 Grant D. Searchfield
Grant D. Searchfield Mithila Durai
Mithila Durai- Section of Audiology, Eisdell Moore Centre, The University of Auckland, Auckland, New Zealand
Background: There are several established, and an increasing number of putative, therapies using sound to treat tinnitus. There appear to be few guidelines for sound therapy selection and application.
Aim: To review current approaches to personalizing sound therapy for tinnitus.
Methods: A “state-of-the-art” review (Grant and Booth, 2009) was undertaken to answer the question: how do current sound-based therapies for tinnitus adjust for tinnitus heterogeneity? Scopus, Google Scholar, Embase and PubMed were searched for the 10-year period 2006–2016. The search strategy used the following key words: “tinnitus” AND “sound” AND “therapy” AND “guidelines” OR “personalized” OR “customized” OR “individual” OR “questionnaire” OR “selection.” The results of the review were cataloged and organized into themes.
Results: In total 165 articles were reviewed in full, 83 contained sufficient details to contribute to answering the study question. The key themes identified were hearing compensation, pitched-match therapy, maskability, reaction to sound and psychosocial factors. Although many therapies mentioned customization, few could be classified as being personalized. Several psychoacoustic and questionnaire-based methods for assisting treatment selection were identified.
Conclusions: Assessment methods are available to assist clinicians to personalize sound-therapy and empower patients to be active in therapy decision-making. Most current therapies are modified using only one characteristic of the individual and/or their tinnitus.
Introduction
State-of-the-art reviews are a specific form of review that focus on current issues and new perspectives, often in areas with a need of further research (Grant and Booth, 2009). The last 10 years has seen the emergence of many new tinnitus therapies using sound (Hoare et al., 2013a, 2014b). Although the heterogeneity of tinnitus is widely acknowledged by clinicians, many common sound-based tinnitus treatments are applied with limited assessment of individual differences (Hoare et al., 2014b). The ambiguity underlying tinnitus mechanisms and the rapid development of commercial interests in digital sound technology for tinnitus treatment have resulted in an increase in treatment options but few selection guidelines (Searchfield, 2016). There appears to be little information as to how to choose between treatments and how to apply them based on individual differences. In this state-of-the-art review we focus on how sound-based therapies are modified for individual characteristics and needs.
Research into the benefits of sound as a tinnitus therapy medium has not been systematic (Mckenna and Irwin, 2008; Hobson et al., 2012). There have been concerns as to whether the claims made regarding the effectiveness of sound therapy are correct (Mckenna and Irwin, 2008). We believe that some of the ambiguity surrounding sound therapy arises by applying the title “sound therapy” as a blanket term to the use of (any) sound that may have a positive effect on tinnitus. There are numerous mechanisms by which sounds could interfere with tinnitus (Norena, 2015). Tinnitus may be masked by sound interfering with encoding (e.g., energetic masking, Vernon, 1977) or pattern recognition (e.g., informational masking, Kidd et al., 1998, 2002). Sounds may desynchronize neural ensembles suspected in tinnitus generation (Eggermont and Tass, 2015). Sounds with positive emotional associations can affect mood and arousal (Handscomb, 2006; Tang et al., 2009). Hearing aids may mask tinnitus and have psychosocial benefits by improving communication (Shekhawat et al., 2013b; Searchfield, 2015). Long-term alleviation of tinnitus may occur through habituation (Jastreboff, 2000), inhibition (Teismann et al., 2011), gain reduction (Norena, 2015) or possible elevations in individual signal detection thresholds (Welch and Dawes, 2008). Attention, cognition and context of perception also appear to be important factors that manipulate long-term adaptation to tinnitus (Searchfield et al., 2012; Searchfield, 2014; Andersson et al., 2016).
Across the health sciences the personalized medicine movement has created a shift in focus from a “one size fits all” model to one that tailors diagnosis and treatment to the individual (Tutton, 2012; Schleidgen et al., 2013). At the same time health services are beginning to shift from evidence-based medicine to evidence-informed individualized care (Miles and Loughlin, 2011). Personalized medicine tends to incorporate traditional assessment methods, genotyping and genomic evaluation to explain and predict risk and treatment outcomes (Ginsburg and Willard, 2009). There is a search for biomarkers and endophenotypes in tinnitus (Sand et al., 2007). The current absence of clear genetic and blood-based biomarkers for tinnitus does not preclude personalization of treatments. The view of personalized medicine should be broadened away from just genetic markers (Anon, 2012). Tinnitus has both psychoacoustic (sound) (Tyler, 2000) and psychological (emotion, reaction) markers (Meikle et al., 2012). The context of tinnitus experience is also likely to affect its perception (Andersson et al., 2016) so that tinnitus is the result of psychosocial, psychoacoustic and individual psychological factors (Searchfield, 2014). In addition to modifying treatments based on assessment outcomes there are good arguments for applying principles of person-centered care to tinnitus therapy. In person-centered care patients are encouraged to be active participants in their treatment through the creation of a power-balanced, therapeutic relationship with their health professionals (Michie et al., 2003). Patients who participate in their own care report greater satisfaction, better adherence and health outcomes (Grenness et al., 2014). Research in the treatment of various health conditions such as chronic pain, balance disorders, and diabetes shows that self-efficacy beliefs also play an important role in treatment outcomes and management of the condition (Smith and Fagelson, 2011). Tinnitus self-efficacy is the confidence that individuals have in their capabilities to perform the treatment courses of action needed to manage their tinnitus successfully (Smith and Fagelson, 2011).
Person-centered needs-based care in rehabilitative audiology is not a new concept (Grenness et al., 2014). Most audiologists will be familiar with needs-based assessment for hearing aid selection (Dillon et al., 1987); similar principles could be applied in tinnitus therapy. Such an approach requires clinicians to take into account the needs of individual tinnitus patients, and provide custom-tailored therapeutic approaches. Our purpose in reviewing the literature was to identify the current state-of-the-art in personalizing sound-based therapies.
Methods
A state-of-art review (Grant and Booth, 2009) was undertaken in December 2016 with cataloging of results in January and February 2017. All studies irrespective of quality were included as long as they addressed the topic and the research occurred in the last 10 years. There were no other inclusion/exclusion criteria. The research question for the current scoping review was: how do current sound-based therapies for tinnitus adjust for tinnitus heterogeneity? Sound-based therapies were defined as those that included the use of sound (either with or without counseling), but not psychological therapies used without sound or based on the scope of practice of psychologists (e.g., Cognitive Behavioral Therapy). From the included studies, all data were charted; themes and key issues were identified.
To identify relevant studies, the search was carried out using the databases Scopus, Google Scholar, Embase and PubMed for the 10-year period 2006–2016. The search strategy used the following key words: “tinnitus” AND “sound” AND “therapy” AND “guidelines” OR “personalized” OR “customized” OR “individual” OR “questionnaire” OR “selection.” The search on Google scholar was terminated when two full pages of consecutive results contained no entries of relevance to the study question. After initial consideration of title relevance to the study by one author (GDS), 199 articles were shortlisted. After reading the abstracts, 150 articles were read in full independently by two authors (GDS and MD). The reference lists of these 150 articles were searched for additional pertinent articles. This returned a further 15 articles for which the text was read in full, of those 165 articles for which full text was reviewed 83 studies described personalization (customization, individual adjustment) methods sufficiently to extract meaningful data. Two authors (GDS and MD) achieved a consensus on classification of content with the third author (TL) verifying categorization.
Studies were charted according to the method used to personalize therapy. The application of psychoacoustical and/or psychosocial assessment tools to treatment selection and management was cataloged along with the method used to customize the treatment for individual characteristics. A therapy might employ multiple types of customization and tools, in which case cross-referencing was used. In addition, evidence for person-centered care was recorded (including: getting to know patient or client as a person, sharing of power and responsibility, informed of treatment choice, accessibility and flexibility of service provider, coordination and integration, environment that is conducive to person-centered care).
Results
Five themes were identified from the literature surveyed as categorical answers to the question: “how do current sound-based therapies for tinnitus adjust for tinnitus heterogeneity?” The themes were “hearing compensation” (adjustment to audiometry) “pitch matched” (adjustment using the predominant tinnitus pitch) “maskability” (adjustment to a desired level of masking) “reaction to sound” (selection based on the emotional or relaxing characteristics of sound) and “psychosocial factors” (use of psychological and/or environmental factors to select therapy). The therapy themes, the treatments using the approach, and the assessment used, are cataloged in Table 1.
