clara, California, USA), for quantification using an “R” script integrated into the SLims server.
2.5.2.2 Amino acid targeted analysis by LC-MS/MS
Sample preparation, which involved a derivatization step, was automated and carried out on a Microlab STAR M liquid handler (Hamilton, Reno, Nevada, USA) to prepare calibration curves, quality controls, and study samples. Serum samples were thawed at room temperature, vortexed, transferred to a polypropylene plate, and precipitated with a solution containing IS in methanol+ 0.1% formic acid before being centrifuged at 2,500 rpm for 10 min. Then, the supernatant was collected for the derivatization step in borate buffer at pH 8.8 with aminoquinolyl-N-hydroxysuccinimidyl carbamate at 55 °C for 10 min and agitated at 500 rpm. Finally, samples were diluted 50 times with a 10 mM solution of ammonium formate and 0.1% FA prior to LC-MS/MS analysis. Amino acid analyses were performed on an Acquity I-class UPLC system (Waters Milford, Massachusetts, USA) composed of a binary solvent pump, a sample manager with a 10 μL fixed-loop injection system (SM-FL) set at 6 °C, and a column oven equipped with an active preheater set at 55 °C. Separations were performed on an AccQtag Ultra C18 column, 1.7 μm, 2.1 x 100 mm in gradient mode using solutions at 10mM AmFo with 0.1% fatty acids (FA) in Milli-Q water and acetonitrile containing 0.1% FA as mobile phases. A constant flow rate of 700 μL/min was used, and a volume of 10 μL was systematically injected. The UPLC system was hyphenated to a Xevo TQ-XS triple quadrupole mass spectrometer. Electrospray ionization parameters were set as follows: capillary voltage: +1 kV; source temperature: 150 °C; desolvation temperature: 600 °C; desolvation gas flow rate (N2): 1,000 L/h. Argon was used as a collision gas with optimum collision energy and cone voltage determined for each compound. Data were acquired using MassLynx 4.2 software (Waters, Wilmslow, UK), and chromatographic peaks were integrated with TargetLynx (Waters, Wilmslow, UK). Then, the data were uploaded to a LIMS system, “SLims” for quantification using an “R” script integrated into the SLims server.
2.5.2.3 Metals/minerals
Minerals were measured using ICP-MS/MS and previously published methods (30). A total of 220 μL of serum sample was thawed at room temperature, vortexed, and spiked with ICP-MS standards for Mg, P, S, K, and Ca. The sample was then diluted with a solution containing 5% 1-butanol, 0.05% EDTA, 0.05% Triton X-100, 0.25% ammonium hydroxide, and Milli-Q H2O, and inverted to homogenize. The analysis was subsequently performed using an Agilent 8800 triple quadrupole ICP-MS (Agilent Technologies, Tokyo, Japan) and the Mass Hunter Workstation software.
2.5.2.4 Plasma and red blood cells
Plasma and red blood cell (RBC) samples were thawed at room temperature and vortexed. From 200 μL of each sample, 200 μL of solvent was added (ethanol for plasma and lysis buffer—a mixture of ammonium chloride, sodium hydrogen carbonate, and EDTA in MilliQ water—for RBCs). An internal standard (fatty acid methyl ester 21:0 and triacylglycerol 13:0 for plasma and phosphatidylcholine 23:0 for RBCs) was added with methanol, methanol/3 N HCl, and hexane. Samples were stirred and heated to 100 °C for 60 min for plasma and 90 min for RBCs and then cooled to room temperature. LC-MS grade water (2 mL) was then added, and the samples were centrifuged at 1,200 g for 5 min. The supernatant was transferred to GC vials and analyzed on an Agilent 7890A gas chromatograph with a flame ionization detector (Agilent Technologies, Palo Alto, California, USA). Chromatographic peaks were integrated using OpenLab 2, v2.4.0.628.
2.5.2.5 Clinical chemistry parameter measurements
The clinical chemistry parameters measured were C-reactive protein (CRP), alpha-1-acid glycoprotein (AGP), ferritin (FER), transferrin (Trf), and soluble transferrin receptor (sTrf). Serum samples were directly analyzed without prior preparation. Analyses were carried out on an Architect Ci4100 analyzer (Abbott, Chicago, Illinois, USA) composed of a C4000 clinical chemistry module and an i1000SR immunoassay module. Specific kits validated on human serum were used and processed according to the instructions of the manufacturer. Samples exceeding the upper limit of quantification were diluted by a factor of 2 according to the recommended instructions and reanalyzed.
2.5.3 Reference values
Micronutrient status was evaluated using the following reference values: Iron deficiency was defined as transferrin concentrations >8.3 mg/L [Ramco Laboratories, Inc.] or serum ferritin concentrations < 15 μg/L (31, 32). Zinc deficiency was classified as serum zinc < 65 μg/dL in children < 10 years, < 70 μg/dL in girls ≥10 years, and < 74 μg/dL in boys ≥10 years. Iodine deficiency was defined as serum iodine concentrations < 40 μg/L (33), while hypocalcemia was defined as serum calcium of < 8.8 mg/dL (34). Vitamin D deficiency was defined as serum 25-hydroxyvitamin D [25(OH)D] of < 50 nmol/L (35). Riboflavin deficiency was defined as plasma riboflavin of < 3 μg/L (36) and folate deficiency as a concentration of < 7 nmol/L (37). Vitamin B12 deficiency was defined as serum concentrations of < 148 pmol/L (38). Inflammation was defined as CRP of >10 mg/L or AGP of >1 g/L. Because several nutritional biomarkers are influenced by inflammation, values from children with elevated inflammatory markers were excluded (21, 39).
2.6 Assessment of cognitive skills
Cognitive skills, especially fluid intelligence, were assessed using the Raven's Colored Progressive Matrices (RCPM). Fluid intelligence is associated with reasoning ability and academic performance in children. The RCPM is a widely used, non-verbal test that minimizes cultural and linguistic bias. It has been repeatedly used in studies across sub-Saharan Africa (6). The RCPM was administered individually to the children by a well-trained researcher, without time limits, in quiet classrooms, according to the procedures described in the manual (40). The test instructions were read in French and in the local language to ensure that each child understood the tasks. The RCPM consists of three sets of 12 problems that measure the ability to solve problems and reason by analogy. The children were presented with a matrix of symbols. They were asked to fill in the missing symbol from a set of six options. One point was awarded for each correct answer. The total score was the sum of the correct answers, with a maximum of 36 points. As no RCPM norms exist for Ivorian children, cognitive performance was classified using approaches previously used in other sub-Saharan African countries (6, 41). Cognitive performance was defined as low if it was below the 50th percentile, medium if it was between the 50th and 75th percentiles, and high if was at or above the 75th percentile of the data distribution. The corresponding threshold scores were as follows: low < 14, medium 14–18, and high ≥18.
2.7 Assessment of school performance
School performance was quantified based on end-of-year results in mathematics and literature. Performance score was classified as low if it was less than 50th, medium if it was 50th−75th, and high if it was ≥75th (41). The corresponding threshold scores were mathematics (low < 6, medium 6–7.6, and high ≥ 7.6) and literature (low < 5, medium 5–6.43, and high ≥6.43). The end-of-year mathematics and literature results were based on regional harmonized examinations administered across all schools under the supervision of the District Education Office of Taabo. In Côte d'Ivoire, primary schools are organized under regional district education offices of the Ministry of Education. Teachers use marking schemes issued by the regional district office in accordance with national curriculum guidelines, which helps minimize potential teacher-related bias in grading. Although evaluation procedures are not standardized at the national level, their standardization at the regional level ensures consistent assessment of children's performance across schools in this study.
2.8 Statistical analysis
Data were analyzed using the Statistical Package for the Social Sciences version 20.0 (SPSS IBM Inc.). Descriptive statistics, including frequencies and percentages for qualitative variables and means and standard deviations for quantitative variables, were calculated. Before assessing the relationship between nutrient biomarkers and outcome variables, principal component analysis and partial least squares regression were used to select nutrients with potential links with cognition (Supplementary Figures S1–S3). We also considered cognitive-related nutrients reported by earlier studies in African school-aged children (Supplementary Table S1). Analysis of variance (ANOVA) was used to assess differences in cognitive and school performance across the sociodemographic and nutritional status groups. In addition, associations between continuous variables were evaluated using Pearson correlation coefficients, while the chi-squared tests were used for categorical variables. The percentage of variance in cognitive and school performance due to each nutrient biomarker was determined using linear regression models, adjusted for age, school grade, and household characteristics (parental education, occupation, and household size). Only biomarkers that were significantly associated with cognition or school outcomes (p < 0.05) were included in the adjusted linear regression models. In this study, raw p-values were used because the nutrient biomarkers were significantly correlated. Additionally, no correction was applied for multiple comparisons as this study is principally exploratory in nature.
3 Results
3.1 Sociodemographic characteristics of the participants
The sociodemographic characteristics of the participants are presented in Table 1. Out of the 252 children initially enrolled in the study, 251 (99.6%) completed all the questionnaires. The mean age was 9.3 ± 1.9 years, and 46.2% of the participants were girls and 53.8% were boys. Additionally, 16.7% children were recruited in each school grade (grades one to six), and more than three-quarters (90.0%) studied at home for 30–60 min. Additionally, 72.5% ate lunch in the school canteen, 62.6% had low absenteeism, and 56.2% had never repeated a grade. At the family level, 80.5% of the participants came from large families (families with more than five members) and 97.2% lived with their parents. More than three-quarters (79.7%) of the fathers work in the primary sector, and 40.6% had primary education. The majority (60.6%) of the mothers were housewives, and less than half of them (45.4%) were illiterate.
