 Qianhong Hu1
Qianhong Hu1 Qianlei Zhao
Qianlei Zhao- 1Department of Pediatrics, The Second Affiliated Hospital and Yuying Children's Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, China
- 2Department of Pediatrics, The Second School of Medicine of Wenzhou Medical University, Wenzhou, Zhejiang, China
Background: Vitamin A deficiency (VAD) continues to pose a significant public health challenge, particularly in low socio-demographic index (SDI) regions, contributing to increased infections, blindness, and child mortality. Its causes include poor diets, absorption issues, and infectious diseases.
Objective: To comprehensively assess the global trends and burden of Vitamin A Deficiency from 1990 to 2021 and to forecast the global VAD-related burden from 2022 to 2050.
Methods: This investigation employed data from the GBD 2021 database to analyze the global burden of nutritional deficiencies attributable to VAD. Disability-adjusted life-years (DALYs) and years lived with disability (YLDs) were systematically evaluated by gender, age groups, geographic regions, and countries over the 32-year study period (1990–2021). Temporal trends in age-standardized DALYs rate (ASDR) and age-standardized YLDs rate (ASYR) were quantified using estimated annual percentage change (EAPC) analysis. Projections of future burden were generated using exponential smoothing (ES) and autoregressive integrated moving average (ARIMA) models.
Results: In 2021, the global burden of VAD was 1,104,931 DALYs, down from 1,970,337 in 1990. The ASDR dropped from 32.56 in 1990 to 15.73 in 2021, with an EAPC of −2.81%. Males had higher ASDR than females, both showing significant declines. The greatest burden was in the <5-year-old age group. An inverse SDI-ASDR associations was evident, with high-SDI regions achieving the fastest rate reductions. Projections to 2050 using ARIMA and ES models predicted a continued decrease in DALYs, with faster declines in males, although the ES model suggested a stabilization in DALYs for both genders.
Conclusion: The GBD 2021 data underscored the persistent global challenge of addressing VAD. Solving this issue necessitates comprehensive strategies that combine targeted interventions, policy reforms, and collaborative efforts.
1 Introduction
Nutritional deficiencies (NDs) continue to pose a substantial global health burden, representing major contributors to morbidity, mortality and disability worldwide (1–3). Within the spectrum of NDs, Vitamin A deficiency (VAD) persists as a significant global health concern, disproportionately affecting populations in low- and middle-income countries (LMICs), where malnutrition is a persistent issue (4). As an essential micronutrient, vitamin A regulates various fundamental biological functions, including visual phototransduction, immune function, cellular differentiation, and reproduction (5, 6). Severe VAD significantly elevates mortality risk, particularly among children under 5 years old, and can lead to irreversible blindness due to xerophthalmia, increased susceptibility to infections, and poor maternal health outcomes (7–9). Despite extensive global efforts to combat VAD, it continues to impose a substantial burden on vulnerable populations, necessitating targeted interventions and continuous monitoring (10).
The etiology of VAD is multifactorial, primarily stemming from inadequate dietary intake, poor absorption due to gastrointestinal diseases, and increased metabolic demand during periods of rapid growth, infection, or pregnancy (11–13). In many LMICs, diets are heavily reliant on staple foods with low vitamin A content, contributing to widespread deficiency (14, 15). Additionally, infectious diseases such as diarrheal illnesses and measles exacerbate vitamin A depletion, further amplifying both morbidity and mortality risks (16–18). The interplay between malnutrition and infectious diseases highlights the need for integrated health policies that address both dietary deficiencies and disease prevention (19).
The Global Burden of Disease (GBD) Study has played a pivotal role in quantifying the worldwide burden of morbidity and mortality related to NDs. Previous analyses, including the GBD 2019 study, demonstrated a decline in both the global age-standardized incidence rate (ASIR) and age-standardized DALY rates (ASDR) for VAD worldwide, with estimated annual percentage changes (EAPC) of −3.11% (95% CI: −3.24 to −2.94%) and −2.18% (95% CI: −2.38 to −1.93%), respectively (1, 20). However, reductions were least pronounced in low sociodemographic index (SDI) regions, which continued to bear the highest burden of VAD globally. Epidemiological data from 2019 revealed Sub-Saharan Africa, and specifically the central region, exhibited the highest ASIR and ASDR in 2019, with Somalia and Niger ranking highest at the national level (10). Additionally, gender-disaggregated analysis revealed VAD remained disproportionately higher among males compared to females, with under-five children in low-SDI regions being the most affected demographic (21).
As the GBD database is updated to include 2021 data, it is imperative to reassess these trends, identify emerging disparities, and anticipate future challenges in the context of global demographic shifts, climate change, and economic instability (22). A nuanced understanding of these evolving patterns will be critical in refining public health strategies and ensuring more targeted and equitable interventions (23).
Utilizing the most recent Global Burden of Disease 2021 dataset, this study provides an updated reassessment of the global NDs burden and its predictive trends through 2050. Our objectives are threefold: (1) to quantify the DALYs of NDs attributable to VAD globally and stratified by demographic strata (age, gender, SDI region and nations) in 2021, identifying population and regions at greatest risk of VAD; (2) to assess VAD-related burden trends from 1990 to 2021; (3) to forecast the global VAD-related burden from 2022 to 2050. This analysis not only updates prior estimates but also explores the impact of recent global crises on nutritional outcomes, offering evidence to guide targeted policy interventions.
2 Methods
2.1 Data source
The GBD 2021 study (accessible via https://vizhub.healthdata.org/gbd-results/) systematically gathers and analyzes up-to-date global disease burden data encompassing 371 diseases and injuries, while simultaneously estimating the associations between 88 risk factors and health outcomes (24, 25). The disability-adjusted life-years (DALYs) in this study, including years lived with disability (YLDs) for VAD -related nutritional disorders, were sourced exclusively from the GBD 2021 database.
2.2 Descriptive analysis
In this study, we examined the distribution characteristics of the burden of NDs attributable to VAD globally and across different genders, age groups, regions and countries in 1990 and 2021. The formula for age-standardized rate (ASR) calculation is as follows:
Where denotes the th age group, represents age-specific rate, is the number of population (or weight) in the corresponding age groups of the selected reference standard population (26). Uncertainty intervals (UIs) were estimated based on the 2.5th and 97.5th percentiles derived from a 1,000-draw distribution for each metric (27). The SDI is a composite metric to evaluate a country or region’s overall socio-demographic development level based on fertility rates, educational attainment, and per capita income. It was used to classify regions and facilitate comparable analyses of disease burden. Countries and territories were classified into five groups according to their SDI scores as follows: low (SDI < 0.46), low-middle (SDI 0.46–0.60), middle (SDI 0.61–0.69), high-middle (SDI 0.70–0.81), and high (SDI > 0.81) (28). All statistical analyses were performed using R software (version 4.1.0), applying statistical significance defined as p < 0.05.
2.3 Trend analysis
The average trends in age-standardized DALYs rate (ASDR) and age-standardized YLDs rate (ASYR) during 1990 to 2021 were assessed using the estimated annual percentage change (EAPC). The formula for calculating EAPC is as follows:
Where represents , denotes the calendar year and represents the slope obtained from the linear regression of the natural logarithm of the ASR on the year (29).
2.4 Forecasting analysis
The autoregressive integrated moving average (ARIMA) model is particularly effective in capturing trends and seasonal patterns in data, while the exponential smoothing (ES) model prioritizes recent observations, providing a comprehensive outlook on potential future developments (30). To ensure comprehensive and multi-perspective forecasting of the potential trends in the burden of VAD-attributable NDs from 2022 to 2050, we employed both ARIMA and ES methods. This dual approach was adopted as each method possesses distinct advantages in capturing different patterns in time series data, thereby providing complementary insights and enhancing the robustness of our projections. Statistical computing software R (Version 4.4.1) was used for all analyses and graphical representations.
3 Results
3.1 Global burden
In 2021, there were 1,104,931 (95% UI: 711,387–1,561,756) DALYs caused by NDs attributable to VAD worldwide, representing a decrease from 1,970,337 (95% UI: 1,316,355–2,813,198) in 1990 (Figure 1). Between 1990 and 2021, the ASDR of VAD-attributable NDs decreased from 32.56 (95% UI: 21.77–46.45) in 1990 to 15.73 (95% UI: 10.09–22.28) in 2021, with a consistent downward trend (EAPC: −2.81, 95% CI: −2.96 to −2.66) (Figure 1). Detailed information on the disease burden of malnutrition is provided in Tables 1, 2.
