 Sungeun You
Sungeun You Moran Park
Moran Park- Department of Psychology, Chungbuk National University, Cheongju, South Korea
Suicide prevention efforts in reducing risk factors have been found to be more beneficial to older women than men, suggesting potential gender differences in effective prevention. The study aimed to examine gender difference in resilience for suicidal behavior in a community sample of older adults in Korea. A community-based survey was conducted to investigate resilience and risk factors of suicidal behavior using the Suicidal Behaviors Questionnaire-Revised, Connor-Davidson Resilience Scale, Center for Epidemiologic Studies Depression Scale (CES-D), as well as questions regarding physical illness and depression history. After accounting for well-known risk factors, resilience was inversely associated with suicidal behavior, but this protective role of resilience was applicable to men only. The findings of this study indicated gender difference in resilience against suicidal behavior in the elderly population. Gender-specific preventive intervention strategies need to be developed for community-based suicide prevention for older adults.
Introduction
Suicide rates in older adults have increased at a faster pace than any other age group over the past decades in Korea (World Health Organization [WHO], 2014). National suicide rates among Korean older adults aged 65 years and older were considerably high, with 95.2 in men and 32.1 in women (Statistics Korea, 2016). Considering that it is a rapidly growing population, not only in Korea but also the world (World Health Organization [WHO], 2012), it is critical to improve our understanding of suicide among the elderly. While incidence rates of suicidal ideation and attempt decreases with age, suicide rate increases as one get older (De Leo et al., 2001; Centers for Disease Control, and Prevention, 2015), suggesting higher likelihood of suicide death among older adults who have thought or attempted suicide compared to other age groups. This tendency seemed stronger for older men than older women (Rubenowitz et al., 2001; Paraschakis et al., 2012), although no consistent gender difference in prevalence of suicidal ideation was reported for older adults (Almeida et al., 2012; Park and Lee, 2015; Kim et al., 2016).
Despite this well-known gender difference in suicidal behavior in the elderly population, our knowledge regarding how older men and women differ in terms of risk and protective factors for suicidal behavior is limited. The most well-known risk factors for elderly suicide are depression and social isolation (Conwell et al., 2002, 2011), and preexisting elderly suicide prevention programs mostly rely on reducing these risk factors (Oyama et al., 2005; Unützer et al., 2006; Alexopoulos et al., 2009). Using randomized controlled trials, both IMPACT (Improving Mood-Promoting Access to Collaborative Treatment, Unützer et al., 2006) and PROSPECT (Prevention of Suicide in Primary Care Elderly: Collaborative Trial, Alexopoulos et al., 2009) programs resulted in a significant reduction in depressive symptoms and suicide risk for depressed older patients. Community-based intervention programs (Oyama et al., 2005, 2008), including depression screening, health education, and group activities were effective in reducing suicide risk for older adults. Interestingly, these empirically supported suicide prevention programs were more beneficial to older women than older men (Oyama et al., 2005, 2008; Drapeau et al., 2009). Moreover, older men and women differed in participation rates and preferences for intervention programs (Drapeau et al., 2009). In fact, older women were more likely to participate in intervention programs utilizing social groups, counseling, and other mental health services while older men were more inclined to engage in action-oriented or problem-solving oriented intervention programs (Oyama et al., 2008; Drapeau et al., 2009; Lapierre et al., 2011).
Gender differences in the effects or participation rates of suicide prevention programs among older adults suggest the need for developing differential strategies to suicide prevention for each gender. More understanding of gender-specific risk and protective factors would enable us to develop gender-specific intervention programs. As evidenced by psychological autopsy studies, depression is one of the strongest risk factors for elderly suicide (Beautrais, 2002; Conwell et al., 2002, 2011) while associations of other psychiatric disorders with suicide in older adults varied across samples and cultural backgrounds (Conwell et al., 2011). In addition, physical illnesses in old ages increased the risk for suicide (Juurlink et al., 2004; Conwell et al., 2010; Erlangsen et al., 2015). However, considering that late-life depression and physical illnesses are common risk factors for morbidity and mortality in this population (Schulz et al., 2002).
Current literature has rarely examined the role of protective factors for elderly suicide. Moreover, gender differences in such protective factors are largely unknown. A few studies examined the association between low resilience and suicidal behavior, although findings have been rather mixed. In a 3-year longitudinal study, resilience had a protective effect for suicidal ideation among veterans even after controlling for baseline suicidal ideation (Youssef et al., 2013). Similarly, low resilience was linked to suicide attempt in substance-dependent outpatients or prisoners (Roy et al., 2007, 2011). On the contrary, Liu et al. (2014, 2016) reported no relationship between resilience and suicidal ideation when several psychological covariates were controlled.
Resilience is a broad term denoting one’s ability to cope with life stress or adversity (Connor and Davidson, 2003; Windle et al., 2011). Based on several personality theories (Kobasa, 1979; Rutter, 1985; Lyons, 1991), Connor and Davidson (2003) developed a measure to quantify one’s resilience, which they called the Connor-Davidson Resilience Scale (CD-RISC). Connor and Davidson (2003) viewed resilience as a modifiable psychological construct that could be enhanced by clinical intervention. Indeed, a number of studies have supported successful modifications of resilience following various forms of intervention (Davidson et al., 2005; Steinhardt and Dolbier, 2008; Loprinzi et al., 2011; Stephens, 2013).
