 Shimeng Pang†
Shimeng Pang† Wei Chen
Wei Chen- Suzhou Stomatological Hospital, Suzhou, China
Background: Based on data from the Global Burden of Disease (GBD) 2021, this study analyzes the global disease burden of lip and oral cavity cancer attributable to high alcohol consumption (LOC-HAC).
Methods: Disability-adjusted life years (DALYs) were used to assess health loss. The Das Gupta decomposition method was employed to analyze the effects of population growth, aging, and epidemiological changes on DALYs. The Nordpred model was applied to project the disease burden trends from 2022 to 2045.
Results: In 2021, the global number of DALY cases for LOC-HAC was 1,191,084 (95% UI: 906,229.2–1,474,007), representing a 90% increase from 628,484.1 (95% UI: 493,522.1–754,895.3) in 1990. The fastest growth occurred in low-middle SDI regions, reaching 279%. A similar increasing trend was observed in deaths, with Southeast Asia showing the most significant rise, where DALYs and deaths increased by 326 and 357%, respectively. The global age-standardized DALY rate (ASDR) of LOC-HAC in 2021 was 13.66 (95% UI: 10.4–16.9) per 100,000 population, with Central Europe having the highest ASDR and Southeast Asia experiencing the fastest growth. DALYs and deaths were significantly higher in males than in females and increased with age, peaking at 55–59 years in males and 60–64 years in females. SDI levels were positively correlated with ASDR and age-standardized mortality rates (ASMR). However, when the SDI exceeded 0.75, ASDR and ASMR showed a declining trend. Over the past 32 years, the global increase in DALYs and deaths has been primarily driven by population aging and growth. Projections indicate that from 2022 to 2045, DALYs and deaths among males will rise significantly, whereas the increase among females will be more gradual.
Conclusion: The global burden of LOC-HAC has risen significantly over the past decades, especially in low-middle SDI regions and Southeast Asia. In the future, efforts should focus on these regions by promoting healthier lifestyles, strengthening early screening, and optimizing healthcare resource allocation to reduce disease burden.
Introduction
Lip and oral cavity cancer (LOC) is one of the more common malignant tumors worldwide (1). In recent years, its incidence has shown a significant upward trend, imposing a substantial burden on global healthcare systems (2). Major risk factors for LOC include tobacco smoking, alcohol consumption, betel nut chewing, human papillomavirus (HPV) infection, and ultraviolet (UV) exposure (2). HPV infection is associated with an increased risk of oral cancer, while UV exposure primarily elevates the risk of lip cancer (3). Therefore, there is an urgent need for comprehensive global research to better understand the epidemiological patterns of LOC and to develop targeted prevention strategies aimed at reducing its incidence and mortality.
In 2020, approximately 741,300 new cancer cases globally were attributed to alcohol consumption, accounting for 4% of all newly diagnosed cancer cases that year (4). A strong association exists between heavy alcohol consumption and the risk of LOC. Studies have shown a positive correlation between alcohol consumption and the risk of oral cancer. For instance, moderate drinkers (more than 12.5 g but less than or equal to 50 g of alcohol per day) have a 1.8-fold higher risk of developing oral cancer compared to non-drinkers, while heavy drinkers (more than 50 g per day) face a fivefold increased risk (5).
Studies have shown that alcohol consumption can lead to LOC through multiple mechanisms (6–9). First, ethanol metabolism in the body produces acetaldehyde, a known carcinogen that can bind to DNA to form adducts, causing DNA damage and mutations, thereby increasing the risk of malignant transformation (10). In addition, ethanol metabolism generates large amounts of reactive oxygen species (ROS), which induce oxidative stress, lipid peroxidation, and DNA damage, while also disrupting cell signaling pathways to promote cell proliferation and metastasis (11). Ethanol can also interfere with DNA methylation and epigenetic modifications, leading to abnormal gene expression and further promoting carcinogenesis (12). Chronic heavy drinking impairs immune system function, allowing malignant cells to escape immune surveillance (13). Moreover, alcohol acts synergistically with other carcinogenic factors, such as tobacco, significantly increasing the risk of LOC (14).
This study, based on data from the Global Burden of Disease Study 2021 (GBD 2021), provides an in-depth analysis of the epidemiological characteristics of lip and oral cavity cancer attributable to high alcohol consumption (LOC-HAC). The research focuses on temporal trends in the age-standardized mortality rates (ASMR) and the age-standardized DALY rates (ASDR) associated with LOC-HAC, revealing its dynamic changes over time. Further analysis shows that gender, age, and Socio-demographic Index (SDI) significantly influence the burden of LOC across different regions and populations. In addition, the study evaluates the contributions of aging, population growth, and epidemiological changes to the LOC-HAC. It also assesses the extent of inequality among countries and projects future trends through 2045. The findings provide critical scientific evidence for the development of public health policies and initiatives aimed at reducing the burden of LOC-HAC, supporting policymakers in implementing targeted strategies to improve global public health outcomes.
Methods
Data sources and disease definition
This study was based on data from the GBD 2021 to analyze the burden of LOC-HAC. LOC refers to malignant tumors of the lip and oral cavity, with ICD-10 codes C00–C08 (3, 15). Disability-adjusted life years (DALYs) were used as the primary measure of health loss, consisting of years of life lost (YLLs) and years lived with disability (YLDs), thereby quantifying the overall disease burden (16–19). Uncertainty intervals (UIs) were used to reflect the reliability of the estimates, generally reported as 95% UIs (16, 20). This means there is a 95% probability that the true value falls within the given range, calculated from the 2.5th and 97.5th percentiles of 1,000 posterior draws. This approach accounts for differences in estimation methods across countries and uncertainties from multiple imputations of missing values. Uncertainty is propagated at each step to ensure that the final UIs fully capture estimation variability. Alcohol consumption was identified as a modifiable behavioral risk factor contributing to the burden of LOC. In GBD 2021, alcohol intake was assessed based on population-based survey data of self-reported consumption. Harmful drinking was defined as alcohol consumption exceeding the theoretical minimum risk exposure level—the level associated with the lowest risk of overall health loss (21).
Decomposition analysis and cross-country inequality analysis
To explore the drivers of changes in disease burden, the Das Gupta decomposition method was applied (22). This statistical technique, widely used in GBD studies, decomposes observed changes in disease burden indicators (e.g., mortality, DALYs) into three independent components: aging, population growth, and epidemiological changes (23). Additionally, cross-country inequality analysis was conducted using the slope index of inequality (SII) and concentration index (CI) to assess socioeconomic disparities in disease burden across countries worldwide (24).
Forecasting analysis
The Nordpred model is a generalized linear model based on the age–period–cohort (APC) framework, widely used to predict epidemiological indicators such as DALY rates and mortality (25, 26). Built upon generalized linear modeling, it incorporates age, period, and cohort effects, and applies linear extrapolation to estimate future disease burden. The mathematical form of the model can be expressed as: log(μijk) = α + βi*Agei + γj*Periodj + δk*Cohortk, where μijk represents the ASDR/ASMR for a specific age group, period, and birth cohort; α is the intercept; and βi, γj, and δk denote the regression coefficients for age, period, and cohort effects, respectively (26–28).
In this study, we used the Nordpred package in R software (version 4.2.1) to perform APC modeling and predict the future burden of LOC-HAC. Age groups were defined in 5-year intervals, and the prediction horizon was set to 24 years. To address uncertainties in future trends, we applied the default trend attenuation scheme of the model to improve robustness.
Results
Global and regional burden of LOC-HAC
In 2021, the global number of DALYs cases from LOC-HAC was 1,191,084 (95% UI: 906,229.2–1,474,007), representing a 90% increase compared with 628,484.1 (95% UI: 493,522.1–754,895.3) in 1990. Middle SDI regions had the highest number of DALYs cases, 372,549.9 (95% UI: 278,922.6–468,908.9), with a percentage change of 192%. The fastest growth occurred in low-middle SDI regions, with a percentage change of 279%. In 2021, global death cases reached 40,038.13 (95% UI: 30,762.25–49,621.09), a 102% increase compared with 19,863.53 (95% UI: 15,571.83–24,071.57) in 1990. Middle SDI regions recorded the highest number of death cases at 12,017.44 (95% UI: 9012.97–15,122.74), with a percentage change of 215%. The fastest growth in death cases occurred in low-middle SDI regions, at 296%. Over the past 32 years, Southeast Asia had the fastest growth among the 21 GBD regions, with DALYs and death cases increasing by 326 and 357%, respectively (Tables 1, 2).
