 Parfait Wouékpé
Parfait Wouékpé Cyriaque Dégbey
Cyriaque Dégbey Alphonse Kpozéhouen
Alphonse Kpozéhouen- 1Doctoral School of Health Sciences, Faculty of Health Sciences, University of Abomey-Calavi, Abomey-Calavi, Benin
- 2Department of Health and Environment, Regional Institute of Public Health, University of Abomey-Calavi, Abomey-Calavi, Benin
- 3Department of Epidemiology and Biostatistics, Regional Institute of Public Health, University of Abomey-Calavi, Abomey-Calavi, Benin
Objectives: This study assessed the level of knowledge of community health workers (CHWs) regarding water, hygiene, and sanitation (WASH) in the Comè-Bopa-Grand Popo-Houéyogbé health zone in Benin.
Methods: A cross-sectional survey was conducted among 160 CHWs selected randomly. Data were collected using a structured questionnaire and analyzed with SPSS 21.0. Logistic regression was used to identify factors associated with CHW knowledge.
Results: Most CHWs (68.8%) had insufficient knowledge of their roles in WASH. Factors significantly associated with good knowledge included Mina ethnicity (OR = 0.3; 95% CI: 0.1–0.9), being married (OR = 10.0; 95% CI: 1.3–77.7), training on activity packages (OR = 3.3; 95% CI: 1.7–10.0), supervision by a qualified agent (OR = 10.2; 95% CI: 2.5–40.6), and participation in group follow-up sessions (OR = 10.0; 95% CI: 5.0–48.9). Multivariate analysis showed that attending at least two group sessions greatly increased the likelihood of good knowledge (OR = 23.9; 95% CI: 5.3–107.7).
Conclusion: Strengthening CHW training, regular follow-up, and incentives is essential to improve WASH-related knowledge and public health impact.
Introduction
Access to quality water, proper hygiene and adequate sanitation is a major public health issue, particularly in developing countries. Several studies show that waterborne diseases, such as diarrhea and cholera, represent a significant cause of morbidity and mortality (1). According to the World Health Organization (WHO) (2), infections linked to contaminated water continue to affect millions of people each year, particularly in regions with inadequate sanitation infrastructure. In Benin, reports from the Ministry of Health indicate that a significant proportion of the population is exposed to health risks due to limited access to drinking water, with a national rural service rate estimated at 79.4% in December 2023, and optimal sanitation conditions (3).
In this context, community health workers, these field actors who act as a link between health authorities and the population, play a key role in disseminating good hygiene and sanitation practices (4). The community health worker is any person, whether a member of the community or not, who has received training to deal with the health problems of individuals and the community and to work in close collaboration with human, animal and environmental health services, local elected officials, the local component of the health system (CoLoSS) and other actors involved in community health, without necessarily being a health professional. He has a threefold mission: (i) to bring health services to the very place where people live and work; (ii) to help communities recognize their own health needs; (iii) to help the population solve their own health problems. He is therefore responsible for ensuring health promotion through information, education and communication on the one hand and, on the other hand, the management of a case (non-drug, without invasive procedures), its referral and follow-up. To do this, he will carry out home visits and focus groups (5, 6).
However, while global statistics on the prevalence of conditions related to poor water quality are available, it is clear that the specific knowledge of community health workers regarding their roles and responsibilities remains poorly documented. Indeed, current literature often focuses on global health indicators without exploring in depth how these local actors perceive and implement guidelines relating to hygiene promotion and sanitation (7, 8). This gap is particularly worrying in specific areas such as Comè-Bopa-Grand Popo-Houéyogbé, where problems related to water quality and sanitation conditions are exacerbated by fragile socio-economic contexts with telling epidemiological data such as the most frequent ailments received in consultations, malaria (47%), acute respiratory infections (16.8%), diarrhea and other gastrointestinal ailments (7%) and at the level of children under 5 years these data are more pronounced acute respiratory infections (28.3%), diarrhea and other gastrointestinal ailments (8.7%) (9).
These health indicators highlight the magnitude of water and sanitation-related challenges in the study area. However, they do not provide information on how community health workers (CHWs), who are the frontline actors for health promotion, understand and implement their roles. If CHWs have limited or inaccurate knowledge, their capacity to influence household practices is reduced, which may partly explain the persistence of preventable diseases. Therefore, assessing their level of knowledge is essential to better understand their effective contribution to the observed health outcomes.
The lack of detailed data on the training, understanding and application of responsibilities by these relays raises questions about the effectiveness of public health interventions in the region.
In view of these findings, this work aims to study the level of knowledge of community health workers on their roles and responsibilities in water quality, hygiene and sanitation in the Comè-Bopa-Grand Popo-Houéyogbé health zone.
Methods
Setting
This study took place in the health zone of Comè, Bopa, Grand-Popo and Houéyogbé. It covers an area of 1,120 km2 and is located in the Mono department of Benin (10). The health zone has three large lakes: Lake Ahémé, Lake Toho and Lake Togbadji. The main rivers are: the Mono, the Couffo and the Sazué (11) (Figure 1).