The study aimed to examine gender difference in the protective role of resilience against suicidal behavior among the elderly, especially after controlling for common risk factors associated with elderly suicide, such as sociodemographic risk factors, depression, and physical illness. In this study, risk factors are considered conditions or variables associated with higher likelihood of suicide or suicidal behavior based on preexisting evidence, and protective factors are those with adverse effect. Informed by previous intervention studies indicating gender differences in potentially effective programs to reduce suicide risk among the elderly, it was hypothesized that the protective role of resilience against suicidal behavior would be stronger for older men as compared to older women.
Materials and Methods
Participants and Procedure
Participants were recruited from Chuncheon, an urban-rural mixed community in Korea. The target number of sample was approximately 2000 older adults in the community, and the sample size was predetermined using a stratified cluster sampling procedure with a proportionate quota sampling strategy. Population sizes by gender and five age groups (65–69, 70–74, 75–79, 80–84, and ≥85 years old) were obtained from 25 administrative districts in Chuncheon. The sample sizes for higher and lower level administrative districts were determined based on the population size of gender by age groups. Eligible participants were 65 years and older, and could speak and understand Korean. Older adults residing in institutions such as nursing homes or hospitals were excluded from the study. A total of 4864 older adults were approached in the community, and 2034 among them agreed to participate in and completed the study. Response rate was 41.8%. The final sample included 833 men (41.0%) and 1201 women (59.0%).
A community-based survey was conducted via home visit by trained interviewers. All interviewers had at least 3 years of community survey experience and more than high school diploma. The mean survey experience of these interviewers was 5.04 years with the range of 3–19. All research personnel were trained by a doctoral level clinical psychologist regarding research ethics, interview procedure, and how to conduct suicide-risk assessment using the SBQ-R (see Materials for more information about the measure). Older adults who scored more than 7 on the SBQ-R were referred to community mental health centers upon agreement. Explanations about the aim of the study and contents of informed consent were presented verbally. All people could freely choose not to participate in the study without any disadvantages. For those who agreed to participate, all questions were read by research assistants. All participants provided written informed consent and received a small gift (less than $5 value) for the study participation. The study protocol was approved by Hallym University Institutional Review Board (IRB).
Materials
The Suicidal Behaviors Questionnaire-Revised (SBQ-R; Osman et al., 2001) was developed to be used as a measure of suicidal behavior in clinical and non-clinical populations. The SBQ-R consisted of four items: (1) lifetime experience of suicidal thoughts and attempts (1 = never to 4 = I have attempted to kill myself, and really hoped to die); (2) frequency of suicidal ideation during the past 12 months (1 = never to 5 = very often, 5 or more times); (3) threat of suicide attempt (1 = no/never to 3 = yes/more than once, and really wanted to do it); and (4) self-reported likelihood of making suicidal behavior in the future (0 = never to 6 = very likely). The SBQ-R was translated into Korean and cross-checked by two doctoral-level psychologists and then confirmed by a bilingual person who is not in the field of psychology or psychiatry. The total scores of the SBQ-R range from 3 to 18, with the higher scores indicating a greater suicide risk. The cut-off score of 7 was suggested in classifying a high-risk group among non-clinical samples (Osman et al., 2001). The internal consistency coefficients of the SBQ-R were 0.76–0.88 in the Osman et al. (2001) study and 0.81 in this study.
The CD-RISC (Connor and Davidson, 2003) is a 25-item self-report measure that assesses one’s ability to cope with stressful life events in multiple domains of life. The CD-RISC measures a variety of characteristics of one’s resilience, such as the ability to control, goal-oriented active coping, adaptability to change, ability to tolerate negative affect, self-efficacy, personal competence, relationship security, and spirituality. The total scores of the CD-RISC range from 0 to 100 with the higher scores representing greater resilience. The participants rated each item on a five point Likert scale from 0 (not true at all) to 4 (true nearly all of the time). In this study, the Korean version of the CD-RISC (K-CD-RISC, Baek et al., 2010) was used. The internal consistency of the K-CD-RISC was 0.93 in Baek et al. (2010)’s study, and 0.95 in this study.
The Center for Epidemiologic Studies Depression Scale (CES-D; Radloff, 1977), a 20-item self-report questionnaire, measures depressive symptom severity in the last week, with a 4-point Likert scale (0 = rarely or none of the time, less than 1 day; 3 = most or all of the time, 5–7 days). In this study, a 10-item brief version of the CES-D (Kohout et al., 1993), translated into Korean by Shin (2011) was used. The brief version of the CES-D had good reliability among the elderly (Andresen et al., 1994; O’Halloran et al., 2014). The total scores of the brief CES-D range from 0 to 30, with the higher scores indicating greater depressive symptoms. The internal consistency of the 10-item brief version of the CES-D was 0.79 in Shin (2011)’s study and 0.87 in this study.
