 Egil Nygaard
Egil Nygaard Venke A. Johansen2,3
Venke A. Johansen2,3 Trond Heir
Trond Heir- 1Department of Psychology, University of Oslo, Oslo, Norway
- 2Resource Centre on Violence, Traumatic Stress and Suicide Prevention, Western Norway (RVTS West), Haukeland University Hospital, Bergen, Norway
- 3Western Norway University of Applied Sciences, Bergen, Norway
- 4Department of Mental Health Services, Akershus University Hospital, Lørenskog, Norway
- 5Institute of Clinical Medicine, University of Oslo, Oslo, Norway
- 6Norwegian Centre for Violence and Traumatic Stress Studies, Oslo, Norway
Self-efficacy is assumed to promote posttraumatic adaption, and several cross-sectional studies support this notion. However, there is a lack of prospective longitudinal studies to further illuminate the temporal relationship between self-efficacy and posttraumatic stress symptoms. Thus, an important unresolved research question is whether posttraumatic stress disorder (PTSD) symptoms affect the level of self-efficacy or vice versa or whether they mutually influence each other. The present prospective longitudinal study investigated the reciprocal relationship between general self-efficacy (GSE) and posttraumatic stress symptoms in 143 physical assault victims. We used an autoregressive cross-lagged model across four assessment waves: within 4 months after the assault (T1) and then 3 months (T2), 12 months (T3) and 8 years (T4) after the first assessment. Stress symptoms at T1 and T2 predicted subsequent self-efficacy, while self-efficacy at T1 and T2 was not related to subsequent stress symptoms. These relationships were reversed after T3; higher levels of self-efficacy at T3 predicted lower levels of posttraumatic stress symptoms at T4, while posttraumatic tress symptoms at T3 did not predict self-efficacy at T4. In conclusion, posttraumatic stress symptoms may have a deteriorating effect on self-efficacy in the early phase after physical assault, whereas self-efficacy may promote recovery from posttraumatic stress symptoms over the long term.
Introduction
Victims of violent physical assault may experience lasting posttraumatic stress symptoms that are sometimes so severe that they meet the diagnostic criteria for PTSD (APA, 2013). In previous articles examining the present sample, the prevalence of probable PTSD was 31% 1 year after a violent assault (Johansen et al., 2007) and 19% after 8 years (Johansen et al., 2013). While many PTSD risk factors (e.g., type and severity of trauma, being female, low socioeconomic status and pre-trauma mental health problems) are well documented (Norris et al., 2002; Ozer et al., 2003), less is known about protective factors. One protective factor may be self-efficacy, that is, “an individual’s belief in their ability to manage their symptoms to unexpected events and to produce desired effects in a given activity” (Bandura, 1997). Self-efficacy is assumed to reduce posttraumatic stress symptoms through engagement in constructive regulation of cognitive, motivational, affective, and decisional processes (Bandura, 1997; Simmen-Janevska et al., 2012). Individuals with high self-efficacy consider anxiety and stress symptoms as controllable and temporary (Cervone, 2000; Leganger et al., 2000). The main aim of this study was to investigate the long-term reciprocal relationship between posttraumatic stress symptoms and general self-efficacy (GSE) after an assault.
Previous studies of posttraumatic stress symptoms and self-efficacy have primarily reported that high self-efficacy is related to lower levels of posttraumatic stress symptoms (Scholz et al., 2002; Luszczynska et al., 2009). If high self-efficacy indeed decreases the severity of posttraumatic stress symptoms, interventions promoting self-efficacy could be helpful for assault victims. However, an important caveat is that most previous research studies are cross-sectional (Luszczynska et al., 2009; Simmen-Janevska et al., 2012). The few existing longitudinal studies have produced mixed findings concerning the temporal relationship between self-efficacy and posttraumatic stress symptoms. Some longitudinal studies of natural disaster survivors found self-efficacy to be related to lower levels of posttraumatic stress symptoms longitudinally (Benight et al., 1999; Benight and Harper, 2002) or to moderate the effect of social support on stress symptoms (Warner et al., 2015). However, we previously found self-efficacy to be related only to concurrent posttraumatic stress symptoms (Johansen et al., 2007) and to be unrelated to posttraumatic stress symptoms beyond 6 months post-disaster (Nygaard et al., 2016). To our knowledge, the only prospective study concerning the temporal relationship between self-efficacy and posttraumatic stress symptoms used three assessments over an 8-month period and found that CSE was significantly related to later reductions in PTSD symptoms, while PTSD symptoms did not predict later reductions in CSE (Bosmans and van der Velden, 2015). Thus, an important unresolved research question is whether PTSD symptoms affect the level of self-efficacy or vice versa or whether they mutually influence each other.
The main aim of this study was to investigate the long-term reciprocal relationship between posttraumatic stress symptoms and GSE after physical assault by investigating the temporal relationship between self-efficacy and posttraumatic stress symptoms in assault victims over an 8-year period. Such a long period is essential because assault victims may experience posttraumatic stress symptoms for an extended period of time (Shalev, 2001; Marshall et al., 2010; Johansen et al., 2013). We hypothesized that higher self-efficacy would promote recovery and be related to the reduced severity of subsequent posttraumatic stress symptoms. A secondary aim was to investigate the stability of GSE over time, which we expected, based on previous studies, to be high, but not high enough to qualify as having trait-like qualities.
Materials and Methods
Design
The present study had a one-group prospective design with 143 physical assault victims. Here, we report the data from four self-reported assessments collected over a period of 8 years combined with the results of a semi-structured interview performed at the first assessment. Most of the respondents (138/143, 97%) completed the initial assessment (T1) between a few days and 16 weeks after the assault, while 5 (3%) completed the assessment more than 16 weeks post-assault. The participants thereafter participated in assessments at 3 months (T2), 12 months (T3), and 8 years (T4) after the first assessment. The flow chart in Figure 1 presents further information about the recruitment procedure.
