 Ángela León Cáceres1,2*‡§
Ángela León Cáceres1,2*‡§ Rohan Michael Ramesh3†‡§
Rohan Michael Ramesh3†‡§ Puisaumaliu Newmai4
Puisaumaliu Newmai4 Rhondemo Kikon4
Rhondemo Kikon4 Andreas Deckert1*
Andreas Deckert1*- 1Heidelberg Institute of Global Health, University of Heidelberg, Heidelberg, Germany
- 2Tropical Herping, Quito, Ecuador
- 3Christian Institute of Health Sciences and Research, Dimapur, India
- 4Community Health Initiative, Dimapur, India
Background: Evidence suggests that healthcare utilization among tribal communities in isolated regions can be influenced by social determinants of health, particularly cultural and geographical factors. The true mortality and morbidity due to these factors in remote tribal communities are often underestimated due to facility-dependent reporting systems often difficult to access. We studied the utilization of health services for maternal and newborn care and explored how cultural beliefs, perceptions, and practices influence the health-seeking behavior (HSB) of an indigenous tribal community in Northeast India.
Methods: Within a concurrent triangulation design, the combined results from 7 focus group discussions and 19 in-depth interviews, and the 109 interviews of mothers from a community-based survey were interpreted in a complementary manner. The qualitative data were analyzed using a conceptual framework adapted from the socio-ecological and three-delays model, using a priori thematic coding. Multivariable logistic regression was carried out to identify factors associated with home delivery.
Results: Only 3.7% of the interviewed mothers received the four recommended antenatal check-ups in health centers, and 40.1% delivered at home. Mothers residing in the villages without a health center or one that was not operational were more likely to deliver at home. HSB was influenced significantly by available finances, the mother’s education, low self-esteem, and a strong belief in traditional medicine favored by its availability and religious affiliation. The community sought health services in facilities only in emergency situations, determined primarily by the tribe’s poor perception of the quality of health services provided in the irregularly open centers, locally available traditional medicine practitioners, and challenges in geographical access. National schemes intended to incentivize access to facilities failed to impact this community due to flawed program implementation that did not consider this region’s cultural, social, and geographical differences.
Conclusion: The health-seeking behavior of the tribe is a complex, interrelated, and interdependent process framed in a medical pluralistic context. The utilization of health centers and HSBs of indigenous communities may improve when policymakers adopt a “bottom-up approach,” addressing structural barriers, tailoring programs to be culturally appropriate, and guaranteeing that the perceived needs of indigenous communities are met before national objectives.
Introduction
The global health agenda has emphasized decreasing maternal and newborn mortality as key components of sustainable human development. Despite the progress, 830 women die every day from causes related to pregnancy or childbirth; of this, 20 percent are from India (1, 2). This country still has significant challenges, even if the maternal mortality ratio was reduced from 212 deaths per 100,000 live births in 2007 to 167 deaths in 2013 (3). However, in 2013, the highest number of neonatal deaths globally (0.75 million) was reported in India (4). Further, within the country, the neonatal mortality rate (NMR) nearly doubles in some rural and tribal areas compared to the urban areas since they face considerable inequalities in access to antenatal, intranatal, and postnatal healthcare services (4). Other reasons that contribute to this disparity in India are low public expenditure on health (1.02% of India’s Gross Domestic Product for 2015–2016), high dependency on private healthcare services (78%-outpatients and 60%-inpatients), and high out-of-pocket (OOP) expenditures especially in Nagaland (61.7%) compared to the rest of India (20.5%) (5–7). To address the aforementioned issues, the Indian Government launched the “Janani Shishu Suraksha Karyakaram” (JSSK) scheme in 2011 for pregnant women and newborns to decrease OOP and neonatal deaths by providing free transport, medicines, and consumables, diagnostic tests, blood transfusions, and food for the duration of a woman’s stay. Sick neonates are also entitled to free treatment and transport (5). Additionally, another program, the “Janani Suraksha Yojana” (JSY) program offers cash assistance to mothers and accredited social health activists (ASHA-local community health volunteers who promote access to health services, mobilize communities, and provide community care) to facilitate institutional deliveries (8).
The Northeast region of India accommodates the country’s largest proportion of scheduled tribes (ST) and ranks the lowest in social indicators (9). One such state in this region is Nagaland, where 61% of the people are multidimensionally poor and live in rural and remote zones that lack connectivity due to inadequate or non-existent public transport systems, which markedly influences timely, affordable, and accessible maternal and child public healthcare services (10). In 2016, the more developed states like Kerala and Tamil Nadu reported almost 100% institutional deliveries, but Nagaland reported only a third of its births in health facilities (11). Nearly 90% of the population living in Nagaland are tribal or indigenous. “Nagas” is a collective term for several indigenous communities in the Northeast Region of India and upper Myanmar that share similar social and cultural characteristics. In India, the majority of the Nagas live in the state of Nagaland, within 16 administrative districts inhabited by 17 major and sub-tribes. In India, Nagas are classified as a scheduled tribe (Indigenous people from India who are officially regarded as socially disadvantaged) under the Indian constitution article 342 (12).
While there is anecdotal evidence suggesting that political unrest, the rugged terrain, and the lack of transport greatly influence access to healthcare services, a paucity of data demonstrates that social and cultural factors also influence health-seeking behavior (HSB) exhibited by this community. This study employed a mixed methods approach to quantitatively study the utilization of maternal and newborn health services while adopting a salutogenic perspective to explore how cultural beliefs, perceptions, and practices influence the HSB of an indigenous tribal community in Northeast India.
Materials and methods
Study setting
The study was conducted in Tening, a block in Peren district, located in the hilly north-eastern state of Nagaland, India. The community’s total population is around 95,000, and the Tening block consists of 23 registered villages, currently home to the Christianized Liangmai Naga tribe (also called “Zeliang”, one of the 17 major tribes in Nagaland) (13). Due to civil conflicts, this territory became a no-go area in 1947, was a restricted area for more than 50 years, and is presently considered a disturbed area, the consequences of which still disrupt everyday life (14). Their lifestyles and social structures are based on a lineage and patriarchal clan system. The Northeastern region of India presents a complicated geographical picture that isolates this region from the rest of the country. The Tening block is landlocked by the neighboring states of Manipur in the southeast and Assam in the southwest. Dimapur is the closest city with tertiary healthcare facilities located ~120 km from the block in the adjacent district; however, it takes nearly 6–8 h to reach there due to the poor condition of the roads, especially during the rainy season (Figure 1). Accessibility is further complicated due to the high costs expected by local private transport agencies in the absence of a functional public transport system. Around 80% of the population is engaged primarily in agricultural activities (15). In 2016, the district reported that 41% of the mothers delivered in health centers, and only 13% of pregnant women received the recommended ≥4 antenatal care (ANC) checkups in a facility (16). In 2018, the government reported four stillbirths, nine infant deaths, and zero maternal deaths during the same period (17). Of the four primary health centers (PHC) and one Health sub-centre (HSC) located in the Tening block, only one PHC is fully functional as a delivery point. The structure of the Indian public health system has been described in detail elsewhere (18). Obstetric and neonatal emergencies are referred to the District hospital located in the adjacent block, but due to the lack of facilities to manage complications, they are further referred to tertiary centers located in Dimapur city (Figure 1).
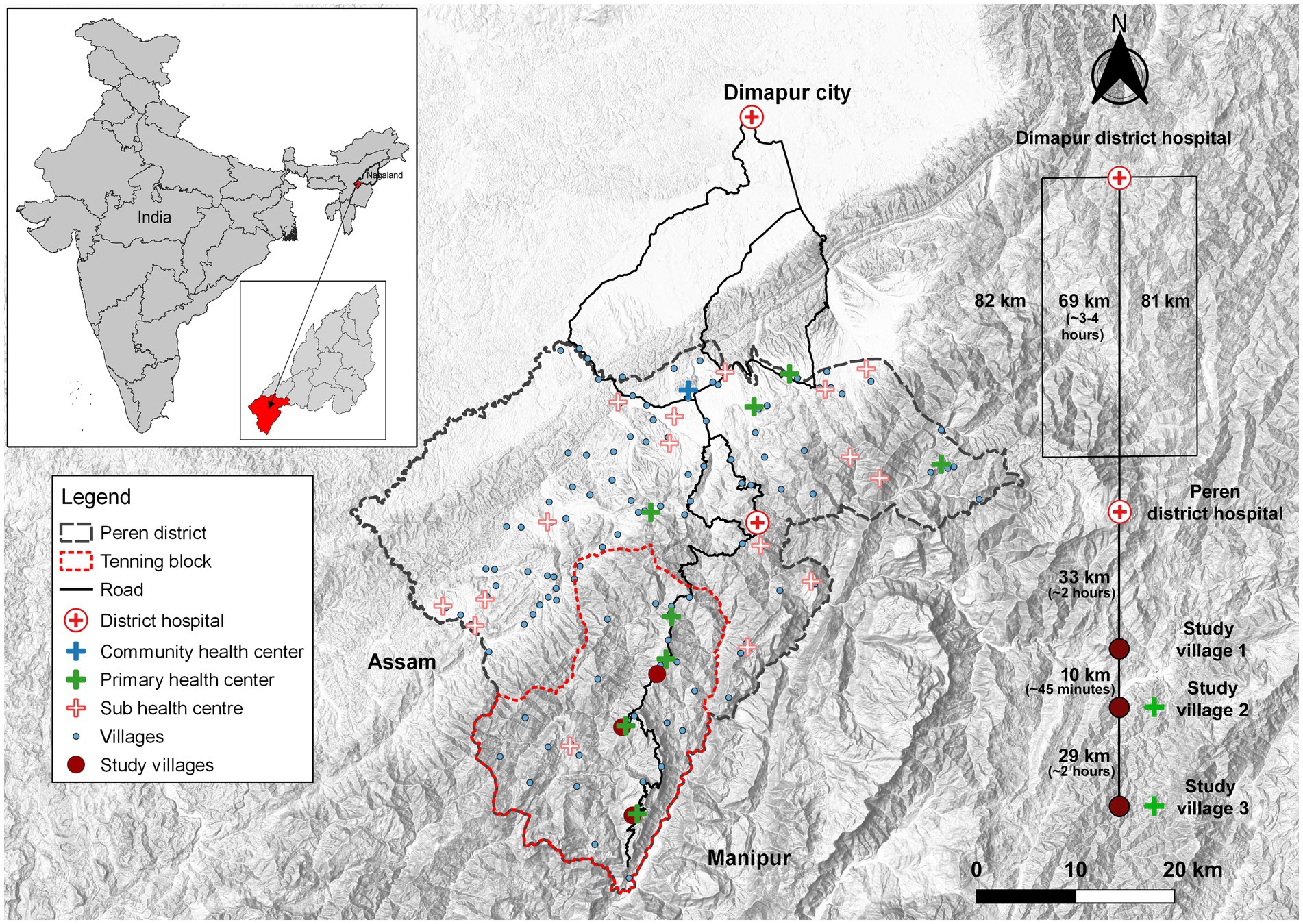
Figure 1. A topographic map of the study area with details of access to health facilities.
