 Catharina Sarkkola1,2
Catharina Sarkkola1,2 Marja H. Leppänen1,3,4Aino-Maija Eloranta4,5,6Laura Räisänen1,7,8Satu Männistö9
Marja H. Leppänen1,3,4Aino-Maija Eloranta4,5,6Laura Räisänen1,7,8Satu Männistö9 Heli Viljakainen1,3*
Heli Viljakainen1,3*- 1Folkhälsan Research Center, Helsinki, Finland
- 2Department of Public Health, Faculty of Medicine, University of Helsinki, Helsinki, Finland
- 3Faculty of Medicine, University of Helsinki, Helsinki, Finland
- 4Institute of Biomedicine, School of Medicine, University of Eastern Finland, Kuopio, Finland
- 5Institute of Public Health and Clinical Nutrition, University of Eastern Finland, Kuopio, Finland
- 6Department of Medicine, Endocrinology and Clinical Nutrition, Kuopio University Hospital, Kuopio, Finland
- 7Faculty of Medicine and Health Technology (MET), Tampere University, Tampere, Finland
- 8Department of Pediatrics, Tampere University Hospital, Tampere, Finland
- 9Finnish Institute for Health and Welfare (THL), Helsinki, Finland
Background: Children’s eating behaviors, including a tendency towards overeating, are strongly influenced by the family. Children prone to overeating are at a high risk of excessive weight gain, which can lead to further adverse health outcomes. Therefore, identifying factors that contribute to overeating is crucial for promoting healthy weight development. Given the inconsistencies in previous research, mostly involving young children, we investigated the child and parental characteristics associated with overeating in preadolescence.
Methods: The cross-sectional study included 5,973 preadolescents aged 9–12 years from the Finnish Health in Teens (Fin-HIT) cohort. A tendency towards overeating was based on a parent-reported question. We utilized extensive parent questionnaire and Medical Birth Register data, and used ordinal and stepwise logistic regression to identify the independent determinants of overeating.
Results: The proportion of preadolescents with a parent-reported tendency towards overeating was 10% (n = 606). In the multivariable model, boys had higher odds of overeating (OR 1.30, 95% CI 1.06–1.58) compared with girls. Preadolescents with overweight and obesity had 9- and 30-fold odds (95% CI 7.31–11.29 and 20.07–44.54, respectively) of overeating compared with healthy-weight preadolescents. Furthermore, parental depression and emotional feeding increased the odds of overeating in the preadolescent (OR 1.48, 95% CI 1.08–2.02 and OR 1.27, 95% CI 1.03–1.57).
Conclusion: Along with child weight status and sex, parental depression and emotional feeding were independently associated with overeating in preadolescence. Therefore, it is important to support parents’ mental health and their healthy feeding practices. Our findings can be targeted to manage overeating and prevent overweight in children and adolescents.
1 Introduction
Children’s eating behavior is influenced by genetics, environmental factors, and neural mechanisms (1, 2). Particularly the family plays a crucial role in shaping eating behaviors during childhood (3). Overeating, i.e., consuming food beyond nutritional needs increases the risk of excessive weight gain in children and has become a topical concern (4). This behavior may result from low satiety responsiveness (SR), which indicates poor regulation of food intake based on feelings of fullness, high food responsiveness (FR), characterized by eating in response to food cues, or a combination of both (5, 6). Other closely related dimensions include emotional overeating (EOE) and external eating, i.e., eating in response to external cues rather than internal hunger cues. Parental questionnaires are often used to assess these eating behaviors in children.
There is limited knowledge on the frequency of overeating among children. In a Portuguese study involving 6–18-year-olds, 24% were considered overeaters (7). The evidence on factors associated with overeating and its different aspects in children is inconsistent. For example, some studies link early-life factors like breastfeeding to better eating control (high SR, low SR or low EOE) later in childhood (8–10), while others found no such associations (11–15). Being born preterm has been linked to SR but not to other aspects of overeating in preadolescence (8, 16).
Similarly, results on family factors such as parental education, body mass index (BMI), depression, and presence of siblings are contradictory, with studies showing varied outcomes depending on the child’s age and study methodology (8, 11, 16–21). Only one study showed a link between maternal depressive symptoms and child overeating (21). Parental feeding practices may either foster or undermine children’s ability to self-regulate their eating (22). These practices include emotional feeding (using food to calm or cheer up the child) and using food as a reward (23). Some (24, 25) studies demonstrate a link between parental emotional feeding and aspects of overeating, but not all (26). In a clinical study of preadolescents living with overweight, maternal emotional feeding was the key predictor of child emotional eating (27). In addition, several parenting factors, such as low maternal support, but high psychological and behavioral control (28), as well as non-authoritative and emotionally non-responsive parenting (29) have been linked to child emotional eating. Associations regarding food as a reward have also been reported, although the results have not been confirmed for all aspects of overeating in longitudinal study settings (24, 30–33).
Previous studies have identified several early-life and family characteristics that may contribute to overeating in children. However, only a few studies have assessed these factors simultaneously to investigate their hierarchy and independent associations. Most studies have focused on children under school age, leaving a gap in research on preadolescents approaching or experiencing puberty—a unique developmental stage characterized by rapid physical growth, hormonal changes, and emotional shifts that can influence eating behaviors. Our study aimed to determine the prevalence of a parent-reported tendency towards overeating (hereafter, simply ‘overeating’) in Finnish 9–12-year-old preadolescents, and to investigate the associated child and parental characteristics.
