 Guillermo Salinas-Escudero1
Guillermo Salinas-Escudero1 Daniela De la Rosa-Zamboni2*
Daniela De la Rosa-Zamboni2* María Fernanda Carrillo-Vega3
María Fernanda Carrillo-Vega3 Ana Estela Gamiño-Arroyo4
Ana Estela Gamiño-Arroyo4 Filiberto Toledano-Toledano5,6,7
Filiberto Toledano-Toledano5,6,7 Fernando Ortega-Riosvelasco8
Fernando Ortega-Riosvelasco8 Víctor Granados-García9
Víctor Granados-García9 Mónica Villa-Guillén10
Mónica Villa-Guillén10 Juan Garduño-Espinosa11
Juan Garduño-Espinosa11- 1Center for Economic and Social Studies in Health, Hospital Infantil de México Federico Gómez, Mexico City, Mexico
- 2Subdirector Comprehensive Patient Attention, Hospital Infantil de México Federico Gómez, Mexico City, Mexico
- 3Research Department, Instituto Nacional de Geriatría, Mexico City, Mexico
- 4Hospital Epidemiology Department, Hospital Infantil de México Federico Gómez, Mexico City, Mexico
- 5Unidad de Investigación en Medicina Basada en Evidencias, Hospital Infantil de México Federico Gómez, National Institute of Health, Mexico City, Mexico
- 6Unidad de Investigación Sociomédica, Instituto Nacional de Rehabilitación Luis Guillermo Ibarra Ibarra, Mexico City, Mexico
- 7Dirección de Investigación y Diseminación del Conocimiento, Instituto Nacional de Ciencias e Innovación para la Formación de Comunidad Científica, INDEHUS, Mexico City, Mexico
- 8Head of Hospital Epidemiology Department, Hospital Infantil de México Federico Gómez, Mexico City, Mexico
- 9Epidemiological and Health Services Research Unit Aging Area, Centro Médico Nacional, Mexico City, Mexico
- 10Medical Director, Hospital Infantil de México Federico Gómez, Mexico City, Mexico
- 11Research Director, Hospital Infantil de México Federico Gómez, Mexico City, Mexico
Background: An automated hand-hygiene monitoring system (AHHMS) was implemented in October 2019 at the Hospital Infantil de México Federico Gómez (HIMFG), a tertiary pediatric referral hospital, in four of the hospital wards with the highest rates of Healthcare Associated Infections (HAIs). The clinical and economic impact of this system had not yet been assessed prior to this study. This study aimed to evaluate if the AHHMS is a cost-effective alternative in reducing HAIs in the HIMFG.
Methodology: A full cost-effectiveness economic assessment was carried out for the hospital. The alternatives assessed were AHHMS implementation vis-a-vis AHHMS non-implementation (historical tendency). The outcomes of interest were infection rate per 1,000 patient-days and cost savings as a result of prevented infections. Infection rate data per 1,000 patient-days (PD) were obtained from the hospital's Department of Epidemiology with respect to the AHHMS. As regards historical tendency, an infection-rate model was designed for the most recent 6-year period. Infection costs were obtained from a review of available literature on the subject, and the cost of the implemented AHHMS was provided by the hospital. The assessment period was 6 months. The incremental cost-effectiveness ratio was estimated. Costs are reported in US Dollars (2021). Univariate sensitivity and threshold analysis for different parameters was conducted.
Results: The total estimated cost of the AHHMS alternative represented potential savings of $308,927–$546,795 US Dollars compared to non-implementation of the system (US$464,102 v. US$773,029–$1,010,898) for the period. AHHMS effectiveness was reflected in a diminished number of infections, 46–79 (−43.4–56.7%) compared to non-implementation (60 v. 106-139 infections).
Conclusion: The AHHMS was found to be a cost-saving alternative for the HIMFG given its cost-effectiveness and lower cost vis-a-vis the alternate option. Accordingly, the recommendation was made of extending its use to other areas in the hospital.
Introduction
Level 1A of Evidence for Clinical Practice Guidelines (1, 2) establishes that hand hygiene (HH) prevents Healthcare Associated Infections (HAIs), these being among the costliest health care risks as regards lives and financial resources worldwide (3). Despite all evidence published in the last two centuries on this subject, and notwithstanding that it has become a worldwide standard for patient safety (4), optimal full adherence to HH protocols at hospitals is still a complex task (5, 6). Performing HH as recommended by WHO guidelines requires not only behavioral changes from health care workers (HCWs), training and constant assessment and feedback, but also an institutional environment that promotes safety by the placement of reminder posters at the workplace. Various studies have reported that hand cleansing is a cost-effective strategy (7–10).
