 Pâmela Gracielle da Fonseca1
Pâmela Gracielle da Fonseca1 Lucas de Carvalho Siqueira2
Lucas de Carvalho Siqueira2 António Raposo3*
António Raposo3* Thamer Alslamah4
Thamer Alslamah4 Najla A. Albaridi5Ariana Saraiva6,7
Najla A. Albaridi5Ariana Saraiva6,7 Nathalia Sernizon Guimarães1*
Nathalia Sernizon Guimarães1*- 1Department of Nutrition, Nursing School, Universidade Federal de Minas Gerais, Belo Horizonte, Minas Gerais, Brazil
- 2Department of Primary Health Care, University Center of Patos (Centro Universitário de Patos), Patos, Paraíba, Brazil
- 3CBIOS (Research Center for Biosciences and Health Technologies), ECTS (School of Health Sciences and Technologies), Lusófona University, Lisboa, Portugal
- 4Department of Public Health, College of Applied Medical Sciences, Qassim University, Buraydah, Saudi Arabia
- 5Department of Health Science, College of Health and Rehabilitation, Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia
- 6Research in Veterinary Medicine (I-MVET), Faculty of Veterinary Medicine, Lisbon University Centre, Lusófona University, Lisboa, Portugal
- 7Veterinary and Animal Research Centre (CECAV), Faculty of Veterinary Medicine, Lisbon University Centre, Lusófona University, Lisboa, Portugal
Inadequate dietary patterns have significantly contributed to the rise of chronic diseases, highlighting the need for effective interventions. Culinary workshops have emerged as a promising strategy by offering practical and interactive food and nutrition education that may enhance food choice autonomy and promote healthier eating behaviors. This scoping review was conducted according to the Joanna Briggs Institute guidelines and the PRISMA-ScR checklist, with a protocol registered in the Open Science Framework. Searches were performed in PubMed, Embase, Cochrane Library, and the Virtual Health Library, including intervention studies published between 2005 and 2025. Study selection and data extraction were independently performed by three reviewers. A total of 30 studies were included, most from the United States (67.6%) and Australia (23.5%), with in-person workshops lasting 4–12 weeks. Improvements were reported in food autonomy, self-efficacy, and culinary practices in 81% of studies. Over 90% reported increased consumption of fruits, vegetables, and whole grains, along with reductions in ultra-processed foods. 15 studies noted improvements in anthropometric parameters, while 14 reported clinical benefits. Quality of life was evaluated in seven studies, with significant improvements in three. Culinary workshops appear to be effective in promoting health, though more standardized studies in diverse populations are warranted.
1 Introduction
The global dietary pattern demonstrates significant disparities, with substantial segments of the population consuming food quantities either below or exceeding established nutritional recommendations (1). Globally, the intake of whole grains, fruits, and vegetables remains consistently below recommended levels, notably in North America and Asia. In contrast, excessive consumption of red and processed meats is particularly prevalent in Oceania (2). Such dietary imbalances have direct implications for public health, substantially contributing to the escalating prevalence of non-communicable chronic diseases (NCDs), including obesity, type 2 diabetes, cardiovascular diseases, and cancer (3).
In response to this context, it is imperative to enhance educational strategies aimed at promoting healthier, sustainable, and culturally relevant dietary choices. Culinary workshops represent one such strategy, providing an experiential, participatory, and sensory-rich environment conducive to developing culinary skills, enhancing dietary autonomy, and appreciating food consumption as both a social and political act. Existing research indicates that participation in culinary workshops correlates with improved dietary quality, reduced consumption of ultraprocessed foods, and increased intake of fresh foods (4, 5). Additionally, culinary workshops can foster communal interaction and knowledge exchange, thereby strengthening social bonds and encouraging more mindful and emotionally engaged dietary practices (6, 7).
In recent years, the concept of adequate and healthy eating has expanded beyond nutritional considerations, encompassing social, cultural, environmental, and economic dimensions. This comprehensive approach aligns with principles advocated by the World Health Organization and the Brazilian Dietary Guidelines, emphasizing health promotion and sustainable development. The intersection of health promotion and sustainable development is increasingly recognized in academic research, highlighting the necessity for an integrated understanding of social determinants influencing dietary behaviors and decisions (8).
Furthermore, the escalating concern regarding socio-environmental impacts of current food systems underscores the importance of interventions that advocate the preparation and consumption of fresh and minimally processed foods, rather than ultraprocessed alternatives. Ultraprocessed foods, characterized by their nutritional inferiority, are linked to environmental degradation, biodiversity loss, and the erosion of traditional dietary practices (9, 10).
Despite documented experiences in existing literature, comprehensive systematic reviews addressing the impact of culinary workshops across multiple health outcomes remain limited. Therefore, this scoping review aims to systematically map the existing scientific literature concerning the influence of culinary workshops on dietary autonomy, habitual food consumption, anthropometric measures, clinical conditions, and biochemical parameters. In this review, the term dietary autonomy is understood in a broad sense, encompassing related constructs such as culinary self-efficacy, confidence in food preparation, and the ability to make informed and independent food choices. Although few studies directly assessed autonomy through validated tools, many reported improvements in participants' capacities to plan, prepare, and select foods, which we interpret as indicative of increased autonomy in practice. By consolidating and systematically evaluating these findings, this review seeks to reinforce culinary workshops as a strategic tool for promoting public health and dietary equity.
2 Materials and methods
We conducted a scoping review based on guidelines from the Joanna Briggs Institute (JBI). This review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRIS-MA-ScR) checklist. The scoping review protocol was previously registered and published in the Open Science Framework (OSF; https://osf.io/3zxn2/).
Given the heterogeneity of the interventions, populations, and outcomes across the included studies, and the exploratory nature of our research question, a scoping review was considered more appropriate than a systematic review or meta-analysis. Furthermore, the lack of standardized outcome measures limited the feasibility of conducting a meta-analysis, particularly for BMI-related data.
2.1 Identification of the research question
The PCC acronym (Population, Context, and Concept) was used to structure the research question. The population (P) included nutritional intervention programs and strategies; the context (C) was culinary workshops; and the concept (C) encompassed food services, public policy actions and strategies related to health and nutrition, community projects, or sustainable public initiatives.
2.2 Information search
To identify eligible studies on characteristics of nutritional intervention programs that focused on using fresh and minimally processed foods for culinary preparations, we searched primary scientific research from four electronic databases (PubMed, Embase, Cochrane Library, and the Virtual Health Library platform, reporting to Lilacs) on February 13, 2025. Local studies were identified through gray literature searches, including Connect Papers, and manual searches of reference lists of selected studies.
Search strategies were developed by an expert and refined through team discussions. Databases such as Medical Subject Headings (MeSH), Emtree, and Health Sciences Descriptors (DeCS) were consulted, and the approach was tailored to each database. The finalized PubMed search strategy and its adaptations for other databases are detailed in Appendix 1. Filters validated for intervention studies (McMaster) and publication years (2005–2025) were applied.
