 Bekir Erhan Orhan1
Bekir Erhan Orhan1 Walaa Jumah Alkasasbeh2
Walaa Jumah Alkasasbeh2 Aydın Karaçam3
Aydın Karaçam3 Umut Canlı4
Umut Canlı4 Niyazi Sıdkı Adıgüzel3
Niyazi Sıdkı Adıgüzel3 Adam Tawfiq Amawi5*
Adam Tawfiq Amawi5*- 1Faculty of Sports Sciences, Istanbul Aydın University, Istanbul, Türkiye
- 2Department of Physical Education, Faculty of Sports Science, The University of Jordan, Amman, Jordan
- 3Faculty of Sports Sciences, Bandırma Onyedi Eylül University, Balıkesir, Türkiye
- 4Faculty of Sports Sciences, Tekirdağ Namık Kemal University, Tekirdağ, Türkiye
- 5Department of Movement Sciences and Sports Training, School of Sports Sciences, The University of Jordan, Amman, Jordan
Background: Diet quality and physical activity shape chronic-disease risk, yet the alignment between what adults know about nutrition and how they evaluate healthy eating remains unclear.
Methods: Adults in Türkiye (N = 408; 46.3% women, 53.7% men; mean age 28.6 years) completed validated measures of nutrition knowledge (NKS) and attitudes toward healthy nutrition [ASHN; subscales: Information on Nutrition (IN), Emotion for Nutrition (EN), Positive Nutrition (PN), Malnutrition (MP)]. Lifestyle factors included smoking, alcohol use, and 7-day physical activity (sedentary/low/moderate/high). Analyses comprised t-tests, one-way ANOVA with Tukey tests, Pearson correlations, and multiple linear regression.
Results: Knowledge and attitudes were only weakly aligned: higher NKS related to lower ASHN Total (r = −0.18, p < 0.001) and to IN (r = −0.21), PN (r = −0.11), and MP (r = −0.17); EN was null (r = −0.01). In regression, IN (β = −0.17, p = 0.001) and MP (β = −0.16, p = 0.006) were independently associated with lower NKS; overall fit was small (R2 = 0.063; F(4,403) = 6.815, p < 0.001). Attitudes varied strongly by physical activity High > Low/Moderate/Sedentary for ASHN Total (F(3,404) = 10.10, η2 = 0.07), IN (F = 8.10), and PN (F = 11.11); EN showed no group difference. Smoking showed a paradox: knowledge was higher among heavier smokers (F(3,404) = 3.47, p = 0.010), whereas attitudes were less favorable (Never/Former > ≥ 11/day for ASHN Total; F = 6.47, η2 = 0.04). Non-drinkers reported higher ASHN than drinkers (t(406) = 2.48, p = 0.013) with lower MP (t(406) = 3.65, p < 0.001). Education displayed clear stepwise gradients for attitudes (e.g., ASHN Total F = 18.97, η2 = 0.12), but not for knowledge. Age correlated positively with ASHN Total (r = 0.27) and EN/PN/MP, but not with NKS (r = −0.07).
Conclusion: In this adult sample, nutrition knowledge and healthy-eating attitudes were largely distinct. Attitudes especially belief- and practice-oriented facets tracked physical activity and other lifestyle factors, whereas knowledge did not. Interventions should pair education with motivation, self-regulation, and contextual supports to convert knowledge into healthier eating.
Introduction
Diet quality remains a central determinant of noncommunicable disease risk, operating alongside physical activity and other lifestyle practices across the life course (1–3). Contemporary public guidance emphasizes patterns rich in minimally processed foods, fruits and vegetables, whole grains, and appropriate energy balance, combined with regular moderate-to-vigorous activity (4). Aligning everyday eating with these recommendations is challenging because dietary choices are influenced by a combination of factors, including knowledge, values, motivation, self-regulation, habits, social context, and environmental constraints that affect time and cost (5–7).
National surveillance indicates that Türkiye faces a substantial burden of modifiable noncommunicable disease risk factors, providing a clear rationale for examining nutrition-related constructs in this context (8, 9). National monitoring data indicate that insufficient physical activity is common among adults and that excess body weight remains a widespread public-health concern (8). Official health statistics likewise show a continuing high prevalence of obesity among individuals aged 15 years and older (9). Consistent with these national indicators, recent evidence in Turkish adults suggests that nutrition-related attitudes vary across physical-activity and body-mass profiles, supporting the inclusion of lifestyle factors when examining evaluative nutrition constructs in Türkiye (10).
Health literacy and life-course perspectives underscore that capacities relevant to navigating food environments evolve with age, education, and accumulated experience, and they extend well beyond the possession of factual information (11, 12). Evidence across diverse adult populations shows that higher factual understanding is only inconsistently mirrored by healthier appraisals or intentions, pointing to gaps between what people know and how they evaluate or plan to act (13, 14). These gaps matter for intervention design because programs that privilege information alone may leave the motivational and regulatory ingredients of behavior change unaddressed.
Dual-process accounts and related social-cognition models position attitudes, perceived control, and habit strength as proximal to behavior, whereas declarative knowledge exerts influence chiefly when it is embedded in motivated, self-regulated action (15, 16). Meta-analytic syntheses consistently find that behavior-change techniques targeting self-regulatory processes goal setting, action and coping planning, self-monitoring, and feedback yield stronger effects than education alone, particularly when delivered in autonomy-supportive ways (17, 18). Randomized and digitally mediated interventions that incorporate motivational interviewing or self-determination theory–informed components further demonstrate added value beyond purely informational content (19–22).
Large population datasets reveal clustering of physical activity, smoking, alcohol use, and dietary behaviors within coherent profiles that appear to share determinants such as self-efficacy, health identity, and planning skill (23–27). Within this constellation, public-health anchors for weekly activity approximately 150 min of moderate intensity offer pragmatic thresholds for classifying exposure (4). Because attitudes index motivational readiness and regulatory capacity, they should align more closely with other health-promoting practices than factual knowledge alone (28).
Cohabitation and social ties can facilitate meal planning and reinforce norms that support healthier eating, whereas living alone is often associated with less favorable dietary patterns (29, 30). These sociodemographic gradients may strengthen evaluative orientations toward healthy eating even when factual knowledge has already reached a basic threshold through schooling or media exposure (11, 31, 32). Together, this literature suggests that attitudes may track lifestyle and social positioning more reliably than knowledge, with implications for the targeting of limited intervention resources.
