 Lorena Gutiérrez Hermoso
Lorena Gutiérrez Hermoso Lilian Velasco Furlong
Lilian Velasco Furlong Sofía Sánchez-Román
Sofía Sánchez-Román Lorena Salas Costumero1
Lorena Salas Costumero1- 1Department of Psychology, Universidad Rey Juan Carlos, Madrid, Spain
- 2Department of Neurology and Psychiatry, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán, Mexico City, Mexico
Breast cancer is a disease that is difficult to face and that often hinders body acceptance. Body changes due to surgery can be very emotionally challenging for those who experience them. The aim of this study is to explore the differences on body image and psychological adjustment on women with breast cancer with high and low alexithymia according to the type of surgery. In this cross-sectional study, 119 women diagnosed with breast cancer (stages I, II, and III) were evaluated with different self-report questionnaires. Afterward, patients were divided into two groups (high and low levels of alexithymia) to analyze dependent variables (body image and psychological adjustment) according to the type of surgery (radical mastectomy or breast conserving therapy). The results of the General Linear Model suggest that when patients show high alexithymia combined with having undergone a radical mastectomy, they show higher levels of Hopelessness. Furthermore, in patients with high alexithymia, higher scores of maladaptive coping styles and greater distortion of body image were found. Alexithymia seems to play an important role in the way in which women cope with their disease, especially in those with radical mastectomy.
Introduction
The high incidence of breast cancer worldwide has led the medical community to consider this disease as a serious public health problem. Epidemiological data shows more than 2,00,000 new cases in the coming years, and the estimate indicates more than 42,000 deaths due to the disease (American Cancer Society, 2019).
Surgical treatment is one of the options that can be offered today to this group of patients. Radical mastectomy (MSTR) is the removal of the entire breast, generally including the nipple. Although the survival rate can reach up to 40%, MSTR is associated with a high probability of lymphedema in the future, in addition to deformities in the affected chest, arm or shoulder (Turkington and Krag, 2005). Breast conserving therapy (BCT) is a type of surgery performed by removing the tumor and surrounding tissue to prevent its growth, and it is usually followed by adjuvant radiotherapy sessions as a substitute for mastectomy. MSTR surgery is the most commonly used method to remove the affected nodes (Hoover et al., 2011). However, many women’s concerns for body image and femininity lead them to opt for BCT in order to preserve the shape of the affected breast as much as possible (Puts et al., 2015; Gu et al., 2018). BCT surgery has been shown to provide greater psychological benefits in most patients diagnosed with early stage invasive breast cancer (I, II or III), as it impacts their body image differently. Body image is understood as the subjective representation of physical appearance and a source of satisfaction or dissatisfaction when this perception does not match with social ideals (Parker et al., 2007), which is why this construct influences self-esteem (Sarwer and Cash, 2008) and sexuality (Fobair and Spiegel, 2009). The diagnosis of breast cancer is likely to increase the probability of distorting body image. However, surgery is one of the factors responsible for the negative body changes that generally cause failed attempts to preserve the physical image (e.g., breast reconstruction) (Sheehan et al., 2007; Zimmerman et al., 2010; Collins et al., 2011) and anxiety related to the new physical condition (Montebarocci et al., 2007; Collins et al., 2011).
A large part of this research was dedicated to studying the relationship between body image and adaptation to the disease in the two types of surgery. Some studies have found that those who have undergone a BCT show an adaptive coping style and the perception they maintain of their own image is more adjusted (Al-Ghazal et al., 2000). Consequently, the quality of life of patients who undergo conservative surgery remains higher compared to those who undergo MSTR (Hoover et al., 2011; Ursaru et al., 2014). However, the results are still controversial, as there are other studies that support the idea that both MSTR and BCT promote maladaptiveness equally in patients (Parker et al., 2007).
Emotional adaptation is intimately linked with coping strategies (Velasco et al., 2020). The emotional distress experienced after breast cancer surgery can be understood by the difference between the ideal physical state of oneself (e.g., good conditioning and physical attractiveness) and the real image (Helms et al., 2008). Premature death or the sudden changes that may occur in their lives due to cancer are usually the type of negative thoughts that increase an altered self-assessment of body image and lead to dissatisfaction with themselves (Przezdziecki et al., 2013). In this context, low adaptation is defined by manifested anxiety and depression (Gregorowitsch et al., 2018) as a consequence of stress caused by personal insecurity, which explains why strategies focused on cognitive avoidance, helplessness or persistent worries tend to be the most common to deal with the disease. These coping styles increase the incidence of physical symptoms such as pain, fatigue, insomnia or loss of limb functionality (specifically, in the arm or armpit of the affected breast), which in turn, influence the probability of recurrence (Kvillemo and Bränström, 2014; Ahadzadeh and Sharif, 2018).
While there is strong evidence that emotional involvement alters overall coping with breast cancer (Parker et al., 2007), less is known about how some constructs that define more stable personality traits can influence efforts dedicated to alleviating the perceived stress associated with the type of surgery and the distortion of the body image of the patients. It is important to understand that the problems that arise in adapting to the continuous changes that the disease causes usually stem from difficulties at the emotional level (Kojima, 2012). Alexithymia, defined as the inability to recognize and express one’s emotional states and those of others, leads to numbness in affective regulation and causes an externally oriented thought pattern (Taylor and Bagby, 2012). In general population, these emotional difficulties are more frequent in people who frequently experience negative emotions than in those who experience positive emotions (De Berardis et al., 2017). Consequently, the appearance of psychiatric problems such as anxiety and depression are highly probable (Carano et al., 2012; De Berardis et al., 2017; Serafini et al., 2020) and, therefore, increases the risk of suicide (De Berardis et al., 2020). In this context, alexithymia has become a factor of special interest as it is considered a risk factor in those people who have previously attempted suicide (Hintikka et al., 2004; Huen et al., 2015). In an oncology population, the studies carried out by Luminet et al. (2007) and De Vries et al. (2012) have confirmed that alexithymia is stable over time and that it increases in the presence of anxious and depressive states. Furthermore, it seems to be related to the way in which patients with cancer and other diseases describe their experience of pain, as well as to maladaptive coping and unhealthy behaviors such as a sedentary lifestyle (Porcelli et al., 2007; Landstra et al., 2013). A study led by Kim et al. (2013) point to depressive symptoms, anxiety and advanced stage of cancer as the factors that influence suicidal thoughts 1 year after surgery. One of the explanations provided by the authors focuses on the difficulties suffered by patients as a result of the body changes caused by breast surgery. The lack of acceptance toward the disease and the physical rejection favor that suicide is considered as an alternative solution to the problems they are experiencing. In relation to body image, some studies have indicated body dissatisfaction as a predictor of suicidal ideation in other clinical populations (Brausch and Decker, 2014; Perkins and Brausch, 2019). However, more research is needed to explain alexithymia’s influence as a personality factor that damages body image and promotes the use of maladaptive coping strategies as possible risk factors for women with breast cancer (Saita et al., 2015). As shown, different studies have analyzed body image and psychological adjustment in patients with breast cancer. But despite the variables studied in this population, little is known about their relation to distinct types of surgery in patients with breast cancer in early phases (stages I, II or III). Going one step further, by addressing alexithymia as a relevant variable in this disease, the aim of the present study is to explore the differences between body image and psychological adjustment on women with breast cancer with high and low alexithymia according to the surgery. We addressed this objective by comparing two groups of patients depending on the surgery (MSTR vs. BCT) and on the level of alexithymia (high alexithymia vs. low alexithymia). Basing ourselves on current literature, we hypothesized that women undergoing MSTR will present a more distorted body image and use maladaptive coping strategies in function of alexithymia levels compared to women undergoing BCT.