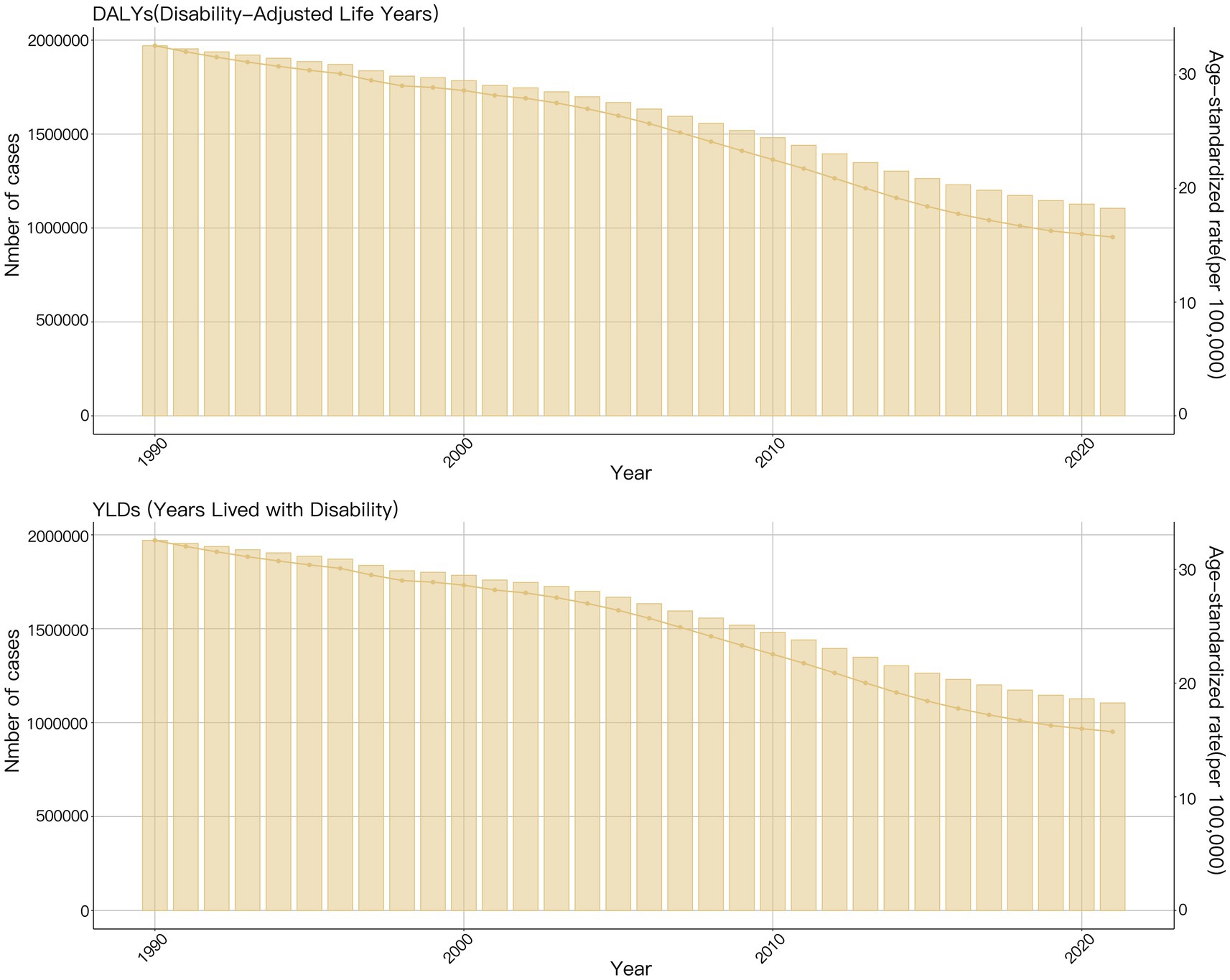
Figure 1. The global burden of nutritional deficiencies attributable to vitamin A deficiency from 1990 to 2021.
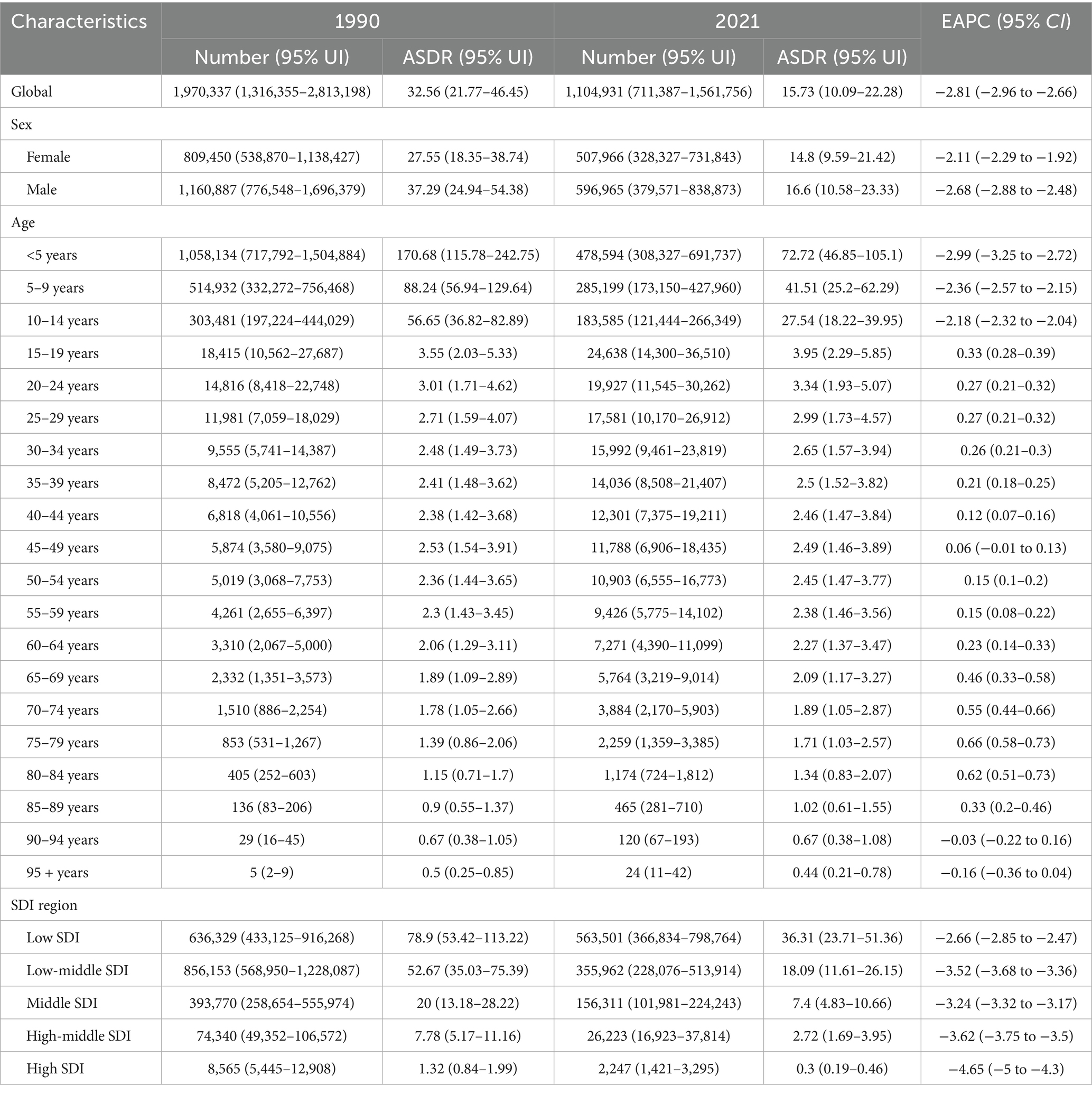
Table 1. The DALYs and ASDR of nutritional deficiencies attributable to vitamin A deficiency in 1990 and 2021.
