Abstract
Background and Aims:
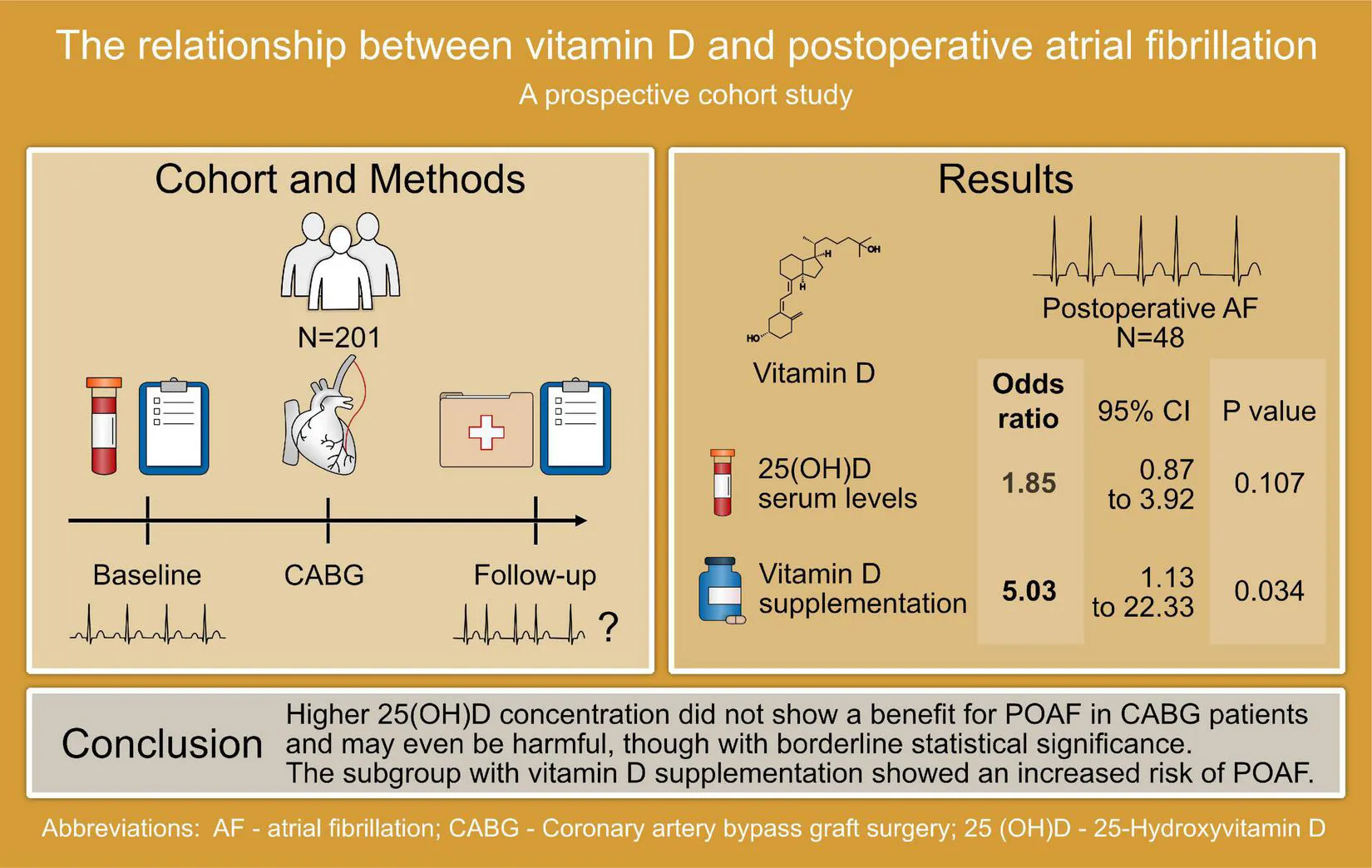
The relationship between postoperative atrial fibrillation (POAF) and 25-hydroxyvitamin D [25(OH)D] concentration as well as vitamin D supplementation has been discussed controversially. The relation of pre-operative vitamin D status and POAF remains unclear.
