 Juliana Costa Liboredo1
Juliana Costa Liboredo1 Lucilene Rezende Anastácio2
Lucilene Rezende Anastácio2 Lívia Garcia Ferreira3
Lívia Garcia Ferreira3 Lívya Alves Oliveira4
Lívya Alves Oliveira4 Ceres Mattos Della Lucia4*
Ceres Mattos Della Lucia4*- 1Department of Food, Universidade Federal de Ouro Preto, Ouro Preto, Brazil
- 2Graduate Program in Food Science, Food Science Department, Faculty of Pharmacy, Universidade Federal de Minas Gerais, Belo Horizonte, Brazil
- 3Graduate Program in Nutrition and Health, Universidade Federal de Lavras, Lavras, Brazil
- 4Graduate Program in Nutrition Science, Universidade Federal de Viçosa, Viçosa, Brazil
The study aimed to assess the eating behavior [uncontrolled eating (UE), emotional eating (EE), and cognitive restraint (CR)], the perceived stress, and independently associated factors among Brazilians during the COVID-19 pandemic. An online survey was conducted and data about 1,368 participants were evaluated. Multivariate logistic regression models were performed to identify factors independently associated (socioeconomic, lifestyle, and eating habits data) with eating behaviors and perceived stress. Working in the COVID-19 frontline (OR = 2.19), increased food delivery (OR = 1.49), increased food intake (OR = 1.48), increased number of meals (OR = 1.13), and EE (OR = 1.05) were factors independently associated with UE. Variables that were independently associated with EE were: increased food intake (OR = 2.57), graduation in a non-health-related course (OR = 1.78), perceived stress (OR = 1.08), UE (OR = 1.07), and CR (OR = 1.02). Reduced snacking (OR = 2.08), female gender (OR = 1.47), having a higher degree (OR = 1.44), increased homemade meals (OR = 1.31), the higher difference in the frequency of instant meals and snacks intake (OR = 0.91), EE (OR = 1.01), not increased alcohol dose intake (OR = 0.57), and increased physical activity (OR = 0.54) were independently associated with CR. Perceived stress was independently associated with changes in the way of working or studying (OR = 2.48), worse sleep quality (OR = 2.22), younger age (OR = 1.06), and EE (OR = 1.02). This study indicates that socioeconomic variables, lifestyle, and eating habits were independently associated with the eating behaviors of Brazilians and perceived stress during the quarantine.
Introduction
The acute respiratory disease caused by the SARS-CoV-2 virus (COVID-19) has already affected individuals in 220 countries, areas, or territories (1). Globally, there have been more than 175 million confirmed cases and more than 3 million deaths (1). The spread of SARS-CoV-2 led health officials worldwide to take several measures, such as complete city locking down, building hospitals, performing strict social distancing, and implementing sanitary measures. Despite the important effect against COVID-19, social distancing can lead to changes in the daily life of the population. There may be changes in access to food, in the habit of eating out (2), and even changes in food purchases by families due to the possibility of losing their jobs or having reduced income during this period (2). Food markets have access restricted and restaurants and bars have been closed, which may affect the food buying and consumption behavior (3, 4). It may further affect the choices of an individual to prepare their meals or buy premade food more often. Social distancing can affect eating patterns (5), promoting snacking, eating palatable meals, and increased alcohol consumption (6). People reported snacking more frequently (7), increased consumption of sweets and snacks rich in calories has been found in studies carried out during the quarantine in different countries (3, 5, 8).
Additionally, facing excessive daily information about the pandemic may cause stress (9). Most people usually change their eating behaviors when stressed, resulting in under or overeating, depending on the stressor severity (10). Furthermore, interruption of the work routine caused by the quarantine could result in boredom, which in turn is associated with a greater energy intake (11).
Some studies have focused on identifying eating habits change (2, 12), but information about the impact of the COVID-19 pandemic on eating behavior and perceived stress is still limited, especially in Brazil. It is believed that the pandemic has resulted in increased food delivery, food intake, number of meals, and emotional eating (EE) behavior in Brazilians. This study aimed to assess the eating behavior, the perceived stress, and their independently associated factors among Brazilians during the pandemic. These results may be useful to define strategies to minimize the problems observed and to encourage healthy behavior during the period of social distancing.
Materials and Methods
Study Design
A cross-sectional online survey, based on a sample for convenience, was conducted from August 14, 2020, to September 9, 2020, approximately 5–5.5 months after the beginning of the social distancing measures in Brazil. At that time, Brazil showed the highest number of cases and deaths in Latin America, and it was the third country with the most cases in the world, behind only the United States of America and India. The lockdown measures implemented in Brazil included: suspension of non-essential activities (closing of restaurants, bars, shopping malls, and gyms), suspension of the activities of schools and universities and with the implementation of emergency remote education, the incentive to adhere to social and physical distance measures, among other issues addressed in Federal Law No. 13,.979, of February 6, 2020. Brazilian residents aged 18 years of age or older were invited to enroll in the study. Pregnant women, individuals under 18 years of age, and residents of other countries were excluded (Figure 1). The study was conducted according to the Declaration of Helsinki. The protocol was approved by the Research Ethics Committee of the Federal University of Viçosa, Minas Gerais, Brazil (Protocol number 35516720.5.0000.5153).