Systems to foster, monitor and improve HH compliance have been developed; among these electronically assisted/enhanced or video monitoring direct surveillance systems, electronic dispenser counters, and automated HH monitoring networks (11). Automated HH monitoring (AHHM) systems offer the advantage of providing constant and individualized feedback on protocol compliance. Generally, an AHHMS includes personalized ID tags for each health care worker; this device establishes wireless contact with alcohol-rub dispensers, after which the information is relayed to a central system that measures HH performance in real time. The success of AHHM systems in improving HH performance has been reported in a number of countries (3), but very little has been said in regard to their impact on HAI rates, as focus has been directed towards assessing compliance, an intermediate stage in the ultimate desired outcome of HAI reduction, which is the main purpose of all HH programs. Consequently, there is no clear evidence as yet showing that the implementation of an AHHMS is a cost-effective alternative for hospitals and health care facilities.
Although Guest FJ. (12) published an assessment based on an economic model, the study takes into consideration theoretical HAI reductions, and does not take into account efficacy and effectiveness data. A study by S. McCalla reports a significant reduction in HAI infection rates, in catheter-associated urinary tract infections: IRR of 0.55, 95% CI, 0.35–0.87, and in central line-associated bloodstream infections: IRR of 0.45; 95% CI, 0.23–0.89 (13). This study aimed at assessing if the “AIDY” AHHMS implemented at the Hospital Infantil de México Federico Gómez (HIMFG) in October 2019 was a cost-effective technological strategy which contributed to the reduction in nosocomial HAIs.
Methodology
A full cost-effectiveness economic assessment on the implementation of the AHHMS was carried out for the hospital. Both the clinical and economic impacts of this technology were evaluated. The compared inputs in the analysis were the AHHMS (intervention) against manual or traditional monitoring (control).
The HIMFG is a public pediatric tertiary referral hospital located in Mexico City. The hospital has well-established HH-compliance protocols which have rendered good outcomes (5). The AHHMS was implemented for all beds in four hospital wards which were chosen on the basis of internet availability, and for all resident physicians and nurses.
The AHHMS was implemented in wards 1 and 2 in October 2019, and in January and February 2020 in wards 3 and 4. Monthly records from all of the wards were obtained until March 2020 when data gathering was interrupted as hospital facilities were subject to COVID-19 reconversion due to the SARS-CoV-2 pandemic outbreak, which prevented gathering of HH unbiased measurements of adherence levels and hospital HAI rates due to the special COVID 19 HH protocols.
Effectiveness
Effectiveness in this analysis was measured as the infection rate per 1,000 Patient Days (PD). Effectiveness of the intervention group was the infection rate reported by the Department of Epidemiology of the hospital for the 2019–2020 period analyzed. This rate was estimated on the basis of the information obtained from wards 1 and 2 for up to 6 monthly monitored opportunities. As regards wards 3 and 4, the length of the observation period was shorter.
Effectiveness of the control group (non-implementation option) was the infection rate per 1,000 PD as estimated by regression models. A polynomial regression model was used for each ward. Expected infection rates were calculated on the basis of the tendency of the previous six-year period from 2013 to 2019 (during the same months taken into account for the intervention).
The estimated infection rate allowed us to calculate the potential number of infections for the non-implementation alternative for each ward, and thus allowed us to make the assessment in terms of the resulting infection rate per 1,000 hospitalized patients and in terms of prevented infections.
Due to the departure from normality of the infection rate data of all wards (Shapiro-Wilk test), polynomial regressions were applied to the 2013–2019 data to achieve good expected predictive values for the 2019–2020 infection rates with a minimum regression coefficient (R2) of 84%. The infection-treatment cost used in the model was US$7,288.37 (14) for a tertiary pediatric hospital in Mexico, adjusted for inflation as of December 2021 (15), expressed in US Dollars [at an exchange rate of $20.46 Pesos Mex. Cy. per US$1.00 (16)]. The cost of the “AIDY” AHHMS reported by the HIMFG is US$1.64 per day per bed. Costs of hand-cleansing agents (such as alcohol rub, soap, water etc.) were not included in the analysis as these are available throughout the hospital as part of its “Let's hit 100” HH program (5), do not depend on the automated monitoring program and should therefore not affect the relationship between the relative costs of the two alternatives.
Approval from the Research and Ethics Committee of the HIMFG for the study was obtained and recorded under registration numbers HIM/2015/048 and HIM/2017/134. Data used in the analysis did not include sensitive information of the patients treated in the hospital during the study period and were restricted to the records provided by the hospital Epidemiology Department.
Cost-effectiveness model
A deterministic mathematical model was constructed for the baseline case which was represented by a decision tree to compare the two management alternatives: AHHMS intervention group v. the non-intervention group (manual/regular surveillance).
The model was built for a cohort of patients admitted at the HIMFG who were provided care under two scenarios: one in which an AHHMS was used, and the other where healthcare was provided under the traditional or regular HH surveillance system. Infection rates were determined on the basis of actual infections occurring while the AHHMS was in use, and for the traditional scenario, the rates were those estimated on the basis of infection rates per 1,000 PD for each of the alternatives (Figure 1).
