 Qi Wang1†
Qi Wang1† Jiachun Xu
Jiachun Xu Ziqi Wang
Ziqi Wang- 1Traditional Chinese Medicine College, North China University of Science and Technology, Tangshan, China
- 2Acupuncture Center for Brain Diseases, The Second Affiliated Hospital of Tianjin University of Traditional Chinese Medicine, Tianjin, China
- 3Department of Pharm, Hua Ren Orthopedic Hospital, Tangshan, China
Introduction: Using data from the Global Burden of Disease Study 2021 (GBD 2021), this study analyzed the 32-year trends (1990–2021) of stroke burden in China, quantified the attributable risk factors, and projected the future trajectories (2022–2035) of stroke and its subtypes. It also emphasized subtype- and gender-specific disparities to provide evidence for precision prevention.
Methods: Age-standardized incidence rate (ASIR), prevalence rate (ASPR), mortality rate (ASMR), and disability-adjusted life years rate (ASDR) of stroke were analyzed using estimated annual percentage change (EAPC) and Joinpoint regression. The population attributable fraction (PAF) was used to quantify the burden of stroke-related disability-adjusted life years (DALYs) attributed to risk factors, and Bayesian age-period-cohort (BAPC) modeling was applied to project future burden.
Results: In 2021, the ASIR, ASPR, ASMR, and ASDR of stroke in China were 204.75, 1301.42, 138.03, and 2,648.02 per 100,000 populations, respectively. From 1990 to 2021, ASMR (EAPC = −1.92; 95% CI: −2.17 to −1.67) and ASDR (EAPC = −2.05; 95% CI: −2.25 to −1.86) of stroke decreased, while ASPR increased (EAPC = 0.34; 95% CI: 0.31 to 0.38). Subtype analysis showed opposing trends: IS ASIR (EAPC = 0.94; 95% CI: 0.88 to 1.00) and ASPR (EAPC = 1.02; 95% CI: 0.96 to 1.08) increased, whereas ICH and SAH burdens decreased (ICH ASIR EAPC = −2.24; SAH ASIR EAPC = −3.70). Males had higher ASRs than females in 2021, except for ICH ASPR. High systolic blood pressure (PAF = 56.04%), ambient particulate matter pollution (PAF = 24.37%), and smoking (PAF = 17.91%) were the top three risk factors for stroke-related DALYs; high LDL cholesterol (PAF = 28.42%) ranked second for IS. Projections indicated that by 2035, overall stroke ASIR (from 208.27 to 194.07 per 100,000) and ASMR (from 139.94 to 100.34 per 100,000) would decrease, but IS ASIR would rise to 156.44 per 100,000 (from 139.98 per 100,000 in 2022).
Conclusions: The stroke burden in China shows a downward trend, with a subtype-specific feature of increasing IS and decreasing ICH/SAH. High systolic blood pressure is the potential risk factor for stroke, with variations across subtypes and genders. Targeted interventions such as smoking control for males, sodium intake reduction for females, and LDL cholesterol management for IS, are urgently needed to mitigate the future IS burden.
1 Introduction
Stroke, a leading non-communicable disease, ranks as the second cause of global death and the third cause of death and disability worldwide (1). According to the Global Burden of Disease Study 2021 (GBD 2021), there were 11.9 million incident stroke cases, 93.8 million prevalent cases, 7.3 million stroke-related deaths, and 160.5 million stroke-related disability-adjusted life years (DALYs) globally in 2021 (2). Although age-standardized rate of incidence (ASIR), prevalence (ASPR), mortality (ASMR), and DALYs (ASDR) of stroke have decreased globally from 1990 to 2021, the overall stroke burden remains substantial, with marked disparities across regions and countries (3). Notably, China contributes ~30% of global stroke deaths and 25% of global stroke DALYs (2), making it a key contributor to the global stroke burden—especially for ischemic stroke (IS), which accounts for over 60% of China's total stroke cases (4).
Previous study based on GBD 2019 data reported that the ASMR of stroke in China decreased by 39.8% (95% CI: 28.6%−50.7%) from 1990 to 2019, while the death number of stroke in China still increased significantly during the same period (5). Also, the study lacked in-depth analysis of subtype-specific of IS, intracerebral hemorrhage (ICH), subarachnoid hemorrhage (SAH) trends, gender-age disparities in burden, and future projections of stroke burden-gaps that are essential for guiding precision prevention strategies.
At present, there is still a lack of analysis on the disease burden related to stroke and its subtypes in China based on the GBD 2021 data. We conducted the present study using data from the GBD 2021 database, which provides comprehensive information on the incidence, prevalence, mortality, and DALYs of total stroke and its three subtypes (IS, ICH, SAH) in China from 1990 to 2021. The specific objectives of this study are: (1) to systematically summarize the temporal trends of ASIR, ASPR, ASMR, and ASDR for total stroke and its three subtypes in China from 1990 to 2021; (2) to identify high-risk groups by gender and age, and clarify the age-specific peak of each stroke burden indicator (incidence, prevalence, mortality, DALYs) for different subtypes; (3) to quantify the contribution of different attributable risk factors to stroke-related DALYs, and explore gender- and subtype-specific differences in these risk factors; (4) to project the incidence, prevalence, mortality, and DALYs of stroke and its subtypes in China from 2022 to 2035, providing evidence for optimizing national stroke prevention and control policies.
2 Methods
2.1 Overview
The Global Burden of Disease Study 2021 (GBD 2021) database is recognized as one of the most comprehensive and systematic global epidemiological resources, integrating data from cohort studies, disease registries, and national surveys (6). Stroke was defined in accordance with the clinical criteria of the World Health Organization (WHO) and classified into three pathological subtypes: ischemic stroke (IS), intracerebral hemorrhage (ICH), and subarachnoid hemorrhage (SAH) (2). In GBD 2021, these subtypes were coded using the International Classification of Diseases, 10th Revision (ICD-10): IS: G45-G46.8, I63-I63.9, I65-I66.9, I67.2-I67.3, I67.5-I67.6, I69.3; ICH: I61-I62, I62.1-I62.9, I68.1-I68.2, I69.1-I69.2; SAH: I60-I60.9, I62.0, I67.0-I67.1, I69.0. This study retrieved and analyzed data on the incidence, prevalence, mortality, and disability-adjusted life years (DALYs) of total stroke, IS, ICH, and SAH in mainland China (excluding Hong Kong, Macao, and Taiwan) from 1990 to 2021. The analysis included two key dimensions: gender and age (20 consecutive 5-year age groups, ranging from 0 to 4 years, 5 to 9 years, …, to 95+ years). This study was conducted in accordance with the Guidelines for Accurate and Transparent Health Estimates Reporting (GATHER) (7) and based on de-identified aggregate data from GBD 2021. No individual-level data were collected, so ethical approval was not required. The GBD data used in this study were accessed and downloaded on February 6, 2025, via the GBD Results Tool (http://ghdx.healthdata.org/gbd-results-tool). Filter criteria: Location = China, Year = 1990–2021, Measure = Incidence/Prevalence/Deaths/DALYs, Metric = Rate & Number, Sex = Male/Female/Both, Age = Age-standardized, All ages, < 5years, Cause = Stroke and its three subtypes [ischemic stroke (IS), intracerebral hemorrhage (ICH), subarachnoid hemorrhage (SAH)] (the downloaded file in Supplementary File S1).
2.2 Risk factors
GBD 2021 automatically matched 23 exposure risk factors to stroke cases in China, which were categorized into three groups based on GBD's risk framework: behavioral factors (smoking, alcohol use, diet high in sodium, diet low in fruits/vegetables), metabolic factors (high systolic blood pressure, high low-density lipoprotein (LDL) cholesterol, high fasting plasma glucose, obesity), environmental factors (ambient particulate matter pollution, household air pollution).
For risk factor analysis, spatiotemporal Gaussian process regression or DisMod-MR 2.1 was used to model exposure data for each risk factor (8). Quantitative relative risk (RR) estimates were generated for each risk-stroke outcome pair. These RR estimates were then combined with corresponding population exposure estimates to calculate the population attributable fraction (PAF) for each risk-outcome association. The PAF was multiplied by the total stroke-related DALYs, years of life lost (YLLs), and years lived with disability (YLDs) to determine the burden (DALYs, YLLs, YLDs) attributable to each risk factor. Detailed calculation procedures have been described in previous GBD-related studies (9).
It must be emphasized that the PAFs reported in this study are estimates based on the GBD counterfactual modeling framework. They represent the theoretical burden of disease attributable to specific risk factors under particular model assumptions and counterfactual exposure distributions, rather than direct estimates of causal effects derived from observational studies. Therefore, the interpretation of PAF values requires caution, and they should not be directly equated with the actual gains achievable through interventions.
2.3 Statistical analysis
All statistical analyses were performed using R software (version 4.3.3), with a two-tailed significance level set at p < 0.05. Graphs were generated using JD_GBDR2021 (V2.7.1, Jingding Medical Technology Co., Ltd.).
