 Taline Lazzarin1*
Taline Lazzarin1* Raquel Simões Ballarin1
Raquel Simões Ballarin1 Paula Schmidt Azevedo1
Paula Schmidt Azevedo1 Barbara R. Cardoso2,3*†
Barbara R. Cardoso2,3*† Marcos Ferreira Minicucci1†
Marcos Ferreira Minicucci1†- 1Internal Medicine Department, Medical School, São Paulo State University (Unesp), Botucatu, Brazil
- 2Department of Nutrition, Dietetics and Food, Monash University, Melbourne, VIC, Australia
- 3Victorian Heart Institute, Monash University, Clayton, VIC, Australia
Introduction: Nuts possess a beneficial nutritional profile with antioxidant and anti-inflammatory properties, potentially improving health outcomes in chronic kidney disease (CKD) patients. This systematic review evaluates the association between nut intake and lipid profile, inflammation, oxidative stress, blood pressure, and mortality in patients with CKD.
Methods: A systematic search was performed in Medline, EMBASE, Scopus, CINAHL, and Cochrane Library databases on 27 May 2024 and repeated on 13 February 2025 without restrictions on date, language, or study type.
Results: The search identified 2,521 records, with four studies (three trials, one cohort) involving 1,270 CKD patients meeting the inclusion criteria. The studies were heterogeneous in terms of intervention and biomarkers assessed, and all of them had moderate-to-high risk of bias. Overall the findings indicate positive effects of Brazil nuts and baru almond oil on oxidative stress and inflammation markers, while walnuts reduced LDL cholesterol and blood pressure while posing no risk regarding electrolytes balance. Further, the consumption of total nuts was associated with reduction in all-cause mortality.
Conclusion: Our review indicates potential benefits for the inclusion of nuts in the diet of patients with CKD, but further studies are required to translate findings into practice.
Systematic review registration: PROSPERO, Registration no CRD42024543880. https://www.crd.york.ac.uk/PROSPERO/view/CRD42024543880.
1 Introduction
Chronic kidney disease (CKD) is characterized by diminished kidney function, shown by a glomerular filtration rate of less than 60 mL/min per 1.73 m2, or markers of kidney damage, or both, present for a minimum of 3 months, causing negative health implications (1). Affecting approximately 850 million people worldwide, CKD is responsible for 41.5 million disability-adjusted life years and 1.43 million deaths annually (1, 2). Traditional risk factors for CKD development and progression include diabetes, hypertension, and obesity. However, non-traditional factors such as chronic inflammation, oxidative stress, endothelial dysfunction, uremic toxins, and gut dysbiosis also play a central role in its pathophysiology and prognosis. In particular, inflammation and oxidative stress contribute to vascular injury, endothelial dysfunction, and accelerated atherosclerosis, which markedly increase the risk of cardiovascular morbidity and mortality in this population (3).
Nutritional therapy is a key part of CKD management aiming at slowing disease progression, reducing albuminuria, and minimizing the harmful effects of uremic toxins (4). The National Kidney Foundation’s Kidney Disease Outcomes Quality Initiative (KDOQI) has provided evidence-based dietary guidelines for the management of kidney diseases since 1999, with great emphasis on an individualized approach to monitor protein intake, as well as control sodium, potassium and phosphorus circulating levels to prevent complications. Further, their most recent guidelines indicate that supplementing the diet of people with CKD with vitamins and trace elements does not improve outcomes and is not routinely recommended for these patients (4). Thus, more research focusing on nutritional interventions is needed to elucidate strategies with the potential to reduce inflammation and oxidative stress in CKD patients.
Nuts, described as dry fruits with an edible seed and a hard shell, are considered nutrient-dense foods due to their high concentration of vitamins, minerals, and bioactive compounds with redox action in addition to a high ratio of omega-3: omega-6 fatty acids (5–8). Peanuts, despite being botanically classified as legumes, have a similar nutritional profile as tree nuts and are thus commonly included in this group (9). The effects of nut intake have been associated with reduced risk of chronic diseases such as diabetes, cancer, cardiovascular diseases and cognitive impairment (10–14). Further, previous research has indicated the benefits of nuts on the oxidative stress and inflammation biomarkers in hemodialysis patients, indicating that this food group could serve as an affordable and manageable alternative for CKD management (15). Nonetheless, the effects of nut intake on CKD patients’ prognosis are still unclear. Further, some concerns have been raised regarding the high content of protein, phosphorus, and potassium present in nuts, since these nutrients are commonly restricted in the diet of CKD patients (4).
Therefore, this systematic review aims to synthesize current evidence on the association between nut consumption and health outcomes in patients with CKD, with a specific focus on mortality, lipid profile, blood pressure, and biomarkers of inflammation and oxidative stress. These outcomes were selected because they encompass both direct prognostic indicators (mortality) and key modifiable risk factors and underlying mechanisms (dyslipidemia, hypertension, chronic inflammation, and oxidative damage) that drive cardiovascular and renal disease (16) progression in this population. Further, we have examined the potential adverse effects of nut interventions on the concentrations of phosphorus and potassium.
2 Methods
This review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting guidelines (17). The review protocol was prospectively registered on the Prospective International Register of Systematic Reviews (PROSPERO, Registration no CRD42024543880).
