 Eszter Laczkó-Zöld1*†
Eszter Laczkó-Zöld1*† Boglárka Csupor-Löffler2†
Boglárka Csupor-Löffler2† Edina-Blanka Kolcsár1†
Edina-Blanka Kolcsár1† Tamás Ferenci3,4Monica Nan5Barbara Tóth6
Tamás Ferenci3,4Monica Nan5Barbara Tóth6 Dezső Csupor2,6,7
Dezső Csupor2,6,7- 1Department of Pharmacognosy and Phytotherapy, "George Emil Palade" University of Medicine, Pharmacy, Sciences, and Technology of Târgu Mureş, Târgu Mureş, Romania
- 2Institute for Translational Medicine, Szentágothai Research Centre, Medical School, University of Pécs, Pécs, Hungary
- 3Physiological Controls Research Center, Óbuda University, Budapest, Hungary
- 4Department of Statistics, Corvinus University of Budapest, Budapest, Hungary
- 5Pharmacy Department, Encompass Health Rehabilitation Hospital of Round Rock, Round Rock, TX, United States
- 6Institute of Clinical Pharmacy, University of Szeged, Szeged, Hungary
- 7Institute of Pharmacognosy, University of Szeged, Szeged, Hungary
Several studies have shown that Momordica charantia L. (Cucurbitaceae, bitter melon) has beneficial effects on metabolic syndrome (MetS) parameters and exerts antidiabetic, anti-hyperlipidemic, and anti-obesity activities. Since the findings of these studies are contradictory, the goal of this systematic review and meta-analysis was to assess the efficacy of bitter melon in the treatment of metabolic syndrome, with special emphasis on the anti-diabetic effect. Embase, Cochrane, PubMed, and Web of Science databases were searched for randomized controlled human trials (RCTs). The meta-analysis was reported according to the PRISMA statement. The primary outcomes of the review are body weight, BMI, fasting blood glucose, glycated hemoglobin A1c, systolic blood pressure, diastolic blood pressure, serum triglyceride, HDL, LDL, and total cholesterol levels. Nine studies were included in the meta-analysis with 414 patients in total and 4–16 weeks of follow-up. In case of the meta-analysis of change scores, no significant effect could be observed for bitter melon treatment over placebo on fasting blood glucose level (MD = −0.03; 95% CI: −0.38 to 0.31; I2 = 34%), HbA1c level (MD = −0.12; 95% CI: −0.35 to 0.11; I2 = 56%), HDL (MD = −0.04; 95% CI: −0.17 to 0.09; I2 = 66%), LDL (MD = −0.10; 95% CI: −0.28 to 0.08; I2 = 37%), total cholesterol (MD = −0.04; 95% CI: −0.17 to 0.09; I2 = 66%,), body weight (MD = −1.00; 95% CI: −2.59–0.59; I2 = 97%), BMI (MD = −0.42; 95% CI: −0.99–0.14; I2 = 95%), systolic blood pressure (MD = 1.01; 95% CI: −1.07–3.09; I2 = 0%) and diastolic blood pressure levels (MD = 0.24; 95% CI: −1.04–1.53; I2 = 0%). Momordica treatment was not associated with a notable change in ALT, AST, and creatinine levels compared to the placebo, which supports the safety of this plant. However, the power was overall low and the meta-analyzed studies were also too short to reliably detect long-term metabolic effects. This highlights the need for additional research into this plant in carefully planned clinical trials of longer duration.
1 Introduction
Metabolic syndrome (MetS) has been defined as a complex group of risk factors for cardiovascular disease and diabetes. These factors include elevated blood pressure (systolic blood pressure ≥ 130 mm Hg, diastolic blood pressure ≥ 85 mmHg), elevated triglyceride levels (TG; ≥150 mg/dL), low high-density lipoprotein cholesterol levels (HDL-C; male <40 mg/dL, female <50 mg/dL), hyperglycemia (fasting blood glucose ≥100 mg/dL), and obesity (waist circumference: male ≥94 cm, female ≥80 cm) (1, 2). It has been reported that approximately 30% of the world population is affected by MetS, making it a major global health challenge, and an important cause of mortality and morbidity (3, 4). The treatment of MetS is based on an improvement of lifestyle, promoting physical activity, and a balanced low-energy diet (2). Some medicinal plants may be useful tools in the treatment of several MetS components before beginning pharmacological therapy or to supplement medical treatment (2, 5).
Diabetes is one of the most common metabolic diseases and its prevalence is increasing steadily worldwide. According to International Diabetes Federation (IDF) data published in 2021, over 530 million adults are living with diabetes worldwide, and by 2045 their number will exceed 783 million (6). Direct complications from diabetes can lead to heart attack, stroke, blindness, kidney failure, and lower limb amputation (7). Many plants used in folk medicine were involved in clinical trials for assessing their potential as antidiabetic agents and for their positive effect on the treatment or prevention of MetS (2, 8–11). Among these are Aloe vera (L.) Burm.f. (10, 11), Capparis spinosa L. (12), Cinnamomum cassia and C. zeylanicum (13, 14), Trigonella foenum-graecum (15), Coffea arabica, Theobroma cacao (16), Allium sativum (2), Gymnema sylvestre (17, 18), Curcuma longa (19, 20), Thea sinensis (21), Ilex paraguariensis (22) and Momordica charantia (23).
Momordica charantia L. (Cucurbitaceae, bitter gourd or bitter melon) is a tropical and subtropical vine, the edible fruits, shoots, and leaves of which are widely used in the East Asian, South Asian, and Southeast Asian cuisines. Various parts of the plant, especially the fruits, are used in folk medicine in Asia and Africa. The medicinal use of the plant is preponderant in the treatment of diabetes. Various preclinical and clinical studies conducted so far showed the protective effects of M. charantia against metabolic syndrome and its associated disorders. The bitter gourd extracts were evaluated for numerous pharmacological activities, and most of them were performed on animals. Fruits and seed extracts reduced fasting glucose and glycosylated hemoglobin A1c in comparison to vehicle control when tested in animal models of type 2 diabetes (24). The water extract of leaves proved to have an anti-obesity effect on a high-fat diet (HFD)-induced obese mouse model through regulating lipid metabolism (25). Hypoglycemic and hypolipidemic effects of different fruit parts were tested on normal, hyperglycemic, and hyperlipidemic rats (26, 27).
The mechanism of action of M. charantia has not been fully elucidated. Charantin, a steroidal saponin mixture isolated from the plant is its main active constituent. Charantin has been shown to have insulin-like activity by augmenting insulin release, reducing gluconeogenesis, increasing hepatic glycogen synthesis, and increasing peripheral glucose oxidation (28). Antidiabetic activity could be confirmed for charantin, but not for steroidal saponin aglycones (29). The charantin-rich fraction of M.charantia reduced blood sugar levels in type 1 and type 2 diabetic animal models (30, 31). The treatment with the M. charantia extracts decreased plasma insulin and increased insulin sensitivity by increasing the expression of GLUT4 in the skeletal muscle and of IRS-1 in the liver of mice with type 2 diabetes. However, no effect on insulin sensitivity was detected in mice with type 2 diabetes (28).
Certain clinical trials suggested that bitter melon products may be promising phytomedicines to manage hyperglycemia (32, 33), ameliorating systemic complications of type 2 diabetes (33), including associated cardiovascular risk factors (34) and it can be considered in obesity management too (35, 36). In the last five years, numerous review articles have been published about bitter melon chemical compounds (37, 38), nutritional value (39, 40), and pharmacological actions (36, 41–43), but only a few are with meta-analysis. Jandari et al. performed a systematic review and meta-analysis of randomized clinical trials regarding the effect of bitter melon on blood pressure (44), Cortez-Navarrete et al. reviewed the metabolic effects of bitter melon reported in clinical trials (45), but without performing a meta-analysis, while Peter et al. evaluated the efficacy in lowering the elevated plasma glucose level in diabetes mellitus (46). The present systematic review and meta-analysis aimed to evaluate the effect of bitter melon on metabolic syndrome parameters.
2 Methods
2.1 Population, intervention, comparison, outcomes, and study design
The following PICO (patients, intervention, comparison, outcome) format was applied: P: patients in prediabetes or diagnosed with type 2 diabetes; I: Momordica; C: placebo; and O: change in metabolic parameters. We used PRISMA statement (47) to report the meta-analysis results.
2.2 Systematic review protocol
This systematic review and meta-analysis were registered in the International Prospective Register of Systematic Reviews (PROSPERO) a priori (ID: CRD42021293139).
