 Fernanda Mucarzel1
Fernanda Mucarzel1 Patricia Guirado Peláez2Virginia Soria Utrilla3,4,5
Patricia Guirado Peláez2Virginia Soria Utrilla3,4,5 Rocío Fernández Jiménez2,5,6,7
Rocío Fernández Jiménez2,5,6,7 Fiorella Palmas Candia1,8*Francisco José Sánchez Torralvo3,4,5
Fiorella Palmas Candia1,8*Francisco José Sánchez Torralvo3,4,5 Rosa Burgos Peláez1,8,9
Rosa Burgos Peláez1,8,9 José Manuel García Almeida2,5,6,7Gabriel Olveira3,4,5
José Manuel García Almeida2,5,6,7Gabriel Olveira3,4,5- 1Nutrition Support Unit, Endocrinology and Nutrition Department, Hospital Universitari Vall d’Hebron, Barcelona, Spain
- 2Department of Endocrinology and Nutrition, Virgen de la Victoria University Hospital, Málaga, Spain
- 3Department of Endocrinology and Nutrition, Quironsalud Málaga Hospital, Málaga, Spain
- 4Unidad de Gestión Clínica de Endocrinología y Nutrición, Hospital Regional Universitario de Málaga, Málaga, Spain
- 5CIBEROBN, Carlos III Health Institute (ISCIII), University of Málaga, Málaga, Spain
- 6Instituto de Investigación Biomédica de Málaga y Plataforma en Nanomedicina-IBIMA Plataforma BINAND, Málaga, Spain
- 7Department of Medicine and Dermatology, Málaga University, Málaga, Spain
- 8Diabetes and Metabolism Research Unit, Vall d’Hebron Institut de Recerca (VHIR), Barcelona, Spain
- 9Department of Medicine, Universitat Autònoma de Barcelona, Barcelona, Spain
Background: Computed Tomography (CT)-derived analysis of Body Composition (BC) provides detailed phenotyping of skeletal muscle and adipose tissue, offering insight into nutritional and metabolic risk in oncology.
Objective: To characterize sex- and age-specific muscle and adipose tissue phenotypes in patients with colon cancer and describe their patterns across postoperative outcomes.
Methods: Multicentric observational cross-sectional study including Colorectal Cancer (CRC) patients undergoing laparoscopic elective surgery. Preoperative CT scans at L3 were analyzed for muscle and adipose tissue quantity and radiodensity. Differences in BC parameters between patient groups (according to presence of complications, hospital stay and disease stage by sex) were assessed using Student’s t-test (p < 0.05).
Results: 502 CRC patients, predominantly males (62.5%) with a mean age of 68.08 ± 10.62 were included. Sex-specific differences in muscle quality and adipose tissue distribution were observed across postoperative outcomes. In women, lower Subcutaneous Adipose Tissue (SAT) values were observed in those with longer hospital stay and complications (p < 0.001), whereas in men, reduced Skeletal Lean Muscle Radiodensity (p < 0.001) and higher Visceral Adipose Tissue (VAT; p = 0.013) were found in those with adverse outcomes. These differences were independent of BMI and age.
Conclusion: CT-based body composition phenotyping identifies distinct metabolic profiles linked to postoperative risk. Incorporating tissue quality and distribution into nutritional assessment may enhance early identification of vulnerable patients and guide personalized perioperative strategies.
1 Introduction
Body mass index (BMI) is widely used as a surrogate marker of nutritional status in oncology patients, primarily due to its simplicity, accessibility, and established associations with clinical outcomes (1). However, it does not distinguish between fat mass and fat-free mass compartments, and may therefore mask muscle depletion or malnutrition in individuals with a normal or elevated BMI (2). As a result, Body Composition (BC) assessment has emerged as a more accurate approach, providing detailed information on skeletal muscle mass quantity and quality, and, depending on the technique, adipose tissue distribution (3–7).
Malnutrition, as defined by the Global Leadership Initiative on Malnutrition (GLIM) criteria, is diagnosed when at least one phenotypic criterion (weight loss, low BMI or reduced skeletal muscle mass) is present along with one etiological criterion (8). However, universally accepted cutoffs for defining moderate versus severe muscle mass loss –adjusted for sex, age and disease—remain limited (9).
In this context, the concept of sarcopenia, as defined by the European Working Group on Sarcopenia in Older People 2 (EWGSOP2) becomes relevant: it is considered probable when low muscle strength is identified and confirmed when reduced muscle quantity is also demonstrated (10).
Among the types of cancer where Computed Tomography (CT) imaging is systematically used for diagnosis, ColoRectal Cancer (CRC) represents a particularly robust model for BC research in surgical outcomes (11). However, most previous studies have combined patients undergoing laparoscopic and open procedures, which may introduce heterogeneity in postoperative outcomes (12–14).
The routine use of preoperative abdominal CT allows for opportunistic assessment of BC. In particular, CT images at the L3 vertebral level provide highly accurate and reproducible measures not only of tissue quantity but also of radiodensity and distribution, allowing for detailed phenotypic characterization (12, 13).
Low Skeletal Muscle Index (SMI) has been linked to adverse outcomes in multiple types of cancers (14–20). However, proposed cut-offs for CT-derived measurements—such as those by Prado et al. or Martin et al.—are based mainly on muscle indices and mortality risk, and may not fully capture the complexity of perioperative outcomes (19, 21–24).
Most studies to date have not adequately considered the inherent differences in body composition based on sex, age, or tumor stage, limiting the generalizability of the proposed cutoff values. Addressing these shortcomings is essential to ensure that CT-derived parameters, such as low SMI or reduced skeletal muscle radiodensity (SMD), truly reflect clinically meaningful malnutrition, sarcopenia, or myosteatosis in the perioperative setting (25–29).
Sex-related differences in body composition are well established: women generally exhibit higher Subcutaneous Adipose Tissue (SAT), whereas men tend to accumulate more Visceral Adipose Tissue (VAT) and greater absolute muscle mass (30). These distinct phenotypes may modulate inflammatory and metabolic responses and influence surgical recovery, but their clinical significance in homogeneous cohorts of CRC patients remains insufficiently defined. Furthermore, aging is accompanied by progressive declines in both muscle mass and muscle quality, adding another layer of variability to risk stratification (31–33).
Based on these considerations, the present study aimed to characterize sex-specific BC phenotypes in patients with colon cancer undergoing surgery, using CT-derived measurements of muscle and adipose compartments. We further examined differences in these phenotypes according to length of hospital stay as well as the presence of postoperative complications, and explored how age and tumor stage might influence these patterns.
2 Materials and methods
2.1 Study design
This was a multicenter, cross-sectional study conducted in accordance with the Declaration of Helsinki between October 2018 and July 2024 at the Endocrinology and Nutrition services of the Regional University Hospital of Malaga, Virgen de la Victoria Hospital of Malaga, and Vall d’Hebron Hospital of Barcelona. The protocol was approved by the Research Ethics Committee for Medicines of Vall d’Hebron University Hospital on February 29, 2024 (reference PR(AG)489/2021), covering inter-hospital data sharing and retrospective analysis of patient data. Data from 171 patients from Vall d’Hebron Hospital, 123 from Virgen de la Victoria Hospital, and 208 from the Regional University Hospital of Malaga were included. An internal protocol was followed to standardize data collection procedures across centers, ensuring consistency in the methodology and the use of comparable equipment for all assessments.
The sample was considered representative, as patients were consecutively recruited from three tertiary public hospitals with heterogeneous populations. With n = 502, the maximum margin of error for estimating a prevalence (95% CI, p = 0.5) is ±4.4%, ensuring adequate precision. For group comparisons of similar size (≈251 per group), the study has 80% power to detect small-to-moderate differences (Cohen’s d ≈ 0.25, α = 0.05).
2.2 Patient selection
For all three hospitals, eligible participants were adults (≥18 years) with histologically confirmed colorectal cancer (CRC) scheduled for elective laparoscopic surgery, with availability of a diagnostic or staging abdominal CT performed < 30 days prior to surgery. All participants were at risk of malnutrition according to the Malnutrition Universal Screening Tool (MUST) and provided written informed consent.
Ineligibility criteria included urgent or non-laparoscopic procedures, lack of lumbar coverage or partial loss of the analyzable area, and image-quality limitations in the region of interest (e.g., metallic prostheses, beam hardening, attenuation distortion, or excessive noise) precluding reliable body-composition assessment.
2.3 Clinical data collection
Data acquisition was centralized and coordinated by the Vall d’Hebron team to ensure uniform procedures and quality control across centers. All participants underwent medical history, anthropometry, nutritional assessment, and abdominal CT. Oncological variables included tumor location, and cancer stage was assigned according to the American Joint Committee on Cancer (AJCC) staging system version 9 (34).
2.4 Anthropometric and nutritional assessment
The following variables were systematically recorded by trained personnel at each hospital: height in meters, weight in kg, Body Mass Index (BMI) in kg/m2, as well as weight loss in the previous 6 months (%). Fat Free Mass Index in Kg/m2 (FFMI) was assessed by Bioelectrical Impedance Analysis (BIA) in all participating institutions using the same portable device (Akern BIA-101/Nutrilab analyzer, Akern SRL, Pontassieve, Florence, Italy). The technical accuracy of the instrument was verified daily with a precision check provided by the manufacturer. This standardized approach minimized inter-hospital variability and ensured measurement consistency across centers.
Nutritional risk was screened with Malnutrition Universal Screening Tool (MUST) as the first-step screening tool (35). The diagnosis of malnutrition was made following Global Leadership Initiative on Malnutrition (GLIM) criteria (8).
It was estimated that all patients presented at least one etiological criterion, as they had colorectal neoplasia (considered a chronic inflammatory process). For the phenotypic criterion of reduced muscle mass, patients were classified using the Fat-Free Mass Index (FFMI) according to the cutoff points (<17 kg/m2 for men and <15 kg/m2 for women) recommended by the consensus itself as measured by BIA (9).
2.5 CT body composition analysis
To assess skeletal muscle and abdominal adipose tissue area, transverse CT images at the level of the third lumbar vertebra (L3) were analyzed using the FocusedON-BC software Version 2.1. These images were acquired with a multidetector CT scanner and DICOM files were provided by the Radiology Department of the participating hospitals. Tissue segmentation was performed by trained personnel at each center, employing the semi-automated tool integrated within the FocusedON-BC software to identify and quantify body composition compartments.
The abdominal muscle groups analyzed included the psoas, erector spinae, quadratus lumborum, transversus abdominis, external and internal obliques, and rectus abdominis. Adipose tissue was categorized into subcutaneous, visceral, and intermuscular compartments (36, 37).
Unlike conventional CT analysis software, which typically assesses muscle mass without distinguishing between lean muscle mass and intermuscular adipose tissue, FocusedON-BC software allows for segmentation of those tissues, providing a more detailed and precise assessment (Figure 1). However, for comparability with previously published data, both conventional and detailed segmentation approaches were applied in this study.