Materials and Methods
Participants
A total of one hundred and thirty-nine women entered as study participants, but the response rate was 85.61%. Women that did not completely fill in all the questionnaires were excluded, leading to a final sample of one hundred and nineteen women, aged 18 years and older. Participants were diagnosed with invasive breast cancer in early stages (stage I, II or III) and they underwent surgery (MSTR or BCT). Patients were recruited from the National Institute of Medical Sciences and Nutrition Salvador Zubirán (México) and Hospital Universitario de Móstoles (Spain). This study was approved by the Committee on Ethics of the collaborating institutions and data collection was carried out between October 2015 and July 2019. Then, the researchers contacted patients interested in participating in order to perform an individual evaluation in person. The inclusion criteria established for the study were: (a) being over 18 years old, (b) having a diagnosis of invasive breast cancer in stages I to III, (c) having undergone surgery for the removal or reduction of the malignant tumor, and (d) signing the informed consent form. The exclusion criteria consisted of: (a) presenting a diagnosis of invasive breast cancer in the metastatic phase, (b) presenting a comorbid diagnosis with a mental illness, mental retardation or cognitive disorder, and (c) presenting any disability that prevented them from completing the evaluation questionnaires. This information was confirmed with the medical record.
The average age for participants was 53.16 (SD = 10.30). Ninety women were Mexican (75.6%) and twenty-nine were Spanish (24.4%). Sixty-six were married or living with a partner (55.4%), 13 were separated or divorced (10.9%), and 8 were widowed (6.7%). One participant had no educational studies (0.8%), 24 participants had primary studies (20.1%), 37 completed high school or secondary studies (31.1%) and 57 women had university level education (48%). Forty-three women were housewives (36.4%), 49 women were working (41.4%) and 27 women were unemployed (22.2%). No significant differences were found according to nationality and stage of diagnosis regarding the study variables (alexithymia, body image, and coping strategies).
With respect to the clinical variables, participants reported an average time of diagnosis at 21.62 months (SD = 3.07). This means that, at the time of the evaluation, there were some patients who were in the process of the disease and others who had been recently diagnosed. On the other hand, there are also women who were in the disease-free phase (being currently treated with hormone therapy for 5 years for relapse prevention). Regarding the stage of disease, forty-eight women were in stage II (40.3%), thirty-nine women in stage I (32.8%) and thirty-two women in stage III (26.9%). Radical mastectomy was the most widely used surgery (n = 71, 59.7%) followed by BCT (n = 48, 40.3%). Finally, hormonal treatment was the most common form of treatment (n = 55, 46.2%), following chemotherapy (n = 50, 42%) and radiotherapy (n = 14, 11.8%).
Procedure
Participants were recruited by physicians from the reference Oncology units based on inclusion and exclusion criteria, and the researchers then called to make an appointment at dedicated facilities for individual evaluations. After a brief interview to collect data about medical history, the participants completed the questionnaires described below.
Measures
Sociodemographic and Clinical Data
An “ad hoc” questionnaire was used including age, marital status, educational level, and working status as socio-demographic variables, and time since diagnosis, stage of disease, type of surgery and medical treatment as clinical variables.
Alexithymia
The Spanish version of the Toronto Alexithymia Scale (TAS-20) was used (Martínez-Sánchez, 1996). It is composed of 20 items with a Likert-type response, which shows the degree of agreement or disagreement with each statement. Scores range between 20 and 100. Equal or higher scores than 61 indicates a high level of emotional difficulty (Páez et al., 1999). In addition to evaluating the level of global alexithymia, it also provides information on three factors within the construct: difficulty in identifying and discriminating emotional cues, difficulty in verbal expression of emotions and feelings, and externally oriented thinking. Its internal reliability is adequate and good for most of the translations (Martínez-Sánchez, 1996) and the stability and replicability of its factor structure has been confirmed in both clinical and non-clinical samples (Bagby et al., 1994; Páez et al., 1999). According to previous research, we used the global score to explore the role of alexithymia as a stable and characteristic construct of personality in the participants (Baudic et al., 2016; Marrazzo et al., 2016). For this scale, Cronbach alpha was 0.84.
Body Image
The Hopwood Body Image Scale (Hopwood et al., 2007) was used. This self-report does not have a consolidated validation in the Spanish-speaking population, but previous reviews confirmed that the instrument has good validity for the population with breast cancer (Sebastián et al., 2007). High scores indicate a high distortion in body image. According to Rosenberg (1965), knowing the relationship that one feels with one’s physical appearance is part of the self-concept (set of judgments and evaluations of oneself regarding one’s own behavior, abilities or appearance) and self-esteem, which are the set of positive or negative feelings that we have about ourselves. The instrument has a high internal consistency. In our sample, we found α = 0.89.
Psychological Adjustment
To identify the coping strategies, the Spanish version of Mental Adjustment to Cancer Scale (MAC) was administered (Ferrero et al., 1994). Coping is conceptualized as the set of personal resources to face the demands of one’s environment, in this case, the demands related to the disease (Lazarus and Folkman, 1984). The factor structure of the scale includes five coping strategies: fighting spirit, hopelessness/helplessness, anxious preoccupation, fatalism, and avoidance. People who maintain a coping style based on the spirit of struggle as a strategy, perceive the disease as a challenge that benefits them in adopting the experience as an opportunity for personal growth. The coping style centered on the hopelessness/helplessness strategy is defined by high levels of anxiety and depression along with low situational control, which causes a person to make decisions with a lack of regard for their health. Anxious preoccupation is a strategy based on high levels of anxiety and recurring concerns regarding the diagnosis and any demands related to the treatment to follow. People who tend to use a fatalism-based coping strategy often give up when faced with challenging circumstances. Finally, the avoidance-based coping style focuses on the tendency to seek peace of mind without getting too informed about the disease. In some clinical studies with non-Hispanic populations, they have confirmed that the use of maladaptive strategies such as hopelessness and anxious preoccupation are effective indicators of the degree of maladjustment and psychological distress (Grassi et al., 2005). According to the original version of the instrument, high scores indicate greater use of these strategies. It has an internal consistency, with an alpha of Cronbach ranging between 0.65 and 0.78. In the present study, the alpha of Cronbach ranged from 0.70 to 0.78.
Statistics
Analyses were performed using the SPSS 22 Statistics Package (Armonk, NY, United States). The descriptive analyses of the total sample were calculated according to the sociodemographic and clinical variables. Internal consistency analysis was performed according to Cronbach’s alpha coefficient. Comparisons between means were performed with Student’s t-test in both groups (high and low alexithymia and both surgeries). The objective of this study was to determine the effects of the level of alexithymia and the type of surgery on body image and coping strategies, as well as the interaction between the level of alexithymia∗ and type of surgery. To do this, we conducted six 2 × 2 factorial design ANOVAs with the between-group factor condition (high or low alexithymia) and type of surgery (MSTR or BCT), with one for each dependent variable (body image, fighting spirit, helplessness, anxious preoccupation, fatalism, and avoidance).