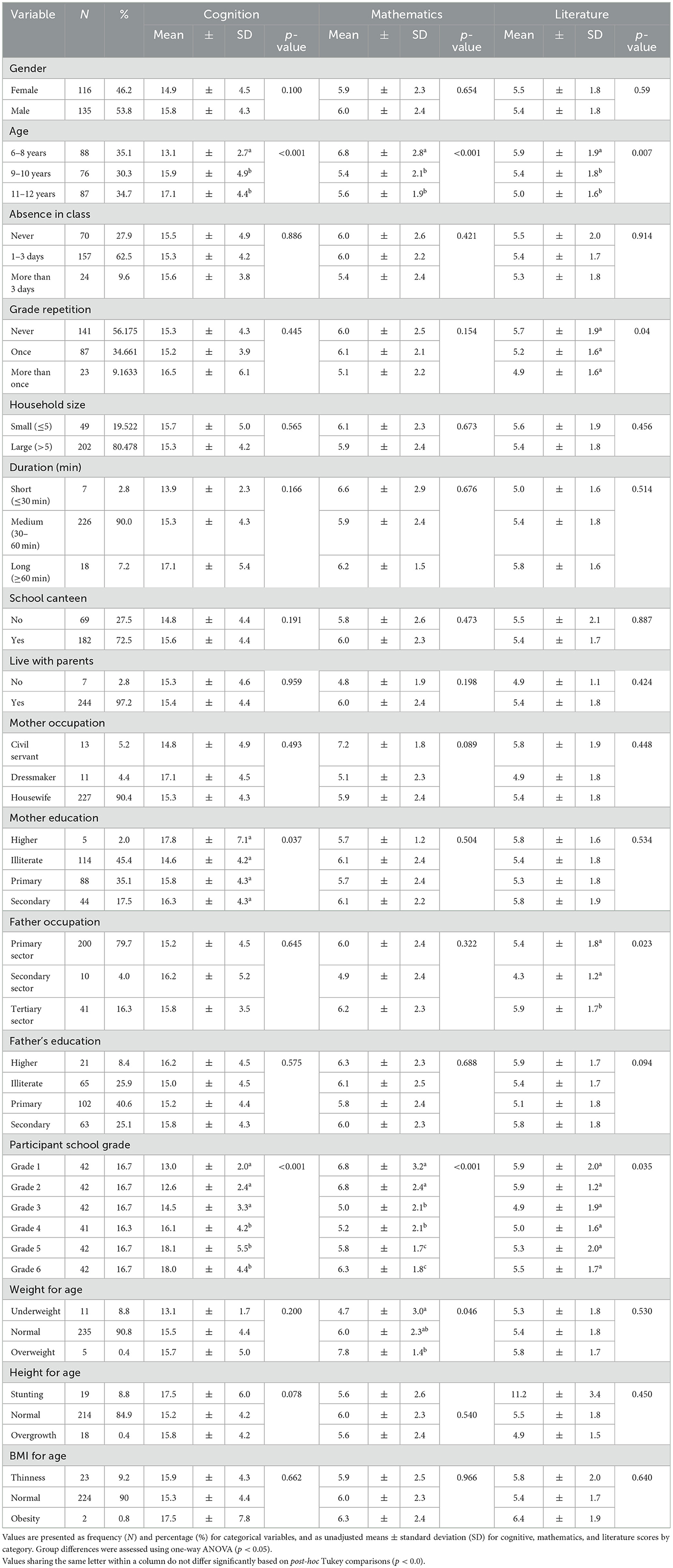
Table 1. Comparison of mean scores in cognitive and school performance by sociodemographic and anthropometric characteristics of the children.
3.2 Nutritional status of the participants
The assessment of nutritional status using anthropometric indicators WAZ, HAZ, and BAZ showed that the majority of participants were within the normal range: 88.7% for WAZ, 85.1% for HAZ, and 90.0% for BAZ (Table 1). The prevalence of underweight (7.9%), stunting (7.6%), and thinness (9.2%) was relatively low, resulting in an overall undernutrition prevalence of 24.7%. For micronutrient status, the majority of the children had low blood concentrations of folate (51%), thiamine (100%), vitamin B12 (100%), ferritin (100%), and transferrin (100%). In contrast, most children had values within the normal range for vitamin D (98%), vitamin B3 (100%), zinc (84%), iodine (64%), calcium (80%), and hemoglobin (53 %), as shown in Figures 3, 4.
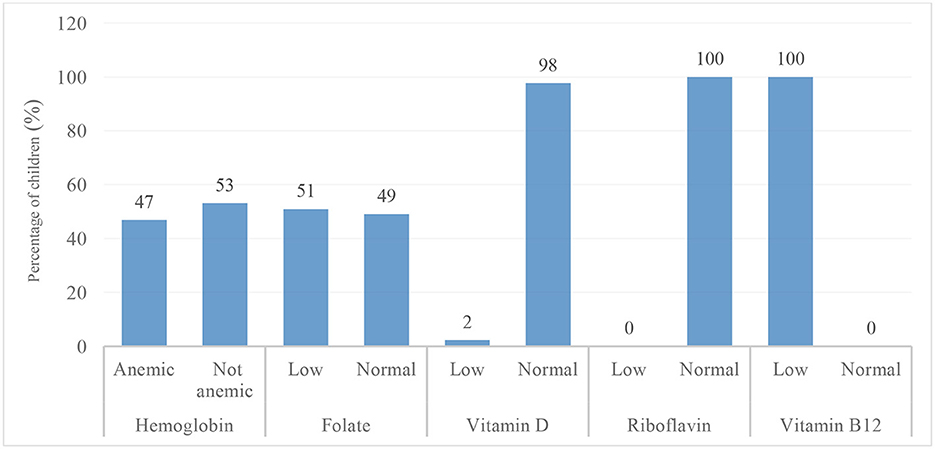
Figure 3. Prevalence of anemia and cognitive-related vitamin deficiencies (folate, vitamin D, riboflavin, and vitamin B12) among school-aged children in the Taabo Health and Demographic Surveillance System, Côte d'Ivoire.
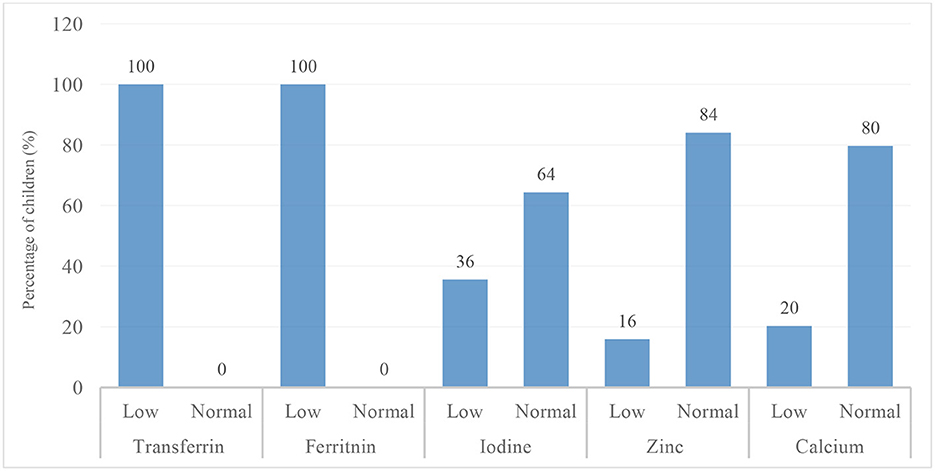
Figure 4. Prevalence of cognitive-related mineral deficiencies (iron, iodine, zinc and calcium) among school-aged children in the Taabo Health and Demographic Surveillance System, Côte d'Ivoire.
3.3 Cognitive and academic performance of the participants
Table 2 presents the overall cognitive and school performance of the participants. The mean score for the cognitive test was 15.4 ± 4.4 (out of 36), while the mean scores were 6.0 ± 2.4 (out of 10) for mathematics and 5.4 ± 1.8 (out of 10) for literature. In addition, 25.9% of the children scored above the 75th percentile (high performance), 30.7% scored between the 50th and the 75th percentile (medium performance), and the majority (43.4%) scored less than the 50th percentile (low performance) in the cognitive test. Regarding school performance, most of the children (49%) scored less than the 50th percentile and 25.5% scored between the 50th and the 75th percentile, 25.5% scored above the 75th percentile in mathematics, while in literature, the majority (37.9%) scored between the 50th and 75th percentile, 36.7% scored below the 50th percentile and 25.5% scored above the 75th percentile.

Table 2. Mean scores and standard deviation (SD) in cognitive tests, mathematics, and literature and distribution of scores across performance categories: low performance (below the 50th percentile), average performance (50th-75th percentile), and high performance (above the 75th percentile).
3.4 Cognitive and school performance by sociodemographic characteristics
Comparing mean scores across sociodemographic groups using ANOVA, significant differences were observed between age groups and school grade levels in cognitive and school performance. Older children aged 11–12 years (17.1 ± 4.4) outperformed younger children aged 6–8 years (13.1 ± 2.7) in the cognitive test. In contrast, older children (11–12 years) had lower performance in mathematics and literature compared to younger children. Regarding grade levels, children in higher grades (five and six) demonstrated better cognitive performance than those in lower grades. For school performance, both lower and higher grades showed higher scores, whereas middle grades (three and four) had significantly lower performance (p < 0.05). No significant differences were observed in the literature across grade levels. Additional significant associations (p < 0.05) were found for maternal education (cognition) and for grade repetition and paternal occupation in the literature; however, post-hoc Tukey tests revealed no consistent pairwise differences across these sociodemographic groups. Furthermore, it can be seen from the data in Table 3 that school cafeteria attendance (χ2 = 6.4, p = 0.041) and school grade (χ2 = 61.3, p < 0.001) were significantly associated with cognitive performance. Mathematics performance was associated with age group (χ2 = 19.9, p < 0.001) and school grade (χ2 = 32.8, p < 0.001), while literature performance was associated with age group, school grade level (χ2 = 29.5, p < 0.001), and grade repetition (χ2 = 11.2, p = 0.025).