2.1 Search strategy and eligibility criteria
We conducted a comprehensive literature search of the Medline, EMBASE, Scopus, CINAHL, and Cochrane Library databases on 27 May 2024 and repeated on 13 February 2025 to identify studies reporting on nut consumption in patients with CKD. All databases were searched from inception date using the terms: Adult* AND (Diet OR Nuts OR “Prunus Dulcis” OR Almond* OR Anacardium OR Cashew* OR Corylus OR Hazelnut* OR Pistacia OR Pistachio* OR Juglans OR Walnut* OR Carya OR Pecan* OR Arachis OR Peanut* OR Pinus OR ‘Pine nut*’ OR Bertholletia OR ‘Brazil nut*’) AND (Chronic Renal Insufficiency* OR Chronic Renal Insufficiencies* OR Chronic Kidney Insufficiency* OR Chronic Kidney Insufficiencies OR Chronic Kidney Diseases* OR Chronic Kidney Disease* OR Chronic Renal Diseases* OR Chronic Renal Disease*). The complete search strategy for each database is described in Supplementary Table 1.
Inclusion and exclusion criteria were formed based on the PICOS (population, intervention, comparison, outcome, and study design) format, described in Table 1. We included articles that assessed nut intake in adults with CKD and were published in any language. Additionally, we evaluated changes in phosphorus and potassium levels as adverse effects of nut consumption in CKD. Excluded articles referred to studies that assessed individuals without CKD, did not have a comparative group, did not quantify dietary nut intake or combined nuts with other foods (e.g., seeds), or did not report on CKD-related outcomes. To complement the electronic search, reference lists from selected studies and reviews were manually examined.
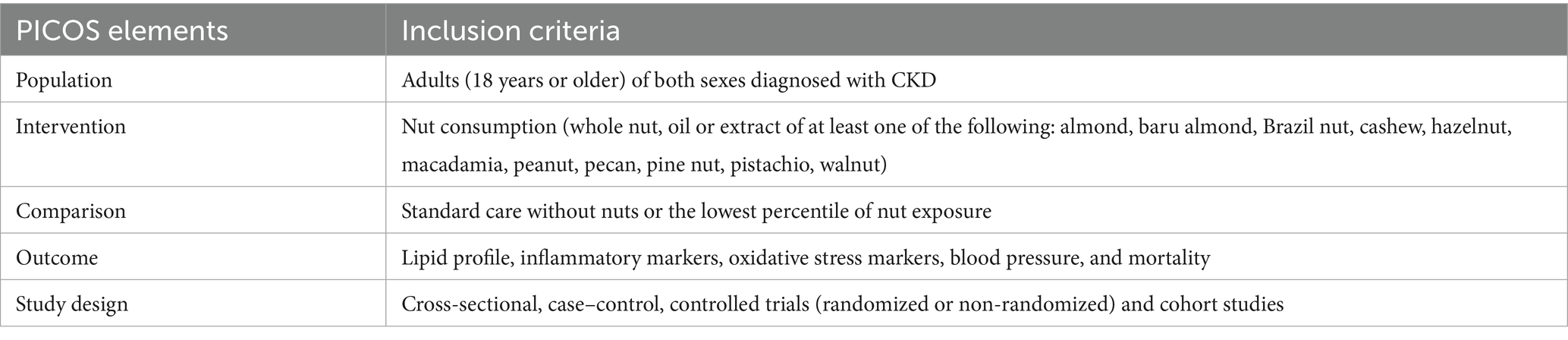
Table 1. PICOS format structured research question.
2.2 Study screening and data extraction
The study screening process was conducted in two stages by two independent authors (TL and RSB) using the systematic review software Rayyan (Cambridge, United States) (18), which automatically identified and excluded duplicate articles. First, titles and abstracts were screened; secondly, the full text of the remaining articles was screened according to the pre-specified inclusion. A third author (MFM) settled disagreements on study screening.
Upon completion of screening, data were independently extracted from each article by two authors (TL and RSB) using a data extraction template on Microsoft Excel. Data collected included first author, year of publication, country in which the study was conducted, study design, participant characteristics (age and gender), type and quantity of nuts consumed, methodology used to assess nut intake, length of the intervention/follow-up, and the health outcomes measured.
2.3 Risk of bias assessment
The risk of bias assessment of eligible articles was performed independently by two authors (RSB and TL). Disagreements were resolved in consultation with a third author (MFM). The Cochrane Risk of Bias 2.0 (RoB 2) tool was used to assess the quality of randomized and crossover trials (19). Studies were determined as having “low risk,” “high risk” or “some concerns.” The Risk of Bias In Non-randomized Studies - of Interventions (ROBINS-I) tool was used to assess the risk of bias in observational studies and non-randomized trials. As per the ROBINS-I tool, the studies were identified as providing “low,” “moderate,” “serious,” “critical,” or “no information” for each of the seven domains (confounding; participants selection; classification of interventions; deviations from intended interventions; missing data; measurement of outcomes; selection of the reported result). A final judgment based on the domains was then made to determine the study as having “low,” “moderate,” “serious,” or “critical” risk of bias (20) (Supplementary Figures 1–3).
3 Results
3.1 Study selection
The initial search identified 2,521 records, and after the exclusion of duplicates (n = 178), a total 2,343 articles were assessed for eligibility. In the first screening step, where abstracts and titles were screened, 2,335 records were excluded, and 8 full texts were comprehensively screened for eligibility. Additionally, one full-text article identified in the search update was also assessed for eligibility. Of these, five trials were excluded because of the absence of a control group (n = 1) wrong study population (n = 1), and unfinished study (n = 1). Thus, this systematic review included a total of four articles involving 1,270 participants (one cohort study (21) and three trials (22–24)) (Figure 1).
