 Jean S. R. Kouame1,2*†
Jean S. R. Kouame1,2*† Ella W. R. Compaore1,3
Ella W. R. Compaore1,3 Sonia Blaney4Estelle A. Bambara2Issaka Ouedraogo5Hamidou Sidibe6
Sonia Blaney4Estelle A. Bambara2Issaka Ouedraogo5Hamidou Sidibe6 Mamoudou H. Dicko1
Mamoudou H. Dicko1- 1Laboratory of Biochemistry, Biotechnology, Food Technology and Nutrition (LABIOTAN), Department of Biochemistry-Microbiology, University Joseph KI-ZERBO (UJKZ), Ouagadougou, Burkina Faso
- 2Direction de la Nutrition, Ministère de la Santé, Ouagadougou, Burkina Faso
- 3Secrétariat Technique Chargé de la Multisectorialité Pour la Nutrition (ST-NUT), Ministère de la Santé, Ouagadougou, Burkina Faso
- 4School of Nutrition Faculty of Agricultural and Food Sciences, Université Laval, Québec, QC, Canada
- 5Department of Agricultural and Food Statistics, Ministry of Agriculture, Ouagadougou, Burkina Faso
- 6Davycas International, Ouagadougou, Burkina Faso
Introduction: Food insecurity is a major challenge in many developing countries and may impede the achievement of Sustainable Development Goal 2 (SDG2). Nearly 15% of Burkina Faso’s population is facing food insecurity. In 2021, 21.6% of children under the age of five (U5) were stunted. This rate remains high. This study aimed to investigate the relationship between Global Acute Malnutrition (GAM) and socio-demographic, economic, and household dietary factors among U5 children in the Sanguié Province in Burkina Faso.
Methods: The method used is based on a quantitative cross-sectional study using primary data on food and nutritional security for 237 children under the age of 5 from 150 households. Data analysis was carried out sequentially: a first univariate descriptive stage was used to characterize the variables studied, with a prevalence of MAG [11.4% (7.35–15.44)], which is higher than the 10% alert threshold set by the WHO; this stage is followed by a bivariate analysis to explore their associations. Finally, a multiple correspondence analysis (MCA) was carried out to identify the independent factors associated with acute malnutrition because of its ability to study complex relationships between variables and to represent their structure in the form of factorial spaces.
Results and discussion: Findings indicate that malnutrition is associated with high household food expenditure; medium dietary diversity; a medium/high demographic dependency ratio; the absence of toilets; and food reserves that cover less than 6 months. These findings highlight the need to strengthen food security by fostering household economic development and to ensure optimal access to improved sanitation.
1 Introduction
Food insecurity refers to the lack of regular access, both in quantity and quality, for sufficient, diverse, and nutritious food necessary for proper physical and cognitive development, as well as for maintaining an active and healthy lifestyle (1). Food insecurity is one of the underlying determinants of malnutrition, as it directly impacts individuals’ food intake (2). It currently poses a significant challenge to many developing countries, particularly those committed to achieving Sustainable Development Goal 2.1/2.2 (SDG 2.1/2.2), which aims to end hunger, achieve food security, improve nutrition, and promote sustainable agricultural practices (3).
Available data show that food insecurity issues are critical and threaten public health worldwide. They particularly affect rural populations and the nutritional status of vulnerable groups, especially children under 5 years of age. Malnutrition among children under 5 years has many well-documented consequences: it limits physical and mental health, thereby compromising their well-being and work capacity (4, 5). Yet, child nutrition remains a major public health priority due to its direct link with infant morbidity and mortality; nearly 45–59% of deaths in this age group in low and middle-income countries are attributable to undernutrition (6, 7). At this age and also during the prenatal period, optimal nutrition is crucial for their physical growth and cognitive development, and any deficiency can have irreversible effects. Conversely, good nutrition strengthens the immune system and promotes cognitive development (8–12, 47). Malnutrition, whether acute, chronic, or linked to specific deficiencies, is a complex, multifactorial phenomenon. It results not only from a lack of food but also from the interaction of several structural, socio-economic, health and environmental dimensions (13, 14). With this in mind, the United Nations has proclaimed the period 2016–2025 as the Decade of Nutrition (15).
In sub-Saharan Africa, despite a relative increase in agricultural production, there is still little diversity in household food consumption (16). Regular access to a diversified diet, in sufficient quantity and quality, is a fundamental determinant of child health (17). Smith and Haddad (18) established a positive relationship between household food security and child nutritional status.
Burkina Faso, a landlocked Sahelian country in West Africa, has a population of around 22 million, nearly 80% of whom depend directly on agriculture for their livelihood. This mainly rain-fed sector contributes around a third of the country’s GDP and food security (19). However, agricultural productivity remains low due to dependence upon rainfall, poor mechanization, and soil degradation. Socio-economically, poverty and food insecurity persist, particularly in rural areas, against a backdrop of rapid population growth and increased vulnerability to climate change (20). Strengthening the resilience of agricultural systems, diversifying production, and adding value to local products are essential levers for sustainably improving the country’s food security and socio-economic development (21).
However, in Burkina Faso, child malnutrition remains a major public health problem, with high prevalence of stunting, wasting, and underweight. Agricultural data and nutritional indicators for the last 5 years in Sanguié province, Central West Region (Burkina Faso) were compared with those for the region as a whole and for the three other provinces (Table 1). The analysis revealed a significantly poorer nutritional situation in Sanguié, reflecting increased food insecurity and nutritional vulnerability compared to the other provinces in the region (22–25). While the causes of malnutrition are multifactorial, access and consumption of nutritious food at the household level are considered fundamental determinants (26). However, the precise link between household food consumption patterns and individual child nutritional status remains insufficiently explored in the Burkinabe context (27).
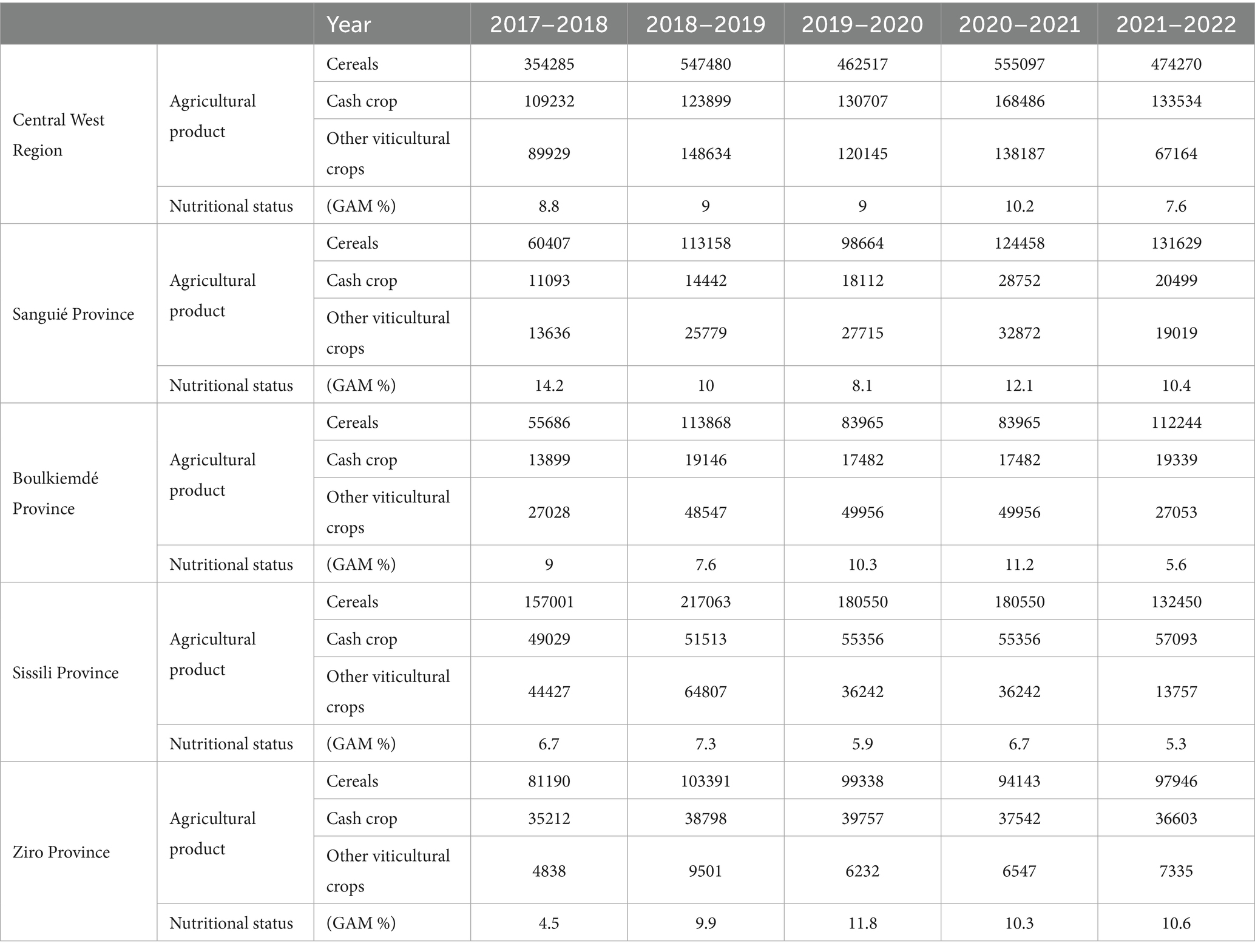
Table 1. Comparison of agricultural and nutritional data from Sanguié and other provinces in the Center-West Region of the country.