This study (i) profiles adults’ nutrition knowledge and healthy-eating attitudes; (ii) quantifies their correspondence and any knowledge–attitude gap; and (iii) tests for differences across lifestyle factors physical activity, smoking, alcohol use, and family history of chronic illness as well as sociodemographic characteristics (education, age, gender, marital status). Guided by behavioral-clustering theory, the a priori expectation is that attitudes being closer to motivation and self-regulation will exhibit stronger and more consistent gradients across lifestyle factors than knowledge, whereas knowledge will show weaker or no gradients after accounting for sociodemographics. A further objective is to evaluate whether healthy-eating attitudes are independently associated with nutrition knowledge in multivariable models, anticipating only small associations if the constructs operate through distinct pathways.
The aim of the study is to determine the relationship between adults’ nutrition knowledge and their attitudes toward healthy eating and to assess how both vary by lifestyle and sociodemographic characteristics, thereby informing whether future programs should target informational, motivational, or contextual strategies for maximal impact.
Methods
Model
This descriptive, cross-sectional correlational study examined associations between adults’ nutrition knowledge and attitudes toward healthy nutrition and compared scores across key sociodemographic characteristics and lifestyle factors. Because data were collected at a single time point, findings should be interpreted as associative and do not permit causal inference (33).
Study group
The study group was assembled through convenience sampling, a pragmatic approach commonly used when rapid recruitment is needed (34). Eligible individuals were ≥18 years, residing in Türkiye, able to provide informed consent, and able to complete an online self-report form. The final analytic sample comprised 408 adults (46.3% women, 53.7% men; M_age = 28.60 years). Descriptive characteristics of the sample are presented in Table 1.

Table 1. Normality test results (skewness and kurtosis).
Sample size and power
A total of 490 adults initiated the questionnaire; after exclusions for ineligibility or incomplete key data, the analytic sample was N = 408. Although sampling was by convenience, this N affords narrow confidence intervals and adequate sensitivity for the planned analyses. For example, the 95% CI half-width for group means is approximately ±1.2 points for ASHN (SD ≈ 12) and ±2.4 points for NKS (SD ≈ 24.8). For two-group comparisons with sizes similar to the gender split (n₁ = 189, n₂ = 219; α = 0.05, two-tailed), the study is sensitive to small effects of about d ≈ 0.28–0.30. One-way ANOVAs with four groups (e.g., physical-activity categories) have adequate sensitivity for small-to-moderate omnibus effects (≈ η2 ≥ 0.03–0.06). For correlations, effects of r ≈ 0.14 are detectable at ~80% sensitivity (α = 0.05) (35, 36). These values indicate the study is equipped to estimate means with reasonable precision and to detect small associations and small-to-moderate group differences typical of lifestyle and attitude research.
Data collections
Nutrition knowledge scale (NKS)
Adapted into Turkish by Öngün Yılmaz et al. (37) for healthy adults, the NKS is a 31-item, 5-point Likert instrument that assesses general nutrition knowledge. Items are scored 4 → 0 from Strongly agree to Strongly disagree; misinformation items are reverse-coded so that higher totals reflect greater knowledge. Consistent with the Turkish validation, reverse-scored items are 1, 5, 6, 9, 10, 16, 17, 21, 27, 28 and the scale functions as a single-factor measure. The total score ranges 0–124. Psychometric properties reported by Yılmaz et al. (2021) support good reliability and construct validity: KMO = 0.862 with a significant Bartlett test (χ2 = 3869.244, p < 0.001); Cronbach’s α = 0.85 (internal consistency) and ICC = 0.86 (test–retest). Confirmatory factor analysis indicated acceptable–good fit (CMIN/df = 2.347, RMSEA ≈ 0.04–0.05, CFI ≈ 0.94, GFI ≈ 0.98–0.99, AGFI ≈ 0.97). For descriptive interpretation in that study, empirical cut-points were used (e.g., low ≤79, medium 80–90, high 91–100, very high ≥101) (37).
Attitude scale for healthy nutrition (ASHN)
The ASHN is a 21-item, 5-point Likert instrument developed by Tekkurşun Demir and Cicioğlu (38) to assess adults’ attitudes toward healthy eating. Items are rated from 1 = Strongly Disagree to 5 = Strongly Agree and summed to yield a total score from 21 to 105, with higher scores indicating more favorable attitudes. The scale comprises four subdomains using the English labels throughout this manuscript: Information on Nutrition (IN; items 1–5), Emotion for Nutrition (EN; items 6–11), Positive Nutrition (PN; items 12–16), and Malnutrition (MP; items 17–21). As in the original validation, negatively worded items (6–11, 17–21) are reverse-coded prior to scoring. For descriptive interpretation, we used published bands: 21–22 very low, 23–42 low, 43–63 moderate, 64–84 high, and 85–105 very high. The developers reported good psychometrics (internal consistency: α = 0.90 for IN, α = 0.84 for EN, α = 0.75 for PN, α = 0.83 for MP; CFA fit: χ2/df = 1.71, RMSEA = 0.04, PGFI = 0.74, PNFI = 0.82, GFI = 0.92, AGFI = 0.90, IFI = 0.98, NFI = 0.95, CFI = 0.98), supporting a four-factor structure with a higher-order attitude construct (38).
Sociodemographic and lifestyle factors
Participants reported age, gender, marital status, and highest educational attainment. Lifestyle factors were assessed as smoking status, alcohol use, and physical activity. In addition, family history of chronic illness was recorded as a health-related background characteristic (presence of at least one chronic condition in a first-degree relative). Physical activity was self-reported via a single 7-day frequency item in the online questionnaire: “During the past 7 days, on how many days did you perform ≥30 minutes of physical activity (e.g., walking, running, sport, or exercise)?” Because this measure relied on self-report, responses may be influenced by recall and social desirability. Responses were categorized as sedentary (0 days), low (1–2 days), moderate (3–4 days), and high (≥5 days/week), aligning with WHO guidance recommending at least 150 min/week of moderate-intensity physical activity (4).