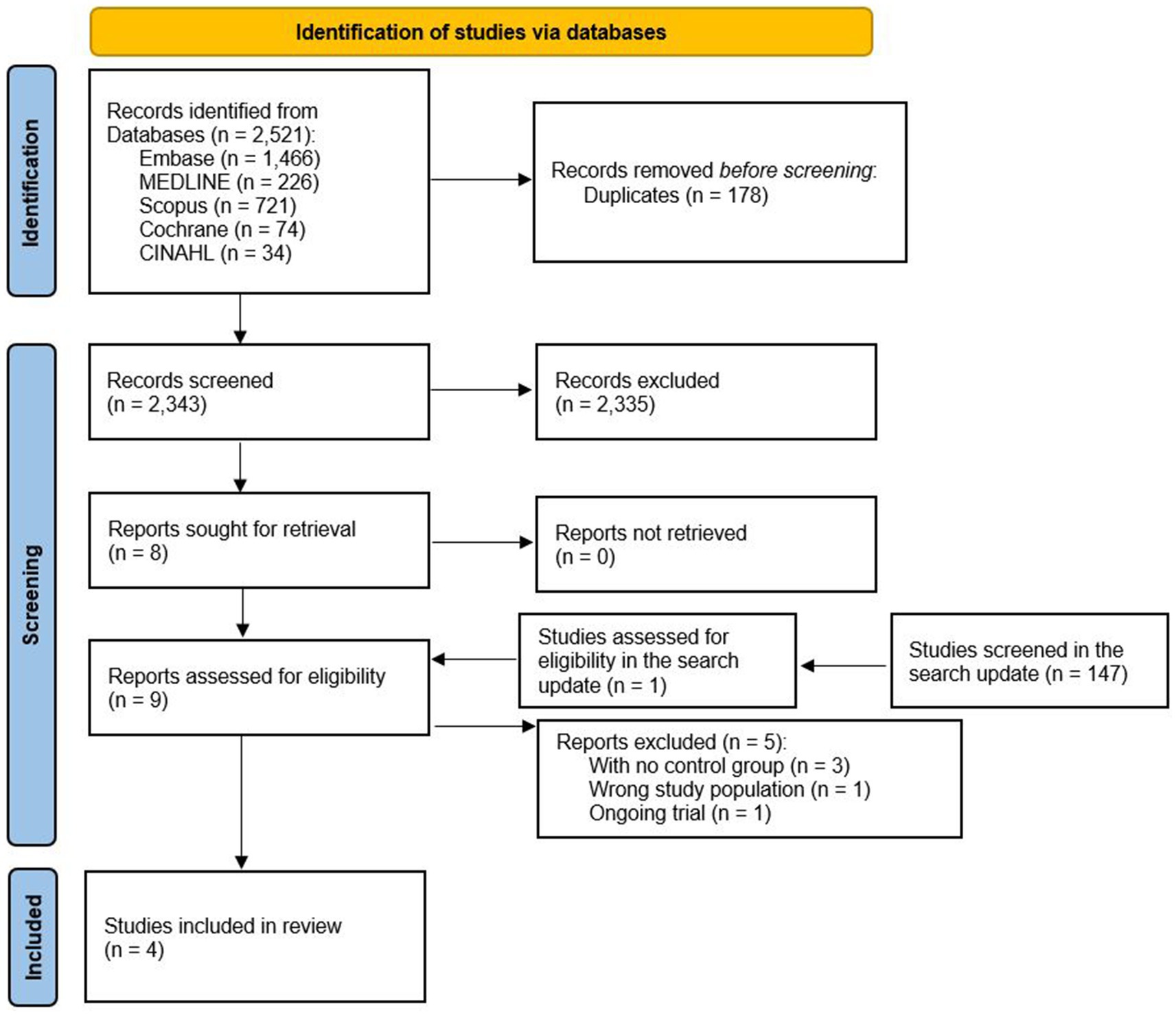
Figure 1. Flowchart of the article selection process.
3.2 Study characteristics
This review included two RCTs (one had a parallel arm (22), and one had a crossover design (23)), one pilot trial (24), and one cohort study (21). Out of the 1,270 participants included in the studies reviewed, 1,203 were part of the cohort study. Two trials were conducted with patients receiving hemodialysis treatment (22, 24), and Sanchis et al. (23) focused on patients receiving conservative management (without dialysis), while Wang et al. (21) did not report whether participants were receiving dialysis. While the observational study reported exposure to different nut types without specifying them (21), the trials supplemented baru almond oil (22), walnuts (23), or Brazil nuts (24). The duration of intervention in the trials ranged from 30 days (walnut study) (23) to 3 months (Brazil nut study; baru almond oil: 12 weeks) (24). Two studies assessed oxidative stress and inflammatory markers (22, 24), and lipid profile (22, 23), while arterial pressure (23), and mortality (21) were assessed. Given the heterogeneity of study designs, types of nuts consumed, and outcome measures reported in the studies included in this review, a meta-analysis of study results was not feasible; therefore, this review focuses on a narrative synthesis of study outcomes. The number of participants in each study, the interventions/exposures, and the outcomes are shown in Table 2 (21–24).