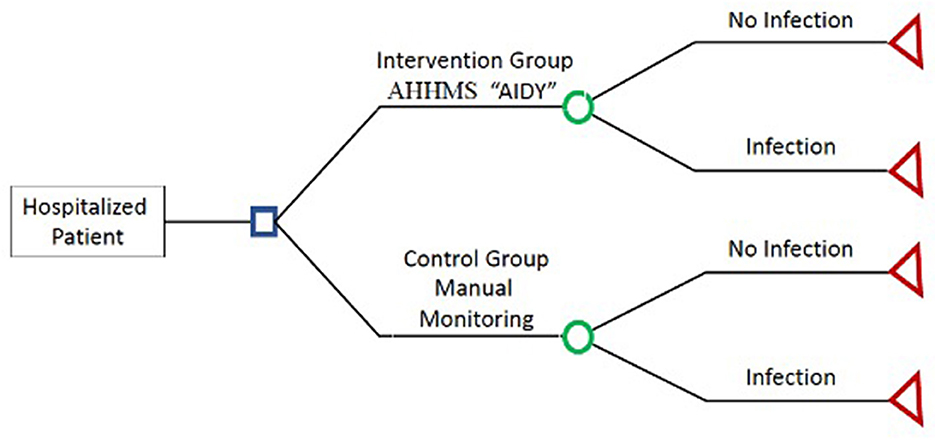
Figure 1. Cost effectiveness decision tree.
The time horizon for the economic evaluation was set at 6 months, and therefore a discount rate was not applied to health outcomes nor was it applied to costs. The expected model outcomes were global costs of each one of the alternatives. For the intervention group the cost of the automated program plus the cost of the reported infections were considered. As regards the control group, the sole cost taken into consideration was the healthcare costs of the infections occurring during the study period. The incremental cost-effectiveness ratio (ICER) was calculated by dividing incremental cost (Costs 1-Costs 2) by the effectiveness (Effectiveness1—Effectiveness2) of each of the compared alternatives, where alternative 1 is the AHHMS v. alternative 2 the traditional surveillance system.
Sensitivity analysis
Threshold univariate sensitivity analysis was conducted for two scenarios contemplated, to ascertain the robustness of the main parameters of the model base case where greater uncertainty was assumed.
The first scenario involved the assessment of the cost per infection, as per the effectiveness reported by the AHHMS and the number of prevented infections at which the implementation of this program ceased to be economically advantageous for the HIMFG.
In this scenario, cost for the period for each ward with the AHHMS intervention was divided by the number of prevented infections and then compared to the number of infections occurring under the non-intervention alternative.