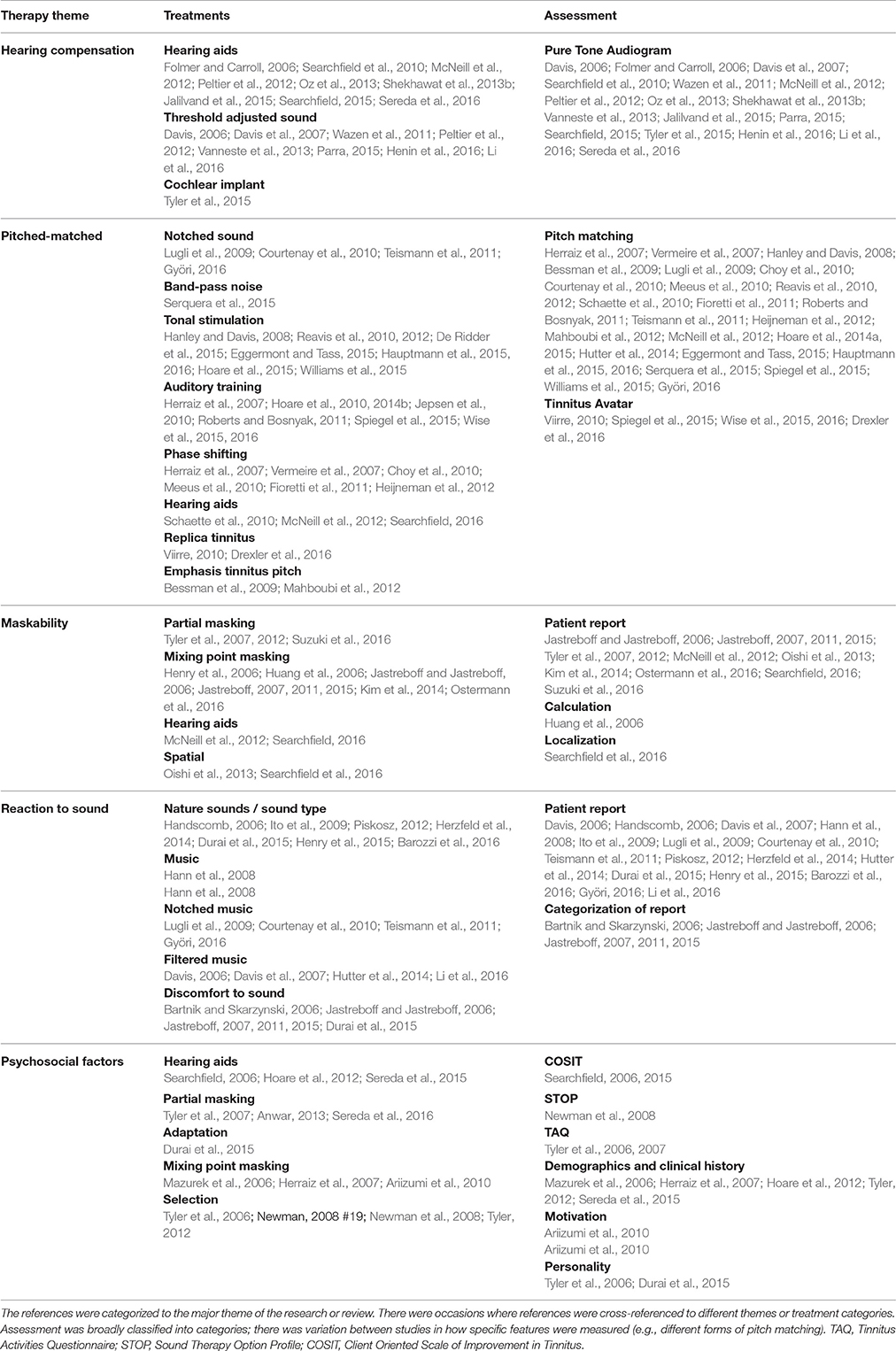
Table 1. Therapy themes and references.
Hearing Compensation
Treatments that modified their response on the basis of hearing sensitivity were hearing aids and sound stimulation compensating for reduced audibility (Table 1). Hearing aids were used to correct for loss of audibility of sounds that accompanied hearing loss. When the primary focus of hearing aid fitting was to improve hearing for speech an emphasis was placed on amplifying sound in a frequency specific manner to improve intelligibility (McNeill et al., 2012; Shekhawat et al., 2013b). When tinnitus was the primary focus a secondary goal for amplification was raising the audibility of environmental sounds (Shekhawat et al., 2013a). The basis for modification was the individuals hearing thresholds obtained using pure-tone audiometry. The amount of amplification was determined using a prescription based on the audiogram (Shekhawat et al., 2013a). Hearing aids were considered to reduce hearing handicap, reduce the levels of attention paid to tinnitus, and compensate for deafferentation, and possibly improve cognition (Searchfield, 2006, 2015; Shekhawat et al., 2013b; Sereda et al., 2015; Zarenoe et al., 2017). McNeill et al. (2012) identified those most likely to achieve benefit from hearing aids as having good low frequency hearing and tinnitus pitch within the amplification range of the hearing aids (McNeill et al., 2012). Jalilvand et al. (2015) suggested that hearing aids might be more successful in management of tinnitus from blast injuries than sound generators (Jalilvand et al., 2015). Frequency lowering processing was suggested as an alternative strategy to conventional amplification (Peltier et al., 2012). Several studies suggested sound therapy device selection based on the audiogram (from hearing aids, combination instruments and cochlear implants) (Folmer and Carroll, 2006; Mazurek et al., 2006; Tyler et al., 2015; Searchfield, 2016). Searchfield (2016) recommended normal hearing would be fitted with sound generators; high frequency hearing loss with hearing aids; hearing loss encompassing low frequencies with combination instruments; severe-profound hearing loss with cochlear implants.
Hearing loss will affect the perception of therapeutic sounds in addition to reducing the audibility of speech and environmental sounds. To address this several sound therapies adjusted the spectrum of music (Davis et al., 2007; Wazen et al., 2011; Peltier et al., 2012; Vanneste et al., 2013; Henin et al., 2016; Li et al., 2016), fractal tones (Herzfeld et al., 2014) or noise (Uriz et al., 2013) for the presence of hearing loss. The intent from threshold-adjusted sounds was to make the sound audible across a broad frequency range rather than stimulating the frequencies with best thresholds (Davis, 2006; Távora-Vieira et al., 2011). In some cases too severe a hearing loss was an exclusion factor for therapy (Davis et al., 2007). One study suggested that adjusting music levels for hearing threshold was of no benefit to tinnitus suppression (Vanneste et al., 2013).
Pitch-Based Therapy
Several therapies used the pitch or spectrum of tinnitus as the basis for stimulation. Sound stimuli were individualized to span a frequency range centered on the dominant tinnitus pitch (Table 1). The sounds used and intended mechanisms of effect varied greatly: some therapies attempt to change the synchronized firing of neural assemblies near tinnitus pitch using tonal stimulation (Hanley and Davis, 2008; Reavis et al., 2010, 2012; Eggermont and Tass, 2015; Hauptmann et al., 2015, 2016; Hoare et al., 2015; Williams et al., 2015); others changed the phase of sounds presented at tinnitus pitch (Herraiz et al., 2007; Vermeire et al., 2007; Choy et al., 2010; Meeus et al., 2010; Fioretti et al., 2011; Heijneman et al., 2012) and another paired tonal stimulation with vagus nerve stimulation (De Ridder et al., 2015). Tinnitus pitch was used as the basis for selecting band-pass noise (Serquera et al., 2015) notched music (Courtenay et al., 2010; Teismann et al., 2011; Györi, 2016) or noise (Lugli et al., 2009) for lateral inhibition (Courtenay et al., 2010) and one method provided extra stimulation at tinnitus pitch (Mahboubi et al., 2012) while another used tinnitus pitch-matched sound embedded in nature sounds as a therapy (Bessman et al., 2009). Another form of pitch-based therapy employed participants undertaking active training tasks in discrimination (Herraiz et al., 2007; Roberts and Bosnyak, 2011; Hoare et al., 2013b, 2014b; Wise et al., 2016) or categorization tasks (Jepsen et al., 2010). The intended mechanism of effect for these training tasks is reorganization of tonotopic maps, but their main effect may be in modifying attention to tinnitus (Hoare et al., 2010). Several studies used more complex replicas (avatars) of tinnitus for passive stimulation (Viirre, 2010) and stimulation only while asleep (Pedemonte et al., 2010). Auditory training in a game format used the individual's tinnitus avatar as a distractor (Wise et al., 2016).