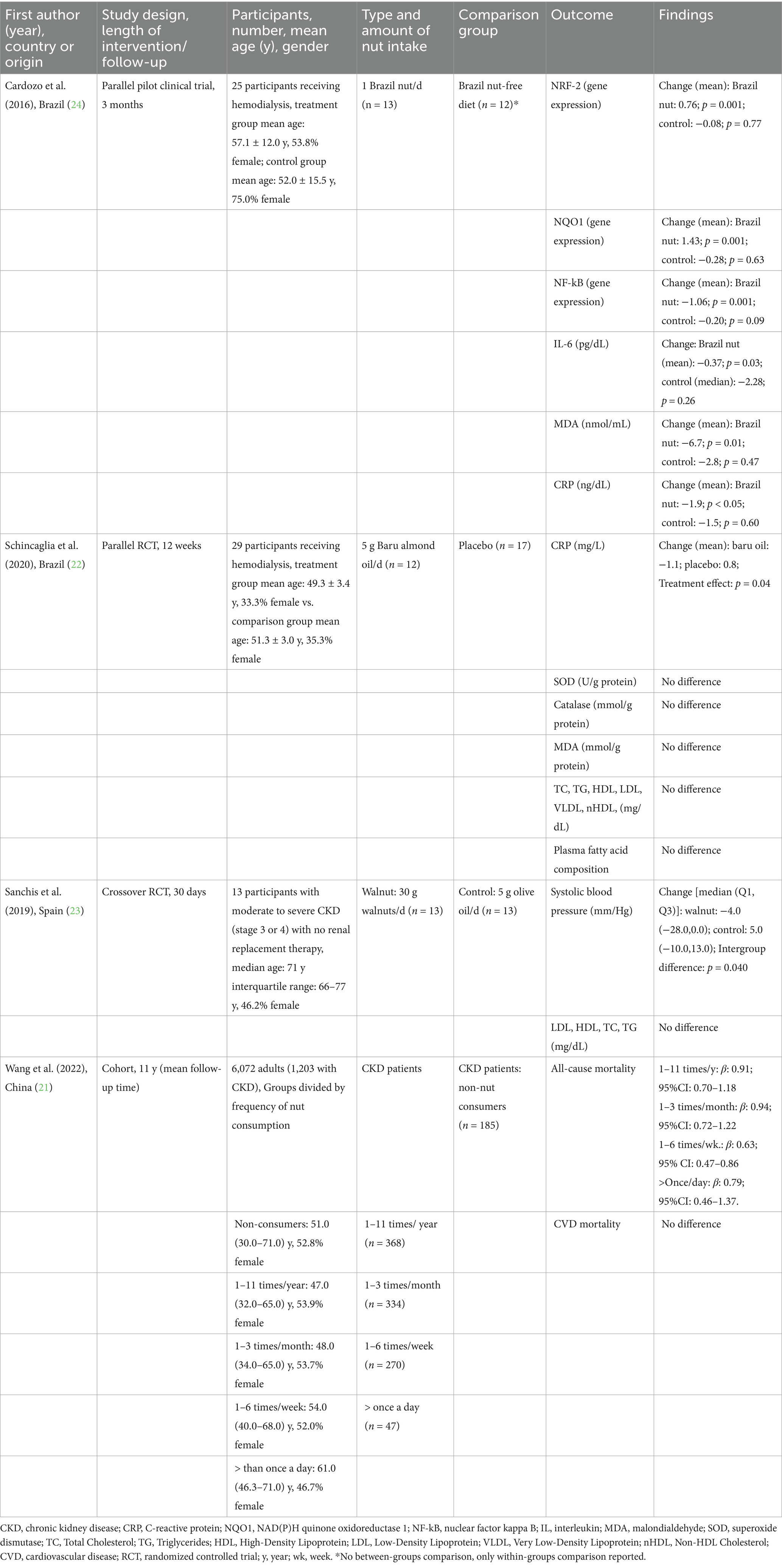
Table 2. Characteristics of studies that assessed the effects of nut consumption in patients with CKD.
3.3 Risk of bias
The study by Cardozo et al. (24) was judged to have a “high” risk of bias, as it did not provide a direct comparison between intervention and control groups, but only reported within-group pre–post analyses. Wang et al. (21) was determined to have “moderate” risk due to confounding bias caused by the intrinsic characteristics of the cohort participants (Supplementary Figure 1). According to the Cochrane RoB 2 tool, the study by Sanchis et al. (23) was rated as having “some concerns” because it was an open-label study and intention-to-treat analysis was not performed (Supplementary Figure 2). The study by Schincaglia et al. (22) was determined as having “high risk” due to the lack of information about randomization or allocation method, missing intention-to-treat analysis and significant loss during the follow-up (more than 30%) (Supplementary Figure 3).
3.4 Oxidative stress and inflammatory markers
Two studies assessed the effects of nuts on inflammatory and oxidative stress markers in hemodialysis patients (22, 24). In a pilot trial, Cardozo et al. (24) reported that the consumption of one Brazil nut a day for 3 months increased the expression of nuclear factor E2-related factor 2 (Nrf-2) and NAD(P)H: quinone oxidoreductase 1 (NQO1), and decreased the expression of nuclear factor kappa B (NF-kB) in relation to baseline. Among oxidative stress and inflammation markers, Brazil nut supplementation reduced plasma malondialdehyde (MDA), CRP and interleukin-6 (IL-6), while no significant changes were observed in the control group. However, it is important to note that statistical analyses were primarily conducted within each group (pre–post comparison) rather than directly testing between-group differences, which increases the risk of confounding and limits causal inference. In the study by Schincaglia et al. (23), supplementation with baru almond oil (5 g/day) for 12 weeks decreased CRP but had no effect on MDA or the antioxidant enzymes superoxide dismutase (SOD) and catalase (CAT) compared to a placebo (22).
