 Mohamed Ali Boujelbane1,2†
Mohamed Ali Boujelbane1,2† Achraf Ammar1,2,3,4*†‡
Achraf Ammar1,2,3,4*†‡ Atef Salem1,2
Atef Salem1,2 Mohamed Kerkeni2,5
Mohamed Kerkeni2,5 Khaled Trabelsi4,5
Khaled Trabelsi4,5 Bassem Bouaziz6,7
Bassem Bouaziz6,7 Liwa Masmoudi2
Liwa Masmoudi2 Juliane Heydenreich8Christiana Schallhorn9
Juliane Heydenreich8Christiana Schallhorn9 Gabriel Müller1Ayse Merve Uyar1
Gabriel Müller1Ayse Merve Uyar1 Hadeel Ali Ghazzawi10
Hadeel Ali Ghazzawi10 Adam Tawfiq Amawi4
Adam Tawfiq Amawi4 Bekir Erhan Orhan11Giuseppe Grosso12
Bekir Erhan Orhan11Giuseppe Grosso12 Osama Abdelkarim13,14
Osama Abdelkarim13,14 Tarak Driss15
Tarak Driss15 Kais El Abed2,5
Kais El Abed2,5 Piotr Zmijewski16Nasreddine Benbettaieb17,18Clément Poulain18Laura Reyes19
Piotr Zmijewski16Nasreddine Benbettaieb17,18Clément Poulain18Laura Reyes19 Amparo Gamero20
Amparo Gamero20 Marta Cuenca-Ortolá20
Marta Cuenca-Ortolá20 Nicola Francesca21
Nicola Francesca21 Concetta Maria Messina22Björn Lorenzen23Stefania Filice23Aadil Bajoub24
Concetta Maria Messina22Björn Lorenzen23Stefania Filice23Aadil Bajoub24 El-Mehdi Ajal24,25El Amine Ajal26Majdouline Obtel25
El-Mehdi Ajal24,25El Amine Ajal26Majdouline Obtel25 Sadjia Lahiani27
Sadjia Lahiani27 Taha Khaldi28
Taha Khaldi28 Nafaa Souissi2
Nafaa Souissi2 Omar Boukhris29,30
Omar Boukhris29,30 Haitham Jahrami31,32
Haitham Jahrami31,32 Waqar Husain33
Waqar Husain33 Walid Mahdi6,7
Walid Mahdi6,7 Hamdi Chtourou2
Hamdi Chtourou2 Wolfgang I. Schöllhorn1
Wolfgang I. Schöllhorn1- 1Department of Training and Movement Science, Institute of Sport Science, Johannes Gutenberg-University Mainz, Mainz, Germany
- 2High Institute of Sport and Physical Education of Sfax, University of Sfax, Sfax, Tunisia
- 3Research Laboratory, Molecular Bases of Human Pathology, LR19ES13, Faculty of Medicine of Sfax, University of Sfax, Sfax, Tunisia
- 4Department of Movement Sciences and Sports Training, School of Sport Science, The University of Jordan, Amman, Jordan
- 5Research Laboratory Education, Motricity, Sport and Health, EM2S, LR19JS01, High Institute of Sport and Physical Education of Sfax, University of Sfax, Sfax, Tunisia
- 6Multimedia InfoRmation systems and Advanced Computing Laboratory (MIRACL), University of Sfax, Sfax, Tunisia
- 7Higher Institute of Computer Science and Multimedia of Sfax (ISIMS), University of Sfax, Sfax, Tunisia
- 8Faculty of Sports Sciences, Department of Experimental Sports Nutrition, Leipzig University, Leipzig, Germany
- 9Department of Sports Economics, Sociology and History, Institute of Sport Science, Johannes Gutenberg-University Mainz, Mainz, Germany
- 10Department of Nutrition and Food Technology, School of Agriculture, The University of Jordan, Amman, Jordan
- 11Faculty of Sports Sciences, Istanbul Aydın University, Istanbul, Türkiye
- 12Department of Biomedical and Biotechnological Sciences, University of Catania, Catania, Italy
- 13Faculty of Sport Sciences, Assiut University, Assiut, Egypt
- 14ESLSCA University Egypt, Giza, Egypt
- 15Interdisciplinary Laboratory in Neurosciences, Physiology and Psychology Physical Activity, Health and Learning (LINP2), UFR STAPS, Paris Nanterre University, Nanterre, France
- 16Department of Biomedical Sciences, Jozef Pilsudski University of Physical Education in Warsaw, Warsaw, Poland
- 17Department BioEngineering, Institut Universitaire de Technologie IUT-Dijon-Auexrre-Nevers, University Burgundy Europe, Dijon, France
- 18Joint Research Unit UMR PAM-PCAV (Physical-Chemistry of Food and Wine Laboratory), Université Bourgogne Europe/Institut AgroDijon/INRAE, Dijon, France
- 19Vitagora Innovation Cluster, Dijon, France
- 20Department of Preventive Medicine and Public Health, Food Science, Toxicology and Forensic Medicine, Faculty of Pharmacy & Food Sciences, University of Valencia, Valencia, Spain
- 21Department of Agricultural Food and Forest Sciences, University of Palermo, Palermo, Italy
- 22Laboratory of Marine Biochemistry and Ecotoxicology, Department of Earth and Marine Sciences DiSTeM, University of Palermo, Trapani, Italy
- 23Microtarians Academy, Luxembourg, Luxembourg
- 24Laboratory of Food and Food By-Products Chemistry and Processing Technology, National School of Agriculture in Meknès, Meknès, Morocco
- 25Laboratory of Social Medicine, Faculty of Medicine and Pharmacy of Rabat, Department of Epidemiology and Public Health, Mohammed V University, Rabat, Morocco
- 26UPR of Pharmacognosy, Faculty of Medicine and Pharmacy of Rabat, Mohammed V University, Rabat, Morocco
- 27VALCORE Laboratory, Faculty of Science, Department of Biology, University of M’hamed Bougara Boumerdes, Boumerdes, Algeria
- 28Biotechnology Research Center (C.R.Bt), Constantine, Algeria
- 29SIESTA Research Group, School of Allied Health, Human Services and Sport, La Trobe University, Melbourne, VIC, Australia
- 30Sport, Performance, and Nutrition Research Group, School of Allied Health, Human Services and Sport, La Trobe University, Melbourne, VIC, Australia
- 31Government Hospitals, Manama, Bahrain
- 32Department of Psychiatry, College of Medicine and Medical Sciences, Arabian Gulf University, Manama, Bahrain
- 33Department of Humanities, COMSATS University Islamabad, Islamabad, Pakistan
Background: The Mediterranean Diet (MedDiet) is widely recognized for its health benefits, though adherence varies across populations and is influenced by multiple lifestyle and demographic factors. This study examined MedDiet adherence patterns and their associations with lifestyle behaviors, with particular attention to gender differences in a large, multinational cohort.
Methods: Data were obtained via the MEDIET4ALL survey, an international cross-sectional study that included 4,010 participants (mean age: 36.04 ± 15.06 years; 59.5% female) across 10 countries. The evaluation of adherence to the MedDiet was conducted using the MedLife Index, a validated tool that assesses adherence to MedDiet patterns and lifestyle behaviors through three blocks: Mediterranean food consumption, MedDiet habits, and lifestyle behaviors. Additionally, validated instruments were used to measure associated factors, including perceived barriers to adherence, physical activity, sleep quality and disturbances, mental health, life satisfaction, social participation, and technology use behaviors.
Results: While total Mediterranean lifestyle (MedLife) scores showed no significant gender differences, women demonstrated better adherence to food consumption components (p < 0.001), while men showed greater physical activity and social participation. Women reported poorer sleep metrics (efficiency, latency, duration) and higher insomnia severity (all p < 0.05). Psychological distress was more prevalent among women, who also expressed greater needs for psychosocial and nutritional support (p < 0.001). The MedLifeMEDLIFE Index showed significant positive correlations with physical activity (r = 0.298), social participation (r = 0.227), and sleep satisfaction (r = 0.181), and negative correlations with mental health measures (insomnia: r = –0.137; depression: r = –0.115; stress: r = –0.089; anxiety: r = –0.076; all p < 0.001).
Conclusion: Our findings reveal distinct gender-specific patterns in MedDiet adherence and associated lifestyle factors. These results underscore the need for differentiated public health approaches that address the unique behavioral and psychosocial needs of men and women to promote MedLife adoption.
1 Introduction
In recent years, scientific interest in dietary patterns impacting global health has surged, with a focus on traditional diets linked to significant reductions in cardiovascular mortality and chronic disease risk (1, 2). Among these, the Mediterranean Diet (MedDiet) is the most extensively studied and is recognized for its association with increased longevity and reduced incidence of type 2 diabetes, neurodegenerative diseases, and certain cancers (3, 4). Originating from the work of Ancel Keys in the Seven Countries Study (5), the MedDiet reflects the traditional eating habits of Mediterranean regions in the 1960s—a period marked by low incidence of diet-related diseases and high life expectancy (6, 7).
Martínez-González et al. (8) described how the MedDiet prioritizes plant-based foods such as fruits, vegetables, whole cereals, legumes, and seeds, with olive oil as the primary fat source - a pattern now shown to reduce systemic inflammation and oxidative stress (9). Red meat and refined foods are consumed in moderation, while poultry, fish, dairy, and moderate red wine consumption complete this dietary pattern, contributing to its distinctive cultural dimension and cardioprotective effects (10).
The health benefits of the MedDiet are supported by a substantial body of research, including population-based studies and clinical trials (11, 12). Notably, the PREDIMED study demonstrated a 30% reduction in major cardiovascular events among those who adhered to a MedDiet supplemented with extra-virgin olive oil or walnuts (8, 13). Systematic reviews and meta-analyses have shown the MedDiet’s impact on reducing risks of various chronic diseases, including obesity (12, 14), hypertension (15), metabolic syndrome (16), cardiovascular diseases (17), neurodegenerative disorders (18), and specific cancers (19).
The MedDiet is valued for its protective role against non-communicable diseases, attributed to its high fiber content, low glycemic index, and abundance of antioxidant and anti-inflammatory compounds (4). However, globalization, urbanization, and Western dietary influences, characterized by ultra-processed foods, refined sugars, and unhealthy fats, have led to a decline in adherence to the MedDiet, both in Mediterranean and non-Mediterranean regions (20, 21). Economic challenges, lifestyle changes, and a preference for convenience foods over traditional home-cooked meals have particularly affected younger generations (22–24).
Adherence to the MedDiet is influenced by socio-demographic factors, including socioeconomic status, education level, and employment type (25). Studies indicate that lower socioeconomic status is associated with higher consumption of refined cereals and added fats, while higher socioeconomic groups show greater consumption of fruits, vegetables and whole grains (26). Barriers such as financial constraints, limited access to nutritious foods, and disparities in dietary knowledge affect adherence, particularly in economically disadvantaged communities (27).
Despite well-documented health benefits, research on gender differences in MedDiet adherence remains inconclusive. While some studies show women have greater adherence due to higher intake of plant-based foods (28), others report no significant gender differences (29). These contradictory findings suggest complex interactions between biological, psychological and cultural factors that require further analysis.
As part of the broader MEDIET4ALL PRIMA project supported by the European Union, which aims to promote the MedDiet and its lifestyle as a sustainable and health-focused model (30), this study aimed to evaluate adherence to the MedDiet and associated lifestyle behaviors within a large, diverse survey population. Using an evidence-based approach, the study established adherence thresholds based on percentiles derived from the surveyed population while examining gender-specific patterns and exploring relationships between adherence scores and lifestyle parameters.
2 Materials and methods
2.1 Survey design and participant recruitment
An international online survey, known as the MEDIET4ALL survey, was conducted in multiple languages to examine adherence to the MedDiet and associated lifestyle behaviors. The survey was developed by a multidisciplinary team of researchers in public health, nutrition, psychology, and social sciences, who used validated instruments to ensure cultural sensitivity and reliability. Items without official translations underwent rigorous translation and back-translation processes, ensuring high test–retest reliability coefficients (r = 0.81–0.94) for all translated items. The survey was disseminated across ten Mediterranean and neighboring countries (Germany, France, Italy, Spain, Luxembourg, Tunisia, Algeria, Morocco, Turkey, and Jordan) during the summer of 2024 for a period of four months.
The survey initially attracted more than 8,000 participants from various regions. After screening for validity and completeness, 4,010 responses were included in the final analysis (Figure 1). Survey completeness was evaluated by ensuring that only fully completed responses were retained, while those with missing data were excluded. To enhance data validity, responses underwent logic-based screening to detect inconsistencies or contradictions, such as claiming no engagement in vigorous physical activity (PA) while simultaneously reporting daily participation in such exercises. Additionally, duplicate entries were identified and removed using a combination of criteria, including matching IP addresses, closely timed submissions, and highly similar demographic and response patterns. Extreme or implausible values, such as reporting unrealistically long sleep durations (e.g., 24 h) or improbable dietary intake, were also filtered out to improve data accuracy and reliability. The survey targeted a broad, general population sample to ensure diversity and improve statistical power across analyses. The survey was hosted on the SoSci Survey platform, a “General Data Protection Regulation” (GDPR) compliant web application, with support from Johannes Gutenberg University.