This relationship has not yet been carried out, nor has it been shown how it is mediated by socioeconomic factors (e.g., head of household level of education, household size and the household food diversity). Therefore, this study aims to identify statistical associations between household food security indicators and wasting (global acute malnutrition) in children aged 6–59 months in the Sanguié province of Burkina Faso.
As a result, we expect global acute malnutrition in children aged 6–59 months to be significantly associated with factors related to household food security. These results would enable the identification of the main predictive factors of infant malnutrition, prioritizing the relative influence of household food consumption in relation to other determinants, such as maternal education, access to drinking water, or health.
They will be used to design nutritional interventions, enabling resources to be targeted more effectively and decision-makers to improve program planning and policies.
2 Methods
2.1 Type of study
It is a quantitative and cross-sectional study based on primary data from a food and nutrition security survey.
2.2 Study site
Between 2018 and 2021, although the nutritional status (with regard to MAG) of children aged under 5 years living in the province of Sanguié has declined from 14.2 to 12.1% in 2021 (22, 25), still with such prevalence of GAM, it shows a high public health problem according to the World Health Organization (WHO) definition (https://www.who.int/data/nutrition/nlis/info/malnutrition-in-children).
The Sanguié Province, a predominantly rural locality of Burkina Faso, has been selected. Agriculture is the main source of livelihood for households, with high exposure to climate hazards and seasonal food shortages.
2.3 Sampling
• The sampling frame used was that of the National Institute of Statistics and Demography (INSD), drawn from the 2019 General Population and Housing Census (RGPH) of Burkina Faso, updated with the village as the primary unit. Villages within the province were selected randomly through systematic sampling with a probability proportional to size (number of households).
The sampling, as described in the first and second stages, is associated with an inclusion probability for each household. The inverse of these inclusion probabilities, in accordance with Horvitz and Thompson (48), constitutes the weighting coefficients used to obtain unbiased estimators. These weighting coefficients were used to extrapolate the results when calculating indicators for all households in the province (number of households, total, etc.).
The household sample size in the Sanguié province, taking into account a non-response rate r , was determined using the following formula (28):
In this formula, the prevalence “p” was 12.1% [9.6–15.2], the desired precision was 10%, and α, the significance level, was p = 0.05. The multiplier coefficient Deff refers to the survey effect, which was set at 1.5.
When, for a given province, the number of households obtained does not reach 150, this number is adjusted to be increased to 150 in order to account for specific factors related to nutritional status. This adjustment aims to ensure a sufficient number of observations in each province to estimate the indicators accurately.
In the case of primary units, a fixed number of 10 households per village was selected. It is then possible to calculate the number of villages for the province as follows:
On this basis, a first stage of sampling consisted of randomly selecting 15 villages throughout the Sanguié province, then, within each of these villages, 10 households were also randomly selected. Sampling was carried out at the household level. A total of 150 households were selected, and all children aged 6–59 months residing in these households were eligible to participate in the study.
2.3.1 Characteristics of the target population
• Children aged 6–59 months, permanent resident in selected households.
• Location: Urban and rural environment, Sanguié province (Burkina Faso).
2.3.1.1 Selection criteria for children surveyed in the household
2.3.1.1.1 Inclusion criteria
Mandatory conditions for participation.
• Be aged between 6 and 59 months (or the day before the birthday) at the time of recruitment.
• Permanent residence in the selected household.
• Informed consent signed by parent or legal guardian.
2.3.1.1.2 Exclusion criteria
Conditions preventing participation.
• Children with severe congenital malformations that could distort measurements.
• Child suffering from a severe acute illness at the time of the survey (requiring immediate hospitalization).
• Child whose guardian is unable to give informed consent or answer questions.
2.3.1.2 Sampling methodology
• Sampling unit: Household.
2.3.1.2.1 Sample size
A sample of 237 children aged 6–59 months was targeted based on a cluster survey of 150 households.
The clearly defined methodology is a randomized two-stage survey to ensure representativeness.
2.3.1.2.2 Survey period
Data collection took place between February and March 2022.
2.3.2 Observations
2.3.2.1 Anthropometric measurements
• Weight (kg), calibrated electronic scale (precision 100 g) with a SECA battery-operated electronic scale for weighing children under 5, with an accuracy of 100 g. All children were weighed in the nude.
• Height/length (cm), recumbent length for <24 months, standing height for ≥24 months (accuracy 1 mm or 0.1 cm), with a SHORR height board.
• Brachial perimeter (BP): Measured at the left mid-arm with MUAC tape (standard MUAC tape), reading at 1 mm.
• Bilateral foot edema (presence/absence) digital pressure test.
• Derived calculations: Z-score for WHZ, HAZ, WAZ (WHO 2006 standards), and lean/acute indicators.
2.3.2.2 Measurement of household food security variables
• Economic and food variables: Food expenditure class, total food stock duration class, food diversity score, HHS class, food consumption class, food insecurity category (obtained from the household questionnaire).
• Household characteristics: Level of education of head of household, occupation of head of household, number of people in household, number of children under 5 in the household, type of sanitation, dependency ratio (obtained from the household questionnaire).
2.3.3 Data applications
• Estimating prevalence: acute malnutrition, chronic malnutrition, and underweight.
• Establish the link between the nutritional status of children aged 6–59 months and household food security variables: determine predictive indicators to inform decision-makers.
The study adopted a cross-sectional approach based on Standardized Monitoring and Assessment of Relief and Transitions (SMART). This methodology enables a quantitative assessment of the nutritional situation and food security. Data collection was based on a standardized observation protocol, incorporating structured questionnaires validated by technical authorities, as well as precise anthropometric measurements (weight, height, and brachial perimeter), carried out using instruments calibrated according to World Health Organization recommendations (WHO, 2006). This approach aims to guarantee the reliability, comparability, and reproducibility of the data collected on the nutritional status of children aged 6 to 59 months, and on the food security conditions of the households surveyed.
2.4 Data collection tools
Data collection was carried out using digital tablets equipped with the CsPro collection application. The following tools were used:
• Digital tablets;
• List of villages;
• List of households to be investigated.
2.5 Data collection
Data collection for this survey was carried out in February 2022 using a standardized methodology. The survey protocol was implemented by a joint team from the Ministries of Agriculture and Health, enabling a multi-sectoral approach.
Primary data collection was carried out over a period of 14 days by trained interviewers, using face-to-face interviews assisted by mobile data collection tools. This approach enabled direct digital capture and real-time quality control.
To guarantee data reliability, a rigorous protocol for selecting and training field staff was implemented. Twelve interviewers were recruited, with at least a high school diploma and previous field survey experience. These interviewers were divided into four three-person teams. Preliminary training, lasting five days, covered:
• Expertise in Standardized Monitoring and Assessment of Relief and Transitions (SMART) methodology for nutritional surveys.
• Standardized anthropometric measurement techniques.
• Collection of food security and nutrition indicators.
• Specific use of digital data collection tools developed for the study. All tools and procedures have been pre-tested.
Each surveyor was equipped with a tablet on which a data collection application was installed. This mobile collection application was developed on CsPro.
2.6 Data analysis
Following the fieldwork phase, the data were processed and then imported into Stata (statistical software) for tabulation and analysis.
The final database was weighted by calculating weighting coefficients according to the sampling design. All indicators resulting from the analysis are calculated with a 95% confidence threshold.
