Abstract
Background:
Research has indicated that both total cholesterol (TC) and low-density lipoprotein (LDL) cholesterol levels may impact the risk of colorectal cancer (CRC). However, as TC and LDL cholesterol consist of multiple lipid species, it remains uncertain which specific species contribute to this risk. Therefore, this study plans to search for the major lipid species that influence the risk of CRC.
Methods:
Initially, a two-sample Mendelian randomization analyses was employed to examine the association between 179 lipid levels and the risk of CRC. Subsequent to this, a meta-analysis was conducted on the results of Mendelian randomization analyses in four CRC cohorts to further determine the relationship between the implicated lipids and CRC risk. Reverse Mendelian randomization was utilized to investigate the potential reverse causal relationship between the relevant lipids and CRC. Lastly, a two-step Mendelian randomization analysis was employed to assess whether the associated lipids acted as mediators in the relationship between TC and LDL cholesterol levels and CRC risk.
Results:
Our study identified five lipid levels across multiple cohorts that were significantly associated with the risk of CRC. Meta-analysis results indicated a positive correlation between sterol ester (27:1/14:0) and sterol ester (27:1/16:0) levels and CRC risk (p < 0.05), with no evidence of reverse causality. Furthermore, sterol ester (27:1/14:0) and sterol ester (27:1/16:0) were found to mediate the relationship between TC and LDL cholesterol levels and the risk of CRC. Specifically, sterol ester (27:1/14:0) accounted for 87.9 and 93.3% of the effects of TC and LDL cholesterol on CRC risk, while sterol ester (27:1/16:0) mediated 44.3 and 44.6% of these effects, respectively.
Conclusion:
Sterol esters (27:1/14:0) and (27:1/16:0) are significant lipids that influence the risk of CRC and act as mediators of TC and LDL cholesterol increasing the risk of CRC.
1 Introduction
Colorectal cancer (CRC) is the most common digestive system cancer, ranking as the third most prevalent cancer globally and the second leading cause of cancer-related mortality (1). In 2022, an estimated 153,020 new cases of CRC and 52,550 deaths were reported worldwide (2). Identifying risk factors, prevention, and early interventions are crucial due to the high incidence and mortality of CRC.
Research has indicated a correlation between blood lipids and various cancer risks, particularly in patients with hyperlipidemia who exhibit an elevated risk of colon, prostate, and testicular cancer (3). Alterations in total cholesterol (TC) and low-density lipoprotein (LDL) cholesterol have been shown to increase the risk of CRC (4, 5). Nevertheless, it is important to note that both TC and LDL cholesterol consist of cholesterol as well as various other lipids (6, 7). At present, the specific lipid species that influence the risk of CRC remains unidentified.
Mendelian randomization (MR) has become a prominent method in investigating disease etiology, particularly in the absence of randomized controlled trials (8). By utilizing single nucleotide polymorphisms (SNPs) as instrumental variables (IV), MR allows for the assessment of causal relationships between exposures and outcomes (9). The IV model effectively mitigates confounding in observational studies by assuming random assignment of genotypes during gamete formation, thereby addressing bias stemming from unmeasured confounders on causal inference (10).
Benefit from the progress of modern efficient lipidomics technologies, Ottensmann et al. have acquired genome-wide association study (GWAS) data on 179 plasma lipid species, including 16 sterols (ST), 15 sphingolipids (SL), 44 glycerolipids (GL), and 104 glycerophospholipids (GP) (6).
The current research conducted an analysis on the correlation between 179 plasma lipid species and the risk of CRC using MR analysis. The findings suggest a significant positive association between sterol ester (27:1/14:0) and sterol ester (27:1/16:0) levels and the risk of CRC. As constituents of TC and LDL, these lipid components act as mediators in the relationship between TC and LDL levels and the risk of CRC. Given the crucial role of lipids in human physiological processes, targeted regulation of specific lipid species, rather than a broad approach targeting all lipids, at the dietary, nutritional, or therapeutic levels may represent a viable strategy for the prevention of CRC.
2 Results
2.1 Association of levels of 179 plasma lipids with risk of CRC
Two-sample Mendelian randomization was utilized to examine the correlation between 179 plasma lipid levels and the risk of CRC. Results indicated that 25 lipid species were significantly linked to CRC risk in one or more cohorts. Specifically, phosphatidylcholine (O-16:1_18:0) levels demonstrated an inverse relationship with CRC risk in two cohorts, while phosphatidylcholine (18:1_20:3) levels and diacylglycerol (16:0_18:1) levels exhibited a positive association with CRC risk in three cohorts. Additionally, sterol ester (27:1/14:0) levels and sterol ester (27:1/16:0) levels were found to be positively correlated with CRC risk in all cohorts analyzed. Furthermore, a total of 21 lipids were identified as being linked to the risk of CRC in a single cohort. These findings are presented in Figure 1. The MR analysis results and tests for heterogeneity and pleiotropy for statistically significant lipid and CRC risk in each cohort are in Supplementary Tables 1–5. The outcomes of the corresponding leave-one-out sensitivity analysis examining the impact of plasma lipid species on CRC, in addition to the funnel plots, scatter plots, and forest plots associated with the primary MR analysis, are presented in Supplementary Figures 1–4.