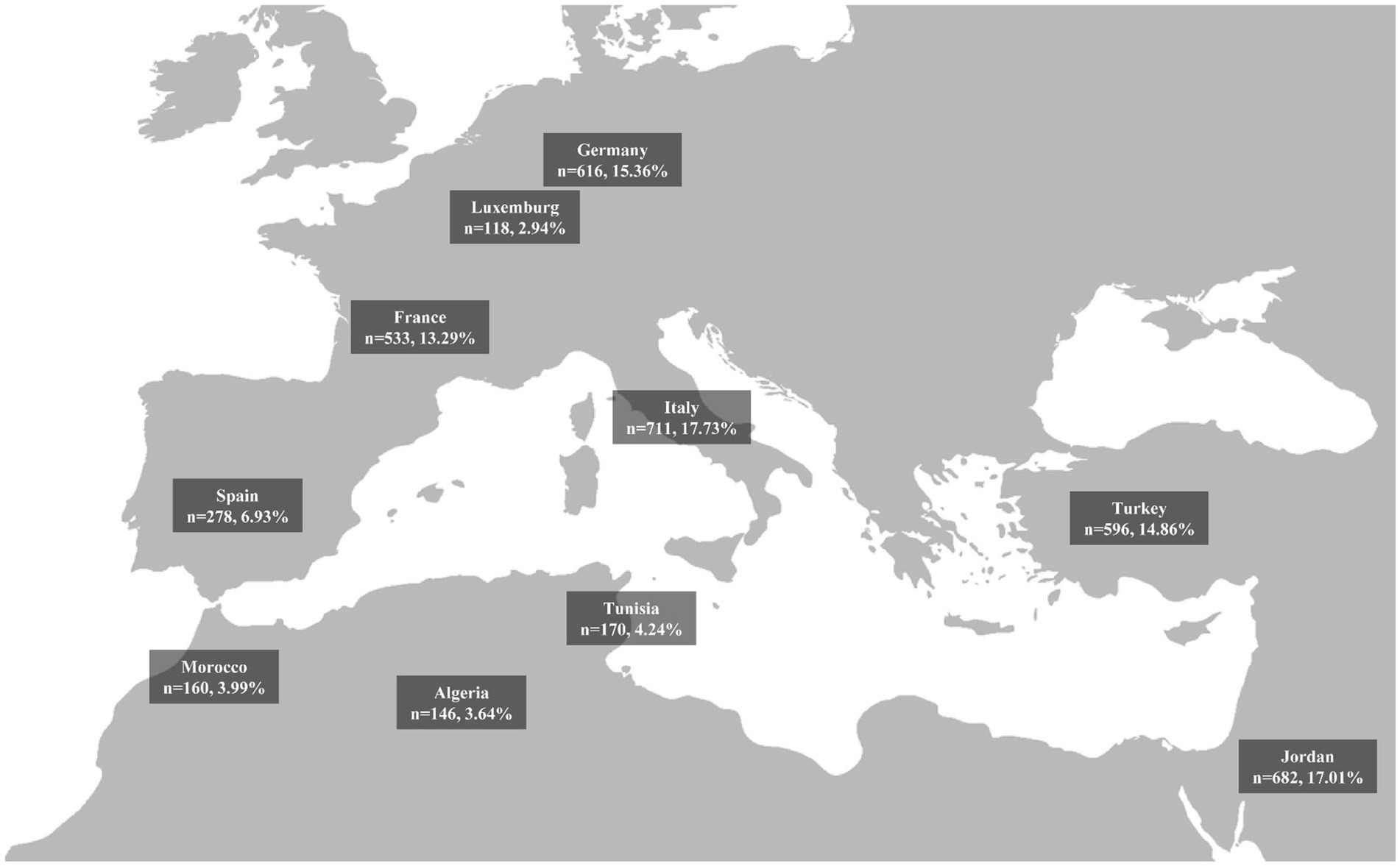
Figure 1. Geographical distribution and sample sizes of study participants from selected mediterranean and non-mediterranean countries.
The MEDIET4ALL survey aimed to provide a comprehensive understanding of dietary adherence and lifestyle patterns by collecting data on demographic and behavioral factors, including dietary behaviors, PA, social participation, sleep quality, mental health, and socio-demographic characteristics. Several validated questionnaires were utilized to assess adherence to the MedDiet and related lifestyle factors, including the MedLife Index (27) for dietary adherence, and others for assessing PA (IPAQ-SF), mental health (DASS-21), and life satisfaction (SLSQ).
The survey was available in seven languages: English, German, French, Italian, Spanish, Arabic, and Turkish, ensuring accessibility for participants across various regions. The survey was disseminated by the MEDIET4ALL consortium and collaborators (e.g., Bilendi solution) through email invitations, university and consortium websites, and social media platforms such as ResearchGate™, LinkedIn™, Facebook™, WhatsApp™, and Twitter™. Additionally, the general public was encouraged to promote the survey within their personal networks.
The survey began with an introductory page that outlined the study’s background, objectives, ethics, data privacy, and consent information, with participants having the option to choose one of the seven available languages. The completion of this survey was estimated to take 15–20 min.
The study was conducted in compliance with the principles outlined in the Declaration of Helsinki, and the protocol and consent form were approved by the Ethics Committee of the Faculty of Medicine at the University of Sfax (approval identification code: 066/24).
Participation was entirely voluntary, and participants were informed that all data would be used solely for research purposes and would remain anonymous and confidential in accordance with the SoSci Survey privacy policy (www.soscisurvey.de/en/privacy). The survey adhered to the Federal Data Protection Act (BDSG) and the EU General Data Protection Regulation (GDPR). Participants were not asked to provide personally identifiable information, and their responses were recorded only upon submitting the survey. Withdrawal was permitted at any stage, with no negative consequences for participants. By completing the survey, participants provided informed consent for the anonymous use of their data for research purposes. Note: While the survey recorded binary male/female categories, we use the term ‘gender’ throughout this manuscript to reflect behavioral and sociocultural dimensions aligned with the public health approach and EU gender-sensitive research policies.
2.2 Measures and questionnaires
Demographic data—including age, biological gender, educational level, and self-rated health status—were collected alongside a comprehensive set of validated instruments to assess adherence to the MedDiet and related lifestyle factors, as outlined by Boujelbane et al. (31). All tools were selected based on their proven reliability and validity in international populations (31).
2.3 MedDiet assessment
MedLife adherence was measured using the MedLife Index, a 28-item questionnaire that evaluates three key dimensions: food consumption frequency (15 items), dietary habits (7 items), and lifestyle behaviors (6 items) (32). This tool has demonstrated good internal consistency (Cronbach’s α = 0.75) in previous validation studies (32–34). Participants were categorized into low (<12), moderate (12–16), or high (>16) adherence groups based on tertile distributions of total scores (range 0–28) (31).
2.4 Sleep evaluation
Sleep characteristics were assessed using two validated measures. First, four core components from the Pittsburgh Sleep Quality Index (PSQI) were used to examine sleep efficiency (<85% vs. ≥ 85% time asleep/time in bed), latency (<20 vs. ≥ 20 min to fall asleep), subjective quality (rated on a 4-point Likert scale), and duration (7–9 h for participants under 65 years; 7–8 h for those 65 and older) (35, 36). Second, the Insomnia Severity Index (ISI) provided a comprehensive evaluation of insomnia symptoms across seven domains, including sleep onset, maintenance, early awakening, and daytime consequences, with total scores ranging from 0–28 (37).
2.5 Mental health assessment
Psychological wellbeing was evaluated using the Depression Anxiety Stress Scales-21 (DASS-21), which contains three 7-item subscales that measure symptoms of depression, anxiety, and stress experienced during the previous week using a 4-point Likert scale (38).
2.6 Psychosocial and behavioral measures
Life satisfaction was assessed with the Short Life Satisfaction Questionnaire-Lockdown (SLSQ), a 3-item adaptation of the Satisfaction with Life Scale that uses a 7-point Likert scale (39, 40). PA patterns were quantified using the International Physical Activity Questionnaire Short Form (IPAQ-SF), which calculates weekly energy expenditure in MET-minutes across vigorous, moderate, and walking activity domains (41, 42). Social interaction patterns were evaluated with the 14-item Short Social Participation Questionnaire-Lockdowns (SSPQL), while technology usage was measured using the 3-item Short Technology-Use Questionnaire-Lockdowns (STuQL) (31, 39, 40).
2.7 Barriers to adherence
The study incorporated the MedDiet Barriers Questionnaire (MBQ), a novel 13-item tool that systematically evaluates potential adherence barriers across four domains: physiological, socioeconomic, cultural-attitudinal, and practical constraints using a dichotomous (yes/no) response format (31).
2.8 Statistical analysis
The statistical analyses were performed using SPSS version 25. The percentage presented in the tables represents the responses for males and females in each item, calculated relative to the total male and female responses. Descriptive statistics were calculated to determine the distribution of MedLife adherence categories across geo-demographic and socio-economic factors. A chi-square test of independence (χ2) was conducted to examine the relationships between gender and various categorical variables. To assess whether the distribution of participants across categorical variables differed significantly by gender, a Z-test for two proportions was conducted using the pooled variance formula, as applied in previous research [e.g., Boujelbane et al. (31)]. This test accounts for the imbalanced sample sizes between genders, with significance thresholds set at ∣Z∣ ≥ 1.96 (p < 0.05), ∣Z∣ ≥ 2.58 (p < 0.01), and ∣Z∣ ≥ 3.29 (p < 0.001) (31).
The Shapiro–Wilk test was applied to assess data normality, revealing that the data were not normally distributed. Therefore, the Mann–Whitney test was used to compare total scores between males and females. Spearman’s rank-order correlation was employed to assess the relationship between the MedLife index and other scores. The significance level for all tests was set at 5% (p < 0.05).
3 Results
This study included 4,010 participants from 10 countries, with a mean age of 37.24 ± 15.38 years overall. Females accounted for 59.5% of the sample, with a mean age of 36.04 ± 15.06 years. Males had a mean age of 39.02 ± 15.68 years.
3.1 Demographic characteristics of the participants
The demographic characteristics of the participants are presented in Table 1. The majority resided in urban areas, with no statistically significant gender-based difference in residential distribution (p = 0.756). However, a pronounced gender disparity was observed in continental representation (p < 0.001). Participants of both genders were predominantly from Europe (p < 0.001), with a higher proportion among males (p < 0.001) compared to females. Females had higher presentiveness in Asia (p < 0.001) and Africa (p < 0.01). Ethnic background also showed significant gender differences (p < 0.001). The most represented ethnic group was White/European, with a significantly higher proportion among males compared to females. This was followed by Middle Eastern/Arab participants, where females were more represented, and Turks participants, with a significantly higher proportion among males (p < 0.001).
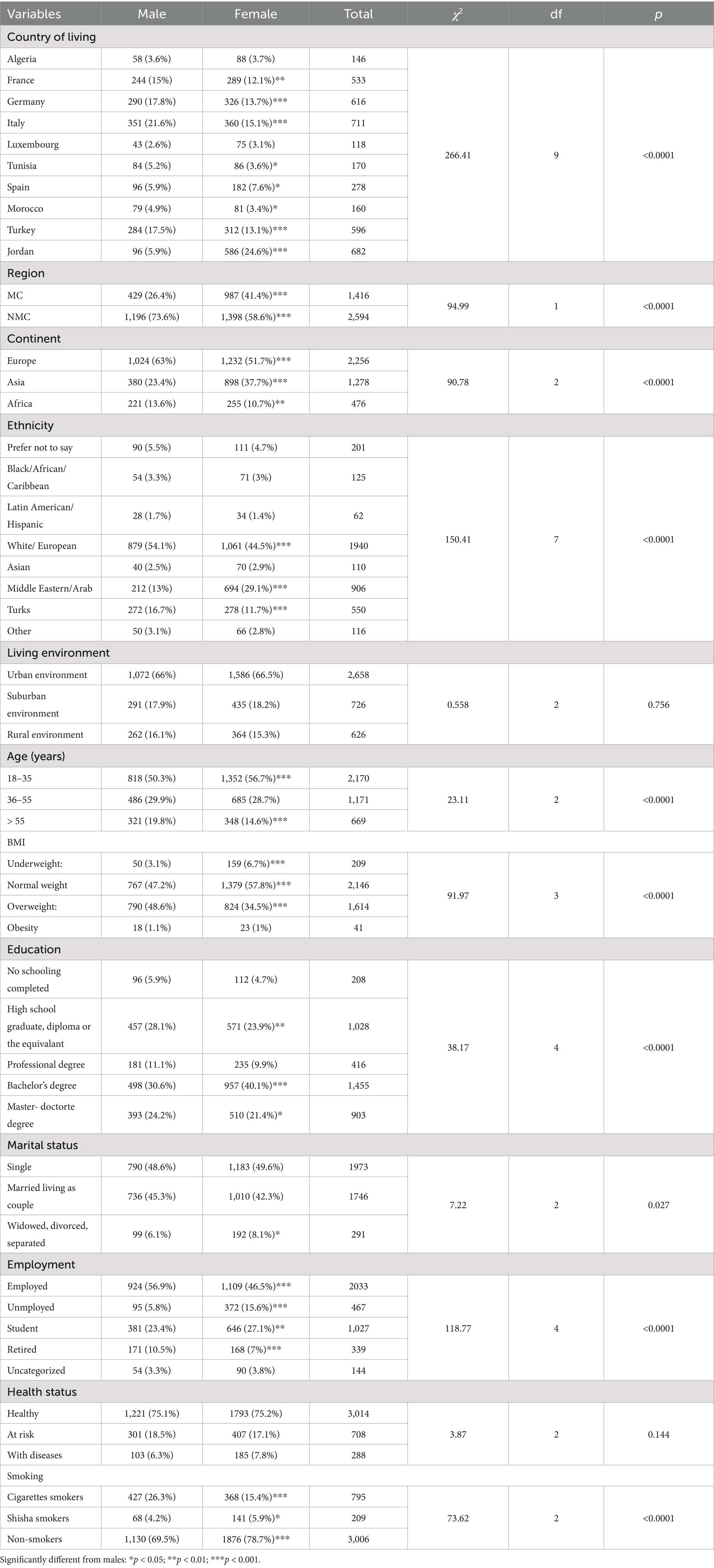
Table 1. Sociodemographic characteristics of the study population (n = 4,010) stratified by gender.
