Abstract
Background:
In the past, studies have compared smokeless tobacco and non-tobacco users for the risk of various chronic diseases. The differences in the risk of chronic diseases between smokeless tobacco user and smokers have not been explored. The objective of this study is to estimate the risk of chronic diseases among smokeless tobacco users compared to smokers.
Methods:
The data were used from the Study on Global Ageing and Adult Health (SAGE) Wave-1, conducted in 2007–2008 in India. The study sample is the respondents who reported consuming any form of tobacco in last 1 month. The total sample size was 4,038 respondents. The odds ratio of chronic morbidities was estimated taking smokers as the reference category.
Results:
The odds ratios for (self-reported) diabetes, asthma, and hypertension were not significant for smokeless tobacco user compared to smoked tobacco users. The odds ratio of chronic lung diseases (CLDs) was significantly lower among smokeless tobacco users compared to smoked tobacco users. The odds ratio of hypertension (measured) combined with low education and belonging to lowest wealth quintiles were not significant for smokeless tobacco users compared to smoked tobacco users. Duration of the use of smokeless tobacco and quantity of use was found to have no significant relation with risk of chronic diseases as compared to smoking.
Conclusion:
This study did not find the significantly higher risk of chronic morbidities except for CLD for smokeless tobacco users compared to smoked tobacco users. The study suggests that the use of any form of tobacco may have a similar risk of chronic diseases.
Introduction
The cardiovascular disease (CVD) is a leading cause of death in India (1, 2). Hypertension is the major risk factor for CVDs and diabetes mellitus (3). Smoking is known for influencing hypertension and chronic diseases, resulting in premature mortality (4, 5). There are a lot of chemical in both types of tobacco. Nicotine is common in both, known to increased blood pressure levels (6). The maximal level of nicotine is similar after a single exposure to smokeless tobacco and smoking (7). Although, smokeless tobacco can cause prolonged nicotine exposure compared to smoked tobacco users.
As per the estimates from Global Adult Tobacco Survey in India, there were 274.9 million tobacco users and out of that 206 million were smokeless tobacco users (8). Smokeless tobacco was responsible for approximately 368,127 deaths in 2010 in India (9). Smokeless tobacco is locally available and sold at a lower price compared to the cigaret and other smoking products and remains the most common form of tobacco use in India (8, 10). As depicted in many studies, the prevalence of smokeless tobacco was high among lower socioeconomic groups; such as in rural and tribal population (11–14). The differences between the smoked and smokeless tobacco use will hold importance for preventing chronic diseases especially among socially disadvantaged groups in India (13). The evidence can be useful in policies preventing the use of tobacco products. Higher taxation, prevention of advertisement of tobacco products and smoking in public places, etc. are more focused on smoking and can continue if smokeless tobacco has a lower risk of chronic diseases compared to smoking (15).
Many studies in the Sweden and United States of America have explored the causal association of CVD risk factors such as hypertension, stroke, and mortality with use of smokeless tobacco (16–19). Haglund et al., Wennberg et al., and Hergens et al. did not find any significant risk of hypertension and stroke (20–22). Hergens et al in Sweden used snuffed tobacco as a smokeless tobacco to study the impact on health (23). Studies have used self-reported hypertension status and duration or amount of smokeless tobacco were not collected. Spit tobacco was found to be associated with increased odds of mortality due to CVDs (24). All these studies that find increased risk of chronic diseases using non-smokers as a reference category. Studies in India have shown that use of smokeless tobacco has increased risks of hypertension and mortality due to chronic diseases compared to non-tobacco users (25, 26). The important question is “does the use of the smokeless tobacco has similar risk of chronic morbidities compared to smoked tobacco?” The objective of the study is to compare the risk of chronic diseases between smoked and smokeless tobacco.
Materials and Methods
Data Source
The data were used from the Study on Global Ageing and Adult Health (SAGE) Wave1, conducted in 2007–2008 in India. A multistage, stratified, random cluster sampling design was used. The data were collected from six states—Assam, Karnataka, Maharashtra, Rajasthan, Uttar Pradesh, and West Bengal. The same primary sampling units (PSUs) and households covered in the World Health Survey (WHS-2003) comprised the baseline sample for SAGE Wave1-India in 2007–2008. The PSUs were stratified by region and location (urban/rural) and, within each stratum, enumeration areas were selected. The enumeration areas in rural and urban areas were villages and Census Enumeration Blocks (CEBs), respectively. Within each selected areas lists of households with at least one member aged 45 and above was prepared. From the list of households, 28 households in each village and 33 household in each CEBs were randomly selected. The details are also given on the SAGE website and published elsewhere (27, 28). It was a cross-sectional household survey, which collected information for adults aged 18 years and above by face-to-face interviews. A cross-sectional study is an observational study. The observations were recorded at a singular point of time without influencing the respondents. Household and individual weights were post-stratified to weight up to population distributions by age and sex. A physical examination was used to collect height, weight, waist circumference, and blood pressure (28). Tobacco-related information was collected from the respondent who reported consuming tobacco. The total sample size was 4,038 respondents who were the current consumer of any form of tobacco.
