 Cinthya Neglia-Cermeño1
Cinthya Neglia-Cermeño1 Susana Edita Paredes-Díaz2,3
Susana Edita Paredes-Díaz2,3 Nancy Soto-Deza3
Nancy Soto-Deza3 Jaime Bazán-Cabellos4
Jaime Bazán-Cabellos4 Nélida Milly Otiniano3,5*
Nélida Milly Otiniano3,5* Jorge Luis Díaz-Ortega1,3*
Jorge Luis Díaz-Ortega1,3* Luz Angélica Castro-Caracholi1
Luz Angélica Castro-Caracholi1 Juan Ernesto Valdiviezo-Campos1
Juan Ernesto Valdiviezo-Campos1 Victoria Ramos Torres1
Victoria Ramos Torres1 Carol Abanto-Quiroa6
Carol Abanto-Quiroa6 Mariana Zariquiey-Rubio6
Mariana Zariquiey-Rubio6 Karla Nazario-Terrones4
Karla Nazario-Terrones4 Gissela Esteban-Dionicio6
Gissela Esteban-Dionicio6- 1Universidad César Vallejo, Escuela de Nutrición, Trujillo, Peru
- 2Universidad César Vallejo, Escuela de Medicina, Piura, Peru
- 3Universidad César Vallejo, Institutos y Centros de Investigación, Trujillo, Peru
- 4Danper, Gerencia de Salud, Trujillo, Peru
- 5Universidad César Vallejo, Escuela de Medicina, Trujillo, Peru
- 6Danper, Gerencia Técnica, Trujillo, Peru
Objective: To demonstrate the preventive effect against anemia in children by the consumption of a blueberry and quinoa drink enriched with iron as part of a nutritional program.
Method: The nutrition program involved 42 children aged 1 to 6 years. They were the children of workers in an agro-industrial company in the city of Trujillo, where they received a blueberry and quinoa drink enriched with iron in the form of ferric pyrophosphate (BQDEI), the content of which in a 200 mL bottle provides 14 mg of Fe. For children without anemia the dose was 1 bottle per day and for children with mild anemia the dose was 2 bottles per day for a period of 6 months. Educational and demonstration sessions were held for parents or caregivers regarding proper food handling, safe water consumption, the importance of personal hygiene and the benefits of a balanced diet rich in iron. In addition, nutritional status evaluation, parasitosis control and ferritin and hemoglobin measurements were performed at the beginning, third and sixth month during the development of the nutritional program.
Results: 50% of the children with short stature reached normal height, and 80% of the children’s weight/height went from overweight to normal, and these changes were significant. Ferritin concentration in the initial, intermediate and final phases was 40.67 ± 25.20 ng/ml, 49.37 ± 22.41 ng/ml and 54.19 ± 35.38 ng/ml, respectively, showing a significant increase. The hemoglobin concentration was 11.71 ± 0.91 g/dl, 11.83 ± 0.88 g/dl and 11.99 ± 1.03 g/dl, respectively, and the increase was not significant.
Conclusion: It was demonstrated that the consumption of BQDEI within a nutritional program contributed to the prevention of anemia in children, by improving hemoglobin and ferritin concentrations. Therefore, it could be implemented in other areas where children are more vulnerable to anemia.
1 Introduction
Anemia is a worldwide health problem characterized by a low hemoglobin (Hb) blood concentration. This nutritional disorder can occur at any stage of life. However, women and preschool children are the most vulnerable (1). It occurs in populations of various regions, genders and ages. Anemia is most prevalent in developing countries (2), and is a health problem of particular concern in third world nations. In this sense, the World Health Organization (WHO) specifies Hb levels below 11 g/dl for this pathology (3) and that, worldwide, it occurs in approximately 40% of children aged 6 to 59 months (4). In 2023, in Peru, anemia affected 43.1% of children aged 6 to 35 months. The highest incidence was in rural areas (50.3%) compared to urban areas (40.2%). This problem was more prevalent in the departments of Puno, Ucayali, and Madre de Dios, at 70.4, 59.4, and 58.3%, respectively (5). In the case of La Libertad, anemia varied from 17.0% in 2001 to 21.1% in 2024 (6). The age group with the highest level of anemia corresponds to children between 6 and 18 months of age between 54 and 65% (7).
Childhood anemia is a multifactorial condition with a high global prevalence, particularly among children under 3 years of age (47%), with higher rates observed in low-income countries (70%) and among disadvantaged indigenous populations (30%). It is associated with deficiencies in the nutrients iron, folate and vitamin B12, as well as intestinal parasitosis, chronic infectious diseases, premature birth, low birth weight and poor breastfeeding practices involving the consumption of cow’s milk (8–15). Conversely, exclusive breastfeeding and a high socioeconomic status act as protective factors (16). Genetic causes affecting Hb synthesis and blood cell formation are also recognized (17). This condition is also related to variables such as age, sex, race, illiteracy (18–21), other nutritional deficiencies such as folate and vitamin B12 (14, 22), and poor sanitary conditions, including limited access to clean drinking water (23, 24), leads to infection by parasites and bacteria that compete for iron in the intestine (22, 25). Finally, the availability of medical services, the family environment, and childcare practices also influence its prevalence (1, 26).
International agencies such as WHO recommend a combination of four basic strategies including iron supplementation, nutritional education, fortification of foods with iron compounds, and control of parasitic and infectious diseases to prevent and control anemia (27). Likewise, the nutrition education applied should be easily adapted to the socioeconomic status, dietary habits and traditional food resources available locally (28, 29).
Nutritional programs play a crucial role not only in the treatment of anemia, but also in its prevention and long-term management, as they provide a comprehensive strategy to address nutrient deficiencies and improve the overall health of children. This is why Soncco-Sucapuca et al. (30) applied a nutritional education program in parents of Peruvian children, achieving a significant decrease in anemia in their children through the consumption of iron-fortified bread, the promotion of healthy practices and the improvement of the level of knowledge about iron deficiency anemia. Likewise, Reyes et al. (31), evaluated the impact of a community intervention program, which included mass campaigns and group workshops for children and parents on issues related to anemia and malnutrition, and showed that the program had a positive influence on the reduction of anemia and malnutrition in children.
It is very important to treat anemia in children under 3 years of age, as it can cause children to become severely and long-term ill, resulting in mental decline, learning and concentration difficulties, poor school performance, stunted growth, impaired motor skills, slow language development, behavioral problems, low immunity, fatigue, lethargy, vulnerability to infections, and an elevated risk of mortality and morbidity (14, 18, 32).
Iron compounds used in food fortification are classified as inorganic salts, organic salts, and chelates. Ferrous sulfate, a low-cost, highly soluble inorganic salt, is widely used, although its high reactivity can affect the sensory properties of certain products. Organic salts (gluconate, lactate, citrate) are also soluble and reactive, while other less soluble salts (saccharate, succinate, fumarate) have good gastric bioavailability but are not suitable for flours due to their tendency to rancidity (33). Ferric pyrophosphate (FPP), an iron compound insoluble in water, is commonly incorporated into cereal products due to its favorable sensory stability. However, its limited gastrointestinal absorption poses a challenge for effective iron delivery (34).
Micronization techniques have been shown to enhance its bioavailability without compromising the organoleptic or functional properties of the food matrix. In contrast, iron–amino acid chelates exhibit superior absorption and minimal reactivity, positioning them as a promising alternative for nutritional supplementation (35).
Hb concentration and serum ferritin are key biomarkers of iron metabolism, as Hb, the main component of erythrocytes, depends on iron for the synthesis of the heme group, a process regulated by erythropoietin in the bone marrow (36).
Blueberries are fruits that, in addition to providing antioxidants, also provide iron, which varies between 2.8 and 8.9% of the daily requirement of this mineral in children, according to different reports (37–39). The protein content of blueberries ranges from 0.32 to 0.62% per 100 g of product (40).
In the present study, a blueberry-based drink has been developed, enriched with iron using FPP, which is also stabilized with amino acids. The addition of quinoa, an Andean grain that provides between 19.34 and 20.90 g per 100 g of product (41), increases the protein content.
Based on the above, the hypothesis was proposed that the administration of a nutritional drink made from blueberries and quinoa enriched with iron, as part of a dietary intervention program, generates a significant increase in Hb and serum ferritin levels in children.
This is why, this research aims to evaluate the prevention of anemia in children through the consumption of a blueberry and quinoa drink enriched with iron within a nutritional program as an option to counteract the rate of childhood anemia.
2 Materials and methods
2.1 Selection of the participants
The participants were children of workers of an agro-industrial company in the city of Trujillo. The selection criteria included children with mild anemia (14%) and children without anemia (86%), and with an age range of 1–6 years. Also, children without parasitosis and those who had an antiparasitic treatment prior to the beginning of the study were considered. On the other hand, those children with incomplete laboratory data, non-tolerance to the product, parental decision not to continue in the study were excluded.
For the sample size calculation, the following formula was considered (42):
In this formula, the value of Zα/2 was set at 1.96; a statistical power of 0.9 was considered, resulting in a Zβ value of 1.28. Cohen’s d was 0.55, derived from the difference in mean Hb concentrations and a standard deviation equal to the square root of the sum of the sample variances divided by two (43). The data corresponded to the period before and after the implementation of a nutritional program developed in Puno (30). The calculated sample size “n” was 35, but a 20% increase was applied to account for potential attrition, resulting in a final sample of 42 participating children.
Initially, 77 children were considered eligible and monitored across three stages: initial, intermediate, and final. Among them, those who did not attend the laboratory tests for Hb and ferritin were excluded, one in the initial stage, four in the intermediate stage, and two in the final stage of the study. Additionally, 17 children were excluded during the intermediate stage for not consuming the product due to lack of acceptance, and 11 children were excluded because their parents withdrew from the study for external and personal reasons. Therefore, the final sample for analysis consisted of 42 children (Figure 1).
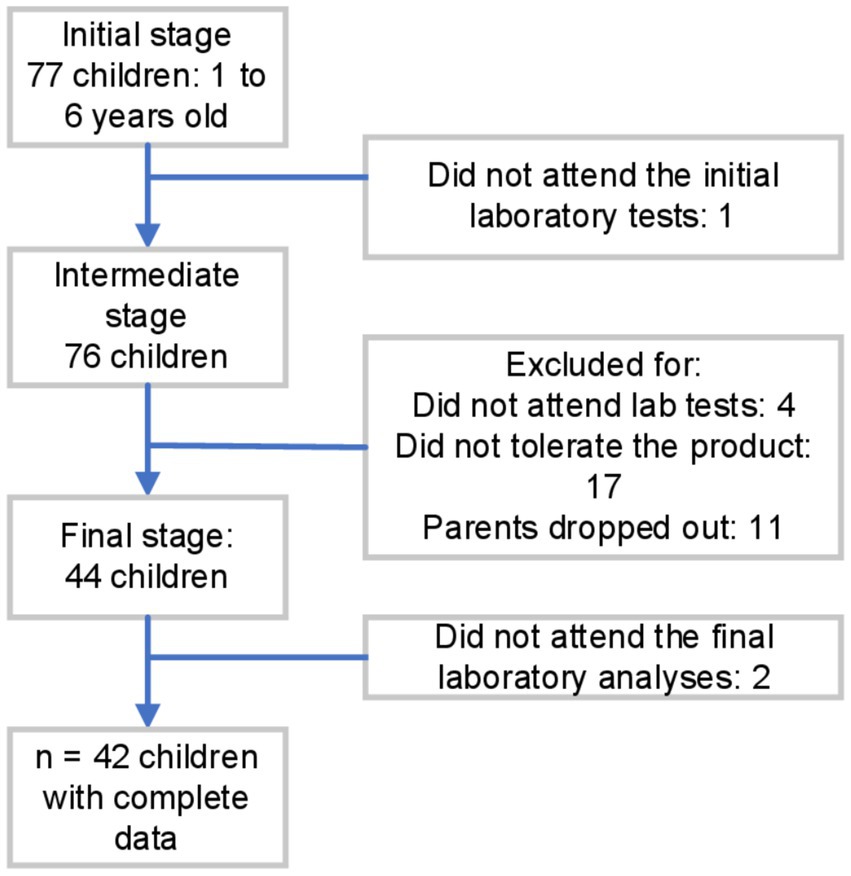
Figure 1. Flow chart of inclusion and exclusion criteria of individuals.