Figure 1
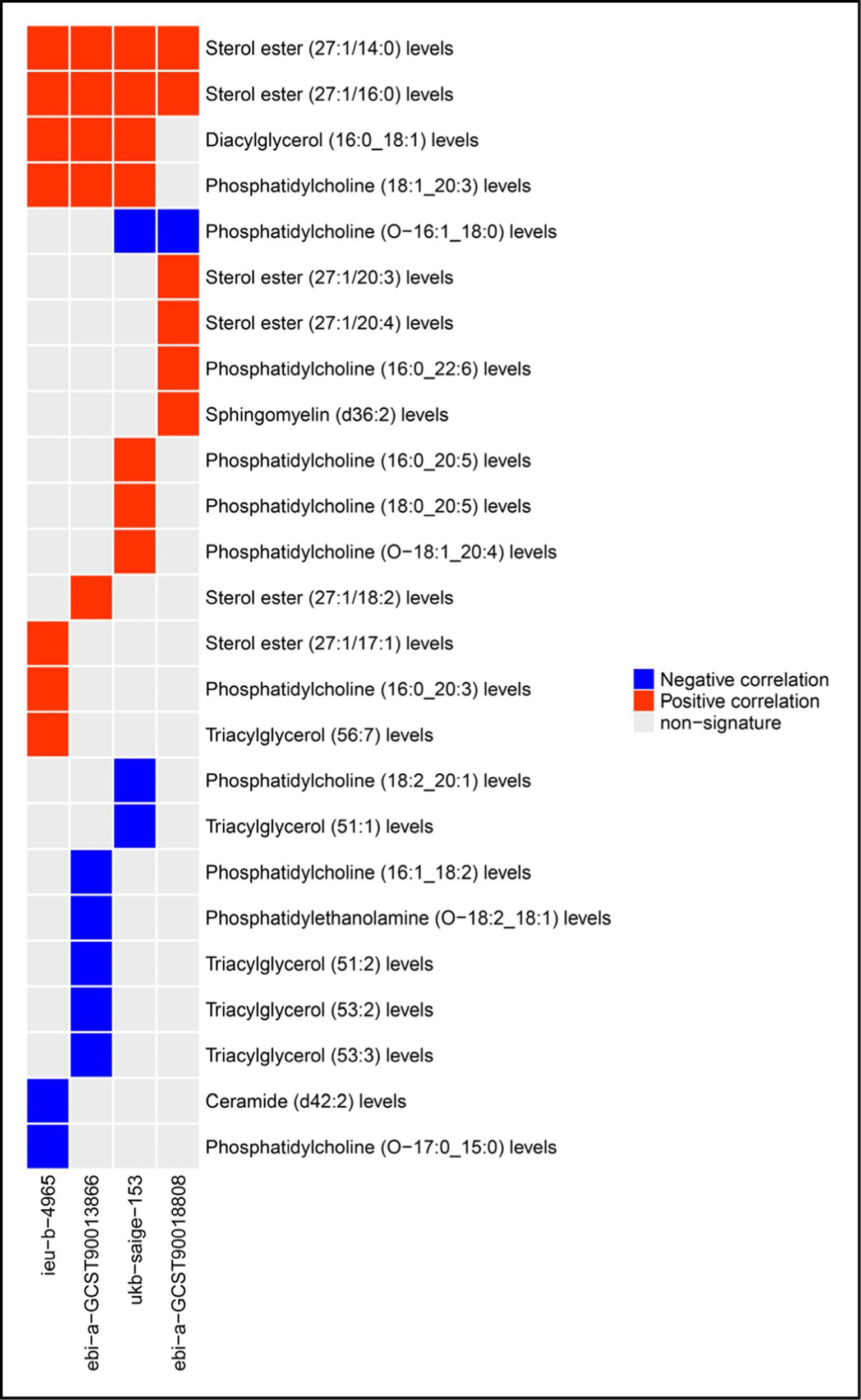
Plasma lipid species associated with CRC risk.
2.2 Meta-analysis of the relationship between lipids and risk of CRC
We identified lipids linked to CRC risk in multiple cohorts and conducted a meta-analysis on the results of the IVW analysis. Sterol ester (27:1/14:0) and Sterol ester (27:1/16:0) levels were found to be positively associated with CRC risk, with p-values of 0.018 and 0.024, respectively (Figures 2A,B). Meta-analysis found no significant association between Diacyl glycerol (16:0 _ 18:1) levels and CRC risk (p = 0.124) (Figure 2C). Phosphatidylcholine (18:1 _ 20:3) levels were positively linked to CRC risk (p = 0.050) (Figure 2D), while Phosphatidylcholine (O-16: 1 _ 18:0) levels were inversely associated with risk (p = 0.052) (Figure 2E).