2 Materials and methods
2.1 Study population
The study included participants from the prospective Finnish Health in Teens cohort (Fin-HIT), a school-based study conducted in 2011–2014 (34). This study consists of 11,407 preadolescent children aged 9–12 years and their 6,046 parents, 87% of them mothers, from Finland’s largest cities and their surrounding areas. In this cross-sectional study, we used a subsample of 5,973 preadolescents with available parental-reported data on overeating. The preadolescents’ mean age, sex distribution, prevalence of overweight and obesity, and maternal socioeconomic status (SES) in the subsample were consistent with those of the entire cohort (Supplementary Table 1). Seventy-nine percent of the preadolescents in the subsample participated at their schools, the rest from home. The participants from school and home recruitment had similar characteristics (Supplementary Table 1) and were therefore analyzed together. No one in the cohort has been diagnosed with any rare syndrome (Cushing, Prader-Willi, Bardet-Biedl, Alström) that may influence BMI, according to data from the national Register of Primary Health Care visits (35).
This study was conducted according to the guidelines in the Declaration of Helsinki, and all procedures were approved by the Coordinating Ethics Committee of the Hospital District of Helsinki and Uusimaa (169/13/03/00/10; August 10, 2010). Written informed consent was obtained from the children and one parent per child.
2.2 Overeating
One of the parents filled in a questionnaire, mostly online. Overeating was assessed with a question based on The Avon Longitudinal Study of Parents and Children (ALSPAC, UK) questionnaire at 10.5 years (36). The question was: Do you agree or disagree with this statement: ‘If I did not guide or regulate my child’s eating, s/he would eat too much.’ Answers were scored on a five-point Likert scale: agree, slightly agree, neither agree nor disagree, slightly disagree, disagree. The two first and two last response options were combined for the analyses composing three overeating categories (groups): overeating, possible overeating, no overeating.
2.3 Child determinants
The parent reported whether the child had two homes or families, siblings living in the main home, or food allergies. Trained fieldworkers measured the preadolescents’ height and weight at school. The preadolescents participating at home provided self-reported measures with an adult’s assistance, which have proven to be accurate for epidemiological studies (37). BMI was calculated (kg/m2) and the preadolescents were classified with thinness, healthy weight, overweight or obesity according to the International Obesity Task Force age-and sex-specific cutoffs (38).
Data from birth and early childhood were also included. Information on gestational age at birth was obtained from the Medical Birth Register maintained by the Finnish Institute for Health and Welfare (39). Gestational age was classified as preterm (<37 weeks), full-term (37 + 0–42 + 0 weeks) and post-term (>42 + 0 weeks). Since the development of oral feeding skills has been reported to be delayed among early preterm infants (40), additional analyses for this subgroup were performed using the cutoff <34 weeks (41). In addition, the parent reported whether the child received breastmilk, infant formula or both during the first 6 months of her/his life, and the child’s age when breastfeeding was stopped. Breastfeeding duration was categorized into <1 month, 1–5 months, 6–11 months and ≥12 months based on Finnish breastfeeding recommendations at the time when the children were born (42, 43). Lastly, the parent was also asked about the age at which the child entered daycare.
2.4 Parental determinants
Maternal SES at the time of the child’s birth was obtained from the Medical Birth Register and used as a five-class variable (upper-level employees, lower-level employees, manual workers, students and others) as previously reported (44). This register includes information only about the mother giving birth, not the father. The parent (either the mother or father) reported her/his own current height and weight in the questionnaire. BMI was calculated and categorized as thinness (<18.5 kg/m2), healthy weight (18.5–24.9 kg/m2), overweight (25.0─29.9 kg/m2) and obesity (≥30.0 kg/m2). The parent also reported whether s/he had been diagnosed or treated for depression or exhaustion/burnout at any time, and whether s/he had experienced an eating disorder, such as anorexia nervosa, bulimia nervosa, or an atypical eating disorder.
The questions on current parental feeding practices included emotional feeding (‘I cheer her/him up with something to eat if s/he is sad or upset’ with the answer scale always, sometimes, never, not applicable) and food as a reward (‘It is OK to offer sweets as a reward for good behavior,’ scored with the five-point Likert scale from ‘agree’ to ‘disagree’). In the analyses, the categories always and sometimes were combined. For the item ‘food as reward’, the first two and the last two categories were combined to create a three-class variable: yes, no opinion, and no. These two question items were adopted from the ALSPAC Study (36).
2.5 Statistical analyses
The child and parental characteristics were compared between the three overeating categories (overeating, possible overeating, no overeating) with the χ2 test for categorical variables and ANOVA for continuous variables. The unadjusted associations of each determinant with overeating were tested with ordinal logistic regression, resulting in odds ratios (OR) with 95% confidence intervals (CI) for overeating in comparison to the reference categories. All statistically significant (p < 0.05) determinants were selected for the stepwise multinomial logistic regression analysis, to define their hierarchy and independent associations with overeating. All these determinants were added in the multivariable model concurrently as stepwise terms with forward entry. The associations were presented with ORs. The third category (no overeating) was used as a reference. There was no interaction by sex between any of the determinants and overeating, so girls and boys were analyzed together. We also tested whether participation at home versus school modified the association between child BMI category and overeating, but we found no proof for interaction. All statistical analyses were performed using the software package IBM SPSS Statistics version 24.0.
2.6 Sensitivity analysis
For the sensitivity analysis we considered medications likely having side effects on appetite and/or BMI, i.e., Methylphenidate, Prednisolone, Mirtazapine, Aripiprazole, Risperidone, Chlorpromazine, Olanzapine, Quetiapine, and other antipsychotics, if the medication was ongoing or was estimated to have been finished within 1 month prior to participation. In addition, Thyroxine purchases within 4 months after participation were considered a proxy for latent hypothyroidism. Data on drug purchases were collected from the national Drug Purchase Register, maintained by the Finnish Social Insurance Institution. We also used information on the child’s possible eating disorder, i.e., anorexia nervosa, bulimia nervosa, or an atypical eating disorder, which was obtained from the parents’ questionnaire.
