 Chao Ma
Chao Ma Bing Yan
Bing Yan Yongsheng Jiang
Yongsheng Jiang- Department of Gastrointestinal Surgery, Central Hospital Affiliated to Shandong First Medical University, Jinan Central Hospital, Jinan, China
Background: This study, based on the Global Burden of Disease (GBD) 2021 database, investigates the global and regional burden of gastric cancer attributable to diet high in sodium (GC-DHIS) from 1990 to 2021 and projects trends through 2045, with the aim of providing evidence to inform public health policymaking.
Methods: Data were obtained from GBD 2021, covering 204 countries and territories. Disability-adjusted life years (DALYs) were used as the primary metric. The Das Gupta method was applied to decompose the drivers of changes in disease burden, and the Nordpred model was used to forecast future trends.
Results: Between 1990 and 2021, the global number of DALYs attributable to GC-DHIS decreased by 2%, while deaths increased by 12%. The largest absolute number of DALYs was observed in middle SDI regions, whereas the most rapid growth occurred in low-middle SDI regions. Health inequality analysis revealed that the burden of GC-DHIS was disproportionately concentrated in regions with higher levels of social development. Projections from 2022 to 2045 suggest a significant increase in DALYs and deaths, with a faster rise among males. However, age-standardized DALY rates (ASDR) and age-standardized mortality rates (ASMR) are expected to decline substantially.
Conclusion: Despite the global decline in ASDR and ASMR of GC-DHIS, the absolute burden is expected to rise in specific regions and populations, highlighting the need for targeted prevention and control strategies.
Introduction
Gastric cancer (GC) is one of the most common malignant tumors worldwide, characterized by high incidence and mortality rates (1, 2). Globally, it ranks as the fifth most prevalent cancer, with particularly high incidence in East Asia (3). The pathogenesis of GC is multifactorial. Helicobacter pylori infection is a major etiological factor and is strongly associated with precancerous conditions such as chronic atrophic gastritis, intestinal metaplasia, and dysplasia (4). In addition, dietary factors—including excessive salt intake, frequent consumption of pickled foods, and insufficient intake of fresh fruits and vegetables—are closely linked to an increased risk of GC (5, 6).
Substantial evidence indicates that a high-sodium diet significantly elevates GC risk (7, 8). Excess salt can directly damage the gastric mucosa, stimulate cellular proliferation, and induce endogenous mutations (9). Furthermore, nitrates and nitrites present in high-salt foods may generate carcinogenic N-nitroso compounds. High sodium intake can also intensify H. pylori infection by enhancing its carcinogenic potential, thereby promoting chronic inflammation and the progression of precancerous lesions (10, 11). Epidemiological studies have shown that a high-salt diet increases the risk of GC by 55%, and excessive sodium intake is estimated to account for approximately 16.6% of GC cases worldwide (12).
To provide a more comprehensive understanding of gastric cancer attributable to a diet high in sodium (GC-DHIS), we conducted a systematic analysis based on the Global Burden of Disease 2021 (GBD 2021) database. This study examines the global, regional, and national epidemiological trends of GC-DHIS. By precisely analyzing the dynamic changes in disease burden over time, we were able to identify regions with the most significant increases during specific periods, thereby offering strong and targeted evidence to support the development of cancer prevention and control strategies. In addition, we explore cross-national health inequalities and apply the Nordpred model to project GC-DHIS trends from 2022 to 2045. The findings of this study are expected to provide essential evidence for public health policymaking and serve as an important reference for global GC prevention efforts.
Methods
Data sources and disease definition
All data in this study were obtained from the GBD 2021 database. Led by the Institute for Health Metrics and Evaluation (IHME) at the University of Washington, GBD 2021 provides estimates for 204 countries and territories, 811 subnational locations, 371 diseases and injuries, and 88 risk factors from 1990 to 2021 (13–15). The GBD employs a unified modeling framework and standardized methodologies to integrate diverse data sources—including vital registration systems, hospital records, population-based surveys, cohort studies, and systematic reviews—ensuring comparability across regions and over time (16, 17). This study focused on GC (ICD-10 code: C16), which encompasses gastric adenocarcinoma, gastric sarcoma, and other malignant tumors of the stomach (18). All disease definitions and classifications followed GBD standards.
Disability-adjusted life years
Disability-Adjusted Life Years (DALYs) were used as the primary metric to quantify the overall burden of GC. DALYs are calculated as the sum of Years of Life Lost (YLLs) due to premature mortality and Years Lived with Disability (YLDs) (19). YLLs are derived by multiplying the number of deaths by the standard life expectancy at the age of death. YLDs are estimated based on the number of prevalent cases, corresponding disability weights, and average disease duration.
Decomposition analysis
To identify the main drivers of change in the GC burden, we applied the Das Gupta standardization decomposition method. This approach attributes variations in DALYs and deaths to three independent components: population growth, population aging, and epidemiological changes (20). By controlling variables and simulating the contribution of each factor separately, this method allows clear differentiation of the underlying drivers of increasing or decreasing disease burden.
Cross-country inequality analysis
In terms of health inequality analysis, this study introduced two methods—Slope Index of Inequality (SII) and Concentration Index (CI)—to assess disparities in health burden across countries (20, 21). The SII quantifies the absolute difference in health outcomes between the highest and lowest SDI countries using regression modeling. The CI, based on the Lorenz curve, measures the relative distribution of disease burden across countries with different SDI levels. A CI greater than 0 indicates that the burden is concentrated in high-SDI countries, whereas a CI less than 0 suggests concentration in low-SDI countries.
Prediction analysis
To forecast future trends in GC burden, we used the Nordpred model, which provides medium- and long-term projections (22). Based on an Age–Period–Cohort (APC) regression framework, the model simultaneously accounts for age structure, period effects, and cohort effects, allowing robust prediction of DALY and mortality trends.
Results
Global and regional burden of GC-DHIS
In 2021, the global number of DALYs due to GC-DHIS was 1,804,592, compared to 1,845,617 in 1990, representing a percentage change of −2%. The Middle SDI regions had the highest number of DALYs (712,581.6), with a percentage change of 7%, while the Low-middle SDI regions experienced the fastest increase, with a percentage change of 56%. Globally, the age-standardized DALY rate (ASDR) was 20.78 per 100,000 population, with an estimated annual percentage change (EAPC) of −2.56 (95% CI, −2.64 to −2.47). The High-middle SDI regions had the highest ASDR at 28.14 per 100,000, with an EAPC of −2.76 (95% CI, −2.90 to −2.63). Among the 21 GBD regions, Oceania had the fastest increase in DALYs, with a percentage change of 101%, while East Asia had the highest ASDR (41.09 per 100,000, EAPC, −2.88; 95% CI: −3.06 to −2.70) (Figure 1 and Table 1).