Based on GBD 2021 statistics, ASIR, ASPR, ASMR, and ASDR (per 100,000 population) were calculated, with their corresponding 95% uncertainty intervals (95% UI) provided to reflect data variability.
Temporal trends in disease rates were analyzed using segmented log-linear regression implemented in R (version 4.3.3) with the segmented package. The function selgmented() was used to automatically identify the optimal number and location of joinpoints based on the Bayesian Information Criterion (BIC), with a maximum of five candidate breakpoints (Kmax = 5) (R scripts in Supplementary File S2).
Annual percentage change (APC) values and their 95% confidence intervals (95% CIs) were derived from the estimated slopes of each time segment. The average annual percentage change (AAPC) and its 95% CI were calculated as the length-weighted mean of segment-specific APCs. Statistical significance was assessed using t or z tests derived from model estimates.
This automated BIC-based approach provides an objective and reproducible framework for detecting inflection points and quantifying temporal trend changes without requiring predefined breakpoints or manual permutation testing.
A log-transformed linear regression model was used to calculate the EAPC and its 95% CI, to characterize the long-term temporal trends of stroke incidence, prevalence, mortality, and DALYs in China from 1990 to 2021 (10). The interpretation of EAPC was as follows: If EAPC > 0 and the lower bound of 95% CI > 0, it indicates a significant upward trend; If EAPC < 0 and the upper bound of 95% CI < 0, it indicates a significant downward trend.
We modeled and projected stroke incidence using a Bayesian age-period-cohort (BAPC) framework implemented with Integrated Nested Laplace Approximations (INLA) (11). Age and cohort effects were specified as second-order random walks (RW2) and the period effect as a first-order random walk (RW1). Precision hyperparameters used weakly informative log-Gamma priors in the main analysis; alternative structural variants (removing the cohort term, toggling an IID over-dispersion component, and alternative RW orders) were explored in sensitivity analyses. Because INLA is a deterministic approximation rather than an MCMC method, burn-in, iteration counts PSRF, and effective sample size are not applicable; we report posterior medians and 95% credible intervals (Crl). Model adequacy followed INLA conventions, summarizing WAIC, DIC, log conditional predictive ordinates (LCPO) and CPO failure rate, and assessing calibration using probability integral transform (PIT) histograms with Kolmogorov-Smirnov tests for uniformity. Age-standardized rates were computed using the WHO world standard population and expressed per 100,000 persons. Projections to 2035 are conditional on the continuation of recent APC patterns; robustness was evaluated via the sensitivity analyses described above.
We used the native INLA APC model as an alternative prediction method for verification. Its prediction results were highly consistent with those of the BAPC model [shown in Figure BAPC vs. native INLA (observed + projected) in Supplementary File S3], further demonstrating the stability of the model.
3 Results
3.1 Temporal trends of stroke burden in China (1990–2021)
3.1.1 Incidence
In 2021, the absolute number of incident cases for total stroke, ischemic stroke (IS), intracerebral hemorrhage (ICH), and subarachnoid hemorrhage (SAH) in China was 4,090,480.12 (95% UI: 3,593,818.73–4,699,827.92), 2,772,053.33 (95% UI: 2,295,713.37–3,319,150.09), 1,173,288.31 (95% UI: 1,003,992.98–1,330,455.36), and 145,138.48 (95% UI: 125,425.42–169,016.38), respectively (Tab.1). Their corresponding age-standardized incidence rates (ASIR) per 100,000 populations were 204.75 (95% UI: 181.03–231.50) for total stroke, 135.79 (95% UI: 113.25–159.83) for IS, 61.15 (95% UI: 52.98–69.06) for ICH, and 7.81 (95% UI: 6.88–8.95) for SAH (Table 1).
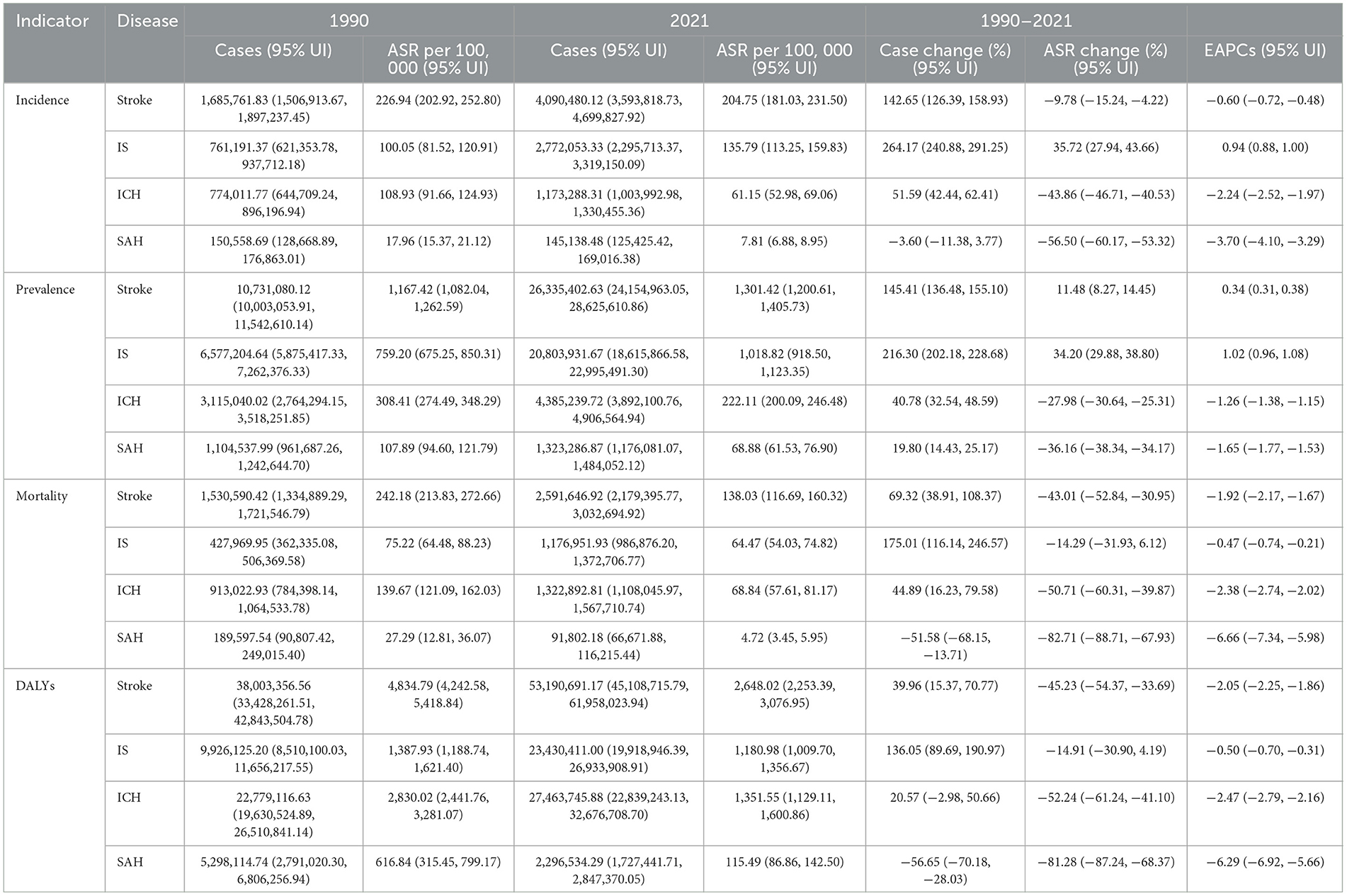
Table 1. Incidence, prevalence, mortality, DALYs of stroke, IS, ICH, SAH in China from 1990 to 2021.
From 1990 to 2021, for total stroke, ASIR showed a fluctuating downward trend (EAPC = −0.60; 95% CI: −0.72 to −0.48), with a 9.78% relative decrease from 226.94/100,000 in 1990 to 204.75/100,000 in 2021) and distinct stage changes: an initial increase during 1990–1993 (APC = 1.24%; 95% CI: 0.313%−2.175%, P = 0.009), a significant decline during 1993–2006 (APC = −0.381%; 95% CI: −0.533% to −0.229%, P < 0.001), and 2006–2013(APC = −1.831%; 95% CI: −2.212% to −1.449%, P < 0.001), with a slight rebound (2013–2021, APC = 0.21%; 95% CI: 0.05%−0.37%, P < 0.001) (Figure 1A, Supplementary Table S1). For IS, ASIR exhibited a continuous upward trend (EAPC = 0.94; 95% CI: 0.88–1.00), with a 35.72% relative increase (from 100.05/100,000 to 135.79/100,000) and an accelerated rise after 2014 (2014–2021, APC = 1.619%; 95% CI: 1.278%−1.962%, P < 0.001) (Figure 1B, Supplementary Table S1). For ICH and SAH (Figures 1C, D), ASIR declined sharply: ICH (EAPC = −2.24; 95% CI: −2.52 to −1.97) and SAH (EAPC = −3.70; 95% CI: −4.10 to −3.29), with no significant rebound in the latest stage (Supplementary Table S1).
