 Jay E. Maddock1*
Jay E. Maddock1* Emma C. Lewis2
Emma C. Lewis2 Deyaun L. Villarreal2
Deyaun L. Villarreal2 Alexandra L. MacMillan Uribe2
Alexandra L. MacMillan Uribe2 Kathryn M. Janda-Thomte3
Kathryn M. Janda-Thomte3 Gang Han4
Gang Han4 Charles R. Hall5
Charles R. Hall5 Rodney X. Sturdivant6Megan S. Patterson7Meredith L. Graham2
Rodney X. Sturdivant6Megan S. Patterson7Meredith L. Graham2 Rebecca A. Seguin-Fowler8M. Renée Umstattd Meyer3
Rebecca A. Seguin-Fowler8M. Renée Umstattd Meyer3- 1Department of Environmental and Occupational Health, School of Public Health, Texas A&M University System, College Station, TX, United States
- 2Institute for Advancing Health Through Agriculture (IHA), Texas A&M AgriLife, Texas A&M University System, Dallas, TX, United States
- 3Department of Public Health, Robbins College of Health and Human Sciences, Baylor University, Waco, TX, United States
- 4Department of Epidemiology and Biostatistics, School of Public Health, Texas A&M Health Science Center, Texas A&M University System, College Station, TX, United States
- 5Department of Horticultural Sciences, College of Agriculture and Life Sciences, Texas A&M University System, College Station, TX, United States
- 6Department of Statistical Science, College of Arts and Sciences, Baylor University, Waco, TX, United States
- 7Department of Health Behavior, School of Public Health, Texas A&M University System, College Station, TX, United States
- 8Institute for Advancing Health Through Agriculture (IHA), Texas A&M AgriLife, Texas A&M University System, College Station, TX, United States
Background: Poor nutrition and inadequate physical activity are key contributors to rising chronic disease rates across the United States. It is well-documented that neighborhood built environments play an important role in shaping these modifiable health behaviors. Agriculturally-integrated neighborhoods (“agrihoods”) offer a relatively new and promising approach to health-promoting residential design and development. Centered around a working farm, agrihoods are designed to connect residents with fresh foods and outdoor spaces that encourage physical activity. However, no rigorous or longitudinal evaluations of their impact on resident health have been conducted to date. We detail the protocol for a naturalistic study that aims to (1) assess short-term changes in dietary intake, physical activity, cardiometabolic health indicators, and social connectedness among agrihood and matched comparison residents; (2) document time use with and preferences for agrihood design features; and (3) examine agrihood economic benefits.
Methods: This mixed-methods, quasi-experimental study will last approximately 6 months including assessment at three timepoints (baseline, 3 months, 6 months). Agrihood participants will be new adult residents in an agrihood residential development (Richmond, TX), while comparison participants will be adults currently residing in a nearby residential development (Katy, TX). All participants will complete three 30-min online surveys, including items to produce geospatial data; agrihood participants will complete two additional 30-min in-person health assessments and three timepoints of accelerometer wear on 7 consecutive days, with a subsample completing three 30-min online dietary recalls. Data will be collected by trained staff, and Difference-in-Differences (DiD) generalized linear mixed-effects models will examine longitudinal change and its interaction with participant groups. The economic analysis will account for break-even time, farmer compensation, maintenance costs, and public incentive programs.
Discussion: This will be the first study to examine a longitudinal cohort of new agrihood residents compared to a master planned residential development to understand the use and health impacts of agrihood living. Our data-driven design, including biological data collection, device-captured physical activity, and validated self-report measures, can pave the way for future research, policy and philanthropic initiatives to adapt and scale models for developments that promote environmental and economic growth, and improve human health and wellbeing.
Clinical trial registration: https://clinicaltrials.gov/study/NCT06950775, Identifier NCT06950775.
Introduction
Poor nutrition and inadequate physical activity are prevalent in many communities across the United States, contributing to rising rates of chronic diseases such as obesity, diabetes, heart disease, and certain cancers (1–3). Consuming a healthy diet and being physically active are not only important for preventing these health conditions but also for managing and, in some cases, improving them (1). While socioeconomic disparities significantly influence access to healthy food and safe places to be active, a range of societal, environmental, and policy factors shape modifiable health behaviors across all socioeconomic groups (4). In fact, neighborhood built environments have been linked to outdoor activity and diet quality as well as social connection (5–10), sometimes regardless of socioeconomic status (11), pointing to an opportunity to improve health on a broader scale through the intentional design of neighborhoods that foster walkability, healthy food retail and agriculture, and social interaction.
Over the last decade, agriculturally-integrated neighborhoods called “agrihoods” have risen in popularity and present a promising avenue for positioning health at the center of land-use development (11). While there are no established definitions or required components to be considered an agrihood, these neighborhoods typically consist of residences ranging from apartments and condos to attached and single-family homes constructed around a working farm. There is often particular emphasis placed on environmental sustainability (i.e., regenerative farming practices, reduced personal vehicle use and food transportation needs) and community engagement (i.e., community-led gardens and farmers markets, educational and recreational events). Agrihoods can also help support local economies through job creation for farming, food production, and community-based enterprises (12). Property values in agrihoods tend to be higher due to the unique appeal of living close to green spaces and farms, attracting buyers seeking a healthier, eco-friendly lifestyle (13, 14). Additionally, these communities can boost tourism and local commerce by hosting farm-to-table events, farmers’ markets, and educational programs, creating a ripple effect of economic growth and resilience throughout the region (12, 15, 16).
Currently, it is believed that more than 200 agrihoods are planned or developed in the United States, spanning nearly 30 states. Despite this, a recent review by our research team found limited peer-reviewed published literature on agrihoods, and none that rigorously or longitudinally evaluate their impact on health (17). Impact evaluations, especially those using validated measures, are needed to better understand agrihood characteristics, community use of and engagement with resources and agriculture by agrihood residents, changes to agrihood residents’ health behaviors, and community involvement in the design and maintenance of agrihood environmental features and agricultural production (17). Doing so could help inform the design of replicable agrihood models that can be tailored to meet the needs of various populations and settings.
Therefore, we detail the protocol for a naturalistic study, referred to as the Neighborhood & Health Study, which aims to assess the impact of relocating to an agrihood on health and economic outcomes among residents of a newly developed agrihood neighborhood in Fort Bend County, Texas, compared to a geographically and socio-demographically matched non-agriculturally-integrated, master-planned neighborhood, located 23 miles away (by car) in neighboring Harris County, Texas. Given the need for evaluations of agrihood impacts over time and in various settings, we present our scalable methodology for (1) assessing short-term changes in dietary intake, physical activity, cardiometabolic health indicators, and social connectedness among agrihood residents compared to those of a matched master-planned neighborhood that is not agriculturally-integrated; (2) documenting resource utilization and time use with and preferences for built and nature design features of the agrihood; and (3) examining economic benefits of the agrihood from resident and developer perspectives.