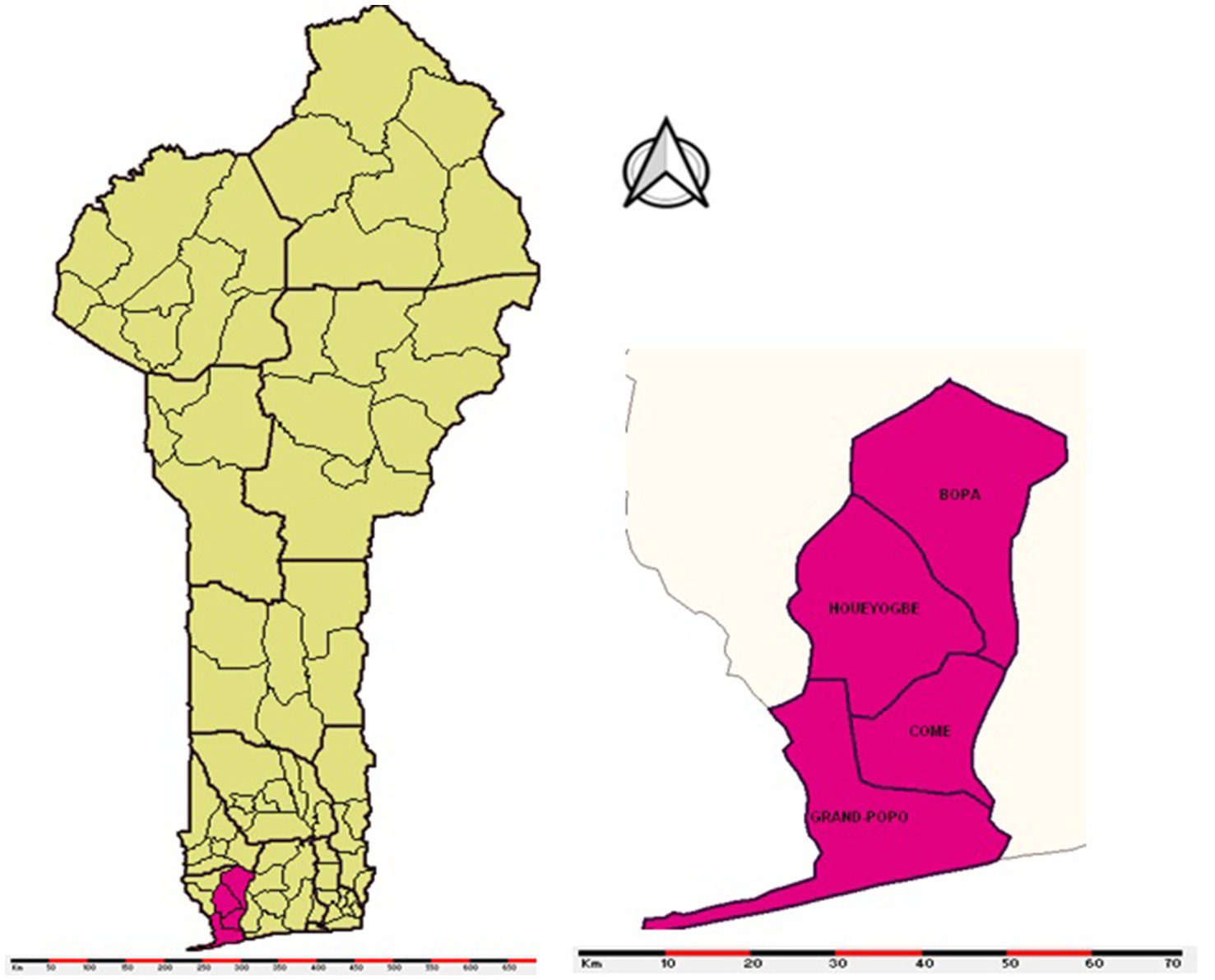
Figure 1. Geographic map of the Comè Bopa Grand Popo Houéyogbé health zone, 2024.
Study design
This was a descriptive and analytical cross-sectional study aimed at assessing the level of knowledge of community health workers regarding their roles and responsibilities in maintaining water quality, hygiene and sanitation. This investigation, conducted in the field, involved three target groups: community health workers, households in the villages covered by these relays and health workers (including post chiefs). Data was collected from September 18 to October 15, 2024.
Participants
To be included in the study, participants were required to meet the following criteria: be a community health worker, a member of a household in a village served by a relay, or a health worker present at the post, and have resided in the area for at least 1 year. Conversely, new community health workers (with less than 1 year of experience), health workers on leave, sick or absent during the survey, as well as people residing in the area for less than 1 year were excluded.
This was a two-stage sampling. In the first stage, the most populated districts were selected in each stratum (each commune in the health zone) proportionally to the size of the population. In the second stage, the villages were selected in the selected districts randomly based on their list (approximately 40 villages per district). Then, in each selected village, the relay was systematically counted. The sample size was calculated by applying the Schwartz formula where n is the size of the sample drawn, p is the theoretical percentage of good knowledge among the RC (p = 0,0375), q (1-p) is the theoretical percentage of poor knowledge, Z 𝜶 is the Z score for the confidence level (95%) (here Z 𝜶 =1.96) and i the margin of error (i = 5%). This calculation made it possible to estimate a minimum size of 154 relays, adjusted to 160 to ensure a fair distribution (i.e., approximately 40 relays per municipality in the Health Zone).