Tobacco Use Classification
The tobacco users reported consuming only smokeless tobacco was categorized as smokeless tobacco users. The respondents who reported only smoked tobacco were categorized as smokers. The respondents who reported using both the product were categorized as user of “both” product. The smokeless tobacco user and smokers were classified by duration of tobacco use, i.e., using less than for 10 years and using it for 10 and more years. Smoking was also categorized by daily uses. Smoking less than 10 U per day were classified as mild/moderate smokers, smoking 10 or more units per day were categorized as severe smokers. Similarly, Smokeless tobacco users consuming less than 10 g per day were classified as a mild/moderate use. Smokeless tobacco users consuming 10 or more grams per day categorized as severe use.
Morbidity Indicators
Systolic and diastolic blood pressure levels were recorded three times for each respondent. The average of these three systolic and diastolic blood pressures was taken as the final systolic and diastolic blood pressure level of the respondent. They were then categorized as hypertensive if systolic blood pressure was greater than 140 mmHg or diastolic blood pressure greater than 90 mmHg. Height and weight of the respondents taken during the survey were used to calculate body mass index (BMI) as per the following formula:
The classification of BMI followed the WHO standard, i.e., ranging from BMI less than 18.5 which was categorized as underweight to BMI greater than 25.0 which was overweight. Self-reported morbidities such as asthma, chronic lung disease (CLD), diabetes mellitus, hypertension, and stroke were also analyzed.
Statistical Analysis
The bivariate analysis was used to see the distribution of tobacco use. The prevalence of chronic morbidities was estimated for smokers and smokeless tobacco users. Missing values were excluded from the analysis. The estimates were weighted using the 2001 Indian Census population for the age–year-specific distribution of the population. The risks (odds ratios) of each chronic condition were estimated for smokeless tobacco users, taking smoking as the reference category. The odds ratio for hypertension with no education and hypertensive with poor household (belonging to lowest wealth quite) was also estimated. The odds ratio was adjusted for age, gender, place of residence, religion, caste, education, wealth quintile, and states. The logistic regression was used to estimate the odds ratio. The outcome variables were binary and logistic regression is appropriate for binary outcomes. Logistic regression converts the binary outcome into probability and generates odds ratios for each response variables. Data analyses were performed using STATA version 12.0 software.
Results
Table 1 shows the socioeconomic distribution of the sample. A high percentage of smokeless tobacco users and smokers belong to higher age groups (aged above 50 years). More than 80% of the sampled tobacco users (both smoker and smokeless) belong to rural areas. Almost 80% of smokers were males, while around half of smokeless tobacco users were males. Education was also similar in both of the tobacco users. Except gender, all the other socioeconomic characteristics are similar for both of the tobacco user in our sampled population.
