 Yu Yu1
Yu Yu1 Zi-wei Liu
Zi-wei Liu Xing-yu Zhang
Xing-yu Zhang Shui-yuan Xiao
Shui-yuan Xiao- 1Xiangya School of Public Health, Central South University, Changsha, China
- 2Mental Health Institute of the Second Xiangya Hospital, National Clinical Research Center on Mental Disorders & National Technology Institute on Mental Disorders, Hunan Key Laboratory of Psychiatry and Mental Health, Central South University, Changsha, China
- 3Xiangya Hospital, Central South University, Changsha, China
- 4Traditional Chinese Medical Hospital of Ya'an, Sichuan, China
Objective: Although various short forms of Zarit Burden Interview (ZBI) have been developed, there is a lack of standard psychometric testing and comparison among them. The study aims to examine the psychometric properties of ten short versions of the most frequently used ZBI among a sample of schizophrenia caregivers and to find the one with the best performance.
Methods: Cross-sectional door-to-door survey of ZBI-22 and a series of validated instrument data from 327 family caregivers of schizophrenia patients in a Chinese rural community were conducted from October 2015 to January 2016. Reliability was assessed using McDonald's omega coefficient (ω). Validity including concurrent validity, known group's validity, and criterion validity were assessed by Spearman correlations and Mann-Whitney U tests. Overall discrimination ability was evaluated using the area under the receiver operating characteristic curve (AUC).
Results: Reliability was generally good for all short forms (ω = 0.69–0.84), except for the Gort ZBI-4 (ω = 0.58), which is acceptable considering its small item numbers. Concurrent validity was good across all various ZBI forms with significant negative correlations with patient's function (r = −0.34 to −0.48, p < 0.01), as well as significant positive correlations with caregiver's depression (r = 0.49–0.65, p < 0.01), and anxiety symptoms (r = 0.45–0.58, p < 0.01). Known groups' validity (carers with disease vs. without disease; carers being parents vs. spouse vs. others) showed inconsistent results among various short forms. Criterion validity was generally good for all short forms with significant positive correlations with Family Burden Interview Schedule (r = 0.67–0.75, p < 0.01), except for the Higginson ZBI-1(r = 0.57, p < 0.01). Discriminative ability was also good for all short forms (AUC range: 0.85–0.99), with various cutpoints proposed. Among all ten short forms, the Ballesteros ZBI-12 and the Gort ZBI-7 outperformed others with almost equally good performance in comprehensive psychometric testing.
Conclusions: This study provides support for the reliability, validity, and discriminative ability of the ten various short forms of ZBI for use among schizophrenia family caregivers, with the Ballesteros ZBI-12 and the Gort ZBI-7 endorsed as the best ones.
Introduction
The Zarit Burden Interview (ZBI) is one of the oldest and most commonly used instruments for assessing caregiving burden at an international level (Knight et al., 2000). Initially developed more than 30 years ago, the ZBI was intended to measure burden and stress experienced by caregivers caring for people with dementia with 29 items on a four-point Likert type scale (Zarit et al., 1980). A revised ZBI (Zarit et al., 1985a,b) was later introduced with 22 items on a five-point Likert type scale, which has been widely translated into various languages, and validated across countries and cultures, such as Europe (Braun et al., 2010; Martin-Carrasco et al., 2010; Chattat et al., 2011), Africa (Imarhiagbe et al., 2017) and Asian countries like China (Wang et al., 2008; Lu et al., 2009) and Japan (Hirono et al., 1998) allowing for international comparison. Evidence also shows that the ZBI can be interpreted similarly across gender or across educational level (Lin et al., 2017a). Furthermore, a meta-analytic study has proved that the ZBI are reliable across populations of caregivers (i.e., spouses/partners, children, and parents), care-recipients (i.e., AD/dementia, physical illness, and mental illness), and most language versions (e.g., French, Spanish, and Chinese) (Bachner and O'Rourke, 2007).
The widespread use of ZBI in both research and clinical settings worldwide has fostered interest in simplification of the 22-item scale for ease of administration, minimization of respondent burden, and quick screening in busy occasions (Lin et al., 2017b). A number of short forms of ZBI have been proposed, with the number of items ranging from 1 to 14, as shown in Table 1. All those short forms are developed or assessed either by using classical test theory or item response theory, with theory-guided choice of item selection. Comparison of various abridged versions of ZBI have been conducted with consistent findings supporting for the reliability and validity of various short forms, while uniformly endorsing as the best one either the Bedard 12-item ZBI (Higginson et al., 2010; Hagell et al., 2017) or the Ballesteros 12-item ZBI (Lin et al., 2017b).