Data analysis
Data were screened for entry errors, outliers, distributional assumptions, and multicollinearity prior to analysis; no miscoded values were detected. Analyses were conducted in SPSS 27. Descriptive statistics were computed for all variables. Normality was evaluated using skewness and kurtosis (|skewness| and |kurtosis| ≤ 1.5) and visual inspection of histograms and Q–Q plots; normality indices for the study variables are summarized in Table 1 and indicated acceptable departures from normality for the planned parametric analyses (39). For two-group comparisons, independent-samples t tests were used, and for multi-group comparisons, one-way ANOVA with Tukey post hoc tests was applied. Bivariate associations were examined using Pearson product–moment correlations. To examine whether ASHN subdimensions were independently associated with nutrition knowledge, multiple linear regression was conducted with ASHN subdimensions—Information on Nutrition (IN), Emotion for Nutrition (EN), Positive Nutrition (PN), and Malnutrition (MP)—entered simultaneously as independent variables and the NKS total score as the dependent variable. Regression assumptions were evaluated using residual diagnostics: normality was assessed via histograms and Normal P–P/Q–Q plots (supported by the Shapiro–Wilk test), and linearity and homoscedasticity were examined using standardized residuals versus predicted values plots; no substantial deviations were observed. Multicollinearity was evaluated using tolerance and variance inflation factor (VIF) statistics (all VIF < 5). Statistical significance was set at p < 0.05. Effect sizes were reported alongside p-values (Cohen’s d for t tests, η2 for ANOVA, and Pearson’s r for correlations) and interpreted using conventional benchmarks (40).
Ethical approval and informed consent
Approved by the Ethics Committee of the Faculty of Social and Human Sciences, Istanbul Aydın University (Decision No. 2025/7, June 25, 2025), and conducted in accordance with the Declaration of Helsinki. Participation was voluntary, and written informed consent was obtained after participants were informed of the study and their right to withdraw at any time. To protect privacy, no directly identifying data were collected; responses were pseudonymized, stored on password-protected systems, and accessible only to the research team. Data were analyzed and reported in aggregate to maintain confidentiality.
Results
The sample included 408 adults (46.3% women, n = 189; 53.7% men, n = 219; mean age = 28.60 years). By highest educational attainment, 48.5% (n = 198) had completed high school, 17.2% (n = 70) held an associate degree, 24.0% (n = 98) held a bachelor’s degree, and 10.3% (n = 42) held a master’s degree. Regarding marital status, 65.2% (n = 266) were single and 34.8% (n = 142) were married (see Table 2).

Table 2. Sample characteristics (N = 408).
As shown in Table 3, men scored higher on NKS than women, t(406) = −3.70, p < 0.001, mean difference (Male − Female) = 8.98 [95% CI (4.21, 13.75)], d = 0.36. ASHN Total and its subscales did not differ by gender (e.g., mean difference (Male − Female) = −0.63, 95% CI [−3.01, 1.75] for ASHN Total; all p > 0.05).

Table 3. Independent samples t-test results for NKS and ASHN scores by gender (female n = 189; male n = 219).
As shown in Table 4, married participants scored higher on ASHN than single participants, t(406) = 3.31, p < 0.001, mean difference (Single − Married) = −4.15 [95% CI (−6.61, −1.69)], d = 0.34. Subscales showed a similar pattern for EN, t(406) = 5.06, p < 0.001, mean difference (Single − Married) = −2.42 [95% CI (−3.36, −1.48)], d = 0.52; for PN, t(406) = 2.64, p = 0.009, mean difference (Single − Married) = −1.15 [95% CI (−2.01, −0.29)], d = 0.27; and for MP, t(406) = 3.06, p = 0.002, mean difference (Single − Married) = −1.35 [95% CI (−2.22, −0.48)], d = 0.31. IN did not differ by marital status, t(406) = −1.83, p = 0.068, mean difference (Single − Married) = 0.82 [95% CI (−0.06, 1.70)], d = −0.19. NKS Total did not differ, t(406) = 0.68, p = 0.490, mean difference (Single − Married) = −1.76 [95% CI (−6.85, 3.33)].

Table 4. Independent samples t-test results for NKS and ASHN scores by marital status (Married n = 142; Single n = 266).
As shown in Table 5, only IN differed by family chronic illness, t(406) = −2.41, p = 0.016, mean difference (No − Yes) = 1.01 [95% CI (0.19, 1.83)], d = 0.24. NKS Total, ASHN Total, EN, PN, and MP did not differ between groups [all p > 0.05; e.g., ASHN Total mean difference (No-Yes) = 1.11, 95% CI (−1.34, 3.56)].
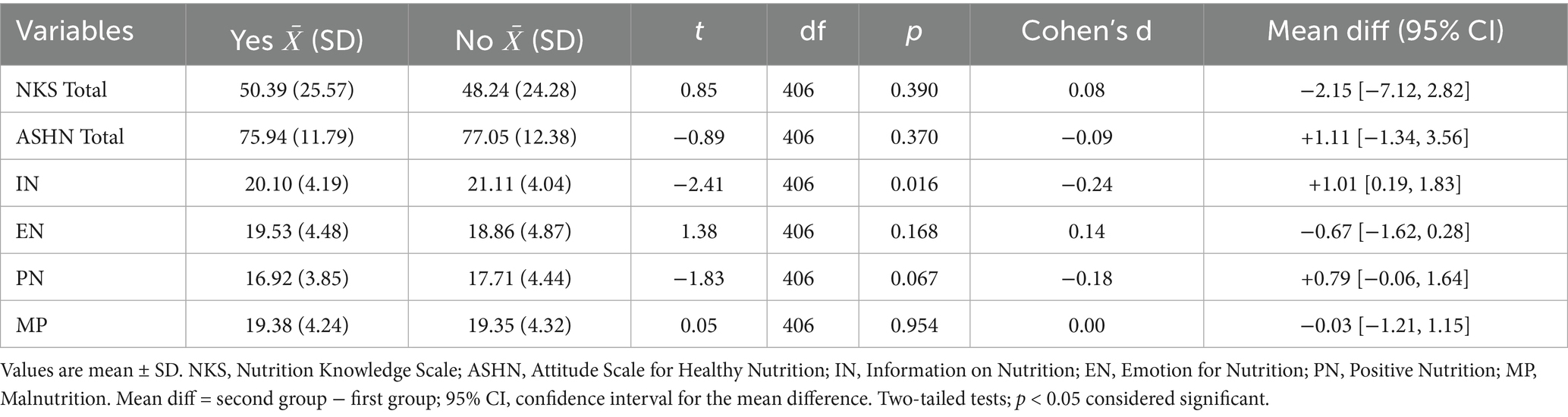
Table 5. Independent samples t-test results for NKS and ASHN scores by family chronic illness (Yes n = 155; No n = 253).