2.3 Search strategy and data sources
We systematically searched PubMed/MEDLINE, Embase, Cochrane, and Web of Science databases for articles reporting randomized, parallel-group, placebo-controlled clinical trials up to October 31, 2023, without limiting the language or publication year. The following main keywords and related terms were used: “momordica” AND “diabetes.” For transparency purposes this meta-analysis relied on publicly available data. There was no need to contact the authors of the articles nor the manufacturers of the products under consideration for any additional information. We removed duplicate and records lacking an abstract and the final selection was based on article titles and abstracts. Two reviewers (EBK, BCL) independently reviewed the full texts of the remaining records. Any disagreement among reviewers was discussed and resolved, a third reviewer was available for consultation at any time (DC). We used Mendeley (version 1.19.8; Mendeley Ltd.) to manage references.
2.4 Study selection
Only randomized, placebo-controlled studies with adult prediabetes or with a type 2 diabetes mellitus diagnosis were included in the meta-analysis. A minimal follow-up duration of 4 weeks was determined as an inclusion criterion since this is the minimum period required for meaningful effects on glucose control as assessed by HbA1c concentration (48). Case series, case reports, non-randomized and open-label studies, and trials performed with patients with concomitant diseases affecting blood glucose levels or in which the intervention contained other active ingredients than M. charantia were not considered for analysis.
2.5 Data extraction
Data collection was executed following the PRISMA guidelines. The two independent reviewers (EBK, DC) extracted study characteristics and results. Any discrepancies in the extracted data were discussed and resolved. The following data items were selected from the included papers: study design, sample size and characteristics of the patient population, duration, intervention details, body weight, BMI, waist circumference, body fat, systolic and diastolic blood pressure, HbA1c, fasting glucose, total cholesterol, triglyceride, HDL, LDL, VLDL, creatinine, ALT, and AST levels. A statistical analysis of at least three clinical trials involving different patient populations was required for each outcome.
2.6 Statistical analysis
Papers included in this meta-analysis reported data in three ways:
A. a pre-intervention value and a change score,
B. a pre- and post-intervention value,
C. a pre- and post-intervention value along with a change score.
Two distinct types of analysis were undertaken:
• Analysis of post-intervention values only (without using baseline or change information); this is unbiased in the case of randomized controlled trials, but is inefficient, however, the loss of efficiency is marginal if the correlation between the pre- and post-intervention values is less than 0.5 (49).
• Analysis of change scores; this is more efficient, especially if the correlation between the pre- and post-intervention values is higher than 0.5.
The first analysis requires the imputation of the post-intervention value in scenario A, the second requires the imputation of the change score in scenario B (no value must be imputed in all other combinations). Both imputation task requires the knowledge of correlation between the pre- and post-intervention values, this was obtained from studies of type C, i.e., studies with all data given were used to calculate the correlation which was then used to impute studies with partial information. The correlation coefficient was calculated as the sum of the variances of pre- and post-intervention values minus the variance of the change divided by two times the product of the standard deviation of the pre- and post-intervention values (50, 51). This was calculated separately for all studies, arms (i.e., placebo or active), and outcomes, and were then averaged across studies, i.e., an average was calculated for each outcome and arm after discarding impossible values (i.e., a correlation larger than 1 in absolute value). This average was used for imputation only if the range of the correlations for the given outcome and arm was less than 0.4, otherwise that outcome and arm’s correlation was not imputed. After the value used for imputation was obtained, the post-intervention values were imputed using scenario A, and the change scores were imputed for scenario B.
Both types of meta-analysis (post-intervention and change score) were then run using the imputed datasets. The outcome measure was the mean difference. In case when median and lower/upper quartile was given, mean and standard deviation was estimated with the quantile estimation method of McGrath et al. (52). Common-effect meta-analysis, and random-effects meta-analysis (with restricted maximum likelihood estimation) was carried out (53).
Results are presented using standard forest plots, depicting both common- and random-effects results, together with the usual τ2 and I2 heterogeneity statistics and a test for the overall effect (both for the random-effects results).
Calculations were conducted under R statistical environment version 4.2.1 (54) using package metafor version 3.8–1 (55). Full source code is available at https://github.com/tamas-ferenci/MomordicaMetaAnalysis.
2.7 Risk of bias analysis
The Cochrane Collaboration tool was used to assess the risk of bias, which includes seven specific domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other bias scores. Studies were classified as having a high (red), unclear (yellow), or low (green) risk of bias in each domain. Disagreements about the quality of the studies were settled through discussion (TF, DC). The risk of bias summary table and figure were generated by the RevMan 5 software (56).
2.8 Ethics statement
Ethical approval was not needed because we only collect non-confidential information from which the patients’ identities cannot be determined.
3 Results
3.1 Search results
The search resulted in 694 hits, after removing the duplicates 519 records remained and were potentially eligible for inclusion. In the full-text section stage, most articles were excluded due to the lack of placebo control (57, 58), lack of blinding (59), lack of numerically reported results (32, 60, 61), and since other plant parts (leaves) than M. charantia fruits were used as study (59, 62–65). We identified nine trials eligible for our review and meta-analysis (33, 66–73). The selection process is presented in Figure 1 (47).
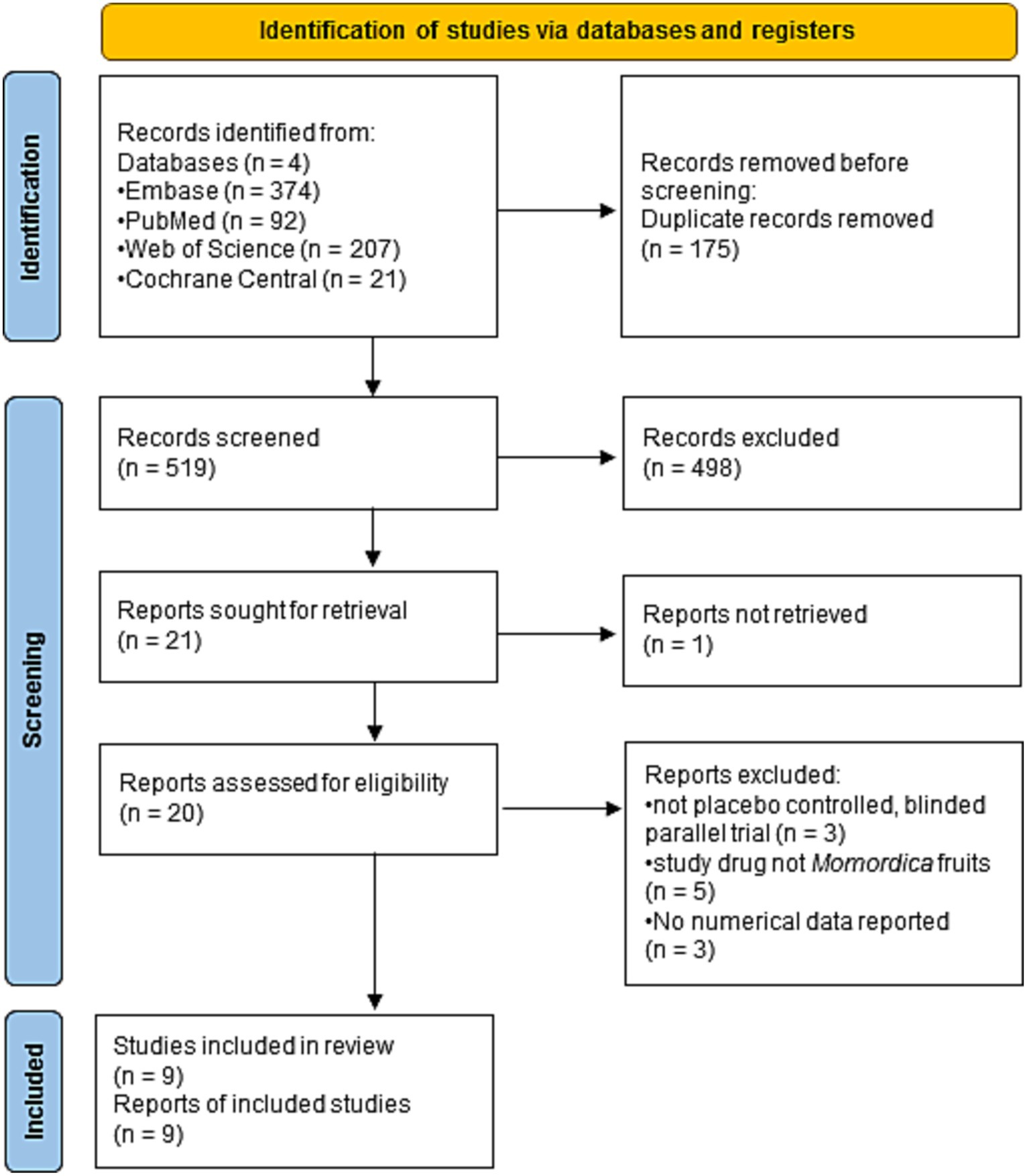
Figure 1. Flow diagram of study identification and selection by PRISMA 2020.