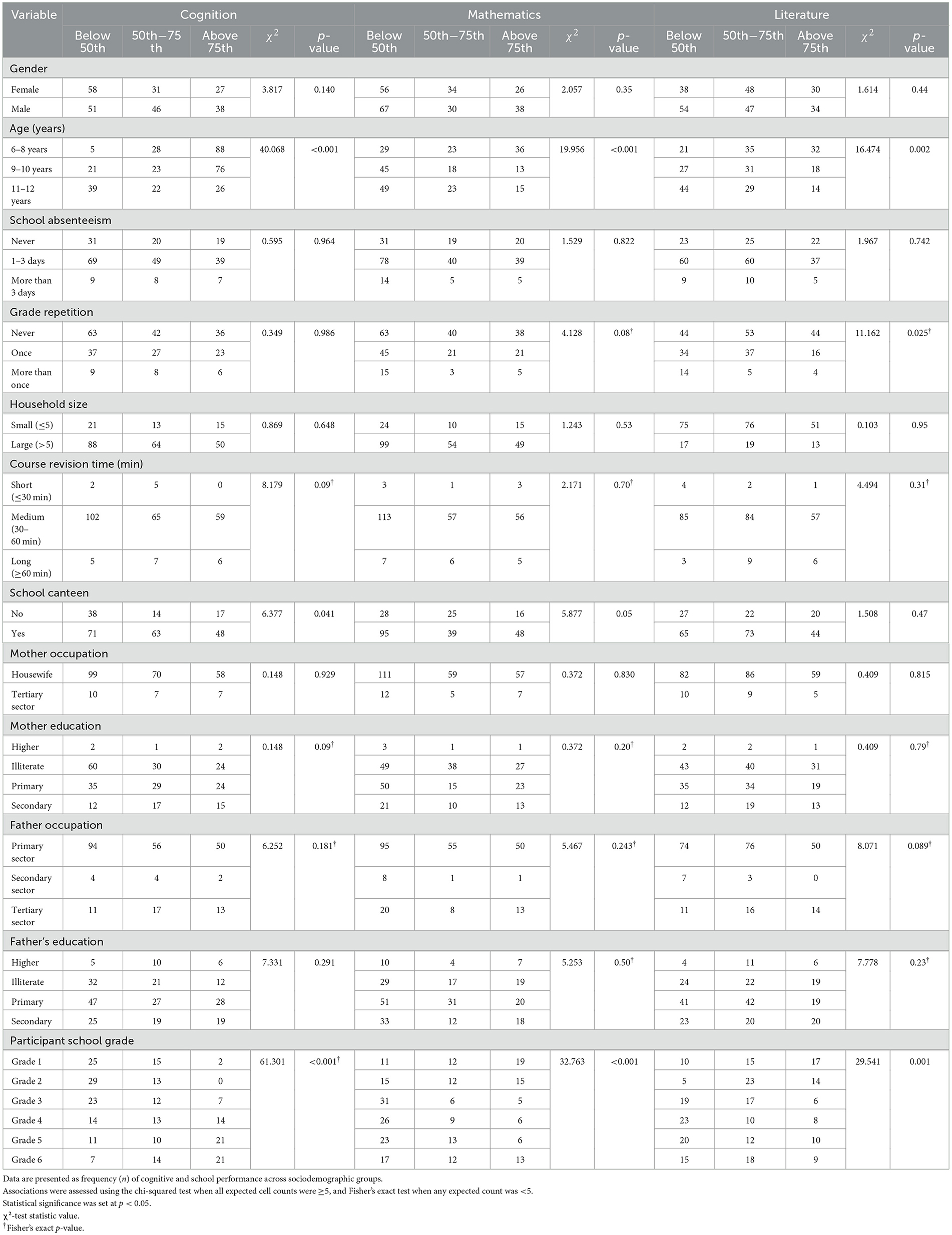
Table 3. Cognitive and academic performance by sociodemographic characteristics with performance category: high (above the 75th percentile), average (50th−75th percentile), and low (below the 50th percentile).
3.5 Cognitive and school performance by nutritional status of the participants
3.5.1 Association between nutritional indicators, cognition, and school performance
The results of the association between nutritional indicators, cognition, and school performance are presented in Table 4. A significant association was found between weight-for-age cognitive test scores (χ2 = 10.6, p = 0.032). Children with normal weight-for-age were more likely to achieve higher cognitive performance, while underweight children were disproportionately represented in the lowest performance group (54.5%). Height-for-age was also associated with literacy performance (χ2 = 15.7, p = 0.016). The majority (73.7%) of children with normal weight were found to score above the 50th percentile. On the other hand, BMI-for-age showed no association (p > 0.05) with cognition, mathematics, or literature performance.
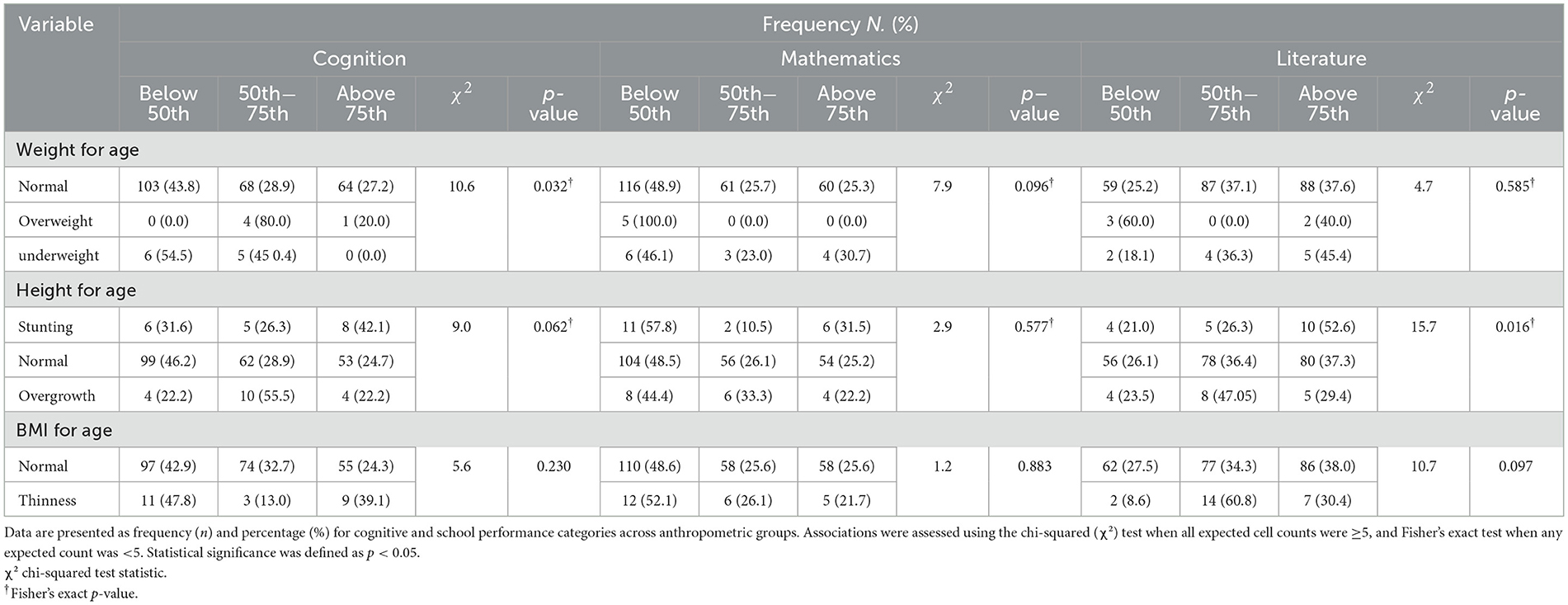
Table 4. Cognitive and academic performance by anthropometric status with performance category: high (above the 75th percentile), average (50th−75th percentile), and low (below the 50th percentile).
3.5.2 Correlation between nutritional biomarkers, cognition, and school performance
The results of the correlational analysis are provided in Table 5. Significant correlations were found between certain biomarkers and cognitive or academic outcomes. For cognition, positive correlations were observed with transferrin (r = 0.20, p = 0.008), tryptophan (r = 0.165, p = 0.017), and calcium (r = 0.14, p = 0.04). For mathematics performance, significant associations were observed with active folate (5-methyltetrahydrofolate; r = 0.22, p = 0.006), potassium (r = 0.193, p = 0.016), RBC omega-3 fatty acids (r = 0.14, p = 0.02), and plasma omega-3 fatty acids (r = 0.14, p = 0.02). For literature, positive correlations were found with active folate (r = 0.20, p = 0.009) and potassium (r = 0.187, p = 0.020). No significant associations were observed for hemoglobin, ferritin, vitamin D, riboflavin, zinc, iodine, omega-6 fatty acids, or fatty acid ratios with cognitive and school performance.
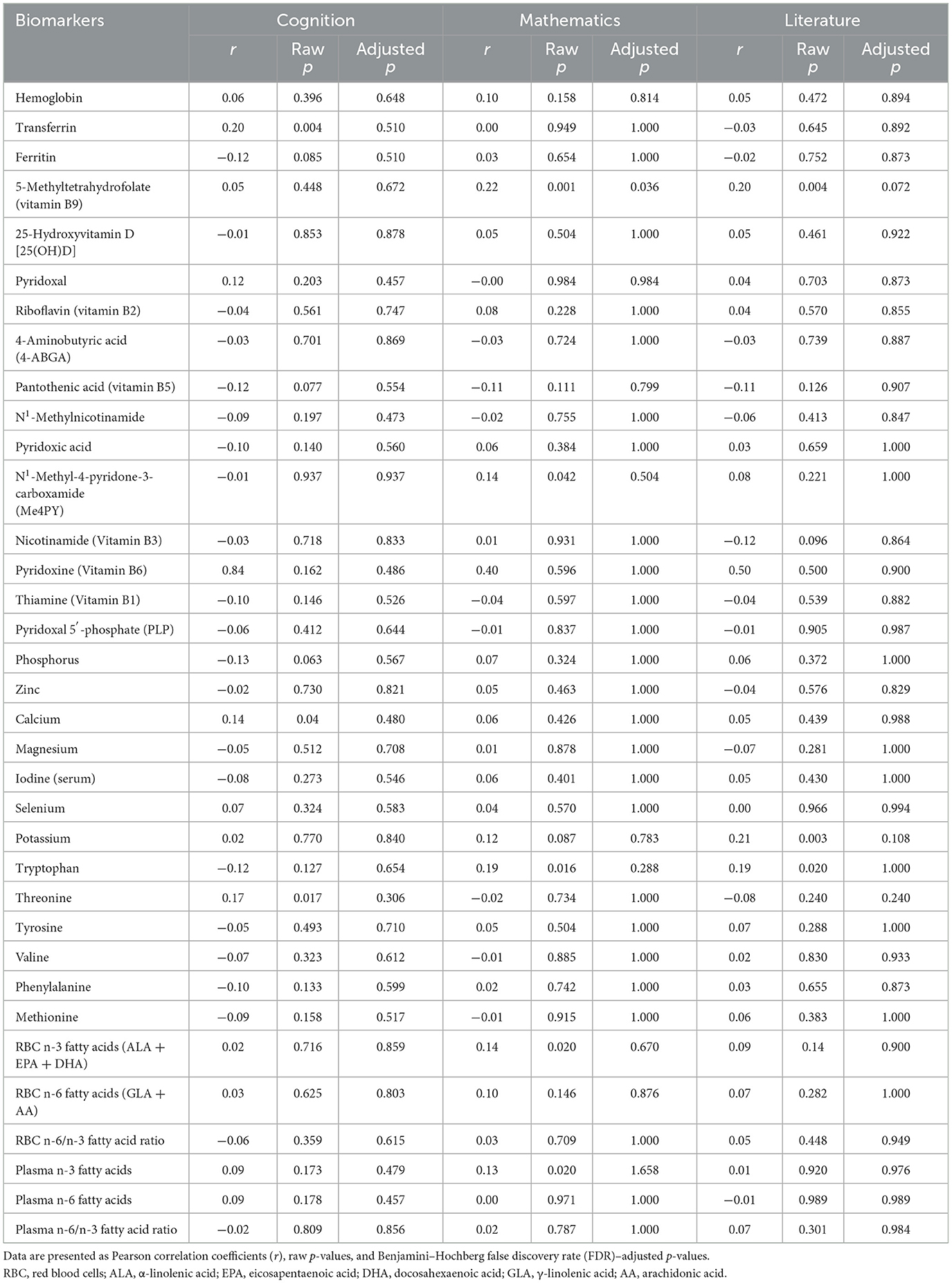
Table 5. Associations between cognitive test scores or school performance and nutrient biomarkers concentrations.
