 Jun Liu
Jun Liu Sheng Yang
Sheng Yang Ming-jiang Luo
Ming-jiang Luo Ting Chen
Ting Chen Xiao-juan Ma1
Xiao-juan Ma1 Na Tao
Na Tao Dong-hong Wang
Dong-hong Wang- 1Experimental Teaching Demonstration Center for Preventive Medicine of Guizhou Province, Zunyi Medical University, Zunyi, China
- 2Department of Pharmacy, Affiliated Hospital of Zunyi Medical University, Zunyi, China
- 3Department of Chronic Disease, Center of Disease Control and Prevention of Zhijin County, Zhijin, China
- 4Department of Gynaecology and Obstetrics, Affiliated Hospital of Zunyi Medical University, Zunyi, China
Objective: Many studies have explored the effects of individual foods or nutrients on fluorosis, but no studies have focused on dietary patterns. This study examined the relationship between dietary patterns and coal-burning fluorosis in Guizhou, China.
Methods: This 1:1 matched case-control study was conducted in Zhijin County of Guizhou province with a sample size of 200 cases of fluorosis and 200 age and gender matched controls. Habitual dietary intake was assessed by face-to-face interviews, using a validated 75-item food frequency questionnaire (FFQ) and various covariates using structured questionnaires. The dietary patterns were identified by factor analysis.
Results: The factor analysis identified three major dietary patterns which were labeled healthy, easy-to-roast and high protein. After adjusting for various confounding factors, a decreased risk for fluorosis was observed in the highest tertile of the healthy dietary pattern relative to the lowest tertile (OR = 0.47, 95% CI = 0.27–0.84, P-trend = 0.003) and a positive association was observed between the easy-to-roast dietary pattern and fluorosis risk (OR = 2.05, 95% CI = 1.15–3.66), with a significant linear trend (P = 0.017). We did not find an association between fluorosis risk and the high protein dietary pattern. The relationships remained significant when the analyses were stratified by gender and fluorosis subtypes.
Conclusion: The healthy dietary pattern may lower coal-burning fluorosis risk; in contrast, the easy-to-roast dietary pattern significantly increases the risk of coal-burning fluorosis.
Introduction
Endemic fluorosis is a disease affecting mainly the bones and teeth, caused by exposure to high levels of fluorine in the environment. Over 70 million people may be affected globally, including China, India, Africa and South America. Reports predicted that over 26 million people in China suffer from fluorosis due to fluoride contamination in their drinking-water. A further 16.5 million people burn fluoride-rich coal indoors for heating and cooking, a process which is termed coal-burning fluorosis (CBF) (1). The most severe CBF case was located in Guizhou, China; 43% of its districts and counties had fluorosis incidents (2). Although CBF cases have been recently reduced through the use of improved stoves and awareness education, the incidence rate of fluorosis remains high (3, 4). This disease seriously restricts economic development and reduces quality of life. Therefore, further strategies are needed to prevent and control fluorosis.
Nutrition may play an important role in the development of fluorosis. Studies have not been successful at establishing a consistent association between CBF risk and specific foods and nutrients [e.g., corn (5, 6) chili (6), sour soup (7), vitamins (8–11), and calcium (12, 13)]. The inconsistent results linking foods and fluorosis may, in part, reflect the difficulty of disentangling the high degree of correlation among dietary constituents. To address this problem, Schwerin et al. proposed using dietary patterns to examine diet-disease relationships (14). Dietary patterns incorporate food interactions in the diet and consider the overall diet, reflecting more closely real-world food intakes, and are therefore more useful to predict disease risk than individual foods or nutrients (15). Factor analysis is a variable consolidation technique that can be applied to dietary data to identify underlying dietary patterns based on the inter-correlations of food groups. To our knowledge, there have been no studies on the association between dietary patterns and fluorosis. Therefore, we conducted this 1:1 matched case–control study to identify major dietary patterns among Chinese residents of Guizhou province and to examine the associations of these dietary patterns with the risk of fluorosis.
Subjects and Methods
Study Subjects
This 1:1 matched case-control study was conducted between July and August 2015 in Zhijin County, Guizhou Province, China, where coal-burning fluorosis is endemic. All of the CBF cases were diagnosed by the Zhijin County Disease Control and Prevention Center according to the Chinese Diagnostic Criteria of Dental Fluorosis (WS/T208-2011, China) and the Chinese Diagnostic Criteria of Endemic Skeletal Fluorosis (WS/T 192-2008, China). Cases were identified by one professional doctor in Zhijin Center for Disease Control and Prevention, and eligible cases, aged 18–75 years old, were recruited through village doctors. Subjects in the following situations were excluded: (1) pathological fractures or fractures from car accidents, falls and other fractures caused by violence; (2) patients with tetracycline stained teeth and dental cavities; (3) patients previously diagnosed with cancer, coronary heart disease, stroke, gout, or kidney disease; (4) patients who self-reported substantial changes in dietary habit within the previous 5 years. For each CBF case, a control participant was selected from residents living in the same county and within the same sex and age group (±3 years). Control participants were required to be at least 18 years old, to have lived in Zhijin County for at least the previous 10 years and were selected according to the same exclusion criteria as CBF patients. The study sample consisted of 200 CBF patients and 200 controls. All of the study participants signed informed consent forms prior to the interview and the Medical Ethics Committee of Zunyi Medical University approved the project (No. 2014-1-003).