Study design
A mixed-methods approach with a concurrent triangulation design was used to capture qualitative and quantitative maternal and newborn health information from the participants residing in the study villages. Three villages from the block were selected after a pilot visit based on the presence and functionality of a PHC in the village. Village 1 did not have a health facility inside the village and the closest functional delivery point is the PHC is located in Village 2. Village 2, has a fully operational PHC in the village and also caters to the entire block. Village 3 was the furthermost village; although there was a physical structure the PHC was not-operational (Figure 1).
Conceptual framework
We explored the HSB of the tribe from a holistic and community-centered perspective based on a theoretical framework that assumes that perceptions are subjective and thus guided by social actions, which can be constructed or deconstructed individually and socially, with an emphasis on the effect of social interactions, relations, and language conventions. This study considered pregnancy and childbirth as social and cultural events guided by different nested norms in a pluralistic medical system. The socio-ecological model (SEM) explored cultural beliefs and practices influencing the decision-making process and perceptions of the provided services. The SEM offers a multi-level approach to understanding the interaction and interdependence of the individual, interpersonal, organizational, community, and public policy levels (19). Furthermore, it includes the individual’s perceptions, cultural beliefs, and knowledge about the issue under investigation. At the organizational level, the model seeks to interpret the reciprocal causation between people’s considerations about the access and utilization of these services in the given environmental circumstances to explore possible barriers that are perceived to influence community and individual behaviors (19). To describe the barriers that might affect access and utilization of maternal and newborn healthcare services and the process of seeking them, we constructed a conceptual framework based on the three delays model (20). We adapted the model, which originally addressed the factors that affect obstetric complications and explored the delays in access to ANC, perinatal care services, postnatal care (PNC), and neonatal care while considering relevant factors that influence maternal and newborn mortality and morbidity. The first and second delays: (1) delay in the decision to seek care, and (2) delay in arrival to the facility, were especially emphasized (20). For the perceptions of the tribe regarding the government’s services, the third delay offered a suitable framework: (3) delay in the provision of adequate care (20).
Data collection
Qualitative data was collected through focus group discussions (FGDs) and in-depth interviews (IDIs) conducted between March 23 – April 19, 2019. To triangulate sources and consider the cultural context in which the study was developed, we selected participants all above 18 years of age from five different groups of the Liangmai tribe: (1) women of childbearing age, (2) male relatives/partners of women of childbearing age, (3) traditional birth attendants (TBA), (4) or ASHAs/ community health workers (CHWs) who are currently residing in each village, and (5) health managers or health professionals at the government health facilities. The cross-lingual IDIs and FGDs were conducted in groups of 5–6 participants and were facilitated by a bilingual moderator.
The quantitative part comprised information from an extensive district-level community-based cross-sectional survey studying the influence of geographical variation on maternal and child health events conducted between November 2018 and December 2019 from 70 villages in the Peren district. In brief, all mothers who delivered in the last 2 years, regardless of the outcome and residing in the study villages, were approached to participate in the in-person interviews. After obtaining the informed consent, the trained field interviewers administered a questionnaire to collect the antenatal, intranatal, and postnatal details from the mother. Details of the child were also collected while corroborating the information provided using the “mother and child tracking card” provided by the government to all mothers, when available. Waypoints of the mother’s house and routes to the nearest health facility were mapped. For this study, the data from the 3 study villages using a subset of relevant questions were extracted to analyze and corroborate with the findings from the qualitative component. The aim of the quantitative part was to describe the scenario rather than testing a certain scientific hypothesis; hence, we waived a sample size calculation and instead used data from the full study population (all mothers who delivered in the last 2 years) to get more precise estimates. Data from the community-based survey: Thirteen pertinent questions from the cross-sectional survey (demographic details, obstetric history, antenatal care, pregnancy outcome, healthcare workers visits, details of the delivery, and transportation) were selected to corroborate with the qualitative demographic questionnaire, the FGD, and the IDI guides.
Data collection tools
The qualitative data collection tools included semi-structured cross-lingual FGDs and IDIs, adapted to the different target groups and supported by participant observation. In the FGDs, free listing and pile sorting techniques were applied to identify which health conditions people were seeking healthcare services for and to prioritize the intensity or severity of their thoughts. This was used to systematically identify robust group schemes and shared knowledge, beliefs, and perceptions. IDIs explored the individuals’ perceptions, experiences, knowledge, beliefs, practices, and behaviors. The questions were also meant to guide the participants to reflect and perceive themselves as community members and to understand the individual and their families within the structure of the macro system. In this cultural setting, we arranged the groups by sex and similar ages to understand their perspectives, obtain information about the social norms, group behaviors, hierarchies, power relations, degree of consensus, and demonstrate group emotional processes.
Additionally, we wanted to understand the group’s influence on an individual and how or in what ways it influences individuals. To facilitate communication with the community, a trained research assistant operated as a bilingual moderator and interviewer in the FGDs/IDIs, and also as an interpreter and translator in the informal conversations with key informants. The principal researcher trained the research assistant before the study on qualitative methods, tools, ethical considerations for research, social determinants of health, and basic concepts of maternal and newborn health. A problem tree analysis was performed to contextualize the problem and study hypothesis. A document with key terms was formulated during the training to guide the interviewer in obtaining answers from the participants.
Semi-structured interview guides were developed for the interviews to avoid potential personal bias. The principal researcher was a passive observer, taking notes of the body language of the participants and occasionally assisting the interviewer. IDIs were used to explore the perceptions, experiences, knowledge, beliefs, practices, and behaviors of the participants. The IDI guides were selected as an appropriate tool to ensure consistency during the interviews and facilitate the analysis process, tailored for each sub-group. FGD as a qualitative tool was chosen understand the perceptions of the group in its social setting and collecting several perspectives on the topic. FGDs helped to obtain information about the social norms, group behaviors, hierarchies, power relations, degree of consensus, and demonstration of group emotional processes. The FGD and IDI guides, the information-sheet, and informed consent forms (for the FGD, IDI, demographic questionnaire, and photograph use) were developed in English and were translated into Nagamese and Liangmai. The FGDs and IDIs were primarily conducted in the local language (Liangmai and Nagamese). No FGD participants were interviewed in the IDIs.
The quantitative data from the survey were collected by a trained interviewer using a mobile-based, semi-structured, translated, pilot-tested questionnaire. The pilot questionnaire was administered in the local language to 12 tribal mothers who had delivered in the last 2 years residing in a non-study village in the adjacent district. When the study commenced, the field interviewer approached a mother and invited her to participate after providing an information sheet printed in the local language. If the mother could not read, the field interviewer was instructed to read it out in the local language. Any queries regarding the study were discussed before obtaining the informed consent sheet if she decided to participate.
Data analysis
Four of the 26 audio-recorded sessions were transcribed verbatim into Liangmai and then translated to English, while the rest were translated directly into English. Additional revisions of the translations were done in collaboration with an external Liangmai native speaker, assuring confidentiality. The study used a combination of both deductive and inductive approaches to coding. The English transcripts were coded a priori according to specific content priority analysis. Two coding approaches were used: concept-driven and data-driven coding; then, the data were analyzed using NVivo 12 Pro [QSR International Pty Ltd., (2018) NVivo (Version 12)]. The codes used were related to the conceptual framework, guiding principles of the study, and social determinants of health. The codes were related to the adapted Three Delays Model in order to describe the barriers that might affect the access and utilization of maternal and newborn healthcare services and the process of seeking them. A special emphasis was put on the first and second delays: (1) delay in the decision to seek care; (2) delay in arrival to the facility. For perceptions of the tribe regarding the government’s services, the third delay; and (3) delay in providing adequate care offered the suitable framework. This was combined with the SEM, because it offered a multiple-level approach to understanding the interaction and interdependence of the individual, interpersonal, organizational, community, and public policy levels.
Emphasis was placed on cultural determinants, barriers to accessing or utilizing healthcare services, motivational determinants, decision-making processes, and linkages between Traditional Medicine (TM) and government healthcare services, human, and interpersonal relationships A qualitative multilevel data analysis approach was applied, complementing it with an analysis of the observation notes and the free-listing and pile sorting techniques conducted in FGDs. We described the characteristics of the FGDs and IDIs participants, using frequencies for age, marital status, education, and occupation, stratified by gender.
Quantitative data: The frequencies for categories of all survey variables were calculated. Additionally, simple descriptive statistics with fisher’s exact test were used to investigate if there were significant differences in each demographic variable between the study villages. The significance level alpha was set at 5%.
To adjust for potential confounders, variables from the univariable analysis were chosen for a multivariable logistic regression model in (i) a full model and (ii) a model with backward selection to study the factors associated with home delivery, using SPSS 21 (IBM Corp. Released 2012. IBM SPSS Statistics for Windows, Version 21.0. Armonk, NY: IBM Corp). The outcome variable was the place of delivery. The backward selection started with all variables included except for marital status (only one unmarried person), the person responsible for the delivery (directly related to the outcome variable), and fully immunized children (immunization was beyond the time point of delivery). The final model consisted of only the villages.