3.6 Cognitive and school performance variations explained by nutritional biomarkers
The multivariable linear regression models, adjusted for age, school grade, parental education, and occupation, identified several blood nutrient biomarkers that significantly explained variations in cognitive and academic performance (Table 6). For cognitive performance assessed using RCPM, calcium was the only significant predictor (R2 = 0.3, p = 0.020), with the 95% CI ranging from 8.2 × 10−6 to 9.3 × 105, while tryptophan and transferrin were not significant. In mathematics performance, 5-methyl-tetrahydrofolate emerged as a strong predictor (R2 = 0.1, p = 0.006; 95% CI: 0.1–0.3), whereas RBC n-3 fatty acids and plasma n-3 fatty acids showed non-significant associations. Similarly, for literature scores, both 5-methyl-tetrahydrofolate (R2 = 0.08, p = 0.005; 95% CI: 0.1–0.2) and potassium (R2 = 0.1, p = 0.008; 95% CI: 1.3 × 10−6−8.4 × 10−6) were significant predictors. When combining mathematics and literature into overall school performance, both 5-methyl-tetrahydrofolate (R2 = 0.1, p = 0.002; 95% CI: 0.1–0.5) and potassium (R2 = 0.1, p = 0.012; 95% CI: 2.2 × 10−6−1.7 × 105) remained significant, whereas RBC n-3 FA and plasma n-3 FA were not.
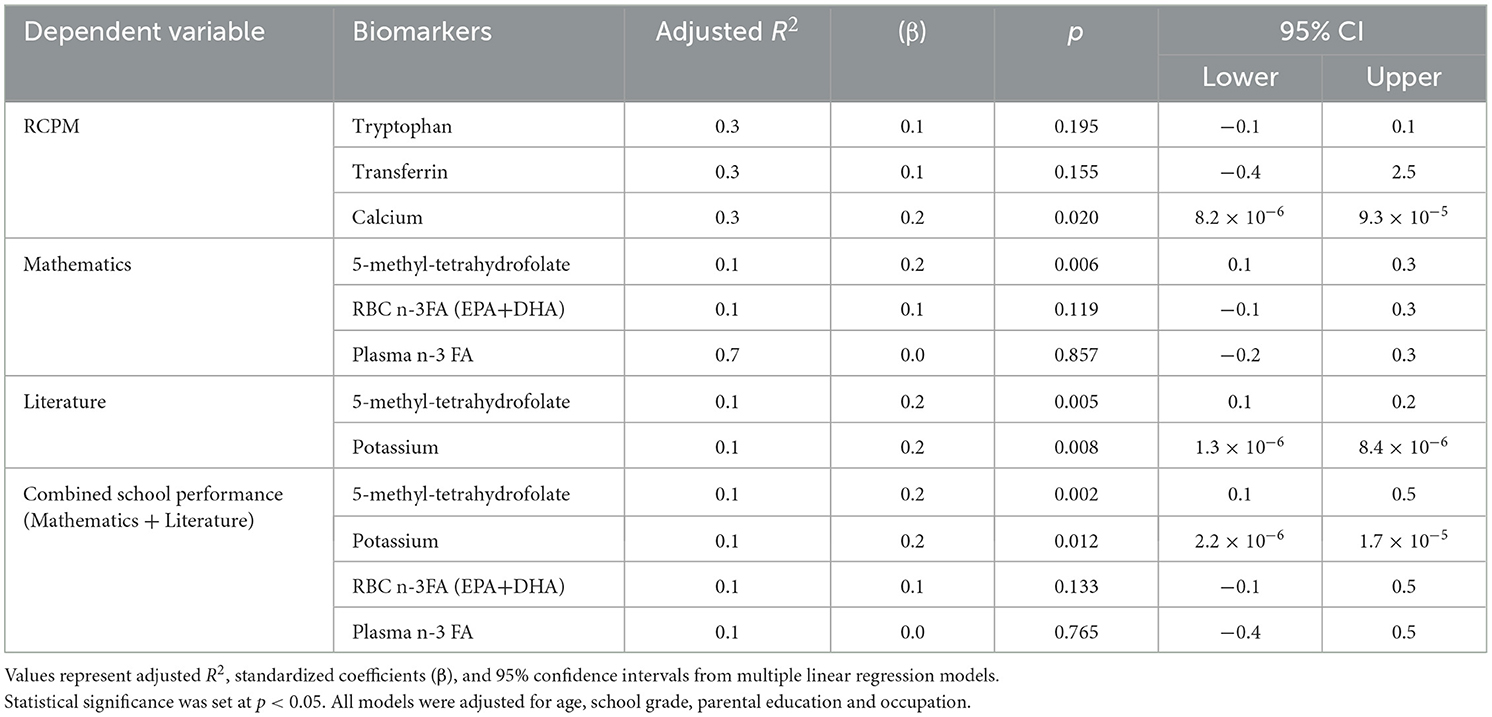
Table 6. Variations in cognitive and academic performance explained by nutritional biomarkers.
4 Discussion
In this study, the overall cognitive score was 15.4 ± 4.4 (out of 36), with 56.6% of the children scoring above the 50th percentile. As currently there are no RCPM normative data available for Ivorian children, it is not possible to determine whether this score reflects lower or higher overall performance. Nevertheless, the performance observed is broadly comparable to findings from other African countries. In Kenya, a study assessing the reliability and validity of the RCPM in school-aged children (6–12 years) from rural and semi-urban schools reported a mean score of 16.7 ± 5.48, which was below the UK norms, and the difference was attributed to cultural and sociodemographic factors (42). Similarly, a study in Ghana among primary school-aged children aged 6–11 years from urban settings found a mean score of 17.9 ± 5.4 (6). Taken together, these comparisons underscore the importance of accounting for contextual factors when interpreting cognitive outcomes and academic performance.
In addition, when assessing cognition and school performance, strong associations were observed with sociodemographic factors, including maternal education, school cafeteria attendance, age, and school grade. These findings suggest that non-nutritional factors can significantly influence cognition and school performance. Research indicates that maternal education predicts neurocognitive function throughout development, with particularly strong effects on language abilities, executive functions, and the health status of the child, which can impact school performance (43). School cafeterias are also known for promoting healthy diets and supporting academic performance, particularly in developing countries where undernutrition and hunger are common problems among children. A lack of nutritious food can significantly affect children's physical and cognitive development and disrupt their learning in the classroom. In response to this reality, school cafeterias are established to provide children with balanced, nutritious meals, improve their health, and support their academic success (44). For example, a study in Benin found that schools with canteens had lower rates of malnutrition and better academic performance than schools without cafeterias (45). Furthermore, the significant associations between RCPM scores and age and school grade, with performance increasing with age and higher grades, clearly suggest the discriminant validity of the RCPM in the school-aged children studied. Similar observations were reported in Kenyan school-aged children, where the RCPM demonstrated good discriminant validity and strong internal consistency reliability (Cronbach's alpha ranging from 0.68 to 0.90). These findings are particularly encouraging regarding the validity of the RCPM among sub-Saharan children, as indicated in a previous study (42). Nevertheless, adapting the RCPM battery to the local context may further enhance the accuracy of cognitive assessments in this population.
The majority of the participants were within the normal nutritional status range according to WHO reference values (28). However, 24.7% were affected by undernutrition in all forms combined (stunting, underweight, and thinness). This prevalence of undernutrition may be attributed to the fact that most of the participants were from rural areas, where dietary diversity is limited and parental education levels are low: 45.4% of mothers were illiterate, and 40.6% of fathers had only a basic education. In rural communities in Côte d'Ivoire, diets are often predominantly carbohydrate-based, with limited intake of animal-source foods such as meat and dairy, which are essential sources of protein and micronutrients. Such deficiencies can contribute to various forms of malnutrition (22). Although national data on malnutrition among school-aged children in Côte d'Ivoire are lacking, our finding is consistent with a previous study in south-central Côte d'Ivoire among children aged 5–11 years, which reported that 19% were underweight and 40% were stunted (26).
In addition, the analysis of micronutrient status showed that plasma concentrations of ferritin and transferrin, along with B vitamins including folate, thiamin, and vitamin B12, were inadequate in most of the participants. Micronutrient deficiencies in children from developing countries continue to be a public health concern due to their persistent prevalence (16). These deficiencies can be attributed to several factors, such as limited dietary diversity, low bioavailability, or inadequate intake of micronutrients. In our previous study involving the children in this research, the intakes of most assessed nutrients, including thiamin, riboflavin, vitamin B2, folate, and iron, were largely inadequate. Another study on Ivorian schoolchildren indicated that riboflavin deficiency was very common, affecting nearly two-thirds of the children studied (22).
