Abstract
Background:
Nurse turnover has become a salient issue in healthcare system worldwide and seriously compromises patient outcomes. Social support is considered an effective contributor to alleviate nurse turnover intention (TI). However, the degree of correlation between social support and nurse TI remains elusive.
Aims:
This study aims to evaluate the strength of the effectiveness of social support on TI among nurses as well as its potential moderators.
Design:
This systematic review and meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Methods:
To obtained qualified studies, two researchers searched Embase, PubMed, Web of science, CINAHL, CNKI, WanFang, and Chinese Medical Journal Full Text Database from inception to January 6, 2024. Meta-analysis, publication bias, and sensitivity analysis were carried out on the included studies using CMA 3.0 software, and the moderating effect was verified through meta-analysis of variance (ANOVA).
Results:
A total of 38 studies were obtained, involving 63,989 clinical nurses. The comprehensive effect size of the random effect model showed a significant medium negative correlation between social support and TI among nurses (p < 0.001). The sample size and TI measurement tools significantly moderated the correlation between social support and TI (p < 0.050). However, nurse department, gender, data collection time, and social support measurement tools did not moderate the correlation between the two variables.
Conclusion:
Social support is negatively associated with TI in nurses. Nursing administrators and the medical community should fully recognize the importance of social support for nurses and take corresponding measures to enhance it, thereby reducing TI and ensuring the stability of the nursing team.
1 Introduction
The demand for nurses is growing rapidly due to the extended life expectancy, aging populations, and increased need for high-quality healthcare services (1–3). By 2035, the aggregate need for nurses is likely to reach 12.9 million (4). In reality, however, there is a significant gap between the supply and demand of nursing staff. Almost all healthcare systems worldwide are facing a nursing shortage and it is expected that by 2030, there will be a shortfall of 10 million nurses (5). The shortage of nursing staff will make a series of negative impacts including but not limited to increasing the hospital infection rate (6), medical error rate (7), patient readmission rate (8), pressure ulcer incidence (7), and even mortality (9), which ultimately compromises the patient safety and quality of medical services.
Nursing shortage is an ongoing issue in health organizations and researchers (10, 11). There is a plenty of factors contributing to the shortage of nursing staff, among which the high nursing turnover rate is considered one of the major ones (12). Frequent turnover behaviors may reduce the organizational efficiency, lead to emotional instability and lax behavior among other employees in the organization, and increase hospital investment in nurse training (13). In the case of a shortage of nurses, it is imperative that nurse managers plan effective retention strategies based on the reasons for staff resignation (14). Turnover intention (TI) refers to the tendency of employees to leave their current job positions and seek other job opportunities (15), which is considered an important cognitive process before turnover behavior occurs, and hence, it is the best and reliable antecedent variable for predicting turnover behavior (16). The higher the TI, the greater the likelihood of turnover behavior occurring (17). Moreover, TI can also subside the work enthusiasm and stability of nurses, and impair the nursing service quality (15).
In recent years, scholars worldwide are dedicated to exploring the factors that affect nurse TI, and determine social support as one of the psychological and social factors beneficial for weakening nurse TI (18, 19). Social support is defined as providing assistance and protection to others, especially individuals (20), including tangible economic assistance and intangible emotional assistance (21). For nurses, social support from supervisors and colleagues is an important source of perceived social support (22, 23). Nurses often face workplace stress in clinical work, including high workloads, complex patient situations, management’s leadership styles, role conflicts, and workplace aggression (24, 25). The buffering model of social support suggests that an effective social support network can alleviate the negative psychological consequences of stress (26) and is also an important protective factor in alleviating employee turnover (23).
Numerous studies have been conducted on the correlation between social support and TI in nurses. However, there are considerable divergences in the results of the existing studies, especially the degree of correlation between the two variables. For instance, Lei et al. (27) conducted a survey on 82 female emergency department nurses using the Social Support Rating Scale (SSRS) and Turnover Intention Questionnaire (TIQ), and found that the correlation coefficient between social support and TI was −0.711. Yu and Gui (28) measured 445 nurses from emergency department (93.03% female) using the Perceived Social Support Scale (PSSS) and a single item in 2020, and found that the r value of the correlation between two variables was −0.478. However, Gülcan (29) evaluated 183 clinical nurses (86.3% female) using a 6-item and 3-item questionnaire, and found that the r value of the correlation between social support and TI was −0.154. In addition to the different degrees of correlation, the correlation between supervisor support and TI, as well as the correlation between colleague support and TI, were also reported in different directions. By using a 4-item questionnaire and a 3-item questionnaire, Adriaenssens and Van Bogaert (30) concluded r values of 0.313 and 0.039 for the correlation between supervisor support and colleague support with TI among nurses, respectively. Galletta et al. (31) used an adapted version of the Perceived Organizational Support Questionnaire and a two-item questionnaire to measure the correlation between supervisor support and TI, yielding a r value of −0.187 for the two variables. In the study of Pisarski et al. (22), a negative correlation (r = −0.296) was also reported between colleague support and TI. The differences in the degree and direction of correlation between social support and TI among nurses may be attributed to the differences in the study sample, study design, and measurement tools. Therefore, it is necessary to synthesize the existing research results to verify the correlation between social support and TI among nurses and to further analyze the moderating variables that affect the correlation between the two.
Regarding the study sample, existing studies involve nurses from different departments (such as emergency department, operating room, or departments that have not been clearly reported) and nurses of different genders. The specific work undertaken by nurses in different departments may affect the TI to varying degrees. For example, as the front-line staff about hospital systems, nurses from emergency department face challenging working conditions due to casualty incidents and potentially violent situations (32, 33). Moreover, the work of the emergency department is characterized by a wide range of pathologies and a broad variety of emergencies, leading to higher nursing requirements (34). In contrast, nurses from operating room are responsible for sterility, equipment, infection, complication control, and biological specimen management during surgery, while also adapting to the different personalities and surgical techniques of different surgeons (35, 36). A previous study showed that the TI of nurses from emergency department and ICU was higher than that of general ward nurses (37). Kim and Park (38) pointed out that pediatric nurses were under greater pressure and had higher TI than general ward nurses. Additionally, there are also gender differences in the TI and perceived social support of nurses. For example, Ma et al. (32) and Zhao et al. (39) reported no significant difference in TI scores of nurses of different genders. Conversely, Xu et al. (19) found that the TI score of male nurses was significantly higher than that of female nurses. Therefore, we propose the following hypothesis: the department and gender of nurses may affect the correlation between social support and TI.
In terms of study design, there are also differences in the sample size and data collection time of existing studies. Sample size is a key parameter for the calculation of comprehensive correlation coefficients (40). In a study with a small sample size, the magnitude of the correlation is quite unstable (41). Previous studies on the correlation between social support and TI showed significant differences in the sample size, ranging from 82 (27) to 16,052 (42). Furthermore, the impact of data collection time on the correlation between the two variables should not be ignored. In particular, the COVID-19 pandemic has increased the demand and workload for nurses. The uncertainty and mortality of diseases also put tremendous psychological pressure on nurses. Mirzaei et al. (43) found that the intense work pressure during the COVID-19 shaped the work attitude of nurses, resulting in stronger TI among nurses. A literature review of 43 studies also revealed a significant increase in TI among nurses following the COVID-19 pandemic (44). Thus, the hypothesis of this study is as follows: sample size and data collection time may be potential moderators of the correlation between social support and TI.
In addition to the variables mentioned above, existing studies have included different measurement tools for social support and TI, which may also moderate the correlation between these two variables. Social Support Rating Scale (SSRS) (18, 27), Perceived Social Support Scale (PSSS) (19, 28), and multiple item measurement questionnaires (43, 45) were mainly used to measure the perceived social support of clinical nurses. Similarly, there are several different measurement tools for TI, such as turnover intention questionnaire (TIQ, 1982) (18, 39), Turnover Intention Scale (TIS) (46), and TIQ (2015) (19). Different measurement tools contain different contents. Therefore, the correlation between social support and TI among nurses may be influenced by the measurement tools.
Given the importance of maintaining professional stability in nurses and the lack of systematic meta-analyses that assess the relationship of social support with nurses’ TI, this study aimed to analyze the strength of the effectiveness of social support on the nurses’ TI as well as its potential moderators. Specifically, this study (a) calculated the overall effect size of the relationship between social support and nurses’ TI and (b) examined whether the relationship is moderated by nurse’s department, sex, sample sizes, data collection time, social support measurement tools, and TI measurement tools. This study enables nursing administrators and the medical field to pay more attention to nurses’ social support and take corresponding measures to improve it, intending to reduce nurses’ TI and promote a more stable nursing team.
2 Methods
2.1 Study design
This study was designed and written following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (47). This agreement has been registered in the International Prospective Register of Systematic Reviews (PROSPERO; number: CRD42023476373).
2.2 Search strategy
A comprehensive search was conducted on CNKI, Wanfang, Chinese Medical Journal Full Text Database, PubMed, Web of Science, Embase, and CINAHL databases to obtain relevant literature on clinical nurses’ social support and TI from the inception of the database to January 6, 2024. The search terms included “nurses,” “social support,” and “turnover intention.” The search terms for nurses included “nurse” and “nursers.” The search term for social support included “social support.” The search terms for TI included “turnover intention,” “turnover to quit,” “turnover to leave,” and “resignation intention.” To further expand the search scope, we checked the list of references included in the literature. The detailed search formula can be found in Supplementary material 1.
2.3 Inclusion criteria
The retrieved literature was screened by two researchers based on the following inclusion and exclusion criteria. Inclusion criteria: (1) considering the availability of data on correlations between the two variables, study types were limited to cross-sectional studies and longitudinal studies reporting multiple cross-sections; (2) published in English or Chinese; (3) participants are clinical nurses, regardless of department; (4) reporting on social support and TI or calculating the Pearson’s correlation coefficient based on existing data; (5) applied clear tools for measuring social support and TI, including, but not limited to, PSSS (1988) and SSRS (1986) for social support and TIQ (1982) and TIS (1991) for TI; (6) the type of literature is limited to journal article. Exclusion criteria: (1) studies with the same data and repeated publications; (2) studies with data errors, such as those where the sample size or the correlation coefficient reported different data.