Results
Differences Between Alexithymia and Surgery Groups on Dependent Variables
As shown in Table 1, according to alexithymia levels, there are significant differences on body image scores and the following maladaptive coping strategies: helplessness, anxious preoccupation, fatalism, and avoidance. The distortion on body image is greater in the group of women with high alexithymia compared to women with low alexithymia (t = −4.08, gl = 63.87). Likewise, the use of maladaptive coping strategies is more pronounced in women with high alexithymia compared to women with low alexithymia. Specifically, helplessness is greater in the group of high alexithymia compared to women with low alexithymia (t = −5.05, gl = 54.95), anxious preoccupation is highest in women with high alexithymia compared to low alexithymia group (t = −2.17, gl = 100.53). Fatalistic perception is again more accentuated in high alexithymia group compared to the group with low alexithymia (t = −2.60, gl = 104.73) and, finally, avoidance is higher in women with high alexithymia compared to women with low alexithymia (t = −2.86, gl = 66.67).
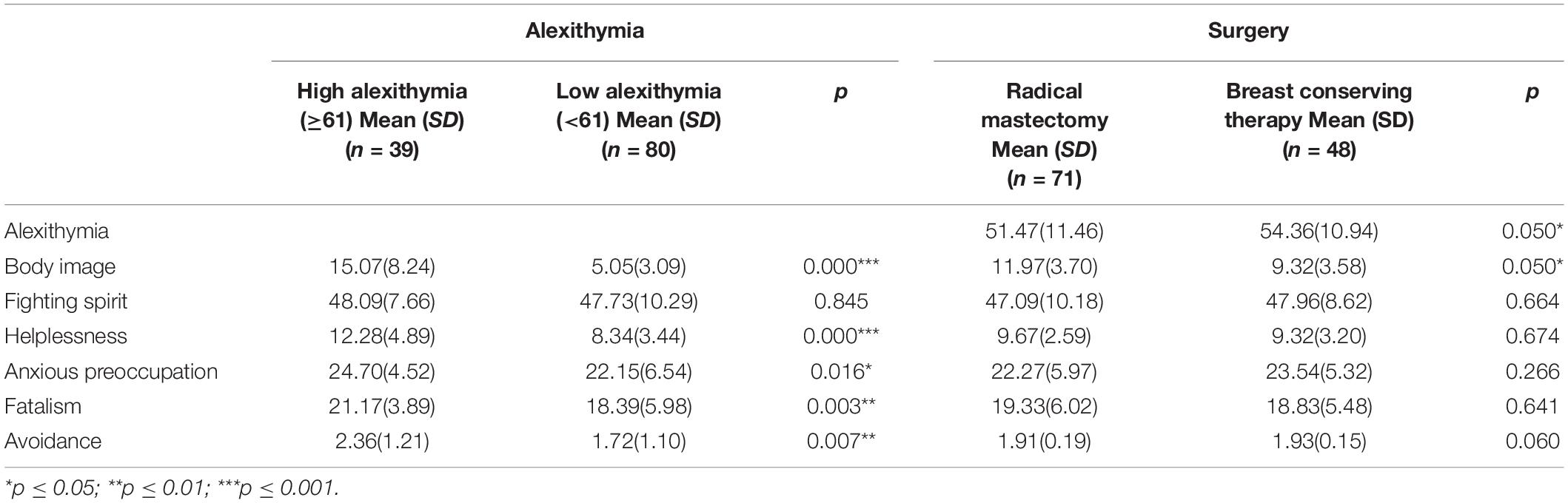
Table 1. Differences between alexithymia and surgery groups on dependent variables.
Regarding the type of surgery, women who have undergone BCT have higher alexithymia scores compared to women with a MSTR (t = −0.938, gl = 110.57) and the surgery that most affects body image is MSTR compared to BCT (t = 1.88, gl = 115.43).
Interaction Effect on Dependent Variables and the Type of Surgery in Breast Cancer Patients in Function of Alexithymia Levels
Table 2 shows the results of the factorial ANOVA for the dependent variables. As it can be seen, statistically significant differences were found in body image and all coping strategies (helplessness, anxious preoccupation, fatalism, and avoidance) except fighting spirit, in function of alexithymia as an independent factor (group). Also, significant differences were found on body image in relation to surgery and interaction effects were only significant for helplessness.
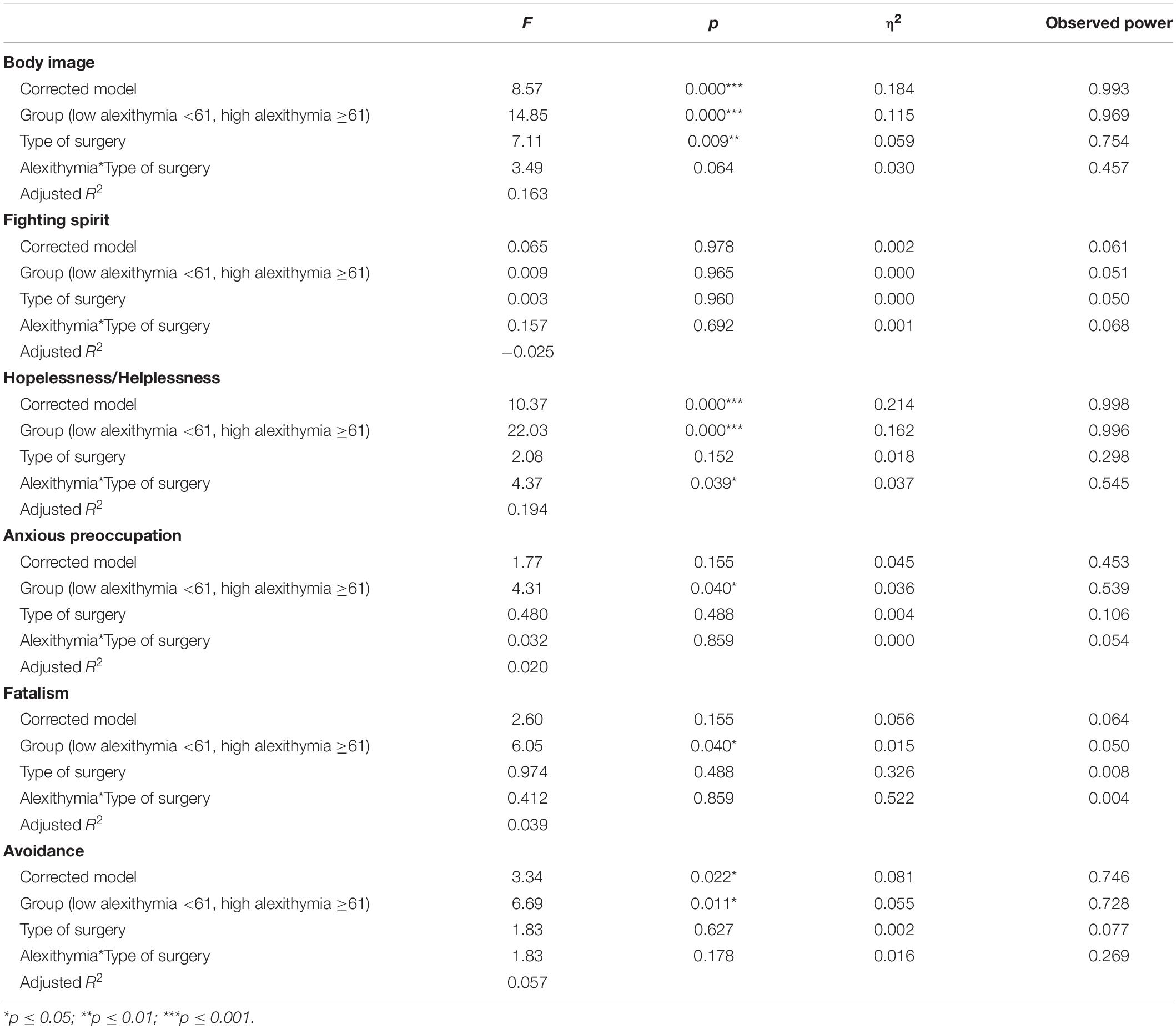
Table 2. Factorial ANOVA (2 × 2) for each dependent variable.