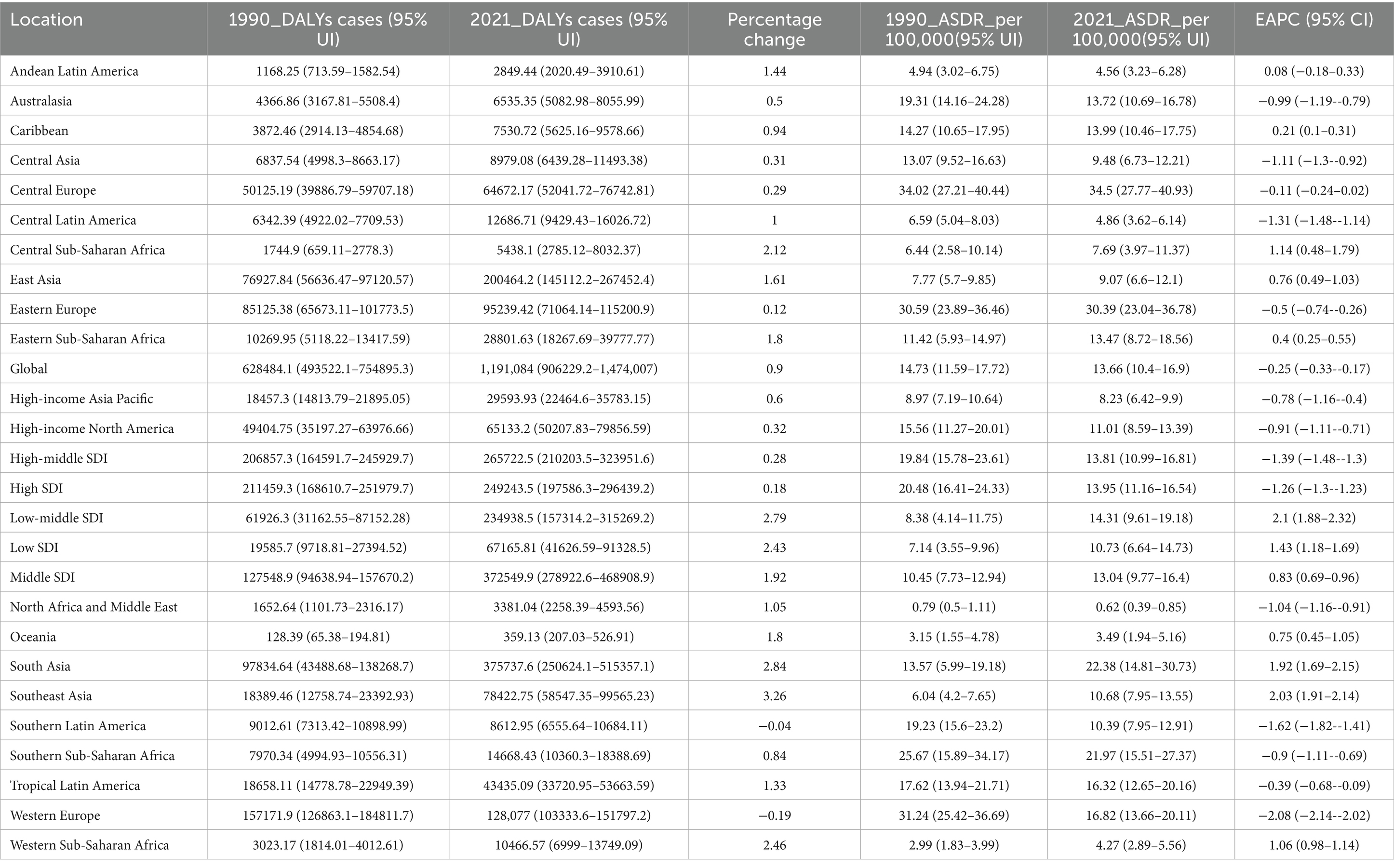
Table 1. Disability-Adjusted Life Years (DALYs) and age-standardized DALY rate (ASDR) of lip and oral cavity cancer attributable to high alcohol consumption in 1990 and 2021, and the PC and EAPC from 1990 to 2021.
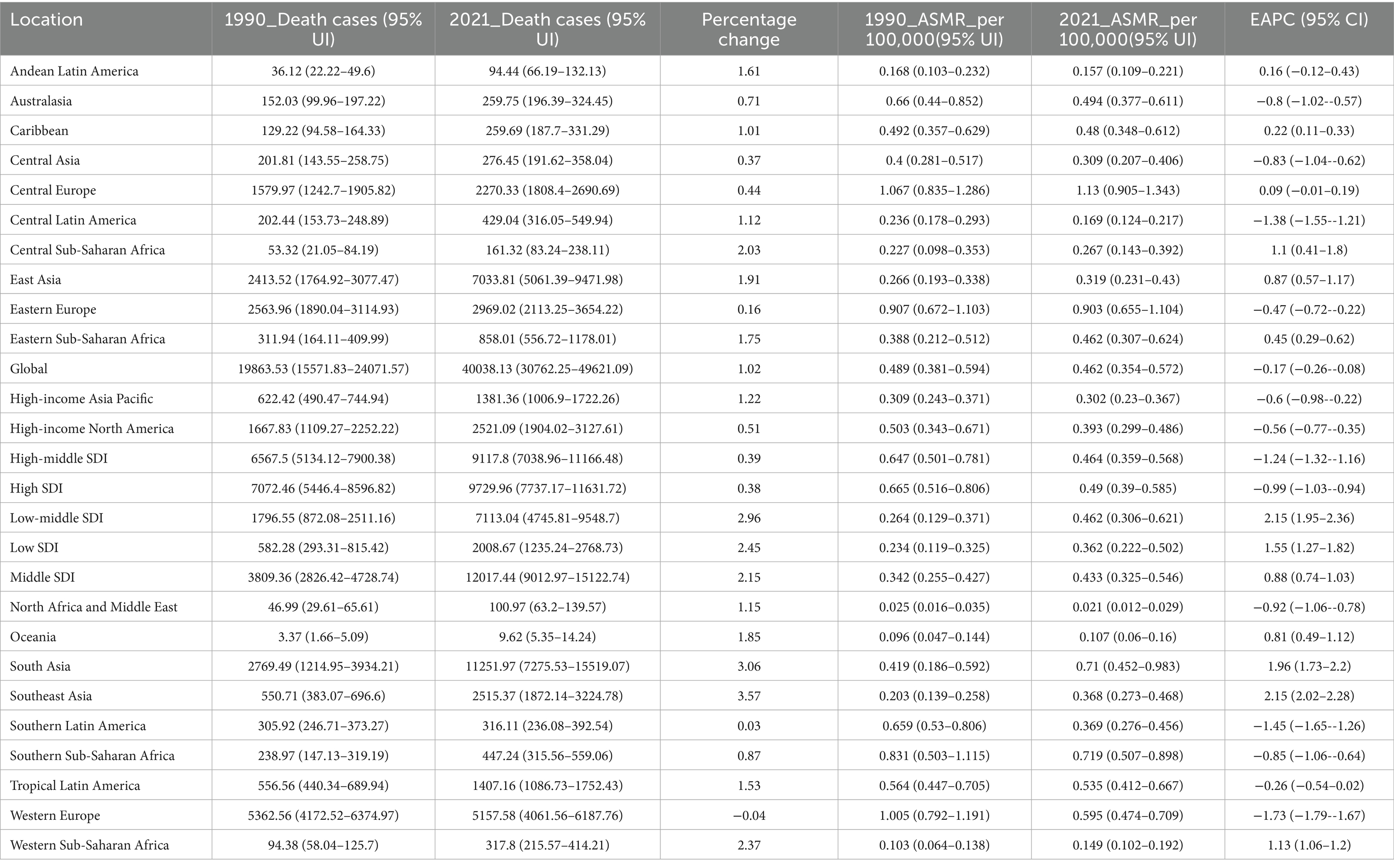
Table 2. Deaths and age-standardized mortality rate (ASMR) of lip and oral cavity cancer attributable to high alcohol consumption in 1990 and 2021, and the PC and EAPC from 1990 to 2021.
In 2021, the global ASDR of LOC-HAC was 13.66 (95% UI: 10.4–16.9) per 100,000 population, with an EAPC of −0.25 (95% CI: −0.33 to −0.17). The highest ASDR was in Central Europe at 34.5 (95% UI: 27.77–40.93) per 100,000. The fastest increase in ASDR occurred in Southeast Asia, with an EAPC of 2.03 (95% CI: 1.91–2.14) (Figure 1). The global ASMR of LOC-HAC was 0.462 (95% UI: 0.354–0.572) per 100,000, with an EAPC of −0.17 (95% CI: −0.26 to −0.08). The highest ASMR was in Central Europe at 1.13 (95% UI: 0.905–1.343) per 100,000. The fastest growth in ASMR was also in Southeast Asia, with an EAPC of 2.15 (95% CI: 2.02–2.28) (Supplementary Figure 1).