Table 1
| Socioeconomic characteristics | Smoking |
Smokeless |
Both (smoking and smokeless) |
|||
|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |
| Age groups | ||||||
| 18–29 | 38 | 2.8 | 143 | 6.1 | 13 | 4.0 |
| 30–49 | 281 | 20.9 | 573 | 24.6 | 70 | 21.3 |
| 50–59 | 472 | 35.1 | 708 | 30.4 | 107 | 32.6 |
| 60–69 | 362 | 26.9 | 545 | 23.4 | 94 | 28.7 |
| 70 and above | 192 | 14.3 | 358 | 15.4 | 44 | 13.4 |
| Place of residents | ||||||
| Urban | 235 | 17.5 | 437 | 18.8 | 51 | 15.5 |
| Rural | 1,110 | 82.5 | 1,890 | 81.2 | 277 | 84.5 |
| Gender | ||||||
| Male | 1,130 | 84.0 | 1,145 | 49.2 | 292 | 89.0 |
| Female | 215 | 16.0 | 1,182 | 50.8 | 36 | 11.0 |
| Religion | ||||||
| Muslim | 192 | 14.3 | 327 | 14.1 | 41 | 12.5 |
| Hindu | 1,129 | 83.9 | 1,914 | 82.3 | 278 | 84.8 |
| Others | 24 | 1.8 | 86 | 3.7 | 9 | 2.7 |
| Caste/tribe | ||||||
| Scheduled caste/tribe | 379 | 28.4 | 701 | 30.6 | 98 | 29.9 |
| Others | 957 | 71.6 | 1,592 | 69.4 | 230 | 70.1 |
| Education | ||||||
| No education/less than primary | 807 | 60.0 | 1,464 | 62.9 | 182 | 55.5 |
| Primary | 227 | 16.9 | 351 | 15.1 | 61 | 18.6 |
| Secondary | 135 | 10.0 | 251 | 10.8 | 43 | 13.1 |
| Higher secondary and above | 176 | 13.1 | 261 | 11.2 | 42 | 12.8 |
| Wealth quintile | ||||||
| Lowest | 284 | 21.1 | 542 | 23.6 | 75 | 22.9 |
| Second | 341 | 25.4 | 520 | 22.6 | 64 | 19.6 |
| Third | 253 | 18.8 | 456 | 19.8 | 86 | 26.3 |
| Fourth | 228 | 17.0 | 460 | 20.0 | 60 | 18.3 |
| Highest | 238 | 17.7 | 323 | 14.0 | 42 | 12.8 |
| States | ||||||
| Assam | 65 | 4.8 | 470 | 20.2 | 40 | 12.2 |
| Karnataka | 154 | 11.4 | 278 | 11.9 | 29 | 8.8 |
| Maharashtra | 79 | 5.9 | 407 | 17.5 | 33 | 10.1 |
| Rajasthan | 415 | 30.9 | 219 | 9.4 | 60 | 18.3 |
| Uttar Pradesh | 295 | 21.9 | 512 | 22.0 | 109 | 33.2 |
| West Bengal | 337 | 25.1 | 441 | 19.0 | 57 | 17.4 |
Socioeconomic characteristics of the sampled population.
The prevalence of hypertension (self-reported) was higher for smokeless tobacco users but the prevalence of hypertension based on blood pressure levels was almost same for smokers and smokeless tobacco users (Figure 1) the prevalence of diabetes, stroke, and CLD was higher for smokers. The prevalence of asthma and underweight was higher for smokeless tobacco.
Figure 1
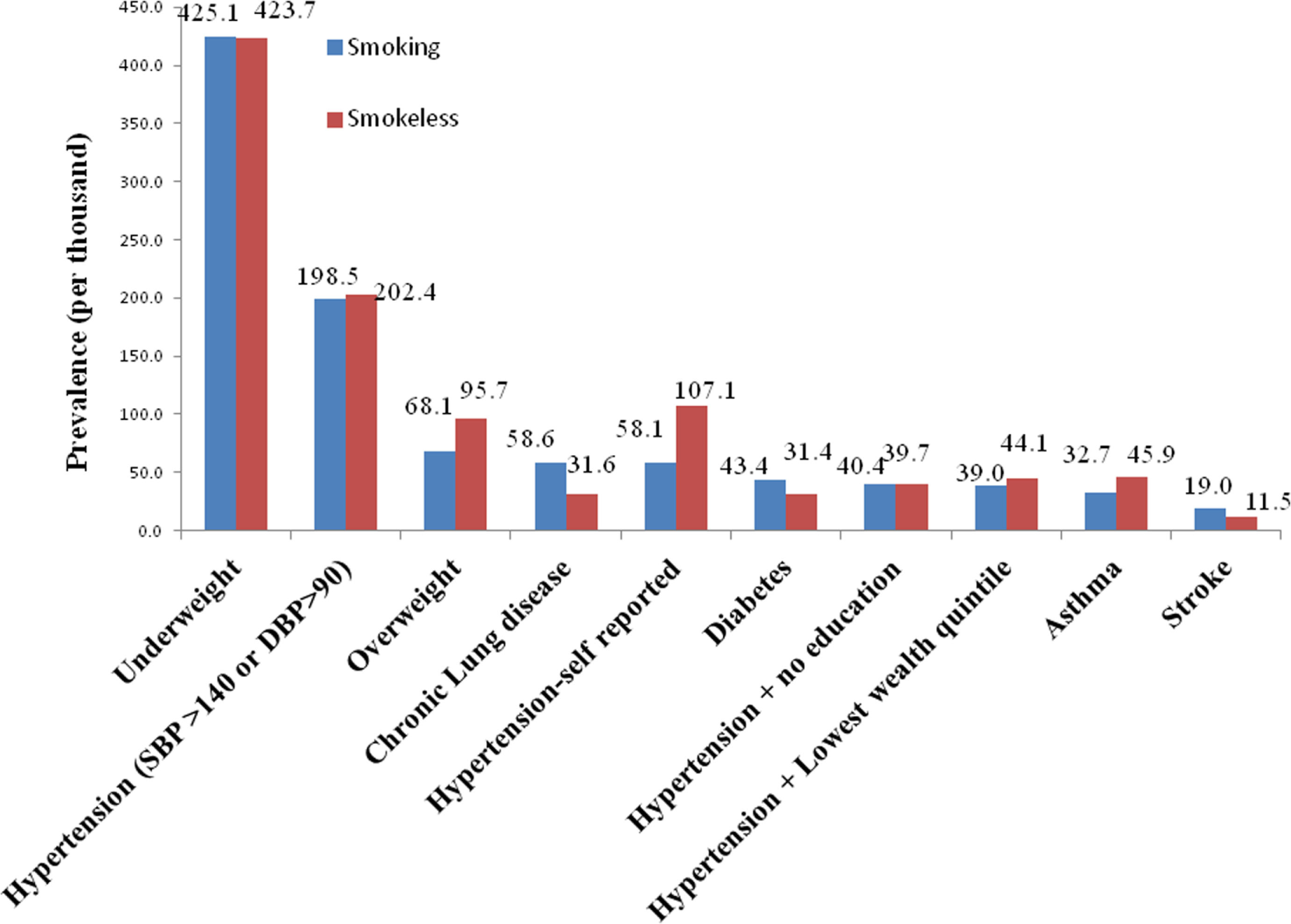