This study found significant associations between weight-for-age, height-for-age, and cognitive or literature test scores, with children of normal weight and height achieving higher performance compared to those who were underweight or stunted. These results suggest that undernutrition may negatively affect cognitive development and academic performance in children. A study has shown that undernutrition can significantly impair cognitive performance and learning capacity (46). It has also been associated with deficits in attention, memory, and executive function, which are essential for academic achievement. For instance, a cross-sectional study of 600 Indian children found that stunted, underweight, and thin children had more than twice the risk of below-average intelligence compared to well-nourished peers (47). Similarly, a study in Ethiopian school-aged children reported that undernourished children had significantly lower academic performance compared to those with normal nutritional status (48). These findings reinforce the importance of integrating nutritional considerations into educational policies, particularly in developing countries.
Significant correlations were also observed between omega-3 fatty acids and mathematics, suggesting a link between omega-3 fatty acids and school performance in the participants. Similar observations were reported in a study among school-aged children (7 years) in the Netherlands, where omega-3 fatty acids, particularly docosahexaenoic acid, showed a positive association with reading and spelling scores (49). In addition, a study conducted among school-aged children (7–15 years) in Italy showed a significant positive association between blood concentrations and reading performance of omega-3 fatty acids (50). Omega-3 fatty acids are the most important polyunsaturated fatty acids (PUFAs) involved in various physiological processes in the body (51). The dry weight of the human brain is 60% fatty acids, of which 35–40% are omega-3 fatty acids (51). The three types of omega-3 fatty acids are α-Linolenic acid (ALA), eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA). They are essential components of neuronal membranes and are critical for proper brain structure. Omega-3 fatty acids are also involved in behavior, cognition, and mood regulation (52). Omega-3 fatty acid deficiency can lead to cognitive impairment with subsequent poor academic performance in children. In the Ivorian context, especially in the study area, the potential dietary source of omega-3 fatty acids is locally caught freshwater fish. The Taabo HDSS is located around Lake Taabo and the Bandama River, where fishing serves both as a livelihood and a local food source (27). Small freshwater fish, such as tilapia and catfish, which are often consumed dried, smoked, or whole, are therefore the most plausible contributors of long-chain omega-3 fatty acids (EPA and DHA). Occasional consumption of dried or smoked marine fish transported inland may also contribute. In our recent study involving the same population of school-aged children, we found that most had an adequate intake of omega-3 fatty acids (53).
This study also found a positive correlation between transferrin concentration and cognitive test scores, suggesting a potential beneficial relationship between iron and cognitive functions in the participants. Transferrin is an iron-binding protein and is considered the primary iron transport protein, binding two iron atoms per molecule and delivering them to cells via receptor-mediated endocytosis (54). The role of iron in the development of cognitive functions has been extensively studied, as iron is involved in several processes in the brain, i.e., in brain energy production, neurotransmitter synthesis, and myelination. Iron deficiency is associated with several brain developmental problems that can lead to cognitive disorders, whereas adequate iron status improves cognitive skills in children. The results of this study support evidence from an earlier study of 389 school-aged children (6–11 years) in Ghana, which found that iron concentration was significantly correlated with cognitive performance (6). Similar findings were reported in an American study, suggesting that subclinical iron status may also affect cognition (55).
Unlike transferrin, ferritin showed no association with cognition or school performance, despite being a key iron biomarker with lower levels in the study participants. The observed controversy may be linked to the distinct roles of transferrin and ferritin in neurocognitive function. Transferrin is a key iron transport protein that facilitates iron delivery to neurons and supports processes essential for cognitive performance. Elevated transferrin levels may reflect increased iron mobilization necessary for optimal cognitive function, which was consistent with studies suggesting a role for transferrin in neuroprotection and memory (56). In contrast, ferritin, which is primarily an iron storage protein, reflects more systemic iron stores and may not directly influence neural activity or synaptic function. A study has shown that, while ferritin is critical for preventing oxidative damage through iron sequestration, its relationship with cognitive function is inconsistent, possibly due to its dual role in both neuroprotection and potential iron overload (57). This divergence between these two biomarkers demonstrates the complexity of iron metabolism in the brain and suggests that dynamic markers, such as transferrin, may be more sensitive indicators of cognitive status than static storage markers, such as ferritin. Thus, our findings contribute to a growing body of literature advocating nuanced interpretations of iron biomarkers in cognitive research and highlight the importance of examining functional biomarkers in neurocognitive assessments.
A positive correlation was observed between 5-methyltetrahydrofolate, known as a folate biomarker, and school performance, indicating a link between improved academic performance. This observation is aligned with previous findings in school-aged children. A study in Swedish school-aged children found that children with higher folate levels or adequate folate intake performed better on school and cognitive tests compared to their peers with lower amounts of folate (58). A recent literature review also highlighted that adequate folate intake was significantly associated with academic performance and attention in school children (59). In fact, 5-methyltetrahydrofolate is the primary biologically active form of folate, also known as vitamin B9 (60). Folate plays a critical role in the brain throughout the lifespan, particularly in cognitive processes (61). It is essential for one-carbon (C1) metabolism, neurotransmitter production, DNA methylation, and brain development, which can significantly influence cognitive functions. In contrast, folate deficiency is associated with reduced brain volume and impairment, which can lead to poorer cognitive and academic performance (62, 63).
A positive correlation was also observed between tryptophan concentrations and cognitive test scores, suggesting a relationship between tryptophan and cognitive functions. This result is consistent with those reported in previous studies. A study among children aged 3–7 years old in Russia found that tryptophan supplementation improved visual memory and thinking (64). Furthermore, other studies conducted in school-aged children have shown that tryptophan improves sleep efficiency and mood (10-years-old) (65) as well as has potential therapeutic effects in children with cognitive delay (66). Tryptophan is an essential amino acid that plays a crucial role in mental functions primarily through its conversion to serotonin, a key neurotransmitter in the brain. Its physiological significance extends beyond mood regulation, influencing various cognitive and behavioral aspects (67, 68). Tryptophan deficiency can lead to global cognitive function and working memory impairment (69). However, due to its ubiquitous role, i.e., tryptophan is involved in several biochemical activities, such as inflammation (70), and its correlation with cognition should be further investigated. It is noteworthy that the relationship between tryptophan status and cognition or school performance in sub-Saharan schoolchildren has rarely been investigated. To the best of our knowledge, this study represents the first attempt to examine this association.
In contrast, no correlation was observed between zinc concentrations and either cognitive scores or school performance in the present study. Several factors may explain this lack of association. First, the prevalence of zinc deficiency was relatively low, with more than three-quarters of the children within the normal physiological range (71). Second, zinc was assessed under non-fasting conditions; since plasma zinc concentrations fluctuate considerably with food intake, this may have introduced measurement error and reduced the sensitivity to detect associations. Although this study was unable to demonstrate a link between zinc status and cognition, it is noteworthy that the existing evidence in school-aged children remains inconclusive. For instance, studies in Brazilian (6–9 years) (72) and Vietnamese (6–8 years) (73) school-aged children reported positive effects of zinc on cognitive functions. In contrast, studies conducted in Canada and Ghana found no association and a negative correlation with cognitive outcomes, respectively. These findings illustrate that the relationship between zinc and cognition may be complex and influenced by multiple interacting factors. Further well-designed studies may enhance our understanding.
In addition, iodine showed no significant association with either cognitive outcomes or school performance, which contrasts with some existing findings (19). Iodine deficiency is recognized as a major public health problem worldwide, particularly in developing countries (74). It is well-established that inadequate iodine intake can significantly impair brain development and cognitive function in children. To address this, several governments across sub-Saharan Africa, including Côte d'Ivoire, have implemented mandatory iodine fortification programs targeting widely consumed food ingredients such as table salt and seasoning cubes. These interventions, in place for decades, have substantially reduced iodine deficiency and related disorders in the region. Consequently, it would be unexpected to observe a high prevalence of iodine deficiency among children living in the present study area, which is under health and demographic surveillance. This interpretation is consistent with the finding that the majority of participants (64%) displayed adequate iodine levels. Given the relatively low prevalence of iodine deficiency in this study, the probability of having an association with cognition may have been limited. Indeed, evidence from intervention studies shows that iodine supplementation in iodine-deficient school-aged children led to significant associations with cognitive performance (19).
Moreover, riboflavin and vitamin B12 showed no correlation with cognitive or school performance in this study. This finding contrasts with previous studies conducted in the United States and India, which have reported positive associations, particularly for riboflavin, with improved cognitive outcomes in school-aged children (75, 76). One possible explanation for this discrepancy is the absence of riboflavin deficiency in the study population. As reported in the results, all participants had plasma riboflavin concentrations within the normal range, which reduces variability and limits the ability to detect potential associations with cognitive performance. Another explanation is related to the non-fasting conditions under which blood samples were collected. Since riboflavin and its biomarkers (e.g., plasma riboflavin) can be influenced by recent dietary intake, non-fasting measurements may have introduced variability unrelated to true status, potentially attenuating the associations with cognitive outcomes (36). For vitamin B12, earlier findings in school-aged children remain mixed. While a limited number of studies have reported positive associations with cognitive function (77, 78), the majority have found no significant associations. Consistent with these observations, the present study found no correlation between vitamin B12 and cognitive or school performance. Similar results were also observed in our recent study assessing dietary vitamin B12 intake and cognition in the same sample of school-aged children (53). The variability in findings highlights the ambiguity surrounding the role of vitamin B12 in cognitive function among school-aged children and underscores the need for further research to clarify this relationship.
No significant association was found between vitamin D concentrations and cognitive or academic performance in this study. Almost all children (98%) had normal vitamin D levels, which may partly explain the lack of association with cognitive or school performance. Consistent with our findings, previous studies among healthy children in sub-Saharan Africa have also reported no association with cognitive outcomes. For example, in Uganda, vitamin D supplementation significantly increased plasma levels but did not affect cognitive scores (35). Similarly, an observational study of 202 children in Seychelles found no association between maternal 25(OH)D levels during pregnancy and neurobehavioral outcomes at the age of five (79). In contrast, some studies have reported positive associations. Karimian and Delavar (80) found significant relationships between vitamin D and cognitive outcomes in Iranian children. Another study in Egypt (n = 45) reported that higher 25(OH)D levels were positively associated with improved cognition in school-aged children (81). To the best of our knowledge, this is the first cross-sectional study to investigate the relationship between vitamin D status and cognitive outcomes in Ivorian school-aged children. Further research in populations of school-aged children with a higher prevalence of vitamin D deficiency may help clarify the potential role of vitamin D in cognitive development.