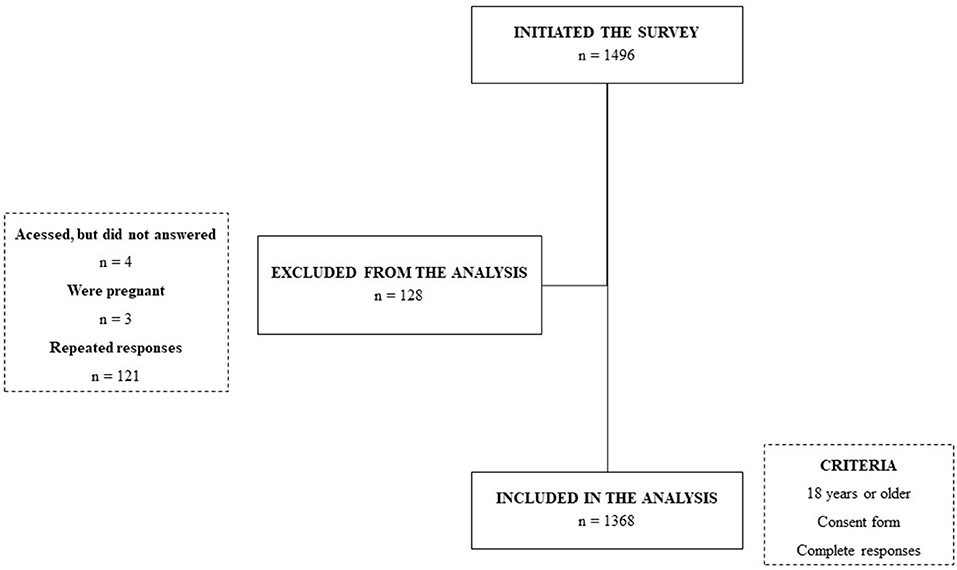
Figure 1. Study recruitment.
Instrument and Procedure
The survey was created on Google Form Platform® and the link was shared via emails, university websites, and social media. The first part of the survey included the consent form. The answers of the participants were anonymous (only the emails of the participants were available), and they were able to stop their participation in the study at any stage before submitting the answers.
Eating behavior was assessed using the Brazilian version of the Three-Factor Eating Questionnaire (TFEQ-R21) translated into Portuguese and validated by Natacci and Ferreira Júnior (13). TFEQ-R21 measures eating behavior based on uncontrolled eating (UE), EE, and cognitive restraint (CR). The TFEQ consisted of 21 questions (a 4-point response format for items 1 to 20, and a numerical rating scale of 8 points for question 21). Responses to each of the questions were given a score between 1 and 4. Before calculating the scores, items 1–16 were reverse coded and item 21 was recorded as follows: 1–2 scores as 1, 3–4 as 2, 5–6 as 3, 7–8 as 4. The CR scale was composed of items 1, 5, 11, 17, 18, and 21. The UE scale was composed of items 3, 6, 8, 9, 12, 13, 15, 19, and 20. The EE scale was composed of items 2, 4, 7, 10, 14, and 16. The mean of each was calculated and transformed into a scale from 0 to 100 points as recommended in the score instruction (13). Perceived Stress (PS) was measured by a 10-item version of the Perceived Stress Scale (PSS) validated for the Brazilian population (14).
The other variables were divided into three sections: socioeconomic data, lifestyle, and eating habits. Socioeconomic data included questions about home state, gender, age, per capita income, the composition of home residents (posterior divided into groups of living with sons vs. others and living with parents vs. others), an education level (divided into groups of complete graduation course vs. incomplete graduation course or less, postgraduation or not, and graduation in a health-related course or not), current occupation (divided into professors or not, students or not, healthcare professionals or not, and workers in the line of the front of COVID-19 or not), working schedule during pandemic (perception of lower, unaltered, or greater time spent in work, including domestic activities), labor situation (alteration in the way of working or studying during a pandemic period or not, to study or work remotely full-time or part-time), and social isolation (total and partial or not).
As for lifestyle habits, participants were also asked about time and quality of sleep, amount of time of physical activity/week, smoking habit, alcohol consumption (dose and frequency), screen time (smartphones, computer, tablet, and TV) before and during the pandemic, and the differences were calculated. These variables were evaluated numerically and dichotomized into greater or not and lower or not about such habits.
Eating habits included differences in the number of meals (before and during a pandemic), the type of meals consumed (breakfast, morning snack, lunch, afternoon snack, dinner, evening snack, and other meals), amount of food, snacking (eating between meals), using food delivery service, habits of cooking at home, and food frequency (times a week) related to the periods before and during the pandemic.
A food frequency questionnaire based on the Food and Nutritional Surveillance System (SISVAN) protocol was used (15), with the following groups: legume (beans, soybeans, lentils, and chickpeas), cereal (rice, corn, and oats), bakery products (bread, cakes, and cookies), milk and dairy, fruit, meat, hamburger or canned products (hamburger, bologna, salami, and sausage), vegetables (except potatoes, cassava, and yams), sugary drinks (soft drink, canned or powdered juice, canned coconut water, guarana/blackcurrant syrup, and fruit juice with sugar), instant foods and snacks (instant noodles, packaged snacks, or crackers), candies (chocolate, pies, lollipops, gum, caramel, and jelly), and fast-food (pizza, sandwich, and finger food). The volunteers filled in information related to the time before and during pandemic for groups of foods and the differences were calculated. The frequency of consumption of the food groups was set to 0 for those who reported never consuming such food, 0.5 for those who reported consuming rarely, 1 for those who consumed once a week, 2.5 for consumption 2–3 times/week, 5 for consumption 4–6 times/week, 7 for consumption once a day, and 10 for more than once a day, and the differences between the frequency of consumption before and during the pandemic were calculated. When the differences were positive, they were classified as increased consumption and when they were negative, they were classified as decreased consumption. The consumption frequencies before and during the pandemic may be found in another study of the team (16).
Questions about lifestyle habits and eating habits were based on other online surveys performed during the COVID-19 pandemic (2, 5). To verify the adequacy and the response time of the questions, a pilot study was carried out with about 30 respondents.
Data Analysis
Data were analyzed using the software Statistical Package for Social Sciences® (SPSS® Inc., Chicago, IL, USA) version 21.0. Data are shown as median, minimum, and maximum values for independently associated factors and interquartile intervals for UE, EE, CR, and PS. Assumption of normality was checked using the Kolmogorov-Smirnov test. The correlations between eating behaviors and PS were obtained by Spearman's correlation test. To evaluate the factors independently associated with the eating behaviors and PS, univariate (by Chi-square and Mann-Whitney) and multivariate logistic regression models, respectively, were performed. The score obtained in each questionnaire was divided into the cutoff point of the third quartile (UE: 48.1, EE: 61.1, CR: 61.1, and PS: 28.0). The highest quartile was chosen because it represents 25% of the most extreme data. The same was performed by other authors that used some scales related to eating behavior (17, 18). The models were obtained by the backward method. The fit of the models was tested by the Hosmer-Lemeshow test (p > 0.05). The level of significance adopted was 0.05.