Following the search, studies were imported into Rayyan Qatar Computing Research Institute (Rayyan®) a collaborative tool for article screening, and blindly reviewed by two reviewers (PGdF and LdCS). Discrepancies were resolved by a third reviewer (NSG).
2.3 Eligibility criteria
Studies included were intervention studies (randomized and/or non-randomized clinical trials), quasi-experimental research, experimental trials, or mixed-methods research. Eligible studies evaluated culinary workshops aimed at enhancing dietary autonomy, dietary practices (participants' habitual food consumption), and health outcomes. Exclusion criteria comprised literature reviews, pilot studies, protocols, conference abstracts, editorials without initial results, studies involving children and adolescents, and culinary workshops not explicitly designed to promote the consumption of fresh and minimally processed foods.
2.4 Study selection and data extraction
To ensure consistency, two reviewers (PGdF and LdCS) participated in both the initial screening of titles and abstracts and the full-text evaluation. Disagreements were resolved by a third reviewer (NSG). Data extraction was conducted by three reviewers using an Excel spreadsheet, capturing variables detailed in Tables 1–3.
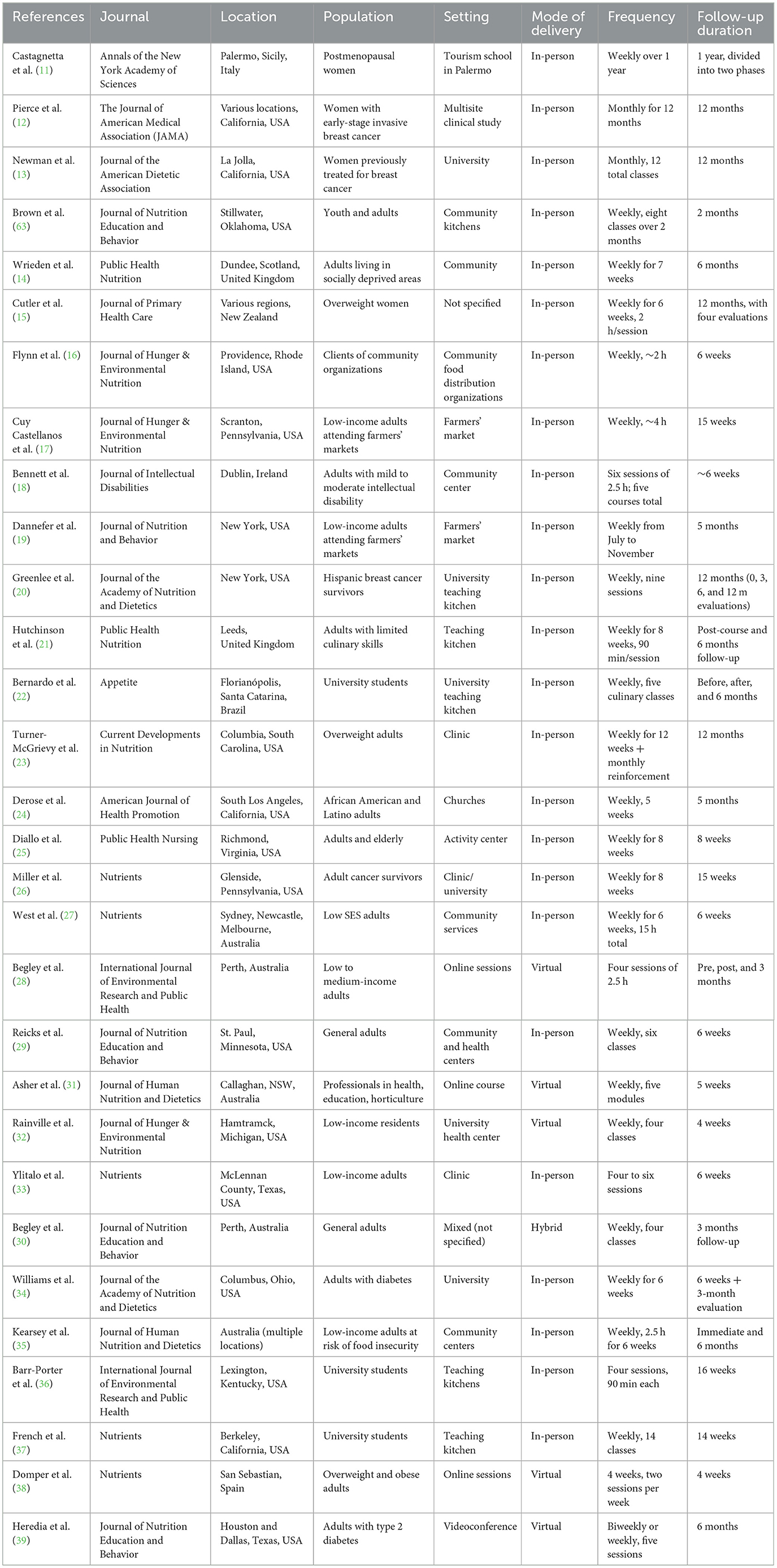
Table 1. Study information: journal, location, population, setting, mode of delivery, frequency, and follow-up duration.
2.5 Synthesis of results
A narrative synthesis was conducted, summarizing study characteristics and organizing results by year of publication. Data were systematically presented in Tables 1–3. Table 1 provides an overview of the general study information, including study references, publication period, country, workshop setting, presentation mode (in-person, virtual, or hybrid), target population, frequency of workshops, and follow-up duration. Table 2 focuses on the specifics of the culinary interventions, such as the fresh foods used, culinary preparations, food consumption patterns, and dietary autonomy, with measures like self-reports and Food Frequency Questionnaires (FFQ). Table 3 summarizes the health outcomes, including changes in anthropometric measures, quality of life, and clinical indicators, alongside the tools used for these assessments, such as self-reported questionnaires and the SF-36.