Ethics approval statement
The ethical approval was obtained from the Ethics Committee of the Medical Faculty, the Ruprecht Karls University of Heidelberg, Germany (#S-138/2019, 13.03.2019), and from the Institutional Review Board (Research and Ethics Committee) of the Christian Institute of Health Sciences and Research, Nagaland, India for the qualitative component and the quantitative data from the cross-sectional survey from the “Project on the use of Geographic Information Systems in Health Systems Research in Rural Areas of Nagaland”. Approved data collection tools were translated into Nagamese and Liangmai languages and submitted to the Institutional Review Board of the Christian Institute of Health Sciences and Research. Written informed consent was obtained from all participants.
Results
A total of 57 community members participated in the seven FGDs (four FGDs with women of childbearing age and three FGDs with male relatives/partners) and 19 IDIs (five with women of childbearing age, four with male partners or relatives of women of childbearing age, four with the ASHAs, four with TBAs and traditional healers, and two with health professionals). Responses from interviews with 109 mothers residing in the 3 study villages were included in the cross-sectional survey.
Characteristics of the survey participants
Of the 109 women who participated in the cross-sectional survey, most (73.4%) were 20 to 29 years of age, with a mean age of 27 years, and married. The majority (46.8%) of the mothers had completed up to middle school education, while 21.1% had completed only up to primary education, and 5.5% were graduates or held higher educational degrees. Most (45.9%) mothers were housewives and farmers (41.3%), but this differed between the three villages (p < 0.01) as farming was the preferred vocation in villages 1 and 3 (Supplementary Table S1).
Characteristics of the FGD and IDI participants
The demographic information collected from the female participants in the FGDs and IDIs portrayed a similar picture. Most 80.0% (n = 28) of the women were currently married, 63.6% of them had completed only up to primary education, 6% held a university degree, and the majority of them were housewives (20%) and farmers (34%). Most (76.2%, n = 16) participating males were married, 20.0% had university or higher degrees, and 52.9% worked as farmers (Supplementary Table S2).
Obstetric details
The cross-sectional survey revealed that 56.0% (61/109) of the mothers had experienced 2–4 pregnancies, while 22.0% (24/109) had up to five or more pregnancies. Only 3.7% (4/109) had completed atleast the four recommended ANC check-ups, and 11.9% (13/109) of the mothers did not receive even one ANC check-up. Around 14.7% (13/109) of the mothers received just one, while most (69.7%, 76/109) received at least 2–3 check-ups in a health facility. The proportion of mothers receiving nil or just one ANC check-up was higher in the village with no health center (village 1) compared to the other two. The difference in proportions between the three villages was statistically significant (p < 0.01). Some (11%, 9/109) mothers reported at least one spontaneous abortion, and 14.7% (16/109) reported 1–2 newborn or infant deaths in the near past. The majority (40.4%, 44/109) of mothers delivered at home, while 41.3% (45/109) at the local PHC located inside the block, 13.8% (15/109) at a public health facility located outside the block, and 4.6% (5/109) in private facilities outside the block. Most (50%) mothers residing in the village with a functional delivery point (village 2) preferred to deliver in a facility hence the proportion of home deliveries was the lowest (22.6%) of the three. Though village 1 did not have a health facility located in the village, many mothers (41.3%) chose to deliver at the closest local PHC located in village 2 (Figure 1). However, 73.9% of the mothers residing in the furthermost village with a non-operational health center (village 3) delivered at home, while only 17.4% of the mothers delivered in a facility that was located 2–3 h away because the delivery point the village was mostly nonfunctional (Figure 2). A statistically significant difference was noticed in the place of delivery between the three villages (p < 0.01). The majority of the deliveries were attended to by a nurse (64.2%), and the rest were attended to by relatives (22.9%), ASHAs (10.1%), TBAs (0.9%), and only 1.8% by a doctor. Most (83.9%) women residing in the village with a functional delivery point informed that nurses conducted the deliveries. In comparison, only 41.7% of women from the village with no health center (Village 1) reported the same. The difference in the person responsible for the deliveries between the three villages was statistically significant (p < 0.01; Supplementary Table S1). Most women (61.3%, 19/31) who chose to deliver in the functional health facility inside their village (Village 2) walked to the delivery point. At the same time, the majority (54.5%, 12/22) who decided to deliver in health facilities outside the block hired a local taxi, and one respondent reported using an ambulance. The multivariable logistic regression model using backward selection revealed that mothers residing in Village 1-without a health center [adjusted odds ratio (aOR), 4.1, 95% CI, 1.5–11.0] and especially Village 3-with a non-operational health center (aOR,9.7, 95%CI, 3.2–29.3) were more likely to deliver at home (Supplementary Table S3).
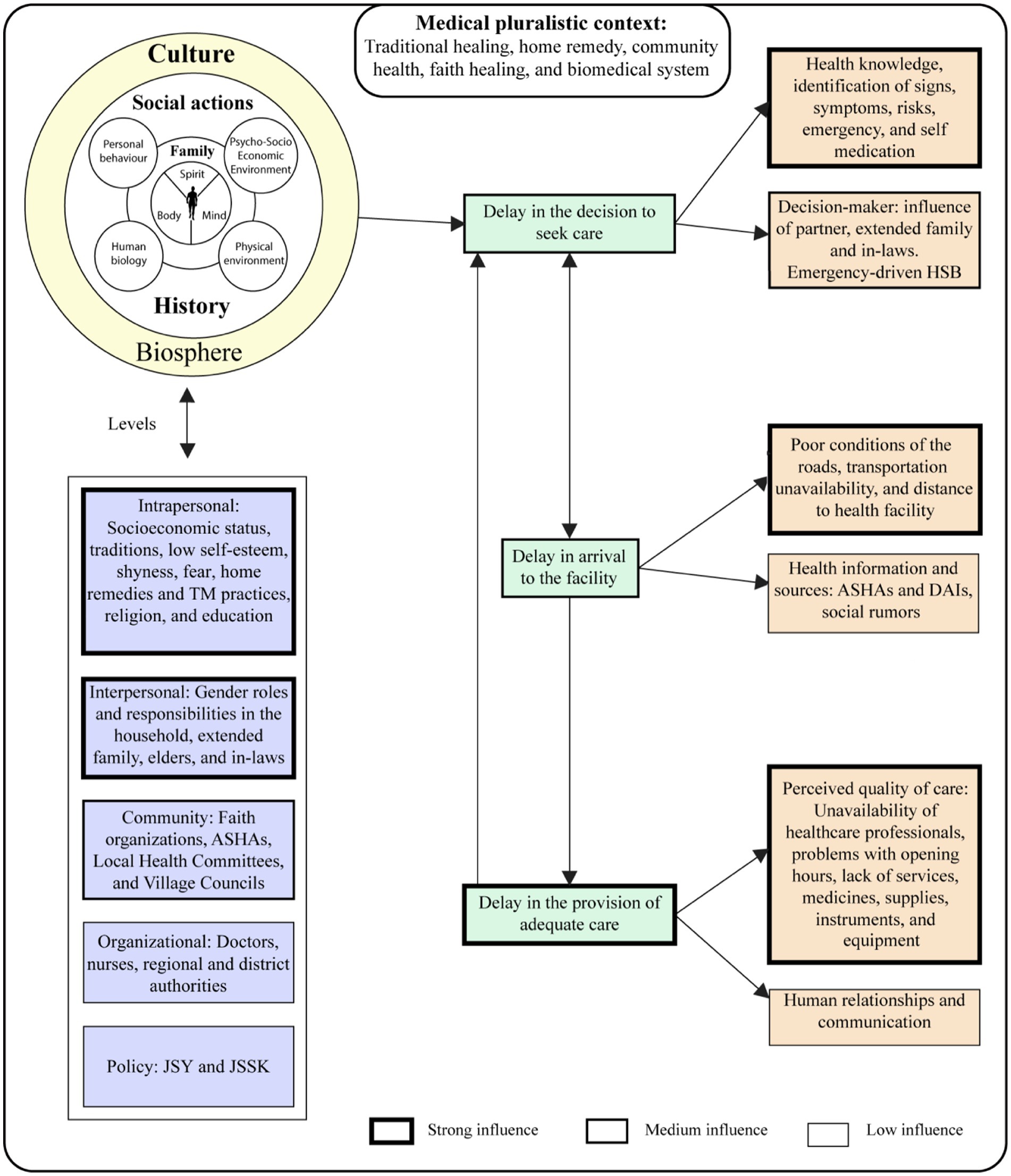
Figure 2. Main determinants and their level of influence regarding the SEM and the adapted-three delays model.
Beliefs, practices, behaviors, and perceptions influencing health-seeking behavior
The SEM was adapted to understand the factors influencing decision-making that affect individual HSBs and their perceptions regarding healthcare facilities. They are subdivided according to the order of influence into three levels.
The intrapersonal and interpersonal level
This level had the most decisive influence on an individual’s perceptions and HSB, as illustrated in Figure 2. The qualitative component identified socio-economic status, education, low self-esteem, shyness, fear, traditions, home remedy/TM practices, and religion immensely influence the individual’s HSB. Most participants stated they could not access healthcare services, including preventive health and medicines, due to the lack of money and their own-self denomination as “poor” (Table 1). The gender disparity in educational levels may also influence decision-making (40% of men with university education compared to 6% of women). The interviewed women showed low confidence and self-esteem; most indicated anxieties, suffering, pain, and fear of pregnancy, especially childbirth (Table 1). These were guided by the idea of dying or watching a partner die during delivery. According to the TBAs, most women in this community expressed ‘shyness’ when deciding on or visiting health facilities. Health professionals also corroborated that most women were shy and reluctant to be treated by a male doctor, compelling them to seek care from female nurses.