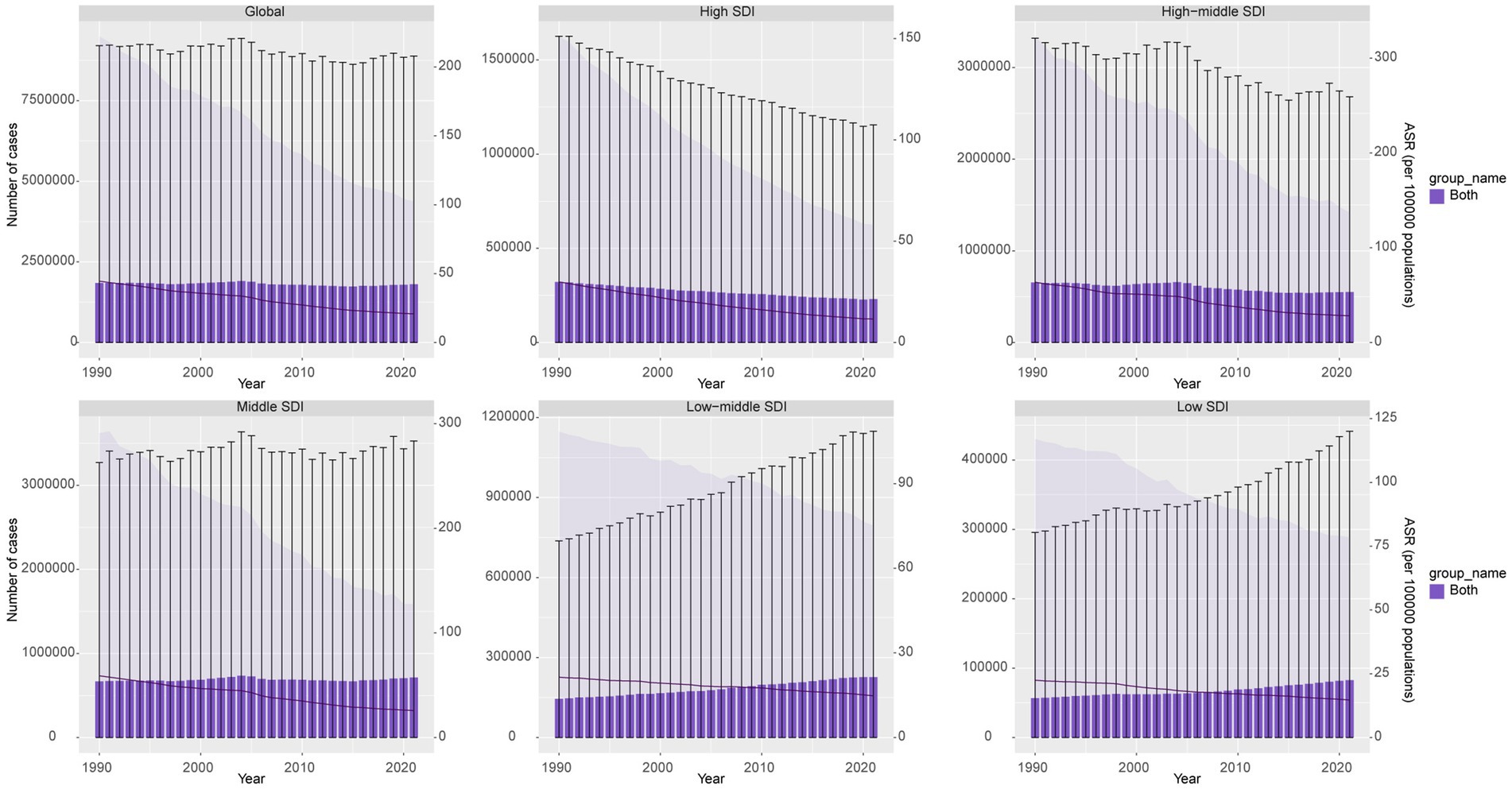
Figure 1. DALYs cases and ASDR of GC-DHIS from 1990 to 2021.
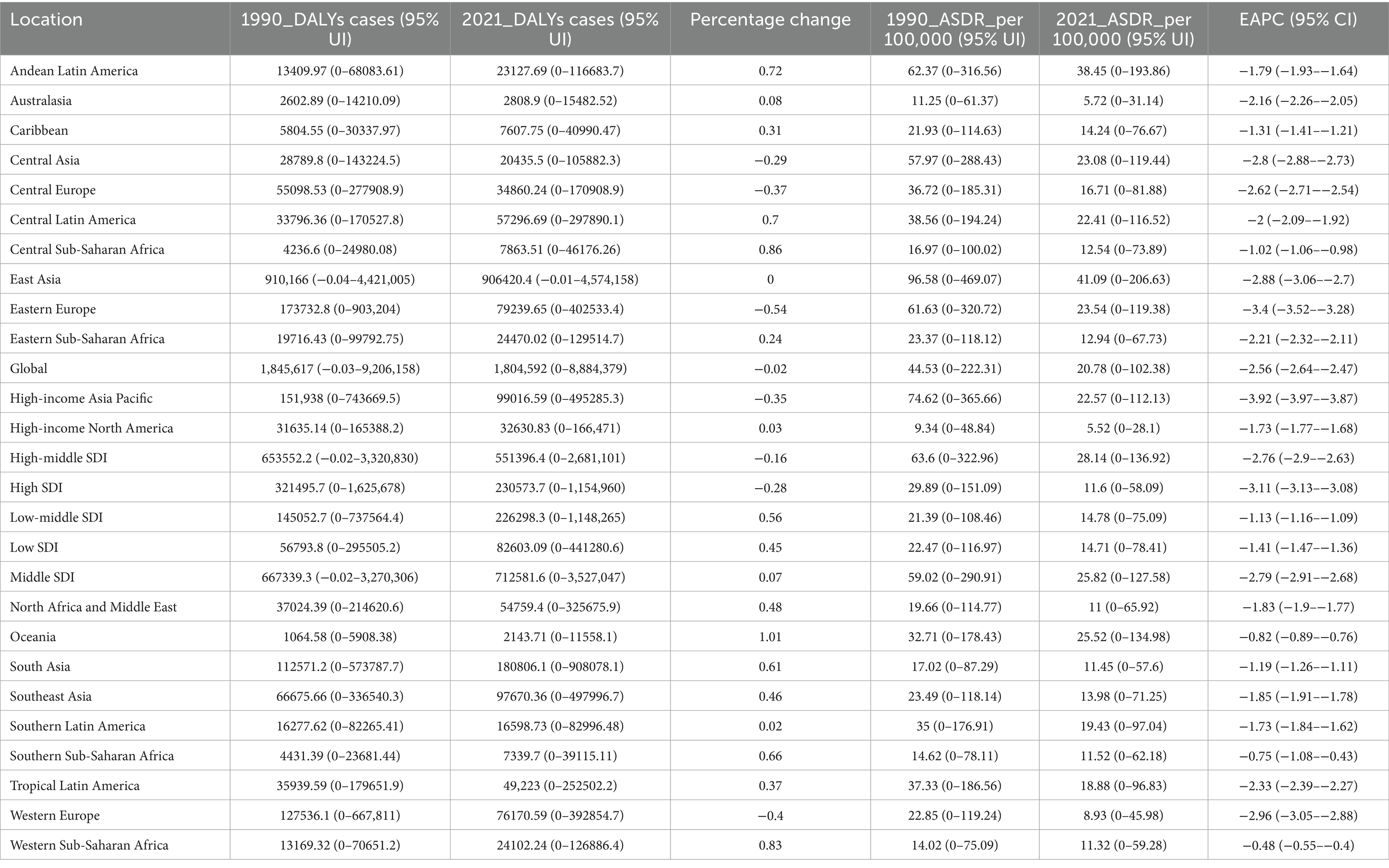
Table 1. Disability-adjusted life years (DALYs) and age-standardized DALY rate (ASDR) of GC-DHIS in 1990 and 2021, and the PC and EAPC from 1990 to 2021.
In 2021, the global number of deaths due to GC-DHIS was 75,661.15, up from 67,844.54 in 1990, representing a 12% increase. The Middle SDI regions had the highest number of deaths (28,816.28), with a percentage change of 24%, while the Low-middle SDI regions showed the fastest increase, with a percentage change of 69%. Additionally, the global age-standardized mortality rate (ASMR) for GC-DHIS was 0.89 per 100,000 population, with an EAPC of −2.26 (95% CI: −2.35 to −2.18). The High-middle SDI regions recorded the highest ASMR at 1.18 per 100,000, with an EAPC of −2.43 (95% CI: −2.56 to −2.31). Among the 21 GBD regions, Oceania showed the fastest increase in death cases, with a percentage change of 101%. East Asia had the highest ASMR, at 1.76 per 100,000, with an EAPC of −2.54 (95% CI: −2.74 to −2.34) (Supplementary Figure 1 and Table 2).

Table 2. Deaths and age-standardized mortality rate (ASMR) of GC-DHIS in 1990 and 2021, and the PC and EAPC from 1990 to 2021.
National burden of GC-DHIS
Over the past 32 years, approximately 65% of countries showed an increasing trend in GC-DHIS-related DALYs. The fastest-growing countries in DALYs were Djibouti (234%), United Arab Emirates (231%), and Honduras (206%). Approximately 70% of countries also experienced an increase in death cases, with the fastest increases observed in Djibouti (254%), Honduras (248%), and United Arab Emirates (231%) (Figure 2A).