For body image, significant effects were found for group (p = 0.000) and type of surgery (p = 0.009), and close for the interaction effect (p = 0.064). The model explains 16.3% of the variability in body image. Table 3 shows the simple effects that compare the effects of presenting high or low alexithymia in the two types of surgery. All comparisons were made using the Bonferroni adjustment to control the type I error rate. As shown in Figure 1, women who have undergone a MSTR have higher scores for body image distortion, these scores are considerably higher in those participants who also have high alexithymia compared to women who have low alexithymia.
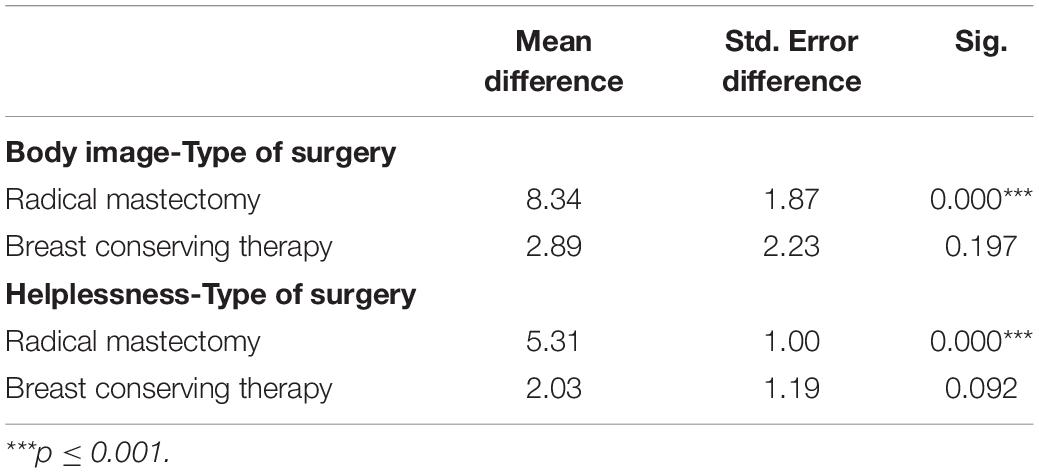
Table 3. Simple effects: comparison between high and low alexithymia groups in different type of surgery.
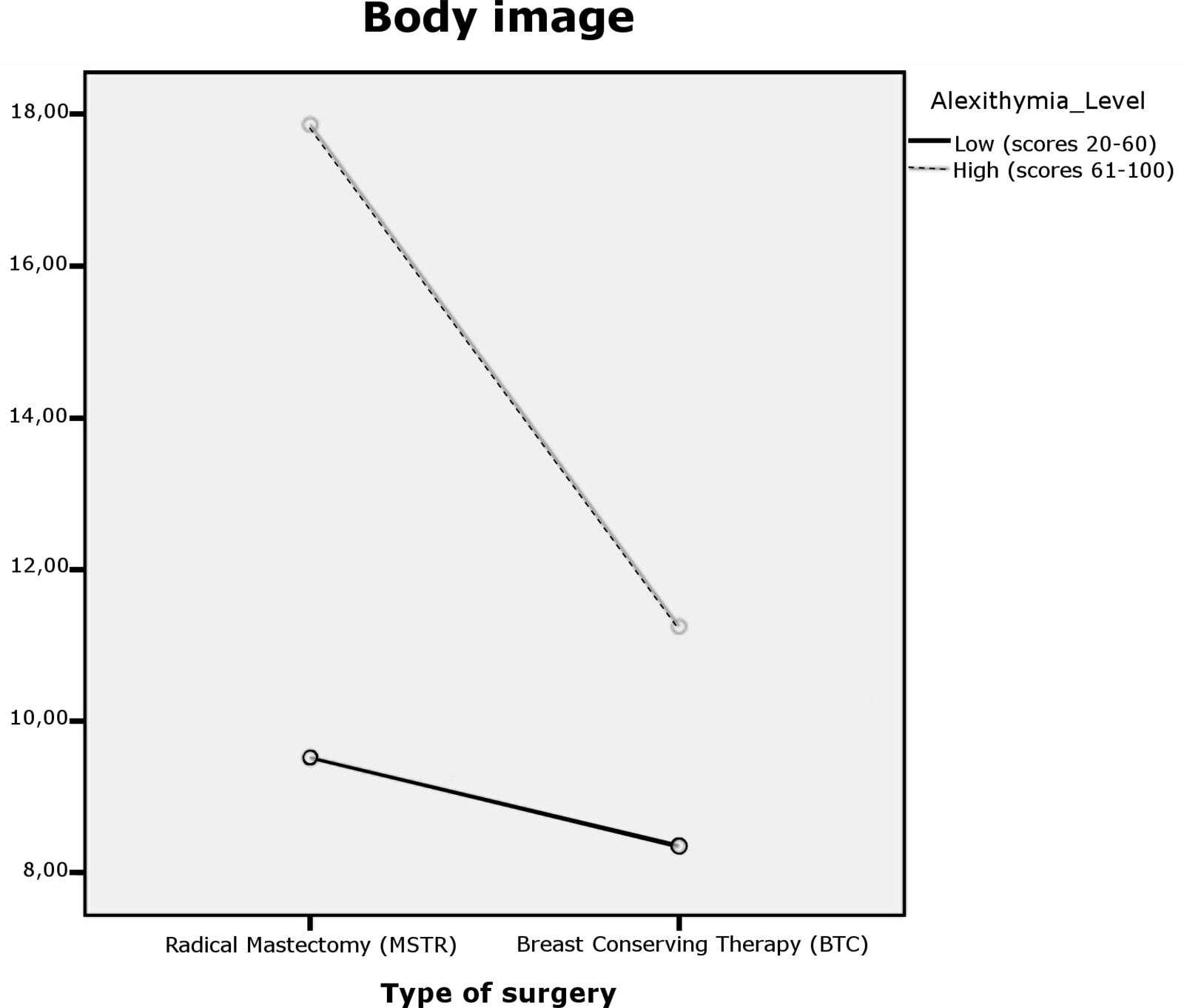
Figure 1. Dual interaction graph for body image.
For hopelessness/helplessness, the main effects were found for the group (p = 0.000) as well as the interaction effect (p = 0.039) but not for type of surgery (p = 0.152). The model explains 19.4% of the variability of helplessness. Figure 2 illustrates the results obtained. Women who have undergone a MSTR have higher scores in this coping strategy, and these scores were even higher in those participants who have high alexithymia. In addition, as shown in Table 3, the type of surgery factor indicates significant differences in helplessness for the group that has undergone MSTR (M = 9.67, SD = 2.59). These differences were analyzed employing the Bonferroni index.