Methods and Results:
We analysed the risk of POAF in a prospective, observational cohort study of n = 201 patients undergoing coronary artery bypass graft surgery (CABG) with 25(OH)D concentration. The median age was 66.6 years, 15.4% were women. The median (25th/75th percentile) vitamin D concentration at baseline was 17.7 (12.6/23.7) ng/ml. During follow-up we observed 48 cases of POAF. In age, sex, and creatinine-adjusted analyses, 25(OH)D was associated with an increased risk of POAF, though with borderline statistical significance [odds ratio (OR) 1.85, 95% confidence interval (CI) 0.87–3.92, p-value 0.107], in further risk factor-adjusted analyses the results remained stable (OR 1.99, 95% CI 0.90–4.39, p-value 0.087). The subgroup with vitamin D supplementation at baseline showed an increased risk of POAF (OR 5.03, 95% CI 1.13–22.33, p-value 0.034).
Conclusion:
In our contemporary mid-European cohort, higher 25(OH)D concentration did not show a benefit for POAF in CABG patients and may even be harmful, though with borderline statistical significance. Our data are in line with a recent randomised study in community-based adults and call for further research to determine both, the clinical impact of elevated 25(OH)D concentration and vitamin D supplementation as well as the possible underlying pathophysiological mechanisms.
Introduction
Atrial fibrillation (AF) is a common and serious cardiac arrythmia, with a lifetime risk of 1 in 3 individuals of European ancestry (1, 2). A relevant increase in prevalence is expected due to a longer lifespan and increasing risk factors over the next decades (3, 4). AF is associated with an elevated risk of stroke, heart failure, dementia, and death (5–12). AF often occurs after surgery as postoperative atrial fibrillation (POAF), especially after thoracic and cardiac surgery with incidence rates reported between 20 and 40% for most cardiac surgeries and up to 60% for valve surgery (13–15). The mechanisms of surgery acting as a trigger of AF are not entirely understood. Electrolyte imbalances, inflammation and ischaemia are discussed as triggering factors. POAF increases the length of hospital stay, as well as short- and long-term risk of stroke, mortality and medical costs (16–18). Further, POAF increases the risk of long-term AF about 4–5-fold (17, 19). Understanding the pathophysiology behind the development of AF is key to risk prediction and for potential preventive efforts.
Vitamin D deficiency is a common condition in many societies and influenced, e.g., by geographical latitude and season. Vitamin D status is usually assessed by measuring circulating 25-hydroxyvitamin D [25(OH)D]. Its deficiency is known to be a major risk factor for musculoskeletal diseases; but has also been debated as a risk factor for many other conditions, such as immunologic, endocrine, or cardiovascular. The role of vitamin D and possible benefits of supplementation in AF development has been discussed controversially over the last decade. Whereas smaller, observational studies have shown an association between vitamin D deficiency and the occurrence of AF (20–23), larger cohort studies as well as randomized controlled trials (RCTs) assessing vitamin D supplementation could not confirm these results (24–29). In contrast, the latest RCT in adults in the community, VITAL (Vitamin D and Omega-3) Rhythm Trial, showed a marginally elevated AF risk, though these results did not reach statistical significance in the overall cohort (25).
Therefore, we aimed understand the relationship between circulating 25-hydroxyvitamin D [25(OH)D] and POAF in a cohort study of patients undergoing coronary artery bypass graft surgery (CABG). Further, we analysed the association of vitamin D supplementation and POAF risk.
Materials and Methods
Study Cohort
The Atrial Fibrillation in High-Risk Individuals - Biopsy (AFHRI-B) study is an ongoing, prospective, monocentre cohort study designed to improve POAF risk prediction. AFHRI-B is a sub-study of the clinical cohort study (CCS) conducted at the University Heart and Vascular Centre Hamburg (Germany). We included patients 18 years or older undergoing CABG with the support of a heart-lung machine. Individuals who did not have sufficient knowledge of the German language skills to understand the informed consent forms and to participate in the interview were excluded. We focused on AF not related to severe heart valve disease and thus excluded individuals with planned valve surgery or high-grade valvular disease. Participation in the study was voluntary. Written informed consent was obtained from all participants. The conduct of this study was approved by the Local Ethics Committee.