2.4 Data extraction
After literature screening, the two researchers read the entire text to extract data. The extracted information was as follows: author, year, country, publication type, sample size, sample gender, department, sample collection time, social support measurement tool, TI measurement tool, as well as Pearson correlation coefficient between social support and TI. If several different samples were investigated in the same study, they were extracted separately. Any disputes during the data extraction process were discussed and decided by two researchers.
2.5 Quality assessment tool
The “Joanna Briggs Report Epidemic Data Research Institute Key Assessment Checklist” (48) was used for quality evaluation. This checklist consists of 9 items, each of which includes four answers (“yes,” “no,” “unclear,” and “not applicable”). If the answer is “yes,” 1 point will be given; If the answer is “no,” “unclear,” or “not applicable,” zero point will be scored. The total score of the scale is 9, and the higher the score, the better the quality of the study.
2.6 Statistical analysis
Pearson correlation coefficient was used to calculate the magnitude of correlation between social support and TI. Firstly, we used the formula Fisher’s Z = 0.5 ln [(1 + r)/(1-r)] to convert the value of r to Fisher’s Z. Then, based on the sample size, the obtained values were weighted using the formula SEz = and the reciprocal of the variance of the correlation coefficient. Finally, the formula Summary r = ()/() was used to convert all values into r to evaluate the correlation between social support and TI. According to the study of Gignac and Szodorai (49), r = 0.10, r = 0.20, and r = 0.30 are indicative of relatively small, medium, and relatively large correlations, respectively. Heterogeneity was determined using Cochran’s Q-test and I2 statistics (50). The random effect model did not assume a common potential effect size for all included studies (51), making the random effect model more suitable for current analysis than the fixed effect model. In addition, a meta-analysis of variance (ANOVA) was used to test the possible moderating variable between social support and TI. Inter- and intra-group comparisons were performed using Q-test. Funnel plots, Begg test (52), and Egger test (53) were applied to evaluate the publication bias. When the funnel plot is symmetrical at both ends and the p-values >0.05 for both Begg test and Egger test, it is considered that there is no publication bias. Simultaneously, sensitivity analysis was conducted to test the robustness of the results. All statistical analyses of this study were conducted using the software Comprehensive Meta-Analysis (CMA), version 3.0.
3 Results
3.1 Study characteristics and quality assessment
A total of 731 records (Embase 62, PubMed 34, Web of Science 426, CINAHL 59, CNKI 94, WanFang 51, Chinese Medical Journal Full Text Database 3, and other sources 2) were preliminarily searched in this study (Figure 1). After duplicate removal, 576 studies were obtained. Thereafter, we read the titles and abstracts and reviewed the full text of 95 studies, obtaining 39 eligible studies. Finally, after discussion between two researchers, studies with poor quality will be excluded. A total of 38 studies were obtained (Table 1), with a total sample size of 63,989. Zhou and Wang (76) reported the correlation between social support and TI among nurses in secondary and tertiary hospitals. van der Heijden et al. (23) and Gabel Shemueli et al. (46) both reported the correlation between two variables in nurses from different countries. In the study of Tei-Tominaga et al. (45), the correlation between social support and TI among nurses at different birth stages was reported. For the quality assessment of the included studies, 10 studies scored 6 points, 14 studies scored 7 points, 13 studies scored 8 points, and only 1 study scored 9 points. The detailed quality assessment of included studies can be found in Supplementary material 2.
Figure 1

The process of literature screening.
Table 1
| Study | Sample size (women/men) | Age (mean ± sd/range) | Country | Department | Study type | Social support measurement tool | Turnover intention measurement tool |
|---|---|---|---|---|---|---|---|
| Schmieder and Smith (54) | 191 (183/8) | 35 | USA | No report | Cross-sectional | 13-item scale developed by House and Wells (55) | Three items from the Michigan Organizational Assessment Questionnaire [Seashore et al. (56)] |
| Baba et al. (57) | 119 (108/11) | 37.29 ± 8.87 | Caribbean | No report | Cross-sectional | 10 items taken from House and Wells (55) | Three items questionnaire adopted from Mobley (58) |
| Pisarski et al. (22) | 1,257 (1,113/144) | Public hospitals: 36 Private hospitals: 39 |
Australia | No report | Cross-sectional | A scale adapted from Caplan et al. (59) | The scales developed by Caplan et al. (59) |
| Widerszal-Bazyl et al. (42) | 16,052 (16,052/0) | 39.4 ± 8.8 | Europe | No report | Cross-sectional | Developed by Van der Heijden (60) | Three items questionnaire adopted from Mobley (58) |
| van der Heijden et al. (23) | Belgium: 1,686 (1,686/0) Germany: 2,048 (2,048/0) Finland: 1,724 (1,724/0) France: 2,182 (2,182/0) Italy: 3,308 (3,308/0) Netherlands: 2,127 (2,127/0) Poland: 3,089 (3,089/0) Slovakia: 1,360 (1,360/0) |
Belgium: 37.7 ± 8.96 Germany: 38.01 ± 9.2 Finland: 42.14 ± 10.04 France: 38.65 ± 9.31 Italy: 38.23 ± 7.56 Netherlands: 37.93 ± 9.45 Poland: 38.71 ± 7.21 Slovakia: 40.37 ± 8.26 |
Belgium Germany Finland France Italy Netherlands Poland Slovakia |
No report | Cross-sectional | Four items [Van der Heijden (61)] | One item |
| Adriaenssens et al. (62) | 254 (140/114) | 37.61 ± 8.82 | Belgium | Emergency | Cross-sectional | 4 items (Leiden Quality of Work Questionnaire for Nurses) | 3 items (Leiden Quality of Work Questionnaire for Nurses) |
| Galletta et al. (31) | 1,240 (1,010/230) | Women: 36.95 ± 7.91 Men: 37.31 ± 8.19 |
Italy | No report | Cross-sectional | The adapted of the survey of perceived organizational support | Two items adapted from Hom et al. (63) |
| He and Sun (64) | 210 (No report) | 28.27 ± 4.27 | China | Emergency | Cross-sectional | SSRS [Xiao (65)] | Turnover Intention Questionnaire [Brough and Frame (66)] |
| Fang et al. (67) | 194 (No report) | 35.82 ± 9.5 | China | No report | Cross-sectional | PSSS [Zimet et al. (68)] | TIQ [Michaels and Spector (69)] |
| Lei et al. (27) | 82 (82/0) | No report | China | Emergency | Cross-sectional | SSRS [Xiao (65)] | TIQ [Michaels and Spector (69)] |
| van Dam et al. (70) | 461 (No report) | 41.9 ± 9.43 | Netherlands | Intensive care | Cross-sectional | van Veldhoven et al. (71) | Turnover intention scale [van Dam (72)] |
| Cai et al. (73) | 133 (128/5) | 21–25 | China | No report | Cross-sectional | PSSS [Zimet et al. (68)] | TIQ [Michaels and Spector (69)] |
| Wu et al. (74) | 632 (617/15) | 27.2 ± 4.34 | China | Multiple departments | Cross-sectional | SSRS [Xiao (65)] | TIQ [Michaels and Spector (69)] |
| Zheng et al. (75) | 858 (850/8) | 34.45 ± 6.5 | China | Multiple departments | Cross-sectional | PSSS [Zimet et al. (68)] | TIQ [Michaels and Spector (69)] |
| Zhou and Wang (76) | Secondary Hospital: 353 (353/0) Tertiary Hospital: 438 (438/0) |
No report | China | Emergency | Cross-sectional | SSRS [Xiao et al. (65)] | TIQ [Michaels and Spector (69)] |
| Gabel Shemueli et al. (46) | Uruguay: 316 (299/17) Spain: 502 (458/44) |
Uruguay: 40.3 ± 9.78 Spain: 44 ± 10.8 |
Uruguay Spain |
No report | Cross-sectional | Dolan et al. (77) | TIS [Arsenault et al. (78)] |
| Adriaenssens and Van Bogaert (30) | 318 (188/130) | 45.7 | Belgium | Multiple departments | Cross-sectional | 4 items (Leiden Quality of Work Questionnaire for Nurses) | 3 items (Leiden Quality of Work Questionnaire for Nurses) |
| Chen et al. (79) | 1,305 (1,247/58) | 35.89 ± 6.36 | China | Operating theatre | Cross-sectional | SSRS [Xiao (65)] | TIQ [Michaels and Spector (69)] |
| Tei-Tominaga et al. (45) | Born in 1950–1964: 673 (673/0) Born in 1965–1979: 1,912 (1,912/0) Born during the 1980s: 1,786 (1,786/0) Boen after 1990: 693 (693/0) |
Born in 1950–1964: 54.23 ± 3.13 Born in 1965–1979: 41.38 ± 4.24 Born during the 1980s: 29.91 ± 7.1 Boen after 1990: 22.99 ± 0.86 |
Japan | No report | Cross-sectional | Three-item original scale, which was developed by the researchers after referring to previous studies | Six-item scale |
| Xie et al. (80) | 175 (174/1) | No report | China | Pediatric | Cross-sectional | SSRS [Xiao (65)] | TIQ [Michaels and Spector (69)] |
| Zhu and Qin (81) | 282 (259/23) | 28.01 ± 4.04 | China | No report | Cross-sectional | SSRS [Xiao (65)] | Turnover intention scale [Zhang (82)] |
| Huang et al. (83) | 370 (348/22) | No report | China | No report | Cross-sectional | The Social Network Model Scale | Departure Disposition Scale [Richard and Johnson (84)] |
| Wang et al. (85) | 2,345 (2,280/65) | 29.74 ± 7.41 | China | Multiple departments | Cross-sectional | SSRS [Xiao (65)] | TIQ [Michaels and Spector (69)] |
| Yeh et al. (86) | 198 (188/10) | No report | China | No report | Cross-sectional | The Chinese version of the Job Content Questionnaire (C–JCQ) [Cheng et al. (87)] | Four questions [Mobley (58)] |
| Cao et al. (88) | 361 (298/63) | 22.38 ± 1.23 | China | Multiple departments | Cross-sectional | PSSS [Zimet et al. (68)] | Turnover intention scale [Lee and Lee (89)] |
| Cole et al. (90) | 111 (No report) | No report | USA | No report | Cross-sectional | Four items | Two items |
| Hognestad Haaland et al. (91) | 2,946 (2,661/285) | No report | Norway | Multiple departments | Cross-sectional | A three-item scale developed by van der Heijden (60) | Three items |
| Meng et al. (92) | 177 (0/177) | 20–45 | China | Multiple departments | Cross-sectional | PIS [Liu et al. (93)] | TIQ [Michaels and Spector (69)] |
| Mirzaei et al. (43) | 479 (295/184) | 33.48 ± 6.77 | Iran | Multiple departments | Cross-sectional | Social support scale (8 items) | Turnover Intention Questionnaire [Kim and Leung (94)] |
| Modaresnezhad et al. (95) | 1,080 (No report) | No report | USA | Multiple departments | Cross-sectional | Finley et al. (96) | Turnover Intention [Price (97)] |
| Zhao et al. (39) | 296 (272/24) | No report | China | Multiple departments | Cross-sectional | SSRS [Xiao (65)] | TIQ [Michaels and Spector (69)] |
| Zhang et al. (98) | 594 (587/7) | 30 ± 7.6 | China | No report | Cross-sectional | SSRS [Xiao (65)] | TIQ [Michaels and Spector (69)] |
| Wu et al. (99) | 118 (105/13) | No report | China | Operating theatre | Cross-sectional | Social Support Scale [Liu et al. (100)] | Cole and Bruch (101) |
| Xiao et al. (18) | 4,865 (4,738/127) | No report | China | Multiple departments | Cross-sectional | SSRS [Xiao (65)] | TIQ [Michaels and Spector (69)] |
| Yu and Gui (28) | 445 (414/31) | 30.74 ± 6.81 | China | Emergency | Cross-sectional | PSSS [Zimet et al. (68)] | One item |
| Zhang et al. (40) | 488 (486/2) | ≥18 | China | Multiple departments | Cross-sectional | Occupational Stress Inventory (1998) | TIQ [Michaels and Spector (69)] |
| Li (102) | 96 (87/9) | 31.12 ± 3.59 | China | Emergency | Cross-sectional | SSRS [Xiao (65)] | TIQ [Michaels and Spector (69)] |
| Xu et al. (19) | 1,060 (985/75) | 32.94 ± 7.876 | China | Operating theatre | Cross-sectional | PSSS [Zimet et al. (68)] | The turnover intention questionnaire [Lee et al. (103)] |
Characteristics of 38 included studies.