Figure 2
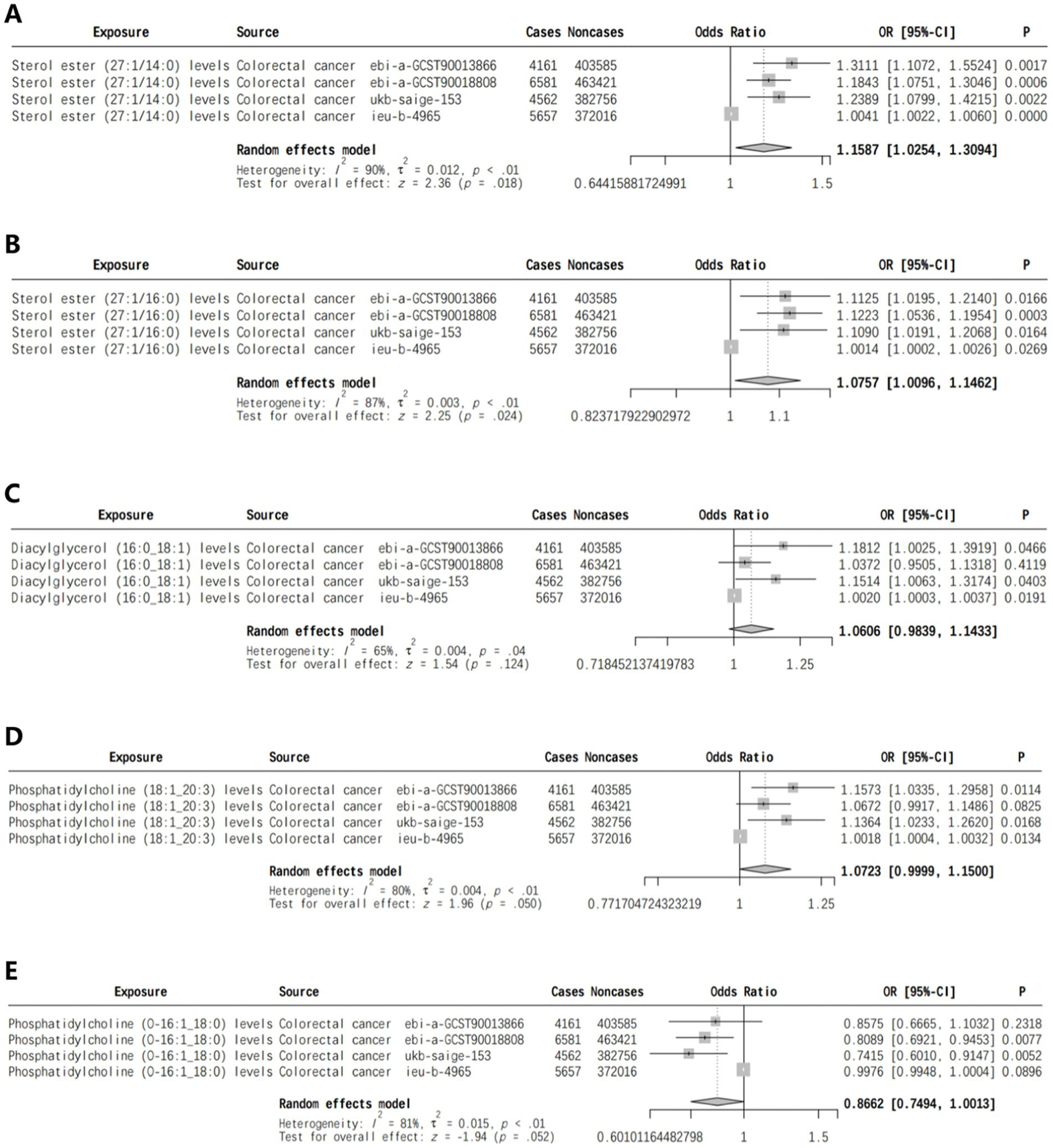
Meta-analysis of lipids associated with CRC risk in two or more cohorts [(A) Sterol ester (27:1/14:0) levels, (B) Sterol ester (27:1/16:0) levels, (C) Diacylglycerol (16:0_18:1) levels, (D) Phosphatidylcholine (18:1_20:3) levels, (E) Phosphatidylcholine (O-16:1_18:0) levels].
2.3 Reverse Mendelian randomization of sterol ester (27:1/14:0) levels, sterol ester (27:1/16:0) levels, and risk of CRC
The reverse Mendelian randomization analysis of sterol ester (27:1/14:0) levels and sterol ester (27:1/16:0) levels in relation to CRC across four cohorts revealed a lack of significant correlation between CRC and sterol ester (27:1/14:0) levels and sterol ester (27:1/16:0) levels (Table 1).