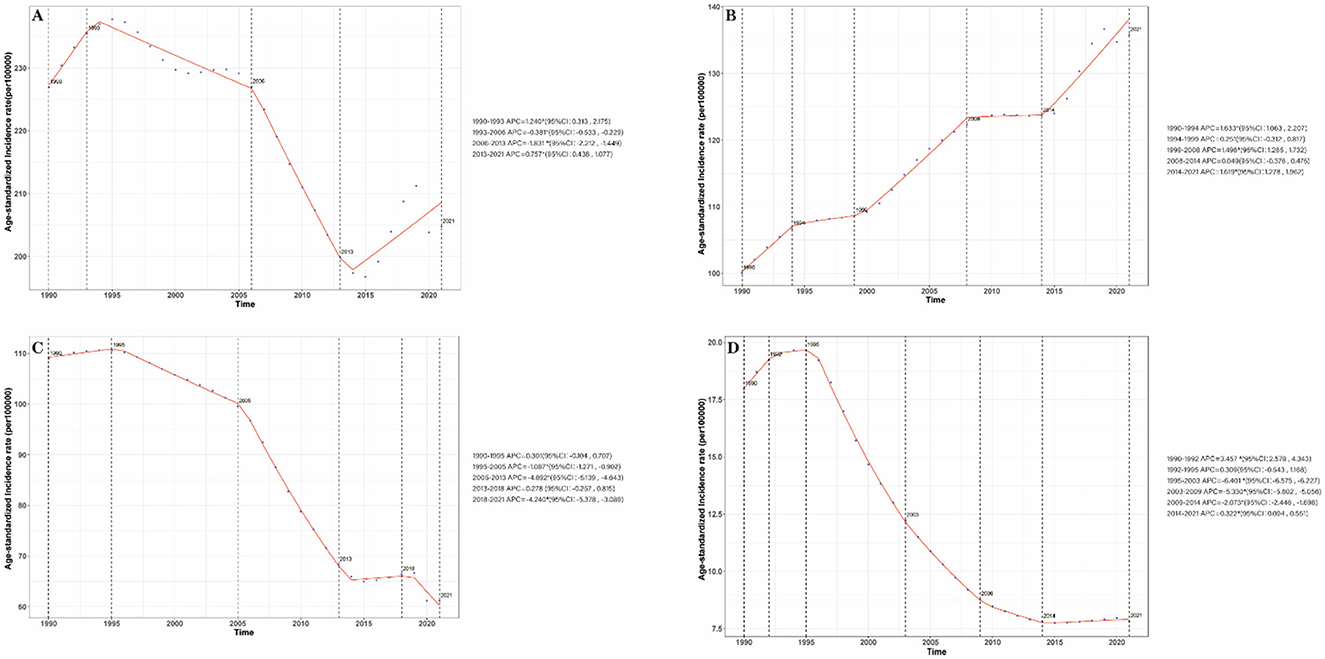
Figure 1. Annual percent change (APC) and trends in China stroke incidence from 1990 to 2021. (A) Stroke; (B) IS; (C) ICH; (D) SAH.
3.1.2 Prevalence
In 2021, the absolute number of prevalent cases for total stroke, IS, ICH, and SAH was 26,335,402.63 (95% UI: 24,154,963.05–28,625,610.86), 20,803,931.67 (95% UI: 18,615,866.58–22,995,491.30), 4,385,239.72 (95% UI: 3,892,100.76–4,906,564.94), and 1,323,286.87 (95% UI: 1,176,081.07–1,484,052.12), respectively (Table 1). Their age-standardized prevalence rates (ASPR) per 100,000 were 1,301.42 (95% UI: 1,200.61–1,405.73) for total stroke, 1,018.82 (95% UI: 918.50–1,123.35) for IS, 222.11 (95% UI: 200.09–246.48) for ICH, and 68.88 (95% UI: 61.53–76.90) for SAH. From 1990 to 2021, for total stroke, ASPR increased by 11.48% (from 1,167.42/100,000 to 1,301.42/100,000, EAPC = 0.34; 95% CI: 0.31–0.38), with a significant acceleration during 2019–2021 (APC=1.581%; 95% CI: 0.949%−2.216%, P < 0.001) (Supplementary Figure S1A, Supplementary Table S1). For IS, ASPR rose by 34.20% (from 759.20/100,000 to 1018.82/100,000, EAPC = 1.02; 95% CI: 0.96–1.08), accounting for 78.9% of total stroke prevalence in 2021 (Table 1). For ICH and SAH: ASPR showed long-term downward trends (ICH: 27.98% relative decrease, EAPC = −1.26; SAH: 36.16% relative decrease, EAPC = −1.65) but rebounded in 2019–2021 for ICH (APC = 3.018%, 95% CI: 2.574%−3.463%, P < 0.001) (Supplementary Figures S1C, D, Supplementary Table S1).
3.1.3 Mortality
In 2021, the absolute number of stroke-related deaths was 2,591,646.92 (95% UI: 2,179,395.77–3,032,694.92) for total stroke, 1,176,951.93 (95% UI: 986,876.20–1,372,706.77) for IS, 1,322,892.81 (95% UI: 1,108,045.97–1,567,710.74) for ICH, and 91,802.18 (95% UI: 66,671.88–116,215.44) for SAH (Table 1). Their age-standardized mortality rates (ASMR) per 100,000 were 138.03 (95% UI: 116.69–160.32) for total stroke, 64.47 (95% UI: 54.03–74.82) for IS, 68.84 (95% UI: 57.61–81.17) for ICH, and 4.72 (95% UI: 3.45–5.95) for SAH. From 1990 to 2021, total stroke ASMR decreased by 43.01% (from 242.18/100,000 to 138.03/100,000, EAPC = −1.92; 95% CI: −2.17 to −1.67), with a brief upward interlude in 1997–2003 (APC = 2.743%, 95% CI: 1.852%−3.641%, P < 0.001) (Supplementary Figure S2A, Supplementary Table S1). The ASMR of IS, ICH, and SAH showed similar downward trends to stroke, with EAPCs of −0.47 (95% CI: −0.74, −0.21), −2.38 (95%CI: −2.74, −2.02), and −6.66 (95% CI: −7.34, −5.98), respectively (Supplementary Figure S2B, Table 1). The ASMR of IS and ICH also showed a brief upward trend from 1998 to 2004, with APCs of 2.914% (95%CI: 2.042%, 3.794%) (Supplementary Figure S2B) and 1.425% (95% CI: 0.739%, 2.115%) (Supplementary Figure S2C).
3.1.4 Disability-adjusted life years (DALYs)
In 2021, total stroke-related DALYs were 53,190,691.17 (95% UI: 45,108,715.79–61,958,023.94), with subtype-specific DALYs of 23,430,411.00 (IS), 27,463,745.88 (ICH), and 2,296,534.29 (SAH) (Table 1). The age-standardized DALY rates (ASDR) per 100,000 were 2,648.02 (95% UI: 2,253.39–3,076.95) for total stroke, 1,180.98 (95% UI: 1,009.70–1,356.67) for IS, 1,351.55 (95% UI: 1,129.11–1,600.86) for ICH, and 115.49 (95% UI: 86.86–142.50) for SAH (Table 1). From 1990 to 2021, total stroke ASDR decreased by 45.23% (from 4,834.79/100,000 to 2,648.02/100,000, EAPC = 2.05; 95% CI: −2.25 to −1.86) (Table 1). The changes in ASDR of IS, ICH, and SAH were similar to those of stroke, and all showed a downward trend, with EAPC being −0.50 (95% CI: −0.70, −0.31), −2.47 (95% CI: −2.79, −2.16), and −6.29 (95% CI: −6.92 to −5.66) respectively. The ASDRs of IS and ICH showed a brief upward trend from 1997 to 2003, with APCs being 2.059% (95% CI: 1.331%−2.792%) (Supplementary Figure S3B) and 0.875% (95% CI: 0.348%, 1.406%) (Supplementary Figure S3C), respectively (Supplementary Table S1).
3.2 Gender and age differences in stroke burden
3.2.1 Gender-specific ASR differences
In 2021, males had higher ASRs than females for all indicators except ICH ASPR, with significant gaps (Table 2). Male stroke ASIR (240.88/100,000, 95% UI: 211.97–274.92) was 41.6% higher than females (170.09/100,000, 95% UI: 150.11–191.12), and male IS ASIR (157.38/100,000) was 36.9% higher than females (114.93/100,000) (Table 2). Male stroke ASPR (1,385.90/100,000, 95% UI: 1,282.65–1,498.26) was 13.8% higher than females (1,218.30/100,000, 95% UI: 1,115.07–1,324.55); SAH was the only subtype with higher female ASPR (73.21/100,000 vs. male 64.32/100,000) (Table 2). Male stroke ASMR (186.83/100,000) and ASDR (3,444.81/100,000) were 80.1% and 73.0% higher than females (103.71/100,000 and 1,990.88/100,000, respectively) (Table 2). From 1990 to 2021, the largest ASR increase was observed in male IS ASIR (42.99% relative increase), while the largest decrease was in female SAH ASMR (84.75% relative decrease) (Table 2).