The sensitivity analysis was conducted in a subset of 5,789 participants, after excluding preadolescents with medication (n = 154), eating disorder (n = 28), or their combinations (n = 2). Since the determinants of overeating were the same in the subsample and the whole sample, we used the whole sample of 5,973 preadolescents throughout the analyses.
3 Results
3.1 Participant characteristics
In the study population of 5,973 preadolescents, 51% were girls (Table 1). The mean age was 11.2 years (standard deviation [SD] 0.8), and 12.1 and 2.4% of the preadolescents were living with overweight and obesity, respectively. The proportion of preadolescents with overeating was 10.1% (n = 606), of which 56% were boys. Overweight and obesity were more common within the overeating group than in the possible overeating or no overeating groups. One-third of the preadolescents had a mother with high SES (Table 2), while maternal SES did not differ between the overeating groups. Of the parents, 41% presented as living with overweight or obesity, and this was more common in the overeating group.
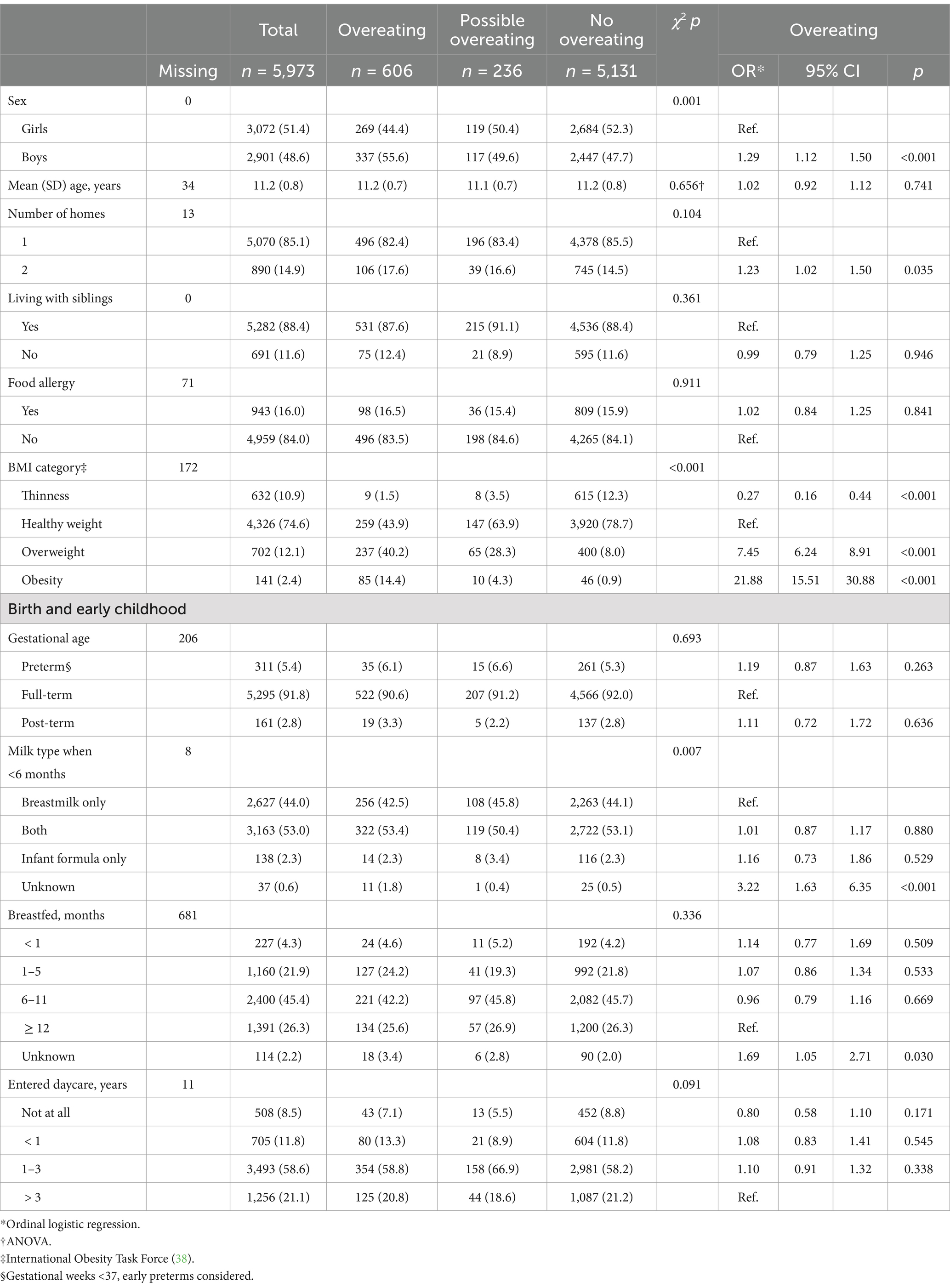
Table 1. Child characteristics for the total sample and overeating categories are reported as n (%), unless noted otherwise, along with their associations with overeating in the unadjusted model.