3.2 Study characteristics
We analyzed nine randomized placebo-controlled trials (33, 66–73). Table 1 contains the summary of the main study and patient characteristics. We included only randomized double or single-blinded studies released between 2003 and 2023. Studies length varied between 4 and 16 weeks, the sample size was low (24–90 participants), the study drugs were inconsistent in quality (dry plant material and dry extracts) and in quantity (the daily dose was 2–6 g fruit or extract of fruit equivalent to 9 g fruit). The total number of participants was 414 and the locations of the studies were different Asian or North American countries. The minimum age of participants was 18 years (67) or 20 years (33), and the oldest patient was 80 years old (71), according to the available information.
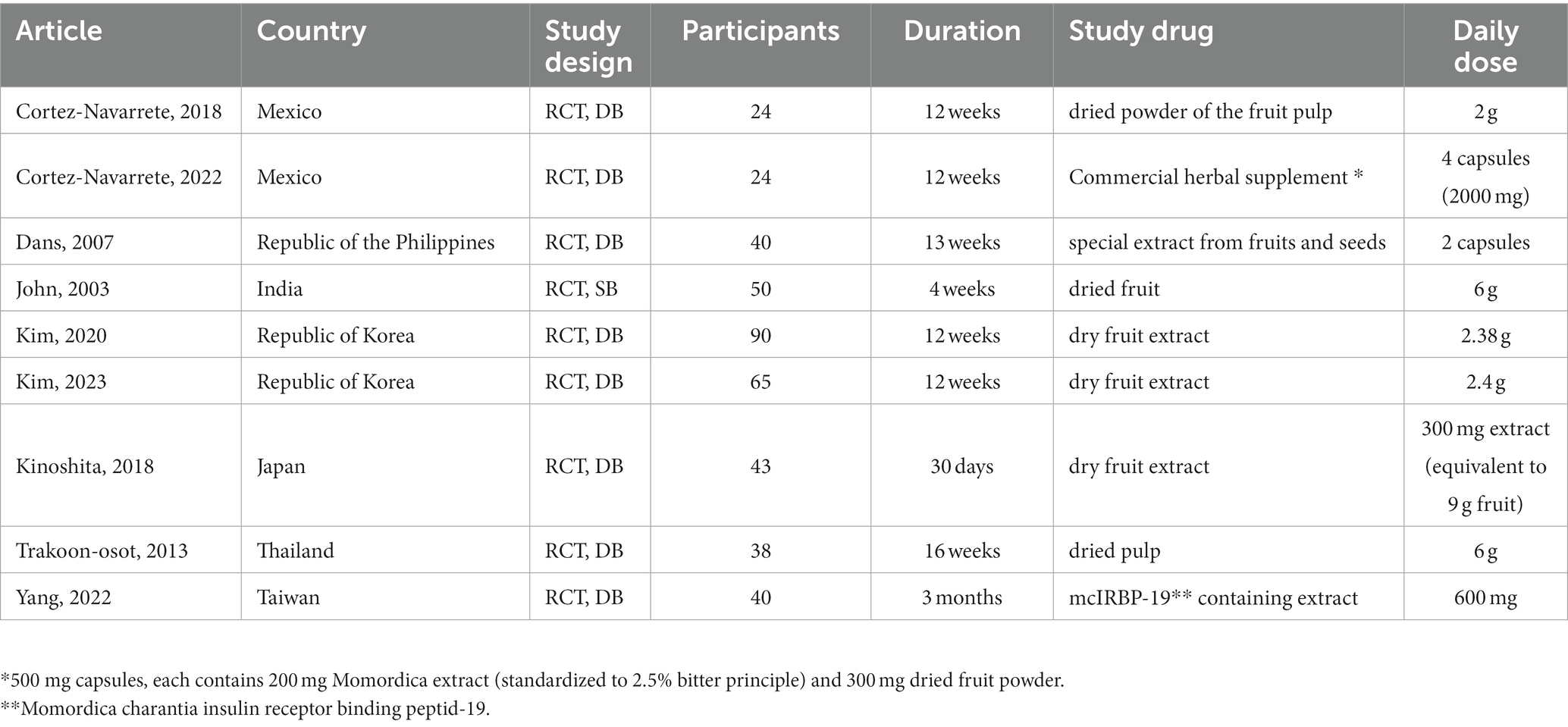
Table 1. Baseline characteristics of studies included in the meta-analysis (RCT: randomized, controlled trial; DB: double blind; SB: single-blind).
3.3 Risk of bias assessment
Overall, the methodical quality of the trials included in our final quantitative analysis was reckoned to be good, only with low or unclear risk of bias for double-blind randomized trials (Supplementary Figures S1, S2).
Random sequence generation was described in six studies (33, 67–70, 72); however, the measures taken to ensure allocation concealment were given in only one trial (67). Performance and detection biases were unclear in five studies (33, 68–71) because the authors of these studies failed to report whether the intervention and the comparator were identical in size, shape, color, and odor; and it remained unclear whether the outcomes were assessed in a blinded manner or not. The study of Cortez-Navarrante (72) was judged to have low risk of performance and detection biases, because based on their article nor the patients neither the investigators were aware of the assigned treatment. Dans et al. stated that the treatment and the placebo capsules were identical, and the patients, the investigators, and the statistician were unaware of the treatments received until the end of the statistical analysis. Therefore, this study had low risk of performance and detection biases (67). However, in the study of John et al. (66) the investigators were not blinded and the tablets were dissimilar; therefore, this study had high risk of performance and detection biases.
All the included studies showed a minimal risk of attrition and reporting biases. The study of Dans et al. was funded by a company, but the authors stated that the sponsor had had no role in the data collection or the analysis of the study; therefore, the risk of other bias in this study remained low (67). However, in the study of John et al., the investigators were not blinded, and the tablets were dissimilar; therefore, this study had a substantial risk of performance bias (66).
3.4 Main findings
3.4.1 Effect of Momordica charantia fruits on glycemic indices
One primary outcome was fasting blood glucose level and relevant data were available from eight trials (Figure 2). Using the random effects model, the superiority of M. charantia over placebo on fasting blood glucose level could not be observed (MD = −0.03; 95% CI: −0.38 to 0.31; I2 = 34%) with the analysis of change scores (Figure 2A). This finding was consistent when analyzing the data with the common-effect model. However, the assessment of the post-intervention suggests that M. charantia is more effective than placebo in decreasing fasting blood glucose levels (MD = −0.40; 95% CI: −0.76 to −0.03; I2 = 0%) (Figure 2B). The primary reason of this contradiction is that the first analysis was based on 4 trials only (143 participants), whereas post-intervention values were available in 7 trials (296 participants) and missing values could not be imputed, because the calculated correlations were unacceptably dissimilar.
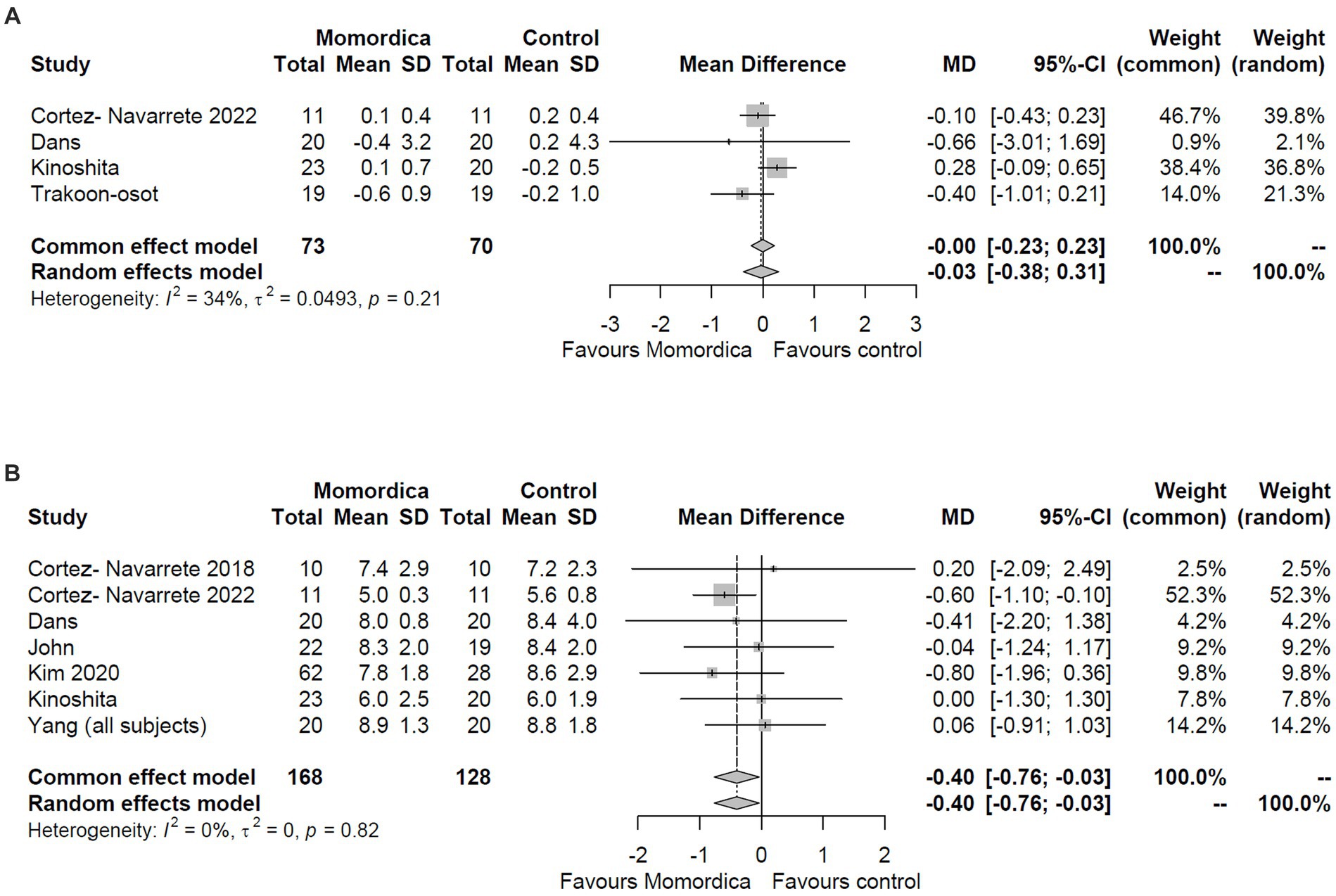
Figure 2. The effect of Momordica charantia on blood glucose level compared to placebo in the meta-analyses of the change scores (A) and post-intervention values (B) using the random effects and common effect models.