Data Collection
The following information was collected by trained interviewers through face-to-face interviews using a structured questionnaire. The questionnaire included (1) socio-demographic characteristics (age, gender, education level); (2) lifestyle habits (alcohol drinking, tea drinking, smoking status, domestic fuel type, use of improved stoves, consumption of roasted food); (3) dietary habits in the year before the interview; and (4) relevant diseases (hypertension, diabetes, gout, kidney disease, cancer, heart-related diseases, and stroke). Tea drinkers were defined as individuals who drank tea at least twice weekly; Likely, smokers are the participants who smoked at least five packs of cigarettes a year and those who drank alcohol at least once a week continuously for at least 6 months were considered alcohol drinkers. CBF patients and controls were required to respond to the same questionnaire.
Dietary Assessment
The participants were instructed to recall their usual dietary consumption using a validated 75-items food frequency questionnaire (FFQ) (16). Foods consumption was estimated in terms of the frequency of use per day, per week, per month, or per year. To help the participants quantify the amounts, they were provided with color pictures of foods with approximate proportion sizes. The selected value for each food was then converted to reflect the daily intake. Energy and nutrient intakes were computed based on the China Food Composition database (17).
Food Grouping and Identification of Dietary Patterns
To reduce the complexity of the data, 75 food items from the FFQ were categorized into 25 predefined food groups according to similarities in their nutrient profiles or processing methods. Dietary factor patterns were then identified by principal component analysis. A varimax (orthogonal) rotation was performed to improve interpretability and minimize the correlation. Factors were retained based on eigenvalues (>1.3 cut-off), scree plots and factor interpretability (18). Factor loadings for each food group were calculated and factor scores per pattern were calculated for each subject by summing the total intake of each food group, weighted by their factor loadings. High scores represented a high intake of food items resulting in a positive loading on the corresponding dietary pattern, whereas low scores represented a low intake of those items. Food groups with absolute values >0.25 are presented in Table 1. Based on the analysis, three categories were selected.
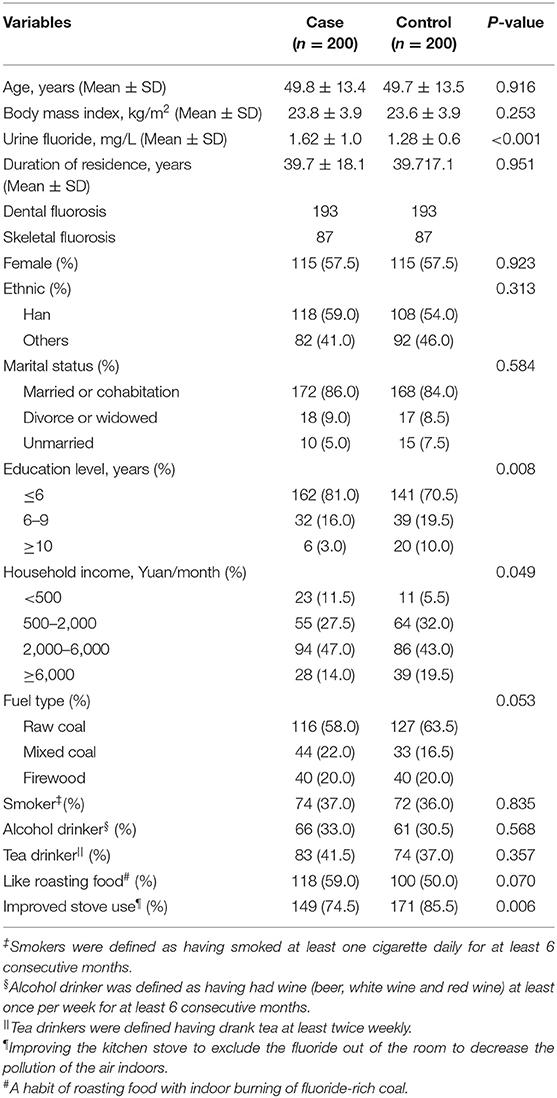
Table 1. Characteristics of fluorosis cases and controls.