Prevalence of morbidities (per thousand) among smokers and smokeless tobacco users.
The odds ratios of chronic diseases were estimated taking smoking as the reference category (Table 2). Adjusted odds ratios for diabetes, asthma, hypertension (self-reported and measured) for smokeless tobacco user were compared to smoking and the differences were not statistically significant. The odds ratio of hypertension for low education and for people belonging to lowest wealth quintiles household was also not significant, except for CLDs. The risk of CLD was less among smokeless tobacco users compared to smokers. A similar finding has also been found for duration and amount of smokeless tobacco user (Tables 3 and 4). The odds ratio of hypertension was not significant for smokeless tobacco users consuming less than 10 g per day as well as consuming 10 g or more when compared to smoking (less than 10 U per day). There was also no significant difference found for the odds ratio of hypertension when compared to the duration of smokeless tobacco use with smoking (Table 4).
Table 2
| Smokeless |
Both (smoking and smokeless) |
Pseudo R-square | |||
|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | ||
| Stroke | 0.73 (0.43–1.24) | 0.372 | 0.73 (0.28–1.93) | 0.575 | 0.056 |
| Diabetes | 1.17 (0.82–1.67) | 0.776 | 1.00 (0.55–1.83) | 0.980 | 0.068 |
| Chronic lung diseases (CLDs) | 0.64 (0.45–0.91) | 0.040 | 0.72 (0.41–1.27) | 0.183 | 0.053 |
| Asthma | 1.21 (0.89–1.64) | 0.131 | 0.74 (0.42–1.30) | 0.304 | 0.049 |
| CLDs and Asthma | 1.04 (0.77–1.31) | 0.950 | 0.80 (0.51–1.23) | 0.310 | 0.052 |
| Hypertension | 1.24 (0.98–1.58) | 0.359 | 0.93 (0.60–1.44) | 0.656 | 0.080 |
| Systolic BP > 140 | 1.17 (0.95–1.43) | 0.259 | 0.84 (0.58–1.21) | 0.438 | 0.049 |
| diastolic BP > 90 | 1.12 (0.93–1.34) | 0.398 | 1.15 (0.86–1.54) | 0.165 | 0.013 |
| Hypertension (systolic BP > 140 or diastolic BP > 90) | 1.13 (0.96–1.34) | 0.352 | 1.09 (0.83–1.45) | 0.299 | 0.019 |
| Underweight | 0.79 (0.68–0.92) | 0.035 | 1.01 (0.78–1.31) | 0.624 | 0.602 |
| Overweight | 1.07 (0.81–1.40) | 0.391 | 0.71 (0.42–1.20) | 0.292 | 0.078 |
| Hypertensive + no education | 1.33 (0.92–1.91) | 0.554 | 1.46 (0.85–2.52) | 0.143 | 0.022 |
| Hypertensive + poor | 1.12 (0.80–1.56) | 0.548 | 1.42 (0.85–2.38) | 0.277 | 0.067 |
Odds ratio (95% CI) of chronic diseases comparing smokeless tobacco with smoking.