The analysis of HbA1c level resulted in somewhat similar results (Figure 3). The analysis of change scores was based on three studies (with data from 121 patients), whereas the analysis of post-intervention values on five trials (with data from 233 patients), and again, values could not be imputed. The meta-analysis of the post-intervention values using the random effects model indicated borderline efficacy for the M. charantia treatment with an MD = −0.24 (95% CI, −0.49 to 0.00, I2 = 0%) (Figure 3B), however, the analysis of the changes scores definitely did not show superiority over placebo (MD = −0.12; 95% CI: −0.35 to 0.11; I2 = 56%) (Figure 3A).
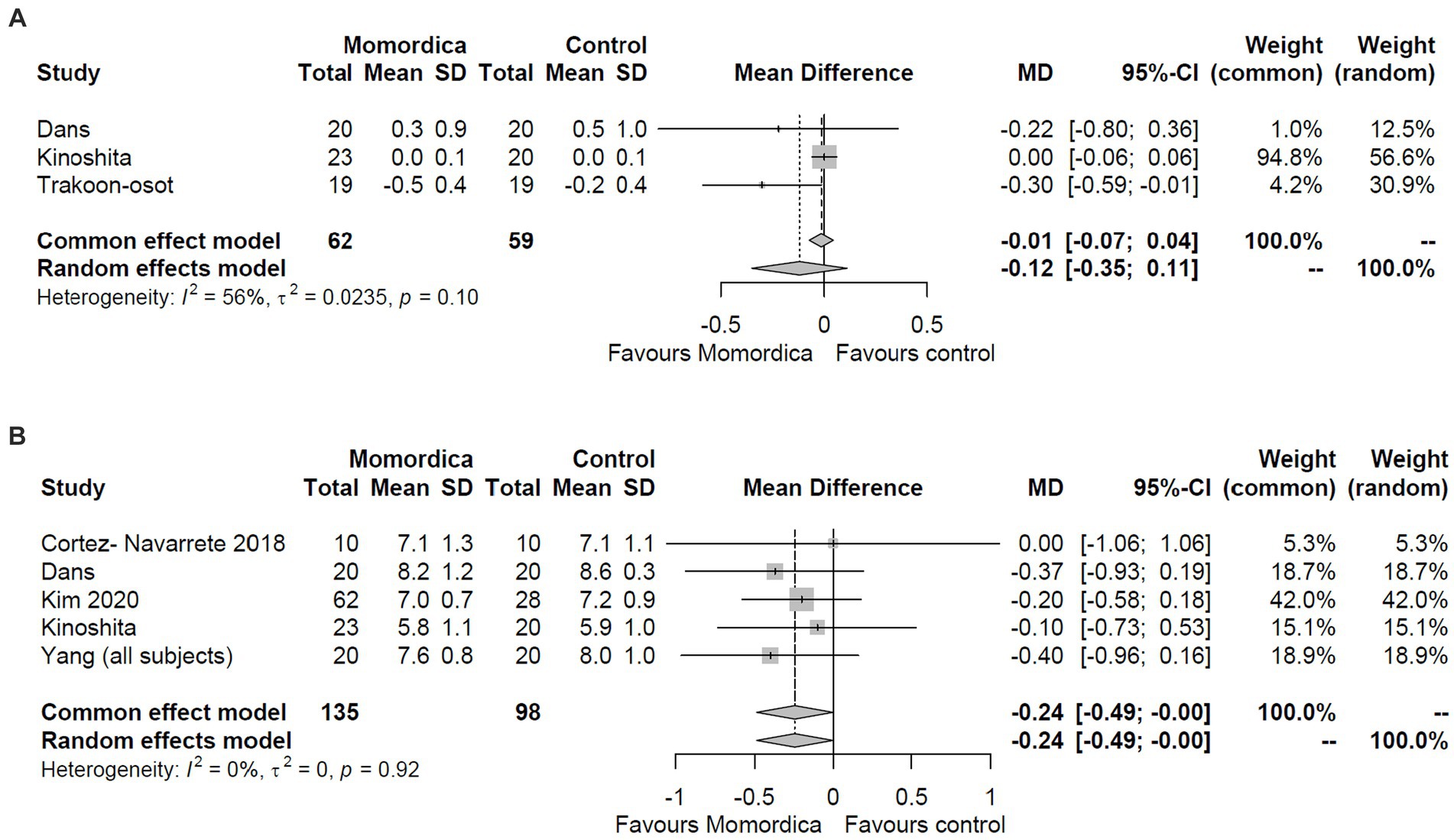
Figure 3. The effect of Momordica charantia on HbA1C level compared to placebo in the meta-analyses of the change scores (A) and post-intervention values (B) using the random effects and common effect models.
One of the recent trials (73) includes clinical indicators to assess insulin sensitivity and glucose metabolism, like HOMA-IR, Matsuda index, insulinogenic index. Because these parameters were not found in the other studies, they could not be evaluated in the meta-analysis.
3.4.2 Effect of Momordica charantia fruits on lipid profile
Regarding serum lipid levels, only the effects on HDL, LDL, and total cholesterol levels could be analyzed. Based on the changes in the mean differences data, as reported in three or four RCTs (Figure 4), M. charantia was not superior in any of these outcomes compared to placebo using the random effects model (MD = −0.04; 95% CI: −0.17 to 0.09; I2 = 66%; MD = −0.10; 95% CI: −0.28 to 0.08; I2 = 37%; and MD = −0.03; 95% CI: −0.15 to 0.22; I2 = 0%, respectively). These results are consistent with those obtained using common effect model.