Materials and methods
Design and setting
The Neighborhood & Health Study employs a quasi-experimental prospective case–control mixed-methods approach. This entails assessing new residents of the agrihood and a comparison group over a period of 6 months (subject to a + 3-month adjustment based on actual move-in date).
The study is primarily situated at Indigo, a new 235-acre, planned 750-home agrihood located in Richmond, Texas (Fort Bend County), about 28 miles southwest of downtown Houston (18). Its developer, Meristem Communities Development Firm, is a Houston-based real estate development firm committed to creating Places for People™ which they envision as being inclusive public spaces (19). Meristem emphasizes resiliency and human-centric design by mindfully and sustainably creating places that connect land, natural systems, and people. For this reason, among others (e.g., proximity to the research team, a development timeline that aligns with the research project timeline, and Meristem’s willingness to partner), Indigo was selected for this study.
The agrihood comprises 42 acres of farm and pasture, over half of the community dedicated to open space, a 12-acre mixed-use town center with a walkable main street design and mixed retail/businesses, a 25-acre lake, integrated trails, “the Filling Station” (welcome center, café, gathering place, farm stand), vehicle-free community areas focused on nature, and spaces for residents to interact and play between rows of houses where there would traditionally be a street. Agriculture in the agrihood will be managed by Agmenity (20), a leader in the local and national agrihood movement, and will include crop fields, orchards, pasture for livestock, year-round production of seasonal produce, farm stand, farm club, agricultural education opportunities, programming, volunteer opportunities, and pastured poultry and egg production. The agrihood was designed to provide a foundational connection to agriculture and a people-first approach that fosters community connection and overall health, while being committed to environmental stewardship.
Set to be completed in December 2026, the agrihood will include a diverse portfolio of home prices ranging from the upper $200,000’s to over $500,000 (800–3,100 sq. ft.). Median home values were $435,099 for the agrihood’s zip code in April 2025 (21, 22), demonstrating the agrihood’s commitment to providing affordable options to a diverse range of buyers in this area. Sales for homes began in March 2024 and initial move-in dates are scheduled for fall 2025. Richmond is a diverse, growing city with a racial and ethnic composition of 45.9% Non-Hispanic White, 48.5% Hispanic/Latino, 26.6% Black, and 13.8% Asian (23, 24).
The comparison community is located in Katy, Texas (Harris County), about 23-miles from the agrihood and 36-miles northwest of downtown Houston (25). The comparison neighborhood is a master-planned, non-agriculturally focused development with an estimated 2,824 single-family homes built since 2016 with build-out completion plans set for 2029. It was selected by the research team for its comparable home prices (resale values range between $419,000–$700,000 and new homes start in the $300,000’s) (21, 22) and square footage (83% 1,400–3,000 sq. ft., n = 2,011), zoning (26), and mixture of housing styles and proximity to mixed-use retail, as the agrihood. The comparison neighborhood differs from the agrihood in that its mixed-use retail is more car-dependent and not located within the community, and it is not agriculturally-integrated. However, the comparison neighborhood does have a small community garden containing 13 rentable plots, parks, connecting sidewalks, two amenity centers with physical activity options (e.g., pool, fitness center), ponds, and a prairie-land walking path. Demographically, Katy has a racial and ethnic composition of 57.4% Non-Hispanic White, 30.1% Hispanic/Latino, 12.2% Black, and 7.0% Asian (23, 24).
Study aims and approaches
The specific aims for the Neighborhood & Health Study are to: (1) assess short-term changes in dietary intake, physical activity, cardiometabolic health indicators, and social connectedness among Texas residents living in the agrihood compared to non-agriculturally-integrated, master-planned neighborhood; (2) document time use with features of the agrihood and assess preferences for built and nature design features to provide resident-driven data for future developments; and (3) examine the resident- and community-level economic benefits of the agrihood.
The study design and selection of measures are guided by the socioecological model, which recognizes that health behaviors are influenced by interacting individual (e.g., diet, physical activity, stress), interpersonal (e.g., social connection), organizational (e.g., community programs), and environmental (e.g., built and natural design features) factors (27). This framework provides a foundation for examining how agrihood design features may affect resident health and wellbeing.
To conduct Aim 1, we will recruit two longitudinal cohorts, one of new agrihood residents (N = 175), and one of current comparison neighborhood residents (N = 175). Agrihood participants completing the baseline assessment will receive $100, those wearing an accelerometer and completing a mid-point survey will receive $150, and those completing the 6-month follow-up will receive $100. Comparison participants will only complete surveys and will receive $50 for the completion of a survey at each timepoint. Physical assessments will be conducted among agrihood participants by trained clinical staff in Mobile Health Assessment Centers (MHACs), which are mobile clinic spaces specifically designed for biometric data collection. MHAC measures will include blood pressure, resting heart rate, hemoglobin A1c (HbA1c), lipids, dermal carotenoids, weight and height. Seven-day accelerometer data collection will occur at baseline, mid-point, and 6-month follow-up to measure 24-h movement behavior (physical activity, sedentary time, and sleep). Geospatial data regarding access to food and physical activity resources, and resource utilization, will be collected as part of each survey timepoint. Locations of food and physical activity resources located within a 5-mile radius of the agrihood and comparison neighborhoods will be obtained via Google Distances API and mapped using ArcGIS. This will help us understand the food and physical activity resource context that these communities are located in. However, just because a resource is located proximally to a neighborhood, does not mean it is utilized (28). Therefore, we also will be asking questions to participants regarding their food acquisition and physical activity behaviors to understand how participants engage in the food and physical activity built environment. These questions include addresses of resources used, frequency of use, and time spent at resources. Survey measures for both agrihood and comparison participants include the Mediterranean Eating Pattern for Americans Screener (MEPA-16) dietary assessment (29), American Heart Association (AHA) Life’s Essential 8 (30), Perceived Stress Scale (31), and Brief Sense of Community Scale (32). The total time commitment for participants at each time point will last approximately 90 min, not including accelerometer wear time. In addition, a subsample of agrihood residents (n = 20) will be asked to provide an online 24-h dietary recall. See Table 1 for a detailed description of each outcome measure.