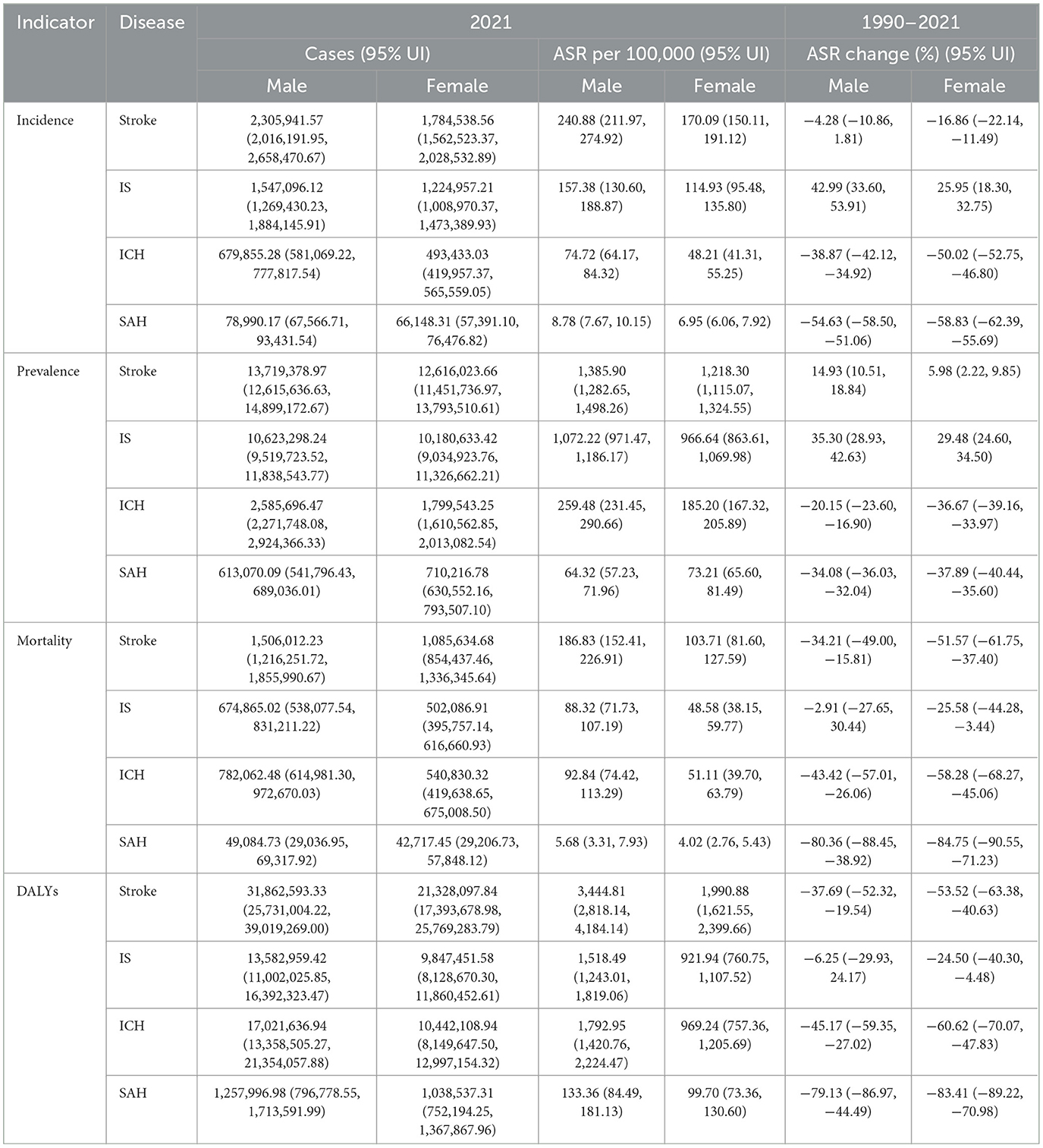
Table 2. Incidence, prevalence, mortality, DALYs of stroke, IS, ICH, SAH in China by gender from 1990 to 2021.
3.2.2 Age-specific peaks of burden
For both genders, stroke burden (incidence, prevalence, mortality, DALYs) increased with age, with distinct peaks (Figure 2, Supplementary Figures S4–S6). For male, the absolute numbers of incidence for stroke, IS, ICH, SAH reached their peaks at the age of 75–79,70–74, 75–79, 75–79 respectively (Figure 2). For female, the absolute numbers of incidence for stroke, IS, ICH, SAH reached their peaks at the age of 70–74, 70–74, 80–84, 75–79. In terms of prevalence, the absolute number of male for stroke, IS, ICH, SAH reached their peaks at the age of 65–69, 70–74, 55–59,75–79, respectively (Supplementary Figure S4). For female, the absolute numbers of prevalence for stroke, IS, ICH, SAH reached their peaks at the age of 65–69, 70–74, 55–59, 70–74. In terms of mortality, the absolute number of male for stroke, IS, ICH, SAH reached their peaks at the age of 75–79, 80–84, 75–79, 70–74, respectively (Supplementary Figure S5). For female, the absolute numbers of mortality for stroke, IS, ICH, SAH reached their peaks at the age of 80–84, 80–84, 80–84, 70–74, respectively (Supplementary Figure S6). In terms of DALYs, the absolute number for stroke, IS, ICH, SAH reached their peaks at the age of 70–74,70–74, 70–74, 65–69, respectively, no matter in male or female.
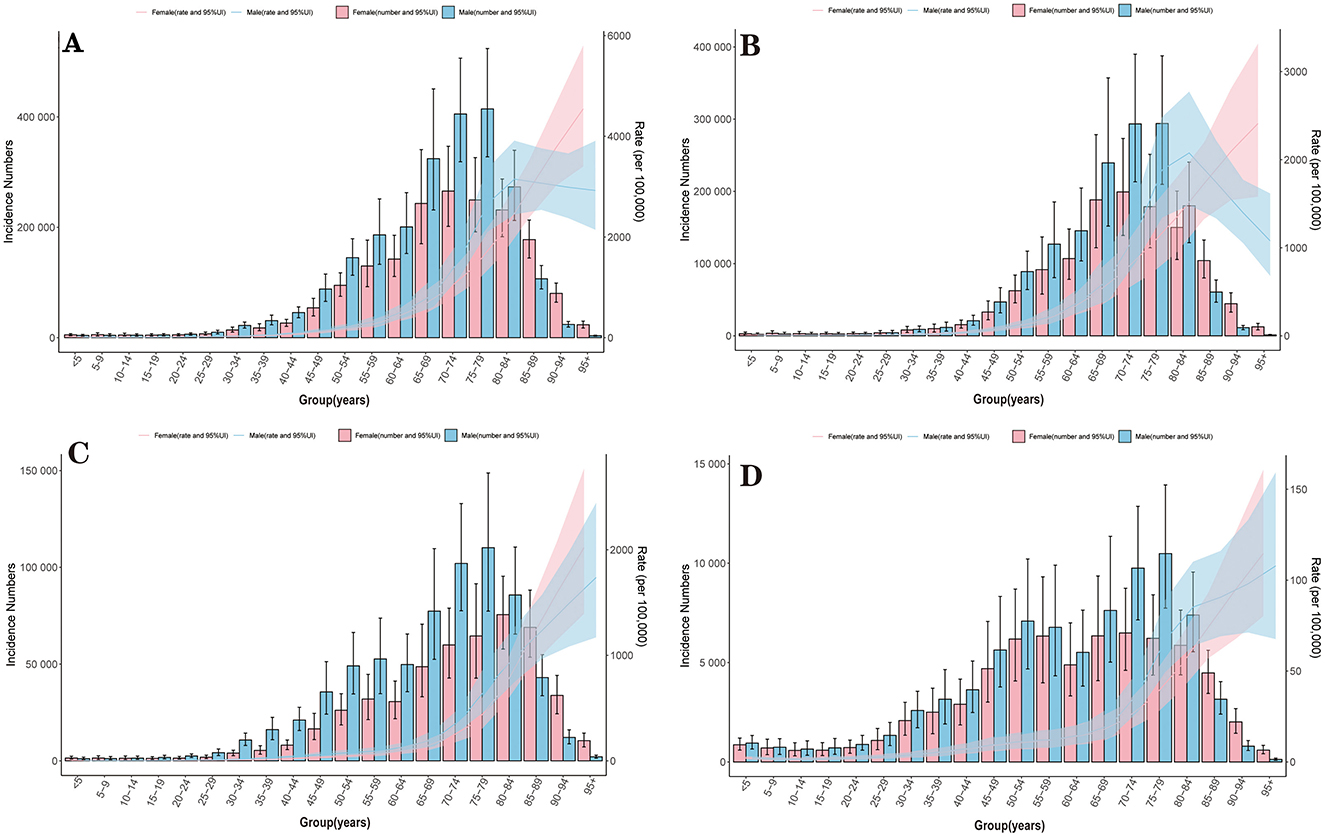
Figure 2. Incidence of stroke and its subtypes by age and sex in China, 2021. (A) Stroke; (B) IS; (C) ICH; (D) SAH.