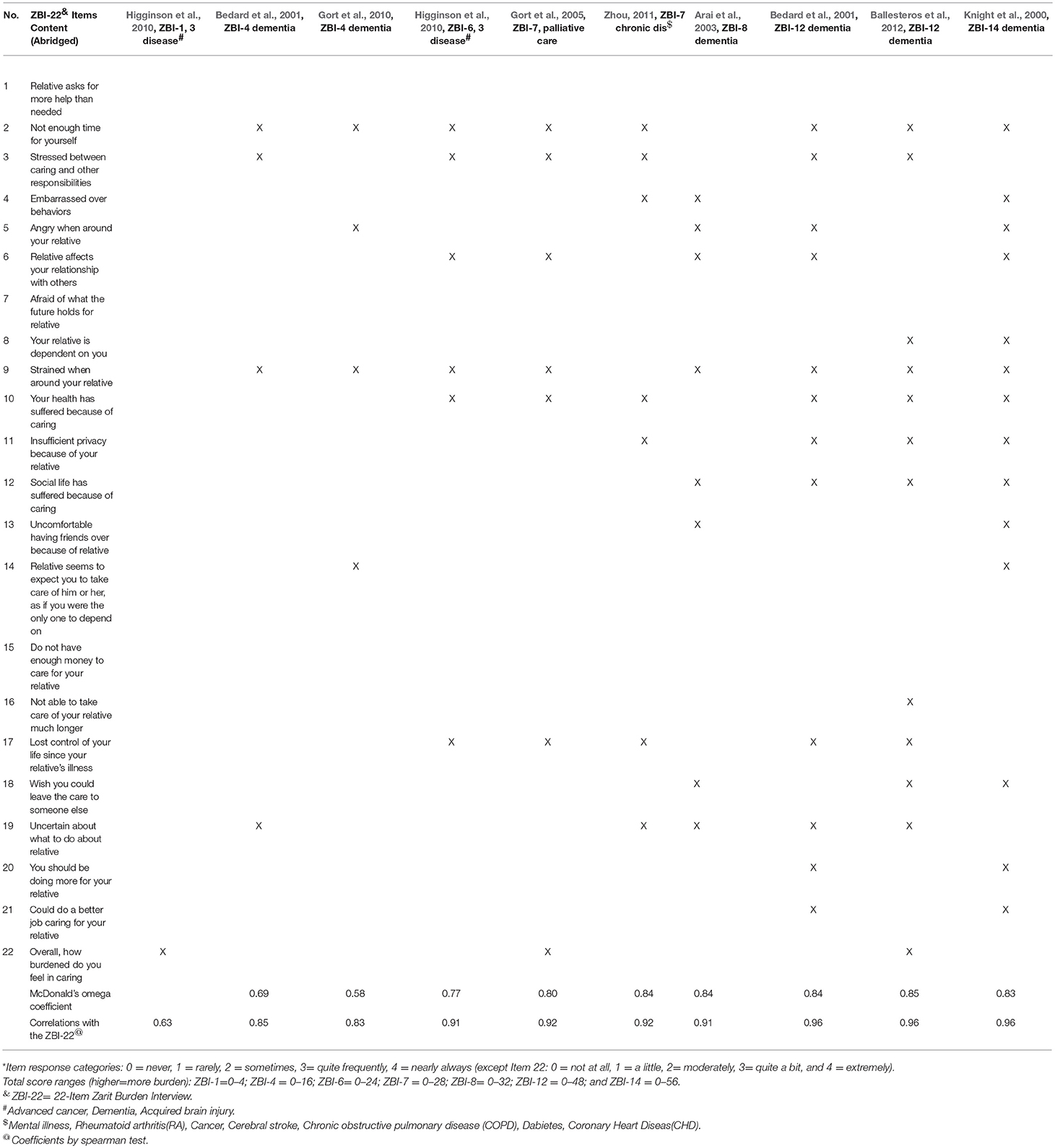
Table 1. Items included in the short forms of the Zarit Burden Interview*.
However, these previous performance comparisons fall short in four key aspects: First, among all ten short forms reported in the literature, only six versions have been assessed, rendering the comparison incomplete, and inconclusive (Higginson et al., 2010; Hagell et al., 2017; Lin et al., 2017b). Secondly, the majority of short forms were developed and tested in a population of dementia caregivers, little evidence exists on their psychometric properties among caregivers of mental illness, although the full 22-item form has already been widely used, and validated among such a population (Higginson et al., 2010; Flynn Longmire and Knight, 2011; Tang et al., 2016; Hagell et al., 2017; Lin et al., 2017b). Thirdly, previous validity tests were based on comparison between short forms of ZBI with self-designed questions, such as informal care hours and financial situations (Lin et al., 2017b), or using the full 22-item version as a self-comparison (Higginson et al., 2010), instead of standardized or validated instrument, thus weakening the robustness of validity results. Lastly, although the 12-item ZBI has been tested as having the best performance in previous studies that were mostly conducted in western countries (O'Rourke and Tuokko, 2003; Higginson et al., 2010; Hagell et al., 2017), it does not incorporate some cultural-sensitive salient concept in Asian societies (Lim et al., 2014), which may limit its use across countries that share similar Confusianism traditions (e.g., Japan, South Korea, and China) (Zhou et al., 2016; Lin et al., 2017b).
In light of the above-mentioned limitations of previous studies, the present study was conducted with the purpose of reassessing the psychometric properties of ten short forms of ZBI-22 among Chinese family caregivers of people with schizophrenia using a series of standardized or validated instrument for validity test.
Materials and Methods
Participants and Procedure
This is a descriptive, cross-sectional study with partial data coming from the research entitled “Family burden and caregiving experiences of schizophrenia in Chinese rural communities” (Yu et al., 2017), conducted in Ningxiang County, Hunan Province of China. The research recruited a sample of 352 primary caregiver s of schizophrenia through China's first program for treatment and management of serious mental illness (“Central Government Support for the Local Management and Treatment of Severe Mental Illnesses Project,” 686 Project) (Ma, 2012). The care recipient must be registered in the 686 Program and fulfilling the Chinese Classification of Mental Disorders-3(CCMD-3) or the International Classification of Diseases-10 (ICD-10) criteria for schizophrenia as diagnosed by special psychiatrist. The primary caregiver must be a family member who is living with the patient and taking the most responsibility of caring, 16 years old or above, and able to understand and communicate. After excluding 14 participants who refused to participate and 11 withdrawals, our final sample included 327 community-dwelling primary caregivers of patients with schizophrenia.
Data collection was conducted from October 2015 to January 2016. A team of nine post-graduates from the School of Public Health of Central South University were recruited as interviewers. The interviewers have a background of public health, psychology or psychiatry. All interviewers received a 1-week uniform formal training to conduct the interviews provided by a psychologist before the formal study. The training was composed of half lecturing and half practice of role plays. All subjects gave written informed consent in accordance with the Declaration of Helsinki. The protocol was approved by the Institutional Review Board of the Xiangya School of Public Health of Central South University. We paid door-to-door visit at the primary caregivers' home and conducted face-to-face interviews with them for an average duration of 50–70 min, after obtaining written consent from primary caregivers for the study. Details of the study enrollment and procedure have been published elsewhere (Yu et al., 2017).
Instruments
Zarit Burden Interview (ZBI)
The ZBI-22 (Table 1) consists of 22 items scored in 5-point Likert scale from 0 (never) to 4 (nearly always), except for the final item on global burden, rated from 0 (not at all) to 4 (extremely). The total score ranges from 0 to 88 with higher scores indicating higher burden. In addition, several short forms of the ZBI-22 have been proposed as a rapid screening tool, which are scored according to the same principle as the original ZBI-22. These short forms include: the 14-item ZBI by Knight et al. (2000), two different 12-item ZBIs by Ballesteros et al. (2012) and Bedard et al. (2001), the 8-item ZBI by Arai et al. (2003), two different 7-item ZBIs by Zhou (2011) and Gort et al. (2005), the 6-item ZBI by Higginson et al. (2010), two different 4-item ZBIs by Gort et al. (2010) and Bedard et al. (2001), and finally, 1-item ZBI by Higginson et al. (2010) (Table 1). In the present study, the Chinese version of ZBI showed acceptable internal consistency with a McDonald's ω coefficient of 0.89.