Data processing was performed using SPSS 25 for descriptive statistics and STATA 18 for modelling.
2.6.1 Statistical and descriptive analysis
Table 2 summarizes and briefly describes the variables used in the study, which are organized into several thematic categories. Each variable is accompanied by its label and modalities.
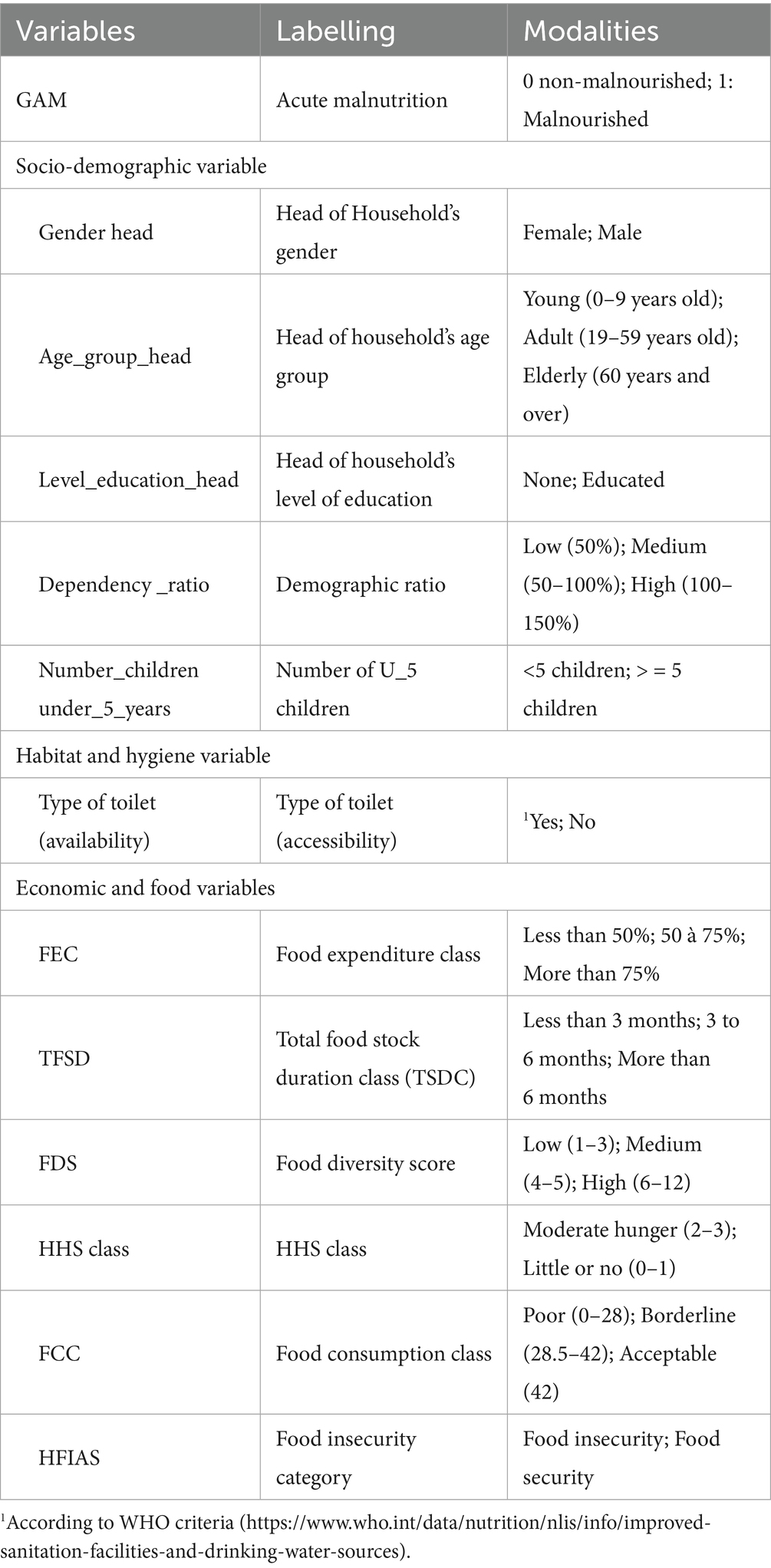
Table 2. Description of the study variables.
2.6.1.1 Dependent variable
Global Acute Malnutrition (GAM): weight/height < −2 SD of standard values or MUAC between 115 mm and <125 mm or the presence of edema is the dependent variable in this study; it is used to assess the impact of food security factors.
2.6.1.2 Explanatory variables (influential factors)
These variables are grouped as follows.
2.6.1.2.1 Socio-demographic variables
Gender of the head of household: This refers to the gender (male or female) of the person identified as the head of the household, that is, the person who makes the main economic, social, and dietary decisions.
Age of the head of household: The age, in completed years, of the main household manager.
Dependency ratio: It is the ratio between the dependent population (people under 15 and over 64) and the active population (people aged 15 to 64) of the household.
Educational level of head of household: Highest level of formal education attained by the head of household (illiterate, primary, secondary, higher, etc.).
Number of children under 5 in the household: It is the total number of children under 5 living in the household at the time of the survey.
Habitat and hygiene variable (Restroom access only): The proportion of households with functional, safe, and hygienic access to sanitation facilities, whether private, shared, or public (29).
2.6.1.2.2 Food-access related variables
Food expenditure class (FEC): It represents the proportion of total household income spent on food over a given period (usually a week or a month).
Total food stock duration class (TSDC): This indicator measures the length of time a household’s food reserves can cover its needs without new supplies.
Household food diversity score (HFDS): It assesses the number of different food groups consumed by the household over a reference period (often 24 h).
There are generally 12 food groups (cereals; roots and tubers; vegetables; fruit; meat; eggs; fish and seafood; pulses, nuts, and seeds; dairy products; oil and fat; sugar and sweet products; and condiments and beverages). Dietary diversity is a simple and reliable indicator of a household’s degree of food security, in relation to food availability, access, and use (30, 31).
HDDS=Number of food groups consumed by the household over 24 h.
Score HDDS is low (1–3); medium (4–5); and high (6–12).
Household Hunger Scale (HHS) is a standardized indicator widely used to measure the severity of hunger and food insecurity at the household level.
It was developed by the FANTA Project (Food and Nutrition Technical Assistance Project) in collaboration with the World Food Programme (WFP) and USAID.
Household food consumption score (HFCS) was developed by the WFP, and it combines dietary diversity, frequency of consumption, and the nutritional importance of different food groups. Each food group is weighted according to its nutritional value (e.g., protein, energy, and micronutrients).
Food security: Household food security was investigated using the Household Food Insecurity Access Scale (HFIAS), a standardized methodology developed by USAID/FANTA to measure households’ access to food, i.e., their level of food insecurity related to access, using a questionnaire with nine basic questions.
2.6.2 Univariate descriptive analysis
Univariate descriptive analysis examines the distribution of the variables in the study, in particular their distribution, frequency, and main characteristics. In this research, it is used to summarize the data, highlight central trends and dispersion, and is an essential preliminary step before any bivariate or multivariate analysis.
2.6.3 Bivariate analysis
Bivariate analyses were used to assess associations between the dependent and independent variables to identify factors potentially linked to acute malnutrition.
The chi-square (χ2) test was used to assess the presence of a statistically significant relationship between each independent variable and acute malnutrition.
The significance of the associations will be assessed at the threshold of 5%.
2.6.4 Multivariate analysis
To identify the factors associated with acute malnutrition, we use a multivariate analysis method that allows for the simultaneous examination of the effects of multiple variables on this condition. To this end, Multiple Correspondence Analysis (MCA) is a particularly suitable statistical tool.
This method highlights the interrelationships between different categorical variables, thus facilitating the detection of groupings based on their statistical proximity (32). It also makes it possible to visualize the relative position of the modalities with respect to each other in a factorial space, thus revealing the underlying structures of the data. This approach enables the extraction of a smaller number of composite dimensions while preserving most of the information contained in the original variables.
3 Results
3.1 Characteristic of the population
Tables 3, 4 present the socio-economic, demographic, and nutritional data of the sample. Table 3 shows a relatively high prevalence of GAM (11.4%), which is above the WHO alert threshold of 10% and indicates a high public health problem. In Table 4, households are mainly headed by men, accounting for 94.9%. Looking at the age range of the household head, adults account for approximately 70%, indicating their predominance. The results also indicate that the majority of household heads have not received any formal education. The dependency ratio is predominantly low to moderate.