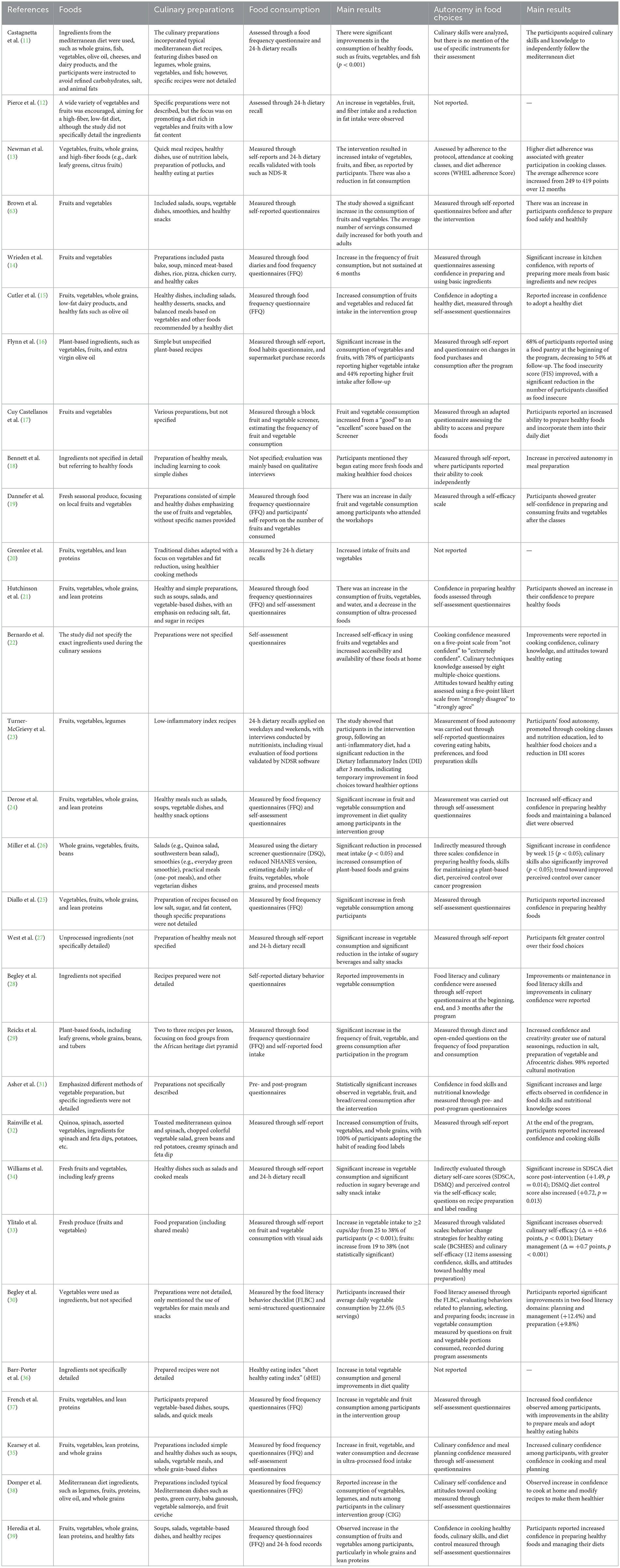
Table 2. Study information: foods, culinary preparations, food consumption, autonomy in food choices, and main results.
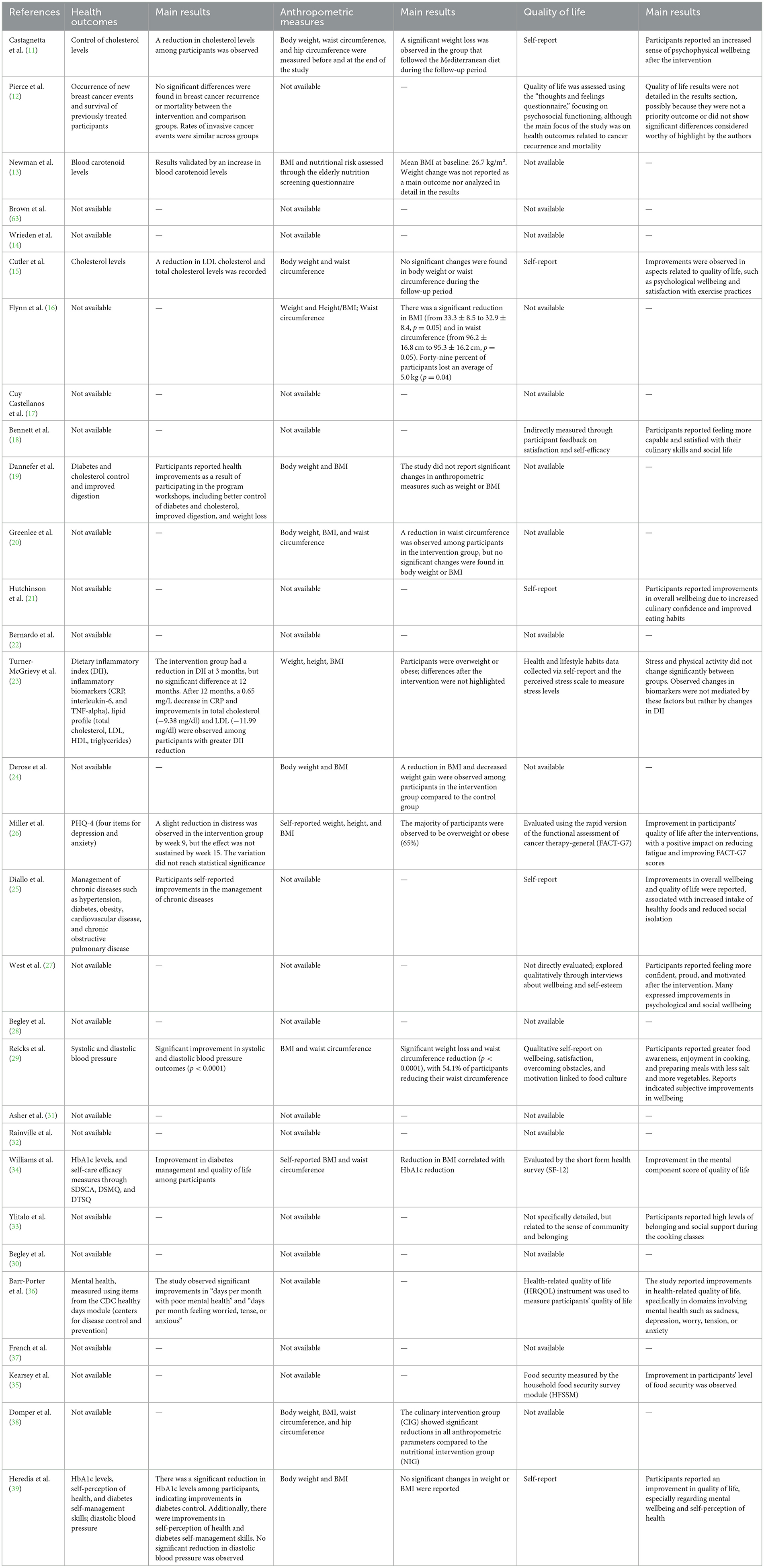
Table 3. Study information: health outcomes, anthropometric measures, quality of life, and main results.
2.6 Outcomes
To characterize comprehensive food utilization, culinary workshops promoting the full use of fresh foods were considered, prioritizing healthier dietary habits. Identified strategies included culinary workshops that taught techniques for recipes using fresh foods.
These workshops also featured educational actions such as meal planning, safe and proper food storage guidelines, and practical recipes and techniques involving fresh and minimally processed foods.
3 Results
The database search yielded 1,658 articles (Figure 1). After removing duplicate manuscripts (n = 261), 1,397 titles and abstracts were screened, resulting in the exclusion of 1,372 studies. An initial full-text analysis was conducted on 25 studies, of which seven were excluded for the following reasons: absence of health outcomes (n = 2), cross-sectional design without pre- and post- culinary workshop measurements (n = 2), inclusion of children as part of the population (n = 2), and being study protocols (n = 1). The Google Scholar search returned numerous results, sorted by relevance; only the first 100 entries were analyzed for inclusion. Following a careful review, 88 studies were excluded due to lack of data on dietary preferences or involving child populations. Ultimately, 30 studies were included for full-text analysis (11–40). The selected studies were published between 2002 and 2025, all of which were written in English.