Data Collection
Baseline data was collected in form of an interview using a detailed questionnaire, including information on pre-existing conditions, medication, family history, lifestyle, and cardiovascular risk factors. Baseline information was supplemented by a review of the electronical medical record. Blood was taken from the patients before surgery and stored at -80°C. In order to collect postoperative data, questionnaires were mailed to the participants and a standardised telephone follow-up interview took place approximately 30 days after study inclusion. In this interview, changes in wellbeing and habits as well as newly diagnosed cardiovascular diseases, including AF, were recorded. For each study participant, all electrocardiograms available in the electronical medical record were analysed by two experienced investigators. In the case of discrepancies in the diagnosis of AF a third cardiologist or electrophysiologist was consulted. Further information on the course of the postoperative treatment were obtained from the discharge report, rehabilitation discharge letters and from the electronical medical record. The primary outcome was newly diagnosed, postoperative AF. 25(OH)D was measured from ethylenediaminetetraacetic acid plasma using the Abbott ARCHITECT i2000 system by a chemiluminescent microparticle immunoassay. After exclusion of 33 patients with AF diagnosed before surgery, n = 201 patients remained for our analysis.
Statistical Analyses
The statistical analyses were performed using R version 4.0.5 and there was no missing data in the sample. A p-value of < 0.05 was considered statistically significant. Levels of 25(OH)D as well as creatinine were log-transformed because visual inspection determined the transformed versions to be closer to a normal distribution. Logistic regression models with POAF as the outcome were fitted and corrected for small numbers in categorical predictors using Firth’s correction.
For the current analyses, clinical covariables besides age and sex comprised body mass index (BMI), ever smoker, diabetes, systolic and diastolic blood pressure, hypertension medication, heart failure, and myocardial infarction.
A secondary set of analyses also included the season (summer/winter) in which the blood sample was taken. Summer was defined as lasting from June 1st to November 30th. Vitamin D deficiency was defined as serum levels below 20 ng/ml. Lastly, vitamin D supplementation was included in another set of analyses.
Results
Baseline Characteristics
The baseline characteristics are given in Table 1. A total of N = 201 patients was included in the analysis. 31 (15.4%) of the included patients were female. The median age was 66.6 years. N = 48 patients (23.9%) of patients developed POAF during follow-up. POAF was persisting in 31 (64,6%) of the patients, whereas 17 (35,4%) of the patients had paroxysmal AF. The median (25th/75th percentile) vitamin D concentration was 17.7 (12.6/23.7) ng/ml, N = 140 (69.7%) of patients were enrolled in summer. Vitamin D deficiency occurred in 121 (60.2%) patients. A total of N = 8 patients (4.0%) took vitamin D supplementation at baseline.
TABLE 1
| Total Cohort N = 201 | Women N = 31 | Men N = 170 | No POAF N = 153 | POAF N = 48 | |
| Postoperative atrial fibrillation | |||||
| POAF No. (%) | 48 (23.9) | 8 (25.8) | 40 (23.5) | – | – |
| Persistent POAF No. (%) | 31 (64.6) | 6 (75.0) | 25 (62.5) | – | 31 (64.6) |
| Paroxysmal POAF No. (%) | 17 (35.4) | 2 (25.0) | 15 (37.5) | – | 17 (35.4) |
| Cardiovascular risk factors | |||||
| Age (years) | 66.6 (58.0, 73.1) | 68.1 (64.7, 75.5) | 65.4 (57.6, 72.7) | 64.1 (57.3, 72.9) | 69.6 (65.3, 74.9) |
| BMI (kg/m2) | 27.7 (24.7, 30.4) | 26.0 (23.8, 28.6) | 27.8 (24.8, 30.5) | 27.7 (24.5, 30.3) | 27.7 (25.4, 31.2) |
| Systolic blood pressure (mm Hg) | 133.0 (120.0, 145.0) | 135.0 (123.5, 143.0) | 133.0 (120.0, 145.0) | 133.0 (120.0, 145.0) | 130.5 (120.0, 145.2) |
| Diastolic blood pressure (mm Hg) | 77.0 (70.0, 82.0) | 75.0 (68.5, 83.0) | 77.0 (70.0, 82.0) | 78.0 (70.0, 82.0) | 73.0 (67.0, 81.5) |
| Hypertension medication No. (%) | 164 (81.6) | 28 (90.3) | 136 (80.0) | 125 (81.7) | 39 (81.2) |
| Ever-smoker No. (%) | 147 (73.1) | 21 (67.7) | 126 (74.1) | 111 (72.5) | 36 (75.0) |
| Pre-existing conditions | |||||
| Heart failure No. (%) | 37 (18.4) | 6 (19.4) | 31 (18.2) | 27 (17.6) | 10 (20.8) |
| Myocardial infarction No. (%) | 78 (38.8) | 10 (32.3) | 68 (40.0) | 61 (39.9) | 17 (35.4) |
| Diabetes No. (%) | 71 (35.3) | 10 (32.3) | 61 (35.9) | 53 (34.6) | 18 (37.5) |
| Vitamin D status | |||||
| Vitamin D (ng/ml) | 17.7 (12.6, 23.7) | 12.6 (10.8, 20.5) | 17.9 (13.2, 23.8) | 16.9 (12.6, 22.7) | 20.7 (13.1, 27.2) |
| Vitamin D deficiency (%) | 121 (60.2) | 22 (71.0) | 99 (58.2) | 98 (64.0) | 23 (47.9) |
| Vitamin D supplementation No. (%) | 8 (4.0) | 2 (6.5) | 6 (3.6) | 3 (2.0) | 5 (10.4) |
| Creatinine (mg/dl) | 0.8 (0.7, 1.0) | 0.8 (0.7, 0.8) | 0.8 (0.7, 1.0) | 0.8 (0.7, 1.0) | 0.8 (0.7, 0.9) |
| Vitamin D measurement in summer No. (%) | 140 (69.7) | 106 (69.3) | 34 (70.8) | 106 (69.3) | 34 (70.8) |
Baseline characteristics by sex and POAF.