As shown in Table 6, ASHN was higher among non-users than users, t(406) = 2.48, p = 0.013, mean difference (Users − Non-users) = −3.13 [95% CI (−5.61, −0.65)], d = 0.26. MP was lower among non-users, t(406) = 3.65, p < 0.001, mean difference (Users − Non-users) = −1.61 [95% CI (−2.48, −0.74)], d = 0.38. NKS Total, IN, EN, and PN did not differ by alcohol use [all p > 0.05; e.g., NKS mean difference (Users − Non-users) = −1.30, 95% CI (−6.41, 3.81)].

Table 6. Independent samples t-test results for NKS and ASHN scores by alcohol use (Non-users n = 269; users n = 139).
As shown in Table 7, Educational attainment was not associated with NKS, F(3,404) = 0.52, p = 0.660, η2 < 0.01. In contrast, healthy-eating attitudes differed substantially by education, ASHN Total: F(3,404) = 18.97, p < 0.001, η2 = 0.12, with master’s degree reporting higher attitudes (M = 86.23, SD = 12.03) than high-school graduates (M = 72.84, SD = 10.81). The same pattern was observed for EN (F(3,404) = 19.26, p < 0.001, η2 = 0.12; MD M = 22.61 vs. HS M = 17.63) and for IN, PN, and MP (all p ≤ 0.006; η2 = 0.03–0.06), indicating an education gradient primarily for attitudinal domains rather than knowledge.

Table 7. One-way ANOVA results for NKS and ASHN (total and subscales) by highest educational attainment.
As shown in Table 8, physical activity frequency showed no statistically significant differences in NKS (F(3,404) = 2.14, p = 0.090, η2 = 0.01). However, physical activity was associated with more favorable healthy-nutrition attitudes, ASHN Total: F(3,404) = 10.10, p < 0.001, η2 = 0.07, with the high-activity group scoring higher (M = 82.45, SD = 9.88) than the sedentary group (M = 71.22, SD = 13.20). Differences were also evident for IN (F(3,404) = 8.10, p < 0.001, η2 = 0.05) and PN (F(3,404) = 11.11, p < 0.001, η2 = 0.07), whereas EN did not differ across activity levels (F(3,404) = 1.74, p = 0.150). MP varied modestly (F(3,404) = 3.29, p = 0.020, η2 = 0.02), suggesting that activity frequency aligned more with information/positive nutrition orientations than with emotion-related attitudes.

Table 8. One-way ANOVA results for NKS and ASHN (total and subscales) by physical activity level (7-day frequency).
As shown in Table 9, smoking status was associated with small but significant differences in NKS (F(3,404) = 3.47, p = 0.010, η2 = 0.02), with heavier smokers reporting higher knowledge (≥11/day: M = 54.39, SD = 23.04) than former smokers (M = 41.73, SD = 22.44). In contrast, healthy-nutrition attitudes were less favorable among heavier smokers: ASHN Total: F(3,404) = 6.47, p < 0.001, η2 = 0.04, with never smokers (M = 78.53, SD = 10.86) and former smokers (M = 78.37, SD = 13.32) scoring higher than ≥11/day smokers (M = 72.30, SD = 12.65). Similar differences were observed for IN (F(3,404) = 4.94, p < 0.001, η2 = 0.03), PN (F(3,404) = 5.86, p < 0.001, η2 = 0.04), and MP (F(3,404) = 6.41, p < 0.001, η2 = 0.04), while EN did not differ (F(3,404) = 1.98, p = 0.110). Overall, smoking status related more consistently to nutrition attitudes than to knowledge.
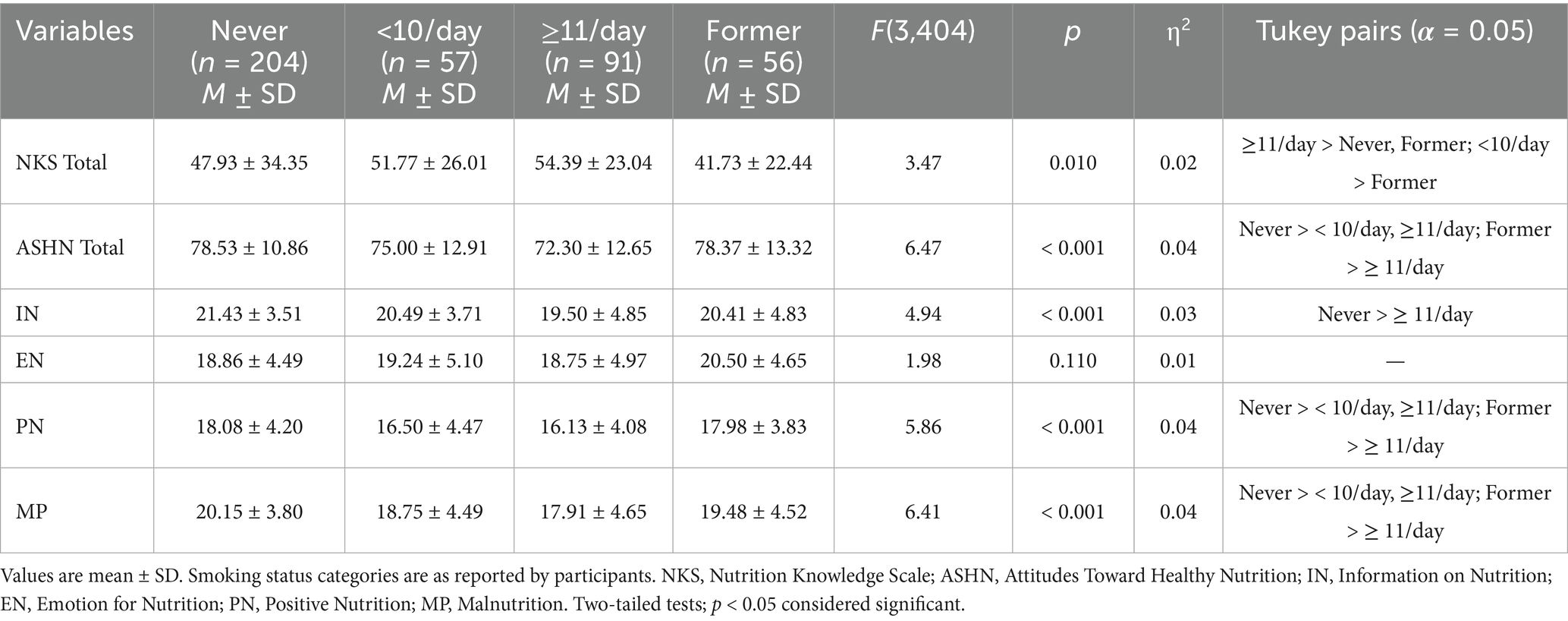
Table 9. One-way ANOVA results for NKS and ASHN (total and subscales) by smoking status.