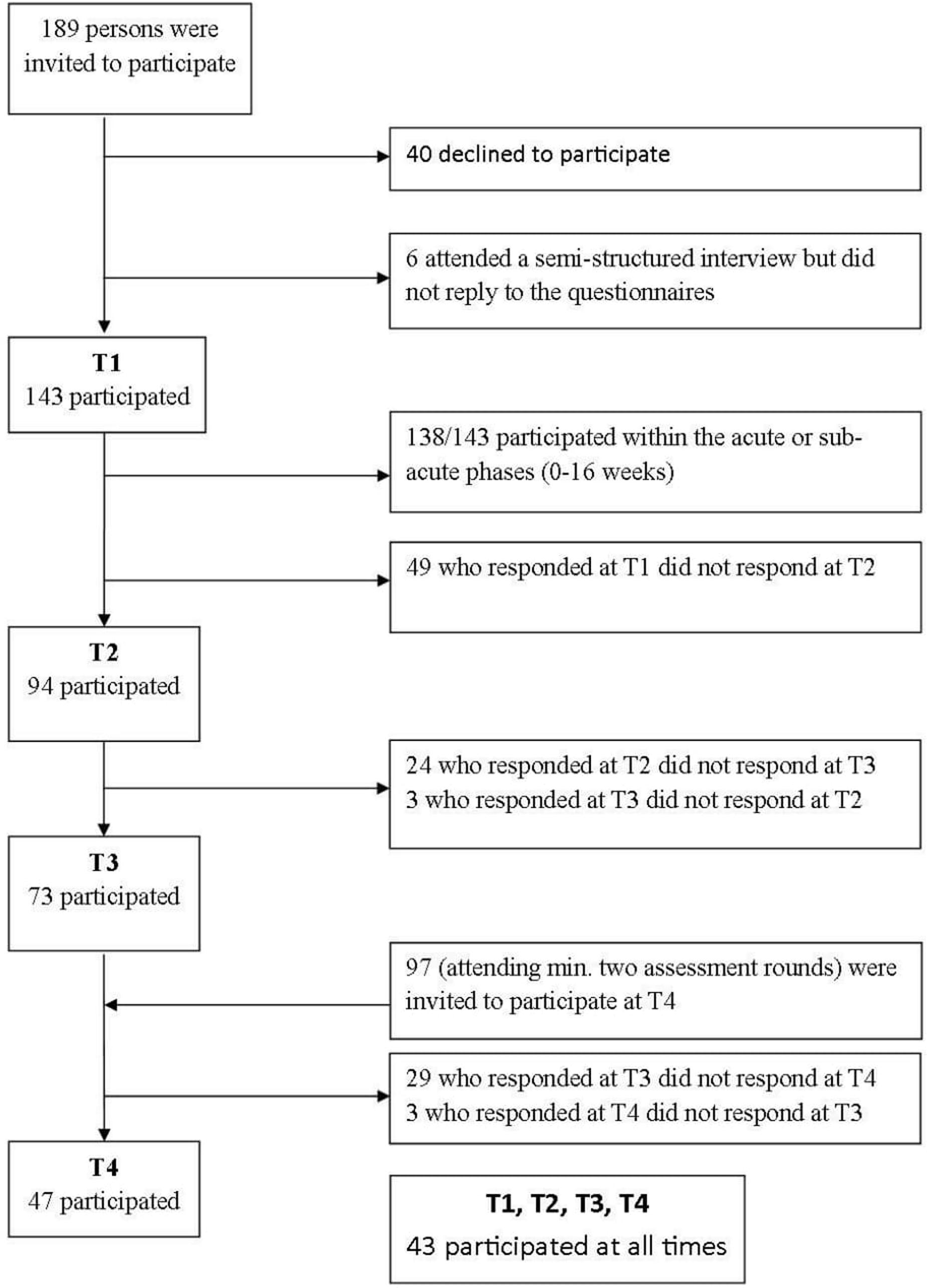
FIGURE 1. Flowchart for inclusion of participants.
Participants and Ethical Approval
All adults receiving care from a medical emergency unit or submitting a police report after being physically assaulted by someone other than a family member or former intimate partner were eligible for inclusion. Potential participants were recruited with the assistance of local police and medical services in the communities of Bergen and Oslo, Norway. All of the participants signed informed consent forms and the study was approved by the regional committee for medical research ethics, West (REK-West, no. 154.01) and by the Privacy Ombudsman, Norwegian Social Science Data Services (NSD, no. 8750). The second author (VJ) conducted all the interviews.
At T1, there were 143 participants, and the response rates were 66% (n = 94) at T2 and 51% (n = 73) at T3. Participants attending at least two out of the first three assessments (n = 97) were invited to participate at T4; the response rate at T4 was 48% (n = 47), or 33% of the original sample (Figure 1).
The majority of the victims were assaulted in a public place (88%) by an unknown perpetrator (93%). At T1, the mean age of the participants was 30.6 years (SD = 11.1), and 80% were male. All participants, except one, were physically injured by the assault. Table 1 provides further descriptive information about the participants at T1, as well as the participants who completed all four assessments. More detailed descriptions of the participants, the crime characteristics and participants’ emotions during the assault have been presented elsewhere (Johansen et al., 2007, 2008).
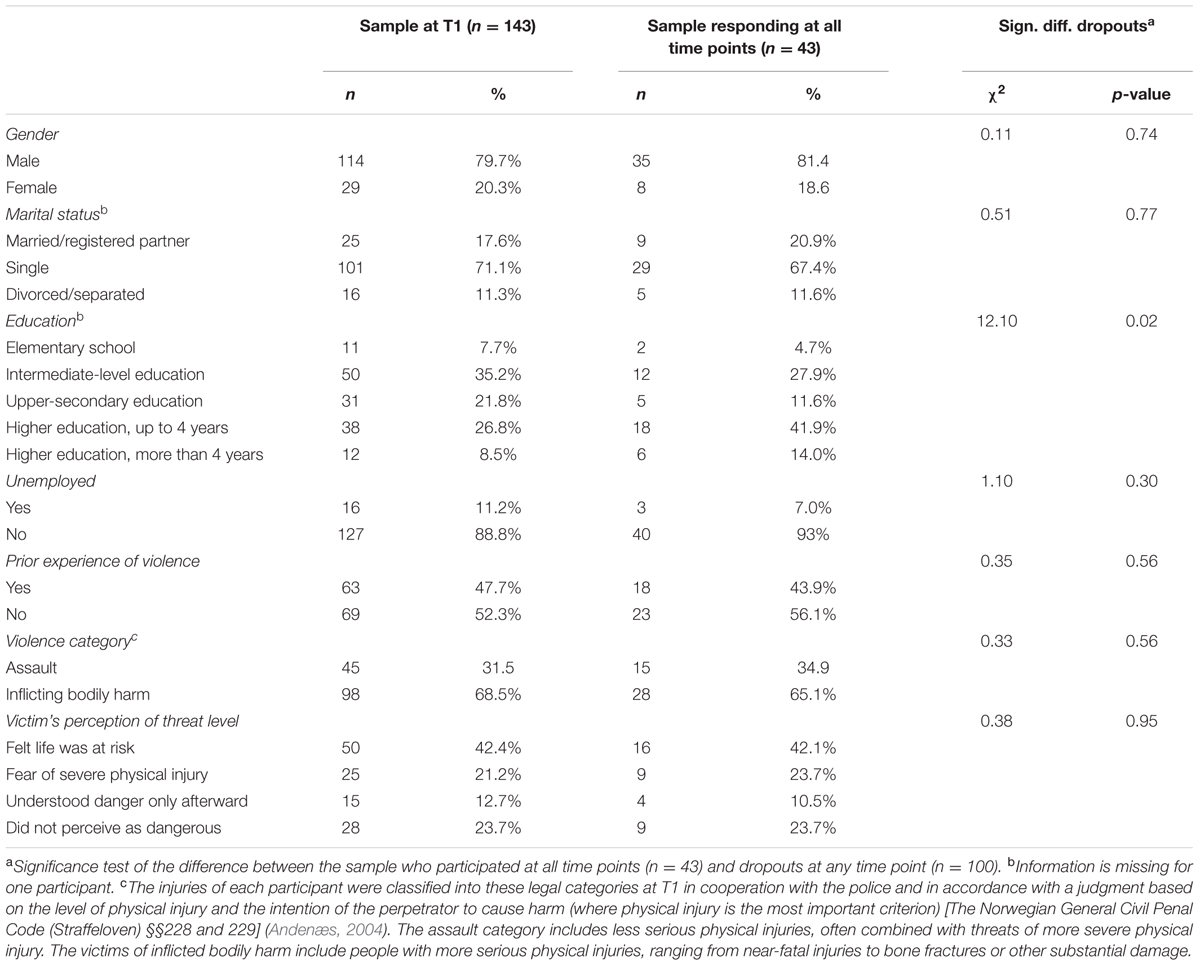
TABLE 1. Descriptive information for participants at T1 (n = 143) and those participating at all time points (n = 43).