Data sources/measurement
Data collection took place from September 18 to October 15, 2024, and was carried out primarily through direct interviews using a structured questionnaire administered to community health workers, households, and health workers. Field observations supplemented these interviews to adequately assess the population’s commitment to promoting a healthy environment.
Variables
Dependent variable
The dependent variable of the study was the level of knowledge of community health workers about their roles and responsibilities. This is the percentage of activities to be carried out notified by the RC. Thus, it was a dichotomous variable with the modalities:
• Good knowledge: a percentage of satisfactory answers greater than 50%
• Insufficient knowledge: A percentage of satisfactory answers less than or equal to 50%
Independent variables
Explanatory variables included:
• Factors: age, gender, level of education, religion, ethnicity, marital status, occupation, place of residence;
• Factors related to the community health workers task: seniority of at least 5 years, possession of an electronic device (smartphone or tablet), training on the activity packages to be carried out, training on hygiene and sanitation, monitoring by a community agent, the number of group monitoring sessions and continuing training;
• Factors: Free consultation at the CS, official presentation of the community health workers to the locality, benefits or bonuses, involvement in mass vaccination campaigns.
Statistical methods
Kobocollect software and data cleaning with SPSS version 21.0 software, we performed all statistical analyses using the same software. The chi-square test was used to assess the relationship between the level of knowledge of community relays and the explanatory variables. Bivariate and multiple logistic regression models were used to examine the probability of the level of knowledge of community relays as a function of the explanatory variables. The p-values obtained from the bivariate regression analysis were used to decide on the inclusion of variables in the multivariate model. Variables with a p-value less than 0.20 were included in the multivariate model. All independent variables that met the selection criterion (p < 0.20) were included in the final model, taking into account potential confounders. The association between the level of knowledge of community health workers and the explanatory variables was assessed by the odds ratio (OR) followed by their 95% confidence interval (95% CI).
Results
Sociodemographic characteristics of community relays
We surveyed 160 community health workers. Three out of four community relays were men and aged 25 to 45 (80%). The Sahouè ethnic group was predominant (56.9%), and the majority practiced a Christian (46.3%) or traditional (48.8%) religion.
Most RCs had a secondary education (71.3%) and lived in a common-law relationship (78.1%). Professionally, they were mainly artisans (30.6%) or retailers (22.6%). Almost all (97.5%) had resided in their village or neighborhood for more than 3 years (Table 1).
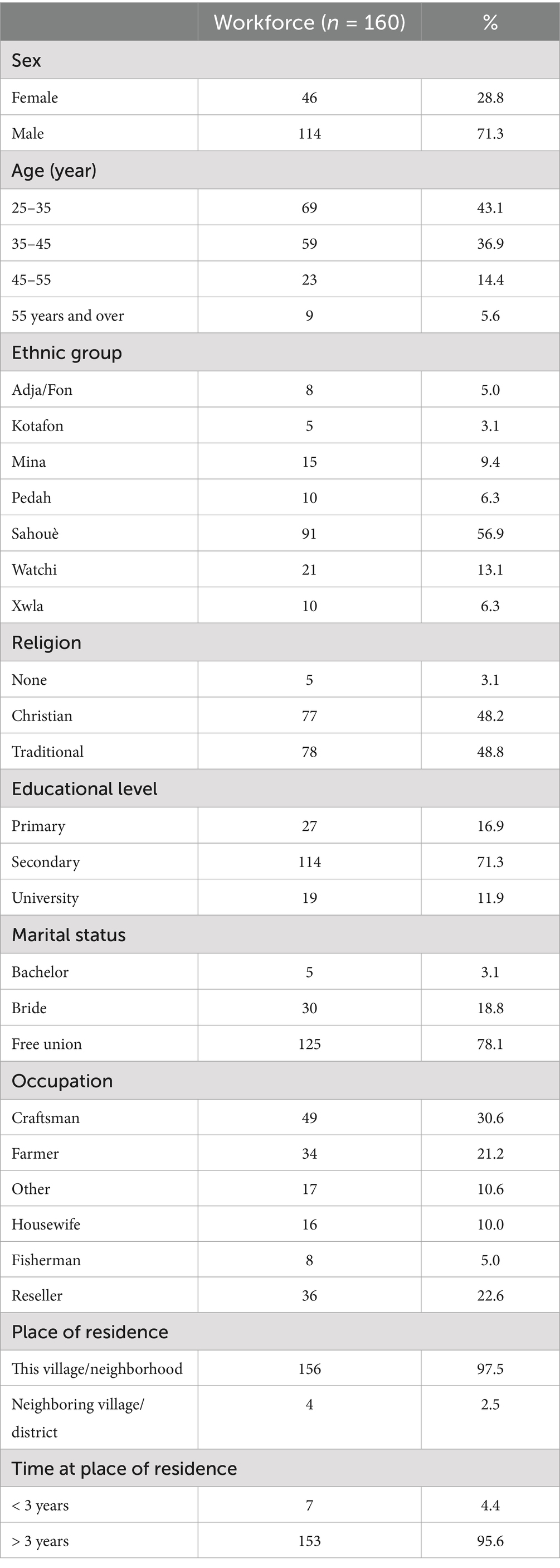
Table 1. Sociodemographic characteristics community relays in the Comè, Bopa, Grand Popo and Houéyogbé health zone in Benin in 2024.