This study revealed a significant correlation (p < 0.05) between calcium and cognitive test scores, suggesting a potential relationship between calcium and cognitive functions in school-aged children. While calcium may be important for child development, its direct influence on cognitive function in school-aged children has been less studied in sub-Saharan Africa. However, our findings are consistent with those of an observational study of non-school-aged children (aged > 18 years) in Italy, which found a significant association between low serum calcium levels and poor cognitive performance, especially executive function and semantic memory (82). Calcium plays a critical role in skeletal health and nerve transmission, affecting both physical and brain development, and its deficiency can lead to developmental problems, including potential effects on cognitive growth (83).
A positive correlation was also observed between potassium concentration and school performance. Similar to tryptophan and calcium, evidence on the link between potassium and cognition or school performance in school-aged children is less documented, particularly in sub-Saharan populations. A study involving animal models has shown that potassium intake improved cognitive performance and reduced inflammation and oxidative stress in the brain (84), while a mechanistic study has suggested that altered potassium dynamics and dysfunction of potassium channels are associated with cognitive impairment (85). However, findings from the National Health and Nutrition Examination Survey (NHANES) indicated that the relationship between potassium and cognitive function is complex and may be significantly influenced by many factors, including sociodemographic and health conditions (86).
5 Limitations
This study has some limitations. Blood samples were collected under non-fasting conditions, which may increase the concentrations of certain biomarkers. For instance, amino acids (84) and triglyceride-associated fatty acids (e.g., linoleic acid, 18:2, n-6) are particularly sensitive to recent dietary intake (87), whereas water-soluble vitamins show moderate variability, and most minerals are more tightly regulated and less affected (88, 89). Non-fasting samples can, therefore, introduce variability and attenuate associations between biomarkers and cognition or school outcomes. Although fasting samples might have been preferable, this study was conducted in school-based, rural settings, where requiring children to fast would have been quite challenging and not ethically justifiable. Nevertheless, relative comparisons across participants remain valid, given the uniform sampling conditions. Furthermore, several pediatric studies have used non-fasting samples to assess nutritional status at the population level rather than precise metabolic control (90–92). Moreover, as this was an observational cross-sectional study, causal inferences cannot be drawn.
6 Conclusion
Overall, this study found that several cognition-related micronutrients, particularly iron and B vitamins, were largely deficient in school-aged children from the HDSS of Taabo, Côte d'Ivoire. Significant correlations were observed between biomarkers of iron, omega-3 fatty acids, folate, tryptophan, calcium, and potassium with cognition or school performance. However, no associations were found with zinc, iodine, riboflavin, vitamin B12, or vitamin D, despite earlier studies indicating possible links, particularly for zinc and iodine biomarkers, as well as riboflavin and vitamin B12 intakes in sub-Saharan school-aged children. Taken together, these findings suggest that cognitive and school performance are associated with some key nutrients in Ivorian schoolchildren, highlighting the need to improve access to national nutrition programmes, as the standard diet often lacks sufficient supply. Furthermore, this study fills an important gap in our understanding of the relationship between nutrition and cognitive as well as academic outcomes in Ivorian school-aged children.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Ethical approval for this study was obtained from the National Committee on Ethics in Life Sciences and Health under the Ministry of Health, Public Hygiene and Universal Health Coverage of Côte d'Ivoire (N/Ref: 118-22/MSHPCMU/CNESVS-kp). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
Author contributions
AT: Data curation, Formal analysis, Investigation, Writing – review & editing, Writing – original draft. JH: Writing – review & editing, Supervision, Funding acquisition, Conceptualization, Project administration, Validation. AK: Funding acquisition, Conceptualization, Project administration, Supervision, Writing – review & editing. OC: Supervision, Writing – review & editing, Validation, Resources, Methodology. YG: Resources, Writing – review & editing, Methodology. FM: Writing – review & editing, Formal analysis, Visualization. GV: Visualization, Formal analysis, Writing – review & editing. AF: Resources, Writing – review & editing. CN: Writing – review & editing, Supervision.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This research was funded by Société des Produits Nestlé SA under the grant reference [Grant Nestlé. Réf : CSRS/Ph.D. School children performance/2021].
Acknowledgments
The authors are grateful to Nestlé Research (NR) and the Centre Suisse de Recherches Scientifiques en Côte d'Ivoire (CSRS) for their support in conducting this study. The authors also thank the schools, all children involved in this study, as well as the parents of each child, for their collaboration.
Conflict of interest
The study received funding from Société des Produits Nestlé SA. The funder had the following involvement in the study: experimental design. JH, OC, FM ,YG, GV, and AF are employees of Nestlé Research, Lausanne, Switzerland.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2025.1630497/full#supplementary-material
References
1. Lamas HA. School performance. Propósitos Represent. (2015) 3:351–86. doi: 10.20511/pyr2015.v3n1.74
2. Liu J, Peng P, Luo L. The relation between family socioeconomic status and academic achievement in China: a meta-analysis. Educ Psychol Rev. (2020) 32:49–76. doi: 10.1007/s10648-019-09494-0
3. Verbitskaya LA, Zinchenko YP, Malykh SB, Gaidamashko IV, Kalmyk OA, Tikhomirova TN. Cognitive predictors of success in learning russian among native speakers of high school age in different educational systems. Psychol Russ State Art. (2020) 13:2–15. doi: 10.11621/pir.2020.0201
4. Ren X, Schweizer K, Wang T, Xu F. The prediction of students' academic performance with fluid intelligence in giving special consideration to the contribution of learning. Adv Cogn Psychol. (2015) 11:97. doi: 10.5709/acp-0175-z
5. Tikhomirova T, Malykh A, Malykh S. predicting academic achievement with cognitive abilities: cross-sectional study across school education. Behav Sci. (2020) 10:158. doi: 10.3390/bs10100158
6. Mantey AA, Annan RA, Lutterodt HE, Twumasi P. Iron status predicts cognitive test performance of primary school children from Kumasi, Ghana. PLoS ONE. (2021) 16:e0251335. doi: 10.1371/journal.pone.0251335
7. Nyaradi A, Li J, Hickling S, Foster J, Oddy WH. The role of nutrition in children's neurocognitive development, from pregnancy through childhood. Front Hum Neurosci. (2013) 7:97. doi: 10.3389/fnhum.2013.00097
8. Sundas Liaqat, Farida Bibi, Zahin Anjum, Jauhar Azeem, Sadaf Ambreen, Ayesha Bibi. A recent review on: effect of nutrients on brain function and development. Indus J Biosci Res. (2025) 3:125–35. doi: 10.70749/ijbr.v3i1.444
9. Richardson AJ, Burton JR, Sewell RP, Spreckelsen TF, Montgomery P. Docosahexaenoic Acid for Reading, Cognition and Behavior in Children Aged 7–9 years: A Randomized, Controlled Trial (the DOLAB Study) (2012). Available online at: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0043909 (Accessed November 12, 2024).
10. Gutema BT, Sorrie MB, Megersa ND, Yesera GE, Yeshitila YG, Pauwels NS, et al. Effects of iron supplementation on cognitive development in school-age children: systematic review and meta-analysis. PLoS ONE. (2023) 18:e0287703. doi: 10.1371/journal.pone.0287703
11. Bourre J-M. Effects of nutrients (in food) on the structure and function of the nervous system: update on dietary requirements for brain. Part 1: micronutrients. J Nutr Health Aging. (2006) 10:377–85.
12. de Moura JE, de Moura ENO, Alves CX, de Lima Vale SH, Dantas MMG, de Araújo Silva A, et al. Oral zinc supplementation may improve cognitive function in school children. Biol Trace Elem Res. (2013) 155:23–8. doi: 10.1007/s12011-013-9766-9
13. Aljaadi AM, Devlin AM, Green TJ. Riboflavin intake and status and relationship to anemia. Nutr Rev. (2022) 81:114–32. doi: 10.1093/nutrit/nuac043
14. Dror DK, Allen LH. Effect of vitamin B12 deficiency on neurodevelopment in infants: current knowledge and possible mechanisms. Nutr Rev. (2008) 66:250–5. doi: 10.1111/j.1753-4887.2008.00031.x
15. Zhang X-M, Huang G-W, Tian Z-H, Ren D-L, Wilson JX. Folate stimulates ERK1/2 phosphorylation and cell proliferation in fetal neural stem cells. Nutr Neurosci. (2009) 12:226–32. doi: 10.1179/147683009X423418
16. Annan RA, Apprey C, Asamoah-Boakye O, Okonogi S, Yamauchi T, Sakurai T. The relationship between dietary micronutrients intake and cognition test performance among school-aged children in government-owned primary schools in Kumasi metropolis, Ghana. Food Sci Nutr. (2019) 7:3042–51. doi: 10.1002/fsn3.1162
17. Gewa CA, Weiss RE, Bwibo NO, Whaley S, Sigman M, Murphy SP, et al. Dietary micronutrients are associated with higher cognitive function gains among primary school children in rural Kenya. Br J Nutr. (2009) 101:1378. doi: 10.1017/S0007114508066804
18. Jinabhai CC, Taylor M, Coutsoudis A, Coovadia HM, Tomkins AM, Sullivan KR, et al. randomized controlled trial of the effect of antihelminthic treatment and micronutrient fortification on health status and school performance of rural primary school children. Ann Trop Paediatr. (2001) 21:319–33. doi: 10.1080/07430170120093508
19. Van Den Briel T, West CE, Bleichrodt N, Van De Vijver FJ, Ategbo EA, Hautvast JG. Improved iodine status is associated with improved mental performance of schoolchildren in Benin. Am J Clin Nutr. (2000) 72:1179–85. doi: 10.1093/ajcn/72.5.1179
20. Staubli Asobayire F. Development of a food fortification strategy to compat iron deficiency in the Ivory Coast (PhD Thesis). ETH Zurich (2000). Available online at: https://www.research-collection.ethz.ch/bitstream/handle/20.500.11850/144858/eth-23739-01.pdf (Accessed July 8, 2024).