SSRS, Social Support Rating Scale; PSSS, Perceived Social Support Scale; PIS, Professional Identity Scale; TIQ, Turnover Intention Questionnaire; TIS, The Turnover Intention Scale.
3.2 Effect size and heterogeneity
3.2.1 The summary correlation between social support and TI
Data on a total of 39,068 clinical nurses was included in 34 effect sizes from 29 studies. Heterogeneity test results showed a high heterogeneity among included studies (Q = 431.338, p < 0.001, I2 = 92.349%). As shown in Figure 2, the random effect model indicated a significant negative correlation between social support and TI (r = −0.278, 95% CI: −0.317, −0.239, p < 0.001).
Figure 2
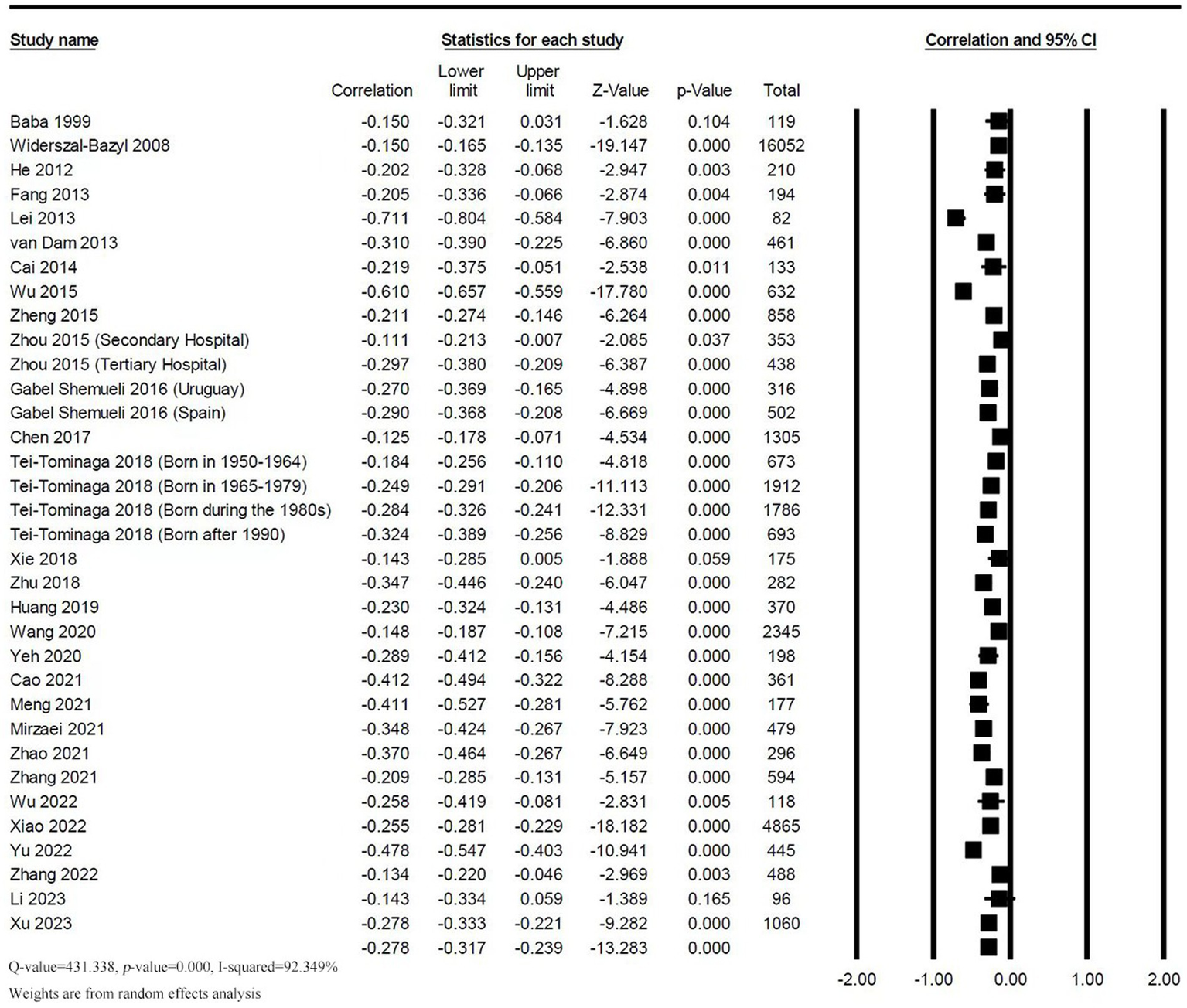
Forest plot of the correlation between social support and TI.
3.2.2 The summary correlation between supervisor support and TI
The correlation between supervisor support and TI was reported in 9 studies with 16 effect sizes. Heterogeneity test found a high heterogeneity (Q = 262.746; p < 0.001; I2 = 94.291%). The random effect model showed a low negative correlation between supervisor support and TI among nurses (r = −0.119, 95% CI: −0.172, −0.065, p < 0.001), as shown in Figure 3.
Figure 3

Forest plot of the correlation between supervisor support and TI.
3.2.3 The summary correlation between colleague support and TI
The correlation between colleague support and TI was reported in 5 studies with 12 effect sizes. There was a high heterogeneity among the combined results (Q = 95.981, p < 0.001, I2 = 88.539%). The random effect model results revealed a significant negative correlation between colleague support and TI among nurses (r = −0.100, 95% CI: −0.143, −0.056, p < 0.001), as shown in Figure 4.