No significant differences were found between participants responding at all time points (n = 43) and dropouts at any time (n = 100) in terms of age, gender, prior experience of violence, physical injury, marital status, employment, perceived life threat, alcohol consumption, self-efficacy, or posttraumatic stress symptoms at T1. The participants responding at all time points did, however, have a higher mean education than the dropouts [Mdiff = 0.57, t(140) = 2.83, p = 0.005].
Assessment
Posttraumatic Stress Symptoms
Posttraumatic stress symptoms were assessed using The IES (Weiss and Marmar, 1997), a 22-item self-report questionnaire assessing current levels of intrusion, avoidance, and hyperarousal associated with the experience of a particular traumatic event. The items are scored on a 4-point scale (0 = not at all, 1 = rarely, 3 = sometimes, and 5 = often). The level of overall posttraumatic stress symptoms is reported as the mean of all 22 items, with a higher score representing more severe posttraumatic stress symptoms. Unlike a previous version of the IES (IES-15), there is no generally accepted diagnostic cutoff score for diagnosing PTSD with the version of the IES used in the present study (Creamer et al., 2003).
Perceived Self-efficacy
The Generalized Self-Efficacy Scale (GSE scale) (Schwarzer and Jerusalem, 1995) was used to measure self-perceived GSE. The GSE scale is a 10-item self-report scale with adequate psychometric properties (Schwarzer, 1993; Leganger et al., 2000; Johansen et al., 2013). The GSE scale assesses the respondent’s belief in his or her ability to adequately respond to novel or difficult situations and to cope with a large variety of stressors, and is scored on a 4-point scale from 1 (not at all true) to 4 (exactly true). The total GSE score is the mean score across all 10 items, with higher scores representing higher self-efficacy.
Analyses
Attrition analyses were performed with Student’s t-tests and Pearson’s chi square tests. Stability in self-efficacy and posttraumatic stress symptoms were assessed with Pearson’s correlations and mixed-effects models using a restricted maximum likelihood (REML) estimation in which all available data without any imputations were used. The GSE and IES scores were transformed to Z-values across the four time points, with time defined as a nominal variable. One participant had extreme scores, and the data were therefore re-analyzed without this participant to check for undue influence (see Supplementary Material).
Whether self-efficacy predicted posttraumatic stress symptoms (at time point t) over and above prior posttraumatic stress symptoms (at time point t - 1) was assessed with a series of autoregressive cross-lagged models where the IES and GSE scores at a given time point (t) were simultaneously regressed on the immediately preceding time point (t - 1). These analyses also modeled the opposite relationship: whether posttraumatic stress symptoms (at time point t) predicted self-efficacy over and above prior self-efficacy (at time point t - 1). The models included gender, age and education as covariates because we considered these predictors for GSE and IES at T1.
All autoregressive models were analyzed with the full information maximum likelihood method (FIML) in SPSS AMOS (Schafer and Graham, 2002). The means and intercepts were estimated from the available raw data on a case-wise basis. Consequently, all participants who had participated at least once were included. The overall fit of the models was assessed with χ2 statistics with degrees of freedom and p-values, root mean square error of approximation (RMSEA) with 90% confidence intervals (CIs) and p-values, comparative fit index (CFI), and Tucker-Lewis index (TLI) (Browne and Cudeck, 1992; Hu and Bentler, 1999). The cutoff for acceptable model fit has been suggested to be 0.95 or above for CFI and TLI and from 0.06 to 0.08 or less for RMSEA (Browne and Cudeck, 1992; Hu and Bentler, 1999).
An unconstrained cross-lagged model (A) was compared for best fit with three more constrained models: model B, in which all cross-lagged paths between the GSE and IES were constrained to 0; model C, in which the paths from the prior GSE to later IES were set to 0; and model D, in which the paths from the prior GSE to later IES were set to be similar to the paths from the IES to GSE.
Results
Our first analysis investigated changes in posttraumatic stress symptoms over time. Univariate mixed-effects analyses showed that the level of IES scores (Table 2) changed significantly over time [F(224.8) = 15.8, p < 0.001], with scores at T1, T2, and T3 being higher than scores at T4 (bz-diff = 0.65, 0.46, and 0.42, respectively, all with p < 0.001). The IES scores at each assessment were highly correlated with the IES scores at all other time points (correlations ranged from 0.53 to 0.85, Table 2).
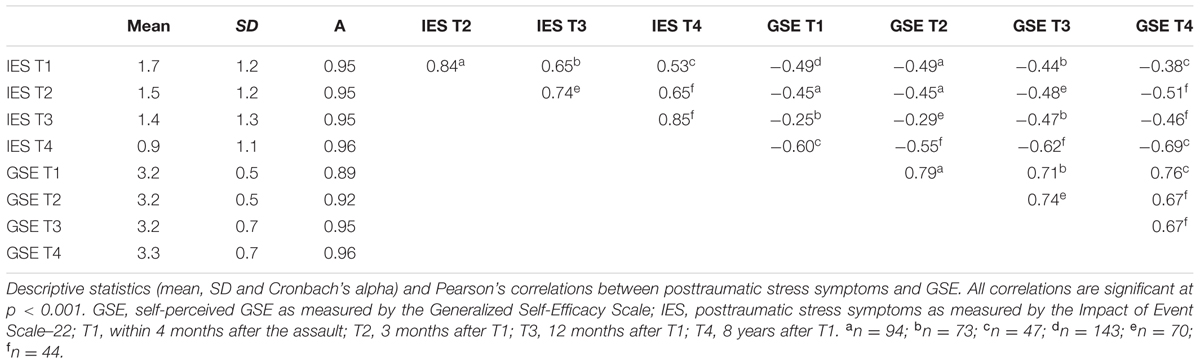
TABLE 2. Descriptive statistics and correlation matrix between posttraumatic stress symptoms and general self-efficacy (GSE) over time.
Our second analysis investigated the level and the stability of participants’ self-efficacy. GSE scores at all time points were highly correlated (between 0.67 and 0.79, Table 2). Many of the participants reported high levels of GSE, and there was a tendency for a ceiling effect. There were, however, also substantial individual differences in the change in GSE scores over time (Figure 2), although the GSE scores were, on average, stable across all four measurements. The main effect of time indicated that the changes in the mean GSE scores from T1 to T4 were not statistically significant [F(233.4) = 1.71, p = 0.17]. The highest levels of GSE were assessed at T4, but the level of GSE at T3 only was significantly lower than that at T4 (bz-diff = -0.23, p = 0.03).