21. Righetti AA, Koua A-YG, Adiossan LG, Glinz D, Hurrell RF, N'Goran EK, et al. Etiology of anemia among infants, school-aged children, and young non-pregnant women in different settings of South-Central Côte d'Ivoire. Am Soc Trop Med Hyg. (2012) 87:425–34. doi: 10.4269/ajtmh.2012.11-0788
22. Rohner F, Northrop-Clewes C, Tschannen AB, Bosso PE, Kouassi-Gohou V, Erhardt JG, et al. Prevalence and public health relevance of micronutrient deficiencies and undernutrition in pre-school children and women of reproductive age in Côte d'Ivoire, West Africa. Public Health Nutr. (2014) 17:2016–28. doi: 10.1017/S136898001300222X
23. Fifi TM, Sylvère ZKYA, Fossou AF, Bitty MLA, Séraphin K-C. Assessment of the Nutritional Status of Schoolchildren in the Commune of Abobo (2023). Available online at: https://www.easpublisher.com/media/features_articles/EASJNFS_55_132-141_FT.pdf (Accessed April 6, 2024).
24. Zahe K, Méité A, Ouattara H, Dally T, Kouame KG, Aké-Tano O. Diet, nutritional status and school performance of schoolchildren in the district of Abidjan: case of Yopougon and Bingerville. J Nutr Health Sci. (2017) 4:102. doi: 10.15744/2393-9060.4.102
25. Yapo P. Nutritional status, sociodemographic status and academic performance of students in two selected secondary schools in Yopougon, Abidjan (Côte d'Ivoire). Age. (2018) 10:70. doi: 10.9790/7388-0804033844
26. Hürlimann E, Yapi RB, Houngbedji CA, Schmidlin T, Kouadio BA, Silué KD, et al. The epidemiology of polyparasitism and implications for morbidity in two rural communities of Côte d'Ivoire. Parasit Vectors. (2014) 7:81. doi: 10.1186/1756-3305-7-81
27. Koné S, Baikoro N., N'Guessan Y, Jaeger FN, Silué KD, Fürst T, Hürlimann E, Ouattara M, Séka M-CY, N'Guessan NA, et al. Health & demographic surveillance system profile: the Taabo health and demographic surveillance system, Côte d'Ivoire. Int J Epidemiol. (2015) 44:87–97. doi: 10.1093/ije/dyu221
28. de Onis M de, Onyango AW, Borghi E, Siyam A, Nishida C, Siekmann J. Development of a WHO growth reference for school-aged children and adolescents. Bull World Health Organ. (2007) 85:660–7. doi: 10.2471/BLT.07.043497
29. WHO. United Nations University/UNICEF., 2001 Iron Deficiency Anemia, Assessment. Geneva: Prev Control Guide Programme Manag Geneva WHO (2001).
30. Konz T, Migliavacca E, Dayon L, Bowman G, Oikonomidi A, Popp J, et al. ICP-MS/MS-based ionomics: a validated methodology to investigate the biological variability of the human ionome. J Proteome Res. (2017) 16:2080–90. doi: 10.1021/acs.jproteome.7b00055
31. WHO. WHO Guideline on Use of Ferritin Concentrations to Assess Iron Status in Populations. 1st ed. Geneva: World Health Organization (2020). 1 p.
32. Taljaard C, Covic NM, Graan AE, van Kruger HS, Smuts CM, Baumgartner J, et al. Effects of a multi-micronutrient-fortified beverage, with and without sugar, on growth and cognition in South African schoolchildren: a randomised, double-blind, controlled intervention. Br J Nutr. (2013) 110:2271–84. doi: 10.1017/S000711451300189X
33. Mayo Clinic Laboratories. Serum Iodine, Serum [Internet]. Rochester (MN): Mayo Foundation for Medical Education and Research (2023). Available online at: https://www.mayocliniclabs.com/test-catalog/overview/81574#Clinical-and-Interpretive (Accessed August 23, 2025).
34. Merck Manual Professional Edition. Hypocalcemia - Endocrine and Metabolic Disorders. Merck Man Prof Ed (2025). Available online at: https://www.merckmanuals.com/professional/endocrine-and-metabolic-disorders/electrolyte-disorders/hypocalcemia (Accessed August 22, 2025).
35. Mutua AM, Nampijja M, Elliott AM, Pettifor JM, Williams TN, Abubakar A, et al. Vitamin D status is not associated with cognitive or motor function in pre-school ugandan children. Nutrients. (2020) 12:1662. doi: 10.3390/nu12061662
36. Powers HJ. Riboflavin (vitamin B-2) and health12. Am J Clin Nutr. (2003) 77:1352–60. doi: 10.1093/ajcn/77.6.1352
37. Pfeiffer CM, Sternberg MR, Hamner HC, Crider KS, Lacher DA, Rogers LM, et al. Applying inappropriate cutoffs leads to misinterpretation of folate status in the US population. Am J Clin Nutr. (2016) 104:1607–15. doi: 10.3945/ajcn.116.138529
38. NHI Office of Dietary Supplements. Vitamin B12 Fact Sheet for Health Professionals (2022). Available online at: https://ods.od.nih.gov/factsheets/VitaminB12-HealthProfessional/ (Accessed August 23, 2025).
39. Suchdev PS, Namaste SM, Aaron GJ, Raiten DJ, Brown KH, Flores-Ayala R. Overview of the biomarkers reflecting inflammation and nutritional determinants of anemia (BRINDA) project. Adv Nutr. (2016) 7:349–56. doi: 10.3945/an.115.010215
40. John, RJ. Raven progressive matrices. In: Handbook of Nonverbal Assessment. McCallum RS, editor. Boston, MA: Springer US (2003). p. 223–37. doi: 10.1007/978-1-4615-0153-4_11
41. Ayalew M, Bayray A, Bekele A, Handebo S. Nutritional status and educational performance of school-aged children in Lalibela Town primary schools, Northern Ethiopia. Int J Pediatr. (2020) 2020:1–9. doi: 10.1155/2020/5956732
42. Costenbader V, Ngari SM, A. Kenya standardization of the Raven's coloured progressive matrices. Sch Psychol Int. (2001) 22:258–68. doi: 10.1177/0143034301223003
43. Morales S, Bowers ME, Shuffrey L, Ziegler K, Troller-Renfree S, Hernandez A, et al. Maternal education prospectively predicts child 783 neurocognitive function: An environmental influences on child health outcomes study. Dev Psychol (2024) 60:1028–40. doi: 10.1037/dev0001642
44. Unicef. La situation des enfants dans le monde 1998: regard sur la nutrition (1998). Available online at: https://www.youthpolicy.org/uploads/documents/1998_UNICEF_State_of_the_worlds_Children_Report_Fre.pdf (Accessed December 5, 2024).
45. Makoutode CP, Agueh D, Djogbenou L, Azandjeme C, Saizonou J. Comparative study of nutritional status and academic performance in schools with and without school canteens in south-west benin. Acta Sci Paediatr. (2022) 5:24–31. doi: 10.31080/ASPE.2022.05.0514
46. Khokhlov NA, Slovenko ED. Neuropsychological predictors of poor school performance. Mosc Univ Psychol Bull. (2020) 4:291–313. doi: 10.11621/vsp.2020.03.13
47. Anitha R. Nature, prevalence, and impact of undernutrition on intelligence among school children: a cross-sectional study from South India. ECS Trans. (2022) 107:637–46. doi: 10.1149/10701.0637ecst
48. Asmare B, Taddele M, Berihun S, Wagnew F. Nutritional status and correlation with academic performance among primary school children, northwest Ethiopia. BMC Res Notes. (2018) 11:805. doi: 10.1186/s13104-018-3909-1
49. van der Wurff ISM, Bakker EC, Hornstra G, Kirschner PA, Gielen M, Godschalk RWL, et al. Association between prenatal and current exposure to selected LCPUFAs and school performance at age 7. Prostaglandins Leukot Essent Fatty Acids. (2016) 108:22–9. doi: 10.1016/j.plefa.2016.03.005
50. Borasio F, De Cosmi V, D'Oria V, Scaglioni S, Syren M-LE, Turolo S, et al. Associations between dietary intake, blood levels of omega-3 and omega-6 fatty acids and reading abilities in children. Biomolecules. (2023) 13:368. doi: 10.3390/biom13020368
51. Scorletti E, Byrne CD. Omega-3 fatty acids, hepatic lipid metabolism, and nonalcoholic fatty liver disease. Annu Rev Nutr. (2013) 33:231–48. doi: 10.1146/annurev-nutr-071812-161230
52. Nazir F, Zahid H. Impact of unconventional Ω-3 sources on cognitive development: a nexus to explore for future brains. Food Sci Appl Biotechnol. (2023) 6:151–66. doi: 10.30721/fsab2023.v6.i1.232
53. Tia A, Konan AG, Hauser J, Ndri KY, Ciclet O, Esso LE, et al. A cross-sectional study of the relationship between dietary micronutrient intake, cognition and academic performance among school-aged children in Taabo, Côte d'Ivoire. (2025) doi: 10.20944/preprints202508.1374.v1
54. Bezkorovainy A. Biochemistry of nonheme iron in man. I Iron proteins and cellular iron metabolism. Clin Physiol Biochem. (1989) 7:1–17.
55. Halterman JS, Kaczorowski JM, Aligne CA, Auinger P, Szilagyi PG. Iron deficiency and cognitive achievement among school-aged children and adolescents in the United States. Pediatrics. (2001) 107:1381–6. doi: 10.1542/peds.107.6.1381
56. Bartzokis G. Age-related myelin breakdown: a developmental model of cognitive decline and Alzheimer's disease. Neurobiol Aging. (2004) 25:5–18. doi: 10.1016/j.neurobiolaging.2003.03.001
57. Georgieff MK. Long-term brain and behavioral consequences of early iron deficiency. Nutr Rev. (2011) 69:S43–8. doi: 10.1111/j.1753-4887.2011.00432.x
58. Nilsson TK, Yngve A, Böttiger AK, Hurtig-Wennlöf A, Sjöström M. High folate intake is related to better academic achievement in Swedish adolescents. Pediatrics. (2011) 128:e358–65. doi: 10.1542/peds.2010-1481
59. Syam A, Palutturi S, Djafar N, Astuti NB, Thaha AR. Micronutrients, academic performance and concentration of study: a literature review. Int J Appl Bus Econ Res. (2016) 14:2831–43.