Age distribution revealed notable gender differences (p < 0.001), with the majority of respondents being young adults aged 18–35 years. Females were predominantly within this age range, while males showed higher representation among older age groups (p < 0.001).
BMI classification also indicated significant gender differences (p < 0.001). Normal weight was the most common category, particularly among females (p < 0.001). Furthermore, females were more frequently classified as underweight, whereas males had a higher prevalence of overweight (p < 0.001). Obesity rates were low in both sexes.
Educational attainment varied significantly by gender (p < 0.001). The most common categories were high school graduates, bachelor’s degree holders, and individuals with a master’s or doctoral degree. Females were more likely to have completed a bachelor’s degree (p < 0.001), while males were more frequently high school graduates (p < 0.01) and more represented among those with a master’s degree (p < 0.05). A slightly higher proportion of males also reported participation in professional training programs.
Marital status distribution differed significantly between sexes (p = 0.027), with a higher number of females reporting being widowed, divorced, or separated (p < 0.05).
Employment status also showed significant gender differences (p < 0.001). While most participants were employed, males were more likely to be employed (p < 0.001). Females were more frequently unemployed (p < 0.001) or students (p < 0.01), whereas males had higher representation in the retired category (p < 0.001).
Self-reported health status did not differ significantly by gender (p = 0.144). The majority reported being in good health, and the proportions of participants “at risk of developing a disease” or “with existing diseases” were similar across gender.
Smoking behavior showed significant gender disparities (p < 0.001). Males had a higher prevalence of cigarette smoking (p < 0.001), whereas females showed a greater prevalence of shisha smoking (p < 0.05). Overall, non-smoking was the most common behavior, with a significantly higher proportion of females identifying as non-smokers (p < 0.001).
3.2 Behavioral characteristics of the participants
3.2.1 MedLife index and perceived barriers
The Mann–Whitney analysis of the total MedLife Index score (Figure 2) revealed no significant gender differences (Z = −1.2, p = 0.219, Cohen’s d = 0.04). A more detailed analysis (Table 2) showed that in Block 1 (Mediterranean Food Consumption), females scored significantly higher than males (Z = −4.83, p < 0.001, Cohen’s d = 0.16). This difference was driven by significant differences in most parameters: out of the 15 total items, females adhered more closely to the recommended intake in 7 items (red meat, processed meat, Eggs, vegetables, olive oil, herbs/spices/garnish, potatoes; p < 0.001), while males showed higher adherence in 3 items (fish/seafood, sweets, Legumes; p = 0.001). No significant gender differences were observed in the remaining 5 items (white meat, low-fat dairy products, nuts and olives, fruit, cereals; p > 0.05).
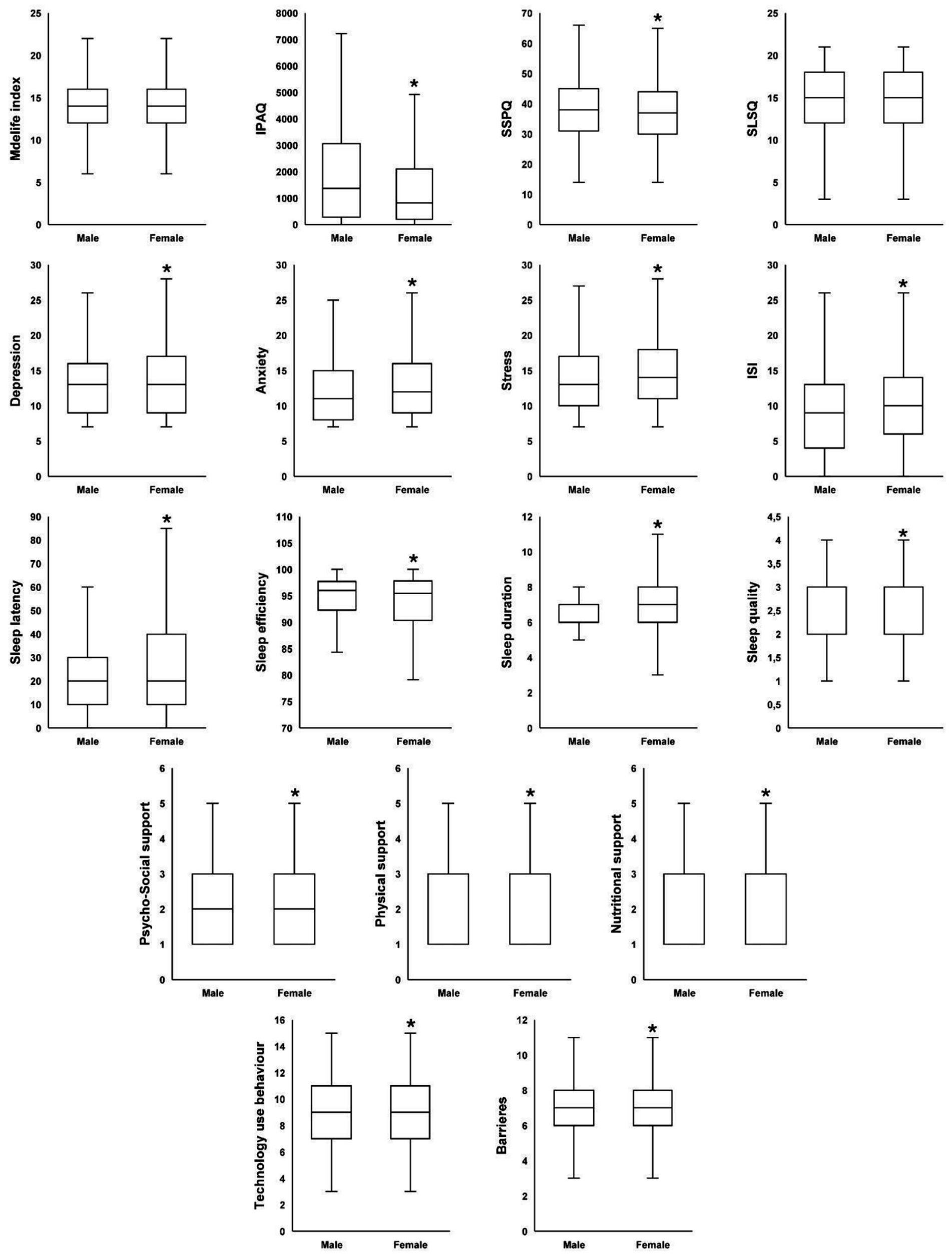
Figure 2. Gender differences in total scores for health and lifestyle parameters. SLSQ-L, short life satisfaction questionnaire; ISI, insomnia severity index; IPAQ, the international physical activity questionnaires; SSPQ-L, short social participation questionnaire; *significantly different compared to males at p < 0.05.
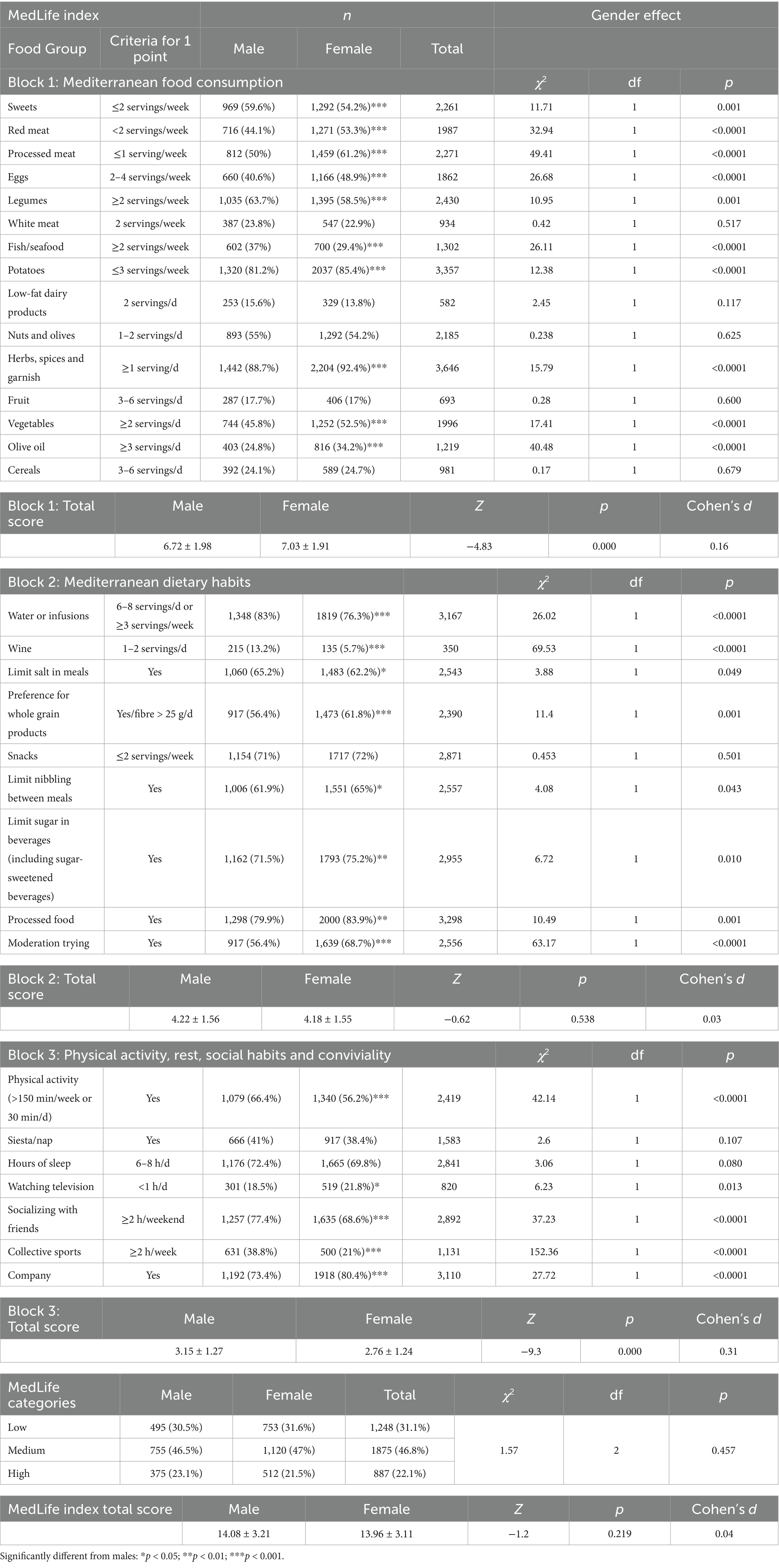
Table 2. Analysis of the MedLife Index: Mediterranean diet adherence, dietary habits, and consumption patterns by gender.
In Block 2 (Mediterranean Dietary Habits), no significant gender differences were observed in the overall score (Z = −0.62, p = 0.538, Cohen’s d = 0.03). However, a more detailed item-level analysis using the Z-test for two proportions (Table 2) revealed significant gender-specific adherence patterns. Females showed greater adherence to recommendations related to whole grain consumption (p < 0.001), limiting snacking between meals (p < 0.05), and reducing sugar intake in beverages (p < 0.01). In contrast, males demonstrated better adherence to recommendations concerning water or infusion consumption, wine intake (p < 0.001), and salt limitation (p < 0.05).
In Block 3 (PA, Rest, Social Habits, and Conviviality), males scored significantly higher than females (Z = −9.3, p < 0.001, Cohen’s d = 0.31). Out of the 6 total items, males followed the recommended activity more frequently in 3 items (PA, collective sports, socializing with friends; p < 0.001), whereas females showed higher adherence in one item (watching television; p < 0.01). No significant gender differences were found in 2 items (siesta/nap, hours of sleep; p > 0.05).
Regarding MedLife Index categories (low, medium, and high adherence; Table 2), gender had no significant impact [χ2(2, N = 4,010) = 1.57, p > 0.05]. Post-hoc analysis confirmed that there were no significant differences in the proportion of males and females across the three MedLife Index categories.
Regarding the impact of gender on perceived barriers, the Mann–Whitney test revealed that females reported significantly higher perceived barriers compared to males (Z = 2.08, p = 0.037, Cohen’s d = 0.08) (Figure 2). A more detailed analysis of gender differences for each item (Table 3) showed significant differences in five specific barriers: a higher proportion of females reported attitude-related barriers (p < 0.001), lack of knowledge (p < 0.05), and taste dislike (p < 0.001), while males reported higher proportions in low motivation (p < 0.05) and medical reasons (p < 0.001).