Urinary Fluoride Detection
A 10 ml urine sample was collected from each participant. Urinary fluoride concentration was analyzed by a standardized method (WS/T 89-2015, China). Briefly, 1 ml of urine was mixed with 24 ml of deionized water, one pill of fluoride adjustment buffer powder was added to each 25 ml mixture. Then, the concentration of urine fluoride in the mixture was measured by a HQ40d portable meter and the concentration of fluorine in the urine of the subjects was calculated according to the corresponding proportion. The coefficient of variation for the urinary fluoride was 2.29%. The urine fluoride concentrations for all participants were categorized into either the normal category (<1.6 mg/L) or the abnormal category (more than 1.6 mg/L), according to national criteria (WS/T 256-2005).
Statistical Analysis
The data were tabulated as mean and SDs for continuous variables, or by proportions for categorical variables. To achieve an approximately normal distribution for statistical analysis, a logarithmic transformation and a square root transformation were performed for intake of energy and dietary nutrients, respectively. Dietary nutrient intake data were controlled for total energy intake by the regression residual method (19). The chi-square test and t-test were used to test the differences in socio-demographics and nutrient intakes of the fluorosis cases and controls. The factor scores were categorized into tertiles. T1, T2, and T3 represented a low, medium and high food intake patterns, respectively.
Conditional logistic regression analysis models were constructed to obtain odd ratios (ORs) and corresponding 95% confidence intervals (95% CIs) as estimates of relative risk, which are shown for the second and third tertiles, with the lowest tertile group as the reference category. We estimated the risk of fluorosis associated with each of the three dietary patterns separately. In the multivariate models, the relationships between dietary patterns and the risk of fluorosis were further examined after adjusting for various potential confounding variables such as duration of residence in Zhijin, ethnicity, marital status, education level, household income, body mass index (BMI), urinary fluoride level, smoking, alcohol drinking, tea drinking, domestic fuel type, and use of improved stove, whether, or not like roasting food. We further examined the association between dietary pattern and CBF across different subgroups stratified by gender (man/women) and whether or not like roasting food (Yes/No). To test the p-value of the trends, the ordinal values of the tertile of each factor score were entered as continuous variables in a logistic regression analysis model. In this study, SPSS 18.0 was used for the statistical analysis, all of the P-values were two sided and statistical significance was determined at the p < 0.05 level.
Results
The characteristics of the CBF cases and controls are presented in Table 1. Of the 200 CBF patient–control pairs, 193 patient pairs had dental fluorosis and 85 patient pairs had skeletal fluorosis. The average age was 49.8 years in the CBF patients and 49.7 years in the control group. The CBF group had lower education levels, household incomes, higher urinary fluoride levels, and were less likely to use an improved stove. No significant differences were found between the CBF cases and control in marital status, BMI, duration of residence in Zhijin, smoking status, alcohol, or tea drinking.
We identified three major dietary patterns using the factor analysis procedure, presented in Table 2. The first pattern, named the high protein dietary pattern, was characterized by a high intake of beef, seafood, poultry, fish and pork. The second pattern, named the healthy dietary pattern, was characterized by a high intake of fruit, dairy, legume, nuts, and fungus. The third pattern was characterized by a high intake of squash, potatoes, corn, dried chili and cured meat. This last group was labeled as the easy-to-roast dietary pattern, because Zhijin County residents commonly roast this last group of foods before consumption. Dietary patterns 1, 2, and 3 accounted for 7.9, 7.1, and 5.7% of the variability, respectively, and 26.7% of the variance in food intake overall.
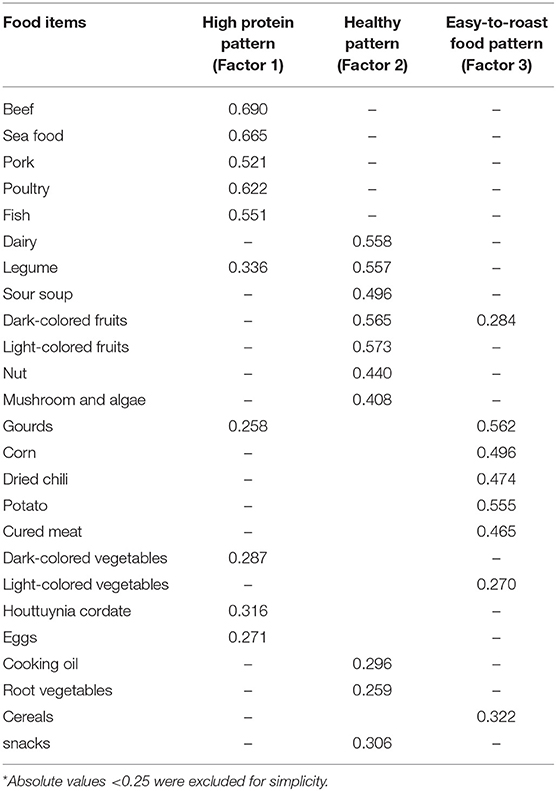
Table 2. Factor-loading matrix for the three major dietary patterns*.