2.2 Design of the study
The research was designed as a pre-experimental study for a period of 6 months, in which the children entered a nutritional program that included the provision of the BQDEI. The study period was chosen because depleted body iron stores require no less than 4 months of iron supplementation for proper recovery (44).
2.3 Characteristics of the drink and administration
The BQDEI was manufactured at the processing plant of the agro-industrial company located in the province of Trujillo, La Libertad region. Glass bottles with a capacity of 200 ml (205 g) were used for packaging, in compliance with current regulations and standards (45). In addition, it had a sanitary registration (RSA P2761222N LADNTU) issued by the General Direction of Environmental Health and Food Safety (DIGESA, from Spanish initials) and official technical validation of Hazard Analysis and Critical Control Points in accordance with Directorial Resolution, file N°24,099-2024-CH (46).
A sensory evaluation of the product was carried out with the aim of determining its acceptability among children. The methodology was based on ASTM E2299-13 (47), Standard Guide for Sensory Evaluation of Products by Children and Minors, which allows the use of facial scales in children from 3 years of age. This guide presents examples of scales from 3 to 9 points, without establishing a mandatory format, provided that it is understandable to minors. In this study, a 5-point facial scale was used, selected for its simplicity and clarity, which facilitates interpretation by children and improves the reliability of responses (Supplementary Instrument S1). Twenty-eight children between the ages of 9 and 10 participated, all with written permission from their parents or guardians. This age group was chosen because of their greater cognitive development, verbal ability, and understanding of scales, which allowed for more accurate sensory data to be obtained. Before the evaluation, a familiarization session was held with the terms and expressions of the scale, using visual examples and explanations adapted to the age of the participants. The product received an average rating of 4.29 points, with 89% favorable responses, demonstrating high acceptance. Subsequently, the delivery of the product was organized to the parents of children aged 1 to 6 who expressed interest in participating, using an individualized schedule that ensured orderly and personalized distribution.
The drink was fortified with iron using FPP stabilized with amino acids and sourced from an international supplier specializing in food-grade supplements. This innovative iron source offers high bioavailability and stability under demanding processing conditions, as well as sensory compatibility. These properties make it suitable for use in fortified foods and drinks. The formulation enables higher concentrations to be achieved without altering the organoleptic properties and reduces iron reactivity, enhancing intestinal absorption while minimizing adverse effects such as gastric discomfort or a metallic aftertaste. It also ensures uniform distribution in liquid matrices (48).
As illustrated in the product processing flow diagram in Supplementary Figure S1, FPP was added during the ingredient incorporation stage of smoothie preparation, at the same time as the quinoa, blueberry and other components.
The BQDEI contains the equivalent of 7.0 mg of iron in 100 ml of the drink. In an external laboratory (accreditation certificate D PL146020100 according to DIN EN ISO/IEC 17025:2018), iron analyses were performed during product development and over the course of the product shelf life, with the iron content remaining stable. The nutritional composition of the BQDEI for 1 bottle (200 ml) is detailed in Table 1.
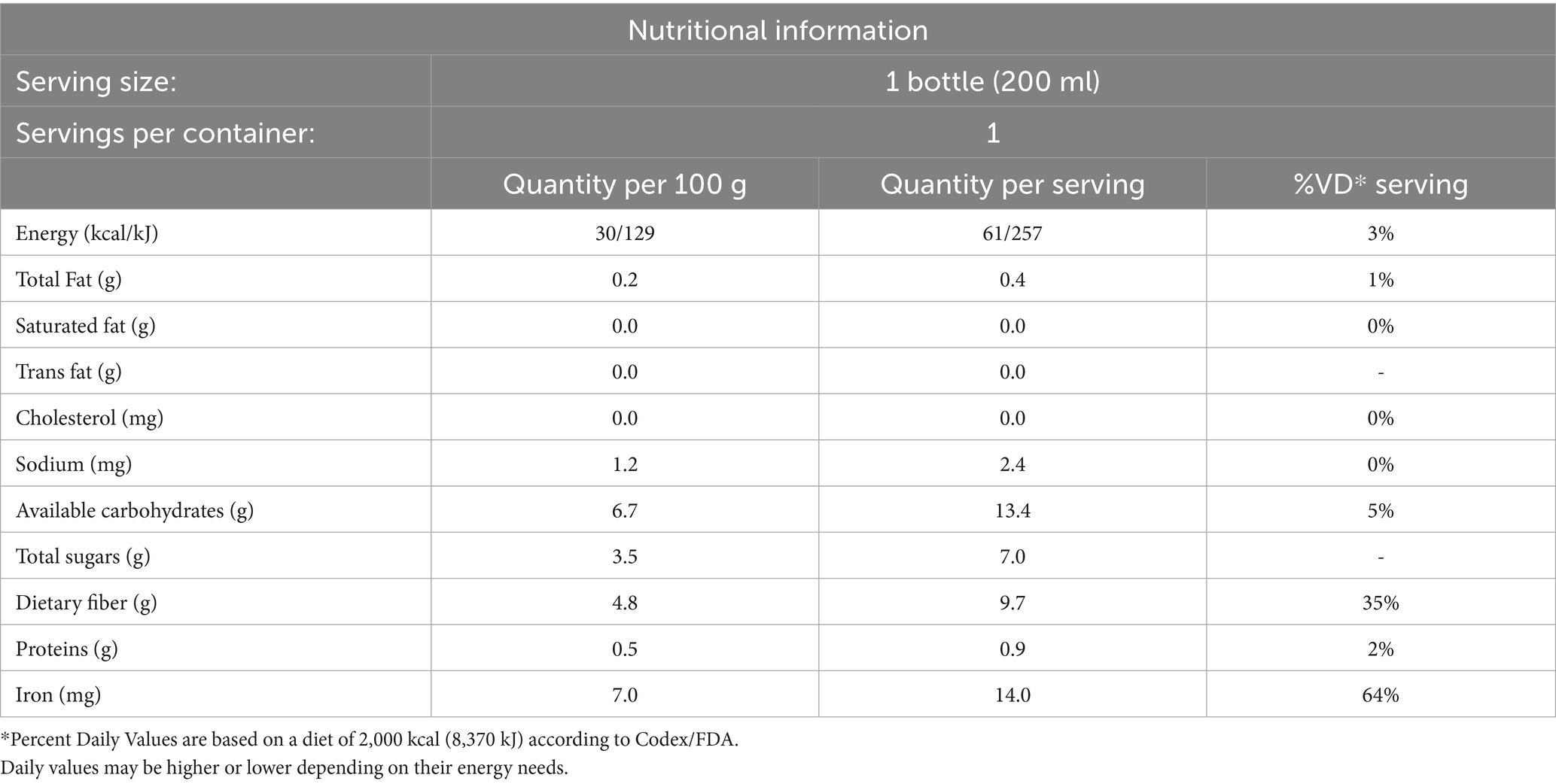
Table 1. Nutritional composition of the BQDEI.
For children without anemia the dose was 1 bottle per day and for children with mild anemia the dose was 2 bottles per day (morning and afternoon).
2.4 Nutritional program
In addition to the consumption of the BQDEI, the nutritional program included a series of activities such as: pediatric care, nutritional care, detection and treatment of parasites. Anemia detection through Hb and ferritin analysis, as well as educational sessions on balanced nutrition and iron-rich foods, and home visits. One of the important aspects of the nutritional program was the follow-up based on a schedule of visits, which made it possible to adjust intervention strategies in real time through direct observation of the children’s eating behavior during the intervention stage. One of the activities carried out was personalized counseling, which used the plate of good eating to specify the appropriate portions and quantities that the child should consume during the day (49). These details ensured that families receive guidance tailored to their needs, thus promoting sustainable eating habits.
In order to optimize its impact, the program was based on two fundamental theories. According to Albert Bandura’s Social Learning Theory (50), parents acquire appropriate behaviors through observation during home visits and practical demonstrations. The positive reinforcement facilitated the consolidation of these habits; The Transtheoretical Model of Behavior Change (51) was used within the study, helping families to move through the stages of change, from awareness of the importance of iron to the sustained adoption of healthy practices.
Educational and demonstration sessions for parents/caregivers included training on proper food handling, safe water consumption, the importance of personal hygiene, and the benefit of an iron-rich diet. Parents/caregivers were educated about high, medium and low iron foods and how they should be combined.
Ongoing nutritional counseling and home visits made it possible to adapt the consumption of the BQDEI within their daily diet through practical demonstrations at home to parents, guiding and reinforcing the consumption of the BQDEI and the recommended intake for each child according to their needs during the nutritional intervention.
2.5 Determination of the socioeconomic characteristics of the children’s families
To identify the socioeconomic characteristics of the children’s families, a data collection form was used according to Pacovilca et al. (52), which was answered by the child’s father, mother or caregiver and included data on family income, occupation, marital status, education level, origin, number of members and basic services (Supplementary Instrument S2).
2.6 Anthropometric nutritional evaluation
The anthropometric nutritional evaluation was carried out by nutritionists and nutrition facilitators in two stages (initial and final) with the application of the technical guide for the anthropometric nutritional evaluation of children aged 0 to 11 years (53). For children under 5 years of age, the weight/height parameter with categories of severe malnutrition, malnutrition, normal, overweight and obesity and height/age with categories of severe low, low, normal and high height were used for the nutritional diagnosis according to sex. For children over 5 years of age with the diagnosis of BMI/age and height/age according to gender. The evaluation protocols of the anthropometrist’s manual and the MINSA tables (54, 55) were applied to establish normal values and refer to their anthropometric conditions (Supplementary Tables S1–S3).
2.7 Evaluation of dietary patterns
We used a card proposed by Arimond et al. (56) in charge of the nutrition facilitators; it considered as indicators the consumption of 6 food groups: cereals, roots and tubers; legumes and nuts; dairy products; meat and red offal and finally fruits and vegetables according to the frequency of daily consumption, 1, 2, 3, 4, 5 and 6 times/week, both at the initial and final moment of the nutritional program, with instruments such as the frequency of consumption of food groups, both at the initial and final moment of the nutritional program (Supplementary Instrument S3). Likewise, the 24-h recall method was applied as described in the nutritional diagnosis protocol of the Association of Nutritionists of Peru, which is governed by MINSA regulations (54). This protocol is based on collecting as much data as possible about the food and drinks consumed the previous day, including type, quantity and method of preparation. Thus, the accuracy of the information collected from the responses to the food pattern questionnaire is reinforced by recalling the short-term memory.
2.8 Evaluation for the presence of intestinal parasites
Stool samples were collected using coded plastic containers given to the mothers or caregivers of the children with detailed instructions for serial collection and storage at three different times every 24 h starting at 7 am of the day. Stool samples contaminated with water or urine were rejected. Stool samples were kept in cold chain (57), until they were transferred to the Home Safety laboratory of the Policlínico de Alta Gracia in the city of Trujillo, where they were analyzed.