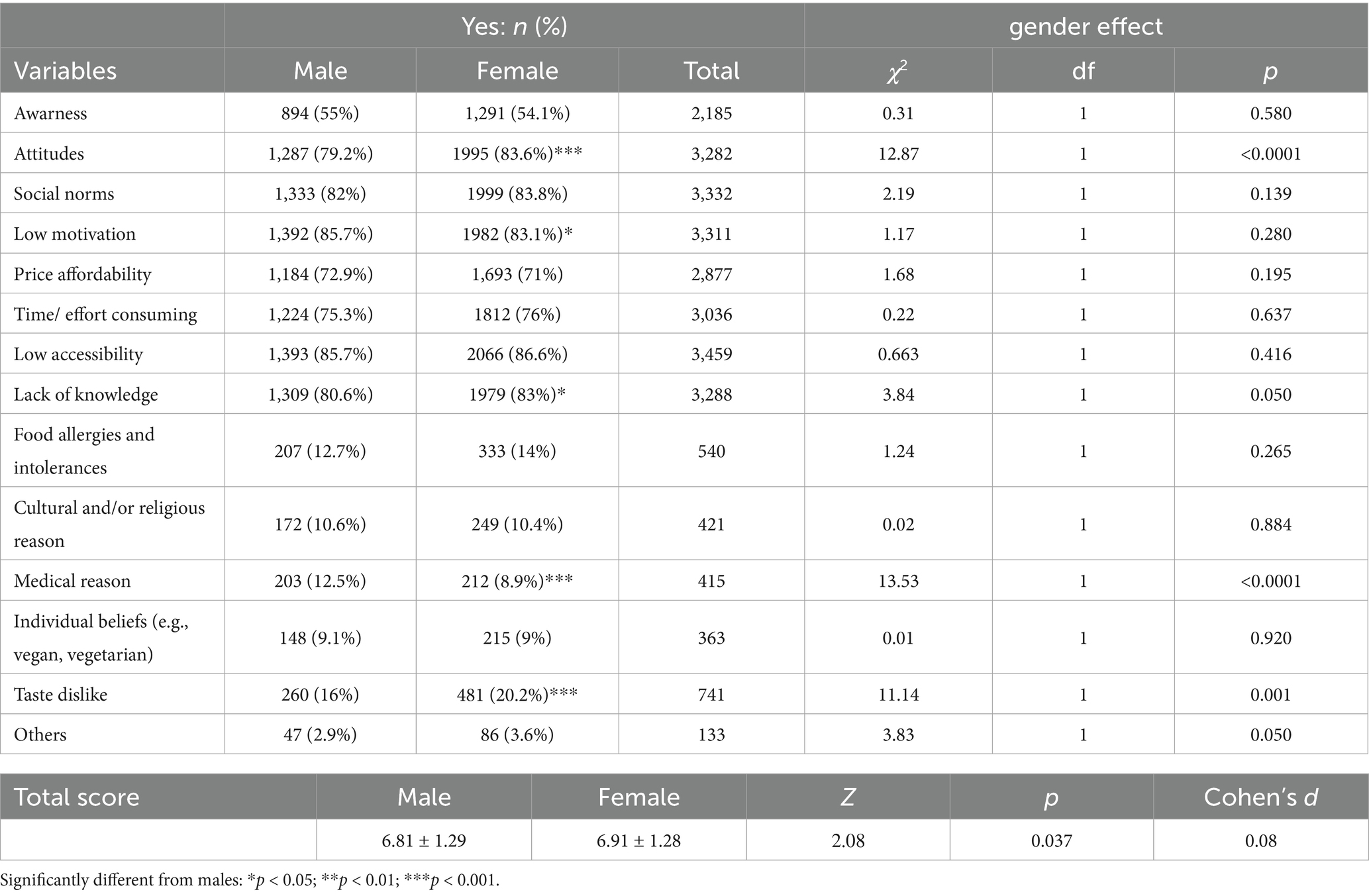
Table 3. Gender differences in awareness and potential barriers influencing their adherence to MedLife.
3.2.2 Physical and social activities, sleep patterns and use of technology behaviors
The Mann–Whitney test revealed that males had significantly higher IPAQ-SF scores than females (Z = −7.93, p < 0.001, Cohen’s d = 0.28), and scored higher on the SSPQ (Z = −2.38, p = 0.017, Cohen’s d = 3.43) indicating greater PA and social participation among this population. Regarding sleep patterns, males exhibited higher sleep efficiency (Z = −4.61, p < 0.001, Cohen’s d = 0.14), whereas females showed longer sleep latency (Z = −5.13, p < 0.001, Cohen’s d = 0.21), poorer sleep quality (Z = −2.09, p = 0.037, Cohen’s d = 0.08), longer sleep duration (Z = −2.18, p = 0.029, Cohen’s d = 0.06), and higher ISI scores (Z = −5.76, p < 0.001, Cohen’s d = 0.2). Females also reported higher overall technology use behavior (Z = −2.8, p = 0.005, Cohen’s d = 0.29) (Figure 2).
In terms of prevalences across categories, gender had no significant impact on social participation categories (Never to all times socially active), sleep duration categories (below, within, or exceeded recommendation), or sleep quality (very good to very bad) (p > 0.05) (Table 4). However, gender significantly influenced PA, sleep latency, sleep efficiency, and ISI categories (p < 0.001). Males were more physically active, as indicated by their lower proportion in the Lowly Active category and higher proportion in the Highly Active category compared to females (p < 0.001, Table 4). Additionally, males also had a lower proportion in the high (>20) sleep latency (p < 0.001), low (<85) sleep efficiency (p < 0.01), and moderate (p < 0.001) to severe (p < 0.01) insomnia categories compared to females (Table 4).
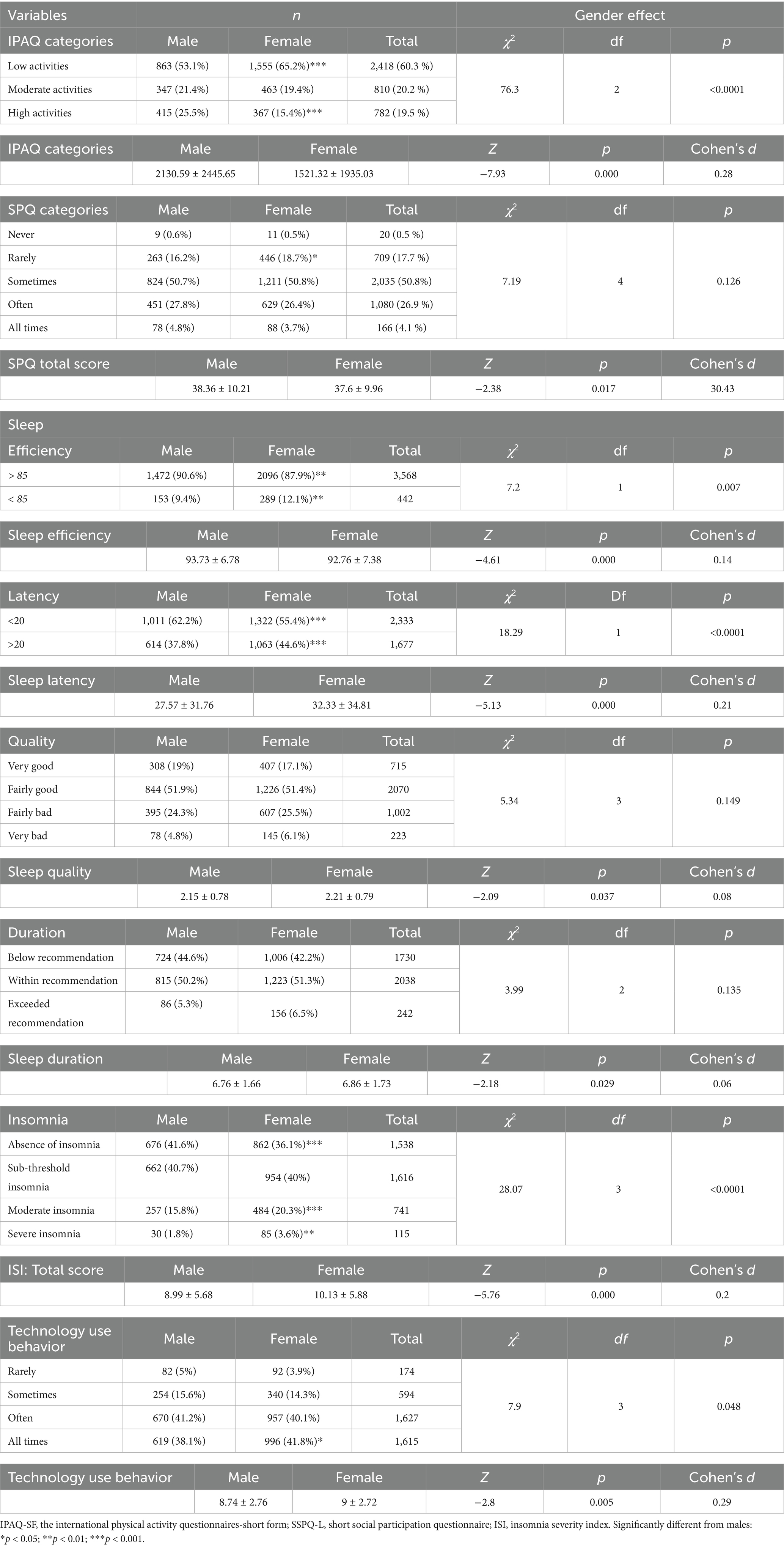
Table 4. Behavioural and sleep outcomes by gender.
3.2.3 Life satisfaction, mental health (DASS-21), and the need for psychosocial, physical, and nutritional support
Gender did not have a significant impact on overall life satisfaction scores (p > 0.05). However, significant gender differences were observed in depression, anxiety, and stress levels, as well as in the need for psycho-social, physical, and nutritional supports (p < 0.001). (Table 5).
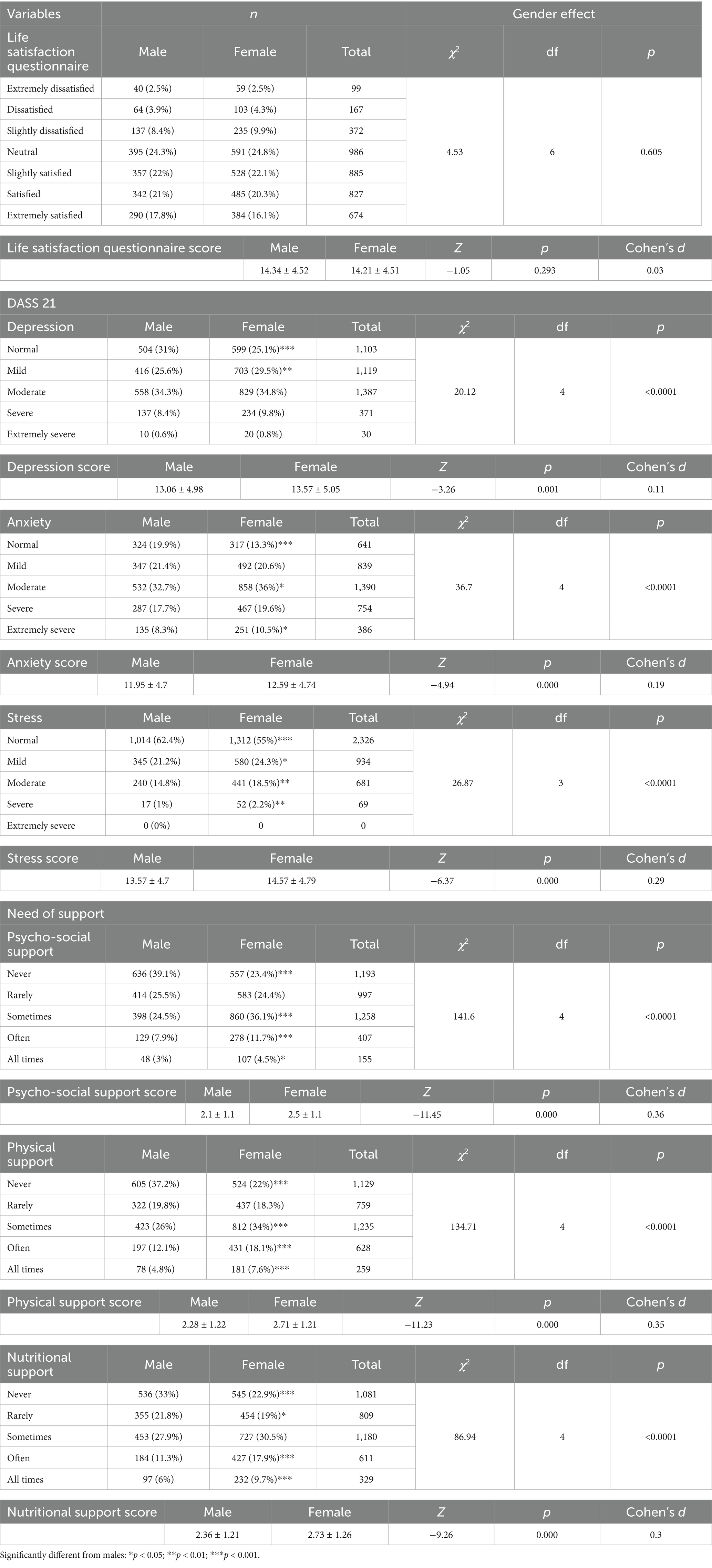
Table 5. Assessment of life satisfaction, mental health (DASS-21), and the demand for psychosocial, physical, and nutritional support.
Specifically, females reported significantly higher total scores for depression (Z = −3.26, p = 0.001, Cohen’s d = 0.11), anxiety (Z = −4.94, p < 0.001, Cohen’s d = 0.19), and stress (Z = −6.37, p < 0.001, Cohen’s d = 0.29), indicating greater psychological distress compared to males (Figure 2). Correspondingly, males had a significantly higher proportion in the normal category for depression, anxiety, and stress (p < 0.001, Table 5). Furthermore, males had a significantly lower proportion in the mild depression (p < 0.01), mild and extremely severe anxiety (p < 0.05), and mild (p < 0.05) to severe (p < 0.01) stress categories (Table 5).