Family Burden Interview Schedule (FBIS)
The FBIS (Pai and Kapur, 1981) was used to assess family burden and consists of 24 items rated on a 3-point Likert scale from 0 (no burden) to 2 (serious burden). The total scores range from 0 to 48 with higher scores showing higher burden. In the present study, the Chinese version of FBIS showed acceptable internal consistency with a McDonald's ω coefficient of 0.87.
Global Assessment of Functioning (GAF)
The GAF was used to assess patient function and consists of only one 100-point single item covering three major domains: social functioning, occupational functioning, and psychological functioning (American Psychiatric Association, 1994). The total scores range from 1 to 100, with higher scores indicating higher function. Examples are given for each ten-level interval.
Patient Health Questionnaire (PHQ-9)
The PHQ-9 (Spitzer et al., 1999) was used to assess caregivers' depression symptoms and consists of 9 items rated on a 4-point Likert scale from 0 (not at all) to 3 (nearly every day). The total scores range from 0 to 27, with a cut-off point of 10 differentiating depression and non-depression (Manea et al., 2015). The Chinese version of the PHQ-9 demonstrated good internal consistency in the current study with a McDonald's ω coefficient of 0.89.
Generalized Anxiety Disorder Scale (GAD-7)
The GAD-7 (Spitzer et al., 2006) was used to assess caregivers' anxiety and consists of 7 items rated on a 4-point Likert scale from 0 (not at all) to 3 (nearly every day). The total scores range from 0 to 21, with a cut-off point of 10 differentiating anxiety and non-anxiety (Schalet et al., 2014). The Chinese version of the GAD-7 demonstrated good internal consistency in the current study with a McDonald's ω coefficient of 0.91.
Data Analysis
For the first step, internal consistency of all short scales was examined with McDonald's ω coefficient (McDonald, 1999; Zhang and Yuan, 2016). An ω value of 0.7–0.9 for long scales and 0.6 for short scales (e.g., four items) indicate good internal consistency, while an ω value of >0.9 suggests redundant items (Youden, 1950; Nunnally and Bernstein, 1994).
Secondly, validity of the scales was tested and compared for the following three tests: concurrent validity, known group's validity and criterion validity. We first tested the normal distribution of FBIS score, GAF score, and GAD score using sktest and found none of them fit normal distribution (p < 0.01), and thus used non-parametric testing in the following validity testing.
Concurrent validity was measured using Spearman correlations with expected significant negative correlations with patient's function (GAF score), as well as significant positive correlations with caregiver's depression (PHQ-9 score), and anxiety symptoms (GAD-7 score) (Ji et al., 2014; Wang et al., 2017; Sun et al., 2018; Yu et al., 2018). We further performed Fisher r-to-Z test to compare the statistical significance of different correlations.
Known group's validity was assessed using Mann-Whitney U tests. We expect that caregivers with physical disease exhibited higher caregiver burden than those without physical disease (Yu et al., 2017). Also, caregiver burden varies according to different caregiving roles, such as parents, spouse, and others (Chang et al., 2017; Yu et al., 2017).
Criterion-related validity were measured by Spearman correlations between short-form total scores and the gold standard—FBIS total scores, with an expected correlation coefficient of above 0.7 (Higginson et al., 2010). The coefficient of determination (r2) was also computed to assess how much the variance of the gold standard can be explained by respective short forms.
Thirdly, the discriminative performance of the short forms was assessed and compared with the receiver operating characteristic (ROC) curve (Coffin and Sukhatme, 1997), using the ZBI-22 cut-off 21 as the reference (Zarit et al., 1985a). The ROC was constructed by plotting sensitivity against 1-specificity, with each point representing a sensitivity/1-specificity pair corresponding to a particular cutoff value. The closer a ROC plot is to the upper-left corner, the higher the overall accuracy of the test. A point closest to (0, 1) on the ROC curve indicates the ideal condition (100% sensitivity and 100% specificity) (Coffin and Sukhatme, 1997). The areas under the curves (AUC) were calculated using the trapezoidal method (Weinstein et al., 1980; Coffin and Sukhatme, 1997) to represent the scale's the ability to correctly classify those with and without burden. The range of the AUC is 0.5–1.0. A discriminative test is considered perfect if AUC = 1.0, good if AUC = 0.8–1.0, moderate if AUC = 0.6–0.8, and poor if AUC = 0.5–0.6; an area of 0.5 reflects a random rating model (Weinstein et al., 1980). 95% Confidence intervals of AUCs were computed. A P-value below 0.05 was considered as statistically significant. Besides, cut-points for the ZBI short forms were estimated based on the Youden index (Fischer et al., 2003).
All analyses were carried out using SPSS 16.0 (SPSS Inc., Chicago, IL, USA) and R 3.5.1.
Results
Table 2 shows the descriptive data on the sample. The mean (SD) age of the caregivers was 57.7 (12.5) years, and most of them were married (82.3%) and with primary education (59.9%). Slightly more than half of the caregivers were female (53.8%) and employed (52.9%). Most of their relationships to the care-recipient were parents (43.8%) and spouses (33.7%). The caregivers spent a median (q1–q3; minimal–maximum) of 15 years (9–25; 1–49) in caring for the patients. The median score of patient function as measured by GAF was 40.0 (20.0–61.0; 1–99). The mean score of depression, anxiety, and family burden as measured by PHQ-9, GAD-7, and FBIS were 9.75 (SD: 7.31), 9.31 (SD: 6.61), 23.62 (SD: 9.76), respectively.