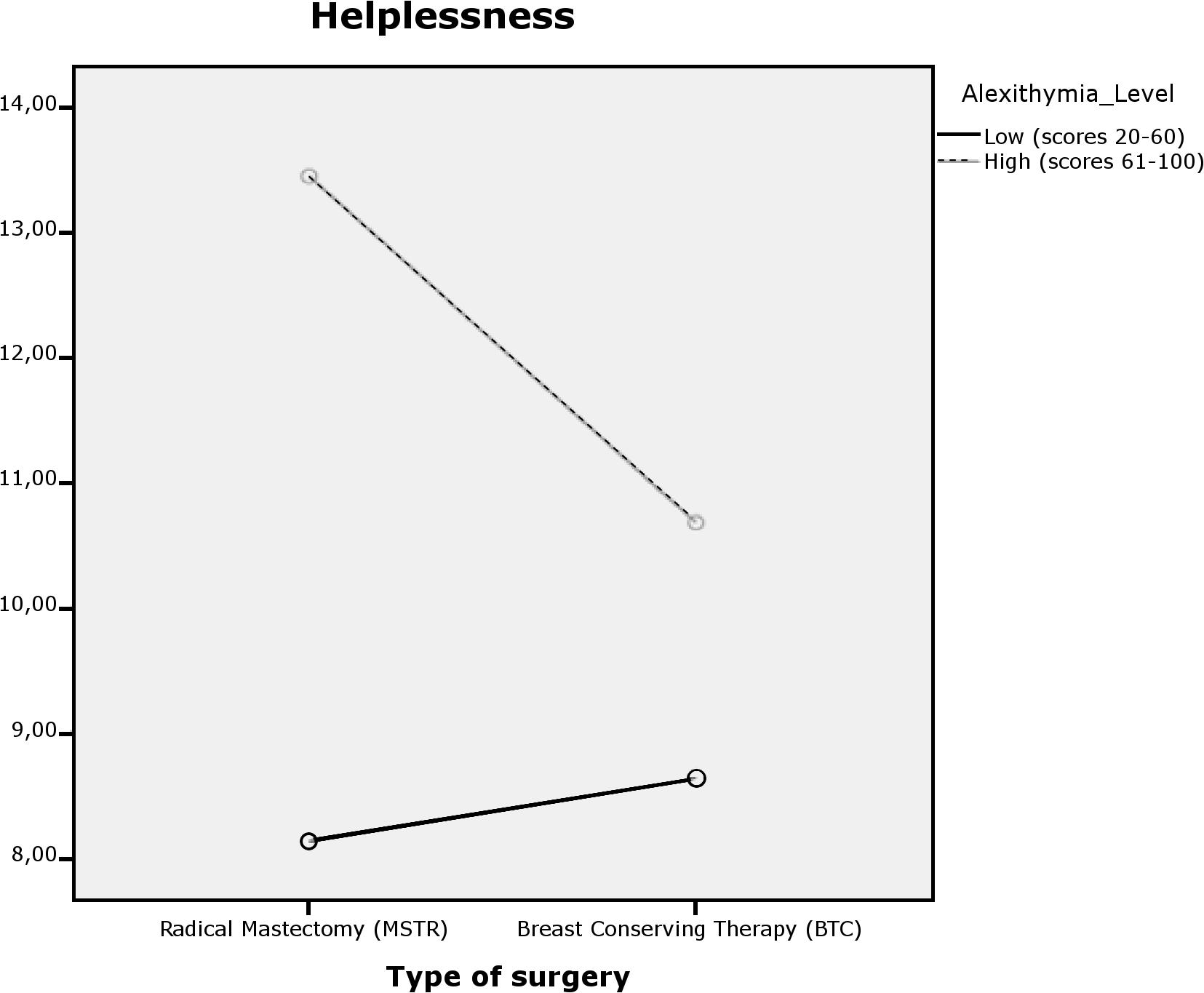
Figure 2. Dual interaction graph for helplessness.
For anxious preoccupation, only significant effects are observed for group (p = 0.040), not for type of surgery (p = 0.488) or the interaction effect (p = 0.859) (see Table 2). Thus, the significant main effect of group factor indicates differences in anxious preoccupation between women with high alexithymia (M = 24.70, SD = 4.52) and with low alexithymia (M = 22.15, SD = 6.54) (t = −2.46, gl = 100.53). When simple effects are observed, depending on the type of surgery, there are no differences in the high and low alexithymia groups.
With respect to fatalism, the differences found can be observed for group (p = 0.040) but not for type of surgery (p = 0.488) or interaction (p = 0.859) (see Table 2). The main effect of the group indicates that women with low alexithymia (M = 18.39, SD = 5.987) score lower in fatalism that women with high alexithymia (M = 21.17, SD = 3.89) (t = −3.03, gl = 104.73).
Last, for avoidance, only significant effects are observed for group (p = 0.011) but not for type of surgery (p = 0.627) or interaction effect (p = 0.178) (see Table 2). This shows that women with high alexithymia (M = 2.36, SD = 1.21) obtain higher avoidance scores than women with low alexithymia (M = 1.72, SD = 1.10) (t = −2.86, gl = 66.67).
Discussion
The main objective of this study was to explore the differences on body image and psychological adjustment on women with breast cancer with high and low alexithymia according to the surgery.
In relation to the results obtained, interaction effects were found only for the Hopelessness/Helplessness strategy. Specifically, high alexithymia and having undergone a MSTR were associated with higher levels of hopelessness. As noted above, hopelessness is a feeling that combines anxiety to achieve unattainable goals at the moment and depression due to the lack of resources to meet those goals (in this case, overcome the disease). In studies carried out with populations with chronic pain, it is observed that alexithymia is related to greater symptoms of anxiety and depression due to the reduced ability to regulate or successfully reduce negative emotions (Aaron et al., 2020). In line with these data, the interaction found between MSTR and alexithymia indicates that women undergoing mastectomies manifest greater difficulties in knowledge about their own emotions. Repression and difficulty in expressing emotions favor the use of strategies based on high levels of anxiety and depression, such as the style of coping centered on hopelessness/helplessness.
The study by Andreu et al. (2012) suggests that the suppression of emotions related to the adverse changes caused by surgery are usually a recurring short-term control strategy. It has been shown that women who have had mastectomies reported higher hopelessness scores compared to women who received BCT (Den Oudsten et al., 2009). Our results support the conclusions described by these authors and, furthermore, emphasize that the role of alexithymia is important in understanding maladjustment in coping that women with breast cancer who have undergone one type of surgery or another experience.
When analyzing coping styles, it was found that hopelessness, anxious preoccupation, fatalism and avoidance had significantly higher scores in women with high alexithymia when compared with those with low alexithymia. No significant differences were found in any of the coping styles between the two types of surgery. According to previous studies, women with breast cancer constantly remember situations that make them suffer and reflect on the negative emotions that these situations awaken in them (Baider and De−Noor, 1997). According to the transactional model of stress developed by Lazarus and Folkman (1984), the disease is perceived as a source of threat that causes negative emotional states. The inability to identify and express these emotional states can leave patients unable to effectively reduce anxiety, such as anxious preoccupation (based on high levels of anxiety), hopelessness/helplessness strategy (based on high levels of anxiety) and depression, fatalism (based on lack of acceptance of circumstances) and avoidance (based on low levels of anxiety and depression). Therefore, the coping pattern of breast cancer patients who present high alexithymia is usually considered maladaptive, since it increases the perception of threat and blocks the implementation of personal resources. In addition, it can increase suicidal ideation as indicated by previous literature on the relationship of negative emotional state with suicidal thoughts in different clinical populations (Carano et al., 2012; De Berardis et al., 2017; De Berardis et al., 2020; Serafini et al., 2020).