Figure 4
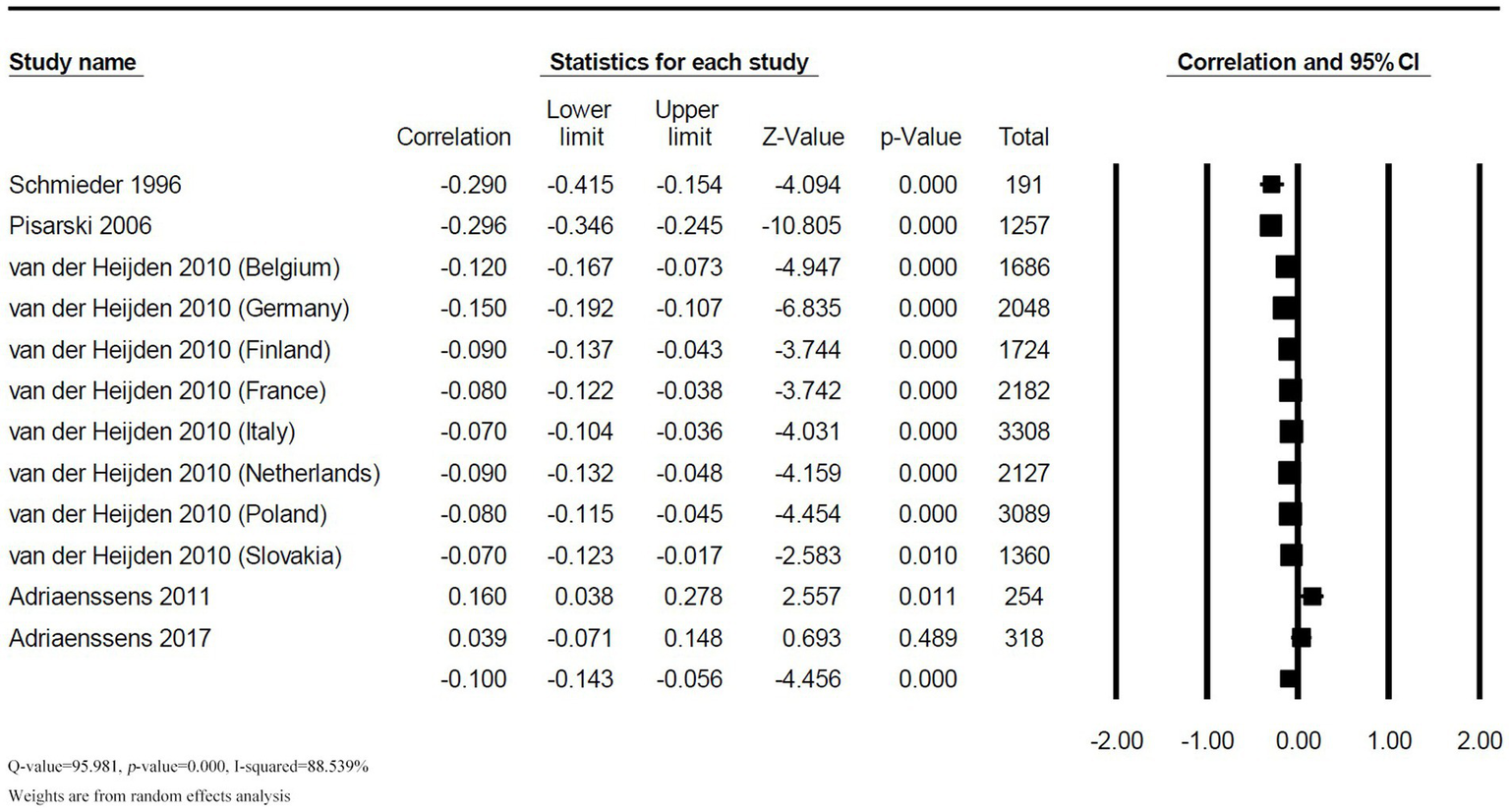
Forest plot of the correlation between colleague support and TI.
3.2.4 Publication bias and sensitivity analysis
This meta-analysis used funnel plot, Begg’s test, and Egger liner regression to evaluated the publication bias. The effect sizes of studies included in the meta-analysis were mostly distributed on the left side of the funnel plot, suggesting a high possibility of publication bias. The results of Begg test did not show publication bias (p = 0.988). However, the Egger liner regression results showed significant publication bias (t = 3.312, p = 0.002). When quantifying the potential effect of small study bias on overall effect size using the trim-and-fill method, 12 studies with missing hypotheses were added, with an estimated effect size of −0.195 (95% CI: −0.238, −0.152), indicating a significant negative correlation between social support and TI (Figure 5). Moreover, sensitivity analysis of one-by-one elimination showed a stable effect size between social support and TI. Therefore, it was suggested that the results drawn from the meta-analysis were reliable (Figure 6).
Figure 5
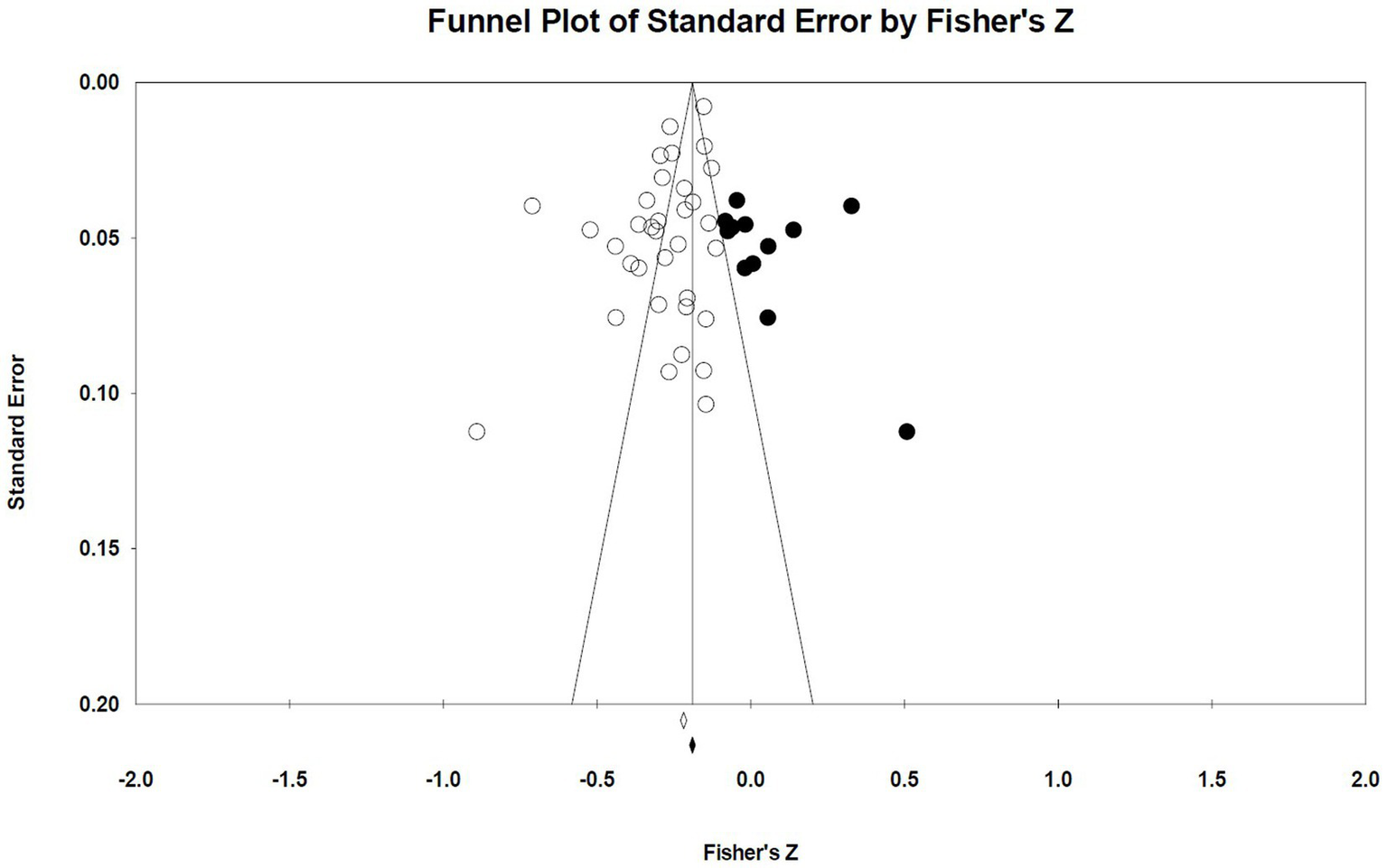
Funnel plot of the correlation between social support and TI.
Figure 6
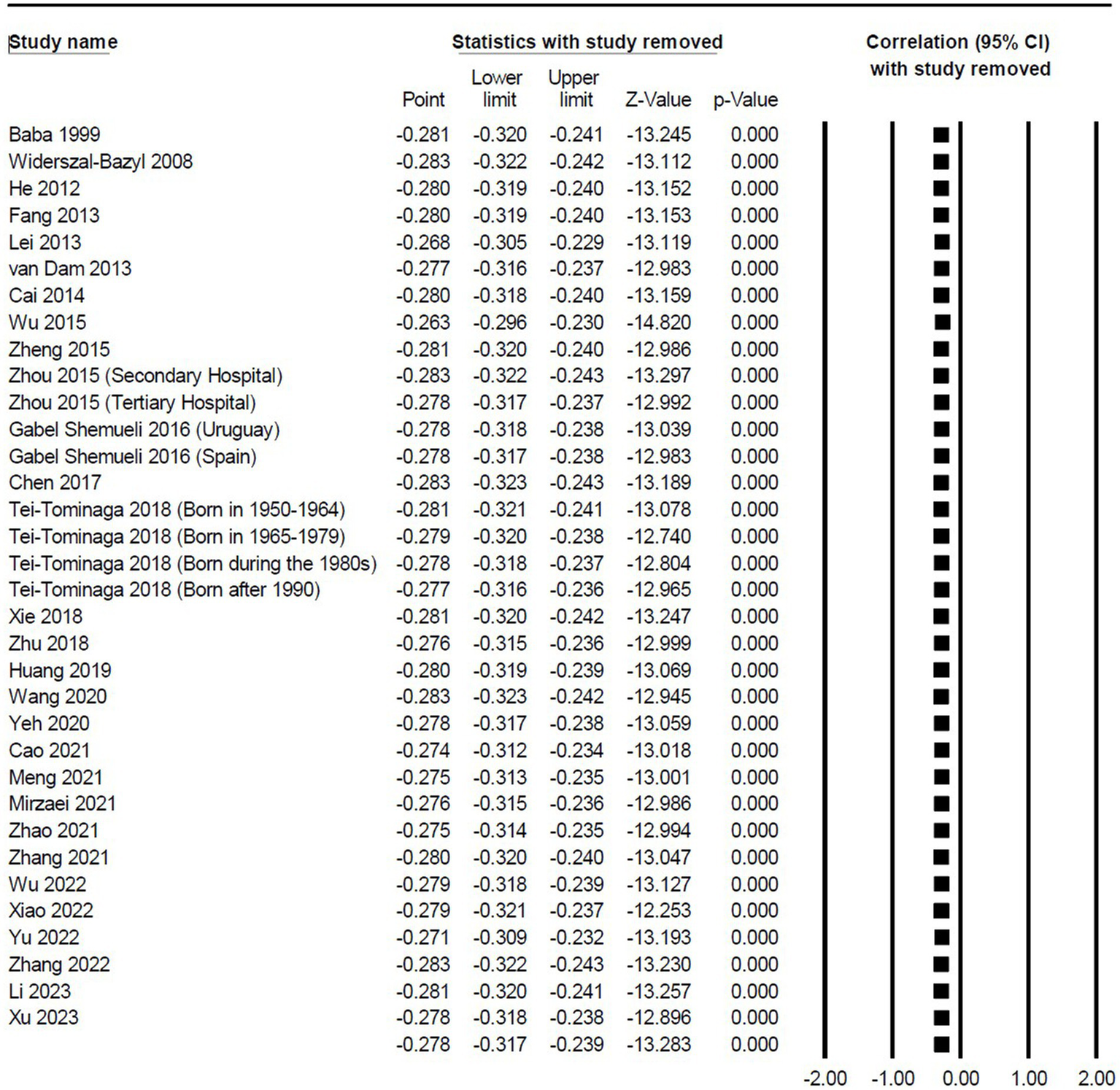
Sensitivity analysis of the correlation between social support and TI.