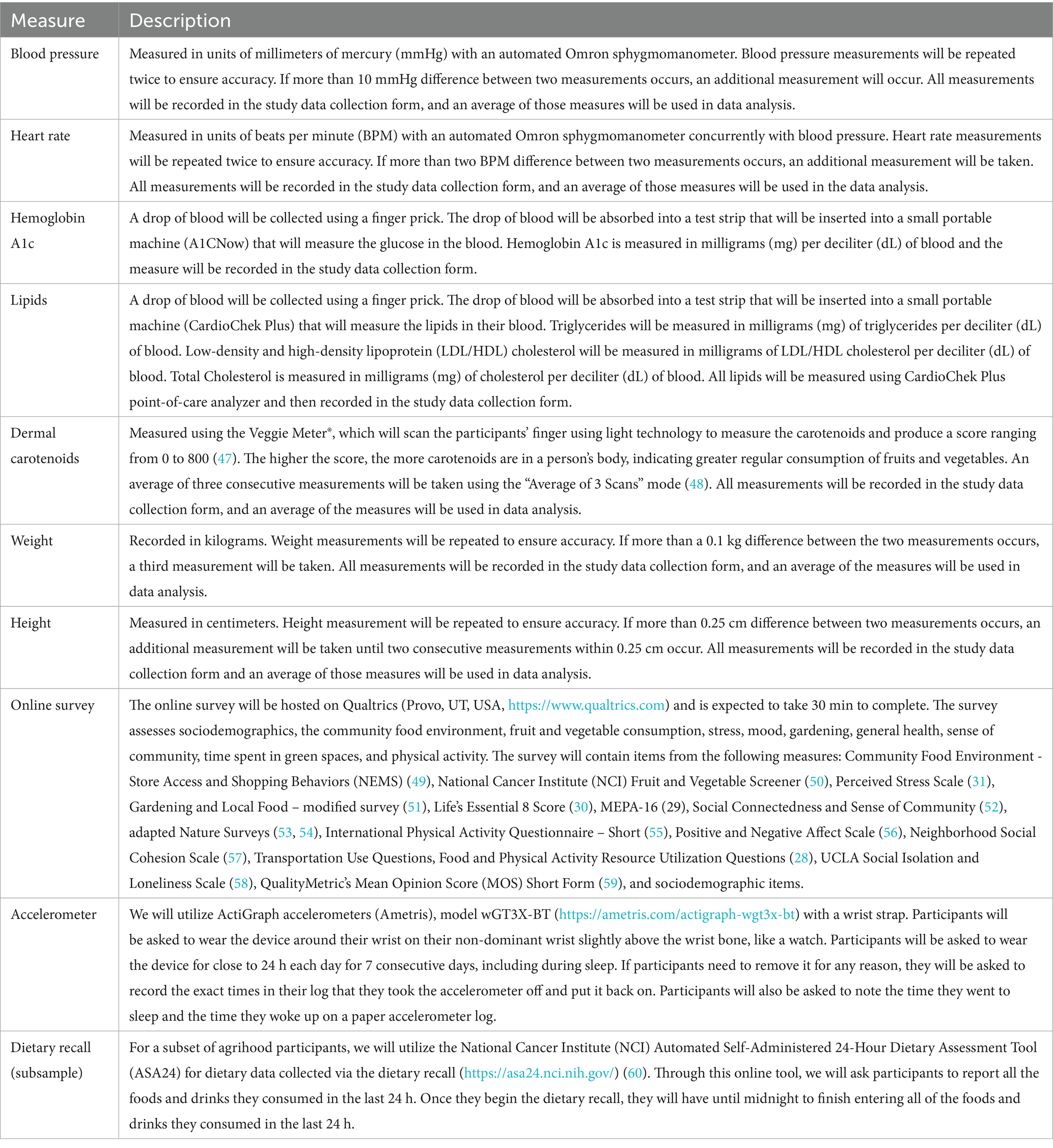
Table 1. Aim 1 outcome measures and their descriptions.
To conduct Aim 2, we will recruit a subsample of adult residents living in the agrihood (n = 48) from the longitudinal cohort to attend a focus group and complete a time-use study. We will conduct a total of four focus groups with 12 people per group, led by trained research staff and lasting approximately 1 hour each. Topics will cover perceived positive and negative changes from living in the agrihood, consumer preferences for agrihood features and programming, including types of produce grown, ability to work on the farm, and aspects of the agrihood’s market (the Filling Station). Focus group participants will then be asked to complete a one-week time-use study. This will include once daily self-reporting via Qualtrics on neighborhood activities such as working on the farm, using the walking trails, attending events hosted at the agrihood, spending time in their home, and participating in external activities like driving, work or school, errands, and leisure activities. Focus groups participants will receive a $100 incentive for their time.
Finally, Aim 3 will be conducted as part of the agrihood resident focus groups, during which participants will be asked their reasons for moving to the agrihood, if they actively participate in the agrihood’s agricultural offerings, sales, and programs, their level of farm volunteering, and neighborhood satisfaction and place attachment. Economic benefits associated with the agrihood benefits explored in Aims 1 and 2 will be monetized. Concurrently, additional data will be acquired from the developer using a survey with items regarding break-even time, farmer compensation, maintenance costs, and public incentive programs such as open space tax credits, easements, and grants. The survey will be developed, conducted, and analyzed by a trained agricultural economist with expertise in financial analysis on the study team. Taken together, these resident- and community-level insights will provide the best current evidence base for how agrihoods create, capture, or redistribute economic value—through property-price premiums, avoided amenity costs, conservation tax policy, and diversified farm revenue.
Participants
Recruitment
All recruitment activities will be overseen by trained research staff. Participants who express interest will complete a Qualtrics online screener to ascertain that they meet the inclusion criteria (described below). Interested individuals will complete the screener either independently or guided by a research staff member via phone or in person at a recruitment event. Once deemed eligible, participants will provide informed consent prior to engaging in study activities.
Agrihood participants
Agrihood participants, including the longitudinal cohort and focus groups, will be recruited using existing Homeowner’s Association marketing efforts, including flyers sent when homes are purchased, community fairs, front door hang tags, as well as word-of-mouth, informational presentations, phone calls, emails, website promotion, and flyers placed in community locations nearby Indigo.
Comparison participants
Comparison participants will be recruited using existing neighborhood marketing efforts, community fairs, front door hang tags, word-of-mouth, phone calls, website promotion, and flyers placed in community locations near the neighborhood.
Inclusion criteria
All participants will be adults, some of whom may be from the same household, and pregnant women may also be included. Specific inclusion criteria are below.
Agrihood participants
Inclusion criteria for agrihood participants are: (1) being 18 years or older; and (2) living in the agrihood as their primary or permanent residence for less than 3 months (cohort) or at least 4 months (focus group) at the time of recruitment.
Comparison participants
Inclusion criteria for comparison participants are: (1) being 18 years or older; and (2) currently living in the comparison neighborhood as their primary or permanent residence at the time of recruitment.
Sample size
A total of 175 agrihood participants and 175 comparison participants will be recruited (N = 350). See Figure 1 for the flow and organization of participants.