History of physical illnesses was assessed using the question of “Have you ever been diagnosed with any of the following illnesses by medical doctors?” Participants were responded to the question for 16 major physical illnesses such as hypertension, heart disease, stroke, cancer, or diabetes. The same question was used to assess history of depression. Also, sociodemographic information of age, gender, years of education, family income, and living status (living alone versus living together with family or others) was collected.
Statistical Analysis
Descriptive statistics and gender comparisons for all variables were examined using t or χ2 tests. Correlation coefficients of the SBQ-R and all variables were examined, and Fisher’s r to z-transformation was used to examine gender differences. The Holm–Bonferroni method was used to adjust p-values for multiple comparisons. Next, hierarchical multiple regression was conducted to examine gender difference in the protective role of resilience for suicidal behavior. After controlling for sociodemographic covariates, physical illness, depressive symptoms, and depression history in the first step, the main effects of resilience and gender were examined in the second step, and then the interaction of gender by resilience were inserted in the third step. Finally, post hoc tests were conducted to depict the interaction effect found in the hierarchical multiple regression analyses (Aiken and West, 1991; Holmbeck, 2002).
Results
Preliminary Analysis
The mean age of the respondents was 74.50 (SD = 6.36) years old with a range of 65–98, and the average years of education was 6.12 (SD = 4.82). Of the sample, 53.8% were married or living with a partner, 41.9% were widowed, 2.6% were divorced, 1.4% were separated, and 0.2% were never married. The majority reported living with family (n = 1414, 69.5%) and 30.5% (n = 620) reported living alone.
As seen in Table 1, women were older, t = -5.66, p < 0.001, and less educated, t = 21.39, p < 0.001, compared to men. Also, women reported significantly higher scores on the CES-D (M = 4.90, SD = 4.67) than men (M = 3.90, SD = 4.62), t = -4.78, p < 0.001, indicating that women were more depressed than men. A significant gender difference was found in living status, in which a greater percentage of women reported living alone (42.1%) compared to men (13.7%), χ2 (1) = 187.82, p < 0.001. No significant gender difference was found in the SBQ-R, t = 1.16, p = 0.248.
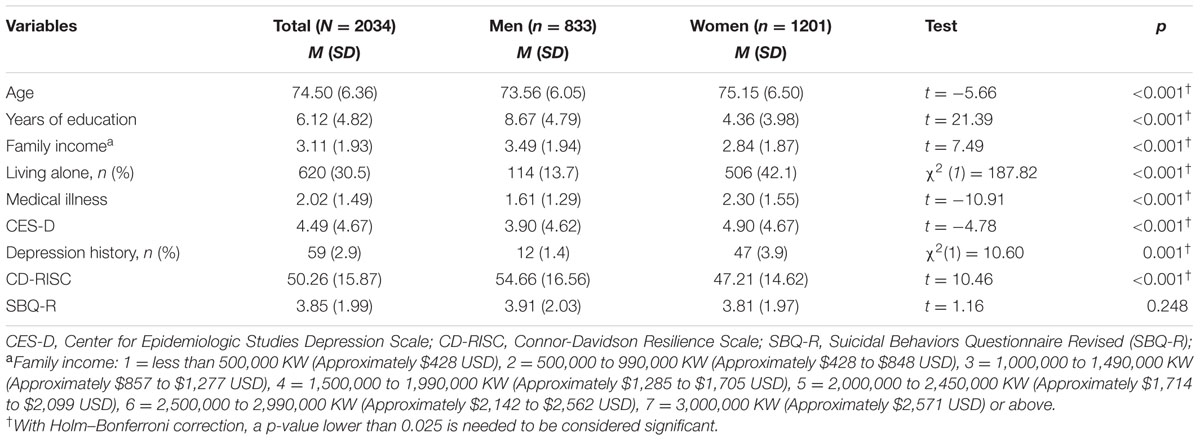
TABLE 1. Preliminary analysis: A gender comparison of variables.
The possible score range of the CD-RISC is 0 to 100. In the current sample, the mean score of the CD-RISC was 50.26 (SD = 15.87) and the score distribution was close to normal distribution (skewness index = -0.08, SEskewness = 0.05; kurtosis index = 0.12, SEkurtosis = 0.11). There was a significant gender difference in scores of the CD-RISC, in which men (M = 54.66, SD = 16.56) reported higher scores than women (M = 47.21, SD = 14.62), t = 10.46, p < 0.001.
Correlation coefficients of the SBQ-R and all variables were produced by gender, and Fisher’s r to z-transformation was used to examine whether these correlations differ by gender (see Table 2). With Holm–Bonferroni correction, the correlation coefficients between the SBQ-R and all variables were significant for both genders except age and years of education. A significant gender difference was found for the strength of correlations between the SBQ-R and the CD-RISC, z = -2.88, p = 0.004, in which the correlation between the SBQ-R and CD-RISC was stronger for older men, r = -0.32, p < 0.001, than women, r = -0.20, p < 0.001. On the contrary, a significant gender difference was found for the correlation between the SBQ-R and depression history, z = -3.55, p < 0.001. The correlation between the SBQ-R and depression history was stronger for older women, r = 0.33, p < 0.001, than men, r = 0.18, p < 0.001.