Table 1
| id.exposure | Exposure | Outcome | Method | No. SNPs | OR (95%CI) | p value |
|---|---|---|---|---|---|---|
| ebi-a-GCST90013866 | Colorectal cancer | Sterol ester (27:1/14:0) levels | IVW | 2 | 0.961(0.808–1.144) | 0.657 |
| ebi-a-GCST90018808 | Colorectal cancer | Sterol ester (27:1/14:0) levels | IVW | 14 | 0.986(0.899–1.082) | 0.763 |
| ieu-b-4965 | Colorectal cancer | Sterol ester (27:1/14:0) levels | IVW | 5 | 0.160(0.000–153.361) | 0.601 |
| ukb-saige-153 | Colorectal cancer | Sterol ester (27:1/14:0) levels | IVW | 3 | 0.950(0.845–1.069) | 0.395 |
| ebi-a-GCST90013866 | Colorectal cancer | Sterol ester (27:1/16:0) levels | IVW | 3 | 0.981(0.836–1.151) | 0.814 |
| ebi-a-GCST90018808 | Colorectal cancer | Sterol ester (27:1/16:0) levels | IVW | 11 | 0.971(0.875–1.076) | 0.572 |
| ieu-b-4965 | Colorectal cancer | Sterol ester (27:1/16:0) levels | IVW | 3 | 0.084(0.000–620.407) | 0.585 |
| ukb-saige-153 | Colorectal cancer | Sterol ester (27:1/16:0) levels | IVW | 2 | 0.973(0.844–1.123) | 0.713 |
Reverse Mendelian randomization of sterol ester (27:1/14:0) levels, sterol ester (27:1/16:0) levels and risk of CRC.
2.4 Mediation analysis
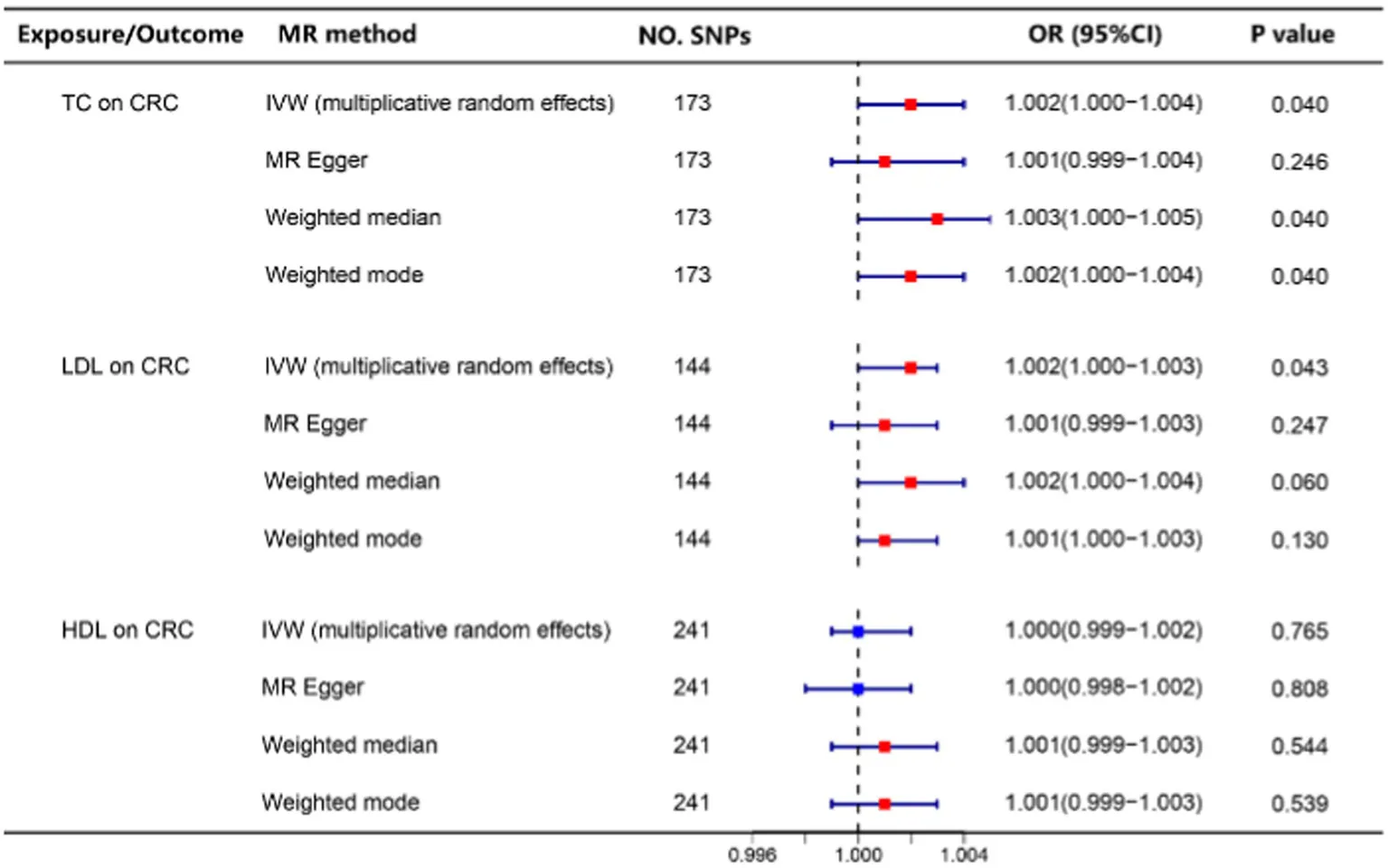
Our study revealed that elevated levels of TC and LDL cholesterol were associated with an increased risk of CRC (Table 2). Subsequently, we employed a two-step Mendelian randomization approach to investigate the mediating effects of sterol ester (27:1/14:0) and sterol ester (27:1/16:0) on the relationship between TC, LDL cholesterol, and CRC risk. Our findings indicated that sterol ester (27:1/14:0) mediated 87.9 and 93.3% of the effects of TC and LDL cholesterol on CRC risk, respectively. Additionally, sterol ester (27:1/16:0) was found to mediate 44.3 and 44.6% of the effects of TC and LDL cholesterol on CRC risk, respectively. The p values of Interactive Mediation Tests were all less than 0.05. The results are shown in Table 3. Relevant MR analysis results and heterogeneity and pleiotropy test results can be found in Supplementary materials 1–4.