3.5 Lipid profile and blood pressure
The effects of nut intake on plasma lipid concentrations were assessed in two studies. Interventions with baru almond oil (22) or walnuts (23) had no effects on blood lipids. In the only study assessing the effects of nuts on blood pressure, Sanchis et al. (23) demonstrated that 30 g walnuts/d for 30 days significantly reduced systolic blood pressure in comparison to the control group.
3.6 Mortality
Only one study examined the association between nut intake and mortality. In their cohort study with a mean follow-up of 11 years, Wang et al. (21) analyzed data from 1,203 US adults with CKD to investigate the association between frequency of nut consumption (total nuts with no distinction of nut type) and cardiovascular and all-cause mortality. Overall, nut consumption was not associated with cardiovascular mortality, but consuming nuts 1–6 times/week was significantly associated with lower all-cause mortality rates (HR: 0.63, 95%CI: 0.47–0.86; p = 0.03; model adjusted for age, gender, ethnicity, glomerular filtration rate and urinary albumin-to-creatinine ratio, dietary intake of energy, carbohydrates, sugar, fats, phosphorus, sodium and potassium, alcohol consumption, smoking status, obesity, blood lipids, serum potassium and phosphorus, and health status [hypertension, diabetes, coronary heart disease, congestive heart failure, stroke, cancer], with no observed benefits seen for the consumption of more than once a day.
3.7 Adverse effects
Two studies evaluated serum phosphorus and potassium levels after walnut consumption in CKD patients (22, 23) and found no significant changes in these parameters, indicating that walnut intake is safe regarding these electrolytes balance.
4 Discussion
This systematic review examined the effects of nut consumption on oxidative stress, inflammatory biomarkers, and mortality in patients with CKD. Despite broad inclusion criteria that encompassed different study designs, only four studies met eligibility for inclusion. Collectively, these studies suggest a potential role for nuts in CKD management, with reported benefits on oxidative stress, inflammatory markers, and all-cause mortality. However, most studies were judged to have a high risk of bias, and considerable heterogeneity was observed, limiting the strength of the evidence and highlighting an important gap in the literature regarding the potential benefits of nuts for this population.
Nuts have an optimal fatty acid profile, with a high concentration of polyunsaturated and monounsaturated fatty acids. Additionally, nuts are a rich source of proteins, fibers, B-vitamins, minerals and polyphenols (5, 8, 25). Nuts have been incorporated into several healthy diets, such as the Mediterranean diet (26), the global planetary health diet (27) and several other plant-based diets (28). There is a growing body of evidence associating the consumption of these diets with lower rates of cancer, cardiovascular disease, obesity, and mortality (29–33). In CKD patients, however, despite a lack of robust RCTs, epidemiological studies suggest the same benefits of whole-food plant-based diets in cardiovascular health and CKD progression (34–36). Whole-food plant-based diets constitute a shift away from the previously accepted diet for CKD that is low in protein (0.55–0.60 g/kg/day for nondiabetics and 0.60–0.80 g/kg/day for those with diabetes), high in fruits and vegetables (with consideration of potassium and phosphorous content to avoid elevated levels of these electrolytes), and low in sodium (<2.3 g/day) (4). Thus, to restrict the intake of protein, phosphorus, and potassium in order to meet the dietary guidelines, CKD patients commonly eat a limited amount of healthy ingredients such as fruits, vegetables, and nuts. However, encouraged by the benefits of healthy diets observed in recent epidemiological studies, some recent studies have assessed the effects of nut consumption in CKD patients, which justifies the fact that the trials included in this review were all recently published. Our review identified two studies showing that walnut intake did not alter serum phosphorus or potassium concentrations (22, 23), suggesting that walnuts do not pose a risk of electrolyte imbalance in patients with advanced CKD receiving conservative treatment. However, further research is needed to determine whether similar effects occur with other types of nuts.
Inflammation and oxidative stress are non-traditional risk factors for CKD development and progression (3). They result from dysregulation caused by an imbalance between reactive oxygen and nitrogen species, and antioxidant systems, prompting the release of pro-inflammatory cytokines (3, 37). These processes are regulated by two transcriptional factors, NF-κβ and Nrf2, the former induced when oxidative stress is high and resulting in a pro-inflammatory state, and the latter is responsible for mitigating inflammation and oxidative stress (37). These risk factors are even more critical in patients with kidney injury. The kidneys are metabolically active organs, making them more vulnerable to damage caused by oxidative stress (38). Further, several uremic toxins are associated with increased oxidative stress in CKD (38). In addition, the increased production of proinflammatory cytokines and oxidative stress mediated by the activation of macrophages and monocytes constitutes the fundamental basis for initiating the inflammatory cascade, worsening renal function (39). The two trials evaluating nuts and their effects on oxidative stress and inflammation found that interventions with both Brazil nuts and baru almond oil reduced CRP, a marker of acute inflammatory response (22, 24). In addition, Brazil nut consumption was associated with reduced NF-κB expression and increased expression of NRF-2 and NQO1, alongside lower IL-6 concentrations, indicating a more favorable inflammatory profile (24). Brazil nuts also reduced MDA levels, a marker of oxidative stress, whereas baru almond oil showed no effect on MDA or on the antioxidant enzymes SOD and catalase. Given the differences in interventions and outcomes assessed, the heterogeneity between these two studies limits firm conclusions. Nevertheless, the findings suggest a potential benefit of nut consumption for oxidative stress and inflammation in CKD, warranting further investigation. In addition to the bioactive compounds found in all the different nut types, Brazil nuts are the richest food source of selenium, an essential micronutrient for humans and animals with a key role in thyroid function, immune response, and maintenance of cell redox balance through its presence in selenoproteins (40). Previous research has demonstrated a clear effect of Brazil nuts in enhancing the antioxidant status in different study populations, such as people with obesity, dyslipidemia, type 2 diabetes, as well as so-called healthy individuals (41).