To detect the presence of intestinal parasites, feces were examined by direct observation with lugol. Positive samples were stored in a plastic tube containing 10% formalin. Single qualitative thick Kato-Katz smears were prepared from each stool sample and examined with a Gretlab microscope, model XSZ159, China at 10X and 40X for the presence of helminths. All participants were given the analyses and the children with positive results underwent a pediatric consultation where they received individualized treatment for parasitosis as appropriate (58, 59).
2.9 Hemoglobin and ferritin analysis
The blood samples were collected by venipuncture in vacutainer; 5 ml of blood were drawn aseptically; in purple tubes with anticoagulant K2E EDTA (ethylenediaminetetraacetic acid) and the samples were coded for identification of each participant. The tubes were placed in a cooler box at 15 °C until analysis in the Home Safety Sac laboratory. The blood samples were centrifuged at 3000 rpm for 10 min at room temperature with a Greetmed centrifuge, model GT119-300, China and stored at −20° C.
The Hb concentration was measured using a Horiba ABX SAS hematological analyzer model ABX Pentra XL80, France. For the classification of the diagnosis of anemia according to the specific age of each child at the end of the study, two technical standards issued by MINSA (60, 61) were considered (Supplementary Table S4).
To measure ferritin concentration, the chemiluminescence method (62) was used with the Snibe immunoassay analyzer, model Maglumi 800, China. These analyses were performed at three time points: Basal, at the third and at the sixth month during the development of the nutritional program.
Anemia was defined as a reduction in Hb levels below the reference values specified in Supplementary Table S4. To assess iron status in children, serum ferritin concentrations were measured, applying a threshold of 20 ng/ml. Values below this cutoff were interpreted as indicative of iron deficiency, given their alignment with the plateau phases of other physiological markers. Specifically, reduced mean corpuscular volume suggested hypochromia, while decreased mean corpuscular Hb reflected microcytosis (63).
2.10 Statistical analysis
The SPSS statistical program Version 26 was used. For descriptive statistics, frequencies and percentages were used for the different categories of baseline characteristics, anthropometric nutritional status, presence of parasites and dietary patterns. Since the means and standard deviation for ferritin and Hb concentrations did not show a normal distribution, the nonparametric Friedman test was used in the inferential analysis (64), to compare them before, during, and after the implementation of the nutritional program, with a 95% confidence interval and a comparative significance level of 0.05. Cohen’s d was applied to calculate the effect size, considering the ferritin and Hb averages and the standard deviation between the baseline and end of the nutritional program. This effect was corroborated with Kendall’s W to analyze the difference between the initial and final ferritin and Hb medians. Values from 0.2 to 0.49 indicate a small difference; from 0.5 to 0.79, a moderate difference; from 0.8 to 1.29, large (65).
2.11 Ethical aspects
The present research has been approved by the Ethics Committee of the Professional School of Nutrition of the Universidad César Vallejo with Report PI-CEI-NUTRITION-2023-001. Ethical principles were considered according to the Declaration of Helsinki (66) in relation to the care of integrity, privacy, confidentiality of personal information and respect for their autonomy. The informed and voluntary consent of the parents was considered, in which the objectives of the study, the procedures to be developed and the information on the risk–benefit of the nutritional program were oriented, in which it was assured that there would be no implication on the physical integrity of the children. The decision of the parent not to continue with the research in special situations or disagreement was also respected, without adversely affecting the researcher-participant relationship.
3 Results
3.1 Socioeconomic characteristics of the children’s families
According to Table 2, among the most relevant socioeconomic characteristics, it was found that the family income is greater than $ 534.76 in 76.2% of the families, the most predominant occupation of the parents is dependent in 85.7%; the majority are married or cohabiting, and the most prevalent level of education is high school in two thirds of the families. More than three-quarters of these families come from urban areas; all have access to sewage systems, but 11.9% lack potable water and 14.3% do not have electricity service.
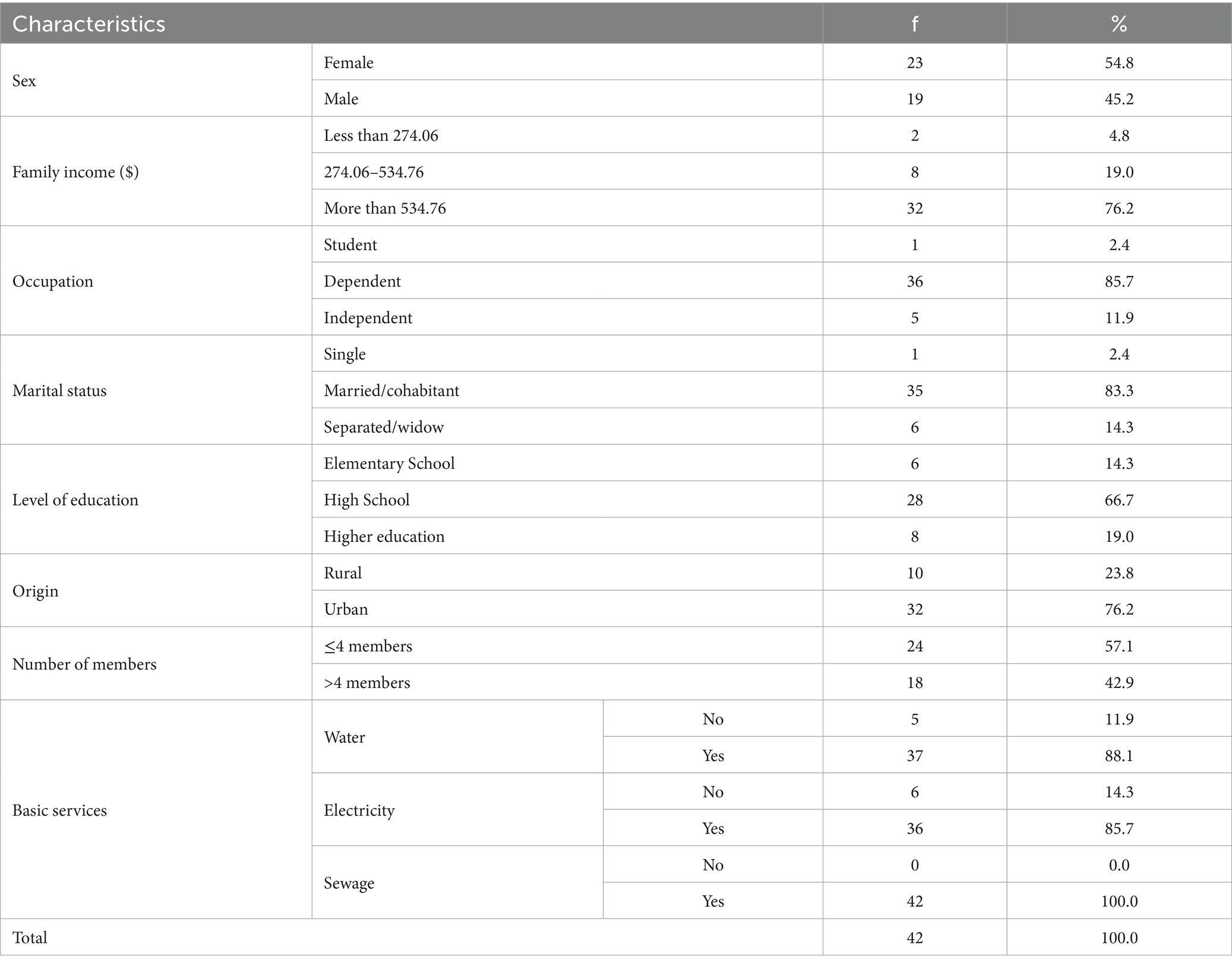
Table 2. Basal socioeconomic characteristics of children under 6 years of age who consumed the BQDEI as part of a nutritional program.
3.2 Anthropometric nutritional status
Table 3 shows that the proportion of children with normal height/age increased from 85.7 to 95.2%, the most important fact being that two of the four children (50%) with low height managed to reach normal height significantly (p < 0.001). Regarding the anthropometric measure weight/height, it was observed that of the five children who started with overweight, 80% managed to reach a normal weight and one child in a state of malnutrition reverted this situation at the end of the study, so the intervention applied was successful (p < 0.001).
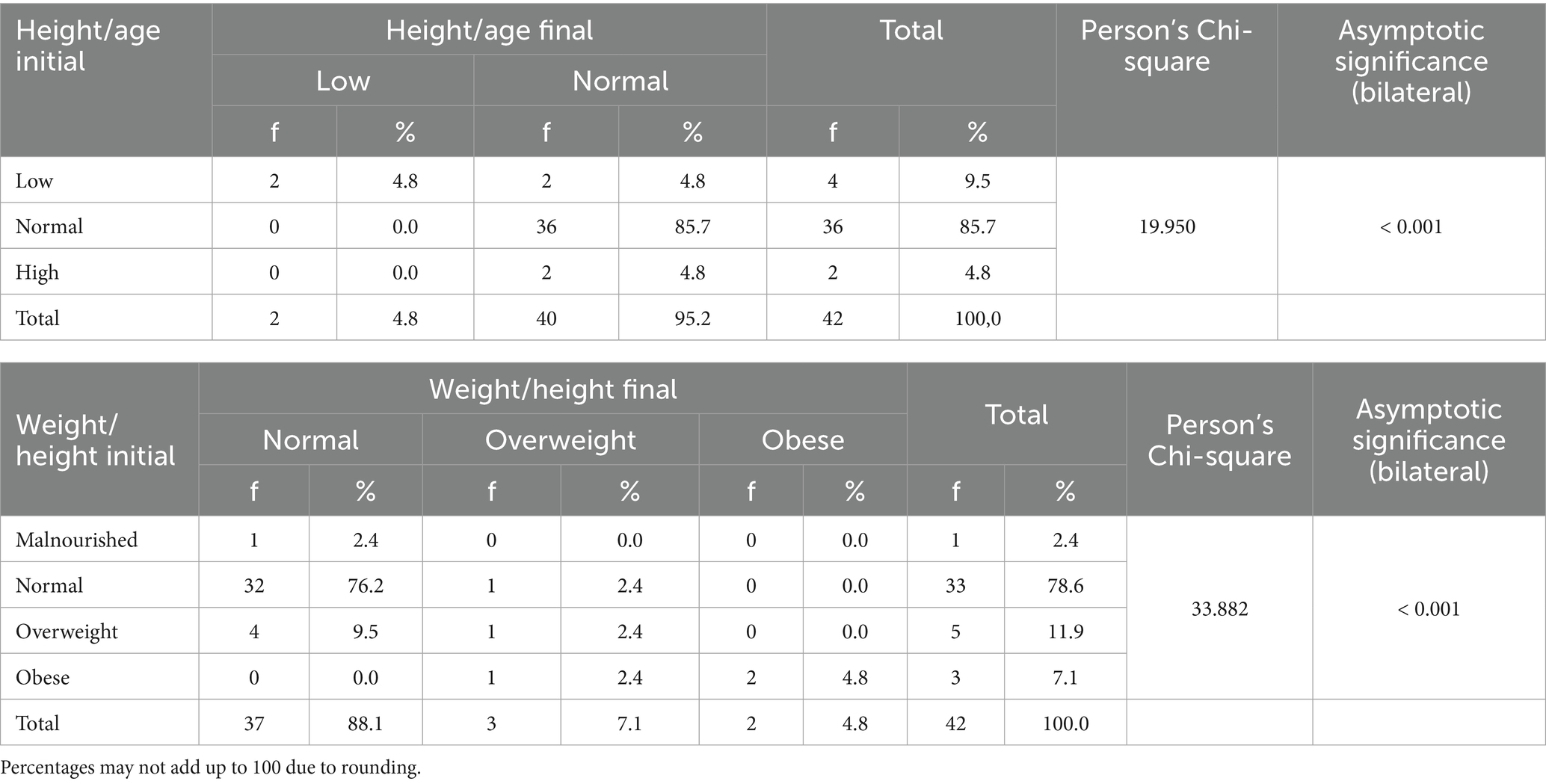
Table 3. Initial and final anthropometric assessment (height/age and weight/height) in children under 6 years of age during the consumption of BQDEI within a nutritional program.