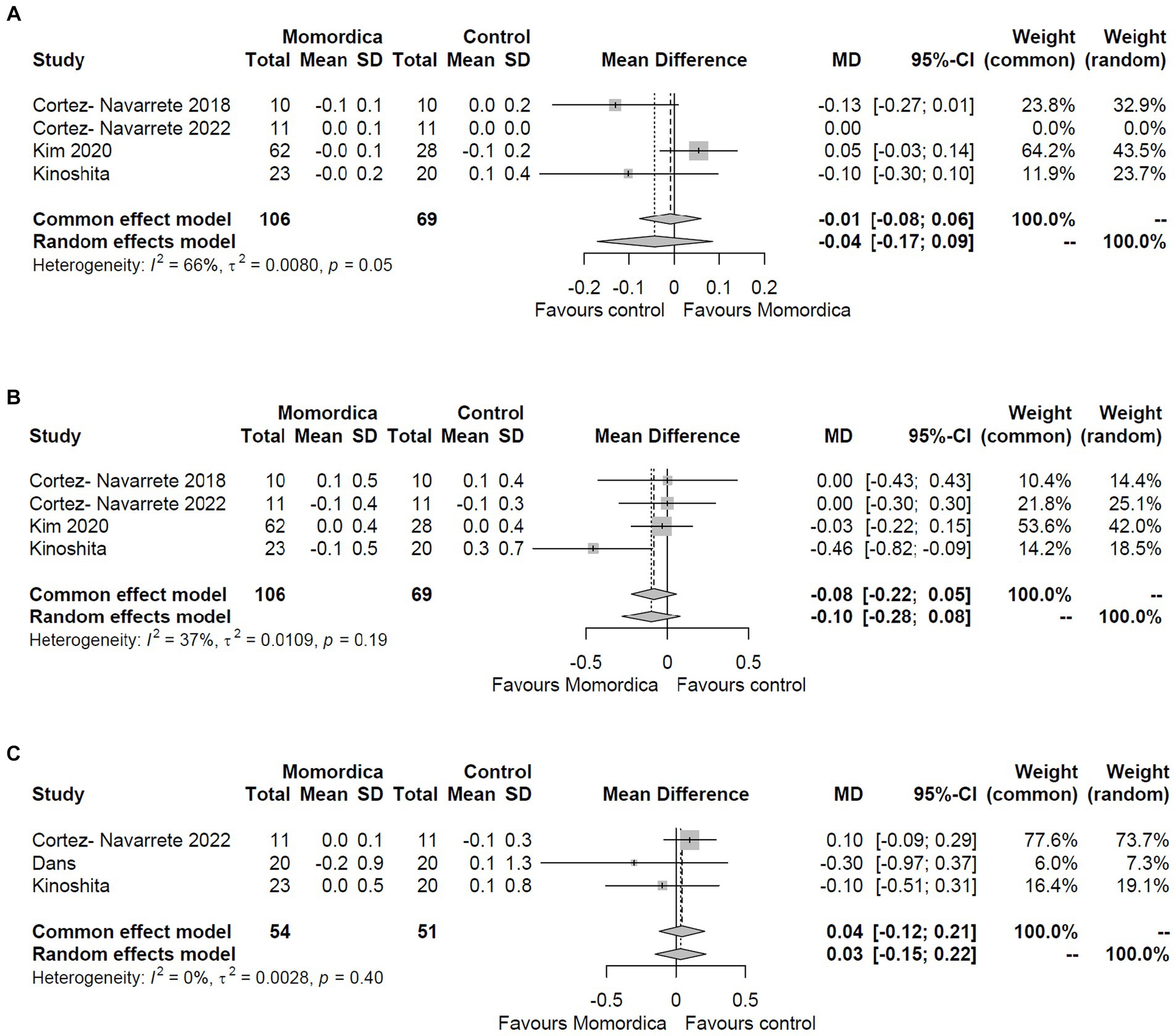
Figure 4. The effect of Momordica charantia on HDL (A), LDL (B), and total cholesterol levels (C) compared to placebo in the meta-analyses of the change scores using the random effects and common effect models.
The assessment of the post-intervention values complemented these results with triglyceride data. There was no evidence of significant effects of M. charantia on HDL (MD = −0.02; 95% CI: −0.12 to 0.09; I2 = 0%), LDL (MD = −0.01; 95% CI: −0.22 to 0.19; I2 = 0%), total cholesterol (MD = −0.04; 95% CI: −0.27 to 0.19; I2 = 0%) and triglyceride levels (MD = −0.09; 95% CI: −0.39 to 0.20; I2 = 22%) (Supplementary Figure S3). The reliability of these results is reassured by low heterogeneity values and the consistency of common and random effects models.
The assessment of the VLDL data is not conclusive, as data from only two studies were available (68, 72).
3.4.3 Effect of Momordica charantia fruits on anthropometric parameters
No significant effect on body weight (MD = −1.00; 95% CI: −2.59 to 0.59; I2 = 97%), body fat (MD = −1.21; 95% CI: −2.62 to 0.20; I2 = 0%) and BMI (MD = −0.42; 95% CI: −0.99 to 0.14; I2 = 95%) was observed in the meta-analyses of change scores. The analysis of the post-intervention values yielded the same results (Supplementary Figure S4). The effect on waist circumference could only be assessed from post-intervention data (MD = 0.72; 95% CI: −3.36 to 4.80; I2 = 13%) (Supplementary Figure S4). Common and random effects models had consistent results.
3.4.4 Effect of Momordica charantia fruits on blood pressure
Administration of M. charantia fruits did not demonstrate any effect on systolic blood pressure (MD = 1.01; 95% CI: −1.07 to 3.09; I2 = 0%) or diastolic blood pressures (MD = 0.24; 95% CI: −1.04 to 1.53; I2 = 0%) when comparing the change scores to that of the placebo group. This is supported by the examination of the post-intervention data (Supplementary Figure S5). Heterogeneity was very low and common and random effects model had similar results.
3.5 Adverse effects
Overall, there were no serious adverse effects reported by the studies included in our meta-analysis. Headache and gastrointestinal complaints were the most reported adverse events. In a double-blind RCT that used a special extract from fruits and seeds of M. charantia in addition to standard antidiabetic medication, adverse effects such as diarrhea and epigastric pain were reported after 1-month of administration (67).
The consumption of 6 g bitter melon pulp per day resulted in a significantly higher frequency of diarrhea and flatulence than in the placebo group (33).
Based on data from four trials (33, 67, 68, 72), M. charantia administration exerted no significant effects on liver enzymes (ALT, AST) and creatinine levels (Supplementary Figure S6) compared to placebo, however confidence intervals were sometimes wide to draw reliable safety conclusions (i.e., power was low).
4 Discussion
4.1 Main findings
A vast number of studies have been conducted, in both animal and human subjects using the M. charantia plant or different extracts prepared with stems, leaves, and fruits of the plant. These studies have allowed the identification of a few health-promoting benefits, including hypolipidemic, hypoglycemic, and anti-obesity effects (25, 26, 32, 33, 35, 36). In this review and meta-analysis, we have systematically evaluated the existing evidence on the potential efficacy of bitter melon in the treatment of metabolic syndrome, based on randomized, parallel-group, placebo-controlled trials. All the included trials, except the studies of Cortez-Navarrete (68, 72) were carried out in different Asian countries. Based on the nine trials included in this study, our findings show that M. charantia mono herbal preparations do not have a significant overall positive influence on blood glucose levels and other cardiovascular risk factors associated with metabolic syndrome. However, M. charantia was found to be statistically significantly more effective than a placebo in terms of reducing HbA1C and (marginally) fasting glucose levels when post-intervention data were analyzed. Even this relatively week conclusion (p = 0.032 and p = 0.050 respectively) was dependent on the analytical approach used, as it vanished when change scores were used. The change score data set had smaller sample size and was much more heterogeneous. Overall, our confidence in this finding is therefore low. The absence of an impact on ALT, AST, and creatinine levels suggests that there were no potential hepato- or nephrotoxic consequences at the doses used, although, the small sample size limits power and does not allow the reliable assessment of safety.
A previous meta-analysis suggested that bitter melon alone or in combination with other herbal medicinal products can reduce the elevated fasting plasma glucose level (FPG), postprandial glucose (PPG), and glycated hemoglobin A1c (HbA1c) (46). Compared to the placebo, M. charantia significantly reduced FPG, PPG, and HBA1c with mean differences of −0.72 mmol/L, − 1.43 mmol/L, and − 0.26%, respectively. M. charantia also lowered FPG in prediabetes (mean difference − 0.31 mmol/L). As discussed above, our meta-analysis found only a very week evidence for the superiority over placebo when assessing the effect on blood glucose and HbA1c levels. The explanation for this discrepancy is that the dataset used for analysis was different. First, we included five trials that were published after the previous meta-analysis (69–73). Second, the positive outcome of the meta-analysis of Peter et al. (46) could be explained by the inclusion of a paper reporting a trial with a size effect in favor of M. charantia (58) that was excluded in the present investigation due to the lack of blinding.
Animal experiments suggest that M. charantia might have the potential for increasing insulin sensitivity in patients with type 2 diabetes (28). According to a recent meta-analysis of animal experiments with type 2 diabetic rats, fruit and seed extracts of M. charantia reduced fasting plasma glucose and after at least 3 months of treatment increased serum insulin level and reduced HbA1c, triglycerides, total cholesterol in comparison to vehicle control (24). However, it should be noted that although the dose of M. charantia applied in different experiments was diverse, the typical range of 150–600 mg dry extract/kg/day is several magnitudes higher than those in the clinical trials. These differences in dosing might be one explanation for the lack of efficacy observed in this meta-analysis. Furthermore, differences in the qualitative and quantitative composition may contribute to the outwardly unreliable efficacy. Although charantin is considered the major active constituent of the plant, in silico studies suggest the importance of further metabolites. Momordicoside D (ligand of Takeda-G-protein-receptor-5, TGR5), cucurbitacin (ligand of glucagon-like peptide-1 receptor, GLP-1r), and charantin (ligand of dipeptidyl peptidase 4, DPP-4) were identified as the antidiabetic constituents of bitter melon in silico. In subsequent animal experiments, these potential mechanisms of action were reassured, since the extract of M. charantia significantly increased the expression of GLP-1r and TGR5 and decreased the expression of DPP-4 (74). The complex mechanism of action and the presence of multiple active components in this plant urge the need for the standardization of clinically studied products.