As shown in Table 3, univariate analyses showed CBF was inversely associated with the healthy dietary pattern (p < 0.001) but positively associated with the easy-to-roast dietary pattern. A significant relationship remained even after adjustments were made for duration of residence in Zhijin, ethnicity, marital status, education level, household income, smoking status, alcohol drinking, tea drinking, daily energy intake, dietary supplement usage, domestic fuel type, use of improved stoves, and whether or not like roasting food. The risk of CBF decreased by approximately 53% in the highest tertile of the healthy dietary pattern group, compared with the reference lowest tertile (OR = 0.47, 95% CI = 0.27–0.84, p = 0.003). Significant relationships were observed between CBF risk and the healthy dietary pattern (T3 vs. T1: OR 2.05, 95% CI 1.15–3.66, p = 0.017). In addition, there was no association between the high protein diet pattern and CBF.
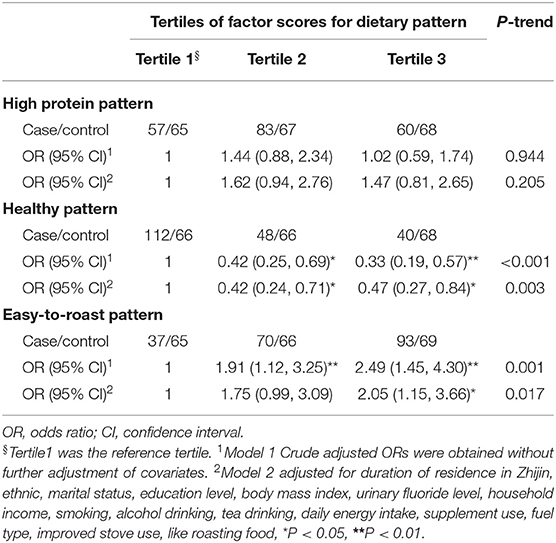
Table 3. Odds ratios (ORs) and 95% confidence intervals (95% CIs) of fluorosis according to tertiles of factor scores for each dietary pattern.
The results of dental and skeletal fluorosis sub-type analyses are shown in Table 4. We observed a similar dental fluorosis incidence in the healthy diet group as in the easy-to-roast diet group. Skeletal fluorosis was negatively associated with the healthy diet group (p = 0.025), but marginally positively associated with the easy-to-roast diet group after adjustment (p = 0.089). Stratified analyses showed a negative association between the healthy dietary pattern and CBF in women but not in men, and a positive association between the easy-to-roast dietary pattern and CBF (Supplementary Table 1).
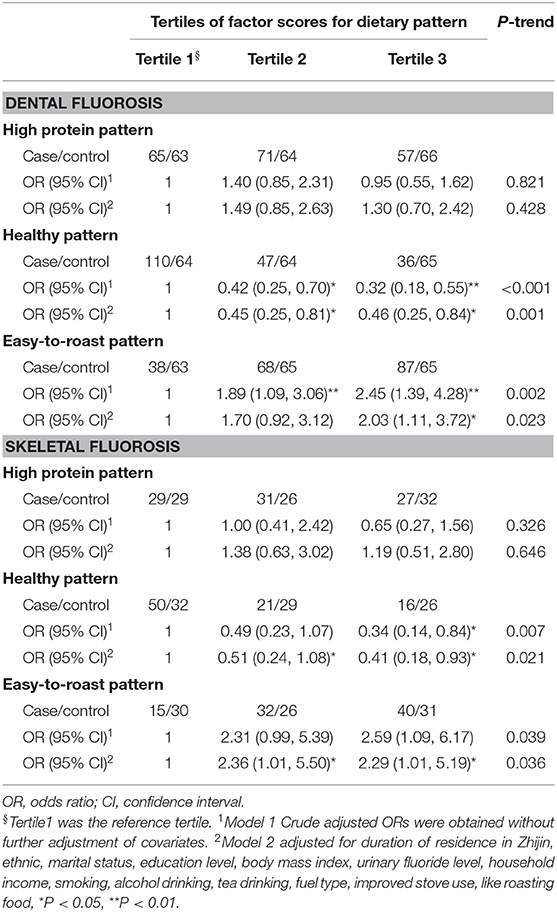
Table 4. Odds ratios (ORs) and 95% confidence intervals (95% CIs) of dental and skeletal fluorosis according to tertiles of factor scores for each dietary pattern.