As shown in Table 10, age was positively associated with ASHN Total (r = 0.27, p < 0.001) and with the EN (r = 0.31), PN (r = 0.19), and MP (r = 0.23) subscales, indicating small-to-moderate increases in healthier attitudes with greater age. By contrast, no association was observed between age and NKS Total (r = −0.07, ns) or IN (r = 0.01, ns).

Table 10. Correlations of age with nutrition knowledge and healthy-eating attitudes (N = 408).
As shown in Table 11, higher NKS scores were modestly associated with lower healthy-eating attitudes overall (ASHN Total: r = −0.18, p < 0.001). Negative associations were also observed for IN (r = −0.21, p < 0.001), PN (r = −0.11, p = 0.020), and MP (r = −0.17, p < 0.001), whereas EN showed no association (r = −0.01, p = 0.760). Collectively, these small effects suggest that greater nutrition knowledge does not necessarily translate into more favorable attitudes across all domains, indicating a possible knowledge–attitude gap.

Table 11. Correlations between nutrition knowledge (NKS) and healthy-eating attitudes (N = 408).
As shown in Table 12, a simultaneous multiple linear regression examined whether ASHN subscales were independently associated with NKS Total. The overall model was significant but explained a small proportion of variance (R2 = 0.063; Adj. R2 = 0.054). Controlling for the other subscales, IN (β = −0.17, p = 0.001) and MP (β = −0.16, p = 0.006) were negative predictors of NKS, whereas EN (β = 0.06, p = 0.270) and PN (β = 0.02, p = 0.620) were not significant. Diagnostics indicated no multicollinearity concerns (Tolerance = 0.64–0.79; VIF = 1.25–1.55) and approximately independent errors (DW ≈ 2.00). Residual-versus-fitted plots indicated approximate linearity and homoscedasticity, Cook’s distance and leverage did not identify influential cases, and the Normal P–P plot showed standardized residuals closely approximating normality (Figure 1). Higher scores on the IN and MP attitude facets were associated with lower nutrition-knowledge scores after adjustment, whereas affective and positive-nutrition attitudes (EN, PN) were unrelated to knowledge. Overall, ASHN subscales accounted for approximately 5–6% of variability in NKS, indicating that nutrition-related attitudes and nutrition knowledge were only weakly linked in this sample.

Table 12. Multiple linear regression examining associations between NKS total and ASHN subscales (IN, EN, PN, MP).

Figure 1. Normal P–P plot of regression standardized residuals for the model with NKS total as the outcome.
Discussion
This study clarified how adults’ NKS relates to their ASHN and how these constructs vary across physical activity, smoking, alcohol use, family chronic illness, and sociodemographic factors. Correlations between NKS and ASHN indices were small and frequently negative (e.g., ASHN Total r ≈ −0.18; IN r ≈ −0.21; PN r ≈ −0.11; MP r ≈ −0.17), and multiple regression showed small negative coefficients for IN and MP when predicting NKS after mutual adjustment. This pattern reflects construct distinctness rather than measurement failure: NKS captures declarative facts, whereas ASHN reflects evaluative orientation agreement with positive nutrition practices (PN/IN) and lower endorsement of malnutrition-congruent statements (MP). People with higher knowledge may also be more risk-attentive and thus more likely to recognize pitfalls that map onto MP items, producing modest inverse links. In some subgroups most visibly heavier smokers greater exposure to health information may not translate into more favorable attitudes, suggesting cognitive–affective misalignment or reactance (7). Unmeasured variables such as time scarcity, cost salience, diet restraint, self-regulation, or food environment plausibly shape knowledge acquisition and attitudes in different ways, further attenuating alignment in cross-section. The modest explained variance and marginal associations are consistent with two complementary explanations: measurement error in brief self-report indicators and construct mismatch, because declarative knowledge does not necessarily translate into motivation, self-regulation, or environmental opportunity. In future work, incorporating psychosocial determinants (e.g., autonomous motivation, self-efficacy, planning, habit strength) and contextual measures (e.g., time pressure, affordability, food availability) alongside richer behavioral indicators (diet quality indices and device-based activity) may improve model fit and clarify pathways.
Attitudes clustered with lifestyle, whereas knowledge did not. ASHN Total and its cognitively evaluative facets (IN and PN) increased monotonically from sedentary to high physical-activity categories, yet NKS did not vary by activity. Parallel gradients appeared for smoking and alcohol: never- and former-smokers and non-drinkers showed more favorable attitudes (higher PN, lower MP), while NKS was comparable across alcohol groups and paradoxically higher among heavier smokers. These converging gradients are consistent with behavioral clustering (23–25): individuals oriented toward one health domain (activity, non-smoking) also endorse more favorable nutrition attitudes, likely via shared determinants such as self-efficacy, planning, goal setting, and health identity (16, 26, 27, 41). Knowledge, by contrast, may accumulate through schooling, media, or clinical encounters and thus remains orthogonal to day-to-day lifestyle patterns (42). Notably, EN was the least discriminating subdomain across activity and lifestyle strata, whereas IN and PN differentiated groups clearly; interventions that emphasize beliefs and concrete practices may therefore tap into the same self-regulatory capacities that sustain physical activity and non-smoking, while purely affective appeals may be less sensitive to existing lifestyle orientation (16, 17).
Sociodemographic gradients favored attitudes over knowledge. Educational attainment displayed a robust stepwise association with ASHN (Master’s > Bachelor’s/Associate > High school) without a corresponding gradient in NKS, consistent with the idea that formal education shapes values, norms, and executive capacities that support favorable appraisals of healthy eating (43, 44) more than it augments domain-specific facts beyond a general threshold. Married participants showed more favorable ASHN, plausibly reflecting shared household routines, meal planning, and diffusion of health priorities within families (10, 29, 30). Age correlated positively with EN, PN, and MP, but not with NKS, suggesting that life-course prioritization of health may gradually strengthen attitudes even when factual knowledge remains relatively stable (11, 13, 45). Taken together, these gradients support a view in which attitudes are embedded in roles and contexts, whereas knowledge is comparatively context-insensitive once basic literacy is achieved (12).