3.3 Dietary patterns
Table 4 shows the dietary patterns at the beginning and end of the nutritional program in which there is an adequate consumption of protein foods such as eggs between 3 and 4 times a week (78.5 and 81%), foods rich in protein and iron such as legumes between 3 and 4 times a week (71.5 and 69.1%) and a high proportion of meat and fruit consumption on a daily basis in 90.5% at both times.
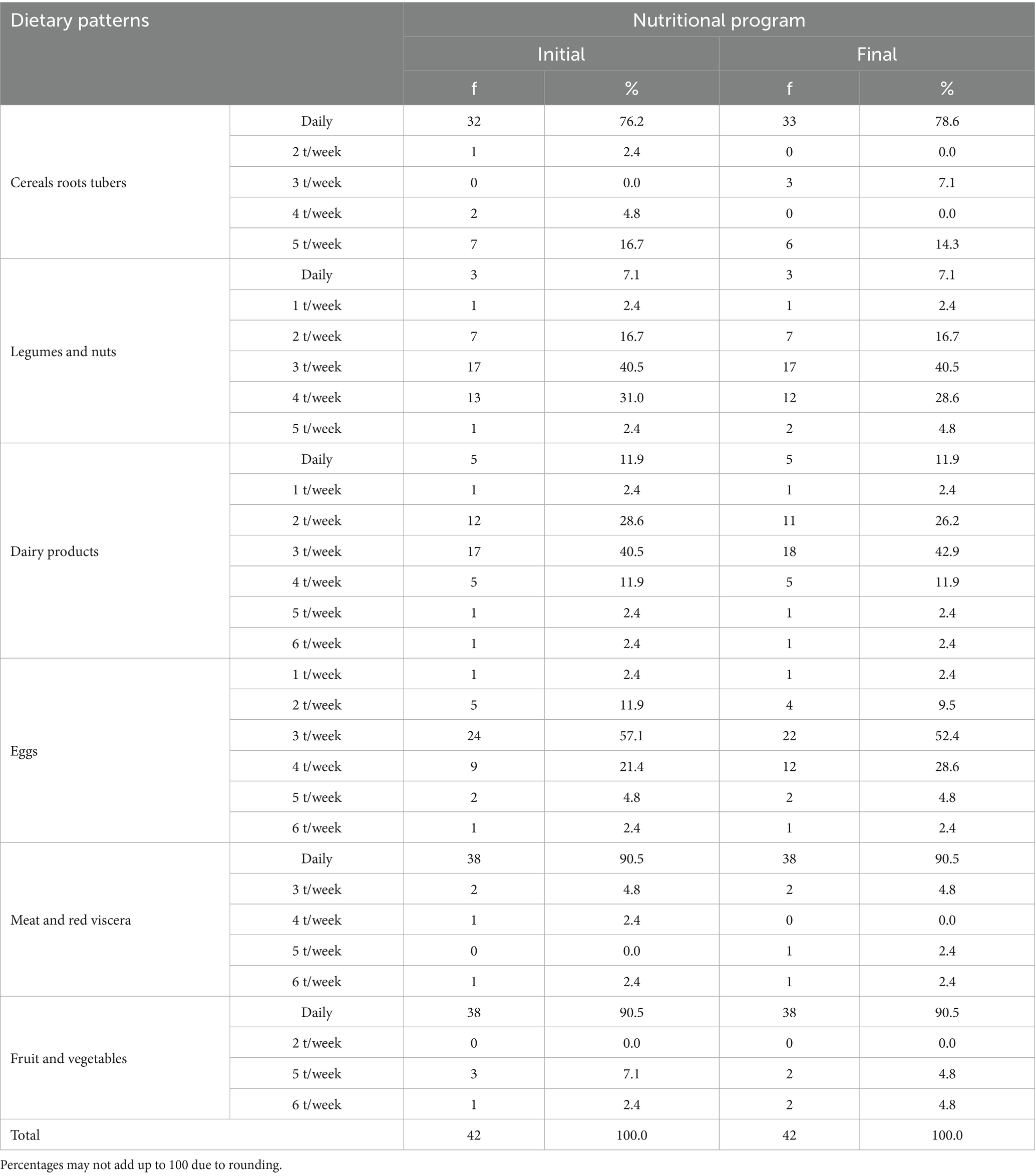
Table 4. Dietary patterns in children under 6 years of age at the beginning and end of the BQDEI consumption within a nutritional program.
3.4 Presence of intestinal parasites
Table 5 shows that parasites were present in 11.9% of children at the start of the nutritional program, 9.5% at the first follow-up and 7.0% at the final follow-up. Entamoeba coli, Blastocystis hominis, and Giardia lamblia cysts were not present at the first or second follow-up appointments, except for G. lamblia in one child. Enterobius vermicularis eggs were also observed, with a higher frequency in four children at the second follow-up.

Table 5. Presence of intestinal parasites in children under 6 years of age who participated in the nutritional program.
3.5 Ferritin and hemoglobin concentration
Table 6 shows the ferritin concentrations of the children in the basal, intermediate and final stages of BQDEI consumption, with an increasing trend and in which there is a very significant increase of approximately 13.5 ng/ml in the ferritin concentration in the final stage compared to the measurement made before the application of the nutritional program.
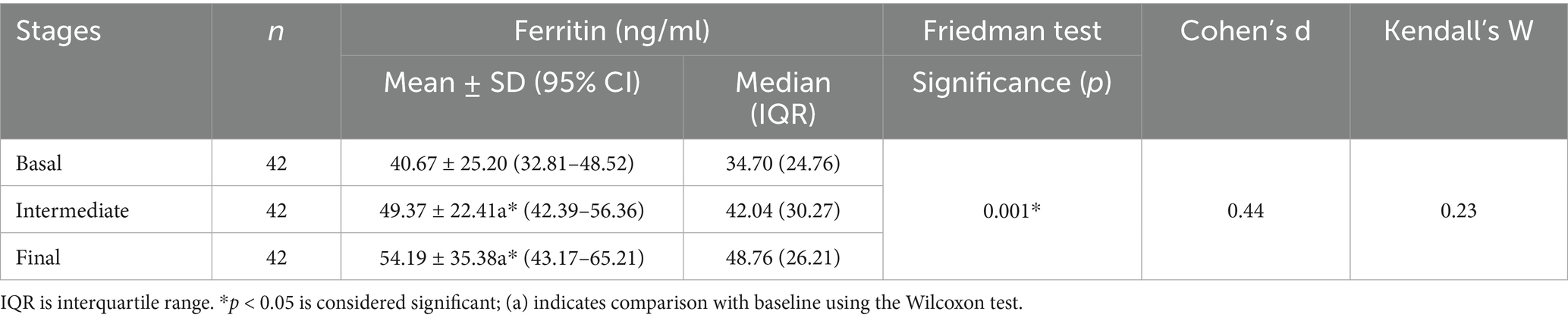
Table 6. Ferritin concentration in children under 6 years of age in the basal, intermediate and final stages of the BQDEI consumption.
However, according to Cohen’s d and Kendall’s W values, the effect size is small when comparing the means and medians of baseline and final ferritin concentrations, respectively. Likewise, no significant difference was observed in ferritin concentration between the intermediate and final stages, as determined by the Wilcoxon test (Supplementary Table S5).
At the beginning, 8 children (19%) were identified with basal ferritin below the normal limit of 20 ng/ml and at the end of the nutritional program only one child (2.4%) was identified below this limit (Supplementary Table S6), which is related to a significant improvement in the average ferritin concentration in the final stage.
Table 7 shows a slight increase of approximately 0.3 g/dl in the Hb concentration of children between the baseline and final stages of the nutritional program; however, this change was not statistically significant (p > 0.05). No significant difference was observed in mean Hb concentration when comparing across the three time points (Supplementary Table S7).

Table 7. Hemoglobin concentration in children under 6 years of age in the basal, intermediate and final stages of the BQDEI consumption within the nutritional program.
At the start of the program, there were 11 children with mild anemia (26.2%) and 3 with moderate anemia (7.1%). Of these, at the final stage of the program, 1 had mild anemia (2.4%) and 1 had moderate anemia (2.4%), respectively. Likewise, an increase in children without anemia was observed from 66.7 to 85.7% between the baseline and final stages (Supplementary Table S8). This qualitatively demonstrates that there was a significant recovery from anemia despite a non-significant increase in Hb concentration in the entire participating group.
4 Discussion
As shown in Table 2, factors traditionally associated with anemia, such as low household income, limited access to basic services (potable water and sewage systems) and predominantly secondary-level parental education, are less prevalent in this sample as most participants reside in urban areas. Nevertheless, the literature indicates that these determinants are more prevalent and have a greater impact in regions with disadvantaged socioeconomic conditions. For example, Rahayuwati et al. (67) in their research mentioned that the socioeconomic characteristics of families in West Java, Indonesia, have a significant influence on the eating habits of children under 5 years of age, in which stunting and the presence of anemia are related to the mother’s unemployment and not to the family economy as a whole. Similarly, Al Kaabi et al. (68) in children under 4 years of age in the Iraqi city of Kut, living in rural locations, have lower Hb levels, which was exacerbated when the mother had only elementary education and low socioeconomic status. Sunuwar et al. (69), reported that in children under 59 months of age from 6 Asian countries, 57.3% were anemic because the mother also had the same disease, which led to a growth deficit. A common characteristic of the mothers was that they came from poor homes with a lack of basic services for proper nutrition.
Table 3 shows that the anthropometric parameters height-for-age and weight-for-height improved significantly (p < 0.001) following the consumption of BQDEI as part of the nutritional program. These results are consistent with other studies (70–73) that have evaluated the impact of iron-fortified food consumption on child growth and improvement of anthropometric parameters. However, a study by Kowalski et al. (74), found that consuming drinks fortified with multiple micronutrients significantly improved Hb levels and reduced the prevalence of anemia in children, although it had no significant effect on their growth. Anthropometric growth outcomes are influenced by socioeconomic conditions and baseline nutritional status. Evidence suggests that micronutrient fortification alone may be insufficient to improve these indicators unless implemented within a comprehensive framework that includes dietary counseling (72, 75). This study integrated the consumption of BQDEI into a nutritional intervention aimed at promoting adherence to the fortified beverage and adoption of healthy eating habits among children. This intervention was primarily supported by their immediate environment, particularly maternal involvement. The programme incorporated structured activities that positively impacted anthropometric outcomes, highlighting the importance of environmental engagement in medium- and long-term nutritional strategies (30).
The findings reinforce the importance of iron fortification in nutrition programmes targeting vulnerable populations, particularly those affected by nutritional deficiencies or endemic malaria (76, 77). In such contexts, BQDEI may be an effective way to improve nutritional status in cases of malnutrition. The observed increase in height-for-age suggests a beneficial effect on linear growth, with potential long-term implications for child health and development. However, the effectiveness of food fortification is influenced by sociocultural factors that impact dietary practices and health conditions within target populations.
Furthermore, improvements in height-for-age and weight-for-height indicators among children consuming BQDEI may be partially attributed to elevated levels of insulin-like growth factor 1 (IGF-1), a peptide regulated by hormonal and nutritional inputs. Previous studies have shown that protein-rich diets, such as those incorporating quinoa, can enhance IGF-1 concentrations (78). Given its role in promoting bone growth and weight gain, IGF-1 serves as a complementary biochemical marker to anthropometric assessments (79), although it was not directly measured in the present study.