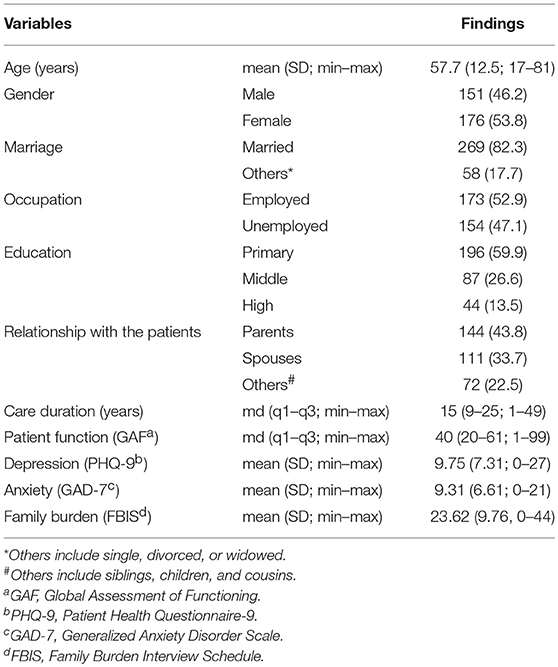
Table 2. Characteristics of Family Caregivers (n = 327).
Reliability and validity results were shown in Table 3. Reliability was generally good with McDonald's ω coefficient ranging from 0.69 to 0.85 across various ZBI formats, except for the Gort ZBI-4 (ω = 0.58). The low ω value for the Gort ZBI-4 may be explained by the property of the McDonald's ω, which is not an independent measure. McDonald's ω is sensitive to the number of items and increase with increased item numbers (Sijtsma, 2009). Based on this theory, we believe a ω of 0.58 being acceptable for such a small item scale like the Gort ZBI-4. Among all short forms, the Ballesteros ZBI-12 showed the highest ω of 0.85, followed closely by Bedard ZBI-12, the Arai ZBI-8, and Zhou ZBI-7 (ω = 0.84 for all).
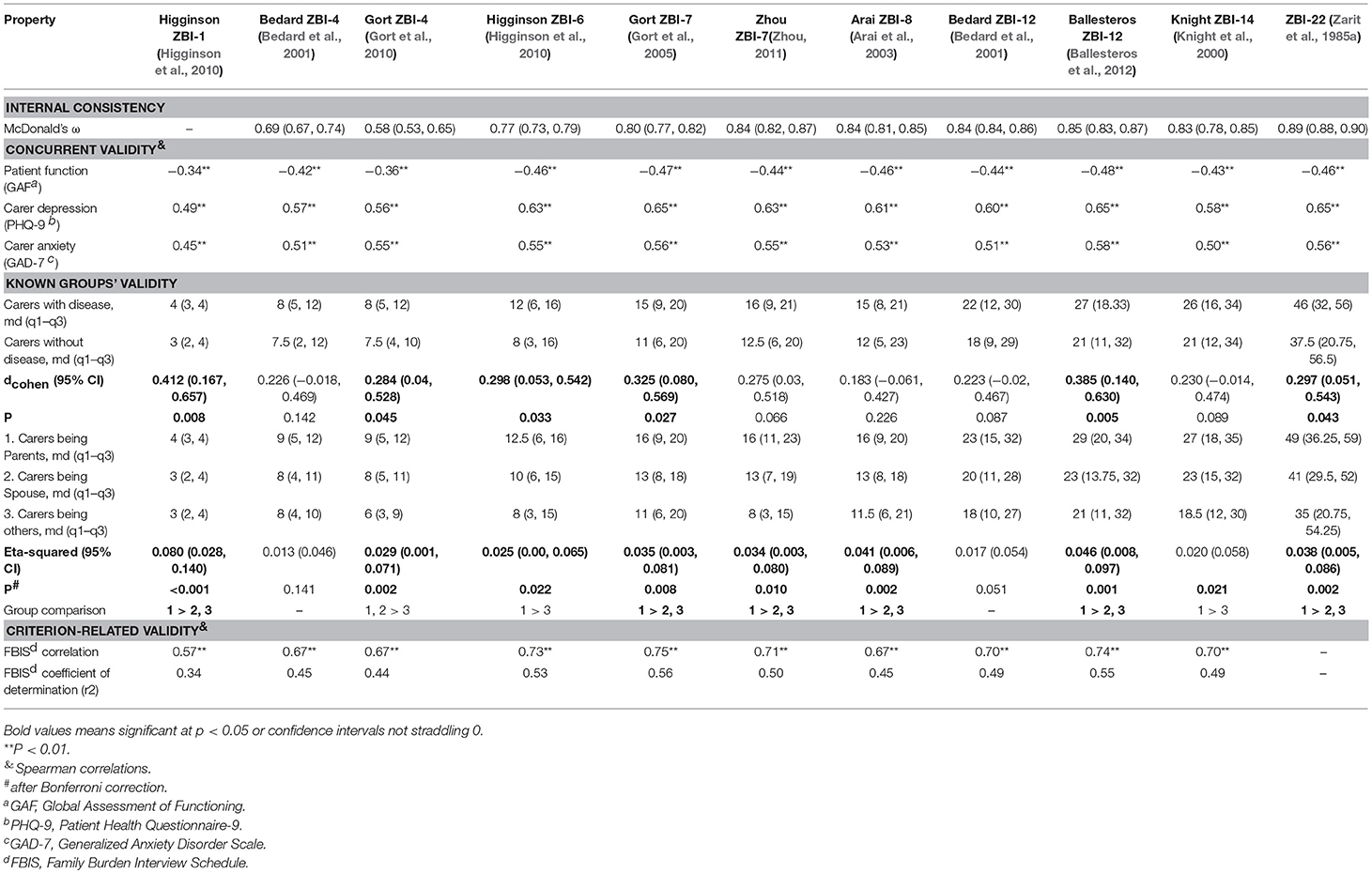
Table 3. Reliability and Validity of the ZBI short forms.
External concurrent validity was in general accordance with expectations and similar across the various ZBI forms, with significant negative correlations with GAF score (r = −0.34 to −0.48), and significant positive correlations with PHQ-9 score (r = 0.49–0.65) and GAD-7 score (r = 0.45–0.58). Among all the various ZBI forms, the Ballesteros ZBI-12 showed the highest correlations with the scores of GAF, PHQ-9, and GAD-7. A subsequent Fisher r-to-Z test found no statistical differences among those correlations of various short forms, indicating that all short forms performed equally well in concurrent validity.