Reference category is smoking.
Table 3
| Smoking (10 years and above) |
Smokeless (less than 10 years) |
Smokeless (10 years and more) |
Both (smoking and smokeless) |
Pseudo R-square | |||||
|---|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | ||
| Chronic lung diseases (CLDs) | 1.08 (0.67–1.73) | 0.763 | 0.75 (0.47–1.17) | 0.206 | 0.55 (0.25–1.23) | 0.144 | 0.69 (0.37–1.32) | 0.266 | 0.061 |
| Asthma | 0.77 (0.48–1.22) | 0.268 | 1.22 (0.83–0.79) | 0.319 | 1.03 (0.55–1.93) | 0.920 | 0.66 (0.35–1.21) | 0.178 | 0.046 |
| CLDs and asthma | 0.88 (0.61–1.27) | 0.485 | 0.98 (0.71–1.36) | 0.909 | 0.75 (0.43–1.29) | 0.292 | 0.75 (0.46–1.20) | 0.225 | 0.054 |
| Hypertensive (Systolic BP > 140 or diastolic BP > 90) | 0.92 (0.60–1.40) | 0.349 | 0.72 (0.46–1.14) | 0.794 | 1.12 (0.74–1.70) | 0.641 | 1.09 (0.80–1.49) | 0.573 | 0.015 |
| Hypertensive + no education | 0.88 (0.24–2.28) | 0.885 | 1.01 (0.37–2.79) | 0.918 | 1.22 (0.48–3.09) | 0.451 | 1.16 (0.46–1.53) | 0.548 | 0.020 |
| Hypertensive + poor | 1.24 (0.48–3.22) | 0.379 | 1.64 (0.62–4.31) | 0.241 | 1.32 (0.52–3.34) | 0.39 | 1.07 (0.45–2.55) | 0.688 | 0.066 |
Odds ratio (95% CI) of chronic diseases comparing amount of smoking and smokeless tobacco consumption.
Reference category is smoking (less than 10 years).
Table 4
| Smoking (10 U per day and more) |
Smokeless (less than 10 g per day) |
Smokeless (10 g per day and more) |
Both (smoking and smokeless) |
Pseudo R-square | |||||
|---|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | ||
| CLDs | 1.31 (0.46–3.75) | 0.619 | 1.21 (0.40–3.71) | 0.734 | 0.80 (0.28–2.29) | 0.675 | 0.86 (0.28–2.30) | 0.675 | 0.082 |
| Asthma | 1.20 (0.42–3.41) | 0.738 | 2.00 (0.68–5.89) | 0.208 | 1.53 (0.54–4.32) | 0.423 | 0.90 (0.29–2.84) | 0.863 | 0.067 |
| CLDs and Asthma | 1.48 (0.63–3.50) | 0.372 | 1.79 (0.73–4.37) | 0.203 | 1.38 (0.5.9–3.25) | 0.459 | 1.17 (0.46–2.95) | 0.741 | 0.054 |
| Hypertensive (systolic BP > 140 or diastolic BP > 90) | 0.85 (0.66–1.10) | 0.204 | 1.04 (0.85–1.28) | 0.828 | 0.99 (0.71–1.36) | 0.952 | 0.88 (0.54–1.42) | 0.596 | 0.0126 |
| Hypertensive + no education | 0.87 (0.50–1.52) | 0.459 | 1.29 (0.82–2.51) | 0.465 | 0.94 (0.45–1.98) | 0.865 | 1.50 (0.52–4.31) | 0.45 | 0.0199 |
| Hypertensive + poor | 1.12 (0.66–1.87) | 0.613 | 1.17 (0.76–1.80) | 0.339 | 1.22 (0.65–2.31) | 0.569 | 1.50 (0.54–4.21) | 0.44 | 0.0665 |
Odds ratio (95% CI) of chronic diseases comparing duration of smoking and smokeless tobacco consumption.
Reference category is smoking (less than 10 U per day).