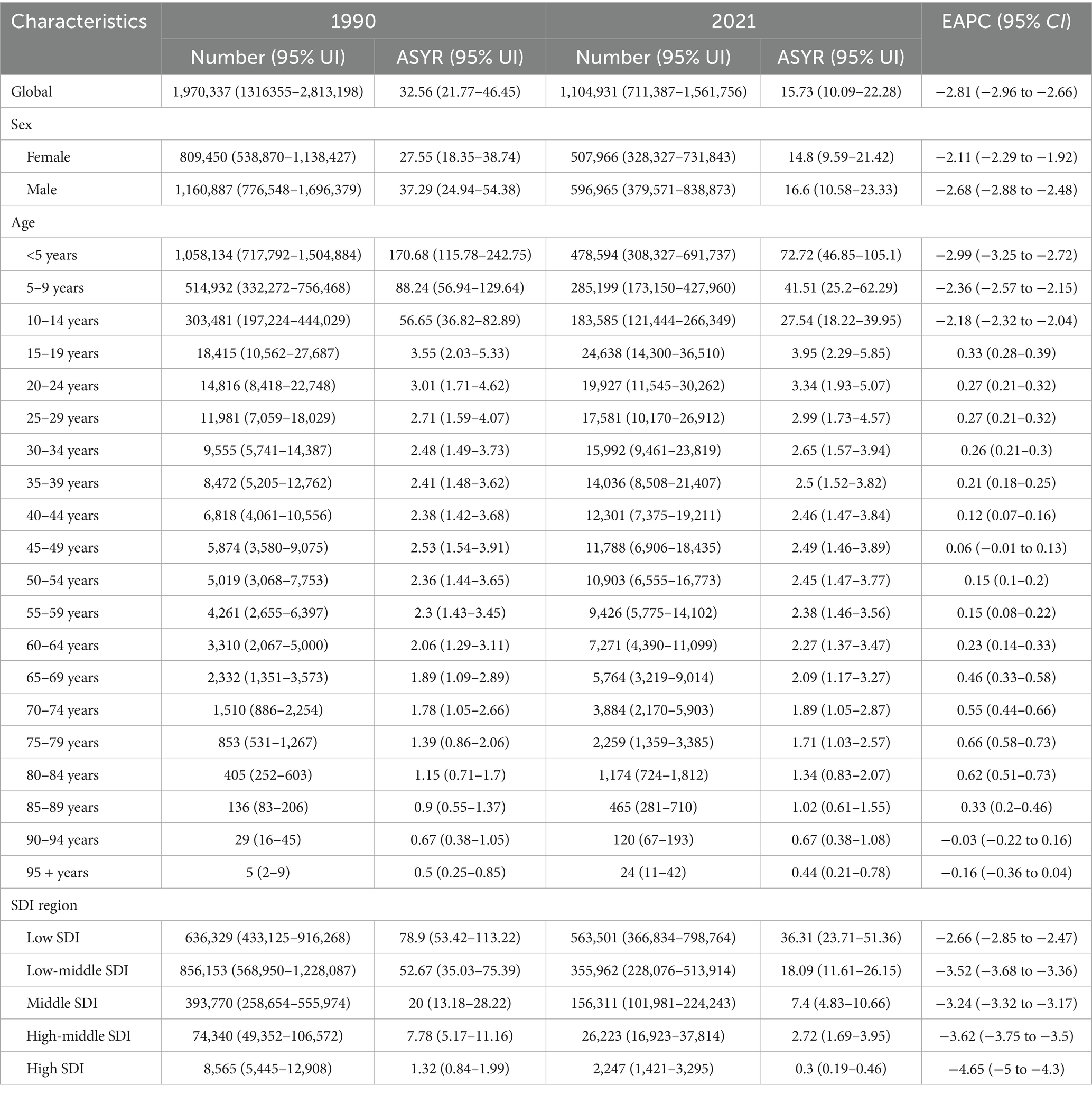
Table 2. The YLDs and ASYR of nutritional deficiencies attributable to vitamin A deficiency in 1990 and 2021.
3.2 Sex-specific burden
In 2021, Table 1 presents the number of the ASDR of NDs attributable to VAD for males was higher than that for females (Supplementary Figure S1). The DALYs and YLDs of NDs attributable to VAD stratified by sex were depicted in Supplementary Figure S2. The ASDR of VAD-attributable NDs for females decreased from 27.55 (95% UI: 18.35–38.74) in 1990 to 14.8 (95% UI: 9.59–21.42) in 2021, with an EAPC of −2.11 (95% CI: −2.29 to −1.92). And the ASDR of VAD-attributable NDs for males decreased from 37.29 (95% UI: 24.94–54.38) in 1990 to 16.6 (95% UI: 10.58–23.33) in 2021, with an EAPC of −2.68 (95% CI: −2.88 to −2.48) (Supplementary Figure S3). Trends in the DALYs and YLDs of VAD-attributable NDs stratified by sex were depicted in Supplementary Figure S4.
3.3 Age-specific burden
Table 2 provides the DALYs and ASDR of NDs attributable to VAD demonstrated significant variation across age strata. In 2021, the ASDR of NDs attributable to VAD decreased with age strata, peaking significantly in children under 5 years old [72.72 (95% UI: 46.85–105.1)] (Supplementary Figure S5). The DALYs and YLDs of VAD-attributable NDs stratified by age were depicted in Supplementary Figure S6. Longitudinal analysis (1990–2021) revealed the most rapid increase in the ASDR of VAD-attributable NDs occurred in the 75–79 age group (EAPC = 0.66, 95% CI: 0.58–0.73), while the steepest decline of the ASDR occurred in the <5 age group (EAPC = -2.99, 95% CI: −3.25 to −2.72) (Supplementary Figure S7). Trends in the DALYs and YLDs of VAD-attributable NDs stratified by age were depicted in Supplementary Figure S8.
3.4 Regional and national burden
As shown in Table 1, the ASDR of VAD-attributable NDs was negatively correlated with the SDI of a region. In 2021, the highest ASDR of occurred in the low-SDI region [36.31 (95% UI: 23.71–51.36)] (Supplementary Figure S9). The results presented in Table 2 demonstrate the DALYs and YLDs of VAD-attributable NDs stratified by SDI region were depicted in Supplementary Figure S10. From 1990 to 2021, the ASDR showed a declining trend across all SDI regions. The fastest decline of the ASDR occurred in the high-SDI region, with an EAPC of −4.65 (95% CI: −5 to −4.3) (Supplementary Figure S11). Trends in the DALYs and YLDs of VAD-attributable NDs stratified by SDI region were depicted in Supplementary Figure S12.
The top three countries with the highest ASDR for VAD-attributable NDs in 2021 were Somalia [108.6 (95% UI: 68.66–169.75)], Niger [94.12 (95% UI: 61.09–136.29)] and Chad [74.27 (95% UI: 46.6–109.78)] (Figure 2). The world map of the DALYs and YLDs of NDs attributable to VAD was depicted in Supplementary Figure S13. Globally, from 1990 to 2021, the ASDR of VAD-attributable NDs decreased across all 204 countries and regions. And the fastest decline of the ASDR occurred in Maldives (EAPC = -9.8, 95% CI: −10.38 to −9.22), Republic of Korea (EAPC = -9.51, 95% CI: −10.3 to −8.72) and Taiwan (Province of China) (EAPC = -9.12, 95% CI: −9.87 to −8.35) (Figure 3).
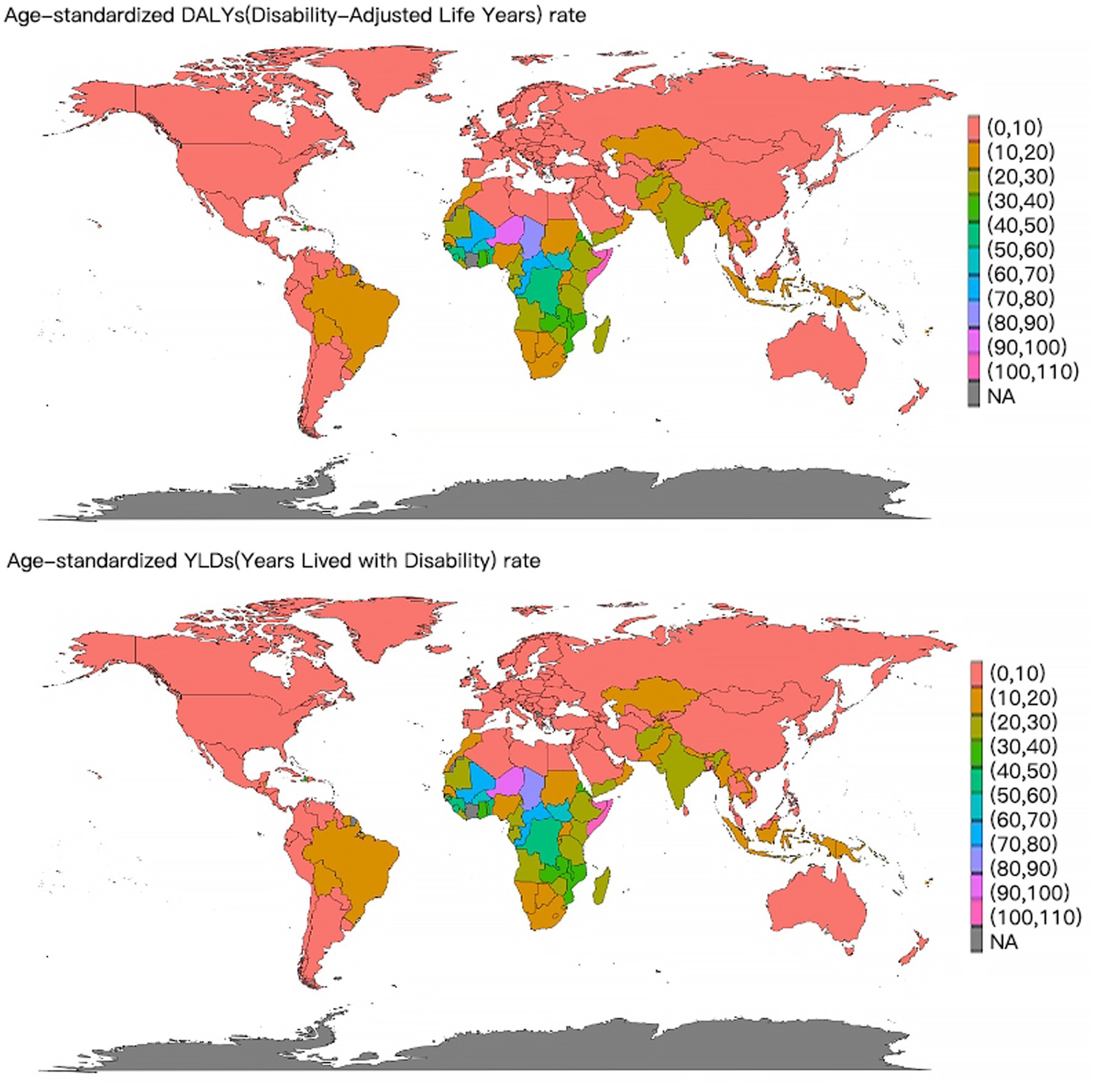
Figure 2. World map of the ASDR and ASYR of nutritional deficiencies attributable to vitamin A deficiency in 2021.