For known groups' validity, among all short forms, five showed significantly higher burden scores in caregivers with disease than those without disease. For caregiving role and caregiver burden, eight forms exhibited significant higher burden scores in parent caregiver group, yet only five showed exactly the same pattern as the full ZBI scale: parents > spouse, others. Among all short forms, only three displayed favorable known group validity consistently: Higginson ZBI-1, the Gort ZBI-7, and the Ballesteros ZBI-12.
For criterion-related validity, all ZBI short forms showed significant high correlations with the FBIS criterion (r = 0.67–0.75) except for Higginson ZBI-1 (r = 0.57), which may be explained by the only one item in Higginson ZBI-1. Among all short forms, Gort ZBI-7 showed the highest criterion-related validity (r = 0.75), followed closely by Ballesteros ZBI-12 (r = 0.74) and Higginson ZBI-6 (r = 0.73).
Optimal cut-points according to the Youden index relative to the gold standard cut-point of 21 on the ZBI-22 are shown in Figure 1 and Table 4. All shorter versions were overall successful in differentiating low- and high-burden individuals with AUCs ranging from 0.85 to 0.99. Among all short forms, the Ballesteros ZBI-12 showed the highest AUC (0.99), followed closely by Knight ZBI-14, Bedard ZBI-12, and Zhou ZBI-7, all with the same AUC of 0.98.
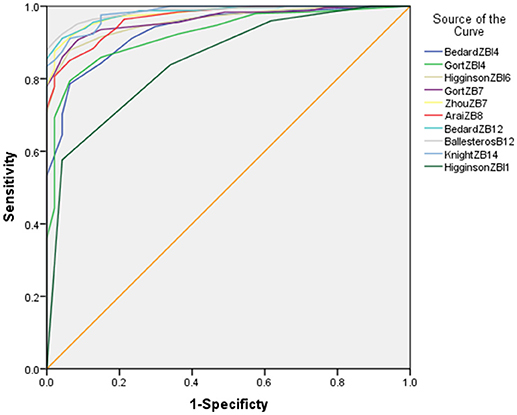
Figure 1. Receiver operating characteristic curves for various short-form versions of the Zarit Burden Interview (ZBI) and areas under the curve (AUC, 95% confidence interval [CI]). A total score of 21 on the full-scale ZBI as the cutoff value between low and high burden.
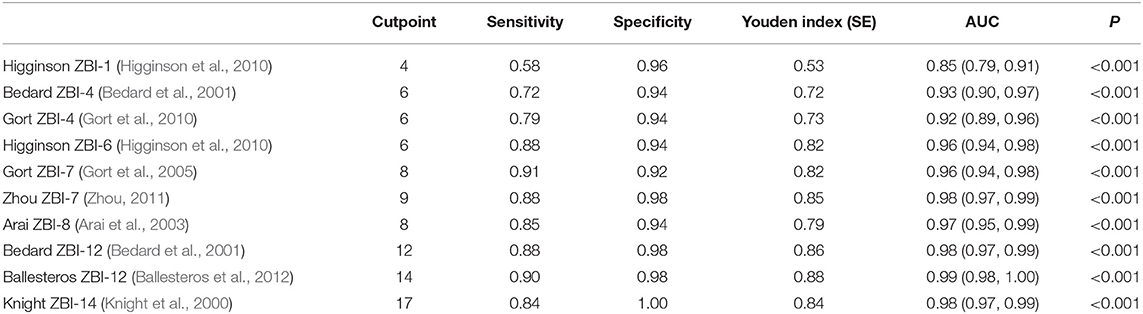
Table 4. Cutpoint Estimations and ROC Curve Analyses of ZBI Short Forms Relative to the Suggested ZBI-22 Cutpoint of 21.
Discussion
This study assessed and validated ten short forms of the Zarit Burden Interview (ZBI) among family caregivers of people with schizophrenia. We found general support for the psychometric testing of all ten short forms. While previous studies proposed either the Bedard 12-item ZBI (Higginson et al., 2010; Hagell et al., 2017) or the Ballesteros 12-item ZBI (Lin et al., 2017b) as the best one, our comparison produced two structures that outperformed other structures in comprehensive psychometric properties: the Ballesteros 12-item and the Gort ZBI-7.
Compared to the full ZBI form, the short forms are easier to administer and less time-consuming due to the abridged items. The use of ZBI short forms facilitates rapid identification of caregiver burden and quick further assessment or referral in busy clinical situations and is thus favored by physicians. Also, it alleviates respondent burden of caregivers who focus more on the patients they cared for than their own feelings and thus only want to answer the briefest questionnaire.
Four key findings emerge from our analysis. First, we found high internal consistency of all short versions of the ZBI with McDonald's ω ≥ 0.70, except for Gort ZBI-4 (McDonald's ω = 0.58). On the one hand, it reflects the property of the McDonald's omega coefficient that is sensitive to the number of items and decreases with reduced items (Sijtsma, 2009). On the other hand, it may imply the potential item redundancy of the full ZBI scale and propose better applicability of short forms, as shown in another study (Lin et al., 2017b).
Second, while all ten ZBI short forms uniformly exhibited desirable concurrent validity correlations and criterion-related validity, there is inconsistency in the result of known groups' validity. Although caregiver burden has been widely proven to be positively associated with physical disease in the literature (Sethabouppha and Kane, 2005; Gater et al., 2014; Yu et al., 2017), only five ZBI short forms demonstrated significant higher burden scores in caregivers with disease than those without in the current study. Moreover, past studies have shown that caregiver burden varies according to caregiving role, with the majority supporting the highest burden in parents, followed by spouse, siblings, children, and others in turn (Lu, 2009; Hsiao and Tsai, 2014a,b). In the present study, eight out of ten short forms have successfully distinguished caregiver burden among various caregiving roles, while only 5 short forms showed exactly the same pattern as the full ZBI scale: parents > spouse, others. In sum, only the Higginson ZBI-1, the Gort ZBI-7, and the Ballesteros 12-item ZBI displayed favorable known group validity consistently, which were highly recommended for future use in screening for various groups.