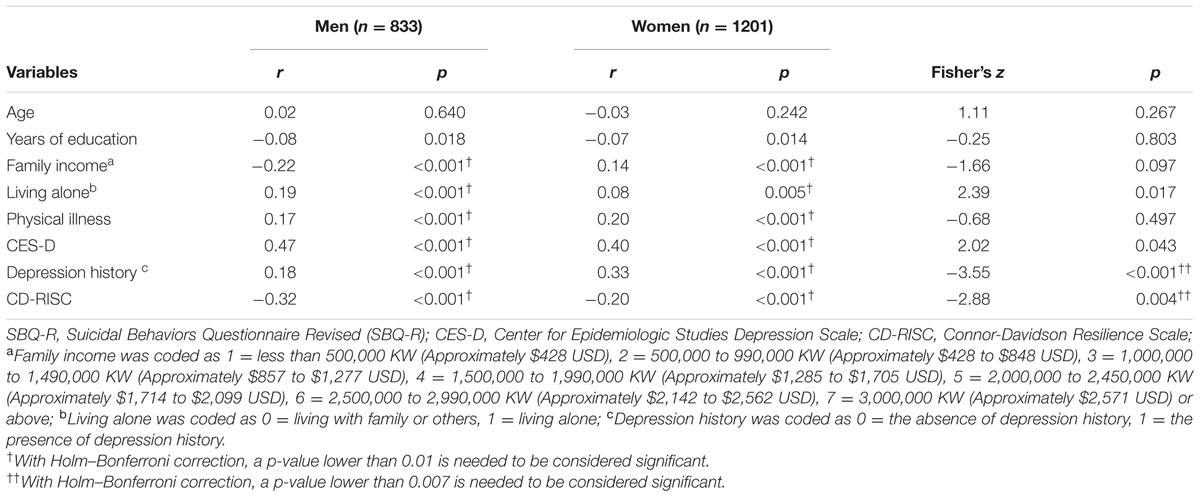
TABLE 2. Gender differences in correlation coefficients of the SBQ-R and variables.
Gender Difference in the Protective Role of Resilience against Suicidal Behavior
Hierarchical multiple regression was conducted to examine the gender difference in the protective role of resilience against suicidal behavior among older adults. As seen in Table 3, after controlling for age, years of education, family income, living alone, physical illness, the CES-D, and depression history, the main effects of the CD-RISC, β = -0.01, t = -3.15, p = 0.002, and gender on the SBQ-R, β = -0.42, t = -4.44, p < 0.001 were significant. Specifically, lower resilience and being men increased scores of the SBQ-R. In an examination of the interaction effect of gender and the CD-RISC in the third step, the interaction was statistically significant, β = 0.01, t = 2.28, p = 0.023, indicating a gender difference. Post hoc tests indicated that the inverse relationship between the CD-RISC and the SBQ-R was significant only for men, β = -0.12, t = -2.98, p < 0.01, whereas the association was not statistically significant for women, β = -0.03, t = -1.04, p = 0.297 (see Figure 1).
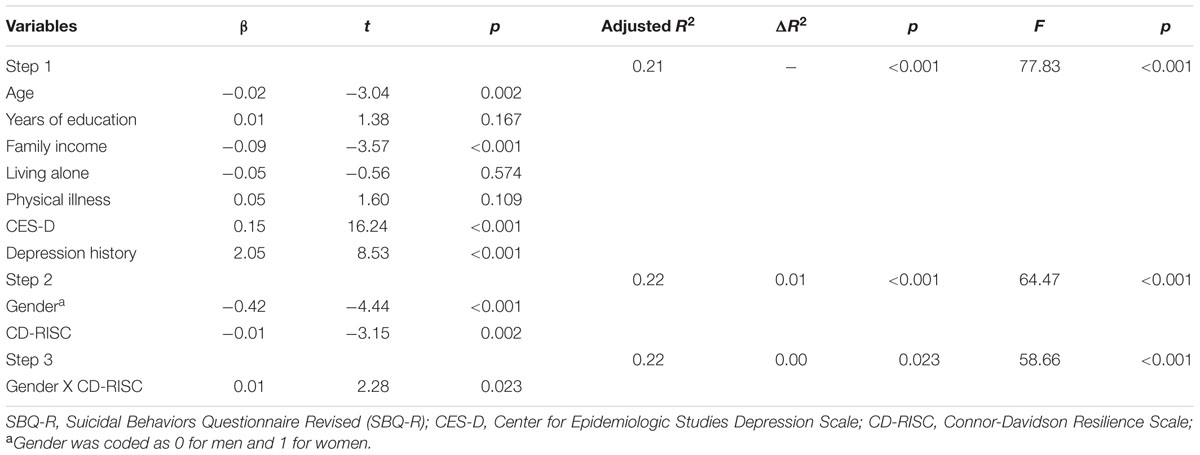
TABLE 3. Hierarchical multiple regression: Gender difference of resilience on the SBQ-R.
