 Jonas J. de Paula1,2*
Jonas J. de Paula1,2* Maria A. Bicalho1,3,4
Maria A. Bicalho1,3,4 Rafaela T. Ávila1,4Marco T. G. Cintra4
Rafaela T. Ávila1,4Marco T. G. Cintra4 Breno S. Diniz1,5
Breno S. Diniz1,5 Marco A. Romano-Silva1,5
Marco A. Romano-Silva1,5 Leandro F. Malloy-Diniz1,5
Leandro F. Malloy-Diniz1,5- 1Faculdade de Medicina, Instituto Nacional de Ciência e Tecnologia de Medicina Molecular, Universidade Federal de Minas Gerais, Belo Horizonte, Brazil
- 2Department of Psychology, Faculdade de Ciências Médicas de Minas Gerais, Belo Horizonte, Brazil
- 3Department of Internal Medicine, Faculdade de Medicina, Universidade Federal de Minas Gerais, Belo Horizonte, Brazil
- 4Reference Center for Geriatrics Instituto Jenny de Andrade Faria, Universidade Federal de Minas Gerais, Belo Horizonte, Brazil
- 5Department of Mental Health, Faculdade de Medicina, Universidade Federal de Minas Gerais, Belo Horizonte, Brazil
Depressive symptoms are associated with cognitive-functional impairment in normal aging older adults (NA). However, less is known about this effect on people with mild Cognitive Impairment (MCI) and mild Alzheimer's disease dementia (AD). We investigated this relationship along with the NA-MCI-AD continuum by reanalyzing a previously published dataset. Participants (N = 274) underwent comprehensive neuropsychological assessment including measures of Executive Function, Language/Semantic Memory, Episodic Memory, Visuospatial Abilities, Activities of Daily Living (ADL), and the Geriatric Depression Scale. MANOVA, logistic regression and chi-square tests were performed to assess the association between depression and cognitive-functional performance in each group. In the NA group, depressed participants had a lower performance compared to non-depressed participants in all cognitive and functional domains. However, the same pattern was not observed in the MCI group or in AD. The results suggest a progressive loss of association between depression and worse cognitive-functional performance along the NA-MCI-AD continuum.
Introduction
Depressive symptoms and cognitive impairment are common in older adults and often coexist in an individual patient. The pattern of cognitive impairment associated with depressive symptoms involves executive dysfunction, reduced processing speed, and deficits in episodic memory (Butters et al., 2004; Sexton et al., 2012; de Paula et al., 2013a), while global intellectual ability, language skills, visuospatial abilities, and semantic processing are usually spared (Naismith et al., 2003). Furthermore, late-life depression is a risk factor for cognitive decline and dementia, in particular Alzheimer's disease dementia (AD) and vascular dementia (Diniz et al., 2013).
The neurobiological mechanisms connecting the depressive symptoms with cognitive and functional performance are heterogeneous. Naismith et al. (2012) reviewed evidences from different types of studies, which discussed changes in monoamine systems dysfunction, hormonal and immunologic changes, inflammatory processes, and alterations on genes expression. These different mechanisms may increase neurodegenerative and vascular factors, which may mediate the cognitive and functional changes associated with depression (Butters et al., 2008). However, as reviewed by Panza et al. (2010), there is an important overlap between depression, mild cognitive impairment (MCI) and dementia: depression may overlap with clinical MCI, may be a reaction to the initial symptoms of MCI, may be one of the behavioral manifestations of MCI, or may mask a clinical MCI. As reviewed by the authors, differences in the studies settings and design, participants' characteristics, and the procedures to diagnose depression and MCI may contribute to the inconsistency found among the studies, including the prevalence of these conditions, its cognitive features and risk of conversion to dementia.
Despite the well-documented impact of depressive symptoms on cognition, the relationship of symptoms' intensity and cognitive performance on older adults with neurocognitive disorders, in particular MCI and AD, is controversial. Previous studies found no association between depressive symptoms and neuropsychological performance in mild AD or MCI patients. Bangen et al. (2010) assessed depressed and non-depressed AD patients with a comprehensive neuropsychological battery and found no differences on the cognitive performance of these participants. On the other hand, AD patients with depression showed a greater impairment in attention and executive function tests when compared to non-depressed AD patients in another study (Nakaaki et al., 2007). A recent study showed that depressive symptoms are related to the cognitive decline in AD, even after controlling for baseline cognitive status (Zahodne et al., 2013). The controversy occurs on the relationship between depression and functional performance. Depressive symptoms are associated with poorer performance on activities of daily living (ADL) in community-dwelling and institutionalized older adults (Nyunt et al., 2012; Tomita and Burns, 2013; de Paula et al., 2015a), and are important predictors of functional status in MCI subjects (Bombin et al., 2012). The presence of cognitive impairment and comorbid depressive symptoms seems to lead to worse functional outcomes (Wadsworth et al., 2012). On the other hand, different studies did not find a significant association between depressive symptoms and functional status along the normal aging (NA)—MCI—AD continuum (Reppermund et al., 2011).
Altogether, these results suggest that depressive symptoms may have a distinct impact on cognitive and functional performance in normal aging, MCI and AD. In this sense, the aim of the present study is to evaluate how depressive symptoms moderate the cognitive and functional performance along this continuum. We have reanalyzed a dataset used in previous studies (de Paula et al., 2013b, 2014, 2015a).
Materials and Methods
Participants
We included 274 older adults in the present study from a convenience sample. This study was approved by the local ethics board (registry 334/06). All subjects gave written informed consent for participation. The caregivers of dementia patients had also filled the consent form. The study is in accordance with the Declaration of Helsinki. These participants and their data were described in previously published studies (de Paula et al., 2013b, 2014, 2015a). Participants were evaluated at the outpatient geriatric clinic in the Federal University of Minas Gerais, Brazil. Patients which in primary-care medical assessment had memory complains or voluntarily asked for a cognitive assessment were referred for the outpatient clinic, where a comprehensive assessment was performed and they were subsequently invited for participation. Most of these patients has a very low formal education (below 5 years) and low socioeconomic status.
Figure 1 shows the methods used for patient's diagnoses and the methods used for this research. The Brazilian version of the Mattis Dementia Rating Scale (Porto et al., 2003), the Mini-Mental State Examination (MMSE; Folstein et al., 2001), subtests of the CERAD Neuropsychological Battery (Morris et al., 1989), and the Clinical Dementia Rating (CDR; Morris, 1993) were adopted. CDR scores below 1 are not indicative of dementia, while those equal or above this value are indicative of mild (1), moderate (2), or severe (3) dementia (Morris, 1993). Only participants with CDR scores equal or below 1 were included. The performance on cognitive tests was adjusted for age and educational status, based on Brazilian norms, and were previously validated for the diagnosis of mild AD and MCI (Brucki et al., 2003; Porto et al., 2003; Nitrini et al., 2004; Foss et al., 2013; Table 1 shows the participants sociodemographic characteristics, performance in cognitive tests used for diagnosis and the median for each test based in normative data).