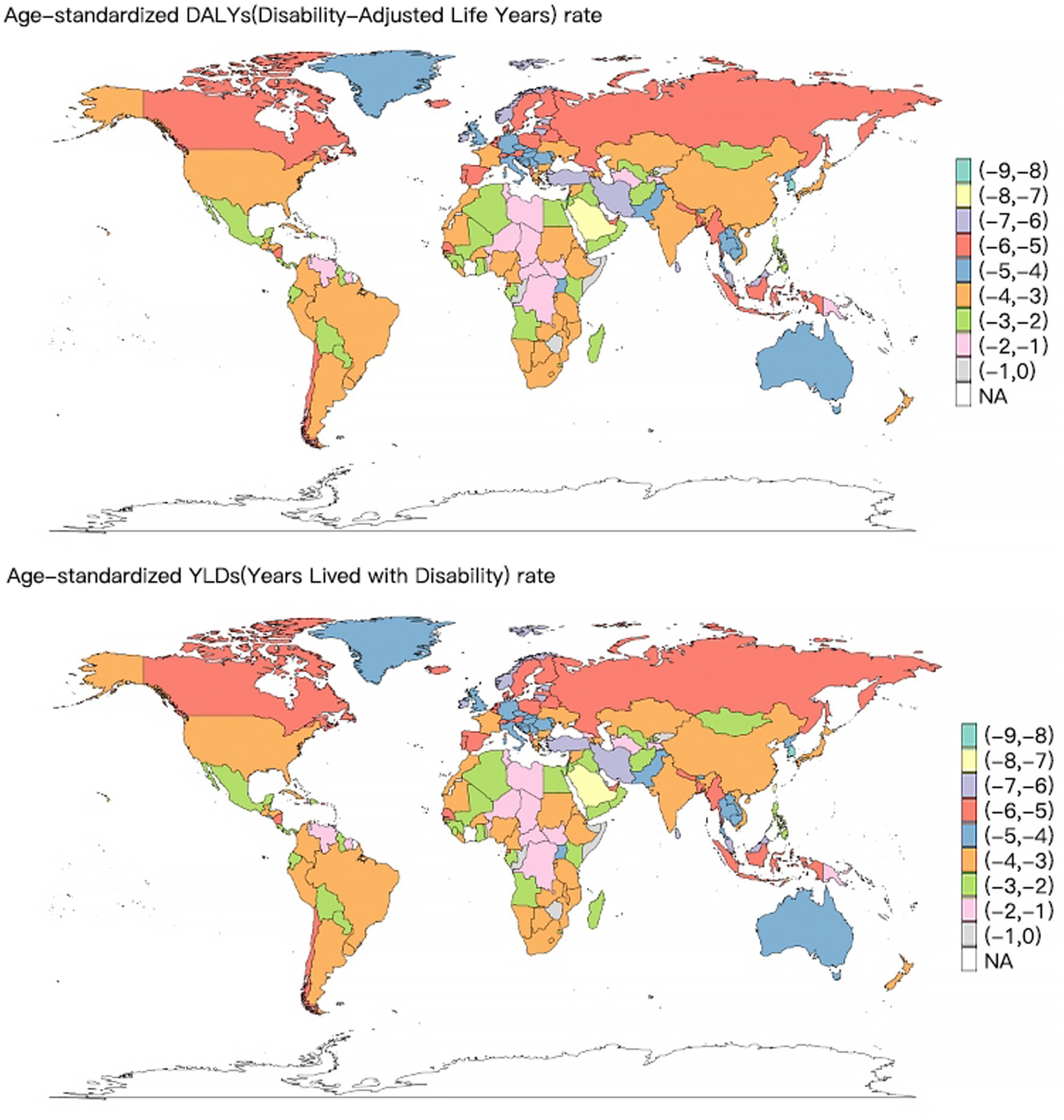
Figure 3. World map of the EAPC of the ASDR and ASYR of nutritional deficiencies attributable to vitamin A deficiency from 1990 to 2021.
3.5 Projections to 2050
Based on the ARIMA model predictions, from 2022 to 2050, the DALYs caused by VAD-attributable NDs are projected to show a slight decrease for both males and females, though the downward trend will be steeper among males. Additionally, the ASDR due to VAD-attributable NDs is expected to decline linearly for both genders during this period, with males demonstrating a more rapid rate of reduction compared to females (Figure 4).
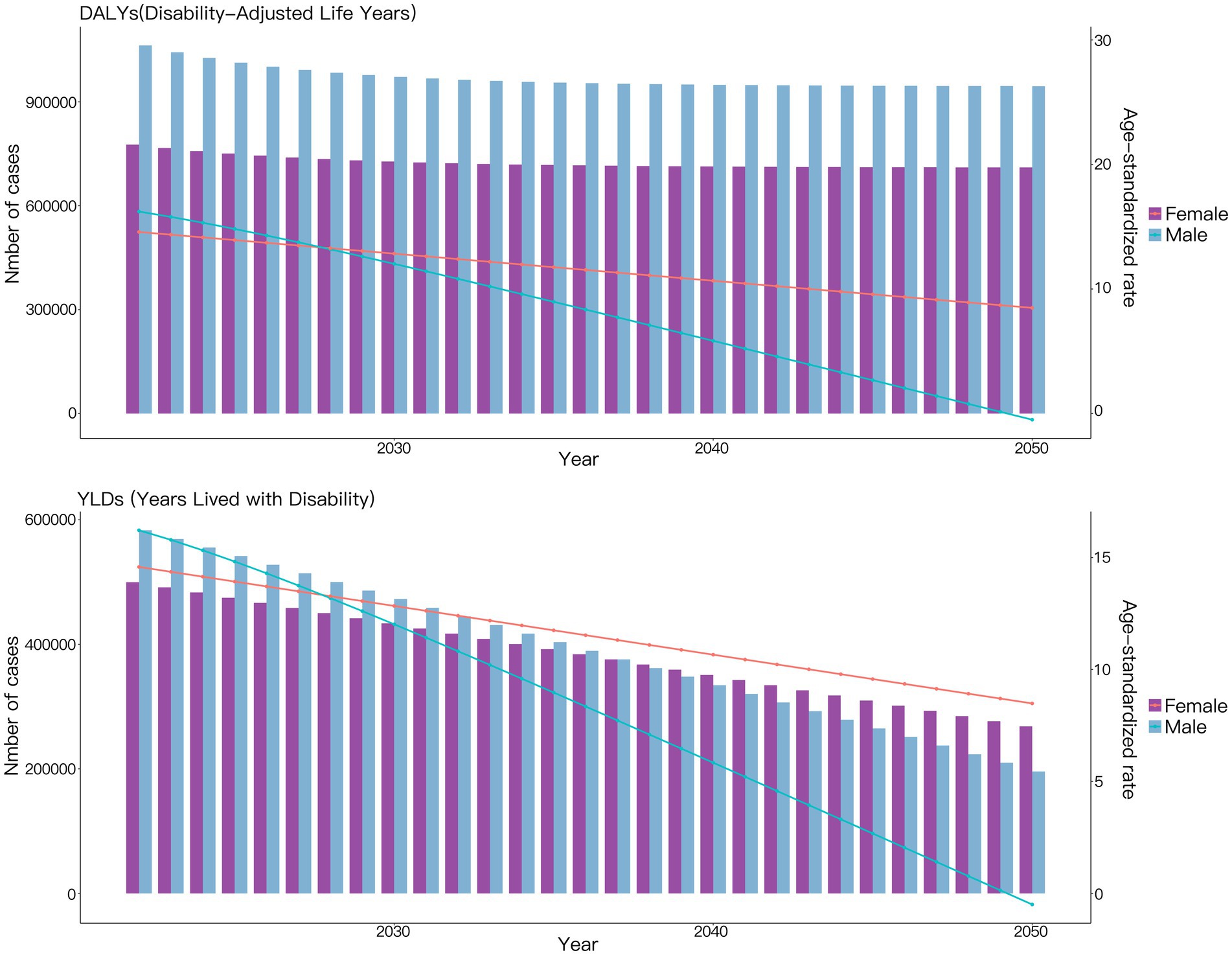
Figure 4. Projections to 2050 of the global burden of nutritional deficiencies attributable to vitamin A deficiency performed using the ARIMA Model.