The variability in tinnitus pitch matching is a critical concern issue for pitch-based treatments (Hoare et al., 2014a; Serquera et al., 2015). Variability in pitch match that is more than one octave between consecutive sessions may preclude some therapies (Hoare et al., 2014a). Pitch matching is not considered very useful in methods based on counseling and broad noise therapy (Baguley et al., 2013). However, tinnitus pitch within the effective range of sound therapy device may be a prognostic factor for treatment success (Schaette et al., 2010; McNeill et al., 2012; Searchfield, 2016). Momentary analysis may have a role in guiding treatments in which the feature measured (e.g., pitch) guides treatment sound selection. Incorporating such assessments into daily routine in a non-threatening manner or even game (Wise et al., 2016) may mitigate the potential negative effects of momentary analysis in priming individuals to focus on their tinnitus.
Maskability
We used a psychoacoustic definition of masking: when the perception of tinnitus is affected by the presence of another sound. The level of sound used in theory has been one of the more contentious issues in audiology-based tinnitus therapy (Jastreboff, 2007; Tyler et al., 2012). Masking can be used to totally or partially reduce the audibility of tinnitus by covering it with another sound. Tinnitus Retraining Therapy (TRT) advocates a masking level in which the sound mixes with, but does not cover, the tinnitus (Henry et al., 2006; Huang et al., 2006; Jastreboff and Jastreboff, 2006; Jastreboff, 2007, 2011, 2015; Kim et al., 2014; Ostermann et al., 2016) while others suggest use of the minimum level resulting in relief (Tyler et al., 2007, 2012; Suzuki et al., 2016). Most therapies set their target level based on patients' reports of tinnitus audibility and sound being comfortable, although Huang et al. (2006) reported that the mixing level could be predicted on the basis of the MML (Huang et al., 2006). Kim et al. (2014) reported TRT with broadband noise to have a higher success rate than mixed or narrowband noise (Kim et al., 2014). TRT and masking is typically practiced using sound presentation to both ears; Oishi et al. suggested that monaural presentation can be successful (Oishi et al., 2013) and Searchfield et al. (2016) showed the potential for binaural sound presentation using interaural cues and Head Related Transfer Function to achieve spatial as well as spectral masking.
Reaction to Sound
In order for sound therapy to be effective it must be comfortable to the user. Under this theme we cataloged therapies that considered individual's sensitivity to, or, reaction to sounds. A key factor in allocating participants to the treatment categories used in TRT was known discomfort to sound (Jastreboff and Jastreboff, 2006; Jastreboff, 2007, 2011, 2015). Personality may be a predictive factor in determining if a participant is sound responsive or sound sensitive (Durai et al., 2015). A positive individual response to therapeutic sounds will increase the individual's ability to achieve treatment goals as well as compliance to treatment. The strong emotional response to music has seen its use as a therapeutic tool (Hann et al., 2008). Music has been adopted as the sound manipulated in the Neuromonics Tinnitus Treatment (Davis et al., 2007; Li et al., 2016) and notched music therapies (Lugli et al., 2009; Courtenay et al., 2010; Teismann et al., 2011; Györi, 2016). Fractal tones also have music-like relaxation properties (Herzfeld et al., 2014). Advances in hearing aid technology allow relaxing music or nature sounds to be directly streamed from a patient's smart phone to their hearing aids (Piskosz, 2012). Studies to date suggest that modulated sounds (Henry et al., 2015) or nature sounds (Barozzi et al., 2016) achieve tinnitus benefits similar to broadband noise stimulation.
Psychosocial
We defined psychosocial factors in sound therapy as social moderators and individual thoughts and behaviors that determine the treatment approach. In an evaluation of tinnitus management in NHS audiology departments in the UK by Hoare et al. (2012) identified a wide range of factors that influenced clinicians management strategies (in order of high-low reporting): level of hearing loss, evidence of stress or anxiety, state of mind, severity, willingness to try treatment, sleep disturbance, health, understanding, lifestyle preferences, coping ability, hyperacusis, age, and depression. Although these results were not described in terms of sound-therapy specific decision-making, three of the top four treatments reported were sound-based or could use sound (hearing aids, sound generator, habituation). In a similar population psychosocial factors were used in selecting hearing aids for tinnitus and mild hearing loss (Sereda et al., 2015). Skepticism, length of treatment and attitude can influence treatment success (Herraiz et al., 2007). Willingness to pay may affect client decision-making (Tyler, 2012). Older patients and tinnitus of longer duration may benefit less from sound therapies (Mazurek et al., 2006; Anwar, 2013). Questionnaires have been used in several person-centered tinnitus therapies to guide treatment (Table 2). In Tinnitus Activities Treatment (TAT), the Iowa Tinnitus Activities Questionnaire is recommended to identify patient's needs and treatment priorities (Tyler et al., 2007). Searchfield (2006) advocated the use of a tinnitus version of the Client Orientated Scale of Improvement (COSIT) to identify and set goals for treatment. Newman et al. (2008) used the Sound Therapy Option Profile (STOP) to assist in therapy selection and understanding patient attitudes to different treatments and the Self-Efficacy for Tinnitus Management Questionnaire (SETMQ) can be used to assess patient confidence in using different treatments (Smith and Fagelson, 2011; Fagelson and Smith, 2016).
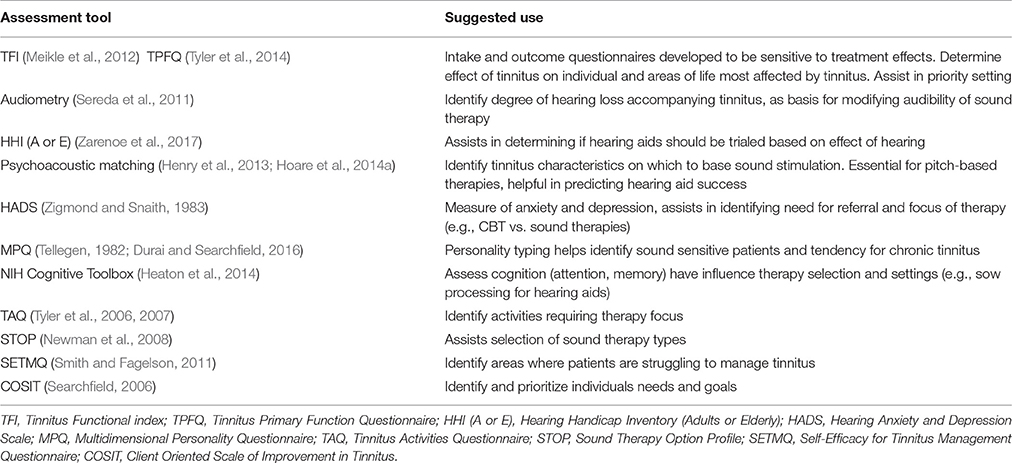
Table 2. Examples of tinnitus assessments that can be chosen to help guide sound therapy selection.
Discussion
Tinnitus is a heterogeneous disorder: tinnitus sound can differ between individuals, it can result from many different types of injury and its effect can vary from a minor annoyance to catastrophic impact on daily life (Stouffer and Tyler, 1990).
The review of the literature identified five sound therapy themes. Some treatments were included across themes. The majority of studies considered tailored or customized therapy to be selection of treatment sound on the basis of either audiometric threshold or tinnitus pitch. There were approaches that used dimensions of tinnitus severity, sound sensitivity and hearing to categorize or subtype groups of sufferers (Jastreboff, 2011). Another approach was a hierarchy or stepped care model in which individually tailored treatments were used if less resource intensive methods were unsuccessful (Myers et al., 2014). Stepped care has been implemented in environments where universal individually focused therapy would be economically unsustainable (Department of Health, 2009; Myers et al., 2014). Unlike single characteristic therapies whole-person approaches involved patients in decision making as to which of several approaches are best suited to them (Tyler et al., 2007; Newman et al., 2008). We believe that a contributing factor to the inconsistent benefit reported with sound therapies (Mckenna and Irwin, 2008; Hobson et al., 2012) is application of a single title “sound therapy” to a very heterogeneous collection of different sound-based approaches. In addition individual needs and reaction to therapy sounds differ (Durai and Searchfield, 2017) we ascribe to the philosophy that individuals are most likely to manage their tinnitus better when the treatment plan is tailored to their needs (Fisher and Boswell, 2016).