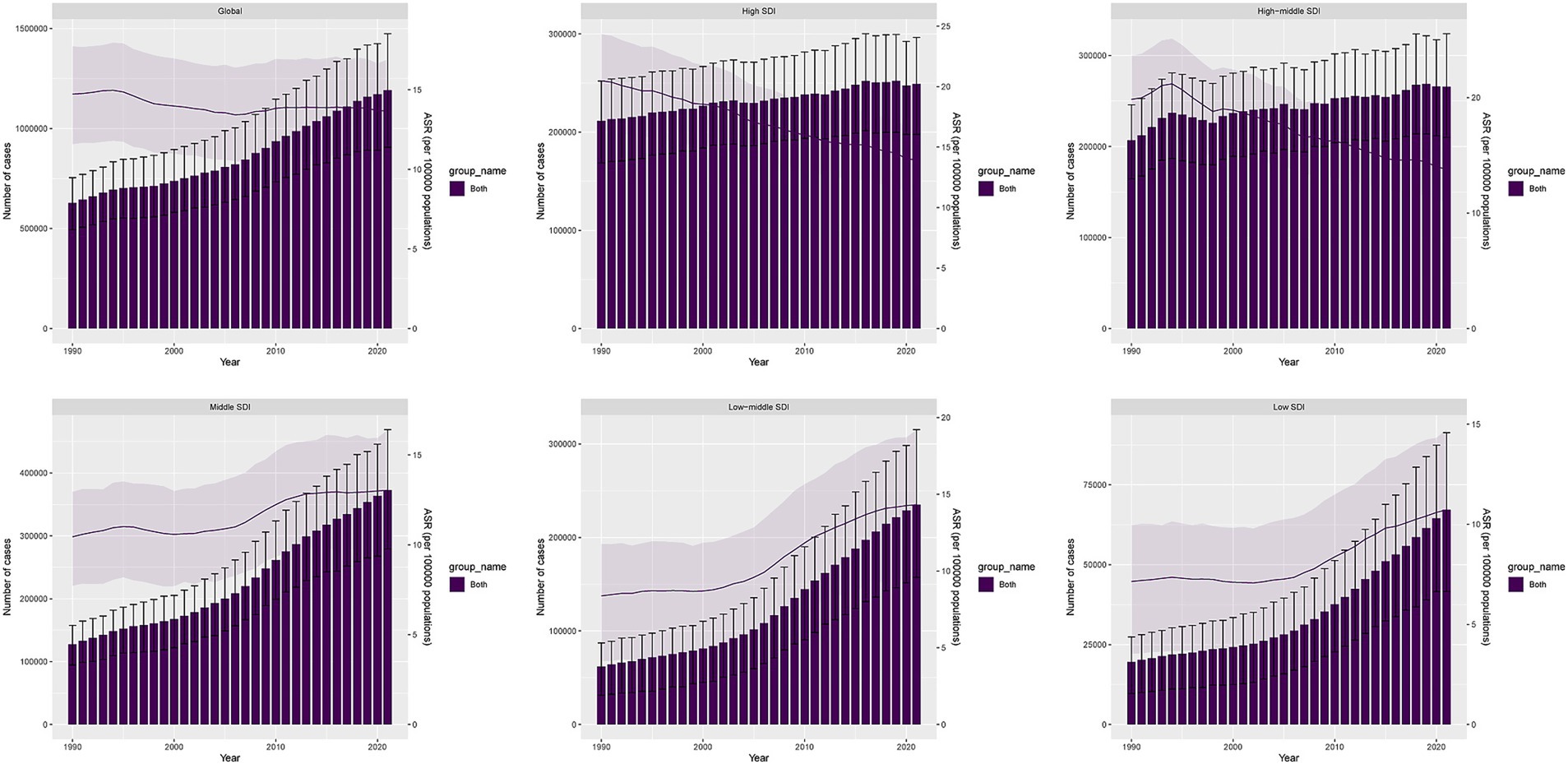
Figure 1. DALYs cases and ASDR of lip and oral cavity cancer attributable to high alcohol consumption from 1990 to 2021.
National Burden of LOC-HAC
From 1990 to 2021, the five countries with the fastest growth in DALYs cases were Iran, Libya, Cape Verde, Viet Nam, and Nepal, with percentage changes of 1,536,100%, 30,485%, 6,955%, 6,924%, and 3,849%, respectively. The five countries with the fastest growth in ASDR were Iran, Libya, Viet Nam, Nepal, and Cape Verde, with EAPCs of 38.43 (95% CI: 31.22–46.04), 11.54 (95% CI: 7.48–15.75), 10.96 (95% CI: 9.47–12.47), 9.44 (95% CI: 8.11–10.78), and 9.05 (95% CI: 6.45–11.71), respectively (Figure 2A and Supplementary Table 1).
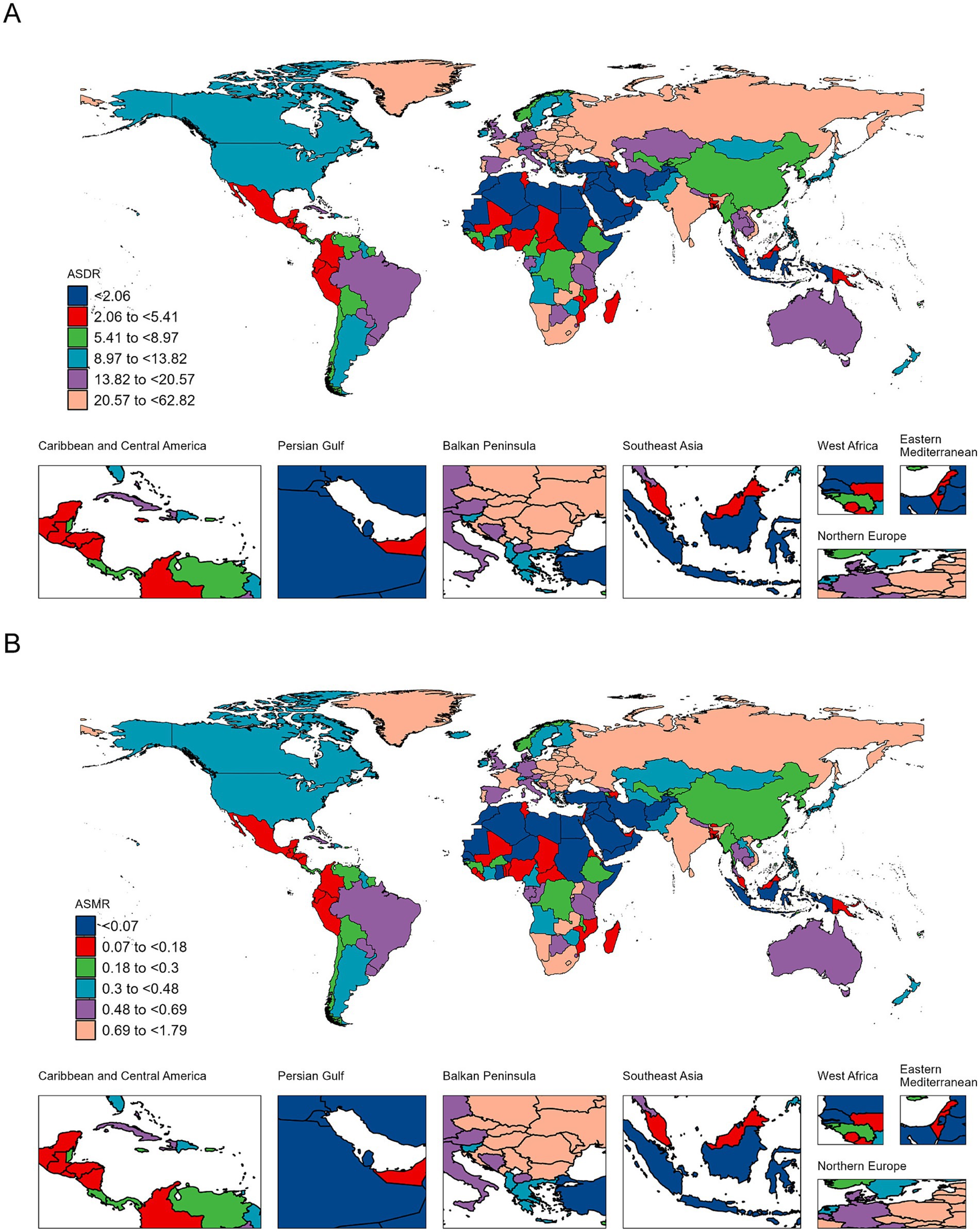
Figure 2. Maps depicting the ASDR (A) and ASMR (B) of lip and oral cavity cancer attributable to high alcohol consumption across 204 countries and territories in 2021.