Characteristics related to the task and benefits of the status of community relays
Almost all RCs (96.9%) had at least 4 years of experience and 81.9% had already used an Android tablet or smartphone. In addition, 85% had received training on the activity package, and 88.1% were trained on water, hygiene and sanitation; a Qualified Community Health Agent (QCHA) followed 91.3%. In addition, 66.3% had received in-service training, and 80% participated in at least three group follow-up sessions (Table 2).
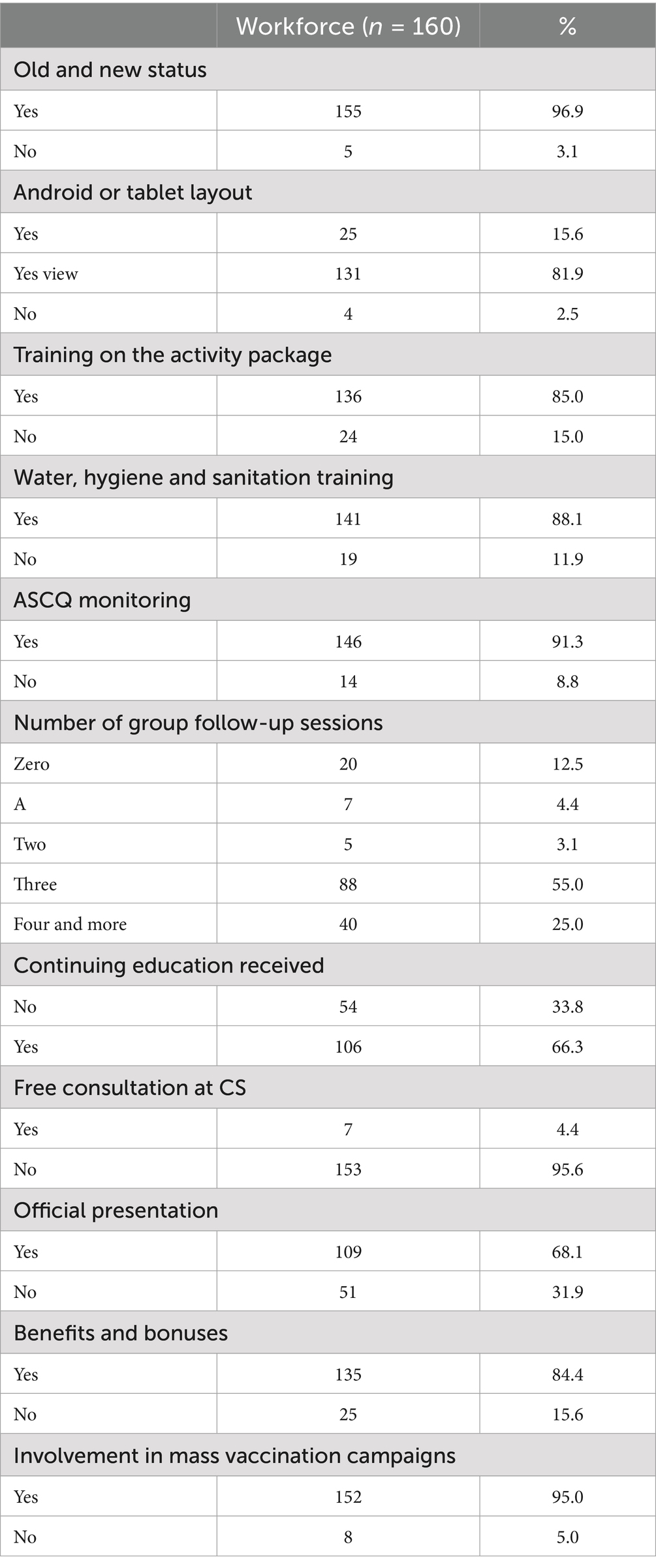
Table 2. Distribution of community relays according to their professional characteristics and the advantages linked to their status, health zone Comè, Bopa, Grand Popo and Houéyogbé, 2024.
Only 4.4% benefited from free consultations at the health center. However, 84.4% received bonuses and 95% participated in vaccination campaigns.
Knowledge of community relays on water, hygiene and sanitation
The results on the knowledge of the RCs show that 50% knew the types of activities carried out, but only 47.5% mastered their roles and responsibilities. Similarly, 93.1% organized communication for behavior change sessions, and 81.3% carried out household visits. Nevertheless, 31.2% had good knowledge while 68.8% had insufficient knowledge on water, hygiene and sanitation (Table 3).