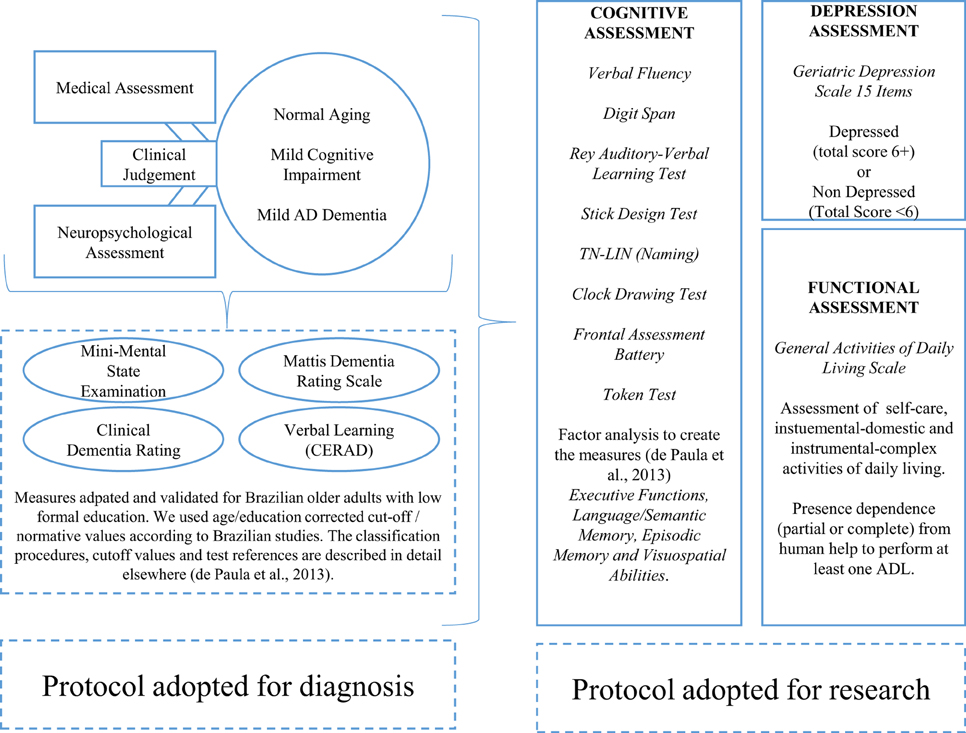
Figure 1. Description of the protocol used for participant's diagnosis/classification, and procedures adopted for this study. Participants initially underwent a medical and neuropsychological assessment for diagnostic procedures. In all, 274 older adults were divided into Normal Aging (NA, N = 96), mild cognitive impairment (MCI, N = 85), mild dementia, and Alzheimer's disease dementia (AD, N = 93). After diagnosis, they performed the procedures of the study, involving the assessment of cognitive functioning, depression and activities of daily living.
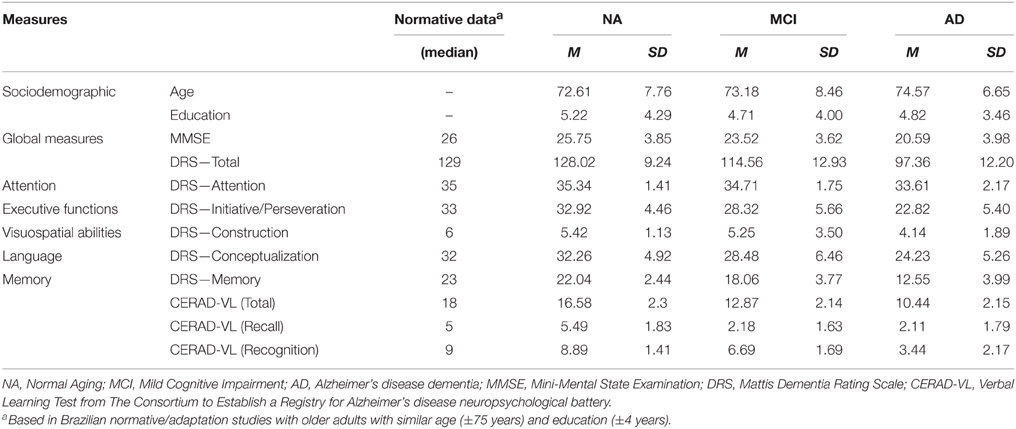
Table 1. Participant's description in sociodemographic and cognitive measures used for diagnosis.
Cognitive status was adjudicated in expert multidisciplinary meetings taking into account clinical, cognitive assessment, laboratorial, and neuroimaging data when available. We performed the diagnosis of probable AD according to the NINCDS-ADRDA criteria (McKhann et al., 1984). It involved cognitive impairment objectively assessed by neuropsychological tests of episodic memory and at least on other cognitive domain (Executive Functions, Visuospatial Abilities, and Language/Semantic Memory) from subtests of the Brazilian versions of the CERAD Neuropsychological Battery and the Mattis Dementia Rating Scale; functional impairment when compared to a previous level of performance (assessed by the functional components of the CDR and by a clinical interview conducted by an experienced geriatrician); insidious onset; clear-cut report of cognitive/functional decline; and no evidence of major neurologic or psychiatric conditions which could respond for the symptom.
The diagnosis of MCI was done according to the following criteria, adapted from Petersen et al. (2001): (1) subjective cognitive complaint, preferably corroborated by an informant; (2) objective impairment in the performance on specific cognitive tests of the assessment battery (verbal learning test from the CERAD battery and subscales from the Mattis Dementia Rating Scale); (3) preserved global cognitive functioning [MMSE above the cut-off for dementia adjusted for education (as in Brucki et al., 2003), and CDR < 1]; (4) preserved or minimal impairments in ADL assessed by a clinical interview and the functional components of the CDR; (5) not demented. The MCI patients included on the study has symptoms and progression characteristic of Alzheimer's disease (amnestic presentation—deficits in learning and recall of new information, insidious onset, and clear-cut history of worsening of cognition by caregiver report).
We also assessed older adults with no evidence of cognitive impairment in the screening protocol to form a control group without clinical history suggestive of Alzheimer's disease. These participants composed the normal aging group (NA). We invited them for participation in the same institution where we assessed the MCI and AD participants. They do not show a CDR suggestive of dementia (CDR < 1) and has cognitive tests above the cut-off values for cognitive impairment. Participants with subjective cognitive complaints did not have a symptomatology or clinical course suggestive of Alzheimer's disease (as cited in AD and MCI participant's description). These participants have none or discrete functional impairment assessed in a clinical interview, no history of neurological diseases and no sensorial or motor impairment, which may compromise the neuropsychological assessment.
Our final sample consisted of 274 participants: 62 NA non-depressed, 34 NA depressed 63 MCI non-depressed, 22 MCI depressed, 66 AD non-depressed, and 27 AD depressed. We described these previous in previously published studies (de Paula et al., 2013b, 2014, 2015a).
Assessment of Depressive Symptoms
We evaluated the presence of depression by the Brazilian version of the Geriatric Depression Scale-15 (GDS-15; Sheikh and Yeasavage, 1986). The cut-off score 5/6 (non-case/case) was chosen to determine the presence of clinically significant depressive. We adopted this cut-off due to its good validity for detection of significant depressive symptoms in our population, which includes patients with low socioeconomic status, low formal education, and cognitive complaints (Almeida and Almeida, 1999). A validation study propose this cut-off for the detection of depression according to the DSM-IV and ICD-10 criteria (Almeida and Almeida, 1999).