The second scenario also involved sensitivity analysis to assess which was the lowest number of infections in the base case (the cost per bed of the AHHMS remaining constant) at which the AHHM program ceased to be economically advantageous for the HIMFG. In this second scenario, cost for the period for each ward with the AHHMS intervention was divided by the cost of infection considered in the base case.
Computations were done on Microsoft Excel and cost-effectiveness analysis was conducted with TreeAge Pro v. 2009.
Results
Table 1 shows HAI rates per 1,000 PD for the wards under study, the 2019–2020 values are those recorded at the time the “AIDY” AHHMS was implemented. Central tendency measures (mean and SD) can be appreciated. Ward 2 presented the highest HAI rate, 7.3 infections/1000 PD (SD 3.3), followed by wards 3, 1, and 4.
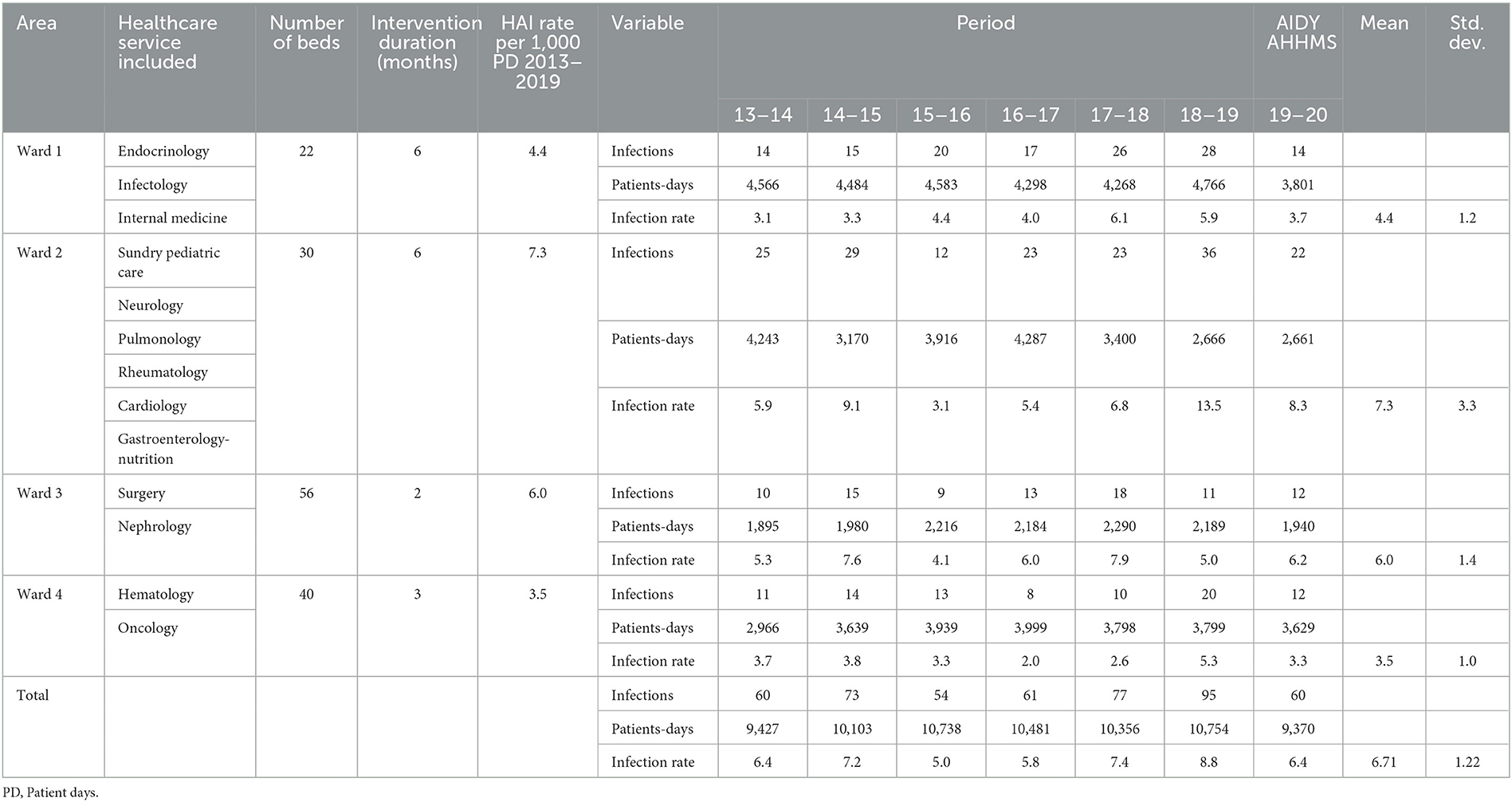
Table 1. Characteristics of the HIMFG wards 2013–2020.
Table 2 shows the polynomial equations used to obtain infection-rate projected values during the 2019–2020 period for the four wards, as well as regression coefficient R2 and the projected value for the model for the same period.
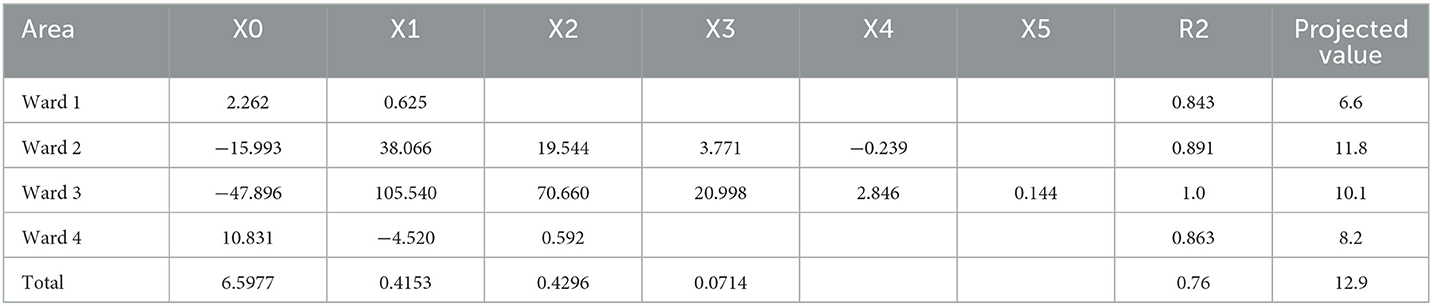
Table 2. Polynominal equations.
When comparing the results of projected infection rates v. the values obtained for the AIDY AHHMS for the 2019–2020 period for the different wards, as well as the number of prevented infections with the AIDY AHHMS intervention (Table 3), a general reduction in the number of infections is observed. This difference was statistically significant (P < 0.01) with the Z-test used to establish rate differences for all wards.