The five countries with the fastest growth in death cases were Viet Nam, Cape Verde, Nepal, Myanmar, and Cambodia, with percentage changes of 7,526%, 6,120%, 4,403%, 1,501%, and 1,289%, respectively. The five countries with the fastest growth in ASMR were Iran, Libya, Viet Nam, Nepal, and Cape Verde, with EAPCs of 41.04 (95% CI: 33.18–49.36), 11.94 (95% CI: 7.71–16.34), 11.26 (95% CI: 9.72–12.83), 9.77 (95% CI: 8.39–11.17), and 8.9 (95% CI: 6.31–11.56), respectively (Figure 2B and Supplementary Table 2).
Age and sex differences in the burden of LOC-HAC
In 2021, DALYs and death cases in males were significantly higher than in females, and both increased with age. DALYs cases in males peaked in the 55–59 age group, while in females they peaked in the 60–64 age group. For both sexes, death cases peaked in the 60–64 age group. DALYs rates and death rates in males were higher than in females. The highest DALYs rate in males was in the 60–64 age group, whereas in females it was in the 95 + age group. For males and females, the death rate was highest in the 95 + age group (Figures 3A,B).
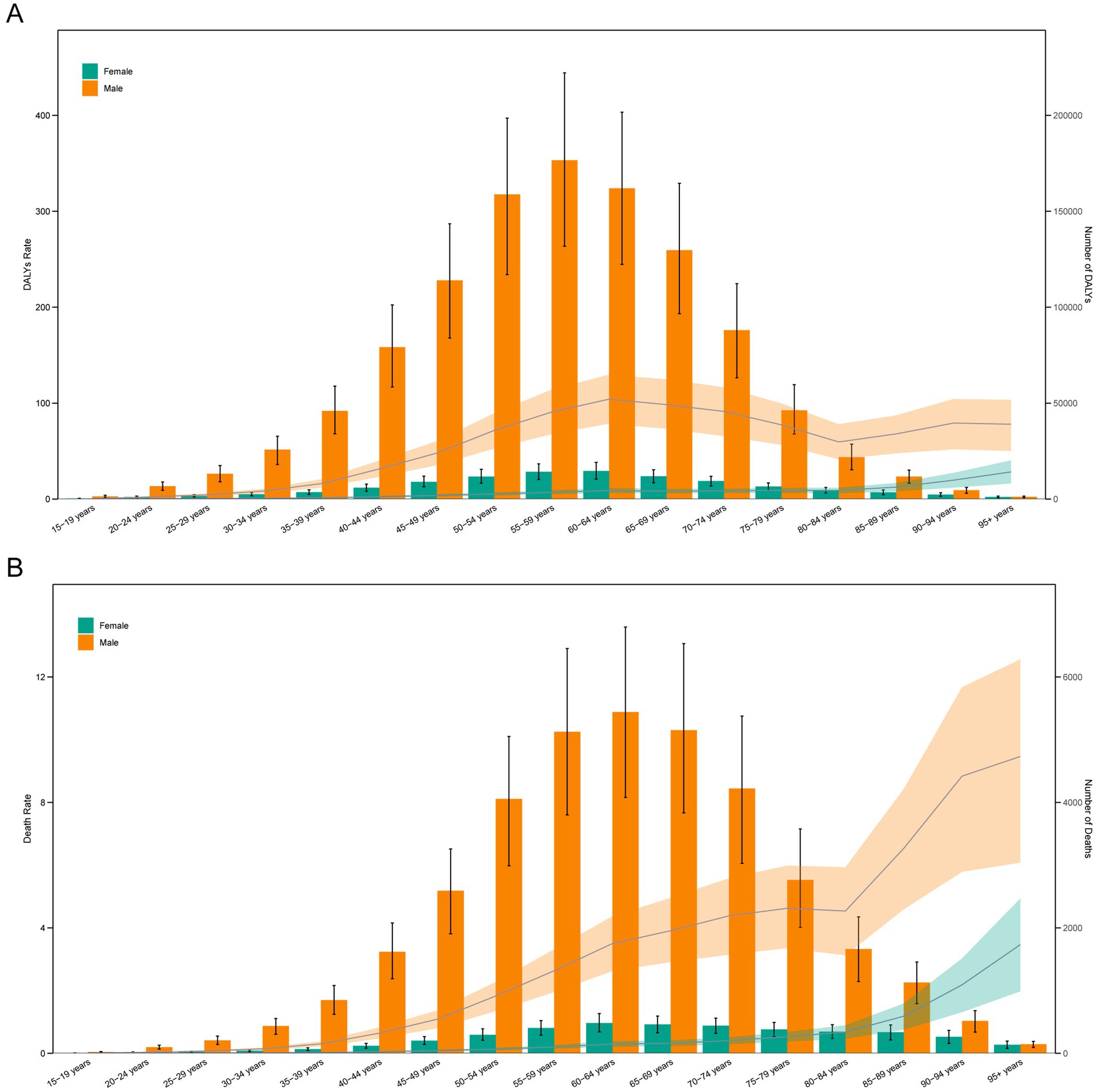
Figure 3. Age-specific numbers and rates of DALYs (A) and deaths (B) of lip and oral cavity cancer attributable to high alcohol consumption by age and sex in 2021.
Relationship between the burden of LOC-HAC and SDI
In 2021, ASDR and ASMR of LOC-HAC showed a significant positive correlation with SDI, indicating that the disease burden increased with higher SDI levels (Figure 4 and Supplementary Figure 2). Specifically, when SDI ranged from 0.6 to 0.75, ASDR and ASMR rose rapidly with increasing SDI. However, when SDI exceeded 0.75, ASDR and ASMR decreased sharply. Notably, regions including Eastern Sub-Saharan Africa, South Asia, Central Europe, Western Europe, and Eastern Europe had burdens significantly higher than expected, whereas North Africa and Middle East, Oceania, Andean Latin America, East Asia, and Southeast Asia had burdens significantly lower than expected, warranting further investigation.
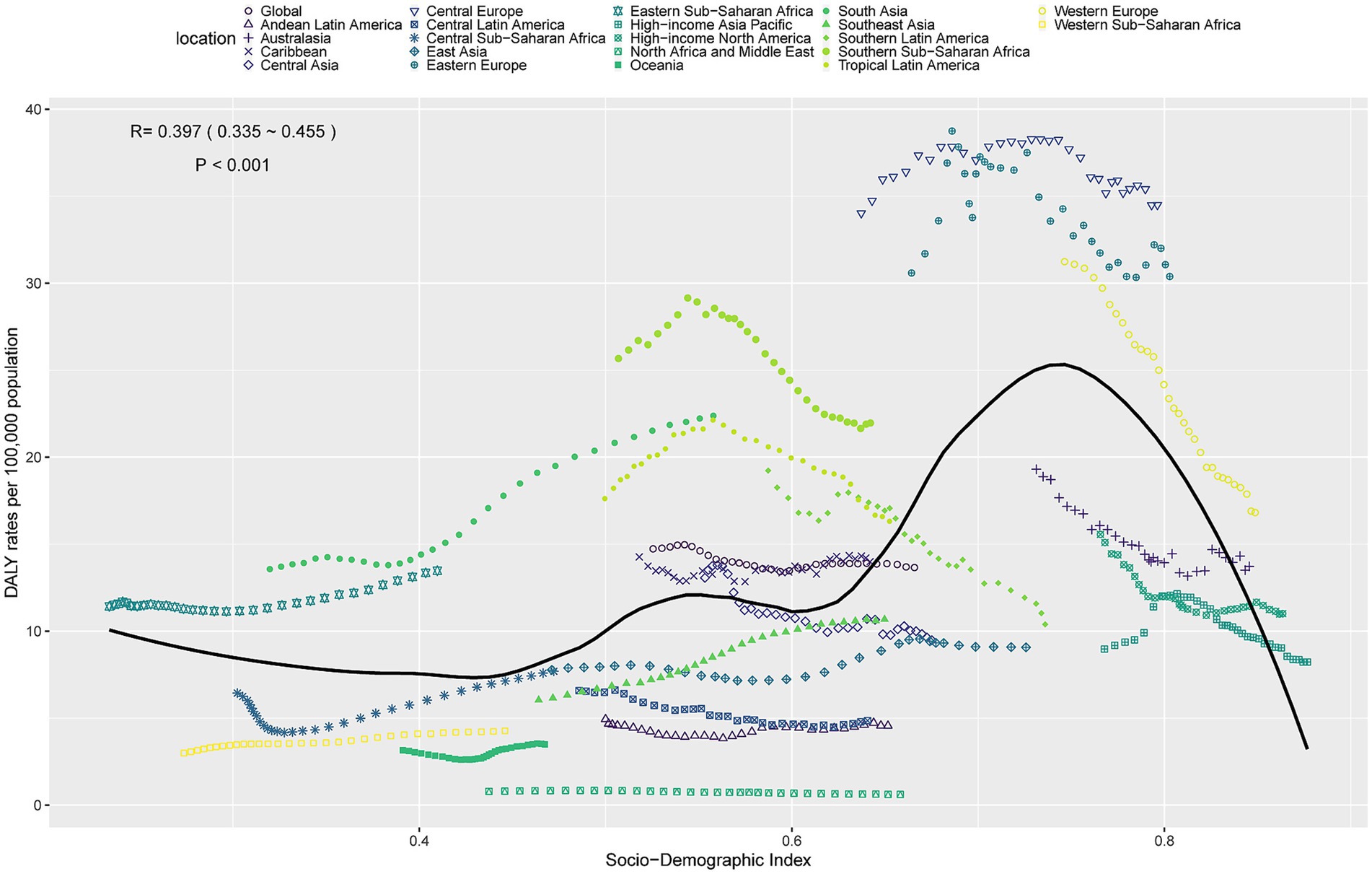
Figure 4. ASDR of lip and oral cavity cancer attributable to high alcohol consumption in 21 GBD regions by SDI, 1990–2021.