Regarding body image, the alexithymia-type of surgery interaction was not found to have an effect on it, although it did independently associate them both. In this sense, it is observed that the surgery affects the perception that each of the participants has about their body, being more distorted in those women who have undergone a mastectomy. However, the ignorance in the identification of the emotional state does not affect the fact that this group of participants who have undergone one or another type of surgery perceives their body image more distorted.
Studies explaining body image distortion in breast cancer patients highlight the role of surgery as a relevant variable (Moyer, 1997; Al-Ghazal et al., 2000; Jabłoński et al., 2018), since the area of the breasts is especially threatened. It is important to highlight that the chest is a part of the body closely linked to sexuality, femininity and the identity attributed to the sense of being a woman (Carver et al., 1998; Petronis et al., 2003; Moreira and Canavarro, 2010; Jabłoński et al., 2018). Body image distortion involves feeling ashamed of body changes (e.g., breast scar, weight gain, loss of function or loss of sensitivity), leading to rejection and problems in sexual intercourse (Han et al., 2010; Jabłoński et al., 2018). Other studies go a step further and specify which type of breast operation causes psychological sequelae (Moyer, 1997; Janni et al., 2001; Parker et al., 2007). Similar to our results, the authors of the previous studies have identified that, in general, patients with breast cancer tend to perceive the body distorted after surgery, the affection of body image in women undergoing an MSTR being more pronounced compared to women who have had a BCT. In line with these results, the findings of the present study confirm that high levels of alexithymia increase thoughts related to rejection toward the body in both groups. Despite the limited empirical background on the impact of alexithymia on body image, the significant effect between these two variables also supports the results of studies carried out with other clinical and non-clinical populations on the influence of alexithymia on body control. In these studies conducted with healthy populations, it is suggested that the difficulty in distinguishing emotional states reinforces the focus of attention on negative aspects of the body, which exacerbates the alterations in body image (Montebarocci et al., 2006; De Berardis et al., 2007). The results found in the participating sample support the conclusions obtained in the previous studies with other clinical populations from the general linear model.
This study has a series of limitations derived from, above all, the type of study. As it is a cross-sectional design, this prevents us from obtaining stable conclusions over time. It would be necessary to develop longitudinal studies to confirm the maintenance of these results over time. Additionally, in the collected data it’s not known if the study participants have already undergone or will undergo breast reconstruction, and it would be important to consider this data, since the psychological impact on body image and coping strategies may vary. According to the previous literature, emotional difficulty is a psychological characteristic that defines cancer population. However, there are few studies that make a comparison between healthy population and cancer population. In this study we used only the global scale to explore the role of alexithymia, future research should also explore the role of the subscales (difficulty in identifying emotions, difficulty in emotional expression, and externally oriented thinking) to identify which of them may also be influencing the distortion of body image and maladaptive coping. In relation to this study, it would be necessary to perform a similar statistical procedure that includes a healthy control group. In this way, it will be possible to confirm if the use of maladaptive strategies is common in breast cancer patients.
There are also several strengths in the present study. First, the comparison of the two types of surgery most commonly performed in early-stage breast cancer and which, as has been proven in the results, also suffer sequelae to a psychological level that prevents them from adaptively facing the disease. Alexithymia has been included in the study variables as a construct that has received little attention from clinical research, and which has been shown to interact with the type of surgical intervention. Expanding knowledge about the coping styles of women with breast cancer allows detection of threatening perceptions of the disease. Finally, the study participants have two different nationalities (Spain and Mexico), allowing the study to conclude that the difference in countries does not interfere with the psychological variables of interest. This benefits the generalization of data in Spanish-speaking populations in future studies replicating this methodology with the intention of improving the limitations found.
In conclusion, the results revealed that alexithymia, as a characteristic personality factor of the sample of participants, plays an essential role in the distortion of body image and in coping with the disease. Lack of knowledge in regulation and emotional identification has consequently the use of maladaptive coping styles. The interaction found with the type of surgery performed together with alexithymia have facilitated an in-depth knowledge of the effect of body image and helplessness and hopelessness as the most prevalent feelings in the participants. To our knowledge, there are no other studies that analyze the interaction of clinical variables such as surgery with personality variables such as alexithymia. For this reason, this study offers findings in clinical practice emphasizing the importance of attending to the emotional needs of patients, empowering by reinforcing the use of existing personal resources and incorporating new resources that benefit them in perceiving the disease as a positive challenge.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary materials, further inquiries can be directed to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by the Universidad Rey Juan Carlos and the Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
LG, LV, and SS-R conducted the evaluation of methodology, supervisions, drafting the manuscript, and revisions for important intellectual content. LG and LS performed data collection, analysis and administrative, technical, and material support. All authors of this study generated the initial research questions, developed the research protocol and defined the inclusion and exclusion criteria.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors thank all the individuals involved in the assessments of the patients included in the study. Paulina Quiroz Friedman, Itzel Alfaro Espejel, Nayeli Gómez Cervantes, Carolina Torres Urquiza, Mariana Álvarez Munguía, Joseline González Torres, Gabriela Caballero Andrade, Alejandro Angulo Domínguez, Alicia CayónMayett, Erika Noemi Gutiérrez López, Tania Tecpanecatl Ortega, Pablo Campillo Dávila, Elisabeth Berzal Pérez, Jesús Camacho López Tofiño.
Abbreviations
BCT, breast conserving therapy; MSTR, radical mastectomy.
References
Aaron, R. V., Fisher, E. A., de la Vega, R., Lumley, M. A., and Palermo, T. M. (2020). Alexithymia in individuals with chronic pain and its relation to pain intensity, physical interference, depression and anxiety: a systematic review and meta-analysis. Pain 160, 994–1006. doi: 10.1097/j.pain.000000000001487
Ahadzadeh, A. S., and Sharif, S. P. (2018). Uncertainty and quality of life in women with breast cancer: moderating role of coping styles. Cancer Nurs. 41, 484–490. doi: 10.1097/NCC.0000000000000552
Al-Ghazal, S. K., Fallowfield, L., and Blamey, R. W. (2000). Comparison of psychosocial aspects and patient satisfaction following breast conserving surgery, simple mastectomy and breast reconstruction. Eur. J. Cancer 36, 1938–1943. doi: 10.1016/s0959-8049(00)00197-0
American Cancer Society (2019). SEER, Cancer Facts & Figures. In: Surveillance, Epidemiology and End Results. Available online at: http://www.cancer.org (accesed January 20, 2020).