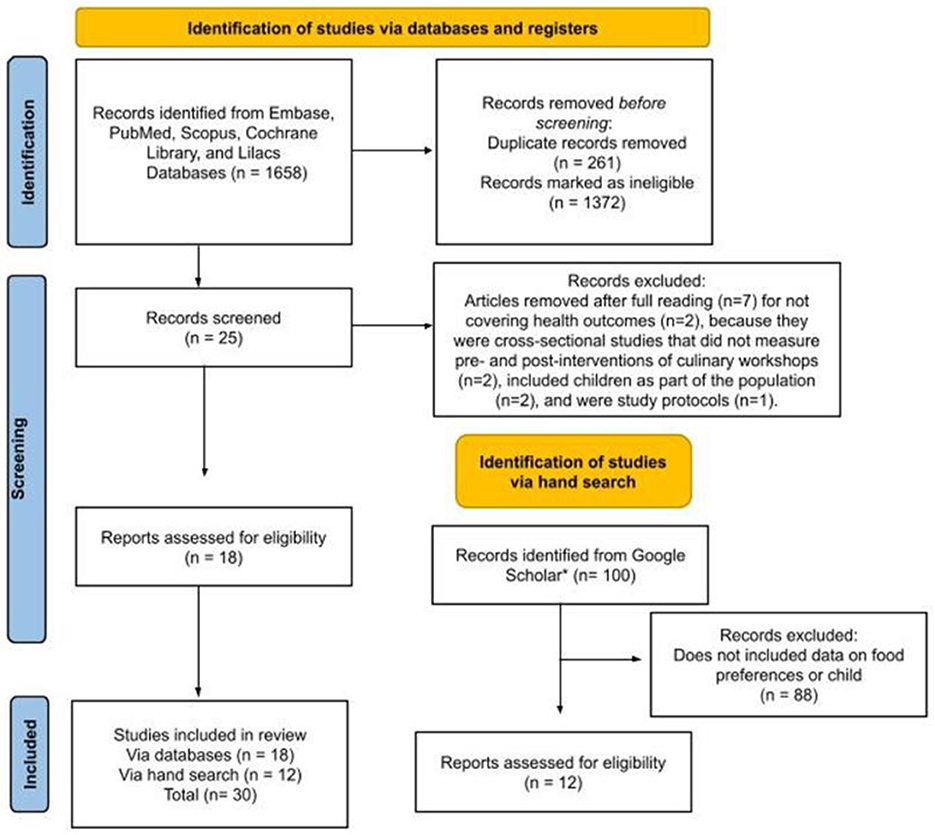
Figure 1. Flowchart of search and selection of studies for inclusion in the scoping review, based on the PRISMA-ScR.
Among the selected studies, the majority were conducted in the United States (60%) and Australia (16.66%), likely reflecting the research funding and infrastructure available in these countries. The United Kingdom (6.66%), Spain, Italy, Ireland, New Zealand, and Brazil each accounted for 3.33% of the studies (Table 1).
Analysis of the target groups revealed a strong focus on vulnerable populations, including individuals with low socioeconomic status, adults with preexisting health conditions (such as diabetes, cancer, and obesity), and ethnically diverse communities, notably Indigenous, African American, and Hispanic groups. Culinary and nutritional interventions were primarily implemented in community and healthcare settings, such as community centers, clinics, and food distribution organizations.
Table 1 summarizes the key characteristics of the studies included in this review, highlighting important details such as the location of the workshops, the populations involved, the delivery modes (whether in-person, virtual, or hybrid), and the frequency and duration of each intervention (Table 1).
Educational contexts, both formal (universities and hospitality schools) and informal (online courses), as well as farmers' markets and rural extension services, were also utilized, reflecting efforts to adapt interventions to local resources and emerging technologies. However, some studies lacked detailed descriptions of their intervention settings, highlighting a need for more contextual information in future research.
Regarding the format of the workshops, 80% were conducted in person, suggesting a preference for direct interaction, while 16.6% were delivered virtually and 3.3% used a hybrid format. This distribution reflects the growing adaptation to digital technologies, potentially accelerated by the COVID-19 pandemic. Sessions typically occurred weekly, lasting from 30 min to 3 h, with most programs spanning 4–8 weeks, although some extended up to 12 months or longer (Table 1).
In Table 2, we present the types of foods used in the workshops and the specific culinary preparations participants engaged with. Additionally, the table includes insights into food consumption patterns and participants' autonomy in making food choices (Table 2).
The analysis of ingredients used in interventions revealed a predominant focus on fruits and vegetables (83.3%), followed by whole grains (36.6%) and lean proteins (23.3%), with some studies referencing specific dietary patterns such as the Mediterranean and Atlantic diets. However, 16.6% of the studies did not provide detailed ingredient information, limiting the scope of analysis. The most common culinary preparations included salads (36.6%), soups (23.3%), and vegetable dishes (17.9%; Table 2).
Table 3 summarizes the health outcomes observed across the studies, focusing on changes in anthropometric measures, quality of life, and other clinical indicators. This overview is essential for understanding the broader impact of the culinary workshops, showing how they can contribute to improvements in both physical health and mental wellbeing (Table 3).
Among the studies included in this review, only fourteen reported clinical health outcomes. A significant reduction in glycated hemoglobin (HbA1c) levels and improved management of type 2 diabetes mellitus were observed following 6–12 weeks of culinary workshops (35, 40). A decrease in C-reactive protein (CRP) levels was also reported, associated with increased consumption of anti-inflammatory foods (24). Improvements in lipid profiles, particularly reductions in total cholesterol and LDL cholesterol, were identified in two studies (11, 16). Only one study directly measured blood pressure as a primary outcome, demonstrating statistically significant reductions in both systolic and diastolic blood pressure values (p < 0.0001) after a 6-week in-person intervention based on plant-based foods. Regarding mental health and wellbeing, several studies reported significant improvements, including reductions in the number of days experiencing feelings of sadness or anxiety (21, 26, 37) (Table 3).
Reductions in anthropometric parameters, such as body weight, BMI, and waist/hip circumference, were reported in 15 of the 33 studies. These outcomes were more commonly observed in interventions lasting 6 weeks or longer, with 53% showing statistically significant changes (11, 17, 25, 30, 35, 39) (Table 3).
Dietary autonomy was assessed in 81% of the studies, with robust and statistically significant evidence of improvements in confidence, culinary self-efficacy, dietary management, practical skills, and attitudes toward healthy eating (24, 27, 31, 34, 35, 39) (Table 3).
Regarding dietary intake, more than 90% of the studies demonstrated significant improvements in eating patterns, particularly with increased consumption of fruits, vegetables, whole grains, and minimally processed foods. Additionally, the interventions had a direct impact on reducing the consumption of added sugars, total calories, and ultra-processed foods (11, 15, 18, 20, 21, 23, 41) (Table 3).
Quality of life was assessed in seven studies, with statistically significant results observed in only three of them (11, 18, 26), which reported improvements in mental, functional, and emotional domains. The remaining studies provided qualitative evidence of enhanced wellbeing, health perception, and social engagement, particularly among vulnerable populations (Table 3).