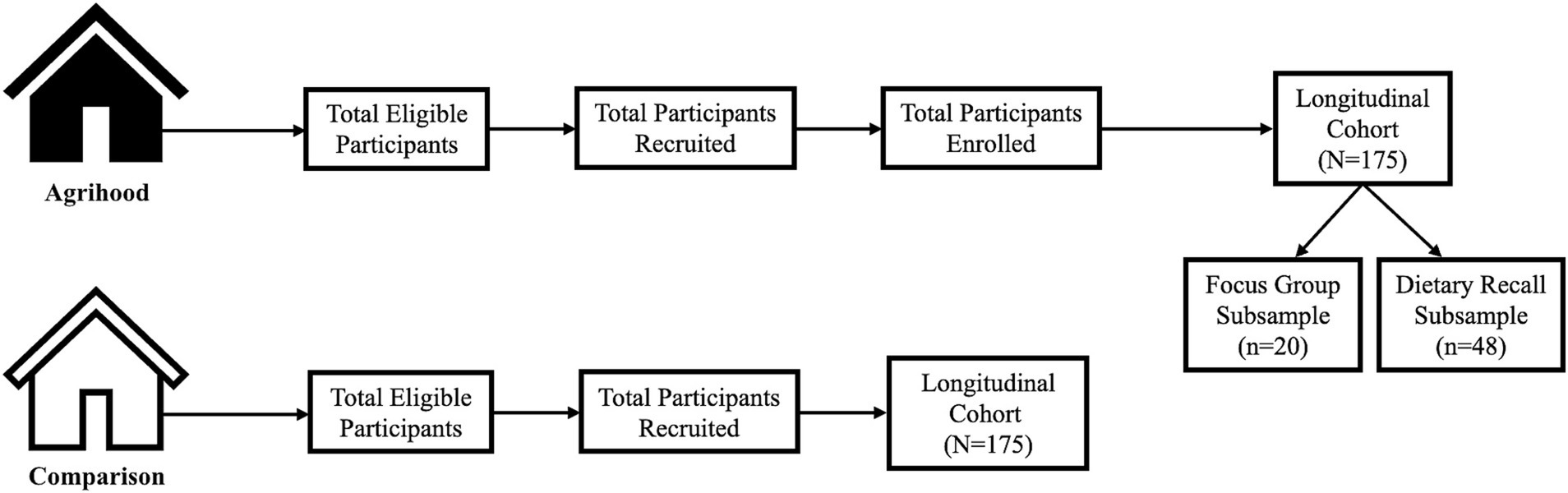
Figure 1. Flow and organization of participants.
Sample size estimation
Power was computed for a natural experiment evaluation (NEE) using Difference-in-Difference (DiD) analysis. For Aim 1, we calculated sample size for a Type I error rate alpha of 0.05, power of 0.8 for comparing the means between two groups considering physical activity outcomes of moderate-to-vigorous physical activity (MVPA); light, moderate, and vigorous physical activity (LMVPA); and time spent in sedentary behavior. Prior research has shown observed effects of moving to an activity-friendly community ranging between 10.4–10.9 min/day of MVPA, indicating small effect sizes of 0.40–0.42 (Cohen’s D) (7). We conservatively powered this study to detect a smaller effect size (Cohen’s D = 0.35). We estimate a sample size of 129 per group will provide adequate power to detect an effect size of Cohen’s D = 0.35 for all physical activity outcomes. The effect size of 0.35 is a conservative estimate based on current literature, equating to minimal detectable differences between 7.9 and 9.6 min/day for MVPA using estimates of standard deviation from previous studies (7, 33–37). This sample size is also adequate for a minimal detectable difference of 13.3 min/day for LMVPA. This sample size is adequate to detect effect sizes that are small to medium for all outcomes based on calculations for other aims. Prior community sampling of an NEE examining accelerometer-measured MVPA found a 20.64% attrition rate from baseline to year 1 and a 6.63% attrition rate from year 1 to year 2 (33). Given recently reported challenges to NEE recruitment, we conservatively overestimate attrition rates, necessitating a sample size of 175 for the agrihood and comparison groups.
Loss to follow-up
A participant will be considered lost to follow-up if they fail to return for any of the scheduled follow-up visits, or do not complete that timepoint’s survey, and cannot be contacted by the research team by the end of the study period. In the case of loss to follow-up or withdrawal, partial data will be used in the data analysis with multiple imputation used to address missing data where appropriate. Intent-to-treat will be used to preserve the group allocation in our analysis (38).
Data collection
The research team conducted an initial survey of demographic and health indicators, neighborhood design preferences, and willingness to pay for specific amenities among 128 prospective buyers of the agrihood between March and July 2024 (Baylor IRB #2158321–1). Findings from the survey provided a formative understanding, which helped to inform the design of the present study and served as a project pilot test for survey recruitment and enrollment procedures (39, 40).
Beginning in Spring 2025, data collection began across three time points (pre-move-in, 3 months after move-in date, and 6 months after move-in date) by trained research and clinical staff (see Table 1). Over the course of 6 months, agrihood participants will be asked to complete (1) three 30-min online surveys; (2) two 30-min in-person health assessments collecting height, weight, blood pressure reading, heart rate, dermal carotenoid scan (Veggie Meter®), HbA1c (finger prick), and lipids (finger prick); (3) three 7-day consecutive accelerometer wears; and (4) three 30-min online dietary recalls (subsample). Comparison participants will be asked to complete three 30-min online surveys at 0 months, 3 months, and 6 months from recruitment.
The focus groups are planned to occur starting in the Fall of 2025. The accompanying one-week time-use study, entailing once-daily self-reports, will begin the following day after each of the four focus group sessions. The gathering of economic data will occur during focus group discussions and concurrently with the agrihood developer as homes continue to be built and residents move into the new units. The developer survey will be designed to capture the full economic arc of an agrihood project—from conception to financial stabilization—by prompting developers to narrate each phase of development (e.g., project origins and strategic intent, land acquisition and zoning, entitlement and permitting processes, capital investment structures, farm-related costs and revenue projections, marketing, sales absorption rates, and plans for long-term stewardship).
Data management
Data including the screening survey, online survey, time-use survey, accelerometer log, and in-person health assessment data collection form will be entered into Qualtrics, a secure data capture system. The data system includes password protection and internal quality checks, such as automatic range checks, to identify data that appears inconsistent, incomplete, or inaccurate. Paper copies of any forms and logs will be stored in a safe cabinet with a lock located at a secure research center. For data captured as part of the online dietary recall, we will utilize the ASA24 system, which comprises a secure database where responses are encrypted during transmission using Secure Socket Layer (SSL) technology.