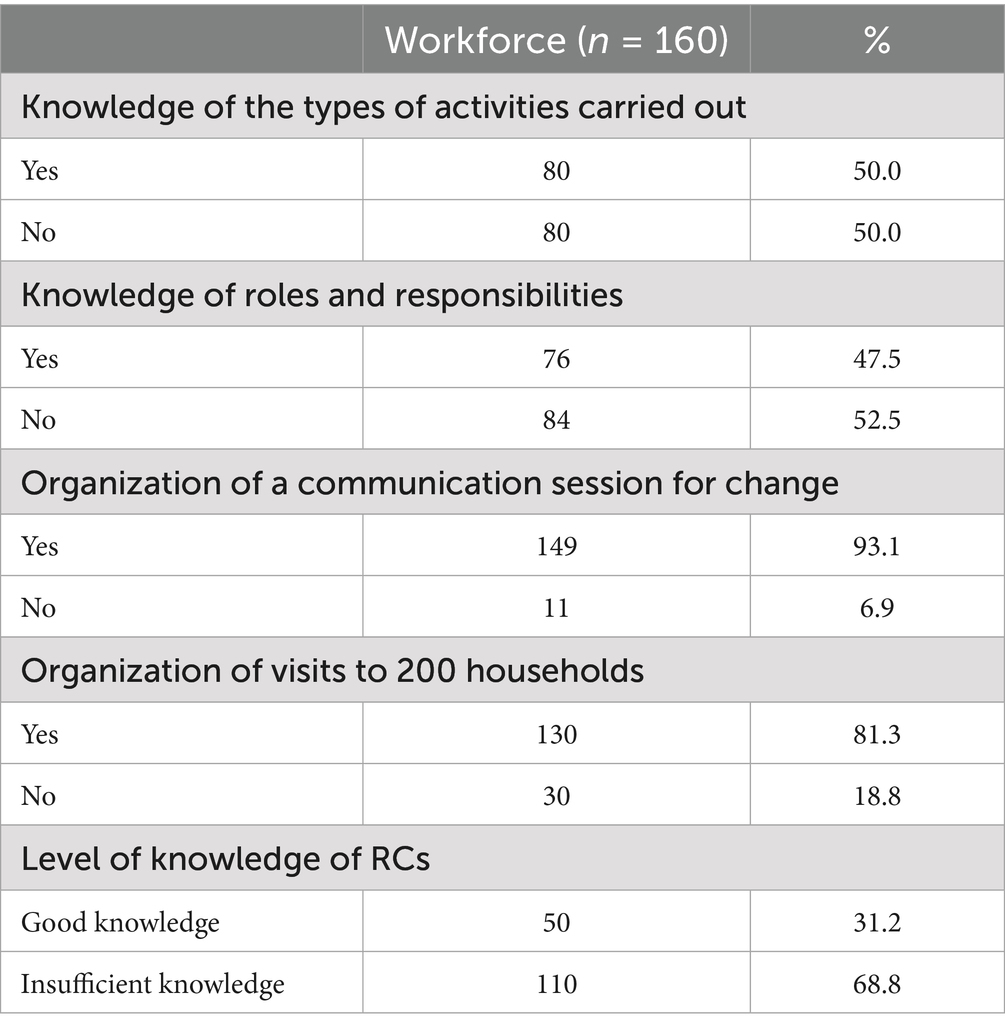
Table 3. Distribution of community relays according to their knowledge of their roles and responsibilities.
Factors influencing knowledge of community health workers
Several factors influenced knowledge of RCs, including: Ethnicity (OR = 0.3; 95% CI = [0.1–0.9]) and marital status (OR = 10.0; 95% CI = [1.3–77.7]) significantly influenced knowledge of RCs. RCs who received training on the activity package (OR = 3.3; 95% CI = [1.7–10.0]) and those followed by an ASCQ (OR = 10.2; 95% CI = [2.5–40.6]) were more likely to have good knowledge. The number of group follow-up sessions was a key factor: those who attended at least three sessions (OR = 10.0; 95% CI = [5.0–48.9]) were more likely to have good knowledge. The official presentation of RC at the locality (OR = 2.0; 95% CI = [1.1–5.0]), bonuses (OR = 2.0; 95% CI = [1.5–10.1]) and involvement in vaccination campaigns (OR = 10.0; 95% CI = [2.0–50.0]) are associated with good knowledge.
In the multivariate analysis, RCs who participated in two group follow-up sessions were 23.9 times more likely to have good knowledge about water, hygiene and sanitation compared to those who did not participate in any session (OR = 23.9; 95% CI = [5.31–107.72]) than the others (Table 4).