The lack of unambiguous efficacy on blood metabolic parameters might also be due to the short duration of the studies. HbA1c level reflects the cumulative glycemic history of the preceding two to three months (75). In the case of lipid levels, the efficacy of lifestyle changes can be expected within 3–6 months, and even in the case of a statin or combined therapy, the maximum percentage change will occur by 4 to 12 weeks after starting (76). Some of the studies meta-analyzed by us were only 30 days long (66, 69).
Regarding the effect on blood pressure, our findings are in accordance with the meta-analysis performed by Jandari et al. (44), which concluded that bitter melon preparations do not exert a significant antihypertensive effect. The effect of M. charantia on systolic and diastolic blood pressure was investigated in five trials (including 163 participants). The pooled effect size showed that neither systolic nor diastolic blood pressure changed following M. charantia supplementation. M. charantia seemed to be more effective in younger adults or when consumed for short durations, however, none of the subgroup analyses revealed significant efficacy compared to placebo. However, the duration of the included studies was 4–16 weeks, which does not allow the assessment of long-term antihypertensive effects (44). The potential long-term effect on blood pressure might be the result of the beneficial effect on blood lipid levels. For the effects on HDL, LDL triglyceride, total cholesterol levels, and ALT, AST, and creatinine concentrations, our meta-analysis is the first independent assessment of previously published clinical data. Our results do not support the hypothesis that the impact of bitter gourd on blood lipid levels might lead to antihypertensive effect.
The strength of our study is that we included only blinded, placebo-controlled studies that assessed the effect of M. charantia for at least four weeks on prediabetic and diabetic patients. The analyzed studies were performed by different research groups in different countries. By excluding complex preparations, we aimed to assess the effect of this herbal component only.
4.2 Limitations
The most important limitation of our meta-analysis is that the number of included studies and the number of patients is low, leading to even a meta-analysis being underpowered, moreover, the applied doses were not uniform. Although we did not find unambiguous efficacy in any of the analyzed outcomes, bitter gourd was found to be effective in some clinical trials. The duration of the studies (4–16 weeks) was too short to reveal the potential effects of M. charantia on metabolic parameters. This highlights the need for additional research into this plant in carefully planned clinical trials.
5 Conclusion
Although bitter melon has been widely used by patients suffering from metabolic syndrome, the meta-analysis of randomized, placebo-controlled trials does clearly not support the rationale of this practice. In agreement with a previous meta-analysis, we did not find an effect on blood pressure. In contrast with the meta-analysis of Peter et al., our assessment did not reveal an unambiguous effect on the blood glucose level. The effect on HDL, LDL triglyceride, and total cholesterol levels was meta-analyzed for the first time by us, and we did not find any significant beneficial effect in any of the parameters. However, lack of efficacy in the short-term studies does not necessarily mean the lack of efficacy in the case of long-term treatment M. charantia use. The limited sample size should also be considered when interpreting this finding.
To assess the clinical efficacy of M. charantia, there is a call for long-term randomized controlled trials with larger sample sizes. The investigation of the dose-dependence of antidiabetic activity in humans should also be considered.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found at: https://github.com/tamas-ferenci/MomordicaMetaAnalysis.
Author contributions
EL-Z and DC: conceptualization. EL-Z, BC-L, and DC: methodology. E-BK and DC: data extraction and abstracts screening. E-BK and BC-L: full texts screening. TF: statistical analysis. EL-Z, MN, and DC: risk of bias analysis. EL-Z and MN: writing—original draft preparation. BC-L, TF, and DC: writing—review and editing. BT: risk of bias analysis and writing—review and editing. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be considered as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2023.1200801/full#supplementary-material
References
1. Alberti, KGMM , Eckel, RH , Grundy, SM , Zimmet, PZ , Cleeman, JI , Donato, KA, et al. Harmonizing the metabolic syndrome. Circulation. (2009) 120:1640–5. doi: 10.1161/CIRCULATIONAHA.109.192644
2. Cicero, AFG , and Colletti, A . Role of phytochemicals in the management of metabolic syndrome. Phytomedicine. (2016) 23:1134–44. doi: 10.1016/j.phymed.2015.11.009
3. Saklayen, MG . The global epidemic of the metabolic syndrome. Curr Hypertens Rep. (2018) 20:12. doi: 10.1007/s11906-018-0812-z
4. Adetunji, CO , Michael, OS , Rathee, S , Singh, KRB , Ajayi, OO , Adetunji, JB, et al. Potentialities of nanomaterials for the management and treatment of metabolic syndrome: a new insight. Mater Today Adv. (2022) 13:100198. doi: 10.1016/j.mtadv.2021.100198
5. Cicero, AFG , Colletti, A , Bajraktari, G , Descamps, O , Djuric, DM , Ezhov, M, et al. Lipid-lowering nutraceuticals in clinical practice: position paper from an international lipid expert panel. Nutr Rev. (2017) 75:731–67. doi: 10.1093/nutrit/nux047
7. WHO . Diabetes-key facts. (2021). Available at: https://www.who.int/news-room/fact-sheets/detail/diabetes
8. Chang, CLT , Lin, Y , Bartolome, AP , Chen, Y-C , Chiu, S-C , and Yang, W-C . Herbal therapies for type 2 diabetes mellitus: chemistry, biology, and potential application of selected plants and compounds. Evidence-based Complement Altern Med. (2013) 2013:1–33. doi: 10.1155/2013/378657
9. Dimple, KA , Kumar, V , and Tomer, V . Traditional medicinal systems for treatment of diabetes mellitus: a review. Int. J Pharm Pharm Sci. (2018) 10:7–17. doi: 10.22159/ijpps.2018v10i5.25374
10. Panda, OP , Sahoo, N , Das, S , Das, S , and Mohanty, D . Phytochemicals in the remedy of diabetes mellitus: a systematic review. J Glob Trends Pharm Sci. (2020) 11:7960–72.
11. Choi, H-C , Kim, S-J , Son, K-Y , Oh, B-J , and Cho, B-L . Metabolic effects of aloe vera gel complex in obese prediabetes and early non-treated diabetic patients: randomized controlled trial. Nutrition. (2013) 29:1110–4. doi: 10.1016/j.nut.2013.02.015
12. Fallah Huseini, H , Hasani-Rnjbar, S , Nayebi, N , Heshmat, R , Sigaroodi, FK , Ahvazi, M, et al. (caper) fruit extract in treatment of type 2 diabetic patients: a randomized double-blind placebo-controlled clinical trial. Complement Ther Med. (2013) 21:447–52. doi: 10.1016/j.ctim.2013.07.003
13. Khan, A , Safdar, M , Ali Khan, MM , Khattak, KN , and Anderson, RA . Cinnamon improves glucose and lipids of people with type 2 diabetes. Diabetes Care. (2003) 26:3215–8. doi: 10.2337/diacare.26.12.3215
14. Akilen, R , Tsiami, A , Devendra, D , and Robinson, N . Cinnamon in glycaemic control: systematic review and meta analysis. Clin Nutr. (2012) 31:609–15. doi: 10.1016/j.clnu.2012.04.003
15. Haber, SL , and Keonavong, J . Fenugreek use in patients with diabetes mellitus. Am J Heal Pharm. (2013) 70:1196–203. doi: 10.2146/ajhp120523
16. Hooper, L , Kay, C , Abdelhamid, A , Kroon, PA , Cohn, JS , Rimm, EB, et al. Effects of chocolate, cocoa, and flavan-3-ols on cardiovascular health: a systematic review and meta-analysis of randomized trials. Am J Clin Nutr. (2012) 95:740–51. doi: 10.3945/ajcn.111.023457
17. Kumar, SN , Mani, UV , and Mani, I . An open label study on the supplementation of Gymnema sylvestre in type 2 diabetics. J Diet Suppl. (2010) 7:273–82. doi: 10.3109/19390211.2010.505901
18. Di Fabio, G , Romanucci, V , Zarrelli, M , Giordano, M , and Zarrelli, A . C-4 gem-Dimethylated Oleanes of Gymnema sylvestre and their pharmacological activities. Molecules. (2013) 18:14892–919. doi: 10.3390/molecules181214892
19. Jerine Peter, S , and Sabina, EP . Global current trends in natural products for diabetes management: a review. Int J Pharm Pharm Sci. (2016) 8:20–8.