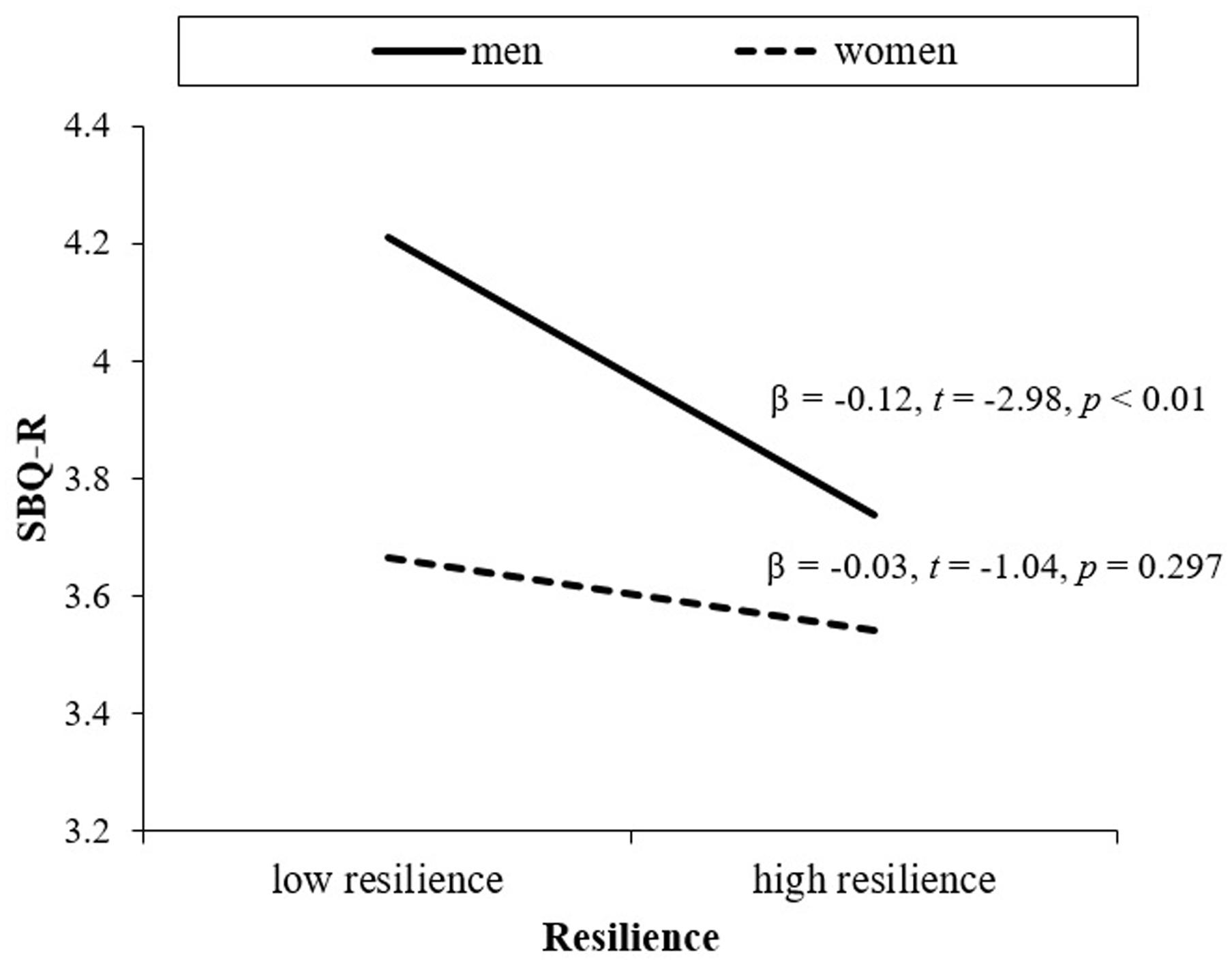
FIGURE 1. Resilience and suicidal behavior in older men and women.
Discussion
The present study examined gender difference in the protective role of resilience against suicidal behavior in a community sample of older adults in Korea. Particularly, this study examined whether resilience would protect against suicidal behavior above and beyond well-known risk factors in older adults, and further such protective function of resilience would differ by gender. The results of the study indicated that gender moderated the relationship between resilience and suicidal behavior, in which the relationship between low resilience and suicidal behavior was found only for older men, but not for older women, after controlling for common risk factors including depression, physical illness, and sociodemographic variables.
This gender difference may be because the CD-RISC (Connor and Davidson, 2003) mostly measures individual, personal strengths and resources, which could be more applicable to men than women. For older women, it is possible that relational resources are more related to their resilience against suicidal behavior. Considering previous research indicating unsuccessful effects of intervention on risk factors among older men (Lapierre et al., 2011), intervention promoting resilience may be an alternative option in reducing suicidal behavior for older men.
The findings of this study indicate the need for developing gender-specific preventive intervention strategies. Depression screening and follow-up care seem to be useful for suicide prevention, but as indicated in Lapierre et al.’s (2011) review, older men were less inclined to use mental health services and preferred action or problem-solving oriented programs. Hinton et al. (2006) reported that older men were rather reluctant to participate in mental health care due to traditional masculine value or stigma of mental illness. Our results indicate that strength-focused, competence-based preventive intervention to promote resilience or personal strengths could be a promising option for older men.