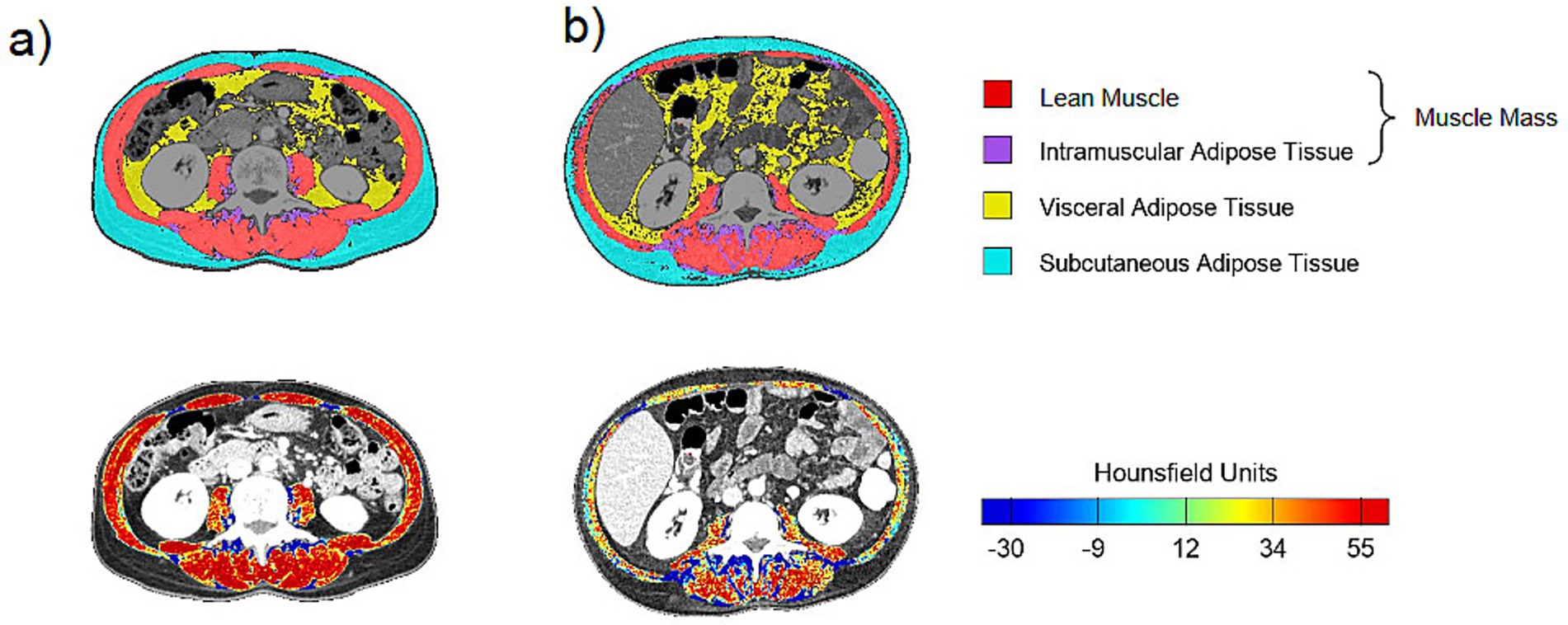
Figure 1. Images extracted from the FocusedON-BC software: patients (a) and (b) presented the same BMI (30.7 kg/m2), but different LMMA percentages (22.84 and 14.25%, respectively) and lean muscle radiodensity (50.61 HU and 34.46 HU, respectively).
The variables recorded included Skeletal Muscle Area (SMA, in cm2 and %), Skeletal Muscle Index (calculated by SMA normalized to the patient’s height squared (cm2/m2), SMI in cm2/m2), Lean Muscle Mass Area (LMMA, in cm2 and %), Lean Muscle Mass Index (LMMI, in cm2/m2), InterMuscular Adipose Tissue area (IMAT, in cm2 and %) and Index (IMATI, in cm2/m2), Visceral Adipose Tissue area (VAT, in cm2 and %) and Index (VATI, in cm2/m2), and, Subcutaneous Adipose Tissue area (SAT, in cm2 and %) and Index (SATI, in cm2/m2).
Tissue quality for muscle mass was assessed based on its radiodensity (D) measured by mean of Hounsfield Units (HU), applying standard radiodensity thresholds: −29 to 150 HU for skeletal muscle mass, −190 to −30 for SAT and −150 to −50 for VAT (24).
2.6 Surgical outcomes
Short-term outcomes comprised length of stay (recorded in days), postoperative complications within 30 days from surgery (presence or absence), and discharge destination. Length of stay was categorized according to previously published criteria (38), with hospitalizations longer than 10 days indicating poorer prognosis and stays shorter than 6 days considered as expected recovery. Postoperative complications were further classified according to the Clavien–Dindo criteria (39). Furthermore, discharge destination was recorded as home, convalescence center, home hospitalization program, or in-hospital death.
Readmission during the 3-month follow-up period and mortality during the 6-month follow-up after discharge were also documented and analyzed to assess long-term surgical outcomes.
2.7 Statistical analysis
Statistical analysis was performed using Python 3.11 (Python Software Foundation).1
Continuous variables are presented as mean ± standard deviation (SD) for normal distributed variables and median ± interquartile range (IR) for non-normal distributed variables. Categorical variables are presented as frequencies and percentages, n (%). Statistical significance was accepted at p < 0.05.
Kolmogorov–Smirnov test was used to assess the normal distribution of the dataset.
Differences between groups were assessed using an independent samples t-test for normally distributed variables, the non-parametric Mann–Whitney U test for non-normally distributed variables and the X2 test for categorical variables.
3 Results
3.1 Study population
A total of 502 patients with Colorectal Cancer (CRC) undergoing elective laparoscopic surgery were included (Table 1). The cohort was predominantly men (63%), with a mean age of 68.08 ± 10.62 years, with no significant sex-related differences (p = 0.457).
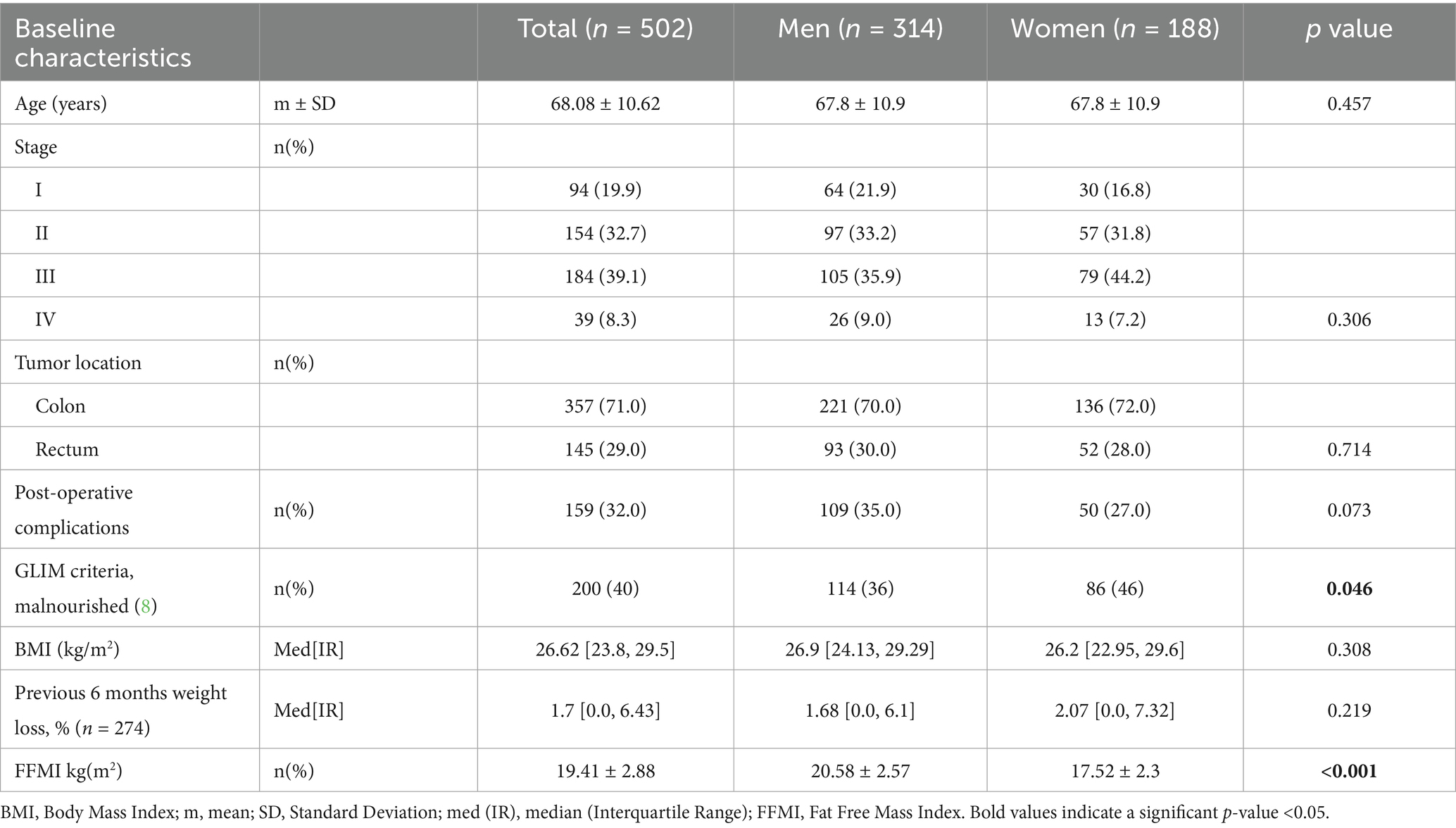
Table 1. General features of the sample.
According to GLIM criteria, 40% presented malnutrition (36% men and 46% women, p = 0.046) despite the average BMI was between the normal range (BMI 26.62 kg/m2 [23.8–29.5]) according to age, without differences by sex (p = 0.308) (38).
Sex-specific differences were observed in the Fat-Free Mass Index (FFMI), with women presenting significantly lower values than men (p < 0.001), as expected according to the cut-off points for low muscle mass. Disease staging was not markedly advanced, with 92% of patients classified as stage ≤3, without differences by sex (p = 0.306).
Overall complication rates were comparable (35% in men vs. 27% in women; p = 0.073), although men appeared to experience a higher incidence of postoperative complications.
Subgroup analyses are presented below, performed as required to address the findings observed.
3.2 Body composition assessment through CT prior to surgery
CT-derived preoperative body composition parameters stratified by sex are shown in Table 2. Distinct sex-related phenotypes were observed.