Regarding the need for support, females reported significantly higher scores in psycho-social support (Z = −11.45, p < 0.001, Cohen’s d = 0.36), physical support (Z = −11.23, p < 0.001, Cohen’s d = 0.35), and nutritional support (Z = −9.26, p < 0.001, Cohen’s d = 0.3). Males, on the other hand, were significantly more likely to report no need for psycho-social support and were less likely than females to report needing such support sometimes or often (p < 0.001, Table 5). A similar pattern was observed for physical support, where males were significantly more likely to report no need for support and were less likely than females to report needing support sometimes, often, or at all times (p < 0.001, Table 5). For nutritional support, males were again significantly more likely to report no need for support and were less likely than females to report needing support often or at all times (p < 0.001, Table 5).
3.3 Correlations between MedLife index and all other parameters
The analysis revealed significant correlations between the MedLife Index and various parameters (p < 0.001). Specifically, the MedLife Index was positively correlated with the IPAQ-SF score (r = 0.298), indicating that higher levels of PA are associated with better lifestyle quality. Additionally, significant positive correlations were observed with sleep satisfaction (r = 0.181) and perceived social support (r = −0.227). Conversely, the MedLife Index demonstrated significant negative correlations with insomnia severity (r = −0.137), stress levels (r = −0.089), anxiety (r = −0.076), and depression (r = −0.115). These results are presented in (Figure 3).
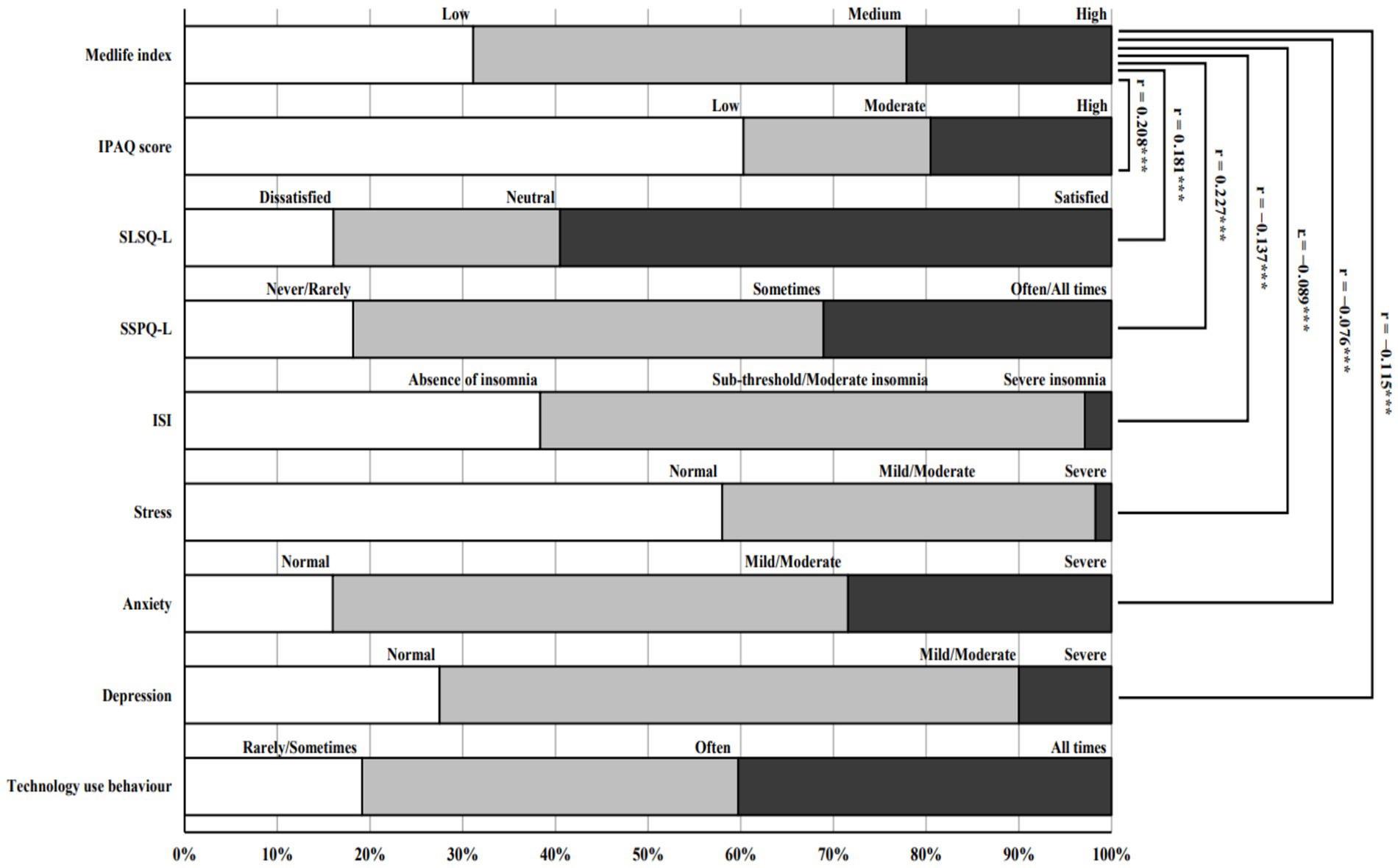
Figure 3. Correlations between the MedLife Index and other health and lifestyle parameters. SLSQ-L, short life satisfaction questionnaire; ISI: Insomnia Severity Index; IPAQ, the international physical activity questionnaires; SSPQ-L, short social participation questionnaire; ***significantly different compared to males at p < 0.001.
4 Discussion
Our multinational study of 4,010 participants across 10 countries provides both confirmatory evidence and novel insights through its comprehensive assessment of lifestyle interactions. In the present study, adherence to the MedDiet and its association with lifestyle behaviors were investigated within a large, diverse survey population. By defining adherence thresholds based on percentiles, the study provided a detailed analysis of dietary patterns and gender differences. Significant associations were identified between MedLife index and key lifestyle parameters, underscoring the relationship between dietary habits and lifestyle behaviors.
4.1 Demographic characteristics of the participants
This study reveals demographic differences that indicate underlying physiological, psychological, and sociocultural mechanisms influencing health-related behaviors. Educational attainment varied significantly by gender. Females were more likely to hold a bachelor’s degree, which may reflect their established cognitive resilience and adaptive strategies within academic settings, as evidenced by research indicating enhanced verbal and social cognitive skills that facilitate learning and collaboration (43). Although females were more represented at the bachelor’s level, males showed higher representation at the master’s level, possibly due to greater participation in male-dominated fields requiring advanced degrees (e.g., STEM, business) (44, 45), delayed entry into graduate education after work experience (46), and structural barriers such as caregiving responsibilities that may limit women’s progression to higher academic levels (47, 48). Furthermore, the slightly higher participation of males in vocational training—though not statistically significant—might stem from evolutionary predispositions favoring risk-taking and manual or technical skills, consistent with traditional gender roles (49).
Significant gender disparities were also observed in BMI classifications, with females showing a higher prevalence in the underweight and normal weight categories compared to males, while males exhibited a higher prevalence in the overweight category compared to females. This reflects fundamental biological differences in fat metabolism influenced by gender hormones, combined with social factors: women face stronger societal pressures for thinness, while men experience greater acceptance of higher body weights. Women’s generally healthier eating patterns as shown in our MedDiet results further contribute to this weight distribution pattern (50).
Gender differences in smoking behaviors, particularly the higher prevalence of non-smokers among females, may reflect physiological sensitivities to nicotine and its metabolism. Evidence suggests that males experience greater dopaminergic reinforcement from smoking, which contributes to stronger addictive patterns (51). In contrast, females may be more inclined toward alternative forms such as shisha, influenced by social context and a perception of reduced harm (51). The present findings support these observations, showing a higher prevalence of cigarette smoking among males compared to females, whereas shisha smoking was more common among females.
The increased participation of young adult females in this study may be due to their heightened engagement with health-related topics and greater responsiveness to surveys. This observation is consistent with existing research indicating that women, especially younger adults, tend to be more proactive in addressing health issues and participating in health-related studies (52). Variations in ethnicity and marital status across gender may indicate wider societal and cultural dynamics, including differences in gender roles, family structures, and migration patterns, which affect lifestyle behaviors (49).
4.2 Dietary, physical, and social activities behaviors
Our analysis extends beyond confirming gender differences to reveal how distinct behavioral pathways lead to equivalent MedLife adherence. The analysis of the MedLife Index revealed several gender-related patterns in adherence to the MedLife, with both overlapping and distinct behaviors observed across its three core dimensions. While no significant differences emerged in the overall MedLife Index score, detailed analysis by block uncovered meaningful gender-specific variations. In Block 1 (Mediterranean Food Consumption), females scored significantly higher than males. This difference was driven by stronger adherence among women in 7 out of 15 dietary components, particularly in reducing red and processed meat intake, and in the consumption of vegetables, olive oil, and herbs. These findings are consistent with previous studies showing that women tend to prioritize long-term health outcomes and demonstrate greater nutritional awareness and restraint in food choices (53). Furthermore, hormonal and physiological differences may also play a role—estrogen, for example, positively influences lipid and glucose metabolism, aligning well with the plant-rich and unsaturated fat profile of the MedDiet (20, 54). In contrast, males reported greater adherence in fish/seafood, legumes, and sweets consumption, reflecting possible cultural preferences or gender-based differences in food availability or preparation habits (53, 55).
No significant gender differences were observed in Mediterranean dietary habits (block 2), indicating comparable general adherence to dietary routines such as moderation and meal timing. However, item-level analysis revealed divergent patterns. Females adhered more closely to recommendations for whole grain consumption, reducing sugar in beverages, and limiting snacking between meals, behaviors typically associated with weight control and preventive health (53, 56). These trends align with evidence that women are more likely to engage in health-protective dietary practices and report higher levels of dietary self-regulation (57, 58).
On the other hand, males showed better adherence in water or infusion consumption, wine intake, and salt limitation. Moderate wine consumption is culturally normalized for men in many Mediterranean societies and may be perceived as socially acceptable or even beneficial for cardiovascular health (59, 60). Higher adherence to hydration and salt limitation could reflect a stronger association with PA routines or awareness of cardiovascular risk (61, 62). This highlights the need for gender-sensitive dietary interventions, as males and females may respond differently to public health messaging depending on their motivations, lifestyles, and sociocultural context.
In Block 3 (PA, Rest, Social Habits, and Conviviality), males exhibited significantly higher scores, pointing to distinct lifestyle patterns between genders. This was particularly evident in components such as PA, collective sports, and social engagement. These trends were further supported by the IPAQ-SF results, which showed a higher prevalence of high-intensity PA among males compared to females, while low-intensity PA were more prevalent among females than males. Collectively, this contributed to higher total PA score in male than female considering that high intensity PA reflect higher MET values. These differences may stem from a combination of social, cultural, and practical factors. Men are often more involved in structured or vigorous activities, such as sports or physically demanding work, driven by societal norms that encourage physical competitiveness and outdoor engagement (63–65). Their participation in collective activities and higher self-reported intensity levels may also reflect greater opportunities or prioritization of leisure-time PA (66, 67).
In contrast, women may face greater barriers to sustained or intense activity due to competing demands such as caregiving and domestic responsibilities, which limit their discretionary time and energy for exercise (68–70). Consequently, even when women engage in PA, it is often of lower intensity or incorporated into daily routines (e.g., walking or household tasks) rather than structured sessions. Social engagement, another aspect of Block 3—is often linked to psychological well-being, and men’s greater participation in group-based activities may serve as both a physical and social health resource (71).
Despite these block-specific differences, the overall MedLife Index categories (low, medium, high adherence) did not differ significantly by gender, suggesting that men and women achieve similar levels of total MedLife adherence, albeit through different behavioral pathways. This reinforces the importance of designing gender-tailored interventions that account for varied motivators and constraints rather than adopting a one-size-fits-all model.
Turning to the perceived barriers, females reported significantly higher levels of perceived obstacles to adopting a MedLife. Detailed analysis showed that women were more likely to cite attitudinal barriers, lack of knowledge, and taste-related issues. These findings may reflect underlying disparities in access to health education, exposure to culturally relevant nutrition information, or a lack of supportive environments that facilitate healthy food choices (72, 73). Additionally, sensory preferences and food aversions are known to differ by gender, with women often more sensitive to taste, texture, or dietary restrictions imposed by family settings (74).
Conversely, men reported higher proportions of low motivation and health-related (medical) reasons, indicating that while women may face more environmental and knowledge-based barriers, men may be more affected by internal motivation or physical constraints. This aligns with previous findings showing that men are less likely to engage in health-promoting behaviors unless prompted by medical necessity or structured settings (64, 75).
4.3 Sleep parameters, insomnia severity and technology use behaviors
Our sleep findings provide new evidence about how gender differences in sleep patterns interact with dietary behaviors across different populations. The present analysis revealed several significant gender differences in sleep-related outcomes. Specifically, females exhibited longer sleep latency, lower sleep efficiency, poorer subjective sleep quality, longer sleep duration (mean value exceeding recommended duration), and greater insomnia severity (ISI scores) compared to males. These findings align with previous studies showing that women are more likely to report disrupted sleep patterns and symptoms of insomnia (76–78). The observed longer sleep latency and lower efficiency in females may be attributable to hormonal fluctuations (e.g., during menstrual cycles, pregnancy, or menopause) that may interfere with sleep regulation and stability (79). In addition, psychological and behavioral factors, such as a heightened stress response, a greater tendency for rumination, and increased exposure to caregiving responsibilities, may further delay sleep onset and contribute to night-time awakenings (80).