Table 2
|
The relationship between TC, LDL, HDL levels, and the risk of CRC.
Table 3
| Mediators | Exposure | Outcome | Mediation effect in total effect | 95%CI | p value of Interactive Mediation Tests |
|---|---|---|---|---|---|
| Sterol ester (27:1/14:0) | Total cholesterol | Colorectal cancer | 87.9% | 41.8~134.0% | 0.000 |
| LDL cholesterol | Colorectal cancer | 93.3% | 44.6~141.9% | 0.000 | |
| Sterol ester (27:1/16:0) | Total cholesterol | Colorectal cancer | 44.3% | 3.3~85.4% | 0.033 |
| LDL cholesterol | Colorectal cancer | 44.6% | 2.5~86.7% | 0.036 |
Proportion of the association between TC or LDL and CRC mediated by sterol ester (27:1/14:0) and sterol ester (27:1/16:0).
3 Discussion
Dyslipidemia has been found to be significantly associated with various types of cancers. A study focusing on the relationship between dyslipidemia and breast cancer revealed a notably higher prevalence of dyslipidemia among breast cancer patients compared to both healthy individuals and those with benign breast disease. Specifically, levels of TC, triglycerides, and LDL cholesterol were markedly elevated in the breast cancer cohort in comparison to individuals with benign breast disease and healthy controls, with the exception of high-density lipoprotein (HDL) cholesterol (11). Furthermore, high levels of HDL-C and apolipoproteins A1 (apoA1) have been shown to potentially decrease the risk of developing breast cancer (12).
Research on hyperlipidemia and its association with bladder cancer has revealed that individuals with this condition, particularly young adult men, are at an increased risk for developing bladder cancer (13). Furthermore, patients with hyperlipidemia are also more susceptible to colon, prostate, and testicular cancer (3). Additionally, elevated levels of cholesterol have been linked to a higher risk of ovarian cancer, while high levels of HDL-C have shown a protective effect against this type of cancer (14). Studies have also demonstrated that TC and LDL levels are correlated with an elevated risk of CRC (4, 5), whereas higher levels of serum HDL are associated with a decreased risk of colon cancer (15).
TC is composed of free cholesterol and various cholesterol esters (6). Within lipoproteins, VLDL contains 12–15% cholesteryl esters and 8–10% cholesterol, while IDL contains 32–35% cholesteryl esters and 8–10% cholesterol. LDL, smaller than IDL, harbors 37–48% cholesteryl esters and 8–10% cholesterol. HDL contains 15–30% cholesteryl esters and 2–10% cholesterol (7). The specific lipid species that may impact CRC risk remain unclear.
This study examined the correlation between 179 plasma lipid species and the likelihood of developing CRC, encompassing 16 sterols (ST), 15 sphingolipids (SL), 44 glycerolipids (GL), and 104 glycerophospholipids (GP) (6).
To ensure the accuracy of the results, we predominantly utilized MR analysis as our methodological approach. MR is a sophisticated technique that leverages genetic variants as instrumental variables to deduce causal relationships, primarily employed to examine the associations between genetic variations and diseases. The pertinent data are chiefly concerned with the presence or absence of diseases. In comparison to traditional observational studies, MR offers substantial advantages by effectively mitigating biases arising from confounding factors and reverse causation, thereby facilitating more accurate causal inferences (16, 17). These confounding factors include variables such as gender, age, and environmental influences, which are often challenging to fully control in observational studies (18). Furthermore, MR enhances the reliability of causal inference through various methodologies. For example, the implementation of two-sample MR, bidirectional MR, and network MR enables researchers to confirm the robustness of causal relationships across diverse research contexts and to investigate potential pleiotropic pathways (17, 19). MR is a powerful tool for causal inference, effectively evaluating a risk factor’s impact on disease outcomes. It surpasses traditional observational studies’ limitations and offers crucial insights into the causal mechanisms of complex diseases.
In this study, bidirectional MR analysis was primarily utilized to mitigate the potential for reverse causation, thereby ensuring the validity of the results. Additionally, to enhance the robustness of the findings, we employed GWAS data on colorectal cancer from four European cohorts, identifying 25 lipid species potentially associated with colorectal cancer risk. To further ensure the precision and reliability of the results, a meta-analysis was conducted on the MR analysis outcomes from the four datasets.
Ultimately, our study identified a positive association between the levels of two cholesterol esters, sterol ester (27:1/14:0) and sterol ester (27:1/16:0), and the risk of CRC across all cohorts. The meta-analysis results also indicated statistical significance with p values less than 0.05.