Results
A total of 1,368 individuals were enrolled in this study (1,496 answers were computed, but four individuals submitted the questionnaire and did not answer, three women were pregnant and there were 121 repeated answers). The responders were from the five regions of Brazil, but most participants (89.6%) reside in the southeast region.
Socioeconomic, Lifestyle, and Eating Habits Status
The median age of volunteers was 31 years old (varying from 18–87), and most responders were female (80%). Regarding the profile of home residents, 38.3% lived with parents and 25.1% lived with children. Most of the responders were graduates (65.9%), 46.5% attended postgraduation courses, and 49.6% were graduates in a health-related course. Most participants of the study reported increased time spent at work (65.9%), to be working or studying remotely full or partial-time (70.7%), and changes in the way of working or studying during the pandemic (89%). Furthermore, 57.2% related total social isolation during the pandemic.
Many respondents reported decreased sleep time (31.1%) and worsened sleep quality (46.3%) during quarantine. There was a positive difference in screen time with a median of 3.5 h, and 64.6% of participants showed longer screen time during the pandemic. The frequency of alcoholic beverages intake was increased by 17.9% of individuals, but 18.6% reported reduced frequency consumption and 20.3% increased the dose of alcoholic beverages consumed. Only 1.2% of the respondents related to increasing cigarette use and 43.3% reduced the physical activity time.
Regarding eating habits, food intake increased in 58.6% of the participants, and 51.5% reported snacking more frequently. The use of delivery food and homemade meals increased by 50.1 and 67.3%, respectively (Table 1).
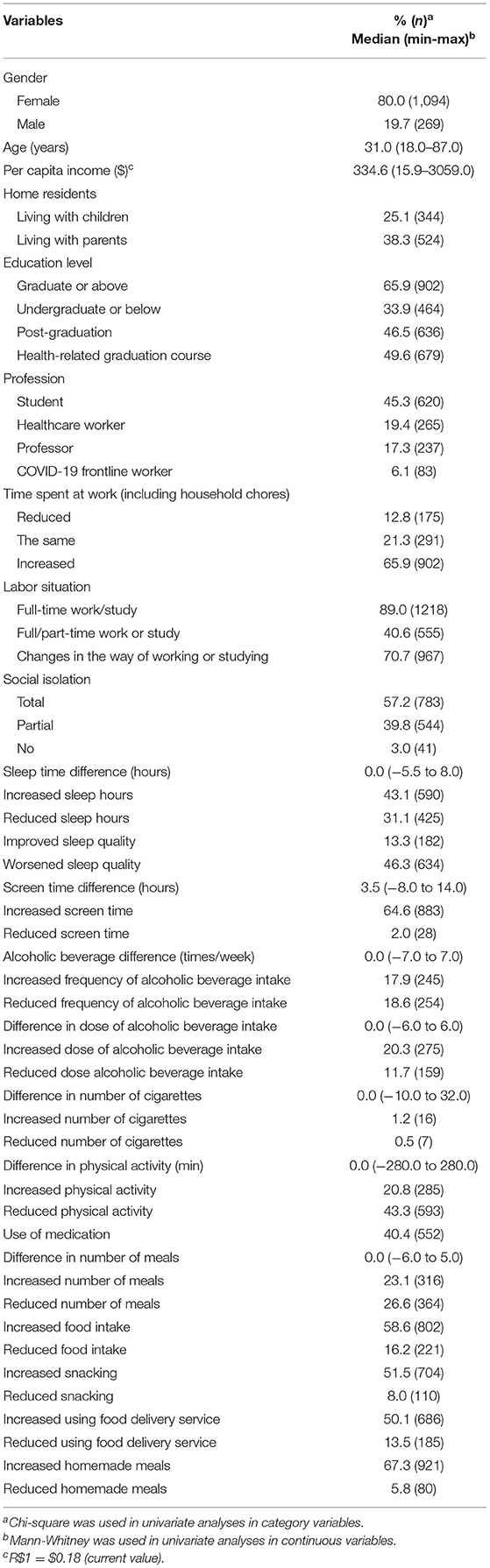
Table 1. Socioeconomic factors, lifestyle, and eating habits of a Brazilian sample during the COVID-19 pandemic period.
Eating Behaviors and Perceptive Stress: Independently Associated Factors
The respective median scores for UE, EE, and CR were 33.9 (interquartile interval: 18.5–48.1), 44.5 (interquartile interval: 27.8–61.1), and 39.5 (interquartile interval: 11.1–61.1) points. PS showed a median of 22.9 (interquartile interval: 19.0–28.0) points. The UE behavior was significantly and positively correlated to all the other behaviors and PS (EE: r = 0.098; CR: r = 0.714; PS: r = 0.257; p < 0.001 for all) and so the EE behavior (CR: r = 0.171 and PS: r = 0.334). However, the correlation between CR behavior and PS was significantly negative (r = −0.030). Variables associated with UE, EE, CR, and PS above the third quartile by univariate analyses are found in the Supplementary Material.
The significant difference in the frequency of food consumption (before and during the pandemic period) among the respondents who were under and above the third quartile of PS, CR, EE, and UE scores are shown in Figure 2.