Meanwhile, the funnel plot of the correlation between supervisor support and TI, as well as the funnel plot of the correlation between colleague support and TI, showed asymmetry, indicating potential publication bias. After a correction for the potential effect of small study bias on overall effect size using the trim-and-fill method, 5 studies with missing hypotheses were added in the correlation between supervisor support and TI, with an estimated effect size of −0.199 (95% CI: −0.255, −0.141); 2 studies with missing hypotheses were added in the correlation between colleague support and TI, with an estimated effect size of −0.123 (95% CI: −0.167, −0.078). The adjusted funnel plots can be found in the Supplementary material 3.
3.3 Moderator analyses
This study used a meta-analysis of variance to test the moderating effects of six variables including nurse department, gender, sample size, data collection time, social support measurement tool, and TI measurement tool. The results showed that the sample size and TI measurement tool moderated the correlation between social support and TI (sample size: WQBET = 5.044, p = 0.025, TI measurement tool: WQBET = 70.714, p < 0.001). Specifically, compared to studies with a sample size >1,000, studies with a sample size ≤1,000 reported a stronger correlation between social support and TI (studies with a sample size >1,000: r = −0.213, 95% CI: −0.262, −0.162, p < 0.001; studies with a sample size ≤1,000: r = −0.299, 95% CI: −0.353, −0.242, p < 0.001). Regarding the TI measurement tool, studies used other measurement tools had the largest effect on social support and TI (r = −0.329, 95% CI: −0.380, −0.277, p < 0.001), while studies used the three-item questionnaire (1977) had the smallest effect on social support and TI (r = −0.150, 95% CI: −0.165, −0.135, p < 0.001). However, the correlation between social support and TI was not significantly moderated by nurse department, gender, data collection time, and social support measurement tool (p > 0.050) (Table 2).
Table 2
| Moderators | QBET | k | N | r | 95% CI | QW | I2 | |
|---|---|---|---|---|---|---|---|---|
| Nurse’s department | ||||||||
| Pediatric | 5.497 | 1 | 175 | −0.143 | −0.285 | 0.005 | 0 | 0% |
| Emergency nurse | 6 | 1,624 | −0.340 | −0.491 | −0.169 | 64.147 | 92.205% | |
| Operating theatre | 3 | 2,483 | −0.215 | −0.333 | −0.091 | 15.395 | 87.009% | |
| Intensive care | 1 | 461 | −0.310 | −0.390 | −0.225 | 0 | 0% | |
| Unreported or multiple departments | 23 | 34,325 | −0.278 | −0.322 | −0.232 | 324.797 | 93.227% | |
| Sex | ||||||||
| Female | 6.140 | 11 | 23,510 | −0.242 | −0.299 | −0.184 | 113.399 | 91.182% |
| Males | 1 | 177 | −0.411 | −0.527 | −0.281 | 0 | 0% | |
| Mixed | 19 | 14,516 | −0.295 | −0.354 | −0.234 | 238.060 | 92.439% | |
| No report | 3 | 865 | −0.254 | −0.329 | −0.177 | 2.779 | 28.044% | |
| Sample sizes | ||||||||
| ≤1,000 | 5.044* | 27 | 9,743 | −0.299 | −0.353 | −0.242 | 230.025 | 88.697% |
| >1,000 | 7 | 29,325 | −0.213 | −0.262 | −0.162 | 93.893 | 93.610% | |
| Data collection time | ||||||||
| During the COVID-19 pandemic | 1.725 | 7 | 7,424 | −0.325 | −0.394 | −0.252 | 40.001 | 85.000% |
| During the non-COVID-19 pandemic | 25 | 30,979 | −0.267 | −0.313 | −0.220 | 327.834 | 92.679% | |
| Unreported data collection time | 2 | 665 | −0.273 | −0.519 | 0.016 | 11.680 | 91.438% | |
| Social support measurement tools | ||||||||
| PSSS 1988 | 1.138 | 6 | 3,051 | −0.309 | −0.400 | −0.212 | 36.891 | 86.447% |
| SSRS 1986 | 13 | 11,673 | −0.290 | −0.372 | −0.205 | 230.716 | 94.799% | |
| Three-item | 4 | 5,064 | −0.262 | −0.308 | −0.214 | 9.062 | 66.896% | |
| Others | 11 | 19,280 | −0.257 | −0.318 | −0.194 | 64.305 | 84.449% | |
| TI measurement tools | ||||||||
| Three items questionnaire 1977 | 70.714*** | 2 | 16,171 | −0.150 | −0.165 | −0.135 | 0 | 0% |
| TIS 1991 | 2 | 818 | −0.282 | −0.344 | −0.218 | 0.091 | 0% | |
| TIQ 1982 | 15 | 12,854 | −0.266 | −0.338 | −0.190 | 233.284 | 93.999% | |
| Six-item | 4 | 5,064 | −0.262 | −0.308 | −0.214 | 9.062 | 66.896% | |
| Others | 11 | 4,161 | −0.329 | −0.380 | −0.277 | 32.064 | 68.812% | |
Social support and TI: univariate analysis of variance for moderator variables.
k, number of effect sizes; N, number of samples; QBET, between groups; QW, within groups; *p < 0.05, ***p < 0.001.
4 Discussion
To our knowledge, the current study is the first meta-analysis to quantitatively examine the correlation between social support and TI among nurses using correlation coefficients. The findings indicated that nurses’ perceived social support was moderately negatively correlated with TI, indicating that nurses with high perceived social support had low TI. This finding is consistent with the buffering hypothesis of social support, suggesting that social support as an effective resource can help nurses cope with work pressure, alleviate negative emotions, and reduce TI (18, 104). Given that the shortage of nursing staff is a prominent problem that is being experienced worldwide. Efforts should be made by nursing managers and researchers to understand and ameliorate the factors that lead to nurse turnover, thereby promoting nurse retention. The promotion of social support for nurses may be a measure worthy of attention.
4.1 The relationship between supervisor support, colleague support and TI
The current study also found that supervisor support and colleague support were negatively correlated with nurse TI. van der Heijden et al. (23) pointed out that working environment factors including social support from supervisors and colleagues could positively preventing nurses from leaving the nursing profession prematurely. Social support from supervisors could enhance the confidence of subordinates in career development (105) and contribute to building an intimate relationship between superiors and subordinates (90). Lack of job satisfaction is an important risk factor for nurse turnover, and a close superior-subordinate relationship is beneficial for organizational outcomes such as job satisfaction and happiness (106). According to the Conservation of Resources (COR) theory, social support from supervisors provides a variety of tangible and intangible resources to alleviate the turnover tendency caused by the job itself (95). Similarly, social support from colleagues was negatively correlated with nurse TI. Since nursing work requires high-quality teamwork and close colleague support (107), lack of support from colleagues can cause low-quality interpersonal relationships and eventually induce turnover behaviors (108). Moreover, compared with nurses who perceived low level of support from colleagues, nurses who perceived high level of support from colleagues were more likely to positively evaluate their team atmosphere and had a stronger sense of work identity (22). The support provided by close colleagues, including clinicians, is an important source of nurses’ perceived support. Therefore, it is crucial to facilitate effective communication and exchange between clinicians and nurses; establish a close team relationship; and ensure the work, information, and emotional support of clinicians for nurses can promote the retention of nurses.
4.2 Discussion of moderation effects
According to the results of the moderating effect analysis, the nursing department had no significant effect on the correlation between social support and TI, which might be related to the department distribution of the participants. In the current analysis, the vast majority of participants did not explicitly report their departments or they were involved in multiple departments, and merely a small number of studies focused on nurses in a single department (70). The number of participants may have affected the results of the analysis. Further research is necessary to effectively assess the impact of the nursing department on the correlation between social support and TI. Similarly, the moderating hypothesis about the gender of the sample was not supported. Previous studies reported that nurses of different genders did not show significant differences in perceived social support (109) and TI (24, 110). Additionally, only one study specifically focused on male nurses in the current included studies, and only four studies had more than 10% male participants. Therefore, the current study results still require further verification due to the insufficient male participants.
In this study, the moderating effect analysis of the study design found that sample size significantly affected the correlation between social support and nurse TI. Specifically, the correlation reported in studies with a sample size ≤1,000 was higher than that reported in studies with a sample size >1,000, which is consistent with the results of a previous meta-analysis (111). Existing evidence shows that there is a considerable correlation between the effect size and the sample size, that is, studies with a small sample size usually produce a larger effect size than those with a large sample size (112). The correlations between sample size and effect size can be interpreted as evidence for publication bias (112). The moderating effect test of data collection time unveiled that the data collection time had no moderating effect on the correlation between social support and TI, indicating that the correlation between social support and TI was not affected by the data collection time. Although the COVID-19 pandemic has increased the challenges and fears faced by nurses, the formation of TI is a complex, multi-stage process that starts with negative psychological responses to the current job (113, 114). As the pandemic progresses and more becomes known about the disease, nurses’ negative responses may also change. Additionally, ideological contracts may reduce the influence of fear on TI (115). Even in crisis situations, the protective effect of ideological motives remains (116).