Subsequent analysis revealed that sterol ester (27:1/14:0) and sterol ester (27:1/16:0), act as mediating factors in the relationship between TC and LDL levels and the risk of CRC. Given the significant physiological roles of lipids in human biology, focusing on specific lipids rather than all lipids in areas such as diet, nutrition, and therapeutic interventions may be a better strategy.
Limitations and deficiencies: This study found two lipid species linked to CRC risk, but did not have enough evidence to draw conclusions about other lipid components. For instance, certain lipid have been linked to CRC risk in one cohort but not in others. Further research is needed to understand their specific relationship to the disease. Some lipid species were suggested to be associated with CRC risk in multiple cohorts, but the meta-analysis did not show statistical significance, particularly for Phosphatidylcholine (O-16:1_18:0) and Phosphatidylcholine (18:1_20:3) with a p value of 0.052 and 0.050. More investigation is needed to determine their relationship with CRC risk.
4 Methods
4.1 Study design
This study initially examined the correlation between 179 lipid species and the risk of CRC across multiple cohorts using a two-sample Mendelian randomization (MR) approach. Subsequently, a meta-analysis was conducted to further clarify the association between lipids and CRC risk, while also investigating the possibility of reverse causation through reverse MR. Finally, a two-step Mendelian randomization method was employed to assess whether the identified lipids acted as mediators in the relationship between TC and LDL cholesterol levels and the risk of CRC.
4.2 Data sources
The Genome-wide association studies (GWAS) data for 179 lipid species in the Finnish population were sourced from Ottensmann et al. (6), while data on TC, LDL, and HDL levels were obtained from Sakaue et al. (20). Additionally, nearly 5 years of GWAS data on CRC were downloaded from the IEU database1 (21), with the exclusion of data from the FinnGen dataset to prevent population duplication. Further GWAS data on CRC from Taliun D et al. (22) were also utilized, all of which pertained to European populations. Specific details regarding the data can be found in Table 4. Because ebi-a-gcst90013862 and ebi-a-gcst90013866 are resulting from distinct correction methods applied to the same population, only the cohort ebi-a-GCST90013866 was chosen for analysis. Details of all data including 179 lipid species, cholesterol, and colorectal cancer can be found in Supplementary materials 5–7.
Table 4
| Trait | ID | Population | Sample size | Year | Author |
|---|---|---|---|---|---|
| Total cholesterol | ebi-a-GCST90018974 | European | 344,278 | 2021 | Sakaue S |
| HDL cholesterol | ebi-a-GCST90018956 | European | 315,133 | 2021 | Sakaue S |
| LDL cholesterol | ebi-a-GCST90018961 | European | 343,621 | 2021 | Sakaue S |
| Colorectal cancer | ebi-a-GCST90018808 | European | 470,002 | 2021 | Sakaue S |
| ieu-b-4965 | European | 377,673 | 2021 | Burrows | |
| ebi-a-GCST90013862 | European | 407,746 | 2021 | Mbatchou J | |
| ebi-a-GCST90013866 | European | 407,746 | 2021 | Mbatchou J | |
| ukb-saige-153 | European | 387,318 | 2021 | Taliun D |
Summary of the data sets.
4.3 Selection of IV
In the Mendelian randomization (MR) analysis conducted in this study, SNPs that met the genome-wide significance threshold (p < 5 × 10–6) and exhibited no linkage disequilibrium (LD) with other SNPs (r2 < 0.001 within a 10,000 kb clumping window) were utilized as IV for the exposures. In the reverse MR analysis, SNPs meeting the genome-wide significance threshold (p < 5 × 10–8) and displaying no LD with other SNPs (r2 < 0.001 within a 10,000 kb clumping window) were employed as IV for the exposures. Outliers that may influence causal effects in the MR-PRESSO global test were identified and eliminated (23), along with SNPs associated with the outcome at a significance level of p < 5 × 10–5. Furthermore, the Steiger test method was employed to identify SNPs showing stronger associations with the outcome variable relative to the exposure variable, and these SNPs were also excluded from the analysis.
4.4 Sensitivity analysis
The study utilized the χ2 Q test to evaluate the diversity in causal impacts of various variants, where a significance level below 0.05 denoted heterogeneity. Additionally, the MR-Egger intercept analysis was employed to investigate horizontal pleiotropy, a condition in which IV affect both the exposure and outcome through a non-causal route. The findings revealed no substantial indication of horizontal pleiotropy (MR-Egger intercept <0.01, p-value >0.05).
4.5 Mediation analysis
In order to assess the extent to which relevant lipids mediate the relationship between TC or LDL and the risk of CRC, a two-step Mendelian randomization (MR) method was employed. The total effect was partitioned into an indirect effect (mediated by lipids) and a direct effect (not mediated by lipids) (24). The proportion of mediation was determined by dividing the indirect effect by the total effect (Figure 3).