One important matter, then, is what to modify to improve resilience in older adults. To answer this question, we need to improve our understanding regarding the construct of resilience and what correlates with resilience in older adults. A few studies reported that resilience in older adults was associated with optimism, successful aging, depression, physical functioning, daily functioning, living with others, and days spent with family and friends per week (Hardy et al., 2004; Lamond et al., 2008; Jeste et al., 2013). Although further studies are needed, these variables are all potential ingredients in psychosocial intervention to improve resilience in older adults.
Limitations of the study should be noted. First, the older adults who participated in the study mostly lived in urban–rural mixed areas in South Korea and those living in nursing homes and hospitals were excluded for the study. Thus, further studies are needed for other samples, such as urban-residing or clinical samples. Second, we used a resilience measure covering a broad, heterogeneous concept of resilience. It is possible that older men and women have different domains of resilience associated with suicidal behavior, which we were unable to examine. Additionally, it was possible that men tended to exaggerate their resilience than women due to their masculine value. Third, most of the scales used for this study were self-report questionnaires that were not developed for oral administration. We did so because older adults vary in terms of reading capability due to various reasons such as vision or educational level. Further research to develop measures specific to older adults is needed. Finally, a single question was used to assess medical history about 16 major physical illnesses and depression. It should be considered that there was a possibility of underreporting.
Strengths of the study included a relatively large community sample of older adults, and the use of the multistage cluster sampling strategies to obtain a representative sample in consideration of regional differences in age and gender distribution. Considering the lack of studies examining gender differences in suicidal behavior in the elderly population, this study provides preliminary data indicating gender difference in factors related to suicidal behavior.
Conclusion
This study highlights gender differences in resilience against suicidal behavior above and beyond the effects of common risk factors in the elderly. Particularly, the results of the study indicate the protective role of resilience for older men. Considering that suicide rate of older men is very high and their participation rates in prevention programs focusing on mental health or social activities are low, alternative prevention efforts are needed for this population. The present study indicates that community-based, universal approach focusing on enhancement of resilience could be an alternative approach for older men. Differential intervention strategies for men and women need to be developed to implement effective suicide prevention programs. For older men, intervention programs focusing on personal strengths or assets, coping skills, or resilience would help reduce suicide risk.
Author Contributions
Both authors have made substantial contributions to the conception and design of the study, data analysis and interpretation of the data. SY drafted the manuscript. Both authors contributed to critical revisions, and approved the final version to be published.
Funding
This work was supported by the National Research Foundation of Korea Grant funded by the Korean Government (NRF-2012S1A6A3A01033504).
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Aiken, L. S., and West, S. G. (1991). Multiple Regression: Testing and Interpreting Interactions. Newbury Park, CA: Sage Publications.
Alexopoulos, G. S., Reynolds, C. F. III, Bruce, M. L., Katz, I. R., Raue, P. J., Mulsant, B. H., et al. (2009). Reducing suicidal ideation and depression in older primary care patients: 24-month outcomes of the PROSPECT study. Am. J. Psychiatry 166, 882–890. doi: 10.1176/appi.ajp.2009.08121779
Almeida, O. P., Draper, B., Snowdon, J., Lautenschlager, N. T., Pirkis, J., Byrne, G., et al. (2012). Factors associated with suicidal thoughts in a large community study of older adults. Br. J. Psychiatry 201, 466–472. doi: 10.1192/bjp.bp.112.110130
Andresen, E. M., Malmgren, J. A., Carter, W. B., and Patrick, D. L. (1994). Screening for depression in well older adults: evaluation of a short form of the CES-D. Am. J. Prev. Med. 10, 77–84.
Baek, H. S., Lee, K. U., Joo, E. J., Lee, M. Y., and Choi, K. S. (2010). Reliability and validity of the Korean version of the Connor-Davidson Resilience Scale. Psychiatry Investig. 7, 109–115. doi: 10.4306/pi.2010.7.2.109
Beautrais, A. L. (2002). A case control study of suicide and attempted suicide in older adults. Suicide Life Threat Behav. 32, 1–9. doi: 10.1521/suli.32.1.1.22184