The moderating effect analysis of the measurement tools showed that the social support measurement tools did not significantly moderate the correlation between social support and TI among nurses. The existing studies mainly rely on SSRS (1986) and PSSS (1988) to measure the social support. Although the two tools have different dimensions, their assessment contents are similar to a certain extent, such as support from family, friends, and colleagues. Given the diversity of social support measurement tools, the categorization of included studies may not fully reflect the impact of social support measurement tools on the correlation between social support and TI. In contrast, the current study found that TI measurement tools could moderate the correlation between social support and TI. Different measurement tools produce different correlation coefficients. In particular, the highest correlation coefficient was reported in other measurement tools, and the results of with TIS (1991) and TIQ (1982) were relatively close, while the lowest correlation coefficients were reported in three-item measurement questionnaires. There are significant differences in the content of the tools used to measure TI. For example, TIS (1991) (78), as a three-item scale, was more concise in content and may have stronger operability. As one of the most widely used tools for measuring TI, TIQ (1982) (69) assesses the likelihood of an individual quitting his current job, the motivation to seek other jobs, and the likelihood of obtaining other jobs, with a certain degree of stability. By comparison, the evaluation content of other one-dimensional measurement tools is limited. Therefore, among existing measurement tools, TIS (1991) may better reflect the association between social support and nurses’ TI. However, given the limited number of studies involving TIS (1991), more research is still needed to validate the current result.
4.3 Limitations and future research
Unlike previous studies that explore the correlation between social support and TI among nurses, the present study conducted a meta-analysis to investigate the correlation between overall social support, supervisor social support, colleague social support, and nurse TI, and further clarify the degree of correlation between variables. By synthesizing existing studies, this meta-analysis can provide more sufficient and stable evidence for implementing corresponding interventions to reduce the TI of nurses. Nevertheless, this study also has some limitations. Firstly, a few studies were published earlier in the included literature, which may not reflect the latest data on the association between social support and TI. The number of studies in some subgroups is relatively small. For instance, only one study targets ICU or pediatric nurses and the included studies mainly involve female participants, resulting in a lack of representativeness and typicality in some of our analysis results. Secondly, in terms of research types, as all included studies were cross-sectional studies, our meta-analysis only reveals the correlation between social support and TI, but fails to explain the causal relationship between the two variables. Future longitudinal study designs are warranted to elucidate the causal relationship between social support and TI among nurses. Finally, this meta-analysis only focuses on the impact of some moderators on the correlation between social support and TI among nurses. Further analysis is needed on other potential moderating variables, such as cultural background.
5 Conclusion
This meta-analysis indicates that social support plays a crucial role in predicting turnover intention among nurses. The institutional measures and working environment aimed at improving nurses’ perceived social support are conducive to reducing nurses’ turnover rates and ensuring the stability of the nursing team. This study’s results will help nursing administrators, hospitals, and policymakers develop corresponding strategies to maximize the perceived social support of nurses and reduce their turnover intention. Furthermore, colleague support, including mutual assistance and cooperation, is also crucial for nurse retention. Therefore, nursing managers should promote an organizational culture characterized by teamwork and integration.
Statements
Author contributions
YC: Conceptualization, Writing – original draft, Writing – review & editing. XZ: Software, Writing – review & editing. XB: Supervision, Writing – review & editing. BL: Methodology, Writing – original draft. FC: Data curation, Writing – original draft. LC: Validation, Writing – review & editing. HL: Conceptualization, Writing – original draft.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1393024/full#supplementary-material
References
1.
Back C-Y Hyun D-S Jeung D-Y Chang S-J . Mediating effects of burnout in the association between emotional labor and turnover intention in Korean clinical nurses. Saf Health Work KR. (2020) 11:88–96. doi: 10.1016/j.shaw.2020.01.002
2.
Sayegh N Gross K . Benign prostatic hyperplasia: a global challenge of the ageing population. Lancet Health Longev. (2022) 3:e725–6. doi: 10.1016/S2666-7568(22)00243-4
3.
Truth AU . No health without a workforce. World health Organisation (WHO) report (2013). Available at:https://www.researchgate.net/publication/270561476_A_Universal_Truth_No_Health_Without_a_Workforce
4.
Adams R Ryan T Wood E . Understanding the factors that affect retention within the mental health nursing workforce: a systematic review and thematic synthesis. Int J Ment Health Nu. (2021) 30:1476–97. doi: 10.1111/inm.12904
5.
Catton H . COVID-19: the future of nursing will determine the fate of our health services. Int Nurs Rev. (2021) 68:9–11. doi: 10.1111/inr.12673
6.
Cimiotti JP Aiken LH Sloane DM Wu ES . Nurse staffing, burnout, and health care–associated infection. Am J Infect Control. (2012) 40:486–90. doi: 10.1016/j.ajic.2012.02.029
7.
O'Brien-Pallas L Murphy GT Shamian J Li X Hayes LJ . Impact and determinants of nurse turnover: a pan-Canadian study. J Nurs Manage. (2010) 18:1073–86. doi: 10.1111/j.1365-2834.2010.01167.x
8.
Ma C McHugh MD Aiken LH . Organization of hospital nursing and 30-day readmissions in Medicare patients undergoing surgery. Med Care. (2015) 53:65. doi: 10.1097/MLR.0000000000000258
9.
Ball JE Bruyneel L Aiken LH Sermeus W Sloane DM Rafferty AM et al . Post-operative mortality, missed care and nurse staffing in nine countries: a cross-sectional study. Int J Nurs Stud. (2018) 78:10–5. doi: 10.1016/j.ijnurstu.2017.08.004
10.
Lu X Yang J Bai D Cai M Wang W He J et al . The effect of psychological contract on turnover intention among nurses: a meta-analytic review. BMC Nurs. (2023) 22:358. doi: 10.1186/s12912-023-01496-2
11.
Nevidion B Erickson J . The nursing shortage: solutions for the short and long term. (2001). Available at:http://www.nursingworld.org/ojin/topic14/tpe144.htm
12.
Lo WY Chien LY Hwang FM Huang N Chiou ST . From job stress to intention to leave among hospital nurses: a structural equation modelling approach. J Adv Nurs. (2018) 74:677–88. doi: 10.1111/jan.13481
13.
Chu X Zhang L Li M . Nurses' strengths use and turnover intention: the roles of job crafting and self-efficacy. J Adv Nurs. (2022) 78:2075–84. doi: 10.1111/jan.15124
14.
Namin BH Øgaard T Røislien J . Workplace incivility and turnover intention in organizations: a meta-analytic review. Int J Env Res Pub He. (2021) 19:25. doi: 10.3390/ijerph19010025
15.
Gilmartin MJ . Thirty years of nursing turnover research: looking back to move forward. Med Care Res Rev. (2013) 70:3–28. doi: 10.1177/1077558712449056
16.
Djupedal ILR Pallesen S Harris A Waage S Bjorvatn B Vedaa Ø . Changes in the work schedule of nurses related to the COVID-19 pandemic and its relationship with sleep and turnover intention. Int J Env Res Pub He. (2022) 19:8682. doi: 10.3390/ijerph19148682
17.
Degen C Li J Angerer P . Physicians’ intention to leave direct patient care: an integrative review. Hum Resour Health. (2015) 13:1–12. doi: 10.1186/s12960-015-0068-5
18.
Xiao S Shi L Lin H Zhao S Ou W Zhang J et al . The impact of psychological capital on turnover intention among Chinese nurses: a moderated mediation model. J Nurs Manage. (2022) 30:3031–40. doi: 10.1111/jonm.13702
19.
Xu J-B Zheng Q-X Jiang X-M Zhuo Q Nian J-X Wang J-T . Mediating effects of social support, mental health between stress overload, fatigue and turnover intention among operating theatre nurses. BMC Nurs. (2023) 22:364. doi: 10.1186/s12912-023-01518-z
20.
Langford CPH Bowsher J Maloney JP Lillis PP . Social support: a conceptual analysis. J Adv Nurs. (1997) 25:95–100. doi: 10.1046/j.1365-2648.1997.1997025095.x
21.
Shirey MR . Social support in the workplace: nurse leader implications. Nurs Econ. (2004) 22:313–9. PMID:
22.
Pisarski A Brook C Bohle P Gallois C Watson B Winch S . Extending a model of shift-work tolerance. Chronobiol Int. (2006) 23:1363–77. doi: 10.1080/07420520601055316
23.
van der Heijden B Kümmerling A van Dam K van der Schoot E Estryn-Béhar M Hasselhorn H . The impact of social support upon intention to leave among female nurses in Europe: secondary analysis of data from the NEXT survey. Int J Nurs Stud. (2010) 47:434–45. doi: 10.1016/j.ijnurstu.2009.10.004
24.
Labrague L Gloe D McEnroe D Konstantinos K Colet P . Factors influencing turnover intention among registered nurses in Samar Philippines. Appl Nurs Res. (2018) 39:200–6. doi: 10.1016/j.apnr.2017.11.027
25.
Lim J Bogossian F Ahern K . Stress and coping in Singaporean nurses: a literature review. Nurs Health Sci. (2010) 12:251–8. doi: 10.1111/j.1442-2018.2010.00514.x
26.
Aneshensel C Stone D . Stress and depression: a test of the buffering model of social support. Arch Gen Psychiat. (1982) 39:1392–6. doi: 10.1001/archpsyc.1982.04290120028005
27.
Lei WA He J Yao HY . The relationship between social support and turnover intention among emergency nurses emergency department. Chin Nurs Manage. (2013) 13:45–8. doi: 10.3969/j.issn.1672-1756.2013.07.015
28.
Yu H Gui L . Compassion fatigue, burnout and compassion satisfaction among emergency nurses: a path analysis. J Adv Nurs. (2022) 78:1294–304. doi: 10.1111/jan.15034
29.
Gülcan C. The relationship between burnout and turnover intention among nurses: The effect of psychological demands, decision authority, and social support on burnout and turnover intention. (Master's dissertation) eastern Mediterranean university (EMU). (2015).
30.
Adriaenssens HA Van Bogaert P . Predictors of occupational stress and well-being in first-line nurse managers: a cross-sectional survey study. Int J Nurs Stud. (2017) 73:85–92. doi: 10.1016/j.ijnurstu.2017.05.007
31.
Galletta M Portoghese I Penna MP Battistelli A Saiani L . Turnover intention among Italian nurses: the moderating roles of supervisor support and organizational support. Nurs Health Sci. (2011) 13:184–91. doi: 10.1111/j.1442-2018.2011.00596.x
32.