Figure 3
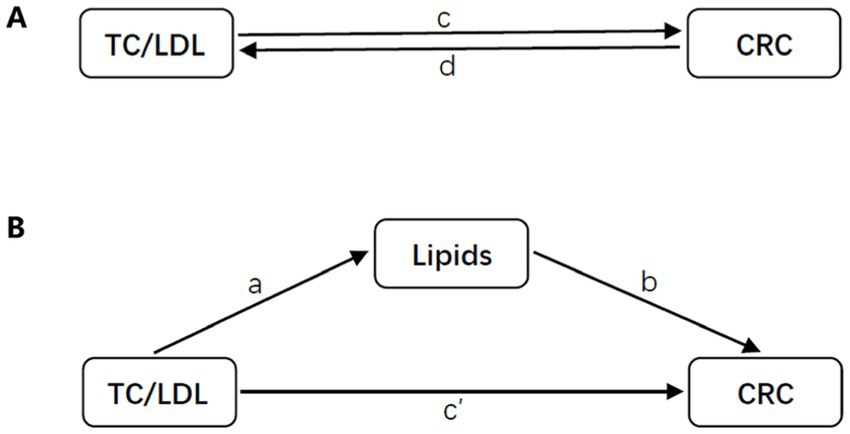
Diagrams illustrating associations examined in this study. (A) The total effect between TC or LDL and CRC. The total effect is represented by c when genetically predicted TC or LDL is the exposure and CRC is the outcome, and by d when genetically predicted CRC is the exposure and TC or LDL is the outcome. (B) The total effect was further analyzed by decomposing it into indirect effects using a two-step approach (where a represents the total effect of TC or LDL on CRC, and b represents the effect of CRC on TC or LDL) and the product method (a × b), as well as direct effects (c′ = c – a × b). The proportion mediated was calculated by dividing the indirect effect by the total effect.
4.6 Statistical analysis
We utilized R (version 4.3.0) along with the packages “TwoSampleMR,” “MendelR,” and “MRPRESSO” for conducting all Mendelian randomization (MR) and meta-analyses. The inverse variance weighted (IVW) method served as our primary MR approach (25), complemented by additional methods such as MR Egger, Weighted Median, and Weighted Mode. The IVW method was employed in the absence of heterogeneity, while the IVW (multiplicative random effects) method was utilized in cases of heterogeneity. In instances of pleiotropic effects, preference was given to the MR Egger method over IVW. A random effects model was used for the meta-analysis due to data heterogeneity. A significance level of p < 0.05 was considered statistically significant for all analyses.
Statements
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
YW: Conceptualization, Data curation, Writing – original draft, Writing – review & editing. TW: Writing – original draft. XS: Data curation, Writing – review & editing. ZZ: Conceptualization, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by Scientific Research of the First Affiliated Hospital of Jinzhou Medical University (No. FYKRGG-202305), Project of Jinzhou Medical University (No. 307202402031), Jinzhou Science and Technology Department project fund (No. JZ2023B073), Joint Science and Technology Program of Liaoning Provincial Science and Technology Department (No. 2024-MSLH-130) and Key Program of Liaoning Provincial Education Department (No. 307202402006).
Acknowledgments
We thank all data providers and appreciate the funding sponsorship from Science and Technology Department and Education Department of Liaoning Province, Jinzhou Medical University, Jinzhou Science and Technology Bureau.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2025.1453523/full#supplementary-material
Abbreviations
CRC, Colorectal cancer; TC, Total cholesterol; LDL, Low-density lipoprotein; SNPs, Single nucleotide polymorphisms; IV, Instrumental variables.
Footnotes
References
1.
Sung H Ferlay J Siegel RL Laversanne M Soerjomataram I Jemal A et al . Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660
2.
Siegel RL Miller KD Wagle NS Jemal A . Cancer statistics, 2023. CA Cancer J Clin. (2023) 73:17–48. doi: 10.3322/caac.21763
3.
Radišauskas R Kuzmickienė I Milinavičienė E Everatt R . Hypertension, serum lipids and cancer risk: a review of epidemiological evidence. Medicina. (2016) 52:89–98. doi: 10.1016/j.medici.2016.03.002
4.
Rodriguez-Broadbent H Law PJ Sud A Palin K Tuupanen S Gylfe A et al . Mendelian randomisation implicates hyperlipidaemia as a risk factor for colorectal cancer. Int J Cancer. (2017) 140:2701–8. doi: 10.1002/ijc.30709
5.
Cornish AJ Law PJ Timofeeva M Palin K Farrington SM Palles C et al . Modifiable pathways for colorectal cancer: a mendelian randomisation analysis. Lancet Gastroenterol Hepatol. (2020) 5:55–62. doi: 10.1016/S2468-1253(19)30294-8
6.
Ottensmann L Tabassum R Ruotsalainen SE Gerl MJ Klose C Widén E et al . Genome-wide association analysis of plasma lipidome identifies 495 genetic associations. Nat Commun. (2023) 14:6934. doi: 10.1038/s41467-023-42532-8
7.
Korber M Klein I Daum G . Steryl ester synthesis, storage and hydrolysis: a contribution to sterol homeostasis. Biochim Biophys Acta Mol Cell Biol Lipids. (2017) 1862:1534–45. doi: 10.1016/j.bbalip.2017.09.002
8.
Zuccolo L Holmes MV . Commentary: Mendelian randomization-inspired causal inference in the absence of genetic data. Int J Epidemiol. (2017) 46:962–5. doi: 10.1093/ije/dyw327
9.