Discussion
To our knowledge, this matched case-control study was the first to use factor analysis to evaluate the associations between dietary patterns and CBF risk in a population living in a coal-burning fluorosis area. We extracted three distinct dietary patterns, which are high protein, healthy and easy-to-roast. We found that the healthy dietary pattern had a significant protective effect against CBF, whereas the easy-to-roast dietary pattern was related to an increased risk of CBF.
In present study, we found that a healthy dietary pattern, typified by a high intake of fruit, dairy, legumes, nuts and fungus, was associated with a decreased risk of CBF. Although no studies specifically reported the association between bone damage and CBF, there were many studies that explored the relationship between dietary pattern and bone health. A similar pattern was observed in a matched case-control study of hip fractures in a Chinese population, where a healthy dietary pattern of nuts, fungus, soy and milk were found to be beneficial to bone health (20). Recently, two meta-analyses assessed the relationship between dietary patterns, bone mineral density and the risk of fracture and suggested a healthy diet reduced risk of low BMD in different age groups. The studies also compared the risk of fracture between high and low food intake categories of healthy diet patients (OR = 0.81; 95% CI: 0.69, 0.95; p = 0.01) (21, 22). The studies indicated a healthy diet was characterized by “Calcium foods,” “Dairy and whole grains,” “Fruit, milk, and whole grains,” “Milk and root vegetables,” “Vegetable-fruit-soy,” and “Dairy-fruit” (21, 22). In the present study, we found similar components to these healthy dietary patterns. Therefore, healthy diet had a beneficial effect on CBF in the present study and may be attributed to its protective role in bone health. The observed healthy dietary pattern has a balanced food composition, which may explain its beneficial effect against CBF. Additionally, Food choices may be influenced by educational level of participant. Participants with higher education were more likely to follow a healthy diet because they had access to healthy food items. No epidemiological studies have explored the association between nuts, mushrooms, and fluorosis, although a few studies have found that dairy and fruit have protective effects against fluorosis (23–25). Patients who adhered to a healthy dietary pattern had a high intake of calcium, magnesium, carotenoids, vitamin C, vitamin E, and isoflavones. Experimental studies have demonstrated that dietary calcium intake promotes the formation of a high bone formation and adequate dietary calcium or calcium supplements may contribute to a lower risk of fluorosis as calcium antagonizes the effects of fluoride (26, 27). Additionally, oxidative stress is a prime contributing mechanism in CDF and antioxidative nutrients may play important role in preventing CDF (28). It was reported that lycopene combated NaF-induced apoptosis of ameloblast cells and dental fluorosis by improving oxidative stress and down-regulating the caspase pathway (29). Furthermore, vitamin E and lycopene have been shown to prevent fluorosis-induced spermatogenic cell apoptosis through the suppression of oxidative stress-mediated JNK and ERK signaling pathways (30). Several studies suggested isoflavones from legumes and vitamin C may prevent fluorosis by antagonizing the oxidative stress damage caused by fluorine (31, 32). Therefore, we speculate that the antioxidant effects and effect of calcium on bone metabolism may partly explain the protective effects of healthy diets.
This analysis noted a positive association between the easy-to-roast food dietary pattern and CBF risk. We compared the factor scores of easy-to-roast dietary patterns between two groups and found high scoring individuals had a preference for roasted foods. The stratified analysis showed that the positive association between the easy-to-roast foods and fluorosis only existed in subjects who like roasting food. These results indicated the cooking method itself may be an actual risk factor for developing CBF. We conducted this case-control study in Zhijin County, where the moist climate requires residents to burn stoves with mixed fluoride-rich coal and clay. Residents were used to roasting foodstuff over it, such as corns, potato, squash and red chili. Cured meat is also a roasted food and residents commonly hang it for more than 2 months in a house polluted by fluoride dust in Zhijin County. Thus, this dietary pattern involved foods which were easy to roast before consumption. The combustion process released fluoride from the coal and fluorine content significantly increases on the roasted foodstuffs. Previous studies reported fluoride contents of roasted chili, corn, squash, potatoes and cured meat reached 419.8 mg/kg (33), 39.5 mg/kg (33), 121.8 mg/kg (34), 134.6 mg/kg (35), and 182.2 mg/kg (36), respectively. Corn and potatoes are the primary foods consumed by residents of Zhijin and daily mean fluoride intake (per person) from corn was 37.6 and 3.5 mg from potatoes (37). Previous studies demonstrated that particular roasted foods, such as corn, chilli, and potatoes, were the primary pathological cause of coal-burning fluorosis, because of the fluorine pollution coming from the coal briquettes and binder clay (6, 37, 38). Therefore, the present study suggests that the easy-to-roast dietary pattern in our study was positively associated with a risk of fluorosis not because the foods themselves were a source of fluorine, but rather roasting food over coal stoves caused the fluorine pollution.