20. Marton, LT , Pescinini-E-Salzedas, LM , Camargo, MEC , Barbalho, SM , Haber, JFDS , Sinatora, RV, et al. The effects of curcumin on diabetes mellitus: a systematic review. Front Endocrinol (Lausanne). (2021) 12:669448. doi: 10.3389/fendo.2021.669448
21. Sánchez, M , González-Burgos, E , Iglesias, I , Lozano, R , and Gómez-Serranillos, MP . The pharmacological activity of Camellia sinensis (L.) Kuntze on metabolic and endocrine disorders: a systematic review. Biomol Ther. (2020) 10:603. doi: 10.3390/biom10040603
22. Ríos, J , Francini, F , and Schinella, G . Natural products for the treatment of type 2 diabetes mellitus. Planta Med. (2015) 81:975–94. doi: 10.1055/s-0035-1546131
23. Kumar, S , Mittal, A , Babu, D , and Mittal, A . Herbal medicines for diabetes management and its secondary complications. Curr Diabetes Rev. (2021) 17:437–56. doi: 10.2174/1573399816666201103143225
24. Peter, EL , Nagendrappa, PB , Kaligirwa, A , Ogwang, PE , and Sesaazi, CD . The safety and efficacy of Momordica charantia L. in animal models of type 2 diabetes mellitus: a systematic review and meta-analysis. Phyther Res. (2021) 35:637–56. doi: 10.1002/ptr.6853
25. Fan, M , Lee, J , Ryu, Y , Choi, Y , Tang, Y , Oh, M, et al. Comparative analysis of metabolite profiling of Momordica charantia leaf and the anti-obesity effect through regulating lipid metabolism. Int J Environ Res Public Heal. (2021) 18:5584. doi: 10.3390/ijerph18115584
26. Mahwish, SF , Arshad, MS , Nisa, MU , Nadeem, MT , and Arshad, MU . Hypoglycemic and hypolipidemic effects of different parts and formulations of bitter gourd (Momordica Charantia). Lipids Health Dis. (2017) 16:211–1. doi: 10.1186/s12944-017-0602-7
27. Wat, E , Wang, Y , Chan, K , Law, HW , Koon, CM , Lau, KM, et al. An in vitro and in vivo study of a 4-herb formula on the management of diet-induced metabolic syndrome. Phytomedicine. (2018) 42:112–25. doi: 10.1016/j.phymed.2018.03.028
28. Wang, H-Y , Kan, W-C , Cheng, T-J , Yu, S-H , Chang, L-H , and Chuu, J-J . Differential anti-diabetic effects and mechanism of action of charantin-rich extract of Taiwanese Momordica charantia between type 1 and type 2 diabetic mice. Food Chem Toxicol. (2014) 69:347–56. doi: 10.1016/j.fct.2014.04.008
29. Harinantenaina, L , Tanaka, M , Takaoka, S , Oda, M , Mogami, O , Uchida, M, et al. Momordica charantia constituents and antidiabetic screening of the isolated major compounds. Chem Pharm Bull (Tokyo). (2006) 54:1017–21. doi: 10.1248/cpb.54.1017
30. Klomann, SD , Mueller, AS , Pallauf, J , and Krawinkel, MB . Antidiabetic effects of bitter gourd extracts in insulin-resistant db/db mice. Br J Nutr. (2010) 104:1613–20. doi: 10.1017/S0007114510002680
31. Han, C , Hui, Q , and Wang, Y . Hypoglycaemic activity of saponin fraction extracted from Momordica charantia in PEG/salt aqueous two-phase systems. Nat Prod Res. (2008) 22:1112–9. doi: 10.1080/14786410802079675
32. Lee, C-D , and Ma, T . Effect of acute bitter melon intake on postprandial glucose and insulin in sedentary, abdominally obese persons. Funct Foods Heal Dis. (2019) 9:384. doi: 10.31989/ffhd.v9i6.605
33. Trakoon-osot, W , Sotanaphun, U , Phanachet, P , Porasuphatana, S , Udomsubpayakul, U , and Komindr, S . Pilot study: hypoglycemic and antiglycation activities of bitter melon (Momordica charantia L.) in type 2 diabetic patients. J Pharm Res. (2013) 6:859–64. doi: 10.1016/j.jopr.2013.08.007
34. Rahman, IU , Khan, RU , Rahman, KU , and Bashir, M . Lower hypoglycemic but higher antiatherogenic effects of bitter melon than glibenclamide in type 2 diabetic patients. Nutr J. (2015) 14:1–7. doi: 10.1186/1475-2891-14-13
35. Bao, B , Chen, Y-G , Zhang, L , Xu, YLN , Wang, X , Liu, J, et al. Momordica charantia (bitter melon) reduces obesity-associated macrophage and mast cell infiltration as well as inflammatory cytokine expression in adipose tissues. PLoS One. (2013) 8:e84075. doi: 10.1371/journal.pone.0084075
36. Fan, M , Kim, E-K , Choi, Y-J , Tang, Y , and Moon, S-H . The role of Momordica charantia in resisting obesity. Int J Environ Res Public Health. (2019) 16:3251. doi: 10.3390/ijerph16183251
37. Jia, S , Shen, M , Zhang, F , and Xie, J . Recent advances in Momordica charantia: functional components and biological activities. Int J Mol Sci. (2017) 18:2555. doi: 10.3390/ijms18122555
38. Sun, L , Zhang, XP , Dong, L , Zhang, CY , Guo, P , and Wu, CM . The triterpenoids of the bitter gourd (Momordica Charantia) and their pharmacological activities: a review. J Food Compos Anal. (2021) 96:103726. doi: 10.1016/j.jfca.2020.103726
39. Wang, S , Li, Z , Yang, G , Ho, C-T , and Li, S . Momordica charantia: a popular health-promoting vegetable with multifunctionality. Food Funct. (2017) 8:1749–62. doi: 10.1039/C6FO01812B
40. Muronga, M , Quispe, C , Tshikhudo, PP , Msagati, TAM , Mudau, FN , Martorell, M, et al. Three selected edible crops of the genus Momordica as potential sources of phytochemicals: biochemical, nutritional, and medicinal values. Front Pharmacol. (2021) 12:12. doi: 10.3389/fphar.2021.625546
41. Fang, EF , Froetscher, L , Scheibye-Knudsen, M , Bohr, VA , Wong, JH , and Ng, TB . Emerging antitumor activities of the bitter melon (Momordica charantia). Curr Protein Pept Sci. (2019) 20:296–301. doi: 10.2174/1389203719666180622095800
42. Bortolotti, M , Mercatelli, D , and Polito, L . Momordica charantia, a nutraceutical approach for inflammatory related diseases. Front Pharmacol. (2019) 10:10 (MAY). doi: 10.3389/fphar.2019.00486
43. Liu, Z , Gong, J , Huang, W , Lu, F , and Dong, H . The effect of Momordica charantia in the treatment of diabetes mellitus: a review. Evid Based Complement Alternat Med. (2021) 2021:1–14. doi: 10.1155/2021/3796265
44. Jandari, S , Ghavami, A , Ziaei, R , Nattagh-Eshtivani, E , Rezaei Kelishadi, M , Sharifi, S, et al. Effects of Momordica charantia L on blood pressure: a systematic review and meta- analysis of randomized clinical trials. Int J Food Prop. (2020) 23:1913–24. doi: 10.1080/10942912.2020.1833916
45. Cortez-Navarrete, M , Méndez-Del Villar, M , Ramos-González, EJ , and Pérez-Rubio, KG . Momordica Charantia: a review of its effects on metabolic diseases and mechanisms of action. J Med Food. (2021) 24:1017–27. doi: 10.1089/jmf.2020.0206
46. Peter, EL , Kasali, FM , Deyno, S , Mtewa, A , Nagendrappa, PB , Tolo, CU, et al. Momordica charantia L. lowers elevated glycaemia in type 2 diabetes mellitus patients: systematic review and meta-analysis. J Ethnopharmacol. (2019) 231:311–24. doi: 10.1016/j.jep.2018.10.033
47. Page, MJ , McKenzie, JE , Bossuyt, PM , Boutron, I , Hoffmann, TC , Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
48. Sidorenkov, G , Haaijer-Ruskamp, FM , de Zeeuw, D , and Denig, P . A longitudinal study examining adherence to guidelines in diabetes care according to different definitions of adequacy and timeliness. PLoS One. (2011) 6:e24278. doi: 10.1371/journal.pone.0024278
49. Higgins, JPT, Thomas, J, Chandler, J, Cumpston, M, Li, T, Page, MJ, et al. (editors). Cochrane Handbook for Systematic Reviews of Interventions version 6.4 (updated August 2023). Cochrane (2023). Available at: www.training.cochrane.org/handbook
50. Abrams, KR , Gillies, CL , and Lambert, PC . Meta-analysis of heterogeneously reported trials assessing change from baseline. Stat Med. (2005) 24:3823–44. doi: 10.1002/sim.2423
51. Follmann, D , Elliott, P , Suh, I , and Cutler, J . Variance imputation for overviews of clinical trials with continuous response. J Clin Epidemiol. (1992) 45:769–73. doi: 10.1016/0895-4356(92)90054-Q
52. McGrath, S , Zhao, X , Steele, R , Thombs, BD , and Benedetti, A . Estimating the sample mean and standard deviation from commonly reported quantiles in meta-analysis. Stat Methods Med Res. (2020) 29:2520–37. doi: 10.1177/0962280219889080
53. Cooper, H , Hedges, LV , and Valentine, JC . The handbook of research synthesis and Meta-analysis. 2nd editio ed. New York: Russell Sage Foundation (2009).