According to the prediction results of the ES model, differing from the predictions of the ARIMA model, the DALYs caused by NDs attributable to VAD are projected to remain almost unchanged for both males and females between 2022 and 2050. Additionally, the ASDR due to NDs attributable to VAD is expected to show only a slight decline during this period (Figure 5).
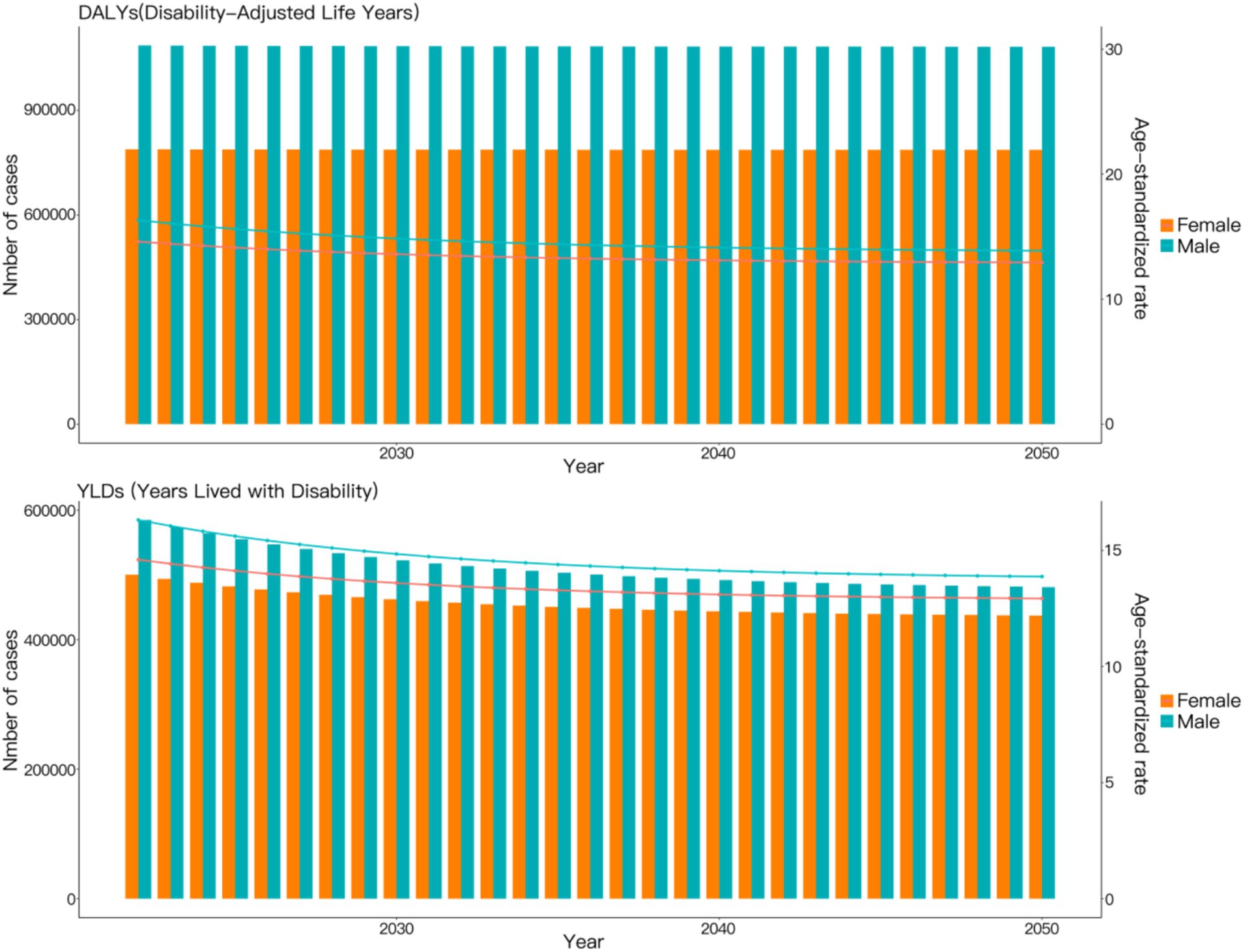
Figure 5. Projections to 2050 of the global burden of nutritional deficiencies attributable to vitamin A deficiency performed using the ES Model.
4 Discussion
NDs remain a pressing worldwide health concern and pose a significant global public health burden, characterized by persistent disparities across geographical regions, age demographics, and socioeconomic strata (31, 32). Building on the evidence from the 2019 GBD study on VAD, this analysis extends to broader NDs trends using updated 2021 GBD data, emphasizing the evolving dynamics of undernutrition, micronutrient deficiencies, and their intersection with emerging issues such as diet-related non-communicable diseases (NCDs) (33, 34). While significant progress has been made in reducing specific forms of malnutrition such as VAD, 2021 data highlight the complex etiology of malnutrition, particularly in many LMICs (35, 36). This discussion synthesizes the latest evidence, identifies persistent gaps, and proposes integrated strategies to address NDs in all its forms.
Vitamin A serves as a crucial nutrient, necessary for preserving visual acuity, strengthening immune defenses, maintaining dermal health, and ensuring proper cellular development (16, 37, 38). Dietary vitamin A can be obtained through both animal sources (like liver and dairy products) and plant sources (like fruits and vegetables), which contain compounds of provitamin A carotenoids (39). Vitamin A deficiency manifests through a spectrum of health issues, including dry skin, night blindness, increased susceptibility to infections, and, in severe cases, permanent blindness and death (40). The WHO recommends daily intakes for vitamin A are 900 mcg for adult men and 700 mcg for adult women to prevent deficiency. In many low-income countries, vitamin A deficiency remains widespread, primarily due to inadequate dietary intake, limited access to fortified foods, and lack of healthcare infrastructure (4, 41, 42). In contrast, overconsumption of vitamin A, often through supplementation, is more common in high-income countries and can lead to toxicity and adverse health effects, such as liver damage and bone fragility (43, 44). Addressing VAD is a critical component of global health strategies, with many nations incorporating vitamin A supplementation programs into national health policies to reduce the burden of related diseases (45).
Children under five remained the most vulnerable group to NDs-related morbidity and mortality (46). In 2021, over 45% of VAD DALYs globally were attributable to this age group, with the highest burden concentrated in sub-Saharan Africa. Early-life deficiencies have lifelong consequences, impairing cognitive development, immune function, and economic productivity (47, 48). The 2021 data highlight a troubling stagnation in reducing stunting and wasting in low-SDI regions, suggesting that current interventions—while effective—are insufficient to address the scale of need. Gender disparities further complicated malnutrition outcomes. Males consistently exhibit higher VAD DALY rates. This may be related to the fact that men generally have a higher basal metabolic rate (BMR), leading to an increased demand for fat-soluble vitamins such as vitamin A, while actual dietary intake often falls short of this requirement. Additionally, occupational exposures (e.g., outdoor labor) and unhealthy lifestyle habits (e.g., smoking, excessive alcohol consumption) may accelerate the depletion of vitamin A reserves (10, 49). Conversely, females face unique risks, including cultural practices favoring male children in resource-limited settings, and sex-specific interactions between supplementation programs and infectious diseases, which affects 30% of women globally (49–52). Adolescence emerges as a critical window for intervention, as nutritional deficits during this period perpetuate intergenerational cycles of malnutrition (53).
Globally, age-standardized rates of VAD incidence and DALYs continued their downward trajectory from 1990 to 2021, reflecting sustained efforts in food fortification, supplementation programs, and improved healthcare access. However, this overall decline conceals significant regional disparities, with low- and middle-income regions-particularly Sub-Saharan Africa and South Asia-experiencing disproportionately higher rates of VAD, still account for over 80% of the global VAD burden (10, 78). The 2021 data reveal that socioeconomic development, as measured by SDI, remains the strongest predictor of NDs outcomes (55). Countries with low SDI values, such as Somalia, Niger, and Mali, exhibit age-standardized VAD incidence rates 30–50 times higher than high-SDI nations like Australia and France (10). These disparities are exacerbated by overlapping crises, including climate change, political instability, and the lingering socioeconomic impacts of the COVID-19 pandemic, which disrupted supply chains and healthcare services in vulnerable regions (54, 56, 57). Although no abrupt changes or trend shifts in the burden of VAD were observed during the COVID-19 pandemic period (2020–2021), and direct evidence remains insufficient to confirm the pandemic’s impact on VAD burden, a limited single-center experience conducted in 2023 since the pandemic has reported significantly lower vitamin A levels in COVID-19 patients (58). This suggests that the influence of the COVID-19 pandemic on VAD burden may exhibit a delayed effect. While undernutrition rates have declined marginally, micronutrient deficiencies (e.g., iron, zinc, and iodine) persist at alarming levels, affecting an estimated 2 billion people worldwide (59). Concurrently, obesity and diet-related NCDs are rising rapidly, even in regions grappling with undernutrition (60). This dual burden reflects systemic failures in food systems, where calorie-dense, nutrient-poor diets dominate due to urbanization, market shifts toward processed foods, and inadequate policies to promote nutrient-rich agricultural production (61, 62).