Within a planned-behavior perspective, IN/PN align more closely with attitudinal and control beliefs that feed intention and action than NKS does (20, 46, 47). Dual-process accounts similarly predict that affective dispositions (EN) and cognitive evaluations (IN/PN) need not rise with knowledge unless interventions also engage motivation, identity, and habit (14, 15). Durable improvements likely require pairing informational content with self-regulatory tools (goal setting, implementation intentions, self-monitoring, environmental prompts), motivational interviewing or values-consistent framing, and social scaffolding (family/peer support) (18, 19, 22, 48). The paradoxical combination of relatively higher NKS and less favorable ASHN among heavier smokers exemplifies where alignment strategies clarifying goals, addressing ambivalence, building coping plans, and translating knowledge into feasible micro-behaviors should supersede additional didactic content (49, 50).
Limitations
The cross-sectional design precludes causal inference; reverse or bidirectional pathways are plausible (e.g., favorable ASHN may promote physical activity, which further reinforces attitudes). Physical activity was assessed using a single self-reported item; therefore, misclassification due to recall or social desirability cannot be ruled out. Convenience sampling limits generalizability and invites selection biases. All variables were self-reported; the single-item physical-activity measure captures frequency but not intensity or domain and likely carries more error than validated multi-item instruments or devices. Although NKS and ASHN showed acceptable psychometrics, common-method variance, item directionality (reverse-scored items), and content mismatch between facts and attitudes may attenuate associations. We did not adjust for potentially important covariates (e.g., BMI, socioeconomic status, diet quality, food insecurity, food environment), any of which could confound knowledge attitude links or lifestyle gradients. The number of comparisons was substantial; future work should consider multiplicity control or pre-registration. The temporal and cultural context may shape both attitudes and behaviors; replication in diverse settings and time periods is warranted.
This study pairs validated measures of knowledge and attitudes with rich lifestyle and sociodemographic data, yielding a clear account of knowledge attitude discordance and attitude behavior clustering. Standardized effect-size reporting improves transparency. Because attitudes more than knowledge track with physical activity and other lifestyle factors, findings support shifting intervention content toward motivation, self-regulation, and environmental supports. Future work should use prospective/experimental designs to test attitude-focused components beyond education (e.g., implementation intentions, self-monitoring, habit formation), incorporate device-based activity measures and fuller dietary/contextual assessments, and conduct mediation (self-efficacy, autonomous motivation) and moderation (education, marital status, smoking) analyses. Attention to food environments, time pressure, and price sensitivity will be critical for converting gains in ASHN into sustained dietary improvements.
The use of convenience sampling limits the generalizability of these findings. In addition, the sample’s gender composition was skewed toward male participants relative to distributions typically reported for comparable populations, which may have affected the magnitude and stability of some estimates. To better evaluate sensitivity to sample composition, future studies should apply post-stratification weights (e.g., by sex, age, and education) and re-estimate key models as robustness checks. Accordingly, the present results should be interpreted as descriptive for this sample rather than as population-level prevalence estimates.
Conclusion
In this adult sample, nutrition knowledge and healthy-eating attitudes were only weakly aligned, sometimes showing small negative associations. Attitudes—but not knowledge—varied systematically across physical activity and lifestyle factors, and age and education related more consistently to attitudes than to knowledge; heavier smoking also illustrated knowledge–attitude misalignment. These patterns suggest that information alone is unlikely to produce sustained change without motivation- and self-regulation–focused supports and reductions in contextual barriers. Accordingly, practice and policy may benefit from embedding attitude-focused components within broader health-behavior platforms, particularly physical-activity promotion and tobacco-control programs. In clinical care, brief screening for attitudinal barriers and readiness can guide counselling beyond information provision (e.g., motivational interviewing and implementation intention planning), while policy implementation through primary care, community programs, and workplace wellness may enable scalable, resource-efficient gains.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Approved by the Ethics Committee of the Faculty of Social and Human Sciences, Istanbul Aydın University (Decision No. 2025/7, June 25, 2025), and conducted in accordance with the Declaration of Helsinki. Participation was voluntary, and written informed consent was obtained after participants were informed of the study and their right to withdraw at any time. To protect privacy, no directly identifying data were collected; responses were pseudonymized, stored on password-protected systems, and accessible only to the research team. Data were analyzed and reported in aggregate to maintain confidentiality. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
BO: Project administration, Supervision, Writing – original draft, Writing – review & editing. WA: Methodology, Writing – original draft, Writing – review & editing. AK: Writing – original draft, Writing – review & editing. UC: Writing – original draft, Writing – review & editing. NA: Writing – original draft, Writing – review & editing. AA: Writing – original draft, Writing – review & editing.
Funding
The author(s) declared that financial support was not received for this work and/or its publication.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declared that Generative AI was not used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Peters, R, Ee, N, Peters, J, Beckett, N, Booth, A, Rockwood, K, et al. Common risk factors for major noncommunicable disease, a systematic overview of reviews and commentary: the implied potential for targeted risk reduction. Ther Adv Chronic Dis. (2019) 10:2040622319880392. doi: 10.1177/2040622319880392,
2. Morze, J, Danielewicz, A, Hoffmann, G, and Schwingshackl, L. Diet quality as assessed by the healthy eating index, alternate healthy eating index, dietary approaches to stop hypertension score, and health outcomes: a second update of a systematic review and Meta-analysis of cohort studies. J Acad Nutr Diet. (2020) 120:1998–2031.e15. doi: 10.1016/j.jand.2020.08.076,
3. Cerf, ME. Healthy lifestyles and noncommunicable diseases: nutrition, the life-course, and health promotion. Lifestyle Med. (2021) 2:e31. doi: 10.1002/lim2.31
4. World Health Organization. WHO guidelines on physical activity and sedentary behaviour. Geneva: World Health Organization (2022).