Andreu, Y., Galdón, M. J., Durá, E., Martínez, P., Pérez, S., and Murgui, S. (2012). A longitudinal study of psychosocial distress in breast cancer: prevalence and risk factors. Psychol. Health 27, 72–87. doi: 10.1080/08870446.2010.542814
Bagby, R. M., Parker, J. D. A., and Taylor, G. J. (1994). The twenty-item Toronto Alexithymia Scale I: item selection and cross-validation of the factor structure. J. Psychosom. Res. 38, 23–32. doi: 10.1016/0022-3999(94)9005-1
Baider, L., and De−Noor, A. (1997). Psychological distress and intrusive thoughts in cancer patients. J. Nervous Ment. Disord. 185, 346–348. doi: 10.1097/00005053-199705000-00010
Baudic, S., Jayr, C., Albi-Feldzer, A., Fermanian, J., Masselin-Dubois, A., Bouhassira, D., et al. (2016). Effect of alexithymia and emotional repression on postsurgical pain in women with breast cancer: a prospective longitudinal 12-month study. J. Pain 17, 90–100. doi: 10.1016/j.jpain.2015.10.001
Brausch, A. M., and Decker, K. M. (2014). Self-esteem and social support as moderators of depression, body image, and disordered eating for suicidal ideation in adolescents. J. Abnorm. Child Psychol. 42, 779–789. doi: 10.1007/s10802-013-9822-0
Carano, A., De Berardis, D., Campanella, D., Serroni, N., Ferri, F., Di Iorio, G., et al. (2012). Alexithymia and suicide ideation in a sample of patients with binge eating disorder. J. Psychiatr. Pract. 18, 5–11. doi: 10.1097/01.pra.0000410982.08229.99
Carver, C. S., Pozo-Kaderman, C., Price, A. A., Noriega, V., Harris, S. D., Derhagopian, R. P., et al. (1998). Concern about aspects of body image and adjustment to early stage breast cancer. Psychosom. Med. 60, 168–174. doi: 10.1097/00006842-199803000-00010
Collins, K. K., Liu, Y., Schootman, M., Aft, R., Yan, Y., Dean, G., et al. (2011). Effects of breast cancer surgery and surgical side effects on body image over time. Breast Cancer Res. Treat. 126, 167–179. doi: 10.1007/s10549-010-1077-7
De Berardis, D., Carano, A., Gambi, F., Campanella, D., Giannetti, P., Ceci, A., et al. (2007). Alexithymia and its relationships with body checking and body image in a non-clinical female sample. Eat. Behav. 8, 296–304. doi: 10.1016/j.eatbeh.2006.11.005
De Berardis, D., Fornaro, M., Orsolini, L., Valchera, A., Carano, A., Vellante, F., et al. (2017). Alexithymia and suicide risk in psychiatric disorders: a mini-review. Front. Psychiatry 8:148. doi: 10.3389/fpsyt.2017.00148
De Berardis, D., Vellante, F., Fornaro, M., Anastasia, A., Olivieri, L., Rapini, G., et al. (2020). Alexithymia, suicide ideation, affective temperaments and homocysteine levels in drug naïve patients with post-traumatic stress disorder: an exploratory study in the everyday ‘real world’ clinical practice. Int. J. Psychiatry Clin. Pract. 24, 83–87. doi: 10.1080/13651501.2019.1699575
De Vries, A. M. M., Forni, V., and Voellinger, R. (2012). Alexithymia in cancer patients: review of the literature. Psychother. Psychosom. 81, 79–86. doi: 10.1159/000330888
Den Oudsten, B. L., Van Heck, G. L., Van der Steeg, A. F. W., Roukema, J. A., and De Vries, J. (2009). Predictors of depressive symptoms 12 months after surgical treatment of early-stage breast cancer. Psychooncology 18, 1230–1237. doi: 10.1002/pon.1518
Ferrero, J., Barreto, M. P., and Toledo, M. (1994). Mental adjustment to cancer and quality of life in breast cancer patients: an exploratory study. Psychooncology 3, 223–232. doi: 10.1002/pon.2960030309
Fobair, P., and Spiegel, D. (2009). Concerns about sexuality. Cancer 15, 19–26. doi: 10.1097/PPO.0b013e31819587bb
Grassi, L., Buda, P., Cavana, L., Annunziata, M. A., Torta, R., and Varetto, A. (2005). Styles of coping with cancer: the Italian version of the mini-mental adjustment to cancer (Mini-MAC) scale. Psychooncology 14, 115–124. doi: 10.1002/pon.826
Gregorowitsch, M. L., van den Bongard, H. J. G. D., Young-Afat, D. A., Pignol, J. P., van Gils, C. H., May, A. M., et al. (2018). Severe depression more common in patients with ductal carcinoma in situ than early-stage invasive breast cancer patients. Breast Cancer Res. Treat. 167, 205–213. doi: 10.1007/s10549-017-4495-y
Gu, J., Groot, G., Boden, C., Busch, A., Holtslander, L., and Lim, H. (2018). Review of factors influencing women’s choice of mastectomy versus breast conserving therapy in early stage breast cancer: a systematic review. Clin. Breast Cancer 18, e539–e557. doi: 10.1016/j.clbc.2017.12.013
Han, J., Grothuesmann, D., Neises, M., Hille, U., and Hillemanns, P. (2010). Quality of life and satisfaction after breast cancer operation. Arch. Gynecol. Obstet. 282, 75–82. doi: 10.1007/s00404-009-1302-y
Helms, R., O’Hea, E., and Corso, M. (2008). Body image issues in women with breast cancer. Psychol. Health 13, 313–325. doi: 10.1080/13548500701405509
Hintikka, J., Honkalampi, K., Koivumaa-Honkanen, H., Antikainen, R., Tanskanen, A., Haatainen, K., et al. (2004). Alexithymia and suicidal ideation: a 12-month follow-up study in a general population. Compr. Psychiatry 45, 340–345. doi: 10.1016/j.comppsych.2004.06.008
Hoover, S., Bloom, E., and Patel, S. (2011). Review of breast conservation therapy: then and now. ISRN Oncol. 2011:617593. doi: 10.5402/2011/617593
Hopwood, C., Haviland, J., Mills, J., Sumo, G., and Bliss, J. (2007). The impact of age and clinical factors on quality of life in early breast cancer: an analysis of 2208 woman recruited to the UK START Trial (Standardisation of Breast Radiotherapy Trial). Breast 16, 241–251. doi: 10.1016/j.breast.2006.11.003
Huen, J. M., Ip, B. Y., Ho, S. M., and Yip, P. S. (2015). Hope and hopelessness: the role of hope in buffering the impact of hopelessness on suicidal ideation. PLoS One 10:e0130073. doi: 10.1371/journal.pone.0130073
Jabłoński, M. J., Streb, J., Mirucka, B., Słowik, A. J., and Jach, R. (2018). The relationship between surgical treatment (mastectomy vs breast conserving treatment) and body acceptance, manifesting femininity and experiencing an intimate relation with a partner in breast cancer patients. Psychiatr. Pol. 52, 859–872. doi: 10.1274/PP/91916
Janni, W., Rjosk, D., Dimpfl, T., Haertl, K., Strobl, B., Hepp, F., et al. (2001). Quality of life influenced by primary surgical treatment for stage I-III breast cancer: long-term follow-up of a matched-pair analysis. Ann. Surg. Oncol. 8, 542–548. doi: 10.1007/s10434-001-0542-2
Kim, J., Jang, J., Stewart, R., Kim, S., Kim, S., Kang, H., et al. (2013). Determinants of suicidal ideation in patients with breast cancer. Psychooncology 22, 2848–2856. doi: 10.1002/pon.3367
Kojima, M. (2012). Alexithymia as a prognostic risk factor for health problems: a brief review of epidemiological studies. Biopsychosoc. Med. 6:21. doi: 10.1186/1751-0759-6-21
Kvillemo, P., and Bränström, R. (2014). Coping with breast cancer: a meta-analysis. PLoS One 9:e112733. doi: 10.1371/journal.pone.0112733
Landstra, J. M. B., Ciarrochi, J., Deane, F. P., Botes, L. P., and Hillman, R. J. (2013). The psychological impact of anal cancer screening on HIV- infected men. Psychooncology 22, 614–620. doi: 10.1002/pon.3040
Luminet, O., Rokbani, L., Ogez, D., and Jadoulle, V. (2007). An evaluation of the absolute and relative stability of alexithymia in women with breast cancer. J. Psychosom. Res. 62, 641–648. doi: 10.1016/j.psychores.2007.01.003
Marrazzo, G., Sideli, L., Rizzo, R., Marinaro, A. M., Mulè, A., Marrazzo, A., et al. (2016). Quality of life, alexithymia, and defence mechanisms in patients affected by breast cancer across different stages of illness. J. Psychopathol. 22, 141–148.