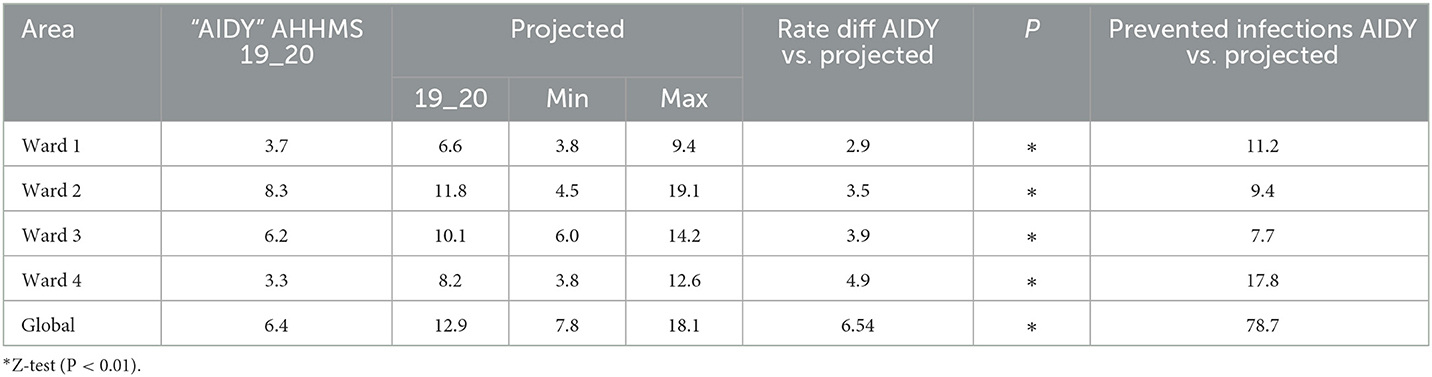
Table 3. Infection rates.
The cost of the AHHM program ranged from $5,409 to $8,939 during the study period for each of the different wards, depending on the number of beds and the time the beds were included, representing a total cost of $26,800 for the four wards as shown in Table 4.
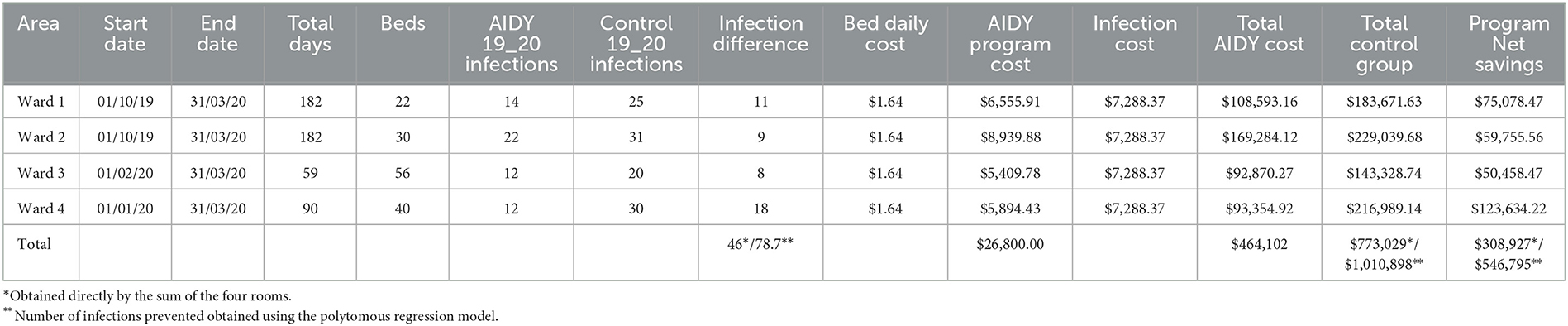
Table 4. Costs of the alternatives.
Total cost for the AHHM alternative, which included both the cost of the program and infection treatment costs were in the range of $92,870 to $169,284, representing a global cost for the hospital of $464,102. In regard to the non-intervention alternative, costs ranged from $143,328 to $229,039, depending on the ward, representing a global expenditure for the hospital of $773,029. Thus, implementation of the AHHM program resulted in net savings in the range of $50,458 to $123,634; and an amount of $308,629 in savings during the study period.
Cost-effectiveness outcomes (base case)
In assessing total costs for each alternative, we found that such costs for implementing the AHHM program in the four wards were lower than those of the non-implementation alternative for the study period (Table 5), resulting in savings in the $50,458 to $123,634 range. With respect to effectiveness, we observed that the number of infections in all wards was lower in the AHHM intervention group when compared to the non-intervention group, keeping in mind that best outcomes are those with the lowest number of infections. Finally, ICER in all wards of the non-intervention group was markedly surpassed by that of the AHHM, as the latter's outcomes were lower numbers of infections at lesser cost for the HIMFG making it a cost-saving alternative.