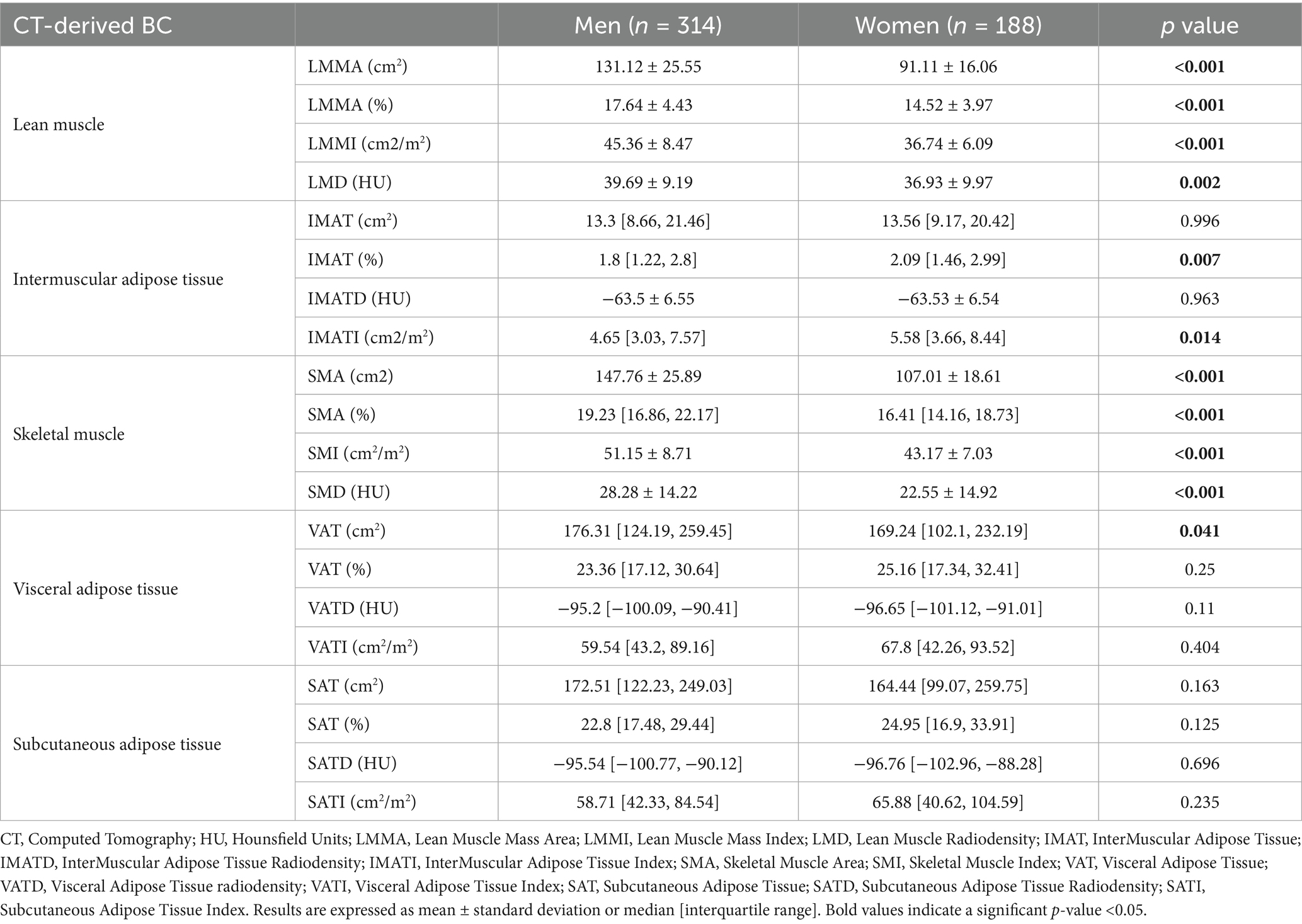
Table 2. CT body composition parameters by sex prior to surgery.
Men exhibited significantly higher absolute and indexed skeletal muscle areas compared with women, including LMMA (131.12 ± 25.55 cm2 vs. 107.01 ± 18.61 cm2, p < 0.001), SMA (147.76 ± 25.89 cm2 vs. 107.01 ± 18.61 cm2, p < 0.001), and their respective indices (LMMI and SMI, both p < 0.001). They also demonstrated higher Lean Muscle Radiodensity (LMD) values (39.69 ± 9.19 HU vs. 36.93 ± 9.97 HU, p = 0.002) as well as Skeletal Muscle Radiodensity (SMD; p < 0.001), indicating better muscle quality at same age (p = 0.457).
In contrast, women showed a higher IMAT percentage compared to men (2.09% vs. 1.80%, p = 0.007) and standardized IMAT index (IMATI) was also greater in women (5.58 cm2/m2 [3.66–8.44] vs. 4.65 cm2/m2 [3.03–7.57], p = 0.014). On the other side, VAT area was higher in men (176.31 cm2 vs. 169.24 cm2; p = 0.041).
Nevertheless, no statistically significant sex differences were observed regarding adipose tissue radiodensity in the studied sample.
3.3 Postoperative outcomes by sex
Postoperative outcomes by sex are further summarized in Table 3.
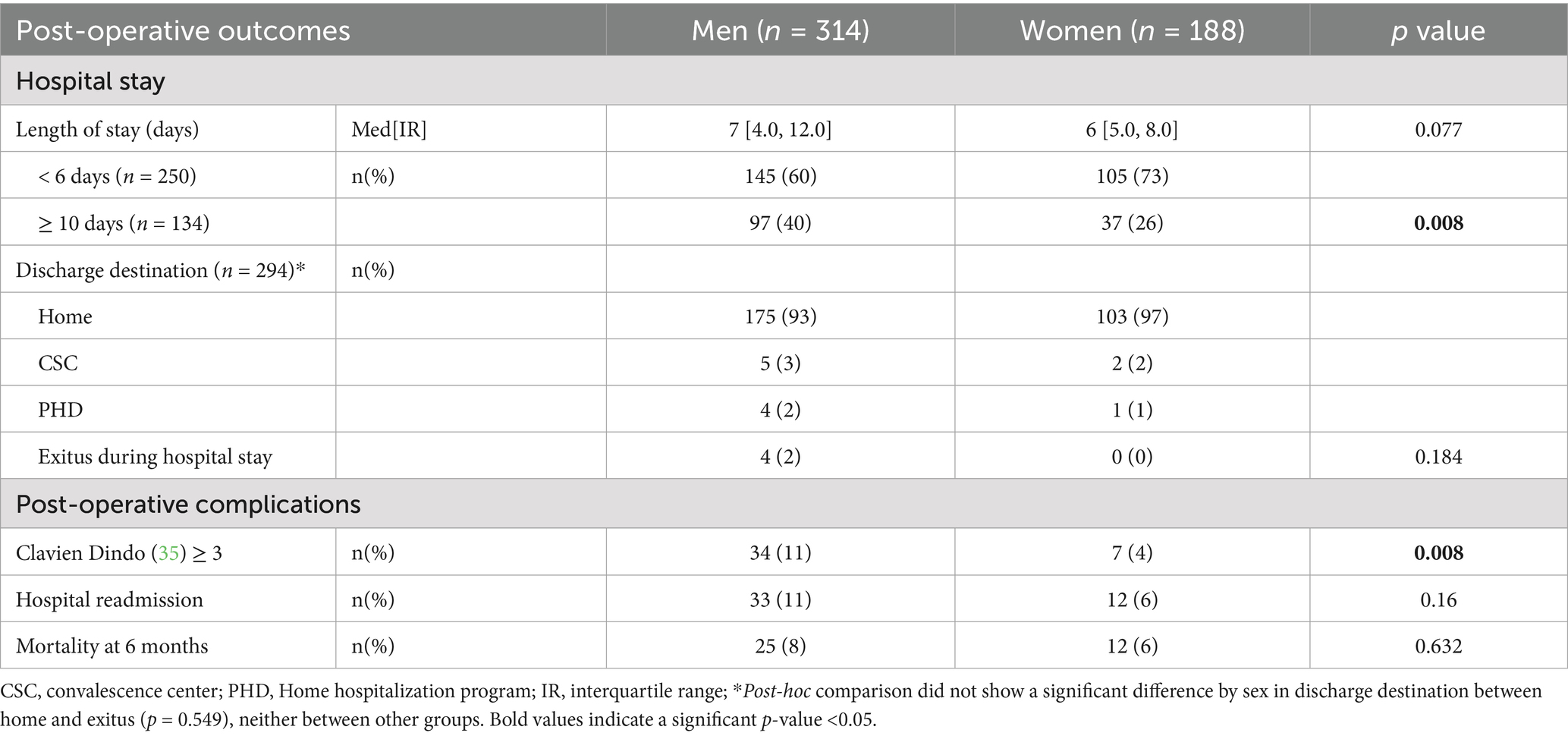
Table 3. Post-operative outcomes by sex.
Median hospital stay was slightly longer in men (7 [4.0–12.0] days) than in women (6 [5.0–8.0] days), although not statistically significant (p = 0.077). However, women were more frequently discharged within < 6 days (73% vs. 60%; p = 0.008) and men more frequently discharged after 10 days (40% vs. 26%; p = 0.008). Discharge destination was predominantly home across sex without significant variation among destinations such as convalescence centers (p = 0.184). Readmission rates were similar across sex (p = 0.16).
Considering that overall complication rates were comparable by sex, (35% in men vs. 27% in women; p = 0.073), major complications (Clavien–Dindo ≥3) were significantly less frequent in women (4% vs. 11%; p = 0.008).
The 6-month postoperative mortality rate in the cohort was 7%, without significant sex-related differences (p = 0.632).
3.4 Body composition and clinical outcomes in men
3.4.1 BC in men considering length of hospital stay
A higher proportion of men experienced prolonged hospital stay (>10 days) compared to women. Therefore, body composition characteristics were further analyzed according to length-of-stay categories (Table 4).
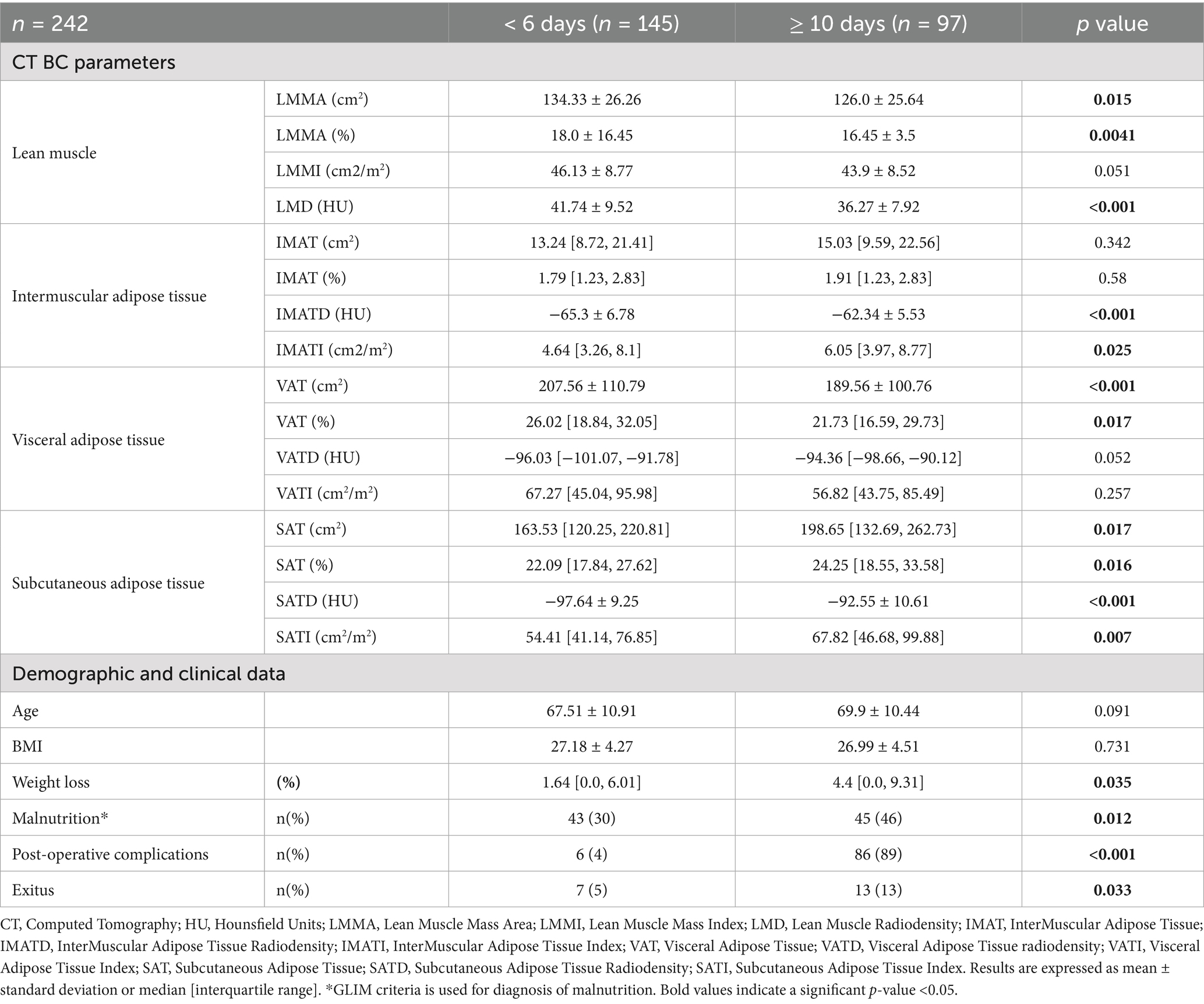
Table 4. Men body composition parameters by CT by hospital stay.