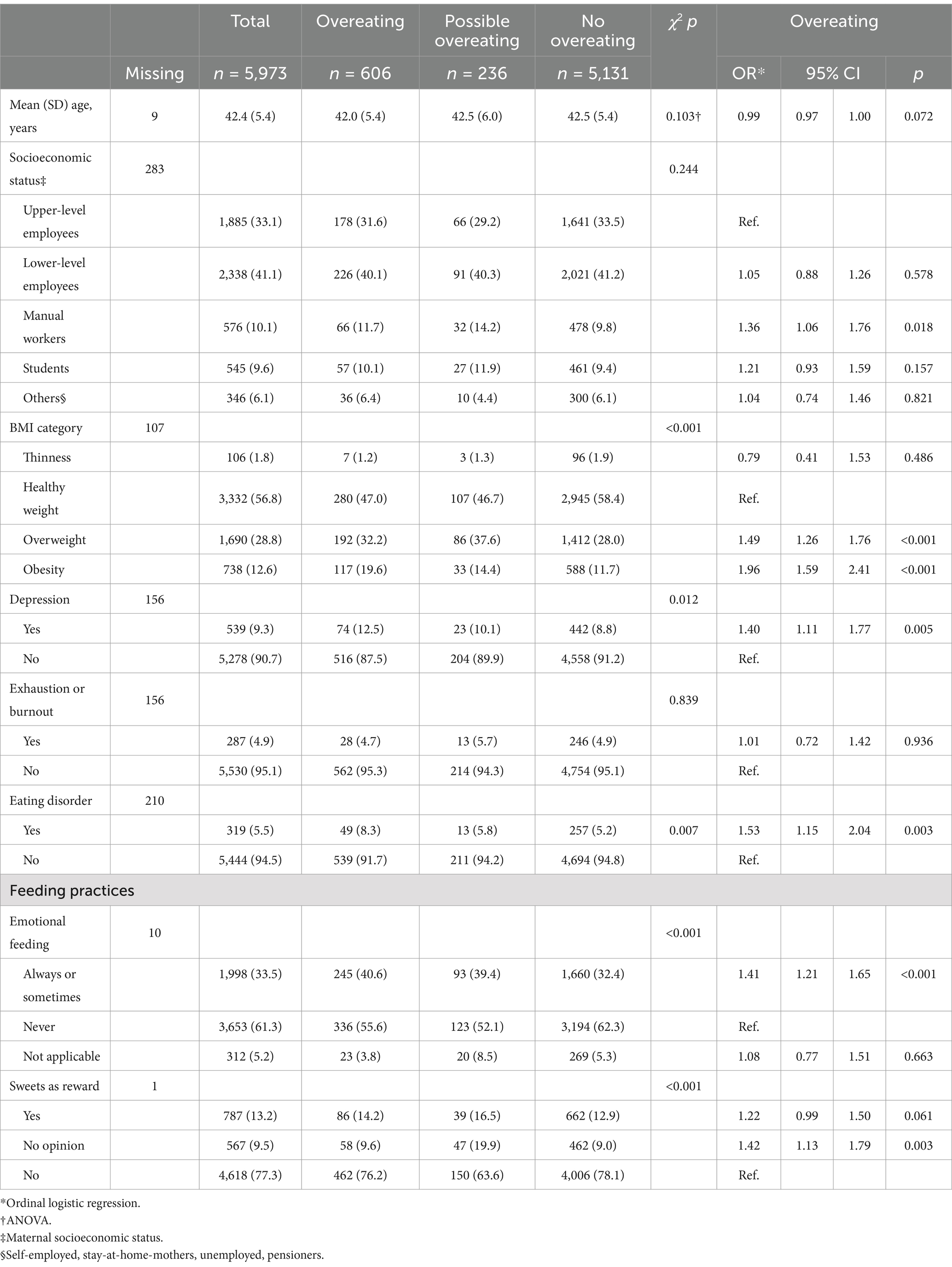
Table 2. Parental characteristics for the total sample and overeating categories are reported as n (%), unless noted otherwise, along with their associations with overeating in the unadjusted model.
3.2 Determinants of overeating
In the unadjusted model, being a boy, having two homes or families, and living with overweight or obesity were associated with overeating (Table 1). Having a parent with lower SES, overweight or obesity, depression or eating disorder were also linked to overeating (Table 2). Additionally, having a parent either practicing emotional feeding or with a liberal attitude toward sweets as a reward had higher odds of overeating compared with those whose parents were against emotional feeding and sweets as a reward.
In the stepwise multivariable model, boys had higher odds of overeating (OR 1.30, 95% CI 1.06–1.58) than girls (Figure 1). Preadolescents living with overweight and obesity had 9- and 30-fold odds (95% CI 7.31–11.29 and 20.07–44.54, respectively) of overeating, compared with preadolescents with healthy weight. Parental history of depression increased the odds of overeating in the preadolescent (OR 1.48, 95% CI 1.08–2.02). Preadolescents whose parents practiced emotional feeding had higher odds of overeating than preadolescents whose parents did not engage in such practices (OR 1.27, 95% CI 1.03–1.57).
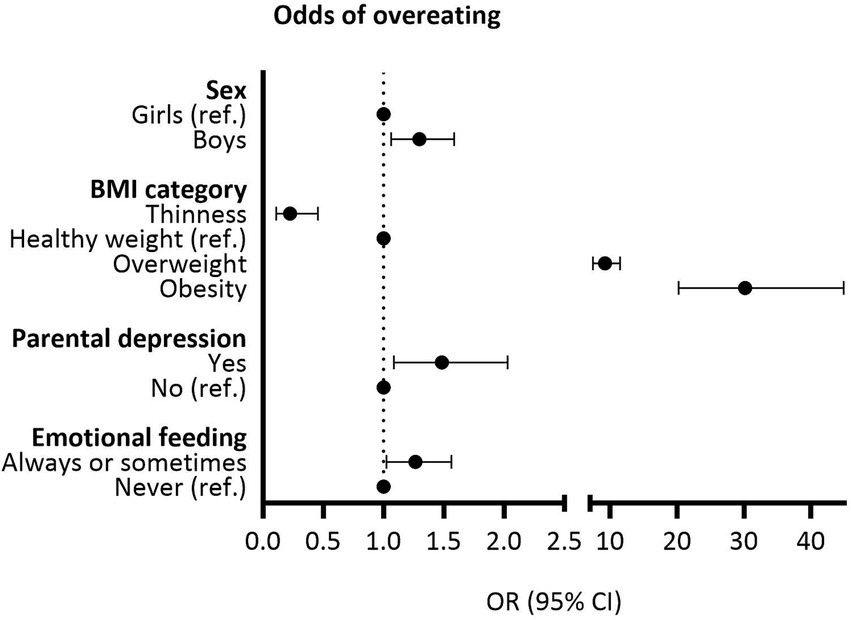
Figure 1. Statistically significant associations (p < 0.05) with overeating in the stepwise multivariable model.