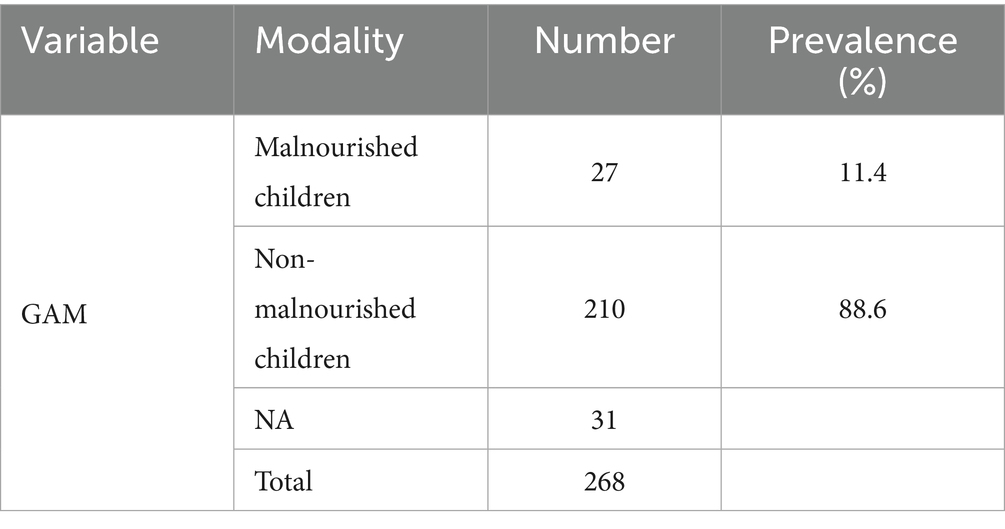
Table 3. GAM representation (n = 237).
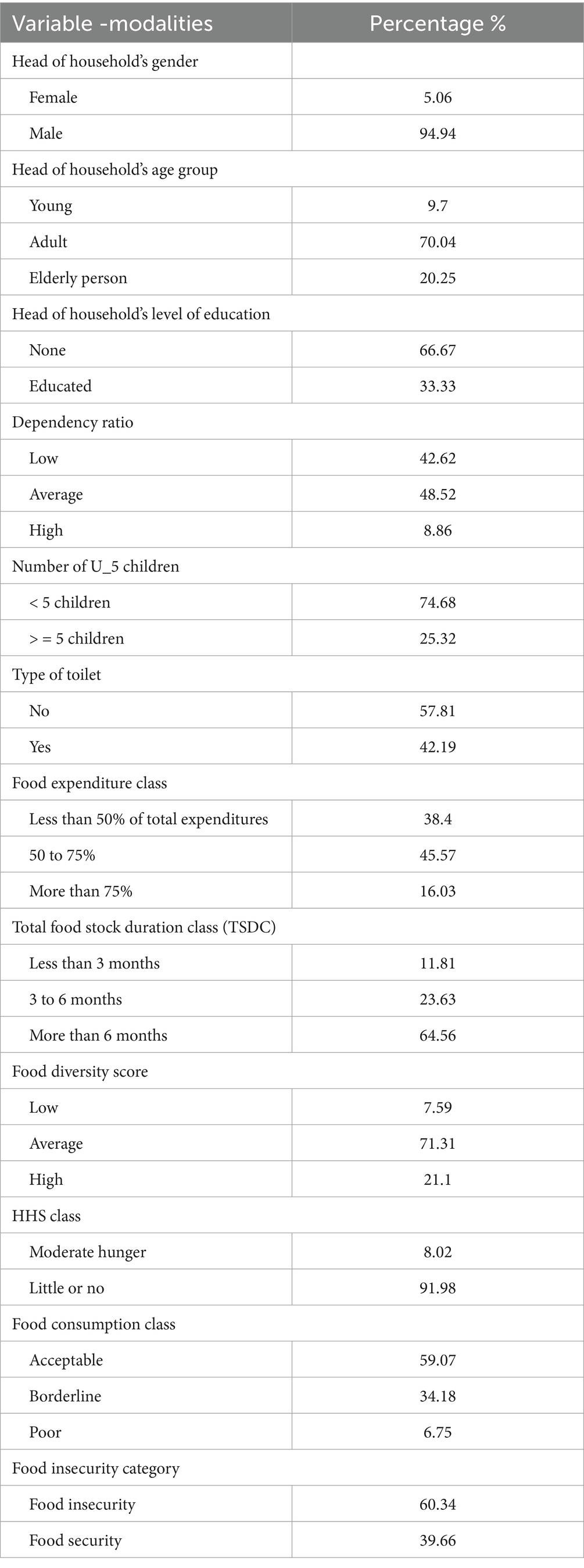
Table 4. Distribution of the food security variables of the study (n = 150).
Data show that over 45% of households spend more than half their budget on food. Furthermore, more than 60% of households have sufficient food stocks to cover their needs beyond a period of 6 months, indicating a certain degree of self-sufficiency and food security in the medium term. This could explain household dietary diversity (71.31%), which is generally moderate, and more than half of households (59%) have an acceptable level of food consumption. However, over 40% experience borderline or poor consumption levels.
More than 60% of households are food insecure.
3.2 Nutritional status of children under 5
Table 5 highlights the prevalence of malnutrition according to the nutritional indicator and the child’s age. The results show that wasting (an indicator of acute malnutrition) impacts approximately 11.4% of children aged 6 to 59 months, with a 95% confidence interval of [7.35–15.44]. Stunting (low height-for-age), an indicator of chronic malnutrition, increases sharply after 6 months of age, rising from 6.9% among children aged below 6 months to 26.6% among those aged 6–59 months.
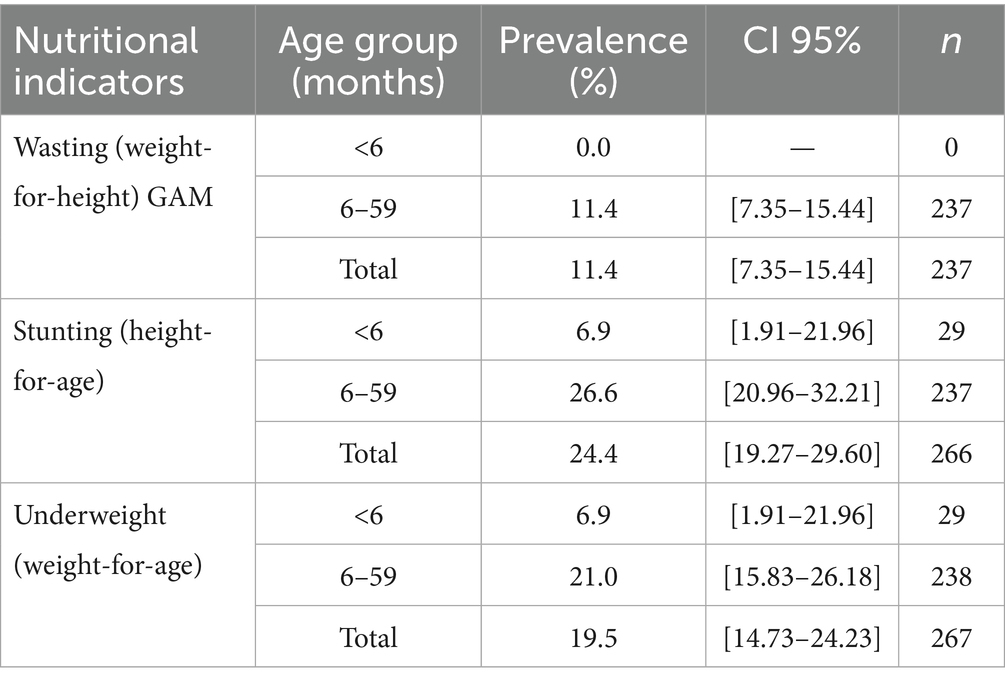
Table 5. Prevalence of malnutrition by nutritional indicators and groups âge (n = 237).
Underweight, which reflects both acute and chronic malnutrition, is also more prevalent among older children, affecting 21.01% of them. In summary, Table 5 clearly indicates an increase in malnutrition with child aging.
3.3 Bivariate analysis
Table 6 presents a bivariate analysis of acute malnutrition in relation to various socio-demographic and nutritional factors.