Third, our findings found the Ballesteros 12-item and the Gort ZBI-7 outperformed other short forms with almost equally good performance in psychometric testing. This finding partly supports Lin's (Lin et al., 2017b) previous conclusion of Ballesteros 12-item ZBI as the best one, yet conflicts with the findings of Hagell and Higginson, both proposed the Bedard 12-item ZBI (Higginson et al., 2010; Hagell et al., 2017) as the best one. A careful comparison between the Gort ZBI-7 and the Bedard ZBI-12 showed that the latter included all items of the former except for the item 22 “Overall, how burdened do you feel in caring.” One possible explanation may be that item 22 acts as an overall summary of the whole scale and is more representative of the full ZBI score than any other item. In fact, some authors even propose reducing the whole scale into an extreme one item—the Higginson ZBI-1 as a rapid assessment of caregiver burden (Higginson et al., 2010; Ballesteros et al., 2012). However, the measurement of item 22 alone is not enough to represent the whole scale because it is based on the answering and learning process of the all previous items, leading to its analysis in isolation from the rest of the information unpractical (Ballesteros et al., 2012). Another explanation may be that the item 22 acts as more like a supplement to the previous items than a summary, as shown in our analysis, the Gort ZBI-7 is actually a combination of the Higginson ZBI-1 and Higginson ZBI-6 but performed much better than the other two. It is likely that item 22 may have measures some salient concept that other items may not be able to capture, especially in Asian cultures. As a result, this item is an integral part of the scale that can neither be isolated, nor deleted.
Our fourth finding is cut-off values ranging from 4 to 17 for the various short forms of ZBI relative to that of the ZBI-22. The results were slightly different from those previously identified among family caregivers of people with cancer, brain injury, and dementia (Higginson et al., 2010; Hagell et al., 2017), which may be explained by the various sample as mentioned above and provides useful guidance for future use of short forms among such a population. Furthermore, all short forms displayed good AUC values of above 0.8, further corroborating their high discriminative performances to distinguish those with and without burden, which accords with past studies (Higginson et al., 2010; Hagell et al., 2017).
The study falls short in several aspects. First, this is a cross-sectional study with no information on short forms' responsiveness to change, which is important for psychometric property in intervention and longitudinal studies (Kirshner and Guyatt, 1985). Second, we did not run test-retest reliability in the current study. Further study may consider collecting data in multiple time points to detect responsiveness to change and test-retest reliability. Third, we did not test the factorial structure of the ZBI and treated all the different short forms of ZBI as a unidimensional structure. Conflicting evidence exists on the factor analysis of both the 22-item ZBI and its short forms in past studies (Ballesteros et al., 2012; Branger et al., 2016; Tang et al., 2017). One possible explanation may be that factor analysis is sample dependent and may vary according to different study populations, thus making testing and comparing factor structures among various short forms in the current single study population implausible (Yu et al., 2015), future research may benefit from adding factor analysis into comparison among short forms across diverse populations. Fourth, the finding of the current study is based on quantitative analysis of different short form versions, there is a lack of qualitative evaluation of each item for cultural adaptation, future research may consider mixed-method comparison for these short forms. Finally, the sample came from one single rural county of Hunan province, which may limit the study's representativeness. Future multi-center large sample comparative studies are warranted for firmer conclusions.
In conclusion, our observations provide initial support for the psychometric properties of various ZBI short forms for use among family caregivers of people with schizophrenia. The Ballesteros ZBI-12 and the Gort ZBI-7 showed the best performance in reliability and validity, which paves the way for future studies to further utilize and validate the scales.
Data Availability Statement
The raw data supporting the conclusions of this manuscript will be made available by the authors, without undue reservation, to any qualified researcher.
Author Contributions
YY and SX contributed to the conception and design of the study. YY, ZL, WZ, XC, MH, and XZ contributed to the research conduction and data collection. YY and ZL contributed to data analyses and interpretation, analysis tools or data. YY drafted the article while ZL, WZ, XC, MH, XZ, and SX critically appraised it and revised it. All authors approved the final version of manuscript for submission and publication.
Funding
This work was supported by the National Natural Science Foundation of China (Grant Number 71804197) and the CMB-CSU Collaborative Program for Mental Health Policy Development (II) (Grant Number 14-188).
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors would like to thank all the families of the schizophrenia individuals we interviewed during the study for openly sharing their feelings and experiences. We'd also like to thank the health and family planning bureau of Ningxiang County and the government of the Liushahe town, Shungfupu town, Chengjiao xiang, and Yutan town for their administrative support, as well as all village/community doctors for guiding us to visit each household of the schizophrenia individuals in the rural areas of Ningxiang county, Hunan province.
References
American Psychiatric Association, (1994). Diagnostic and Statistical Manual of Mental Disorders: DSM-IV, 4th Edn. Washington DC, American Psychiatric Association.