5. Sogari, G, Velez-Argumedo, C, Gómez, MI, and Mora, C. College students and eating habits: a study using an ecological model for healthy behavior. Nutrients. (2018) 10:1823. doi: 10.3390/nu10121823,
6. Chen, P-J, and Antonelli, M. Conceptual models of food choice: influential factors related to foods, individual differences, and society. Foods. (2020) 9:1898. doi: 10.3390/foods9121898,
7. Orhan, BE, Karaçam, A, Canli, U, Astuti, Y, and Govindasamy, K. Exploring the relationship between exercise addiction and attitudes towards healthy nutrition. J Phys Educ Sport. (2024) 24:1590–601. doi: 10.7752/jpes.2024.07179
8. World Health Organization National household health survey—prevalence of noncommunicable disease risk factors in Turkey 2017 (2018). Available online at: https://cdn.who.int/media/docs/default-source/ncds/ncd-surveillance/data-reporting/turkey/factsheet-steps-turkey-eng-08.10.2018.pdf?sfvrsn=efb51f62_1&download=true
9. Turkish Statistical Institute (TurkStat). Türkiye health survey. (2022) Press Release No.: 49747. Available online at: https://data.tuik.gov.tr/Bulten/Index?p=Turkiye-Saglik-Arastirmasi-2022-49747 (Accessed June 1, 2023).
10. Orhan, BE, Alkasasbeh, WJ, Karaçam, A, Amawi, AT, and Canli, U. Exploring the impact of BMI and physical activity on caffeine use disorder and nutritional attitudes among adults in Türkiye. Front Nutr. (2025) 12:1639852. doi: 10.3389/fnut.2025.1639852,
11. Maindal, HT, and Aagaard-Hansen, J. Health literacy meets the life-course perspective: towards a conceptual framework. Glob Health Action. (2020) 13:1775063. doi: 10.1080/16549716.2020.1775063,
12. McAnally, K, and Hagger, MS. Health literacy, social cognition constructs, and health behaviors and outcomes: a meta-analysis. Health Psychol. (2023) 42:213–34. doi: 10.1037/hea0001266,
13. Alves, F, and The, R. Relationship between health-related knowledge and attitudes and health risk behaviours among Portuguese university students. Glob Health Promot. (2024) 31:36–44. doi: 10.1177/17579759231195561,
14. Lindbloom, M, Asirvatham, J, Moon, W, and Altman, I. Motivation mediates the influence of the knowledge of nutrients’ function on diet. J Food Nutr Sci. (2021) 9:1. doi: 10.11648/j.jfns.20210901.11
15. Brown, DJ, Charlesworth, J, Hagger, MS, and Hamilton, K. A dual-process model applied to two health-promoting nutrition Behaviours. Behav Sci (Basel). (2021) 11:170. doi: 10.3390/bs11120170,
16. Hennessy, EA, Johnson, BT, Acabchuk, RL, McCloskey, K, and Stewart-James, J. Self-regulation mechanisms in health behavior change: a systematic meta-review of meta-analyses, 2006–2017. Health Psychol Rev. (2020) 14:6–42. doi: 10.1080/17437199.2019.1679654,
17. Spring, B, Champion, KE, Acabchuk, R, and Hennessy, EA. Self-regulatory behaviour change techniques in interventions to promote healthy eating, physical activity, or weight loss: a meta-review. Health Psychol Rev. (2021) 15:508–39. doi: 10.1080/17437199.2020.1721310,
18. Ntoumanis, N, Ng, JYY, Prestwich, A, Quested, E, Hancox, JE, Thøgersen-Ntoumani, C, et al. A meta-analysis of self-determination theory-informed intervention studies in the health domain: effects on motivation, health behavior, physical, and psychological health. Health Psychol Rev. (2021) 15:214–44. doi: 10.1080/17437199.2020.1718529,
19. Coumans, JMJ, Bolman, CAW, Oenema, A, and Lechner, L. The effects of a web-based computer-tailored diet and physical activity intervention based on self-determination theory and motivational interviewing: a randomized controlled trial. Internet Interv. (2022) 28:100537. doi: 10.1016/j.invent.2022.100537,
20. Daher, J, Mountjoy, M, and El Khoury, D. An online nutrition education program targeting intentions and related determinants towards dietary supplement use: an application of the theory of planned behavior. Nutrients. (2025) 17:557. doi: 10.3390/nu17030557,
21. Orhan, EB, Alkasasbeh, W, Karaçam, A, and Govindasamy, K. Exploring motivation and enjoyment as key determinants of sustained physical activity across diverse demographics. Sport Mont. (2025) 23:63–9. doi: 10.26773/smj.250610
22. AlKasasbeh, WJ, Amawi, AT, Al-Nawaiseh, SJ, Alshorman, D, Alshdaifat, K, Alawamleh, T, et al. Educational intervention using a mobile app to enhance sports nutrition knowledge and dietary habits in student-athletes: a randomized controlled trial. Front Educ. (2025) 10:1–8. doi: 10.3389/feduc.2025.1622166
23. Klompstra, L, Löf, M, Björkelund, C, Hellenius, M-L, Kallings, LV, Orho-Melander, M, et al. Co-occurrence of unhealthy lifestyle behaviours in middle-aged adults: findings from the Swedish CArdioPulmonary bioImage study (SCAPIS). Sci Rep. (2024) 14:22853. doi: 10.1038/s41598-024-71092-0,
24. Bjørnerud Korslund, S, Hansen, BH, and Bjørkkjær, T. Association between sociodemographic determinants and health behaviors, and clustering of health risk behaviors among 28,047 adults: a cross-sectional study among adults from the general Norwegian population. BMC Public Health. (2023) 23:541. doi: 10.1186/s12889-023-15435-y,
25. van Allen, Z, Bacon, SL, Bernard, P, Brown, H, Desroches, S, Kastner, M, et al. Clustering of health behaviors in Canadians: a multiple behavior analysis of data from the Canadian longitudinal study on aging. Ann Behav Med. (2023) 57:662–75. doi: 10.1093/abm/kaad008,
26. Boujelbane, MA, Ammar, A, Salem, A, Kerkeni, M, Trabelsi, K, Bouaziz, B, et al. Gender-specific insights into adherence to Mediterranean diet and lifestyle: analysis of 4,000 responses from the MEDIET4ALL project. Front Nutr. (2025) 12:1570904. doi: 10.3389/fnut.2025.1570904,
27. Boujelbane, MA, Ammar, A, Salem, A, Kerkeni, M, Trabelsi, K, Bouaziz, B, et al. Regional variations in Mediterranean diet adherence: a sociodemographic and lifestyle analysis across Mediterranean and non-Mediterranean regions within the MEDIET4ALL project. Front Public Health. (2025) 13:1596681. doi: 10.3389/fpubh.2025.1596681,
28. Orhan, BE, AlKasasbeh, WJ, Karaçam, A, Canlı, U, and Amawi, AT. Awareness of exercise addiction and exercise motivation attitudes: a cross-sectional study. Front Sports Act Living. (2025) 7:1691151. doi: 10.3389/fspor.2025.1691151,
29. Mehranfar, S, Madani Civi, R, Plunkett, R, Murphy, RA, Cohen, TR, and Conklin, AI. The longitudinal evidence on social ties and fruit and vegetable intake among aging adults: a systematic review. Nutr Rev. (2025) 83:1047–60. doi: 10.1093/nutrit/nuae134,
30. Sandri, E, Pérez-Bermejo, M, Cabo, A, and Cerdá-Olmedo, G. Living alone: associations with diet and health in the Spanish young adult population. Nutrients. (2023) 15:2516. doi: 10.3390/nu15112516,
31. Carbonneau, E, Lamarche, B, Provencher, V, Desroches, S, Robitaille, J, Vohl, M-C, et al. Associations between nutrition knowledge and overall diet quality: the moderating role of sociodemographic characteristics—results from the PREDISE study. Am J Health Promot. (2021) 35:38–47. doi: 10.1177/0890117120928877,
32. Hanslian, E, Schiele, JK, Jeitler, M, Michalsen, A, Wischnewsky, M, Storz, MA, et al. Attitudes toward healthy nutrition in Germany—results from an online-representative cross-sectional survey. Front Nutr. (2025) 11:1480980. doi: 10.3389/fnut.2024.1480980,
33. Fraenkel, JR, and Wallen, NE. How to design and evaluate research in education. New York, New York: McGraw-Hill (2009).