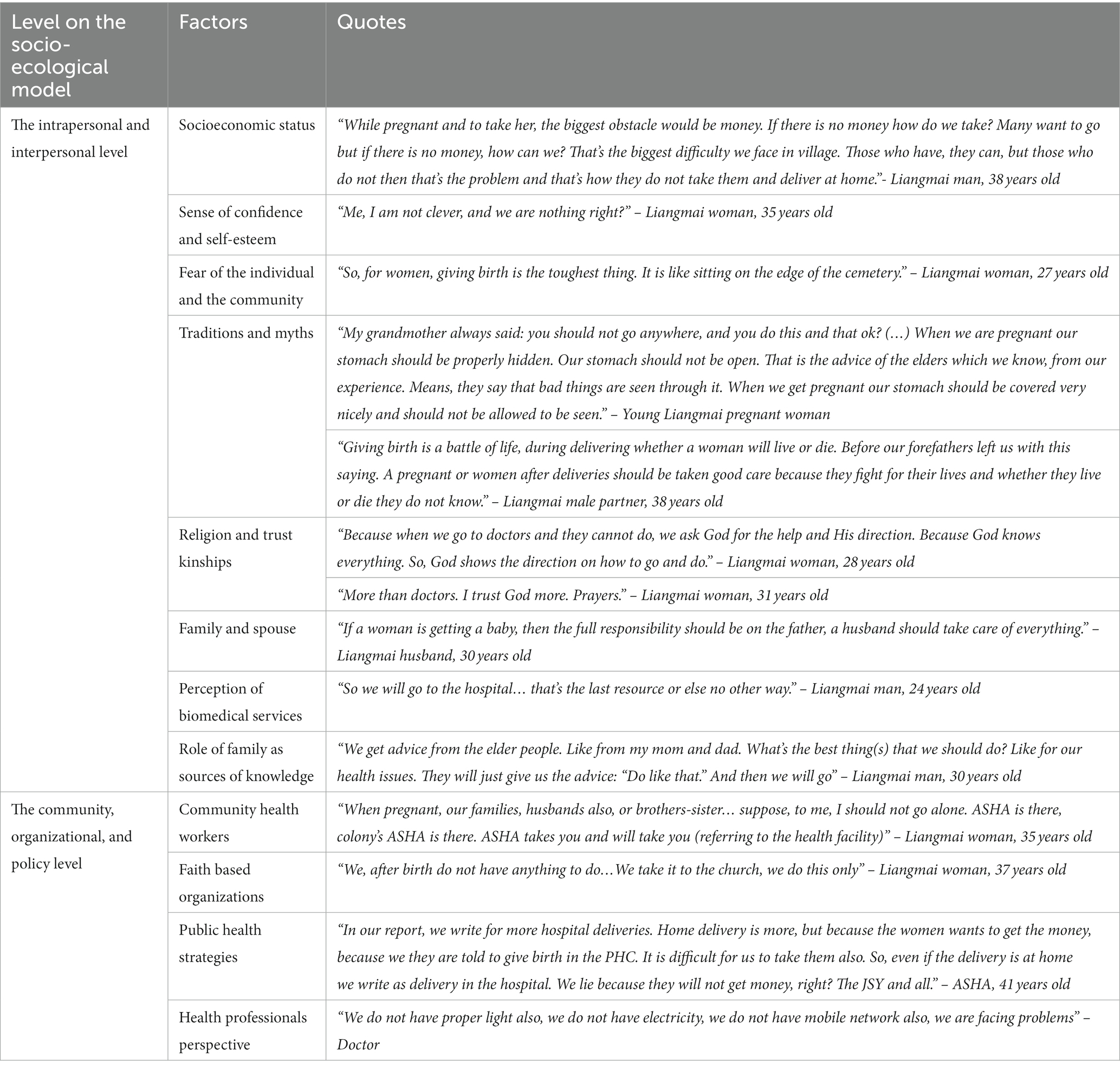
Table 1. Highlights from the focus group discussions and in-depth interviews included in the socio-ecological model.
Traditions, myths, religion, and perceptions about biomedical services and TM influence the tribe’s HSB. Most participants expressed that their forefathers believed pregnancy and childbirth could endanger the mother’s life (Table 1). They also reluctantly spoke about the myths surrounding the practices of a primordial religious minority community. The latter was associated with black magic and witchcraft, which contradicts their strong faith in Christianity for healing, as evident through the discussions (Table 1). All participants responded that praying and their belief in God will resolve their health issues, indicating that most healing practices, either traditional or biomedical, are accompanied by individual or group praying sessions. Some participants believe that praying protects the baby from “abnormalities”. Strong religious beliefs were also observed in the responses from TBAs, ASHAs, and traditional healers as well. The latter believe their healing is a gift from God and is also achieved through the individual’s faith.
Most participants stated they would access a healthcare facility only when “feeling sick” or when there was a complication or emergency, such as when the woman is “unable to deliver at home”. Participants expressed mixed feelings regarding biomedical services and TM; while some felt health centers were unsafe since appropriate care may not be provided, others thought the TM healers were not trained and thus opted out (Table 2). TM, home remedies, services of the ASHA, and self-medication practices were preferred over accessing biomedical services or even faith-based organizations for their health needs, as illustrated in Figure 3.
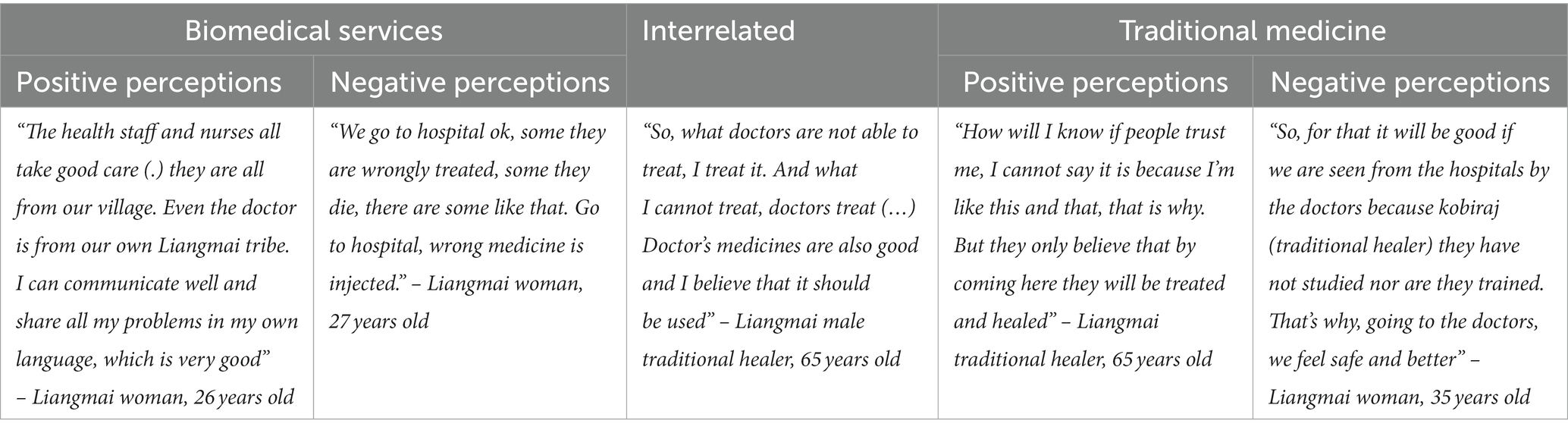
Table 2. Perceptions toward biomedical services and traditional medicine.
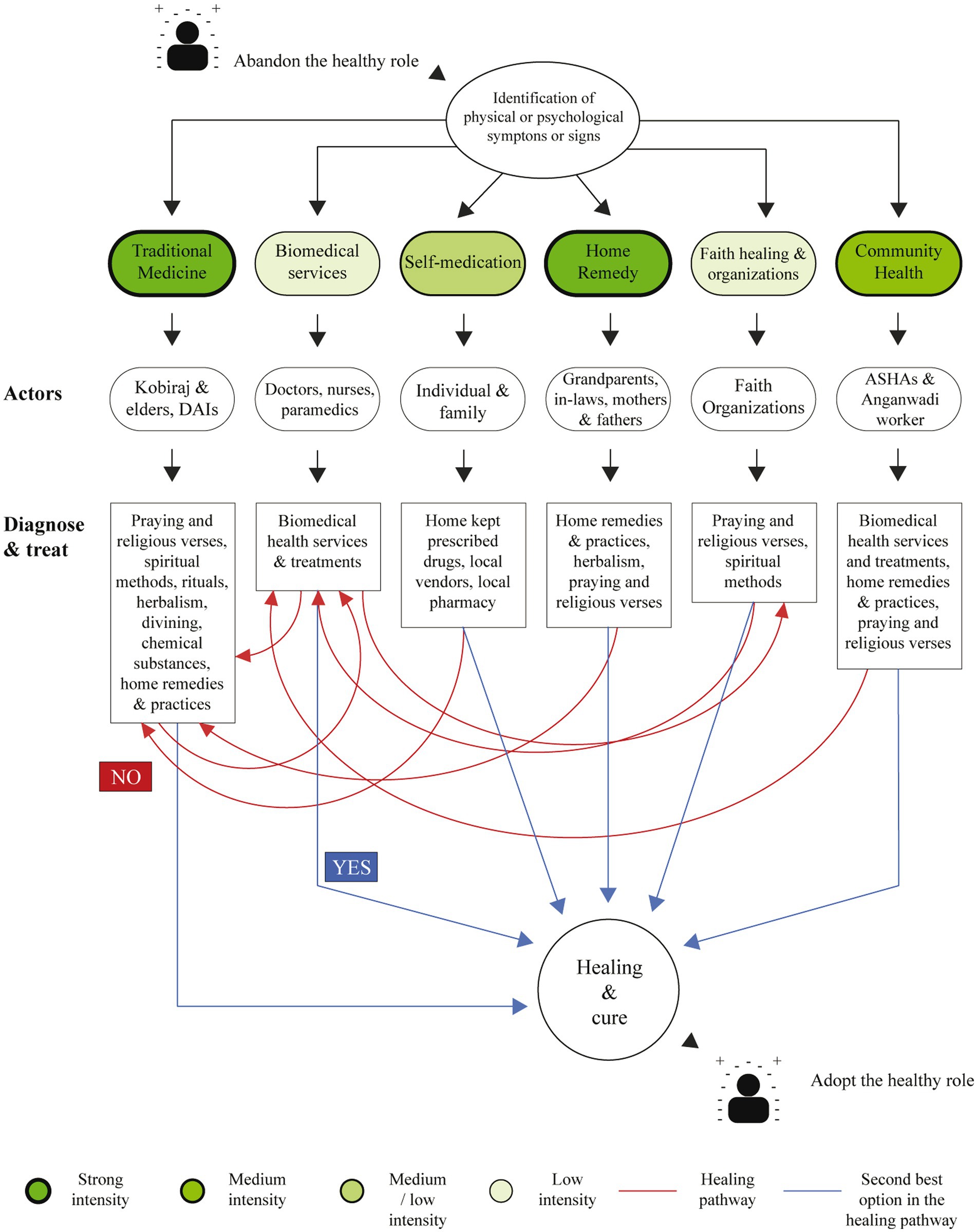
Figure 3. Health-seeking behavior and preferences of the tribe for maternal and newborn health services.