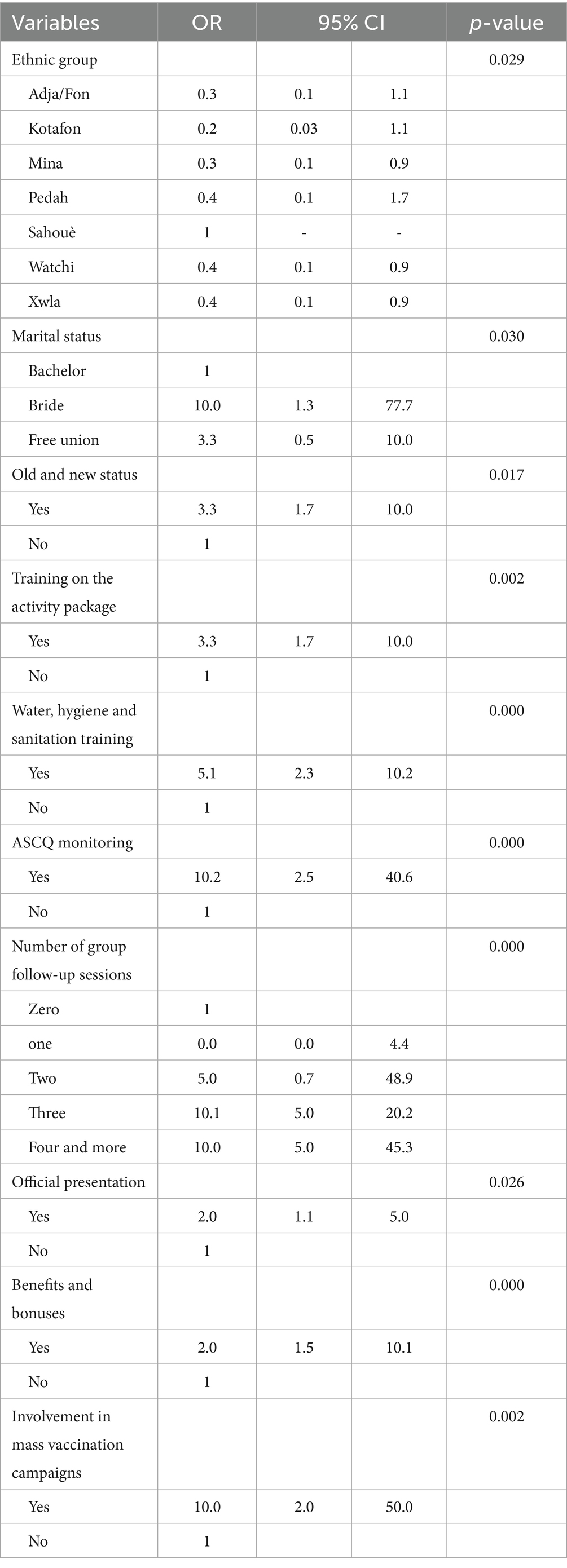
Table 4. Factors associated with knowledge of community relays in the Comè, Bopa, Grand Popo and Houéyogbé health zones in Benin in 2024.
Discussion
The results of this study show that 31.2% of RCs had good knowledge. Our findings highlight that CHW knowledge is strongly influenced by programmatic factors such as training, supervision, and recognition, rather than by individual characteristics such as age, sex, or education level. Specifically, CHWs who received refresher training, were supervised by a qualified agent, and participated in multiple group follow-up sessions had significantly better knowledge. Incentives such as official recognition and bonuses also played an important role. These results suggest that institutional support mechanisms are decisive for CHW performance. This aligns with evidence from other West African studies, which found that capacity building, continuous supervision, and motivational strategies are essential to ensure effective community health promotion in WASH (Table 5).
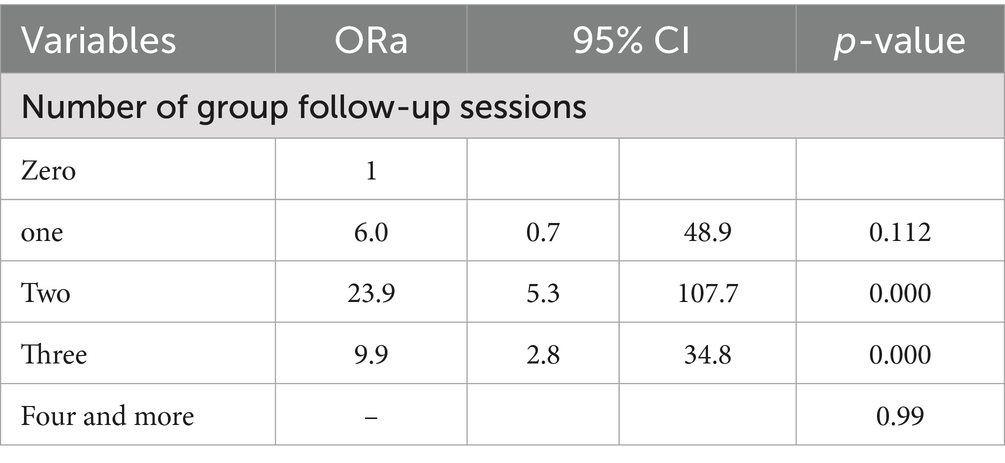
Table 5. Final model of the multivariate analysis resulting from logistic regression in the Comè, Bopa, Grand Popo and Houéyogbé health zones in Benin in 2024.
Nearly three-quarters of the CHWs were men and were predominantly between the ages of 25 and 45. The male predominance could be explained by sociocultural norms that favor men’s involvement in community roles. Studies conducted in Kenya and Côte d’Ivoire had observed a male predominance among community health workers, suggesting that this could be linked to the perception of community work as a responsibility requiring frequent travel and increased social interaction (12, 13). In contrast, a study from Ethiopia have reported a predominance of female CHWs, often explained by cultural acceptance of women in maternal and child health roles, and the perception that women can more effectively reach households for health promotion activities (14). This contrast highlights the influence of cultural norms and gender roles on CHW recruitment patterns.