The use of the GDS for the detection of depressive symptoms and diagnosis of a depressive episode in AD patients is controversial. Some studies report a loss of validity in patients with dementia (Feher et al., 1992), while others do not (Brown et al., 2007). The previous reports suggests that patients in moderate or severe dementia may not report depressive symptoms accurately. To reduce these biases we selected only patients with mild dementia for the AD group (CDR ≤ 1). Due to participant's low formal education, to ensure the questions comprehension and validity of the report the examiner read the questions aloud. The diagnosis of AD, MCI or NA, was irrespective of the GDS-15 scores.
Neuropsychological Assessment (Research Protocol)
All participants underwent a comprehensive neuropsychological assessment protocol focused on the assessment of executive functions, memory, language, and visuospatial cognitive domains. The protocol was designed for the assessment of older adults with low formal education level. We detailed these procedures in a previous study conducted in this sample (de Paula et al., 2013b). We have not used these neuropsychological tests were for diagnostic purpose, and they were administered by trained neuropsychologists.
The battery is comprised by the following tests: Digit Span Forward and Backward (Kessels et al., 2008), verbal fluency “fruits,” “animals,” and letter (“S”) (de Paula et al., 2013b), and the Frontal Assessment Battery (Dubois et al., 2000) [Factor Executive Functions]; the three components of the Laboratory of Neuropsychological Investigations Naming Test (Malloy-Diniz et al., 2007a) [Factor Language/Semantic Memory]; the Brazilian Portuguese Rey Auditory-Verbal Learning Test (Malloy-Diniz et al., 2007b) [Factor Episodic Memory]; Token Test components of attention and comprehension (De Renzi and Faglioni, 1978; de Paula et al., 2013b), the Clock Drawing Test (Shulman, 2000); and the Stick Design Test (Baiyewu et al., 2004) [Factor Visuospatial Abilities]. Supplementary Table 1 shows the participant's performance in each neuropsychological measures, its clinical cut-offs and maximum possible score. Supplementary Table 2 shows the factor analysis.
Activities of Daily Living Assessment
Participant's caregivers (usually spouses or other relatives) answered an adapted Activities of Daily Living Scale (ADL) based on the Lawton and Brody (1969), and Katz et al. (1970) indexes of ADL. The scale assess 13 basic and instrumental activities (de Paula et al., 2014). The scale consists of three ADL aspects: Self-Care (Basic ADL), Domestic (Instrumental ADL performed at home), and Complex (Instrumental ADL involving activities outside home, financial management and medication control). Scores on Basic ADL range from 0 to 10, and 0 to 8 on Domestic or Complex ADL; with lower scores indicating greater impairment. Due to data distribution, we categorized the functional performance (impairment × no-impairment) based in dependence of human help (full or partial) to perform at least one ADL. Supplementary Table 1 shows the participant's functional performance in each subscale, while Supplementary Table 3 shows the frequency of responses by each group, stratified by depression status, in each specific ADL.
Statistical Analysis
Prior to this study analysis, we carried out a factor analysis with all neuropsychological measures for data reduction, as previously reported (de Paula et al., 2013b, 2015a). Principal axis factoring and oblique rotation were adopted. We extracted and saved the cognitive factors as standardized (z-Scores) variables based on non-depressed NA performance. The procedures produced four distinct cognitive factors (Executive Functions, Language/Semantic Memory, Episodic Memory, and Visuospatial Abilities), used as dependent variables in the multivariate analysis. All the factors showed adequate factor loadings and internal consistency assessed by the Cronbach's Alpha (all >0.800).
For cognitive data we carried out MANOVA analysis to assess the main effect of group (NA × MCI × AD) and clinically significant depressive symptoms according to GDS cut-off (Depressed × Non-Depressed) on each neuropsychological factor. Age and education were used as covariates as they are significantly correlated with cognitive performance in these subjects (Supplementary Table 4). We analyzed the MANOVA residuals to check if their distribution meet the analysis assumptions. We reported effect sizes by partial eta-squared (η). Since neither age nor education correlated with functional measures after controlling for global cognitive functioning in this sample (Supplementary Table 4), we adopted a multinomial logistic regression model to compare the frequency of impairment in each aspect of ADL. Group and depression were added as fixed factors and chi-square tests were adopted for post-hoc analysis. Effect sizes for chi-square tests were estimated by the Cramér's phi (φ). Post-hoc analysis comparisons were corrected for multiple comparisons.
We performed most of the statistical procedures on the SPSS 20.0. Statistical significance was established at 0.05 (two-tailed). Power analysis for main effects was done in G-Power software (Faul et al., 2007). For MANOVA, our sample size (n = 274) has a 99% power to detect a large effect size, 86% power to detect a moderate effect size and only 17% power to detect a small effect size. We computed power analysis for logistic regression based in the effect sizes represented by different odds ratio, as proposed by Chen et al. (2010): 1.68 (small effect size), 3.47 (medium effect size), 6.71 (large effect size). Based on our sample size we have 93% power to detect a small effect size and 99% power to detect a small or large effect size in logistic regression.
Results
Our final sample consisted of 274 participants: 62 NA non-depressed, 34 NA depressed, 63 MCI non-depressed, 22 MCI depressed, 66 AD non-depressed and 27 AD depressed. We did not observe a statistically significant difference in the distribution of depression according to diagnostic groups (χ2 = 2.05, p = 0.359). Table 2 shows neuropsychological and functional data for each subgroup. Supplementary Tables 1, 2 shows the scores in specific neuropsychological tests and functional status in each ADL. Performance of NA participants were relatively similar to what is expected for older adults with low formal education, according to Brazilian normative studies, but lower than what is expected for young adults (Brucki and Rocha, 2004; Banhato and Nascimento, 2007; Malloy-Diniz et al., 2007b; Aprahamian et al., 2009; Moreira et al., 2011; de Paula et al., 2015b).