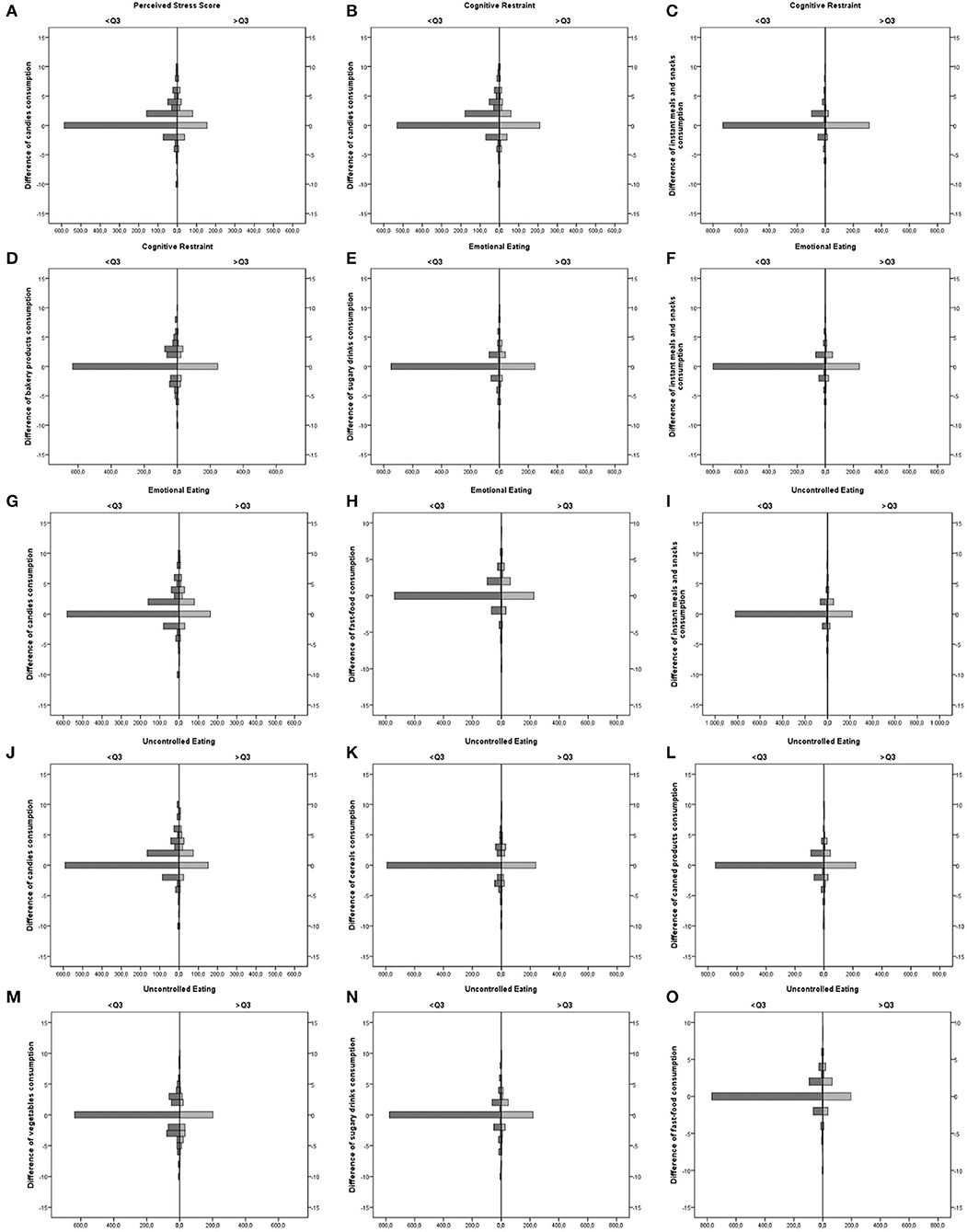
Figure 2. Difference of food consumption among Brazilians who were under and above the third quartile of perceived stress, cognitive restraint (CR), emotional eating (EE), and uncontrolled eating (UE) scores. (A) Difference of candies consumption among Brazilian who were below and above the 3rd Quartile of Perceived Stress score; (B) Difference of candies consumption among Brazilian who were below and above the 3rd Quartile of Cognitive Restraint score; (C) Difference of instant meals and snacks consumption among Brazilian who were below and above the 3rd Quartile of Cognitive Restraint score; (D) Difference of bakery products consumption among Brazilian who were below and above the 3rd Quartile of Cognitive Restraint score; (E) Difference of sugary drinks consumption among Brazilian who were below and above the 3rd Quartile of Emotional Eating score; (F) Difference of instant meals and snacks consumption among Brazilian who were below and above the 3rd Quartile of Emotional Eating score; (G) Difference of candies consumption among Brazilian who were below and above the 3rd Quartile of Emotional Eating score; (H) Difference of fast-food consumption among Brazilian who were below and above the 3rd Quartile of Emotional Eating score; (I) Difference of instant meals and snacks consumption among Brazilian who were below and above the 3rd Quartile of Uncontrolled Eating score; (J) Difference of candies consumption among Brazilian who were below and above the 3rd Quartile of Uncontrolled Eating score; (K) Difference of cereals consumption among Brazilian who were below and above the 3rd Quartile of Uncontrolled Eating score; (L) Difference of canned products consumption among Brazilian who were below and above the 3rd Quartile of Uncontrolled Eating score; (M) Difference of vegetables consumption among Brazilian who were below and above the 3rd Quartile of Uncontrolled Eating score; (N) Difference of sugary drinks consumption among Brazilian who were below and above the 3rd Quartile of Uncontrolled Eating score; (O) Difference of fast-food consumption among Brazilian who were below and above the 3rd Quartile of Uncontrolled Eating score.
The multiple logistic regression analysis is summarized in Table 2. Factors that independently increased the probability of being in the highest quartile of UE score were: being a COVID-19 frontline worker (OR: 2.196; CI: 1.233–3.911), increased food delivery (OR: 1.498; CI: 1.105–2.031), increased food intake (OR: 1.483; CI: 1.049–2.097), increased number of meals (OR: 1.483; CI: 1.049–2.097), and emotional eating (OR: 1.054; CI: 1.047–1.061). Increased food intake (OR: 2.579; CI: 1.817–3.660), graduation in another non-health-related course (OR: 1.785; CI: 1.305–2.443), PS (OR: 1.080; CI: 1.052–1.108), UE (OR: 1.078; CI: 1.068–1.088), and CR (OR: 1.020; CI: 1.012–1.028) increased the probability of being in the highest quartile of EE score. Finally, factors positively and independently associated with CR were: reduced frequency of snacking (OR: 2.080; CI: 1.376–3.144), female gender (OR: 1.468; CI: 1.447–2.053), graduate status (OR: 1.443; CI: 1.097–1.893), increased frequency of homemade meals (OR: 1.314; CI: 1.004–1.722), increased difference in the frequency of ultra-processed food intake (OR: 0.91; CI: 0.849–0.981), and EE score (OR: 1.007; CI: 1.003–1.012). On the other hand, unincreased alcohol dose intake (OR: 0.573; CI: 0.405–0.811) and increased physical activity time (OR: 0.537; CI: 0.402–0.711) decreased the chance of being in the highest quartile of CR score. About PS, factors independently associated were: changes in the way of working or studying during quarantine (OR: 2.480; CI: 1.470–4.183), worsened sleep quality (OR: 2.222; CI: 1.700–2.904), younger age (OR: 1.069; CI: 1.053–1.085), and EE (OR: 1.016; CI: 1.012–1.021).