4 Discussion
We simultaneously evaluated various early-life and family determinants of a parent-reported tendency towards overeating in a large cohort of Finnish preadolescents. This is the first study to investigate these relationships, and it fulfils the gap of knowledge concerning eating behaviors in preadolescents. There is sparse data on the frequency of overeating among children and adolescents. In our sample, overeating was reported in 10%, which is less than in a Portuguese study with 6─18-year-olds (24%) (7).
Overeating was strongly linked to preadolescent’s overweight and obesity in this study, consistent with previous reports (5, 45). Overeating and its various aspects are considered mediating factors for overweight and obesity (5). For example, low SR is likely to contribute to higher energy intake and it is also one of the mechanisms through which genetic predisposition leads to weight gain (46, 47). In fact, determinants such as parental emotional feeding and rewarding practices have also been connected with overweight (48).
In addition to weight, we identified several independent determinants of overeating. In our study, boys were more prone to overeating than girls. This may be partly explained by differences in parental feeding practices towards sons and daughters (49). Sons are encouraged to eat more and are served larger portions (50, 51), while daughters are taught food avoidant strategies, and parents are in general more concerned about their daughters’ than their sons’ weight status (52, 53).
The finding that parental depression increased the odds of overeating is both interesting and concerning. This might reflect preadolescents’ response to parent ill-health through overeating. Moreover, parents with depression may have altered feeding behaviors and give their children less autonomy in eating (54). Our findings align with results from the ALSPAC study, UK, where maternal depressive symptoms during the first 5 years of the child’s life predicted greater parental worry about child overeating at age 8, and greater self-reported emotional and external eating at age 14 among 3,887 participants (21). The question on overeating in that study was different from ours, as it specifically covered parental worry about child overeating. Moreover, mothers completed a questionnaire on postnatal depression (55), while our question addressed any history of diagnosed and/or treated depression. Contrasting our findings, a Danish study (n = 1,939) demonstrated that maternal psychiatric disorders were not associated with child-reported emotional or external eating at ages 11–12 (16). Register data on psychiatric disorders, and The Eating Pattern Inventory for children (EPI-C) (56) were used in the Danish study. No association was found between parental depression and SR or FR either, as measured with the Children’s Eating Behavior Questionnaire (CEBQ) (6) in 2–5-year-old Australian children (n = 977) (11). Given that all studies rely on different methodologies, future research should replicate these findings.
Furthermore, we observed that parental emotional feeding was linked to overeating. This finding is plausible, since receiving food for other purposes than hunger might disturb the natural satiety signals, resulting in overeating (57). However, this aspect has been sparsely studied with conflicting results. Previous studies are based on rather small samples with less than 550 children (24–26), and most included much younger children than our study. In line with our findings, an Australian study reported a link between maternal emotional feeding at age 2 and a tendency to overeat at age 3 (24). The researchers used a factor called ‘tendency to overeat’ based on items from the parent version of the Dutch Eating Behavior Questionnaire (58) and CEBQ (6). A US study using CEBQ and including children from low-income and minority households also observed a longitudinal association between emotional feeding and FR, but the results on SR were opposite at different ages (25). Higher emotional feeding at the age of 3 years predicted higher SR 1 year later, but higher emotional feeding at the age of 4 years was associated with lower SR 1 year later. On the other hand, a Chinese study involving 7–12-year-old children did not find associations between emotional feeding and any of these eating behaviors measured by the CEBQ (26).
The main strength of the Fin-HIT study is its large sample size. The sample is representative of school children in urban and semi-urban areas of Finland. Thus, the findings may be generalized to similar populations in areas with moderate population density in Western countries. We included a wide variety of variables from several data sources: parent-reported questionnaire, anthropometric measures made mainly by trained fieldworkers, and objective register data. This allowed us to cover multiple aspects of the topic and address their hierarchy in a systematic way. In addition, a sensitivity analysis was conducted, and it confirmed our findings.
The main limitation relates to the cross-sectional study design: we were unable to indicate causality between the determinants and outcomes. Moreover, we used a single question to assess overeating, instead of a validated questionnaire such as the CEBQ with mean scores for the SR, FR and EOE subscales (6). Our measure did not give a continuous ranking for the children on a scale, but divided them into groups, which might affect the results.
Many determinants were not measured objectively since reported by the parents. We do not have verified diagnoses of parental depression, nor do we know when it manifested. However, our question is considered easy to answer and suitable for epidemiological study purposes. Breastfeeding was reported retrospectively and reflects the situation on average 11 years before estimating overeating. However, it has been proved that breastfeeding can be reliably reported several years later (14). The register data on maternal SES was from the time of the child’s birth. We assume the SES to be similar or higher at the time of data collection; higher in particular among the tenth of the mothers who were previously studying.
Future research should explore the mechanisms underlying the associations between parental depression, emotional feeding, and overeating in preadolescents. Longitudinal studies would allow to establish causal relationships and examine how these factors interact over time. A crucial next step is to investigate how interventions aimed at improving parental mental health, and promoting healthy feeding practices, impact children’s eating behaviors and weight trajectories.
5 Conclusion
Our findings highlighted that along with weight status, sex, parental depression, and emotional feeding are linked to a parent-reported tendency towards overeating in preadolescence. Since overeating predisposes to obesity, and childhood obesity is a substantial public health issue, all efforts to recognize the causes of obesity and to prevent it are needed. To promote health, parents should be taught to use other ways than food to console their child. Finally, it is important to support parental mental health since this might affect the child’s eating behavior.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: the datasets are available from the corresponding author on reasonable request. Requests to access these datasets should be directed to Heli Viljakainen, aGVsaS52aWxqYWthaW5lbkBoZWxzaW5raS5maQ==.