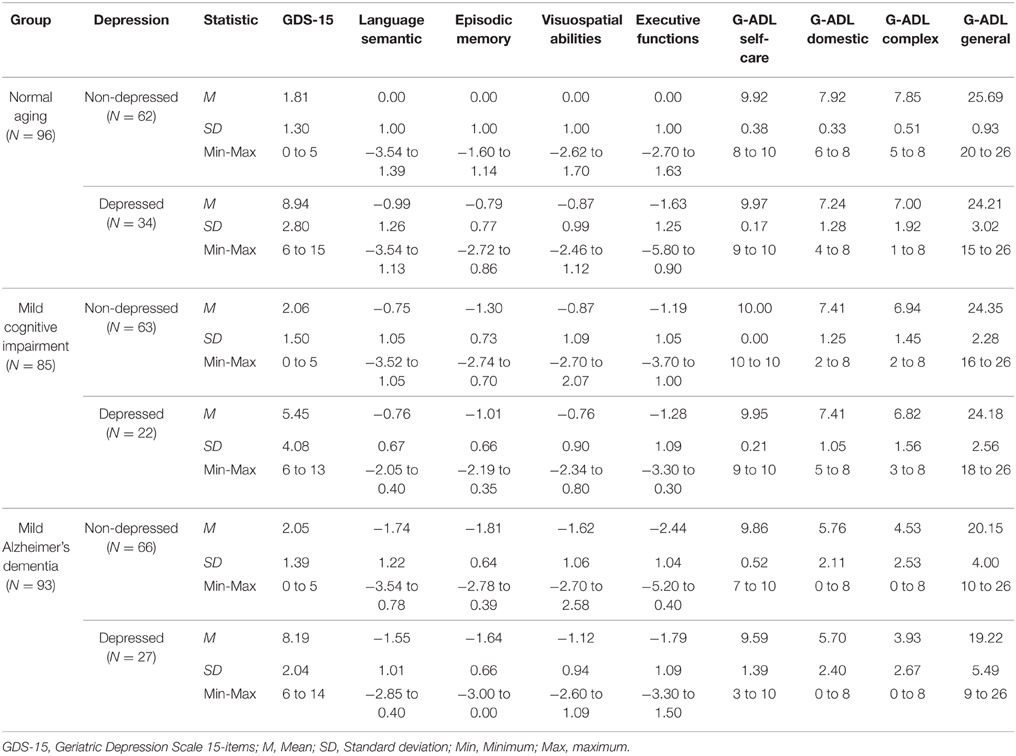
Table 2. Participant's scores in GDS-15 and performance in the neuropsychological factors obtained by factor analysis of the research protocol stratified by group and depression.
Since, in previous studies we explored the effect of group in the neuropsychological and functional measures (de Paula et al., 2013b, 2014), we focused in the interaction between group and depression in cognitive and functional measures. We found significant interactions for all measures (Table 3).
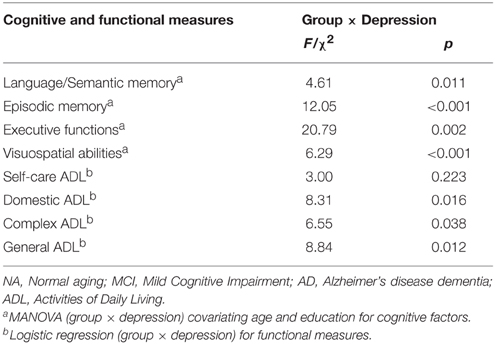
Table 3. Interactions between group (NA × MCI × AD) and depression (present × absent) in cognitive factors and functional measures.
For cognitive measures, interactions were significant between depressed and non-depressed NA participants, and the largest effect size occurred in executive functions (ηp2 = 0.37), followed by episodic memory (ηp2 = 0.21), language/semantic memory (ηp2 = 0.14) and visuospatial abilities (ηp2 = 0.12). However, in MCI and AD participant depression was not associated with cognitive performance (non-significant effect sizes ranging from ηp2 < 0.01 to ηp2 = 0.03). Differences remained significant after multiple comparisons correction. These data is show in Table 4 and Figure 2.
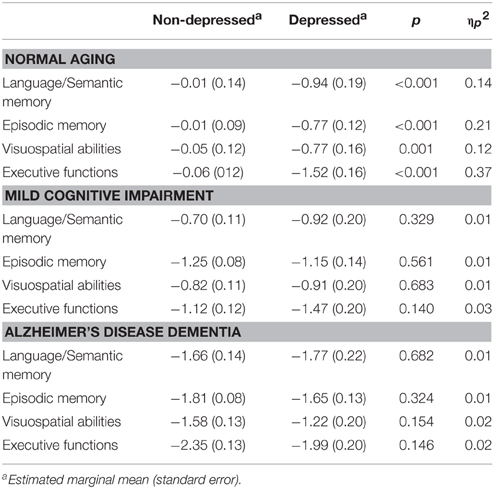
Table 4. Main effect of depression in cognitive functions and group comparison's after covariating age and education.
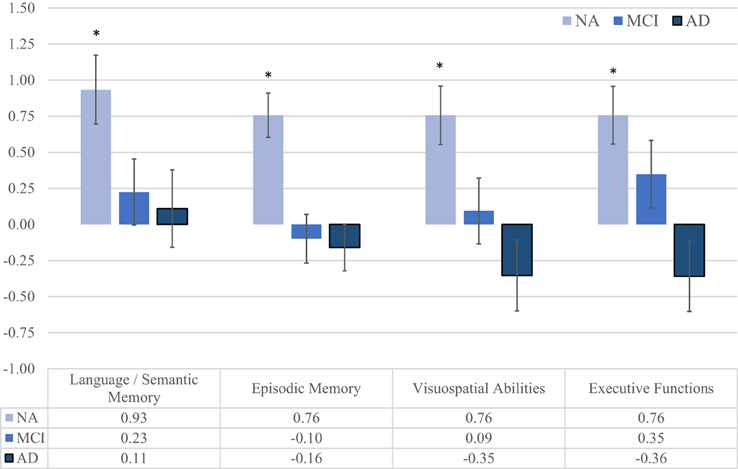
Figure 2. Differences between the estimated marginal means (with age and education as covariates) on neuropsychological measures of depressed and non-depressed participants in each of the three groups. When we compared depressed and non-depressed participants in each group, we found significant differences only in NA participants. In this group, participants with clinically significant symptoms of depression showed lower performance in Executive Functions (p < 0.001, ηp2 = 0.37), Episodic Memory (p < 0.001, ηp2 = 0.21), Language/Semantic Memory (p < 0.001, = 0.14), and Visuospatial Abilities (p = 0.001, ηp2 = 0.12). Effect sizes from MCI and AD patients ranged from *p < 0.01 to 0.03.
The interaction for group × depression in self-care ADL was not significant (p = 0.223). For instrumental-domestic activities, we found a significant difference in the NA group (φ = 0.341), where difficulties were more frequent in depressed (32%) than non-depressed (6%) participants. The same pattern occurred for instrumental-complex activities (φ = 0.314), where depressed patients (35%) showed more difficulties than non-depressed participants (10%). Considering all the 13 activities, a significant difference also occurred in the NA group (φ = 0.333), where depressed participants were more likely to show impairment in at least one activity (47%) than non-depressed participants (16%). However, for both MCI and AD participants, no significant differences were found on instrumental-domestic, instrumental-complex, or in the general index of ADL (non-significant effect sizes ranging from φ = 0.004 to φ = 0.185). Differences remained significant after multiple comparisons correction. Table 5 and Figure 3 show these analyses.