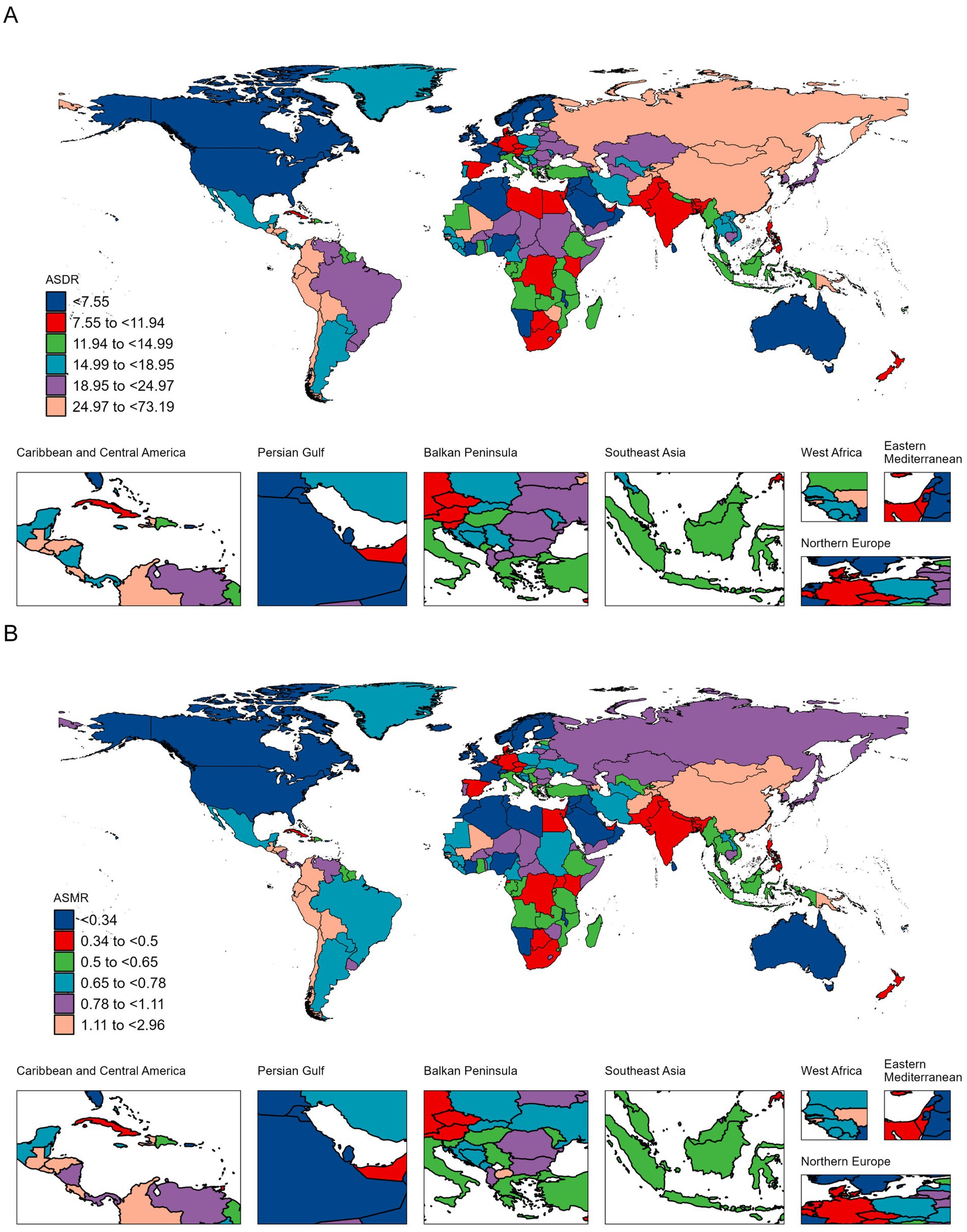
Figure 2. ASDR (A) and ASMR (B) of GC-DHIS per 100,000 population in 2021, by country.
The countries with the highest ASDR were Mongolia (73.19 per 100,000), Bolivia (56.47 per 100,000), and the Democratic People’s Republic of Korea (48.47 per 100,000). The highest ASMR were observed in Mongolia (2.96 per 100,000), Bolivia (2.58 per 100,000), and Guatemala (1.98 per 100,000). In terms of trends, the fastest increases in ASDR were recorded in Egypt, Lesotho, and Zimbabwe, with EAPCs of 2.07 (95% CI: 1.52–2.63), 1.76 (95% CI: 1.29–2.24), and 1.38 (95% CI: 0.81–1.95), respectively. The fastest increases in ASMR were also seen in Egypt, Lesotho, and Zimbabwe, with EAPCs of 2.49 (95% CI: 1.88–3.10), 1.49 (95% CI: 1.07–1.92), and 1.11 (95% CI: 0.62–1.59), respectively (Figure 2B and Supplementary Tables 1, 2).
Age and sex differences in the burden of GC-DHIS
In 2021, the highest DALYs cases for both sexes occurred in the 65–69 age group, with 190,995 cases for males and 79,182 for females. The highest number of deaths occurred in the 70–74 age group, with 8,159 male and 3,589 female deaths. The highest ASDR among females was observed in the 95 + age group (116 per 100,000), while for males it was in the 85–89 age group (191 per 100,000). The highest ASMR for females was in the 95 + age group (14.3 per 100,000), and for males in the 90–94 age group (21.3 per 100,000) (Figures 3A,B).
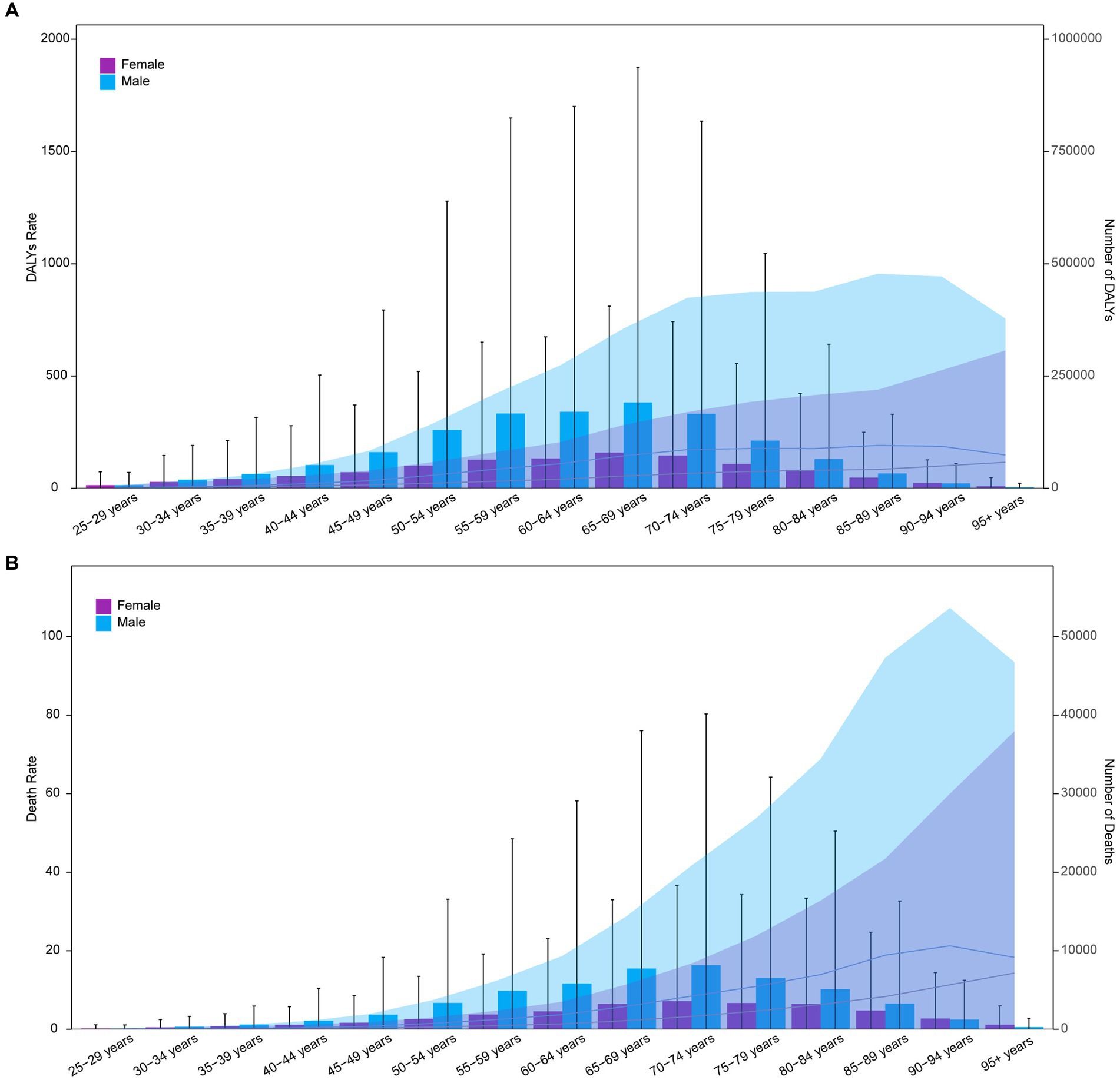
Figure 3. Age-specific numbers and rates of DALYs (A) and deaths (B) of GC-DHIS by age and sex in 2021.