Ethics statement
The studies involving humans were approved by the Coordinating Ethics Committee of the Hospital District of Helsinki and Uusimaa. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
CS: Conceptualization, Formal analysis, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing. ML: Conceptualization, Formal analysis, Methodology, Writing – review & editing. A-ME: Conceptualization, Methodology, Writing – review & editing. LR: Conceptualization, Methodology, Writing – review & editing. SM: Conceptualization, Methodology, Supervision, Writing – review & editing. HV: Conceptualization, Funding acquisition, Methodology, Project administration, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. Funding for this study was provided by Folkhälsan Research Foundation and the University of Helsinki. Marja H. Leppänen was supported by the Research Council of Finland (grant number 350820). The funders had no role in the study design, collection, analysis or interpretation of the data, writing the manuscript, or the decision to submit the paper for publication.
Acknowledgments
We thank the children and their parents for participating in the Fin-HIT study, as well as the school personnel, fieldworkers and research coordinators who contributed to the data collection. We also thank Kris Elomaa for data management, and Sohvi Lommi for help with the figure.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2024.1497509/full#supplementary-material
Abbreviations
CEBQ, Children’s Eating Behavior Questionnaire; EOE, Emotional Overeating; FR, Food Responsiveness; SR, Satiety Responsiveness.
References
1. Hughes, SO, and Frazier-Wood, AC. Satiety and the self-regulation of food take in children: a potential role for gene-environment interplay. Curr Obes Rep. (2016) 5:81–7. doi: 10.1007/s13679-016-0194-y
2. Carnell, S, Haworth, CM, Plomin, R, and Wardle, J. Genetic influence on appetite in children. Int J Obes. (2008) 32:1468–73. doi: 10.1038/ijo.2008.127
3. Savage, JS, Fisher, JO, and Birch, LL. Parental influence on eating behavior: conception to adolescence. J Law Med Ethics. (2007) 35:22–34. doi: 10.1111/j.1748-720X.2007.00111.x
4. Syrad, H, Johnson, L, Wardle, J, and Llewellyn, CH. Appetitive traits and food intake patterns in early life. Am J Clin Nutr. (2016) 103:231–5. doi: 10.3945/ajcn.115.117382
5. Boutelle, KN, Manzano, MA, and Eichen, DM. Appetitive traits as targets for weight loss: the role of food cue responsiveness and satiety responsiveness. Physiol Behav. (2020) 224:113018. doi: 10.1016/j.physbeh.2020.113018
6. Wardle, J, Guthrie, CA, Sanderson, S, and Rapoport, L. Development of the Children's eating behaviour questionnaire. J Child Psychol Psychiatry. (2001) 42:963–70. doi: 10.1111/1469-7610.00792
7. Machado, BC, Dias, P, Sousa Lima, V, Carneiro, A, and Gonçalve, S. Frequency and correlates of picky eating and overeating in school-aged children: a Portuguese population-based study. J Child Fam Stud. (2021) 30:1198–213. doi: 10.1007/s10826-021-01936-0
8. Omar, OM, Massoud, MN, Ibrahim, AG, and Khalaf, NA. Effect of early feeding practices and eating behaviors on body composition in primary school children. World J Pediatr. (2022) 18:613–23. doi: 10.1007/s12519-022-00559-9
9. Reyes, M, Hoyos, V, Martinez, SM, Lozoff, B, Castillo, M, Burrows, R, et al. Satiety responsiveness and eating behavior among Chilean adolescents and the role of breastfeeding. Int J Obes. (2014) 38:552–7. doi: 10.1038/ijo.2013.191
10. Yelverton, CA, Geraghty, AA, O'Brien, EC, Killeen, SL, Horan, MK, Donnelly, JM, et al. Breastfeeding and maternal eating behaviours are associated with child eating behaviours: findings from the ROLO kids study. Eur J Clin Nutr. (2021) 75:670–9. doi: 10.1038/s41430-020-00764-7
11. Boswell, N, Byrne, R, and Davies, PSW. Eating behavior traits associated with demographic variables and implications for obesity outcomes in early childhood. Appetite. (2018) 120:482–90. doi: 10.1016/j.appet.2017.10.012
12. Hathcock, A, Krause, K, Viera, AJ, Fuemmeler, BF, Lovelady, C, and Østbye, T. Satiety responsiveness and the relationship between breastfeeding and weight status of toddlers of overweight and obese women. Matern Child Health J. (2014) 18:1023–30. doi: 10.1007/s10995-013-1331-9
13. Higgins, RC, Keller, KL, Aruma, JC, Masterson, TD, Adise, S, Fearnbach, N, et al. Influence of exclusive breastfeeding on hippocampal structure, satiety responsiveness, and weight status. Matern Child Nutr. (2022) 18:e13333. doi: 10.1111/mcn.13333
14. Möller, LM, de Hoog, ML, van Eijsden, M, Gemke, RJ, and Vrijkotte, TG. Infant nutrition in relation to eating behaviour and fruit and vegetable intake at age 5 years. Br J Nutr. (2013) 109:564–71. doi: 10.1017/S0007114512001237
15. Pang, WW, McCrickerd, K, Quah, PL, Fogel, A, Aris, IM, Yuan, WL, et al. Is breastfeeding associated with later child eating behaviours? Appetite. (2020) 150:104653. doi: 10.1016/j.appet.2020.104653
16. Munkholm, A, Olsen, EM, Rask, CU, Clemmensen, L, Rimvall, MK, Jeppesen, P, et al. Early predictors of eating problems in preadolescence-a prospective birth cohort study. J Adolesc Health. (2016) 58:533–42. doi: 10.1016/j.jadohealth.2016.01.006