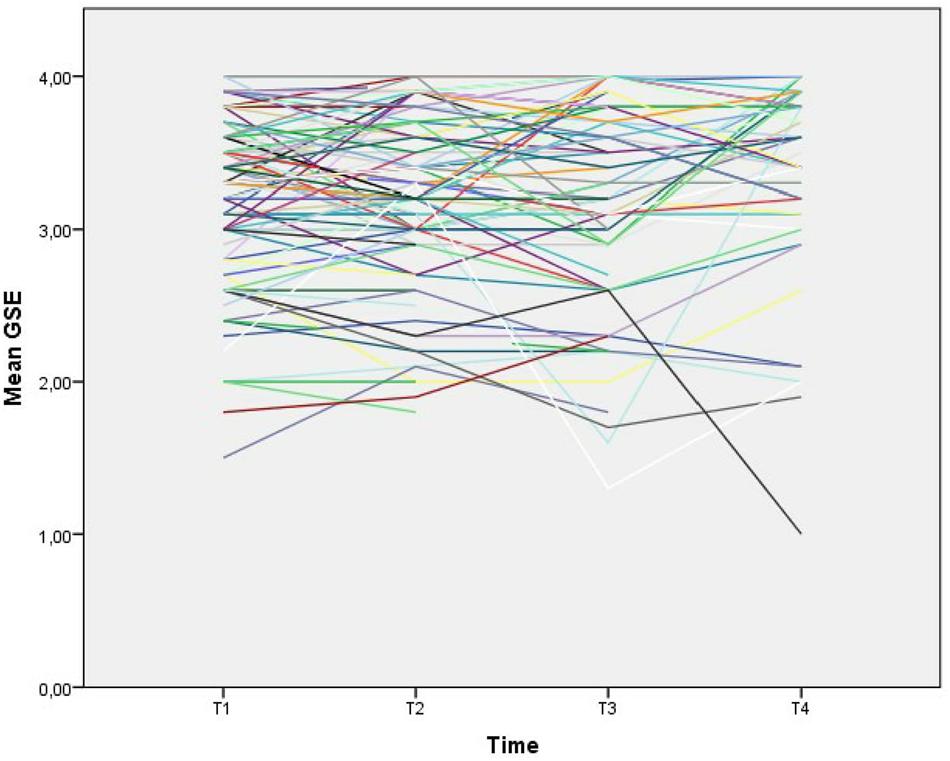
FIGURE 2. Individual levels of self-efficacy over time. Individuals’ mean levels of self-efficacy were measured with the Generalized Self-Efficacy Scale at each assessment point.
GSE and posttraumatic stress symptoms scores at all assessments were significantly negatively correlated, both concurrently (r = -0.45 to -0.69) and longitudinally (r = -0.25 to -0.62) (Table 2), with a tendency for posttraumatic stress symptoms at the last assessment having the highest correlation to self-efficacy at all time points (r = -0.55 to -0.69).
In our last analysis, we modeled the relationship between self-efficacy and posttraumatic stress symptoms across time in a series of autoregressive cross-lagged models. The unconstrained model had adequate model fits: χ2 = 56.38; df = 30; p ≤ 0.002; RMSEA = 0.08; 90% CI = 0.05–0.11; p-close = 0.07; CFI = 0.95; and TLI = 0.89 (Table 3). The RMSEA and TLI values were at or below the recommended cutoff values for model fit. However, these parameters are prone to over-reject true population models for small samples such as ours (Browne and Cudeck, 1992; Hu and Bentler, 1999). CFI was within an acceptable level of model fit.

TABLE 3. Model fits and model comparisons.
The unconstrained model is presented in Figure 3 and Table 4. The cross-lagged parameters from T1 to T2 and from T2 to T3 indicated a significant relationship between prior posttraumatic stress symptoms and later self-efficacy (IES-T1 → GSE-T2 b∗ = -0.15, p = 0.04; IES-T2 → GSE-T3 b∗ = -0.20, p = 0.02) but no significant relationship between prior self-efficacy and later posttraumatic stress symptoms. However, this result was reversed between T3 and T4, where prior self-efficacy was significantly related to later posttraumatic stress symptoms (GSE-T3 → IES-T4 b∗ = -0.23, p = 0.004), whereas posttraumatic stress symptoms at T3 were not significantly related to self-efficacy at T4 (b∗ = -0.18, p = 0.16). The critical ratios (CRs) between the concurrent cross-lagged estimates were all non-significant (CR of the cross-lagged estimates T1 to T2 = -0.52, p = 0.60; CR of the cross-lagged estimates T2 to T3 = 0.90, p = 0.37; CR of the cross-lagged estimates T3 to T4 = 1.83, p = 0.07). Thus, although only one of the cross-lagged estimates was significant at each time point (IES → GSE at T1 to T2 and T2 to T3, and GSE → IES at T3 to T4), the differences between the two concurrent estimates were not significantly different.
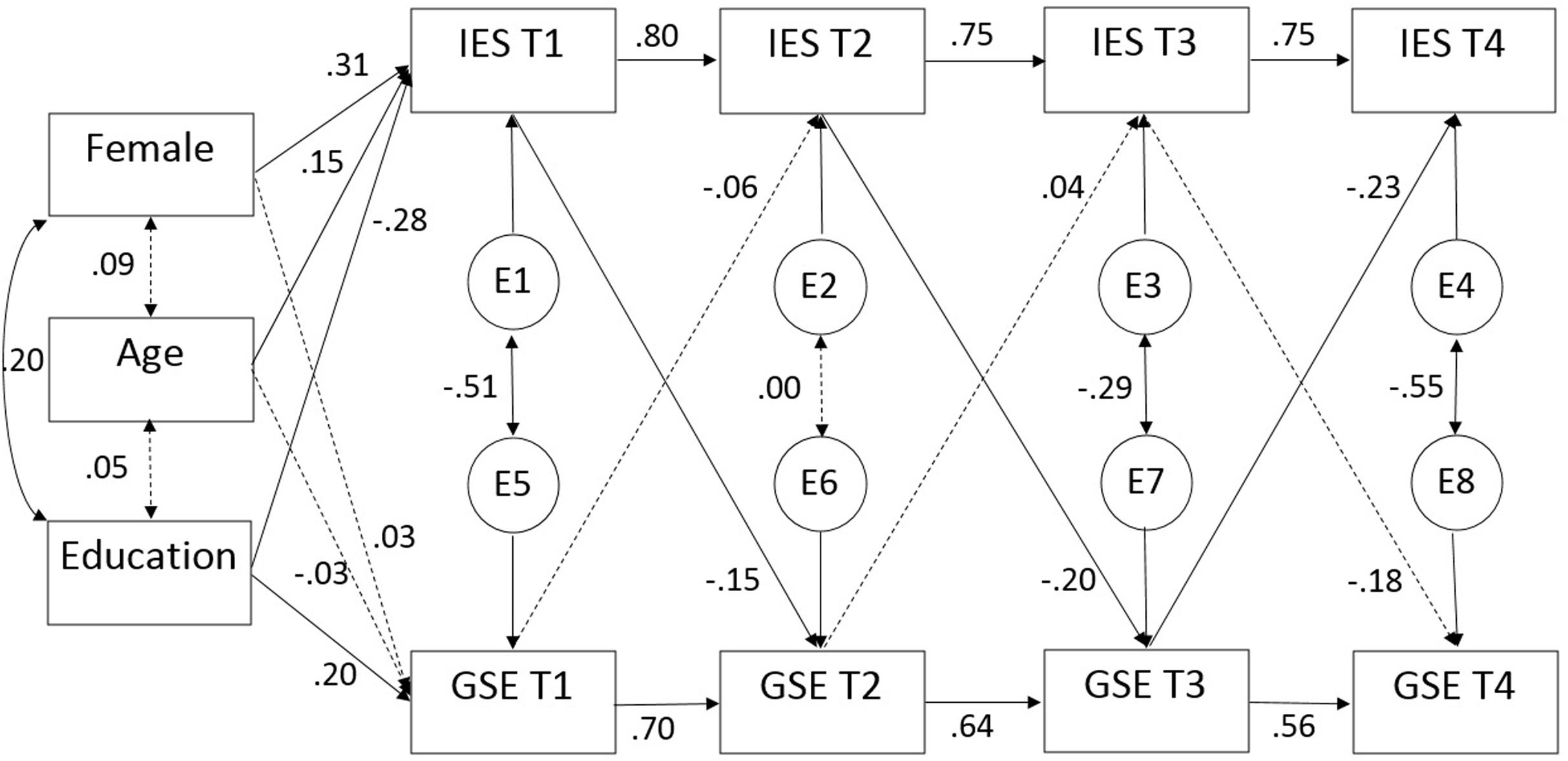
FIGURE 3. Cross-lagged SEM analyses of posttraumatic stress symptoms and self-efficacy across time. Autoregressive cross-lagged SEM analyses with standardized regression weights across four time points. Covariates were restricted to covary only with measures at T1. Insignificant relationships are indicated by dotted lines, whereas continuous lines indicate statistically significant (p < 0.05) relationships. GSE, self-perceived GSE as measured by the Generalized Self-Efficacy Scale; IES, posttraumatic stress symptoms as measured by the Impact of Event Scale-22.