In subgroup analysis, we observed a protective effect of the healthy dietary pattern against fluorosis in women but not in men. The gender difference in the association between dietary pattern and fluorosis has not been clearly explained. Diet might influence fluorosis between men and women differently due to sex hormones, or sex-specific genes, which are related to the control of fluorosis. Additionally, one of the main foods in this healthy dietary pattern were legumes, which contain the phytoestrogen isoflavone. Meta-analysis and randomized controlled trials demonstrated soy isoflavones have potential bone-specific effects in women (39, 40). The matrix of soy protein-enriched soy isoflavones may improve their bioavailability and biologic efficacy, improving tibia bone architecture (41). Thus, the negative association between the healthy dietary pattern and CBF in women may be attributed to estrogen's effect on isoflavones. Further studies are needed to clarify underlying mechanisms of this process.
The present study had several limitations. First, given the case-control design, we were unable to evaluate the causal associations between dietary patterns and the risk of fluorosis, which need to be confirmed in future studies. Second, it is known that FFQs have measurement error to some extent, although the FFQ used in this study has been validated (16). Third, the factor analysis requires many subjective decisions related to the selection of food groups, including decisions about the number of factors extracted, the type of rotation, and the interpretation and labeling of the factors. Although, this 1:1 matched case-control study was based on community populations, fluorosis and control were not randomly selected, which limited the generalization of findings. Finally, although we adjusted many factors for the statistical analysis, residual confounding was still unavoidable due to potential measurement errors and missing adjustments for some unmeasured factors.
In summary, the present study identified that a healthy dietary pattern has a protective effect against CBF, and that an easy-to-roast dietary pattern was significantly associated with an increased risk of CBF. Our findings suggest that a high consumption of fruit, dairy, legumes, nuts, mushrooms, and a low consumption of roasted corn, potatoes, chillis, and squash may protect against CBF in populations living in coal-burning fluorosis areas.
Data Availability Statement
The datasets generated for this study are available on request to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by Medical Ethics Committee of Zunyi Medical University. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
JL designed the study, and conducted the study, and revised the manuscript. SY and ML was responsible for the data management, analysis, and wrote the first draft of the manuscript. XM critically revised the manuscript. NT, XZ, and TC assisted in conducting the research and data collection. DW developed the idea and proofread the manuscript.
Funding
This study was supported by the National Natural Science Foundation of China (grant number 81460497) and Doctoral Foundation of Zunyi Medical University (F706).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors want to thank the study subjects for their willingness to participate and the students who participated in the recruitment of subjects and the interviews in this study. We also thank the Center of Disease Control and Prevention of Zhijin County for providing administrative support to our study.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2019.00189/full#supplementary-material
References
1. Fawell J, Bailey K, Chilton J, Dahi E, Fewtrell L, Magara Y. Fluoride in Drinking-Water. Zunyi: WHO Press (2006). 6–45 p.
2. Jha SK, Mishra VK, Sharma DK, Damodaran T. Fluoride in the environment and its metabolism in humans. Rev Environ Contam Toxicol. (2011) 211:121–42. doi: 10.1007/978-1-4419-8011-3_4
3. Guan ZZ, Wu CX, Qi XL. Evaluation of health status of coal-burning fluorosis areas in Guizhou province after comprehensive management. J Guizhou Med Univ. (2018) 43:1124–28.
4. Liu YL, M P, Luo KL, Li L. The state and trend of endemic fluorosis from 1991 to 2012 in China. J Chongqing Norm Univ. (2016) 33:142–51. doi: 10.11721/cqnuj20160228