Centers for Disease Control, and Prevention (2015). Statistics Fatal Injury Report. Centers for Disease Control and Prevention (CDC), National Center for Injury Prevention and Control. Available at: https://webappa.cdc.gov/sasweb/ncipc/mortrate10_us.html
Connor, K. M., and Davidson, J. R. T. (2003). Development of a new resilience scale: the Connor-Davidson Resilience Scale (CD-RISC). Depress. Anxiety 18, 76–82. doi: 10.1002/da.10113
Conwell, Y., Duberstein, P. R., and Caine, E. D. (2002). Risk factors for suicide in later life. Biol. Psychiatry 52, 193–204. doi: 10.1016/S0006-3223(02)01347-1
Conwell, Y., Duberstein, P. R., Hirsch, J. K., Conner, K. R., Eberly, S., and Caine, E. D. (2010). Health status and suicide in the second half of life. Int. J. Geriatr. Psychiatry 25, 371–379. doi: 10.1002/gps.2348
Conwell, Y., Van Orden, K., and Caine, E. D. (2011). Suicide in older adults. Psychiatr. Clin. North Am. 34, 451–468. doi: 10.1016/j.psc.2011.02.002
Davidson, J. R., Payne, V. M., Connor, K. M., Foa, E. B., Rothbaum, B. O., Hertzberg, M. A., et al. (2005). Trauma, resilience and saliostasis: effects of treatment in post-traumatic stress disorder. Int. Clin. Psychopharmacol. 20, 43–48. doi: 10.1097/00004850-200501000-00009
De Leo, D., Padoani, W., Scocco, P., Lie, D., Bille-Brahe, U., Arensman, E., et al. (2001). Attempted and completed suicide in older subjects: results from the WHO/EURO multicentre study of suicidal behaviour. Int. J. Geriatr. Psychiatry 16, 300–310. doi: 10.1002/gps.337
Drapeau, A., Boyer, R., and Lesage, A. (2009). The influence of social anchorage on the gender difference in the use of mental health services. J. Behav. Health Serv. Res. 36, 372–384. doi: 10.1007/s11414-009-9168-0
Erlangsen, A., Stenager, E., and Conwell, Y. (2015). Physical disease as predictors of suicide in older adults: a nationwide, register-based cohort study. Soc. Psychiatry Psychiatr. Epidemiol. 50, 1427–1439. doi: 10.1007/s00127-015-1051-0
Hardy, S. E., Concato, J., and Gill, T. M. (2004). Resilience of community-dwelling older persons. J. Am. Geriatr. Soc. 52, 257–262. doi: 10.1111/j.1532-5415.2004.52065.x
Hinton, L., Zweifach, M., Tang, L., Unützer, J., and Oishi, S. (2006). Gender disparities in the treatment of late-life depression: qualitative and quantitative findings from the IMPACT trial. Am. J. Geriatr. Psychiatry 14, 884–892. doi: 10.1097/01.JGP.0000219282.32915.a4
Holmbeck, G. N. (2002). Post-hoc probing of significant moderational and mediational effects in studies of pediatric populations. J. Pediatr. Psychol. 27, 87–96. doi: 10.1093/jpepsy/27.1.87
Jeste, D. V., Savla, G. N., Thompson, W. K., Vahia, I. V., Glorioso, D. K., Martin, A. V. S., et al. (2013). Association between older age and more successful aging: critical role of resilience and depression. Am. J. Psychiatry 170, 188–196. doi: 10.1176/appi.ajp.2012.12030386
Juurlink, D. N., Herrmann, N., Szalai, J. P., Kopp, A., and Redelmeier, D. A. (2004). Medical illness and the risk of suicide in the elderly. JAMA Intern. Med. 164, 1179–1184. doi: 10.1001/archinte.164.11.1179
Kim, J., Lee, Y. S., and Lee, J. (2016). Living arrangements and suicidal ideation among the Korean older adults. Aging Ment. Health 20, 1305–1313. doi: 10.1080/13607863.2015.1078280
Kobasa, S. C. (1979). Stressful life events, personality, and health: an inquiry into hardiness. J. Pers. Soc. Psychol. 37, 1–11. doi: 10.1037/0022-3514.37.1.1
Kohout, F. J., Berkman, L. F., Evans, D. A., and Cornoni-Huntley, J. (1993). Two shorter forms of the CES-D depression symptoms index. J. Aging Health 5, 179–193. doi: 10.1177/089826439300500202
Lamond, A. J., Depp, C. A., Allison, M., Langer, R., Reichstadt, J., Moore, D. J., et al. (2008). Measurement and predictors of resilience among community-dwelling older women. J. Psychiatr. Res. 43, 148–154. doi: 10.1016/j.jpsychires.2008.03.007
Lapierre, S., Erlangsen, A., Waern, M., De Leo, D., Oyama, H., Scocco, P., et al. (2011). A systematic review of elderly suicide prevention programs. Crisis 32, 88–98. doi: 10.1027/0227-5910/a000076
Liu, D. W., Fairweather-Schmidt, A. K., Burns, R., Roberts, R. M., and Anstey, K. J. (2016). Psychological resilience provides no independent protection from suicidal risk. Crisis 37, 130–139. doi: 10.1027/0227-5910/a000364
Liu, D. W., Fairweather-Schmidt, A. K., Roberts, R. M., Burns, R., and Anstey, K. J. (2014). Does resilience predict suicidality? A lifespan analysis. Arch. Suicide Res. 18, 453–464. doi: 10.1080/13811118.2013.833881
Loprinzi, C. E., Prasad, K., Schroeder, D. R., and Sood, A. (2011). Stress management and resilience training (SMART) program to decrease stress and enhance resilience among breast cancer survivors: a pilot randomized clinical trial. Clin. Breast Cancer 11, 364–368. doi: 10.1016/j.clbc.2011.06.008