Gender roles and the extended family played an essential role in influencing HSB.
During pregnancy, there is a strong tendency for women to depend on their male partners, assuming that it is the husband’s responsibility to take care of the woman. Most male participants considered themselves responsible for the delivery as the head of the family (Table 1). However, the health professionals stated that it’s uncommon to see the partners accompanying their wives during the ANC visits. Most husbands admitted to participating in the home delivery by assisting with the birth, cutting the umbilical cord, or burying the placenta. Although the husband’s participation is limited in institutional deliveries mainly due to restrictions imposed in the health facility, they were responsible for facilitating the transportation, communication, and financial arrangements. Extended family (mothers, fathers, grandparents, and in-laws of the mother) also participated during childbirth. Home delivery was a common practice among the elders, and there is a strong belief among the participants that since elders are knowledgeable and experienced, their advice should be followed (Table 1). During home delivery, the family members were summoned to primarily attend to the delivery, take care of the newborn, do the household chores, or occasionally for financial support.
The community level
This level moderately influenced the tribe’s HSB, as illustrated in Figure 2. The FGDs identified key community-level actors who influence HSB, such as the ASHAs (CHWs), faith-based organizations (FBO), local health committees, and village councils. The ASHAs were the most influential since most participants referred positively to them. Women considered them as a source of information, advice, emotional and economic support, and primary healthcare providers in their village (Table 1). Some highlighted their importance, as doctors or nurses are usually unavailable in the village. However, most ASHAs and TBAs stated that they were hesitant to help the parturient with home deliveries, especially if the woman is experiencing a “bad delivery” (obstetric complications), since they perceive themselves as insufficiently trained to manage complications confidently. They also expressed difficulties in recognizing neonatal conditions.
The IDIs noted that some interviewees were mildly influenced by faith-based organizations, as they are perceived as sources of salvation and healing (Table 1). A few participants even admitted giving birth in prayer centers near their homes. We observed that prior permission from the local church authorities is a prerequisite for conducting any community activity. Almost everyone referred to church leaders with reverence and obedience. Few interviewees regarded Village Health Committees (VHC) and village councils as sources of information but were perceived hierarchically.
The organizational and policy level
This level was noted to have the most negligible influence on HSB. At the organizational level, health professionals perceived that their services were underutilized because of the lack of awareness, social mobilization, and proper health facilities; however, they reported no official complaints from the community (Table 1). There was a general lack of awareness of health policies at the policy level, and only a few interviewees referred to the JSSK and JSY programs. The majority of ASHAs reported insufficient and inconsistent payments of the monetary incentives, often paying from their own pockets to cover costs incurred while accompanying the patient. Most interviewees reported attempting to go to the health facility even if the distance was considered a challenge. According to one ASHA, even with the monetary benefits of the JSSK scheme, the mother would need to use additional money to cover travel costs since the villages are far away from the delivery points.
An ASHA also confided in having to confabulate data for the community members to benefit from the financial incentives (Table 1). Most of them were reluctant to promote the schemes since it failed to cover basic expenses.
Barriers to accessing and utilizing maternal and newborn health services
According to our adapted-three delays model, the most decisive influence was found on the third delay related to the provision of adequate care, which had a negative effect on the first delay associated with the decision to seek healthcare. Consequently, the second delay regarding the arrival at the health facility appeared to be the one with the lowest influence. The results of this model have been summarized and illustrated in Figure 2.
Delay in the provision of adequate care
The most relevant factor deterring access to health services is the perceived deficient quality of care in health centers. The limited availability of healthcare professionals, low quality of services/medicines, and irregular facility opening hours were key factors influencing this domain. A typical response noted was that staff are often absent in the facilities. Some interviewees mentioned that the health centers are closed on most days and only functional for a few hours when opened. Respondents also wished the centers were open to conducting deliveries at night (Table 3). The majority perceived that the health centers’ facilities were inadequate as there was a dearth of instruments, supplies, medicines, and equipment. The shortage of essential drugs and supplies in the health centers was corroborated by a doctor, too (Table 3). However, most participants and doctors agreed that vaccines were always available for newborns and mothers.
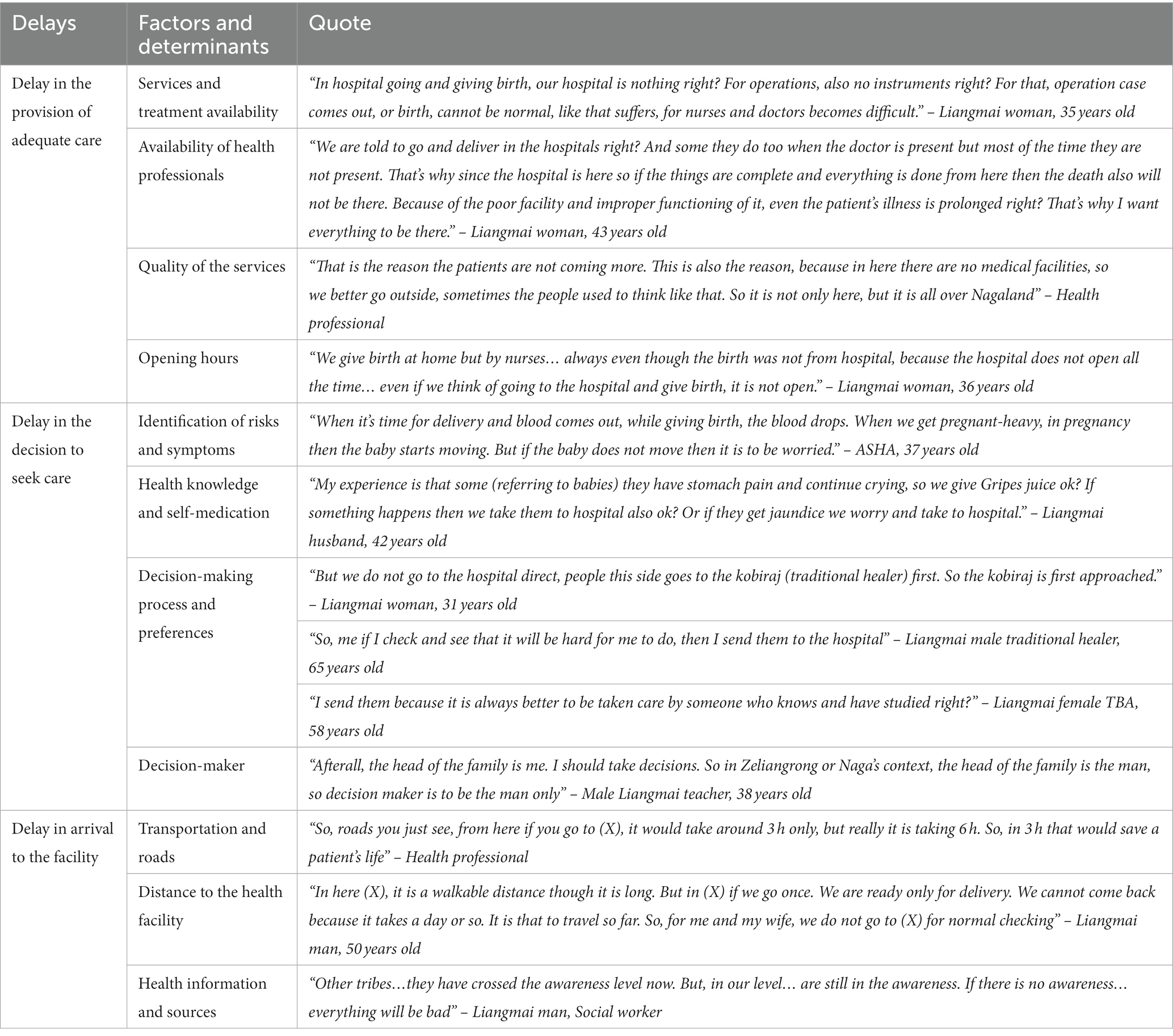
Table 3. Highlights from the focus group discussions and in-depth interviews included in the adapted three-delays model.
Delay in the decision to seek care
In this domain, we identified the key factors that influence the decision of a mother to seek healthcare facilities. Most participants preferred home delivery if it was considered an “easy delivery” since it is deemed a familiar and comfortable environment to deliver in (Table 4). Conversely, they perceived complicated obstetric emergencies necessitated an institutional delivery as it is best managed in a health center and may be unsafe at home (Table 4). Specific uncommon or alarming symptoms like retained placenta, non-progress in labor, vaginal bleeding, mal presentations, large abdomen, and swelling triggered the individual or the family to visit healthcare facilities. Newborns were only taken to a health center in case of incessant crying, seizures, jaundice, and any suspected gastrointestinal or respiratory tract infection. A few women and men opted for ANC services offered in health centers, while only some respondents elucidated to seeking postpartum services in health facilities, as homecare was predominantly favored. They perceive visiting a health facility related to sickness, complications, and emergencies and prefer seeking TM first (Table 4). Few women informed that they adopt a vertical position during labor and deliver the baby by kneeling, contrary to what is done in health facilities (Table 4).