For continuous variables the median, the 25th, and the 75th percentile are displayed.
1BMI, body mass index; POAF, postoperative atrial fibrillation.
Patients, who developed POAF were older, had higher vitamin D concentrations and took vitamin D supplementation more often. They also had higher rates of diabetes or heart failure and were more frequently current or former smokers.
Correlations Between Biomarkers and Covariates
We calculated the correlations between the biomarkers and covariates as shown in Figure 1. Continuous variables are shown as medians [interquartile range; binary variables are shown as counts (frequencies)].
FIGURE 1
The strongest correlations were observed between 25(OH)D concentration and vitamin D supplementation (r = 0.27). 25(OH)D concentration and measurement in summer showed a correlation of 0.22. Weak correlations between vitamin D and the following covariates were observed: creatinine, age, sex, ever smoking, diabetes.
Logistic Regressions
A first logistic regression model showed higher 25(OH)D concentration to be related to incident AF with borderline statistical significance [odds ratio (OR) 1.85, 95% confidence interval (CI) 0.87–3.92, p-value 0.107] when adjusted for age, sex, and creatinine. In analyses further adjusted for clinical variables the results remained stable (OR 1.99, 95% CI 0.90–4.39, p-value 0.087).
In a secondary analysis, vitamin D supplementation in a model adjusted for age and sex was associated with an increased risk (OR 5.03, 95% CI 1.13 to 22.33, p-value 0.034). The ORs and CIs of all models are compared in Figure 2.
FIGURE 2
Discussion
In our contemporary cohort we did not observe a benefit for higher 25(OH)D concentration or vitamin D supplementation in relation to POAF. In contrast, elevated 25(OH)D concentration showed an increased risk for the occurrence of POAF, though these results reached only borderline statistical significance. Vitamin D supplementation at baseline was significantly associated with an increased risk of POAF in this subgroup, however, the small size of this subgroup needs to be taken into consideration and these findings must thus be treated with caution.
The effects of vitamin D are pleiotropic and involve the modulation of the renin-angiotensin-aldosterone-system, inflammation, and vascular calcification among others (30–32). Cardiomyocytes express the vitamin D receptor. Alterations of this receptor have genomic effects and change contractility and relaxation of the heart (33, 34). Vitamin D affects K+- and Ca2+- currents in mouse ventricular myocytes (35, 36). Here, a link to the arrhythmia might be established. Another pathophysiological attempt of explanation focuses on the interaction between vitamin D and electrolytes, in particular calcium, but also phosphate and magnesium through parathyroid hormones. Electrolyte imbalance may be causal in the development of AF. It needs to be considered that most of the published literature describes pathophysiological findings for vitamin D deficiency, not for elevated concentration.
The role of 25(OH)D concentration across the whole range of blood concentration for the development of AF remains unclear. Small case-control studies have shown an association between low vitamin D serum levels and incident AF (20–23), whereas larger cohort studies could not confirm these results (26–29). Two recent, large, prospective, randomised, placebo-controlled studies could not show any benefit of vitamin D supplementation for the occurrence of AF (24, 25). In contrast, the VITAL Rhythm Study, a double-blind, randomised, placebo-controlled study, also showed a tendency for an increased AF risk associated with long-term 2,000 IU of vitamin D3 supplementation (25).