Table 4 shows that the children evaluated have adequate dietary patterns in terms of the frequency of consumption of protein foods rich in iron, such as meats and legumes, as well as vegetables, and that these dietary patterns did not undergo significant changes after the implementation of the nutritional program. There is evidence that the consumption of foods rich in heme iron such as red meat, poultry, viscera and fish, in addition to the consumption of fruits and vegetables rich in folic acid and vitamin C are associated with less anemia in children (80). However, in the present study, the adequate patterns in the participants did not vary at baseline and at the end of the program; so the increases in Hb and ferritin in children are mainly due to the most immediate dietary sources of iron with formulations that allow for better bioavailability (76), which can be achieved with fortified foods, such as the drink used in the PFP.
Data from Table 5 indicate that the prevalence of parasites was higher in children prior to the initiation of the nutritional program. At this stage, cysts of Entamoeba coli, Blastocystis hominis, and Giardia lamblia were identified. Additionally, Enterobius vermicularis eggs were detected in all three evaluations, with a particularly elevated frequency observed during the second follow-up. These parasites are generally found on fruits and vegetables due to contamination with cysts (81). The parasite frequencies observed in this study are lower compared to those reported in Argentina, where 54% of the studied child population presented enteroparasites, with the most frequent being Blastocystis spp., Giardia intestinalis, and Ascaris lumbricoides (82). In the present investigation, Ascaris lumbricoides was not detected, but Enterobius vermicularis was identified. Furthermore, the findings differ from another study conducted in Argentina, where E. coli was more frequently found in fecal samples than other Entamoeba species, such as E. histolytica and E. dispar (83).
On the other hand, it has been reported that, worldwide, approximately 400 million people are affected by Enterobius, especially children in developing countries. Blastocystis sp. affects one billion people and Giardia lamblia affects 200 million. The prevalence of these parasites is higher in temperate climate regions and has much to do with personal hygiene, type of housing, lack of drinking water and sewage service, bed sharing, overcrowding in the home, living in a non-urban area, and poor access to health education and diagnosis and treatment of these parasites (84–86). In this study, although the frequency of parasitosis is low, it may be related to the 11.9% lack of drinking water and 14.3% lack of sewage in the children’s homes.
Although E. coli is considered as a non-pathogenic protozoan, which does not present symptoms in infected persons, it must be taken into account that infection by E. coli and Giardia lamblia can cause malabsorption and promote a proinflammatory response and therefore has long-term consequences for human health. On the other hand, E. coli infection can alter the homeostasis of the microbiota causing changes in appetite and metabolism (87), whereas Enterobius vermicularis can cause the formation of granulomas in the kidney, in the peritoneal cavity in the female genital tract, the male urinary tract and in the appendix (88, 89). For this reason, although the parasitosis was found in low percentage during the development of the program, it was treated with broad-spectrum antiparasitics to reduce its influence on the results.
Table 6 shows the increase in ferritin concentration observed in participants who consumed the drink proposed in this study. Although a direct comparison with other interventions is not included, it is relevant to contextualize these findings within the existing literature. For example, Kowalski et al. (74) reported an increase of approximately 26 ng/ml in children in a rural area of Guatemala after administration of a drink fortified with multiple micronutrients (MMN), compared to an increase of approximately 20 ng/ml in the placebo group. In this study, the increase was approximately half that reported in Guatemala. This difference could be related to the fact that most of the participants belong to urban areas, despite the fact that both studies applied a similar treatment time and worked with child populations of comparable age.
The positive variation of ferritin up to either the intermediate or final stage with BQDEI is higher than that determined in a meta-analysis by Aaron et al. (87), who found that in school-aged children from lower-middle income countries, ferritin levels improve with an increase of 6.86 ng/ml when given non-dairy drinks fortified with MMN for a period of 8 weeks to 6 months.
In a setting closer to our reality in Viçosa, a city in the state of Minas Gerais in Brazil, they also developed a study with fortified milk powder drink (89) that included vitamin A, iron in the form of ferrous fumarate, zinc and copper in the form of sulfate and prebiotics, administered to preschool children, but in that study the increase in ferritin was approximately twice as high as that found in the present work. This is mainly due to the addition of the added nutrients that add to the effect established by the iron provided in the product. With regard to BQDEI, it could only have an effect on the increase in ferritin, iron in the form of FPP, organic acids, and vitamin C (the latter two promote iron absorption); however, its use may exceed its effect on ferritin concentration compared to fortified milk drinks, because milk as a vehicle has some inhibitory effects on iron absorption due to casein and whey proteins (90).
In subjects with sufficient iron, there is a decrease in the expression of divalent metal transporter-1 (DMT-1), so it is considered a limiting factor, important in the absorption of this metal as it reduces the differences in absorption in the face of variable solubility of iron compounds. Although duodenal cytochrome b expression is not down-regulated, it allows the available ferric iron to be converted to the ferrous form for absorption. In iron deficiency, there is an increased expression of DMT1 on the apical surface of the microvilli of the intestine and in this condition, solubility is the main limiting factor in iron absorption. At the same time, duodenal cytochrome b is not up-regulated in its expression. Therefore, it favors even more the absorption of ferrous iron over ferric iron (91). It appears that in children receiving BQDEI, an increased activity of duodenal cytochrome b was mainly established to favor the absorption of iron from FPP.
A low serum ferritin concentration suggests deficient iron stores, whereas elevated levels are indicative of iron overload, but also an infectious or inflammatory process. However, low iron stores are considered the first stage of a process that can lead to iron deficiency anemia (92). Clearly, in the present study, the increase in ferritin concentration by 13.5 ng/ml demonstrates storage of absorbed iron overload, enough to prevent anemia in children and maintain normal Hb concentration.
The slight increase in Hb after consumption of BQDEI is similar to the study by Kowalsky et al. (74), where the drink “Chispuditos” showed no significant differences in Hb between groups. In contrast, Vuvor et al. (93) reported significant increases with cereals fortified with ferrous fumarate (1.97 g/dl in the intervention group). Csölle et al. (76), also showed substantial improvements in Hb (3.44 g/L) and a lower prevalence of anemia with fortified foods. Finally, Castro et al. (89), achieved a 0.42 g/dl increase in Hb with a fortified powdered prebiotic, showing results comparable to BQDEI, supported by a robust methodological design.
The results may differ due to the fortifier used in the aforementioned studies, such as inorganic and organic ferrous salts with higher iron bioavailability for the body (33, 94). On the other hand, iron pyrophosphate is an interesting alternative for cases where tolerance and stability are priorities, although it may be less efficient compared to more bioavailable forms such as ferrous sulfate (95) or ferrous ascorbate (96). However, studies have been conducted with different forms of FPP to improve its bioavailability and compare it with ferrous sulfate, with similar results in both ferritin and Hb with the use of the micronized form (34) and liposomal form (97).
In the present study, a form of FPP stabilized with amino acids was used as a fortifying agent in blueberry and quinoa drinks. Although no significant increase in average Hb was observed after the intervention, analysis of frequencies and proportions using the McNemar test showed a significant reduction in the prevalence of anemia (Supplementary Table S6). Similar results were reported by Radhika et al. (98), who used micronized ferric pyrophosphate (MFPP) in extruded rice grains incorporated into a rice-based meal, obtaining positive effects in children aged 5 to 11 years in a control group design.
However, the complementary finding observed in the present study should be interpreted with caution, as the pre-experimental design without a control group limits the ability to attribute the changes exclusively to the intervention. In addition, external variables could not be fully controlled, such as factors inherent to the product, including the presence of phenolic compounds that affect iron absorption, the specific bioavailability of FPP as a fortifier, and possible food or drug interactions with the iron in the product that are difficult to evaluate in the field (94) which is why a weak effect of BQDEI on ferritin and Hb concentration was obtained.
There is evidence that the consumption of fortified complementary foods significantly reduced the likelihood of children developing anemia (99, 100), provided that nutritional education, dietary monitoring, and parasitic control are implemented within a nutritional program, as demonstrated in the present study.
One of the limitations of the study was the absence of a control group, because it was decided to give the same treatment to the participants who accepted the study. Likewise, it was not planned to elaborate a control product, with similar characteristics to that of the BQDEI, due to the production schedules of the plant of the agro-industrial company where the work was coordinated as a whole.
Although complementary actions were carried out, such as monitoring nutrition, controlling parasitic infections, and providing guidance on the adequate consumption of iron-enriched cranberry and quinoa drinks, these measures do not replace the methodological rigor provided by a control group. Therefore, the results should be interpreted with caution, due to other uncontrolled factors that may have influenced the observed effects and which have been discussed above. However, as blueberries have a low iron content in the formulation, approximately 0.28 mg/100 g of edible portion of the fruit (37), it is considered that the positive effect observed in ferritin concentration and, to a lesser extent, in Hb, is due to the fortification provided in the drink with ferric pyrophosphate, in addition to the fact that their diet remained constant during the nutritional program.
Another important limitation is the non-adherence at the beginning of the intermediate stage of the study, which represented 22%. However, this aspect was improved with recommendations by the nutritionists for strategies regarding the ways of how to consume the BQDEI and the times of such consumption, to ensure the completion of the children’s participation in the research.
Preliminary results support the potential of BQDEI as a functional food in complementary feeding strategies, and longitudinal studies are recommended to establish a causal relationship between consumption of the drink, combined with monitoring of protein food consumption and IGF-1 modulation in contexts of prevention of anemia and child malnutrition.
For ethical reasons, all children were considered regardless of their Hb level, which was a slight disadvantage since most of the children had normal Hb levels (see Supplementary Table S8). For that reason, a slight increase in this parameter was evident and therefore not significant after the BQDEI. Nevertheless, the results indicate that, if developed in other settings where malnutrition and iron deficiency exist, the BQDEI would have a great impact not only in the prevention of anemia by its positive influence on ferritin concentration, but also in the increase of Hb. Likewise, the BQDEI could be used before and during pregnancy to promote iron storage in the fetus, which would be preventive even in preterm infants who are more likely to develop iron deficiency anemia (101).
As a strength, we consider the work of two groups linked in the research, one by the technological development of the product by the Company with the sanitary guarantees and also of the standardized chemical composition, and another by the University researchers in the orientation of the feeding and monitoring of the consumption of the product, in which the only interest is to contribute to the solution of a relevant social problem such as anemia in children, without economic benefits and contributing to the solution of the Sustainable Development Goal (SDG) 3 that refers to health and well-being (102). The results of the research were obtained by an external and certified laboratory, so it is assumed that there was no manipulation of any kind by the researchers.
It would be advisable to add other nutrients to the BQDEI to verify a significant increase in Hb concentration in relation to that obtained in the present investigation. Likewise, its combination with iron in the ferrous form should also be considered in drinks with FPP, to increase the absorption of iron in children from areas more vulnerable to anemia, due to the fact that there is a greater expression of the DMT-1 in those children (91).
5 Conclusion
It was demonstrated that the nutritional program based on the consumption of the BQDEI added to the educational sessions and nutritional follow-up can prevent anemia in children, slightly improve nutritional status and increase the concentration of Hb and ferritin, being more significant in ferritin. This program can be applied in children in regions where anemia is more prevalent.