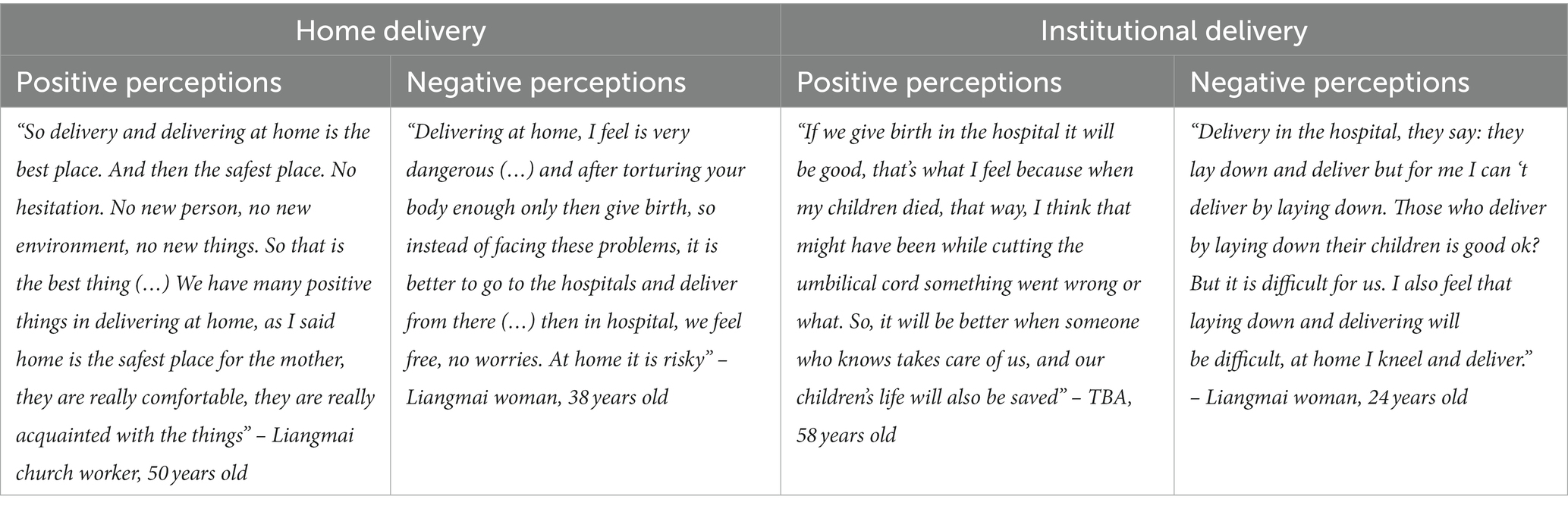
Table 4. Perceptions toward home delivery and institutional delivery.
For most women, TM was the preferred option for primary healthcare due to their availability and since their beliefs and relationships; are assumed to be spiritual or religious. ASHAs, TBAs, and traditional healers informed that they also refer patients to the health centers if they cannot manage an obstetric complication (Table 3). Notably, the TM actors positively perceived the skills of health professionals and considered them “experts” (Table 3). However, health professionals were unfamiliar with TM practices and thus felt disconnected from the TM healers.
Some women indicated that they self-medicate using biomedical medicines on themselves or their babies to avoid visiting a facility. Most interviewees mentioned that they procure the drugs from informal local pharmacies, the local hospital, ASHAs, or local taxi delivery from other villages and stock them at home. Due to the lack of available pediatric preparations, a woman described manually pulverizing tablets and diluting them with hot water to give them to the baby. Women agreed that the husband is the decision-maker and his permission regarding health decisions is essential; however, this was not stated as a rule (Table 3).
Delay in arrival at the facility
Three significant factors were identified under this domain: transportation and roads, distance to the health facility, and health information and sources (Table 3). The dilapidated condition of the roads appeared to be the most influential factor, as the majority of respondents, specifically men, mentioned challenges in arranging a vehicle to transport patients due to bad roads. Some preferred to travel by foot, and some had either experienced or heard about women delivering on the way. The price quoted by private transportation agencies was often higher than the average costs, especially after dark, increasing the OOP expenditure incurred due to the lack of alternatives like ambulance services or public transportation. An ASHA disclosed that the incentive received to cover transportation costs in the JSSK scheme did not suffice in these circumstances.
The female participants informed that the ASHA was the primary source for information on the services provided in the health centers and health in general. Few respondents indicated receiving information from nurses and doctors, while others received it from the TBAs. A general sense of lack of awareness in their tribe compared to other tribes was conveyed (Table 3).
We visited three health centers located in and around our study villages to corroborate the findings from the IDIs and FGDs. One was open, had an ambulance, and implemented a functional newborn care corner in the labor room. Multiple educational posters and signs of maternal and newborn health were available, informing about immunizations, ANC, PNC, clean delivery practices, governmental incentives like JSY and JSSK, family planning, breastfeeding, malaria and HIV awareness, newborn resuscitation, and the ASHA program. However, almost all the information was presented in English, not in Liangmai. The other facility we visited was sub-optimally functional, with non-availability of running water, improper biohazardous waste disposal, fluctuant electricity, and a lack of modern medical equipment. Some medicines were expired, and others were not properly stored. Supplies seemed to be lacking in the delivery room too. No patient was in the out-patient or in-patient ward during the observation. One visited facility was closed and not functional apparently for a long time.
Discussion
In this concurrent mixed-methods study, we studied the HSB of the mothers and women from the Liangmai tribe and the factors that influence them. To our knowledge, this is the first study to be conducted in this region concerning this topic. The maternal HSB exhibited by this community was influenced by several social, economic, cultural, geographic, and political factors that were closely interlinked.
We identified that the interpersonal and intrapersonal factors significantly influenced the HSB of this tribe. As their perception of risk was low, the tribe has an emergency-driven health-seeking behavior only with evident physical signs of danger. Thus, there is a low preventive-driven health-seeking behavior for ANC and PNC (21). This explains why only 4% of women reported four routine antenatal visits and 41% delivered at home. Functional health centers were better utilized for deliveries by locals living in that village than the villages with no or non-functional health centers. Another dominant reason for low healthcare facility utilization was that community members physically accessed biomedical services only when they perceived severe sickness, complications, or an emergency. It was sought secondary to failure of primary treatment with TM, home remedy, or self-medication. Similar findings were reported in a study of the socio-cultural and service delivery dimensions of maternal mortality in central India (22).
Since pregnancy for this tribe is a normal process and primarily not associated with a disease or a health problem, the decision to visit a health facility is often limited in childbirth, which is additionally determined by obstetric emergencies or in moments of fear. A similar emergency-driven HSB for newborn conditions was observed, except for seeking preventive health associated with receiving immunizations, perhaps because vaccines were most often available in the health centers. This protective behavior can be leveraged as an entry point for mothers and babies to access other health services. Since access to a health center is challenging in this arduous terrain and preventive health is not a priority to this community. Routine preventive antenatal, postnatal, and immunization services could alternatively be delivered monthly by a mobile medical unit linked with the health center allocated for that area in collaboration with the ASHAs as implemented successfully in other Indian states like Tamil Nadu (23).
Previous cases of death of the mother or newborn during childbirth influenced the HSB of the individuals, especially since infant mortality and spontaneous abortions were commonly reported and complemented by the survey results. This contradicts the governmental statistics, where only four stillbirths were reported in the district from 2018 to 19 (17). Any health event occurring in a healthcare facility is more likely to be captured formally by the health information system, but since access to these facilities is limited in remote tribal areas, deaths, and events occurring in these villages are likely to be missed. A national-level survey in India revealed that out of 10,109 scheduled tribe women, 44% reported difficulties accessing healthcare services because of the distance to the health facility and 42% due to inadequate transportation options (24). The results from the multivariable logistic regression analysis also supported this by suggesting that mothers residing in the villages without a health center or one that was not operational were more likely to deliver at home, suggesting that challenges in access may influence the decision to deliver at home.
Traditions and practices handed down from generation to generation influenced the current behavior of the tribe, which still firmly believes in faith healing. This belief is reinforced since TM healers are always locally available, accessible, and conforming to their religious beliefs. Therefore, culture determines the perceptions of the individual and the community regarding their definition of health and well-being (25). This also influences or shapes their sense of coherence, initiating or stopping the individual on the health-ease-disease continuum. In a medical pluralistic system, the Liangmais are struggling between traditional practices and the biomedical health system representing a mixed, interrelated, interdependent, and in a way, competing structure.
From a non-cognitive perspective, the individual’s socioeconomic status influences their decision to seek healthcare services, as highlighted by other studies conducted in Bangladesh and Africa (26–29). The direct and indirect costs incurred to access public services are strongly associated with considerable personal expenditure since the services are not perceived as free. Therefore, they chose to stick to their traditions and prioritize other financially viable options, such as TM or home remedies, as biomedical health expenditures pose a high economic burden on their families. Another study conducted in India also reported financial barriers associated with the lack of access to ANC and safe delivery with lower socioeconomic characteristics (4). The Government of Nagaland has also acknowledged this high OOP expenditure experienced by patients in the state in the State Human Development Report (7). Nevertheless, our observations indicate that in emergency situations, when alternative local healthcare options have been exhausted, financial resources do not play a determining role in visiting healthcare facilities.
When analyzing the adapted three-delays model, we noticed that a delay in one level significantly affects the other subsequent levels. The delay in providing adequate care strongly enhances the uncertainty in the decision to seek care with moderate influence from the delay in arrival to the facility, thus impeding people of the tribe from effectively and promptly seeking biomedical healthcare. Nevertheless, the community finds alternatives to the presented barriers by accessing TM actors, self-medicating using biomedical drugs, or home remedies. As observed in various medical pluralistic studies conducted in South America, a combination of the three alternate modalities has also been demonstrated by the Liangmais (30–32). Since access to essential biomedical medication in the village and health centers is difficult, women tend to store medicines at home and adopt various dosage mechanisms for their babies. Pregnant women and their babies risk experiencing untoward side effects or overdosage due to unsupervised self-medication, as described in a study conducted among pregnant women from Iran (33).