Decomposition analysis of the burden of LOC-HAC
Decomposition analysis showed that over the past 32 years, global DALYs cases increased by 562,600.36, of which aging contributed 200,222.09 (35.59%), population growth contributed 432,682.39 (76.91%), and epidemiological change contributed −70,304.13 (−12.5%). Among males, DALYs cases increased by 517,802.3, with aging contributing 186,677.18 (36.05%), population growth contributing 390,698.27 (75.45%), and epidemiological change contributing −59,573.14 (−11.5%). Among females, DALYs cases increased by 44,798.05, with aging contributing 18,886.41 (42.16%), population growth contributing 39,500.81 (88.18%), and epidemiological change contributing −13,589.17 (−30.33%) (Figure 5A).
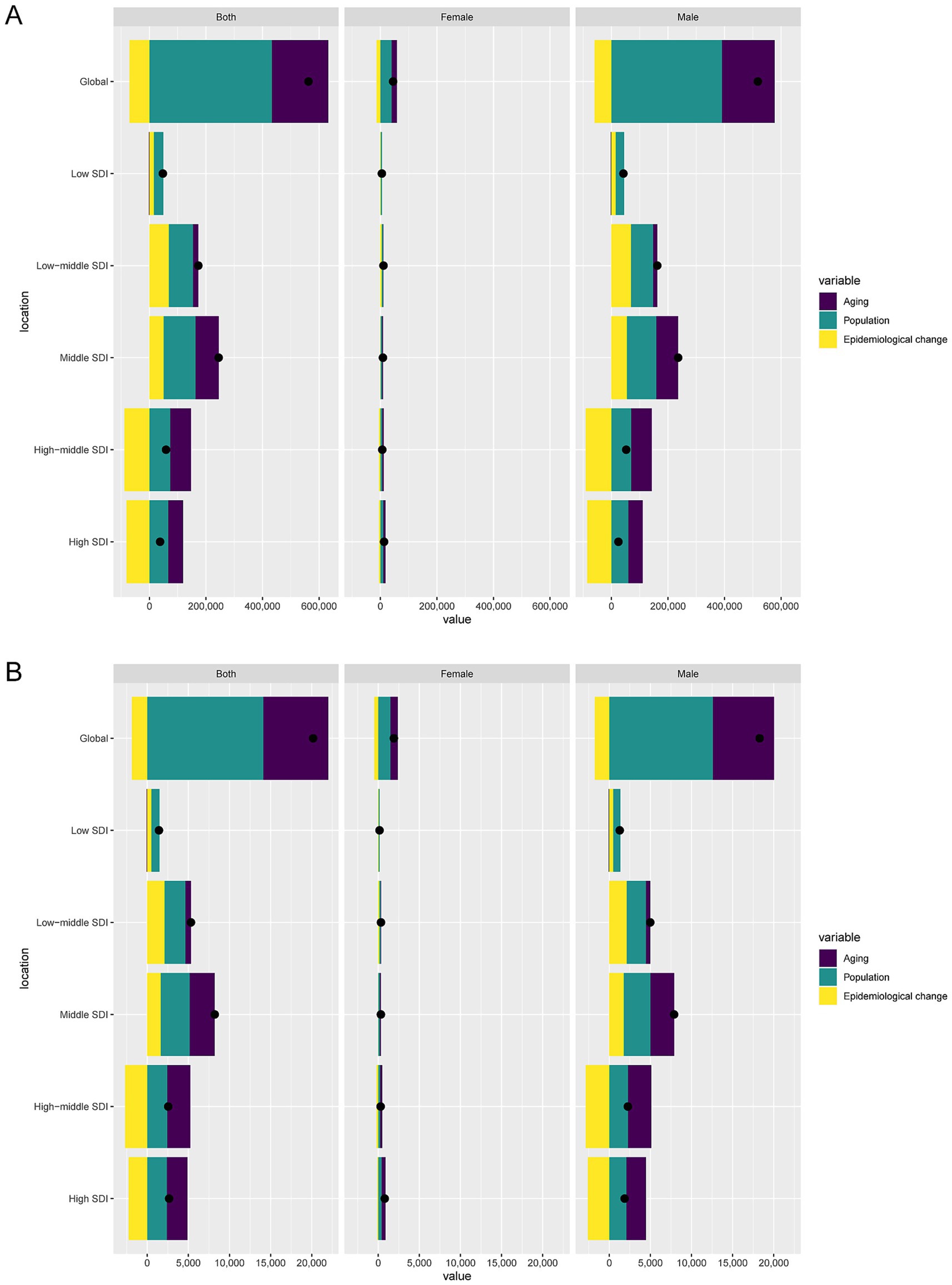
Figure 5. Decomposition analysis of changes in DALYs (A) and deaths (B) of lip and oral cavity cancer attributable to high alcohol consumption between 1990 and 2021 across SDI regions.
Globally, death cases increased by 20,174.61, with aging contributing 7,902.96 (39.17%), population growth contributing 14,121.34 (70%), and epidemiological change contributing −1,849.7 (−9.17%). Among males, death cases increased by 18,276.3, with aging contributing 7,441.35 (40.72%), population growth contributing 12,581.82 (68.84%), and epidemiological change contributing −1,746.87 (−9.56%). Among females, death cases increased by 1,898.31, with aging contributing 917.42 (48.33%), population growth contributing 1,470.21 (77.45%), and epidemiological change contributing −489.33 (−25.78%) (Figure 5B).
Cross-country inequality analysis of the burden of LOC-HAC
Between 1990 and 2021, there were significant health inequalities in LOC-HAC burden across countries with different development levels. Specifically, the SII for DALYs rates increased from 17 in 1990 to 21 in 2021, indicating a widening gap in DALYs rates between the highest-SDI and lowest-SDI regions. The SII for death rates increased from 0.60 in 1990 to 0.84 in 2021. Meanwhile, the CI for DALYs rates decreased from 0.39 in 1990 to 0.19 in 2021, and the CI for death rates decreased from 0.42 to 0.24, suggesting that relative inequality was alleviated. However, higher-SDI regions still bore a heavier disease burden (Figures 6A-D).