Richmond RC Davey SG . Mendelian randomization: concepts and scope. Cold Spring Harb Perspect Med. (2022) 12:a040501. doi: 10.1101/cshperspect.a040501
10.
Davies NM Holmes MV Davey SG . Reading Mendelian randomisation studies: a guide, glossary, and checklist for clinicians. BMJ. (2018) 362:k601. doi: 10.1136/bmj.k601
11.
Chowdhury FA Islam MF Prova MT Khatun M Sharmin I Islam KM et al . Association of hyperlipidemia with breast cancer in Bangladeshi women. Lipids Health Dis. (2021) 20:52. doi: 10.1186/s12944-021-01480-2
12.
His M Zelek L Deschasaux M Pouchieu C Kesse-Guyot E Hercberg S et al . Prospective associations between serum biomarkers of lipid metabolism and overall, breast and prostate cancer risk. Eur J Epidemiol. (2014) 29:119–32. doi: 10.1007/s10654-014-9884-5
13.
Shih HJ Lin KH Wen YC Fan YC Tsai PS Huang CJ . Increased risk of bladder cancer in young adult men with hyperlipidemia: a population-based cohort study. Medicine (Baltimore). (2021) 100:e28125. doi: 10.1097/MD.0000000000028125
14.
Zhang D Xi Y Feng Y . Ovarian cancer risk in relation to blood lipid levels and hyperlipidemia: a systematic review and meta-analysis of observational epidemiologic studies. Eur J Cancer Prev. (2021) 30:161–70. doi: 10.1097/CEJ.0000000000000597
15.
van Duijnhoven FJ Bueno-De-Mesquita HB Calligaro M Jenab M Pischon T Jansen EHJM et al . Blood lipid and lipoprotein concentrations and colorectal cancer risk in the European prospective investigation into Cancer and nutrition. Gut. (2011) 60:1094–102. doi: 10.1136/gut.2010.225011
16.
Nguyen K Mitchell BD . A guide to understanding Mendelian randomization studies. Arthritis Care Res. (2024) 76:1451–60. doi: 10.1002/acr.25400
17.
Davey Smith G Hemani G . Mendelian randomization: genetic anchors for causal inference in epidemiological studies. Hum Mol Genet. (2014) 23:R89–98. doi: 10.1093/hmg/ddu328
18.
Larsson SC . Mendelian randomization as a tool for causal inference in human nutrition and metabolism. Curr Opin Lipidol. (2021) 32:1–8. doi: 10.1097/MOL.0000000000000721
19.
Zhang Y Ou G Li R Peng L Shi J . Causal relationship between benign prostatic hyperplasia and prostate cancer: a bidirectional Mendelian randomization analysis. Postgrad Med J. (2024). doi: 10.1093/postmj/qgae163
20.
Sakaue S Kanai M Tanigawa Y Karjalainen J Kurki M Koshiba S et al . A cross-population atlas of genetic associations for 220 human phenotypes. Nat Genet. (2021) 53:1415–24. doi: 10.1038/s41588-021-00931-x
21.
Hemani G Zheng J Elsworth B Wade KH Haberland V Baird D et al . The MR-base platform supports systematic causal inference across the human phenome. eLife. (2018) 7:34408. doi: 10.7554/eLife.34408
22.
Taliun D Harris DN Kessler MD Carlson J Szpiech ZA Torres R et al . Sequencing of 53,831 diverse genomes from the NHLBI TOPMed program. Nature. (2021) 590:290–9. doi: 10.1038/s41586-021-03205-y
23.
Ong JS MacGregor S . Implementing MR-PRESSO and GCTA-GSMR for pleiotropy assessment in Mendelian randomization studies from a practitioner's perspective. Genet Epidemiol. (2019) 43:609–16. doi: 10.1002/gepi.22207
24.
Carter AR Sanderson E Hammerton G Richmond RC Davey Smith G Heron J et al . Mendelian randomisation for mediation analysis: current methods and challenges for implementation. Eur J Epidemiol. (2021) 36:465–78. doi: 10.1007/s10654-021-00757-1
25.
Burgess S Butterworth A Thompson SG . Mendelian randomization analysis with multiple genetic variants using summarized data. Genet Epidemiol. (2013) 37:658–65. doi: 10.1002/gepi.21758
Summary
Keywords
lipids, colorectal cancer, Mendelian randomization, cancer risk, cholesterol
Citation
Wang Y, Wang T, Shen X and Zhu Z (2025) The main mediating lipid species in cholesterol-induced colorectal cancer risk. Front. Nutr. 12:1453523. doi: 10.3389/fnut.2025.1453523
Received
23 June 2024
Accepted
11 March 2025
Published
16 May 2025
Volume
12 - 2025
Edited by
Lian-Ping He, Taizhou University, China
Reviewed by
Fangliang Zhang, University of Miami, United States
Miljana Z. Jovandaric, University of Belgrade, Serbia
Updates
Copyright
© 2025 Wang, Wang, Shen and Zhu.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhitu Zhu, zhuzhitu@jzmu.edu.cn
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.