Planning Individual Tinnitus Care
The review did not identify any comprehensive guidelines for optimal sound therapy selection. We believe that many of the sound therapies identified could be effective when selected for the right patients at the right time and appropriate context. To do this we suggest careful assessment and then use of an individual care plan. In this review we deliberately focus on sound therapy, but we strongly believe any treatment plan should consider counseling (Tyler et al., 2007; Searchfield et al., 2011), and referral for psychological therapies such as Cognitive Behavioral Therapy (Martinez-Devesa et al., 2006) when appropriate. By determining individual needs and priorities, alongside assessment measures such as pure-tone audiometry and pitch matching, a plan can be developed that we believe reduces the risk for ineffective treatment. An effective individual care plan may also reduce the time required for treatment, reducing stress, anxiety and loss of hope for the sufferer. We believe those factors of the individual's complaint that are likely to be driving other symptoms should be addressed by therapy first (Fisher and Boswell, 2016).
Based on the review, along with our clinical experience, we suggest that the individual care plan use various clinical assessment methods. When patients first attend the clinic their clinical history, a thorough hearing assessment and tinnitus matching should be undertaken (Langguth et al., 2007). A questionnaire assessing aspects of tinnitus effects on quality of life should be used to provide an overview of tinnitus impact, and serve as a baseline for future assessments of outcomes. The Tinnitus Functional Index (Meikle et al., 2012) and Tinnitus Primary Function Questionnaire (Tyler et al., 2014) are two recent questionnaires developed for this purpose. Based on a clinical history an evaluation of anxiety and depression (e.g., the Hospital Anxiety and Depression Scale, Andersson et al., 2003) or cognition [e.g., National Institutes for Health (NIH) Toolbox Cognition Battery, Heaton et al., 2014] may be important. The comorbidity of anxiety and depression with tinnitus is well known (Andersson et al., 2003). The Hospital Anxiety and Depression Scale (HADS) (Zigmond and Snaith, 1983) or similar questionnaire scores can assist decision-making as to the necessity and priorities for psychological therapies. Tinnitus negatively impacts on cognition (Zarenoe et al., 2017). We do not know yet if differences in cognition should influence selection of sound therapy type, however research suggests that slow-acting hearing aid processing strategies may lead to better hearing when users memory is impaired (Lunner et al., 2009). We also recommend the assessment of personality. The use of personality questionnaires such as the Multidimensional Personality Questionnaire (MPQ) subscales (Tellegen, 1982) in clinics may be useful in identifying at-risk individuals for distressing tinnitus. Four key “maladaptive” personality traits are suspected in playing a role in diverting attention and processing resources toward tinnitus and which may subsequently act to prevent adaptation. These include higher levels of stress reaction, lower social closeness, lower self-control and higher alienation (Durai and Searchfield, 2016). If, for example, an individual has high stress reactions and low self-control and reacts negatively to sound psychological-based interventions may be needed before sound therapy.
Hoare et al. (2014b) recommended that clinicians be guided by the patient's point of care, patient motivation and expectations of sound therapy. The acceptability of the intervention both in terms of the sound stimuli to be used and whether patients are willing to use sound extensively or intermittently is important (Hoare et al., 2014b). A step in this direction is counseling patients about the therapies that are available. Information should be provided about the basis of the treatment, evidence for effectiveness, speed of effects, and costs. Aazh et al. (2009) suggest a poster format for this pre-consultation information; clinics websites and marketing material also can provide useful appointment scene setting. A tinnitus needs assessment can assist in the shared decision making process. The Hearing and Tinnitus clinic at the University of Auckland has used the COSIT as a decision making and goal setting tool for over a decade (Searchfield, 2006). The COSIT is a modification of the COSI, a tool frequently used in needs assessment for hearing problems (Dillon et al., 1987). Other questionnaires that may assist needs assessment include the TAQ (Tyler et al., 2007), STOP (Newman et al., 2008) and SETMQ (Smith and Fagelson, 2011). The TAQ determines the areas in which tinnitus creates problems (emotion, sleep, communication and/or concentration). The TAQ can highlight areas of life in which tinnitus is having the most debilitating effect, which can then be used to focus or tailor treatment (Tyler et al., 2007). The STOP is an 11-item tool that takes into account motivation, acceptance, expectations and willingness to use sound therapy devices (Newman et al., 2008). The SETMQ is a 40-item measure that quantifies the patient's confidence in managing tinnitus in five areas: (1) routine management, (2) emotional response, (3) internal thoughts and interaction with others, (4) tinnitus concepts, and (5) use of assistive devices such as hearing aids and maskers (Smith and Fagelson, 2011).
The relative effectiveness of these questionnaires in informing successful treatment has to be determined. However the usefulness and time savings achieved by use of these questionnaires should not be underestimated, as they can be completed by the patient prior to their appointment and can be assessed by the clinician prior to meeting the patient; saving time during the appointment. There is overlap in the questions asked by the questionnaires so not all need be used. It is important that clinicians choose those questionnaires best suited to the treatments they offer and their health care setting and patient population. We suggest that many audiologists will find the open-ended format of the COSIT familiar, and may wish to combine with one or more closed question formats (TAQ, STOP, SETMQ). The outcome of appropriately selected assessments can result in an efficient tinnitus clinic. Unnecessary or inappropriate treatments can be avoided, reducing the risk that patients become disillusioned with the clinician's methods. With patient “buy-in,” motivation and compliance to treatments should be high. Understanding and choosing the treatments to use immediately, and as the impact of tinnitus changes, may be empowering to the patient.
Advancing Sound Therapy and Recognizing Its Limitations
The literature review highlighted the diverse basis and application of sound therapy. Researchers and publications need to be clear on what aspect or type of sound therapy is being used. Mckenna and Irwin (2008) wrote a useful critique of sound therapy with the provocative title “Sound therapy: sacred cow or idol worship?” Mckenna and Irwin's (2008) main arguments were that the mechanisms of sound therapy were not necessarily those claimed, effects may be cognitive or psychological rather than purely auditory, and benefits were modest, if any, above counseling alone. Sound therapy is potentially confusing, given the numerous approaches and various potential mechanisms of effect. While more evidence for sound therapies is becoming available there is still a need to prove benefits. The individualized sound therapy approach also needs to be validated relative to single therapy protocols. In order to provide this evidence we may a need to move away from the dominant nomothetic research approach to an idiographic method that embraces individual variance (Fisher and Boswell, 2016). Group comparisons are limited in their ability to identify effective sound therapies when there is heterogeneity. Sound therapy is, in general, a slow-acting therapy that requires long-term use of some form of sound delivery device; so longitudinal data is needed. Research also needs to continue to investigate whether auditory-based therapies can be enhanced, or sped up, by combining with non-invasive brain (Shekhawat et al., 2014; De Ridder et al., 2015) or multisensory (Spiegel et al., 2015) stimulation.
Conclusions
The basis of sound therapy is the belief that increasing extrinsic sound driven activity of the auditory system reduces tinnitus. This does not mean sound therapy is uniform in its application; instead it covers many dimensions and presumed mechanisms of effect. Current commentary on sound therapy fails to fully recognize this heterogeneity in application. At the same time few sound therapies can truly be considered personalized to make the most of their purported mechanisms. Much of the literature surveyed used the terms “customized” or “tailored” in terms of a single dimension rather than viewing tinnitus as a complex combination of dimensions. Tools exist for personalizing and planning treatments, they should be integrated into patient care, and their usefulness tested.
Author Contributions
GS undertook the initial database search, cataloging, and prepared the manuscript and revisions. MD was involved in manuscript preparation and cataloging of results. TL reviewed the cataloging and contributed to the manuscript with a focus on clinical application.
Funding
The researchers are supported by the JM Cathie Trust Fund of the Auckland Medical Research Foundation, the American Tinnitus Association, and the Oticon Foundation of NZ.
Conflict of Interest Statement
GS is the scientific director of the University of Auckland Hearing and Tinnitus Clinic and Tinnitus Tunes, an online Tinnitus Therapy resource.