The majority of RCs had reached a secondary level, which should theoretically make it easier for them to acquire knowledge about water, hygiene and sanitation. However, the high proportion of RCs with insufficient knowledge (68.8%) highlights that the level of education does not automatically guarantee a good understanding of health issues. A study conducted in Burkina Faso also showed that knowledge about hygiene and sanitation did not depend solely on the educational level, but also on the quality of the training received (15). Similarly, evidence from Ghana indicates that targeted, practical training adapted to local contexts significantly improves WASH knowledge compared to general health education, regardless of formal education level (16).
Training plays a key role in knowledge acquisition. Our results show that community workers who received training on the activity package (OR = 3.3; [1.7–10.0]) are more likely to have good knowledge. Studies in Côte d’Ivoire have shown that training adapted to local realities significantly improves the practices of community workers (15, 17).
Our results indicate that follow-up by the Qualified Community Health Worker and participation in-group follow-up sessions are determining factors. An analysis conducted in Uganda also highlighted the positive impact of monitoring community workers on improving their knowledge and commitment (18). Community workers who receive incentives and participate in mass vaccination campaigns have better knowledge of water, hygiene and sanitation practices; official recognition and financial benefits are key elements to motivate and retain community workers (12).
The results of our study are consistent with those of other research conducted in West Africa. An assessment conducted around Lake Nokoué in Benin showed that 56.79% of respondents had never received hygiene training and 84.29% did not have access to latrines (19, 20). Furthermore, a study conducted in Côte d’Ivoire highlighted the importance of continuing education to ensure a sustainable impact of health interventions (15). These findings suggest that national health policies should institutionalize periodic WASH-focused training and ensure infrastructure improvements, especially in underserved areas, to maximize CHWs’ impact.
Self -reported knowledge by RCs may also introduce social desirability bias. Longitudinal research would be needed to better understand the evolution of knowledge and identify predictors of good understanding of hygiene and sanitation practices (21, 22). Despite a relatively high level of education, a significant proportion of RCs have insufficient knowledge of good water, hygiene and sanitation practices. Training, regular monitoring and adequate incentives could improve this situation, making RCs more effective in their community awareness-raising role. In resource-constrained settings, strengthening CHWs’ WASH competencies is a strategic priority for reducing preventable diseases. Policies should therefore align training, supervision, and incentive structures to ensure sustainability and scalability of interventions.
Conclusion
Community health workers (CHW) play a central role in advancing public health, particularly in water, hygiene, and sanitation (WASH). However, insufficient knowledge among many CHW limits their impact. To address this, ongoing training, regular monitoring, and motivation strategies (e.g., official recognition or incentives) are essential to enhance their effectiveness. These measures would strengthen public health outcomes in communities. Longitudinal studies are further needed to assess CHW’ evolving knowledge and their direct impact on improving community hygiene and sanitation practices.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/supplementary material.
Ethics statement
According to Law No. 2010–40 OF 08 DECEMBER 2010 on the code of ethics and deontology for health research in the Republic of Benin in Title III: CONDITIONS FOR EXECUTION OF HEALTH RESEARCH CHAPTER ONE: RESEARCH EPIDEMIOLOGICAL, ethical approval is not required to conduct an epidemiological study. Our study took place within the framework of epidemiological research the aim of which was to study the level of knowledge of community relays on water quality, hygiene and sanitation. It was carried out in compliance with ethical and professional rules. Articles 20 and 21 of this law specify the following: Article 20: Any epidemiological research applied to a group of individuals or to a community must require the prior agreement of its legal representatives. Authorization to collect data was obtained from the head of the Health and Environment Department of the IRSP on August 28, 2024. Article 21: The informed consent of individuals participating in any epidemiological research is compulsory. In our study, data was collected with the free and informed consent of each respondent. Participation in this study was strictly voluntary. This study was carried out in accordance with articles 20 and 21 of the Law on the code of ethics and deontology for health research in the Republic of Benin and in compliance with the principles of the current version of the Declaration of Helsinki.
Author contributions
PW: Conceptualization, Investigation, Software, Formal analysis, Writing – review & editing, Supervision, Project administration, Writing – original draft, Validation, Methodology. AK: Software, Formal analysis, Validation, Data curation, Methodology, Project administration, Writing – review & editing, Conceptualization, Supervision. CD: Investigation, Supervision, Writing – review & editing, Software, Project administration, Validation, Methodology, Conceptualization, Formal analysis, Data curation.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Summary Progress Update. Water and sanitation for all (2021). Available online at: https://www.unwater.org/publications/summary-progress-update-2021-sdg-6-water-andsanitation-all. [Consultéle 09 aout 2024]
2. Organisation mondiale de la santé. L’eau, l’assainissement et l’hygiène dans les établissements de santé: Mesures pratiques pour instaurer l’accès universel à des soins de santé (2025) Available online at: https://www.who.int/fr/publications/i/item/9789241515511 [Consulté le 10 février 2025]
4. Djagadou, KA, Tchamdja, T, Némi, KD, Balaka, A, and Djibril, MA. Connaissances, attitudes et pratiques des populations de la ville de Lomé en matière de prévention de la bilharziose: cas du canton de Légbassito. Pan Afr Med J. (2029) 34:19. doi: 10.11604/pamj.2019.34.19.18918
5. Ministère de la santé. Politique Nationale de santé communautaire au Bénin. Cotonou: CNLSTP (2020).
6. Ministère de la santé. Directives de mise en œuvre de la Politique Nationale de santé communautaire au Bénin. Cotonou, CNLSTP (2020).