17. Albuquerque, G, Severo, M, and Oliveira, A. Early life characteristics associated with appetite-related eating behaviors in 7-year-old children. J Pediatr. (2017) 180:38–46.e2. doi: 10.1016/j.jpeds.2016.09.011
18. Ayine, P, Selvaraju, V, Venkatapoorna, CMK, Bao, Y, Gaillard, P, and Geetha, T. Eating behaviors in relation to child weight status and maternal education. Children. (2021) 8:32. doi: 10.3390/children8010032
19. Haycraft, E, Karasouli, E, and Meyer, C. Maternal feeding practices and children's eating behaviours: a comparison of mothers with healthy weight versus overweight/obesity. Appetite. (2017) 116:395–400. doi: 10.1016/j.appet.2017.05.033
20. Kininmonth, AR, Smith, AD, Llewellyn, CH, and Fildes, A. Socioeconomic status and changes in appetite from toddlerhood to early childhood. Appetite. (2020) 146:104517. doi: 10.1016/j.appet.2019.104517
21. Doom, JR, Deer, LK, Mickel, T, Infante, A, and Rivera, KM. Eating behaviors as pathways from early childhood adversity to adolescent cardiometabolic risk. Health Psychol. (2024) 43:448–61. doi: 10.1037/hea0001340
22. McCrickerd, K. Cultivating self-regulatory eating behaviours during childhood: the evidence and opportunities. Nutr Bull. (2018) 43:388–99. doi: 10.1111/nbu.12355
23. Vaughn, AE, Ward, DS, Fisher, JO, Faith, MS, Hughes, SO, Kremers, SP, et al. Fundamental constructs in food parenting practices: a content map to guide future research. Nutr Rev. (2016) 74:98–117. doi: 10.1093/nutrit/nuv061
24. Rodgers, RF, Paxton, SJ, Massey, R, Campbell, KJ, Wertheim, EH, Skouteris, H, et al. Maternal feeding practices predict weight gain and obesogenic eating behaviors in young children: a prospective study. Int J Behav Nutr Phys Act. (2013) 10:24. doi: 10.1186/1479-5868-10-24
25. Berge, JM, Miller, J, Veblen-Mortenson, S, Kunin-Batson, A, Sherwood, NE, and French, SA. A bidirectional analysis of feeding practices and eating behaviors in parent/child dyads from low-income and minority households. J Pediatr. (2020) 221:93–8.e20. doi: 10.1016/j.jpeds.2020.02.001
26. Qiu, C, Hatton, R, Li, Q, Xv, J, Li, J, Tian, J, et al. Associations of parental feeding practices with children's eating behaviors and food preferences: a Chinese cross-sectional study. BMC Pediatr. (2023) 23:84. doi: 10.1186/s12887-023-03848-y
27. Braden, A, Rhee, K, Peterson, CB, Rydell, SA, Zucker, N, and Boutelle, K. Associations between child emotional eating and general parenting style, feeding practices, and parent psychopathology. Appetite. (2014) 80:35–40. doi: 10.1016/j.appet.2014.04.017
28. Snoek, HM, Engels, RC, Janssens, JM, and van Strien, T. Parental behaviour and adolescents' emotional eating. Appetite. (2007) 49:223–30. doi: 10.1016/j.appet.2007.02.004
29. Topham, GL, Hubbs-Tait, L, Rutledge, JM, Page, MC, Kennedy, TS, Shriver, LH, et al. Parenting styles, parental response to child emotion, and family emotional responsiveness are related to child emotional eating. Appetite. (2011) 56:261–4. doi: 10.1016/j.appet.2011.01.007
30. Jansen, E, Williams, KE, Mallan, KM, Nicholson, JM, and Daniels, LA. Bidirectional associations between mothers' feeding practices and child eating behaviours. Int J Behav Nutr Phys Act. (2018) 15:3. doi: 10.1186/s12966-018-0644-x
31. Steinsbekk, S, Belsky, J, and Wichstrøm, L. Parental feeding and child eating: an investigation of reciprocal effects. Child Dev. (2016) 87:1538–49. doi: 10.1111/cdev.12546
32. Jansen, PW, Derks, IPM, Mou, Y, van Rijen, EHM, Gaillard, R, Micali, N, et al. Associations of parents' use of food as reward with children's eating behaviour and BMI in a population-based cohort. Pediatr Obes. (2020) 15:e12662. doi: 10.1111/ijpo.12662
33. Roberts, L, Marx, JM, and Musher-Eizenman, DR. Using food as a reward: an examination of parental reward practices. Appetite. (2018) 120:318–26. doi: 10.1016/j.appet.2017.09.024
34. Figueiredo, RAO, Simola-Ström, S, Rounge, TB, Viljakainen, H, Eriksson, JG, Roos, E, et al. Cohort profile: The Finnish health in teens (Fin-HIT) study: a population-based study. Int J Epidemiol. (2019) 48:23–4. doi: 10.1093/ije/dyy189
35. THL. (2024). Register of primary health care visits. Available at: https://thl.fi/en/web/thlfi-en/statistics-and-data/data-and-services/register-descriptions/register-of-primary-health-care-visits (Accessed December 17, 2024).
36. Boyd, A, Golding, J, Macleod, J, Lawlor, DA, Fraser, A, Henderson, J, et al. Cohort profile: the ‘children of the 90s’—the index offspring of the Avon Longitudinal Study of Parents and Children. Int J Epidemiol. (2013) 42:111–27. doi: 10.1093/ije/dys064
37. Sarkkola, C, Rounge, TB, Simola-Ström, S, von Kraemer, S, Roos, E, and Weiderpass, E. Validity of home-measured height, weight and waist circumference among adolescents. Eur J Pub Health. (2016) 26:975–7. doi: 10.1093/eurpub/ckw133
38. Cole, TJ, and Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr Obes. (2012) 7:284–94. doi: 10.1111/j.2047-6310.2012.00064.x
39. THL. (2024). Medical birth register. Available at: https://thl.fi/en/web/thlfi-en/statistics-and-data/data-and-services/register-descriptions/newborns (Accessed December 17, 2024).