The consumption of nuts has been associated with reduction of all-cause mortality in several studies, summarized in an umbrella review which identified that a daily consumption of 28 g of nuts was associated with 22% reduction in all-cause mortality in CKD-free cohorts (42). It appears that the protective effects of nuts on all-cause mortality is also observed in CKD patients as reported by Wang et al. (21). Nonetheless, we highlight that besides being the only study this far to investigate such association, it has several limitations such as a lack of information on the types and amounts of nuts consumed. Considering that CKD contributes to over 1.43 million deaths per year (1, 2), we highly encourage future studies to investigate the long-term effects of nuts on mortality in this population.
The limitations of this systematic review, which includes only four studies, highlights the need for additional research to better understand the potential benefits of adding nuts to the diet for improving the prognosis of patients with CKD. The studies included in this review used different nut types and had small sample sizes, which hinders generalization of findings across all nut types. Further, we acknowledge that all the four studies papers in this systematic review presented moderate-to-high risk of bias, compromising the quality of evidence provide. Even though we found that overall nut consumption seems to be safe for patients with CKD in terms of electrolytes balance, we acknowledge that further studies investigating the different nut types with larger sample sizes are necessary for the translation of evidence into clinical practice on the management of CKD patients.
5 Conclusion
Although the small trials included in this systematic review suggest that nuts might have the potential to mitigate non-traditional risk factors for CKD progression and thus improve the prognosis of people with this chronic condition, lack of high-quality trials involving nut intake as a strategy for CKD management hinders clear evidence. Thus, we highlight the necessity for more trials using nuts in CKD treatment in order to translate the findings into clinical practice.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author/s.
Author contributions
TL: Conceptualization, Formal analysis, Investigation, Methodology, Writing – original draft. RS: Conceptualization, Formal analysis, Investigation, Methodology, Writing – original draft. PA: Formal analysis, Writing – review & editing. BC: Conceptualization, Formal analysis, Methodology, Project administration, Writing – review & editing. MM: Conceptualization, Formal analysis, Investigation, Methodology, Project administration, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by Coordination for the Improvement of Higher Education Personnel – Brazil (CAPES) – Finance Code 001 through Sao Paulo State University, UNESP in collaboration with CAPES (CAPES-PRINT), and by FAPESP [2022/15993-4].
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2025.1659516/full#supplementary-material
Abbreviations
CAT, Catalase; CKD, Chronic kidney disease; CRP, C-reactive protein; MDA, Malondialdehyde; NF-Kb, Nuclear factor kappa B; NQO1, NAD(P)H quinone oxidoreductase 1; Nrf-2, Nuclear factor E2-related factor 2; SOD, Superoxide dismutase.
References
1. Kidney disease: improving global outcomes (KDIGO) CKD work group. KDIGO 2024 clinical practice guideline for the evaluation and Management of Chronic Kidney Disease. Kidney Int. (2024) 105:S117–314. doi: 10.1016/j.kint.2023.10.018
2. Cockwell, P, and Fisher, LA. The global burden of chronic kidney disease. Lancet. (2020) 395:662–4. doi: 10.1016/S0140-6736(19)32977-0
3. Altamura, S, Pietropaoli, D, Lombardi, F, Del Pinto, R, and Ferri, C. An overview of chronic kidney disease pathophysiology: the impact of gut dysbiosis and oral disease. Biomedicine. (2023) 11:3033. doi: 10.3390/biomedicines11113033
4. Ikizler, TA, Burrowes, JD, Byham-Gray, LD, Campbell, KL, Carrero, JJ, Chan, W, et al. KDOQI clinical practice guideline for nutrition in CKD: 2020 update. Am J Kidney Dis. (2020) 76:S1–S107. doi: 10.1053/j.ajkd.2020.05.006
5. Gonçalves, B, Pinto, T, Aires, A, Morais, MC, Bacelar, E, Anjos, R, et al. Composition of nuts and their potential health benefits – an overview. Foods. (2023) 12:942. doi: 10.3390/foods12050942
6. de Souza, RGM, Schincaglia, RM, Pimentel, GD, and Mota, JF. Nuts and human health outcomes: a systematic review. Nutrients. (2017) 9:1311. doi: 10.3390/nu9121311