In this subgroup, men with a standard hospital stay (<6 days) consistently showed higher lean mass parameters, including LMMA and radiodensity, compared with those with a prolonged hospital stay (≥10 days), despite having comparable BMI (p = 0.731) and age (p = 0.091).
Visceral adipose tissue (VAT) was higher in men with a standard hospital stay, as indicated by a greater percentage of VAT (p < 0.017). In contrast, subcutaneous adipose tissue (SAT) compartments were increased among men hospitalized for more than 10 days, as reflected by higher SAT, SATD, and SAT values (all p < 0.005).
3.4.2 BC in men considering presence of postoperative complications
Given their higher rate of severe postoperative complications (Clavien Dindo >3), men were further analyzed by complication status (Table 5).
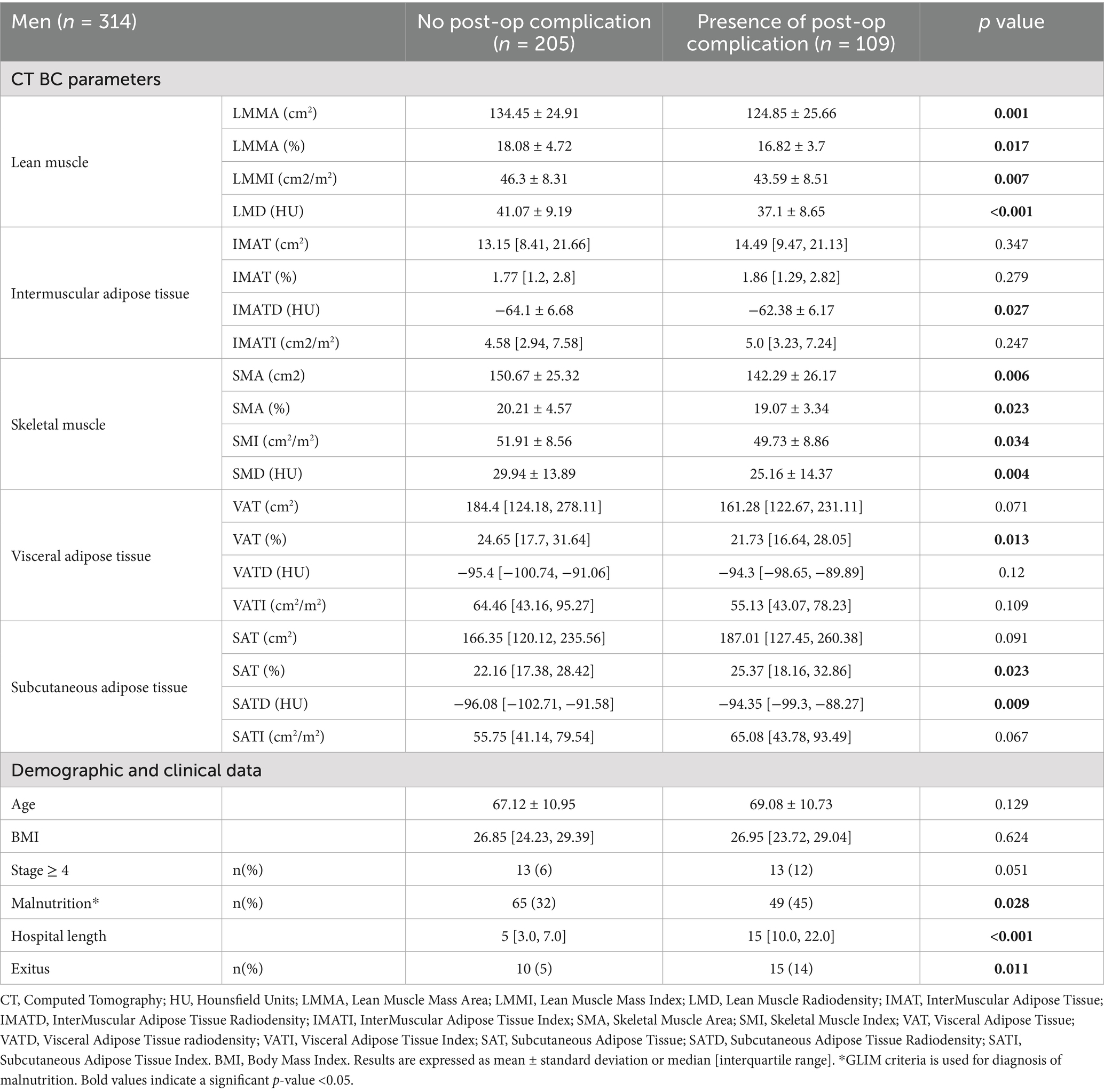
Table 5. Men body composition parameters by CT by presence of post-operative complication.
Those with complications showed significantly lower lean muscle mass (area, index, and radiodensity; all p < 0.01) and less favorable adipose tissue profiles (higher SAT percentage and radiodensity, lower VAT percentage; all p < 0.05).
Despite comparable age and BMI, men with complications had a markedly longer hospital stay (p < 0.001), a higher prevalence of GLIM-defined malnutrition (p = 0.028), and increased 6-month mortality (p = 0.011).
Overall, the body composition patterns observed in men across length-of-stay categories were similar to those seen in men who experienced postoperative complications.
3.4.3 BC in men considering disease stage
Because men who presented postoperative complications included more patients with advanced-stage disease (12% vs. 6%; p = 0.051), body composition was further compared by stage (Table 6).
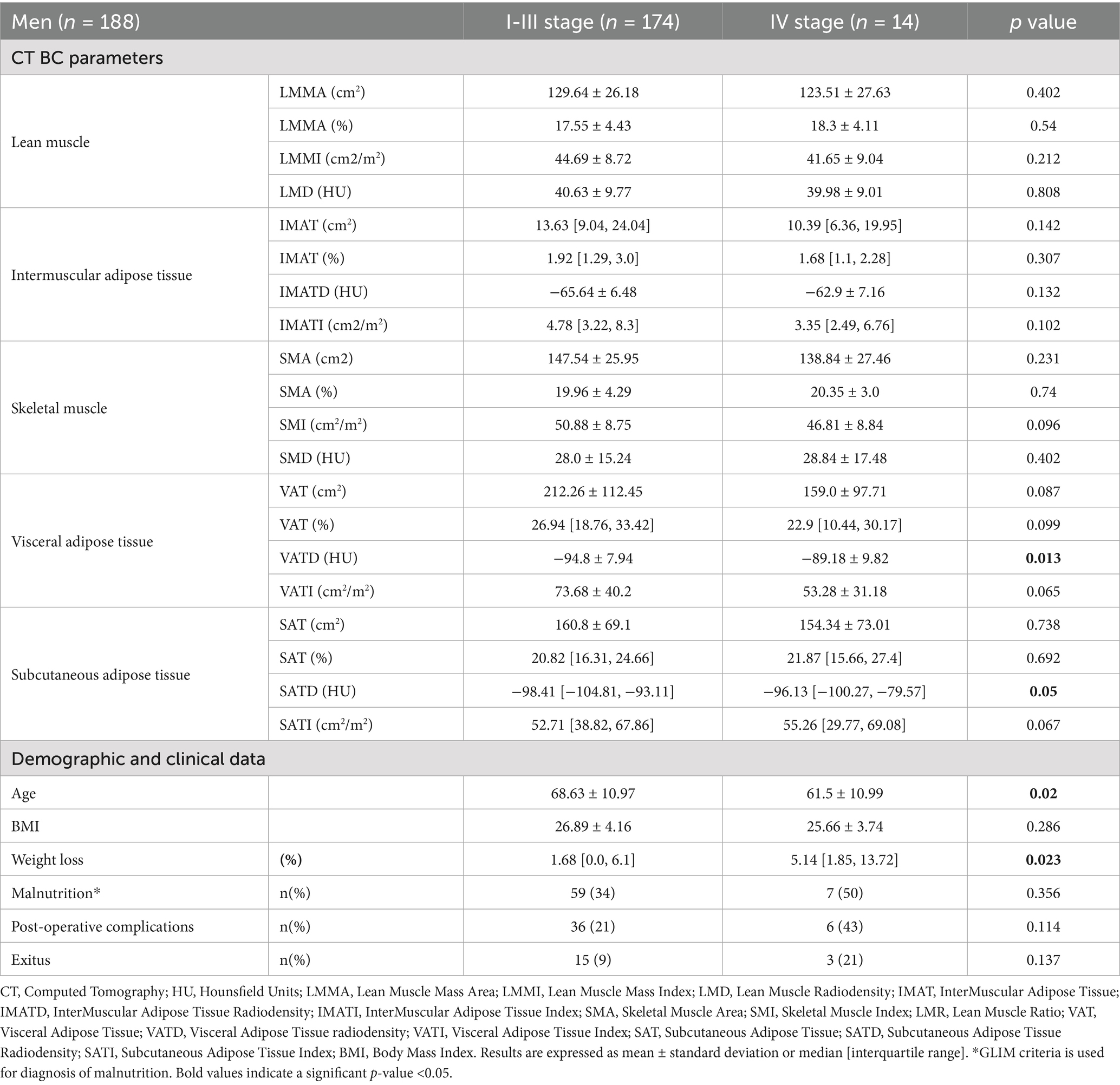
Table 6. Men body composition parameters by CT by disease stage.
Men with advanced disease stage were younger (p = 0.02), reported greater preoperative weight loss (p = 0.023), exhibited a tendency of less quantity of AT, and significant higher adipose tissue radiodensity (subcutaneous and visceral), while muscle parameters remained similar between groups, as shown in Table 7.