Poverty, inadequate education, and limited healthcare access are root causes of NDs (63). In low-SDI regions, over 60% of households cannot afford diverse diets rich in vitamins and minerals (64). Food insecurity is compounded by reliance on staple crops with low micronutrient bioavailability, such as maize and rice (65). Even in regions where supplementation programs (e.g., vitamin A capsules) are implemented, coverage remains inconsistent due to logistical challenges, cultural resistance, and funding shortfalls (66). Economic downturns pushed an additional 100 million people into extreme poverty, reducing access to nutritious foods (67). Post-pandemic recovery efforts have largely prioritized economic stabilization over nutrition, risking further divergence between high- and low-SDI regions (68). Beyond economic and educational factors, local dietary cultures profoundly shape nutritional status. Dietary patterns are inherently shaped by the interplay of traditions, customs, and food accessibility. Alongside economic constraints, it can similarly limit access to animal-derived foods containing preformed vitamin A and plant-based foods rich in provitamin A carotenoids (69).
Approximately two-thirds of the 10.8 million child deaths that presently occur can be prevented by available interventions of which vitamin A supplementation (VAS) is one (70–72). Early reports indicated that improved vitamin A status was projected to prevent approximately 1–2 million deaths annually among children aged 1–4 years (73). Randomized controlled trials (RCTs) and cluster-RCTs also supported that VAS was associated with a clinically meaningful reduction in morbidity and mortality in children (8). However, these findings remain subject to certain challenges. Differing from the GBD 2019, VAS was omitted as a covariate in the VAD model due to its lack of statistical significance in the Spatio-Temporal Gaussian Process Regression (ST-GPR) model in GBD 2021and an implausible temporal trend was also observed when the coverage of VAS was included as a covariate in the VAD ST-GPR model (74). This highlights the highly complex nature of evaluating the real-world effectiveness of public health interventions. Although RCTs have established the biological efficacy of VAS, assessing its impact at the population level can be confounded by factors such as data quality and socioeconomic variables. Addressing inequities is equally critical, particularly among marginalized populations, where gender-responsive programs empowering women can drive improved household nutrition (75, 76). Additionally, leveraging disaggregated data and real-time monitoring systems can enhance targeted interventions, while machine learning models predicting NDs risk based on environmental and socioeconomic variables remain underutilized despite their potential (77).
While the GBD 2021 data provide valuable insights into the global burden of NDs attributable to VAD, several limitations warrant consideration. First, underreporting and diagnostic variability in LMICs may lead to an underestimate of VAD prevalence, particularly in conflict zones and remote areas (41). Second, the SDI framework, while useful for identifying high-burden regions, oversimplifies the multidimensional drivers of NDs, such as cultural factors and intra-country disparities (20). Future studies should incorporate granular indicators, such as household dietary diversity and women’s empowerment metrics, to refine inequality analyses. Third, this study thoroughly examines the global and stratified disease burden of NDs attributed to VAD. However, when applying the data to specific regions, caution is needed. Further research is needed to clarify the regional burden of VAD-attributable NDs. In addition, a limitation of our analysis is the absence of formal goodness-of-fit statistics (e.g., AIC/BIC) and cross-validation. This choice was motivated by our goal to present complementary forecasting scenarios rather than to select a superior model. We suggest that subsequent studies could further compare predictions from different models (e.g., ARIMA and ES) to generate more robust forecasting outcomes.
5 Conclusion
The GBD 2021 data highlight the complexity of addressing VAD as a global public health challenge. Despite the burden of VAD in high-income nations having been significantly reduced, LMICs remain a critical focus for global health efforts. Addressing the disparities in VAD prevalence requires comprehensive strategies combining targeted interventions, policy reforms, and cross-sectional collaboration. While the GBD offers extensive coverage, its temporal constraints and potential underreporting in conflict-affected regions and health system-weak areas highlight the need for additional data collection to enhance predictive accuracy. By leveraging the insights from the GBD 2021 data, future research and policy initiatives can better inform the development of sustainable strategies to combat VAD and improve the health outcomes of vulnerable populations worldwide.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found here: https://vizhub.healthdata.org/gbd-results/.
Author contributions
QH: Data curation, Investigation, Methodology, Writing – original draft. JuL: Investigation, Data curation, Writing – original draft. JiL: Data curation, Writing – original draft, Formal analysis. XL: Software, Writing – original draft, Data curation, Investigation. SL: Writing – original draft, Data curation. YB: Data curation, Visualization, Writing – original draft. QZ: Conceptualization, Project administration, Writing – review & editing, Supervision.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
The GBD database has served as a critical foundation in worldwide efforts to comprehend health challenges and shape corresponding policies. We express our sincere appreciation to the GBD database contributors for their generous sharing of these precious data assets.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2025.1673576/full#supplementary-material
References
1. Liu, J, Qi, X, Wang, X, Qin, Y, Jiang, S, Han, L, et al. Evolving patterns of nutritional deficiencies burden in low- and middle-income countries: findings from the 2019 global burden of disease study. Nutrients. (2022) 14:931. doi: 10.3390/nu14050931
2. Chen, J, Li, Z, and Liu, H. Analysis of study global burden of disease in 2021: global, regional, and national burden of nutritional deficiency from 1990 to 2021. Front Nutr. (2025) 11:1540485. doi: 10.3389/fnut.2024.1540485
3. Jiang, W, Li, X, Wang, R, Du, Y, and Zhou, W. Cross-country health inequalities of four common nutritional deficiencies among children, 1990 to 2019: data from the global burden of disease study 2019. BMC Public Health. (2024) 24:486. doi: 10.1186/s12889-024-17942-y
4. Stevens, GA, Bennett, JE, Hennocq, Q, Lu, Y, De-Regil, LM, Rogers, L, et al. Trends and mortality effects of vitamin a deficiency in children in 138 low-income and middle-income countries between 1991 and 2013: a pooled analysis of population-based surveys. Lancet Glob Health. (2015) 3:e528–36. doi: 10.1016/S2214-109X(15)00039-X
5. Chopra, DP, Klinger, MM, and Sullivan, JK. Effects of vitamin a on growth and differentiation of human tracheobronchial epithelial cell cultures in serum-free medium. J Cell Sci. (1989) 93:133–42. doi: 10.1242/jcs.93.1.133
6. Yang, Y, Luo, J, Yu, D, Zhang, T, Lin, Q, Li, Q, et al. Vitamin a promotes Leydig cell differentiation via alcohol dehydrogenase 1. Front Endocrinol (Lausanne). (2018) 9:644. doi: 10.3389/fendo.2018.00644
7. Ishaq, MU, Kunwar, D, Qadeer, A, Komel, A, Safi, A, Malik, A, et al. Effect of vitamin a on maternal, fetal, and neonatal outcomes: an overview of deficiency, excessive intake, and intake recommendations. Nutr Clin Pract. (2024) 39:373–84. doi: 10.1002/ncp.11096