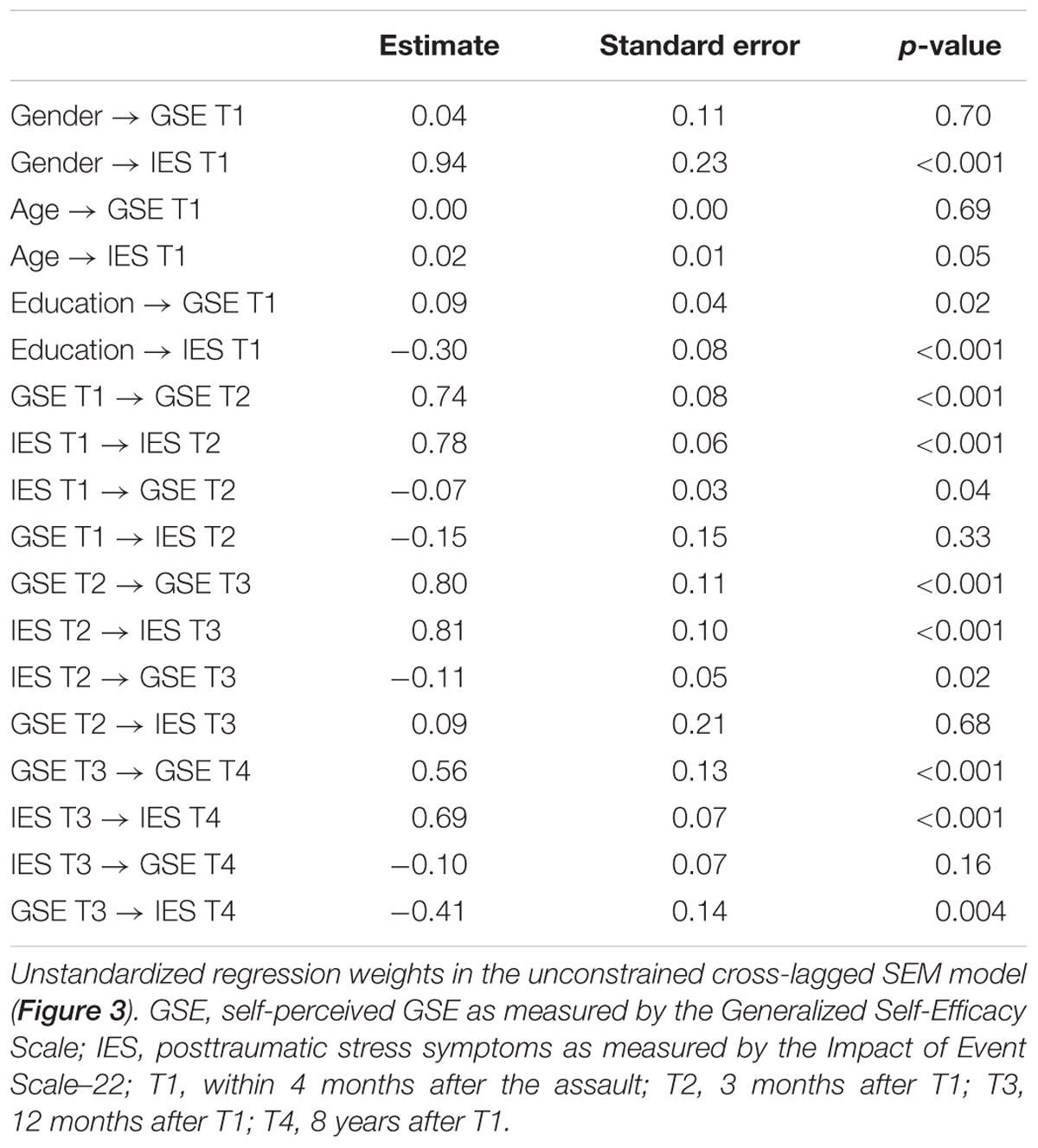
TABLE 4. Regression weights for cross-lagged SEM model of posttraumatic stress symptoms and self-efficacy over time.
The model (Figure 3 and Table 4) indicated high consistency over time for both posttraumatic stress symptoms (standardized regression coefficients b∗ = 0.75 to 80, all p ≤ 0.001) and self-efficacy (b∗ = 0.56 to 0.70, all p ≤ 0.001).
Gender was significantly related to posttraumatic stress symptoms but not to self-efficacy at T1. Women reported a higher level of posttraumatic stress symptoms than men (b∗ = 0.31, p < 0.001) (Table 5). Age was significantly positively related to posttraumatic stress symptoms (b∗ = 0.15, p = 0.05) but not to self-efficacy at T1. Higher education was significantly related to lower posttraumatic stress symptoms (b∗ = -0.28, p < 0.001) and higher levels of self-efficacy (b∗ = 0.20, p = 0.02) at T1.
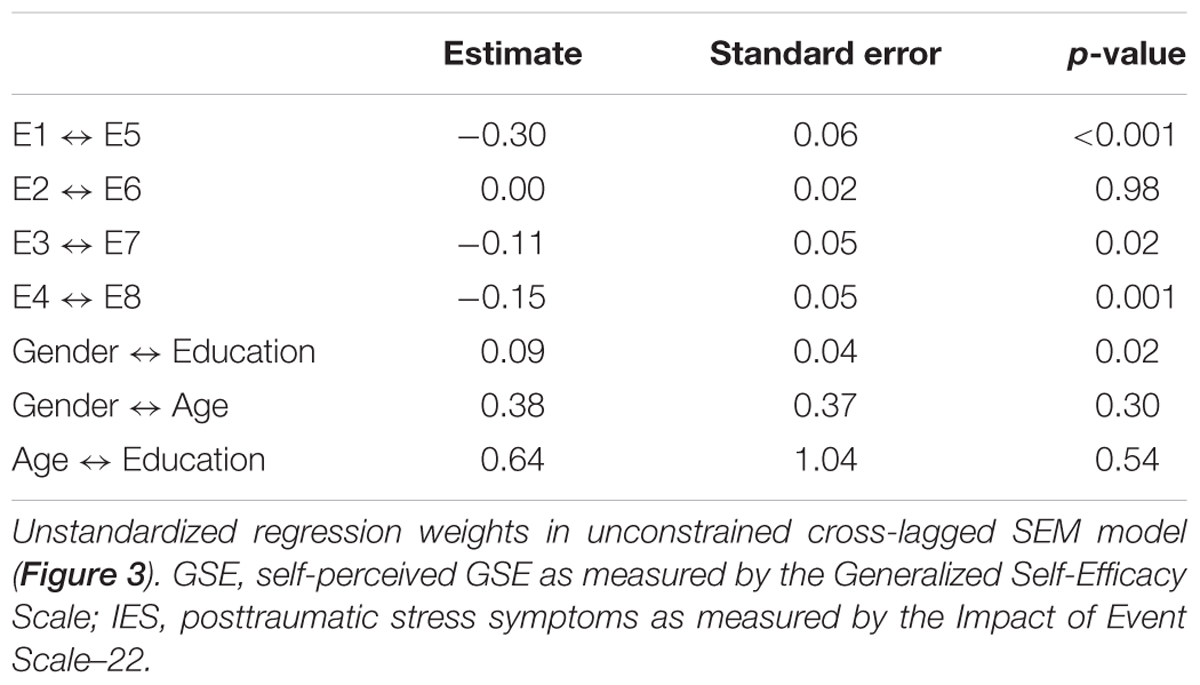
TABLE 5. Regression weights (unstandardized) for covariates in the autoregressive cross-lagged model.