60. Saindane KK, Talapadatur H, Parab U, Kumar V. Simultaneous estimation of folic acid and methotrexate in tablet dosage form by high-performance liquid chromatography. World J Pharm Res. (2022) 11:1662–7.
61. McGarel C, Pentieva K, Strain JJ, McNulty H. Emerging roles for folate and related B-vitamins in brain health across the lifecycle. Proc Nutr Soc. (2015) 74:46–55. doi: 10.1017/S0029665114001554
62. Ars CL, Nijs IM, Marroun HE, Muetzel R, Schmidt M, Steenweg-de Graaff J, et al. Prenatal folate, homocysteine and vitamin B12 levels and child brain volumes, cognitive development and psychological functioning: the Generation R Study. Br J Nutr. (2019) 122:S1–9. doi: 10.1017/S0007114515002081
63. Virdi S, Jadavji NM. The impact of maternal folates on brain development and function after birth. Metabolites. (2022) 12:876. doi: 10.3390/metabo12090876
64. Polyakov VM, Rychkova LV, Belogorova TA, Mikhnovich VI, Bugun OV, Berdina ON, et al. Influence of L-tryptophan use on the dynamics of cognitive functions in the complex therapy of delayed psycho-speech development in children. Bull Sib Med. (2018) 17:71–9. doi: 10.20538/1682-0363-2018-2-71-79
65. Galán C, Sánchez S, Franco L, Bravo R, Rivero M, Rodríguez AB, et al. Tryptophan-enriched antioxidant cereals improve sleep in children with autistic spectrum and attention deficit hyperactivity disorders. J Cell Neurosci Oxidative Stress. (2017) 9:608–16. doi: 10.37212/jcnos.334393
66. Friedman M. Analysis, nutrition, and health benefits of tryptophan. Int J Tryptophan Res. (2018) 11:1178646918802282. doi: 10.1177/1178646918802282
67. Roth W, Zadeh K, Vekariya R, Ge Y, Mohamadzadeh M. Tryptophan metabolism and gut-brain homeostasis. Int J Mol Sci. (2021) 22:2973. doi: 10.3390/ijms22062973
68. Silva LCA, Viana MB, Andrade JS, Souza MA, Céspedes IC, D'almeida V. Tryptophan overloading activates brain regions involved with cognition, mood and anxiety. An Acad Bras Ciênc. (2017) 89:273–83. doi: 10.1590/0001-3765201720160177
69. Porter RJ, Lunn BS, O'brien JT. Effects of acute tryptophan depletion on cognitive function in Alzheimer's disease and in the healthy elderly. Psychol Med. (2003) 33:41–9. doi: 10.1017/S0033291702006906
70. Visconti G, De Figueiredo M, Strassel O, Boccard J, Vuilleumier N, Jaques D, et al. Multitargeted internal calibration for the quantification of chronic kidney disease-related endogenous metabolites using liquid chromatography–mass spectrometry. Anal Chem. (2023) 95:13546–54. doi: 10.1021/acs.analchem.3c02069
71. Escobedo-Monge MF, Torres-Hinojal MC, Barrado E, Escobedo-Monge MA, Marugán-Miguelsanz JM. Zinc nutritional status in a series of children with chronic diseases: a cross-sectional study. Nutrients. (2021) 13:1121. doi: 10.3390/nu13041121
72. De Souza AS, Fernandes FS, Tavares do Carmo M das G. Effects of maternal malnutrition and postnatal nutritional rehabilitation on brain fatty acids, learning, and memory. Nutr Rev. (2011) 69:132–44. doi: 10.1111/j.1753-4887.2011.00374.x
73. Nga TT, Winichagoon P, Dijkhuizen MA, Khan NC, Wasantwisut E, Wieringa FT. Decreased parasite load and improved cognitive outcomes caused by deworming and consumption of multi-micronutrient fortified biscuits in rural vietnamese schoolchildren. Am J Trop Med Hyg. (2011) 85:333–40. doi: 10.4269/ajtmh.2011.10-0651
74. WHO. Iodine Status Worldwide: WHO Global Database on Iodine Deficiency. Geneva: Department of Nutrition for Health and Development, World Health Organization. (2004).
75. Schoenthaler SJ, Bier ID, Young K, Nichols D, Jansenns S. The Effect of vitamin-mineral supplementation on the intelligence of american schoolchildren: a randomized, double-blind placebo-controlled trial. J Altern Complement Med. (2000) 6:19–29. doi: 10.1089/acm.2000.6.19
76. Vazir S, Nagalla B, Thangiah V, Kamasamudram V, Bhattiprolu S. Effect of micronutrient supplement on health and nutritional status of schoolchildren: mental function. Nutrition. (2006) 22:S26–32. doi: 10.1016/j.nut.2004.07.021
77. Cruz-Rodríguez J, Canals-Sans J, Hernández-Martínez C, Voltas-Moreso N, Arija V. Prenatal vitamin B12 status and cognitive functioning in children at 4 years of age: The ECLIPSES Study. Matern Child Nutr. (2024) 20:e13580. doi: 10.1111/mcn.13580
78. Venkatramanan S, Armata IE, Strupp BJ, Finkelstein JL. Vitamin B-12 and cognition in children. Adv Nutr. (2016) 7:879–88. doi: 10.3945/an.115.012021
79. Laird E, Thurston SW, Van Wijngaarden E, Shamlaye CF, Myers GJ, Davidson PW, et al. Maternal vitamin D status and the relationship with neonatal anthropometric and childhood neurodevelopmental outcomes: results from the seychelles child development nutrition study. Nutrients. (2017) 9:1235. doi: 10.3390/nu9111235
80. Karimian P, Delavar MA. The effect of vitamin D deficiency on neurobehavioral outcomes and approaches in children: a systematic review. Ann Romanian Soc Cell Biol (2021) 25:4811–21.
81. Nassar MF, Amin DA, Hamed AI, Nassar JF, Abou-Zeid A-EK, Attaby MA. Vitamin D status and scholastic achievement in middle age childhood. J Egypt Soc Parasitol. (2012) 42:349–58. doi: 10.12816/0006322
82. Saponaro F, Alfi G, Cetani F, Matrone A, Mazoni L, Apicella M, et al. Serum calcium levels are associated with cognitive function in hypoparathyroidism: a neuropsychological and biochemical study in an Italian cohort of patients with chronic post-surgical hypoparathyroidism. J Endocrinol Invest. (2022) 45:1909–18. doi: 10.1007/s40618-022-01822-6
83. Katiyar A. Calcium's role in child growth and development and it's complications. J Res Appl Sci Biotechnol. (2022) 1:1–6. doi: 10.55544/jrasb.1.1.1
84. Fukagawa NK. Protein and amino acid supplementation in older humans. Amino Acids. (2013) 44:1493–509. doi: 10.1007/s00726-013-1480-6
85. de Curtis M, Uva L, Gnatkovsky V, Librizzi L. Potassium dynamics and seizures: why is potassium ictogenic? Epilepsy Res. (2018) 143:50–9. doi: 10.1016/j.eplepsyres.2018.04.005
86. Kou C, Zhao X, F X, Lin X, Wang Q, Jing Y. Dietary sodium/potassium intake and cognitive impairment in elderly patients with hypertension: data from NHANES 2011-2014. J Hypertens. (2023) 41:e274. doi: 10.1097/01.hjh.0000941848.06878.b3
87. Folwaczny A, Waldmann E, Altenhofer J, Henze K, Parhofer KG. Postprandial lipid metabolism in normolipidemic subjects and patients with mild to moderate hypertriglyceridemia: effects of test meals containing saturated fatty acids, mono-unsaturated fatty acids, or medium-chain fatty acids. Nutrients. (2021) 13:1737. doi: 10.3390/nu13051737
88. Paparella R, Panvino F, Leonardi L, Pucarelli I, Menghi M, Micangeli G, et al. Water-soluble vitamins: hypo- and hypervitaminosis in pediatric population. Pharmaceutics. (2025) 17:118. doi: 10.3390/pharmaceutics17010118
89. Rai PS, Bhandary YP, Shivarajashankara YM, Akarsha B, Bhandary R, Prajna RH, et al. Interlinking the cross talk on branched chain amino acids, water soluble vitamins and adipokines in the type 2 diabetes mellitus etiology. Endocr Metab Immune Disord - Drug Targets. (2025) 25:757–66. doi: 10.2174/0118715303305579241014112730
90. Fairweather-Tait SJ. Biomarkers of micronutrient status. Br J Nutr. (2008) 99:S1. doi: 10.1017/S0007114508006788
91. Suchdev PS, Williams AM, Mei Z, Flores-Ayala R, Pasricha S-R, Rogers LM, et al. Assessment of iron status in settings of inflammation: challenges and potential approaches. Am J Clin Nutr. (2017) 106:1626S−33. doi: 10.3945/ajcn.117.155937
Keywords: nutrient, cognition, school performance, school-aged children, sub-Saharan Africa, Côte d'Ivoire
Citation: Tia A, Hauser J, Konan AG, Ciclet O, Grzywinski Y, Mainardi F, Visconti G, Frézal A and Nindjin C (2025) Unraveling the relationship between nutritional status, cognitive function, and school performance among school-aged children in Taabo, Côte d'Ivoire: a school-based observational study. Front. Nutr. 12:1630497. doi: 10.3389/fnut.2025.1630497
Received: 17 May 2025; Accepted: 08 September 2025;
Published: 21 October 2025.
Edited by:
Enrico Collantoni, University of Padua, ItalyReviewed by:
Soumyadip Mukherjee, Rajiv Academy for Pharmacy, IndiaWatson Ray Gyan, Guangdong Medical University, China
Copyright © 2025 Tia, Hauser, Konan, Ciclet, Grzywinski, Mainardi, Visconti, Frézal and Nindjin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Achil Tia, YWNoaWwudGlhMjNAZ21haWwuY29t; YWNoaWwudGlhQGNzcnMuY2k=