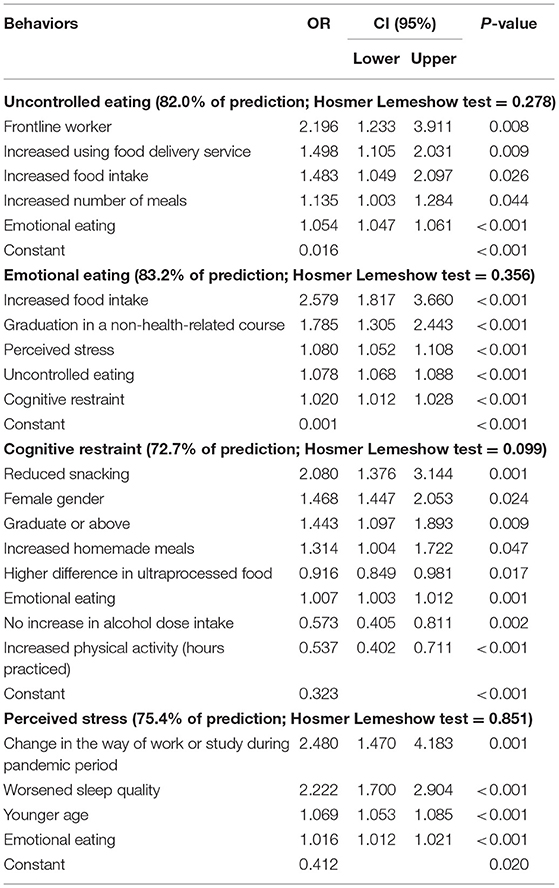
Table 2. Factors independently associated with the last quartile of the eating behaviors and stress among Brazilians during the pandemic period in multivariate analyses.
Discussion
The findings revealed that many respondents showed altered habits during the COVID-19 pandemic. Sleeping changes and physical activity reduction were observed, as found by Ammar et al. (12). Increased number of daily meals, increased food intake, snacking, increased use of food delivery, and homemade meals were also verified. Likewise, changes in diet during the pandemic have also been previously reported (2, 5). Studies carried out with Brazilian samples also found negative changes in eating habits (19, 20).
Furthermore, people during quarantine might experience severe disturbances in eating behavior, such as extremely reduced food intake or overeating, which could increase body weight and shape concerns (21). The lack of data about the eating behavior of Brazilians during the COVID-19 pandemic and the use of different questionnaires in other populations during quarantine limit comparisons. However, volunteers of the present research reported similar scores of EE [44.5 (27.8–61.1)] and lower scores of UE [33.9 (18.5–48.1)] and CR [39.5 (11.1–61.1)] in comparison to the study of de Medeiros et al. (22), performed before the pandemic, with healthy adult Brazilians (EE: 45.8 ± 29.2; UE: 55.6 ± 25.0, and CR: 70.8 ± 25.0). However, Papandreou et al. (23) found higher scores of eating behaviors in the Spanish and Greek population than other pre-COVID-19 data, supporting the idea that these behaviors may be affected during quarantine. Elmacioglu et al. (24), in a study that evaluated the eating behavior during the social isolation in the COVID-19 pandemic, found an increase in the EE and UE of individuals, but no significant changes in CR occurred.
In this study, the number of meals, food intake, and use of food delivery increased the chance to have UE scores in the highest quartile in 13.5, 48.3, and 49.8%, respectively. Increased food consumption and changes in eating behaviors are frequent in subjects ordered to follow stay-at-home during the pandemic (5). In the present study, the highest quartile of the behaviors studied was associated with differences in the frequency of candies (PS, CR, UE, and EE), instant meals and snacks (CR, UE), bakery products (CR), sugary drinks (EE, UE), cereals (UE), canned product (UE), vegetables (UE), and fast-food (EE, UE) consumption (Figure 2).
Furthermore, COVID-19 frontline workers showed a 2.2 higher chance to have greater UE scores. Beyond the risk of exposure to COVID-19 by contact with patients and coworkers, healthcare workers are under increasing stress and mental health risks due to higher workload, shortages of protective equipment (25), death of their colleagues after exposure to the virus, and fear of spreading it to their families (26). The context experienced by these workers may probably have contributed to the higher UE scores observed in this study.
Individuals with higher scores of EE showed higher chances to have UE scores above the third quartile. Studies have attempted to identify the influence of emotions on food consumption (27, 28). Humor and emotions can influence food choice, in the same way, that consumption of certain foods can change a mood or emotional state (27). People who have EE seem to be more susceptible to the effects of stress and may try to obtain comfort through food (29). Stress may promote irregular eating patterns and strengthen networks toward hedonic overeating, choosing more pleasurable, and palatable foods irrespective of caloric intake changes (30). In an Italian study (9) carried out during the COVID-19 pandemic, almost half of respondents felt anxious about their eating habits, consumed comfort foods, and increased food intake to feel better.
Emotional eating is related to the tendency of individuals to overconsumption of food in response to negative emotional stimuli (13). Increased food intake and UE, CR, and PS were associated with higher scores of EE. These results indicate that EE is determined by other eating behaviors and by PS, and probably affected food choice, as the strong association among EE and an increase in food intake during quarantine. Emotional factors probably impede the control of food intake in situations of stress. The EE behavior can occur as a coping strategy concerning negative emotions (31). Other authors reported the association between stress and eating behavior of EE (30, 31). In a study carried out during the COVID-19 outbreak, in which the majority (73.6%) of the participants reported moderate to high levels of perceived stress, the EE was significantly correlated with four of the nine reasons for food choice: mood, convenience, price, and familiarity (32). In a study conducted with mothers from Los Angeles, California, the authors observed that the most common strategy that mothers indicated to deal with stress related to COVID-19 was to eat comfort foods (e.g., sweets and snacks) (58.7%). The PS related to COVID-19 was positively associated with the BMI of the mother and emotional eating (33).