Ma CF Xing D Meng Q Zhang Y . Study on the associated factors of turnover intention among emergency nurses in China and the relationship between major factors. Int Emerg Nurs. (2022) 60:101106. doi: 10.1016/j.ienj.2021.101106
33.
Wu H Sun W Wang L . Factors associated with occupational stress among Chinese female emergency nurses. Emerg Med J. (2012) 29:554–558. doi: 10.1136/emj.2010.094391
34.
Hooper C Craig J Janvrin DR Wetsel MA Reimels E . Compassion satisfaction, burnout, and compassion fatigue among emergency nurses compared with nurses in other selected inpatient specialties. J Emerg Nurs. (2010) 36:420–7. doi: 10.1016/j.jen.2009.11.027
35.
Blomberg AC Lindwall L Bisholt B . Operating theatre nurses’ self-reported clinical competence in perioperative nursing: a mixed method study. Nurs Open. (2019) 6:1510–8. doi: 10.1002/nop2.352
36.
von Vogelsang AC Swenne CL Gustafsson BÅ Falk BK . Operating theatre nurse specialist competence to ensure patient safety in the operating theatre: a discursive paper. Nurs Open. (2020) 7:495–502. doi: 10.1002/nop2.424
37.
Chen H Li G Li M Lyu L Zhang T . A cross-sectional study on nurse turnover intention and influencing factors in Jiangsu Province, China. Inte J Nurs Sci. (2018) 5:396–402. doi: 10.1016/j.ijnss.2018.09.012
38.
Kim A-S Park S-J . Nursing environment, job stress, and turnover intention of pediatric ward nurses and general ward nurses. J Korea Contents Assoc. (2017) 17:124–32. doi: 10.5392/JKCA.2017.17.07.124
39.
Zhao Y Wang H Sun D Ma D Li H Li Y et al . Job satisfaction, resilience and social support in relation to nurses' turnover intention based on the theory of planned behaviour: a structural equation modelling approach. Int J Nurs Pract. (2021) 27:e12941. doi: 10.1111/ijn.12941
40.
Zhang J Zhang X Zhang K Lu X Yuan G Yang H et al . An updated of meta-analysis on the relationship between mobile phone addiction and sleep disorder. J Affect Disorders. (2022) 305:94–101. doi: 10.1016/j.jad.2022.02.008
41.
Schönbrodt FD Perugini M . At what sample size do correlations stabilize?J Res Pers. (2013) 47:609–12. doi: 10.1016/j.jrp.2013.05.009
42.
Widerszal-Bazyl M Radkiewicz P Hasselhorn H-M Maurice Conway P van der Heijden B Group NS . The demand-control-support model and intent to leave across six European countries: the role of employment opportunities. Work Stress. (2008) 22:166–84. doi: 10.1080/02678370801999750
43.
Mirzaei A Rezakhani Moghaddam H Habibi SA . Identifying the predictors of turnover intention based on psychosocial factors of nurses during the COVID-19 outbreak. Nurs Open. (2021) 8:3469–76. doi: 10.1002/nop2.896
44.
Falatah R . The impact of the coronavirus disease (COVID-19) pandemic on nurses’ turnover intention: an integrative review. Nurs Rep. (2021) 11:787–810. doi: 10.3390/nursrep11040075
45.
Tei-Tominaga M Asakura K Asakura T . Generation-common and-specific factors in intention to leave among female hospital nurses: a cross-sectional study using a large Japanese sample. Int J Env Res Pub He. (2018) 15:1591. doi: 10.3390/ijerph15081591
46.
Gabel Shemueli R Dolan SL Suárez Ceretti A Núñez del Prado P . Burnout and engagement as mediators in the relationship between work characteristics and turnover intentions across two Ibero-American nations. Stress Health. (2016) 32:597–606. doi: 10.1002/smi.2667
47.
Moher D Liberati A Tetzlaff J Altman G Prisma Group . Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg. (2010) 8:336–41. doi: 10.1016/j.ijsu.2010.02.007
48.
Munn Z Moola S Lisy K Riitano D Tufanaru C . Methodological guidance for systematic reviews of observational epidemiological studies reporting prevalence and cumulative incidence data. JBI Evid Implement. (2015) 13:147–53. doi: 10.1097/XEB.0000000000000054
49.
Gignac GE Szodorai ET . Effect size guidelines for individual differences researchers. Pers Indiv Differ. (2016) 102:74–8. doi: 10.1016/j.paid.2016.06.069
50.
Higgins JP Thompson SG Deeks JJ Altman DG . Measuring inconsistency in meta-analyses. BMJ. (2003) 327:557–60. doi: 10.1136/bmj.327.7414.557
51.
Borenstein M Hedges LV Higgins JT Rothstein HR . Effect sizes based on means. Introduction to meta-analysis. USA: John Wiley & Sons, Ltd. (2009).
52.
Begg CB Mazumdar M . Operating characteristics of a rank correlation test for publication bias. Biometrics. (1994) 50:1088–101. doi: 10.2307/2533446
53.
Egger M Smith GD Schneider M Minder C . Bias in meta-analysis detected by a simple, graphical test. BMJ. (1997) 315:629–34. doi: 10.1136/bmj.315.7109.629
54.
Schmieder RA Smith CS . Moderating effects of social support in shift working and non-shift working nurses. Work Stress. (1996) 10:128–40. doi: 10.1080/02678379608256792
55.
House JS Wells JA . Occupational stress, social support and health In: McLeanABlackGColliganM, editors. Reducing occupational stress: Proceedings of a conference. New York: DHEW (NIOSH) publication (1978). 78–140.
56.
Seashore SE Lawler EE Mirvis P Cammann C . Observing and Mcascrritig organization change: A guide to field practice. New York: Wiley (1982).
57.
Baba VV Galperin BL Lituchy TR . Occupational mental health: a study of work-related depression among nurses in the Caribbean. Int J Nurs Stud. (1999) 36:163–9. doi: 10.1016/S0020-7489(99)00002-4
58.
Mobley WH . Intermediate linkages in the relationship between job satisfaction and employee turnover. J Appl Psychol. (1977) 62:237–40. doi: 10.1037/0021-9010.62.2.237
59.
Caplan RD Cobb S French JR Harrison RV Pinneau SR . Job demands and worker health. Ann Arbor, Mich: The Institute of Social Research. The University of Michigan (1980).
60.
van der Heijden BM . The measurement and development of professional expertise throughout the career. A retrospective study among higher level Dutch professionals. (Doctoral dissertation) University of Twente. (1998).
61.
van Der Heijden BI . Organizational influences upon the development of professional expertise in SMES in the Netherlands. J Enterp Cult. (2002) 9:367–406. doi: 10.1142/S0218495801000201
62.
Adriaenssens J De Gucht V Van Der Doef M Maes S . Exploring the burden of emergency care: predictors of stress-health outcomes in emergency nurses. J Adv Nurs. (2011) 67:1317–28. doi: 10.1111/j.1365-2648.2010.05599.x
63.
Hom PW Griffeth RW Sellaro CL . The validity of Mobley's (1977) model of employee turnover. Organ Behav Hum Perform. (1984) 34:141–74. doi: 10.1016/0030-5073(84)90001-1
64.
He M Sun Y . Study on correlation between work-family conflict and turnover intention and social support of emergency nurses. Chin Nurs Res. (2012) 26:2986–9. doi: 10.3969/j.issn.1009-6493.2012.32.005
65.
Xiao SY . Theoretical basis and research application of the social support assessment scale. J Clin Psychiatry. (1994) 2:98–100.
66.
Brough P Frame R . Predicting police job satisfaction and turnover intentions: the role of social support and police organisational variables. New Zeal J Psychol. (2004) 33:8–18.
67.
Fang Y Wang L Zhang M . Correlations between Nurse's turnover intention and social support. Mil Nurs. (2013) 30:20–2. doi: 10.3969/j.issn.1008-9993.2013.04.006
68.
Zimet GD Dahlem NW Zimet SG Farley GK . The multidimensional scale of perceived social support. J Pers Assess. (1988) 52:30–41. doi: 10.1207/s15327752jpa5201_2
69.
Michaels CE Spector PE . Causes of employee turnover: a test of the Mobley, Griffeth, hand, and Meglino model. J Appl Psychol. (1982) 67:53–9. doi: 10.1037/0021-9010.67.1.53
70.
van Dam K Meewis M van der Heijden BI . Securing intensive care: towards a better understanding of intensive care nurses’ perceived work pressure and turnover intention. J Adv Nurs. (2013) 69:31–40. doi: 10.1111/j.1365-2648.2012.05981.x
71.
van Veldhoven M Broersen JJ Fortuin RJ Handleiding V. SKB Vragenlijst services, Amsterdam. Warr P . Age and work behavior: physical attributes, cognitive abilities, knowledge, personality traits and motives. Int Rev Ind Organ Psychol. (2001) 2002:1–36.
72.
van Dam K . Time frames for leaving: an explorative study of employees' intentions to leave the organization in the future. Career Dev Int. (2008) 13:560–71. doi: 10.1108/13620430810901697
73.
Cai LZ Li YM Luo H Lu J Ning L . Analysis on correlation between new nurses' turnover intension and social support, anxiety level. J Nurs Rehabil. (2014) 13:645–8. doi: 10.3969/j.issn.1671-9875.2014.07.009
74.
Wu D Zhang M Yan L Li J Wu DQ Wei ZZ et al . Current status and influence factors of turnover intention of nurses in a third-level first-class Hospital in Anhui Province. J Nurs. (2015) 22:37–41. doi: 10.16460/j.issn1008-9969.2015.24.037
75.
Zheng QX Han W Zhu Y Yang FT Wu SP Chen CY . Study on the correlation between nurses' turnover intention and social support and countermeasures. J Tradit Chin Med. (2015) 23:61–3. doi: 10.16690/j.cnki.1007-9203.2015.13.038
76.
Zhou F Wang D . Correlation of emergency nurses’ demission intention and social support in hospitals of different levels. J Nurs Admin. (2015) 15:611–4.