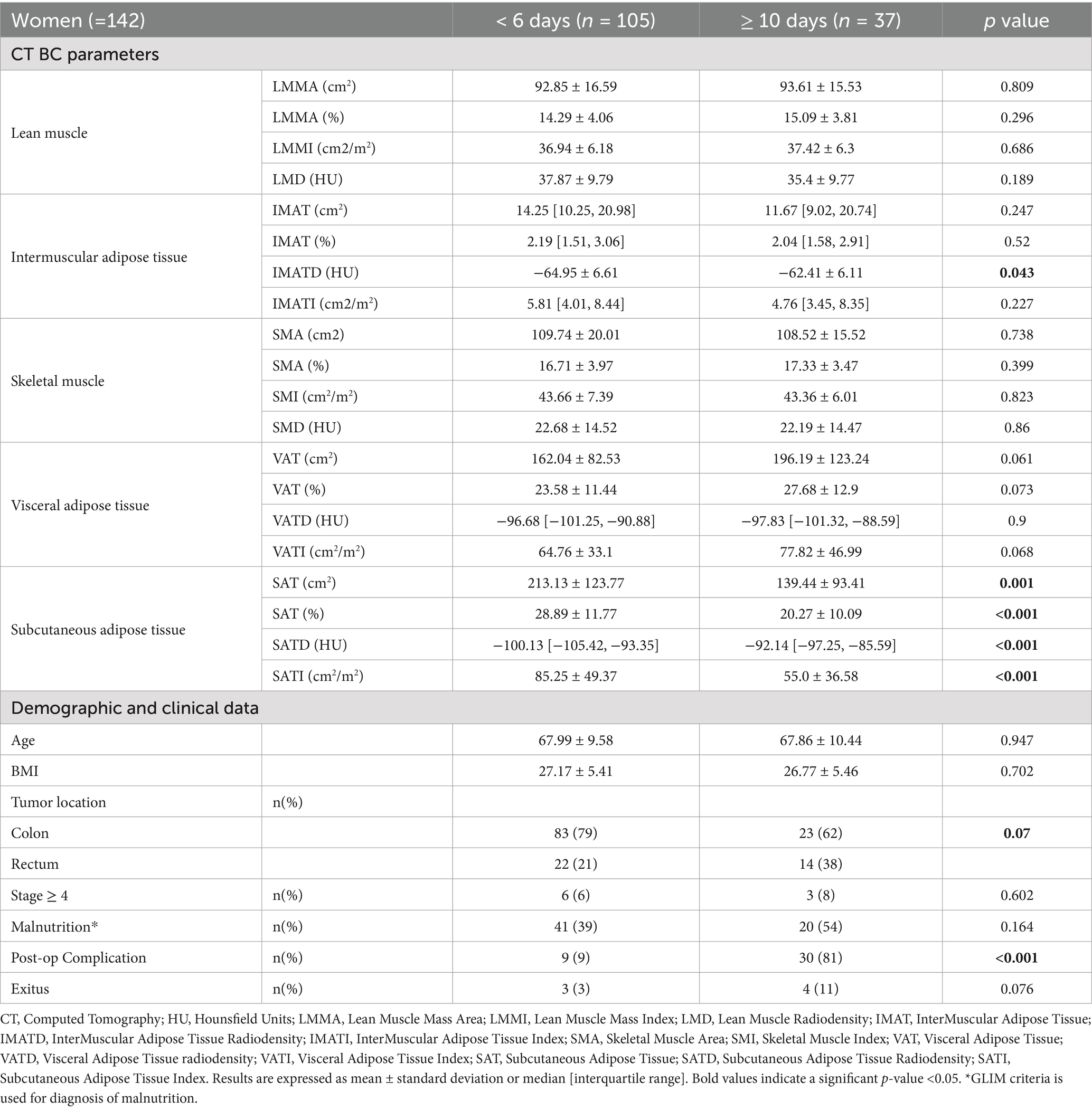
Table 7. Women body composition parameters by CT according to length of hospital stay.
3.5 Body composition and clinical outcomes in women
3.5.1 BC in women considering length of hospital stay
As previously mentioned, distinct sex-related differences in length of hospital stay were observed, with women being less likely to remain hospitalized for more than 10 days compared to men.
Considering these results, when stratified women by length of hospital stay (<6 vs. ≥10 days; Table 7), those with prolonged hospitalization exhibited significantly lower Subcutaneous Adipose Tissue (SAT) area, percentage, radiodensity, and index (all p < 0.05). A nonsignificant trend toward higher Visceral Adipose Tissue (VAT) was also observed, whereas muscle parameters (LMM area, percentage, index and radiodensity) did not differ between the two groups.
Patients with prolonged hospital stay had more postoperative complications (p < 0.001), together with a trend toward higher mortality (p = 0.076) and a greater prevalence of rectal cancer (p = 0.07). Age, BMI, and cancer stage did not differ significantly.
3.5.2 BC in women considering presence of postoperative complications
Women’s body composition parameters assessed by CT according to the presence of postoperative complications can be found in Supplementary Table 2. No significant differences in body composition were observed between women with or without complications.
3.5.3 BC in women considering disease stage
Women BC parameters assessed by CT according to disease stage can be found in Supplementary Table 3. No significant differences in body composition were observed between women according to disease stage.
3.6 Comparative analysis of body composition in stage I–III by sex
Men with IV disease stage presented higher rates of postoperative complications compared to the same stage for women (50% vs. 15%, p = 0.045) as well as higher inflammatory burden in adipose tissue (VAT HU −90.07 ± 10.21 vs. − 99.15 ± 10.36; p = 0.013). Considering these results (found in Supplementary Table 1), we next restricted the analysis to patients with stage I–III colorectal cancer in order to minimize the influence of tumor burden on body composition (Table 8).
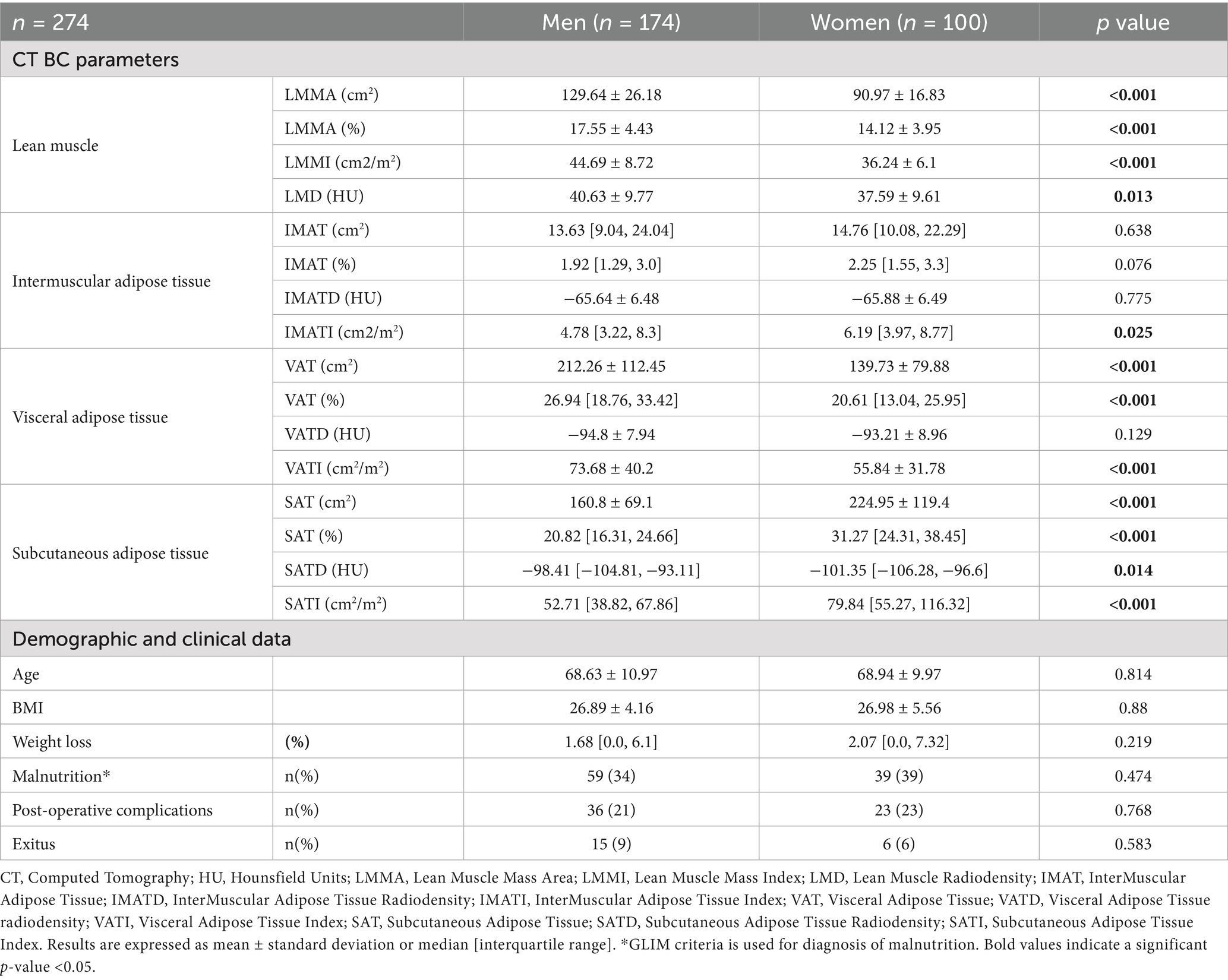
Table 8. Body composition parameters by CT by sex considering I-III cancer stages.
In this subgroup, men consistently presented higher lean mass metrics, including LMMA, LMMI, and radiodensity, compared with women, despite having similar BMI (26.9 ± 4.7 kg/m2; p = 0.880) and age (68.7 ± 10.6 years; p = 0.814). Conversely, women displayed significantly greater Subcutaneous Adipose Tissue (SAT) across all measures (area, %, radiodensity, and index; all p < 0.05), as well as a higher IMAT index (p = 0.025). Visceral Adipose Tissue remained higher in men, as reflected by VATI (p < 0.001). No differences by sex were observed in weight loss considering I-III cancer stages.
3.7 Body composition-related clinical outcomes by sex
Despite the marked sex-related differences in body composition, no significant differences were observed in postoperative outcomes as reported previously in Table 8. The prevalence of malnutrition according to GLIM criteria was similar in men and women (36%; p = 0.474). Postoperative complications occurred in 22% of patients (p = 0.768), with comparable median hospital stay (5 [3.0–7.0] vs. 5 [3.0–7.0] days; p = 0.884) and 6-month mortality (8%; p = 0.583).
On the other hand, Table 9 presents the prevalence of low muscle mass, low muscle radiodensity, and high subcutaneous and visceral adipose tissue by sex in our sample, based on established cut-off points. Notably, although a high proportion of patients exhibited these adverse body composition features, current cut-offs may not capture the prognostic impact of sex-specific body composition phenotypes.
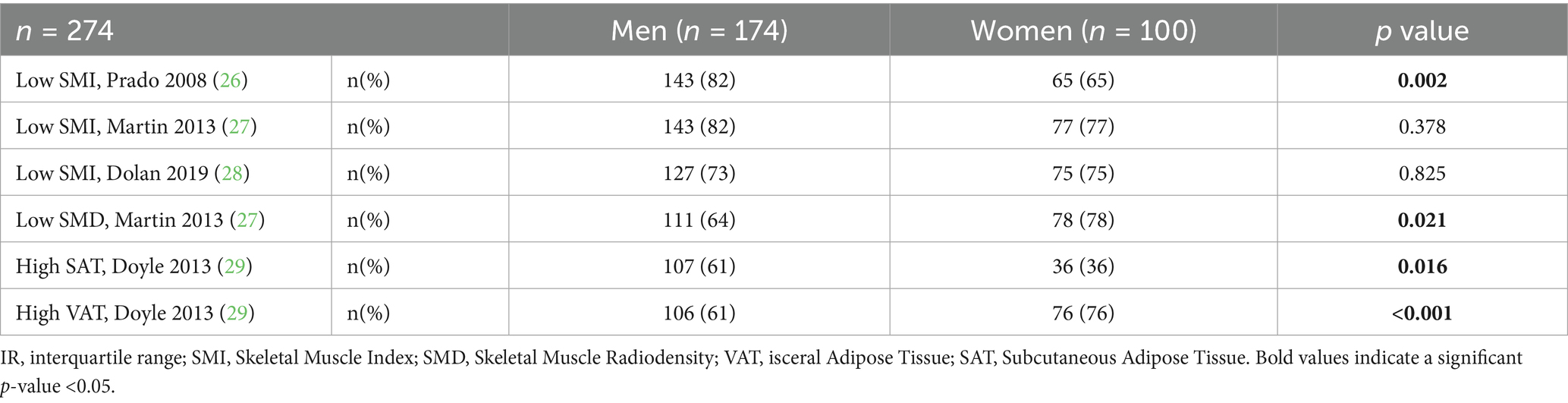
Table 9. Clinical outcomes by sex in stage I–III cancer patients according to established cut-off points for low muscle mass, low radiodensity, and high adipose tissue.