34. Büyüköztürk, Ş, Akgün, ÖE, Demirel, F, Karadeniz, Ş, and Çakmak, EK. Scientific research methods. Ankara, Turkey: Pegem Akademi Yayıncılık. (2015)
35. Faul, F, Erdfelder, E, Buchner, A, and Lang, A-G. Statistical power analyses using G*power 3.1: tests for correlation and regression analyses. Behav Res Methods. (2009) 41:1149–60. doi: 10.3758/BRM.41.4.1149,
37. Öngün Yılmaz, H, Aydın Haklı, D, Toğuç, H, Çobanoğlu, Z, Önel Sayar, C, Erkul, C, et al. Nutrition knowledge scale (NKS): development, factor structure, and validation for healthy adults. Prog Nutr. (2021) 23:e2021104. doi: 10.23751/pn.v23i3.11030
38. Tekkurşun Demir, G, and Cicioğlu, Hİ. Sağlıklı Beslenmeye İlişkin Tutum Ölçeği (SBİTÖ): Geçerlik ve Güvenirlik Çalışması. Gaziantep Üniv Spor Bilim Derg. (2019) 4:256–74. doi: 10.31680/gaunjss.559462
39. Tabachnick, BG, and Fidell, LS. Using multivariate statistics. 7th ed. Boston, MA, USA: Pearson Education. (2019).
40. Cohen, J. The analysis of variance and covariance In: Statistical power analysis for the behavioural sciences. New York: Routledge. (1988)
41. Plaitano, EG, McNeish, D, Bartels, SM, Bell, K, Dallery, J, Grabinski, M, et al. Adherence to a digital therapeutic mediates the relationship between momentary self-regulation and health risk behaviors. Front Digit Health. (2025) 7:1467772. doi: 10.3389/fdgth.2025.1467772,
42. Rahmadhani, APS, Simamora, D, and Sahadewa, S. Relationship between knowledge and attitude of healthy living with healthy behavior patterns in medical students. J Ilm Kedokt Wijaya Kusuma. (2023) 12:7. doi: 10.30742/jikw.v12i1.1955
43. Chaudhary, A, Sudzina, F, and Mikkelsen, BE. Promoting healthy eating among young people—a review of the evidence of the impact of school-based interventions. Nutrients. (2020) 12:2894. doi: 10.3390/nu12092894,
44. Jiang, K, Zhang, L, Xie, C, Li, Z, Shi, Z, Sharma, M, et al. Understanding the knowledge, attitudes, and practices of healthy eating among adolescents in Chongqing, China: an empirical study utilizing structural equation modeling. Nutrients. (2024) 16:167. doi: 10.3390/nu16010167,
45. Meyerhof, H, Jones, CM, and Schüz, B. Intra-individual trajectories of subjectively prioritizing health over other life domains. Appl Psychol Health Well-Being. (2022) 14:1448–63. doi: 10.1111/aphw.12368,
46. Teo, CJH, Burns, SF, and Kawabata, M. Developing nutrition knowledge and attitude measures for athletes with the knowledge–attitude–behavior model. Res Q Exerc Sport. (2023) 94:110–7. doi: 10.1080/02701367.2021.1942771,
47. Chilón-Troncos, RF, García-Salirrosas, EE, Escobar-Farfán, M, Millones-Liza, DY, and Villar-Guevara, M. Predicting willingness to consume healthy brand foods using the theory of planned behavior: the role of nutritional literacy. Front Nutr. (2024) 11:1353569. doi: 10.3389/fnut.2024.1353569,
48. Melo, GLR, Santo, RE, Mas Clavel, E, Bosque Prous, M, Koehler, K, Vidal-Alaball, J, et al. Digital dietary interventions for healthy adolescents: a systematic review of behavior change techniques, engagement strategies, and adherence. Clin Nutr. (2025) 45:176–92. doi: 10.1016/j.clnu.2025.01.012,
49. Haq, I u, Liu, Y, Liu, M, Xu, H, Wang, H, Liu, C, et al. Association of smoking-related knowledge, attitude, and practices (KAP) with nutritional status and diet quality: a cross-sectional study in China. Biomed Res Int. (2019) 2019:1–9. doi: 10.1155/2019/5897478,
Keywords: behavioral clustering, healthy-eating attitudes, nutrition knowledge, physical activity, smoking
Citation: Orhan BE, Alkasasbeh WJ, Karaçam A, Canlı U, Adıgüzel NS and Amawi AT (2026) Nutrition knowledge and healthy-eating attitudes: the role of physical activity and lifestyle factors in adults. Front. Nutr. 13:1754963. doi: 10.3389/fnut.2026.1754963
Edited by:
Krista Austin, Performance & Nutrition Coaching, United StatesReviewed by:
Mack Shelley, Iowa State University, United StatesSepta Puspikawati, Airlangga University, Indonesia
Copyright © 2026 Orhan, Alkasasbeh, Karaçam, Canlı, Adıgüzel and Amawi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Adam Tawfiq Amawi, YS5hbWF3aUBqdS5lZHUuam8=