Data analysis
For Aim 1, we will compare the changes in physical activity outcomes (moderate to vigorous physical activity [MVPA], light, moderate, and vigorous physical activity [LMVPA], walking, sedentary behavior) between the agrihood and comparison participant groups across three time points (Agrihood: pre-move-in, 3 months after move-in date, 6 months after move-in date; Comparison: 0, 3, 6 months) using DiD analysis (linear mixed-effects longitudinal models). Regression models will include the group, time period, and the group by time period interaction terms. Random cluster effects will be included to account for correlations between participants in the same neighborhood and a priori covariates of age, sex, and educational attainment. Random effects for the participants will be included to account for correlation in observations. To address multicollinearity, we will assess variance inflation factors (VIF > 5) and pairwise correlations (|r| > 0.70); collinear variables will be excluded, combined, or tested in sensitivity analyses to avoid attenuation of the group × time effect. Confounders showing baseline imbalance (standardized mean difference > 0.10) will be prioritized for inclusion. Restricted maximum likelihood will be used for complete case analysis to incorporate all available data, and intention-to-treat analysis will include all participants included at baseline. Multiple imputation will be used to estimate missing data points and standard errors. Imputations will follow standardized procedures, including auxiliary variables, and will follow hierarchical approaches. We will examine the potential for missingness of data to not be at random by comparing baseline characteristics of participants who have completed physical activity data with those who do not. If there are differences by age, education, race, or self-reported perceived health, any variables that differ will be used as an auxiliary variable in multiple imputation. Fraction of missing information will be used to measure level of uncertainty about the values imputed for missing values. We will use a number of imputations that satisfy the recommendation to have the number of imputations (at least) equal the highest fraction of missing information (FMI) percentage. Using the geographic information system (GIS) data and resulting maps, for physical activity resources we will: (1) count the number of resources located within the 5-mile network buffer using ArcGIS; (2) measure the distances to the closest resources for different types of resources (e.g., closest park or trail) using ArcGIS and Google Distances API; (3) assess how these counts and distances change over time; and (4) assess changes in time spent in transportation to go to resources. Specifically, we will compare the changes in number of physical activity resources, distance (in miles) to closest objectively measured resources, and distance (in miles) to utilized resources and associated transportation-related time spent between the groups across 3 time points (Agrihood: 0, 3 months after move-in date, 6 months after move-in date; Comparison: 0, 3, 6 months) using DiD analysis, and assess if any of these variables are associated with device-measured physical activity outcomes using linear mixed-effects multilevel models. All statistical analysis will be conducted using SAS and/or R software. We will also generate maps showing changing patterns in physical activity resource utilization in ArcMap. This two-pronged approach of mapping and analyzing objective physical activity environments as well as physical activity resource utilization and time use behaviors are important to better understand how the built environment in these communities are or are not conducive to physical activity, as well as how participants are (or are not) engaging in the resources designed to promote physical activity.
We will use the same strategy above to compare changes in food sourcing and dietary intake between groups across 3 time points (Agrihood: 0, 3 months after move-in date, 6 months after move-in date; Comparison: 0, 3, 6 months) using DiD analysis. MEPA-16 score will serve as the main dietary intake outcome for all participants, while ASA-24 nutrient and food group data will be examined among the Agrihood subsample. We will also compare the changes in number of food resources (by type), distance (in miles) to closest objectively measured food resources, and distance (in miles) to utilized food resources and associated changes in time spent in transportation to food resources between the groups across three time points (Agrihood: 0, 3 months after move-in date, 6 months after move-in date; Comparison: 0, 3, 6 months) using DiD analysis. We will assess if any of these variables are associated with dietary intake using linear mixed-effects multilevel models, with MEPA-16 score as the main outcome of interest. We will generate maps showing changing patterns in food resource utilization in ArcMap. Similar to the physical activity built environment, this approach of mapping and analyzing objective food resource environments, food resource utilization, and time use behaviors can help better understand how the built environment in these communities are or are not conducive to improving food access, connection to agriculture, and healthy eating, as well as how participants are (or are not) engaging in the resources designed to promote connection to agriculture and healthy eating.
In addition, we will explore the impact of social connection and loneliness on physical activity and healthy eating using the same DiD analyses but including social connection and loneliness terms into each of the regression models. We will analyze the survey data for loneliness and social connection over time using random effects models to assess change, and determine factors related to the changes. Additionally, we will explore mediation models using the changes in loneliness/connection scores as mediators for physical activity and dietary intake changes, using methods for analysis of mediation in generalized linear models.
For Aim 2, as described for Aim 1, we will use DiD analysis to explore longitudinal changes for residential time use and engagement outcomes (i.e., assess consumer preferences for built and nature design features). Self-report commuting time and time spent outside of the agrihood will also be measured to create dose measures for overall time spent in the neighborhood. Comparison participants will be asked about the time they spend engaging in features of their neighborhoods to allow for comparisons.
For Aim 3, an exploratory economic benefits analysis will be conducted using monetized data collected from participants (as part of Aims 1 and 2) accompanied by financial data and survey measures gathered from the developer. In regard to analysis of the resident data, descriptive analysis of demographics will be coupled with a thematic analysis of responses to open-ended questions asking residents to rate their perceived importance of the working farm, open-space views, trail networks, school quality, and other standard amenities, and price premiums they believe they will pay for these. This analysis will also examine estimated monthly expenditures on farm products compared to spending at conventional grocery stores or farmers’ markets; hypothetical willingness-to-pay to retain farm amenities; anticipated influence of the farm on diet, outdoor activity, sense of community, and children’s environmental awareness; understanding of any farm-related HOA fees and decision-making processes; and perceived risks and desires. Findings will yield comparable metrics for future cross-case analyses across agrihoods, linking residents’ expectations and preferences based on their open-ended responses, to community-level economic outcomes gathered from the developer survey.
Discussion
Consuming a healthy diet and being physically active are crucial for preventing, managing, and improving chronic diseases, yet many communities lack access to fresh foods or safe spaces for physical activity. Neighborhood built environments, particularly those that integrate agricultural production, can be intentionally designed to facilitate walkability, healthy food purchasing, and social interaction. With more than 200 planned or developed agrihoods across the country, a need has been identified for rigorous, longitudinal evaluations to better understand the impact these neighborhoods have on residents’ health and surrounding economies. The present paper details our scalable protocol for a naturalistic study in Fort Bend County, Texas.
By combining two longitudinal cohorts of matched residents, we will address three specific aims with the following expected outcomes based on our team’s experience and formative research. First, from Aim 1 (assessing short-term changes in dietary intake, physical activity, cardiometabolic health indicators, and social connectedness), we expect to demonstrate how physical activity and sedentary behaviors and locations change for adults who relocate to the agrihood compared to adults who do not. We will examine the impact of relocating to the agrihood on MVPA, LMVPA, walking, and sedentary behavior, and expect to find changes in physical activity resource utilization. We expect to explain how living in the agrihood impacts social connection and determine how connection relates to physical activity and healthy eating among participants across time. With this newly generated knowledge, we will be able to more fully explain the dynamic relationship between social connection, built environment, and chronic disease prevention. From exploratory Aim 2 (documenting time use with features of the agrihood and assessing consumer preferences for built and nature design features to provide resident-driven data for future developments), we expect to describe how residents utilize the various features of the agrihood and how much time they spend engaging in these features of their neighborhood. Finally, from exploratory Aim 3 (assessing the economic benefits of the agrihood), we expect to describe resident and developer perspectives of the cost-efficiency of living in and running an agrihood and agrihood farm model.
Our study design has several strengths, including multiple matched cohorts of residents. In addition, we propose a strong data-driven approach involving biological data collection from the mobile health assessment clinics and device-captured physical activity, along with highly valid and reliable self-report measures that capture individual and community-level preferences and perspectives. Given our multi-disciplinary team and established partnerships with the developers, we anticipate the aims will be achievable, and the results generated from this work will translate into meaningful considerations for residents of these neighborhoods. Moreover, we believe the results will allow us to understand not only how agrihoods affect health and wellbeing, but also how residents engage with them, thereby informing future models for development that are effective for improving health and are economically sustainable.