7. Kornsteiner, M, Wagner, K-H, and Elmadfa, I. Tocopherols and total phenolics in 10 different nut types. Food Chem. (2006) 98:381–7. doi: 10.1016/j.foodchem.2005.07.033
8. Bolling, BW, Chen, CY, McKay, DL, and Blumberg, JB. Tree nut phytochemicals: composition, antioxidant capacity, bioactivity, impact factors: a systematic review of almonds, Brazils, cashews, hazelnuts, macadamias, pecans, pine nuts, pistachios and walnuts. Nutr Res Rev. (2011) 24:244–75. doi: 10.1017/S095442241100014X
9. Ros, E, Tapsell, LC, and Sabate, J. Nuts and berries for heart health. Curr Atheroscler Rep. (2010) 12:397–406. doi: 10.1007/s11883-010-0132-5
10. Guasch-Ferré, M, Liu, X, Malik, VS, Sun, Q, Willett, WC, Manson, JE, et al. Nut consumption and risk of cardiovascular disease. J Am Coll Cardiol. (2017) 70:2519–32. doi: 10.1016/j.jacc.2017.09.035
11. Becerra-Tomás, N, Paz-Graniel, I, WC Kendall, C, Kahleova, H, Rahelić, D, Sievenpiper, JL, et al. Nut consumption and incidence of cardiovascular diseases and cardiovascular disease mortality: a meta-analysis of prospective cohort studies. Nutr Rev. (2019) 77:691–709. doi: 10.1093/nutrit/nuz042
12. Aune, D, Keum, N, Giovannucci, E, Fadnes, LT, Boffetta, P, Greenwood, DC, et al. Nut consumption and risk of cardiovascular disease, total cancer, all-cause and cause-specific mortality: a systematic review and dose-response meta-analysis of prospective studies. BMC Med. (2016) 14:207. doi: 10.1186/s12916-016-0730-3
13. Ma, Y, Njike, VY, Millet, J, Dutta, S, Doughty, K, Treu, JA, et al. Effects of walnut consumption on endothelial function in type 2 diabetic subjects: a randomized controlled crossover trial. Diabetes Care. (2010) 33:227–32. doi: 10.2337/dc09-1156
14. Cardoso, BR, Tan, SY, Daly, RM, Via, JD, Georgousopoulou, EM, and George, ES. Intake of nuts and seeds is associated with lower prevalence of nonalcoholic fatty liver disease in US adults: findings from 2005-2008 NHANES. J Nutr. (2021) 151:3507–15. doi: 10.1093/jn/nxab253
15. Stockler-Pinto, MB, Mafra, D, Moraes, C, Lobo, J, Boaventura, GT, Farage, NE, et al. Brazil nut (Bertholletia excelsa, H.B.K.) improves oxidative stress and inflammation biomarkers in hemodialysis patients. Biol Trace Elem Res. (2014) 158:105–12. doi: 10.1007/s12011-014-9904-z
16. Schiffrin, EL, Lipman, ML, and Mann, JF. Chronic kidney disease: effects on the cardiovascular system. Circulation. (2007) 116:85–97. doi: 10.1161/CIRCULATIONAHA.106.678342
17. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: and updated guideline for reporting systematic reviews. BMJ. (2021) 372:71. doi: 10.1136/bmj.n71
18. Ouzzani, M, Hammady, H, Fedorowicz, Z, and Elmagarmid, A. Rayyan—a web and mobile app for systematic reviews. Syst Rev. (2016) 5:210. doi: 10.1186/s13643-016-0384-4
19. Sterne, JAC, Savović, J, Page, MJ, Elbers, RG, Blencowe, NS, Boutron, I, et al. RoB 2: a revised tool for assessing risk of bias in editerran trials. BMJ. (2019) 366:nl4898. doi: 10.1136/bmj.l4898
20. Sterne, JA, Hernán, MA, Reeves, BC, Savović, J, Berkman, ND, Viswanathan, M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. (2016) 355:i4919. doi: 10.1136/bmj.i4919
21. Wang, K, Qian, D, Hu, Y, Cheng, Y, Ge, S, and Yao, Y. Nut consumption and effects on chronic kidney disease and mortality in the United States. Am J Nephrol. (2022) 53:503–12. doi: 10.1159/000524382
22. Schincaglia, RM, Cuppari, L, Neri, HFS, Cintra, DE, Sant’Ana, MR, and Mota, JF. Effects of baru almond oil (Dipteryx alata Vog.) supplementation on body composition, inflammation, oxidative stress, lipid profile, and plasma fatty acids of hemodialysis patients: a randomized, double-blind, placebo-controlled clinical trial. Complement Ther Med. (2020) 52:102479. doi: 10.1016/j.ctim.2020.102479
23. Sanchis, P, Molina, M, Berga, F, Muñoz, E, Fortuny, R, Costa-Bauzá, A, et al. A pilot randomized crossover trial assessing the safety and short-term effects of walnut consumption by patients with chronic kidney disease. Nutrients. (2020) 12:63. doi: 10.3390/nu12010063
24. Cardozo, LFMF, Stockler-Pinto, M, and Mafra, D. Brazil nut consumption modulates Nrf2 expression in hemodialysis patients: a pilot study. Mol Nutr Food Res. (2016) 60:1719–24. doi: 10.1002/mnfr.201500658
25. Farazi, M, Houghton, MJ, Nicolotti, L, Murray, M, Cardoso, BR, and Williamson, G. Inhibition of human starch digesting enzymes and intestinal glucose transport by walnut polyphenols. Food Res Int. (2024) 189:114572. doi: 10.1016/j.foodres.2024.114572