Discussion
Globally, smoking is one of the leading causes of premature mortality (29, 30). The reports also suggest that the impact of smoking have been subdued in low-middle-income countries compared to high-income countries (12, 13, 31). There had been a little debate over the impact of smokeless tobacco use on chronic diseases, due to variability in the type of smokeless tobacco products available globally as well as within countries. Smokeless tobacco is the most common form of tobacco use in India (8, 32, 33). Smokeless tobacco use is very common among women tobacco users, which is similar to other studies (9, 34, 35). Many studies have found statistical significant differences for smokers and smokeless tobacco users on non-communicable disease incidence compared to non-tobacco users (19, 35, 36). We found only the odds ratio of CLD to be significantly lower in smokeless tobacco users compared to smoked tobacco users. Smoking is related to an increased risk of type 2 diabetes compared to non-smokers (36). Studies in Sweden have observed higher risk of stroke among smokeless tobacco user compared with non-tobacco user (22). The mortality due to CVDs has also reported higher among smokeless tobacco users compared to non-tobacco users (21). Studies in India have also exhibited higher chances of chronic illness among smokeless tobacco compared with non-tobacco users (25, 26). We did not found studies comparing smokeless with smoking in the context of chronic illness. Our study adds to the previous finding, that there are no less risk of chronic diseases for smokeless tobacco users compared to smoking.
The chemical composition of both form of tobacco is very similar (6). However, chemical properties due to burning of the tobacco may have contributed to higher risk of lung related diseases (6, 7). Chewing tobacco can be related to more exposure to the chemicals causing cancers related with mouth and throat (7). Studies have also found that use of less harmful smokeless tobacco is related to more risk of smoked tobacco (37). Therefore, smokeless tobacco cannot be used as cessation tool for smoking (37).
We have also not found significant influence on non-communicable diseases by duration and amount of tobacco consumption, comparing smoking and smokeless tobacco users. Our study suggests that the use of smokeless tobacco may be as harmful as smoking in the context of chronic diseases. As we know that the smokeless tobacco is the most common form of tobacco consumed in India (8, 34, 35). The policies preventing tobacco epidemic must focus on containing the use of smokeless tobacco along with smoking.
There are several limitations of the study. The analysis is based on the cross-sectional survey; based on secondary data, the causal relationships cannot be established. Data on various types of smokeless tobacco use were not available; the risks may also differ by types of smokeless tobacco. Some of the chronic conditions and tobacco use were self-reported, which may influence the result.
Conclusion
The study has shown that there is no difference for the risk of chronic conditions between smoked and smokeless tobacco users. The risk of hypertension was also similar in both form of tobacco when comparing amount and duration of smoking with smokeless tobacco consumption. As the smokeless tobacco is the most common form of tobacco used in India, the policy must address in decreasing as well as preventing the use of any form of tobacco in India.
Statements
Ethics statement
The study is based on secondary data analysis. No data were collected for this study. The data are available for free on the WHO (World Health Organization) website. The WHO-SAGE 2007-08 study is approved by WHO and their partner organization in various countries (www.who.int/healthinfo/systems/sage). There is no need for ethical clearance.
Author contributions
AA has contributed toward conceptualization of the study, data analysis and writing the manuscript. MS has contributed toward data analysis, writing, and revising the manuscript.
Funding
We did not receive any grants from any funding agency in public, commercial, or non-profit sectors for conducting this study.
Acknowledgments
We would like to thank WHO (World Health Organization) for allowing us to use the India level Global Ageing and Adult Health (SAGE) 2007-08 data for our analysis. We would like to thank Mr. Abhijit Basu Biswas (State Routine Immunization MIS & SBCC Consultant, Assam) for providing guidance and support for the study. We are thankful to Dr. Pinaki Sen Sarma (State RMNCH+A Consultant, Arunachal Pradesh) for providing suggestion to improve the writing of the manuscript.
Conflict of interest
The authors have declared that there are no competing interests exist in the preparation of this article.
Abbreviations
CVD, cardiovascular diseases, WHO, World Health Organization, BMI, body mass index, SAGE, Study on Global Ageing and Adult Health, PSU, primary sampling units.
References
1
World Atlas. The Leading Causes of Death in India. (2017). Available from: http://www.worldatlas.com/articles/the-leading-causes-of-death-in-india.html
2
Patel V Chatterji S Chisholm D Ebrahim S Gopalakrishna G Mathers C et al Chronic diseases and injuries in India. Lancet (2011) 377:413–28.10.1016/S0140-6736(10)61188-9
3
Kshatriya GK Acharya SK . Triple burden of obesity, undernutrition, and cardiovascular disease risk among Indian tribes. PLoS One (2016) 11(1):e0147934.10.1371/journal.pone.0147934
4
Panwar RB Gupta R Gupta BK Raja S Vaishnav J Khatri M et al Atherothrombotic risk factors & premature coronary heart disease in India: a case control study. Indian J Med Res (2011) 134(1):26–32.