The delay in providing adequate care was also attributed to all previous individual or community experiences, rumors, and beliefs related mainly to the low quality of the services available in the health facilities. Our findings corroborated with Singh et al.’s findings that the lack of resources and services in health centers affects institutional delivery rates in Northeast India (34). Significant concerns regarding the availability of healthcare professionals, opening hours, and lack of medicines and health services deterred them from even attempting to seek maternal or newborn biomedical healthcare services. This was complemented by a study conducted in rural Nigeria that reported that low utilization of government facilities was due to staff irregularities, low quality of services, and the high costs incurred to access them (35). Even health professionals agreed that the facilities were not offering adequate services, which demotivates them from promoting the services, obliging them to adopt risky treatment options and plan strategies for emergency referrals. Given the community’s perception that the quality of services provided at the health centers is defective, the conventional approach to increase the overall knowledge to improve HSB in these communities may prove futile unless the quality and quantity of services in the health centers improve. The state has launched a World Bank-aided project to strengthen a few health centers to mitigate this issue (36). However, this impact is yet to be ascertained in the few communities they serve.
The generalized feeling of shyness among women was an essential attitudinal determinant that discouraged them from consulting male doctors and visiting the health facility since they associate biomedical practices with examining reproductive and sexual organs. Similar findings where feelings of embarrassment influenced the HSB of mothers from Amazonian communities in Peru were reported by Westgard et al. (37). The gender of the healthcare provider (female TBAs, ASHAs, or nurses) is preferred during childbirth. However, this cannot be assumed as the only factor, as male relatives attended deliveries, also denoting a complementary behavior that prefers trust or familiar relationships over gender preferences.
There is no kinship or formal communication between the doctors and the traditional actors, which explains the misunderstandings or incompatibilities between the two systems. It can be assumed that reluctance toward TM originates from the health professional’s perspective. Nonetheless, TM actors see biomedicine, to some extent, as complementary. Some of these elements are also stated in a study of medical pluralism and its implications on health policy in Northeast India (38). Similarly, a rural Ghana study showed that health personnel did not consider traditional birth attendants’ contribution (39). There is also a weak relationship between the community and the doctors, as doctors are not perceived to be present in the facilities when needed. However, a better relationship exists between the community and the nurses, especially for delivery. The most substantial relationship was noted between the ASHAs and the women, especially in the village with a non-functional health center as corroborated by another study from India (40). ASHAs are perceived to have gained credibility in the community, leading to social recognition and increased legitimacy as service providers. Consequently, this kinship can be a potential mechanism to reduce maternal and newborn mortality and morbidity, considering community-oriented primary healthcare as an essential strategy to reduce inequalities by adequately training them and proportionately officially recognizing their efforts and health work, especially in rural, remote indigenous areas such as this. In addition to the ASHAs, traditional healers and TBAs are also primary contact points for mothers seeking treatment. They can also be sensitized and engaged in disseminating information regarding preventive health and be trained to recognize red flags to initiate early referrals.
Another approach to address the low uptake of health services is to strengthen a process named “Communitization,” which formulates a Health Centre Managing Committee (HCMC) that consists of members from the village council, FBOs, and staff from the health center located in the village to closely monitor the functioning of the health center along with the Government. Even before being endorsed nationwide by the National Health Mission, this system originated from a policy implemented by the Government of Nagaland in 2002, titled “The Nagaland Communization of Public Institutions and Services Act” (40). The health component of the scheme purports to ensure that the community is sufficiently and meaningfully represented and empowered to participate in the health center’s planning, implementation, and utilization of services. The HCMC can be further empowered to monitor the performance of government schemes that are intended to influence healthcare delivery uptake positively. The impact and challenges faced by HCMCs in Nagaland have been comprehensively documented by Tushi and Kaur (41).
Our study highlights that if the perceived basic needs of the community are unmet, all other efforts become irrelevant, and services will not be utilized satisfactorily by the community. In a setting such as this, where the community functions around socio-cultural norms, it may be pragmatic for policymakers to adopt a “bottom-up approach” and tailor programs by placing the community’s needs before national objectives. Policies must focus on primarily empowering local village councils, FBOs, and VHCs to monitor their health centers effectively. Inter-sectoral policies from the educational, economic, employment, infrastructure, housing, sanitation, and essential services must also be considered to address the social determinants contributing to this issue. It is relevant to design and implement salutogenic enabling environments that allow individuals to make informed decisions about their health. The objective is to attain health and well-being by guaranteeing substantive freedom and respect for the self-determination of indigenous people.
Conclusion
The HSB of this community is influenced by multiple social, economic, cultural, geographic, and political factors that are closely related. Health facilities are sought only in emergencies, secondary to locally available traditional medicine, determined primarily by the tribe’s perception of the quality of services provided and challenges in geographical access.
Economic reasons, low awareness, unrealistic reimbursements, and inadequate implementation of national schemes were pivotal in deterring access to health facilities. Engaging, recognizing, integrating, and supporting local actors like ASHAs, TBAs, TM healers, and FBOs may be a more realistic approach to influence individual or familial decisions to seek health facilities for maternal and child health. Community agents trained to consider the needs of vulnerable population groups represent a key catalyst in the community system. In addition, community perspectives can provide crucial insight into why health interventions may struggle or succeed in various locations. Moreover, community-led monitoring can provide a vital tool for accountability. This framework must also be supported with adequate financing for these community systems.
At the policy level, the two national programs to financially incentivize institutional deliveries and decrease OOP expenses failed to impact the local health center utilization rates due to inadequate program implementation at the grassroots as it did not consider this region’s cultural and geographical differences. The amount intended to incentivize mothers and ASHAs failed to cover the basic costs they incurred to reach a delivery point. The “one size fits all” approach to planning these policies implemented countrywide has to be tailored to the local needs of the region and must factor in the exorbitant direct and indirect costs involved with travel on rugged terrains.
Strengthening and empowering existing Health Centre Managing Committees to monitor their health centers may improve service quality. The crucial role and impact of communities stem from their strengths, which include but are not limited to legitimacy among individuals, a strong understanding of the contexts, trust, social solidarity, social motivation, and adaptation abilities. Community systems offer critical support in the areas where the conventional health system fails. The extent to which the terrain influences the delays in healthcare access should be comprehensively studied.
Study strengths and limitations
This study is strengthened by its mixed-method approach, reinforcing its implementation with community actors, empowering people as agents who can investigate their own situation, and providing an alternative to traditional research, especially in remote and indigenous areas. The quantitative evidence from a community-based survey was supported by the findings that evolved from the qualitative components of this marginalized population. This study was conducted in one of the region’s most remote areas, being indicative of logistical problems and organizational/financial difficulties.
Due to time constraints, 22 of the 26 audio recordings were directly transcribed and translated to English, with additional revisions of the translations in collaboration with an external Liangmai native speaker.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by the Ethics Committee of the Medical Faculty, the Ruprecht Karls University of Heidelberg, Germany (#S-138/2019, 13.03.2019), and the Institutional Review Board (Research and Ethics Committee) of the Christian Institute of Health Sciences and Research, Nagaland, India. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
AD, ÁLC, RK, and RR developed the idea and designed the study. ÁLC and RR elaborated the methodology and data collection tools with the support of AD. ÁLC, PN, and RK collected the data. PN translated and transcribed the data. ÁLC analyzed the qualitative data with the backing of AD. RR analysed the quantitative data. ÁLC, RR, PN, RK, and AD contributed to data interpretation. ÁLC drafted the manuscript. ÁLC, AD, and RR revised the final version of this manuscript. All authors contributed to the article and approved the submitted version.
Funding
A research grant from the German Academic Exchange Service (DAAD) covered logistical costs for the fieldwork. All the other costs were covered by ÁLC. The Science and Engineering Research Board, Department of Science and Technology (Sanction Order: ECR/2016/002059), funded the community-based survey (Project on the use of Geographic Information Systems in Health Systems Research in Rural Areas of Nagaland). For the publication fee we acknowledge financial support by Deutsche Forschungsgemeinschaft within the funding programme “Open Access Publikationskosten” as well as by Heidelberg University.
Acknowledgments
This research would not have been possible without the unique collaboration and the indispensable support and kindness of the members of the Liangmai tribe. The authors also thank Sedevi Angami, Director, Christian Institute of Health Sciences and Research, Nagaland, India, for his unending support. The authors also thank Venkateshprabhu Janagaraj for his help with the map.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1139334/full#supplementary-material
Abbreviations
ASHA, Accredited social health activist; ANC, Antenatal care; CHW, Community health worker; TBA, Traditional birth attendant; FGD, Focus group discussion; HSB, Health seeking behavior; IDI, In-depth interviews; JSSK, Janani Shishu Suraksha Karyakaram; JSY, Janani Suraksha Yojana; OOP, Out-of-pocket expenditure; PNC, Postnatal care; TH, Traditional healers; TM, Traditional medicine; SEM, Socio-ecological model.
References
1. The United Nations Children's fund. Maternal health . (2016). Available at: http://unicef.in/Whatwedo/1/Maternal-Health (Accessed January 23, 2019).
2. The United Nations Population Fund. Maternal health-digital . (2016). Available at: https://www.unfpa.org/maternal-health. (Accessed January 23, 2019).
3. The United Nations Children's fund. Maternal health . (2015). Available at: http://unicef.in/Whatwedo/1/Maternal-Health (Accessed January 23, 2019).
4. Sankar, MJ , Neogi, SB , Sharma, J , Chauhan, M , Srivastava, R , Prabhakar, PK, et al. State of newborn health in India. J Perinatol. (2016) 36:S3–8. doi: 10.1038/jp.2016.183
5. Ministry of Health and Family Welfare . National Health Profile − 2018. New Delhi: (2018). 336 p.
6. Swedish Agency for Growth and Policy Analysis . (2013). India’s healthcare system: Overview and quality improvements. Available at: https://www.tillvaxtanalys.se/in-english/publications/direct-response/direct-response/2013-05-20-indias-healthcare-system-----overview-and-quality-improvements.html (Accessed May 1, 2019).