Arai, Y., Tamiya, N., and Yano, E. (2003). The short version of the Japanese version of the Zarit Caregiver Burden Interview (J-ZBI_8): its reliability and validity. Nihon Ronen Igakkai Zasshi 40, 497–503. doi: 10.3143/geriatrics.40.497
Bachner, Y. G., and O'Rourke, N. (2007). Reliability generalization of responses by care providers to the Zarit Burden Interview. Aging Ment. Health 11, 678–685. doi: 10.1080/13607860701529965
Ballesteros, J., Santos, B., Gonzalez-Fraile, E., Munoz-Hermoso, P., Dominguez-Panchon, A. I., and Martin-Carrasco, M. (2012). Unidimensional 12-item zarit caregiver burden Interview for the assessment of dementia caregivers' burden obtained by item response theory. Value Health 15, 1141–1147. doi: 10.1016/j.jval.2012.07.005
Bedard, M., Molloy, D. W., Squire, L., Dubois, S., Lever, J. A., and O'Donnell, M. (2001). The zarit burden interview: a new short version and screening version. Gerontologist 41, 652–657. doi: 10.1093/geront/41.5.652
Branger, C., O'Connell, M. E., and Morgan, D. G. (2016). Factor analysis of the 12-item zarit burden interview in caregivers of persons diagnosed with dementia. J. Appl. Gerontol. 35, 489–507. doi: 10.1177/0733464813520222
Braun, M., Scholz, U., Hornung, R., and Martin, M. (2010). The burden of spousal caregiving: a preliminary psychometric evaluation of the German version of the Zarit burden interview. Aging Ment. Health 14, 159–167. doi: 10.1080/13607860802459781
Chang, C. C., Yen, C. F., Jang, F. L., Su, J. A., and Lin, C. Y. (2017). Comparing affiliate stigma between family caregivers of people with different severe mental illness in Taiwan. J. Nerv. Ment. Dis. 205, 542–549. doi: 10.1097/NMD.0000000000000671
Chattat, R., Cortesi, V., Izzicupo, F., Del Re, M. L., Sgarbi, C., Fabbo, A., et al. (2011). The Italian version of the Zarit burden interview: a validation study. Int. Psychogeriatr. 23, 797–805. doi: 10.1017/S1041610210002218
Coffin, M., and Sukhatme, S. (1997). Receiver operating characteristic studies and measurement errors. Biometrics 53, 823–837. doi: 10.2307/2533545
Fischer, J., Bachmann, L., and Jaeschke, R. (2003). A readers' guide to the interpretation of diagnostic test properties: clinical example of sepsis. Intensive Care Med. 29, 1043–1051. doi: 10.1007/s00134-003-1761-8
Flynn Longmire, C. V., and Knight, B. G. (2011). Confirmatory factor analysis of a brief version of the Zarit burden interview in black and white dementia caregivers. Gerontologist 51, 453–462. doi: 10.1093/geront/gnr011
Gater, A., Rofail, D., Tolley, C., Marshall, C., Abetz-Webb, L., Zarit, S. H., et al. (2014). Sometimes it's difficult to have a normal life: results from a qualitative study exploring caregiver burden in schizophrenia. Schizophr. Res. Treat. 2014:368215. doi: 10.1155/2014/368215
Gort, A. M., March, J., Gomez, X., de Miguel, M., Mazarico, S., and Balleste, J. (2005). Short Zarit scale in palliative care. Med. Clin. 124, 651–653. doi: 10.1157/13074742
Gort, A. M., Mingot, M., March, J., Gomez, X., Soler, T., and Nicolas, F. (2010). Short zarit scale in dementias. Med. Clin. 135, 447–449. doi: 10.1016/j.medcli.2010.05.006
Hagell, P., Alvariza, A., Westergren, A., and Arestedt, K. (2017). Assessment of burden among family caregivers of people with parkinson's disease using the zarit burden interview. J. Pain Symptom. Manage. 53, 272–278. doi: 10.1016/j.jpainsymman.2016.09.007
Higginson, I. J., Gao, W., Jackson, D., Murray, J., and Harding, R. (2010). Short-form zarit caregiver burden interviews were valid in advanced conditions. J. Clin. Epidemio. 63, 535–542. doi: 10.1016/j.jclinepi.2009.06.014
Hirono, N., Kobayashi, H., and Mori, E. (1998). Caregiver burden in dementia: evaluation with a Japanese version of the Zarit caregiver burden interview. No To Shinkei 50, 561–567.
Hsiao, C. Y., and Tsai, Y. F. (2014a). Caregiver burden and satisfaction in families of individuals with schizophrenia. Nurs. Res. 63, 260–269. doi: 10.1097/NNR.0000000000000047
Hsiao, C. Y., and Tsai, Y. F. (2014b). Factors of caregiver burden and family functioning among Taiwanese family caregivers living with schizophrenia. J. Clin. Nurs. 24, 1546–1556. doi: 10.1111/jocn.12745
Imarhiagbe, F. A., Asemota, A. U., Oripelaye, B. A., Akpekpe, J. E., Owolabi, A. A., Abidakun, A. O., et al. (2017). Burden of informal caregivers of stroke survivors: validation of the zarit burden interview in an African population. Ann. Afr. Med. 16, 46–51. doi: 10.4103/aam.aam_213_16
Ji, B., Zhao, I., Turner, C., Sun, M., Yi, R., and Tang, S. (2014). Predictors of health-related quality of life in Chinese caregivers of children with autism spectrum disorders: a cross-sectional study. Arch. Psychiatr. Nurs. 28, 327–332. doi: 10.1016/j.apnu.2014.06.001
Kirshner, B., and Guyatt, G. (1985). A methodological framework for assessing health indices. J. Chronic. Dis. 38, 27–36. doi: 10.1016/0021-9681(85)90005-0
Knight, B. G., Fox, L. S., and Chou, C. (2000). Factor structure of the burden interview. J. Clin. Geropsychol. 6, 249–258. doi: 10.1023/A:1009530711710
Lim, W. S., Cheah, W. K., Ali, N., Han, H. C., Anthony, P. V., Chan, M., et al. (2014). Worry about performance: a unique dimension of caregiver burden. Int. Psychogeriatr. 26, 677–686. doi: 10.1017/S1041610213002445
Lin, C. Y., Ku, L. E., and Pakpour, A. H. (2017a). Measurement invariance across educational levels and gender in 12-item Zarit Burden Interview (ZBI) on caregivers of people with dementia. Int. Psychogeriatr. 29, 1841–1848. doi: 10.1017/S1041610217001417
Lin, C. Y., Wang, J. D., Pai, M. C., and Ku, L. E. (2017b). Measuring burden in dementia caregivers: confirmatory factor analysis for short forms of the Zarit Burden interview. Arch. Gerontol. Geriatr. 68, 8–13. doi: 10.1016/j.archger.2016.08.005
Lu, C. (2009). Correlates of caregiver burden for schizophrenia patients. J. Clin. Exp. Med. 8, 90–91.
Lu, L., Wang, L., Yang, X., and Feng, Q. (2009). Zarit caregiver burden interview: development, reliability and validity of the chinese version. Psychiatr. Clin. Neurosci. 63, 730–734. doi: 10.1111/j.1440-1819.2009.02019.x
Ma, H. (2012). Integration of hospital and community services-the ‘686 Project'-is a crucial component in the reform of China's mental health services. Shanghai Arch. Psychiatr. 24, 172–174. doi: 10.3969/j.issn.1002-0829.2012.03.007
Manea, L., Gilbody, S., and McMillan, D. (2015). A diagnostic meta-analysis of the Patient Health Questionnaire-9 (PHQ-9) algorithm scoring method as a screen for depression. Gen. Hosp. Psychiatr. 37, 67–75. doi: 10.1016/j.genhosppsych.2014.09.009
Martin-Carrasco, M., Otermin, P., Perez-Camo, V., Pujol, J., Aguera, L., Martin, M. J., et al. (2010). EDUCA study: psychometric properties of the Spanish version of the zarit caregiver burden scale. Aging Ment. Health 14, 705–711. doi: 10.1080/13607860903586094
O'Rourke, N., and Tuokko, H. A. (2003). The relative utility of four abridged versions of the Zarit Burden Interview. J. Ment. Health Aging 9:55e64.