54. R Core Team . R: A language and environment for statistical computing. R foundation for statistical computing. Vienna, Austria: (2022) Available at: https://www.r-project.org/.
55. Viechtbauer, W . Conducting Meta-analyses in R with the metafor package. J Stat Softw. (2010) 36:1–48. doi: 10.18637/jss.v036.i03
56. Higgins, J , Thomas, J , Chandler, J , Cumpston, M , and Li, T . Cochrane handbook for systematic reviews of interventions. (2019)
57. Ahmad, N , Hassan, MR , Halder, H , and Bennoor, KS . Effect of Momordica charantia (Karolla) extracts on fasting and postprandial serum glucose levels in NIDDM patients. Bangladesh Med Res Counc Bull. (1999) 25:11–3.
58. Suthar, AC , Deshmukh, A , Babu, V , Mohan, VS , Chavan, MV , Kumar, D, et al. Efficacy and safety of Glycebal (PDM011011) capsules as adjuvant therapy in subjects with type 2 diabetes mellitus: an open label, randomized, active controlled, phase II trial. Clin Diabetol. (2016) 5:88–94. doi: 10.5603/DK.2016.0015
59. Thomford, KP , Thomford, AK , Yorke, J , Yeboah, R , and Appiah, AA . Momordica charantia L. for hyperlipidaemia: a randomised controlled assessment of the Ghanaian herbal medicinal product MCP-1. J Herb Med. (2021) 28:100453. doi: 10.1016/j.hermed.2021.100453
60. Kasbia, GS , Arnason, JT , and Imbeault, P . No effect of acute, single dose oral administration of Momordica charantia Linn., on glycemia, energy expenditure and appetite: a pilot study in non-diabetic overweight men. J Ethnopharmacol. (2009) 126:127–33. doi: 10.1016/j.jep.2009.07.035
61. Krawinkel, MB , Ludwig, C , Swai, ME , Yang, RY , Chun, KP , and Habicht, SD . Bitter gourd reduces elevated fasting plasma glucose levels in an intervention study among prediabetics in Tanzania. J Ethnopharmacol. (2018) 216:1–7. doi: 10.1016/j.jep.2018.01.016
62. Hongliang, X , Fan, W , Qing, N , Zhexin, Y , Ran, A , Qiuju, Z, et al. Observation of effects with natural medicine and food in metabolic syndrome. Acta Medica Mediterr. (2021) 37:613–9. doi: 10.19193/0393-6384_2021_1_94
63. Rosyid, FN , Dharmana, E , Suwondo, A , and Heri Nugroho, KHS . The effect of bitter melon (Momordica charantia L.) leaves extract on TNF-α serum levels and diabetic foot ulcers improvement: randomized controlled trial. Biomed Pharmacol J. (2018) 11:1413–21. doi: 10.13005/bpj/1505
64. Rosyid, FN , Muhtadi, M , Hudiyawati, D , Sugiyarti, S , and Rahman, AF . Improving diabetic foot ulcer healing with adjuvant bitter melon leaf extract (Momordica charantia L.). Open access Maced. J Med Sci. (2022) 10:122–6. doi: 10.3889/oamjms.2022.9503
65. Rosyid, FN , Dharmana, E , Suwondo, A , and HS, KHN . The effect of bitter melon (Momordica charantia L.) leaves Extractonon glycated albumin in diabetic foot ulcers: randomized controlled trial. Bangladesh. J Med Sci. (2021) 20:281–7. doi: 10.3329/bjms.v20i2.51536
66. John, AJ , Cherian, R , Subhash, HS , and Cherian, AM . Evaluation of the efficacy of bitter gourd (Momordica charantia) as an oral hypoglycemic agent - a randomized controlled clinical trial [3]. Indian J Physiol Pharmacol. (2003) 47:363–5.
67. Dans, AML , Villarruz, MVC , Jimeno, CA , Javelosa, MAU , Chua, J , Bautista, R, et al. The effect of Momordica charantia capsule preparation on glycemic control in type 2 diabetes mellitus needs further studies. J Clin Epidemiol. (2007) 60:554–9. doi: 10.1016/j.jclinepi.2006.07.009
68. Cortez-Navarrete, M , Martínez-Abundis, E , Pérez-Rubio, KG , González-Ortiz, M , and Méndez-Del, VM . Momordica charantia administration improves insulin secretion in type 2 diabetes mellitus. J Med Food. (2018) 21:672–7. doi: 10.1089/jmf.2017.0114
69. Kinoshita, H , and Ogata, Y . Effect of bitter melon extracts on lipid levels in Japanese subjects: a randomized controlled study. Evidence-based Complement Altern Med. (2018) 2018:1–6. doi: 10.1155/2018/4915784
70. Kim, SK , Jung, J , Jung, JH , Yoon, NA , Kang, SS , Roh, GS, et al. Hypoglycemic efficacy and safety of Momordica charantia (bitter melon) in patients with type 2 diabetes mellitus. Complement Ther Med. (2020) 52:102524. doi: 10.1016/j.ctim.2020.102524
71. Yang, Y-S , Wu, N-Y , Kornelius, E , Huang, C-N , and Yang, N-C . A randomized, double-blind, placebo-controlled trial to evaluate the hypoglycemic efficacy of the mc IRBP-19-containing Momordica charantia L. fruit extracts in the type 2 diabetic subjects. Food Nutr Res. (2022) 66:66. doi: 10.29219/fnr.v66.3685
72. Cortez-Navarrete, M , Méndez-Del Villar, M , Martínez-Abundis, E , López-Murillo, LD , Escobedo-Gutiérrez, MDJ , Rosales-Rivera, LY, et al. Effect of Momordica charantia administration on anthropometric measures and metabolic profile in patients with obesity: a pilot clinical trial. J Med Food. (2022) 25:645–51. doi: 10.1089/jmf.2021.0164
73. Kim, B , Lee, HS , Kim, HJ , Lee, H , Lee, I , Young, OS, et al. Momordica charantia (bitter melon) efficacy and safety on glucose metabolism in Korean prediabetes participants: a 12-week, randomized clinical study. Food Sci Biotechnol. (2023) 32:697–704. doi: 10.1007/s10068-022-01214-9
74. Elekofehinti, OO , Ariyo, EO , Akinjiyan, MO , Olayeriju, OS , Lawal, AO , Adanlawo, IG, et al. Potential use of bitter melon (Momordica charantia) derived compounds as antidiabetics: in silico and in vivo studies. Pathophysiology. (2018) 25:327–33. doi: 10.1016/j.pathophys.2018.05.003
75. Sherwani, SI , Khan, HA , Ekhzaimy, A , Masood, A , and Sakharkar, MK . Significance of HbA1c test in diagnosis and prognosis of diabetic patients. Biomark Insights. (2016) 11:95–104. doi: 10.4137/BMI.S38440
76. Grundy, SM , Stone, NJ , Bailey, AL , Beam, C , Birtcher, KK , Blumenthal, RS, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the Management of Blood Cholesterol: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. Circulation. (2019) 139:e1082–143. doi: 10.1161/CIR.0000000000000625
Keywords: Momordica charantia, bitter melon, metabolic syndrome, insulin resistance, obesity, cardiovascular disease, dyslipidemia
Citation: Laczkó-Zöld E, Csupor-Löffler B, Kolcsár E-B, Ferenci T, Nan M, Tóth B and Csupor D (2024) The metabolic effect of Momordica charantia cannot be determined based on the available clinical evidence: a systematic review and meta-analysis of randomized clinical trials. Front. Nutr. 10:1200801. doi: 10.3389/fnut.2023.1200801
Edited by:
Shivraj Hariram Nile, Zhejiang Chinese Medical University, ChinaReviewed by:
Ralf Jäger, Increnovo LLC, United StatesNikita Saraswat, DY Patil College of Pharmacy, Akurdi, India
Copyright © 2024 Laczkó-Zöld, Csupor-Löffler, Kolcsár, Ferenci, Nan, Tóth and Csupor. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Eszter Laczkó-Zöld, ZXN6dGVyLmxhY3prb0B1bWZzdC5ybw==
†These authors have contributed equally to this work and share first authorship