77.
Dolan SL van Amerigaen MR Arsenault A . The role personality and social support in the etiology of workers’ stress and psychological strain. Ind Relat. (1992) 47:1.
78.
Arsenault A Dolan SL Van Ameringen MR . Stress and mental strain in hospital work: exploring the relationship beyond personality. J Organ Behav. (1991) 12:483–93. doi: 10.1002/job.4030120603
79.
Chen MY Zhu S Li LZ . Factors analysis of the turnover intention of operating room specialist nurses in Hunan Province and its influencing factors. Mil Nurs. (2017) 34:8–12. doi: 10.3969/j.issn.1008-9993.2017.11.002
80.
Xie JH Zhu LH Deng FL Liu X Xiong H Zhang Q et al . A correlation study on the turnover intention, job satisfaction, and social support characteristics of pediatric specialty nurses. J Clin Res. (2018) 35:4. doi: 10.3969/j.issn.1671-7171.2018.10.020
81.
Zhu DM Qin W . Relationship between turnover intention, job burnout and social support of Contract nurses in a 3A grade Hospital in Shanghai. Chin J Health Psychol. (2018) 26:909–12. doi: 10.13342/j.cnki.cjhp.2018.06.031
82.
Zhang L. A study on effect of organizational career management, perceived organizational support on turnover intension of knowledge employee. (Master's dissertation) Xiamen University. (2009).
83.
Huang CC Lin SH Zheng KW . The relationship among emotional intelligence, social support, job involvement, and turnover intention–a study of nurses in Taiwan. J Econ Bus. (2019) 2:652–659. doi: 10.31014/aior.1992.02.03.116
84.
Richard OC Johnson NB . Strategic human resource management effectiveness and firm performance. Int J Hum Resour Man. (2001) 12:299–310. doi: 10.1080/09585190121674
85.
Wang HC Zhao JX Wang YX Ayijiamali SL He GP . Mediating effects of psychological capital between social support and turnover intention in nurses of Class II grade a hospitals in Ürümqi. Chin J Mod Nurs. (2020) 26:1–5. doi: 10.3760/cma.j.cn115682-20190916-03352
86.
Yeh TF Chang YC Feng WH Yang CC . Effect of workplace violence on turnover intention: the mediating roles of job control, psychological demands, and social support. INQUIRY J Health Car. (2020) 57:0046958020969313. doi: 10.1177/0046958020969313
87.
Cheng Y Luh WM Guo YL . Reliability and validity of the Chinese version of the job content questionnaire in Taiwanese workers. Int J Behav Med. (2003) 10:15–30. doi: 10.1207/S15327558IJBM1001_02
88.
Cao X Li J Gong S . Effects of resilience, social support, and work environment on turnover intention in newly graduated nurses: the mediating role of transition shock. J Nurs Manage. (2021) 29:2585–93. doi: 10.1111/jonm.13418
89.
Lee G Lee D . A study on the relationships among role conflict, organizational commitment and intent to quit matrix organizational structure: Using employees from industrial technology research institute as example. Taiwan: Graduate School of management, National Chiao Tung University (2000).
90.
Cole A Ali H Ahmed A Hamasha M Jordan S . Identifying patterns of turnover intention among Alabama frontline nurses in hospital settings during the COVID-19 pandemic. J Multidiscip Health. (2021) 14:1783–94. doi: 10.2147/JMDH.S308397
91.
Hognestad Haaland G Olsen E Mikkelsen A . The association between supervisor support and ethical dilemmas on Nurses' intention to leave: the mediating role of the meaning of work. J Nurs Manage. (2021) 29:286–93. doi: 10.1111/jonm.13153
92.
Meng Q Jia YZ Xue Y Leng LY Zhang LC . Investigation and correlation study on occupational identity and resignation intention of male nurses in Weifang. Chin J Convalescent Med. (2021) 30:789–97. doi: 10.13517/j.cnki.ccm.2021.08.002
93.
Liu L Hao YF Liu XH . Development of professional identity scale for nurses. Mil Nurs. (2011) 28:18–20.
94.
Kim TY Leung K . Forming and reacting to overall fairness: a cross-cultural comparison. Organ Behav Hum Dec. (2007) 104:83–95. doi: 10.1016/j.obhdp.2007.01.004
95.
Modaresnezhad M Andrews MC Mesmer-Magnus J Viswesvaran C Deshpande S . Anxiety, job satisfaction, supervisor support and turnover intentions of mid-career nurses: a structural equation model analysis. J Nurs Manage. (2021) 29:931–42. doi: 10.1111/jonm.13229
96.
Finley AP Mueller CW Gurney CA . Organizational and professional commitment in professional and non-professional organizations: the case of nurse doctorates. Res Soc Strat Mobil. (2004) 20:325–58. doi: 10.1016/S0276-5624(03)20008-1
97.
Price JL . Reflections on the determinants of voluntary turnover. Int J Manpow. (2001) 22:600–24. doi: 10.1108/EUM0000000006233
98.
Zhang YA Zhang XN Xu N Yun E . Nurses’ turnover intention in secondary hospitals in China: a structural equation modelling approach. J Nurs Manage. (2021) 29:2216–24. doi: 10.1111/jonm.13379
99.
Wu L Wu XF Fang YR Wang HZ . A survey on social support degree and turnover intention of operating room nurses in a general hospital. Ind Health Occup Dis. (2022) 48:388–91. doi: 10.13692/j.cnki.gywsyzyb.2022.05.011
100.
Liu JW Li FY Lian YL . Investigation of reliability and validity of the social support scale. J Xinjiang Med Univ. (2008) 1:1–3.
101.
Cole MS Bruch H . Organizational identity strength, identification, and commitment and their relationships to turnover intention: does organizational hierarchy matter?J Organ Behav. (2006) 27:585–605. doi: 10.1002/job.378
102.
Li X . The mediating effect of psychological capital of emergency nurses on social support and turnover intention. Mod Nurs. (2023) 30:108–11. doi: 10.19793/j.cnki.1006-6411.2023.30.025
103.
Lee YW Dai YT McCreary LL . Quality of work life as a predictor of nurses' intention to leave units, organisations and the profession. J Nurs Manage. (2015) 23:521–31. doi: 10.1111/jonm.12166
104.
Cohen S Wills TA . Stress, social support, and the buffering hypothesis. Psychol Bull. (1985) 98:310–57. doi: 10.1037/0033-2909.98.2.310
105.
Bratton JA Gold J . Human resource management: theory and practice. London: Palgrave Macmillan. (1999).
106.
Gerstner CR Day DV . Meta-analytic review of leader–member exchange theory: correlates and construct issues. J Appl Psychol. (1997) 82:827–44. doi: 10.1037/0021-9010.82.6.827
107.
van Der Heijden BI Demerouti E Bakker AB NEXT Study Group coordinated by Hans-Martin Hasselhorn . Work-home interference among nurses: reciprocal relationships with job demands and health. J Adv Nurs. (2008) 62:572–84. doi: 10.1111/j.1365-2648.2008.04630.x
108.
Uhl-Bein M Graen GB Scandura TA . Implications of leader-member exchange (LMX) for strategic human resource management systems: relationships as social capital for competitive advantage. Res Pers Hum Resour Manage. (2000) 18:137–85. doi: 10.2307/1239142
109.
Park M-S Oh C-U Han H-S . Influences of the workplace bullying and social support on turnover intension of nurse. J Korea Acad Ind Coop Soc. (2018) 19:166–73. doi: 10.5762/KAIS.2018.19.9.166
110.
Sokhanvar M Kakemam E Chegini Z Sarbakhsh P . Hospital nurses' job security and turnover intention and factors contributing to their turnover intention: a cross-sectional study. Nurs Midwifery Stud. (2018) 7:133–40. doi: 10.4103/nms.nms_2_17
111.
Huang H Wan X Liang Y Zhang Y Peng Q Ding Y et al . Correlations between social support and loneliness, self-esteem, and resilience among left-behind children in mainland China: a meta-analysis. Front Psych. (2022) 13:874905. doi: 10.3389/fpsyt.2022.874905
112.
Kühberger A Fritz A Scherndl T . Publication bias in psychology: a diagnosis based on the correlation between effect size and sample size. PLoS One. (2014) 9:e105825. doi: 10.1371/journal.pone.0105825
113.
Takase M . A concept analysis of turnover intention: implications for nursing management. Collegian. (2010) 17:3–12. doi: 10.1016/j.colegn.2009.05.001
114.
Tolksdorf KH Tischler U Heinrichs K . Correlates of turnover intention among nursing staff in the COVID-19 pandemic: a systematic review. BMC Nurs. (2022) 21:174. doi: 10.1186/s12912-022-00949-4
115.
Irshad M Khattak SA Hassan MM Majeed M Bashir S . How perceived threat of covid-19 causes turnover intention among Pakistani nurses: a moderation and mediation analysis. Int J Ment Health Nurs. (2020) 30:350. doi: 10.1111/inm.12775
116.
Kim SS Shin D Vough HC Hewlin PF Vandenberghe C . How do callings relate to job performance? The role of organizational commitment and ideological contract fulfillment. Hum Relat. (2018) 71:1319–47. doi: 10.1177/0018726717743310
Summary
Keywords
nurses, social support, turnover intention (TI), meta-analysis, moderators
Citation
Chen Y, Zhou X, Bai X, Liu B, Chen F, Chang L and Liu H (2024) A systematic review and meta-analysis of the effectiveness of social support on turnover intention in clinical nurses. Front. Public Health 12:1393024. doi: 10.3389/fpubh.2024.1393024
Received
28 February 2024
Accepted
17 May 2024
Published
06 June 2024
Volume
12 - 2024
Edited by
Shay-Lee Bolton, University of Manitoba, Canada
Reviewed by
Jacopo Fiorini, Policlinico Tor Vergata, Italy
Robert Yockey, University of North Texas Health Science Center, United States
Updates
Copyright
© 2024 Chen, Zhou, Bai, Liu, Chen, Chang and Liu.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xue Bai, sdslicubx@163.com
†These authors have contributed equally to this work
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.