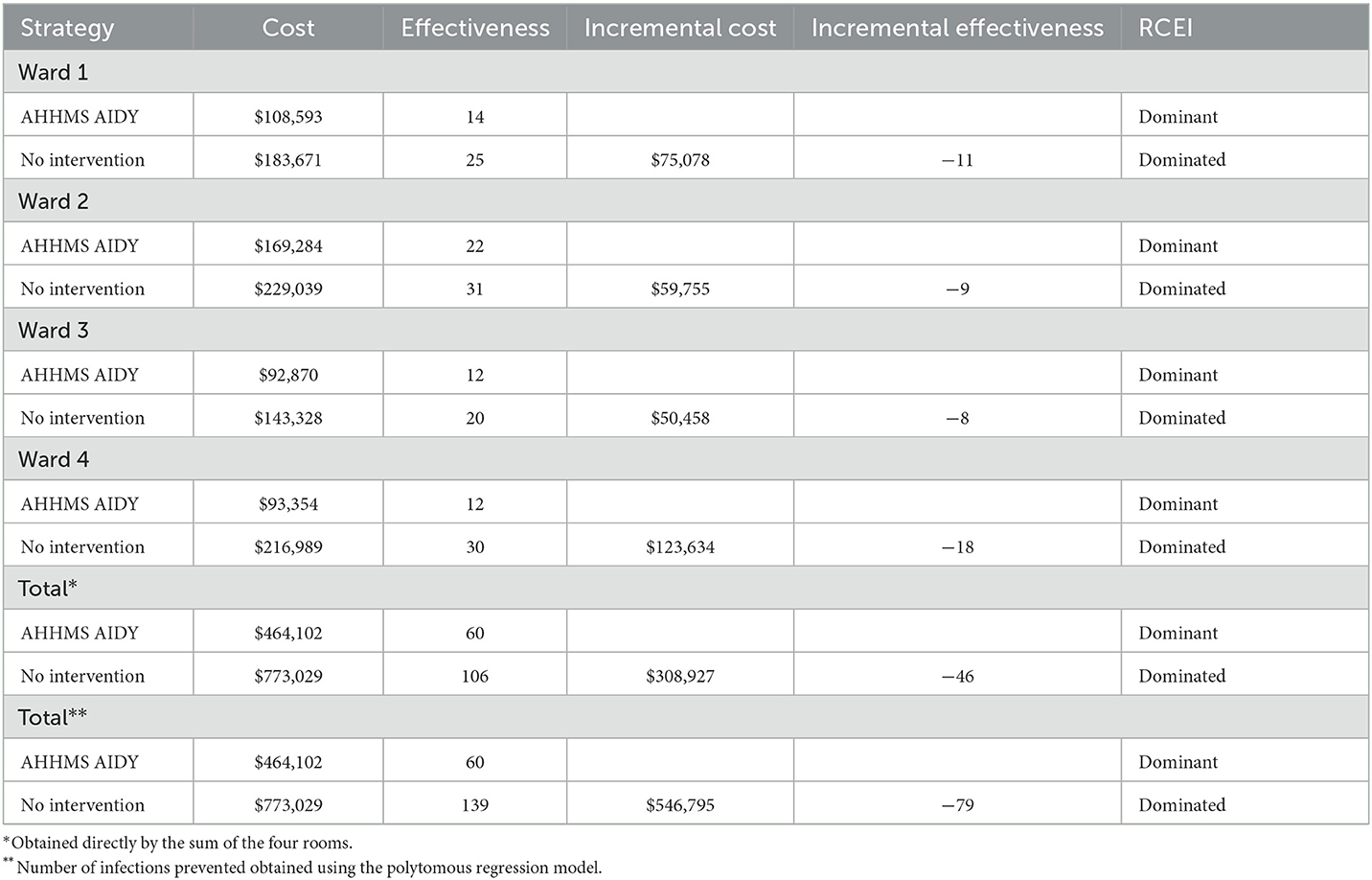
Table 5. Cost effectiveness results.
If the global sum of infections prevented for the four HIMFG wards is used as the total scenario, the program had a cost of US$ 464,102 vs. the non-implementation of US$773,029. The implementation reduced 46 infections (43.4%) (60 vs. 106), resulting in the hospital's net saving of US$308,927. If the estimate of the infection rate is obtained through global polytomous regression, the program had a cost of US$464,102, while a non-implementation cost of US$1,010,898. The program reduced 79 infections (56.7%) (60 vs. 139), resulting in net savings for the hospital of US$546,795, so both results allow considering the program's implementation as a cost-saving alternative.
Sensitivity analysis results
Two scenarios were established to assess robustness of the main parameters of the base model.
Scenario 1
The minimum cost per infection for the different wards was $331 (ward 4), $585 (ward 1), $705 (ward 3) and $948 (ward 2), with an average minimum cost per infection for the hospital of $582, taking into account a total of 46 prevented infections and the global implementation cost of the AHHM alternative.
Scenario 2
The minimum number of prevented infections required to offset the cost of the AHHMS vis-à-vis non-implementation of the system in the different wards was: 0.82 (ward 2), 1.11 (ward 1), 1.24 (ward 4) and 1.35 (ward 3), the overall minimum of prevented infections for the HIMFG for the period being 3.68.
Discussion
Our results showed that the AHHMS was a cost-effective and cost-savings alternative in reducing infection rates per 1,000 PD, and in reducing HAIs, representing substantial savings for the HIMFG. This is the first study showing the cost-effectiveness of an AHHMS in comparison with manual monitoring which we conducted by shadowing techniques, since the results reported by Guest et al. were based on effectiveness data of other studies (12). Although implementation of an AHHMS may entail a significant investment for healthcare providers as reported in other studies (17); our results show that the return obtained as a consequence of the reduction in infections is greater and may even result in savings.
Daily costs of AHHM per bed, reported by us for the HIMFG closely resemble those reported internationally ($450–$650 per annum) (18), thus we conclude that there is no bias in our results. However, healthcare facilities may strive to obtain a reduction in cost from the supplier to obtain better outcomes, provided the quality of both the service and equipment monitoring is not sacrificed.