Similarly, even though vitamin D deficiency has been shown to be a risk factor for many cardiovascular conditions in multiple observational studies, in many areas large RCTs examining vitamin D supplementation could not demonstrate a convincing benefit of this intervention on hypertension (37), cardiovascular events (38), cardiovascular or all-cause mortality (39). It is possible, that vitamin D deficiency is not causal, but confounded by its association with lifestyle, cardiovascular risk factors, and comorbidities.
Our subgroup results in patients on vitamin D supplementation who showed an increased risk of POAF should be viewed cautiously and in the light of potential confounding-by-indication. These are observational findings. Patients undergoing major cardiac surgery such as CABG often are a particularly vulnerable and frail group which is not directly comparable to the general population. The median age in our cohort was 66.6 years. Many patients had significant comorbidities such as heart failure, prior myocardial infarction, or diabetes mellitus. The perioperative period is marked by physical and psychological stress as well as severe changes in the daily habits like reduced physical and mental activity (40). In addition, there can be alterations in nutrition caused by aspects such as decreased appetite or hospital diet with short-term effects on vitamin D concentrations (41–43). The pre-existing conditions that cause the prescription of vitamin D supplementation in the primary care setting might also increase the risk for AF. Furthermore, patients who take over the counter supplements may significantly differ in lifestyle. On the other hand, including recent evidence from RCTs an actual harmful effect of vitamin D on the development of AF should be considered. Thus, further research on the mechanisms of vitamin in AF is required.
Limitations
This study is limited by its observational nature which is prone to bias and confounding. The number of outcomes was relatively small, in particular the subgroup of patients with vitamin D supplementation was too small to derive final conclusions. Therefore, the results need to be interpreted with caution. Also, the examined objective was POAF, which in its pathophysiology, patient characteristics as well as clinical presentation is different from incident AF without preceding cardiac surgery. Thus, these results are not entirely transferrable to AF in the general population. However, our findings are in line with recent studies on vitamin D in AF in settings other than POAF. Therefore, further research is necessary to determine both, the clinical impact of 25(OH)D concentration and vitamin D supplementation as well as the potential underlying pathophysiological mechanisms to generate robust evidence on this central vitamin and frequently used supplement. Ideally, clinical trials of vitamin D supplementation could be set up.
Conclusion
In contrast to previous observational data, higher 25(OH)D concentration and vitamin D supplementation were not beneficial in relation to the risk of POAF in our study of patients undergoing CABG. Elevated 25(OH)D concentration and vitamin D supplementation rather revealed an increased OR for POAF. Whereas our data need confirmation, they also show the need for further research on the role of vitamin D and the serious and costly disease POAF.
Disclosure
RS has received lecture fees and advisory board fees from BMS/Pfizer outside this work.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Statements
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by the Ethikkommission Ärztekammer Hamburg. The patients/participants provided their written informed consent to participate in this study.
Author contributions
AO, JB, TZ, and RS: conceptualization. AO, JB, FO, and RS: methodology. JB and FO: formal analysis and writing—original draft preparation. VR, CB, SP, LC, and TZ: resources. VR and RS: data curation. JB, FO, SP, CB, LC, VR, SB, TZ, and RS: writing—review and editing. RS and FO: supervision. RS: project administration and funding acquisition. All authors contributed to the article and approved the submitted version.
Funding
RS has received funding from the European Research Council (ERC) under the European Union’s Horizon 2020 Research and Innovation Programme under the grant agreement No. 648131, from the European Union’s Horizon 2020 Research and Innovation Programme under the grant agreement No. 847770 (AFFECT-EU) and German Center for Cardiovascular Research (DZHK e.V.) (81Z1710103); German Ministry of Research and Education (BMBF 01ZX1408A) and ERACoSysMed3 (031L0239).
Acknowledgments
We thank all study participants for their generous participation in the AFHRI-B cohort.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Abbreviations
- AF
atrial fibrillation
- BMI
body mass index
- CABG
coronary artery bypass graft surgery
- CI
confidence interval
- EDTA
ethylenediaminetetraacetic acid
- OR
odds ratio
- POAF
postoperative atrial fibrillation
- RCT
randomised controlled trial
- 25(OH)D
25-hydroxyvitamin D.
References
1.