8. Imdad, A, Mayo-Wilson, E, Haykal, MR, Regan, A, Sidhu, J, Smith, A, et al. Vitamin a supplementation for preventing morbidity and mortality in children from six months to five years of age. Cochrane Database Syst Rev. (2022) 3:Cd008524. doi: 10.1002/14651858.CD008524.pub4
9. Radhika, MS, Bhaskaram, P, Balakrishna, N, Ramalakshmi, BA, Devi, S, and Kumar, BS. Effects of vitamin a deficiency during pregnancy on maternal and child health. BJOG. (2002) 109:689–93. doi: 10.1111/j.1471-0528.2002.01010.x
10. Zhao, T, Liu, S, Zhang, R, Zhao, Z, Yu, H, Pu, L, et al. Global burden of vitamin a deficiency in 204 countries and territories from 1990-2019. Nutrients. (2022) 14:950. doi: 10.3390/nu14050950
11. Johnson, EJ, Krasinski, SD, Howard, LJ, Alger, SA, Dutta, SK, and Russell, RM. Evaluation of vitamin a absorption by using oil-soluble and water-miscible vitamin a preparations in normal adults and in patients with gastrointestinal disease. Am J Clin Nutr. (1992) 55:857–64. doi: 10.1093/ajcn/55.4.857
12. Borel, P, Pasquier, B, Armand, M, Tyssandier, V, Grolier, P, Alexandre-Gouabau, MC, et al. Processing of vitamin a and E in the human gastrointestinal tract. Am J Physiol Gastrointest Liver Physiol. (2001) 280:G95–G103. doi: 10.1152/ajpgi.2001.280.1.G95
13. Patil, S, Zamwar, UM, and Mudey, A. Etiology, epidemiology, pathophysiology, signs and symptoms, evaluation, and treatment of vitamin a (retinol) deficiency. Cureus. (2023) 15:e49011. doi: 10.7759/cureus.49011
14. Hombali, AS, Solon, JA, Venkatesh, BT, Nair, NS, and Peña-Rosas, JP. Fortification of staple foods with vitamin a for vitamin a deficiency. Cochrane Database Syst Rev. (2019) 5:Cd010068. doi: 10.1002/14651858.CD010068.pub2
15. Keats, EC, Neufeld, LM, Garrett, GS, Mbuya, MNN, and Bhutta, ZA. Improved micronutrient status and health outcomes in low- and middle-income countries following large-scale fortification: evidence from a systematic review and meta-analysis. Am J Clin Nutr. (2019) 109:1696–708. doi: 10.1093/ajcn/nqz023
16. Stephensen, CB. Vitamin a, infection, and immune function. Annu Rev Nutr. (2001) 21:167–92. doi: 10.1146/annurev.nutr.21.1.167
17. Villamor, E, and Fawzi, WW. Vitamin a supplementation: implications for morbidity and mortality in children. J Infect Dis. (2000) 182:S122–33. doi: 10.1086/315921
18. Semba, RD. Vitamin a, immunity, and infection. Clin Infect Dis. (1994) 19:489–99. doi: 10.1093/clinids/19.3.489
19. Schaible, UE, and Kaufmann, SH. Malnutrition and infection: complex mechanisms and global impacts. PLoS Med. (2007) 4:e115. doi: 10.1371/journal.pmed.0040115
20. Chong, B, Jayabaskaran, J, Kong, G, Chan, YH, Chin, YH, Goh, R, et al. Trends and predictions of malnutrition and obesity in 204 countries and territories: an analysis of the global burden of disease study 2019. EClinicalMedicine. (2023) 57:101850. doi: 10.1016/j.eclinm.2023.101850
21. Suzuki, M, Wang, T, Garretto, D, Isasi, CR, Cardoso, WV, Greally, JM, et al. Disproportionate vitamin a deficiency in women of specific ethnicities linked to differences in allele frequencies of vitamin A-related polymorphisms. Nutrients. (2021) 13:1743. doi: 10.3390/nu13061743
22. Hess, SY, McLain, AC, Lescinsky, H, Brown, KH, Afshin, A, Atkin, R, et al. Basis for changes in the disease burden estimates related to vitamin a and zinc deficiencies in the 2017 and 2019 global burden of disease studies. Public Health Nutr. (2022) 25:2225–31. doi: 10.1017/S1368980021004821
23. DeMaeyer, EM. The WHO programme of prevention and control of vitamin a deficiency, xerophthalmia and nutritional blindness. Nutr Health. (1986) 4:105–12. doi: 10.1177/026010608600400206
24. GBD 2021 Risk Factors Collaborators. Global burden and strength of evidence for 88 risk factors in 204 countries and 811 subnational locations, 1990-2021: a systematic analysis for the global burden of disease study 2021. Lancet. (2024) 403:2162–203. doi: 10.1016/S0140-6736(24)00933-4
25. GBD 2021 Diseases and Injuries Collaborators. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the global burden of disease study 2021. Lancet. (2024) 403:2133–61. doi: 10.1016/S0140-6736(24)00757-8
26. Zhang, M, Yuan, L, Cui, M, Chen, J, Jia, J, Zhao, M, et al. Analysis the burden of breast Cancer among adolescents and young adults using the global burden of disease 2021. Ann Surg Oncol. (2025) 32:2056–69. doi: 10.1245/s10434-024-16648-0
27. GBD 2021 Causes of Death Collaborators. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the global burden of disease study 2021. Lancet. (2024) 403:2100–32. doi: 10.1016/S0140-6736(24)00367-2
28. Zhang, J, Ma, B, Han, X, Ding, S, and Li, Y. Global, regional, and national burdens of HIV and other sexually transmitted infections in adolescents and young adults aged 10-24 years from 1990 to 2019: a trend analysis based on the global burden of disease study 2019. Lancet Child Adolesc Health. (2022) 6:763–76. doi: 10.1016/S2352-4642(22)00219-X
29. Zi, H, He, SH, Leng, XY, Xu, XF, Huang, Q, Weng, H, et al. Global, regional, and national burden of kidney, bladder, and prostate cancers and their attributable risk factors, 1990-2019. Mil Med Res. (2021) 8:60. doi: 10.1186/s40779-021-00354-z
30. Huang, P, and Zhang, J. Global leukemia burden and trends: a comprehensive analysis of temporal and spatial variations from 1990-2021 using GBD (global burden of disease) data. BMC Public Health. (2025) 25:262. doi: 10.1186/s12889-025-21428-w
31. Alao, R, Nur, H, Fivian, E, Shankar, B, Kadiyala, S, and Harris-Fry, H. Economic inequality in malnutrition: a global systematic review and meta-analysis. BMJ Glob Health. (2021) 6:e006906. doi: 10.1136/bmjgh-2021-006906
32. Chamanoor, M, Juneja, RK, Sami, S, Arefin, S, Al-Sabbagh, D, Thota, AN, et al. Disparities in place of death among malnourished individuals in the United States. Cureus. (2024) 16:e55503. doi: 10.7759/cureus.55503
33. Ahmad, R, Akter, F, and Haque, M. Editorial: diet and nutrition for non-communicable diseases in low and middle-income countries. Front Nutr. (2023) 10:1179640. doi: 10.3389/fnut.2023.1179640
34. Lopes, SO, Abrantes, LCS, Azevedo, FM, Morais, NS, Morais, DC, Gonçalves, VSS, et al. Food insecurity and micronutrient deficiency in adults: a systematic review and meta-analysis. Nutrients. (2023) 15:1074. doi: 10.3390/nu15051074
35. Kolčić, I. Double burden of malnutrition: a silent driver of double burden of disease in low- and middle-income countries. J Glob Health. (2012) 2:020303. doi: 10.7189/jogh.02.020303
36. Bruins, M, and Kraemer, K. Public health programmes for vitamin a deficiency control. Commun Eye Health. (2013) 26:69–70. Available online at: https://pubmed.ncbi.nlm.nih.gov/24782583/
37. Varani, J, Warner, RL, Gharaee-Kermani, M, Phan, SH, Kang, S, Chung, JH, et al. Vitamin a antagonizes decreased cell growth and elevated collagen-degrading matrix metalloproteinases and stimulates collagen accumulation in naturally aged human skin. J Invest Dermatol. (2000) 114:480–6. doi: 10.1046/j.1523-1747.2000.00902.x
38. Huang, Z, Liu, Y, Qi, G, Brand, D, and Zheng, SG. Role of vitamin a in the immune system. J Clin Med. (2018) 7:258. doi: 10.3390/jcm7090258
39. Tang, G, Qin, J, Dolnikowski, GG, Russell, RM, and Grusak, MA. Spinach or carrots can supply significant amounts of vitamin a as assessed by feeding with intrinsically deuterated vegetables. Am J Clin Nutr. (2005) 82:821–8. doi: 10.1093/ajcn/82.4.821
40. Roche, FC, and Harris-Tryon, TA. Illuminating the role of vitamin a in skin innate immunity and the skin microbiome: a narrative review. Nutrients. (2021) 13:302. doi: 10.3390/nu13020302
41. Song, P, Adeloye, D, Li, S, Zhao, D, Ye, X, Pan, Q, et al. The prevalence of vitamin a deficiency and its public health significance in children in low- and middle-income countries: a systematic review and modelling analysis. J Glob Health. (2023) 13:04084. doi: 10.7189/jogh.13.04084