5. Zhou YX, Mo SL, Wang RH, Liu WF, Liu JC, Wang JQ, et al. Corn baked by burning coal triggered overexpression of osteopontin in hepatocytes of rats following fluorosis. Toxicol Ind Health. (2012) 28:195–202. doi: 10.1177/0748233711410905
6. Luo KL, Li L, Zhang SX. Coal-burning roasted corn and chili as the cause of dental fluorosis for children in Southwestern China. J Hazard Mater. (2011) 185:1340–7. doi: 10.1016/j.jhazmat.2010.10.052
7. Liu J, Luo MJ, Zhao X, Yang S, Zhang YM, Zhou D. Study on relationship between edible sour soup and coal-burning fluorosis. Chongqing Med J. (2019) 48:156–60. doi: 10.3969/j.issn.1671-8348.2019.04.024
8. Liu J, Yang S, Luo MJ, Zhao X, Zhang YM, Tao N. Analysis on the correlation between dietary vitamin C intake and coal-burning fluorosis. J Mod Med Health. (2018) 34:2119–21. doi: 10.3969/j.issn.1009-5519.2018.14.004
9. Yang S, Luo MJ, Tao N, Zhang YM, Zhao X, Liu J. Relationship between dietary intake of vitamin A and coal burning fluorosis. Shandong Med J. (2018) 58:28–31. doi: 10.3969/j.issn.1002-266X.2018.06.007
10. Yang S, Luo MJ, Tao N, Zhang YM, Zhao X, Liu J. Association between dietary intake of vitamin E and coal-burning fluorosis. Guangdong Med J. (2018) 39:2054–57. doi: 10.13820/j.cnki.gdyx.2018.13.018
11. Liu J, Yang S, Luo MJ, Zhao X, Zhang YM, Luo Y. Association of dietary carotenoids intake with skeletal fluorosis in the coal-burning fluorosis area of Guizhou province. Biomed Environ Sci. (2018) 31:438–47. doi: 10.3967/bes2018.057
12. Patel PP, Patel PA, Zulf MM, Yagnik B, Kajale N, Mandlik R, et al. Association of dental and skeletal fluorosis with calcium intake and serum vitamin D concentration in adolescents from a region endemic for fluorosis. Indian J Endocrinol Metab. (2017) 21:190–5. doi: 10.4103/2230-8210.196013
13. Simon MJ, Beil FT, Ruther W, Busse B, Koehne T, Steiner M, et al. High fluoride and low calcium levels in drinking water is associated with low bone mass, reduced bone quality and fragility fractures in sheep. Osteoporos Int. (2014) 25:1891–903. doi: 10.1007/s00198-014-2707-4
14. Schwerin HS, Stanton JL, Smith JL, Riley AMJ, Brett BE. Food, eating habits, and health: a further examination of the relationship between food eating patterns and nutritional health. Am J Clin Nutr. (1982) 35:1319–25. doi: 10.1093/ajcn/35.5.1319
15. Hu FB. Dietary pattern analysis: a new direction in nutritional epidemiology. Curr Opin Lipidol. (2002) 13:3–9. doi: 10.1097/00041433-200202000-00002
16. Zhang CX, Ho SC. Validity and reproducibility of a food frequency Questionnaire among Chinese women in Guangdong province. Asia Pac J Clin Nutr. (2009) 18:240–50. doi: 10.6133/apjcn.2009.18.2.13
17. Yang YX, Wang GY, Pan XC. China Food Composition. 2nd ed. Beijing: University Medical Publishing House (2009).
18. Varraso R, Garcia-Aymerich J, Monier F, Moual NL, Batlle JD, Miranda J, et al. Assessment of dietary patterns in nutritional epidemiology: principal component analysis compared with confirmatory factor analysis. Am J Clin Nutr. (2012) 96:1079–92. doi: 10.3945/ajcn.112.038109
19. Willett WC, Howe GR, Kushi LH. Adjustment for total energy intake in epidemiologic studies. Am J Clin Nutr. (1997) 65:1220S–8S. doi: 10.1093/ajcn/65.4.1220S
20. Zeng FF, Wu BH, Fan F, Xie HL, Xue WQ, Zhu HL, et al. Dietary patterns and the risk of hip fractures in elderly Chinese: a matched case-control study. J Clin Endocrinol Metab. (2013) 98:2347–55. doi: 10.1210/jc.2013-1190
21. Denova-Gutierrez E, Mendez-Sanchez L, Munoz-Aguirre P, Tucker KL, Clark P. Dietary patterns, bone mineral density, and risk of fractures: a systematic review and meta-analysis. Nutrients. (2018) 10:E1922. doi: 10.3390/nu10121922
22. Fabiani R, Naldini G, Chiavarini M. Dietary patterns in relation to low bone mineral density and fracture risk: a systematic review and meta-analysis. Adv Nutr. (2019) 10:219–36. doi: 10.1093/advances/nmy073
23. Liu GJ, Ye QF, Chen W, Zhao ZJ, Li L, Lin P. Study of the relationship between the lifestyle of residents residing in fluorosis endemic areas and adult skeletal fluorosis. Environ Toxicol Pharmacol. (2015) 40:326–32. doi: 10.1016/j.etap.2015.06.022
24. Susheela AK, Mondal NK, Tripathi N, Gupta R. Early diagnosis and complete recovery from fluorosis through practice of interventions. J Assoc Physicians India. (2014) 62:572–9.