The other authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Aazh, H., Moore, B. C., and Roberts, P. (2009). Patient-centered tinnitus management tool: a clinical audit. Am. J. Audiol. 18, 7–13. doi: 10.1044/1059-0889(2009/08-0037)
Andersson, G., Heesser, H., and McKenna, L. (2016). “Psychological mechanisms and tinnitus,” in Tinnitus Clinical and Research Perspectives, eds D. Baguley and M. Fagelson (San Diego, CA: Plural Publishing), 63–74.
Andersson, G., Kaldo-Sandstrom, V., Strom, L., and Stromgren, T. (2003). Internet administration of the hospital anxiety and depression scale in a sample of tinnitus patients. J. Psychosom. Res. 55, 259–262. doi: 10.1016/S0022-3999(02)00575-5
Anon (2012). What happened to personalized medicine? Nature Biotechnology 30:1. doi: 10.1038/nbt.2096
Anwar, M. N. (2013). Mining and analysis of audiology data to find significant factors associated with tinnitus masker. Springerplus 2:1. doi: 10.1186/2193-1801-2-595
Ariizumi, Y., Hatanaka, A., and Kitamura, K. (2010). Clinical prognostic factors for tinnitus retraining therapy with a sound generator in tinnitus patients. J. Med. Dent. Sci. 57, 45–53. doi: 10.11480/jmds.570106
Baguley, D., McFerran, D., and Hall, D. (2013). Tinnitus. Lancet 382, 1600–1607. doi: 10.1016/S0140-6736(13)60142-7
Barozzi, S., Del Bo, L., Crocetti, A., Dyrlund, O., Passoni, S., Zolin, A., et al. (2016). A comparison of nature and technical sounds for tinnitus therapy. Acta. Acust. United Acust. 102, 540–546. doi: 10.3813/AAA.918971
Bartnik, G. M., and Skarzynski, H. (2006). “Tinnitus retraining therapy,” in Tinnitus Treatment: Clinical Protocols, ed R. Tyler (New York, NY: Thieme Medical Publishers, Inc.), 133–145.
Bessman, P., Heider, T., Watten, V. P., and Watten, R. G. (2009). The tinnitus intensive therapy habituation program: a 2-year follow-up pilot study on subjective tinnitus. Rehabil. Psychol. 54, 133–137. doi: 10.1037/a0015660
Choy, D., Lipman, R., and Tassi, G. (2010). Worldwide experience with sequential phase-shift sound cancellation treatment of predominant tone tinnitus. L. Laryngol Otol. 124, 366–369. doi: 10.1017/S0022215109992167
Courtenay, E. W., Schlaug, G., and Pantev, C. (2010). Listening to filtered music as a treatment option for tinnitus: a review. Music Percept. 27, 327–330. doi: 10.1525/mp.2010.27.4.327
Davis, P. (2006). “Music and the acoustic desensitization protocol for tinnitus,” in Tinnitus Treatment, ed R. S. Tyler (New York, NY: Thieme), 146–160.
Davis, P. B., Paki, B., and Hanley, P. J. (2007). Neuromonics tinnitus treatment: third clinical trial. Ear. Hear. 28, 242–259. doi: 10.1097/AUD.0b013e3180312619
Department of Health (2009). Provision of Services for Adults with Tinnitus: A Good Practice Guide. London: Central office of information.
De Ridder, D., Kilgard, M., Engineer, N., and Vanneste, S. (2015). Placebo-controlled vagus nerve stimulation paired with tones in a patient with refractory tinnitus: a case report. Otol. Neurotol. 36, 575–580. doi: 10.1097/MAO.0000000000000704
Dillon, H., James, A., and Ginis, J. (1987). Client oriented scale of improvement (COSI) and its relationship to several other measures of benefit and satisfaction provided by hearing aids. J. Am. Acad. Audiol. 8, 27–43.
Drexler, D., Lopez-Paullier, M., Rodio, S., Gonzalez, M., Geisinger, D., and Pedemonte, M. (2016). Impact of reduction of tinnitus intensity on patients' quality of life. Int. J. Audiol. 55, 11–19. doi: 10.3109/14992027.2015.1072772
Durai, M., Kobayashi, K., and Searchfield, G. (2015). A preliminary examination of the roles of contextual stimuli and personality traits under the adaptation level theory model of tinnitus. Acta. Acust United Acust. 101, 543–551. doi: 10.3813/AAA.918851
Durai, M., and Searchfield, G. (2016). Anxiety and depression, personality traits relevant to tinnitus: a scoping review. Int. J. Audiol. 55, 605–615. doi: 10.1080/14992027.2016.1198966
Durai, M., and Searchfield, G. D. (2017). A mixed-methods trial of broad band noise and nature sounds for tinnitus therapy: group and individual responses modeled under the adaptation level theory of tinnitus. Front. Aging. Neurosci. 9:44. doi: 10.3389/fnagi.2017.00044
Eggermont, J. J., and Tass, P. A. (2015). Maladaptive neural synchrony in tinnitus: origin and restoration. Front. Neurol. 6:29. doi: 10.3389/fneur.2015.00029
Fagelson, M. A., and Smith, S. L. (2016). Tinnitus self-efficacy and other tinnitus self-report variables in patients with and without post-traumatic stress disorder. Ear Hear. 37, 541–546. doi: 10.1097/AUD.0000000000000290
Fioretti, A., Eibenstein, A., and Fusetti, M. (2011). New trends in tinnitus management. Open Neurol. J. 5:12. doi: 10.2174/1874205X01105010012
Fisher, A. J., and Boswell, J. F. (2016). Enhancing the personalization of psychotherapy with dynamic assessment and modeling. Assessment 23, 496–506. doi: 10.1177/1073191116638735
Folmer, R. L., and Carroll, J. R. (2006). Long-term effectiveness of ear-level devices for tinnitus. Otol. Head Neck Surg. 134, 132–137. doi: 10.1016/j.otohns.2005.09.030
Ginsburg, G. S., and Willard, H. F. (2009). Genomic and personalized medicine: foundations and applications. Transl. Res. 154, 277–287. doi: 10.1016/j.trsl.2009.09.005
Grant, M. J., and Booth, A. (2009). A typology of reviews: an analysis of 14 review types and associated methodologies. Health Info. Libr. J. 26, 91–108. doi: 10.1111/j.1471-1842.2009.00848.x
Grenness, C., Hickson, L., Laplante-Lévesque, A., and Davidson, B. (2014). Patient-centred care: a review for rehabilitative audiologists. J. Audiol. 53, S60–S67. doi: 10.3109/14992027.2013.847286
Györi, A. (2016). “Tailor-made notched music training-a therapy of chronic tinnitus,” in Computer Music Seminar Aachen. Available online at: https://www.researchgate.net/publication/310046636_Tailor-Made_Notched_Music_Training_-_a_therapy_of_chronic_tinnitus
Handscomb, L. (2006). Use of bedside sound generators by patients with tinnitus-related sleeping difficulty: which sounds are preferred and why? Acta Otolaryngol. 126, 59–63. doi: 10.1080/03655230600895275
Hanley, P. J., and Davis, P. B. (2008). Treatment of tinnitus with a customized, dynamic acoustic neural stimulus: underlying principles and clinical efficacy. Trends Amp. 12, 210–222. doi: 10.1177/1084713808319942
Hann, D., Searchfield, G. D., Sanders, M., and Wise, K. (2008). Strategies for the selection of music in the short-term management of mild tinnitus. ANZ. J. Audiol. 30:129. doi: 10.1375/audi.30.2.129
Hauptmann, C., Ströbel, A., Williams, M., Patel, N., Wurzer, H., von Stackelberg, T., et al. (2015). Acoustic coordinated reset neuromodulation in a real life patient population with chronic tonal tinnitus. BioMed. Res. Int. 2015:569052. doi: 10.1155/2015/569052
Hauptmann, C., Wegener, A., Poppe, H., Williams, M., Popelka, G., and Tass, P. A. (2016). Validation of a mobile device for acoustic coordinated reset neuromodulation tinnitus therapy. J. Am. Acad. Audiol. 27, 720–731. doi: 10.3766/jaaa.15082
Heaton, R. K., Akshoomoff, N., Tulsky, D., Mungas, D., Weintraub, S., Dikmen, S., et al. (2014). Reliability and validity of composite scores from the NIH toolbox cognition battery in adults. J. Int. Neuropsychol. Soc. 20, 588–598. doi: 10.1017/S1355617714000241
Heijneman, K. M., De Kleine, E., and Van Dijk, P. (2012). A randomized double-blind crossover study of phase-shift sound therapy for tinnitus. Otolaryngol. Head Neck Surg. 147, 308–315. doi: 10.1177/0194599812442615
Henin, S., Fein, D., Smouha, E., and Parra, L. C. (2016). The effects of compensatory auditory stimulation and high-definition transcranial direct current stimulation (hd-tdcs) on tinnitus perception - a randomized pilot study. PLoS ONE 11:e0166208. doi: 10.1371/journal.pone.0166208
Henry, J. A., Frederick, M., Sell, S., Griest, S., and Abrams, H. (2015). Validation of a novel combination hearing aid and tinnitus therapy device. Ear Hear. 36, 42–52. doi: 10.1097/AUD.0000000000000093
Henry, J. A., Roberts, L. E., Ellingson, R. M., and Thielman, E. J. (2013). Computer-automated tinnitus assessment: noise-band matching, maskability, and residual inhibition. J. Am. Acad. Audiol. 24, 486–504. doi: 10.3766/jaaa.24.6.5
Henry, J. A., Schechter, M. A., Zaugg, T. L., Griest, S., Jastreboff, P. J., Vernon, J. A., et al. (2006). Outcomes of clinical trial: tinnitus masking versus tinnitus retraining therapy. J. Am. Acad. Audiol. 17, 104–132. doi: 10.3766/jaaa.17.2.4
Herraiz, C., Hernandez, F. J., Toledano, A., and Aparicio, J. M. (2007). Tinnitus retraining therapy: prognosis factors. Am. J. Otol. 28, 225–229. doi: 10.1016/j.amjoto.2006.09.004
Herzfeld, M., Enza, C., and Sweetow, R. (2014). Clinical trial on the effectiveness of widex zen therapy for tinnitus. Hear. Rev. 21, 24–29.