In the present study, EE was a factor independently associated with CR, increasing the chance of individuals to show a higher CR score. A positive correlation between CR and EE was also previously observed in a cohort study (34), reporting that the CR impairment can leave the individual vulnerable to emotional eating and more reactive to sensory or cognitive exposure linked to food. The cognitively restricted individual imposes a set of dietary obligations and prohibitions to maintain or lose weight, but many of them, when exposed to certain situations, such as stress, tend to overeat (28). Restrained eaters may become hypervigilant to threat stimuli, accentuated by having to remember these during eating, at the expense of maintaining self-awareness or monitoring dietary concerns and goals (35).
In this study, individuals who practiced more physical activity and those who did not increase their alcohol dose intake showed 46.3 and 42.7% less probability of being CR scores above the third quartile, respectively. CR has been previously associated with higher cortisol levels which can activate the stress response (36). It is well-recognized that sustained exercise may influence basal cortisol levels (37) and might affect the response to stressors (38). Although, high restraint scores have been associated with more hours of weekly exercise (39), these findings have not been shown in the study. The relation between alcohol intake and CR has been reported previously, as restrained behaviors of individuals show disinhibition/impulsive episodes of food eating as the binge drinking ones (40). Hunt and Forbush (41) found that CR predicted the presence of alcohol misuse and drunkorexia in college students.
In contrast to what was expected from the pandemic, increased food intake was not associated with CR. Other factors such as female gender, graduation, reduced snacking, and increased frequency of homemade meals to the period before the pandemic increased the probability of individuals having higher CR scores. On the other hand, a higher frequency of ultra-processed food intake reduced the probability of higher CR scores. Regarding gender, studies have shown that many young women are motivated to both obtain and maintain their perceived ideal body shape (42). Furthermore, women who constantly monitor their bodies tend to put an extreme emphasis on outward appearance and weight and are also more likely to be motivated in adopting stressful behaviors to obtain a body that meets societal expectations (43).
In relation to PS, the multivariate model indicated that changes in the way of working or studying in relation to the period prior to the pandemic showed a 2.48 higher chance to produce PS scores above the third quartile. The results showed that most participants related changes in their way of work or study and increased time spent at work. During the pandemic, corporations and governments encouraged the practice of working from home to reduce exposure to COVID-19 (44). However, the responsibilities of people were amplified, including teleworking, doing domestic activities, minding their children, and facilitating homeschooling (44).
Sleep quality, younger age, and higher EE score were also factors independently associated with PS. Sleep deprivation is a common chronic stressor that may contribute to an increased risk of obesity and metabolic diseases (45). However, long-term studies that may assess the relationship between stress during the pandemic and the outcomes of chronic disorders have not yet been published. Additionally, the social isolation necessary to flatten the epidemic curve restricts young people from having physical contact with friends, causing increased feelings of loneliness, and stress (46). The relationship between stress and emotional eating has been discussed previously in this study.
PS showed a median of 22.9 (interquartile interval: 19.0–28.0) points. During the pandemic, other studies showed moderate (total mean scores between 14 and 26) or high- stress levels (total mean scores between 27 and 40) in most participants (32, 47). Considering these cutoff values, 88% of the volunteers showed moderate or high-stress levels, and 26.1%, high levels. COVID-19 is a stressor with great impact and unknown long-term implications, but may not be stressful or cause the same degree of stress for everyone (48).
The main limitation of this study is related to the lack of data about the eating behavior of participants and PS before the pandemic or the lack of a comparison group that has not been through isolation during the COVID-19 outbreak. Longitudinal studies are necessary to explain better the association of the pandemic between eating behavior and perceived stress. The studied sample may not be representative of the entire Brazilian population since the number of respondents was higher in the Southeast region and most participants were women. Also, other limitations may involve the self-reported data and the fact that only individuals who had access to a computer and were technically savvy may have taken this study. Despite these limitations, this research contributes to a better understanding of pandemic effects on eating behavior and stress.
We observed that many individuals experienced modification of their habits, manifested by reduced sleeping time, worsened sleep quality, increased frequency in consuming alcoholic beverages, reduced physical activity, and increased food intake. Working in the pandemic and increased food delivery were some of the factors associated with the eating behaviors. Perceived stress was associated with changes in the way of working or studying and by worse sleep quality.
Data Availability Statement
The datasets presented in this article are not readily available because the database is being used for other studies by the research group that has not yet been published. Requests to access the datasets should be directed to Ceres Mattos Della Lucia, Y21kZWxsYWx1Y2lhQHVmdi5jb20=.
Ethics Statement
The studies involving human participants were reviewed and approved by Research Ethics Committee of the Federal University of Viçosa, Minas Gerais, Brazil (Protocol number 35516720.5.0000.5153). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
JL, LA, LF, LO, and CD participated in the design of the project, analysis, and interpretation of the data. The orientation and critical review of the content were carried out by JL, LA, LF, and CD. All the authors were responsible for the final approval of the version to be published.
Funding
This work was supported by Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) Finance Code 001, and by Pró-Reitoria de Pesquisa (PRPq) Universidade Federal de Minas Gerais.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2021.704619/full#supplementary-material
References
1. WHO. WHO Coronavirus Disease (COVID-19) Dashboard. World Health Organization (2020). Available online at: https://covid19.who.int/ (accessed May 3, 2021).