Martínez-Sánchez, F. (1996). Adaptación española de la escala de Alexitimia de Toronto (TAS-20)=The Spanish versión of the Toronto Alexithymia Scale (TAS-20). Clin. Salud 7, 19–32.
Montebarocci, O., Codispoti, M., Surcinelli, P., Franzoni, E., Baldaro, B., and Rossi, N. (2006). Alexithymia in female patients with eating disorders. Eat. Weight Disord. 11, 14–21. doi: 10.1007/BF03327739
Montebarocci, O., Lo Dato, F., Baldaro, B., Morselli, P., and Rossi, N. C. (2007). Anxiety and body satisfaction before and six months after mastectomy and breast reconstruction surgery. Psyhol. Rep. 101, 100–106. doi: 10.2466/pr0.101.1.100-106
Moreira, H., and Canavarro, M. C. (2010). A longitudinal study about the body image and psychosocial adjustment of breast cancer patients during the course of the disease. Eur. J. Oncol. Nurs. 14, 263–270. doi: 10.1016/j.ejon.2010.04.001
Moyer, A. (1997). Psychosocial outcomes of breast-conserving surgery versus mastectomy: a meta-analytic review. Health Psychol. 16, 284–293. doi: 10.1037//0278-6133.16.3.284
Páez, D., Martínez-Sánchez, F., Velasco, C., Mayordomo, S., Fernández, I., and Blanco, A. (1999). Validez psicométrica de la escala de alexitimia de Toronto (TAS-20): un estudio transcultural. Bol. Psicol. 63, 55–76.
Parker, P. A., Youssef, A., Walker, S., Basen-Engquist, K., Cohen, L., Gritz, E. R., et al. (2007). Short-term psychosocial adjustment and quality of life in women undergoing different surgical procedures for breast cancer. Ann. Surg. Oncol. 14, 3078–3089. doi: 10.1245/s10434-007-9413-9
Perkins, N. M., and Brausch, A. M. (2019). Body dissatisfaction and symptoms of bulimia nervosa prospectively predict suicide ideation in adolescents. Int. J. Eat. Disord. 52, 941–949. doi: 10.1002/eat.23116
Petronis, V. M., Carver, C. S., Antoni, M. H., and Weiss, S. (2003). Investment in body image and psychosocial well-being among women treated for early stage breast cancer: partial replication and extension. Psych Health 18, 1–13. doi: 10.1080/0887044021000020941
Porcelli, P., Tulipani, C., Maiello, E., Cilenti, G., and Todarello, O. (2007). Alexithymia, coping and illness behaviour correlates of pain experience in cancer patients. Psychooncology 16, 644–650. doi: 10.1002/pon.115
Przezdziecki, A., Sherman, K., Baillie, A., Taylor, A., Foley, E., and Stalgis-Bilinski, K. (2013). My changed body: Breast cancer, body image, distress and self-compassion. Psychooncology 22, 1872–1879. doi: 10.1002/pon.3230
Puts, M. T., Tapscott, B., Fitch, M., Howell, D., Monette, J., Wan-Chow-Wah, D., et al. (2015). A systematic review of factors influencing older adults’ decision to accept or decline cancer treatment. Cancer Treat. Rev. 41, 197–215. doi: 10.1016/j.ctrv.2014.12.010
Rosenberg, M. (1965). Society and the Adolescent Self-Image. Princeton, NJ: Princeton University Press.
Saita, E., Acquati, C., and Kayser, K. (2015). Coping with early stage breast cancer: examining the influence of personality traits and interpersonal closeness. Front. Psychol. 6:88. doi: 10.3389/fpsyg.2015.00088
Sarwer, D., and Cash, T. (2008). Body image: interfacing behavioral and medical sciences. Aesthet. Surg. J. 28, 357–358. doi: 10.1016/j.asj.2008.03.007
Sebastián, J., Manos, D., Bueno, M. J., and Mateos, N. (2007). Imagen corporal y autoestima en mujeres con cáncer de mama participantes en un programa de intervención psicosocial. Clin. Salud 18, 137–161.
Serafini, G., De Berardis, D., Valchera, A., Canepa, G., Geoffroy, P. A., Pompili, M., et al. (2020). Alexithymia as a possible specifier of adverse outcomes: clinical correlates in euthymic unipolar individuals. J. Affect. Disord. 15, 428–436. doi: 10.1016/j.jad.2019.10.046
Sheehan, J., Sherman, K., Lam, T., and Boyages, J. (2007). Association of information satisfaction, psychological distress and monitoring coping style with post-decision regret following breast cancer reconstruction. Psychooncology 16, 342–351. doi: 10.1002/pon.1067
Taylor, G. J., and Bagby, R. M. (2012). “The alexithymia personality dimension,” in The Oxford Handbook of Personality Disorders, ed. T. A. Widiger (New York, NY: Oxford University Press), 648–673.
Turkington, C., and Krag, K. (2005). The Encyclopaedia of Breast Cancer. New York, NY: Facts On File.
Ursaru, M., Crumpei, I., and Crumpei, G. (2014). Quality of life and religious coping in women with breast cancer. Proced. Soc. Behav. Sci. 114, 322–326. doi: 10.1016/j.sbspro.2013.12.705
Velasco, L., Gutiérrez Hermoso, L., Alcocer Castillejos, N., Quiroz Friedman, P., Peñacoba, C., Catalá, P., et al. (2020). Association between quality of life and positive coping strategies in breast cancer patients. Women Health 60, 1063–1069. doi: 10.1080/03630242.2020.1802398
Keywords: breast cancer, body image, coping strategies, psychological adjustment, alexithymia
Citation: Gutiérrez Hermoso L, Velasco Furlong L, Sánchez-Román S and Salas Costumero L (2020) The Importance of Alexithymia in Post-surgery. Differences on Body Image and Psychological Adjustment in Breast Cancer Patients. Front. Psychol. 11:604004. doi: 10.3389/fpsyg.2020.604004
Received: 08 September 2020; Accepted: 30 November 2020;
Published: 18 December 2020.
Edited by:
Marina Prista Guerra, University of Porto, PortugalReviewed by:
Domenico De Berardis, Azienda Usl Teramo, ItalyFrancisco Javier Cano-García, University of Seville, Spain
Copyright © 2020 Gutiérrez Hermoso, Velasco Furlong, Sánchez-Román and Salas Costumero. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lilian Velasco Furlong, bGlsaWFuLnZlbGFzY29AdXJqYy5lcw==