Our results on the effectiveness of an AHHMS in reducing infections differ from those reported in previous works on the subject (19), since the latter all mention that various additional measures need to be implemented together with the system. However, as the HIMFG does have a well-established HH program, our results serve to provide evidence of the potential benefits to be obtained from implementing an AHHMS in enhancing permanent and interactive compliance, while providing proof of its impact on infection reduction. As reported by McCalla et al., we did observe a positive impact (decline) in the number of infections (13).
Our study was subject to certain time limitations, as we were unable to monitor the intervention due to the COVID-19 pandemic, which modified healthcare protocols and forced us to halt monitoring as potential biases would have affected new infection rates estimates for the different hospital wards. Although there is evidence that the COVID-19 outbreak modified HH adherence (20), there is no clear evidence that it had an effect on the number of infections, though the likelihood of such impact is to be expected.
Another limitation was the lack of cost estimates of pediatric infections for the HIMFG in particular. Such estimates would have been an ideal complement for our study. Nevertheless, the costs taken into account for our model were conservative if compared to other costs reported for the adult population in Mexico (21) or internationally (22).
With respect to the sensitivity analysis conducted, the parameters employed in estimating costs and effectiveness were consistent, given that the values used were conservative and allowed for the assumption of extreme values of much lower effectiveness, or significantly smaller infections costs, and the results in both instances would have nevertheless provided favorable outcomes in the implementation of the AHHMS at the HIMFG.
We expect to analyze infection rates when the COVID-19 pandemic in over at the HIMFG, once healthcare protocols are again fully in place, to assess long-term outcomes when AHHM is implemented in other areas of the hospital.
Conclusion
The AHHMS proved to be a cost-saving alternative for the HIMFG given its greater effectiveness and lower costs when compared to the present one. Accordingly, the recommendation was made to extend the AHHMS to the remaining hospital wards with similar internet access and comparable infection rates.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by Research and Ethics Committee of the HIMFG for the study was obtained and recorded under Registration Numbers HIM/2015/048 and HIM/2017/134. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Author contributions
Conceptualization and formal analysis: GS-E and DR-Z. Data curation and supervision: GS-E, DR-Z, AG-A, and FO-R. Investigation: GS-E, MC-V, and MV-G. Methodology: GS-E, DR-Z, AG-A, FO-R, JG-E, and VG-G. Writing—original draft: GS-E, DR-Z, MC-V, AG-A, and FO-R. Writing—review and editing: GS-E, DR-Z, MC-V, AG-A, FT-T, FO-R, VG-G, MV-G, and JG-E. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1117680/full#supplementary-material
References
1. Larson E. A causal link between handwashing and risk of infection? Examination of the evidence. Infect Cont. (1988) 9:28–36. doi: 10.2307/30144131
2. Boyce JM, Pittet D;, Healthcare Infection Control Practices Advisory Committee; HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Guideline for hand hygiene in health-care settings. recommendations of the healthcare infection control practices advisory committee and the HICPAC/SHEA/APIC/IDSA hand hygiene task force. Society for healthcare epidemiology of America/association for professionals in infection control/infectious diseases society of America. MMWR Recomm Rep. (2002) 51:1–45; quiz CE1-4.
3. De la Rosa-Zamboni D, Ochoa SA, Laris-González A, Cruz-Córdova A, Escalona-Venegas G, Pérez-Avendaño G, et al. Everybody hands-on to avoid ESKAPE: Effect of sustained hand hygiene compliance on healthcare-associated infections and multidrug resistance in a paediatric hospital. J Med Microbiol. (2018) 67:1761–71. doi: 10.1099/jmm.0.000863
4. Best M. Ignaz Semmelweis and the birth of infection control. Qual Safe Health Care. (2004) 13:233–4. doi: 10.1136/qshc.2004.010918
5. World Health Organization WHO Patient Safety. (2009). A Guide to the Implementation of the WHO Multimodal Hand Hygiene Improvement Strategy. Available online at: https://apps.who.int/iris/handle/10665/70030 (accessed November 17, 2022).