3.8 Comparative analysis of body composition by age
As current cut-off points do not account for age-related changes in body composition, we stratified the analysis by both sex and age to better capture these variations.
As expected, older patients exhibited lower muscle indices and radiodensity, along with higher adipose tissue levels in both sexes (Table 10).
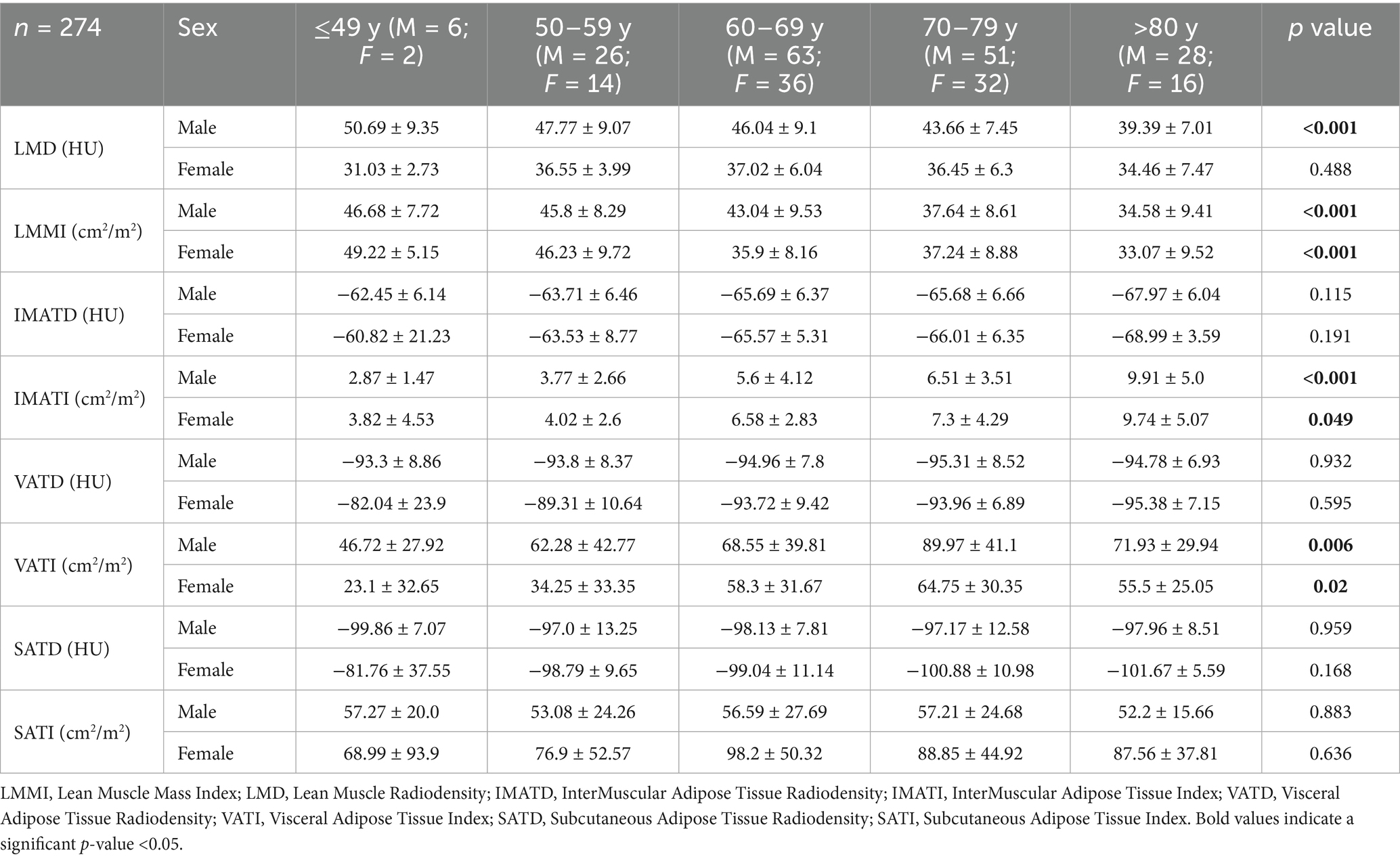
Table 10. Age composition parameters by CT according to sex.
The observed differences in body composition between men and women in CRC patients prior to elective surgery are illustrated in Figure 2, showing phenotypic variations measured by CT imaging.
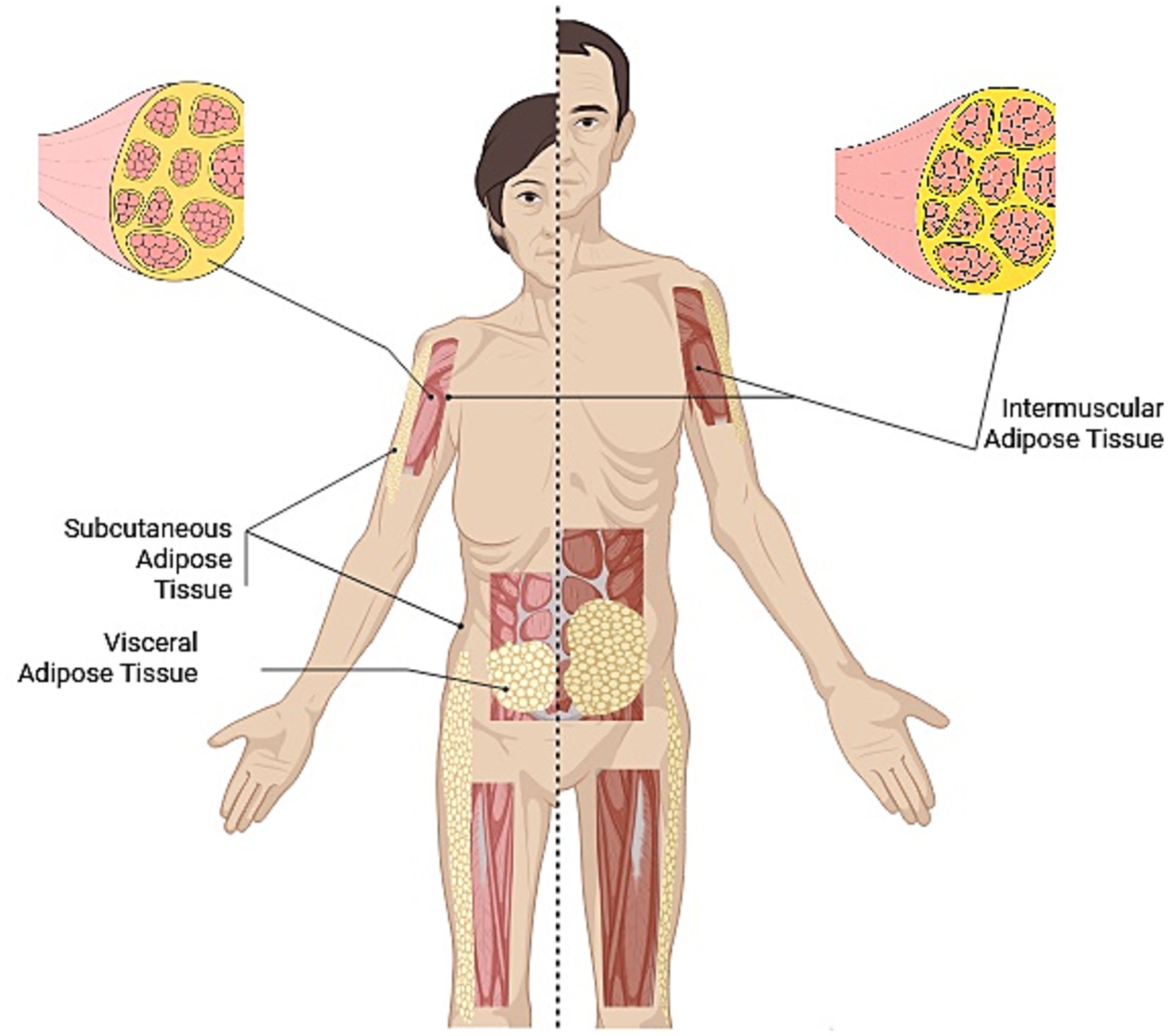
Figure 2. Phenotypic illustration of differences in body composition measured through TC according to sex patients with CRC prior to elective surgery.
4 Discussion
This study provides new evidence on sex-specific body composition phenotypes in patients undergoing colon cancer surgery. These results highlight how differences in muscle and adipose tissue distribution assessed by CT were observed according to postoperative outcomes, underscoring the importance of both qualitative and quantitative parameters.
Consistent with previous literature, men had greater skeletal muscle mass and visceral adiposity, whereas women had greater subcutaneous and intermuscular adipose tissue (40). Critically, these differences were not only descriptive but also reflected distinct patterns according to clinical outcomes. In women, lower SAT was consistently observed among prolonged hospital stay and complications, supporting the hypothesis that peripheral fat depots act as protective metabolic reserves in the perioperative period (41, 42). Multiple studies have demonstrated that SAT serves as a critical energy reserve and is associated with favorable outcomes in surgical and critical illness settings. Specifically, in female patients with cirrhosis, lower SAT index was independently associated with higher mortality, suggesting that depletion of subcutaneous fat reflects loss of a major metabolic reserve and leads to poor clinical outcomes (43). Similarly, in patients undergoing cardiovascular surgery, higher subcutaneous fat composition was associated with reduced all-cause and cardiac-cause mortality, while visceral fat was not predictive of outcomes (44). In men, patterns characterized by lower muscle quality (lower lean muscle radiodensity) as well as muscle quantity, and higher visceral adiposity were more frequently observed among those with adverse outcomes, emphasizing that both muscle quantity and quality are relevant in this group (45–47). These patterns were consistent across all age groups and tumor stages, reinforcing the robustness of sex-specific phenotypes.
Radiodensity, as a marker of tissue quality, emerged as a strong predictor of outcomes (27). This is consistent with growing evidence in other oncology settings that muscle attenuation provides additional prognostic information beyond simple muscle mass (47–49). In our cohort, lower preoperative Hounsfield units reflected poorer muscle quality and were more frequently observed in patients who experienced complications, often alongside reduced muscle mass. Similarly, increased HU values in adipose tissue suggested fibrotic or inflammatory remodeling, indicating early qualitative changes that may precede overt tissue depletion (50, 51).
Interestingly, our cohort challenges common assumptions regarding colorectal cancer patients (52). Among patients with advanced tumor stage (IV), individuals were younger and did not meet GLIM criteria for malnutrition, despite weight loss (8). This suggests that weight loss may serve as an early indicator of nutritional risk before formal diagnostic thresholds are reached. Body composition patterns in patients with advanced tumor stage (IV) did not appear worse than those in earlier stages (I–III), possibly reflecting timely diagnosis through screening and surgical referral before cachexia develops. However, they showed a tendency toward lower adipose tissue quantity and higher radiodensity in both SAT and VAT. This pattern may reflect early qualitative changes in adipose tissue, such as inflammatory or fibrotic remodeling, occurring before measurable losses in muscle mass or fat area. Although our sample size in advanced stages was limited, this finding reinforces the concept that qualitative alterations in adipose tissue may be among the earliest detectable metabolic disruptions in cancer progression.