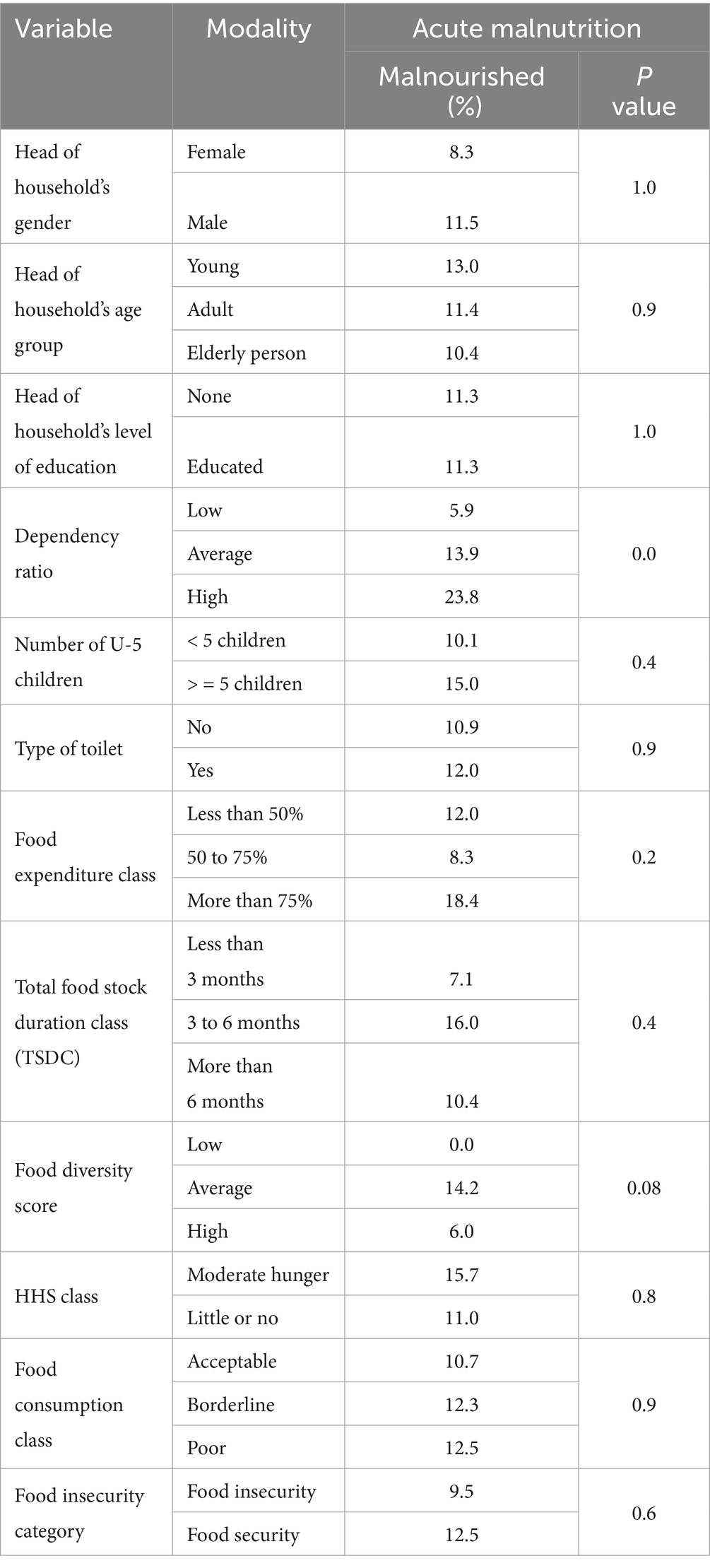
Table 6. Distribution (%) of global acute malnutrition according to food security factors.
Indeed, the results of the bivariate analysis reveal two significant variables: the dependency ratio and the dietary diversity. A higher prevalence of acute malnutrition (23.8%) is noted among children living in households with a high dependency ratio (p = 0.0). This proportion is lower for children living in households with lower (5.9%) and average (13.9%) demographic ratios.
Households with an average dietary diversity show a 14.2% prevalence of children affected by GAM, whereas those with low dietary diversity report no cases of malnutrition (0%) (p = 0.08).
3.4 Multivariate analysis
The statistical method Multiple Correspondence Analysis (MCA) was used to analyze the link between certain household food security variables and the GAM. It is based on a graphical representation (Figure 1; Table 7) in which the variable modalities are projected into a reduced-dimensional space.
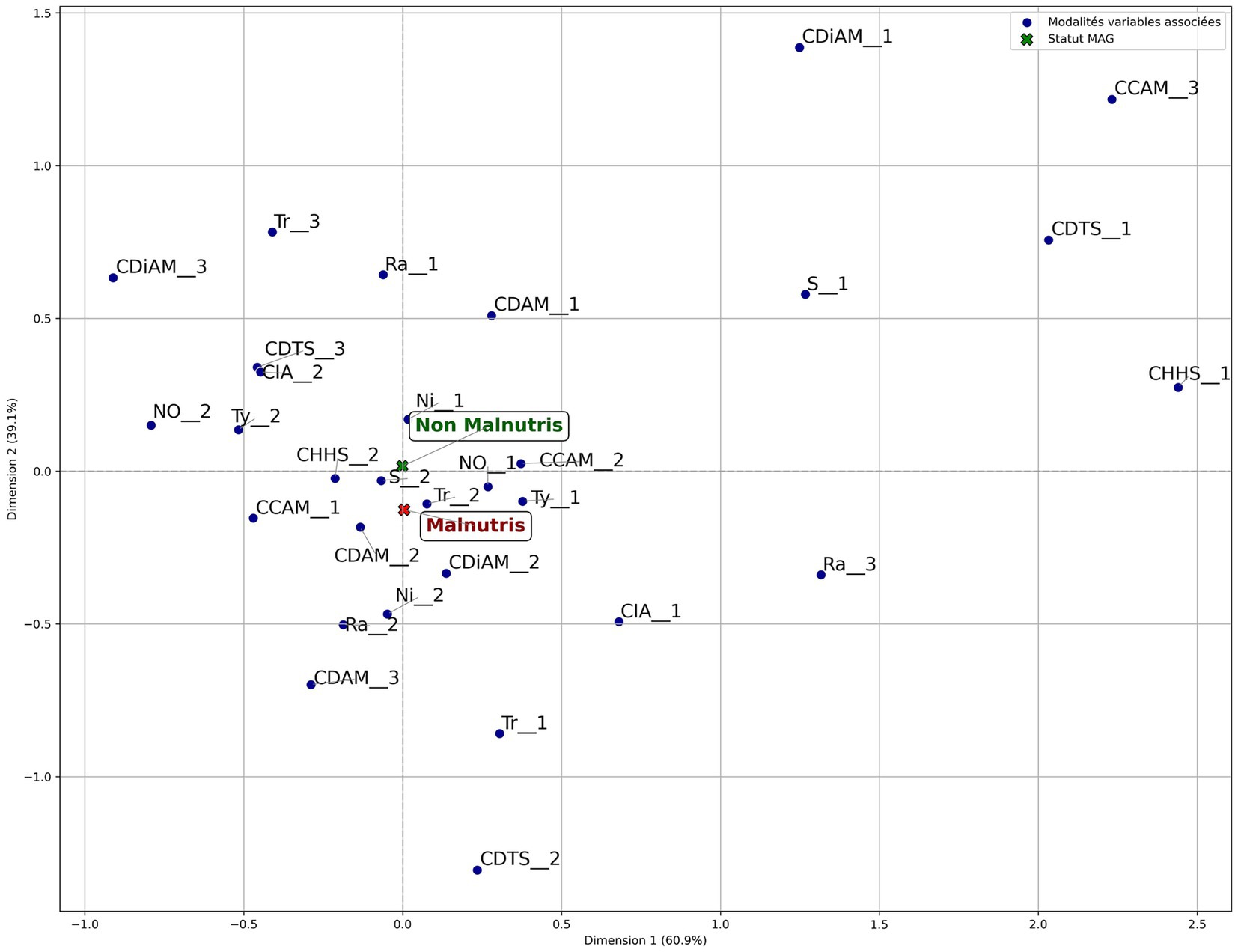
Figure 1. Projection of food security and nutritional status variables for children aged 6–59 months (MCA).