Hoare, D. J., Adjamian, P., Sereda, M., and Hall, D. A. (2013a). Recent technological advances in sound-based approaches to tinnitus treatment: a review of efficacy considered against putative physiological mechanisms. Noise Health 15, 107. doi: 10.4103/1463-1741.110292
Hoare, D. J., Edmondson-Jones, M., Gander, P. E., and Hall, D. A. (2014a). Agreement and reliability of tinnitus loudness matching and pitch likeness rating. PLoS ONE 9:e114553. doi: 10.1371/journal.pone.0114553
Hoare, D. J., Gander, P. E., Collins, L., Smith, S., and Hall, D. A. (2012). Management of tinnitus in english nhs audiology departments: an evaluation of current practice. J. Eval. Clin. Prac. 18, 326–334. doi: 10.1111/j.1365-2753.2010.01566.x
Hoare, D. J., Pierzycki, R. H., Thomas, H., McAlpine, D., and Hall, D. A. (2013b). Evaluation of the acoustic coordinated reset (CR ®) neuromodulation therapy for tinnitus: study protocol for a double-blind randomized placebo-controlled trial. Trials 14:207. doi: 10.1186/1745-6215-14-207
Hoare, D. J., Searchfield, G. D., El Refaie, A., and Henry, J. A. (2014b). Sound therapy for tinnitus management: practicable options. J. Am. Acad. Audiol. 25, 62–75. doi: 10.3766/jaaa.25.1.5
Hoare, D. J., Stacey, P. C., and Hall, D. A. (2010). The efficacy of auditory perceptual training for tinnitus: a systematic review. Annals. Behav. Med. 40, 313–324. doi: 10.1007/s12160-010-9213-5
Hoare, D. J., Whitham, D., Henry, J. A., and Shorter, G. W. (2015). Neuromodulation (desynchronisation) for tinnitus in adults. Cochrane Database Syst. Rev. 6:CD011760. doi: 10.1002/14651858.CD011760
Hobson, J., Chisholm, E., and El Refaie, A. (2012). Sound therapy (masking) in the management of tinnitus in adults. Cochrane Database Syst. Rev. 11:CD006371. doi: 10.1002/14651858.CD006371.pub3
Huang, C.-Y., Wu, J.-L., Cheng, C.-C., Sher, Y.-J., and Chung, K.-C. (2006). Evaluation of the mixing point in tinnitus sound therapy by a psychoacoustic matching protocol with a digital tinnitus evaluation system. Orl 68, 110–114. doi: 10.1159/000091213
Hutter, E., Grapp, M., Argstatter, H., and Bolay, H. V. (2014). Music therapy for chronic tinnitus: variability of tinnitus pitch in the course of therapy. J. Am. Acad. Audiol. 25, 335–342. doi: 10.3766/jaaa.25.4.5
Ito, M., Soma, K., and Ando, R. (2009). Association between tinnitus retraining therapy and a tinnitus control instrument. Auris Nasus Larynx 36, 536–540. doi: 10.1016/j.anl.2009.01.003
Jalilvand, H., Pourbakht, A., and Haghani, H. (2015). Hearing aid or tinnitus masker: which one is the best treatment for blast-induced tinnitus? The results of a long-term study on 974 patients. Audiol. Neurotol. 20, 195–201. doi: 10.1159/000377617
Jastreboff, M. M. (2007). Sound therapies for tinnitus management. Prog. Brain Res. 166, 435–440. doi: 10.1016/S0079-6123(07)66042-7
Jastreboff, P. (2015). 25 Years of tinnitus retraining therapy. HNO 63, 307–311. doi: 10.1007/s00106-014-2979-1
Jastreboff, P. J. (2000). “Tinnitus habituation therapy (THT) and tinnitus retraining therapy (TRT),” in Tinnitus Handbook, ed R. Tyler (San Diego, CA: Singular Publishing Group), 357–376.
Jastreboff, P. J. (2011). “Tinnitus retraining therapy,” in Textbook of Tinnitus, eds A. R. Møller, B. Langguth, D. DeRidder, and T. Kleinjung (New York, NY: Springer-Verlag), 575–596.
Jastreboff, P., and Jastreboff, M. M. (2006). Tinnitus retraining therapy: a different view on tinnitus. Orl 68, 23–30. doi: 10.1159/000090487
Jepsen, K., Sanders, M., Searchfield, G., and Kobayashi, K. (2010). Perceptual training of tinnitus. proceedings of ‘tinnitus discovery’: Asia-Pacific tinnitus symposium, 11-12 Sept 2009. NZ. Med. J. 123, 141–153.
Kidd, G. Jr., Arbogast, T. L., Mason, C. R., and Walsh, M. (2002). Informational masking in listeners with sensorineural hearing loss. JARO 3, 107–119. doi: 10.1007/s101620010095
Kidd, G. J., Mason, C. R., Rothla, T. L., and Deliwala, P. S. (1998). Release from masking due to spatial separation of sources in the identification of nonspeech auditory patterns. J. Acous. Soc. Am. 104, 422–431. doi: 10.1121/1.423246
Kim, B. J., Chung, S. W., Jung, J. Y., and Suh, M. W. (2014). Effect of different sounds on the treatment outcome of tinnitus retraining therapy. Clin. Exp. Otorhinolaryn 7, 87–93. doi: 10.3342/ceo.2014.7.2.87
Langguth, B., Goodey, R., Azevedo, A., Bjorne, A., Cacace, A., Crocetti, A., et al. (2007). Consensus for tinnitus patient assessment and treatment outcome measurement: tinnitus research initiative meeting, regensburg, july 2006. Prog. Brain Res. 166, 525–536. doi: 10.1016/S0079-6123(07)66050-6
Li, S.-A., Bao, L., and Chrostowski, M. (2016). Investigating the effects of a personalized, spectrally altered music-based sound therapy on treating tinnitus: a blinded, randomized controlled trial. Audiol. Neurotol. 21, 296–304. doi: 10.1159/000450745
Lugli, M., Romani, R., Ponzi, S., Bacciu, S., and Parmigiani, S. (2009). The windowed sound therapy: a new empirical approach for an effective personalized treatment of tinnitus. Int. Tin. J. 15, 51–61.
Lunner, T., Rudner, M., and Ronnberg, J. (2009). Cognition and hearing aids. Scand. J. Psychol. 50, 395–403. doi: 10.1111/j.1467-9450.2009.00742.x
Mahboubi, H., Ziai, K., and Djalilian, H. R. (2012). Customized web-based sound therapy for tinnitus. Int. Tin. J. 17, 26–30.