These sleep-based lifestyle disruptions, when combined with other social factors, such as increased caregiving, likely contribute to the significantly higher ISI scores observed in females, along with their higher proportion in the moderate-to-severe insomnia categories (81, 82). Interestingly, although females reported longer sleep duration, this may represent a compensatory behavior to offset the lower sleep quality and efficiency. Women often extend total sleep time in an effort to achieve restorative rest, despite experiencing more frequent awakenings and difficulty falling asleep (83, 84). This finding is consistent with the hypothesis that sleep quantity alone may not reflect true restfulness, especially in the presence of fragmented sleep architecture.
While significant differences were found in continuous scores for sleep quality and duration, no gender differences were observed in categorical classifications of sleep duration or quality (e.g., recommended duration or self-rated sleep quality categories). This discrepancy may suggest that while men and women differ in sleep patterns and subjective scores, they may be similarly distributed in terms of broader public health classifications.
The higher reported technology use among females may further contribute to impaired sleep outcomes. Excessive screen time—particularly before bedtime—has been associated with delayed sleep onset and reduced melatonin secretion, disproportionately affecting women who already exhibit greater sensitivity to sleep-disrupting stimuli (85–87).
4.4 Mental health: depression, anxiety, stress, and needs of support
Our mental health results strengthen evidence for gender-specific patterns while suggesting new directions for integrated interventions. The findings of this study revealed significant gender differences in psychological distress and perceived need for support. Females reported significantly higher levels of depression, anxiety, and stress, as measured by the DASS-21, with small-to-moderate effect sizes across all domains. These results are consistent with a broad body of literature indicating that women are more prone to internalizing disorders, likely due to a complex interplay of biological, psychological, and social factors (88, 89).
Hormonal fluctuations associated with the menstrual cycle, pregnancy, and menopause may contribute to increased vulnerability to mood dysregulation and heightened emotional reactivity in women (88). In addition, gender differences in emotional processing and coping styles may also play a role. Women tend to engage in emotion-focused coping strategies and are more likely to ruminate on negative experiences, which can exacerbate stress and depressive symptoms (89). In contrast, men are more likely to employ problem-focused coping and often underreport emotional difficulties, due in part to sociocultural norms that discourage emotional expression and promote stoicism (90). This may explain the significantly higher proportion of males in the “normal” range across all three psychological distress categories and their underrepresentation in mild to severe categories.
In terms of perceived need for support, females consistently reported significantly higher needs across all three domains: psycho-social, physical, and nutritional support. These findings reflect women’s greater inclination to recognize and express the need for help, particularly in response to emotional and physical strain (91). Women may also be more likely to seek social connection and professional assistance as part of their coping process, which is aligned with gender socialization patterns that emphasize interdependence, caregiving, and relational well-being (92).
On the other hand, males were significantly more likely to report no perceived need for support in any domain. This aligns with prior research suggesting that men often minimize their perceived need for help, particularly in health and emotional contexts, due to internalized beliefs about self-reliance and the stigma associated with vulnerability (93). This reluctance to acknowledge or seek support may contribute to unmet needs and could partially obscure underlying psychological struggles that are not outwardly expressed or captured by self-report measures.
4.5 Correlations
The interconnectedness of lifestyle factors revealed by our multinational sample provides robust evidence for holistic interventions. The MedLife Index demonstrates a significant correlation between adherence to the MedDiet and multiple health and lifestyle factors, such as PA, mental health, sleep quality, and social support.
The positive correlation observed between the MedLife Index and IPAQ-SF scores (r = 0.208) illustrates the relationship between dietary adherence and PA. This relationship indicates the broader concept of a MedLife, characterized by the integration of regular PA and a nutrient-rich diet. Engaging in PA improves energy balance, metabolic efficiency, and mental health, thereby complementing the anti-inflammatory and cardiovascular advantages associated with the MedDiet (94). Integrating bidomain interventions, combining PA with the MedDiet, may enhance health outcomes, particularly in populations with low PA levels (95).
The negative correlation between dietary adherence and insomnia severity suggests that the MedDiet may reduce insomnia severity through metabolic and neurological mechanisms. Its high fiber content helps stabilize blood sugar levels, while its anti-inflammatory components alleviate conditions that disrupt sleep (96). Furthermore, the MedDiet, characterized by a high intake of fruits, vegetables, whole grains, and omega-3 fatty acids, enhances sleep quality. These foods promote the synthesis of melatonin and serotonin, essential for regulating sleep–wake cycles and improving restorative sleep (97, 98). Promoting the MedDiet may improve sleep satisfaction and provide a non-pharmacological strategy for addressing sleep disturbances (99).
The positive correlation between the MedLife Index and social participation illustrates the significance of social connections in enhancing adherence to the MedDiet. Social networks influence dietary choices, promote the adoption of Mediterranean eating patterns, and offer emotional reinforcement (99). Individuals in supportive social environments are more likely to maintain adherence to diets, benefiting from shared meals, cultural practices, and collective motivation (99).
The positive correlation between the MedLife Index and life satisfaction, along with the inverse relationships observed between the MedLife Index and stress, anxiety, and depression, underscore the potential protective benefits of a MedDiet on mental health. This finding is consistent with research indicating that the anti-inflammatory and neuroprotective effects of the MedDiet can alleviate symptoms of psychological distress (100, 101). This diet high in antioxidants, polyphenols, and omega-3 fatty acids can mitigate oxidative stress and enhance cognitive function, which are essential for the management of anxiety, depression, and stress (101).
4.6 Potential inflation of significance due to large sample size
Although the large sample size in this study enhances statistical power and improves the potential generalizability of the findings, it may also contribute to the inflation of statistical significance. In large datasets, even minimal differences can yield statistically significant results, which do not necessarily reflect meaningful or practically relevant effects. As such, while the associations identified are noteworthy, they should be interpreted with caution. Further research, particularly studies employing targeted sampling or intervention-based designs, is needed to confirm these associations and evaluate their clinical or practical significance.
4.7 Strength and limitation
This study has several notable strengths, particularly its multinational scope and demographically diverse sample, which enhance the generalizability of findings across cultural contexts. The use of validated tools to assess demographic, behavioral, and psychosocial factors provides a comprehensive overview of participants’ lifestyle characteristics and their associations with MedDiet adherence. Additionally, gender-specific analyses offer nuanced insights into differences in dietary and lifestyle behaviors between men and women, contributing to a more differentiated understanding of adherence dynamics.
However, several limitations must be acknowledged. The cross-sectional design inherently limits the ability to draw causal inferences between adherence patterns and health outcomes. The study also faces the potential for self-selection bias, as participation was voluntary and conducted online, which may have attracted younger, more educated, urban, and health-conscious individuals—while underrepresenting older adults and those in rural settings. Social desirability and recall biases may have been introduced through the reliance on self-reported data, even when collected using validated instruments such as the MedLife Index and IPAQ-SF. Unmeasured confounders, including socioeconomic disparities, cultural influences, or region-specific food environments, may also have influenced the results and reduced precision in subgroup comparisons.
Furthermore, cultural biases in survey responses across different countries should be considered. Despite using validated instruments, cultural differences in dietary practices, health perceptions, and response styles may have influenced participants’ answers. For example, varying interpretations of food-related behaviors and lifestyle choices across countries could impact the accuracy of self-reported data. Additionally, cultural norms around health and nutrition may have led to different levels of social desirability bias, particularly in more health-conscious populations. Regional differences in food availability, traditional eating habits, and lifestyle factors may have introduced further variability in the results, potentially reducing the comparability of data across countries.
While we conducted gender-specific analyses to explore key differences between men and women, the unequal gender distribution and potential selection bias may have affected the robustness of subgroup comparisons. To address this, we applied proportional analytical approaches and statistical techniques, such as Z-tests for two proportions, to detect gender-related differences while accounting for unequal sample sizes.
Future studies should aim for more balanced gender representation, adopt stratified sampling methods, incorporate objective data collection (e.g., biomarkers or wearable devices), and employ longitudinal or interventional designs to strengthen causal interpretation and validate these findings in more representative populations.
5 Conclusion
This study highlights the complex and gender-specific patterns underlying adherence to the Mediterranean lifestyle. While females demonstrated greater compliance with Mediterranean dietary recommendations, males reported higher engagement in PA, rest, and social participation. Furthermore, the MedLife Index was positively associated with favorable outcomes such as PA levels, life satisfaction, and social engagement, and negatively associated with insomnia severity, stress, anxiety, and depressive symptoms.
These findings emphasize the need for gender-sensitive and behaviorally targeted interventions that consider the distinct motivations, barriers, and cultural contexts influencing lifestyle choices. Tailoring public health strategies to these differences may enhance the adoption and sustainability of the Mediterranean lifestyle and ultimately improve population health outcomes.
6 Practical applications
The findings of this study carry important implications for public health strategies aimed at promoting adherence to the MedLife, particularly in diverse populations. Although overall adherence to the MedLife Index was comparable between sexs, the behavioral components contributing to these scores varied significantly, indicating the need for gender-tailored interventions.
For instance, women demonstrated higher adherence to dietary components of the Mediterranean lifestyle, yet lower engagement in PA, greater psychological distress, and higher perceived barriers to healthy behaviors. Accordingly, initiatives targeting women should emphasize flexible, time-efficient, and culturally appropriate PA options, such as group fitness classes, outdoor walking groups, or family-oriented activities that can be integrated into daily routines. At the same time, interventions should address the attitudinal and structural barriers reported by women, including taste preferences, time constraints, and lack of nutrition knowledge. Empowerment through community-based cooking workshops, peer-led support groups, and the use of digital tools (e.g., mobile apps for meal planning or stress management) could enhance self-efficacy and engagement.
In contrast, men reported greater PA levels and higher scores in social participation and rest-related behaviors but showed lower adherence to dietary recommendations. For this group, strategies should focus on improving nutrition behaviors through targeted education on key dietary components, such as reducing sugar intake and increasing whole grain consumption, while also promoting awareness about hydration and salt moderation. Practical approaches might include structured nutrition counseling, goal-setting interventions, or hands-on cooking sessions that align with men’s reported preferences for performance-oriented or outcome-driven programs. Furthermore, addressing motivational and health-related barriers, including medical concerns and low perceived risk, may enhance dietary engagement among men.
Importantly, the MedLife Index was positively associated with PA, life satisfaction, and social participation, and negatively associated with insomnia, stress, anxiety, and depression. This highlights the potential of comprehensive lifestyle interventions that not only target diet and activity but also integrate mental health support and sleep hygiene strategies. For women in particular, interventions should address psychosocial stressors such as caregiving burden and emotional regulation difficulties, possibly through mindfulness training, peer support networks, or flexible access to mental health services. For men, outreach efforts may need to tackle help-seeking stigma and encourage early engagement with psychological support, even in the absence of severe symptoms.
The gender-specific disparities in sleep quality, latency, efficiency, and insomnia severity also point to the need for tailored sleep promotion initiatives. For women, this may include education on the impact of hormonal cycles, stress management tools, and limiting technology use before bedtime. For men, reinforcing existing protective behaviors and encouraging consistent sleep routines can help maintain optimal sleep health.
Finally, the significantly higher perceived need for psychosocial, physical, and nutritional support among women, alongside the tendency for men to underreport such needs, further supports the use of personalized health strategies. Public health policies should promote inclusive and culturally sensitive education campaigns, ensure equitable access to support services, and leverage digital health solutions to deliver timely, scalable, and adaptable interventions that meet the unique needs of each gender.
Together, these practical insights underscore the necessity of multi-dimensional, gender-sensitive, and context-specific interventions to sustainably promote the Mediterranean lifestyle and its associated health benefits across diverse populations.
Data availability statement
The datasets generated and analyzed during the current study are not publicly available at this time as further analyses are ongoing, and additional publications based on these data are in preparation. Data may be made available upon reasonable request to the corresponding author once all planned analyses and publications are completed.
Ethics statement
The studies involving humans were approved by the Ethics Committee of the Faculty of Medicine of Sfax (protocol code 58/24). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
MAB: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. AA: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AS: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing. MK: Conceptualization, Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. KT: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing. BB: Conceptualization, Data curation, Funding acquisition, Investigation, Resources, Validation, Visualization, Writing – review & editing. LM: Data curation, Formal analysis, Investigation, Resources, Validation, Visualization, Writing – review & editing. JH: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. CS: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. GM: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. AMU: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. HAG: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. ATA: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. BEO: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. GG: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. OA: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. TD: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. KE: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. PZ: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. NB: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. CP: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. LR: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. AG: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. MC-O: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. NF: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. CMM: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. BL: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. SF: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. AB: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. E-MA: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. EAA: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. MO: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. SL: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. TK: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. NS: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. OB: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. HJ: Data curation, Formal analysis, Investigation, Resources, Validation, Visualization, Writing – review & editing. WH: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. WM: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. HC: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. WIS: Data curation, Investigation, Resources, Supervision, Validation, Visualization, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work is part of the MEDDIET4ALL PRIMA PROJECT, supported by the European Union (Section 2-Multi-topic 2022, thematic Area 3-Food Value Chain, Topic 2.3.1-202-RIA) and multiple national organizations, including the Federal Ministry of Education and Research (BMBF) (grant no. 02WPM1681) and the national research agencies in France (ANR) (grant no. ANR-23-P012-0008-04).