26. Davis, C, Bryan, J, Hodgson, J, and Murphy, K. Definition of the mediterranean diet; a literature review. Nutrients. (2015) 7:9139–53. doi: 10.3390/nu7115459
27. Willett, W, Rockstrom, J, Loken, B, Springmann, M, Lang, T, Vermeulen, S, et al. Food in the Anthropocene: the EAT-lancet commission on healthy diets from sustainable food system. Lancet. (2019) 393:447–92. doi: 10.1016/S0140-6736(20)31828-6
28. Marchese, LE, McNaughton, SA, Hendrie, GA, Wingrove, K, Dickinson, KM, and Livingstone, KM. A scoping review of approaches used to develop plant-based diet quality indices. Curr Dev Nutr. (2023) 7:100061. doi: 10.1016/j.cdnut.2023.100061
29. Baden, MY, Liu, G, Satija, A, Li, Y, Sun, Q, Fung, TT, et al. Changes in plant-based diet quality and total and cause-specific mortality. Circulation. (2019) 140:979–91. doi: 10.1161/CIRCULATIONAHA.119.041014
30. Hemler, EC, and Hu, FB. Plant-based diets for cardiovascular disease prevention: all plant foods are not created equal. Curr Atherosclerosis Rep. (2019) 21:1–8. doi: 10.1007/s11883-019-0779-5
31. Pant, A, Gribbin, S, McIntyre, D, Trivedi, R, Marschner, S, and Laranjo, L. Primary prevention of cardiovascular disease in women with a Mediterranean diet: systematic review and meta-analysis. Heart. (2023) 109:1208–15. doi: 10.1136/heartjnl-2022-321930
32. Bui, LP, Pham, TT, Wang, F, Chai, B, Sun, Q, Hu, FB, et al. Planetary health diet index and risk of total and cause-specific mortality in three prospective cohorts. Am J Clin Nutr. (2024) 120:80–91. doi: 10.1016/j.ajcnut.2024.03.019
33. Maroto-Rodriguez, J, Delgado-Velandia, M, Ortolá, R, Perez-Cornago, A, Kales, SN, Rodríguez-Artalejo, F, et al. Association of a Mediterranean lifestyle with all-cause and cause-specific mortality: a prospective study from the UK biobank. Mayo Clin Proc. (2024) 99:551–63. doi: 10.1016/j.mayocp.2023.05.031
34. Kim, H, Caulfield, LE, Garcia-Larsen, V, Steffen, LM, Grams, ME, Coresh, J, et al. Plant-based diets and incident CKD and kidney function. Clin J Am Soc Nephrol. (2019) 14:682–91. doi: 10.2215/CJN.12391018
35. Chen, X, Wei, G, Jalili, T, Metos, J, Giri, A, Cho, ME, et al. The associations of plant protein intake with all-cause mortality in CKD. Am J Kidney Dis. (2016) 67:423–30. doi: 10.1053/j.ajkd.2015.10.018
36. Oosterwijk, MM, Soedamah-Muthu, SS, Geleijnse, JM, Bakker, SJL, Navis, G, Binnenmars, SH, et al. High dietary intake of vegetable protein is associated with lower prevalence of renal function impairment: results of the Dutch DIALECT-1 cohort. Kidney Int Rep. (2019) 4:710–9. doi: 10.1016/j.ekir.2019.02.009
37. Rajaram, S, Damasceno, NRT, Braga, RAM, Martinez, R, Kris-Etherton, P, and Sala-Vila, A. Effects of nuts on markers of inflammation and oxidative stress: a narrative review. Nutrients. (2023) 15:1099. doi: 10.3390/nu15051099
38. Frąk, W, Kućmierz, J, Szlagor, M, Młynarska, E, Rysz, J, and Franczyk, B. New insights into molecular mechanisms of chronic kidney disease. Biomedicine. (2022) 10:2846. doi: 10.3390/biomedicines10112846
39. Graterol Torres, F, Molina, M, Soler-Majoral, J, Romero-González, G, Rodríguez Chitiva, N, Troya-Saborido, M, et al. Evolving concepts on inflammatory biomarkers and malnutrition in chronic kidney disease. Nutrients. (2022) 14:4297. doi: 10.3390/nu14204297
40. Cardoso, BR, Duarte, GBS, Reis, BZ, and Cozzolino, SMF. Brazil nuts: nutritional composition, health benefits and safety aspects. Food Res Int. (2017) 100:9–18. doi: 10.1016/j.foodres.2017.08.036
41. Silva, A, Silveira, BKS, Freitas, BVM, Hermsdorff, HHM, and Bressan, J. Effects of regular Brazil nut (Bertholletia excelsa H.B.K.) consumption on health: a systematic review of clinical trials. Foods. (2022) 11:2925. doi: 10.3390/foods11182925
Keywords: nuts, chronic kidney disease, nutrition, inflammation, oxidative stress, blood pressure, mortality
Citation: Lazzarin T, Ballarin RS, Azevedo PS, Cardoso BR and Minicucci MF (2025) Nut consumption in chronic kidney disease: a systematic review. Front. Nutr. 12:1659516. doi: 10.3389/fnut.2025.1659516
Edited by:
Johannes le Coutre, University of New South Wales, AustraliaReviewed by:
Mahdi Vajdi, Isfahan University of Medical Sciences, IranAnjali Srivastava, Indian Council of Medical Research (ICMR), India
Copyright © 2025 Lazzarin, Ballarin, Azevedo, Cardoso and Minicucci. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Barbara R. Cardoso, YmFyYmFyYS5jYXJkb3NvQG1vbmFzaC5lZHU= Taline Lazzarin, dGFsaW5lLmxhenphcmluQHVuZXNwLmJy
†These authors have contributed equally to this work and share senior authorship