Relationship between the burden of GC-DHIS and SDI
In 2021, ASDR and ASMR for GC-DHIS showed a positive correlation with SDI (Figure 4 and Supplementary Figure 2). As SDI increased, ASDR and ASMR exhibited a W-shaped pattern. Notably, when the SDI exceeded 0.7, ASDR and ASMR showed a marked decline. Some regions—such as High-income Asia Pacific, Eastern Europe, and East Asia—had a higher disease burden than expected, while others—such as Australasia, Western Europe, and Southern Sub-Saharan Africa—had a lower-than-expected burden.
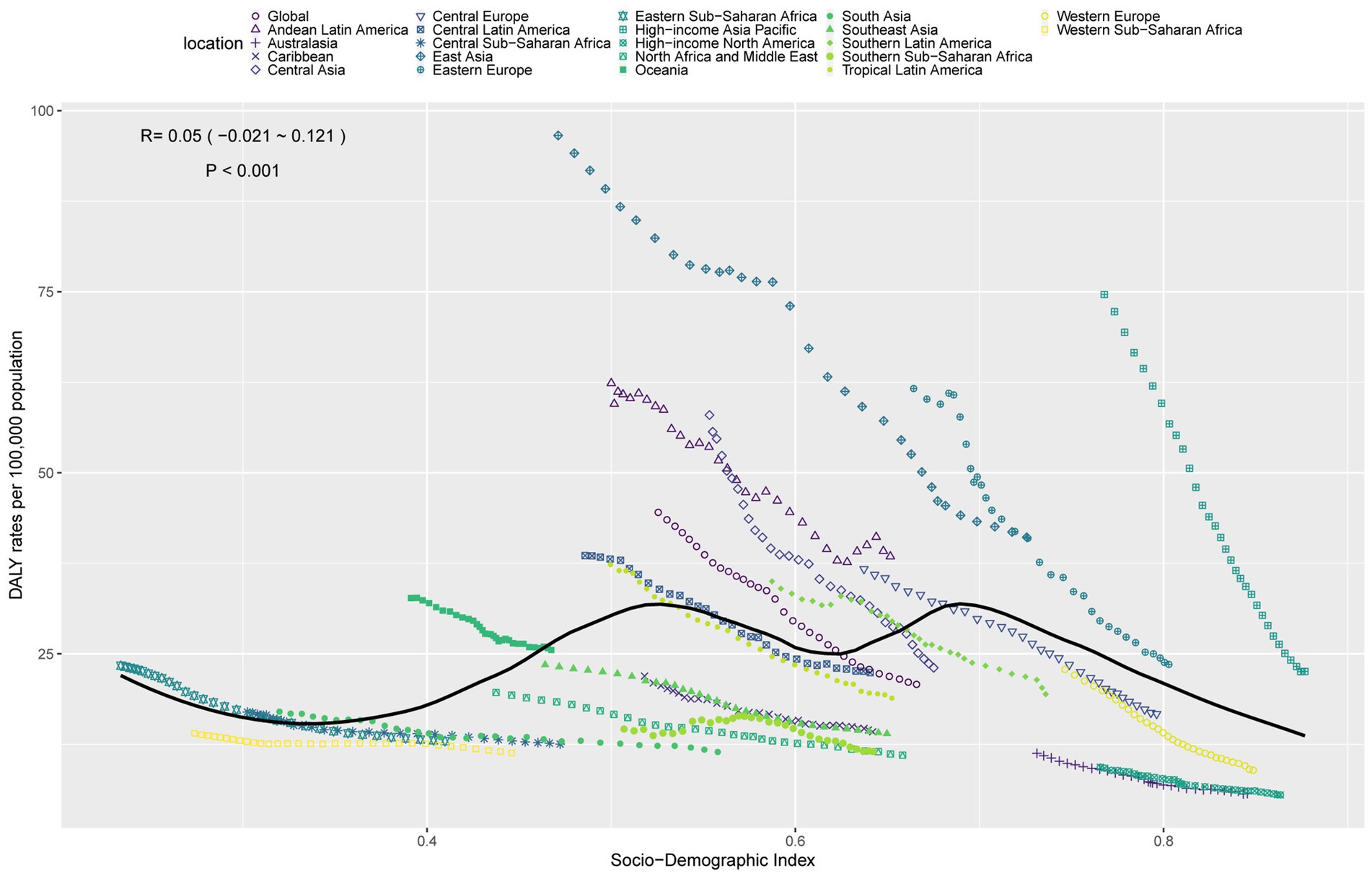
Figure 4. ASDR of GC-DHIS in 21 GBD regions by SDI, 1990–2021.
Decomposition analysis of the burden of GC-DHIS
Over the past 32 years, global GC-DHIS-related DALYs decreased by 41,025.28. Of this change, aging contributed 316,903.01 (−772.46%), population growth contributed 1,163,570.06 (−2,836.23%), and epidemiological change contributed −1,521,498.36 (3,708.69%). Among males, DALYs increased by 10,231.96, with aging contributing 238,400.95 (2,329.96%), population growth contributing 771,902.63 (7,544.03%), and epidemiological change contributing −1,000,071.62 (−9,774%). Among females, DALYs decreased by 51,257.24, with aging contributing 93,628.57 (−182.66%), population growth 391,667.43 contributing (−764.05%), and epidemiological change contributing −533,576.56 (1,040.98%) (Figure 5A).