Given funding and scope of work parameters, this study also has several limitations worth noting. First, the comparison community consists of existing residents, meaning we are unable to capture their baseline prior to moving in, unlike with the agrihood participant sample. Capturing residents as they move into a new development is extremely challenging, and it was not feasible to find a comparison community that was being occupied at the same time as the agrihood. Second, due to budgetary constraints, accelerometer-based physical activity measurement and biological data collection are only feasible among participants in the agrihood community, which may reduce cross-group comparability. Third, the funding support received for this work only covers 13 months, thereby allowing for 6 months of follow-up which may be too short to observe meaningful or sustained behavioral and health changes.
Additional challenges may arise with retention from recruitment events to follow-up in-person physical assessments. The MHACs are based in Dallas, Texas, and our team has limited days for on-site biological data collection, which may create scheduling barriers. To mitigate this, participants will be offered flexible options such as completing online surveys remotely and receiving accelerometers by mail or at a designated community pick-up location (the Filling Station). Higher-than-usual attrition was anticipated and accounted for in our study design. The protocol also allows for multiple adults (e.g., married couples) within the same household to participate. This decision was made to help achieve recruitment and enrollment goals given the number of households under contract. Interclass correlations within households will be accounted for statistically in the analysis.
For cholesterol and HbA1c data, we are using finger prick sampling rather than venipuncture. Although venipuncture is often considered more precise, capillary testing has been shown to produce comparable results when performed properly and is substantially less invasive and more acceptable in community-based research settings (41–45). Self-reported survey data also introduce potential recall and social desirability bias. The economic analysis component is exploratory, drawing on developer-provided data and resident perceptions. While this approach supports early feasibility insights, it limits the ability to conduct standardized cost–benefit or return-on-investment modeling. Future work will incorporate objective financial metrics (e.g., property values, healthcare cost offsets) to strengthen policy and planning relevance.
Finally, this study is limited to one agrihood in a single region (Fort Bend County, Texas), which may restrict generalizability to other cultural, climatic, or socio-economic contexts. Despite these limitations, this pilot study represents a critical first step in establishing the feasibility, logistics, and interdisciplinary partnerships needed for more rigorous future work. The present phase provides foundational data to inform a larger, multi-site randomized controlled trial with extended follow-up, expanded objective data collection, and greater diversity among participants.
In conclusion, agrihoods present an innovative and relatively novel idea for building healthier communities. As people have reduced outdoor time and moved away from farms over the last few decades, many are now disconnected from nature and the process of growing food (46). If this study is successful, it may provide evidence of the health benefits of this type of urban design and help to shape future neighborhoods. Like all natural experiments, this research design does have some limitations. These are counterbalanced by a high level of external validity. The data collection methodologies are solid and provide short-term indications of changes in biological indicators and health behaviors. We will actively seek funding to include 12- and 24-month follow-ups, as well as to support future scale-up to larger evaluations and the development of interventions and initiatives informed by the findings from the present study.
Ethics statement
The studies involving humans were approved by Texas A&M University Institutional Review Board. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
JM: Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing. EL: Conceptualization, Supervision, Writing – original draft, Writing – review & editing. DV: Conceptualization, Investigation, Project administration, Supervision, Writing – original draft, Writing – review & editing. AM: Conceptualization, Investigation, Project administration, Supervision, Writing – review & editing. KJ-T: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Writing – review & editing. GH: Conceptualization, Data curation, Formal analysis, Methodology, Writing – review & editing. CH: Conceptualization, Data curation, Formal analysis, Methodology, Writing – review & editing. RS: Conceptualization, Data curation, Formal analysis, Methodology, Writing – review & editing. MP: Conceptualization, Investigation, Project administration, Supervision, Writing – review & editing. MG: Conceptualization, Data curation, Methodology, Writing – review & editing. RS-F: Conceptualization, Funding acquisition, Project administration, Supervision, Writing – review & editing. MU: Conceptualization, Data curation, Funding acquisition, Investigation, Project administration, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This material is based upon work supported by the Texas A&M AgriLife Institute for Advancing Health Through Agriculture (IHA) and the U.S. Department of Agriculture, Agricultural Research Service, under Agreement No. 58–3091–1-018.
Acknowledgments
The authors would like to thank the students and staff who have aided in the planning and design of the study, as well as the agrihood and comparison neighborhood developers, staff, and community residents for their time and effort in helping us to facilitate study activities. We also thank the Texas A&M AgriLife Institute for Advancing Health Through Agriculture (IHA) for providing funding to support this foundational work.
Conflict of interest
RS-F is the co-founder and owner of www.strongpeopleprogram.org.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Author disclaimer
Any opinions, findings, conclusion, or recommendations expressed in this publication are those of the author(s) and do not necessarily reflect the view of the U.S. Department of Agriculture or the authors’ employing organizations.
Abbreviations
AHA, American Heart Association; ASA24, Automated Self-Administered 24-Hour Dietary Assessment Tool; BMI, Body mass index; BPM, Beats per minute; CSA, Community supported agriculture; DiD, Difference-in-Difference; FMI, Fraction of missing information; GIS, Geographic information system; HbA1c, Hemoglobin A1C; HOA, Homeowners association; LMVPA, Light, moderate, and vigorous physical activity; MEPA-16, Mediterranean Eating Pattern for Americans-16 Screener; MHAC, Mobile health assessment center; MOS, Mean opinion score; MVPA, Moderate to vigorous physical activity; NCI, National Cancer Institute; NEMS, Nutritional Environment Measures Survey; SSL, Secure Socket Layer.
References
1. Centers for Disease Control and Prevention. About the division of nutrition, physical activity, and obesity (DNPAO). Atlanta, GA: CDC (2025).
2. Ward, ZJ, Bleich, SN, Long, MW, and Gortmaker, SL. Association of body mass index with health care expenditures in the United States by age and sex. PLoS One. (2021) 16:e0247307. doi: 10.1371/journal.pone.0247307
3. Centers for Disease Control and Prevention. CDC releases updated maps of America’s high levels of inactivity. Atlanta, GA: CDC (2025).