3.3 Attributable risk factors for stroke-related DALYs
3.3.1 Overall risk factors
In 2021, 23 risk factors accounted for 45,467,333.89 (95% UI: 37,873,525.27–53,193,593.72) stroke-related DALYs in China. The top three risk factors for total stroke were (Table 3) high systolic blood pressure (PAF = 56.04%; 95% UI: 41.75–68.07), the dominant risk factor across all subtypes (IS: 56.68%; ICH: 55.76%; SAH: 52.72%); ambient particulate matter pollution (PAF = 24.37%; 95% UI: 16.37–29.92), with consistent contributions to IS (24.96%), ICH (23.94%), and SAH (23.48%); and smoking (PAF = 17.91%; 95% UI: 15.03–21.07), with higher contributions to ICH (19.81%) than IS (15.70%).
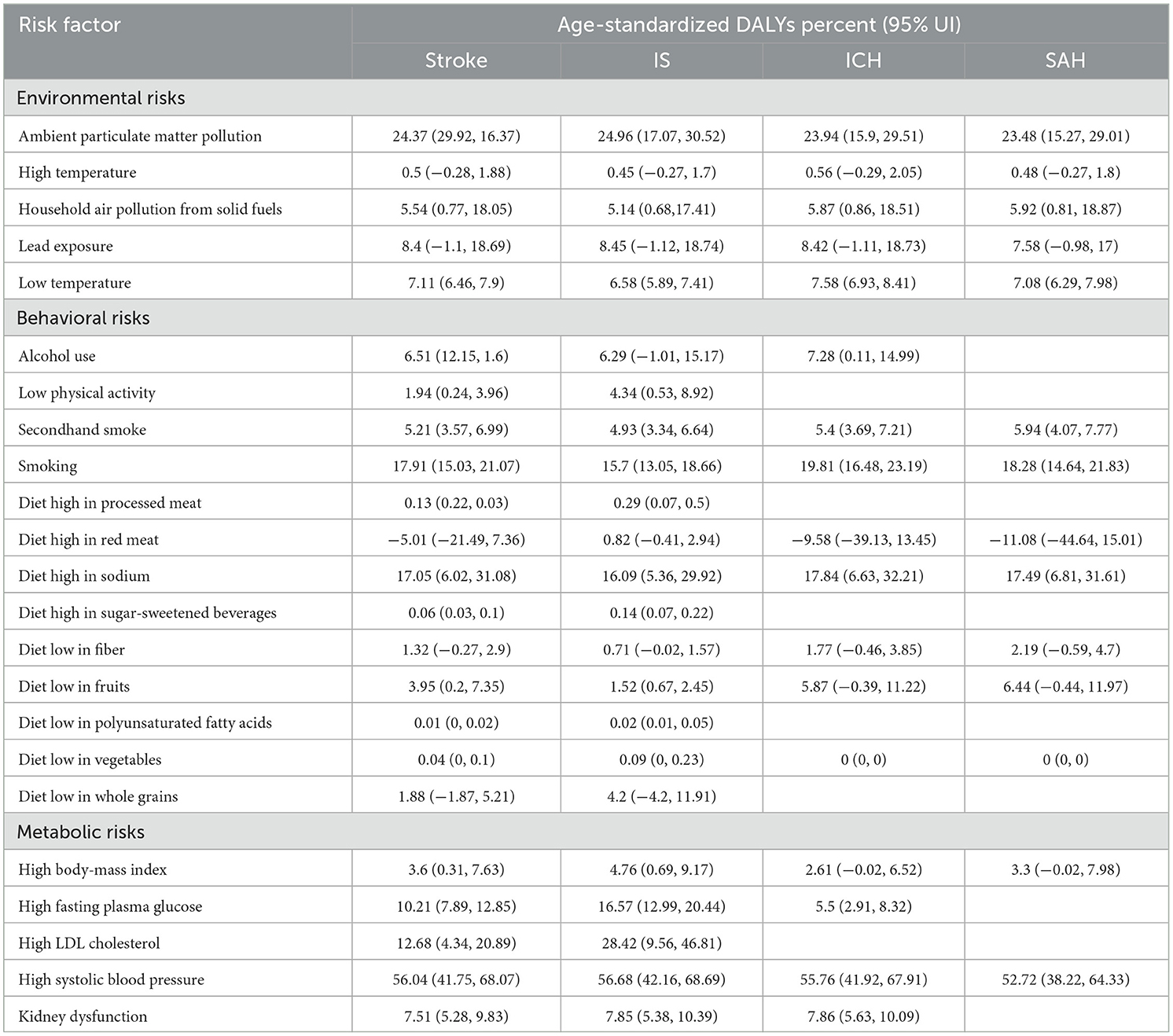
Table 3. Attributable age-standardized DALYs percent by stroke and its subtypes risk factors in 2021 in China.
Notably, high LDL cholesterol ranked second for IS (PAF = 28.42%; 95% UI: 9.56–46.81) but had minimal impact on ICH and SAH. Additionally, diet high in red meat showed negative PAF for ICH (−9.58%; 95% UI: −39.13–13.45) and SAH (−11.08%; 95% UI: −44.64–15.01), likely due to residual confounding (socioeconomic status-related healthcare access) (Table 3).
3.3.2 Gender-specific risk factors
Risk factor contributions differed significantly by gender (Table 4). For males, the top three risk factors for total stroke were high systolic blood pressure (55.57%; 95% UI: 40.64–68.65), smoking (26.82%; 95% UI: 23.18–30.47; 7.8 times higher than females), and ambient particulate matter pollution (24.66%; 95% UI: 17.36–30.06) (Table 4). Smoking also had the highest PAF for male ICH (29.05%) and SAH (29.84%). For females, the top three risk factors were high systolic blood pressure (56.49%; 95% UI: 39.80–69.32), ambient particulate matter pollution (24.00%; 95% UI: 14.93–29.91), and diet high in sodium (14.47%; 95% UI: 4.05–27.83; 1.3 times higher than males) (Table 4). Females also had higher PAF for secondhand smoke (7.25% vs. male 3.89%) and household air pollution (6.53% vs. male 4.85%).
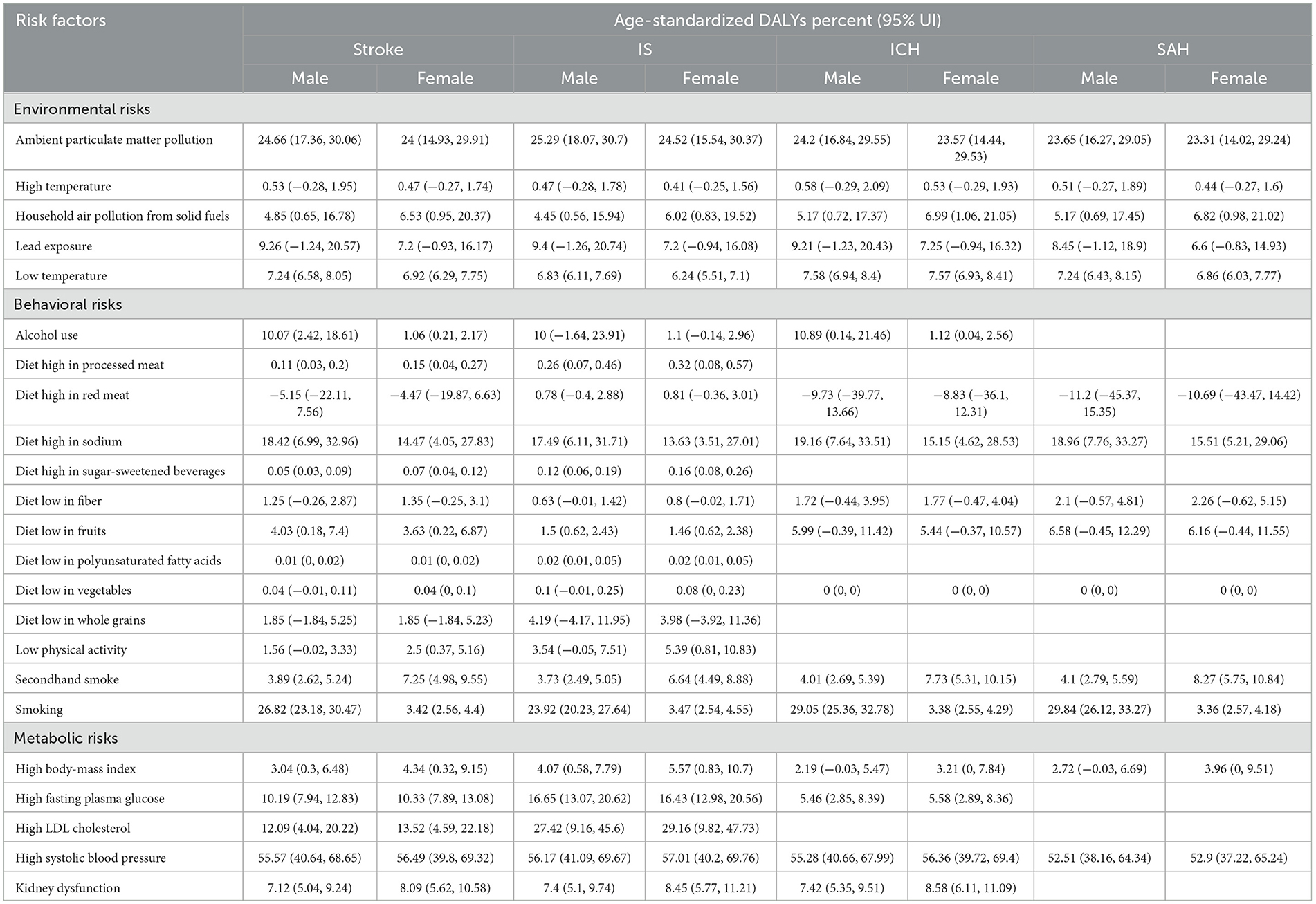
Table 4. Attributable age-standardized DALYs percent by stroke and its subtypes risk factors in 2021 and by sex in China.