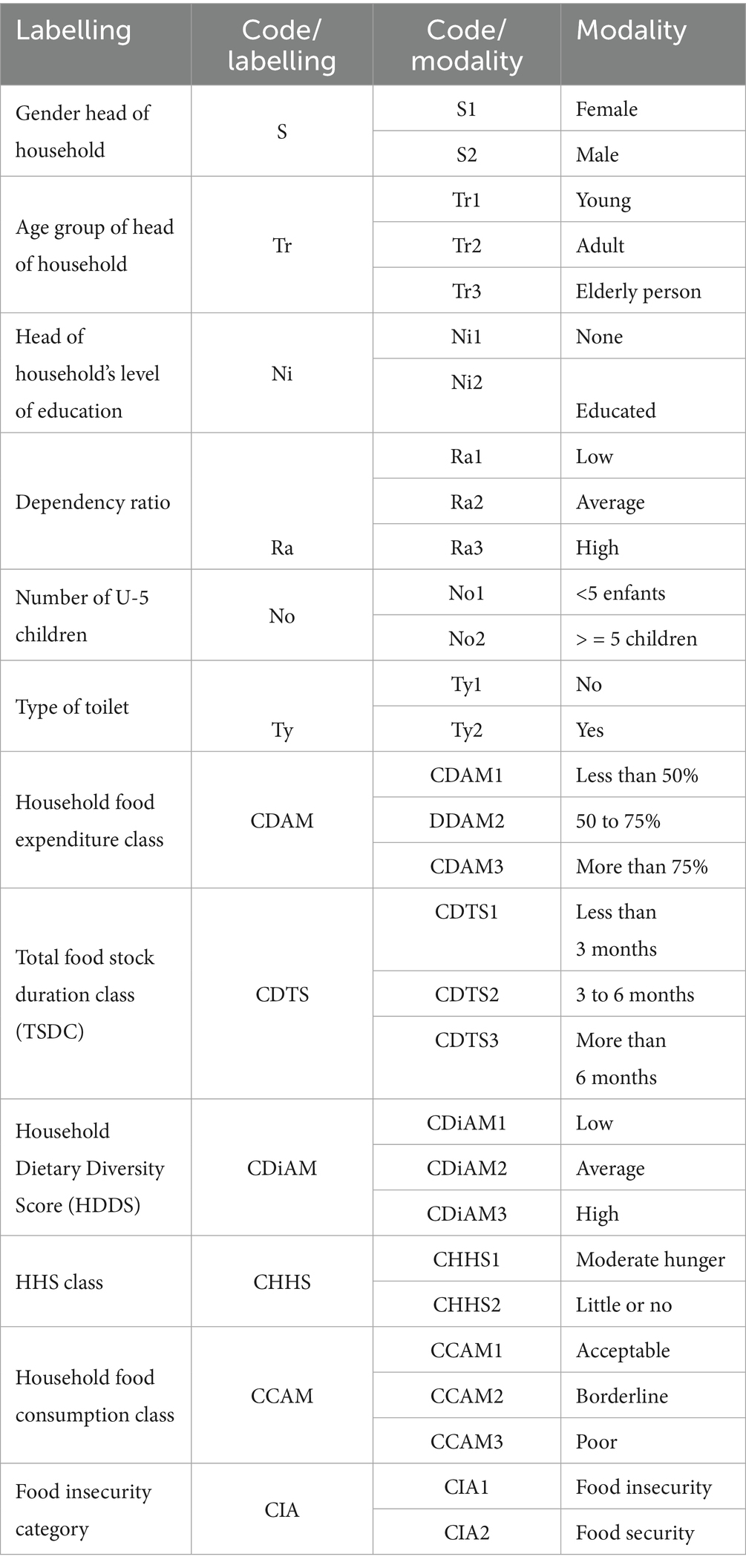
Table 7. Codification of indicators in Figure 1.
3.4.1 Modalities significantly associated with acute malnutrition
The MCA of this article is made according to the analysis methodology proposed by Moschidis et al. (33). The analysis of the factorial plan shows that the first axis (Horizontal) explains 61.3% of the variations observed. It accounts for most of the inertia (variance). It could represent a socio-economic or nutritional gradient, contrasting households with malnourished children with those with non-malnourished children. Analysis of the projected plan reveals that malnutrition is present in households with the following characteristics.
3.4.1.1 Dependency ratio (Ra)
• Modalities involved: medium and high dependency ratios:
A statistically significant link was found between a higher dependency ratio and a greater prevalence of acute malnutrition. Acute malnutrition affected 13.91% of households with an average dependency ratio (p = 0.03) and jumped to 23.81% in those with a high ratio (p = 0.03).
3.4.1.2 Household dietary diversity class (CDiAM)
• Modality involved: average household diversity
The data analysis indicates a trend suggesting that moderate dietary diversity is associated with an increased prevalence of acute malnutrition among children. Indeed, 14.2% of children from households with average dietary diversity are malnourished, while the remaining 85.8% are not.
3.4.1.3 Household food expenditure class (CDAM)
• Modality involved: More than 75% of household food expenditures among households allocating over 75% of their total expenditure to food, 18.42% of children are malnourished, while 81.58% are not.
3.4.1.4 Total food stock duration class (TSDC)
• Modality involved: stock duration between 3 and 6 months
The data show that, in households with food stocks covering 3 to 6 months, 16.07% of children are acutely malnourished, compared to 83.93% who are not malnourished.
3.4.1.5 Type of toilet
• Modality involved: absence of toilet (Ty1)
The survey results show that 10.95% of children in households lacking toilets are acutely malnourished, compared to 89.05% who are not.
3.4.1.6 Food insecurity (CIA)
• Modality involved: food insecurity
In households experiencing food insecurity, as measured by the HFIAS, 9.57% of children are malnourished, while 90.43% are not.
3.4.2 Less significant, but notable variable
• Level of education of the head of household:
While households with an educated head show a higher incidence of malnutrition (11.39%), MCA suggests that this is an indirect link, mediated by other factors.
4 Discussion
This study aims to identify potential determinants associated with acute malnutrition in children aged 6–59 months in the Sanguié province. There is no direct correlation between low household dietary diversity and children’s nutritional status. This result may seem counterintuitive, as we would generally expect higher rates of malnutrition in young children living in households with limited dietary diversity. However, this could be explained by the fact that in households with low dietary diversity, young children often receive special foods, so household dietary diversity does not reflect what is potentially accessible and given to children under 5. It could be that the number of households classified as “low diversity” is too low, reducing the likelihood of observing cases of malnutrition in this specific group. Finally, unobserved factors such as hygiene practices toward young children could influence these results. The results of this study support previous articles, in particular that of Yessoufou et al. (34) and Hasanah et al. (35). These unobserved factors (hygiene practices and health) play a decisive role in the nutritional status and food security of children under the age of five. Inadequate hygiene, particularly the failure to wash hands with soap, the use of contaminated water, or the unhygienic disposal of excreta, encourages the transmission of pathogens responsible for diarrhoeal and parasitic diseases. These conditions lead to malabsorption of nutrients, loss of appetite, and increased energy requirements, compromising the child’s growth and development.
Improving hygiene practices within households, in particular hand-washing with soap, access to safe drinking water, and adequate sanitation, is, therefore, an essential means of breaking the cycle of infection and malnutrition (36). This convergence of results reinforces the hypothesis that low household dietary diversity, reflecting qualitative food insecurity, is a major determinant associated with infant malnutrition (6–59 months), over and above quantitative aspects of food availability alone. With food expenses accounting for over half of total household expenditures, these households face a precarious food security situation that could negatively affect the nutritional status of children under 5. A study conducted by Jean et al. (37) found that roughly 73% of households in the TONPKI region of Côte d’Ivoire allocate 15 to 45% of their income to food expenses, particularly during the lean season when malnutrition rates are high. Furthermore, Zhang et al. (38) research highlights that the sheer amount spent on food by a household is not synonymous with the consumption of quality food. This result, highlighted by the MCA, underscores the importance of balancing food expenditure and overall living conditions in malnutrition prevention strategies.
In the context of this study, the MCA’s finding of a high demographic dependency ratio linked to acute malnutrition in young children suggests that the substantial number of economically dependent individuals compared to the smaller active population within households, could be a contributing factor. However, the high number of children under and over five places pressure on the household, potentially worsening its food security situation (39). This result could be explained by the increased pressure on household resources, including food, within families carrying a high demographic load. The necessity to allocate food and health resources among numerous household members can result in reduced quantity and quality of nutritional intake available to each child. This structural constraint is especially detrimental to the youngest children, who are more nutritionally vulnerable (40). This is confirmed by the demographic burden faced by some sub-Saharan countries, including Burkina Faso, where a disproportionately large young population compared to working adults and high annual birth rates coincide with limited public spending aimed at improving nutrition (41).