42. Mkambula, P, Mbuya, MNN, Rowe, LA, Sablah, M, Friesen, VM, Chadha, M, et al. The unfinished agenda for food fortification in low- and middle-income countries: quantifying Progress, gaps and potential opportunities. Nutrients. (2020) 12:354. doi: 10.3390/nu12020354
43. Fox, R, Stace, N, Wood, K, and French, C. Liver toxicity from vitamin a. JGH Open. (2020) 4:287–8. doi: 10.1002/jgh3.12201
44. Hough, S, Avioli, LV, Muir, H, Gelderblom, D, Jenkins, G, Kurasi, H, et al. Effects of hypervitaminosis a on the bone and mineral metabolism of the rat. Endocrinology. (1988) 122:2933–9. doi: 10.1210/endo-122-6-2933
45. Mayo-Wilson, E, Imdad, A, Herzer, K, Yakoob, MY, and Bhutta, ZA. Vitamin a supplements for preventing mortality, illness, and blindness in children aged under 5: systematic review and meta-analysis. BMJ. (2011) 343:d5094. doi: 10.1136/bmj.d5094
46. Govender, I, Rangiah, S, Kaswa, R, and Nzaumvila, D. Malnutrition in children under the age of 5 years in a primary health care setting. S Afr Fam Pract (2004). (2021) 63:e1–6. doi: 10.4102/safp.v63i1.5337
47. Kar, BR, Rao, SL, and Chandramouli, BA. Cognitive development in children with chronic protein energy malnutrition. Behav Brain Funct. (2008) 4:31. doi: 10.1186/1744-9081-4-31
48. Kirolos, A, Goyheneix, M, Kalmus Eliasz, M, Chisala, M, Lissauer, S, Gladstone, M, et al. Neurodevelopmental, cognitive, behavioural and mental health impairments following childhood malnutrition: a systematic review. BMJ Glob Health. (2022) 7:e009330. doi: 10.1136/bmjgh-2022-009330
49. Nordhagen, S, Bauck, A, and Doledec, D. Gender equity and vitamin a supplementation: moving beyond equal coverage. Food Nutr Bull. (2020) 41:38–49. doi: 10.1177/0379572119860310
50. GBD 2021 Anaemia Collaborators. Prevalence, years lived with disability, and trends in anaemia burden by severity and cause, 1990-2021: findings from the global burden of disease study 2021. Lancet Haematol. (2023) 10:e713–34. doi: 10.1016/S2352-3026(23)00160-6
51. Wei, X, Zhao, L, Fang, H, Chen, M, Piao, W, Ju, L, et al. Deficiency of energy and nutrient and gender differences among Chinese adults: China nutrition and health survey (2015-2017). Nutrients. (2024) 16:2371. doi: 10.3390/nu16142371
52. Jiang, S, Liu, J, Qi, X, Wang, R, Wang, X, Wang, K, et al. Global, regional, and National Estimates of nutritional deficiency burden among reproductive women from 2010 to 2019. Nutrients. (2022) 14:832. doi: 10.3390/nu14040832
53. Arlinghaus, KR, Truong, C, Johnston, CA, and Hernandez, DC. An intergenerational approach to break the cycle of malnutrition. Curr Nutr Rep. (2018) 7:259–67. doi: 10.1007/s13668-018-0251-0
54. Dallazen, C, Tietzmann, DC, da Silva, SA, Nilson, EAF, Gonçalves, VSS, Lang, RMF, et al. Vitamin a deficiency and associated risk factors in children aged 12-59 months living in poorest municipalities in the south region of Brazil. Public Health Nutr. (2023) 26:132–42. doi: 10.1017/S1368980022000325
55. Okutse, AO, and Athiany, H. Socioeconomic disparities in child malnutrition: trends, determinants, and policy implications from the Kenya demographic and health survey (2014 - 2022). BMC Public Health. (2025) 25:295. doi: 10.1186/s12889-024-21037-z
56. Al-Saidi, M. Caught off guard and beaten: the Ukraine war and food security in the Middle East. Front Nutr. (2023) 10:983346. doi: 10.3389/fnut.2023.983346
57. McGowan, VJ, and Bambra, C. COVID-19 mortality and deprivation: pandemic, syndemic, and endemic health inequalities. Lancet Public Health. (2022) 7:e966–75. doi: 10.1016/S2468-2667(22)00223-7
58. Li, T, Cui, X, Li, X, Yang, J, Wang, H, Yang, J, et al. Association between vitamin a and D status and the risk of COVID-19 in the elderly population: a single-center experience. J Inflamm Res. (2025) 18:8233–41. doi: 10.2147/JIR.S522566
59. Ramakrishnan, U. Prevalence of micronutrient malnutrition worldwide. Nutr Rev. (2002) 60:S46–52. doi: 10.1301/00296640260130731
60. Bhurosy, T, and Jeewon, R. Overweight and obesity epidemic in developing countries: a problem with diet, physical activity, or socioeconomic status? ScientificWorldJournal. (2014) 2014:964236. doi: 10.1155/2014/964236
61. Ren, Y, Castro Campos, B, Peng, Y, and Glauben, T. Nutrition transition with accelerating urbanization? Empirical evidence from rural China. Nutrients. (2021) 13:921. doi: 10.3390/nu13030921
62. Seferidi, P, Hone, T, Duran, AC, Bernabe-Ortiz, A, and Millett, C. Global inequalities in the double burden of malnutrition and associations with globalisation: a multilevel analysis of demographic and health surveys from 55 low-income and middle-income countries, 1992-2018. Lancet Glob Health. (2022) 10:e482–90. doi: 10.1016/S2214-109X(21)00594-5
63. Ma, ZF, Wang, CW, and Lee, YY. Editorial: malnutrition: a cause or a consequence of poverty? Front Public Health. (2021) 9:796435. doi: 10.3389/fpubh.2021.796435
64. Nisa, H, and Kurotani, K. Editorial: diet quality, socioeconomic differences, and health disparities. Front Nutr. (2023) 10:1250439. doi: 10.3389/fnut.2023.1250439
65. Yilmaz, H, and Yilmaz, A. Hidden hunger in the age of abundance: the nutritional pitfalls of modern staple crops. Food Sci Nutr. (2025) 13:e4610. doi: 10.1002/fsn3.4610
66. Wallace, SK. Global health in conflict. Understanding opposition to vitamin a supplementation in India. Am J Public Health. (2012) 102:1286–97. doi: 10.2105/AJPH.2012.300759
67. Munialo, CD, and Mellor, DD. A review of the impact of social disruptions on food security and food choice. Food Sci Nutr. (2024) 12:13–23. doi: 10.1002/fsn3.3752
68. Panghal, A, Mor, RS, Kamble, SS, Khan, SAR, Kumar, D, and Soni, G. Global food security post COVID-19: dearth or dwell in the developing world? Agron J. (2022) 114:878–84. doi: 10.1002/agj2.20932
69. Hong, S. Essential micronutrients in children and adolescents with a focus on growth and development: a narrative review. J Yeungnam Med Sci. (2025) 42:25. doi: 10.12701/jyms.2025.42.25
70. Jones, G, Steketee, RW, Black, RE, Bhutta, ZA, and Morris, SS. Bellagio child survival study group. How many child deaths can we prevent this year? Lancet. (2003) 362:65–71. doi: 10.1016/S0140-6736(03)13811-1
71. Ahmad, OB, Lopez, AD, and Inoue, M. The decline in child mortality: a reappraisal. Bull World Health Organ. (2000) 78:1175–91.
72. Sanjoaquin, MA, and Molyneux, ME. Malaria and vitamin a deficiency in African children: a vicious circle? Malar J. (2009) 8:134. doi: 10.1186/1475-2875-8-134
73. Humphrey, JH, West, KP Jr, and Sommer, A. Vitamin a deficiency and attributable mortality among under-5-year-olds. Bull World Health Organ. (1992) 70:225–32.
74. Global Burden of Disease (GBD) (2021). Methods appendices. Available online at: https://www.healthdata.org/gbd/methods-appendices-2021/vitamin-deficienc.
75. Lufuke, M, Bai, Y, Fan, S, and Tian, X. Women's empowerment, food security, and nutrition transition in Africa. Int J Environ Res Public Health. (2022) 20:254. doi: 10.3390/ijerph20010254
76. Christian, AK, Atiglo, DY, Okyere, MA, Obeng-Dwamena, A, Marquis, GS, and Jones, AD. Women's empowerment, children's nutritional status, and the mediating role of household headship structure: evidence from sub-Saharan Africa. Matern Child Nutr. (2023) 19:e13520. doi: 10.1111/mcn.13520
77. Silva, BVRE, Rad, MG, Cui, J, M, MC, and Pan, K. A Mobile-based diet monitoring system for obesity management. J Health Med Inform. (2018) 9:307. doi: 10.4172/2157-7420.1000307
Keywords: nutritional deficiencies, vitamin A deficiency, global burden of disease, future predictions, public health
Citation: Hu Q, Lyu J, Li J, Lin X, Li S, Bu Y and Zhao Q (2025) A comprehensive analysis of vitamin a deficiency burden and trends: insights from the global burden of disease study 2021 and future predictions to 2050. Front. Nutr. 12:1673576. doi: 10.3389/fnut.2025.1673576
Edited by:
U. Venkatesh, All India Institute of Medical Sciences Gorakhpur, IndiaCopyright © 2025 Hu, Lyu, Li, Lin, Li, Bu and Zhao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Qianlei Zhao, d3ptY3pocWxAd211LmVkdS5jbg==