Constraining the model caused changes in model fit. The more constrained model B, with all cross-lagged paths being constrained to equal 0, had worse fit indices (Table 3). Thus, the cross-lagged paths contributed significantly to explaining the GSE and IES scores over time. Moreover, the constrained model C, with the paths from GSE to IES constrained to be equal to 0, showed a worse model fit (Table 3). This finding indicates that the paths from GSE to IES contributed significantly to the model fit in the unconstrained model. However, model D, in which the paths from GSE to IES were set as equal to the paths from IES to GSE, did not have significantly worse fit indices than the unconstrained original model (Table 3), thus indicating that the paths from GSE to IES may not be different from the paths from IES to GSE.
Discussion
The present study examined the relationship between posttraumatic stress symptoms and self-efficacy in assault victims during an 8-year follow-up period. We hypothesized that higher levels of self-efficacy at the first assessment would be related to subsequently lower levels of posttraumatic stress symptoms.
We found levels of bivariate cross-sectional and longitudinal relationships between self-efficacy and posttraumatic stress symptoms that were similar to those reported in previous reviews (Luszczynska et al., 2009; Simmen-Janevska et al., 2012). However, the results are more complex when all the longitudinal aspects and possible reciprocal relationships are considered, and our hypothesis was only partly supported by these longitudinal models. We did not find evidence for an association between self-efficacy and subsequent posttraumatic stress symptoms in the first year after the assault. Higher levels of posttraumatic stress symptoms in the first 3 months after the assault were related to lower levels of self-efficacy at 3 and 12 months post-assault. However, from 12 months to 8 years after the assault, although self-efficacy was negatively associated with subsequent posttraumatic stress symptoms, no evidence was found for the reverse relation.
We were not able to replicate the findings from previous studies showing that self-efficacy is related to lower levels of posttraumatic stress symptoms during the first 12 months after a traumatic incident (Benight and Harper, 2002; Bosmans and van der Velden, 2015). The reason for these divergent findings may be that we investigated generalized self-efficacy, while these prior studies investigated trauma-related coping self-efficacy. However, our findings indicate that GSE may facilitate posttraumatic stress symptom recovery over a longer period, i.e., after 1 year. As expressed by several of our participants during the interviews, during the posttraumatic stress recovery process, it is important to first be aware of and accept one’s own reactions and symptoms; then, as a second step, one should choose strategies to combat these symptoms.
Our novel finding that posttraumatic stress symptoms in the first year after the assault are negatively related to subsequent self-efficacy indicates that cross-sectional relationships (Luszczynska et al., 2009; Simmen-Janevska et al., 2012) may be partially due to a reversed causality between self-efficacy and posttraumatic stress symptoms. Participants’ beliefs in their ability to succeed may have been shattered by the posttraumatic stress symptoms they experienced (Janoff-Bulman, 1992; Nygaard and Heir, 2012). There might also be processes specifically related to being a victim of an assault that are important for these processes. Compared to victims of non-intentional trauma (e.g., natural disasters or accidents), assault victims more often experience a chronic PTSD course (Santiago et al., 2013). In addition to the personal violation, assault victims must address a variety of stressors, such as insurance claims, pain, inability to work, difficult decisions about reporting the trauma to authorities and facing their attacker in court. The waiting time for the case to be processed in the juridical system can also cause substantial stress. The relatively slow recovery process from assault may thus be partly explained by the demands of such ongoing court processes (Osenbach et al., 2009). As one participant in the present study reported in an in-depth interview after 8 years, “I feel that the adverse experience consisted of the entire process, including the court process. Even though what occurred that night was actually the most important part, when I think back on it now, afterward, it feels like the entire first year was part of the experience.” Additionally, some of our victims reported symptom deterioration if the police closed their case or they lost in court. Over time, as the symptom levels decrease and the victims regain confidence in their ability to cope, the influence of self-efficacy on posttraumatic stress symptoms may increase. Our results are partially supported by a study of motor vehicle accident survivors, which reported an increase in self-efficacy levels only among those whose PTSD symptoms were significantly reduced during therapy (Cyniak-Cieciura et al., 2015).
Average self-efficacy was remarkably stable over time, while posttraumatic stress symptoms decreased. The stability of GSE in post-trauma populations is in line with findings from previous studies (Heinrichs et al., 2005; Johansen et al., 2007; Nygaard et al., 2016), and self-efficacy in general may be stable over time (Solomon et al., 1991; Heinrichs et al., 2005; Johansen et al., 2007; Simmen-Janevska et al., 2012) with a trait-like structure (Chen et al., 2001). The trait-like qualities of self-efficacy are corroborated by research on twins indicating that these trait-like qualities might be related to genetic factors (Waaktaar and Torgersen, 2013). Nevertheless, there were some differences in individual trajectories (Figure 2). Furthermore, posttraumatic stress symptoms appeared to have some effect on individual levels of GSE in the first year. Thus, there were also changes in individuals’ self-efficacy levels over time, which were, in part, related to posttraumatic stress symptoms. High levels of posttraumatic stress symptoms may be related to lower self-efficacy in the short term, while other processes related to trauma experiences work in the opposite direction, maintaining a similar mean level of self-efficacy at the group level. However, the present study was not able to disentangle these processes.
The possibility that posttraumatic stress symptoms may lower self-efficacy may have some clinical implications for the ideal time at which to treat stress symptoms. An increased risk of chronic PTSD 5 months post-trauma (Morina et al., 2014) emphasizes the importance of early prevention and treatment. Possible negative consequences of PTSD on self-efficacy in the first year post-trauma substantiate guidelines recommending treatment for PTSD that lasts more than 3 months (NICE, 2005) to accelerate the recovery process and avoid its negative impact on self-efficacy.
Strengths and Limitations
The main strength of our study is the longitudinal design, which allowed cross-lagged statistics. Assessing posttraumatic stress symptoms and perceived self-efficacy at four time points over an 8-year period had not previously been performed. This study design offered the possibility of studying the effects of these variables in short, intermediate, and longer terms.
Another important strength of our study is the homogeneity of the potential traumatic event. All of the respondents were exposed to physical assault by a perpetrator other than a family member. The gender distribution at T1 was representative of exposure to a violent crime (other than domestic assault) in Norway (Steen and Hunskaar, 2004; Statistics Norway, 2009).