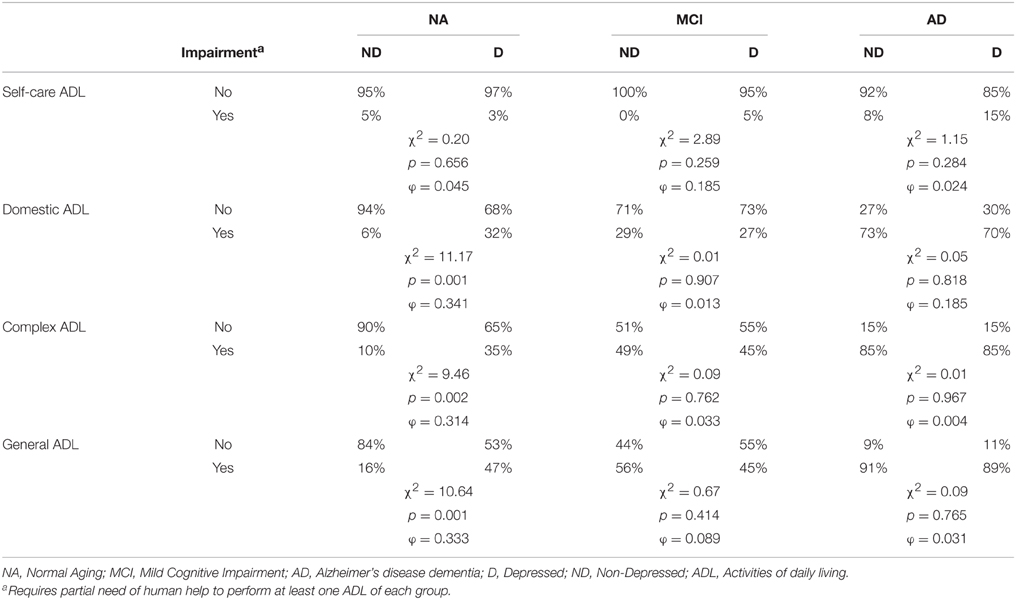
Table 5. Frequency of impairment in at least one activity of daily living in each group and group comparison's (chi-square test) between depressed and non-depressed participants.
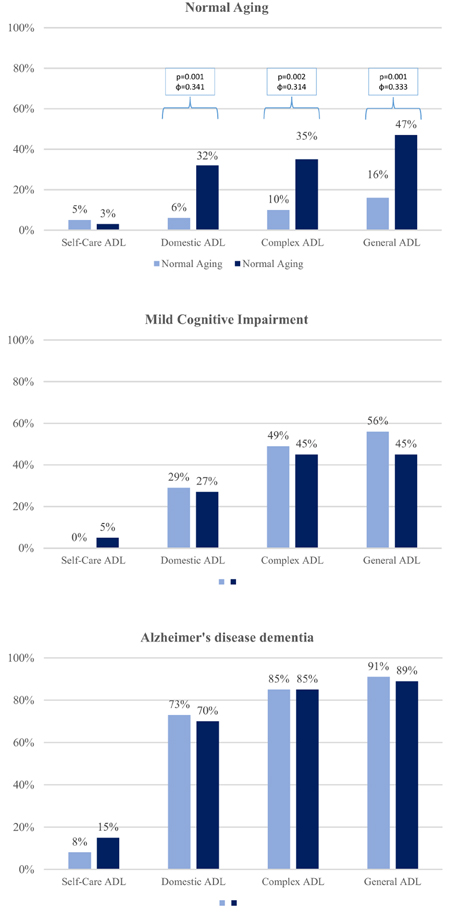
Figure 3. Associations between the frequency deficits in different types of ADL and the presence of clinically significant symptoms of depression in each group. We found significant differences in frequency of impairment (partial or complete) of at least one ADL and the presence of clinically significant symptoms of depression only in the NA group. Impairment in instrumental-domestic ADL (p = 0.001, φ = 0.341), instrumental-complex ADL (p = 0.002, φ = 0.314), and ADL general (p = 0.001, φ = 0.333) were more frequent in participants with clinically significant depressive Symptoms. The association between depression and ADL was found in MCI or AD participants (effect sizes ranged from 0.004 to 0.185).
Discussion
The present results suggest that the association of depressive symptoms with cognitive and functional performance is dependent on the degree of global impairment across the NA-MCI-AD continuum. The effect of depression on cognitive functions such as episodic memory, language, executive functions, and visuospatial abilities, was more intense in the NA group. Depressive symptoms in subjects with MCI or AD had no significant effect on cognitive performance, with very low effect sizes. We found an association between depression and functional measures only in the NA group, and this effect occurred in instrumental-domestic, instrumental-complex, and general-ADL. In this sense, our results suggest that depression not be strongly associated with a worse cognitive and functional phenotype in patients with MCI or AD.
The effect of depressive symptoms was more pronounced in executive function in comparison to the other cognitive domains. Executive dysfunction impairment is an important feature of late-life depression and is associated with negative outcomes such as suicide behavior, development of neuropsychiatric symptoms, and higher risk of dementia (Moreira et al., 2012; Richard-Devantoy et al., 2012; Diniz et al., 2013). As the integrity of the fronto-striatal circuitry and dopaminergic neurotransmission are main correlates of executive functions, we can hypothesize that these neurobiological correlates are particularly vulnerable to the deleterious effects of depression (Fitzgerald et al., 2008; Malloy-Diniz et al., 2013). In this sense, cognitive interventions, neuromodulation, psychotherapy, or pharmacological treatment may restore or reduce the intensity of both cognitive deficits and psychiatric symptoms (Lenze et al., 2014; Mackin et al., 2014; Diamond et al., 2015). However, this is a complex relationship, since improvement of depressive symptoms may not necessarily lead to remission in cognitive deficits (Nebes et al., 2003; Bhalla et al., 2006) or improvement in cognitive functioning may not reduce symptoms of depression (McDermott and Gray, 2012).
Cognitive impairment in depression has been associated to distinct neurobiological changes. Depression is associated with the hypothalamic-pituitary-adrenal axis dysfunction, a factor related to higher secretion of glucocorticoids (Butters et al., 2008). This mechanism relates to hippocampal atrophy and may be a neurobiological causal factor to the episodic memory impairment in depressed subjects (Panza et al., 2010; Naismith et al., 2012). Another important mechanism with may explain the current findings is the increase of vascular burden, especially white matter lesions, found in depressed subjects (Tham et al., 2011). These lesions may reflect on the overall brain functioning by ischemia or the disruption of frontostriatal connections, aspects closely related to the executive functions and processing speed (Royall et al., 2002). A third pathway relates to amyloid burden: late-life depression is associated to an increase of β-amyloid, a factor associated with the severity of cognitive impairment and overall severity of depression (Piccinni et al., 2013).
However, similar changes were reported in MCI subjects and patients with AD (Forlenza et al., 2010; Panza et al., 2010). Therefore, the presence of these neurobiological changes in subjects with depressive symptoms and MCI/AD seems not to confer a synergic or an additive effect on cognitive performance in older adults. On the other hand, the emergence of neurodegenerative changes in the MCI/AD continuum may reduce the impact of depression-related neurobiological changes on cognitive performance. Additional studies, including neuroimaging and biological markers, are necessary to disentangle the mechanisms by which depressive symptoms moderate cognitive performance in these subjects.
We evaluated the impact of depressive symptoms over a broad range of ADLs. Depressive symptoms were associated with worse performance only on instrumental-domestic or instrumental-complex ADL. This pattern of association might be explained by the complex nature of the tasks by itself, which my demand more pronounced involvement motivation, emotional regulation, and cognitive control. In addition, the effects of depression in ADL seems weaker than its impact in cognitive functioning. Our results are in line with recent reports of the literature (Reppermund et al., 2011; Park et al., 2013; de Paula et al., 2015a). Previous studies also showed no significant impact of depression in ADLs. Methodological differences between studies may help to explain the effects results, in particular sample setting (population-based, memory clinic and nursing homes) and different strategies and scales to assess ADLs (objective assessment, informant-based assessment; Reppermund et al., 2011). Given the importance of this topic, additional studies are necessary to address the impact of late-life depression in the performance on ADLs.