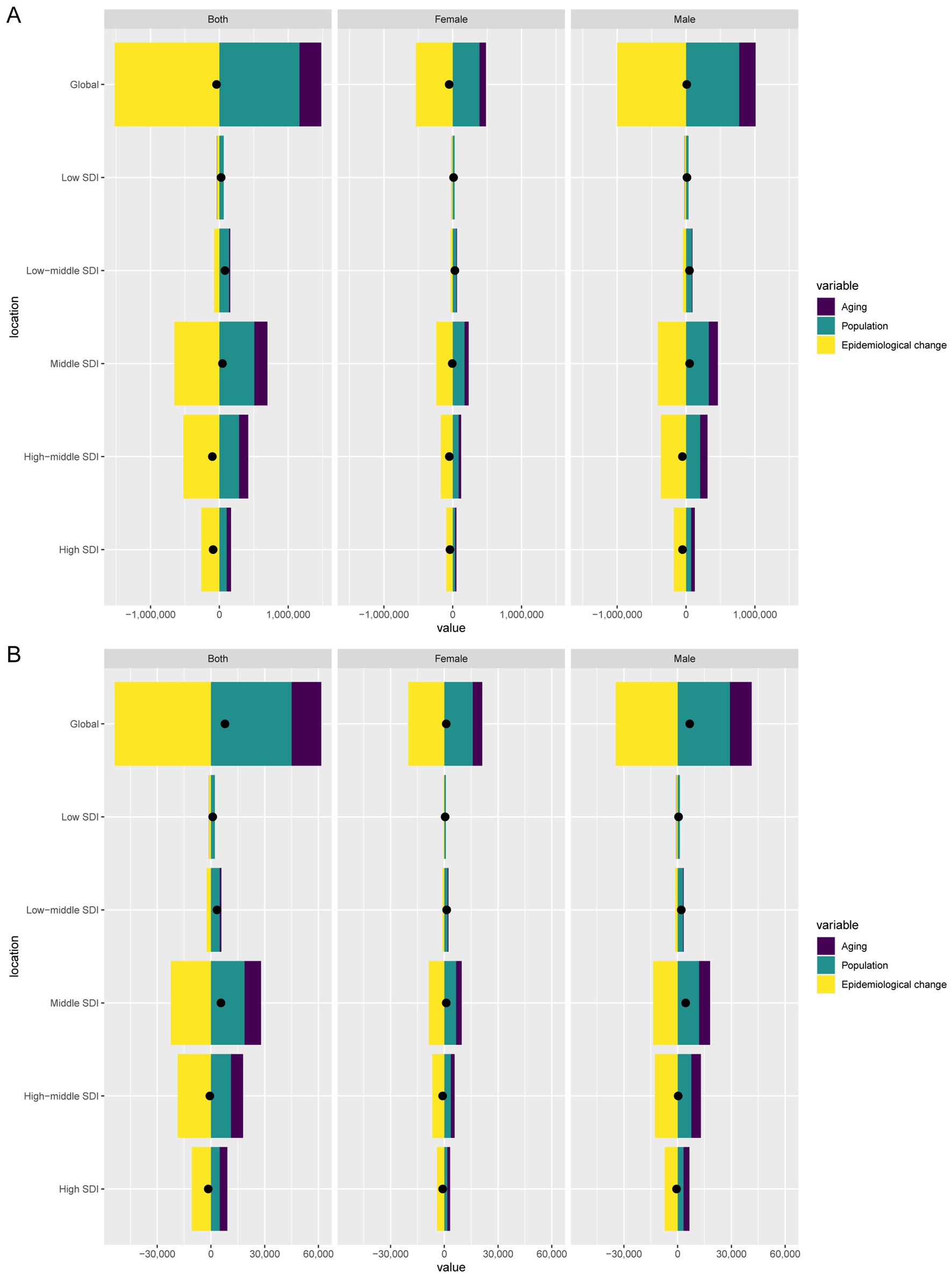
Figure 5. Decomposition analysis of changes in DALYs (A) and deaths (B) of GC-DHIS between 1990 and 2021 across SDI regions.
Globally, GC-DHIS-related deaths increased by 7,816.61, with aging contributing 16,534.17 (211.53%), population growth contributing 45,023.99 (576%), and epidemiological change contributing −53,741.54 (−687.53%). Among males, deaths increased by 6,731.52, with aging contributing 12,191.44 (181.11%), population growth contributing 29,129.89 (432.74%), and epidemiological change contributing −34,589.82 (−513.85%). Among females, deaths increased by 1,085.09, with aging contributing 5,358.93 (493.87%), population growth contributing 15,821.85 (1,458.11%), and epidemiological change contributing −20,095.69 (−1,851.98%) (Figure 5B).
Cross-country inequality in the burden of GC-DHIS
The SII for DALYs rates declined from 20 in 1990 to 11 in 2021, and the CI for DALYs rates dropped from 0.97 to 0.65 over the same period, indicating a narrowing of absolute inequalities between the highest and lowest SDI countries. However, the CI for DALYs rates increased from 0.22 in 1990 to 0.32 in 2021, and for death rates from 0.26 to 0.36, suggesting that the burden has become increasingly concentrated in higher-SDI regions (Figures 6A–D).
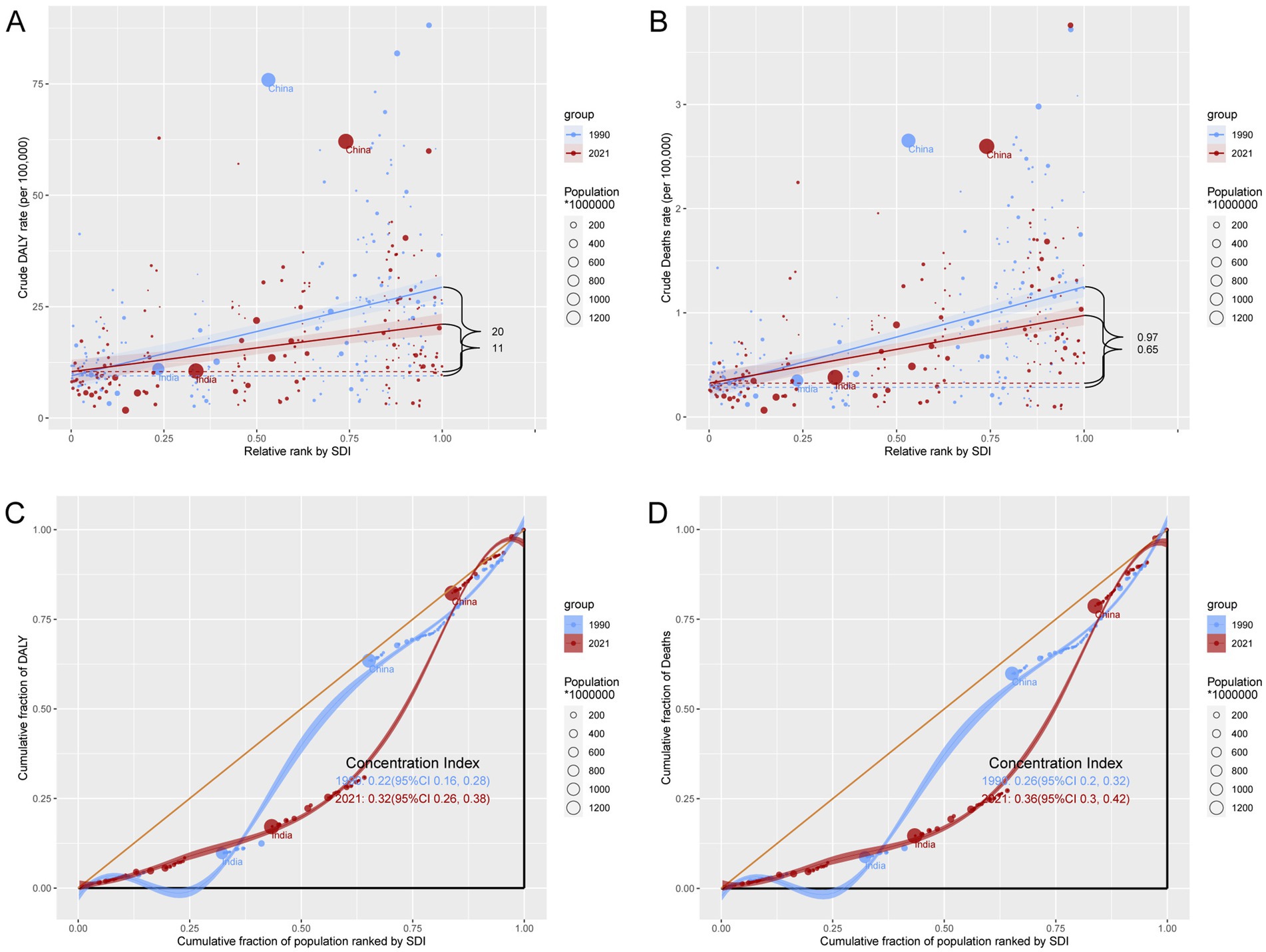
Figure 6. Inequality analysis of DALYs and mortality in GC-DHIS in 1990 and 2021 across the world. (A) Health inequality regression curves for DALYs. (B) Health inequality regression curves for mortality. (C) Concentration curves for DALYs. (D) Concentration curves for mortality.