The cross-lagged statistical models allowed us to minimize the undesirable effect of confounders. It is, however, important to be aware of the possibility that other models may fit the data equally well (Blunch, 2013). While we compared the fit of the proposed cross-lagged model (A) with that of three other theoretically relevant models, future research may identify other models fitting the data equally well or better. Furthermore, to improve the validation of our study by minimizing recall bias, we performed the interviews at T1 as soon as possible after the event. We also knew the exact date of exposure and the elapsed time from the exposure to the interview for all participants.
The prime methodological limitation of this study is the small sample size; only 43 participants completed all the assessments over the full 8 years. Small sample sizes and high dropout levels are a common problem in longitudinal studies of assault victims (Shalev et al., 1998; Andrews et al., 2003; Brewin et al., 2003; Elklit and Brink, 2004). Fourteen of the 143 invited participants at T3 and 10 of the 97 invited participants at T4 could not be reached by mail due to unknown addresses. However, the respondents at all time points (n = 43) were comparable to the dropouts in all respects except the level of education. All information given by any participant at any time was included in the model analyses, thus reducing the dropout effect.
Both the IES and the GSE scale are among the most-used questionnaires for measuring posttraumatic stress symptoms and self-efficacy, and they have been found to be both reliable and valid measures (Schwarzer, 1993; Leganger et al., 2000; Creamer et al., 2003). An advantage of using self-reports at all time points is that their dimensional view provided information on relative changes in posttraumatic stress symptoms and self-efficacy over time.
There may be discrepancies between studies of GSE, such as the present study, and studies of CSE. Whereas GSE is the belief in one’s competence to tackle novel tasks and to cope with adversity over a broad range of stressful or challenging encounters, specific self-efficacy or CSE is constrained to the belief in one’s ability to cope with a particular task. Parts of some measures of trauma CSE may therefore be quite similar to posttraumatic stress cognitions and symptoms, just with the opposite sign. Finally, specific trauma-related beliefs about coping are more closely related to PTSD symptoms in the first months after the trauma, while the effect of GSE is more prominent over longer periods (Cyniak-Cieciura et al., 2015).
We have no nuanced information about the pharmacological and/or psychological treatments the participants may have received, their duration, or their effects. Victims exposed to non-domestic violence are typically not systematically offered follow-up treatment through the Norwegian public health service.
Conclusion
The relationship between GSE and posttraumatic stress symptoms seems to be complex; these constructs can affect each other over the course of many years. From a long-term perspective, strengthening GSE can have effects on posttraumatic stress symptoms in trauma survivors, assuming that GSE is actually responsive to intervention. Further research is needed to determine whether GSE can be altered externally over time. Our study shows that many assault victims have high levels of posttraumatic stress symptoms after as long as 8 years. Further research is necessary to identify measures that can help this group and determine how effective interventions can be performed.
Author Contributions
EN analyzed and interpreted the data and drafted the manuscript. VJ designed the study and acquired the data. VJ, JS, AH, and TH contributed substantially to the interpretation of the data and drafting of the manuscript, and they revised the manuscript critically for important intellectual content. All authors have approved the final version of the manuscript and have agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank the local police and the local outpatient workers in Bergen and Oslo for assisting with the recruitment of assault victims. We also thank Tore Wentzel-Larsen for statistical advice and Irmelin B. Christensen for her contribution by contacting the participants again after 8 years.
Supplementary Material
The Supplementary Material for this article can be found online at: http://journal.frontiersin.org/article/10.3389/fpsyg.2017.00913/full#supplementary-material
Abbreviations
CSE, coping self-efficacy; GSE, general self-efficacy; IES, Impact of Event Scale–22; PTSD, posttraumatic stress disorder.
References
Andenæs, J. (2004). Alminnelig Strafferett. 5. Utgave ved Magnus Matningsdal og Georg Fr. Rieber-Mohn. Oslo: Universitetsforlaget.
Andrews, B., Brewin, C. R., and Rose, S. (2003). Gender, social support, and PTSD in victims of violent crime. J. Trauma Stress 16, 421–427. doi: 10.1023/A:1024478305142
APA (2013). Diagnostic and Statistical Manual of Mental Disorders DSM-5, 5th Edn. Arlington, VA: American Psychiatric Association.
Benight, C. C., and Harper, M. L. (2002). Coping self-efficacy perceptions as a mediator between acute stress response and long-term distress following natural disasters. J. Trauma Stress 15, 177–186. doi: 10.1023/A:1015295025950
Benight, C. C., Ironson, G., Klebe, K., Carver, C. S., Wynings, C., Burnett, K., et al. (1999). Conservation of resources and coping self-efficacy predicting distress following a natural disaster: a causal model analysis where the environment meets the mind. Anxiety Stress Coping 12, 107–126. doi: 10.1080/10615809908248325
Blunch, N. J. (2013). Introduction to Structural Equation Modeling Using IBM SPSS Statistics and AMOS, 2nd Edn. London: Sage Publications Ltd.
Bosmans, M. W. G., and van der Velden, P. G. (2015). Longitudinal interplay between posttraumatic stress symptoms and coping self-efficacy: a four-wave prospective study. Soc. Sci. Med. 134, 23–29. doi: 10.1016/j.socscimed.2015.04.007
Brewin, C. R., Andrews, B., and Rose, S. (2003). Diagnostic overlap between acute stress disorder and PTSD in victims of violent crime. Am. J. Psychiatry 160, 783–785.
Browne, M. W., and Cudeck, R. (1992). Alternative ways of assessing model fit. Sociol. Methods Res. 21, 230–258. doi: 10.1177/0049124192021002005
Cervone, D. (2000). Thinking about self-efficacy. Behav. Modif. 24, 30–56. doi: 10.1177/0145445500241002
Chen, G., Gully, S. M., and Eden, D. (2001). Validation of a new general self-efficacy scale. Organ. Res. Methods 4, 62–83. doi: 10.1177/109442810141004
Creamer, M., Bell, R., and Failla, S. (2003). Psychometric properties of the impact of event scale - revised. Behav. Res. Ther. 41, 1489–1496. doi: 10.1016/j.brat.2003.07.010
Cyniak-Cieciura, M., Popiel, A., and Zawadzki, B. (2015). General self-efficacy level and changes in negative posttraumatic cognitions and posttraumatic stress disorder (PTSD) symptoms among motor vehicle accident survivors after PTSD therapy. Stud. Psychol. 53, 18–29. doi: 10.2478/V10167-010-0117-8
Elklit, A., and Brink, O. (2004). Acute stress disorder as a predictor of post-traumatic stress disorder in physical assault victims. J. Interpers. Violence 19, 709–726. doi: 10.1177/0886260504263872
Heinrichs, M., Wagner, D., Schoch, W., Soravia, L. M., Hellhammer, D. H., and Ehlert, U. (2005). Predicting posttraumatic stress symptoms from pretraumatic risk factors: a 2-year prospective follow-up study in firefighters. Am. J. Psychiatry 162, 2276–2286. doi: 10.1176/appi.ajp.162.12.2276
Hu, L.-T., and Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct. Equ. Model. 6, 1–55. doi: 10.1080/10705519909540118
Janoff-Bulman, R. (1992). Shattered Assumptions: Towards a New Psychology of Trauma. New York, NY: Free press.