6. Lambe KA, Lydon S, Madden C, Vellinga A, Hehir A, Walsh M, et al. Hand hygiene compliance in the ICU: a systematic review. Crit Care Med. (2019) 47:1251–7. doi: 10.1097/CCM.0000000000003868
7. Chen YC, Sheng WH, Wang JT, et al. Effectiveness and limitations of hand hygiene promotion on decreasing healthcare–associated infections. PLoS ONE. (2011) 6:e27163. doi: 10.1371/journal.pone.0027163
8. Thi Anh Thu L, Thi Hong Thoa V, Thi Van Trang D, Phuc Tien N, Thuy Van D, Thi Kim Anh L, et al. Cost-effectiveness of a hand hygiene program on health care-associated infections in intensive care patients at a tertiary care hospital in Vietnam. Am J Infect Cont. (2015) 43:e93–9. doi: 10.1016/j.ajic.2015.08.006
9. Graves N, Page K, Martin E, Brain D, Hall L, Campbell M, et al. Cost-effectiveness of a national initiative to improve hand hygiene compliance using the outcome of healthcare associated staphylococcus aureus bacteraemia. PLoS ONE. (2016) 11:e0148190. doi: 10.1371/journal.pone.0148190
10. Azor-Martinez E, Garcia-Mochon L, Lopez-Lacort M, et al. Child care center hand hygiene programs' cost-effectiveness in preventing respiratory infections. Pediatrics. (2021) 148:e2021052496. doi: 10.1542/peds.2021-052496
11. Wang C, Jiang W, Yang K, Yu D, Newn J, Sarsenbayeva Z, et al. Electronic monitoring systems for hand hygiene: systematic review of technology. J Med Int Res. (2021) 23:e27880. doi: 10.2196/27880
12. Guest JF, Keating T, Gould D, Wigglesworth N. Modelling the costs and consequences of reducing healthcare-associated infections by improving hand hygiene in an average hospital in England. BMJ Open. (2019) 9:e029971. doi: 10.1136/bmjopen-2019-029971
13. McCalla S, Reilly M, Thomas R, McSpedon-Rai D, McMahon LA, Palumbo M. An automated hand hygiene compliance system is associated with decreased rates of health care-associated infections. Am J Infect Cont. (2018) 46:1381–6. doi: 10.1016/j.ajic.2018.05.017
14. Valdez RJA, Hernández OHG, González SN, Cravioto QP. Costo de la neumonía asociada a ventilador en la unidad de terapia intensiva pediátrica. Rev Latin Infect Pediatr. (2017) 30:62–7.
15. INEGI. Calculadora de inflación. Available online at: https://www.inegi.org.mx/app/indicesdeprecios/calculadorainflacion.aspx (accessed, November 23, 2022).
16. Banxico. SIE - Mercado cambiario. (2022). Available at: https://www.banxico.org.mx/tipcamb/main.do?page=tipandidioma=sp (Accessed: 23 November 2022).
17. Durant DJ, Willis L, Duvall S. Adoption of electronic hand hygiene monitoring systems in New York state hospitals and the associated impact on hospital-acquired C. difficile infection rates. Am J Infect Cont. (2020) 48:733–9. doi: 10.1016/j.ajic.2020.04.005
18. Cawthorne KR, Cooke RPD. Are electronic hand hygiene monitoring systems cost-effective? Stepped wedge cluster randomized controlled trials are needed to assess their impact on reducing healthcare-associated infections. J Clean Prod. (2020) 106:200–1. doi: 10.1016/j.jhin.2020.05.033
19. Boyce JM, Laughman JA, Ader MH, Wagner PT, Parker AE, Arbogast J. Impact of an automated hand hygiene monitoring system and additional promotional activities on hand hygiene performance rates and healthcare-associated infections. Infect Cont Hosp Epidemiol. (2019) 40:741–7. doi: 10.1017/ice.2019.77
20. Wang Y, Yang J, Qiao F, Feng B, Hu F, Xi ZA, et al. Compared hand hygiene compliance among healthcare providers before and after the COVID-19 pandemic: a rapid review and meta-analysis. Am J Infect Cont. (2022) 50:563. doi: 10.1016/j.ajic.2021.11.030
21. Sosa-Hernández O, Matías-Téllez B, Estrada-Hernández A, Cureño-Díaz MA, Bello-López JM. Incidence and costs of ventilator-associated pneumonia in the adult intensive care unit of a tertiary referral hospital in Mexico. Am J Infect Cont. (2019) 47:e21–5. doi: 10.1016/j.ajic.2019.02.031
Keywords: hand hygiene, infection control and prevention, cost-effectiveness, infection rate per 1,000 patient days, automated hand hygiene monitoring system (AHHMS)
Citation: Salinas-Escudero G, Rosa-Zamboni DDl, Carrillo-Vega MF, Gamiño-Arroyo AE, Toledano-Toledano F, Ortega-Riosvelasco F, Granados-García V, Villa-Guillén M and Garduño-Espinosa J (2023) Cost-effectiveness analysis of a hand hygiene monitoring system in a tertiary pediatric hospital in Mexico. Front. Public Health 11:1117680. doi: 10.3389/fpubh.2023.1117680
Received: 06 December 2022; Accepted: 17 February 2023;
Published: 09 March 2023.
Edited by:
Constantinos Tsioutis, European University Cyprus, CyprusReviewed by:
Houssein Gbaguidi-Haore, Centre Hospitalier Universitaire de Besançon, FranceMiriam Kessi, Xiangya Hospital, Central South University, China
Copyright © 2023 Salinas-Escudero, Rosa-Zamboni, Carrillo-Vega, Gamiño-Arroyo, Toledano-Toledano, Ortega-Riosvelasco, Granados-García, Villa-Guillén and Garduño-Espinosa. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Daniela De la Rosa-Zamboni, cnpkYW5pZWxhQGhvdG1haWwuY29t