4 Discussion
Culinary workshops have expanded their reach as an effective means to promote healthy eating habits and strengthen food and nutrition education (FNE). The results of this review directly corroborate this trend, highlighting that this type of intervention encompasses not only technical-cooking instruction but also a space for critical learning about food and its myriad possibilities, including the exchange of knowledge and cultural particularities that impact health, eating behavior, autonomy, and wellbeing.
In particular, although autonomy was not always directly measured, several studies documented improvements in culinary self-efficacy, confidence in food preparation, and greater independence in dietary choices. These findings support the interpretation of dietary autonomy as a multidimensional construct, often indirectly captured through behavioral and self-perception changes.
This analysis identified that eight studies reported statistically significant reductions in anthropometric parameters, such as body weight, BMI, and waist circumference. These findings reinforce the experiences reported by Freitas et al. (40), who used workshops as a training strategy for Nutrition students, evidencing that applied knowledge has the potential to positively influence participants' physical health. However, more robust clinical effects tend to emerge when workshops are combined with other systematic nutrition education actions and multidisciplinary approaches (41).
Although the presented data suggest the potential of workshops to positively influence metabolic health, the magnitude of the effects varies widely, as sustainability over the long term is often a determining factor (42). Therefore, there is a need to standardize protocols and assessments that address clinical and anthropometric parameters.
The results related to significant improvements in dietary intake are largely consistent with other studies found in the literature (7, 43), which describe culinary workshops as “sensitizing settings” capable of encouraging more conscious and sustainable eating practices. The study by Begley et al. (30), included in this review, showed significant gains in meal planning and preparation domains, reinforcing the idea that culinary practice is indeed a mechanism for food empowerment.
Moreover, as indicated by the data obtained from this synthesis and in line with the studies by Vaughan et al. (44) and Luz et al. (45), longer interventions tend to generate more consistent effects on eating behavior, as well as increased acceptance of new foods through repeated exposure and sensory engagement, favoring changes in food preferences.
Although data on quality of life were scarce among the included studies, the subjective effects reported on mental wellbeing, self-esteem, and positive health perception align harmoniously with findings related to the recovery of affective memories associated with cooking, the strengthening of social bonds, and the appreciation of culinary practices (46).
Among the aspects addressed in this review, it is confirmed that the duration of workshops is a fundamental factor for their effectiveness. Longer interventions, going beyond one-off meetings and offering follow-up or reinforcement of content, were associated with greater adherence, improvements in food consumption, and autonomy. Additionally, continuous approaches adapted to the realities of participants have proven to be much more effective, as they strengthen bonds and cultural appreciation (47). However, few studies conducted follow-up assessments, limiting the understanding of the long-term sustainability of the effects.
In Brazil, the promotion of healthy eating is supported by a robust set of public policies and structural programs. Among the most prominent are the National School Feeding Program (PNAE), which ensures balanced meals and nutrition education activities in public schools (48); the Dietary Guidelines for the Brazilian Population, an internationally recognized reference for its emphasis on fresh and minimally processed foods (49); and the Health in Schools Program (PSE), which integrates intersectoral actions focused on health and nutrition (50).
Additionally, local initiatives such as community gardens, solidarity kitchens, and university extension projects expand access to healthy foods and reinforce sustainable practices (51–53). These actions form an ecosystem of strategies aimed at improving food quality and promoting food and nutritional security, in which culinary workshops emerge as an educational and community tool with high potential for impact.
Despite growing interest in cooking workshops as a tool for improving eating habits and promoting health, there is still a significant gap in research focused on the impact of these interventions in developing countries such as Brazil. Most existing studies have mainly involved university students, a population that, although it shows beneficial results with these interventions, does not accurately reflect the broader demographic characteristics of most developing countries (22, 54). University students generally represent a more educated and higher-income group, which contrasts with the socioeconomic reality of the general population in countries such as Brazil, where lower levels of education, income disparity, and limited access to resources prevail (55).
While many successful interventions have been conducted in developed countries, the approach to culinary workshops can be adapted to the Brazilian context by considering local food habits, cultural diversity, and available resources. Workshops in Brazil, for example, could emphasize the use of traditional and locally available foods, making them more accessible and relevant to local populations. Additionally, adapting recipes to incorporate affordable ingredients and leveraging local knowledge on food preparation can increase the effectiveness and sustainability of these interventions (56).
Considering their multiple facets—from physical health to emotional wellbeing—culinary workshops should be integrated into public food and nutrition policies. Programs mentioned in the scope of the studies, such as “Cooking Matters” conducted in the United States, have already demonstrated applicability in vulnerable populations, while in Brazil, reported experiences (7, 43, 46) highlight the potential of workshops to strengthen fairer, more inclusive, and sustainable eating practices. It is essential to foster collaboration among universities, research centers, healthcare services, and social movements to support the implementation of culinary workshops as a health promotion tool, as they can become powerful pedagogical, community, and political instruments to tackle non-communicable chronic diseases and food insecurity.
Incorporating culinary workshops into public health initiatives in Brazil and similar countries requires a broader and more inclusive approach. Future studies should aim to include diverse populations, such as low-income communities, rural areas, and individuals with lower levels of formal education, to better capture the challenges and potential benefits for these groups. Additionally, adapting the content and delivery of culinary workshops to the specific needs and preferences of these populations, considering factors such as local food availability, cultural relevance, and economic constraints will be key to ensuring the success and sustainability of these interventions (57).
The standardization of culinary workshops can be achieved by establishing clear guidelines to ensure consistency across interventions. This includes defining specific objectives for each workshop, such as enhancing food autonomy or increasing the consumption of fresh and minimally processed foods. Moreover, it is essential to set recommended durations and frequencies for the workshops, with most programs running between 4 and 8 weeks to facilitate adherence and the practical application of learned concepts (14, 16, 18, 19, 24–26, 29, 31, 33–35, 38).
In addition, standardization should encompass the use of consistent assessment methods, such as self-report questionnaires and food diaries, which allow for comparability across different studies and contexts. Embracing digital platforms, increasingly prominent in the 21st century, is also a key strategy for expanding access to culinary workshops. Virtual and hybrid models offer flexible alternatives, particularly for individuals in remote areas or those with mobility challenges. The use of digital tools, such as apps and online videos, can further enhance the accessibility and adaptability of these interventions (58, 59).
Encouraging the participation of health professionals, such as nutritionists, during culinary workshops to provide accurate and personalized information is a way to ensure that participants receive appropriate and safe dietary guidance. Nutritionists can also play a key role in adapting recipes for specific health conditions, such as diabetes or hypertension, promoting healthy and safe eating. Integrating culinary workshops with other health services can enhance results and ensure continuity of care (60).
Another important aspect is the need to address food safety issues in culinary workshops, offering information about accessible and safe ingredients for consumption, as well as emphasizing food hygiene practices and allergy prevention (61, 62).