Acknowledgments
We sincerely thank all MEDIET4ALL project collaborators for their valuable contributions to this study, with particular gratitude to Prof. Frédéric Debeaufort, the principal investigator at the University of Bourgogne, France.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Correction note
A correction has been made to this article. Details can be found at: 10.3389/fnut.2025.1692429.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Sikalidis, AK, Kelleher, AH, and Kristo, AS. Mediterranean diet. Encyclopedia. (2021) 1:371–87. doi: 10.3390/encyclopedia1020031
2. Ahmad, S, Moorthy, MV, Lee, IM, Ridker, PM, Manson, JE, Buring, JE, et al. Mediterranean diet adherence and risk of all-cause mortality in women. JAMA Netw Open. (2024) 7:e2414322. doi: 10.1001/jamanetworkopen.2024.14322
3. Guasch-Ferré, M, and Willett, WC. The Mediterranean diet and health: a comprehensive overview. J Intern Med. (2021) 290:549–66. doi: 10.1111/joim.13333
4. Xiao, Y, Xiao, X, Zhang, X, Yi, D, Li, T, Hao, Q, et al. Mediterranean diet in the targeted prevention and personalized treatment of chronic diseases: evidence, potential mechanisms, and prospects. EPMA J. (2024) 15:207–20. doi: 10.1007/s13167-024-00333-5
5. Menotti, A, and Puddu, PE. Ancel keys, the Mediterranean diet, and the seven countries study: a review. J Cardiovasc Dev Dis. (2025) 12:141. doi: 10.3390/jcdd12040141
6. Willett, W, Sacks, F, Trichopoulou, A, Drescher, G, Ferro-Luzzi, A, Helsing, E, et al. Mediterranean diet pyramid: a cultural model for healthy eating. Am J Clin Nutr. (1995) 61:1402S–6S. doi: 10.1093/ajcn/61.6.1402S
7. Mattavelli, E, Olmastroni, E, Bonofiglio, D, Catapano, AL, Baragetti, A, and Magni, P. Adherence to the Mediterranean diet: impact of geographical location of the observations. Nutrients. (2022) 14:2040. doi: 10.3390/nu14102040
8. Martínez-González, M, Hershey, M, Zazpe, I, and Trichopoulou, A. Transferability of the Mediterranean diet to non-Mediterranean countries: what is and what is not the Mediterranean diet. Nutrients. (2017) 9:1226. doi: 10.3390/nu9111226
9. Riolo, R, De Rosa, R, Simonetta, I, and Tuttolomondo, A. Olive oil in the Mediterranean diet and its biochemical and molecular effects on cardiovascular health through an analysis of genetics and epigenetics. Int J Mol Sci. (2022) 23:16002. doi: 10.3390/ijms232416002
10. Qian, F, Riddle, MC, Wylie-Rosett, J, and Hu, FB. Red and processed meats and health risks: How strong is the evidence? Diabetes Care. (2020) 43:265–71. doi: 10.2337/dci19-0063
11. Gotsis, E, Anagnostis, P, Mariolis, A, Vlachou, A, Katsiki, N, and Karagiannis, A. Health benefits of the Mediterranean diet: an update of research over the last five years. Angiology. (2015) 66:304–18. doi: 10.1177/0003319714532169
12. Franquesa, M, Pujol-Busquets, G, García-Fernández, E, Rico, L, Shamirian-Pulido, L, Aguilar-Martínez, A, et al. Mediterranean diet and cardiodiabesity: a systematic review through evidence-based answers to key clinical questions. Nutrients. (2019) 11:655. doi: 10.3390/nu11030655
13. Guasch-Ferré, M, Salas-Salvadó, J, Ros, E, Estruch, R, Corella, D, Fitó, M, et al. The PREDIMED trial, Mediterranean diet and health outcomes: how strong is the evidence? Nutr Metab Cardiovasc Dis. (2017) 27:624–32. doi: 10.1016/j.numecd.2017.05.004
14. Lotfi, K, Saneei, P, Hajhashemy, Z, and Esmaillzadeh, A. Adherence to the Mediterranean diet, five-year weight change, and risk of overweight and obesity: a systematic review and dose-response meta-analysis of prospective cohort studies. Adv Nutr. (2022) 13:152–66. doi: 10.1093/advances/nmab092
15. Nissensohn, M, Román-Viñas, B, Sánchez-Villegas, A, Piscopo, S, and Serra-Majem, L. The effect of the Mediterranean diet on hypertension: a systematic review and meta-analysis. J Nutr Educ Behav. (2016) 48:42–53.e1. doi: 10.1016/j.jneb.2015.08.023
16. Esposito, K, Kastorini, CM, Panagiotakos, DB, and Giugliano, D. Mediterranean diet and metabolic syndrome: an updated systematic review. Rev Endocr Metab Disord. (2013) 14:255–63. doi: 10.1007/s11154-013-9253-9
17. Rosato, V, Temple, NJ, La Vecchia, C, Castellan, G, Tavani, A, and Guercio, V. Mediterranean diet and cardiovascular disease: a systematic review and meta-analysis of observational studies. Eur J Nutr. (2019) 58:173–91. doi: 10.1007/s00394-017-1582-0
18. Sharma, S, Gialluisi, A, Donati, MB, De Gaetano, G, Maglione, V, Iacoviello, L, et al. Adherence to a Mediterranean diet and risks of Alzheimer and Parkinson diseases: a systematic review of population-based studies. Proc 14th Eur Nutr Conf FENS. (2023) 91:80.
19. Schwingshackl, L, Schwedhelm, C, Galbete, C, and Hoffmann, G. Adherence to Mediterranean diet and risk of cancer: an updated systematic review and meta-analysis. Nutrients. (2017) 9:1063. doi: 10.3390/nu9101063
20. Kamiński, M, Skonieczna-Żydecka, K, Nowak, JK, and Stachowska, E. Global and local diet popularity rankings, their secular trends, and seasonal variation in Google trends data. Nutrition. (2020) 79-80:110759. doi: 10.1016/j.nut.2020.110759
21. Baker, P, Machado, P, Santos, T, Sievert, K, Backholer, K, Hadjikakou, M, et al. Ultra-processed foods and the nutrition transition: global, regional and national trends, food-systems transformations and political-economy drivers. Obes Rev. (2020) 21:e13126. doi: 10.1111/obr.13126
22. Popkin, BM. Nutrition in transition: the changing global nutrition challenge. Asia Pac J Clin Nutr. (2001) 10. doi: 10.1046/j.1440-6047.2001.0100s1S13.x
23. Kihlstrom, L, Long, A, and Himmelgreen, D. Barriers and facilitators to the consumption of fresh produce among food-pantry clients. J Hunger Environ Nutr. (2019) 14:168–82. doi: 10.1080/19320248.2018.1512923
24. Naja, F, Hwalla, N, Hachem, F, Abbas, NA, Chokor, FAZ, Kharroubi, S, et al. Erosion of the Mediterranean diet among adolescents: evidence from an eastern-Mediterranean country. Br J Nutr. (2021) 125:346–56. doi: 10.1017/S0007114520002731
25. Cavaliere, A, De Marchi, E, Donzelli, F, and Banterle, A. Is the Mediterranean diet for all? An analysis of socioeconomic inequalities and food consumption in Italy. Br Food J. (2019) 121:1327–41. doi: 10.1108/BFJ-06-2018-0373
26. Dijkstra, SC, Neter, JE, van Stralen, MM, Knol, DL, Brouwer, IA, Huisman, M, et al. The role of perceived barriers in explaining socioeconomic-status differences in adherence to the fruit, vegetable and fish guidelines in older adults: a mediation study. Public Health Nutr. (2015) 18:797–808. doi: 10.1017/S1368980014001487
27. Pinho, MGM, Mackenbach, JD, Charreire, H, Oppert, JM, Bárdos, H, Glonti, K, et al. Exploring the relationship between perceived barriers to healthy eating and dietary behaviours in European adults. Eur J Nutr. (2018) 57:1761–70. doi: 10.1007/s00394-017-1458-3
28. Arvaniti, F, Panagiotakos, DB, Pitsavos, C, Zampelas, A, and Stefanadis, C. Dietary habits in a Greek sample of men and women: the ATTICA study. Cent Eur J Public Health. (2006) 14:74–7. doi: 10.21101/cejph.a3374
29. Abellán Alemán, J, Zafrilla Rentero, M, Montoro-García, S, Mulero, J, Pérez Garrido, A, Leal, M, et al. Adherence to the Mediterranean diet in Spain and its relationship with cardiovascular risk (DIMERICA study). Nutrients. (2016) 8:680. doi: 10.3390/nu8110680
30. Ammar, A. A transnational movement to support the sustainable transition towards a healthy and eco-friendly Agri-food system through the promotion of MEDIET and its lifestyle in modern society: MEDIET4ALL. Eur J Pub Health. (2024) 34:ckae144.643. doi: 10.1093/eurpub/ckae144.643
31. Boujelbane, MA, Ammar, A, Salem, A, Kerkeni, M, Trabelsi, K, Bouaziz, B, et al. Regional variations in Mediterranean-diet adherence: a sociodemographic and lifestyle analysis across Mediterranean and non-Mediterranean regions within the MEDIET4ALL project. Front Public Health. (2025) 13:1596681. doi: 10.3389/fpubh.2025.1596681
32. Sotos-Prieto, M, Moreno-Franco, B, Ordovás, JM, León, M, Casasnovas, JA, and Peñalvo, JL. Design and development of an instrument to measure overall lifestyle habits for epidemiological research: the Mediterranean lifestyle (MEDLIFE) index. Public Health Nutr. (2015) 18:959–67. doi: 10.1017/S1368980014001360
33. Zaragoza-Martí, A, Cabañero-Martínez, M, Hurtado-Sánchez, J, Laguna-Pérez, A, and Ferrer-Cascales, R. Evaluation of Mediterranean-diet adherence scores: a systematic review. BMJ Open. (2018) 8:e019033. doi: 10.1136/bmjopen-2017-019033
34. Bach-Faig, A, Berry, EM, Lairon, D, Reguant, J, Trichopoulou, A, Dernini, S, et al. Mediterranean-diet pyramid today: science and cultural updates. Public Health Nutr. (2011) 14:2274–84. doi: 10.1017/S1368980011002515
35. Buysse, DJ, Reynolds, CF, Monk, TH, Berman, SR, and Kupfer, DJ. The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. (1989) 28:193–213. doi: 10.1016/0165-1781(89)90047-4
36. Watson, NF, Badr, MS, Belenky, G, Bliwise, DL, Buxton, OM, Buysse, D, et al. Recommended amount of sleep for a healthy adult: a joint consensus statement of the American Academy of sleep medicine and Sleep Research Society. J Clin Sleep Med. (2015) 11:591–2. doi: 10.5664/jcsm.4758
37. Bastien, C, Vallières, A, and Morin, CM. Validation of the insomnia severity index as an outcome measure for insomnia research. Sleep Med. (2001) 2:297–307. doi: 10.1016/S1389-9457(00)00065-4
38. Lovibond, PF, and Lovibond, SH. The structure of negative emotional states: comparison of the depression anxiety stress scales with the Beck depression and anxiety inventories. Behav Res Ther. (1995) 33:335–43. doi: 10.1016/0005-7967(94)00075-U
39. Ammar, A, Brach, M, Trabelsi, K, Chtourou, H, Boukhris, O, Masmoudi, L, et al. Effects of COVID-19 home confinement on eating behaviour and physical activity: results of the ECLB-COVID19 international online survey. Nutrients. (2020) 12:1583. doi: 10.3390/nu12061583
40. Ammar, A, Trabelsi, K, Brach, M, Chtourou, H, Boukhris, O, Masmoudi, L, et al. Effects of home confinement on mental health and lifestyle behaviours during the COVID-19 outbreak: insight from the ECLB-COVID19 multicenter study. Biol Sport. (2021) 38:9–21. doi: 10.5114/biolsport.2020.96857
41. Craig, CL, Marshall, AL, Sjöström, M, Bauman, AE, Booth, ML, Ainsworth, BE, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. (2003) 35:1381–95. doi: 10.1249/01.MSS.0000078924.61453.FB
42. Lee, PH, Macfarlane, DJ, Lam, T, and Stewart, SM. Validity of the international physical activity questionnaire short form (IPAQ-SF): a systematic review. Int J Behav Nutr Phys Act. (2011) 8:115. doi: 10.1186/1479-5868-8-115
43. Halpern, GM. “We only eat what we like” or do we still? Flavour. (2012) 1:17. doi: 10.1186/2044-7248-1-17
45. Ceci, SJ, Ginther, DK, Kahn, S, and Williams, WM. Women in academic science: a changing landscape. Psychol Sci Public Interest. (2014) 15:75–141. doi: 10.1177/1529100614541236
46. Purcell, K, Elias, P, Atfield, G, Behle, H, and Ellison, R. Applying for higher education: The diversity of career choices, plans and expectations. Higher Education Career Services Unit and Universities and Colleges Admissions Service (2008).