4. Oude Groeniger, J, Kamphuis, CBM, Mackenbach, JP, Beenackers, MA, and van Lenthe, FJ. Are socio-economic inequalities in diet and physical activity a matter of social distinction? A cross-sectional study. Int J Public Health. (2019) 64:1037–47. doi: 10.1007/s00038-019-01268-3
5. Prochnow, T, Curran, LS, Amo, C, and Patterson, MS. Bridging the built and social environments: a systematic review of studies investigating influences on physical activity. J Phys Act Health. (2023) 20:438–59. doi: 10.1123/jpah.2022-0403
6. Sallis, JF, Bowles, HR, Bauman, A, Ainsworth, BE, Bull, FC, Craig, CL, et al. Neighborhood environments and physical activity among adults in 11 countries. Am J Prev Med. (2009) 36:484–90. doi: 10.1016/j.amepre.2009.01.031
7. Lee, C, Xu, M, Zhu, X, Towne, SD, Sang, H, Lee, H, et al. Moving to an activity-friendly community can increase physical activity. J Phys Act Health. (2023) 20:1058–66. doi: 10.1123/jpah.2023-0045
8. Leonard, T, McKillop, C, Carson, JA, and Shuval, K. Neighborhood effects on food consumption. J Behav Exp Econ. (2014) 51:99–113. doi: 10.1016/j.socec.2014.04.002
9. Janda, KM, Ranjit, N, Salvo, D, Nielsen, A, Kaliszewski, C, Hoelscher, DM, et al. Association between fresh fruit and vegetable consumption and purchasing behaviors, food insecurity status and geographic food access among a lower-income, racially/ethnically diverse cohort in Central Texas. Nutrients. (2022) 14:5149. doi: 10.3390/nu14235149
10. Sharkey, JR, Johnson, CM, and Dean, WR. Food access and perceptions of the community and household food environment as correlates of fruit and vegetable intake among rural seniors. BMC Geriatr. (2010) 10:32. doi: 10.1186/1471-2318-10-32
11. Sallis, JF, Conway, TL, Cain, KL, Carlson, JA, Frank, LD, Kerr, J, et al. Neighborhood built environment and socioeconomic status in relation to physical activity, sedentary behavior, and weight status of adolescents. Prev Med. (2018) 110:47–54. doi: 10.1016/j.ypmed.2018.02.009
12. Breger, B. Understanding Agrihoods: an exploration into the growing trend of farm-to-table communities across the United States. Massachusetts: University of Massachusetts Amherst (2020).
13. Norris, M. Agrihoods: cultivating best practices. Washington, D.C.: Urban Land Institute (2020).
15. Donnally, T. Growing sociability: integrating communal spaces with development. Washington, DC: Urban Land Magazine (2015).
17. Lewis, E C, Umstattd Meyer, M R, Janda-Thomte, K M, Maddock, J E, Palma, M A, McNeely, A C, et al. (2025) Cultivating connection between community, agriculture, food, and green space: a narrative review of agrihoods and their impact on health and wellbeing. Public Health in Practice.
19. Meristem Communities. Meristem communities: places for people. Houston: Meristem Communities (2025).
20. Agmenity (2025) Agmenity: agricultural amenities made easy. Available online at: https://agmenity.com/. [Accessed May 1 2025]
21. Zillow Inc. (2024) Zillow home value index (ZHVI). Available online at: www.zillow.com/home-values [Accessed February 4, 2024]
22. Zillow Inc. (2023). Zillow's home value index: built on the database of all homes with the real time adaptive power of neural net technology. Available online at: https://www.zillow.com/research/methodology-neural-zhvi-32128/. [Accessed February 4, 2024]
23. United States Census Bureau (2024). Quick facts. Available online at: https://www.census.gov/quickfacts/fact/table/US/PST045224. [Accessed February 4, 2024]
24. Hidalgo, C.Deloitte, Datawheel. (2024). Datausa: Explore, map, compare, and download U.S. data. Available online at: https://datausa.io/. [Accessed February 4, 2024]
25. Elyson (2024). Elyson by Newland. Available online at: https://www.elyson.com/ [Accessed May 1. 2025]
26. GreatSchools (2024). GreatSchools rating. Available online at: https://www.greatschools.org/ [Accessed February 4, 2024]
27. Bronfenbrenner, U. Toward an experimental ecology of human development. Am J Psychol. (1977) 32:513–31. doi: 10.1037/0003-066X.32.7.513
28. Janda, KM, Salvo, D, Ranjit, N, Hoelscher, DM, Nielsen, A, Lemoine, P, et al. Who shops at their nearest grocery store? A cross-sectional exploration of disparities in geographic food access among a low-income, racially/ethnically diverse cohort in Central Texas. J Hunger Environ Nutr. (2024) 19:355–75. doi: 10.1080/19320248.2022.2128962
29. Cerwinske, LA, Rasmussen, HE, Lipson, S, Volgman, AS, and Tangney, CC. Evaluation of a dietary screener: the Mediterranean eating pattern for Americans tool. J Hum Nutr Diet. (2017) 30:596–603. doi: 10.1111/jhn.12451
30. Lloyd-Jones, DM, Allen, NB, Anderson, CAM, Black, T, Brewer, LC, Foraker, RE, et al. Life’s essential 8: updating and enhancing the American Heart Association’s construct of cardiovascular health. Circulation. (2022) 146:e18–43. doi: 10.1161/CIR.0000000000001078
31. Cohen, S, Kamarck, T, and Mermelstein, R. A global measure of perceived stress. J Health Soc Behav. (1983) 24:385–96. doi: 10.2307/2136404
32. Peterson, NA, Speer, PW, and McMillan, DW. Validation of a brief sense of community scale: confirmation of the principal theory of sense of community. J Community Psychol. (2008) 36:61–73. doi: 10.1002/jcop.20217
33. Saelens, BE, Hurvitz, PM, Zhou, C, Colburn, T, Marchese, A, and Moudon, AV. Impact of a light rail transit line on physical activity: findings from the longitudinal travel assessment and community (TRAC) study. J Transp Health. (2022) 27:101527. doi: 10.1016/j.jth.2022.101527
34. Stamatakis, E, Koemel, NA, Biswas, RK, Allman-Farinelli, Margaret, Trost, Stewart G., and Eroglu, Elif I., (2023). Minimum changes in sleep, physical activity, and nutrition associated with clinically important reductions in all-cause mortality risk: a prospective cohort study. Available online at: https://www.medrxiv.org/content/10.1101/2023.11.19.23298747v1. [Accessed November 20, 2023].
35. Byker Shanks, C, Vanderwood, K, Grocke, M, Johnson, N, Larison, LA, Wytcherley, B, et al. The UnProcessed pantry project (UP3): a community-based intervention aimed to reduce ultra-processed food intake among food pantry clients. Fam Community Health. (2022) 45:23–33. doi: 10.1097/FCH.0000000000000310
36. Dubowitz, T, Ghosh-Dastidar, B, Beckman, R, Richardson, AS, Hunter, GP, Burns, RM, et al. Community investments and diet-related outcomes: a longitudinal study of residents of two urban neighborhoods. Am J Prev Med. 66:681–9. doi: 10.1016/j.amepre.2023.11.005
37. Full, KM, Berger, AT, Erickson, D, Berry, KM, Laska, MN, Lenk, KM, et al. Assessing changes in adolescents’ sleep characteristics and dietary quality in the START study, a natural experiment on delayed school START time policies. J Nutr. (2021) 151:2808–15. doi: 10.1093/jn/nxab169
39. Maddock, JE, Janda-Thomte, KM, Seguin-Fowler, R, Patterson, MS, Beattie, C, Vigil, J, et al. (2025). Community design preferences in a sample of interested buyers of an agrihood community. Poster presentation at the American Academy of Health Behavior Annual Scientific Meeting, AAN: San Diego, CA.