Forecasted burden of GC-DHIS
Forecast analysis indicates a significant upward trend in DALYs and death cases from 2022 to 2045, with male cases consistently higher than female cases (Figures 7A,B). By 2045, the number of DALYs cases is projected to reach 1,447,797 for males and 730,873 for females. The number of death cases is expected to reach 67,686 for males and 37,828 for females. In contrast, the ASDR and ASMR are projected to decline significantly over time. By 2045, the ASDR is expected to be 21.92 per 100,000 for males and 9.95 per 100,000 for females. The ASMR is projected to be 0.96 per 100,000 for males and 0.44 per 100,000 for females.
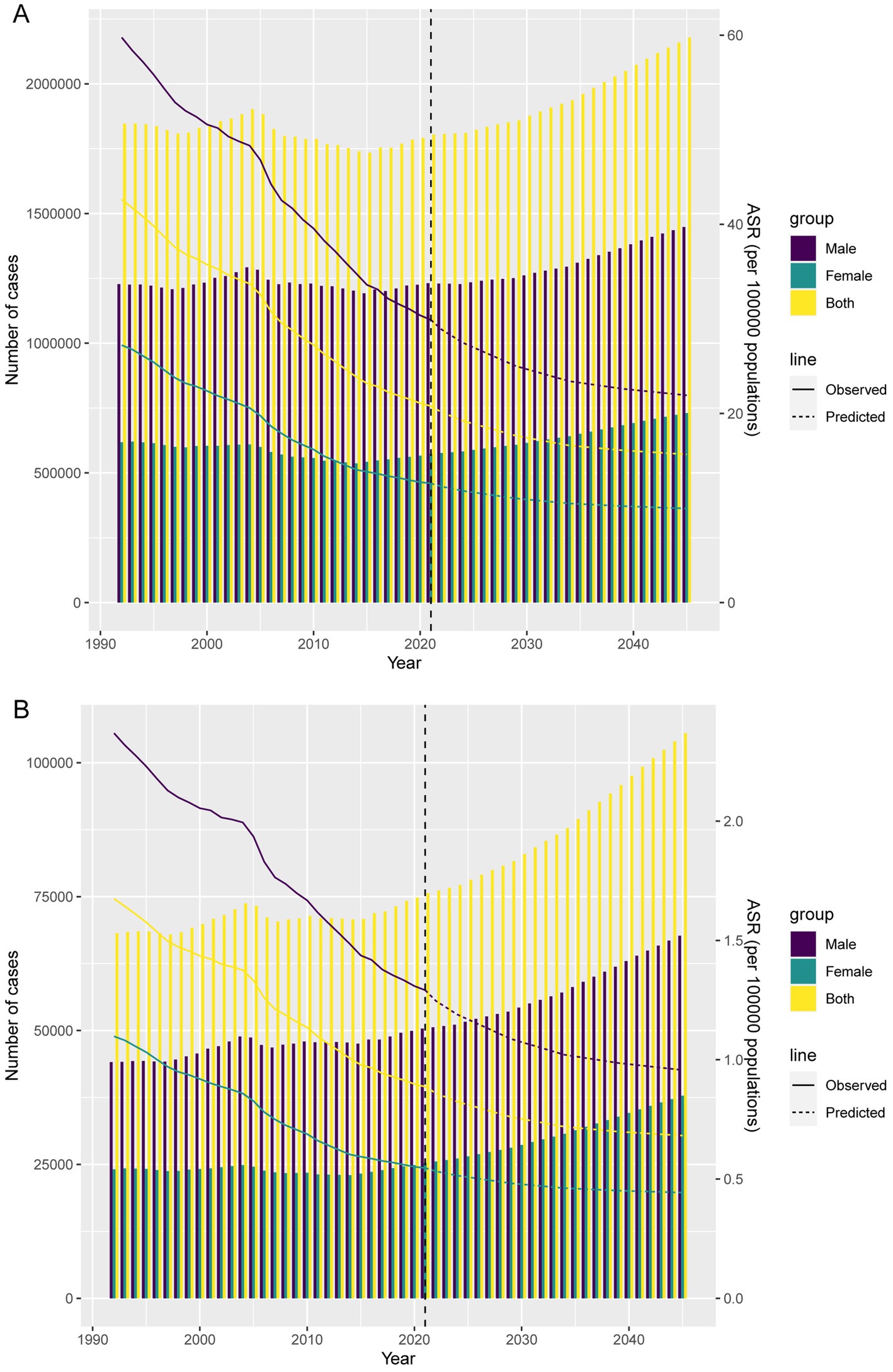
Figure 7. Projections of the temporal trends of the number of DALYs cases, mortality cases, ASDR, and ASMR of GC-DHIS globally up to 2045. (A) The number and ASDR of GC-DHIS by year and gender. (B) The number and ASMR of GC-DHIS by year and gender.
Discussion
The pathogenesis of GC is multifactorial, involving H. pylori infection, genetic susceptibility, and other dietary habits such as high consumption of preserved foods and insufficient intake of fresh fruits and vegetables (23–25). In the present study, we specifically focused on high-sodium diet as a major risk factor. This choice was primarily driven by the availability of detailed and standardized data in the GBD 2021 database, which enabled systematic analyses and reliable trend projections. Moreover, high sodium intake represents a globally prevalent dietary pattern, and its carcinogenic effect on GC has been consistently demonstrated in previous epidemiological and experimental studies. By concentrating on this modifiable risk factor, our study aims to provide actionable evidence and more concrete intervention targets for public health policymaking.
Studies have shown that a high-sodium diet significantly affects the therapeutic outcomes of certain cancers (26–29). Evidence suggests that in GC patients, excessive sodium intake may exacerbate edema and the risk of hypertension, irritate the gastrointestinal tract, and potentially increase the risk of tumor recurrence (8). Furthermore, although this study reveals an association between high sodium intake and GC risk, the underlying biological mechanisms remain to be elucidated. A key future direction will be to actively explore the role of sodium metabolism pathways in the translational application of liquid biopsy technologies. By focusing on the analysis of ctDNA mutational profiles, fragmentomics features, exosomal RNA, and microbe-derived cfRNA in patient plasma, we aim to identify specific molecular biomarkers driven by high sodium exposure (30). Our ultimate vision is to integrate these “sodium footprint” biomarkers into a future multi-cancer joint screening system, thereby establishing an early-warning model for GC that incorporates dietary risk factors and is applicable to multinational populations (31). Finally, a high-sodium diet may lead to elevated sodium ion concentrations within the tumor microenvironment (32). Increasing evidence indicates that this localized high-sodium milieu may activate or upregulate voltage-gated sodium channels (VGSCs) on tumor cell membranes (33–35). VGSCs are frequently aberrantly expressed in various cancers, including GC, and their activity is closely linked to the invasive, migratory, and metastatic capabilities of tumor cells (33, 36). Therefore, we hypothesize that dietary sodium intake may, at least in part, modulate sodium levels in the tumor microenvironment, thereby influencing the functional state of VGSCs and ultimately “empowering” tumor cells with enhanced invasive and metastatic potential.
From 1990 to 2021, the global number of DALYs due to GC-DHIS slightly declined, while the number of deaths increased. This seemingly paradoxical phenomenon can be explained by population growth and aging. Although population growth and aging contributed to an absolute increase in GC burden, effective public health interventions and advances in medical technology have led to a decline in ASDR and ASMR. Middle SDI regions had the highest number of DALYs, while the fastest growth occurred in low-middle SDI regions, possibly due to limited health awareness and medical resources during economic development. In low SDI regions, high sodium intake, compounded by scarce medical resources and low health literacy, may further exacerbate the GC burden. In contrast, in high SDI regions, although health awareness and medical resources are more abundant, high sodium dietary habits persist, contributing to relatively high GC incidence. Oceania experienced a sharp increase in DALYs and deaths, while East Asia had the highest ASDR and ASMR, which may be linked to the traditionally high-sodium diet in this region. Overall, despite the global decline in age-standardized rates of GC-DHIS, the burden continues to rise in certain regions and populations. Targeted public health policies are therefore needed, particularly in high-risk regions and populations, to reduce sodium consumption, improve health awareness, and optimize medical resource allocation. These measures are essential to mitigate the GC burden in the context of rapid population growth and aging.