25. Hussain J, Hussain I, Sharma KC. Fluoride and health hazards: community perception in a fluorotic area of central Rajasthan (India): an arid environment. Environ Monit Assess. (2010) 162:1–14. doi: 10.1007/s10661-009-0771-6
26. Li GS, Ren LQ. Effects of excess fluoride on bone turnover under conditions of diet with different calcium contents. Zhonghua Bing Li Xue Za Zhi. (1997) 26:277–80. doi: 10.1111/j.1439-0264.1997.tb00136.x
27. Xu H, Liu QY, Zhang JM, Zhang H, Li GS. Elevation of PTH and PTHrp induced by excessive fluoride in rats on a calcium-deficient diet. Biol Trace Elem Res. (2010) 137:79–87. doi: 10.1007/s12011-009-8561-0
28. Suzuki M, Bandoski C, Bartlett JD. Fluoride induces oxidative damage and SIRT1/autophagy through ROS-mediated JNK signaling. Free Radic Biol Med. (2015) 89:369–78. doi: 10.1016/j.freeradbiomed.2015.08.015
29. Li WS, Jiang BH, Cao XL, Xie YJ, Huang T. Protective effect of lycopene on fluoride-induced ameloblasts apoptosis and dental fluorosis through oxidative stress-mediated Caspase pathways. Chem Biol Interact. (2017) 261:27–34. doi: 10.1016/j.cbi.2016.11.021
30. Tian Y, Xiao YH, Wang BL, Sun C, Tang KF, Sun F. Vitamin E and lycopene reduce coal burning fluorosis-induced spermatogenic cell apoptosis via oxidative stress-mediated JNK and ERK signaling pathways. Biosci Rep. (2018) 38:1–4. doi: 10.1042/BSR20171003
31. Peng W, Xu SR, Zhang J, Zhang Y. Vitamin C attenuates sodium fluoride-induced mitochondrial oxidative stress and apoptosis via Sirt1-SOD2 pathway in F9 cells. Biol Trace Elem Res. (2019) 191:189–98. doi: 10.1007/s12011-018-1599-0
32. Zhu JZ, Liu JH, Zhao WT, Zhang HF. Protective effects of soy isoflavones on liver and kidney damage in rats with fluorosis. Chin J Contr Endem Dis. (2016) 31:527.
33. Li DS, Wang SQ, Li P, Duan RX, He GY, Hu XQ, et al. Analysis of 7 years' monitoring on coal-burning pollution endemic fluorosis in the state test spot in Zhijin County of Guizhou province. Chin J Endemiol. (1999) 18:349–51.
34. Xie L, Wei X, Pan NS, Zeng CS, Zhang XQ, Wu XY, et al. Detection of Fluoride in gourd and eggplant in coal area of Zunyi city. For All Health. (2015) 303–4. doi: 10.3969/j.issn.1009-6019.2015.03.393
35. Xie L, Wei X, Pan NS, Zeng CS, Zhang XQ, Wu XY, et al. Detection of fluoride sweet potato and potato in coal area of Zunyi city. Chin Baby. (2015) 354–5.
36. Zeng GH, Long XJ, Hu DF, X QW, Zhang B, Wang QS, et al. Investigation on current prevalence of endemic fluorosis in Loudi city, Hunan province. Chin J Endemiol. (2004) 23:240–1. doi: 10.3760/cma.j.issn.1000-4955.2004.03.018
37. Qin X, Wang S, Yu M, Zhang L, Li X, Zuo Z, et al. Child skeletal fluorosis from indoor burning of coal in southwestern China. J Environ Public Health. (2009) 2009:969764. doi: 10.1155/2009/969764
38. Li L, Luo KL, Tang YG, Liu YL. The daily fluorine and arsenic intake for residents with different dietaries and fluorosis risk in coal-burning fluorosis area, Yunnan, Southwest China. Environ Sci Pollut Res Int. (2015) 22:2031–40. doi: 10.1007/s11356-014-3485-4
39. Zhang X, Liu Y, Xu Q, Zhang Y, Liu L, Li H, et al. The effect of soy isoflavone combined with calcium on bone mineral density in perimenopausal Chinese women: a 6-month randomised double-blind placebo-controlled study. Int J Food Sci Nutr. (2019) 4:1–9. doi: 10.1080/09637486.2019.1673703
40. Akhlaghi M, Ghasemi Nasab M, Riasatian M. Soy isoflavones prevent bone resorption and loss, a systematic review and meta-analysis of randomized controlled trials. Crit Rev Food Sci Nutr. (2019) 10:1–15. doi: 10.1080/10408398.2019.1635078
Keywords: dietary pattern, factor analysis, fluorosis, coal burning, case-control and matched study
Citation: Liu J, Yang S, Luo M, Chen T, Ma X, Tao N, Zhao X and Wang D (2020) Association Between Dietary Patterns and Fluorosis in Guizhou, China. Front. Nutr. 6:189. doi: 10.3389/fnut.2019.00189
Received: 19 September 2019; Accepted: 06 December 2019;
Published: 21 January 2020.
Edited by:
Francesco Sofi, University of Florence, ItalyReviewed by:
Omar Cauli, University of Valencia, SpainRosilene Ventura Ribeiro, University of Sydney, Australia
Copyright © 2020 Liu, Yang, Luo, Chen, Ma, Tao, Zhao and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dong-hong Wang, d2FuZ2Rvbmdob25nMTk3MEAxMjYuY29t