40. Umstattd Meyer, MR, Janda-Thomte, KM, Seguin-Fowler, R, Patterson, MS, Carter, JR, Vigil, J, et al. (2025). Demographics and health behaviors among interested buyers of an agrihood community. Poster presentation at the American Academy of health behavior annual scientific meeting, AAN: San Diego, CA.
41. Kuniyoshi, Y, Kimoto, T, Tokutake, H, Takahashi, N, Kamura, A, and Tashiro, M. Comparison between point-of-care testing from capillary samples and conventional laboratory testing from venous samples for white blood cells and C-reactive protein in a pediatric outpatient setting. J Gen Fam Med. (2024) 26:79–84. doi: 10.1002/jgf2.741
42. Barrett, SC, Huffman, FG, and Johnson, P. Validation of finger-prick testing of fasting blood glucose, total cholesterol, and HbA1c in adolescents. POC. (2011) 10:51–8. doi: 10.1097/POC.0b013e31821bd65e
43. Fliervoet, LAL, Tiel Groenestege, WM, and Huisman, A. Comparison of capillary and venous blood sampling for routine coagulation assays. Clin Biochem. (2022) 104:30–5. doi: 10.1016/j.clinbiochem.2022.01.010
44. Bhavadharini, B, Mahalakshmi, MM, Maheswari, K, Kalaiyarasi, G, Anjana, RM, Deepa, M, et al. Use of capillary blood glucose for screening for gestational diabetes mellitus in resource-constrained settings. Acta Diabetol. (2016) 53:91–7. doi: 10.1007/s00592-015-0761-9
45. Parikh, M, Wimmer, C, DiPasquale, C, Barr, RL, and Jacobson, JW. Evaluation of a novel capillary blood collection system for blood sampling in nontraditional settings as compared with currently marketed capillary and venous blood collection systems for selected general chemistry analytes. J Appl Lab Med. (2025) 10:639–52. doi: 10.1093/jalm/jfaf005
46. Satterthwaite, D, McGranahan, G, and Tacoli, C. Urbanization and its implications for food and farming. Philos Trans R Soc Lond Ser B Biol Sci. (2010) 365:2809–20. doi: 10.1098/rstb.2010.0136
47. Ermakov, IV, Whigham, L, Redelfs, A, Jahns, L, Stookey, J, Bernstein, PS, et al. Skin carotenoids as biomarker for vegetable and fruit intake: validation of the reflection-spectroscopy based “veggie meter”. Federation of American Societies for Experimental Biology Conference; (2016); San Diego, CA: FASEB
48. Radtke, MD, Poe, M, Stookey, J, Jilcott Pitts, S, Moran, NE, Landry, MJ, et al. Recommendations for the use of the veggie meter® for spectroscopy-based skin carotenoid measurements in the research setting. Curr Dev Nutr. (2021) 5:104. doi: 10.1093/cdn/nzab104
49. Glanz, K, Sallis, JF, Saelens, BE, and Frank, LD. Nutrition environment measures survey in stores (NEMS-S): development and evaluation. Am J Prev Med. (2007) 32:282–9. doi: 10.1016/j.amepre.2006.12.019
50. Thompson, F, Subar, A, Smith, A, Midthune, D, Radimer, K, Kahle, L, et al. Fruit and vegetable assessment: performance of 2 new short instruments and a food frequency questionnaire. J Am Diet Assoc. (2002) 102:1764–72. doi: 10.1016/j.jada.2002.09.004
51. Seguin, R, Morgan, E, Hanson, K, Seguin, RA, Morgan, EH, Hanson, KL, et al. Farm fresh foods for healthy kids (F3HK): an innovative community supported agriculture intervention to prevent childhood obesity in low-income families and strengthen local agricultural economies. BMC Public Health. (2017) 17:306. doi: 10.1186/s12889-017-4202-2
52. Lee, RM, and Robbins, SB. Measuring belongingness: the social connectedness and the social assurance scales. J Couns Psychol. (1995) 42:232–41. doi: 10.1037/0022-0167.42.2.232
53. Natural England. People and nature survey for England, 2020–2024. United Kingdom: Data Service (2025).
54. Kellert, SR, Case, DJ, Escher, D, Witter, D. J., Mikels-Carrasco, J., and Seng, P. T., (2017). The nature of Americans national report: disconnection and recommendations for reconnection. Available online at: https://lccnetwork.org/sites/default/files/Resources/Nature-of-Americans_National_Report_1.2_4-26-17.pdf. [Accessed August 17, 2022].
55. Craig, CL, Marshall, AL, Sjöström, M, Bauman, AE, Booth, ML, Ainsworth, BE, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. (2003) 35:1381–95. doi: 10.1249/01.MSS.0000078924.61453.FB
56. Watson, D, Clark, LA, and Tellegen, A. Development and validation of brief measures of positive and negative affect: the PANAS scales. J Pers Soc Psychol. (1988) 54:1063–70. doi: 10.1037/0022-3514.54.6.1063
57. Dupuis, M, Baggio, S, and Gmel, G. Validation of a brief form of the perceived Neighborhood social cohesion questionnaire. J Health Psychol. (2017) 22:218–27. doi: 10.1177/1359105315600234
58. Russell, DW. UCLA loneliness scale (version 3): reliability, validity, and factor structure. J Pers Assess. (1996) 66:20–40. doi: 10.1207/s15327752jpa6601_2
59. Ware, JE, Kosinski, M, and Dewey, JE. How to score version two of the SF-36 health survey. Lincoln, RI: QualityMetric Incorporated (2000).
60. Subar, AF, Kirkpatrick, SI, Mittl, B, Zimmerman, TP, Thompson, FE, Bingley, C, et al. The automated self-administered 24-hour dietary recall (ASA24): a resource for researchers, clinicians, and educators from the National Cancer Institute. J Acad Nutr Diet. (2012) 112:1134–7. doi: 10.1016/j.jand.2012.04.016
Keywords: agrihood, built environment, community health, nutrition, diet, physical activity, mixed methods, protocol
Citation: Maddock JE, Lewis EC, Villarreal DL, MacMillan Uribe AL, Janda-Thomte KM, Han G, Hall CR, Sturdivant RX, Patterson MS, Graham ML, Seguin-Fowler RA and Umstattd Meyer MR (2025) Protocol for a naturalistic study of residents living in an agriculturally-integrated (“agrihood”) neighborhood. Front. Public Health. 13:1679602. doi: 10.3389/fpubh.2025.1679602
Edited by:
Sebastian Elgueta, San Sebastián University, ChileReviewed by:
P. E. Rajasekharan, Indian Institute of Horticultural Research (ICAR), IndiaHao Du, Yale University, United States
Gabriel Nastase, Transilvania University of Brașov, Romania
Copyright © 2025 Maddock, Lewis, Villarreal, MacMillan Uribe, Janda-Thomte, Han, Hall, Sturdivant, Patterson, Graham, Seguin-Fowler and Umstattd Meyer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jay E. Maddock, bWFkZG9ja0B0YW11LmVkdQ==