To incorporate culinary workshops into public policies in Brazil and similar countries, several mechanisms should be considered. First, integrating these workshops into existing programs such as PNAE or PSE could provide a framework for reaching large-scale populations. Workshops could be offered as part of nutrition education and health promotion initiatives, particularly in low-income and vulnerable communities, where access to nutritional education and healthy food is limited.
Another key mechanism would be aligning culinary workshops with local health and nutrition policies, ensuring they are incorporated into the broader strategy for improving diet quality and food security. Partnerships between universities, community organizations, and local governments could facilitate the implementation and scaling up of these workshops, while also considering the cultural, social, and economic realities of different regions.
5 Conclusions
Culinary workshops have shown positive impacts on health, but methodological limitations—such as short follow-ups and underrepresentation of studies in vulnerable settings—affect the generalizability of findings. Integrating these workshops into public policies through interdisciplinary, intersectoral, and community-based approaches can enhance their social relevance and long-term impact. Beyond cooking skills, workshops that embrace social and educational dimensions contribute to healthier, more equitable, and sustainable food practices.
Author contributions
PF: Conceptualization, Software, Validation, Visualization, Investigation, Data curation, Writing – review & editing, Formal analysis, Resources, Writing – original draft. LS: Writing – review & editing, Formal analysis, Software, Data curation, Writing – original draft, Resources, Investigation, Visualization, Conceptualization, Validation. AR: Project administration, Investigation, Supervision, Writing – review & editing, Funding acquisition. TA: Investigation, Funding acquisition, Writing – review & editing. NA: Writing – review & editing, Investigation, Funding acquisition. AS: Funding acquisition, Writing – review & editing, Investigation. NG: Methodology, Supervision, Investigation, Conceptualization, Validation, Data curation, Writing – review & editing, Writing – original draft, Formal analysis, Visualization, Resources.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by the project UIDB/00772/2020 (doi: 10.54499/UIDB/00772/2020) funded by the Portuguese Foundation for Science and Technology (FCT). This work was also funded by the Fundação para a Ciência e a Tecnologia (FCT) through the CBIOS projects UIDB/04567/2025 and UIDP/04567/2025.
Acknowledgments
The author NA would like to thank the Princess Nourah bint Abdulrahman University Researchers Supporting Project (number PNURSP2025R130), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia. The author NG would like to thank the National Council for Scientific and Technological Development of Brazil (Conselho Nacional de Desenvolvimento Científico e Tecnológico) 309183/2025-1 for the provided funds.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2025.1653406/full#supplementary-material
References
1. da Costa GG, Nepomuceno GdC, Pereira AdS, Simões BF. Worldwide dietary patterns and their association with socioeconomic data: an ecological exploratory study. Glob Health. (2022) 18:31. doi: 10.1186/s12992-022-00820-w
2. Independent Expert Group. 2021 Global Nutrition Report: The State of Global Nutrition. Bristol, UK: Development Initiatives (2021). Available online at: https://globalnutritionreport.org/reports/2021-global-nutrition-report/ (Accessed May 2025).
3. Afshin A, Sur PJ, Fay KA, Cornaby L, Ferrara G, Salama JS, et al. Health effects of dietary risks in 195 countries, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet. (2019) 393:1958–72. doi: 10.1016/S0140-6736(19)30041-8
4. Cain J, Silva V, Franco B, Luz L, Santos E, Novello D. Oficinas de culinária melhoram a aceitabilidade de alimentos entre crianças de idade escolar. Res Soc Develop. (2020) 9:e20942952. Portuguese. doi: 10.33448/rsd-v9i4.2952
5. Fernandes L, Inácio M, Carvalho G, Machado M, Maciel L, Pereira M. Food and nutrition education actions based on pestalozzi's intuitive method. O Mundo Da Saúde. (2021) 45:424–35. doi: 10.15343/0104-7809.202145424439
6. Frois SFB, Dourado LM, Pinho L. Promoção da alimentação saudável entre profissionais de saúde na atenção primária. Rev Bras Promoc Saúde. (2016) 29:621–6. Portuguese. doi: 10.5020/18061230.2016.p621
7. Oliveira M, Oliveira A. Oficina culinária como troca de saberes, educação alimentar e nutricional, e inclusão produtiva. Revista Em Extensão. (2022) 20:196–212. Portuguese. doi: 10.14393/REE-v20n22021-60873
8. Ihlebæk C, Ånestad R, Nordbø E. Bridging discourses on health promotion and social sustainability towards healthy community development. Scand J Public Health. (2024) 53(1_suppl):16–23. doi: 10.1177/14034948241290282
9. Monteiro CA, Cannon G, Moubarac JC, Levy RB, Louzada MLC, Jaime PC. The UN Decade of Nutrition, the NOVA food classification and the trouble with ultra-processing. Public Health Nutr. (2018) 21:5–17. doi: 10.1017/S1368980017000234
10. Swinburn BA, Kraak VI, Allender S, Atkins VJ, Baker PI, Bogard JR, et al. The global syndemic of obesity, undernutrition, and climate change: the lancet commission report. Lancet. (2019) 393:791–846. Erratum in: Lancet. (2019) 393:746. doi: 10.1016/S0140-6736(18)32822-8
11. Castagnetta L, Granata OM, Cusimano R, Ravazzolo B, Liquori M, Polito L, et al. The MEDIET project. Ann NY Acad Sci. (2002) 963:282–9. doi: 10.1111/j.1749-6632.2002.tb04119.x
12. Pierce JP, Faerber S, Wright FA, Rock CL, Newman V, Flatt SW, et al. A randomized trial of the effect of a plant-based dietary pattern on additional breast cancer events and survival: the women's healthy eating and living (WHEL) study. Control Clin Trials. (2002) 23:728–56. doi: 10.1016/S0197-2456(02)00241-6
13. Newman VA, Thomson CA, Rock CL, Flatt SW, Kealey S, Bardwell WA, et al. Achieving substantial changes in eating behavior among women previously treated for breast cancer—an overview of the intervention. J Am Diet Assoc. (2005) 105:382–91. doi: 10.1016/j.jada.2004.12.008
14. Wrieden WL, Anderson AS, Longbottom PJ, Valentine K, Stead M, Caraher M, et al. The impact of a community-based food skills intervention on cooking confidence, food preparation methods and dietary choices–an exploratory trial. Public Health Nutr. (2007) 10:203–11. doi: 10.1017/S1368980007246658