40. Lau, C. Development of infant oral feeding skills: what do we know? Am J Clin Nutr. (2016) 103:616s–21s. doi: 10.3945/ajcn.115.109603
41. Engle, WA, Tomashek, KM, and Wallman, C. "Late-preterm" infants: a population at risk. Pediatrics. (2007) 120:1390–401. doi: 10.1542/peds.2007-2952
43. Hasunen, K, Kalavainen, M, Keinonen, H, Lagström, H, Lyytikäinen, A, Nurttila, A, et al. Lapsi, perhe ja ruoka. Imeväis- ja leikki-ikäisten lasten, odottavien ja imettävien äitien ravitsemussuositus. Sosiaali- ja terveysministeriön julkaisuja. (2004) 11.
44. Lommi, S, Engberg, E, Tuorila, H, Kolho, KL, and Viljakainen, H. Sex-and weight-specific changes in the frequency of sweet treat consumption during early adolescence: a longitudinal study. Br J Nutr. (2021) 126:1592–600. doi: 10.1017/S0007114521001112
45. Kininmonth, A, Smith, A, Carnell, S, Steinsbekk, S, Fildes, A, and Llewellyn, C. The association between childhood adiposity and appetite assessed using the child eating behavior questionnaire and baby eating behavior questionnaire: a systematic review and meta-analysis. Obes Rev. (2021) 22:e13169. doi: 10.1111/obr.13169
46. Emond, JA, Tovar, A, Li, Z, Lansigan, RK, and Gilbert-Diamond, D. FTO genotype and weight status among preadolescents: assessing the mediating effects of obesogenic appetitive traits. Appetite. (2017) 117:321–9. doi: 10.1016/j.appet.2017.07.009
47. Llewellyn, CH, Trzaskowski, M, van Jaarsveld, CHM, Plomin, R, and Wardle, J. Satiety mechanisms in genetic risk of obesity. JAMA Pediatr. (2014) 168:338–44. doi: 10.1001/jamapediatrics.2013.4944
48. Beckers, D, Karssen, LT, Vink, JM, Burk, WJ, and Larsen, JK. Food parenting practices and children's weight outcomes: a systematic review of prospective studies. Appetite. (2021) 158:105010. doi: 10.1016/j.appet.2020.105010
49. Keller, KL, Kling, SMR, Fuchs, B, Pearce, AL, Reigh, NA, Masterson, T, et al. A biopsychosocial model of sex differences in Children's eating behaviors. Nutrients. (2019) 11:682. doi: 10.3390/nu11030682
50. Orrell-Valente, JK, Hill, LG, Brechwald, WA, Dodge, KA, Pettit, GS, and Bates, JE. "Just three more bites": an observational analysis of parents' socialization of children's eating at mealtime. Appetite. (2007) 48:37–45. doi: 10.1016/j.appet.2006.06.006
51. Bouhlal, S, McBride, CM, Ward, DS, and Persky, S. Drivers of overweight mothers' food choice behaviors depend on child gender. Appetite. (2015) 84:154–60. doi: 10.1016/j.appet.2014.09.024
52. Tiggemann, M, and Lowes, J. Predictors of maternal control over children's eating behaviour. Appetite. (2002) 39:1–7. doi: 10.1006/appe.2002.0487
53. Phares, V, Steinberg, AR, and Thompson, JK. Gender differences in peer and parental influences: body image disturbance, self-worth, and psychological functioning in preadolescent children. J Youth Adolesc. (2004) 33:421–9. doi: 10.1023/B:JOYO.0000037634.18749.20
54. Goulding, AN, Rosenblum, KL, Miller, AL, Peterson, KE, Chen, YP, Kaciroti, N, et al. Associations between maternal depressive symptoms and child feeding practices in a cross-sectional study of low-income mothers and their young children. Int J Behav Nutr Phys Act. (2014) 11:75. doi: 10.1186/1479-5868-11-75
55. Cox, JL, Holden, JM, and Sagovsky, R. Detection of postnatal depression. Development of the 10-item Edinburgh postnatal depression scale. Br J Psychiatry. (1987) 150:782–6. doi: 10.1192/bjp.150.6.782
56. Schacht, M, Richter-Appelt, H, Schulte-Markwort, M, Hebebrand, J, and Schimmelmann, BG. Eating pattern inventory for children: a new self-rating questionnaire for preadolescents. J Clin Psychol. (2006) 62:1259–73. doi: 10.1002/jclp.20300
57. Birch, LL. Learning to eat: behavioral and psychological aspects. Nestle Nutr Inst Workshop Ser. (2016) 85:125–34. doi: 10.1159/000439503
Keywords: overeating, eating behavior, children and adolescents, overweight and obesity, parental depression, emotional feeding, parental feeding practices, family
Citation: Sarkkola C, Leppänen MH, Eloranta A-M, Räisänen L, Männistö S and Viljakainen H (2025) Parental depression and emotional feeding practices are associated with a tendency towards overeating in preadolescents. Front. Nutr. 11:1497509. doi: 10.3389/fnut.2024.1497509
Edited by:
Agnieszka Kozioł-Kozakowska, Jagiellonian University Medical College, PolandReviewed by:
Claudia Hunot-Alexander, University of Guadalajara, MexicoOctavian Vasiliu, Dr. Carol Davila University Emergency Military Central Hospital, Romania
Copyright © 2025 Sarkkola, Leppänen, Eloranta, Räisänen, Männistö and Viljakainen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Heli Viljakainen, aGVsaS52aWxqYWthaW5lbkBoZWxzaW5raS5maQ==