The present study should be viewed in light of some limitations, which hinders its generalization to other populations. First, we used the GDS-15 to evaluate depressive symptoms and we did not carry out a structured psychiatric interview to confirm the presence of a depressive episode. Despite the fact that GDS-15 is widely used in clinical and research settings, there is criticism about the use of the GDS-15 on the assessment of depressive symptoms in AD and other dementias. Therefore, we might have misidentified cases of depression in AD group, what may have influenced the present results. The cross-sectional design and the recruitment of participants among individuals referred to a cognitive evaluation due to memory complaints also limit the generalization of the present results. On the other hand, cognitive performance was evaluated by a comprehensive neuropsychological protocol, which was not used to define each subject diagnosis. This is a major strength of our study and reduces the risk of circularity and bias in the present analyses.
In conclusion, the present study reanalyzed a previously published dataset and showed a significant association of depressive symptoms on multiples domains of cognition only in older subjects with no evidence of global cognitive impairment. In addition, the effect of depressive symptoms on functional performance was restricted to domestic and complex ADLs. Additional studies, with a prospective design and with population-based samples are necessary to replicate the present findings.
Funding
This work was supported by the following grants: APQ-01972/12-10, APQ-02755-10, APQ-04706-10, CBB-APQ-00075-09 from FAPEMIG, and 573646/2008-2 from CNPq. The funders had no role in study design, data collection, analysis, decision to publish, or preparation of the manuscript.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer, Maria Semkovska, and the handling Editor declared their shared affiliation, and the handling Editor states that the process nevertheless met the standards of a fair and objective review.
Supplementary Material
The Supplementary Material for this article can be found online at: http://journal.frontiersin.org/article/10.3389/fpsyg.2015.02061
References
Almeida, O. P., and Almeida, S. A. (1999). Short versions of the geriatric depression scale: a study of their validity for the diagnosis of a major depressive episode according to ICD-10 and DSM-IV. Int. J. Geriatr. Psychiatry 14, 858–865.
Aprahamian, I., Martinelli, J. E., Neri, A. L., and Yassuda, M. S. (2009). The clock drawing test: a review of its accuracy in screening for dementia. Dement. Neuropsychol. 3, 74–80.
Baiyewu, O., Unverzagt, F. W., Lane, K. A., Gureje, O., Ogunniyi, A., Musick, B., et al. (2004). The stick design test: a new measure of visuoconstructional ability. J. Int. Neuropsychol. Soc. 11, 598–605. doi: 10.1017/S135561770505071X
Bangen, K. J., Delano-Wood, L., Wierenga, C. E., McCauley, A., Jeste, D. V., Salmon, D. P., et al. (2010). Associations between stroke risk and cognition in normal aging and Alzheimer's disease with and without depression. Int. J. Geriatr. Psychiatry 25, 175–182. doi: 10.1002/gps.2317
Banhato, E. F. C., and Nascimento, E. (2007). Executive functions in elderly: a study using WAIS-III subtests scale. Psico-USF 12, 65–73.
Bhalla, R. K., Butters, M. A., Mulsant, B. H., Begley, A. E., Zmuda, M. D., Schoderbek, B., et al. (2006). Persistence of neuropsychologic deficits in the remitted state of late-life depression. Am. J. Geriatr. Psychiatry 14, 419–427. doi: 10.1097/01.jgp.0000203130.45421.69
Bombin, I., Santiago-Ramajo, S., Garolera, M., Vega-González, E. M., Cerulla, N., Caracuel, A., et al. (2012). Functional impairment as a defining feature of: amnestic MCI cognitive, emotional, and demographic correlates. Int. Psychogeriatr. 24, 1494–1504. doi: 10.1017/S1041610212000622
Brown, P. J., Woods, C. M., and Storandt, M. (2007). Model stability of the 15-item geriatric depression scale across cognitive impairment and severe depression. Psychol. Aging 22, 372–379. doi: 10.1037/0882-7974.22.2.372
Brucki, S. M. D., and Rocha, M. S. G. (2004). Category fluency test: effects of age, gender and education on total scores, clustering and switching in Brazilian Portuguese-speaking subjects. Braz. J. Med. Biol. Res. 37, 1771–1777. doi: 10.1590/S0100-879X2004001200002
Brucki, S. M., Nitrini, R., Caramelli, P., Bertolucci, P. H. F., and Okamoto, I. H. (2003). Sugestões para o uso do mini-exame do estado mental no Brasil. Arq. Neuropsiquiatr. 61, 777–781. doi: 10.1590/S0004-282X2003000500014
Butters, M. A., Whyte, E. M., Nebes, R. D., Begley, A. E., Dew, M. A., Mulsant, B. H., et al. (2004). The nature and determinants of neuropsychological functioning in late-life depression. Arch. Gen. Psychiatry 61, 587–595. doi: 10.1001/archpsyc.61.6.587
Butters, M. A., Young, J. B., Lopez, O., Aizenstein, H. J., Mulsant, B. H., Reynolds, C. F. III, et al. (2008). Pathways linking late-life depression to persistent cognitive impairment and dementia. Dialogues Clin. Neurosci. 10, 345–357.