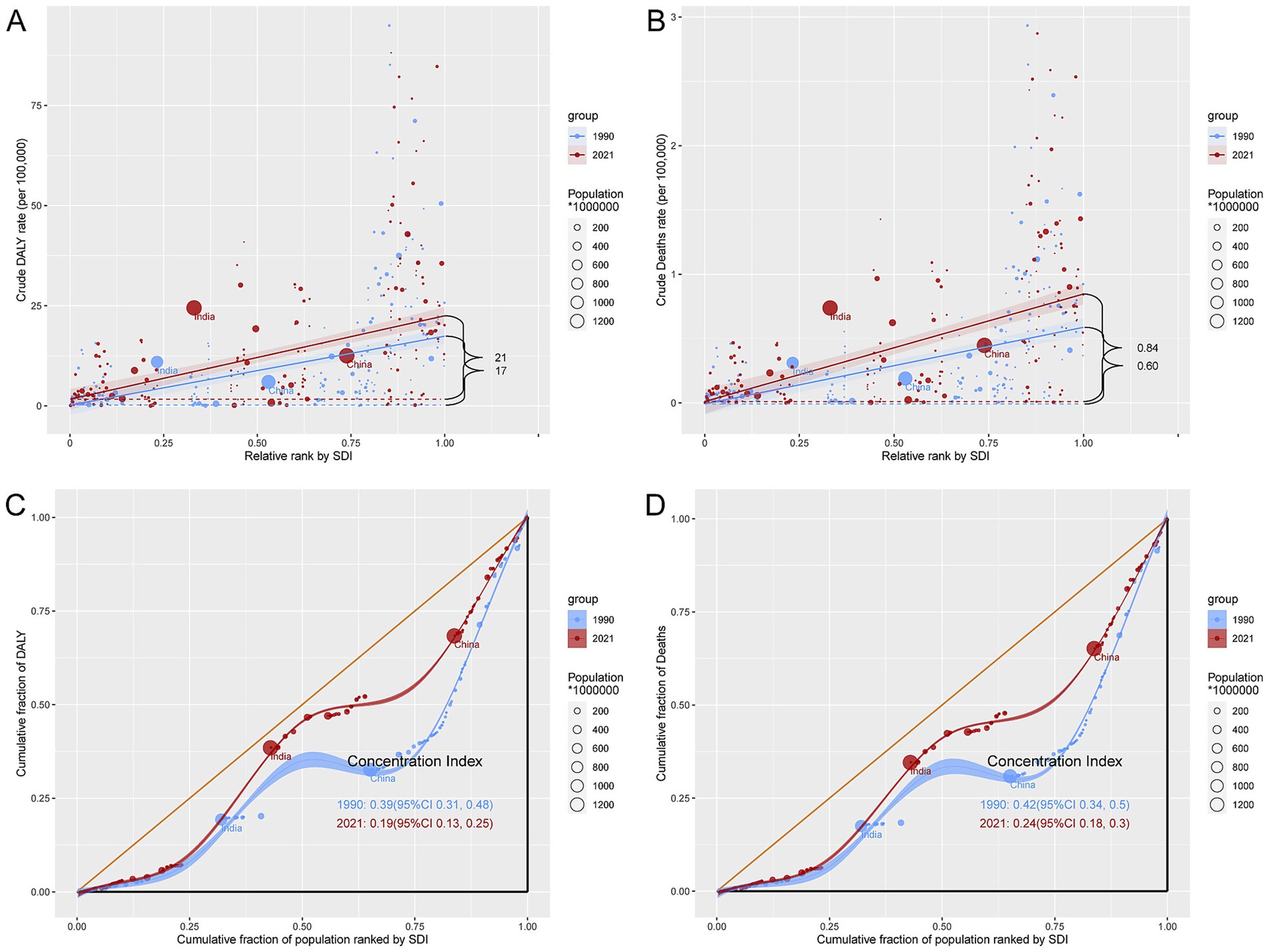
Figure 6. Inequality analysis of DALYs and mortality in lip and oral cavity cancer attributable to high alcohol consumption in 1990 and 2021 across the world. (A) Health inequality regression curves for DALYs. (B) Health inequality regression curves for mortality. (C) Concentration curves for DALYs. (D) Concentration curves for mortality.
Forecast analysis of the burden of LOC-HAC
Forecast analysis suggests that from 2022 to 2045, DALYs and death cases in males will rise significantly, while those in females will increase slowly. Meanwhile, the DALY rates and death rates for males and females will remain relatively stable, with males having much higher DALY rates and death rates than females (Figures 7A,B).
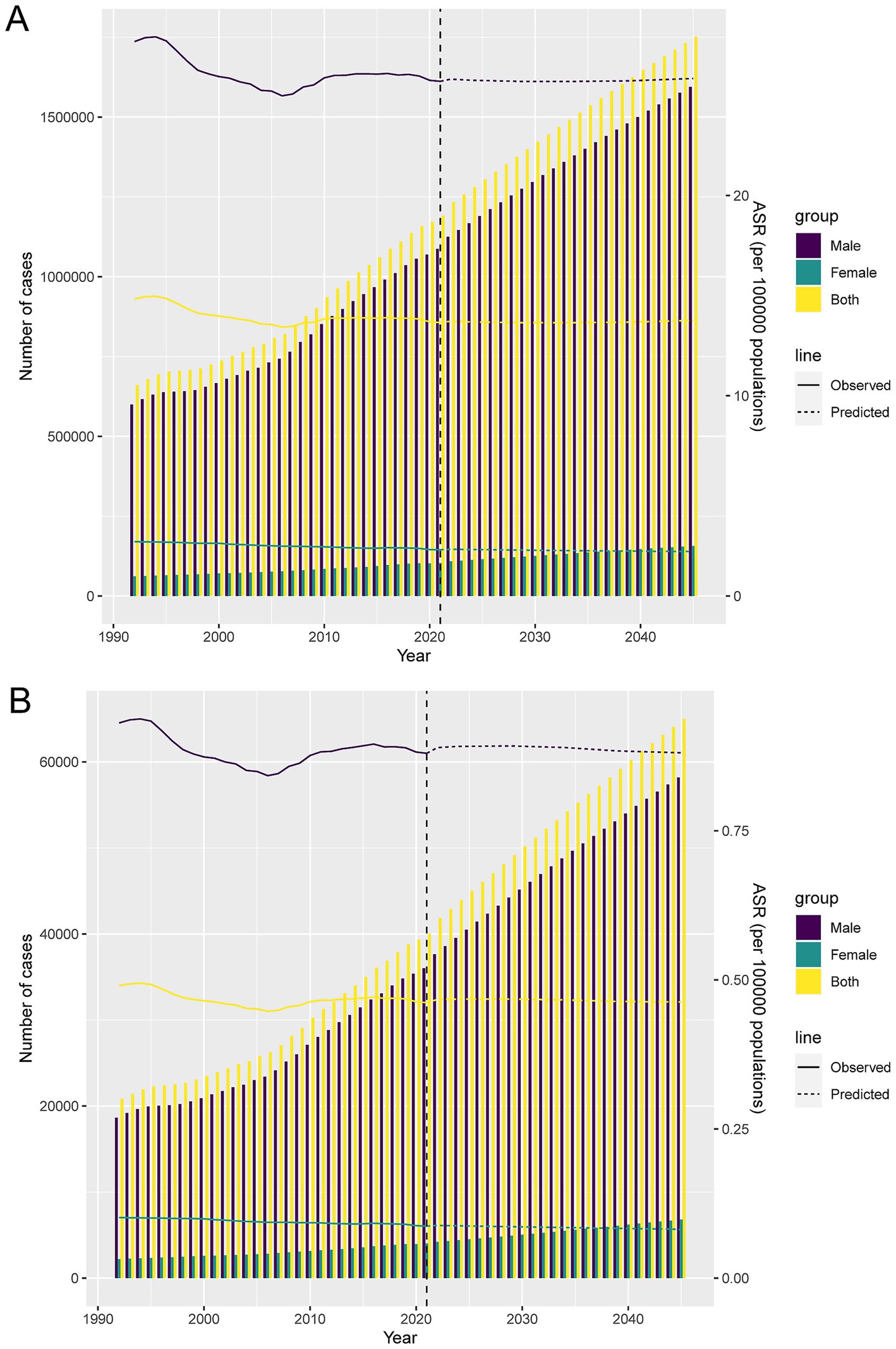
Figure 7. Projections of the temporal trends of the number of DALYs cases, mortality cases, ASDR, and ASMR of lip and oral cavity cancer attributable to high alcohol consumption globally up to 2045. (A) The number and ASDR of lip and oral cavity cancer attributable to high alcohol consumption by year and gender. (B) The number and ASMR of lip and oral cavity cancer attributable to high alcohol consumption by year and gender.
Discussion
The global burden of LOC-HAC has increased significantly over the past few decades, especially in regions with a low to middle SDI and Southeast Asia. In 2021, the number of DALY cases globally had risen by 90% compared to 1990, with the fastest growth occurring in low to middle SDI regions, where the percentage change was 279%. The number of death cases also showed a similar trend, with a 296% increase in low-middle SDI regions. Among the 21 GBD regions, Southeast Asia saw the most significant rise in DALY and death cases, with increases of 326 and 357%, respectively. This may be related to local lifestyle factors, such as betel nut chewing, and inadequate allocation of medical resources (29).