Over the past 32 years, approximately 65% of countries experienced an upward trend in DALYs due to GC-DHIS, and about 70% saw an increase in deaths. Countries such as Djibouti, the United Arab Emirates, and Honduras showed particularly notable increases in DALYs and deaths. Additionally, countries like Mongolia and Bolivia had relatively high ASDR and ASMR, reflecting significant geographic disparities in the impact of high sodium intake on GC. In terms of age and sex, in 2021, the 65–69 age group had the highest number of DALYs, while the 70–74 age group had the highest number of deaths. The highest ASDR was recorded in females aged 95+ and males aged 85–89, whereas the highest ASMR was found in females aged 95+ and males aged 90–94. These findings suggest that older populations are more severely affected by the consequences of high sodium intake, and the burden of GC is particularly pronounced among elderly males.
Decomposition analysis revealed that while the global number of DALYs due to GC-DHIS has decreased overall, DALYs among males have increased, whereas those among females have declined significantly. Meanwhile, the number of death cases has shown an upward trend, with the increase being more pronounced in males than in females. These changes have been significantly influenced by population aging, growth, and epidemiological changes. Aging and population growth have contributed to the increase in DALYs and death cases, while epidemiological changes have partially mitigated this upward trend.
Health inequality analysis indicated that although the absolute disparity between countries with the highest and lowest SDI levels has narrowed, the disease burden remains more concentrated in higher SDI regions. This may be attributed to factors such as high-sodium dietary habits, and lifestyle patterns in these more developed areas.
Forecasting analysis indicated that by 2045, the absolute burden of GC-DHIS will continue to rise, with men experiencing more DALYs and deaths than women. This disparity may stem from differences in exposure levels, biological factors, and access to healthcare (37, 38). First, men may consume more sodium than women due to dietary preferences, such as a greater tendency to consume salty foods. Second, biological differences, including hormone levels and gene expression, may influence GC development differently in men and women. Finally, men may be less likely than women to participate in regular health checkups and cancer screening, leading to delayed diagnosis and treatment, which in turn contributes to higher disease severity and mortality. Meanwhile, ASDR and ASMR are projected to continue declining, suggesting that despite population pressures, the population-level risk is decreasing. These findings underscore the urgency of implementing targeted interventions for high-risk male populations, while continuing broader efforts to reduce dietary sodium intake. However, it should be noted that the forecasting model assumes no major policy or intervention changes in the coming decades. If effective public health interventions are implemented in the future—such as sodium reduction policies and health awareness campaigns—the actual burden may be lower than predicted.
This study also has several limitations. First, there may be inconsistencies in the definition and quantification of high-sodium diets. Dietary habits vary across countries and regions, leading to potential discrepancies in how “high-sodium diet” is defined, which could introduce bias in cross-regional comparisons. Second, although the study covers 204 countries and territories, data from some small countries or regions may be incomplete or not fully representative, potentially affecting the global representativeness of the findings.
Conclusion
This study, based on the GBD 2021 database, analyzed the global and regional burden of GC-DHIS from 1990 to 2021, and projected trends from 2022 to 2045. The results showed that from 1990 to 2021, the global number of DALYs due to GC-DHIS slightly declined, while deaths increased. Middle SDI regions bore the highest disease burden, but the fastest increase occurred in Low-middle SDI regions. Around 65% of countries experienced an increase in DALYs, and approximately 70% saw an increase in deaths, with significant rises observed in Djibouti, the United Arab Emirates, and Honduras. In 2021, the highest number of DALYs occurred in the 65–69 age group, and the highest number of deaths in the 70–74 age group. Additionally, while the absolute inequality gap between countries with the highest and lowest SDI levels has narrowed, the disease burden has become more concentrated in higher-SDI regions. Projections from 2022 to 2045 indicate a significant increase in DALYs and deaths due to GC-DHIS, with faster growth among males, although ASDR and ASMR are expected to decline notably. Therefore, GC-DHIS remains a major global public health concern. Despite the overall decline in ASDR and ASMR, the burden continues to rise in certain regions and populations. More effective health interventions targeting older adults and male populations are needed to address the potentially increasing burden of GC.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
CM: Conceptualization, Writing – original draft, Writing – review & editing, Formal analysis. BY: Writing – review & editing, Investigation. GL: Writing – review & editing, Methodology. YJ: Writing – review & editing, Conceptualization, Data curation, Writing – original draft.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
We sincerely appreciate all the participants of the GBD 2021 for their contribution.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2025.1674979/full#supplementary-material
References
1. Chen, YC, Malfertheiner, P, Yu, HT, Kuo, CL, Chang, YY, Meng, FT, et al. Global prevalence of Helicobacter pylori infection and incidence of gastric Cancer between 1980 and 2022. Gastroenterology. (2024) 166:605–19. doi: 10.1053/j.gastro.2023.12.022
2. Vanegas, JC, Herrero, R, Barboza-Solís, C, Ocampo, R, Torres, G, Ortiz-Barboza, A, et al. Descriptive epidemiology of gastric cancer in Costa Rica from 1990 to 2022 and projection of deaths to 2050: a population-based study. Lancet Regional Health Americas. (2025) 49:101194. doi: 10.1016/j.lana.2025.101194
3. Mithany, RH, Shahid, MH, Manasseh, M, Saeed, MT, Aslam, S, Mohamed, MS, et al. Gastric cancer: a comprehensive literature review. Cureus. (2024) 16:e55902. doi: 10.7759/cureus.55902
4. Jayakrishnan, T, and Ng, K. Early-onset gastrointestinal cancers: a review. JAMA. Epub ahead of print. (2025). doi: 10.1001/jama.2025.10218
5. Fu, J, Shin, W-K, Huang, D, De la Torre, K, Kang, D, and Shin, S. Fruit and salt consumption are related to the risk of gastric cancer incidence in Asian populations: a comprehensive systematic review and meta-analysis of cohort studies. Epidemiol Rev. (2025) 47:mxaf007. doi: 10.1093/epirev/mxaf007
6. Tan, N, Wu, H, Cao, M, Yang, F, Yan, X, He, S, et al. Global, regional, and national burden of early-onset gastric cancer. Cancer Biol Med. (2024) 21:667–78. doi: 10.20892/j.issn.2095-3941.2024.0159
7. Liu, W, Peng, ZZ, Zhao, DQ, Liu, Y, and Liao, K. The burden of gastric cancer attributed to high salt intake and predictions through the year 2042: a cross-national comparative analysis of China, Japan, and South Korea. Front Nutr. (2025) 12:1584400. doi: 10.3389/fnut.2025.1584400