2. Scarmozzino F, Visioli F. Covid-19 and the subsequent lockdown modified dietary habits of almost half the population in an Italian sample. Foods. (2020) 9:1–8. doi: 10.3390/foods9050675
3. Eftimov T, Popovski G, Petković M, Seljak BK, Kocev D. COVID-19 pandemic changes the food consumption patterns. Trends Food Sci Technol. (2020) 104:268–72. doi: 10.1016/j.tifs.2020.08.017
4. Hassen TB, El Bilali H, Allahyari MS, Berjan S, Fotina O. Food purchase and eating behavior during the COVID-19 pandemic: a cross-sectional survey of Russian adults. Appetite. (2021) 165:105309. doi: 10.1016/j.appet.2021.105309
5. Sidor A, Rzymski P. Dietary choices and habits during COVID-19 lockdown: experience from Poland. Nutrients. (2020) 12:1–13. doi: 10.3390/nu12061657
6. Wu P, Liu X, Fang Y, Fan B, Fuller CJ, Guan Z, et al. Alcohol abuse/dependence symptoms among hospital employees exposed to a SARS outbreak. Alcohol Alcohol. (2008) 43:706–12. doi: 10.1093/alcalc/agn073
7. Robinson E, Boyland E, Chisholm A, Harrold J, Maloney NG, Marty, L, et al. Obesity, eating behavior, and physical activity during COVID-19 lockdown: a study of UK adults. Appetite. (2021) 156:104853. doi: 10.1016/j.appet.2020.104853
8. Pellegrini M, Ponzo V, Rosato R, Scumaci E, Goitre I, Benso A, et al. Changes in weight and nutritional habits in adults with obesity during the “lockdown” period caused by the COVID-19 virus emergency. Nutrients. (2020) 12:2016. doi: 10.3390/nu12072016
9. Di Renzo L, Gualtieri P, Pivari F, Soldati L, Attinà, A, et al. Eating habits and lifestyle changes during COVID-19 lockdown: an Italian survey. J Transl Med. (2020) 18:229. doi: 10.1186/s12967-020-02399-5
10. Torres SJ, Nowson, CA. Relationship between stress, eating behavior, and obesity. Nutrition. (2007) 23:887–94. doi: 10.1016/j.nut.2007.08.008
11. Moynihan AB, van Tilburg WAP, Igou ER, Wisman A, Donnelly AE, Mulcaire JB. Eaten up by boredom: consuming food to escape awareness of the bored self. Front Psychol. (2015) 6:1–10. doi: 10.3389/fpsyg.2015.00369
12. Ammar A, Brach M, Trabelsi K, Chtourou H, Boukhris O, Masmoudi L, et al. Effects of COVID-19 home confinement on eating behaviour and physical activity: results of the ECLB-COVID19 international online survey. Nutrients. (2020) 12:1583. doi: 10.3390/nu12061583
13. Natacci LC, Ferreira Júnior M. The three factor eating questionnaire - R21: tradução para o português e aplicação em mulheres brasileiras. Rev Nutr. (2011) 24:383–94. doi: 10.1590/S1415-52732011000300002
14. Siqueira Reis R, Ferreira Hino AA, RomÉlio Rodriguez AÑez C. Perceived stress scale: reliability and validity study in Brazil. J Health Psychol. (2010) 15:107–14. doi: 10.1177/1359105309346343
15. Ministério da Saúde, Secretaria de Atenção à Saúde, Departamento de Atenção Básica. Protocolos do Sistema de Vigilância Alimentar e Nutricional – SISVAN na assistência à saúde. Brasília: Ministério da Saúde (2008).
16. Souza TCM, Oliveira LA, Daniel MM, Ferreira LG, Della Lucia CM, Liboredo JC, et al. Lifestyle and eating habits before and during COVID-19 quarantine in Brazil. Public Health Nutr. (2021) 10:1–29. doi: 10.1017/S136898002100255X
17. Konttinen H, Silventoinen K, Sarlio-Lähteenkorva S, Männistö S, Haukkala A. Emotional eating and physical activity self-efficacy as pathways in the association between depressive symptoms and adiposity indicators. Am J Clin Nutr. (2010) 92:1031–9. doi: 10.3945/ajcn.2010.29732
18. Lampuré A, Deglaire A, Schlich P, Castetbon K, Péneau S, Hercberg S, et al. Liking for fat is associated with sociodemographic, psychological, lifestyle and health characteristics. Br J Nutr. (2014) 112:1353–63. doi: 10.1017/S0007114514002050
19. Malta DC, Szwarcwald CL, Barros MB, Gomes CS, Machado ÍE, Souza Júnior PR, et al. A pandemia da COVID-19 e as mudanças no estilo de vida dos brasileiros adultos: um estudo transversal, 2020. Epidemiol Serv Saúde. (2020) 29:e2020407. doi: 10.1590/s1679-49742020000400026
20. Steele EM, Rauber F, Costa CD, Leite MA, Gabe KT, Louzada ML, et al. Mudanças alimentares na coorte NutriNet Brasil durante a pandemia de covid-19. Rev Saúde Pública. (2020) 4:54–91. doi: 10.11606/s1518-8787.2020054002950
21. Haddad C, Zakhour M, Bou Kheir M, Haddad R, Al Hachach M, Sacre H, et al. Association between eating behavior and quarantine/confinement stressors during the coronavirus disease 2019 outbreak. J Eat Disord. (2020) 8:1–12. doi: 10.1186/s40337-020-00317-0
22. de Medeiros ACQ, Yamamoto ME, Pedrosa LFC, Hutz CS. The Brazilian version of the three-factor eating questionnaire-R21: psychometric evaluation and scoring pattern. Eat Weight Disord. (2017) 22:169–75. doi: 10.1007/s40519-016-0256-x
23. Papandreou C, Arija V, Aretouli E, Tsilidis KK, Bulló M. Comparing eating behaviours, and symptoms of depression and anxiety between Spain and Greece during the COVID-19 outbreak: cross-sectional analysis of two different confinement strategies. Eur Eat Disord Rev. (2020) 28:836–46. doi: 10.1002/erv.2772
24. Elmacioglu F, Emiroglu E, Ülker MT, Özyilmaz Kircali B, Oruç S. Evaluation of nutritional behaviour related to COVID-19. Public Health Nutr. (2021) 24:512–8. doi: 10.1017/S1368980020004140
25. Sim MR. The COVID-19 pandemic: major risks to healthcare and other workers on the front line. Occupat Environ Med. (2020) 77:281–2. doi: 10.1136/oemed-2020-106567