Chen, H., Cohen, P., and Chen, S. (2010). How big is a big odds ratio? Interpreting the magnitudes of odds ratios in epidemiological studies. Commun. Stat. Simul. Comput. 39, 860–864. doi: 10.1080/03610911003650383
de Paula, J. J., Bertola, L., Ávila, R. T., Assis, L. O., Albuquerque, M., Bicalho, M.A., et al. (2014). Development, validity, and reliability of the general activities of daily living scale: a multidimensional measure of activities of daily living for older people. Rev. Bras. Psiquiatr. 36, 143–152. doi: 10.1590/1516-4446-2012-1003
de Paula, J. J., Bertola, L., Ávila, R. T., Moreira, L., Coutinho, G., Moraes, E. N., et al. (2013b). Clinical applicability and cutoff values for an unstructured neuropsychological assessment protocol for older adults with low formal education. PLoS ONE 8:e73167. doi: 10.1371/journal.pone.0073167
de Paula, J. J., Diniz, B. S., Bicalho, M. A., Albuquerque, M. R., Nicolato, R., Moraes, E. N., et al. (2015a). Specific cognitive functions and depressive symptoms as predictors of activities of daily living in older adults with heterogeneous cognitive backgrounds. Front. Aging Neurosci. 7:139. doi: 10.3389/fnagi.2015.00139
de Paula, J. J., Miranda, D. M., Nicolato, R., Moraes, E. N., Bicalho, M. A., and Malloy-Diniz, L. F. (2013a). Verbal learning on depressive pseudodementia: accentuate impairment of free recall, moderate on learning processes, and spared short-term and recognition memory. Arq. Neuropsiquiatr. 71, 596–599. doi: 10.1590/0004-282X20130102
de Paula, J. J., Paiva, G. C. C., and Costa, D. S. (2015b). Use of a modified version of the switching verbal fluency test for the assessment of cognitive flexibility. Dement. Neuropsychol. 9, 258–264. doi: 10.1590/1980-57642015DN93000008
De Renzi, E., and Faglioni, P. (1978). Normative data and screening power of a shortened version of the token test. Cortex 14, 41–49. doi: 10.1016/S0010-9452(78)80006-9
Diamond, K., Mowszowski, L., Cockayne, N., Norrie, L., Paradise, M., Hermens, D. F., et al. (2015). Randomized controlled trial of a healthy brain ageing cognitive training program: effects on memory, mood, and sleep. J. Alzheimers Dis. 44, 1181–1191. doi: 10.3233/JAD-142061
Diniz, B. S., Butters, M. A., Albert, S. M., Dew, M. A., and Reynolds, C. F. III. (2013). Late-life depression and risk of vascular dementia and Alzheimer's disease: systematic review and meta-analysis of community-based cohort studies. Br. J. Psychiatry 202, 329–335. doi: 10.1192/bjp.bp.112.118307
Dubois, B., Slachevsky, A., Litvan, I., and Pilon, B. (2000). The FAB: a frontal assessment battery at bedside. Neurology 55, 1621–1626. doi: 10.1212/WNL.55.11.1621
Faul, F., Erdfelder, E., Lang, A.-G., and Buchner, A. (2007). G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 39, 175–191. doi: 10.3758/BF03193146
Feher, E. P., Larrabee, G. J., and Crok, T. H. III. (1992). Factors attenuating the validity of the geriatric depression scale in a dementia population. J. Am. Geriatr. Soc. 40, 906–909. doi: 10.1111/j.1532-5415.1992.tb01988.x
Fitzgerald, P. B., Laird, A. R., Maller, J., and Daskalakis, Z. J. (2008). A meta-analytic study of changes in brain activation in depression. Hum. Brain Mapp. 29, 683–695. doi: 10.1002/hbm.20426
Folstein, M. F., Folstein, S. E., McHugh, P. R., and Fanjiang, G. (2001). Mini-Mental State Examination User's Guide. Odessa, FL: Psychological Assessment Resources.
Forlenza, O. V., Diniz, B. S., Teixeira, A. L., Ojopi, E. B., Talib, L. L., Mendonça, V. A., et al. (2010). Effect of brain-derived neurotrophic factor Val66Met polymorphism and serum levels on the progression of mild cognitive impairment. World J. Biol. Psychiatry 11, 774–780. doi: 10.3109/15622971003797241
Foss, M. P., Carvalho, V. A., Machado, T. H., Reis, G. C., Tumas, V., Caramelli, P., et al. (2013). Mattis dementia rating scale: normative data for the Brazilian middle-age and elderly populations. Dement. Neuropsychol. 7, 374–379.
Katz, S., Downs, T. D., Cash, H. R., and Grotz, R. C. (1970). Progress in the development of the index of ADL. Gerontologist 10, 20–30. doi: 10.1093/geront/10.1_Part_1.20
Kessels, R. P., van den Berg, E., Ruis, C., and Brands, A. (2008). The backward span of the corsi block-tapping task and its association with the WAIS-III digit span. Assessment 15, 426–434. doi: 10.1177/1073191108315611
Lawton, M. P., and Brody, E. M. (1969). Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist 9, 179–186. doi: 10.1093/geront/9.3_Part_1.179
Lenze, E. J., Hickman, S., Hershey, T., Wendleton, L., Ly, K., Dixon, D., et al. (2014). Mindfulness-based stress reduction for older adults with worry symptoms and co-occurring cognitive dysfunction. Int. J. Geriatr. Psychiatry 29, 991–1000. doi: 10.1002/gps.4086
Mackin, R. S., Nelson, J. C., Delucchi, K., Raue, P., Byers, A., Barnes, D., et al. (2014). Cognitive outcomes after psychotherapeutic interventions for major depression in older adults with executive dysfunction. Am. J. Geriatr. Psychiatry 22, 1496–1503. doi: 10.1016/j.jagp.2013.11.002
Malloy-Diniz, L. F., Bentes, R. C., Figueiredo, P. M., Brandão-Bretas, D., Costa-Abrantes, S., Parizzi, A. M., et al. (2007a). Normalización de una batería de tests para evaluar las habilidades de comprensión del lenguaje, fluidez verbal y denominación en niños brasileños de 7 a 10 años: resultados preliminares. Rev. Neurol. 44, 275–280.
Malloy-Diniz, L. F., Lage, G. M., Campos, S. B., de Paula, J. J., Costa, D. S., Romano-Silva, M. A., et al. (2013). Association between the Catechol O-Methyltransferase (COMT) Val158met polymorphism and different dimensions of impulsivity. PLoS ONE 8:e73509. doi: 10.1371/journal.pone.0073509
Malloy-Diniz, L. F., Lasmar, V. A. P., Gazinelli, L. S. R., Fuentes, D., and Salgado, J. V. (2007b). The rey auditory-verbal learning test: applicability for the Brazilian elderly population. Rev. Bras. Psiquiatr. 29, 324–329. doi: 10.1590/S1516-44462006005000053
McDermott, C. L., and Gray, S. L. (2012). Cholinesterase inhibitor adjunctive therapy for cognitive impairment and depressive symptoms in older adults with depression. Ann. Pharmacother. 46, 599–605. doi: 10.1345/aph.1Q445
McKhann, G., Drachman, D., Folstein, M., Katzman, R., Price, D., and Stadlan, E. M. (1984). Clinical diagnosis of Alzheimer's disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer's disease. Neurology. 34, 939–944. doi: 10.1212/WNL.34.7.939
Moreira, L., Lage, G. M., Coutinho, G., Couto, T., Bicalho, M. A. C., Correa, H., et al. (2012). What role do executive functions play in the etiology of behavioral and psychological symptoms of dementia? An integrative review. Acta. Neuropsychol. 10, 519–535.