The absence of toilets, as observed in this study, is widely recognized as a significant aggravating factor in malnutrition; finally, more than half of households do not have access to toilets, increasing the risk of diarrheal diseases and, consequently, malnutrition among children.
Ademas et al. (42) noted that the high rate of illness and malnutrition among young children (6–59 month) is due to the absence of toilets and inadequate sanitation services. In sub-Saharan Africa, approximately 88–89% of the population lacks access to toilets, contributing to stunting in 28–49% of children under 5 years of age (43). In the municipality of Karimama (northern Benin), a nutritional survey found that 11.9% of children under five suffered from acute malnutrition, while 39% were affected by chronic malnutrition These results were linked to the lack of a healthy environment, characterized by unsafe water sources, poor household waste management, inadequate handwashing practices, and open defecation (44).
A relationship has been observed between households headed by individuals with limited education and the presence of acute malnutrition in children under five. This explains its less significant link when it is correlated with acute malnutrition in the Sanguié Province (45).
Households with food stocks lasting less than six months show higher rates of acute malnutrition. Food stocks are primarily used to meet daily household needs, provide cash flow through sales when necessary, and enhance the availability of agricultural products that boost dietary diversity (46). This highlights the necessity for households to maintain food stocks exceeding 6 months to successfully cope with the lean season, which may reflect a better ability to adapt to seasonal fluctuations in food availability.
Despite the existence of determinants already well documented in the literature, such as dietary diversity and access to sanitation, this study provides recent, contextualized empirical data for the Sanguié province, an area hitherto little explored in terms of nutrition. This regional contribution provides a relevant baseline for guiding local interventions and situating the nutritional situation in Sanguié in relation to other provinces in Burkina Faso. In addition, the combination of multivariate analysis and MCA gives the study a solid methodological foundation, enabling us to highlight the complex interactions between socio-economic factors, food, and nutritional status. This integrated approach represents significant added value for the design and implementation of nutrition policies and programs adapted to the local context.
5 Conclusion
This study examines the links between global acute malnutrition and household socioeconomic and dietary characteristics in Sanguié province, Burkina Faso. MCA has also been used as a method because of its ability to study complex relationships between variables and to represent their structure in the form of factorial spaces. Acute malnutrition is particularly prevalent in households facing a high dependency ratio, with an average dietary diversity, and low food stock (available stocks for less than six months). This is further compounded by a significant food budget weight (over 75% of total household expenses), the lack of basic hygiene infrastructure (toilet), and a high proportion of children under 5 years old within the household. These results confirm that global acute malnutrition is a multifactorial phenomenon, stemming from intricate interactions among food insecurity, precarious socioeconomic conditions, and inadequate health practices.
The fact that most households are headed by uneducated men, coupled with limited financial capacity, may partly account for the persistence of malnutrition in some households.
These results highlight the need for targeted intervention strategies. Interventions integrating improved food availability, nutrition education, and the strengthening of household purchasing power appear to be effective levers for reducing child malnutrition. Approaches combining home fortification with micronutrient powders, the promotion of fortified local foods, dietary diversification, the cultivation of biofortified varieties, and the development of community nutrition gardens are proving particularly promising. In addition, community involvement in the early detection and management of malnutrition, supported by digital technology, as well as the implementation of warning systems, hygiene, and sanitation actions strengthen the nutritional resilience of households. Finally, participatory economic approaches, such as microcredit and community mobilization, help target vulnerable populations. The adoption of these multi-sectoral strategies should be prioritized in order to optimize nutritional gains during the first 1,000 days of life.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
JK: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Visualization, Writing – original draft, Writing – review & editing. EC: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. SB: Formal analysis, Writing – review & editing. EB: Formal analysis, Writing – review & editing. IO: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – review & editing. HS: Data curation, Formal analysis, Methodology, Software, Validation, Writing – review & editing. MD: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
We would like to express our gratitude to Mr. Vincent Naty for his decisive support in accessing documentation from the Burkina Faso Ministry of Agriculture. We would also like to thank Mr. Daouda Sanguisso for his pertinent comments and suggestions, which contributed significantly to the enrichment and improvement of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. UNICEF. The state of food security and nutrition in the world 2023: urbanization, agrifood systems, transformation and healthy diets across the rural-urban continuum.(2023). 2023 p.
2. Betebo, B, Ejajo, T, Alemseged, F, and Massa, D. Household food insecurity and its association with nutritional status of children 6–59 months of age in east Badawacho District, South Ethiopia. J Environ Public Health. (2017) 2017:1–17. doi: 10.1155/2017/6373595
3. FAO, IFAD, UNICEF, WFP, and WHO. The state of food security and nutrition in the world 2025: Safeguarding food security and nutrition through inclusive transformation. Rome: FAO (2025).
4. Elgar, FJ, Pickett, W, Pförtner, T-K, Gariépy, G, Gordon, D, Georgiades, K, et al. Relative food insecurity, mental health and wellbeing in 160 countries. Soc Sci Med. (2021) 268:113556. doi: 10.1016/j.socscimed.2020.113556
5. Gundersen, C, and Ziliak, JP. Food insecurity and health outcomes. Health Aff. (2015) 34:1830–9. doi: 10.1377/hlthaff.2015.0645
6. Madewell, ZJ, Keita, AM, Das, PM-G, Mehta, A, Akelo, V, Oluoch, OB, et al. Contribution of malnutrition to infant and child deaths in sub-Saharan Africa and South Asia. BMJ Glob Health. (2024) 9:e017262. doi: 10.1136/bmjgh-2024-017262
7. Wambua, J, Ali, A, Ukwizabigira, JB, and Kuodi, P. Prevalence and risk factors of under-five mortality due to severe acute malnutrition in Africa: a systematic review and meta-analysis. Syst Rev. (2025) 14:29. doi: 10.1186/s13643-024-02740-9
8. Freijer, K, Tan, SS, Koopmanschap, MA, Meijers, JM, Halfens, RJ, and Nuijten, MJ. The economic costs of disease related malnutrition. Clin Nutr. (2013) 32:136–41. doi: 10.1016/j.clnu.2012.06.009
9. Hoddinott, J, Maluccio, JA, Behrman, JR, Flores, R, and Martorell, R. Effect of a nutrition intervention during early childhood on economic productivity in Guatemalan adults. Lancet. (2008) 371:411–6. doi: 10.1016/S0140-6736(08)60205-6
10. Mahmassani, HA, Switkowski, KM, Scott, TM, Johnson, EJ, Rifas-Shiman, SL, Oken, E, et al. Maternal diet quality during pregnancy and child cognition and behavior in a us cohort. Am J Clin Nutr. (2022) 115:128–41. doi: 10.1093/ajcn/nqab325
11. Perrella, S, Gridneva, Z, Lai, CT, Stinson, L, George, A, Bilston-John, S, et al. Human milk composition promotes optimal infant growth, development and health. Seminars Perinatology. (2021) 45:151380. doi: 10.1016/j.semperi.2020.151380
12. Prado, EL, and Dewey, KG. Nutrition and brain development in early life. Nutr Rev. (2014) 72:267–84. doi: 10.1111/nure.12102
13. Salm, L, Verstraeten, R, Nisbett, N, and Booth, A. Exploring the drivers of malnutrition in West Africa from health and social science perspectives: a comparative methodological review. Methodol Innov. (2021) 14. doi: 10.1177/20597991211051445
14. Wubetie, BY, Tsunekawa, A, Haregeweyn, N, Tsubo, M, Nigussie, Z, Meshesha, TM, et al. Analysis of malnutrition among children under five years across contrasting agroecosystems of Northwest Ethiopia: application of structural equation modeling. Nutrients. (2024) 16:1208. doi: 10.3390/nu16081208
15. Assemblée Mondiale De La Santé (2016). Décennie d’action des Nations Unies pour la nutrition (2016–2025). Décennie d’action des Nations Unies pour la nutrition (2016–2025).
16. Lourme-Ruiz, A., Dury, S., and Martin-Prével, Y. (2016). Une production plus diversifiée et/ou un revenu agricole plus élevé peuvent-ils améliorer la diversité alimentaire des femmes au sein des ménages agricoles? Le cas du Burkina Faso. 2016. Sfer.
17. Organisation Mondiale De La Santé (2023). Alimentation du nourrisson et du jeune enfant. Available online at: https://www.who.int/fr/news-room/fact-sheets/detail/infant-and-young-child-feeding.