3.4 Prediction of stroke burden in China (2022–2035)
Based on Bayesian age-period-cohort (BAPC) modeling, the following trends are predicted (Table 5, Figure 3, Supplementary Figures S7–S9): for total stroke, ASIR will decrease by 6.8% (from 208.27/100,000 in 2022 to 194.07/100,000 in 2035, 95% UI: 168.61–219.54); ASMR will decrease by 28.3% (from 139.94/100,000 to 100.34/100,000, 95% UI: 85.80–114.88); ASDR will decrease by 25.6% (from 2698.04/100,000 to 2007.00/100,000, 95% UI: 1720.99–2293.02).
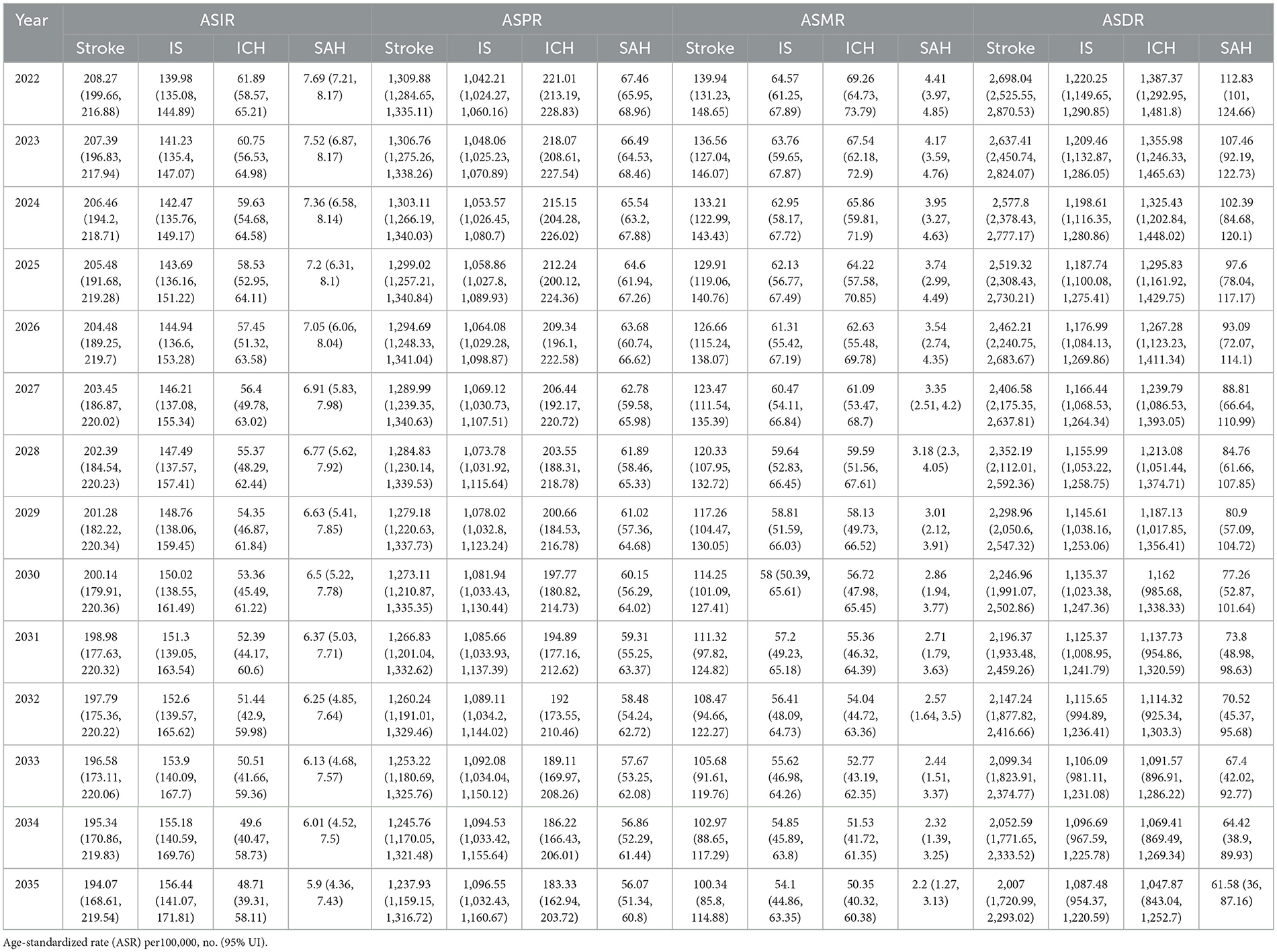
Table 5. Prediction of ASR for stroke and its subtypes in China from 2022 to 2035.
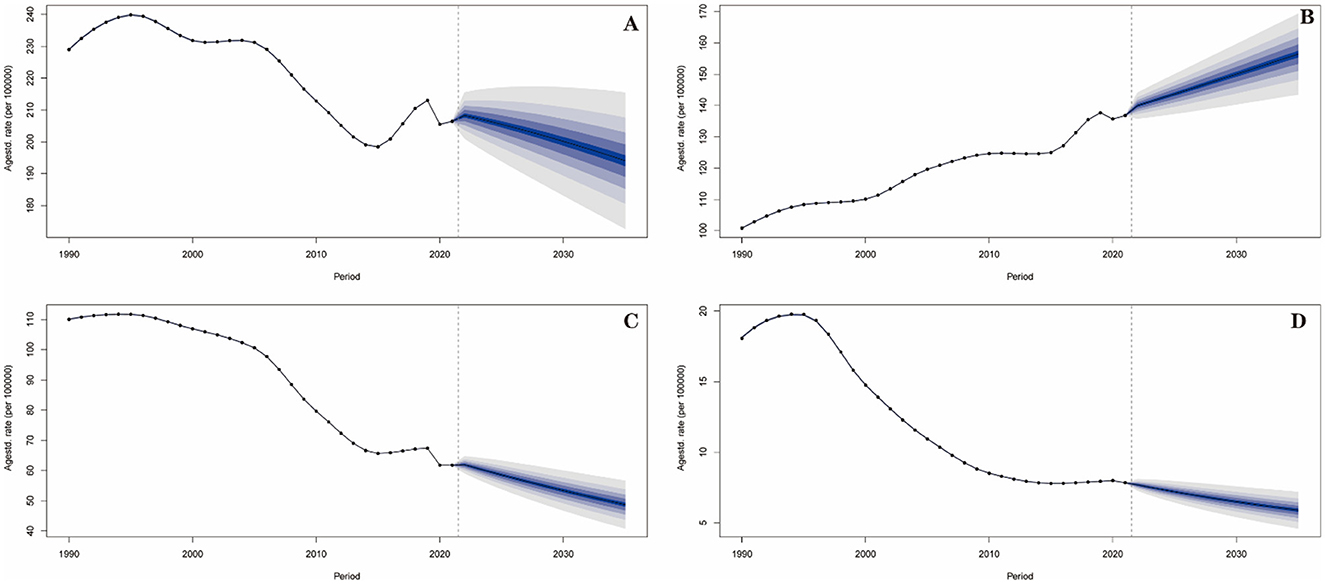
Figure 3. Prediction of incidence trend for stroke and its subtypes in China from 2022 to 2035. (A) Stroke; (B) IS; (C) ICH; (D) SAH.
For IS, ASIR will increase by 11.7% (from 139.98/100,000 to 156.44/100,000, 95% UI: 141.07–171.81); ASPR will increase by 5.2% (from 1,042.21/100,000 to 1,096.55/100,000, 95% UI: 1,032.43–1,160.67), becoming the dominant subtype by 2035.
For ICH and SAH, ASIR will decrease continuously (ICH: 21.3% decrease, from 61.89/100,000 to 48.71/100,000; SAH: 23.3% decrease, from 7.69/100,000 to 5.90/100,000); ASMR of SAH will drop to 2.20/100,000 (from 4.41/100,000 in 2022), a 49.9% reduction. All subtypes, the ASMR and ASDR are predicted to decline, with SAH showing the steepest mortality reduction.