MagnussenCNiiranenTJOjedaFMGianfagnaFBlankenbergSNjølstadIet alSex differences and similarities in atrial fibrillation epidemiology, risk factors, and mortality in community cohorts: results from the biomarcare consortium (biomarker for cardiovascular risk assessment in europe).Circulation. (2017) 136:1588–97. 10.1161/circulationaha.117.028981
2.
StaerkLWangBPreisSRLarsonMGLubitzSAEllinorPTet alLifetime risk of atrial fibrillation according to optimal, borderline, or elevated levels of risk factors: cohort study based on longitudinal data from the Framingham Heart Study.BMJ. (2018) 2018:k1453. 10.1136/bmj.k1453
3.
ColillaSCrowAPetkunWSingerDESimonTLiuX. Estimates of Current and Future Incidence and Prevalence of Atrial Fibrillation in the U.S. Adult Population.Am J Cardiol. (2013) 112:1142–7. 10.1016/j.amjcard.2013.05.063
4.
KrijtheBPKunstABenjaminEJLipGYHFrancoOHHofmanAet alProjections on the number of individuals with atrial fibrillation in the European Union, from 2000 to 2060.Eur Heart J. (2013) 34:2746–51. 10.1093/eurheartj/eht280
5.
AnderssonTMagnusonABryngelssonI-LFrøbertOHenrikssonKMEdvardssonNet alAll-cause mortality in 272 186 patients hospitalized with incident atrial fibrillation 1995–2008: a Swedish nationwide long-term case–control study.Eur Heart J. (2013) 34:1061–7. 10.1093/eurheartj/ehs469
6.
De FerrariGMKlersyCFerreroPFantoniCSalerno-UriarteDMancaLet alAtrial fibrillation in heart failure patients: prevalence in daily practice and effect on the severity of symptoms. data from the alpha study registry.Eur J Heart Fail. (2007) 9:502–9. 10.1016/j.ejheart.2006.10.021
7.
KokkinidisDGZareifopoulosNTheochariCAArfaras-MelainisAPapanastasiouCAUppalDet alAssociation between atrial fibrillation and cognitive impairment in individuals with prior stroke: a meta-analysis and meta-regression analysis.Stroke. (2020) 51:1662–6. 10.1161/STROKEAHA.119.027815
8.
LipGYHLarocheCPopescuMIRasmussenLHVitali-SerdozLDanG-Aet alHeart failure in patients with atrial fibrillation in Europe: a report from the EURObservational research programme pilot survey on atrial fibrillation: heart failure in patients with AF in Europe.Eur J Heart Fail. (2015) 17:570–82. 10.1002/ejhf.254
9.
PistoiaFSaccoSTiseoCDeganDOrnelloRCaroleiA. The epidemiology of atrial fibrillation and stroke.Cardioembolic Stroke. (2016) 34:255–68. 10.1016/j.ccl.2015.12.002
10.
PokorneySDPicciniJPStevensSRPatelMRPieperKSHalperinJLet alCause of death and predictors of all-cause mortality in anticoagulated patients with nonvalvular atrial fibrillation: data from ROCKET AF.J Am Heart Assoc. (2021) 2021:2197. 10.1161/JAHA.115.002197
11.
VermondRAGeelhoedBVerweijNTielemanRGVan der HarstPHillegeHLet alIncidence of atrial fibrillation and relationship with cardiovascular events, heart failure, and mortality.J Am Coll Cardiol. (2015) 66:1000–7. 10.1016/j.jacc.2015.06.1314
12.
WolfPAAbbottRDKannelWB. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study.Stroke. (1991) 22:983–8. 10.1161/01.str.22.8.983
13.
BessissowAKhanJDevereauxPJAlvarez-GarciaJAlonso-CoelloP. Postoperative atrial fibrillation in non-cardiac and cardiac surgery: an overview.J Thromb Haemost. (2015) 13:S304–12. 10.1111/jth.12974
14.
DobrevDAguilarMHeijmanJGuichardJ-BNattelS. Postoperative atrial fibrillation: mechanisms, manifestations and management.Nat Rev Cardiol. (2019) 16:417–36. 10.1038/s41569-019-0166-5
15.
YadavaMHugheyABCrawfordTC. Postoperative atrial fibrillation: incidence, mechanisms, and clinical correlates.Atr Fibrillation. (2016) 12:299–308.
16.
BhavePDGoldmanLEVittinghoffEMaselliJAuerbachA. Incidence, predictors, and outcomes associated with postoperative atrial fibrillation after major noncardiac surgery.Am Heart J. (2012) 164:918–24. 10.1016/j.ahj.2012.09.004
17.