Johansen, V. A., Eilertsen, D. E., Nordanger, D., and Weisaeth, L. (2013). Prevalence, comorbidity and stability of post-traumatic stress disorder and anxiety and depression symptoms after exposure to physical assault: an 8-year prospective longitudinal study. Nord. J. Psychiatry 67, 69–80. doi: 10.3109/08039488.2012.732112
Johansen, V. A., Wahl, A. K., Eilertsen, D. E., and Weisaeth, L. (2007). Prevalence and predictors of post-traumatic stress disorder (PTSD) in physically injured victims of non-domestic violence - A longitudinal study. Soc. Psychiatry Psychiatr. Epidemiol. 42, 583–593. doi: 10.1007/s00127-007-0205-0
Johansen, V. A., Wahl, A. K., and Weisaeth, L. (2008). Assaulted victims of nondomestic violence in Norway - injury, crime characteristics and emotions during the assault. Scand. J. Caring Sci. 22, 445–454. doi: 10.1111/j.1471-6712.2007.00550.x
Leganger, A., Kraft, P., and Roysamb, E. (2000). Perceived self-efficacy in health behaviour research: conceptualisation, measurement and correlates. Psychol. Health 15, 51–69. doi: 10.1080/08870440008400288
Luszczynska, A., Benight, C. C., and Cieslak, R. (2009). Self-efficacy and health-related outcomes of collective trauma a systematic review. Eur. Psychol. 14, 51–62. doi: 10.1027/1016-9040.14.1.51
Marshall, G. N., Miles, J. N. V., and Stewart, S. H. (2010). Anxiety sensitivity and PTSD symptom severity are reciprocally related: evidence from a longitudinal study of physical trauma survivors. J. Abnorm. Psychol. 119, 143–150. doi: 10.1037/a0018009
Morina, N., Wicherts, J. M., Lobbrecht, J., and Priebe, S. (2014). Remission from post-traumatic stress disorder in adults: a systematic review and meta-analysis of long term outcome studies. Clin. Psychol. Rev. 34, 249–255. doi: 10.1016/j.cpr.2014.03.002
NICE (2005). NICE Clinical Guideline on Post-Traumatic Stress Disorder. Available at: http://www.nice.org.uk/Guidance/CG26
Norris, F. H., Friedman, M. J., Watson, P. J., Byrne, C. M., Diaz, E., and Kaniasty, K. (2002). 60,000 disaster victims speak: part I. An empirical review of the empirical literature, 1981-2001. Psychiatry 65, 207–239. doi: 10.1521/psyc.65.3.207.20173
Nygaard, E., and Heir, T. (2012). World assumptions, posttraumatic stress and quality of life after a natural disaster: a longitudinal study. Health Qual. Life Outcomes 10:76. doi: 10.1186/1477-7525-10-76
Nygaard, E., Hussain, A., Siqveland, J., and Heir, T. (2016). General self-efficacy and posttraumatic stress after a natural disaster: a longitudinal study. BMC Psychol. 4:15. doi: 10.1186/s40359-016-0119-2
Osenbach, J. E., Stubbs, J., Wang, J., Russo, J., and Zatzick, D. (2009). Legal events as predictors of posttraumatic stress in injured trauma survivors. Psychiatry 72, 70–78. doi: 10.1521/psyc.2009.72.1.70
Ozer, E. J., Best, S. R., Lipsey, T. L., and Weiss, D. S. (2003). Predictors of posttraumatic stress disorder and symptoms in adults: a meta-analysis. Psychol. Bull. 129, 52–73. doi: 10.1037/0033-2909.129.1.52
Santiago, P. N., Ursano, R. J., Gray, C. L., Pynoos, R. S., Spiegel, D., Lewis-Fernandez, R., et al. (2013). A systematic review of PTSD prevalence and trajectories in DSM-5 defined trauma exposed populations: intentional and non-intentional traumatic events. PLoS ONE 8:e59236. doi: 10.1371/journal.pone.0059236
Schafer, J. L., and Graham, J. W. (2002). Missing data: our view of the state of the art. Psychol. Methods 7, 147–177. doi: 10.1037/1082-989X.7.2.147
Scholz, U., Dona, B. G., Sud, S., and Schwarzer, R. (2002). Is general self-efficacy a universal construct? Psychometric findings from 25 countries. Eur. J. Psychol. Assess. 18, 242–251. doi: 10.1027//1015-5759.18.3.242
Schwarzer, R. (1993). Measurement of Perceived Self-efficacy: Psychometric Scales for Cross-cultural Research. Berlin: Free Universität Berlin.
Schwarzer, R., and Jerusalem, M. (1995). “Generalized self-efficacy scale,” in Measures in Health Psychology: A User’s Portfolio. Causal and Control Beliefs, eds J. Weinman, S. Wright, and M. Johnston (Windsor: nferNelsen), 35–37.
Shalev, A. Y. (2001). Post-traumatic stress disorder - Disorder takes away human dignity and character. Br. Med. J. 322, 1301–1301. doi: 10.1136/bmj.322.7297.1301
Shalev, A. Y., Freedman, S., Peri, T., Brandes, D., Sahar, T., Orr, S. P., et al. (1998). Prospective study of posttraumatic stress disorder and depression following trauma. Am. J. Psychiatry 155, 630–637. doi: 10.1176/ajp.155.5.630
Simmen-Janevska, K., Brandstatter, V., and Maercker, A. (2012). The overlooked relationship between motivational abilities and posttraumatic stress: a review. Eur. J. Psychotraumatol. 3:18560. doi: 10.3402/ejpt.v3i0.18560
Solomon, Z., Benbenishty, B., and Mikulincer, M. (1991). The contribution of wartime, pre-war, and post-war factors to self-efficacy: a longitudinal study of combat stress reaction. J. Trauma Stress 4, 345–361. doi: 10.1002/jts.2490040304
Statistics Norway (2009). Crime Statistics 2008. Available at: https://www.ssb.no/sosiale-forhold-og-kriminalitet/statistikker/lovbruddo/aar/2009-06-24#content
Waaktaar, T., and Torgersen, S. (2013). Self-efficacy is mainly genetic, not learned: a multiple-rater twin study on the causal structure of general self-efficacy in young people. Twin Res. Hum. Genet. 16, 651–660. doi: 10.1017/thg.2013.25
Warner, L. M., Gutierrez-Dona, B., Villegas Angulo, M., and Schwarzer, R. (2015). Resource loss, self-efficacy, and family support predict posttraumatic stress symptoms: a 3-year study of earthquake survivors. Anxiety Stress Coping 28, 239–253. doi: 10.1080/10615806.2014.955018
Keywords: assault, autoregressive cross-lagged, longitudinal, posttraumatic stress symptoms, PTSD, self-efficacy
Citation: Nygaard E, Johansen VA, Siqveland J, Hussain A and Heir T (2017) Longitudinal Relationship between Self-efficacy and Posttraumatic Stress Symptoms 8 Years after a Violent Assault: An Autoregressive Cross-Lagged Model. Front. Psychol. 8:913. doi: 10.3389/fpsyg.2017.00913
Received: 10 March 2017; Accepted: 17 May 2017;
Published: 01 June 2017.
Edited by:
Lorys Castelli, University of Turin, ItalyReviewed by:
Taiwo Lateef Sheikh, Federal Neuropsychiatric Hospital, NigeriaAlexander Neumeister, Institute of Mental Health Research at The Royal Ottawa, Canada
Copyright © 2017 Nygaard, Johansen, Siqveland, Hussain and Heir. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Egil Nygaard, ZWdpbG55QHBzeWtvbG9naS51aW8ubm8=