Martinez-Devesa, P., Waddell, A., and Theodoulou, M. (2006). Cognitive behavioural therapy for tinnitus. Cochrane Database Syst. Rev. 1:1. doi: 10.1002/14651858.CD005233.pub3
Mazurek, B., Fischer, F., Haupt, H., Georgiewa, P., Reisshauer, A., and Klapp, B. F. (2006). A modified version of tinnitus retraining therapy: observing long-term outcome and predictors. Audiol. Neurotol. 11, 276–286. doi: 10.1159/000093526
Mckenna, L., and Irwin, R. (2008). Sound therapy for tinnitus–sacred cow or idol worship? an investigation of the evidence. Audiol. Med. 6, 16–24. doi: 10.1080/16513860801899389
McNeill, C., Távora-Vieira, D., Alnafjan, F., Searchfield, G. D., and Welch, D. (2012). Tinnitus pitch, masking, and the effectiveness of hearing aids for tinnitus therapy. Int. J. Audiol. 51, 914–919. doi: 10.3109/14992027.2012.721934
Meeus, O., Heyndrickx, K., Lambrechts, P., De Ridder, D., and Van de Heyning, P. (2010). Phase-shift treatment for tinnitus of cochlear origin. Eur. Arch. Otorhinolaryngol. 267, 881–888. doi: 10.1007/s00405-009-1145-y
Meikle, M. B., Henry, J. A., Griest, S. E., Stewart, B. J., Abrams, H. B., McArdle, R., et al. (2012). The tinnitus functional index: development of a new clinical measure for chronic, intrusive tinnitus. Ear Hear. 32, 153–176. doi: 10.1097/AUD.0b013e31822f67c0
Michie, S., Miles, J., and Weinman, J. (2003). Patient-centredness in chronic illness: what is it and does it matter? Patient Ed. Couns. 51, 197–206. doi: 10.1016/S0738-3991(02)00194-5
Miles, A., and Loughlin, M. (2011). Models in the balance: evidence-based medicine versus evidence-informed individualized care. J. Eval. Clin. Prac. 17, 531–536. doi: 10.1111/j.1365-2753.2011.01713.x
Myers, P. J., Griest, S., Kaelin, C., Legro, M. W., Schmidt, C. J., Zaugg, T., et al. (2014). Development of a progressive audiologic tinnitus management program for veterans with tinnitus. J. Rehab. Res. Dev. 51:609. doi: 10.1682/JRRD.2013.08.0189
Newman, C. W., Sandridge, S. A., Meit, S. S., and Cherian, N. (2008). Strategies for managing patients with tinnitus: a clinical pathway model. Sem. Hear. 29, 300–309. doi: 10.1055/s-0028-1082035
Norena, A. J. (2015). Revisiting the cochlear and central mechanisms of tinnitus and therapeutic approaches. Audiol. Neurootol. 20(Suppl. 1), 53–59. doi: 10.1159/000380749
Oishi, N., Shinden, S., Kanzaki, S., Saito, H., Inoue, Y., and Ogawa, K. (2013). Effects of tinnitus retraining therapy involving monaural noise generators. Eur. Arch. Oto. Rhino. Laryngol. 270, 443–448. doi: 10.1007/s00405-012-1951-5
Ostermann, K., Lurquin, P., Horoi, M., Cotton, P., Herve, V., and Thill, M. P. (2016). Somatic tinnitus prevalence and treatment with tinnitus retraining therapy. B-ENT 12, 59–65.
Oz, I., Arslan, F., Hizal, E., Erbek, S. H., Eryaman, E., Senkal, O. A., et al. (2013). Effectiveness of the combined hearing and masking devices on the severity and perception of tinnitus: a randomized, controlled, double-blind study. ORL J. Otorhinolaryngol. Relat. Spec. 75, 211–220. doi: 10.1159/000349979
Parra, P. C. (2015). Tinnitus: mechanisms, measures and sound treatments. Loquens 2:24. doi: 10.3989/loquens.2015.024
Pedemonte, M., Drexler, D., Rodio, S., Geisinger, D., Bianco, A., Pol-Fernandes, D., et al. (2010). Tinnitus treatment with sound stimulation during sleep. Inter. Tin. J. 16, 37–43.
Peltier, E., Peltier, C., Tahar, S., Alliot-Lugaz, E., and Cazals, Y. (2012). Long-term tinnitus suppression with linear octave frequency transposition hearing AIDS. PLoS ONE 7:e51915. doi: 10.1371/journal.pone.0051915
Reavis, K. M., Chang, J. E., and Zeng, F.-G. (2010). Patterned sound therapy for the treatment of tinnitus. Hear. J. 63, 21–22. doi: 10.1097/01.HJ.0000390817.79500.ed
Reavis, K. M., Rothholtz, V. S., Tang, Q., Carroll, J. A., Djalilian, H., and Zeng, F.-G. (2012). Temporary suppression of tinnitus by modulated sounds. JARO 13, 561–571. doi: 10.1007/s10162-012-0331-6
Roberts, L. E., and Bosnyak, D. J. (2011). “Auditory training in tinnitus,” in Textbook of Tinnitus, eds A. R. Møller, B. Langguth, D. DeRidder, and T. Kleinjung (New York, NY: Springer-Verlag), 563–573.
Sand, P., Langguth, B., Kleinjung, T., and Eichhammer, P. (2007). Genetics of chronic tinnitus. Prog. Brain Res. 166, 159–168. doi: 10.1016/S0079-6123(07)66014-2
Schaette, R., Konig, O., Hornig, D., Gross, M., and Kempter, R. (2010). Acoustic stimulation treatments against tinnitus could be most effective when tinnitus pitch is within the stimulated frequency range. Hear. Res. 269, 95–101. doi: 10.1016/j.heares.2010.06.022
Schleidgen, S., Klingler, C., Bertram, T., Rogowski, W. H., and Marckmann, G. (2013). What is personalized medicine: sharpening a vague term based on a systematic literature review. BMC Med. Ethics 14:55. doi: 10.1186/1472-6939-14-55
Searchfield, G. D. (2006). “Hearing aids and tinnitus,” in Tinnitus Protocols, ed R. Tyler (New York, NY: Thieme), 161–175.
Searchfield, G. D. (2014). Tinnitus what and where: an ecological framework. Front. Neurol. 5:271. doi: 10.3389/fneur.2014.00271
Searchfield, G. D. (2015). “Hearing aids for tinnitus,” in Tinnitus: Clinical and Research Perspectives, eds D. Baguley and M. Fagelson (San Diego, CA: Plural Publishing), 197–212.
Searchfield, G. D. (2016). “Tinnitus sound therapy options,” in The Consumer Handbook on Tinnitus, 2nd Edn. ed R. Tyler (Sedona, AZ: Auricle Ink Publishers), 179–195.
Searchfield, G. D., Kaur, M., and Martin, W. H. (2010). Hearing aids as an adjunct to counseling: tinnitus patients who choose amplification do better than those that don't. Int. J. Audiol. 49, 574–579. doi: 10.3109/14992021003777267
Searchfield, G. D., Kobayashi, K., Hodgson, S.-A., Hodgson, C., Tevoitdale, H., and Irving, S. (2016). Spatial masking: development and testing of a new tinnitus assistive technology. Assist Tech 28, 115–125. doi: 10.1080/10400435.2015.1110214
Searchfield, G. D., Kobayashi, K., and Sanders, M. (2012). An adaptation level theory of tinnitus audibility. Front. Syst. Neurosci. 6:46. doi: 10.3389/fnsys.2012.00046
Searchfield, G. D., Magnusson, J., Shakes, G., Biesinger, E., and Kong, O. (2011). “Counseling and psycho-education for tinnitus management,” in Textbook of Tinnitus, eds A. R. Møller, B. Langguth, D. DeRidder, and T. Kleinjung (New York, NY: Springer-Verlag), 535–556.
Sereda, M., Davies, J., and Hall, D. A. (2016). Pre-market version of a commercially available hearing instrument with a tinnitus sound generator: feasibility of evaluation in a clinical trial. Int. J. Audiol. 56, 286–294. doi: 10.1080/14992027.2016.1254822
Sereda, M., Hall, D. A., Bosnyak, D. J., Edmondson-Jones, M., Roberts, L. E., Adjamian, P., et al. (2011). Re-examining the relationship between audiometric profile and tinnitus pitch. Int. J. Audiol. 50, 303–312. doi: 10.3109/14992027.2010.551221
Sereda, M., Hoare, D. J., Nicholson, R., Smith, S., and Hall, D. A. (2015). Consensus on hearing aid candidature and fitting for mild hearing loss, with and without tinnitus: delphi review. Ear Hear. 36:417. doi: 10.1097/AUD.0000000000000140
Serquera, J., Schlee, W., Pryss, R., Neff, P., and Langguth, B. (2015). “Music technology for tinnitus treatment within tinnet,” in Audio Engineering Society Conference: 58th International Conference: Music Induced Hearing Disorders: Audio Engineering Society (Aalborg).