26. Xiang YT, Yang Y, Li W, Zhang L, Zhang Q, Cheung T, et al. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry. (2020) 7:228–9. doi: 10.1016/S2215-0366(20)30046-8
27. Gilhooly CH, Das SK, Golden JK, McCrory MA, Dallal GE, Saltzman E, et al. Food cravings and energy regulation: the characteristics of craved foods and their relationship with eating behaviors and weight change during 6 months of dietary energy restriction. Int J Obes. (2007) 31:1849–58. doi: 10.1038/sj.ijo.0803672
28. Wallis DJ, Hetherington MM. Stress and eating: the effects of ego-threat and cognitive demand on food intake in restrained and emotional eaters. Appetite. (2004) 43:39–46. doi: 10.1016/j.appet.2004.02.001
29. Rutters F, Nieuwenhuizen AG, Lemmens SGT, Born JM, Westerterp-Plantenga MS. Acute stress-related changes in eating in the absence of hunger. Obesity. (2009) 17:72–7. doi: 10.1038/oby.2008.493
31. Penaforte FR, Matta NC, Japur CC. Associação entre estresse e comportamento alimentar em estudantes universitários. DEMETRA: Aliment Nutr Saúde. (2016) 11:225–38 doi: 10.12957/demetra.2016.18592
32. Shen W, Long LM, Shih CH, Ludy MJ. A humanities-based explanation for the effects of emotional eating and perceived stress on food choice motives during the COVID-19 pandemic. Nutrients. (2020) 12:2712. doi: 10.3390/nu12092712
33. Wang SD, Devjani S, Chillakanti M, Dunton GF, Mason TB. The COMET study: examining the effects of COVID-19-related perceived stress on Los Angeles Mothers' dysregulated eating behaviors, child feeding practices, and body mass index. Appetite. (2021) 163:105209. doi: 10.1016/j.appet.2021.105209
34. Provencher V, Drapeau V, Tremblay A, Després JP, Bouchard C, Lemieux S. Eating behaviours, dietary profile and body composition according to dieting history in men and women of the Québec Family Study. Br J Nutr. (2004) 91:997–1004. doi: 10.1079/BJN20041115
35. Lattimore P, Maxwell L. Cognitive load, stress, and disinhibited eating. Eat Behav. (2004) 5:315–24. doi: 10.1016/j.eatbeh.2004.04.009
36. McLean JA, Barr SI, Prior JC. Cognitive dietary restraint is associated with higher urinary cortisol excretion in healthy premenopausal women. Am J Clin Nutr. (2001) 73:7–12. doi: 10.1093/ajcn/73.1.7
37. Brundu B, Loucks TL, Adler LJ, Cameron JL, Berga SL. Increased cortisol in the cerebrospinal fluid of women with functional hypothalamic amenorrhea. J Clin Endocrinol Metabol. (2006) 91:1561–5. doi: 10.1210/jc.2005-2422
38. McComb JJR, Qian XP, Veldhuis JD, McGlone JJ, Norman RL. Neuroendocrine responses to psychological stress in eumenorrheic and oligomenorrheic women. Stress. (2006) 9:41–51. doi: 10.1080/10253890600591678
39. McLean JA, Barr SI. Cognitive dietary restraint is associated with eating behaviors, lifestyle practices, personality characteristics and menstrual irregularity in college women. Appetite. (2003) 40:185–92. doi: 10.1016/S0195-6663(02)00125-3
40. Hofmann W, Friese M. Impulses got the better of me: alcohol moderates the influence of implicit attitudes toward food cues on eating behavior. J Abnorm Psychol. (2008) 117:420–7. doi: 10.1037/0021-843X.117.2.420
41. Hunt TK, Forbush KT. Is “drunkorexia” an eating disorder, substance use disorder, or both? Eat Behav. (2016) 22:40–5. doi: 10.1016/j.eatbeh.2016.03.034
42. Sabiston C, Crocker PR, Munroe-Chandler K. Examining current-ideal discrepancy scores and exercise motivations as predictors of social physique anxiety in exercising females. J Sport Behav. (2005) 28:68.
43. Yao L, Niu G, Sun X, Duan C, Zheng Y. Selfie-posting on social networking sites, body surveillance, and exercise for weight control among Chinese young women with low body mass index. Psychol Sport Exerc. (2020) 51:101767. doi: 10.1016/j.psychsport.2020.101767
44. Bouziri H, Smith DRM, Smith DRM, Descatha A, Dab W, Jean K. Working from home in the time of COVID-19: how to best preserve occupational health? Occup Environ Med. (2020) 77:509–10. doi: 10.1136/oemed-2020-106599
45. Knutson KL, Van Cauter E. Associations between sleep loss and increased risk of obesity and diabetes. Ann N Y Acad Sci. (2008) 1129:287–304. doi: 10.1196/annals.1417.033
46. Sinton MM, Goldschmidt AB, Aspen V, Theim KR, Stein RI, Saelens BE, et al. Psychosocial correlates of shape and weight concerns in overweight pre-adolescents. J Youth Adolesc. (2012) 41:67–75. doi: 10.1007/s10964-011-9686-y
47. Mrklas K, Shalaby R, Hrabok M, Gusnowski A, Vuong W, Surood S, et al. Prevalence of perceived stress, anxiety, depression, and obsessive-compulsive symptoms in health care workers and other workers in Alberta during the COVID-19 pandemic: cross-sectional survey. JMIR Ment Health. (2020) 7:e22408. doi: 10.2196/22408
Keywords: feeding behavior, habits, pandemics, quarantine, life style, stress
Citation: Liboredo JC, Anastácio LR, Ferreira LG, Oliveira LA and Della Lucia CM (2021) Quarantine During COVID-19 Outbreak: Eating Behavior, Perceived Stress, and Their Independently Associated Factors in a Brazilian Sample. Front. Nutr. 8:704619. doi: 10.3389/fnut.2021.704619
Received: 03 May 2021; Accepted: 24 June 2021;
Published: 26 July 2021.
Edited by:
Igor Pravst, Institute of Nutrition (Slovenia), SloveniaReviewed by:
Jennifer L. Scheid, Daemen College, United StatesJeanette Mary Andrade, University of Florida, United States
Copyright © 2021 Liboredo, Anastácio, Ferreira, Oliveira and Della Lucia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ceres Mattos Della Lucia, Y21kZWxsYWx1Y2lhQHVmdi5icg==