Taken together, these findings illustrate that tumor stage alone is not sufficient to define metabolic and clinical risk, and that body composition phenotyping provides substantial discriminatory power.
Interestingly, when applying some established cut-offs, women in our cohort appeared to have higher rates of sarcopenia compared to Prado et al. (26), and greater myosteatosis compared to Martin et al. (27), a higher VAT compared to Doyle et al. (29), whereas men showed higher SAT compared to Doyle et al. (29). However, our own analyses highlighted a different pattern: adverse outcomes in men were mainly driven by low muscle quality and excess VAT, while in women SAT depletion emerged as the predominant risk factor. In line with this, age-stratified analyses further emphasized that body composition variability should be interpreted not only by sex but also by age, highlighting the need for refined phenotyping strategies. These differences underscore the limitations of uniform cutoff values and support the need for context-specific, sex- and age-adjusted thresholds that integrate both muscle quality and adipose tissue distribution.
The clinical implications are clear. Opportunistic CT in oncology provides highly accurate information on tissue quantity, quality, and distribution, allowing for the development of phenotypic profiles that can improve perioperative risk stratification and guide personalized nutritional strategies.
Recent advances have proposed ultrasound and other non-radiological techniques as potential alternatives for assessing muscle mass and quality in oncology patients. However, most of these approaches rely on single-muscle measurements and show limited validation against CT-based parameters or clinical outcomes (53–57). In this context, our findings reinforce the value of CT-derived assessment, which uniquely integrates tissue quality and adipose distribution, providing a more comprehensive reflection of the patient’s metabolic and functional reserve.
This study has some limitations. Its retrospective design precludes causal inference, and although multicenter and relatively large, the number of patients with advanced stages was limited. Only patients undergoing elective laparoscopic surgery were included; therefore, the findings may not be generalizable to those receiving open or emergency procedures. Data on (neo)adjuvant chemotherapy, which could also influence body composition, were not available. Otherwise, only bivariate comparisons are reported. Further studies adjusting for potential confounders such as BMI, cancer stage, age, and sex are required to confirm these associations and better elucidate the independent contribution of each body composition parameter to postoperative outcomes. Despite these limitations, the standardized CT methodology, multicenter design, and consistent patterns observed in muscle and adipose compartments support the validity of our findings.
This study provides new evidence on sex-specific body composition phenotypes in patients undergoing surgery for colon cancer. These results highlight the patterns of muscle and adipose tissue distribution assessed by CT in relation to postoperative outcomes. To our knowledge, this is one of the first studies to stratify both lean and adipose compartments by sex and age, offering insight into how tissue phenotypes may differentially influence metabolic and clinical risk.
5 Conclusion
In this multicenter cohort of colorectal cancer patients, preoperative CT-derived body composition parameters, encompassing both muscle and adipose compartments, differed according to surgical outcomes. These findings highlight the importance of nutritional assessment that considers not only muscle mass but also muscle quality and fat distribution, thereby complementing current GLIM criteria and providing a more accurate reflection of metabolic reserve. Integrating CT-based body composition into clinical pathways may improve risk stratification and guide targeted nutritional and prehabilitation strategies. Future research should examine these patterns in larger and more diverse populations, across different tumor types, and establish clinically relevant sex- and age-specific cut-offs for routine use.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by CEIC Institut de Recerca Vall d’Hebron. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
FM: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. PP: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – review & editing. VU: Investigation, Writing – review & editing. RJ: Formal analysis, Investigation, Methodology, Resources, Writing – review & editing. FC: Conceptualization, Formal analysis, Investigation, Methodology, Resources, Writing – original draft, Writing – review & editing. FT: Conceptualization, Data curation, Investigation, Methodology, Writing – review & editing. RP: Project administration, Supervision, Validation, Writing – review & editing. JA: Project administration, Writing – review & editing. GO: Project administration, Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
The authors express their gratitude to all individuals who participated in this study for their willingness to collaborate.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2025.1728741/full#supplementary-material
Footnotes
References
1. Ishida, Y, Maeda, K, Murotani, K, Shimizu, A, Ueshima, J, Nagano, A, et al. Association of body mass index and weight change with death in patients with advanced cancer. Nutrition. (2023) 115:112152. doi: 10.1016/j.nut.2023.112152
2. Casirati, A, Vandoni, G, Della Valle, S, Greco, G, Platania, M, Colatruglio, S, et al. Nutritional status and body composition assessment in patients with a new diagnosis of advanced solid tumour: exploratory comparison of computed tomography and bioelectrical impedance analysis. Clin Nutr. (2021) 40:1268–73. doi: 10.1016/j.clnu.2020.08.009
3. Heymsfield, SB, Wang, ZM, Baumgartner, RN, and Ross, R. Human body composition: advances in models and methods. Annu Rev Nutr. (1997) 17:527–58. doi: 10.1146/annurev.nutr.17.1.527
4. Brown, JC, Cespedes Feliciano, EM, and Caan, BJ. The evolution of body composition in oncology-epidemiology, clinical trials, and the future of patient care: facts and numbers. J Cachexia Sarcopenia Muscle. (2018) 9:1200–8. doi: 10.1002/jcsm.12379
5. Prado, CM, and Heymsfield, SB. Lean tissue imaging: a new era for nutritional assessment and intervention. JPEN J Parenter Enteral Nutr. (2014) 38:940–53. doi: 10.1177/0148607114550189
6. Mourtzakis, M, Prado, C, Lieffers, J, Reiman, T, McCargar, L, and Baracos, V. A practical and precise approach to quantification of body composition in cancer patients using computed tomography images acquired during routine care. Appl Physiol Nutr Metab. (2008) 33:997–1006. doi: 10.1139/H08-075
7. Soria-Utrilla, V, Sánchez-Torralvo, FJ, Palmas-Candia, FX, Fernández-Jiménez, R, Mucarzel-Suarez-Arana, F, Guirado-Peláez, P, et al. AI-assisted body composition assessment using CT imaging in colorectal Cancer patients: predictive capacity for sarcopenia and malnutrition diagnosis. Nutrients. (2024) 16:1869. doi: 10.3390/nu16121869
8. Cederholm, T, Jensen, GL, Correia, MITD, Gonzalez, MC, Fukushima, R, Higashiguchi, T, et al. GLIM Core leadership committee; GLIM working group. GLIM criteria for the diagnosis of malnutrition - a consensus report from the global clinical nutrition community. Clin Nutr. (2019) 38:1–9. doi: 10.1016/j.clnu.2018.08.002
9. Barazzoni, R, Jensen, GL, Correia, MITD, Gonzalez, MC, Higashiguchi, T, Shi, HP, et al. Guidance for assessment of the muscle mass phenotypic criterion for the global leadership initiative on malnutrition (GLIM) diagnosis of malnutrition. Clin Nutr. (2022) 41:1425–33. doi: 10.1016/j.clnu.2022.02.001
10. Cruz-Jentoft, AJ, Bahat, G, Bauer, J, Boirie, Y, Bruyère, O, Cederholm, T, et al. Writing Group for the European Working Group on sarcopenia in older people 2 (EWGSOP2), and the extended group for EWGSOP2. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. (2019) 48:16–31. doi: 10.1093/ageing/afy169
11. Kanth, P, and Inadomi, JM. Screening and prevention of colorectal cancer. BMJ. (2021) 374:n1855. doi: 10.1136/bmj.n1855
12. Mourtzakis, M, Prado, CM, Lieffers, JR, Prado, CMM, Reiman, T, McCargar, LJ, et al. A practical and precise approach to quantification of body composition in cancer patients using computed tomography images acquired during routine care. Appl Physiol Nutr Metab. (2008) 33:997–1006. doi: 10.1139/H08-075
13. Fearon, K, Strasser, F, Anker, SD, Bosaeus, I, Bruera, E, Fainsinger, RL, et al. Definition and classifi- cation of cancer cachexia: an international consensus. Lancet Oncol. (2011) 12:489–95. doi: 10.1016/S1470-2045(10)70218-7
14. Palmas, FX, Ricart, M, Lluch, A, Mucarzel, F, Cartiel, R, Zabalegui, A, et al. Prognostic value of computed tomography-derived muscle density for postoperative complications in enhanced recovery after surgery (ERAS) and non-ERAS patients. Nutrients. (2025) 17:2264. doi: 10.3390/nu17142264
15. Schwenk, W. Optimized perioperative management (fast-track, ERAS) to enhance postoperative recovery in elective colorectal surgery. GMS Hyg Infect Control. (2022) 17:Doc10. doi: 10.3205/dgkh000413
16. Heil, TC, Verdaasdonk, EGG, Maas, HAAM, van Munster, BC, Rikkert, MGMO, de Wilt, JHW, et al. Improved postoperative outcomes after Prehabilitation for colorectal Cancer surgery in older patients: an emulated target trial. Ann Surg Oncol. (2023) 30:244–54. doi: 10.1245/s10434-022-12623-9
17. Zhou, H, Tian, L, Wu, Y, and Liu, S. Computed tomography-measured body composition can predict long-term outcomes for stage I-III colorectal cancer patients. Front Oncol. (2024) 14:1420917. doi: 10.3389/fonc.2024.1420917
18. Martin, L, Hopkins, J, Malietzis, G, Jenkins, JT, Sawyer, MB, Brisebois, R, et al. Assessment of computed tomography (CT)-defined muscle and adipose tissue features in relation to short-term outcomes after elective surgery for colorectal cancer: a multicenter approach. Ann Surg Oncol. (2018) 25:2669–80. doi: 10.1245/s10434-018-6652-x
19. Takiguchi, K, Furuya, S, Sudo, M, Saito, R, Yamamoto, A, Ashizawa, N, et al. Prognostic effect of sarcopenia incolorectal cancer recurrence. Nutrition. (2021) 91–92:111362. doi: 10.1016/j.nut.2021.111362
20. Mai, DVC, Drami, I, Pring, ET, Gould, L, Rai, J, Malietzis, G, et al. Automated three-dimensional body composition analysis identifies visceral adipose tissue radiodensity as a predictor of mortality and recurrence in colorectal cancer. Clin Nutr. (2025) 51:9–17. doi: 10.1016/j.clnu.2025.04.019
21. Zhou, H, Tian, L, Wu, Y, and Liu, S. Computed tomography-measured body composition can predict long-term outcomes for stage I-III colorectal cancer patients. Front Oncol. (2024) 14:1420917. doi: 10.3389/fonc.2024.1420917
22. Hirdel, M, Andersson, F, Myte, R, Axelsson, J, Rutegård, M, Blomqvist, L, et al. Body composition measured by computed tomography is associated with colorectal cancer survival, also in early-stage disease. Acta Oncol. (2020) 59:799–808. doi: 10.1080/0284186X.2020.1744716
23. Lee, MH, Pickhardt, SG, Garrett, JW, Perez, AA, Zea, R, Valle, KF, et al. Utility of fully automated body composition measures on pretreatment abdominal CT for predicting survival in patients with colorectal Cancer. AJR Am J Roentgenol. (2023) 220:371–80. doi: 10.2214/AJR.22.28043
24. Carvalho, ALM, Gonzalez, MC, Sousa, IM, das Virgens, IPA, Medeiros, GOC, Oliveira, MN, et al. Low skeletal muscle radiodensity is the best predictor for short-term major surgical complications in gastrointestinal surgical cancer: a cohort study. PLoS One. (2021) 16:e0247322. doi: 10.1371/journal.pone.0247322
25. Kemper, M, Melling, N, Krause, L, Kühn, K, Graß, JK, Izbicki, JR, et al. Muscle quality, not quantity, is associated with outcome after colorectal cancer surgery. Eur J Surg Oncol. (2023) 49:107098. doi: 10.1016/j.ejso.2023.107098
26. Prado, CM, Lieffers, JR, McCargar, LJ, Reiman, T, Sawyer, MB, Martin, L, et al. Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: a population-based study. Lancet Oncol. (2008) 9:629–35. doi: 10.1016/S1470-2045(08)70153-0
27. Martin, L, Birdsell, L, Macdonald, N, Reiman, T, Clandinin, MT, McCargar, LJ, et al. Cancer cachexia in the age of obesity: skeletal muscle depletion is a powerful prognostic factor, independent of body mass index. J Clin Oncol. (2013) 31:1539–47. doi: 10.1200/JCO.2012.45.2722
28. Dolan, RD, Almasaudi, AS, Dieu, LB, Horgan, PG, McSorley, ST, and McMillan, DC. The relationship between computed tomography-derived body composition, systemic inflammatory response, and survival in patients undergoing surgery for colorectal cancer. J Cachexia Sarcopenia Muscle. (2019) 10:111–22. doi: 10.1002/jcsm.12357
29. Doyle, SL, Bennett, AM, Donohoe, CL, Mongan, AM, Howard, JM, Lithander, FE, et al. Establishing computed tomography-defined visceral fat area thresholds for use in obesity-related cancer research. Nutr Res. (2013) 33:171–9. doi: 10.1016/j.nutres.2012.12.007
30. Tokunaga, R, Nakagawa, S, Miyamoto, Y, Ohuchi, M, Izumi, D, Kosumi, K, et al. The clinical impact of preoperative body composition differs between male and female colorectal cancer patients. Color Dis. (2020) 22:62–70. doi: 10.1111/codi.14793
31. Gustafsson, T, and Ulfhake, B. Aging skeletal muscles: what are the mechanisms of age-related loss of strength and muscle mass, and can we impede its development and progression? Int J Mol Sci. (2024) 25:10932. doi: 10.3390/ijms252010932
32. Draganidis, D, Jamurtas, AZ, Chondrogianni, N, Mastorakos, G, Jung, T, Grune, T, et al. Low-grade systemic inflammation interferes with anabolic and catabolic characteristics of the aged human skeletal muscle. Oxidative Med Cell Longev. (2021) 2021:8376915:154–96. doi: 10.1155/2021/8376915
33. Nakanishi, R, Oki, E, Sasaki, S, Hirose, K, Jogo, T, Edahiro, K, et al. Sarcopenia is an independent predictor of complications after colorectal cancer surgery. Surg Today. (2018) 48:151–7. doi: 10.1007/s00595-017-1564-0
34. Jessup, J, Benson, A, and Chen, V. Colon and Rectum In: MB Amin, SB Edge, and FL Greene, editors. AJCC Cancer staging manual. 8th ed: Springer (2017). 251–74.