Shekhawat, G. S., Searchfield, G. D., Kobayashi, K., and Stinear, C. M. (2013a). Prescription of hearing-aid output for tinnitus relief. Int. J. Audiol. 52, 617–625. doi: 10.3109/14992027.2013.799787
Shekhawat, G. S., Searchfield, G. D., and Stinear, C. M. (2013b). Role of hearing aids in tinnitus intervention: a scoping review. J. Am. Acad. Audiol. 24, 747–762. doi: 10.3766/jaaa.24.8.11
Shekhawat, G. S., Searchfield, G. D., and Stinear, C. M. (2014). Randomized trial of transcranial direct current stimulation and hearing aids for tinnitus management. Neurorehabil. Neural Repair 28, 410–419. doi: 10.1177/1545968313508655
Smith, S. L., and Fagelson, M. (2011). Development of the self-efficacy for tinnitus management questionnaire. J. Am. Acad. Audiol. 22, 424–440. doi: 10.3766/jaaa.22.7.4
Spiegel, D. P., Linford, T., Thompson, B., Petoe, M. A., Kobayashi, K., Stinear, C. M., et al. (2015). Multisensory attention training for treatment of tinnitus. Sci. Rep. 5:10802. doi: 10.1038/srep10802
Stouffer, J. L., and Tyler, R. S. (1990). Characterization of tinnitus by tinnitus patients. J. Speech Hear. Dis. 55, 439–453. doi: 10.1044/jshd.5503.439
Suzuki, B., Suzuki, F. A., Yonamine, F. A., Onishi, F. K., Penido, E. T., and Oliveira, N. (2016). Effectiveness of sound therapy in patients with tinnitus resistant to previous treatments: importance of adjustments. Brazil J. Otorhinolaryngol. 82, 297–303. doi: 10.1016/j.bjorl.2015.05.009
Tang, H. Y., Harms, V., Speck, S. M., Vezeau, T., and Jesurum, J. T. (2009). Effects of audio relaxation programs for blood pressure reduction in older adults. Eur. J. Cardiovasc. Nurs. 8, 329–336. doi: 10.1016/j.ejcnurse.2009.06.001
Távora-Vieira, D., Eikelboom, R. H., and Miller, S. (2011). Neuromonics tinnitus treatment for patients with significant level of hearing loss: an adaptation of the protocol. In. J. Audiol. 50, 881–886. doi: 10.3109/14992027.2011.606286
Teismann, H., Okamoto, H., and Pantev, C. (2011). Short and intense tailor-made notched music training against tinnitus: the tinnitus frequency matters. PLoS ONE 6:e24685. doi: 10.1371/journal.pone.0024685
Tellegen, A. (1982). Brief Manual for the Multidimensional Personality Questionnaire. Minneapolis: University of Minnesota Minneapolis, 1031–1010.
Tutton, R. (2012). Personalizing medicine: futures present and past. Soc. Sci. Med. 75, 1721–1728. doi: 10.1016/j.socscimed.2012.07.031
Tyler, R. (2000). “Psychoacoustical measurement,” in Handbook of Tinnitus, ed R. Tyler (San Diego, CA: Singular Publications), 149–180.
Tyler, R., Ji, H., Perreau, A., Witt, S., Noble, W., and Coelho, C. (2014). Development and validation of the tinnitus primary function questionnaire. Am. J. Audiol. 23, 260–272. doi: 10.1044/2014_AJA-13-0014
Tyler, R. S. (2012). Patient preferences and willingness to pay for tinnitus treatments. J. Am. Acad. Audiol. 23, 115–125. doi: 10.3766/jaaa.23.2.6
Tyler, R. S., Coelho, C., and Noble, W. (2006). Tinnitus: standard of care, personality differences, genetic factors. ORL 68, 14–22. doi: 10.1159/000090486
Tyler, R. S., Gogel, S. A., and Gehringer, A. K. (2007). Tinnitus activities treatment. Prog. Brain Res. 166, 425–434. doi: 10.1016/S0079-6123(07)66041-5
Tyler, R. S., Keiner, A. J., Walker, K., Deshpande, A. K., Witt, S., Killian, M., et al. (2015). A series of case studies of tinnitus suppression with mixed background stimuli in a cochlear implant. Am. J. Audiol. 24, 398–410. doi: 10.1044/2015_AJA-15-0005
Tyler, R. S., Noble, W., Coelho, C. B., and Ji, H. (2012). Tinnitus retraining therapy: mixing point and total masking are equally effective. Ear. Hear. 33, 588–594. doi: 10.1097/AUD.0b013e31824f2a6e
Uriz, A. J., Agüero, P. D., Tulli, J. C., Moreira, J. C., González, E. L., Moscardi, G., et al. (2013). “A development and implementation of a tinnitus treatment method,” in Journal of Physics: Conference Series, Vol. 477 (Tucumán: IOP Publishing), 012026.
Vanneste, S., van Dongen, M., De Vree, B., Hiseni, S., van der Velden, E., Strydis, C., et al. (2013). Does enriched acoustic environment in humans abolish chronic tinnitus clinically and electrophysiologically? A double blind placebo controlled study. Hear. Res. 296, 141–148. doi: 10.1016/j.heares.2012.10.003
Vermeire, K., Heyndrickx, K., De Ridder, D., and Van de Heyning, P. (2007). Phase-shift tinnitus treatment: an open prospective clinical trial. B-ENT 3(Suppl. 7), 65–69.
Viirre, E. (2010). Customized Sound Therapy (CST): a therapy for low-level tinnitus. Hear. J. 63, 30–34. doi: 10.1097/01.HJ.0000390819.17619.2c
Wazen, J. J., Daugherty, J., Pinsky, K., Newman, C. W., Sandridge, S., Battista, R., et al. (2011). Evaluation of a customized acoustical stimulus system in the treatment of chronic tinnitus. Otol. Neurotol. 32, 710–716. doi: 10.1097/MAO.0b013e318217d459
Welch, D., and Dawes, P. J. (2008). Personality and perception of tinnitus. Ear Hear. 29, 684–692. doi: 10.1097/AUD.0b013e318177d9ac
Williams, M., Hauptmann, C., and Patel, N. (2015). Acoustic CR neuromodulation therapy for subjective tonal tinnitus: a review of clinical outcomes in an independent audiology practice setting. Front. Neurol. 6:54. doi: 10.3389/fneur.2015.00054
Wise, K., Kobayashi, K., and Searchfield, G. (2015). Feasibility study of a game integrating assessment and therapy of tinnitus. J. Neurosci. Methods 249, 1–7. doi: 10.1016/j.jneumeth.2015.04.002
Wise, K., Kobayashi, K., Magnusson, J., Welch, D., and Searchfield, G. D. (2016). Randomized controlled trial of a perceptual training game for tinnitus therapy. Games Heal. J. 5, 141–149. doi: 10.1089/g4h.2015.0068
Zarenoe, R., Hallgren, M., Andersson, G., and Ledin, T. (2017). Working memory, sleep, and hearing problems in patients with tinnitus and hearing loss fitted with hearing aids. J. Am. Acad. Audiol. 28, 141–151. doi: 10.3766/jaaa.16023
Keywords: tinnitus, treatment, therapy, review, person-centered
Citation: Searchfield GD, Durai M and Linford T (2017) A State-of-the-Art Review: Personalization of Tinnitus Sound Therapy. Front. Psychol. 8:1599. doi: 10.3389/fpsyg.2017.01599
Received: 29 April 2017; Accepted: 31 August 2017;
Published: 20 September 2017.
Edited by:
Nuno Conceicao, Universidade de Lisboa, PortugalReviewed by:
Rüdiger Christoph Pryss, University of Ulm, GermanyJose Antonio Lopez-Escamez, Hospital Universitario Virgen de las Nieves, Spain
Copyright © 2017 Searchfield, Durai and Linford. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Grant D. Searchfield, Zy5zZWFyY2hmaWVsZEBhdWNrbGFuZC5hYy5ueg==