15. Cutler L, King B, McCarthy N, Hamilton G, Cook L. Appetite for life: an evaluation of a primary care lifestyle programme. J Prim Health Care. (2010) 2:281–7. doi: 10.1071/HC10281
16. Flynn MM, Reinert S, Schiff AR. A six-week cooking program of plant-based recipes improves food security, body weight, and food purchases for food pantry clients. J Hunger Environ Nutr. (2013) 8:73–84. doi: 10.1080/19320248.2012.758066
17. Cuy Castellanos DC, Christaldi J, Borer K. Using the diffusion of innovations to develop healthy cooking demonstrations at a farmers' market. J Hunger Environ Nutr. (2014) 9:471–84. doi: 10.1080/19320248.2014.908448
18. Bennett AE, Cunningham C. A qualitative evaluation of a healthy cookery course in Ireland designed for adults with mild to moderate intellectual disability. J Intellect Disabil. (2014) 18:270–81. doi: 10.1177/1744629514544074
19. Dannefer R, Abrami A, Rapoport R, Sriphanlop P, Sacks R, Johns M, et al. mixed-methods evaluation of a SNAP-Ed farmers' market–based nutrition education program. J Nutr Educ Behav. (2015) 47:516–25. doi: 10.1016/j.jneb.2015.08.021
20. Greenlee H, Gaffney AO, Aycinena AC, Koch P, Contento I, Karmally W, et al. ¡Cocinar para su salud!: randomized controlled trial of a culturally based dietary intervention among Hispanic breast cancer survivors. J Acad Nutr Diet. (2015) 115:709–23. doi: 10.1016/j.jand.2014.11.002
21. Hutchinson J, Watt JF, Strachan EK, Cade JE. Evaluation of the effectiveness of the ministry of food cooking programme on self-reported food consumption and confidence with cooking. Public Health Nutr. (2016) 19:3417–27. doi: 10.1017/S1368980016001476
22. Bernardo GL, Jomori MM, Fernandes AC, Colussi CF, Condrasky MD, Proença RPC. Positive impact of a cooking skills intervention among Brazilian university students: six months follow-up of a randomized controlled trial. Appetite. (2018) 130:247–55. doi: 10.1016/j.appet.2018.08.014
23. Turner-McGrievy GM, Wirth MD, Shivappa N, Dunn CG, Crimarco A, Hurley TG, et al. Impact of a 12-month inflammation management intervention on the Dietary Inflammatory Index, inflammation, and lipids. Clin Nutr ESPEN. (2019) 30:42–51. doi: 10.1016/j.clnesp.2019.02.008
24. Derose KP, Williams MV, Flórez KR, Griffin BA, Payán DD, Seelam R, et al. Eat, pray, move: a pilot cluster randomized controlled trial of a multilevel church-based intervention to address obesity among African Americans and Latinos. Am J Health Promot. (2019) 33:586–96. doi: 10.1177/0890117118813333
25. Diallo AF, Falls K, Hicks K, McQueen Gibson E, Obaid R, Slattum P, et al. The healthy meal program: a food insecurity screening and referral program for urban dwelling older adults. Public Health Nurs. (2020) 37:671–6. doi: 10.1111/phn.12778
26. Miller MF Li Z, Habedank M. A randomized controlled trial testing the effectiveness of coping with cancer in the kitchen, a nutrition education program for cancer survivors. Nutrients. (2020) 12:3144. doi: 10.3390/nu12103144
27. West EG, Lindberg R, Ball K, McNaughton SA. The role of a food literacy intervention in promoting food security and food literacy—OzHarvest's NEST Program. Nutrients. (2020) 12:2197. doi: 10.3390/nu12082197
28. Begley A, Paynter E, Butcher L, Bobongie V, Dhaliwal SS. Identifying who improves or maintains their food literacy behaviours after completing an adult program. Int J Environ Res Public Health. (2020) 17:4462. doi: 10.3390/ijerph17124462
29. Reicks M, Gold A, Tran N, LeBlanc K. Impacts of a taste of African heritage: a culinary heritage cooking course. J Nutr Educ Behav. (2022) 54:388–96. doi: 10.1016/j.jneb.2021.11.008
30. Begley A, Fisher I, Butcher L, Foulkes-Taylor F, Giglia R, Dhaliwal SS. Determining the effectiveness of an adult food literacy program using a matched control group. J Nutr Educ Behav. (2023) 55:659–66. doi: 10.1016/j.jneb.2023.06.001
31. Asher RC, Clarke ED, Bucher T, Shrewsbury VA, Roberts S, Collins CE. Impact and evaluation of an online culinary nutrition course for health, education and industry professionals to promote vegetable knowledge and consumption. J Hum Nutr Diet. (2023) 36:967–80. doi: 10.1111/jhn.13109
32. Rainville AJ, Ford O, Bessire R, Wu T-Y. Field notes: implementation of healthy for life® virtual cook-along classes. J Hunger Environ Nutr. (2023) 18:731–5. doi: 10.1080/19320248.2022.2157692
33. Ylitalo KR, Janda KM, Clavon R, Raleigh-Yearby S, Kaliszewski C, Rumminger J, et al. Cross-sector partnerships for improved cooking skills, dietary behaviors, and belonging: findings from a produce prescription and cooking education pilot program at a federally qualified health center. Nutrients. (2023) 15:4098. doi: 10.3390/nu15194098
34. Williams A, Shrodes JC, Radabaugh JN, Braun A, Kline D, Zhao S, et al. Outcomes of cooking matters for diabetes: a 6-week randomized, controlled cooking and diabetes self-management education intervention. J Acad Nutr Diet. (2023) 123:477–91. doi: 10.1016/j.jand.2022.07.021
35. Kearsey JL, West E, Vairinhos N, Constable N, Chu A, Douglas N, et al. Evaluation of a nutrition education and skills training programme in vulnerable adults who are at high risk of food insecurity. J Hum Nutr Diet. (2024) 37:418–29. doi: 10.1111/jhn.13264
36. Barr-Porter M, Sullivan A, Watras E, Winn C, McNamara J. Community-based designed pilot cooking and texting intervention on health-related quality of life among college students. Int J Environ Res Public Health. (2024) 21:293. doi: 10.3390/ijerph21030293
37. French CD, Gomez-Lara A, Hee A, Shankar A, Song N, Campos M, et al. Impact of a food skills course with a teaching kitchen on dietary and cooking self-efficacy and behaviors among college students. Nutrients. (2024) 16:585. doi: 10.3390/nu16050585
38. Domper J, Gayoso L, Goni L, Perezábad L, Razquin C, de la O V, et al. An intensive culinary intervention programme to promote healthy ageing: the SUKALMENA-InAge feasibility pilot study. Nutrients. (2024) 16:1735. doi: 10.3390/nu16111735
39. Heredia NI, Macias-Navarro L, Guevara DC, Sharma SV, Chow J, Bentley SS, et al. Testing of a culinary medicine intervention for racially/ethnically diverse adults with type 2 diabetes. J Nutr Educ Behav. (2025) 57:263–73. doi: 10.1016/j.jneb.2024.11.006
40. Freitas B, Japúr C, Silva A, Penaforte F, Rinaldi A. Oficina culinária como estratégia didático-pedagógica interdisciplinar na formação do nutricionista. Medicina (Ribeirão Preto). (2023) 56:e-194043. Portuguese doi: 10.11606/issn.2176-7262.rmrp.2023.194043