7. Government of Nagaland . (2016). Nagaland: State human development report. Kohima. Available at: https://es.scribd.com/document/381850403/Nagaland-SHDR-2016-Final-Mail (Accessed January 25, 2022).
8. Ministry of Health and Family Welfare . (2011). Update on the ASHA Programme. Available at: https://nhsrcindia.org/sites/default/files/2021-06/Update%20on%20ASHA%20Programme%20%20July%202011.pdf (Accessed May 1, 2019).
9. Expert Committee on Tribal Health . (2018). Tribal health in India: bridging the gap and a roadmap for the future. Available at: http://nhm.gov.in/nhm_components/tribal_report/Executive_Summary.pdf (Accessed May 01, 2019).
10. Poverty and Inequality in Nagaland . (2017). Available at: http://ijahms.com/upcomingissue/09.06.2017.pdf (Accessed May 28, 2022).
11. Ministry of Health and Family Welfare . (2016). National Family Health Survey (NFHS-4). Available at: http://rchiips.org/nfhs/nfhs-4Reports/India.pdf (Accessed May 01, 2019).
12. Census India . (2001). Nagaland data highlights: the scheduled tribes. Available at: https://censusindia.gov.in/Tables_Published/SCST/dh_st_nagaland.pdf (Accessed May 01, 2019)
13. Directorate of census operations, census of India 2011: Nagaland . District census handbook Peren. (2011). Available at: https://www.censusindia.gov.in/2011census/dchb/1311_PART_B_DCHB_PEREN.pdf (Accessed May 01, 2019).
14. Oppitz, M , Kaiser, T , von Stockhausen, A , and Wettstein, M . Naga Identities: Changing Local Cultures in the Northeast of India. Ghent, Belgium: Snoeck Publishers (2008). 464 p.
15. Government of Nagaland . District plan-Peren. (2018). Available at: https://cdn.s3waas.gov.in/s32dea61eed4bceec564a00115c4d21334/uploads/2018/08/2018082872.pdf (Accessed May 01, 2019).
16. Ministry of Health and Family Welfare . Nagaland-National Family Health Survey (NFHS-4). (2016). Available at: http://rchiips.org/nfhs/NFHS-4Reports/Nagaland.pdf (Accessed May 01, 2019).
17. Ministry of Health and Family Welfare . (2019). Performance of key HMIS indicators for Peren, 2018-19. Available at: https://hmis.nhp.gov.in/#!/standardReport. (Accessed February 01, 2019).
18. Chokshi, M , Patil, B , Khanna, R , Neogi, SB , Sharma, J , Paul, VK, et al. Health systems in India. J Perinatol. (2016) 36:S9–S12. doi: 10.1038/jp.2016.184
19. Glanz, K . Theory at a glance: a guide for health promotion practice, vol. viii. 2nd ed. Washington, USA: Dept of Health and Human Services, National Cancer Institute (2005). 52 p.
20. Thaddeus, S , and Maine, D . Too far to walk: maternal mortality in context. Soc Sci Med. (1994) 38:1091–110. doi: 10.1016/0277-9536(94)90226-7
21. Sychareun, V , Somphet, V , Chaleunvong, K , Hansana, V , Phengsavanh, A , Xayavong, S, et al. Perceptions and understandings of pregnancy, antenatal care and postpartum care among rural Lao women and their families. BMC Pregnancy Childbirth. (2016) 16:245. doi: 10.1186/s12884-016-1031-8
22. Jat, TR , Deo, PR , Goicolea, I , Hurtig, AK , and San, SM . Socio-cultural and service delivery dimensions of maternal mortality in rural Central India: a qualitative exploration using a human rights lens. Glob Health Action. (2015) 8:24976. doi: 10.3402/gha.v8.24976
23. Department of Health & family welfare Govt. of Tamil Nadu, India . (2022). Mobile medical units (MMU) National Health Mission-Tamil Nadu. Available at: https://nhm.tn.gov.in/en/r-c-h/mobile-medical-units-mmu (Accessed April 1, 2022).
24. Ministry of Health and Family Welfare . (2006). National Family Health Survey (NFHS-3). Available at: https://dhsprogram.com/pubs/pdf/frind3/frind3-vol1andvol2.pdf (Accessed March 23, 2023).
25. Graner, S , Klingberg-Allvin, M , Duong le, Q , Krantz, G , and Mogren, I . Pregnant women's perception on signs and symptoms during pregnancy and maternal health care in a rural low-resource setting. Acta Obstet Gynecol Scand. (2013) 92:1094–100. doi: 10.1111/aogs.12170
26. Amin, R , Shah, NM , and Becker, S . Socioeconomic factors differentiating maternal and child health-seeking behavior in rural Bangladesh: a cross-sectional analysis. Int J Equity Health. (2010) 9:9. doi: 10.1186/1475-9276-9-9
27. Tuyisenge, G , Hategeka, C , Kasine, Y , Luginaah, I , Cechetto, D , and Rulisa, S . Mothers' perceptions and experiences of using maternal health-care services in Rwanda. Women Health. (2019) 59:68–84. doi: 10.1080/03630242.2018.1434591
28. Babalola, S , and Fatusi, A . Determinants of use of maternal health services in Nigeria--looking beyond individual and household factors. BMC Pregnancy Childbirth. (2009) 9:43. doi: 10.1186/1471-2393-9-43
29. Firoz, T , Vidler, M , Makanga, PT , Boene, H , Chiau, R , Sevene, E, et al. Community perspectives on the determinants of maternal health in rural southern Mozambique: a qualitative study. Reprod Health. (2016) 13:112. doi: 10.1186/s12978-016-0217-x
30. Zank, S , and Hanazaki, N . The coexistence of traditional medicine and biomedicine: a study with local health experts in two Brazilian regions. PLoS One. (2017) 12:e0174731. doi: 10.1371/journal.pone.0174731
31. Calvet-Mir, L , Reyes-Garcia, V , and Tanner, S . Is there a divide between local medicinal knowledge and Western medicine? A case study among native Amazonians in Bolivia. J Ethnobiol Ethnomed. (2008) 4:18. doi: 10.1186/1746-4269-4-18
32. Vandebroek, I , Calewaert, JB , De Jonckheere, S , Sanca, S , Semo, L , Van Damme, P, et al. use of medicinal plants and pharmaceuticals by indigenous communities in the Bolivian Andes and Amazon. Bull World Health Organ. (2004) 82:243–50.
33. Ebrahimi, H , Atashsokhan, G , Amanpour, F , and Hamidzadeh, A . Self-medication and its risk factors among women before and during pregnancy. Pan Afr Med J. (2017) 27:183. doi: 10.11604/pamj.2017.27.183.10030
34. Singh, K , and Kanika, G . Factors affecting maternal health care seeking behaviour in northeast states, India: evidence from district level household survey-4 (2012-2013). Int J Res Med Sci. (2016) 4:4949–56. doi: 10.18203/2320-6012.ijrms20163797
35. Osubor, KM , Fatusi, AO , and Chiwuzie, JC . Maternal health-seeking behavior and associated factors in a rural Nigerian community. Matern Child Health J. (2006) 10:159–69. doi: 10.1007/s10995-005-0037-z
36. Morung Express . (2017). 4 major health projects launched in Nagaland. Available at: https://morungexpress.com/4-major-health-projects-launched-nagaland (Accessed April 9, 2022).
37. Westgard, CM , Rogers, A , Bello, G , and Rivadeneyra, N . Health service utilization, perspectives, and health-seeking behavior for maternal and child health services in the Amazon of Peru, a mixed-methods study. Int J Equity Health. (2019) 18:155. doi: 10.1186/s12939-019-1056-5
38. Albert, S , Nongrum, M , Webb, EL , Porter, JD , and Kharkongor, GC . Medical pluralism among indigenous peoples in Northeast India – implications for health policy. Tropical Med Int Health. (2015) 20:952–60. doi: 10.1111/tmi.12499
39. Adatara, P , Afaya, A , Baku, EA , Salia, SM , and Asempah, A . Perspective of traditional birth attendants on their experiences and roles in maternal health Care in Rural Areas of northern Ghana. Int J Reprod Med. (2018) 2018:2165627–10. doi: 10.1155/2018/2165627
40. Hamal, M , de Cock, BT , De Brouwere, V , Bardaji, A , and Dieleman, M . How does social accountability contribute to better maternal health outcomes? A qualitative study on perceived changes with government and civil society actors in Gujarat, India. BMC Health Serv Res. (2018) 18:653. doi: 10.1186/s12913-018-3453-7
Keywords: maternal and newborn health, health seeking behavior, tribal, access to health services, health service utilization, social determinants of health, universal health coverage (UHC), India
Citation: Cáceres ÁL, Ramesh RM, Newmai P, Kikon R and Deckert A (2023) Perceptions, health seeking behavior and utilization of maternal and newborn health services among an indigenous tribal community in Northeast India—a community-based mixed methods study. Front. Public Health. 11:1139334. doi: 10.3389/fpubh.2023.1139334
Edited by:
Lorena Binfa, University of Chile, ChileReviewed by:
Cristina González Blázquez, Universidad Autónoma de Madrid, SpainXavier Espada-Trespalacios, Universitat Ramon Llull, Spain
Olga Canet-Vélez, Universitat Ramon Llull, Spain
Copyright © 2023 Cáceres, Ramesh, Newmai, Kikon and Deckert. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ángela León Cáceres, YW5nZWxhbGVvbmNhY2VyZXNAZ21haWwuY29t; Andreas Deckert, YS5kZWNrZXJ0QHVuaS1oZWlkZWxiZXJnLmRl
†Present address: Rohan Michael Ramesh, Division of Gastrointestinal Sciences, The Wellcome Trust Research Laboratory, Christian Medical College, Vellore, India
‡These authors have contributed equally to this work and share first authorship
§ORCID: Ángela León Cáceres https://orcid.org/0000-0002-4517-9409
Rohan Michael Ramesh https://orcid.org/0000-0002-1089-6037