8. Tang, S, Xu, J, Wan, P, Jin, S, Zhang, Y, Xun, L, et al. Recent advances in the role of high-salt diet in anti- and pro-cancer progression. Front Immunol. (2025) 16:1542157. doi: 10.3389/fimmu.2025.1542157
9. Wu, B, Yang, D, Yang, S, and Zhang, G. Dietary salt intake and gastric Cancer risk: a systematic review and Meta-analysis. Front Nutr. (2021) 8:801228. doi: 10.3389/fnut.2021.801228
10. Balendra, V, Amoroso, C, Galassi, B, Esposto, J, Bareggi, C, Luu, J, et al. High-salt diet exacerbates H. pylori infection and increases gastric Cancer risks. J Personal Med. (2023) 13:1325. doi: 10.3390/jpm13091325
11. Ou, L, Liu, H, Peng, C, Zou, Y, Jia, J, Li, H, et al. Helicobacter pylori infection facilitates cell migration and potentially impact clinical outcomes in gastric cancer. Heliyon. (2024) 10:e37046. doi: 10.1016/j.heliyon.2024.e37046
12. Wang, XQ, Terry, PD, and Yan, H. Review of salt consumption and stomach cancer risk: epidemiological and biological evidence. World J Gastroenterol. (2009) 15:2204–13. doi: 10.3748/wjg.15.2204
13. Chen, J, Li, Z, and Liu, H. Analysis of study global burden of disease in 2021: global, regional, and national burden of nutritional deficiency from 1990 to 2021. Front Nutr. (2024) 11:1540485. doi: 10.3389/fnut.2024.1540485
14. Liang, S, Xi, SZ, Liu, JY, Tang, GC, Zhang, WG, Guo, XR, et al. Global burden and cross-country inequalities of nutritional deficiencies in adults aged 65 years and older, 1990-2021: population-based study using the GBD 2021. BMC Geriatr. (2025) 25:74. doi: 10.1186/s12877-025-05728-9
15. Chen, B, Zhan, Z, Xu, Y, Yu, S, Huang, J, Fang, Y, et al. Long-term trends in the burden of nasopharyngeal carcinoma in China: a comprehensive analysis from 1990 to 2021 and projections to 2030 based on the global burden of disease study 2021. Radiother Oncol. (2025) 202:110613. doi: 10.1016/j.radonc.2024.110613
16. Chen, QF, Ni, C, Jiang, Y, Chen, L, Liao, H, Gao, J, et al. Global burden of disease and its risk factors for adults aged 70 and older across 204 countries and territories: a comprehensive analysis of the global burden of disease study 2021. BMC Geriatr. (2025) 25:462. doi: 10.1186/s12877-025-06095-1
17. Bai, Z, Han, J, An, J, Wang, H, Du, X, Yang, Z, et al. The global, regional, and national patterns of change in the burden of congenital birth defects, 1990-2021: an analysis of the global burden of disease study 2021 and forecast to 2040. EClinicalMedicine. (2024) 77:102873. doi: 10.1016/j.eclinm.2024.102873
18. Yan, S, Cheng, M, Peng, W, Liu, T, Zhang, J, Sheng, M, et al. Incidence and risk of remnant gastric cancer after gastrectomy for gastric cancer: a population-based study from the SEER database. BMC Gastroenterol. (2024) 24:35. doi: 10.1186/s12876-024-03133-x
19. Xie, F, Xiong, F, Yang, B, Yan, Z, Shen, Y, Qin, H, et al. Global, regional, and national burden of mortality and DALYs attributable to high body mass index from 1990 to 2021 with projections to 2036. BMC Public Health. (2025) 25:2053. doi: 10.1186/s12889-025-23237-7
20. Wu, R, Guo, Y, Chen, Y, and Zhang, J. Osteoarthritis burden and inequality from 1990 to 2021: a systematic analysis for the global burden of disease study 2021. Sci Rep. (2025) 15:8305. doi: 10.1038/s41598-025-93124-z
21. Yao, L, Cao, J, Cheng, S, Shan, S, Jiang, D, Luo, Z, et al. Inequalities in disease burden and care quality of chronic obstructive pulmonary disease, 1990-2021: findings from the global burden of disease study 2021. J Glob Health. (2024) 14:04213. doi: 10.7189/jogh.14.04213
22. Wang, K, Chen, S, Wang, M, Han, Q, Hou, Y, and Wang, X. Global, regional, and national burden of chronic kidney disease attributable to dietary risks from 1990 to 2021. Front Nutr. (2025) 12:1555159. doi: 10.3389/fnut.2025.1555159
23. Ali, A, and AlHussaini, KI. Helicobacter pylori: a contemporary perspective on pathogenesis, diagnosis and treatment strategies. Microorganisms. (2024) 12:222. doi: 10.3390/microorganisms12010222
24. Liou, JM, Malfertheiner, P, Hong, TC, Cheng, HC, Sugano, K, Shah, S, et al. Screening and eradication of Helicobacter pylori for gastric cancer prevention: Taipei global consensus II. Gut. (2025). gutjnl-2025-336027. doi: 10.1136/gutjnl-2025-336027
25. Drnovsek, J, Homan, M, Zidar, N, and Smid, LM. Pathogenesis and potential reversibility of intestinal metaplasia – a milestone in gastric carcinogenesis. Radiol Oncol. (2024) 58:186–95. doi: 10.2478/raon-2024-0028
26. Deng, Y, Hou, X, Fang, Q, Wang, H, Li, X, Hu, Z, et al. High-salt diet decreases FOLFOX efficacy via gut bacterial tryptophan metabolism in colorectal cancer. Mol Med. (2025) 31:66. doi: 10.1186/s10020-025-01122-8
27. Tucker, L, Ali, U, Zent, R, Lannigan, DA, Rathmell, JC, and Tiriveedhi, V. Chronic high-salt diet activates tumor-initiating stem cells leading to breast Cancer proliferation. Cells. (2024) 13:912. doi: 10.3390/cells13110912
28. Sonkin, D, Thomas, A, and Teicher, BA. Cancer treatments: past, present, and future. Cancer Genet. (2024) 286-287:18–24. doi: 10.1016/j.cancergen.2024.06.002
29. R, MJ, Telang, B, Soni, G, and Khalife, A. Overview of perspectives on cancer, newer therapies, and future directions. J Oncol Translat Med. (2024) 10:105–9. doi: 10.1097/ot9.0000000000000039
30. Jahangiri, L. Updates on liquid biopsies in neuroblastoma for treatment response, relapse and recurrence assessment. Cancer Genet. (2024) 288-289:32–9. doi: 10.1016/j.cancergen.2024.09.001
31. Chen, Z, and Er Saw, P. Integration in biomedical science 2024: emerging trends in the post-pandemic era. BIO Integr. (2024) 5:1–2. doi: 10.15212/bioi-2024-1001
32. Ali, U, and Tiriveedhi, V. High-salt tumor microenvironment: not as bad as it sounds, not as good as it seems. Cancer. (2025) 17:1924. doi: 10.3390/cancers17121924
33. Liu, H, Weng, J, Huang, CL, and Jackson, AP. Voltage-gated sodium channels in cancers. Biomark Res. (2024) 12:70. doi: 10.1186/s40364-024-00620-x
34. Bian, Y, Tuo, J, He, L, Li, W, Li, S, Chu, H, et al. Voltage-gated sodium channels in cancer and their specific inhibitors. Pathol Res Pract. (2023) 251:154909. doi: 10.1016/j.prp.2023.154909
35. Zhao, LM, Hong, WY, Xu, JG, Lin, SQ, Liu, MS, Wang, LH, et al. Nav1.6 drives colorectal cancer proliferation and invasion through MAPK signaling pathway. World J Gastrointestinal Oncol. (2025) 17:105264. doi: 10.4251/wjgo.v17.i7.105264
36. Liu, H, Hamaia, SW, Dobson, L, Weng, J, Hernández, FL, Beaudoin, CA, et al. The voltage-gated sodium channel β3 subunit modulates C6 glioma cell motility independently of channel activity. Biochim Biophys Acta. (2025) 1871:167844. doi: 10.1016/j.bbadis.2025.167844
37. Song, Y, Liu, X, Cheng, W, Li, H, and Zhang, D. The global, regional and national burden of stomach cancer and its attributable risk factors from 1990 to 2019. Sci Rep. (2022) 12:11542. doi: 10.1038/s41598-022-15839-7
Keywords: diet high in sodium, gastric cancer, DALYs, SDI, cross-national inequality
Citation: Ma C, Yan B, Li G and Jiang Y (2025) Global, regional, and national burden of gastric cancer attributable to diet high in sodium from 1990 to 2021. Front. Nutr. 12:1674979. doi: 10.3389/fnut.2025.1674979
Edited by:
Hailin Tang, Sun Yat-sen University Cancer Center (SYSUCC), ChinaReviewed by:
Wei Gao, Central South University, ChinaHengrui Liu, University of Cambridge, United Kingdom
Xiaofei Fan, Shandong Medical College, China
Copyright © 2025 Ma, Yan, Li and Jiang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yongsheng Jiang, anlzMTQ3NkB6eHl5LmNu