Although global ASDR and ASMR have declined overall, rapid increases in Southeast Asia highlight the need for strengthened health education and medical interventions. Central Europe had the highest ASDR and ASMR, indicating ongoing challenges. In the future, low-middle SDI and Southeast Asia should be prioritized, with measures such as lifestyle improvement, early screening, and optimized healthcare resource allocation to reduce the incidence and mortality of LOC-HAC (30).
From 1990 to 2021, LOC-HAC burden rose markedly in several countries, with Iran, Libya, Cape Verde, Viet Nam, and Nepal experiencing the fastest increases in DALYs and death cases. These findings suggest that these countries may face high-risk behaviors (e.g., smoking, alcohol use) and limited healthcare resources. In Iran, major health system reforms and improved reporting may have contributed to the substantial increases. Some data may also have been influenced by exceptional events such as policy changes or targeted health interventions.
In 2021, DALYs and death cases in males were significantly higher than in females, and both increased with age. Male DALYs peaked at 55–59 years, while female DALYs peaked at 60–64 years. These differences may be due to variations in survival, exposure levels, and diagnostic practices between sexes. Men may be more likely to engage in high-risk behaviors earlier, while women may experience later exposures. Additionally, differences in diagnosis may account for the variation in peak ages.
Although SDI was positively correlated with ASDR and ASMR, both declined when SDI exceeded 0.75. This may be explained by better healthcare access, preventive strategies, and changing alcohol consumption patterns in high-SDI regions. Comprehensive health education, early detection, and effective public health policies in these regions may have reduced the burden of LOC-HAC.
Over the past 32 years, the global disease burden of LOC-HAC has increased significantly, driven mainly by population aging and population growth, while epidemiological changes have had a certain mitigating effect. In addition, global health inequality has become more pronounced between countries at different levels of socio-economic development, with the gap in disease burden between high SDI regions and low SDI regions gradually widening, and high SDI regions still bearing a heavier burden. This means that the improvement in health status in high SDI regions may be faster than that in low SDI regions, or the deterioration in health status in low SDI regions may be more rapid. Therefore, it suggests that policymakers need to pay more attention to low SDI regions in terms of resource allocation and health interventions to narrow the health gap.
Assuming current alcohol consumption trends and policies remain unchanged, forecasts suggest that from 2022 to 2045, DALYs and death cases among males will rise substantially, while increases among females will be modest. ASDR and ASMR are expected to remain relatively stable but consistently higher in males. This underscores the need for interventions targeting high-risk behaviors in men while continuing to address women’s health needs.
Extensive evidence has established alcohol and its metabolite acetaldehyde as Group 1 carcinogens, acting through multiple mechanisms (31). Ethanol metabolism produces acetaldehyde, which damages DNA and impairs repair pathways, and generates ROS that drive oxidative stress and genomic instability (32). Alcohol also alters hormone levels, suppresses immune surveillance, and enhances the carcinogenicity of tobacco and other agents (33). Together, these pathways markedly increase the risk of several cancers, including oral cancer.
Several policy interventions have proven effective in substantially reducing alcohol consumption (34). For instance, increasing taxation on alcoholic beverages has been shown to decrease consumption, with particularly strong effects observed among low-income populations and younger individuals. Similarly, the implementation of minimum unit pricing policies can discourage the excessive intake of inexpensive alcoholic products, thereby mitigating harmful drinking behaviors (34, 35). Moreover, restricting the hours and days of alcohol sales and limiting outlet density have demonstrated efficacy in reducing alcohol availability, leading to lower consumption and associated health risks (36). Given the considerable disease burden of LOC, a multifaceted approach is warranted. In low-middle SDI regions and in Southeast Asia, health education campaigns should be prioritized to improve public awareness of high-risk behaviors, including tobacco use, alcohol consumption, and betel quid chewing, and to promote healthier lifestyle choices. The establishment of early screening programs for LOC is also crucial, particularly in high-incidence countries and among older populations, to enhance early detection and improve treatment outcomes. In parallel, optimizing the allocation of healthcare resources by expanding treatment facilities and increasing the availability of trained specialists in resource-limited settings will be essential. Furthermore, the development and enforcement of alcohol- and tobacco-control policies can reduce the prevalence of high-risk behaviors, with tailored interventions targeting men, who remain disproportionately affected. Finally, strengthening international collaboration to share best practices and coordinate responses will be vital, with a focus on regions and populations carrying the heaviest burden, in order to achieve meaningful reductions in the incidence and mortality of LOC.
This study has some limitations. First, GBD data quality and representativeness in low- and middle-income countries may be limited due to less robust data collection and reporting systems. Second, while this study systematically analyzed epidemiological changes across regions and countries, it did not explore subpopulations (e.g., provincial, urban–rural differences). Third, LOC-HAC may suffer from underreporting or misclassification. Fourth, the COVID-19 pandemic may have affected data collection and reporting for 2021, leading to bias or incompleteness.
Conclusion
Based on GBD 2021 data, this study analyzed global trends in LOC-HAC burden from 1990 to 2021. The results show significant increases in DALYs and death cases, with the greatest rises in low-middle SDI regions and Southeast Asia. Males had higher DALYs cases than females, with peaks at ages 55–59 for males and 60–64 for females. Substantial global health inequalities were observed, with widening absolute differences between the highest and lowest SDI regions. Forecasts suggest that from 2022 to 2045, DALYs and death cases will increase significantly in males, while females will show slower increases. This study recommends prioritizing low-middle SDI and Southeast Asia by promoting healthy lifestyles, strengthening early screening, and optimizing healthcare resource allocation to reduce the incidence and mortality of LOC-HAC.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author/s.
Ethics statement
This research adhered to the principles of the Declaration of Helsinki and complied with applicable local laws. As the study utilized publicly available data, it was exempted from ethical review by the institutional ethics committee.
Author contributions
SP: Writing – review & editing, Writing – original draft, Data curation. WD: Data curation, Writing – review & editing. WC: Investigation, Data curation, Writing – review & editing, Conceptualization. LL: Data curation, Writing – review & editing, Conceptualization, Writing – original draft.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
We sincerely appreciate all the participants of the GBD 2021 for their contribution.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2025.1648788/full#supplementary-material
References
1. Li, Y , Tian, J , You, Y , Ru, C , Zheng, R , Wang, S, et al. Global variations and socioeconomic inequalities in lifetime risk of lip, Oral cavity, and pharyngeal Cancer: a population-based systematic analysis of Globocan 2022. Int J Surg. (2025) 111:3698–709. doi: 10.1097/js9.0000000000002408
2. Dai, R , Zhang, Y , Zou, H , Li, H , and Zhang, S . Increased burden of lip, Oral, and pharyngeal Cancer in adolescents and young adults from 1990 to 2021. BMC Oral Health. (2025) 25:758. doi: 10.1186/s12903-025-06166-0