LeeS-HKangDRUhmJ-SShimJSungJ-HKimJ-Yet alNew-onset atrial fibrillation predicts long-term newly developed atrial fibrillation after coronary artery bypass graft.Am Heart J. (2014) 167:593.e–600.e. 10.1016/j.ahj.2013.12.010
18.
LinM-HKamelHSingerDEWuY-LLeeMOvbiageleB. Perioperative/postoperative atrial fibrillation and risk of subsequent stroke and/or mortality: a meta-analysis.Stroke. (2019) 50:1364–71. 10.1161/strokeaha.118.023921
19.
KonstantinoYYovelDZFrigerMDSaharGKnyazerBAmitG. Postoperative atrial fibrillation following coronary artery bypass graft surgery predicts long-term atrial fibrillation and stroke. (2016) 18:5.
20.
BelenEAykanAKalayESungurMSungurACetinM. Low-level vitamin d is associated with atrial fibrillation in patients with chronic heart failure.Adv Clin Exp Med. (2016) 25:51–7. 10.17219/acem/34690
21.
ChenWRLiuZYShiYYinDWWangHShaYet alRelation of low vitamin D to nonvalvular persistent atrial fibrillation in chinese patients: vitamin D and atrial fibrillation.Ann Noninvasive Electrocardiol. (2014) 19:166–73. 10.1111/anec.12105
22.
OzcanOUGurlekAGursoyEGeredeDMErolC. Relation of vitamin D deficiency and new–onset atrial fibrillation among hypertensive patients.J Am Soc Hypertens. (2015) 9:307–12. 10.1016/j.jash.2015.01.009
23.
DemirMUyanUMelekM. The effects of vitamin D deficiency on atrial fibrillation.Clin Appl Thromb. (2014) 20:98–103. 10.1177/1076029612453762
24.
BoursiquotBCLarsonJCShalashOAVitolinsMZSolimanEZPerezMV. Vitamin D with calcium supplementation and risk of atrial fibrillation in postmenopausal women.Am Heart J. (2019) 209:68–78. 10.1016/j.ahj.2018.12.006
25.
AlbertCMCookNRPesterJMoorthyMVRidgeCDanikJSet alEffect of Marine Omega-3 Fatty Acid and Vitamin D Supplementation on Incident Atrial Fibrillation: A Randomized Clinical Trial.JAMA. (2021) 325:1061. 10.1001/jama.2021.1489
26.
VitezovaACartolanoNSHeeringaJZillikensMCHofmanAFrancoOHet alVitamin D and the Risk of Atrial Fibrillation - The Rotterdam Study.PLoS One. (2015) 10:e0125161. 10.1371/journal.pone.0125161
27.
AlonsoAMisialekJRMichosEckfeldtJSelvinESolimanEZet alSerum 25-hydroxyvitamin D and the incidence of atrial fibrillation: the Atherosclerosis Risk in Communities (ARIC) study.Europace. (2016) 18:1143–9. 10.1093/europace/euv395
28.
RienstraMChengSLarsonMGMcCabeELBoothSLJacquesPFet alVitamin D status is not related to development of atrial fibrillation in the community.Am Heart J. (2011) 162:538–41. 10.1016/j.ahj.2011.06.013
29.
TrevisanCPiovesanFLucatoPZanforliniBMDe RuiMMaggiSet alParathormone, vitamin D and the risk of atrial fibrillation in older adults: A prospective study.Nutr Metab Cardiovasc Dis. (2019) 29:939–45. 10.1016/j.numecd.2019.05.064
30.
CantornaMTSnyderLLinY-DYangL. Vitamin D and 1,25(OH)2D Regulation of T cells.Nutrients. (2015) 7:3011–21. 10.3390/nu7043011
31.
FormanJPWilliamsJSFisherNDL. Plasma 25-Hydroxyvitamin D and Regulation of the Renin-Angiotensin System in Humans.Hypertension. (2010) 55:1283–8. 10.1161/HYPERTENSIONAHA.109.148619
32.
TurinABaxJJDoukasDJoyceCLopezJJMathewVet alInteractions Among Vitamin D, Atrial Fibrillation, and the Renin-Angiotensin-Aldosterone System.Am J Cardiol. (2018) 122:780–4. 10.1016/j.amjcard.2018.05.013
33.