5
Buttar SH Li T Ravi N . Prevention of cardiovascular diseases: role of exercise, dietary interventions, obesity and smoking cessation. Exp Clin Cardiol (2005) 10(4):229–49.
6
Stepanov I Jensen J Hatsukami D Hecht SS . New and traditional smokeless tobacco: comparison of toxicant and carcinogen levels. Nicotine Tob Res (2008) 10(12):1773–82.10.1080/14622200802443544
7
Benowitz NL Porchet H Sheiner L Jacob P . Nicotine absorption and cardiovascular effects with smokeless tobacco use: comparison with cigarettes and nicotine gum. Clin Pharmacol Ther (1988) 44(1):23–8.10.1038/clpt.1988.107
8
International Institute for Population Sciences and Ministry of Health and Family Welfare, Government of India. Global Adult Tobacco Survey (GATS): India: 2009-2010. (2010). Available from: http://www.searo.who.int/tobacco/documents/2010-pub2.pdf
9
Ministry of Health and Family Welfare: Government of India. Smokeless Tobacco and Public Health in India. New Delhi (2016). Available from: http://www.searo.who.int/india/tobacco/smokeless_tobacco_and_public_health_in_india.pdf?ua=1
10
Reddy SS Shaik Hyder Ali KH . Estimation of nicotine content in popular Indian brands of smoking and chewing tobacco products. Indian J Dent Res (2008) 19(2):88–9.10.4103/0970-9290.40458
11
Toppo NA Gupta V Saklecha D . Tobacco consumption among tribal adolescents of central India: a cross sectional study. J Evol Med Dent (2016) 5(59):4137–41.10.14260/jemds/2016/945
12
Hosseinpoor AR Parker LA d’Espaignet ET Chatterji S . Social determinants of smoking in low- and middle-income countries: results from the world health survey. PLoS One (2011) 6(5):e20331.10.1371/journal.pone.0020331
13
Hajat A Kaufman JS Rose KM Siddiqi A Thomas JC . Do the wealthy have a health advantage? Cardiovascular disease risk factors and wealth. Soc Sci Med (2010) 71:1935–42.10.1016/j.socscimed.2010.09.027
14
Rani M Bonu S Jha P Nguyen SN Jamjoum L . Tobacco use in India: prevalence and predictors of smoking and chewing in a national cross sectional household survey. Tob Control (2003) 12(4):e4.10.1136/tc.12.4.e4
15
Mohan P Lando HA Sigamani P . Taxation on tobacco in India tool for tobacco control. Econ Polit Wkly (2017) 52(5):20–3.
16
WHO, International Agency for Research on Cancer (IARC). Monographs on the Evaluation of Carcinogenic Risks to Humans: Tobacco Smoke and Involuntary Smoking. Lyon: IARC Press (2004). Available from: https://monographs.iarc.fr/ENG/Monographs/vol83/mono83.pdf
17
Centers for Disease Control and Prevention (US), National Center for Chronic Disease Prevention and Health Promotion (US), Office on Smoking and Health (US). How Tobacco Smoke Causes Disease: The Biology and Behavioral Basis for Smoking-Attributable Disease: A Report of the Surgeon General. Atlanta (2010). Available from: https://www.ncbi.nlm.nih.gov/books/NBK53017/
18
Yatsuya H Folsom AR ARIC Investigators . Risk of incident cardiovascular disease among users of smokeless tobacco in the atherosclerosis risk in communities (ARIC) study. Am J Epidemiol (2010) 172(5):600–5.10.1093/aje/kwq191
19
Boffetta P Straif K . Use of smokeless tobacco and risk of myocardial infarction and stroke: systematic review with meta-analysis. Br Med J (2009) 339:b3060.10.1136/bmj.b3060
20
Haglund B Eliasson M Stenbeck M Rosen M . Is moist snuff use associated with excess risk of IHD or stroke? A longitudinal follow-up of snuff users in Sweden. Scand J Public Health (2007) 35(6):618–22.10.1080/14034940701436949
21
Wennberg P Eliasson M Hallmans G Johansson L Boman K Jansson JH . The risk of myocardial infarction and sudden cardiac death amongst snuff users with or without a previous history of smoking. J Intern Med (2007) 262(3):360–7.10.1111/j.1365-2796.2007.01813.x