Lyons, J. A. (1991). Strategies for assessing the potential for positive adjustment following trauma. J. Trauma. Stress 4, 93–111. doi: 10.1002/jts.2490040108
O’Halloran, A. M., Kenny, R. A., and King-Kallimanis, B. L. (2014). The latent factors of depression from the short forms of the CES-D are consistent, reliable and valid in community-living older adults. Eur. Geriatr. Med. 5, 97–102. doi: 10.1016/j.eurger.2013.12.004
Osman, A., Bagge, C. L., Gutierrez, P. M., Konick, L. C., Kopper, B. A., and Barrios, F. X. (2001). The Suicidal Behaviors Questionnaire-Revised (SBQR): validation with clinical and nonclinical samples. Assessment 8, 443–454. doi: 10.1177/107319110100800409
Oyama, H., Sakashita, T., Ono, Y., Goto, M., Fujita, M., and Koida, J. (2008). Effect of community-based intervention using depression screening on elderly suicide risk: a meta-analysis of the evidence from Japan. Community Ment. Health J. 44, 311–320. doi: 10.1007/s10597-008-9132-0
Oyama, H., Watanabe, N., Ono, Y., Sakashita, T., Takenoshita, Y., Taguchi, M., et al. (2005). Community-based suicide prevention through group activity for the elderly successfully reduced the high suicide rate for females. Psychiatry Clin. Neurosci. 59, 337–344. doi: 10.1111/j.1440-1819.2005.01379.x
Paraschakis, A., Douzenis, A., Michopoulos, I., Christodoulou, C., Vassilopoulou, K., Koutsaftis, F., et al. (2012). Late onset suicide: distinction between “young-old” vs. “old-old” suicide victims. How different populations are they? Arch. Gerontol. Geriatr. 54, 136–139. doi: 10.1016/j.archger.2011.02.011
Park, E. O., and Lee, H. Y. (2015). Factors influencing suicidal ideation among korean adults by age: results of the 2010–2011 korean health and nutrition examination survey. Community Ment. Health J. 51, 987–993. doi: 10.1007/s10597-015-9863-7
Radloff, L. S. (1977). The CES-D scale: a self-report depression scale for research in the general population. Appl. Psychol. Meas. 1, 385–401. doi: 10.1177/014662167700100306
Roy, A., Carli, V., and Sarchiapone, M. (2011). Resilience mitigates the suicide risk associated with childhood trauma. J. Affect. Disord. 133, 591–594. doi: 10.1016/j.jad.2011.05.006
Roy, A., Sarchiapone, M., and Carli, V. (2007). Low resilience in suicide attempters: relationship to depressive symptoms. Depress. Anxiety 24, 273–274. doi: 10.1002/da.20265
Rubenowitz, E., Waern, M., Wilhelmson, K., and Allebeck, P. (2001). Life events and psychosocial factors in elderly suicides–a case–control study. Psychol. Med. 31, 1193–1202. doi: 10.1017/S0033291701004457
Rutter, M. (1985). Resilience in the face of adversity: protective factors and resistance to psychiatric disorder. Br. J. Psychiatry 147, 598–611. doi: 10.1192/bjp.147.6.598
Schulz, R., Drayer, R. A., and Rollman, B. L. (2002). Depression as a risk factor for non-suicide mortality in the elderly. Biol. Psychiatry 52, 205–225. doi: 10.1016/S0006-3223(02)01423-3
Shin, S. Y. (2011). Validity Study of Short Forms of the Korean Version Center for Epidemiologic Studies Depression Scale (CES-D). [Master’s thesis]. Seoul National University. Available at: http://dcollection.snu.ac.kr/jsp/common/DcLoOrgPer.jsp?sItemId=000000030438
Statistics Korea (2016). Elderly Statistics. Available at: http://kostat.go.kr/
Steinhardt, M., and Dolbier, C. (2008). Evaluation of a resilience intervention to enhance coping strategies and protective factors and decrease symptomatology. J. Am. Coll. Health 56, 445–453. doi: 10.3200/JACH.56.44.445-454
Stephens, T. M. (2013). Nursing student resilience: a concept clarification. Nurs. Forum 48, 125–133. doi: 10.1111/nuf.12015
Unützer, J., Tang, L., Oishi, S., Katon, W., Williams, J. W., Hunkeler, E., et al. (2006). Reducing suicidal ideation in depressed older primary care patients. J. Am. Geriatr. Soc. 54, 1550–1556. doi: 10.1111/j.1532-5415.2006.00882.x
Windle, G., Bennett, K. M., and Noyes, J. (2011). A methodological review of resilience measurement scales. Health Qual. Life Outcomes 9, 1–18. doi: 10.1186/1477-7525-9-8
World Health Organization [WHO] (2012). Good Health Adds Life to Years. Global Brief for World Health Day 2012. Geneva: World Health Organization.
World Health Organization [WHO] (2014). Preventing Suicide: A Global Imperative. Geneva: World Health Organization.
Keywords: suicide, suicidal behavior, older adults, resilience, gender difference
Citation: You S and Park M (2017) Resilience Protected against Suicidal Behavior for Men But Not Women in a Community Sample of Older Adults in Korea. Front. Psychol. 8:401. doi: 10.3389/fpsyg.2017.00401
Received: 01 February 2017; Accepted: 02 March 2017;
Published: 15 March 2017.
Edited by:
Roumen Kirov, Institute of Neurobiology (BAS), BulgariaReviewed by:
Timo Partonen, National Institute for Health and Welfare, FinlandPaul William George Surgenor, Pieta House, Ireland
Copyright © 2017 You and Park This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sungeun You, c3VuZ2V1bnlvdUBnbWFpbC5jb20=