TishkoffDXNibbelinkKAHolmbergKHDanduLSimpsonRU. Functional Vitamin D Receptor (VDR) in the T-Tubules of Cardiac Myocytes: VDR Knockout Cardiomyocyte Contractility.Endocrinology. (2008) 149:558–64. 10.1210/en.2007-0805
34.
MenegazDMizwickiMTBarrientos-DuranAChenNHenryHLNormanAW. Vitamin D Receptor (VDR) Regulation of Voltage-Gated Chloride Channels by Ligands Preferring a VDR-Alternative Pocket (VDR-AP).Mol Endocrinol. (2011) 25:1289–300. 10.1210/me.2010-0442
35.
TamayoMManzanaresEBasMMartín-NunesLVal-BlascoAJesús LarribaMet alCalcitriol (1,25-dihydroxyvitamin D3) increases L-type calcium current via protein kinase A signaling and modulates calcium cycling and contractility in isolated mouse ventricular myocytes.Heart Rhythm. (2017) 14:432–9. 10.1016/j.hrthm.2016.12.013
36.
TamayoMMartin-NunesLVal-BlascoAPiedrasMJLarribaMJGómez-HurtadoNet alCalcitriol, the Bioactive Metabolite of Vitamin D, Increases Ventricular K+ Currents in Isolated Mouse Cardiomyocytes.Front Physiol. (2018) 9:1186. 10.3389/fphys.2018.01186
37.
ZhangDChengCWangYSunHYuSXueYet alEffect of Vitamin D on Blood Pressure and Hypertension in the General Population: An Update Meta-Analysis of Cohort Studies and Randomized Controlled Trials.Prev Chronic Dis. (2020) 17:190307. 10.5888/pcd17.190307
38.
BarbarawiMKheiriBZayedYBarbarawiODhillonHSwaidBet alVitamin D Supplementation and Cardiovascular Disease Risks in More Than 83 000 Individuals in 21 Randomized Clinical Trials: A Meta-analysis.JAMA Cardiol. (2019) 4:765. 10.1001/jamacardio.2019.1870
39.
ZhangYFangFTangJJiaLFengYXuPet alAssociation between vitamin D supplementation and mortality: systematic review and meta-analysis.BMJ. (2019) 2019:l4673. 10.1136/bmj.l4673
40.
LopezVSek YingCPoonC-YWaiY. Physical, psychological and social recovery patterns after coronary artery bypass graft surgery: A prospective repeated measures questionnaire survey.Int J Nurs Stud. (2007) 44:1304–15. 10.1016/j.ijnurstu.2006.06.005
41.
CasaerMPVan den BergheG. Nutrition in the acute phase of critical illness.N Engl J Med. (2014) 370:1227–36. 10.1056/nejmra1304623
42.
BartonABeiggCMacdonaldIAllisonS. High food wastage and low nutritional intakes in hospital patients.Clin Nutr. (2000) 19:445–9. 10.1054/clnu.2000.0150
43.
PathiranaAKLokunarangodaNRanathungaISantharajWSEkanayakeRJayawardenaR. Prevalence of hospital malnutrition among cardiac patients: results from six nutrition screening tools.SpringerPlus. (2014) 3:412–412. 10.1186/2193-1801-3-412
Summary
Keywords
atrial fibrillation, postoperative atrial fibrillation, vitamin D, vitamin D supplementation, 25-hydroxyvitamin D
Citation
Ohlrogge AH, Brederecke J, Ojeda FM, Pecha S, Börschel CS, Conradi L, Rimkus V, Blankenberg S, Zeller T and Schnabel RB (2022) The Relationship Between Vitamin D and Postoperative Atrial Fibrillation: A Prospective Cohort Study. Front. Nutr. 9:851005. doi: 10.3389/fnut.2022.851005
Received
08 January 2022
Accepted
05 April 2022
Published
10 May 2022
Volume
9 - 2022
Edited by
Gaetano Santulli, Albert Einstein College of Medicine, United States
Reviewed by
Telmo Pereira, Politécnico de Coimbra, ESTESC, Fisiologia Clínica, Portugal; Pasquale Mone, University of Campania Luigi Vanvitelli, Italy
Updates
Copyright
© 2022 Ohlrogge, Brederecke, Ojeda, Pecha, Börschel, Conradi, Rimkus, Blankenberg, Zeller and Schnabel.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Renate B. Schnabel, r.schnabel@uke.de
This article was submitted to Clinical Nutrition, a section of the journal Frontiers in Nutrition
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.