Moreira, L., Schlottfeldt, C. G., de Paula, J. J., Daniel, M. T., Paiva, A., Cazita, V., et al. (2011). Normative study of the Token Test (short version): preliminary data for a sample of Brazilian seniors. Rev. Psiq. Clín. 38, 97–101. doi: 10.1590/S0101-60832011000300003
Morris, J. C. (1993). The Clinical Dementia Rating (CDR): current version and scoring rules. Neurology 43, 2412–2414. doi: 10.1212/WNL.43.11.2412-a
Morris, J. C., Heyman, A., Mohs, R. C., Hughes, J. P., van Belle, G., Fillenbaum, G., et al. (1989). The Consortium to Establish a Registry for Alzheimer's disease (CERAD). Part I. Clinical and neuropsychological assessment of Alzheimer's disease. Neurology 39, 1159–1165. doi: 10.1212/WNL.39.9.1159
Naismith, S. L., Hickie, I. B., Turner, K., Little, C. L., Winter, V., Ward, P. B., et al. (2003). Neuropsychological performance in patients with depression is associated with clinical, etiological and genetic risk factors. J. Clin. Exp. Neuropsychol. 25, 866–877. doi: 10.1076/jcen.25.6.866.16472
Naismith, S. L., Norrie, L. M., Mowszowski, L., and Hickie, I. B. (2012). The neurobiology of depression in later-life: clinical, neuropsychological, neuroimaging and pathophysiological features. Prog. Neurobiol. 98, 99–143. doi: 10.1016/j.pneurobio.2012.05.009
Nakaaki, S., Murata, Y., Sato, J., Shinagawa, Y., Tatsumi, H., Hirono, N., et al. (2007). Greater impairment of ability in the divided attention task is seen in Alzheimer's disease patients with depression than in those without depression. Dement. Geriatr. Cogn. Disord. 23, 231–240. doi: 10.1159/000099633
Nebes, R. D., Pollock, B. G., Houck, P. R., Butters, M. A., Mulsant, B. H., Zmuda, M. D., et al. (2003). Persistence of cognitive impairment in geriatric patients following antidepressant treatment: a randomized, double-blind clinical trial with nortriptyline and paroxetine. J. Psychiatr. Res. 37, 99–108. doi: 10.1016/S0022-3956(02)00085-7
Nitrini, R., Caramelli, P., Herrera Júnior, E., Porto, C. S., Charchat-Fichman, H., Carthery, M. T., et al. (2004). Performance of illiterate and literate nondemented elderly subjects in two tests of long term memory. J. Int. Neuropsychol. Soc. 10, 634–638. doi: 10.1017/S1355617704104062
Nyunt, M. S., Lim, M. L., Yap, K. B., and Ng, T. P. (2012). Changes in depressive symptoms and functional disability among community-dwelling depressive older adults. Int. Psychogeriatr. 24, 1633–1641. doi: 10.1017/S1041610212000890
Panza, F., Frisardi, V., Capurso, C., D'Introno, A., Colacicco, A. M., Imbimbo, B. P., et al. (2010). Late-Life depression, mild cognitive impairment, and dementia: Possible Continuum? Am. J. Geriatr. Psychiatry 18, 98–116. doi: 10.1097/JGP.0b013e3181b0fa13
Park, B., Jun, J. K., and Park, J. (2013). Cognitive impairment and depression in the early 60s: which is more problematic in terms of instrumental activities of daily living? Geriatr. Gerontol. Int. 14, 62–70. doi: 10.1111/ggi.12055
Petersen, R. C., Doody, R., Kurz, A., Mohs, R. C., Morris, J. C., Rabins, P. V., et al. (2001). Current concepts in mild cognitive impairment. Arch. Neurol. 58, 1985–1992. doi: 10.1001/archneur.58.12.1985
Piccinni, A., Origlia, N., Veltri, A., Vizzaccaro, C., Marazziti, D., Vanelli, F., et al. (2013). Neurodegeneration, β-amyloid and mood disorders: state of the art and future perspectives. Int. J. Geriatr. Psychiatry 28, 661–671. doi: 10.1002/gps.3879
Porto, C. S., Fichman, H. C., Caramelli, P., Bahia, V. S., and Nitrini, R. (2003). Brazilian version of the Mattis Dementia Rating Scale: diagnosis of mild dementia in Alzheimer's disease. Arq. Neuropsiquiatr. 61, 339–345. doi: 10.1590/S0004-282X2003000300004
Reppermund, S., Brodaty, H., Crawford, J. D., Kochan, N. A., Slavin, M. J., Trollor, J. N., et al. (2011). The relationship of current depressive symptoms and past depression with cognitive impairment and instrumental activities of daily living in an elderly population: the Sydney Memory and Ageing Study. J. Psychiatr. Res. 45, 1600–1607. doi: 10.1016/j.jpsychires.2011.08.001
Richard-Devantoy, S., Jollant, F., Kefi, Z., Turecki, G., Olié, J. P., and Annweiler, C. (2012). Deficit of cognitive inhibition in depressed elderly: a neurocognitive marker of suicidal risk. J. Affect. Disord. 140, 193–199. doi: 10.1016/j.jad.2012.03.006
Royall, D. R., Lauterbach, E. C., Cumming, J. L., Reeve, A., Rummans, T. A., Kaufer, D. I., et al. (2002). Executive control function: a review of its promise and challenges for clinical research. J. Neuropsychiatry. Clin. Neurosci. 14, 377–405. doi: 10.1176/jnp.14.4.377
Sexton, C. E., McDermott, L., Kalu, U. G., Herrmann, L. L., Bradley, K. M., Allan, C. L., et al. (2012). Exploring the pattern and neural correlates of neuropsychological impairment in late-life depression. Psychol. Med. 42, 1195–1202. doi: 10.1017/S0033291711002352
Sheikh, J. I., and Yeasavage, J. A. (1986). Geriatric Depression Scale (GDS): recent evidence and development of a shorter version. Clin. Gerontol. 5, 165–172. doi: 10.1300/J018v05n01_09
Shulman, K. (2000). Clock-drawing: is it the ideal cognitive screening test? Int. J. Geriatr. Psychiatry 15, 548–561. doi: 10.1002/1099-1166(200006)15:6<548::AID-GPS242>3.0.CO;2-U
Tham, M. W., Woon, P. S., Sum, M. Y., Lee, T. S., and Sim, K. (2011). White matter abnormalities in major depression: evidence from post-mortem, neuroimaging and genetic studies. J. Affect. Disord. 132, 26–36. doi: 10.1016/j.jad.2010.09.013
Tomita, A., and Burns, J. K. (2013). Depression, disability and functional status among community-dwelling older adults in South Africa: evidence from the first South African National Income Dynamics Study. Int. J. Geriatr. Psychiatry 28, 1270–1279. doi: 10.1002/gps.3954
Wadsworth, L. P., Lorius, N., Donovan, N. J., Locascio, J. J., Rentz, D. M., Johnson, K. A., et al. (2012). Neuropsychiatric symptoms and global functional impairment along the Alzheimer's continuum. Dement. Geriatr. Cogn. Disord. 34, 96–111. doi: 10.1159/000342119
Keywords: older adults, depression, cognitive assessment, activities of daily living, neuropsychological assessment, mild cognitive impairment, Alzheimer's disease
Citation: de Paula JJ, Bicalho MA, Ávila RT, Cintra MTG, Diniz BS, Romano-Silva MA and Malloy-Diniz LF (2016) A Reanalysis of Cognitive-Functional Performance in Older Adults: Investigating the Interaction Between Normal Aging, Mild Cognitive Impairment, Mild Alzheimer's Disease Dementia, and Depression. Front. Psychol. 6:2061. doi: 10.3389/fpsyg.2015.02061
Received: 12 August 2015; Accepted: 31 December 2015;
Published: 26 January 2016.
Edited by:
Rachel M. Msetfi, University of Limerick, IrelandReviewed by:
Diana Kornbrot, University of Hertfordshire, UKMaria Semkovska, University of Limerick, Ireland
Copyright © 2016 de Paula, Bicalho, Ávila, Cintra, Diniz, Romano-Silva and Malloy-Diniz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jonas J. de Paula, am9uYXNqYXJkaW1AZ21haWwuY29t