47. Misra, J, Lundquist, JH, Holmes, E, and Agiomavritis, S. The ivory ceiling of service work. Academe. (2012) 98:22–6.
48. Heath, S, Fuller, A, and Johnston, B. Young people, social capital and network-based educational decision-making. Br J Sociol Educ. (2010) 31:395–411. doi: 10.1080/01425692.2010.484918
49. Wood, W, and Eagly, AH. Biosocial construction of sex differences and similarities in behavior. Advances Experimental Social Psychology. (2012) 46:55–123. doi: 10.1016/B978-0-12-394281-4.00002-7
50. Mueller, K, Möller, HE, Horstmann, A, Busse, F, Lepsien, J, Blüher, M, et al. Physical exercise in overweight to obese individuals induces metabolic- and neurotrophic-related structural brain plasticity. Front Hum Neurosci. (2015) 9:372. doi: 10.3389/fnhum.2015.00372
51. Benowitz, NL. Pharmacology of nicotine: addiction, smoking-induced disease, and therapeutics. Annu Rev Pharmacol Toxicol. (2009) 49:57–71. doi: 10.1146/annurev.pharmtox.48.113006.094742
52. Sundbom, L, and Bingefors, K. Influence of anxiety and depression symptoms on medication non-adherence and its causes: a population-based survey. Patient Prefer Adherence. (2013) 7:805–12. doi: 10.2147/PPA.S50055
53. Wardle, J, Haase, AM, Steptoe, A, Nillapun, M, Jonwutiwes, K, and Bellisie, F. Sex differences in food choice: the contribution of health beliefs and dieting. Ann Behav Med. (2004) 27:107–16. doi: 10.1207/s15324796abm2702_5
54. Mauvais-Jarvis, F, Clegg, DJ, and Hevener, AL. Role of estrogens in control of energy balance and glucose homeostasis. Endocr Rev. (2013) 34:309–38. doi: 10.1210/er.2012-1055
55. Gorini, S, Camajani, E, Cava, E, Feraco, A, Armani, A, Amoah, I, et al. Sex differences in eating habits and sports preferences across age groups: a cross-sectional study. J Transl Med. (2025) 23:312. doi: 10.1186/s12967-025-06311-x
56. Gough, B, and Conner, MT. Barriers to healthy eating among men. Psychol Health. (2006) 21:233–46.
57. Croll, JK, Neumark-Sztainer, D, and Story, M. Healthy eating: what does it mean to adolescents? J Nutr Educ. (2001) 33:193–8. doi: 10.1016/S1499-4046(06)60031-6
58. Feraco, A, Armani, A, Amoah, I, Guseva, E, Camajani, E, Gorini, S, et al. Assessing sex differences in food preferences and physical activity: a population-based survey. Front Nutr. (2024) 11:1348456. doi: 10.3389/fnut.2024.1348456
59. Room, R, and Mäkelä, K. Typologies of the cultural position of drinking. J Stud Alcohol. (2000) 61:475–83. doi: 10.15288/jsa.2000.61.475
60. Chiva-Blanch, G, and Badimon, L. Benefits and risks of moderate alcohol consumption on cardiovascular disease: current findings and controversies. Nutrients. (2019) 12:108. doi: 10.3390/nu12010108
61. Maughan, RJ, and Shirreffs, SM. Dehydration and rehydration in competitive sport. Scand J Med Sci Sports. (2010) 20:40–7. doi: 10.1111/j.1600-0838.2010.01207.x
62. Grillo, A, Salvi, L, Coruzzi, P, Salvi, P, and Parati, G. Sodium intake and hypertension. Nutrients. (2019) 11:1970. doi: 10.3390/nu11091970
63. Azevedo, MR, Araújo, CLP, Reichert, FF, Siqueira, FV, da Silva, MC, and Hallal, PC. Sex differences in leisure-time physical activity. Int J Public Health. (2007) 52:8–15. doi: 10.1007/s00038-006-5062-1
64. Courtenay, WH. Constructions of masculinity and their influence on men’s well-being: a theory of sex and health. Soc Sci Med. (2000) 50:1385–401. doi: 10.1016/S0277-9536(99)00390-1
65. Owen, KB, Corbett, L, Ding, D, Eime, R, and Bauman, A. Sex differences in physical activity and sport participation in adults across 28 European countries between 2005 and 2022. Ann Epidemiol. (2025) 101:52–7. doi: 10.1016/j.annepidem.2024.12.011
66. Ahmadi, MN, Ferrari, G, Rezende, LF, et al. Intensity-specific leisure-time physical activity and mortality in 3.36 million adults from 17 countries: pooled analysis. medRxiv. (2024)
67. Mielke, GI, Malta, DC, Nunes, BP, and Cairney, J. All are equal, but some are more equal than others: social determinants of leisure-time physical activity through the lens of intersectionality. BMC Public Health. (2022) 22:36. doi: 10.1186/s12889-021-12428-7
68. Pacheco Barzallo, D, Schnyder, A, Zanini, C, and Gemperli, A. Sex differences in family caregiving: do female caregivers do more or undertake different tasks? BMC Health Serv Res. (2024) 24:730. doi: 10.1186/s12913-024-11191-w
69. Rütten, A, Abu-Omar, K, Frahsa, A, and Morgan, A. Assets for policy making in health promotion: overcoming barriers inhibiting women from engaging in physical activity. Soc Sci Med. (2013) 74:136–43. doi: 10.1016/j.socscimed.2011.10.005
70. Craig, L, and Brown, JE. Feeling rushed: sexed time quality, work hours, non-standard schedules, and spousal crossover. J Marriage Fam. (2017) 79:225–42. doi: 10.1111/jomf.12320
71. Eime, RM, Young, JA, Harvey, JT, et al. Psychological and social benefits of participation in sport for adults: a systematic review. Int J Behav Nutr Phys Act. (2013) 10:135. doi: 10.1186/1479-5868-10-135
72. Sam-Yellowe, TY. Nutritional barriers to adherence to the Mediterranean diet in non-Mediterranean populations. Food Secur. (2024) 13:1750. doi: 10.3390/foods13111750
73. Aridi, YS, Walker, JL, Roura, E, and Wright, ORL. Nutritional knowledge of the Mediterranean diet is associated with positive attitudes and adherence in a non-Mediterranean multi-ethnic society. Die Dermatol. (2022) 1:124–36. doi: 10.3390/dietetics1020013
74. Michon, C, O'Sullivan, MG, Delahunty, CM, and Kerry, JP. Sex-related sensitivity differences in food perception. J Sens Stud. (2009) 24:922–37. doi: 10.1111/j.1745-459X.2009.00245.x
75. Ilić, A, Rumbak, I, Dizdarić, D, Matek Sarić, M, Colić Barić, I, and Guiné, RPF. Motivations associated with food choices among adults from an urban setting. Food Secur. (2023) 12:3546. doi: 10.3390/foods12193546
76. Li, RH, Wing, YK, Ho, SC, and Fong, SY. Sex differences in insomnia in the Hong Kong Chinese population. J Psychosom Res. (2002) 53:601–9. doi: 10.1016/S0022-3999(02)00437-3
77. Mong, JA, and Cusmano, DM. Sex differences in sleep: impact of biological sex and sex steroids. Philos Trans R Soc Lond Ser B Biol Sci. (2016) 371:20150110. doi: 10.1098/rstb.2015.0110
78. Zhang, B, and Wing, YK. Sex differences in insomnia: a meta-analysis. Sleep. (2006) 29:85–93. doi: 10.1093/sleep/29.1.85
79. Krishnan, V, and Collop, NA. Sex differences in sleep disorders. Curr Opin Pulm Med. (2006) 12:383–9. doi: 10.1097/01.mcp.0000245705.69440.6a
80. Verma, R, Balhara, YS, and Gupta, C. Sex differences in stress response: developmental and biological determinants. Indian J Psychiatry. (2011) 20:4–9. doi: 10.4103/0972-6748.98407
81. Byun, E, Lerdal, A, Gay, CL, and Lee, KA. How adult caregiving impacts sleep: a systematic review. Curr Sleep Med Rep. (2016) 2:191–205. doi: 10.1007/s40675-016-0058-8
82. Carskadon, MA. Sleep deprivation: health consequences and societal impact. Med Clin North Am. (2004) 88:767–76. doi: 10.1016/j.mcna.2004.03.001
83. Hirshkowitz, M, Whiton, K, Albert, SM, Alessi, C, Bruni, O, DonCarlos, L, et al. National sleep foundation’s updated sleep-duration recommendations: final report. Sleep Health. (2015) 1:233–43. doi: 10.1016/j.sleh.2015.10.004
84. Jonasdottir, SS, Minor, K, and Lehmann, S. Sex differences in nighttime sleep patterns across the adult lifespan: a wearables study. Sleep. (2021) 44:zsaa169. doi: 10.1093/sleep/zsaa169
85. Wacks, Y, and Weinstein, AM. Excessive smartphone use and health problems in adolescents and young adults. Front Psych. (2021) 12:669042. doi: 10.3389/fpsyt.2021.669042
86. Hale, L, and Guan, S. Screen time and sleep among school-aged children and adolescents: a systematic review. Sleep Med Rev. (2015) 21:50–8. doi: 10.1016/j.smrv.2014.07.007
87. Exelmans, L, and van den Bulck, J. Bedtime mobile-phone use and sleep in adults. Soc Sci Med. (2016) 148:93–101. doi: 10.1016/j.socscimed.2015.11.037
88. Kundakovic, M, and Rocks, D. Sex-hormone fluctuation and increased female risk for depression and anxiety disorders. Front Neuroendocrinol. (2022) 66:101010. doi: 10.1016/j.yfrne.2022.101010
89. Chaplin, TM. Sex and emotion expression: a developmental contextual perspective. Emotion Rev. (2015) 7:14–21. doi: 10.1177/1754073914544408
90. Doornbos, MM, Zandee, GL, and Bjelland, C. Men’s mental health: conceptualization, effects, and coping. Arch Psychiatr Nurs. (2024) 50:100–7. doi: 10.1016/j.apnu.2024.03.014
91. Hurdle, DE. Social support: a critical factor in women’s health and health promotion. Health Soc Work. (2001) 26:72–9. doi: 10.1093/hsw/26.2.72
92. Lathren, C. Self-compassion in relationships and caregiving contexts. In: Handbook of Self-Compassion. (2023):251–61.
93. Galdas, PM, Cheater, F, and Marshall, P. Men and health help-seeking behaviour: literature review. J Adv Nurs. (2005) 49:616–23. doi: 10.1111/j.1365-2648.2004.03331.x
94. Dinu, M, Pagliai, G, Casini, A, and Sofi, F. Mediterranean diet and multiple health outcomes: an umbrella review of meta-analyses. Eur J Clin Nutr. (2018) 72:30–43. doi: 10.1038/ejcn.2017.58
95. Hershey, MS, Martínez-González, MÁ, Álvarez-Álvarez, I, Martínez Hernández, JA, and Ruiz-Canela, M. The Mediterranean diet and physical activity: better together for prevention of premature mortality. Br J Nutr. (2022) 128:1413–24. doi: 10.1017/S0007114521002877
96. Castro-Diehl, C, Wood, AC, Redline, S, Reid, M, Johnson, DA, Maras, JE, et al. Mediterranean-diet pattern and sleep duration and insomnia symptoms in the multi-ethnic study of atherosclerosis. Sleep. (2018) 41:zsy158. doi: 10.1093/sleep/zsy158
97. Godos, J, Ferri, R, Lanza, G, Caraci, F, Vistorte, AOR, Yelamos Torres, V, et al. Mediterranean diet and sleep features: a systematic review. Nutrients. (2024) 16:282. doi: 10.3390/nu16020282
98. Kerkeni, M, Kerkeni, M, Ammar, A, Aziz, AR, Jallouli, A, AlSaleh, A, et al. Four-week kiwifruit and small-sided soccer intervention improves sleep in children with obesity. Nutr Health. (2025). doi: 10.1177/02601060241311385
99. Mieziene, B, Emeljanovas, A, Novak, D, and Kawachi, I. Social capital and adherence to a Mediterranean diet among Lithuanian adolescents. Nutrients. (2019) 11:1332. doi: 10.3390/nu11061332
100. Sánchez-Villegas, A, Delgado-Rodríguez, M, Alonso, A, Schlatter, J, Lahortiga, F, Serra-Majem, L, et al. Mediterranean diet and incidence of depression: the SUN cohort. Arch Gen Psychiatry. (2009) 66:1090–8. doi: 10.1001/archgenpsychiatry.2009.129
Keywords: Mediterranean diet, gender differences, MedLife index, physical activity, mental health
Citation: Boujelbane MA, Ammar A, Salem A, Kerkeni M, Trabelsi K, Bouaziz B, Masmoudi L, Heydenreich J, Schallhorn C, Müller G, Uyar AM, Ghazzawi HA, Amawi AT, Orhan BE, Grosso G, Abdelkarim O, Driss T, El Abed K, Zmijewski P, Benbettaieb N, Poulain C, Reyes L, Gamero A, Cuenca-Ortolá M, Francesca N, Messina CM, Lorenzen B, Filice S, Bajoub A, Ajal E-M, Ajal EA, Obtel M, Lahiani S, Khaldi T, Souissi N, Boukhris O, Jahrami H, Husain W, Mahdi W, Chtourou H and Schöllhorn WI (2025) Gender-specific insights into adherence to Mediterranean diet and lifestyle: analysis of 4,000 responses from the MEDIET4ALL project. Front. Nutr. 12:1570904. doi: 10.3389/fnut.2025.1570904
Edited by:
Roberto Vicinanza, University of Southern California, United StatesReviewed by:
Monica Tarcea, George Emil Palade University of Medicine, Pharmacy, Sciences, and Technology of Târgu Mureş, RomaniaBoris C. Rodríguez-Martín, International University of La Rioja, Spain
Bilge Meral Koc, Izmir Democracy University, Türkiye
Copyright © 2025 Boujelbane, Ammar, Salem, Kerkeni, Trabelsi, Bouaziz, Masmoudi, Heydenreich, Schallhorn, Müller, Uyar, Ghazzawi, Amawi, Orhan, Grosso, Abdelkarim, Driss, El Abed, Zmijewski, Benbettaieb, Poulain, Reyes, Gamero, Cuenca-Ortolá, Francesca, Messina, Lorenzen, Filice, Bajoub, Ajal, Ajal, Obtel, Lahiani, Khaldi, Souissi, Boukhris, Jahrami, Husain, Mahdi, Chtourou and Schöllhorn. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Achraf Ammar, YWNhbW1hckB1bmktbWFpbnouZGU=
†These authors share first authorship
‡ORCID: Achraf Ammar, https://orcid.org/0000-0003-0347-8053