22
Asplund K Nasic S Janlert U Stegmayr B . Smokeless tobacco as a possible risk factor for stroke in men: a nested case-control study. Stroke (2003) 34(7):1754–9.10.1161/01.STR.0000076011.02935.A1
23
Hergens MP Alfredsson L Bolinder G Lambe M Pershagen G Ye W . Long-term use of Swedish moist snuff and the risk of myocardial infarction amongst men. J Intern Med (2007) 262(3):351–9.10.1111/j.1365-2796.2007.01816.x
24
Ebbert JO Rowland LC Montori VM Vickers KS Erwin PJ Dale LC . Treatments for spit tobacco use: a quantitative systematic review. Addiction (2003) 98(5):569–83.10.1046/j.1360-0443.2003.00378.x
25
Gupta R Gupta N Khedar RS . Smokeless tobacco and cardiovascular disease in low and middle income countries. Indian Heart J (2013) 65(4):369–77.10.1016/j.ihj.2013.06.005
26
Pandey A Patni N Sarangi S Singh M Sharma K Vellimana AK et al Association of exclusive smokeless tobacco consumption with hypertension in an adult male rural population of India. Tob Induc Dis (2009) 5(1):15.10.1186/1617-9625-5-15
27
World Health Organization. Health Statistics and Information Systems: WHO Study on Global Ageing and Adult Health (SAGE): 2007-08. (2012). Available from: http://www.who.int/healthinfo/sage/en/
28
Kowal P Chatterji S Naidoo N Biritwum R Fan W Lopez Ridaura R et al Data resource profile: the World Health Organization STudy on global AGEing and adult health (SAGE). Int J Epidemiol (2012) 41(6):1639–49.10.1093/ije/dys210
29
World Health Organization. WHO-Media Centre: Tobacco Fact Sheet 2016. (2016). Available from: http://www.who.int/mediacentre/factsheets/fs339/en/
30
Samet JM . Tobacco smoking: the leading cause of preventable disease worldwide. Thorac Surg Clin (2013) 23(2):103–12.10.1016/j.thorsurg.2013.01.009
31
Hu T Mao Z Liu Y de Beyer J Ong M . Smoking, standard of living, and poverty in China. Tob Control (2005) 14(4):247–50.10.1136/tc.2004.010777
32
Mishra GA Pimple SA Shastri SS . An overview of the tobacco problem in India. Indian J Med Paediatr Oncol (2012) 33(3):139–45.10.4103/0971-5851.103139
33
Chadda RK Sengupta SN . Tobacco use by Indian adolescents. Tob Induc Dis (2003) 1(2):111–9.10.1186/1617-9625-1-8
34
Asplund K . Smokeless tobacco and cardiovascular disease. Prog Cardiovasc Dis (2003) 45(5):383–94.10.1053/pcad.2003.00102
35
Martin-Timon I Sevillano-Collantes C Segura-Galindo A del Canizo-Gomez FJ . Type 2 diabetes and cardiovascular disease: have all risk factors the same strength?World J Diabetes (2014) 5(4):444–70.10.4239/wjd.v5.i4.444
36
Thankappan KR Thresia CU . Tobacco use & social status in Kerala. Indian J Med Res (2007) 126(4):300–8.
37
Bask M Melkersson M . Should one use smokeless tobacco in smoking cessation programs?Eur J Health Econ (2003) 4(4):263–70.10.1007/s10198-003-0197-y
Summary
Keywords
smokeless tobacco, smoking, hypertension, chronic diseases, India
Citation
Anand A and Sk MIK (2017) The Risk of Hypertension and Other Chronic Diseases: Comparing Smokeless Tobacco with Smoking. Front. Public Health 5:255. doi: 10.3389/fpubh.2017.00255
Received
26 May 2017
Accepted
07 September 2017
Published
22 September 2017
Volume
5 - 2017
Edited by
Su Yon Jung, University of California, Los Angeles, United States
Reviewed by
Setor K. Kunutsor, University of Bristol, United Kingdom; Eugenia M. Bastos, Bastos Consulting, United States
Updates
Copyright
© 2017 Anand and Sk.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Md Illias Kanchan Sk, illiaskanchan90@gmail.com
Specialty section: This article was submitted to Epidemiology, a section of the journal Frontiers in Public Health
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.