35. Kondrup, J, Allison, SP, Elia, M, Vellas, B, and Plauth, M. ESPEN guidelines for nutritional screening. Clin Nutr. (2003) 22:415–21. doi: 10.1016/s0261-5614(03)00098-0
36. Tolonen, A, Pakarinen, T, Sassi, A, Kyttä, J, Cancino, W, Rinta-Kiikka, I, et al. Methodology, clinical applications, and future directions of body composition analysis using computed tomography (CT) images: a review. Eur J Radiol. (2021) 145:109943. doi: 10.1016/j.ejrad.2021.109943
37. Winder, C, Clark, M, Frood, R, Smith, L, Bulpitt, A, Cook, G, et al. Automated extraction of body composition metrics from abdominal CT or MR imaging: a scoping review. Eur J Radiol. (2024) 181:111764. doi: 10.1016/j.ejrad.2024.111764
38. Palmas, F, Mucarzel, F, Ricart, M, Lluch, A, Zabalegui, A, Melian, J, et al. Body composition assessment with ultrasound muscle measurement: optimization through the use of semi-automated tools in colorectal cancer. Front Nutr. (2024) 11:1372816. doi: 10.3389/fnut.2024.1372816
39. Dindo, D, Demartines, N, and Clavien, PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. (2004) 240:205–13. doi: 10.1097/01.sla.0000133083.54934.ae
40. Hassler, EM, Deutschmann, H, Almer, G, Renner, W, Mangge, H, Herrmann, M, et al. Distribution of subcutaneous and intermuscular fatty tissue of the mid-thigh measured by MRI-A putative indicator of serum adiponectin level and individual factors of cardio-metabolic risk. PLoS One. (2021) 16:e0259952. doi: 10.1371/journal.pone.0259952
41. Karastergiou, K, Smith, SR, Greenberg, AS, and Fried, SK. Sex differences in human adipose tissues - the biology of pear shape. Biol Sex Differ. (2012) 3:13. doi: 10.1186/2042-6410-3-13
42. Tchernof, A, Bélanger, C, Morisset, A-S, Richard, C, Mailloux, J, Laberge, P, et al. Regional differences in adipose tissue metabolism in women: minor effect of obesity and body fat distribution. Diabetes. (2006) 55:1353–60. doi: 10.2337/db05-1439
43. Ebadi, M, Tandon, P, Moctezuma-Velazquez, C, Ghosh, S, Baracos, VE, Mazurak, VC, et al. Low subcutaneous adiposity associates with higher mortality in female patients with cirrhosis. J Hepatol. (2018) 69:608–16. doi: 10.1016/j.jhep.2018.04.015
44. Bae, J, Ju, JW, Lee, S, Nam, K, Kim, TK, Jeon, Y, et al. Association between abdominal fat and mortality in patients undergoing cardiovascular surgery. Ann Thorac Surg. (2022) 113:1506–13. doi: 10.1016/j.athoracsur.2021.05.049
45. Lee, M-J, Wu, Y, and Fried, SK. Adipose tissue heterogeneity: implication of depot differences in adipose tissue for obesity complications. Mol Asp Med. (2013) 34:1–11. doi: 10.1016/j.mam.2012.10.001
46. Cypess, AM. Reassessing human adipose tissue. N Engl J Med. (2022) 386:768–79. doi: 10.1056/NEJMra2032804
47. Bian, L, Wu, D, Chen, Y, Ni, J, Qu, H, Li, Z, et al. Associations of radiological features of adipose tissues with postoperative complications and overall survival of gastric cancer patients. Eur Radiol. (2022) 32:8569–78. doi: 10.1007/s00330-022-08918-w
48. Wei, LH, Zheng, HL, Liu, ZY, Du, XQ, Chen, CS, Xu, BB, et al. Preoperative visceral fat area predicts intraoperative adverse events during lymphadenectomy in laparoscopic gastrectomy for gastric cancer: a post hoc analysis. Surg Endosc. (2025) 39:2275–87. doi: 10.1007/s00464-025-11602-x
49. Aleixo, GFP, Shachar, SS, Nyrop, KA, Muss, HB, Malpica, L, and Williams, GR. Myosteatosis and prognosis in cancer: systematic review and meta-analysis. Crit Rev Oncol Hematol. (2019) 145:102839. doi: 10.1016/j.critrevonc.2019.102839
50. Lee, CM, and Kang, J. Prognostic impact of myosteatosis in patients with colorectal cancer: a systematic review and meta-analysis. J Cachexia Sarcopenia Muscle. (2020) 11:1270–82. doi: 10.1002/jcsm.12575
51. Nogajski, Ł, Mazuruk, M, Kacperska, M, Kurpias, M, Mączewski, M, Nowakowski, M, et al. Epicardial fat density obtained with computed tomography imaging - more important than volume? Cardiovasc Diabetol. (2024) 23:389. doi: 10.1186/s12933-024-02474-x
52. Lake, JE, Moser, C, Johnston, L, Magyar, C, Nelson, SD, Erlandson, KM, et al. CT fat density accurately reflects histologic fat quality in adults with HIV on and off antiretroviral therapy. J Clin Endocrinol Metab. (2019) 104:4857–64. doi: 10.1210/jc.2018-02785
53. Arends, J, Bachmann, P, Baracos, V, Barthelemy, N, Bertz, H, Bozzetti, F, et al. ESPEN guidelines on nutrition in cancer patients. Clin Nutr. (2017) 36:11–48. doi: 10.1016/j.clnu.2016.07.015
54. López-Gómez, JJ. Artificial intelligence-assisted ultrasound assessment of muscle quality and quantity in oncology patients: correlation with CT-derived measurements. Front Nutr. (2025) 12:1678989. doi: 10.3389/fnut.2025.1678989
55. de la Fuente, A. Comparison of ultrasound and computed tomography for the assessment of muscle quality in cancer patients: implications for nutritional evaluation. Forum Nutr. (2025) 112:112451. doi: 10.1002/ncp.11234
56. Ferrero-Moreno, L. Body composition assessment by ultrasonography in oncology: reproducibility, validity, and comparison with CT imaging. Life. (2025) 15:236
57. Di Renzo, L, Itani, L, Gualtieri, P, Pellegrini, M, El Ghoch, M, and De Lorenzo, A. New BMI cut-off points for obesity in middle-aged and older adults in clinical nutrition settings in Italy: a cross-sectional study. Nutrients. (2022) 14:4848. doi: 10.3390/nu14224848
Glossary
BC - Body Composition
BMI - Body Mass Index
CRC - Colorectal Cancer
CT - Computed Tomography
GLIM - Global Leadership Initiative on Malnutrition
EWGSOP2 - European Working Group on Sarcopenia in Older People 2
LMMA - Lean Muscle Mass Area
LMMI - Lean Muscle Mass Index
LMD - Lean Muscle Radiodensity
SMI - Skeletal Muscle Index
SMA - Skeletal Muscle Area
SMD - Skeletal Muscle Radiodensity
SAT - Subcutaneous Adipose Tissue
SATI - Subcutaneous Adipose Tissue Index
SATD - Subcutaneous Adipose Tissue Radiodensity
VAT - Visceral Adipose Tissue
VATI - Visceral Adipose Tissue Index
VATD - Visceral Adipose Tissue Radiodensity
IMAT - Intermuscular Adipose Tissue
IMATI - Intermuscular Adipose Tissue Index
IMATD - Intermuscular Adipose Tissue Radiodensity
FFMI - Fat Free Mass Index
BIA - Bioelectrical Impedance
IR - Interquartile Range
SD - Standard Deviation
Keywords: computed tomography, colorectal cancer, body composition, Hounsfield units, postoperative complications
Citation: Mucarzel F, Peláez PG, Utrilla VS, Jiménez RF, Candia FP, Torralvo FJS, Peláez RB, Almeida JMG and Olveira G (2025) Sex-specific CT-derived muscle and fat phenotypes in colon cancer: implications for nutritional and metabolic assessment. Front. Nutr. 12:1728741. doi: 10.3389/fnut.2025.1728741
Edited by:
Nallely Bueno-Hernández, General Hospital of Mexico, MexicoReviewed by:
Alison Santoyo, General Hospital of Mexico, MexicoKarolina Alvarez-Altamirano, General Hospital of Mexico, Mexico
Copyright © 2025 Mucarzel, Peláez, Utrilla, Jiménez, Candia, Torralvo, Peláez, Almeida and Olveira. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fiorella Palmas Candia, ZmlvcmVsbGF4aW1lbmEucGFsbWFzQHZhbGxoZWJyb24uY2F0