7. Perry, H, Zulliger, R, and Rogers, M. Community health workers in low-, middle-, and high-income countries: an overview of their history, recent evolution, and current effectiveness. Annu Rev Public Health. (2014) 35:399. doi: 10.1146/annurev-publhealth-032013-182354
8. Yamontché, SKH, Johnson, R, Gouissi, FM, Boni, G, Degbey, C, and Houssou, CS. Etat Des Lieux et Facteurs Associés en Matière D’eau, D’hygiène Et D’assainissement Dans la Commune d’Abomey-Calavi Au Bénin. Eur Sci J ESJ. (2020) 16:524–4. doi: 10.19044/esj.2020.v16n6p524
9. Zone sanitaire Comè Bopa Grand popo Houeyogbé. Annuaire des statistiques sanitaires. Comè, BZ (2022).
10. Institut National de la Statistique et de l’Analyse Économique (INSAE) Bénin. Cahier des villages et quartiers de ville Département du MONO. Cotonou: MEPD (2016).
11. Institut National de la Statistique et de l’Analyse Économique (INSAE) Bénin. Enquête Démographique de la Santé du Bénin 2017-2018. Cotonou: MEPD (2018).
12. Kawakatsu, Y, Sugishita, T, Kioko, J, Ishimura, A, and Honda, S. Factors influencing the performance of community health workers in Kisumu west, Kenya. Prim Health Care Res Dev. (2012) 13:294–300. doi: 10.1017/S1463423612000138
13. Gnamien Konan Bah, M. La problématique de l’implication des Agents de Santé Communautaire dans la gestion du VIH/Sida - Analyse anthropologique d’un récit dans l’ouest de la Côte d’Ivoire. Eur Sci J ESJ (2019) 15:33. doi:doi: 10.19044/esj.2019.v15n6p33
14. Closser, S, Napier, H, Maes, K, Abesha, R, Gebremariam, H, Backe, G, et al. Does volunteer community health work empower women? Evidence from Ethiopia’s women’s development Army. Health Policy Plan. (2019) 34:298–306. doi: 10.1093/heapol/czz025
15. Dakouo, WB, and Ouedraogo, N. étude « CAP » finale sur la rive droite (couvrant une partie des communes de Bartiebougou, Foutouri et Gayeri) de la zone de compétence du CLE en queue de la SIRBA. Glob Water Initiat. Komondjari (2012).
16. Agbofa, FJK. Evaluating the impact of (WASH) program on education in the new Juaben north municipal of Ghana: evidence from SDA college demonstration basic schools. RA J Appl Res 1 janv (2022);8:01–06. doi:doi: 10.47191/rajar/v8i1.01
17. Gbaguidi, S, Sekongo, A, and Coulibaly, S. Gestion des connaissances et apprentissage sectoriel en matière d’eau potable, hygiène et assainissement en Côte d’Ivoire. IRC UNICEF Cote D’Ivoire. (2016)
18. Adama, OZ. La santé par et pour la communauté: diagnostic socio-anthropologique du paradigme Agent de Santé Communautaire en Côte d’Ivoire. Rev Afr Sci Soc Sante Publique. (2024) 6:33–51. doi: 10.4314/rasp.v6i3.3
19. Semugabo, C, Wafula, ST, Ndejjo, R, Oporia, F, Osuret, J, Musoke, D, et al. Knowledge and practices of households on safe water chain maintenance in a slum community in Kampala City, Uganda. Environ Health Prev Med. (2019) 24:45. doi: 10.1186/s12199-019-0799-3
20. Sachi, SPA, Yaou, IB, Tchekessi, CCK, Banon, SBJ, Bleoussi, R, Djogbe, AA, et al. Evaluation de la connaissance et de la mise en oeuvre des bonnes pratiques d’hygiène par les populations riveraines du lac Nokoué (Sud-Bénin). Int J Biol Chem Sci. (2016) 10:1823–31. doi: 10.4314/ijbcs.v10i4.30
21. Koslengar, M, and Nansi, J. Gestion des connaissances et l’apprentissage sectoriel en matière d’approvisionnement en eau potable, hygiène et assainissement au Burkina Faso. The Hague, The Netherlands: IRC, UNICEF Burkina Faso (2016).
Keywords: community health workers, WASH, knowledge, supervision, training, Benin
Citation: Wouékpé P, Dégbey C and Kpozéhouen A (2025) Assessing community health workers’ level of knowledge concerning their roles in water, hygiene, and sanitation in Comè-Bopa-Grand Popo-Houéyogbé, Benin (2024). Front. Public Health. 13:1646722. doi: 10.3389/fpubh.2025.1646722
Edited by:
Lori Edwards, University of Maryland, United StatesReviewed by:
Priscila Neves Silva, Oswaldo Cruz Foundation (Fiocruz), BrazilHamed Sidwaya Ouedraogo, University Ouaga I Prof Joseph Ki Zerbo, Burkina Faso
Copyright © 2025 Wouékpé, Dégbey and Kpozéhouen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Parfait Wouékpé, cGVyZmVjdGNvQGhvdG1haWwuZnI=