After validating BQDEI as a preventive strategy for anemia within the framework of a nutrition program, the formation of strategic alliances is proposed to scale this initiative to the national level. The objective is to expand its reach to more families and communities in Peru, thus promoting a replicable model with the potential for a direct impact on the sustained reduction of anemia. This proposal seeks to contribute to strengthening the country’s productivity, human development, and competitiveness through an innovative, evidence-based nutritional intervention.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
Ethics statement
The studies involving humans were approved by PI-CEI-NUTRICION-2023-001/Universidad César Vallejo. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
CN-C: Conceptualization, Methodology, Validation, Writing – original draft, Funding acquisition, Project administration, Resources, Supervision. SP-D: Conceptualization, Funding acquisition, Methodology, Project administration, Supervision, Validation, Writing – original draft, Visualization, Writing – review & editing. NS-D: Conceptualization, Funding acquisition, Project administration, Supervision, Writing – original draft, Resources. JB-C: Conceptualization, Methodology, Validation, Visualization, Writing – original draft, Funding acquisition, Resources, Supervision. NO: Conceptualization, Methodology, Validation, Writing – original draft, Data curation, Formal analysis, Visualization, Writing – review & editing. JD-O: Conceptualization, Data curation, Formal analysis, Methodology, Validation, Visualization, Writing – original draft, Writing – review & editing. LC-C: Conceptualization, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Writing – original draft. JV-C: Conceptualization, Project administration, Supervision, Writing – original draft, Data curation, Formal analysis, Methodology, Validation. VR: Conceptualization, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Writing – original draft. CA-Q: Conceptualization, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Writing – original draft. MZ-R: Conceptualization, Investigation, Methodology, Project administration, Resources, Validation, Writing – original draft. KN-T: Conceptualization, Investigation, Methodology, Supervision, Validation, Writing – original draft, Resources. GE-D: Conceptualization, Methodology, Supervision, Validation, Writing – original draft, Investigation, Project administration.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This research was funded by César Vallejo University and the Health Management Department of the agroindustrial company, both of which are based in Trujillo, Peru. The collaborative work was authorised under official letter number 078-2025-VI-UCV.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2025.1639894/full#supplementary-material
References
1. Montalvo, YJ, Romaní, KJ, Trujillo, BS, Revilla, SC, and Balta, GL. Sociodemographic and prenatal factors associated with anemia in Peruvian pregnant women. Enferm Glob. (2019) 18:273–81. doi: 10.6018/eglobal.18.4.358801
2. Ranque, B, Kitenge, R, Ndiaye, DD, Ba, MD, Adjoumani, L, Traore, H, et al. Estimating the risk of child mortality attributable to sickle cell anaemia in sub-Saharan Africa: a retrospective, multicentre, case-control study. Lancet Haematol. (2022) 9:e208-16. doi: 10.1016/S2352-3026(22)00004-7
3. Muchie, KF, Lakew, AM, Teshome, DF, Yenit, MK, Sisay, MM, Mekonnen, FA, et al. Epidemiology of preterm birth in Ethiopia: systematic review and meta-analysis. BMC Pregnancy Childbirth. (2020) 20:574. doi: 10.1186/s12884-020-03271-6
4. World Health Organization. (2023). Anemia. Available online at: https://www.who.int/es/news-room/fact-sheets/detail/anaemia [Accessed 15 March 2023]
5. National Institute of Statistics and Informatics. (2023). 43.1% of the population aged 6 to 35 months suffered from anemia in 2023. Available online at: https://m.inei.gob.pe/prensa/noticias/el-431-de-la-poblacion-de-6-a-35-meses-de-edad-sufrio-de-anemia-en-el-ano-2023-15077/ [Accessed 15 March 2023]
6. National Institute of Health. (2024). Anaemia in Peruvian children under 5 years of age SIEN724 HIS 2023. Available online at: https://www.gob.pe/institucion/ins/informes-publicaciones/5517486-sala-situacional-anemia-en-ninos-peruanos-menores-de-5-anos-sien-his-2023 [Accessed April 20, 2024]
7. Medical College of Peru. (2023). Report of the seminar on childhood Anaemia in Peru: Situation and challenges, a new perspective. Lima: Arte Perú SAC. p. 16. Available online at: https://www.cmp.org.pe/wp-content/uploads/2023/11/INFORME-DEL-SEMINARIO-LA-ANEMIA-INFANTIL-EN-EL-PERU.pdf [Accessed 15 March 2023]
8. Kumar, SB, Arnipalli, SR, Mehta, P, Carrau, S, and Ziouzenkova, O. Iron deficiency anemia: efficacy and limitations of nutritional and comprehensive mitigation strategies. Nutrients. (2022) 14:2976. doi: 10.3390/nu14142976
9. Mitchinson, C, Strobel, N, McAullay, D, McAuley, K, Bailie, R, and Edmond, KM. Anemia in disadvantaged children aged under five years; quality of care in primary practice. BMC Pediatr. (2019) 19:178. doi: 10.1186/s12887-019-1543-2
10. Li, S, Bo, Y, Ren, H, Zhou, C, Lao, X, Zhao, L, et al. Regional differences in the prevalence of anaemia and associated risk factors among infants aged 0–23 months in China: China nutrition and health surveillance. Nutrients. (2021) 13:1293. doi: 10.3390/nu13041293
11. Al-kassab-Córdova, A, Méndez-Guerra, C, and Robles-Valcarcel, P. Sociodemographic and nutritional factors associated with anemia in children aged 1 to 5 years old in Peru. Rev Chil Nutr. (2020) 47:925–32. doi: 10.4067/S0717-75182020000600925
12. Moschovis, PP, Wiens, MO, Arlington, L, Antsygina, O, Hayden, D, Dzik, W, et al. Individual, maternal and household risk factors for anaemia among young children in sub-Saharan Africa: a cross-sectional study. BMJ Open. (2018) 8:e019654. doi: 10.1136/bmjopen-2017-019654
13. Nambiema, A, Robert, A, and Yaya, I. Prevalence and risk factors of anemia in children aged from 6 to 59 months in Togo: analysis from Togo demographic and health survey data, 2013–2014. BMC Public Health. (2019) 19:215. doi: 10.1186/s12889-019-6547-1
14. Dutta, M, Bhise, M, Prashad, L, Chaurasia, H, and Debnath, P. Prevalence and risk factors of anemia among children 6–59 months in India: a multilevel analysis. Clin Epidemiol Glob Health. (2020) 8:868–78. doi: 10.1016/j.cegh.2020.02.015
15. Gedfie, S, Getawa, S, and Melku, M. Prevalence and associated factors of iron deficiency and iron deficiency anemia among under-5 children: a systematic review and meta-analysis. Glob Pediatr Health. (2022) 9:2333794X2211108. doi: 10.1177/2333794X221110860
16. Ortiz Romaní, KJ, Ortiz Montalvo, YJ, Escobedo Encarnación, JR, Neyra de la Rosa, L, and Jaimes Velásquez, CA. Analysis of the multicausal model of anemia level in children 6-35 months old in Peru. Enferm Glob. (2021) 20:426–55. doi: 10.6018/eglobal.472871
17. Shimanda, PP, Amukugo, HJ, and Norström, F. Socioeconomic factors associated with anemia among children aged 6-59 months in Namibia. J Public Health Afr. (2020) 11:1131. doi: 10.4081/jphia.2020.1131
18. Tesema, GA, Worku, MG, Tessema, ZT, Teshale, AB, Alem, AZ, Yeshaw, Y, et al. Prevalence and determinants of severity levels of anemia among children aged 6–59 months in sub-Saharan Africa: a multilevel ordinal logistic regression analysis. PLoS One. (2021) 16:e0249978. doi: 10.1371/journal.pone.0249978
19. Da Silva, FH, De Assunção, BM, Lopes, DA, and Egito, DM. Prevalence of and factors associated with anemia in school children from Maceió, northeastern Brazil. BMC Public Health. (2016) 16:1–12. doi: 10.1186/s12889-016-3073-2
20. Gosdin, L, Martorell, R, Bartolini, RM, Mehta, R, Srikantiah, S, and Young, MF. The co-occurrence of anaemia and stunting in young children. Matern Child Nutr. (2018) 14:e12597. doi: 10.1111/mcn.12597
21. Cabada, MM, Goodrich, MR, Graham, B, Villanueva-Meyer, PG, Deichsel, EL, Lopez, M, et al. Prevalence of intestinal helminths, anemia, and malnutrition in Paucartambo, Peru. Rev Panam Salud Publica. (2015) 37:69–75.
22. Engle-Stone, R, Aaron, GJ, Huang, J, Wirth, JP, Namaste, SML, Williams, AM, et al. Predictors of anemia in preschool children: biomarkers reflecting inflammation and nutritional determinants of anemia (BRINDA) project. Am J Clin Nutr. (2017) 106:402S–15S. doi: 10.3945/ajcn.116.142323
23. Montag, D, Delgado, CA, Quispe, C, Wareham, D, Gallo, V, Sanchez-Choy, J, et al. Launching of the Anaemia research Peruvian cohort (ARPEC): a multicentre birth cohort project to explore the iron adaptive homeostasis, infant growth and development in three Peruvian regions. BMJ Open. (2021) 11:e045609. doi: 10.1136/bmjopen-2020-045609
24. Ercumen, A, Benjamin-Chung, J, Arnold, BF, Lin, A, Hubbard, AE, Stewart, C, et al. Effects of water, sanitation, handwashing and nutritional interventions on soil-transmitted helminth infections in young children: a cluster-randomized controlled trial in rural Bangladesh. PLoS Negl Trop Dis. (2019) 13:e0007323. doi: 10.1371/journal.pntd.0007323
25. De Medeiros, PHQS, Pinto, DV, De Almeida, JZ, Rêgo, JMC, Rodrigues, FAP, Lima, AÂM, et al. Modulation of intestinal immune and barrier functions by vitamin a: implications for current understanding of malnutrition and enteric infections in children. Nutrients. (2018) 10:1128. doi: 10.3390/nu10091128