Pai, S., and Kapur, R. L. (1981). The burden on the family of a psychiatric patient: development of an interview schedule. Br. J. Psychiatr. 138, 332–335. doi: 10.1192/bjp.138.4.332
Schalet, B. D., Cook, K. F., Choi, S. W., and Cella, D. (2014). Establishing a common metric for self-reported anxiety: linking the MASQ, PANAS, and GAD-7 to PROMIS Anxiety. J. Anxiety Disord. 28, 88–96. doi: 10.1016/j.janxdis.2013.11.006
Sethabouppha, H., and Kane, C. (2005). Caring for the seriously mentally ill in Thailand: buddhist family caregiving. Arch. Psychiatr. Nurs. 19, 44–57. doi: 10.1016/j.apnu.2005.02.004
Sijtsma, K. (2009). On the use, the misuse, and the very limited usefulness of Cronbach's Alpha. Psychometrika 74, 107–120. doi: 10.1007/s11336-008-9101-0
Spitzer, R. L., Kroenke, K., and Williams, J. B. (1999). Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. Primary Care Evaluation of Mental Disorders. Patient Health Questionnaire. JAMA 282, 1737–1744.
Spitzer, R. L., Kroenke, K., Williams, J. B., and Lowe, B. (2006). A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch. Intern. Med. 166, 1092–1097. doi: 10.1001/archinte.166.10.1092
Sun, M., Mainland, B. J., Ornstein, T. J., Sin, G. L., and Herrmann, N. (2018). Correlates of nursing care burden among institutionalized patients with dementia. Int. Psychogeriatr. 30, 1549–1555. doi: 10.1017/S104161021800025X
Tang, B., Yu, Y., Liu, Z., Lin, M., Chen, Y., Zhao, M., et al. (2017). Factor analyses of the Chinese Zarit Burden interview among caregivers of patients with schizophrenia in a rural Chinese community. BMJ Open 7:e015621. doi: 10.1136/bmjopen-2016-015621
Tang, J. Y., Ho, A. H., Luo, H., Wong, G. H., Lau, B. H., Lum, T. Y., et al. (2016). Validating a Cantonese short version of the Zarit Burden Interview (CZBI-Short) for dementia caregivers. Aging Ment. Health 20, 996–1001. doi: 10.1080/13607863.2015.1047323
Wang, G., Cheng, Q., Wang, Y., Deng, Y. L., Ren, R. J., Xu, W., et al. (2008). The metric properties of Zarit caregiver burden scale: validation study of a Chinese version. Alzheimer. Dis. Assoc. Disord. 22, 321–326. doi: 10.1097/WAD.0b013e3181902334
Wang, X., Chen, Q., and Yang, M. (2017). Effect of caregivers' expressed emotion on the care burden and rehospitalization rate of schizophrenia. Patient Prefer Adherence 11, 1505–1511. doi: 10.2147/PPA.S143873
Weinstein, M. C., Fineberg, H. V., Elstein, A. S., Frazier, H. S., Neuhauser, D., Neutra, R. R., et al. (1980). Clinical Decision Analysis. Philadelphia, PA: WB Saunders.
Youden, W. J. (1950). Index for rating diagnostic tests. Cancer 3, 32–35. doi: 10.1002/1097-0142(1950)3:1<32::AID-CNCR2820030106>3.0.CO
Yu, Y., Liu, Z. W., Tang, B. W., Zhao, M., Liu, X. G., and Xiao, S. Y. (2017). Reported family burden of schizophrenia patients in rural China. PLoS ONE 12:e0179425. doi: 10.1371/journal.pone.0179425
Yu, Y., Shiu, C. S., Yang, J. P., Wang, M., Simoni, J. M., Chen, W. T., et al. (2015). Factor analyses of a social support scale using two methods. Qual. Life Res. 24, 787–794. doi: 10.1007/s11136-014-0815-4
Yu, Y., Tang, B. W., Liu, Z. W., Chen, Y. M., Zhang, X. Y., and Xiao, S. (2018). Who cares for the schizophrenia individuals in rural China–a profile of primary family caregivers. Compr. Psychiatry 84, 47–53. doi: 10.1016/j.comppsych.2018.04.002
Zarit, S. H., Orr, N. K., and Zarit, J. M. (1985a). The Hiddenvictims of Alzheimer's Disease: Families Under Stress. New York, NY: University Press.
Zarit, S. H., Orr, N. K., and Zarit, J. M. (1985b). Families Under stress: Caring for the Patient With Alzheimer's Disease and Related Disorders. New York, NY: University Press.
Zarit, S. H., Reever, K. E., and Bach-Peterson, J. (1980). Relatives of the impaired elderly: correlates of feelings of burden. Gerontologist 20, 649–655. doi: 10.1093/geront/20.6.649
Zhang, Z., and Yuan, K. H. (2016). Robust coefficients alpha and omega and confidence intervals with outlying observations and missing data: methods and software. Educ. Psychol. Meas. 76, 387–411. doi: 10.1177/0013164415594658
Zhou, R. (2011). The Development of Burden Evaluation System for Family Caregivers of Chronic Diseases, Huazhong University of Science and Technology, thesis, Hubei, China (in Chinese).
Keywords: Zarit Burden Interview (ZBI), short-forms, psychometric testing, reliability, validity
Citation: Yu Y, Liu Z, Zhou W, Chen X, Zhang X, Hu M and Xiao S (2018) Assessment of Burden Among Family Caregivers of Schizophrenia: Psychometric Testing for Short-Form Zarit Burden Interviews. Front. Psychol. 9:2539. doi: 10.3389/fpsyg.2018.02539
Received: 09 September 2018; Accepted: 28 November 2018;
Published: 19 December 2018.
Edited by:
Laura Badenes-Ribera, University of Valencia, SpainReviewed by:
Chung-Ying Lin, Hong Kong Polytechnic University, Hong KongCesar Merino-Soto, Universidad de San Martín de Porres, Peru
Copyright © 2018 Yu, Liu, Zhou, Chen, Zhang, Hu and Xiao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shui-yuan Xiao, eGlhb3N5QGNzdS5lZHUuY24=