41. Lang R, Jennings M, Lam C, Yeh H, Zhu C, Kumra T. Community culinary workshops as a nutrition curriculum in a preventive medicine residency program. MedEdPORTAL. (2019) 15:10859. doi: 10.15766/mep_2374-8265.10859
42. Hasan B, Thompson WG, Almasri J, Wang Z, Lakis S, Prokop LJ, et al. The effect of culinary interventions (cooking classes) on dietary intake and behavioral change: a systematic review and evidence map. BMC Nutr. (2019) 5:29. doi: 10.1186/s40795-019-0293-8
43. Peres B, Vidal M, Gama L, Pires É, Reis D, Silva M, et al. Oficina culinária como estratégia de articulação entre os movimentos sociais e a comunidade acadêmica para a promoção da alimentação saudável e sustentável: relato de experiência. Rev Bras Ext Univ. (2021) 12:179–89. Portuguese. doi: 10.36661/2358-0399.2021v12i2.11611
44. Vaughan KL, Cade JE, Hetherington MM, Webster J, Evans CEL. The impact of school-based cooking classes on vegetable intake, cooking skills and food literacy of children aged 4-12 years: a systematic review of the evidence 2001-2021. Appetite. (2024) 195:107238. doi: 10.1016/j.appet.2024.107238
45. Luz L, Menezes M, Santos E, Novello D. Elaboração de produtos adicionados de casca de berinjela em oficinas de culinária. Vivências. (2022) 18:287–99. Portuguese doi: 10.31512/vivencias.v18i37.507
46. Costa A, Grimes L, Antunes A, Silva L, Lima N, Miranda N, et al. Oficina culinária como estratégia de educação alimentar e nutricional para promoção da saúde. Revista Contemporânea. (2024) 4:e4458. Portuguese. doi: 10.56083/RCV4N5-184
47. Kumra T, Rajagopal S, Johnson K, Garnepudi L, Apfel A, Crocetti M. Patient centered medical home cooking: community culinary workshops for multidisciplinary teams. J Prim Care Community Health. (2021) 12:2150132720985038. doi: 10.1177/2150132720985038
48. Boklis-Berer M, Rauber F, Azeredo CM, Levy RB, Louzada ML, da C. School meals consumption is associated with a better diet quality of Brazilian adolescents: results from the PeNSE 2015 survey. Public Health Nutr. (2021) 24:6512–20. doi: 10.1017/S1368980021003207
49. Gabe KT, dos Santos Costa C, dos Santos FS, Souza TN, Jaime PC. Is the adherence to the food practices recommended by the dietary guidelines for the Brazilian population associated with diet quality? Appetite. (2023) 190:107011. doi: 10.1016/j.appet.2023.107011
50. DallaCosta M, Rodrigues RM, Schütz G, Conterno S. School health program: challenges and possibilities for health promotion from the perspective of healthy eating. Saúde em Debate. (2023) 46:244–60. doi: 10.1590/0103-11042022e318
51. dos Santos M, Machado MCM. Agricultura Urbana e Periurbana: Segurança Alimentar e Nutricional, comportamento alimentar e transformações sociais em uma horta comunitária. Segurança Alimentar e Nutricional. (2020) 27:e020010. Portuguese. doi: 10.20396/san.v27i0.8650689
52. Sousa M, Akutsu RC, Silva CMdS, Teixeira CS, Silva ICd. Food security in Brazil: evaluation of the effectiveness of community restaurants in the north and northeast regions. Int J Environ Res Public Health. (2025) 22:315. doi: 10.3390/ijerph22020315
53. Claudino MB, Carnaúba LAC, Nunes DdS, Cavalcante AL, Barbosa LB. Atividades Educativas No Projeto “Comida De Verdade: Ações Educativas Para Promoção Da Alimentação Saudável Na Universidade. Rev Eletr Extensao em Debate. (2025) 14. Portuguese. doi: 10.28998/rexd.v23.19452
54. Jorge L, Kraemer M, Fernandes A, Geraldo A, Hauschild D, Uggioni P, et al. Sustained impact of a culinary intervention with university students: a multimethod approach. Acad Nutr Diet. (2025) 2. doi: 10.20935/AcadNutr7577
55. Bertolin J, Fioreze C, Barão FR. Educação superior e desigualdade educacional no Brasil: herança elitista em contexto de expansão do acesso. Horizontes. (2024) 42:e023133. Portuguese. doi: 10.24933/horizontes.v42i1.1688
56. Van Kesteren R, Evans A. Cooking without thinking: how understanding cooking as a practice can shed new light on inequalities in healthy eating. Appetite. (2020) 147:104503. doi: 10.1016/j.appet.2019.104503
57. Partiwi N. Investigate the effectiveness, mechanisms, and scalability of community-based interventions designed to reduce health disparities. Adv Health Res. (2024) 2:49–65. doi: 10.60079/ahr.v2i1.371
58. Yousef NM, Wallace RJ, Harlan GA, Beale E. Bringing the “joy of healthy eating” to advanced medical students: utilizing a remote learning platform to teach culinary medicine: findings from the first online course based on the ACLM's whole-food plant-based culinary medicine curriculum. Am J Lifestyle Med. (2022) 16:447–59. doi: 10.1177/15598276221092971
59. Barnett A, Wright C, Stone C, Ho NY, Adhyaru P, Kostjasyn S, et al. Effectiveness of dietary interventions delivered by digital health to adults with chronic conditions: systematic review and meta-analysis. J Hum Nutr Diet. (2023) 36:632–56. doi: 10.1111/jhn.13125
60. Wood N, Stone T, Siler M, Goldstein M, Albin J. Physician-chef-dietitian partnerships for evidence-based dietary approaches to tackling chronic disease: the case for culinary medicine in teaching kitchens. J Healthc Leadersh. (2023) 15:129–37. doi: 10.2147/JHL.S389429
61. Cervato-Mancuso AM, Vincha KRR, Santiago DA. Educação Alimentar e Nutrici-onal como prática de intervenção: reflexão e possibilidades de fortalecimento. Physis: Revista de Saúde Coletiva. (2016) 26:225–49. Portuguese. doi: 10.1590/S0103-73312016000100013
62. Santos MJL, Merrill KA, Ben-Shoshan M, Gerdts JD, Giesbrecht D, Lavine E, et al. Food allergy education and management in early learning and childcare centres: a scoping review on current practices and gaps. Children. (2023) 10:1175. doi: 10.3390/children10071175
Keywords: culinary workshops, dietary intake, feeding behavior, nutrition education, public health
Citation: da Fonseca PG, Siqueira LdC, Raposo A, Alslamah T, Albaridi NA, Saraiva A and Guimarães NS (2025) From kitchen to health: how culinary workshops influence eating habits, autonomy, and wellbeing in adults–A scoping review. Front. Nutr. 12:1653406. doi: 10.3389/fnut.2025.1653406
Received: 25 June 2025; Accepted: 11 August 2025;
Published: 29 August 2025.
Edited by:
Zumin Shi, Qatar University, QatarReviewed by:
Carla Gonçalves, Universidade de Trás-os-Montes e Alto Douro, PortugalEmanuel Orozco, National Institute of Public Health, Mexico
Copyright © 2025 da Fonseca, Siqueira, Raposo, Alslamah, Albaridi, Saraiva and Guimarães. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: António Raposo, YW50b25pby5yYXBvc29AdWx1c29mb25hLnB0; Nathalia Sernizon Guimarães, bmFzZXJuaXpvbkBnbWFpbC5jb20=