18. Smith, LC, and Haddad, L. Reducing child undernutrition: past drivers and priorities for the post-Mdg era. World Dev. (2015) 68:180–204. doi: 10.1016/j.worlddev.2014.11.014
19. Usaid / Climate Centre / Insd (2022). Burkina Faso: Country profile. Economic security & climate fact sheet.” Climate Centre. Profil présentant la vulnérabilité climatique, le rôle de l’agriculture dans l’économie, et les défis agricoles. Sujet: Vulnérabilité climatique pour le Burkina Faso, rôle de l’agriculture dans l’économie, défis agricoles et de résilience.
20. Zanré, KP, and Combary, OS. The heterogeneous effects of climate variability on cotton farming productivity in Burkina Faso. Environ Dev Sustain. (2024) 26:12707–35.
21. Tapsoba-Maré, G., Badolo, M., and Bokonon-Ganta, B. (2021). Agricultural resilience to climate change in Burkina Faso: New methodological tools for innovative approaches. Handbook of Climate Change Management: Research, Leadership, Transformation. Springer.
22. Ministère De La Santé. BF. Enquête Nutritionnelle Nationale: Basée sur la Méthodologie Smart, Burkina Faso-Décembre 2018. Ouagadougou: Direction de la Nutrition (2018).
23. Ministère De La Santé. BF. Enquête Nutritionnelle Nationale: Basée sur la Méthodologie Smart, Burkina Faso-Février 2020. Ouagadougou: Direction de la Nutrition (2019).
24. Ministère De La Santé. BF. Enquête Nutritionnelle Nationale: Basée sur la Méthodologie Smart, Burkina Faso-Décembre 2020. Ouagadougou: Direction de la Nutrition (2020).
25. Ministère De La Santé. BF. Enquête Nutritionnelle Nationale: Basée sur la Méthodologie Smart, Burkina Faso – Décembre 2021. Ouagadougou: Direction de la Nutrition (2021).
26. Ouédraogo, O, Garanet, F, Compaoré, E, Hermann, L, Zoma, LR, Kaboré, S, et al. Prévalence et facteurs associés au retard de croissance chez des écoliers à Dori, Burkina Faso. Sante Publique. (2019) 31:153–63. doi: 10.3917/spub.191.0153
27. Kere, N, Compaore, EWR, Keita, Y, Ouedraogo, DS, Tirogo, S, Bambara, EA, et al. Impact of Iycf practices, as measured by national nutrition surveys from 2018 to 2022, on stunting and under-5 survival in Burkina Faso: a list analysis. Front Nutr. (2024) 11:1504564. doi: 10.3389/fnut.2024.1504564
28. Lwanga, SK, and Lemeshow, S. Sample size determination in health studies. Geneva: World Health Organization (1991). 1 p.
29. Girmay, AM, Weldetinsae, A, Mengesha, SD, Adugna, EA, Alemu, ZA, Wagari, B, et al. Associations of who/Unicef joint monitoring program (Jmp) water, sanitation and hygiene (wash) service ladder service levels and sociodemographic factors with diarrhoeal disease among children under 5 years in Bishoftu town, Ethiopia: a cross-sectional study. BMJ Open. (2023) 13:e071296. doi: 10.1136/bmjopen-2022-071296
30. Kennedy, G, Ballard, T, and Dop, M. Guidelines for measuring household and individual dietary diversity FAO (2011).
31. Swindale, A, and Bilinsky, P. Household dietary diversity score (Hdds) for measurement of household food access: Indicator guide. Washington, DC: Food and Nutrition Technical Assistance Project, Academy for Educational Development (2006). 220 p.
32. Chavent, M. (2015). L’Analyse des Correspondances multiples (ACM). Université de Bordeaux. Consulté à l’adresse. Available online at: https://www.Math.U-Bordeaux.Fr/~machaven/wordpress/wpcontent/uploads/2013/10/Acm.Pdf.
33. Moschidis, S, Markos, A, and Thanopoulos, AC. “Automatic” interpretation of multiple correspondence analysis (Mca) results for nonexpert users, using R programming. Applied Computing Informatics. (2022) doi: 10.1108/ACI-07-2022-0191
34. Yessoufou, G, Ahokpe, M, Behanzin, J, Kountori, R, Senou, M, and Sezan, A. Prevalence de la malnutrition aigue chez les enfants de moins de cinq ans dans la plaine de Pendjari au nordouest du Benin. J Rech Sci L’Université Lomé. (2014) 1
35. Hasanah, A, Kharisma, B, Remi, SS, Adam, AM, and Siregar, AY. Food diversity: its relation to children’s health and consequent economic burden. BMC Public Health. (2024) 24:1155. doi: 10.1186/s12889-024-18530-w
36. World Health Organization. Burden of disease attributable to unsafe drinking-water, sanitation and hygiene, 2019 update. France, à Clermont-Ferrand: World Health Organization (2023).
37. Jean, G, Assunta, AA, and Yolande, K-BC. Les Déterminants De La Malnutrition Dans La Région Du Tonkpi (Côte D’ivoire). Kafoudal La Revue Des Sciences Sociales De L’universite Peleforo Gon Coulibaly. (2019) 129
38. Zhang, B, Wrenn, DH, Joshi, J, and Jaenicke, EC. Housing wealth, food spending, and diet quality: evidence from panel data. Agricultural Resource Economics Review. (2022) 51:517–41. doi: 10.1017/age.2022.12
39. Fentaw, R, Bogale, A, and Abebaw, D. Prevalence of child malnutrition in agro-pastoral households in Afar regional state of Ethiopia. Nutr Res Pract. (2013) 7:122–31. doi: 10.4162/nrp.2013.7.2.122
40. Saif, S, and Anwar, S. Unraveling the south Asian enigma: concurrent manifestations of child anthropometric failures and their determinants in selected south Asian countries. BMC Nutr. (2023) 9:120. doi: 10.1186/s40795-023-00771-4
41. Ndamobissi, R. Les défis sociodémographiques et politiques de la malnutrition des enfants dans les pays d'Afrique du Sahel et de la Corne de l'Afrique. Franche-Comté: Université Bourgogne (2017).
42. Ademas, A, Adane, M, Keleb, A, Berihun, G, and Tesfaw, G. Water, sanitation, and hygiene as a priority intervention for stunting in under-five children in Northwest Ethiopia: a community-based cross-sectional study. Ital J Pediatr. (2021) 47:174. doi: 10.1186/s13052-021-01128-y
43. Akono, RA. Les Etats d’Afrique Subsaharienne à l’épreuve des toilettes publiques: entre crise d’accès, crise d’assainissement, risques et solutions. Revue Francophone du Développement Durable. (2020):33–50.
44. Moucktarou, AA, Janvier, KM, Jean, K, Mariam, EA, Dagui, OB, Albert, SK, et al. Malnutrition en relation avec les pratiques d'approvisionnement en eau, hygiène et assainissement dans la commune de Karimama au Nord Bénin. Int J Innov Appl Stud. (2023) 39:1557–69.
45. Fagbamigbe, AF, Kandala, N-B, and Uthman, OA. Decomposing the educational inequalities in the factors associated with severe acute malnutrition among under-five children in low-and middle-income countries. BMC Public Health. (2020) 20:555. doi: 10.1186/s12889-020-08635-3
46. Marcel, K, Kabirou, S, Mouzoun, S, and Ibouraïma, Y. Gestion des stocks alimentaires dans les communes de Lokossa et de Dogbo au Sud-Benin. Espace Géographique et Société Marocaine. (2022) 1:32.
47. Behrman, JR. The economic rationale for investing in nutrition in developing countries. World Development. (1993) 21:1749–71.
Keywords: global acute malnutrition, food security, multiple correspondence analysis, Sanguié Province, Burkina Faso
Citation: Kouame JSR, Compaore EWR, Blaney S, Bambara EA, Ouedraogo I, Sidibe H and Dicko MH (2025) Links between household food consumption and nutritional status of children aged 6–59 months: a case study in Burkina Faso. Front. Nutr. 12:1696003. doi: 10.3389/fnut.2025.1696003
Edited by:
Elisabete Pinto, Catholic University of Portugal, PortugalReviewed by:
Mona Hashim, University of Sharjah, United Arab EmiratesRaju Bhardwaj, Agriculture University, Jodhpur, India
Copyright © 2025 Kouame, Compaore, Blaney, Bambara, Ouedraogo, Sidibe and Dicko. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jean S. R. Kouame, cm9kcmlndWVfa291YW1lQHVqa3ouYmY=
†ORCID: Jean S. R. Kouame, orcid.org/0009-0003-0188-6587