4 Discussion
Our study reveals a paradox in China's stroke burden over three decades: while total stroke mortality (ASMR, EAPC = −1.92) and DALYs (ASDR, EAPC = −2.05) declined significantly, ischemic stroke (IS) incidence (ASIR, EAPC = 0.94) and prevalence (ASPR, EAPC = 1.02) rose sharply. This phenomenon may be related to the fact that the aging of Chinese population has intensified the process of atherosclerosis (12) and the prevalence of metabolic syndrome has increased the risk of IS (13, 14). The IS ASIR increased by 35.72% from 100.05/100,000 in 1990 to 135.79/100,000 in 2021, with an accelerated rise after 2014 (APC = 1.619%). This time window coincides with China's adult diabetes prevalence exceeding 12.8% (15), as diabetes promotes atherosclerosis-a potential pathogenesis of IS.
In addition, there is a significant scissors gap between the prevalence and mortality of stroke in China. The ASPR of stroke has been continuously rising (EAPC = 0.34%), while the ASMR has significantly decreased (EAPC = −1.92%), forming a striking “survivor cumulative effect”. The emergence of this phenomenon may be related to the establishment of China's Stroke Treatment Centers and Stroke Emergency Maps. As of December 2020, a total of 154 cities in China have launched Stroke Emergency Maps, and 1,917 hospitals have joined the construction of Stroke Emergency Maps (16). In other words, the improvement in the acute-stage treatment level achieved through the construction of Stroke Emergency Maps, is hypothesized to be a key driver behind the reduction in stroke mortality in China. While, the secondary prevention of stroke in China may be insufficient, leading to an increase in recurrence and disability rates (17, 18).
The long-term decline and slight recent fluctuation in ischemic stroke (IS) incidence may be related to multiple epidemiological and healthcare system factors. The overall downward trend is mainly attributed to the popularization of hypertension screening and treatment, improved lipid management, and the implementation of tobacco control policies. The increased accessibility of primary healthcare and antihypertensive treatment for middle-aged and elderly populations has played a crucial role in reducing stroke risk. However, the slight rebound observed since 2015 may be associated with population aging and improved diagnostic rates via imaging techniques, particularly the widespread application of magnetic resonance imaging (MRI) in urban areas, which has enhanced the detection of stroke cases. Meanwhile, the persistent presence of metabolic risk factors such as obesity, diabetes, and dyslipidemia may have partially offset the benefits of previous prevention and control measures. The interaction of these factors suggests that to sustain the effectiveness of stroke prevention and control, it is necessary to strengthen comprehensive cardiovascular risk management and lifestyle interventions.
The dramatic declines in intracerebral hemorrhage (ICH) and subarachnoid hemorrhage (SAH) burdens are temporally associated with improved hypertension control efforts in China. Although the hypertension control rate in China remains low, targeted interventions have reduced severe, uncontrolled hypertension, the primary cause of ICH/SAH. Notably, the 2019–2021 rebound in ICH ASPR may reflect delayed diagnosis during this period, requiring further regional data verification.
Our study demonstrate that males bear a heavier stroke burden than females, with distinct gender-specific risk profiles-findings critical for precision prevention. In 2021, male stroke ASIR was 41.6% higher than females, and male IS ASIR was 36.9% higher than females. The gender gap widened over time: male IS ASIR increased by 42.99% during 1990–2021, nearly 1.7 times that of females (25.95%). This disparity is driven by male-specific behavioral risks: the PAF of smoking for males (26.82%) is 7.8 times that of females (3.42%), which was demonstrated in other studies that the smoking rate among Chinese men is significantly higher than that among women (19, 20). Nicotine exacerbates endothelial damage via α7-nAChR receptors (21), accelerating IS pathogenesis. Females, however, face unique risks tied to diet and environment. Our study shows that females have higher secondhand smoke PAF (7.25% vs. male 3.89%) and household air pollution PAF (6.53% vs. male 4.85%). These differences likely reflect gendered lifestyle patterns: females are more likely to prepare high-sodium home-cooked meals and have longer indoor exposure to air pollution. On the other hand, women have a significant protective effect of estrogen, and estrogen inhibits atherosclerosis by upregulating eNOS expression (22). Additionally, the negative PAFs, such as red meat intake for ICH/SAH (−9.58%, −11.08%) may stem from confounding factors, for example, the accessibility of high-quality medical resources associated with high income among individuals with red meat intake, and the uncertainty in relative risk (RR) estimation. These negative PAFs do not imply a protective effect of red meat, instead, they should be interpreted cautiously in conjunction with the Chinese Residents' Dietary Guidelines (2022).
In the analysis of risk factors, high systolic blood pressure is the primary risk factor for stroke-related DALYs in China. A survey conducted throughout China from 2012 to 2015 revealed that the awareness rate of hypertension in China was 46.9%, while the control rate for hypertension was only 15.3%, which was much lower than that of developed countries (23). This indicates that the construction of the hypertension management network urgently needs to be strengthened. Among the three subtypes, high LDL cholesterol ranked as the second risk factors for IS-related DALYs. This might be closely related to the atherosclerotic pathological mechanism of IS (24). A meta-analysis that included 41 original studies indicated that the prevalence, awareness rate, treatment rate and control rate of dyslipidemia among Chinese adults were 42.1%, 18.2%, 11.6% and 5.4% respectively (25), suggesting that it is necessary to enhance lipid screening and the standardized use of lipid-lowering drugs. Furthermore, smoking has the second contribution to stroke-related DALYs for male in China. While, among the burden of stroke for female, diet high in sodium has replaced smoking to rank among the top three. Therefore, when formulating prevention and control strategies, it is necessary to adopt differentiated measures for different genders: for men, smoking control should be prioritized. While for women, intervention on dietary sodium intake should be emphasized, especially in some regions where the consumption of pickled foods is high.
The prediction also highlights a critical challenge that IS burden will rise despite overall stroke reduction, demanding proactive strategy adjustments. By 2035, total stroke ASMR is projected to decrease by 28.3%, and ASDR by 25.6%, a trend that can be accelerated by strengthening existing hypertension management. However, IS presents a major threat: its ASIR will increase by 11.7% and ASPR by 5.2%. To counter this, we propose integrating LDL cholesterol screening into annual physical exams and promoting polypharmacy for high-risk IS patients. In contrast, ICH and SAH burdens are projected to decline further (ICH ASIR: −21.3%, SAH ASIR: −23.3%), which can be sustained by expanding hypertension outreach in rural areas and scaling aneurysm screening for high-risk groups. The 49.9% reduction in SAH ASMR is particularly promising, likely driven by improved neurosurgical care.
Our study has several limitations. Firstly, all burden and PAF estimates are derived from GBD 2021 models, and their accuracy is inherently dependent on the quality of input data and the underlying model assumptions. Data sparsity issues may exist in some regions of China, particularly in rural areas, which could affect the precision of subtype- and gender-specific estimates. Despite provincial heterogeneity, the national-level results remain valid for guiding overarching national stroke prevention and control policies. The national policies targeting universal risk factors will benefit all regions, even if local implementation requires adjustments. China's national stroke prevention strategy focuses on standardized management of potential risk factors and universal access to stroke care, goals that are best informed by national-level trends, and provincial variations can be addressed through targeted local adaptations of national policies. Secondly, this study was conducted only at the national level and could not reveal substantial inter-provincial or urban-rural disparities. China's stroke burden exhibits significant geographical heterogeneity, and national-level averages may mask certain high-burden “hotspot” regions, thereby limiting the development of targeted intervention policies. Thirdly, our projections are based on historical trends and do not account for potential future major policy reforms, breakthroughs in medical technology, or public health events (such as emerging pandemics), all of which could alter the future trajectory of stroke. A further limitation pertains to the generalizability of the relative risk (RR) estimates. The RR values utilized in calculating PAFs were primarily derived from global or mixed-population meta-analyses and epidemiological studies as part of the GBD framework. Applying these RRs directly to the Chinese population may introduce bias, particularly for risk factors where exposure patterns, genetic background, cultural contexts, and behavioral nuances differ significantly. For instance, the composition of diets (e.g., specific types of red meat or sodium sources), smoking habits (e.g., cigarette types, inhalation patterns), and their interactions with other local factors might not be fully captured by global estimates. Consequently, the magnitude of the PAFs for such risk factors, diet high in red meat, sodium, or smoking, should be interpreted with caution, as they may not precisely reflect the attributable burden within the specific context of China. In the future, updating RR parameters based on Chinese local cohorts or prospective studies will help further improve the accuracy of PAF estimates.