26. Guizado, GLG. Anemia infantil y anemia en gestantes en el Perú. Rev Int Salud Materno Fetal. (2018) 3:20–1.
27. Lopez de Romaña, D, Mildon, A, Golan, J, Jefferds, MED, Rogers, LM, and Arabi, M. Review of intervention products for use in the prevention and control of anemia. Ann N Y Acad Sci. (2023) 1529:42–60. doi: 10.1111/nyas.15071
28. Cusquisibán-Alcantara, Y, Toledo-Garrido, C, Calizaya-Milla, YE, Carranza-Cubas, SP, and Saintila, J. Impact of a nutrition education intervention on knowledge, healthy eating index, and biochemical profile in a rural community in Peru. J Multidiscip Healthc. (2024) 17:1111–25. doi: 10.2147/JMDH.S453279
29. Irandegani, F, Arbabisarjou, A, Ghaljaei, F, Navidian, A, and Karaji bani, M. The effect of a date consumption-based nutritional program on iron deficiency anemia in primary school girls aged 8 to 10 years old in Zahedan (Iran). Pediatr Health Med Ther. (2019) 10:183–8. doi: 10.2147/phmt.s225816
30. Soncco-Sucapuca, M, Brousett-Minaya, MA, and Pumacahua-Ramos, A. Impact of an educational program including a fortified bread to reduce levels of anemia in school children of Yocará, Puno-Perú. Rev Investig Altoandin. (2018) 20:73–84. doi: 10.18271/ria.2018.331
31. Reyes, NS, Contreras, CA, and Oyola, CM. Anemia y desnutrición infantil en zonas rurales: impacto de una intervención integral a nivel comunitario. Rev Investig Altoandinas. (2019) 21:205–14. doi: 10.18271/ria.2019.478
32. Ntenda, PAM. Association of low birth weight with undernutrition in preschool-aged children in Malawi. Nutr J. (2019) 18:51. doi: 10.1186/s12937-019-0477-8
33. Wan, D, Wu, Q, Ni, H, Liu, G, Ruan, Z, and Yin, Y. Treatments for iron deficiency (ID): prospective organic iron fortification. Curr Pharm Des. (2019) 25:325–32. doi: 10.2174/1381612825666190319111437
34. El-Gendy, FM, El-Gendy, AA, and El-Hawy, MA. A comparative study between the dispersible ferric pyrophosphate particles and ferrous sulfate in treatment of pediatric patients with iron deficiency anemia. Iran J Pediatr Hematol Oncol. (2021) 11:78–90. doi: 10.18502/ijpho.v11i2.5840
35. Shubham, K, Anukiruthika, T, Dutta, S, Kashyap, AV, Moses, JA, and Anandharamakrishnan, C. Iron deficiency anemia: a comprehensive review on iron absorption, bioavailability and emerging food fortification approaches. Trends Food Sci Technol. (2020) 99:58–75. doi: 10.1016/j.tifs.2020.02.021
36. Sermini, CG, Acevedo, MJ, and Arredondo, M. Biomarcadores del metabolismo y nutrición de hierro. Rev Peru Med Exp Salud Publica. (2017) 34:690–8. doi: 10.17843/rpmesp.2017.344.3182
37. Sun, R, Sun, L, and Wang, K. Partial least squares analysis of the relationship between chemical composition and phenolic compounds in blueberry cultivars. Food Anal Methods. (2017) 10:1024–33. doi: 10.1007/s12161-016-0671-7
38. Krishna, P, Pandey, G, Thomas, R, and Parks, S. Improving blueberry fruit nutritional quality through physiological and genetic interventions: a review of current research and future directions. Antioxidants. (2023) 12:713. doi: 10.3390/antiox12040713
39. Karlsons, A, Osvalde, A, Čekstere, G, and Ponnale, J. Research on the mineral composition of cultivated and wild blueberries and cranberries. Agron Res. (2018) 16:454–63. doi: 10.15159/AR.18.039
40. Cho, WJ, Song, BS, Lee, JY, Kim, JK, Kim, JH, Yoon, YH, et al. Composition analysis of various blueberries produced in Korea and manufacture of blueberry jam by response surface methodology. J Korean Soc Food Sci Nutr. (2010) 39:319–23. doi: 10.3746/jkfn.2010.39.2.319
41. Manzanilla-Valdez, ML, Boesch, C, Orfila, C, Montaño, S, and Hernández-Álvarez, AJ. Unveiling the nutritional spectrum: a comprehensive analysis of protein quality and antinutritional factors in three varieties of quinoa (Chenopodium quinoa wild). Food Chem X. (2024) 24:100812. doi: 10.1016/j.fochx.2024.100812
42. García-García, JA, Reding-Bernal, A, and López-Alvarenga, JC. Cálculo del tamaño de la muestra en investigación en educación médica. Investig En Educ Medica. (2013) 2:217–24. doi: 10.1016/S2007-5057(13)72605-7
43. Lakens, D. Calculating and reporting effect sizes to facilitate cumulative science: a practical primer for t-tests and ANOVAs. Front Psychol. (2013) 4:863. doi: 10.3389/fpsyg.2013.00863
44. Pattrakornkul, N, Ngamcherdtrakul, P, Kriangburapa, W, Tangjaturonrasme, S, and Yampratoom, R. Daily and weekly iron supplementations to improve iron status in infants: a randomized controlled trial. J Med Assoc Thail. (2021) 104:1511–8. doi: 10.35755/jmedassocthai.2021.09.12978
45. FAO. (2023). Codex Alimentarius. International foods standards. Available online at: https://www.fao.org/fao-who-codexalimentarius/codex-texts/list-standards/es/(2023) [Accessed March 15, 2023]
46. Ministerio de Salud. (1998). Decreto Supremo n° 007-98-SA. Available online at: https://www.gob.pe/institucion/minsa/normas-legales/256394-007-98-sa [Accessed December 26, 2024]
47. Advancing Standards Transforming Markets. ASTM E2299-13: Standard guide for sensory evaluation of products by children and minors. West Conshohocken (USA): ASTM International (2021).
48. Salgueiro, MJ, Arnoldi, S, Kaliski, MA, Torti, H, Messeri, E, Weill, R, et al. Stabilized–solubilized ferric pyrophosphate as a new iron source for food fortification. Bioavailability studies by means of the prophylactic–preventive method in rats. Biol Trace Elem Res. (2009) 127:143–7. doi: 10.1007/s12011-008-8229-1
49. Muñoz, JM. “El Plato del Bien Comer”, ¿evidencia científica o conocimiento transpuesto? CPU-e, Rev Investig Educativa. (2015) 20:45–71. doi: 10.25009/cpue.v0i20.1287
50. Rodríguez-Rey, R, and Cantero-García, M. Albert Bandura: Impacto en la educación de la teoría cognitiva social del aprendizaje. PYM. (2020) 384:72–6. doi: 10.14422/pym.i384.y2020.011
51. Northeast and Caribbean Addiction Technology Transfer Center. Transtheoretical model of change: a model for the treatment of substance use disorders. Bayamón: Institute for Research, Education and Services in Addiction, Universidad Central del Caribe (2021).
52. Pacovilca, O, Zea, C, and Nieva, L. Relation between socioeconomic characteristics and academic performance in undergraduate students of a public university. Sciéndo. (2018) 21:119–24. doi: 10.17268/sciendo.2018.012
53. Instituto Nacional de Estadística e Informática. (2020). Manual de la antropometrista. Available online at: https://proyectos.inei.gob.pe/iinei/srienaho/Descarga/DocumentosMetodologicos/2020-5/ManualAntropometrista.pdf [Accessed December 26, 2024]
54. Ministerio de Salud. (2024). Resolución Ministerial N° 034-2024-MINSA. Guía técnica para la valoración nutricional antropométrica de la niña y el niño de 0 a 11 años. Available online at: https://bvs.minsa.gob.pe/local/fi-admin/RM-034-2024-minsa.pdf [Accessed December 26, 2024]
55. Ministerio de Salud. (2017). Resolución Ministerial N° 537-2017-MINSA. Norma técnica de salud para el control del crecimiento y desarrollo de la niña y el niño menores de cinco años. Available online at: https://www.gob.pe/institucion/minsa/normas-legales/190581-537-2017-minsa [Accessed December 26, 2024]
56. Arimond, M, Torheim, LE, Wiesmann, D, Joseph, M, and Carriquiry, A. Dietary diversity as a measure of the micronutrient adequacy of women’s diets: Sults from rural Bangladesh site. Washington, DC: Food and Nutrition Technical Assistance II Project (FANTA-2) (2009).
57. Abrahamson, M, Hooker, E, Ajami, NJ, Petrosino, JF, and Orwoll, ES. Successful collection of stool samples for microbiome analyses from a large community-based population of elderly men. Contemp Clin Trials Commun. (2027) 7:158–62. doi: 10.1016/j.conctc.2017.07.002
58. Osman, KA, Zinsstag, J, Tschopp, R, Schelling, E, Hattendorf, J, Umer, A, et al. Nutritional status and intestinal parasites among young children from pastoralist communities of the Ethiopian Somali region. Matern Child Nutr. (2020) 16:e12955. doi: 10.1111/mcn.12955
59. Yanola, J, Nachaiwieng, W, Duangmano, S, Prasannarong, M, Somboon, P, and Pornprasert, S. Current prevalence of intestinal parasitic infections and their impact on hematological and nutritional status among Karen hill tribe children in Omkoi District, Chiang Mai Province, Thailand. Acta Trop. (2018) 180:1–6. doi: 10.1016/j.actatropica.2018.01.001
60. Ministerio de Salud del Perú. (2017). Resolución Ministerial N° 250-2017-MINSA. Norma Técnica- Manejo Terapéutico y Preventivo y Control de la Anemia por deficiencia de Hierro en el niño y la niña, adolescente, mujeres en edad fértil, gestantes y puerpera. Available online at: https://www.gob.pe/institucion/minsa/informes-publicaciones/280854-norma-tecnica-manejo-terapeutico-y-preventivo-de-la-anemia-en-ninos-adolescentes-mujeres-gestantes-y-puerperas [Accessed July 26, 2024]
61. Ministerio de Salud del Perú. (2024). Resolución Ministerial N° 213-2024-MINSA. Norma Técnica de Salud: Prevención y Control de la Anemia por deficiencia de Hierro en el niño y la niña, adolescente, mujeres en edad fértil, gestantes y puerpera. Available online at: https://www.gob.pe/institucion/minsa/normas-legales/5440166-251-2024-minsa [Accessed July 26, 2024]
62. Lukovac, T, Hil, OA, Popović, M, Jovanović, V, Savić, T, Pavlović, AM, et al. Serum biomarker analysis in pediatric ADHD: implications of homocysteine, vitamin B12, vitamin D, ferritin, and iron levels. Children. (2024) 11:497. doi: 10.3390/children11040497
63. Mei, Z, Addo, OY, Jefferds, MED, Sharma, AJ, Flores-Ayala, RC, Pfeiffer, CM, et al. Comparison of current World Health Organization guidelines with physiologically based serum ferritin thresholds for Iron deficiency in healthy Young children and nonpregnant women using data from the third National Health and nutrition examination survey. J Nutr. (2023) 153:771–80. doi: 10.1016/j.tjnut.2023.01.035
64. Hazra, A, and Gogtay, N. Biostatistics series module 3: comparing groups: numerical variables. Indian J Dermatol. (2016) 61:251–60. doi: 10.4103/0019-5154.182416
65. Rendón-Macías, ME, Zarco-Villavicencio, IS, and Villasís-Keever, MÁ. Statistical methods for effect size analysis. Rev Alerg Mex. (2021) 68:128–36. doi: 10.29262/ram.v658i2.949
66. World Medical Association. (2023). WMA declaration of Helsinki – Ethical principles for medical research involving human participants. Available online at: https://www.wma.net/es/policies-post/declaracion-de-helsinki-de-la-amm-principios-eticos-para-las-investigaciones-medicas-en-seres-humanos/ [Accessed November 30, 2023]
67. Rahayuwati, L, Komariah, M, Sari, CWM, Yani, DI, Hermayanti, Y, Setiawan, A, et al. The influence of mother’s employment, family income, and expenditure on stunting among children under five: a cross-sectional study in Indonesia. J Multidiscip Healthc. (2023) 16:2271–8. doi: 10.2147/JMDH.S417749