3. Chen, S , Yang, X , Huang, L , Xie, Y , Li, Y , and Lin, Y . Increasing incidence, prevalence, and mortality of lip and Oral cavity Cancer in adults aged 70 and older globally: findings from Gbd 2021. World J Surg Oncol. (2025) 23:276. doi: 10.1186/s12957-025-03933-9
4. Rumgay, H , Shield, K , Charvat, H , Ferrari, P , Sornpaisarn, B , Obot, I, et al. Global burden of cancer in 2020 attributable to alcohol consumption: a population-based study. Lancet Oncol. (2021) 22:1071–80. doi: 10.1016/s1470-2045(21)00279-5
5. Bagnardi, V , Rota, M , Botteri, E , Tramacere, I , Islami, F , Fedirko, V, et al. Alcohol consumption and site-specific Cancer risk: a comprehensive dose-response Meta-analysis. Br J Cancer. (2015) 112:580–93. doi: 10.1038/bjc.2014.579
6. Seitz, HK , and Stickel, F . Molecular mechanisms of alcohol-mediated carcinogenesis. Nat Rev Cancer. (2007) 7:599–612. doi: 10.1038/nrc2191
7. Reidy, J , McHugh, E , and Stassen, LF . A review of the relationship between alcohol and oral cancer. Surgeon. (2011) 9:278–83. doi: 10.1016/j.surge.2011.01.010
8. Goldstein, BY , Chang, SC , Hashibe, M , La Vecchia, C , and Zhang, ZF . Alcohol consumption and cancers of the Oral cavity and pharynx from 1988 to 2009: an update. Eur J Cancer Prevent. (2010) 19:431–65. doi: 10.1097/CEJ.0b013e32833d936d
9. Koyama, S , Tabuchi, T , Morishima, T , and Miyashiro, I . Alcohol consumption and 10-year mortality in Oral and pharyngeal Cancer. Cancer Epidemiol. (2024) 89:102540. doi: 10.1016/j.canep.2024.102540
10. Seitz, HK , and Stickel, F . Acetaldehyde as an underestimated risk factor for Cancer development: role of genetics in ethanol metabolism. Genes Nutr. (2010) 5:121–8. doi: 10.1007/s12263-009-0154-1
11. Obe, G , Jonas, R , and Schmidt, S . Metabolism of ethanol in vitro produces a compound which induces sister-chromatid exchanges in human peripheral lymphocytes in vitro: acetaldehyde not ethanol is mutagenic. Mutat Res. (1986) 174:47–51. doi: 10.1016/0165-7992(86)90075-8
12. Purohit, V , Rapaka, R , Kwon, OS , and Song, BJ . Roles of alcohol and tobacco exposure in the development of hepatocellular carcinoma. Life Sci. (2013) 92:3–9. doi: 10.1016/j.lfs.2012.10.009
13. Kruman, II , Henderson, GI , and Bergeson, SE . DNA damage and neurotoxicity of chronic alcohol abuse. Exp Biol Med (Maywood). (2012) 237:740–7. doi: 10.1258/ebm.2012.011421
14. Rumgay, H , Murphy, N , Ferrari, P , and Soerjomataram, I . Alcohol and Cancer: epidemiology and biological mechanisms. Nutrients. (2021) 13:173. doi: 10.3390/nu13093173
15. Chen, M , Li, J , Su, W , Huang, J , Yang, C , Li, R, et al. Global burden of lip and Oral cavity Cancer from 1990 to 2021 and projection to 2040: findings from the 2021 global burden of disease study. Cancer Med. (2025) 14:e70957. doi: 10.1002/cam4.70957
16. GBD 2021 Diseases and Injuries Collaborators . Global incidence, prevalence, years lived with disability (Ylds), disability-adjusted life-years (Dalys), and healthy life expectancy (Hale) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the global burden of disease study 2021. Lancet (London, England). (2024) 403:2133–61. doi: 10.1016/s0140-6736(24)00757-8
17. Shedrawy, J , Ernst, P , Lönnroth, K , and Nyberg, F . The burden of disease due to Covid-19 in Sweden 2020-2021: a disability-adjusted life years (Dalys) study. Scand J Public Health. (2023) 51:673–81. doi: 10.1177/14034948231160616
18. Damiri, S , Goharimehr, M , Nasehi, MM , Effatpanah, M , Shahali, Z , Ranjbaran, H, et al. Covid-19 burden in Iran: disability-adjusted life years analysis from hospital data, 2020-2021. Arch Public Health. (2024) 82:135. doi: 10.1186/s13690-024-01355-9
19. Shen, DY , Li, J , Hu, P , Qi, C , and Yang, H . Global, regional, and National Prevalence and disability-adjusted life-years for endometriosis in 204 countries and territories, 1990-2019: findings from a global burden of disease study. Eur J Obstet Gynecol Reprod Biol X. (2025) 25:100363. doi: 10.1016/j.eurox.2024.100363
20. GBD 2021 US Burden of Disease Collaborators . The burden of diseases, injuries, and risk factors by state in the USA, 1990-2021: a systematic analysis for the global burden of disease study 2021. Lancet (London, England). (2024) 404:2314–40. doi: 10.1016/s0140-6736(24)01446-6
21. Lu, Z , Yang, S , Dai, M , Wu, G , Wang, F , and Zhang, K . Global burden of nasopharyngeal carcinoma attributable to alcohol use: a 1990-2021 analysis with projections to 2040. Front Public Health. (2025) 13:1623089. doi: 10.3389/fpubh.2025.1623089
22. Zhang, L , Zhang, J , Guo, Y , and Yan, J . The disease burden of Ild at the global, regional, and National Levels from 1990 to 2021, and projections until 2035: the 2021 global burden of disease study. Front Med. (2025) 12:1637654 20: 44. doi: 10.3389/fmed.2025.1637654
23. Zhou, J , Zhu, J , Zhang, P , Tao, C , Hong, X , and Zhang, Z . Global, regional, and national burdens of Clostridioides difficile infection over recent decades: a trend analysis informed by the global burden of disease study. Microbiol Spectr. (2025) 13:e0129024. doi: 10.1128/spectrum.01290-24
24. Zhao, M , Zheng, Y , and Chen, Z . Analysis of the burden of colorectal Cancer attributable to high body mass index in 204 countries and regions worldwide from 1990 to 2021. Front Nutr. (2025) 12:1589250. doi: 10.3389/fnut.2025.1589250
25. Chenyu, L , Haochao, L , Pengfei, C , Mingjian, C , Diming, Z , and Liqing, W . Global, regional, and national burden of non-rheumatic valvular heart diseases in women: a systematic analysis of global burden of disease 1990-2021. Glob Heart. (2025) 20:33. doi: 10.5334/gh.1422
26. Møller, B , Fekjaer, H , Hakulinen, T , Sigvaldason, H , Storm, HH , Talbäck, M, et al. Prediction of Cancer incidence in the Nordic countries: empirical comparison of different approaches. Stat Med. (2003) 22:2751–66. doi: 10.1002/sim.1481
27. Riebler, A , and Held, L . The analysis of heterogeneous time trends in multivariate age-period-cohort models. Biostatistics (Oxford, England). (2010) 11:57–69. doi: 10.1093/biostatistics/kxp037
28. Bray, F , and Møller, B . Predicting the future burden of cancer. Nat Rev Cancer. (2006) 6:63–74. doi: 10.1038/nrc1781
29. Fan, KM , Rimal, J , Zhang, P , and Johnson, NW . Stark differences in Cancer epidemiological data between Globocan and Gbd: emphasis on Oral Cancer and wider implications. EClinicalMedicine. (2022) 54:101673. doi: 10.1016/j.eclinm.2022.101673
30. Yu, Z , Wu, Y , Cao, Y , and Cheng, P . Epidemiological trends and age-period-cohort effects on lip and Oral cavity Cancer burden across the Brics from 1992 to 2021. Front Oncol. (2025) 15:1539417. doi: 10.3389/fonc.2025.1539417
31. Okaru, AO , and Lachenmeier, DW . Margin of exposure analyses and overall toxic effects of alcohol with special consideration of carcinogenicity. Nutrients. (2021) 13:785. doi: 10.3390/nu13113785
32. Tagaino, R , Washio, J , Otani, H , Sasaki, K , and Takahashi, N . Bifacial biological effects of ethanol: acetaldehyde production by Oral Streptococcus species and the antibacterial effects of ethanol against these Bacteria. J Oral Microbiol. (2021) 13:1937884. doi: 10.1080/20002297.2021.1937884
33. Lachenmeier, DW , and Monakhova, YB . Short-term salivary acetaldehyde increase due to direct exposure to alcoholic beverages as an additional Cancer risk factor beyond ethanol metabolism. J Exp Clin Cancer Res. (2011) 30:3. doi: 10.1186/1756-9966-30-3
34. Kilian, C , Lemp, JM , Llamosas-Falcón, L , Carr, T , Ye, Y , Kerr, WC, et al. Reducing alcohol use through alcohol control policies in the general population and population subgroups: a systematic review and Meta-analysis. EClinicalMedicine. (2023) 59:101996. doi: 10.1016/j.eclinm.2023.101996
35. Jiang, H , Livingston, M , Room, R , Callinan, S , Marzan, M , Brennan, A, et al. Modelling the effects of alcohol pricing policies on alcohol consumption in subpopulations in Australia. Addiction. (2020) 115:1038–49. doi: 10.1111/add.14898
Keywords: lip and oral cavity cancer, high alcohol consumption, global burden of disease, DALYs, SDI, epidemiological trends
Citation: Pang S, Duan W, Chen W and Lu L (2025) Global burden of lip and oral cavity cancer attributable to high alcohol consumption from 1990 to 2021. Front. Nutr. 12:1648788. doi: 10.3389/fnut.2025.1648788
Edited by:
Ruchi Roy, University of Illinois Chicago, United StatesReviewed by:
Konda Mani Saravanan, Bharath Institute of Higher Education and Research, IndiaXiaoyi Zhang, Jacobi Medical Center, United States
Copyright © 2025 Pang, Duan, Chen and Lu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Le Lu, MzA2OTg4NjQ0QHFxLmNvbQ==
†These authors have contributed equally to this work