5 Conclusions
The burden of stroke in China is characterized by an overall decrease, with divergent trends across subtypes, and significant gender disparities. High systolic blood pressure remains the potential risk factor, while IS's rising burden and gender-specific risks demand targeted interventions. The future strategies should prioritize: (1) scaling up hypertension control to sustain ICH/SAH mortality reduction; (2) strengthening IS prevention via LDL cholesterol management and smoking cessation; (3) gender-tailored measures (e.g., female sodium reduction, male alcohol control). These steps will be critical to mitigating the future stroke burden in China.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found here: https://vizhub.healthdata.org/gbd-results/.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent from the patients/participants or patients/participants legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Author contributions
QW: Data curation, Formal analysis, Project administration, Methodology, Writing – review & editing, Investigation, Conceptualization, Writing – original draft. JX: Funding acquisition, Resources, Writing – review & editing, Formal analysis, Writing – original draft, Investigation, Conceptualization, Data curation. JZ: Software, Conceptualization, Methodology, Writing – original draft, Formal analysis. JT: Writing – original draft, Software, Data curation, Investigation. ZW: Writing – original draft, Resources, Methodology. DW: Data curation, Methodology, Writing – review & editing. ZZ: Conceptualization, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The work was supported by Tianjin Municipal Health Commission's Research Project on Integrated Traditional Chinese and Western Medicine (2025066).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2025.1687411/full#supplementary-material
Abbreviations
GBD, Global Burden of Disease; ASIR, age-standardized incidence rate; ASPR, age-standardized prevalence rate; ASMR, age-standardized mortality rate; ASDR, age-standardized disability-adjusted life years rate; EAPC, estimated annual percentage change; IS, ischemic Stroke; ICH, intracerebral hemorrhage; SAH, subarachnoid hemorrhage; PAF, population attributable fraction; DALYs, disability-adjusted life years; ICD-10, international classification of diseases, 10th revision; WHO, World Health Organization; GATHER, guidelines for accurate and transparent health estimates reporting; RR, relative risk; YLLs, years of life lost; YLDs, years lived with disability; BAPC, Bayesian age-period-cohort; INLA, integrated nested laplace approximations; PSRF, potential scale reduction factor; LDL, low-density lipoprotein; CI, confidence interval; UI, uncertainty interval.
References
1. Feigin VL, Brainin M, Norrving B, Martins SO, Pandian J, Lindsay P, et al. World stroke organization: global stroke fact sheet 2025. Int J Stroke. (2025) 20:132–44. doi: 10.1177/17474930241308142
2. GBD 2021 Stroke Risk Factor Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet Neurol. (2024) 23:973–1003. doi: 10.1016/S1474-4422(24)00369-7
3. He Q, Wang W, Zhang Y, Xiong Y, Tao C, ma L, et al. Global, Regional, and national burden of stroke, 1990-2021: a systematic analysis for global burden of disease 2021. Stroke. (2024) 55:2815–24. doi: 10.1161/STROKEAHA.124.048033
4. Ye Y, Zhu YT, Zhang JC, Zhang H-L, Fan R-W, Jin Y-X, et al. Burden and attributable risk factors of ischemic stroke in China from 1990 to 2019: an analysis from the Global Burden of Disease Study 2019. Front Neurol. (2023) 14:1216777. doi: 10.3389/fneur.2023.1216777
5. Ma Q, Li R, Wang L, Yin P, Wang Y, Yan C, et al. Temporal trend and attributable risk factors of stroke burden in China, 1990–2019: an analysis for the Global Burden of Disease Study 2019. Lancet Public Health. (2021) 6:e897–906. doi: 10.1016/S2468-2667(21)00228-0
6. GBD 2021 Diseases and Injuries Collaborators. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. (2024) 403:2133–61. doi: 10.1016/S0140-6736(24)00757-8
7. Stevens GA, Alkema L, Black RE, Boerma JT, Collins GS, Ezzati M, et al. Guidelines for accurate and transparent health estimates reporting: the GATHER statement. Epidemiol Serv Saude. (2017) 26:215–22. doi: 10.1016/S0140-6736(16)30388-9
8. GBD 2019 Demographics Collaborators. Global age-sex-specific fertility, mortality, healthy life expectancy (HALE), and population estimates in 204 countries and territories, 1950–2019: a comprehensive demographic analysis for the Global Burden of Disease Study 2019. Lancet. (2020) 396:1160–203. doi: 10.1016/S0140-6736(20)30977-6
9. Kuang Z, Wang J, Liu K, Wu J, Ge Y, Zhu G, et al. Global, regional, and national burden of tracheal, bronchus, and lung cancer and its risk factors from 1990 to 2021: findings from the global burden of disease study 2021. EClinicalMedicine. (2024) 75:102804. doi: 10.1016/j.eclinm.2024.102804
10. Cao G, Liu J, Liu M. Global, regional, and national incidence and mortality of neonatal preterm birth, 1990–2019. JAMA Pediatr. (2022) 176:787–96. doi: 10.1001/jamapediatrics.2022.1622
11. Riebler A, Held L. Projecting the future burden of cancer: Bayesian age-period-cohort analysis with integrated nested Laplace approximations. Biom J. (2017) 59:531–49. doi: 10.1002/bimj.201500263
12. Luo Y, Su B, Zheng X. Trends and challenges for population and health during population aging - China, 2015–2050. China CDC Weekly. (2021) 3:593–8. doi: 10.46234/ccdcw2021.158
13. Liu C, Yang X, Chen C. Correlation between metabolic syndrome and intracranial versus extracranial arteriosclerosis among Chinese patients with stroke. Iran J Public Health. (2019) 48:1997–2006. doi: 10.18502/ijph.v48i11.3518
14. Wu S, Wu B, Liu M, Chen Z, Wang W, Anderson CS, et al. Stroke in China: advances and challenges in epidemiology, prevention, and management. Lancet Neurol. (2019) 18:394–405. doi: 10.1016/S1474-4422(18)30500-3
15. Li Y, Teng D, Shi X, Qin G, Qin Y, Quan H, et al. Prevalence of diabetes recorded in mainland China using 2018 diagnostic criteria from the American Diabetes Association: national cross sectional study. BMJ. (2020) 369:m997. doi: 10.1136/bmj.m997
16. Stroke Stroke Report of prevention and treatment, Group TiCW. Brief report on stroke prevention and treatment in China, 2021. Chin J Cerebrovasc Dis. (2023) 20:783–93. doi: 10.3969/j.issn.1672-5921.2023.11.009 (In Chinese).
17. Chen Y, Wright N, Guo Y, Turnbull I, Kartsonaki C, Yang L, et al. Mortality and recurrent vascular events after first incident stroke: a 9-year community-based study of 0·5 million Chinese adults. Lancet Global Health. (2020) 8:e580–e90. doi: 10.1016/S2214-109X(20)30069-3
18. Stroke Stroke Report of prevention and treatment, Group TiCW. Brief report on stroke prevention and treatment in China, 2020. Chin J Cerebrovasc Dis. (2022) 19:136–44. doi: 10.3969/j.issn.1672-5921.2022.02.011 (In Chinese).
19. Sansone N, Yong HH, Li L, Jiang Y, Fong GT, et al. Perceived acceptability of female smoking in China. Tob Control. (2015) 24:iv48-54. doi: 10.1136/tobaccocontrol-2015-052380
20. Li Q, Hsia J, Yang G. Prevalence of smoking in China in 2010. N Engl J Med. (2011) 364:2469–70. doi: 10.1056/NEJMc1102459
21. Qin W, Zhang L, Li Z, Xiao D, Zhang Y, Zhang H, et al. Endothelial to mesenchymal transition contributes to nicotine-induced atherosclerosis. Theranostics. (2020) 10:5276–89. doi: 10.7150/thno.42470
22. Novella S, Dantas AP, Segarra G, Medina P, Hermenegildo C. Vascular aging in women: is estrogen the fountain of youth? Front Physiol. (2012) 3:165. doi: 10.3389/fphys.2012.00165
23. Wang Z, Chen Z, Zhang L, Wang X, Hao G, Zhang Z, et al. Status of hypertension in China: results from the China hypertension survey, 2012–2015. Circulation. (2018) 137:2344–56. doi: 10.1161/CIRCULATIONAHA.117.032380
24. Joint Committee For Guideline Revision. 2016 Chinese guidelines for the management of dyslipidemia in adults. J Geriatr Cardiol. (2018) 15:1–29. doi: 10.11909/j.issn.1671-5411.2018.01.011
Keywords: stroke, China, Global Burden of Disease Study 2021, subtype-specific, gender difference
Citation: Wang Q, Xu J, Zhang J, Tan J, Wang Z, Wang D and Zhou Z (2025) Subtype and gender-differentiated burden of stroke in China (1990–2021): attributable risk factors and future projections based on the Global Burden of Disease Study 2021. Front. Nutr. 12:1687411. doi: 10.3389/fnut.2025.1687411
Received: 17 August 2025; Accepted: 27 October 2025;
Published: 19 November 2025.
Edited by:
Mariagiovanna Cantone, Gaspare Rodolico Hospital, ItalyReviewed by:
Yang Liu, Fudan University, ChinaKamalesh Tayade, All India Institute of Medical Sciences, India
Copyright © 2025 Wang, Xu, Zhang, Tan, Wang, Wang and Zhou. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhen Zhou, emhvdXpoZW43NjgxQDEyNi5jb20=
†These authors share first authorship