68. Al Kaabi, SZ, Al-Saad, DS, Al-Rubaye, AK, and Alkinani, AAA. The association between the severity of anemia and socio-demographic factors among children under five years of age in Kut City. J Public Health Afr. (2023) 14:6. doi: 10.4081/jphia.2023.2676
69. Sunuwar, DR, Singh, DR, Pradhan, PMS, Shrestha, V, Rai, P, Shah, SK, et al. Factors associated with anemia among children in south and Southeast Asia: a multilevel analysis. BMC Public Health. (2023) 23:343. doi: 10.1186/s12889-023-15265-y
70. Ash, DM, Tatala, SR, Frongillo, EA, Ndossi, GD, and Latham, MC. Randomized efficacy trial of a micronutrient-fortified beverage in primary school children in Tanzania. Am J Clin Nutr. (2003) 77:891–8. doi: 10.1093/ajcn/77.4.891
71. Beinner, MA, Lamounier, JA, and Tomaz, C. Effect of iron-fortified drinking water of daycare facilities on the hemoglobin status of young children. J Am Coll Nutr. (2005) 24:107–14. doi: 10.1080/07315724.2005.10719451
72. Ekoe, T, Bianpambe, OI, Nguefack, F, Pondi, DM, Kana-Sop, MM, Hays, NP, et al. Efficacy of an iron-fortified infant cereal to reduce the risk of iron deficiency anemia in young children in East Cameroon. Food Sci Nutr. (2020) 8:3566–77. doi: 10.1002/fsn3.1639
73. Paz-Olivas, Y, Ignacio-Cconchoy, F, Meza-Flores, P, Acosta-Claros de Postigo, A, and Benites-Zapata, V. A dairy mixture fortified with iron and zinc improves hemoglobin levels in children aged 2 to 10 years in an andean community in Peru: randomized, double-blind controlled trial. Rev Cuerpo Med HNAAA. (2021) 14:304–10. doi: 10.35434/rcmhnaaa.2021.143.1250
74. Kowalski, AJ, Mayen, VA, de Ponce, S, Lambden, KB, Tilton, N, Villanueva, LM, et al. The effects of multiple micronutrient fortified beverage and responsive caregiving interventions on early childhood development, hemoglobin, and ferritin among infants in rural Guatemala. Nutrients. (2023) 15:2062. doi: 10.3390/nu15092062
75. Gelli, A, Margolies, A, Santacroce, M, Roschnik, N, Twalibu, A, Katundu, M, et al. Using a community-based early childhood development center as a platform to promote production and consumption diversity increases children’s dietary intake and reduces stunting in Malawi: a cluster-randomized trial. J Nutr. (2018) 148:1587–97. doi: 10.1093/jn/nxy148
76. Csölle, I, Felső, R, Szabó, É, Metzendorf, MI, Schwingshackl, L, Ferenci, T, et al. Health outcomes associated with micronutrient-fortified complementary foods in infants and young children aged 6–23 months: a systematic review and meta-analysis. Lancet Child Adolesc Health. (2022) 6:533–44. doi: 10.1016/S2352-4642(22)00147-X
77. Tam, E, Keats, EC, Rind, F, Das, JK, and Bhutta, AZA. Micronutrient supplementation and fortification interventions on health and development outcomes among children under-five in low- and middle-income countries: a systematic review and meta-analysis. Nutrients. (2020) 12:289. doi: 10.3390/nu12020289
78. Ruales, J, de Grijalva, Y, Lopez-Jaramillo, P, and Nair, BM. The nutritional quality of an infant food from quinoa and its effect on the plasma level of insulin-like growth factor-1 (IGF-1) in undernourished children. Int J Food Sci Nutr. (2002) 53:143–54. doi: 10.1080/09637480220132870
79. Ekbote, VH, Khadilkar, VV, Khadilkar, AV, Mughal, Z, Chiplonkar, SA, Palande, SA, et al. Relationship of insulin-like growth factor 1 and bone parameters in 7–15 years old apparently healthy Indian children. Indian J Endocrinol Metab. (2015) 19:770–4. doi: 10.4103/2230-8210.167553
80. Visser, M, Van Zyl, T, Hanekom, SM, Baumgartner, J, van der Hoeven, M, Taljaard-Krugell, C, et al. Nutrient patterns and their relation to anemia and iron status in 5- to 12-y-old children in South Africa. Nutrition. (2019) 62:194–200. doi: 10.1016/j.nut.2019.01.016
81. Li, J, Wang, Z, Karim, MR, and Zhang, L. Detection of human intestinal protozoan parasites in vegetables and fruits: a review. Parasit Vectors. (2020) 13:380. doi: 10.1186/s13071-020-04255-3
82. Gutiérrez, CE, Jaras Horno, MA, Aro, C, Gómez Colussi, AF, Belén Cheirano, M, Soledad Rodríguez, É, et al. Educational intervention as a prevention strategy for intestinal parasitosis, and assessment of the enteroparasitological status in child development centers in the city of Santa Fe, Argentina. Rev Argent Microbiol. (2024) 57:8–13. doi: 10.1016/j.ram.2024.07.002
83. Servián, A, Zonta, LM, and Navone, GT. Differential diagnosis of human Entamoeba infections: morphological and molecular characterization of new isolates in Argentina. Rev Argent Microbiol. (2024) 56:16–24. doi: 10.1016/S0325754123000494
84. Cociancic, P, Torrusio, SE, Zonta, ML, and Navone, GT. Risk factors for intestinal parasitoses among children and youth of Buenos Aires, Argentina. One Health. (2020) 9:100116. doi: 10.1016/j.onehlt.2019.100116
85. Moussavi, E, Houssaini, M, Salari, N, Hemmati, M, Abdullahi, A, Khaleghi, AA, et al. Prevalence of Enterobius vermicularis among children in Iran: a comprehensive systematic review and meta-analysis. Parasite Epidemiol Control. (2023) 22:e00315. doi: 10.1016/j.parepi.2023.e00315
86. Rattaprasert, P, Nitatsukprasert, C, Thima, K, and Chavalitshewinkoon-Petmitr, P. Development of nested PCR for identification of Entamoeba coli in human fecal samples. Southeast Asian J Trop Med Public Health. (2022) 53:21–36.
87. Aaron, G, Dror, D, and Yang, Z. Multiple-micronutrient fortified non-dairy beverage interventions reduce the risk of anemia and iron deficiency in school-aged children in low-middle income countries: a systematic review and meta-analysis. Nutrients. (2015) 7:3847–68. doi: 10.3390/nu7053847
88. Pogorelić, Z, Babić, V, Bašković, M, Ercegović, V, and Mrklić, I. Management and incidence of Enterobius vermicularis infestation in appendectomy specimens: a cross-sectional study of 6359 appendectomies. J Clin Med. (2024) 13:3198. doi: 10.3390/jcm13113198
89. Castro, LC, Costa, NM, Sant’Anna, HM, Ferreira, CL, and Franceschini, SC. Improvement the nutritional status of pre-school children following intervention with a supplement containing iron, zinc, copper, vitamin a, vitamin C and prebiotic. Ciênc Saúde Colet. (2017) 22:359–68. doi: 10.1590/1413-81232017222.15902015
90. Kuriyan, R, Thankachan, P, Selvam, S, Pauline, M, Srinivasan, K, Kamath-Jha, S, et al. The effects of regular consumption of a multiple micronutrient fortified milk beverage on the micronutrient status of school children and on their mental and physical performance. Clin Nutr. (2016) 35:190–8. doi: 10.1016/j.clnu.2015.02.001
91. Zimmermann, MB, Biebinger, R, Egli, I, Zeder, C, and Hurrell, RF. Iron deficiency up-regulates iron absorption from ferrous sulphate but not ferric pyrophosphate and consequently food fortification with ferrous sulphate has relatively greater efficacy in iron-deficient individuals. Br J Nutr. (2011) 105:1245–50. doi: 10.1017/S0007114510004903
92. Pérez-Acosta, A, Duque, X, Trejo-Valdivia, B, Flores-Huerta, S, Flores-Hernández, S, Martínez-Andrade, G, et al. Cut-off points for serum ferritin to identify low iron stores during the first year of life in a cohort of Mexican infants. Matern Child Nutr. (2021) 17:e13205. doi: 10.1111/mcn.13205
93. Vuvor, F, Paul, S, Ansong, R, Baah, RO, Annor, DA, Harrison, OA, et al. Effect of an iron-fortified complementary food on anemia and nutritional status of infants aged 6–18 months in Ghana. Curr Dev Nutr. (2019) 3:nzz034. doi: 10.1093/cdn/nzz034.P10-103-19
94. Hurrell, R, and Egli, I. Iron bioavailability and dietary reference values. Am J Clin Nutr. (2010) 91:1461S–7S. doi: 10.3945/ajcn.2010.28674F
95. Hackl, L, Zimmermann, MB, Zeder, C, Parker, M, Johns, PW, Hurrell, RF, et al. Iron bioavailability from ferric pyrophosphate in extruded rice cofortified with zinc sulfate is greater than when cofortified with zinc oxide in a human stable isotope study. J Nutr. (2017) 147:377–83. doi: 10.3945/jn.116.241778
96. Divya Sri,, Keerthika, B, Priyanka, B, Harith, P, Gomasa, M, and Boddupally, S. Study on efficacy and compliance of oral supplements with ferric pyrophosphate and ferrous ascorbate in iron deficiency anaemia during pregnancy. J Pharm Sci. (2025) 3:1080–6. doi: 10.5281/zenodo.15354355
97. Sharma, A, Bellad, RM, and Charantimath, US. Effectiveness and safety of liposomal ferric pyrophosphate vs. ferrous sulfate for intermittent iron prophylaxis in children aged 6–59 months: a randomized controlled trial. Indian J Pediatr. (2025) 92:423. doi: 10.1007/s12098-025-05436-7
98. Radhika, MS, Nair, KM, Kumar, RH, Rao, MV, Ravinder, P, Reddy, CG, et al. Micronized ferric pyrophosphate supplied through extruded rice kernels improves body iron stores in children: a double-blind, randomized, placebo-controlled midday meal feeding trial in Indian schoolchildren. Am J Clin Nutr. (2011) 94:1202–10. doi: 10.3945/ajcn.110.007179
99. Diniz Largueza, CB, Mocellin, MC, Nunes, JC, and Ribas, SA. Effect of intake of iron-fortified milk on levels of ferritin and hemoglobin in preschoolers: a systematic review and meta-analysis. Clin Nutr ESPEN. (2023) 54:1–11. doi: 10.1016/j.clnesp.2023.01.001
100. Gahagan, S, Delker, E, Blanco, E, Burrows, R, and Lozoff, B. Randomized controlled trial of Iron-fortified versus low-Iron infant formula: developmental outcomes at 16 years. J Pediatr. (2019) 212:124–130.e1. doi: 10.1016/j.jpeds.2019.05.030
101. Ruan, S, Li, J, Xiong, F, Qie, D, Lu, Y, Yang, S, et al. The effect of iron supplementation in preterm infants at different gestational ages. BMC Pediatr. (2024) 24:530. doi: 10.1186/s12887-024-04996-5
102. United Nations. (2024). Sustainable Development Goals. Goal 3: Ensure healthy lives and promote well-being for all at all ages. Available online at: https://www.un.org/sustainabledevelopment/health/ [Accessed December 26, 2024]
Keywords: anemia, nutritional program, hemoglobin, ferritin, anthropometric indicators
Citation: Neglia-Cermeño C, Paredes-Díaz SE, Soto-Deza N, Bazán-Cabellos J, Otiniano NM, Díaz-Ortega JL, Castro-Caracholi LA, Valdiviezo-Campos JE, Ramos Torres V, Abanto-Quiroa C, Zariquiey-Rubio M, Nazario-Terrones K and Esteban-Dionicio G (2025) Prevention of anemia in children through the consumption of a blueberry and quinoa drink enriched with iron as part of a nutritional program. Front. Nutr. 12:1639894. doi: 10.3389/fnut.2025.1639894
Edited by:
Juan E. Andrade Laborde, University of Florida, United StatesReviewed by:
Flora Christine Amagloh, CSIR—Savanna Agricultural Research Institute, GhanaJiyan Aslan Ceylan, Mardin Artuklu University, Türkiye
Copyright © 2025 Neglia-Cermeño, Paredes-Díaz, Soto-Deza, Bazán-Cabellos, Otiniano, Díaz-Ortega, Castro-Caracholi, Valdiviezo-Campos, Ramos Torres, Abanto-Quiroa, Zariquiey-Rubio, Nazario-Terrones and Esteban-Dionicio. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jorge Luis Díaz-Ortega, amRpYXpvQHVjdi5lZHUuZWR1; Nélida Milly Otiniano, bm90aW5pYW5vQHVjdi5lZHUucGU=